
Alterations in resting-state regional cerebral blood flow demonstrate ongoing pain in...
11
ARTHRITIS & RHEUMATISM Vol. 64, No. 12, December 2012, pp 3936–3946 DOI 10.1002/art.37685 © 2012, American College of Rheumatology Alterations in Resting-State Regional Cerebral Blood Flow Demonstrate Ongoing Pain in Osteoarthritis An Arterial Spin-Labeled Magnetic Resonance Imaging Study Matthew A. Howard, 1 Duncan Sanders, 1 Kristina Krause, 1 Jonathan O’Muircheartaigh, 1 Aikaterini Fotopoulou, 1 Fernando Zelaya, 1 Michael Thacker, 1 Nathalie Massat, 2 John P. Huggins, 2 William Vennart, 2 Ernest Choy, 3 Maxine Daniels, 1 and Steven C. R. Williams 1 Objective. Increasing evidence suggests a central nervous system (CNS) component underpinning persis- tent pain disease states. This study was undertaken to determine regional cerebral blood flow (rCBF) changes representing ongoing pain experienced by patients with painful osteoarthritis (OA) of the carpometacarpal (CMC) joint and to examine rCBF variability across sessions. We used pulsed continuous arterial spin label- ing (pCASL), a perfusion magnetic resonance imaging (MRI) technique. Methods. The study included 16 patients with CMC OA and 17 matched controls. Two pCASL scans and numerical rating scale (NRS) estimates of ongoing pain were acquired in each of two identical sessions. Voxelwise general linear model analyses were performed to determine rCBF differences between OA and control groups, rCBF differences between sessions within each group, and whether sessionwise rCBF differences were related to variability in perceived ongoing pain. Results. In the OA group, rCBF increases repre- senting ongoing pain were identified in the primary and secondary somatosensory, insula, and cingulate corti- ces; thalamus; amygdala; hippocampus; and dorsal midbrain/pontine tegmentum, including the periaque- ductal gray/nucleus cuneiformis. Sessionwise rCBF dif- ferences in the OA group in the postcentral, rostral/ subgenual cingulate, mid/anterior insula, prefrontal, and premotor cortices were related to changes in per- ceived ongoing pain. No significant sessionwise rCBF differences were observed in controls. Conclusion. This is the first quantitative endoge- nous perfusion MRI study of the cerebral representa- tion of ongoing, persistent pain due to OA. Observed rCBF changes potentially indicate dysregulated CNS appraisal and modulation of pain, most likely the maladaptive neuroplastic sequelae of living with painful OA. Understanding the neural basis of ongoing pain is likely to be important in developing novel treatment strategies. Persistent pain is a major health care problem. As many as 100 million people in Europe alone experience an intractable, ongoing malaise that affects quality of life, places an increasing burden on health care re- sources, and costs the economy in excess of €50 billion every year (1). While multidisciplinary pain manage- ment strategies help patients cope (2), there is a recog- nized, unmet need for the development of novel, more Supported by Pfizer Global Research and Development, UK. Dr. Howard, Mr. Sanders, and Ms Krause’s work was supported by a grant from Pfizer Global Research and Development, UK to King’s College London. 1 Matthew A. Howard, PhD, Duncan Sanders, MSc Med, Kristina Krause, Dipl Psych, MA, Jonathan O’Muircheartaigh, PhD, Aikaterini Fotopoulou, PhD, Fernando Zelaya, PhD, Michael Thacker, PhD, Maxine Daniels, Steven C. R. Williams, PhD: King’s College London, London, UK; 2 Nathalie Massat, PhD, John P. Huggins, PhD, William Vennart, PhD: Pfizer Global Research and Development, Sandwich, UK; 3 Ernest Choy, MD, FRCP: Cardiff University, Cardiff, UK. Drs. Huggins and Vennart own stock or stock options in Pfizer. Dr. Huggins has received consulting fees from Pfizer (more than $10,000). Dr. Choy has received consulting fees, speaking fees, and/or honoraria from Pfizer (less than $10,000). Address correspondence to Matthew A. Howard, PhD, King’s College London, Institute of Psychiatry, Centre for Neuroimaging Sciences, Box 89, De Crespigny Park, London SE5 8AF, UK. E-mail: [email protected]. Submitted for publication August 19, 2011; accepted in revised form August 23, 2012. 3936
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Alterations in resting-state regional cerebral blood flow demonstrate ongoing pain in...
ARTHRITIS & RHEUMATISMVol. 64, No. 12, December 2012, pp 3936–3946DOI 10.1002/art.37685© 2012, American College of Rheumatology
Alterations in Resting-State Regional Cerebral Blood FlowDemonstrate Ongoing Pain in Osteoarthritis
An Arterial Spin-Labeled Magnetic Resonance Imaging Study
Matthew A. Howard,1 Duncan Sanders,1 Kristina Krause,1 Jonathan O’Muircheartaigh,1
Aikaterini Fotopoulou,1 Fernando Zelaya,1 Michael Thacker,1
Nathalie Massat,2 John P. Huggins,2 William Vennart,2
Ernest Choy,3 Maxine Daniels,1 and Steven C. R. Williams1
Objective. Increasing evidence suggests a centralnervous system (CNS) component underpinning persis-tent pain disease states. This study was undertaken todetermine regional cerebral blood flow (rCBF) changesrepresenting ongoing pain experienced by patients withpainful osteoarthritis (OA) of the carpometacarpal(CMC) joint and to examine rCBF variability acrosssessions. We used pulsed continuous arterial spin label-ing (pCASL), a perfusion magnetic resonance imaging(MRI) technique.
Methods. The study included 16 patients withCMC OA and 17 matched controls. Two pCASL scansand numerical rating scale (NRS) estimates of ongoingpain were acquired in each of two identical sessions.Voxelwise general linear model analyses were performed
to determine rCBF differences between OA and controlgroups, rCBF differences between sessions within eachgroup, and whether sessionwise rCBF differences wererelated to variability in perceived ongoing pain.
Results. In the OA group, rCBF increases repre-senting ongoing pain were identified in the primary andsecondary somatosensory, insula, and cingulate corti-ces; thalamus; amygdala; hippocampus; and dorsalmidbrain/pontine tegmentum, including the periaque-ductal gray/nucleus cuneiformis. Sessionwise rCBF dif-ferences in the OA group in the postcentral, rostral/subgenual cingulate, mid/anterior insula, prefrontal,and premotor cortices were related to changes in per-ceived ongoing pain. No significant sessionwise rCBFdifferences were observed in controls.
Conclusion. This is the first quantitative endoge-nous perfusion MRI study of the cerebral representa-tion of ongoing, persistent pain due to OA. ObservedrCBF changes potentially indicate dysregulated CNSappraisal and modulation of pain, most likely themaladaptive neuroplastic sequelae of living with painfulOA. Understanding the neural basis of ongoing pain islikely to be important in developing novel treatmentstrategies.
Persistent pain is a major health care problem. Asmany as 100 million people in Europe alone experiencean intractable, ongoing malaise that affects quality oflife, places an increasing burden on health care re-sources, and costs the economy in excess of €50 billionevery year (1). While multidisciplinary pain manage-ment strategies help patients cope (2), there is a recog-nized, unmet need for the development of novel, more
Supported by Pfizer Global Research and Development, UK.Dr. Howard, Mr. Sanders, and Ms Krause’s work was supported by agrant from Pfizer Global Research and Development, UK to King’sCollege London.
1Matthew A. Howard, PhD, Duncan Sanders, MSc Med,Kristina Krause, Dipl Psych, MA, Jonathan O’Muircheartaigh, PhD,Aikaterini Fotopoulou, PhD, Fernando Zelaya, PhD, MichaelThacker, PhD, Maxine Daniels, Steven C. R. Williams, PhD:King’s College London, London, UK; 2Nathalie Massat, PhD, John P.Huggins, PhD, William Vennart, PhD: Pfizer Global Research andDevelopment, Sandwich, UK; 3Ernest Choy, MD, FRCP: CardiffUniversity, Cardiff, UK.
Drs. Huggins and Vennart own stock or stock options inPfizer. Dr. Huggins has received consulting fees from Pfizer (morethan $10,000). Dr. Choy has received consulting fees, speaking fees,and/or honoraria from Pfizer (less than $10,000).
Address correspondence to Matthew A. Howard, PhD, King’sCollege London, Institute of Psychiatry, Centre for NeuroimagingSciences, Box 89, De Crespigny Park, London SE5 8AF, UK. E-mail:[email protected].
Submitted for publication August 19, 2011; accepted inrevised form August 23, 2012.
3936

efficacious treatments of persistent pain (3). In theabsence of a recordable biologic marker, patients’ self-reports have been relied upon uniquely to quantify boththe pain experience and treatment responses; the diffi-culties of this approach are compounded by interindi-vidual differences in reporting (4). Novel indices for painmeasurement are required, ideally ones that relate to anunderlying aspect of pain transduction, take biopsycho-social factors into account, and translate between pre-clinical and human studies (4,5).
Neuroimaging techniques, such as functionalmagnetic resonance imaging (fMRI) and positron emis-sion tomography (PET), have shown promise in painresearch, enabling noninvasive investigation of the cere-bral underpinnings of pain (6–8). Studies to date haveadded to our knowledge of the central representation ofpain as a distributed network of brain regions underpin-ning the sensory–discriminative, cognitive–evaluative,and affective–motivational features of pain (5). Untilrecently, many have focused primarily on eliciting cere-bral responses to repeated, evoked painful stimuli inhealthy volunteers (9). For ethical reasons, these studiesare constrained to painful stimuli that do not inducelasting tissue damage; as such, functional, biochemical,and structural alterations now known to occur during thedevelopment of persistent pain states are challenging torepresent in healthy volunteers (10).
Recent studies have focused on understandingdisease-specific representations of individual persistentpain states themselves (for review, see refs. 6 and 9).However, with few exceptions (for example, refs. 11 and12), most studies have examined responses to evokedstimulation in patient groups, rather than the repre-sentation of ongoing pain experienced in all chronicpain disease states. This is most likely due to technicalconstraints; conventional “evoked-response” blood oxy-genation level–dependent (BOLD) fMRI techniquesare best suited to the comparison of repeated, rapidlychanging stimuli over the course of seconds, rather thanlonger periods, as may be required in monitoring long-term treatment effects (13). Resting-state fMRI evalu-ates temporal synchrony across brain regions, and recentreports have indicated sensitivity to persistent paindisease states (11,12). However, all BOLD fMRI mea-surements suffer from signal losses and distortions inbrain regions close to air/bone/tissue interfaces. WhileH2
15O PET does not have these constraints, its impact inpain research has been limited by comparatively poorspatial resolution, expense, availability, and safety con-cerns regarding repeated radiotracer administration(6,7). In contrast, arterial spin labeling (ASL), a perfu-
sion MRI technique, provides quantitative, reproduciblewhole-brain measures of regional cerebral blood flow(rCBF) without the need for exogenous tracers and witha spatial resolution superior to PET (14). The use ofASL remains comparatively novel in pain research, butresults from our laboratory and elsewhere have recentlyshown that ASL has suitable characteristics for the studyof both clinical (15,16) and experimental phasic andtonic pain (17–19).
In this study, we applied pulsed continuous ASL(pCASL) (14) to the challenge of describing the cerebralrepresentation of ongoing pain in participants withpainful osteoarthritis (OA) of the carpometacarpal(CMC) joint of the thumb. OA is one of the mostpredominant causes of persistent pain in the Westernworld (1). While traditionally considered to be relatedonly to biomechanical damage of synovial joints andassociated tissue (20), recent evidence suggests a sig-nificant central nervous system (CNS) component inmaintaining the recurrent bouts of ongoing pain char-acteristic of the disease (21,22). Despite the prevalenceof OA, there remain relatively few neuroimaging re-ports of systems-level alterations in participants with OA(22–26).
We sought to demonstrate changes in rCBFrepresenting ongoing pain in patients with CMC OAcompared to age- and sex-matched controls. We hypoth-esized that there would be rCBF differences betweenOA and control groups in a network of brain regionsspecified a priori to underpin the experience of pain,based on previous studies of the cerebral representationof pain (6,8,9). Our second aim was to examine thereproducibility of pCASL-derived rCBF in both OA andcontrol groups. We hypothesized that between-sessionrCBF differences in OA participants would relate tovariation in their perceived ongoing pain, whereas pain-free controls would not demonstrate significant session-to-session rCBF differences.
PATIENTS AND METHODS
Subjects and materials. Twenty-four right-handedpostmenopausal female participants (with a mean age of 60.8years) who fulfilled the American College of Rheumatologycriteria for CMC OA (27) in their dominant (right) hand and20 age- and sex-matched controls (with a mean age of 64.7years) participated. Informed consent was obtained from allsubjects. Ethical approval for the study was granted by the localNHS research ethics committee (Ref 07/H0807/69). All pa-tients with OA reported an average estimate of ongoing pain atrest during the week prior to screening of �3 on a numericalrating scale (NRS) of 0–10. All participants were required toremain on a stable drug regimen throughout the course of the
EVALUATION OF ONGOING PAIN IN HAND OA USING PERFUSION MRI 3937

study. Additional use of acetaminophen (up to a maximumdaily dose of 4 gm) was permitted except during the 24 hoursprior to each visit. Eight OA patients and 3 control subjectswere excluded due to claustrophobia, image artifacts, develop-ment of pain in other body sites, or use of analgesic medicationother than the stable drug regimen. Rescue medication wasavailable to all participants upon request.
Study design and procedure. The study consisted of2 identical sessions, separated by a minimum of 7 days and amaximum of 21 days. Each session involved a screeningand familiarization stage prior to MRI. During screening, allparticipants underwent a detailed examination by a specialistclinician to assess for the presence and severity of CMC OA.Questionnaires were administered to assess pain and psycho-logical status, as described below. Participants were introducedto a simulated mock scanning environment before their “real”MRI examination to minimize anxiety and familiarize themwith the requirements of the imaging environment. Each MRIexamination comprised acquisition of high-resolution ana-tomic images and 2 pCASL scans. Each of the pCASL scanslasted 6 minutes, spaced 20 minutes apart. The maximumsession duration was �1 hour.
Baseline psychometry. Screening assessments wereperformed for all participants. Subjects were screened fordepression using the Beck Depression Inventory II (PearsonAssessments) and for anxiety using the State-Trait AnxietyQuestionnaire (MindGarden). State anxiety was assessed priorto both sessions. Additional estimates of ongoing hand pain, onan NRS of 0 (no pain) to 10 (worst pain imaginable), wererecorded at the beginning and end of each session in eachgroup.
Imaging procedure. Imaging was performed on a 3TSigna HDx whole-body MRI scanner (General Electric) fittedwith an 8-channel, phased-array receive-only head coil. High-resolution T1- and T2-weighted images were acquired forradiologic assessment and image registration. Resting-staterCBF measurements were made using pCASL (14), with anirradiation time of 1.5 seconds and postlabeling delay of 1.5seconds. The pCASL images were acquired using a single-shot,fast spin-echo (3D-FSE) spiral multislice readout resulting inwhole-brain blood flow maps. Scanning parameters were asfollows: time to echo 32 msec, repetition time 5,500 msec; echotrain length 64, matrix size 48 � 64 � 60, field of view 18 �24 � 18 cm, and number of excitations 3. Full details of thepCASL sequence are available online at http://www.kcl.ac.uk/iop/depts/neuroimaging/research/pain/pCASLdetail.pdf.
Image preprocessing. Preprocessing was performedusing FSL software version 4.1.5 (http://www.fmrib.ox.ac.uk/fsl) and statistical parametric mapping software (SPM5; http://www.fil.ion.ucl.ac.uk/spm). Preprocessing consisted of skullstripping (FSL-BET), normalization to the Montreal Neuro-logical Institute (MNI) template (SPM-NORMALIZE), andspatial smoothing (FSL-SUSAN: � � 8 mm full-width half-maximum). The pCASL data were masked to include graymatter voxels only. Probabilistic gray matter images in MNIspace, derived from the FSL voxel-based morphometry tool-box, were thresholded to produce a mask which included allvoxels from all subjects with a �20% likelihood of being graymatter. A global CBF value, defined as the mean of all graymatter voxels within the mask, was computed for each individ-ual pCASL CBF map in each subject.
Analysis of demographic data, psychometric data, andNRS pain scores. Demographic, psychometric, and pain scoredata were analyzed using SPSS version 18.0 (http://www.spss.com). Between-group differences in age, state and traitanxiety, depression, and coping strategies were assessed usingindependent-groups t-tests. Groupwise differences in averageNRS pain scores were assessed using a Mann-Whitney U test.Intrasubject and intersession differences in NRS estimates ofpain in the OA group were examined using a paired t-test.
Global CBF analysis. A general linear mixed-effectsmodel, with subject and subject-by-session as random effects,and group, session, and time point as a 3-way factorial, wasfitted to the global CBF data using SAS version 9.1.3 (http://www.sas.com) to assess differences in CBF global mean withinand between diagnostic groups, between sessions, and betweenscans within sessions.
Analysis of pCASL data. The pCASL data were ana-lyzed using a voxelwise optimized general linear model (FSL-
Table 1. Demographic characteristics, NRS estimates of ongoingpain, and psychometric variables in the OA and control groups*
Mean t(df)
AgeControl 64.17 1.07 (31)CMC OA 60.87
NRS ongoing painControl 0 NACMC OA 3.65
NRS ongoing painCMC OA session 1 3.15 2.92 (15)†CMC OA session 2 4.15
State anxiety (session 1)Control 43.41 �0.18 (31)CMC OA 44.06
State anxiety (session 2)Control 39.47 �0.48 (31)CMC OA 41.56
Trait anxietyControl 42.47 �0.97 (31)CMC OA 46.00
Depression per BDI (session 1)Control 4.24 �0.88 (30)CMC OA 6.20
Depression per BDI (session 2)Control 4.00 �0.36 (31)CMC OA 4.75
CCSI-R distractionControl 1.99 0.71 (30)CMC OA 1.79
CCSI-R catastrophizingControl 1.44 0.04 (30)CMC OA 1.44
CCSI-R copingControl 2.23 �0.11 (30)CMC OA 2.26
* Results of between-group and within-group statistical comparisons,as appropriate, are shown. The control group included 17 subjects, andthe carpometacarpal (CMC) osteoarthritis (OA) patient group in-cluded 16 subjects. NRS � numerical rating scale; NA � not applica-ble; BDI � Beck Depression Inventory; CCSI-R � Cognitive CopingStrategies Inventory-Revised.† 2-tailed P � 0.01.
3938 HOWARD ET AL
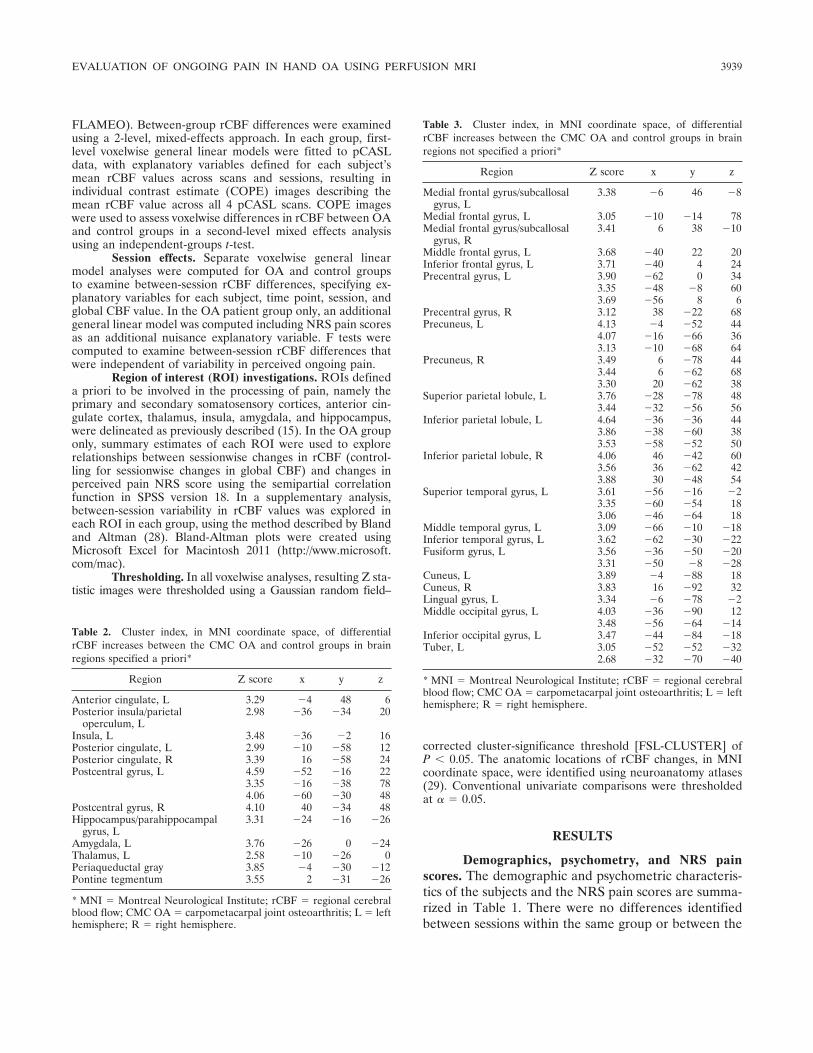
FLAMEO). Between-group rCBF differences were examinedusing a 2-level, mixed-effects approach. In each group, first-level voxelwise general linear models were fitted to pCASLdata, with explanatory variables defined for each subject’smean rCBF values across scans and sessions, resulting inindividual contrast estimate (COPE) images describing themean rCBF value across all 4 pCASL scans. COPE imageswere used to assess voxelwise differences in rCBF between OAand control groups in a second-level mixed effects analysisusing an independent-groups t-test.
Session effects. Separate voxelwise general linearmodel analyses were computed for OA and control groupsto examine between-session rCBF differences, specifying ex-planatory variables for each subject, time point, session, andglobal CBF value. In the OA patient group only, an additionalgeneral linear model was computed including NRS pain scoresas an additional nuisance explanatory variable. F tests werecomputed to examine between-session rCBF differences thatwere independent of variability in perceived ongoing pain.
Region of interest (ROI) investigations. ROIs defineda priori to be involved in the processing of pain, namely theprimary and secondary somatosensory cortices, anterior cin-gulate cortex, thalamus, insula, amygdala, and hippocampus,were delineated as previously described (15). In the OA grouponly, summary estimates of each ROI were used to explorerelationships between sessionwise changes in rCBF (control-ling for sessionwise changes in global CBF) and changes inperceived pain NRS score using the semipartial correlationfunction in SPSS version 18. In a supplementary analysis,between-session variability in rCBF values was explored ineach ROI in each group, using the method described by Blandand Altman (28). Bland-Altman plots were created usingMicrosoft Excel for Macintosh 2011 (http://www.microsoft.com/mac).
Thresholding. In all voxelwise analyses, resulting Z sta-tistic images were thresholded using a Gaussian random field–
corrected cluster-significance threshold [FSL-CLUSTER] ofP � 0.05. The anatomic locations of rCBF changes, in MNIcoordinate space, were identified using neuroanatomy atlases(29). Conventional univariate comparisons were thresholdedat � � 0.05.
RESULTS
Demographics, psychometry, and NRS painscores. The demographic and psychometric characteris-tics of the subjects and the NRS pain scores are summa-rized in Table 1. There were no differences identifiedbetween sessions within the same group or between the
Table 2. Cluster index, in MNI coordinate space, of differentialrCBF increases between the CMC OA and control groups in brainregions specified a priori*
Region Z score x y z
Anterior cingulate, L 3.29 �4 48 6Posterior insula/parietal
operculum, L2.98 �36 �34 20
Insula, L 3.48 �36 �2 16Posterior cingulate, L 2.99 �10 �58 12Posterior cingulate, R 3.39 16 �58 24Postcentral gyrus, L 4.59 �52 �16 22
3.35 �16 �38 784.06 �60 �30 48
Postcentral gyrus, R 4.10 40 �34 48Hippocampus/parahippocampal
gyrus, L3.31 �24 �16 �26
Amygdala, L 3.76 �26 0 �24Thalamus, L 2.58 �10 �26 0Periaqueductal gray 3.85 �4 �30 �12Pontine tegmentum 3.55 2 �31 �26
* MNI � Montreal Neurological Institute; rCBF � regional cerebralblood flow; CMC OA � carpometacarpal joint osteoarthritis; L � lefthemisphere; R � right hemisphere.
Table 3. Cluster index, in MNI coordinate space, of differentialrCBF increases between the CMC OA and control groups in brainregions not specified a priori*
Region Z score x y z
Medial frontal gyrus/subcallosalgyrus, L
3.38 �6 46 �8
Medial frontal gyrus, L 3.05 �10 �14 78Medial frontal gyrus/subcallosal
gyrus, R3.41 6 38 �10
Middle frontal gyrus, L 3.68 �40 22 20Inferior frontal gyrus, L 3.71 �40 4 24Precentral gyrus, L 3.90 �62 0 34
3.35 �48 �8 603.69 �56 8 6
Precentral gyrus, R 3.12 38 �22 68Precuneus, L 4.13 �4 �52 44
4.07 �16 �66 363.13 �10 �68 64
Precuneus, R 3.49 6 �78 443.44 6 �62 683.30 20 �62 38
Superior parietal lobule, L 3.76 �28 �78 483.44 �32 �56 56
Inferior parietal lobule, L 4.64 �36 �36 443.86 �38 �60 383.53 �58 �52 50
Inferior parietal lobule, R 4.06 46 �42 603.56 36 �62 423.88 30 �48 54
Superior temporal gyrus, L 3.61 �56 �16 �23.35 �60 �54 183.06 �46 �64 18
Middle temporal gyrus, L 3.09 �66 �10 �18Inferior temporal gyrus, L 3.62 �62 �30 �22Fusiform gyrus, L 3.56 �36 �50 �20
3.31 �50 �8 �28Cuneus, L 3.89 �4 �88 18Cuneus, R 3.83 16 �92 32Lingual gyrus, L 3.34 �6 �78 �2Middle occipital gyrus, L 4.03 �36 �90 12
3.48 �56 �64 �14Inferior occipital gyrus, L 3.47 �44 �84 �18Tuber, L 3.05 �52 �52 �32
2.68 �32 �70 �40
* MNI � Montreal Neurological Institute; rCBF � regional cerebralblood flow; CMC OA � carpometacarpal joint osteoarthritis; L � lefthemisphere; R � right hemisphere.
EVALUATION OF ONGOING PAIN IN HAND OA USING PERFUSION MRI 3939

OA and control groups with regard to age, state or traitanxiety, or depression score. Groups differed signifi-cantly in NRS estimates of ongoing pain (Z � �5.105,P � 0.001 by Mann-Whitney U test) (mean NRS acrosssessions 0 in controls and 3.65 in OA patients). Session-wise NRS scores in the OA group were significantlyhigher in session 2 (mean � SD 4.15 � 2.21) than insession 1 (mean � SD 3.15 � 1.84) (t[15] � 2.916, P �0.011 by paired t-test).
Mean global CBF. Mean global CBF did notdiffer between the OA and control groups (mean 50.20in controls and 52.84 in OA patients; standard error of
between-group difference 2.21; P � 0.22) and there wasno main effect of session across the 2 groups (P � 0.39).
Groupwise rCBF differences. A distributed net-work of brain regions demonstrated local increases inCBF in participants with CMC OA compared tomatched controls. Tables 2 and 3 detail the anatomiclocations and Z score statistics for cluster maximaindicating relative rCBF increases in the OA group, inbrain regions specified a priori and those not specified apriori, respectively. There were no increases in rCBFidentified in the control group compared to the OAgroup.
Figure 1. Local increases in regional cerebral blood flow in patients with osteoarthritis of the carpometacarpal joint compared to controls. a–c, Axialsections of the dorsal pontine tegmentum (a), periaqueductal gray/nucleus cuneiformis (b), and ventral thalamus (c). d–f, Coronal sections of thebilateral primary somatosensory cortex and contralateral secondary somatosensory cortex (d), hippocampus/parahippocampal gyrus (e), andamygdala (f). g–i, Sagittal sections of the subgenual cingulate/medial orbital frontal cortex (g), posterior and mid insula cortex (h), andperiaqueductal gray/dorsal pontine tegmentum (i).
3940 HOWARD ET AL

In the OA group, several clusters of increasedrCBF were identified in brain regions specified a priorito be associated with the processing of pain (Figure 1).Bilateral clusters were identified in the postcentralgyrus, corresponding to the somatotopic representationof the hand in the primary somatosensory cortex, andthe caudal inferior parietal lobule. In the left hemi-sphere only, increases in rCBF extended into the rostralsuperior parietal lobule and ventrally to the secondarysomatosensory cortex, including the parietal operculum,the dorsalmost aspect of the posterior insula, and amid-insula region proximal to the central sulcus of theinsula.
Further rCBF increases in the OA group wereobserved in the left hemisphere rostral anterior cingu-late cortex, extending ventrally into the subcallosalgyrus and the orbital portion of the medial frontal gyrus.An additional cluster was observed in the posteriorcingulate cortex, dorsal to the splenium, extending pos-teriorly into precuneus bilaterally. In the left hemispheretemporal lobe, rCBF increases in the OA group wereidentified in the amygdala, hippocampal head, and sur-rounding entorhinal/parahippocampal cortices. In-creases in rCBF in the thalamus were confined to the lefthemisphere only, approximating to the ventral posteriornuclei. Increases in rCBF in the ventral posterior formedthe anterior tip of a midline cluster that descended intothe dorsalmost aspect of the midbrain tegmentum, peri-aqueductal gray, and nucleus cuneiformis, terminatingproximal to the floor of the fourth ventricle in the dorsalpontine tegmentum.
Several additional increases in rCBF were ob-served in brain regions not specified a priori. Theseregions were the left hemisphere middle and inferiorfrontal gyri and precentral gyrus bilaterally; the superior,middle, inferior-temporal, and fusiform gyri; and themedial and lateral occipital cortex, cerebellar vermis,and lateral-anterior cerebellar lobes bilaterally.
Assessment of sessionwise variability in the OAgroup. F tests revealed sessionwise differences in rCBFin the OA group (Table 4 and Figure 2a) bilaterally inthe postcentral gyrus, rostral and subgenual anteriorcingulate cortex, and mid/anterior insula cortex. Lefthemisphere insula rCBF differences were located ante-riorly toward the frontal operculum. Further bilateralcontiguous clusters extended into the medial–lateralaspect of the dorsal prefrontal cortex, including superiorand middle frontal gyri, precentral gyrus, right hemi-sphere superior and middle temporal gyri, and medialcerebellar hemispheres bilaterally.
We hypothesized that sessionwise rCBF differ-
ences in the OA group would relate to between-sessionvariability in NRS estimates of perceived ongoing pain.In a revised general linear model analysis, including anuisance covariate describing participants’ perceivedpain, sessionwise differences in frontal, parietal, andtemporal lobes were no longer present. Only a single,small cluster in the lateral occipital cortex showeddifferences in rCBF values between session 1 and session2. Additional investigations of the relationship betweensessionwise differences in rCBF and perceived ongoingpain, explored using semipartial regression, were per-formed in ROIs specified a priori. Significant correla-
Table 4. Cluster index, in MNI coordinate space, of differential rCBFincreases between sessions in the CMC OA group, with and without theinclusion of NRS estimates of pain as a nuisance covariate*
Region Z score x y z
Anterior cingulate, L 4.63 0 8 �8Anterior cingulate, R 4.17 2 28 �10
3.34 8 38 6Cingulate gyrus, L 5.21 �12 20 36Cingulate gyrus, R 4.82 20 2 50
4.34 4 20 42Insula, R 5.01 42 �2 4
3.67 34 18 12Medial frontal gyrus, L 3.36 �6 �20 74Superior frontal gyrus, L 3.9 �10 44 38
3.45 �14 2 74Superior frontal gyrus, R 5.33 12 40 48
3.64 6 �2 74Middle frontal gyrus, L 4.62 �32 32 44
3.93 �40 0 62Middle frontal gyrus, R 4.92 42 22 30
4.48 48 14 464.64 16 �22 62
Inferior frontal gyrus, L 4.47 �54 26 �64 �44 46 4
Inferior frontal gyrus, R 4.14 46 18 �23.83 32 22 �163.72 48 40 4
Precentral gyrus, L 3.61 �40 �22 663.57 �14 �34 76
Precentral gyrus, R 5.06 54 0 63.96 12 �22 76
Postcentral gyrus, R 4.58 58 �20 483.89 18 �50 66
Postcentral gyrus, L 3.3 �22 �48 67Superior temporal gyrus, R 3.16 64 �34 10Middle temporal gyrus, R 3.76 56 �2 �10
3.71 58 �56 4Declive, L 3.86 �36 �88 �26Declive, R 4.74 16 �70 �16Tuber, L 3.55 �40 �74 �32Uvula, R 3.97 30 �78 �34Middle occipital gyrus, L† �3.95 �38 �92 4
* MNI � Montreal Neurological Institute; rCBF � regional cerebralblood flow; CMC OA � carpometacarpal joint osteoarthritis; NRS �numerical rating scale; L � left hemisphere; R � right hemisphere.† With pain score as a covariate.
EVALUATION OF ONGOING PAIN IN HAND OA USING PERFUSION MRI 3941
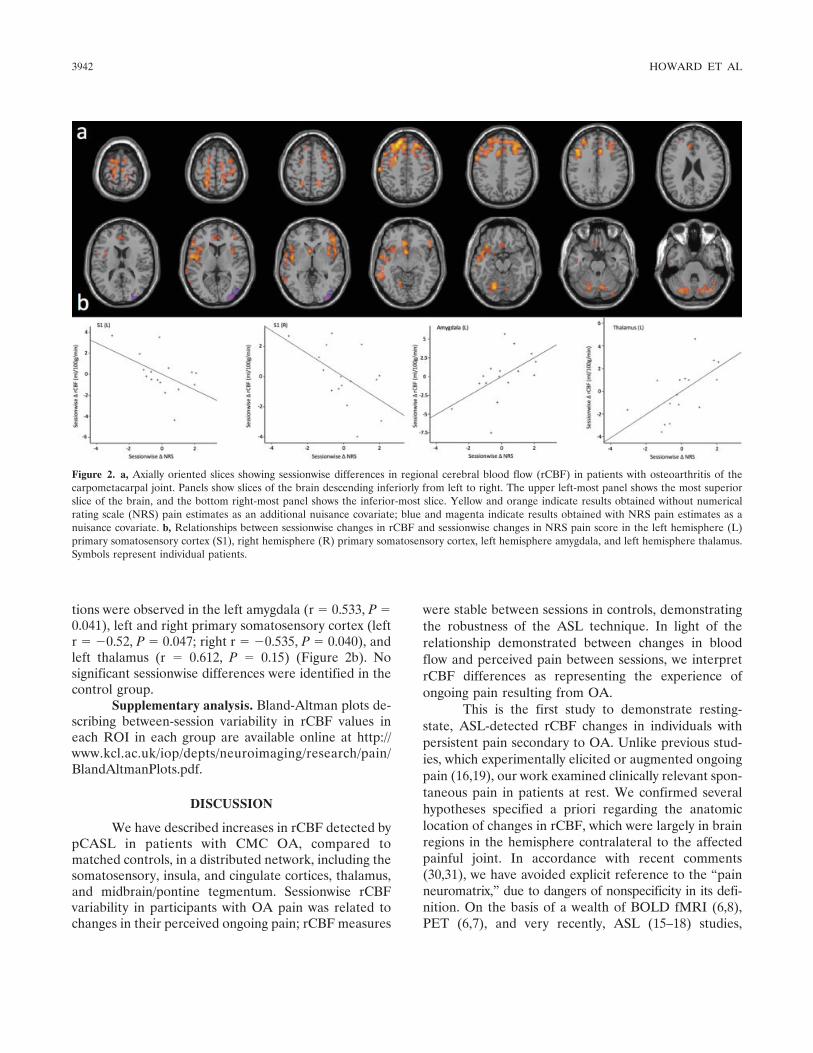
tions were observed in the left amygdala (r � 0.533, P �0.041), left and right primary somatosensory cortex (leftr � �0.52, P � 0.047; right r � �0.535, P � 0.040), andleft thalamus (r � 0.612, P � 0.15) (Figure 2b). Nosignificant sessionwise differences were identified in thecontrol group.
Supplementary analysis. Bland-Altman plots de-scribing between-session variability in rCBF values ineach ROI in each group are available online at http://www.kcl.ac.uk/iop/depts/neuroimaging/research/pain/BlandAltmanPlots.pdf.
DISCUSSION
We have described increases in rCBF detected bypCASL in patients with CMC OA, compared tomatched controls, in a distributed network, including thesomatosensory, insula, and cingulate cortices, thalamus,and midbrain/pontine tegmentum. Sessionwise rCBFvariability in participants with OA pain was related tochanges in their perceived ongoing pain; rCBF measures
were stable between sessions in controls, demonstratingthe robustness of the ASL technique. In light of therelationship demonstrated between changes in bloodflow and perceived pain between sessions, we interpretrCBF differences as representing the experience ofongoing pain resulting from OA.
This is the first study to demonstrate resting-state, ASL-detected rCBF changes in individuals withpersistent pain secondary to OA. Unlike previous stud-ies, which experimentally elicited or augmented ongoingpain (16,19), our work examined clinically relevant spon-taneous pain in patients at rest. We confirmed severalhypotheses specified a priori regarding the anatomiclocation of changes in rCBF, which were largely in brainregions in the hemisphere contralateral to the affectedpainful joint. In accordance with recent comments(30,31), we have avoided explicit reference to the “painneuromatrix,” due to dangers of nonspecificity in its defi-nition. On the basis of a wealth of BOLD fMRI (6,8),PET (6,7), and very recently, ASL (15–18) studies,
Figure 2. a, Axially oriented slices showing sessionwise differences in regional cerebral blood flow (rCBF) in patients with osteoarthritis of thecarpometacarpal joint. Panels show slices of the brain descending inferiorly from left to right. The upper left-most panel shows the most superiorslice of the brain, and the bottom right-most panel shows the inferior-most slice. Yellow and orange indicate results obtained without numericalrating scale (NRS) pain estimates as an additional nuisance covariate; blue and magenta indicate results obtained with NRS pain estimates as anuisance covariate. b, Relationships between sessionwise changes in rCBF and sessionwise changes in NRS pain score in the left hemisphere (L)primary somatosensory cortex (S1), right hemisphere (R) primary somatosensory cortex, left hemisphere amygdala, and left hemisphere thalamus.Symbols represent individual patients.
3942 HOWARD ET AL

however, it is clear that several of our findings representthe identification of rCBF differences indicating sensory–discriminative, affective–motivational, and cognitive–evaluative aspects of ongoing OA pain (5). For example,our findings of postcentral gyrus rCBF changes in theprimary somatosensory cortex, secondary somatosen-sory cortex, and insula are consistent with previousaccounts of responses in these regions using variousevoked-pain stimulation paradigms, in both healthy con-trol and patient groups (6–8). These similarities indicatethat changes in rCBF are coupled to the pain experience,rather than being solely consequences of increased levelsof cytokines, chemokines, inflammatory mediators,matrix-degrading proteases, and prostaglandins readilyidentifiable as blood-borne markers of active OA patho-physiology (20). This coupling is highly complex, how-ever, and increasing evidence indicates that when theimmune system is strongly activated by infection, injury,or persistent stresses (for example, chronic inflamma-tion), morphologic and functional changes occur inblood–brain barrier permeability, nonneuronal cells (in-cluding glia), and neuronal cells with immune functions(32,33). While a detailed discussion of neuroinflamma-tion is not possible here, it is important to acknowledgethat neuroimmune interactions have the capacity tomodulate CBF, either directly or indirectly, but thatthese interactions remain far from fully understood.From a philosophical viewpoint, immune system changesare an important component of an emergent pain expe-rience, comprised of multiple physiologic processes andactivated in response to the threat of damage to the body(34). Neuroimmune processes are likely to be a keydriver of the neuroplastic changes seen in persistent painconditions (10).
While relative rCBF decreases representing per-sistent pain have been described previously using PET(35), in this study we identified only increases in rCBFin the OA group compared to controls. This finding ofonly increases in rCBF is consistent with other recentASL studies examining ongoing pain (15,16,19). Withinthe OA group, however, several ROIs defined a prioridemonstrated relationships between changes in per-ceived ongoing OA pain and change in rCBF, includinga negative correlation in the primary somatosensorycortex bilaterally; local reductions in rCBF were associ-ated with an increase in perceived pain. Unlike previousASL studies (16,19), correlations between rCBF andNRS in the present study were identified only afteraccounting for sessionwise differences in global CBF;consideration of relationships between rCBF and globalCBF should be employed in future ASL studies. These
findings indicate that the relationship between rCBFand perceived pain is complex, both between patient andhealthy control groups and within individual groups ofpatients with persistent pain. Patterns of rCBF changesmay be disease-state specific (10) and are likely tointeract with endogenous pain modulation systems (36).Finally, while correlations between rCBF and perceivedpain are important, we urge caution in their overinter-pretation. Given the multifaceted nature of the painexperience, seeking analogs of perceived pain scores inindividual brain regions is unlikely to be wholly success-ful. Arguably, neuroimaging end points should be con-sidered in terms of the information they provide overand above subjective reporting.
Sessionwise differences in rCBF identified in theOA group related to variability in subjective reports ofthe severity of pain experienced. In light of significantbetween-session differences in NRS scores, most likely aconsequence of natural variability in OA pain, rCBFchanges are entirely expected. The core premise of thisstudy was that rCBF changes would relate to the painexperienced. Sessionwise rCBF differences were onlyindependent of variability in perceived pain in the lateraloccipital cortex. Pain influences both attention (37) andvisuomotor outputs (34), and previous reports (38) havedemonstrated that pain modulates this region of thevisual cortex, governed by the rostral anterior cingulatecortex. Changes in rCBF in this region are likely torepresent modulation of mechanisms of visuospatialattention, rather than pain perception per se.
Between-session rCBF variations were not iden-tified in pain-free control group participants. This find-ing is consistent with those of previous studies of repeat-ability within and between subjects and scanning sitesusing both pulsed and continuous ASL techniques (39).Concerns over measurement stability are more likely torelate to reduced rCBF values in an older population,with ages characteristic of patients with OA (40,41).Understanding the nature of sessionwise rCBF variabil-ity will be of vital importance should the efficacy of noveltherapies be examined using crossover trial designs (42);for this reason, we have provided Bland-Altman plotsof between-session variability as supplementary data toinform these future studies.
Consistent with previous reports using other im-aging modalities, rCBF differences in participants withOA are likely to indicate altered processing of theaffective qualities of the ongoing pain (23,24,26). How-ever, the pattern of rCBF increases observed in anetwork of brain regions, including the cingulate cortex,parietal lobe, medial temporal lobe, and prefrontal
EVALUATION OF ONGOING PAIN IN HAND OA USING PERFUSION MRI 3943

cortex, may represent a broader change than solelyemotional processing and self-assessment. Such a net-work may signify perturbed CNS functioning, represent-ing revised, maladaptive assessment and response topotential damage or “threat” to the body from painfulOA (34,43).
While rCBF changes could be interpreted asresulting solely from tonic nociceptive input from peri-pheral tissue (15,18,29), recent evidence, including neu-roimaging examination of individuals with painful OAand other diseases, suggests that maintenance of persis-tent pain is mediated by mechanisms such as CNSplasticity (10,25,44). Some CNS changes may be revers-ible; for example, many patients with hip joint OAexperience reversal of painful neuropathic symptomsfollowing arthroplasty. Ten percent of patients, however,continue to report ongoing hip pain for more than 1 yearpostsurgery (21,45), supporting a theory of centrallymediated maintenance of persistent pain. Alterations inthe functional roles of such brain regions, followingneuroplastic changes initiated by tonic input from thepainful OA joint, could provide the necessary biologicmachinery to support a “kindled” pain appraisal andresponse system (46).
Our findings are compatible with a theory ofmaladaptive assessment and response to threats to theintegrity of the body tissues in patients with persistentpain. While the posterior cingulate cortex has frequentlybeen described as important in visuospatial attention,additional evidence supports its putative role as a com-ponent in an “early warning” system orienting attentiontoward pain. Previous reports have described the impor-tance of the posterior cingulate cortex and the posteriorparietal cortex in assessing the emotional relevance ofstimuli and orienting attention toward threats to homeo-stasis (47). Differential rCBF in the posterior cingulatecortex has been described previously in individualswith traumatic neuropathic pain (35). Increases in rCBFin the posterior cingulate cortex were continuous withregions of inferior and superior parietal lobule andanterior precuneus. These regions are reported to beinvolved in higher-level cognitive functioning, includingmemory, self-related processing, and aspects of con-sciousness (37,48). The posterior cingulate cortex alsohas reciprocal connections with the subgenual anteriorcingulate cortex, a region important in the storage ofnegative events and memories of personal relevance(47). The subgenual anterior cingulate cortex has ex-tensive reciprocal connections throughout the brain,including regions with autonomic projections, includingthe amygdala, parabrachial nucleus, and periaqueductal
gray (47), and others, including the orbital medial pre-frontal cortex, hippocampus, and thalamus, all brainregions which showed rCBF increases in participantswith CMC OA. Together, these regions may plausiblyrepresent a network capable of underpinning abnormalassessment and response to the threat to homeostasispresented by pain secondary to OA. Clearly, the exis-tence of such a network in painful OA, and potentiallyother persistent pain states, is speculative and requiresconsiderable further study. However, systems-level dys-regulation of select cortical, subcortical, and limbicstructures (including the subgenual anterior cingulatecortex/amygdala), representing disruption of homeostaticmechanisms, have also been reported in nonpainfulchronic conditions such as depression (34,43,49), provid-ing an appropriate rationale for further investigation.
Our findings of rCBF changes in the midbrainand brainstem, in particular periaqueductal gray/nucleuscuneiformis and dorsal pontine tegmentum, suggestthat development of persistent pain in OA, and poten-tially in other persistent pain states, might occur viadysregulation of descending modulatory pain controlsystems. The findings of this study are consistent withreports implicating the brainstem in supraspinal mech-anisms of sensitization, derived from both experimentalpain (50) and OA (22,25) studies. Increased rCBF in thedorsal pontine tegmentum parallels a recent reportdescribing the importance of this region in the mainte-nance of central sensitization following intradermal cap-saicin injection (50). Similarly, our findings are consis-tent with reports of differential periaqueductal grayactivity following punctate stimulation of hyperalgesicareas of referred pain in patients with hip OA, comparedto healthy control participants (22). A further relation-ship between periaqueductal gray activity during evokedpain and questionnaire-based indices of neuropathic-like symptoms was also identified (22). In this study,increased rCBF values in these regions, in the absence ofevoked stimulation, indicate altered midbrain and brain-stem functioning in OA. A theory of perturbed descend-ing modulatory systems in OA pain may well predictadditional changes in the hindbrain, for example, theoutput pathways of the rostral ventromedial medulla(36). Unfortunately, we were unable to examine rostralventromedial medulla functioning using pCASL. Therostral ventromedial medulla was located inferiorly tothe prescribed field of view, and further methodologicdevelopment will be required to include the hindbrainwithin the imaging volume. Extended brainstem cover-age would further our ability to examine descendingmodulatory systems in greater depth.
3944 HOWARD ET AL

In summary, we have demonstrated the firstapplication of pCASL to the study of ongoing pain dueto OA. Our findings suggest that the pattern of rCBFincreases observed in a group of participants with pain-ful CMC OA represents the experience of ongoing painsecondary to the disease. The observed pattern of rCBFchanges suggests dysregulation of systems that includeevaluation of threat to the body from ongoing pain andthe ability of the brain to modulate pain via descendingmodulatory mechanisms. Improving our understandingof supraspinal mechanisms of ongoing pain in diseaseshould assist in the development of new approaches fortherapeutic intervention.
ACKNOWLEDGMENTS
We are grateful to Ms Caroline Wooldridge and Dr.Ellen Migo for helpful comments and suggestions on themanuscript. We would like to thank all of the participants ofthe Chingford Women Study and Dr. Deborah Hart (King’sCollege London) for their time and dedication. The authorsalso wish to acknowledge the ongoing support of the King’sCentre of Excellence in Medical Engineering.
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising itcritically for important intellectual content, and all authors approvedthe final version to be published. Dr. Howard had full access to all ofthe data in the study and takes responsibility for the integrity of thedata and the accuracy of the data analysis.Study conception and design. Howard, Sanders, Fotopoulou, Massat,Huggins, Vennart, Williams.Acquisition of data. Howard, Sanders, Krause, Fotopoulou, Zelaya,Choy, Daniels.Analysis and interpretation of data. Howard, Krause, O’Muircheartaigh,Zelaya, Thacker, Massat, Huggins, Vennart, Daniels, Williams.
ROLE OF THE STUDY SPONSOR
This project was an academic–industrial collaboration be-tween King’s College London and the study sponsor, Pfizer GlobalResearch and Development, UK. Pfizer and King’s College Londonscientists worked in collaboration on the following areas: study design,data analysis, interpretation of data, and the writing of the manuscript.All data collection was performed by King’s College London scientistsonly. Pfizer approved the content of the manuscript prior to submission.
REFERENCES
1. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D.Survey of chronic pain in Europe: prevalence, impact on daily life,and treatment. Eur J Pain 2006;10:287–333.
2. Eccleston C, Williams AC, Morley S. Psychological therapies forthe management of chronic pain (excluding headache) in adults.Cochrane Database Syst Rev 2009:CD007407.
3. Kupers R, Kehlet H. Brain imaging of clinical pain states: a criticalreview and strategies for future studies. Lancet Neurol 2006;5:1033–44.
4. Coghill RC, McHaffie JG, Yen YF. Neural correlates of inter-
individual differences in the subjective experience of pain. ProcNatl Acad Sci U S A 2003;100:8538–42.
5. Melzack R. From the gate to the neuromatrix. Pain 1999;Suppl6:S121–6.
6. Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Humanbrain mechanisms of pain perception and regulation in health anddisease. Eur J Pain 2005;9:463–84.
7. Peyron R, Laurent B, Garcia-Larrea L. Functional imaging ofbrain responses to pain: a review and meta-analysis (2000).Neurophysiol Clin 2000;30:263–88.
8. Tracey I, Mantyh PW. The cerebral signature for pain perceptionand its modulation. Neuron 2007;55:377–91.
9. Tracey I, Bushnell MC. How neuroimaging studies have chal-lenged us to rethink: is chronic pain a disease? J Pain 2009;10:1113–20.
10. May A. Chronic pain may change the structure of the brain. Pain2008;137:7–15.
11. Baliki MN, Chialvo DR, Geha PY, Levy RM, Harden RN, ParrishTB, et al. Chronic pain and the emotional brain: specific brainactivity associated with spontaneous fluctuations of intensity ofchronic back pain. J Neurosci 2006;26:12165–73.
12. Napadow V, LaCount L, Park K, As-Sanie S, Clauw DJ, HarrisRE. Intrinsic brain connectivity in fibromyalgia is associated withchronic pain intensity. Arthritis Rheum 2010;62:2545–55.
13. Cahana A, Carota A, Montadon ML, Annoni JM. The long-termeffect of repeated intravenous lidocaine on central pain and pos-sible correlation in positron emission tomography measurements.Anesth Analg 2004;98:1581–4.
14. Dai W, Garcia D, De Bazelaire C, Alsop DC. Continuous flow-driven inversion for arterial spin labeling using pulsed radiofrequency and gradient fields. Magn Reson Med 2008;60:1488–97.
15. Howard MA, Krause K, Khawaja N, Massat N, Zelaya F,Schumann G, et al. Beyond patient reported pain: perfusionmagnetic resonance imaging demonstrates reproducible cerebralrepresentation of ongoing post-surgical pain. PLoS One 2011;6:e17096.
16. Wasan AD, Loggia ML, Chen LQ, Napadow V, Kong J, GollubRL. Neural correlates of chronic low back pain measured byarterial spin labeling. Anesthesiology 2011;115:364–74.
17. Owen DG, Bureau Y, Thomas AW, Prato FS, St. Lawrence KS.Quantification of pain-induced changes in cerebral blood flow byperfusion MRI. Pain 2008;136:85–96.
18. Owen DG, Clarke CF, Ganapathy S, Prato FS, St Lawrence KS.Using perfusion MRI to measure the dynamic changes in neuralactivation associated with tonic muscular pain. Pain 2010;148:375–86.
19. Owen DG, Clarke CF, Bureau Y, Ganapathy S, Prato FS,St Lawrence KS. Measuring the neural response to continuousintramuscular infusion of hypertonic saline by perfusion MRI.J Magn Reson Imaging 2012;35:669–77.
20. Wieland HA, Michaelis M, Kirschbaum BJ, Rudolphi KA. Osteo-arthritis: an untreatable disease? [published erratum appears inNat Rev Drug Discov 2005;4:543]. Nat Rev Drug Discov 2005;4:331–44.
21. Kosek E, Ordeberg G. Abnormalities of somatosensory percep-tion in patients with painful osteoarthritis normalize followingsuccessful treatment. Eur J Pain 2000;4:229–38.
22. Gwilym SE, Keltner JR, Warnaby CE, Carr AJ, Chizh B, ChessellI, et al. Psychophysical and functional imaging evidence supportingthe presence of central sensitization in a cohort of osteoarthritispatients. Arthritis Rheum 2009;61:1226–34.
23. Baliki MN, Geha PY, Jabakhanji R, Harden N, Schnitzer TJ,Apkarian AV. A preliminary fMRI study of analgesic treatment inchronic back pain and knee osteoarthritis. Mol Pain 2008;4:47.
24. Kulkarni B, Bentley DE, Elliott R, Julyan PJ, Boger E, Watson A,et al. Arthritic pain is processed in brain areas concerned withemotions and fear. Arthritis Rheum 2007;56:1345–54.
EVALUATION OF ONGOING PAIN IN HAND OA USING PERFUSION MRI 3945

25. Gwilym SE, Filippini N, Douaud G, Carr AJ, Tracey I. Thalamicatrophy associated with painful osteoarthritis of the hip is revers-ible after arthroplasty: a longitudinal voxel-based morphometricstudy. Arthritis Rheum 2010;62:2930–40.
26. Parks EL, Geha PY, Baliki MN, Katz J, Schnitzer TJ, ApkarianAV. Brain activity for chronic knee osteoarthritis: dissociatingevoked pain from spontaneous pain. Eur J Pain 2011;15:843.31–14.
27. Altman R, Alarcon G, Appelrouth D, Bloch D, Borenstein D,Brandt K, et al. The American College of Rheumatology criteriafor the classification and reporting of osteoarthritis of the hand.Arthritis Rheum 1990;33:1601–10.
28. Bland JM, Altman DG. Statistical methods for assessing agree-ment between two methods of clinical measurement. Lancet1986;1:307–10.
29. Duvernoy HM. The human brain: surface, three-dimensionalsectional anatomy with MRI, and blood supply. 2nd ed. New York:Springer-Verlag Wien; 1999.
30. Iannetti GD, Mouraux A. From the neuromatrix to the pain matrix(and back). Exp Brain Res 2010;205:1–12.
31. Tracey I, Johns E. The pain matrix: reloaded or reborn as weimage tonic pain using arterial spin labelling. Pain 2010;148:359–60.
32. Hess A, Axmann R, Rech J, Finzel S, Heindl C, Kreitz S, et al.Blockade of TNF-� rapidly inhibits pain responses in the centralnervous system. Proc Natl Acad Sci U S A 2011;108:3731–6.
33. Yirmiya R, Goshen I. Immune modulation of learning, memory,neural plasticity and neurogenesis. Brain Behav Immun 2011;25:181–213.
34. Moseley GL. A pain neuromatrix approach to patients withchronic pain. Man Ther 2003;8:130–40.
35. Hsieh JC, Belfrage M, Stone-Elander S, Hansson P, Ingvar M.Central representation of chronic ongoing neuropathic pain stud-ied by positron emission tomography. Pain 1995;63:225–36.
36. Fields HL, Basbaum AI, Heinricher MM. Central nervous systemmechanisms of pain modulation. In: McMahon S, Koltzenburg M,editors. Wall and Melzack’s textbook of pain. 5th ed. Philadelphia:Elsevier; 2006. p. 125–42.
37. Eccleston C, Crombez G. Pain demands attention: a cognitive-affective model of the interruptive function of pain. Psychol Bull1999;125:356–66.
38. Bingel U, Rose M, Glascher J, Buchel C. fMRI reveals how pain
modulates visual object processing in the ventral visual stream.Neuron 2007;55:157–67.
39. Gevers S, van Osch MJ, Bokkers RP, Kies DA, Teeuwisse WM,Majoie CB, et al. Intra- and multicenter reproducibility of pulsed,continuous and pseudo-continuous arterial spin labeling methodsfor measuring cerebral perfusion. J Cereb Blood Flow Metab2011;31:1706–15.
40. Parkes LM, Rashid W, Chard DT, Tofts PS. Normal cerebralperfusion measurements using arterial spin labeling: reproduc-ibility, stability, and age and gender effects. Magn Reson Med2004;51:736–43.
41. Leenders KL, Perani D, Lammertsma AA, Heather JD,Buckingham P, Healy MJ, et al. Cerebral blood flow, blood volumeand oxygen utilization: normal values and effect of age. Brain1990;113:27–47.
42. Borsook D, Bleakman D, Hargreaves R, Upadhyay J, Schmidt KF,Becerra L. A ‘BOLD’ experiment in defining the utility of fMRI indrug development. Neuroimage 2008;42:461–6.
43. Craig AD. How do you feel? Interoception: the sense of thephysiological condition of the body. Nat Rev Neurosci 2002;3:655–66.
44. Apkarian AV, Baliki MN, Geha PY. Towards a theory of chronicpain. Prog Neurobiol 2009;87:81–97.
45. Nikolajsen L, Brandsborg B, Lucht U, Jensen TS, Kehlet H.Chronic pain following total hip arthroplasty: a nationwide ques-tionnaire study. Acta Anaesthesiol Scand 2006;50:495–500.
46. Malcangio M, editor. Synaptic plasticity in pain. New York:Springer-Verlag; 2009.
47. Vogt BA. Pain and emotion interactions in subregions of thecingulate gyrus. Nat Rev Neurosci 2005;6:533–44.
48. Cavanna AE, Trimble MR. The precuneus: a review of itsfunctional anatomy and behavioural correlates. Brain 2006;129:564–83.
49. Giacobbe P, Mayberg HS, Lozano AM. Treatment resistantdepression as a failure of brain homeostatic mechanisms: implica-tions for deep brain stimulation. Exp Neurol 2009;219:44–52.
50. Lee MC, Zambreanu L, Menon DK, Tracey I. Identifying brainactivity specifically related to the maintenance and perceptualconsequence of central sensitization in humans. J Neurosci 2008;28:11642–9.
3946 HOWARD ET AL




















