
High Incidence of Intramural Thrombus After Overlapping Paclitaxel-Eluting Stent Implantation...
9
Jabara, Sarah Geva, Takafumi Ueno, Nicolas Chronos, Keith Robinson and Dongming Hou Toshiro Shinke, Jinsheng Li, Jack P. Chen, Lakshmana Pendyala, Traci Goodchild, Refat Implantation: Angioscopic and Histopathologic Analysis in Porcine Coronary Arteries High Incidence of Intramural Thrombus After Overlapping Paclitaxel-Eluting Stent Print ISSN: 1941-7640. Online ISSN: 1941-7632 Copyright © 2008 American Heart Association, Inc. All rights reserved. Avenue, Dallas, TX 75231 is published by the American Heart Association, 7272 Greenville Circulation: Cardiovascular Interventions doi: 10.1161/CIRCINTERVENTIONS.108.770008 2008;1:28-35 Circ Cardiovasc Interv. http://circinterventions.ahajournals.org/content/1/1/28 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circinterventions.ahajournals.org//subscriptions/ is online at: Circulation: Cardiovascular Interventions Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Answer Permissions and Rights Question and under Services. Further information about this process is available in the permission is being requested is located, click Request Permissions in the middle column of the Web page Clearance Center, not the Editorial Office. Once the online version of the published article for which can be obtained via RightsLink, a service of the Copyright Circulation: Cardiovascular Interventions in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on April 9, 2014 http://circinterventions.ahajournals.org/ Downloaded from by guest on April 9, 2014 http://circinterventions.ahajournals.org/ Downloaded from
Transcript of High Incidence of Intramural Thrombus After Overlapping Paclitaxel-Eluting Stent Implantation...
Jabara, Sarah Geva, Takafumi Ueno, Nicolas Chronos, Keith Robinson and Dongming HouToshiro Shinke, Jinsheng Li, Jack P. Chen, Lakshmana Pendyala, Traci Goodchild, Refat
Implantation: Angioscopic and Histopathologic Analysis in Porcine Coronary ArteriesHigh Incidence of Intramural Thrombus After Overlapping Paclitaxel-Eluting Stent
Print ISSN: 1941-7640. Online ISSN: 1941-7632 Copyright © 2008 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleCirculation: Cardiovascular Interventions
doi: 10.1161/CIRCINTERVENTIONS.108.7700082008;1:28-35Circ Cardiovasc Interv.
http://circinterventions.ahajournals.org/content/1/1/28World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circinterventions.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Interventions Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Answer
Permissions and Rights Question andunder Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the Web pageClearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the CopyrightCirculation: Cardiovascular Interventionsin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from

High Incidence of Intramural Thrombus After OverlappingPaclitaxel-Eluting Stent Implantation
Angioscopic and Histopathologic Analysis in Porcine Coronary Arteries
Toshiro Shinke, MD, PhD; Jinsheng Li, MD, PhD; Jack P. Chen, MD; Lakshmana Pendyala, MD;Traci Goodchild, PhD; Refat Jabara, MD; Sarah Geva, PhD; Takafumi Ueno, MD, PhD;
Nicolas Chronos, MD; Keith Robinson, PhD; Dongming Hou, MD, PhD
Background—Systematic analysis of in vivo angioscopy and postmortem histopathology for paclitaxel-eluting stents(PES) has not been previously reported. We assessed 1-month angioscopic and histopathologic sequelae of overlappingPES in pig coronary arteries.
Methods and Results—Overlapping PES and bare-metal stents (BMS; n�9, one pair per pig) were implanted, and animalswere euthanized at 1 month. Late lumen loss was reduced in PES compared with BMS (0.46�0.63 mm versus1.30�0.50 mm; P�0.01). Angioscopically, PES stent struts were clearly visible and accompanied by substantial redmaterial indicating mural thrombi. In contrast, stent struts and mural thrombi were barely visible in BMS (P�0.001versus PES). Macroscopically, mural thrombi were abundant but distributed irregularly throughout the PES, with greaterconcentration in overlapping segments. Only occasional mural thrombi were noted for BMS. Microscopically, neointimaof BMS was fibrocellular and mature, whereas only a thin layer of immature neointima was seen in PES. Neointimalthickness was less in PES than BMS (0.11�0.07 mm versus 0.33�0.12 mm; P�0.018). Additionally, extensivepara-strut and intramural thrombi, red blood cell debris, and minute luminal thrombi were observed in PES. Despitenormal angioscopic appearance of both proximal and distal nonstented reference segments, endothelium-dependentrelaxation to substance P was notably diminished (PES, 0�7% versus BMS, 10�6%; P�0.007), whereas nitroglycerinresponse was preserved (PES, 9�5% versus BMS, 12�7%; P�0.34).
Conclusions—In the porcine coronary model, overlapping PES is associated with marked intramural thrombi, which wasaccurately detected on angioscopy at 1 month. Moreover, despite normal luminal angioscopic appearance, adjacentnonstented reference segments demonstrated impaired endothelium-dependent vasoreactivity. (Circ CardiovascIntervent. 2008;1:28-35.)
Key Words: stents, drug-eluting � angioscopes � histology � endothelium � thrombus
Drug-eluting stents (DES) have become the predominantinterventional modality for treatment of patients with
coronary artery disease. Although multiple DES clinical trialshave demonstrated significant reductions in target lesionrevascularization,1–3 late stent thrombosis (LST), with theattendant risks of vessel closure, myocardial infarction, anddeath, has emerged as a major concern.4–7 Human autopsystudies have implicated delayed arterial healing and poorreendothelialization as potential mechanisms in the pathogen-esis of LST.8–10 Recently, the latest meta-analysis of random-ized trials showed no difference between bare-metal stents(BMS) and DES for the cumulative 4-year incidences ofdeath or myocardial infarction using Academic ResearchConsortium definitions.11 However, a numeric increase in theincidence of LST after DES still has been observed.2 There-
fore, additional research into the vascular pathophysiologicalresponse to DES as it potentially relates to LST is warranted.
Editorial see p 7Clinical Perspective see p 35
Angioscopy allows for direct visualization of the vascularlumen, as well as stent strut (SS) surfaces. It has been used forthrombus assessment in vivo, with ample clinical data sup-porting its superiority over angiography for this purpose.12
Several clinical angioscopic studies have demonstrated DES-associated delayed vessel healing, as well as sustained (intra-)mural thrombus (MT) formation. However, there have beenno published studies evaluating angioscopic appearance ofcoronary arteries with DES conducted in parallel with assess-ment of arterial wall histological characteristics. To date,
Received January 30, 2008; accepted April 24, 2008.From the Saint Joseph’s Translational Research Institute/Saint Joseph’s Hospital of Atlanta (T.S., J.L., J.P.C., L.P. T.G., R.J., S.G., N.C., K.R., D.H.),
Atlanta, GA; and Fukuoka City Medical Association Hospital (T.U.), Fukuoka, Japan.Correspondence to Dongming Hou, MD, PhD, Saint Joseph’s Translational Research Institute/ Saint Joseph’s Hospital of Atlanta, 5673 Peachtree
Dunwoody Rd, Suite 675, Atlanta, GA 30342. [email protected]© 2008 American Heart Association, Inc.
Circ Cardiovasc Intervent is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.108.770008
28 by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from

most of the existing angioscopic DES literature involvessingle de novo sirolimus-eluting stents.13–15 The angioscopicappearance and histological findings after overlappingpaclitaxel-eluting stent (PES) implantation are still largelyunknown.
Clinically, overlapping DES are at times required fordiffuse, long coronary lesions to assure full coverage. Indeed,the incidence of multiple stent placement is up to 28% inpaclitaxel-eluting stent (TAXUS) trials.16,17 Even more thansingle stents, overlapping PES might be expected to elicitdelayed healing responses, including increased MT as well asreduced neointimal coverage (NC). Furthermore, vasomotordysfunction in coronary segments adjacent to DES has beenreported18–20 and may be associated with delayed healing ineither a causative fashion or as a bystander phenomenon.Therefore, in the present study, we aimed to evaluate 1-monthangioscopic, macroscopic, and histopathological features inoverlapping PES versus BMS in a coronary artery experi-mental animal model. We also measured the vasomotorfunction in proximal and distal adjacent nonstented referencesegments (NSRS).
MethodsAnimals and Experimental ProtocolAnimal handling and care followed the recommendations of theNational Institutes of Health guide for the care and use of laboratoryanimals and was consistent with guidelines of the American HeartAssociation. All protocols were approved by the Animal Care andUse Committee and were consistent with Association for Assessmentand Accreditation of Laboratory Animal Care guidelines. Ninejuvenile female or castrated male Yorkshire farm pigs (weight,31.2�2.4 kg) were enrolled onto this study.
All animals received a combination of 81 mg of aspirin and 75 mgof clopidogrel by mouth daily for 3 days before stent implantation,continued until termination, and were fasted overnight before theprocedure. The animals were sedated by intramuscular injection ofketamine 20 mg/kg, xylazine 2 mg/kg, and atropine 0.05 mg/kg.After intubation, general anesthesia was induced and maintainedwith isoflurane (2.5%). The ECG and blood pressure were continu-ously monitored.
Cardiac catheterization was performed with full heparinization(200 U/kg), and stents were implanted with quantitative coronaryangiography guidance to obtain a stent-to-arterial diameter ratio of�1.1:1 to 1.2:1. Activated clotting time measurements were per-formed. Overlapping PES (TAXUS, Express 2; Boston ScientificCorp, Natick, Mass) or BMS (Express 2, Boston Scientific Corp, orMulti-Link Penta, Abbott Vascular, Abbott Park, Ill) were implantedinto the coronary arteries by a scheme of constrained randomization(2 pairs of overlapping stents/animal). There were no between-groupdifferences for the total stent length (BMS, 26.0�1.7 mm versusPES, 26.8�1.2 mm; P�0.28) or stent overlap length (BMS,5.1�1.3 mm versus PES, 5.2�1.2 mm; P�0.85). Angiographictarget-vessel diameter, stent-to-arterial diameter ratio, poststent min-imal lumen diameter, and late lumen loss were measured in allanimals either at implantation or at 1-month follow-up.
Angioscopic AnalysisAll stents were assessed by angioscopy during the terminal proce-dure. The system consisted of a 4.5F rapid-exchange catheter(Vecmova Neo; FiberTech, Tokyo, Japan) and a light source (3charge-coupled device Imaging System Ft-203; FiberTech). Theangioscope catheter was advanced into the distal segment of thecoronary artery, followed by infusion of room temperature lactatedRinger’s solution through the outer catheter at a rate of 0.5 to 1.0mL/s. The occlusion balloon was then hand-inflated at the proximal
portion of the stented segment; after clearance of blood from the fieldof view, the angioscope catheter was then manually retracted throughthe stented segment.21
Angioscopic images for proximal single-strut, overlap, and distalsingle-strut areas were analyzed for degrees of NC over SS, MT, andluminal thrombi according to a modified grading system.22 Thearterial segments 1.5 cm proximal and distal to the stent were alsoanalyzed. NC score was classified into 4 semiquantitative gradingcategories: grade 0, fully visible SS (similar to immediate postim-plantation); grade 1, SS covered but protruding into lumen andtransparently visible; grade 2, SS embedded by neointima but stilltranslucent; and grade 3, SS fully embedded and invisible. MT scorewas likewise classified into 4 grades: grade 0, no visible red spot;grade 1, focal red or pink spots along the SS; grade 2, red spotpartially extending to interstrut space; and grade 3, red spot spanningacross interstrut space. The presence or absence of luminal thrombi(a coalescent, red or pink, or white protruding mass adhering to thevessel surface but clearly a separate structure) was also evaluated.
All angioscopic imaging was evaluated and scored in an indepen-dent fashion by 2 experienced investigators, who were unaware oftreatment group assignments. There was no interobserver variability,as the angioscopic scorings were identical between the 2 observers.
Macroscopic EvaluationAt 1 month after interventional procedures, all animals were eutha-nized. The hearts were explanted and perfusion-rinsed with 0.9%NaCl solution. The stented coronary vessels were quickly butcarefully excised and trimmed free of adherent adjacent myocardiumand adipose tissue. Each artery was longitudinally incised, and thecoronary luminal surface was exposed. Digital images were obtainedunder uniform exposure conditions. The proximal and distal single-stent regions and overlap sites were analyzed separately. NC wasscored and classified into 4 semiquantitative grades similar to thoseused in angioscopic analysis. For MT assessment, the overall redspots on the luminal surfaces were measured by planimetry andexpressed as a percentage of the stented area.
Microscopic AnalysisSamples for histopathological analysis were fixed with a mixture ofbuffered 1.25% glutaraldehyde and 5% formalin and then immersedin formalin overnight. After dehydration in graded ethanol series to100%, the vessels were finally embedded in methyl methacrylate.Sections from the proximal, overlap, and distal stent regions were cutusing a heavy-duty microtome and collected on glass slides; theywere stained with hematoxylin-eosin and Movat pentachrome. Mor-phometric analysis for neointimal thickness at each SS site wasperformed by computerized planimetry using Image Pro Plus soft-ware (Image Pro-Plus, Silver Spring, Md) on proximal, overlapping,and distal sections. Sections from each stented vessel were scored forintramural thrombus (a mixture of fibrin, para-strut amorphousmaterial, and red blood cell debris) deposition on the basis of thefollowing semiquantitative grading scale: grade 0, not present; grade1, mild (scattered); grade 2, moderate (encompassing �50% of astrut in at least 25% to 50% of the circumference length); and grade3, severe (surrounding a strut in at least 50% of the circumferencelength) according to previously published methods.23 Reendotheli-alization was also scored by the circumferential extent of luminalsurface coverage in each section with flattened, confluent endothelialor endothelial-like cells as follows: 0, 0% to 25% coverage ofcircumference length; 1, 25% to 50% coverage; 2, 50% to 75%coverage; and 3, 75% to 100% coverage.
Evaluation of Endothelial FunctionAt follow-up, endothelium-dependent and -independent coronaryvasorelaxation capacities were assessed after intracoronary infusionof the endothelium-dependent receptor-mediated dilator substance P(sP; 2 ng/kg) followed by the endothelium-independent vasodilatornitroglycerin (200 �g) administered via the guide catheter. sP wasinfused over a period of 30 seconds.24 After a 10-minute interval,nitroglycerin was administered as a bolus. Coronary angiography
Shinke et al Intramural Thrombus After Overlapping PES Implantation 29
by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from
was performed with identical angiographic projections before andafter vasoactive drug administration. The percent diameter changefrom baseline to after infusion at 1.5 cm proximal and distal to thestented segment (NSRS) was considered to reflect vasorelaxationcapacity.
Statistical AnalysisAll numeric data were expressed as mean�SD. Statistical analysiswas performed by Sigma Stat version 3.5 (Systat Software, Erkrath,Germany). Angiographic percent diameter change in the referencesegments were evaluated between the groups by the Student unpaired2-tailed t test. Differences among the segments (proximal, overlap,and distal) for both BMS and PES groups were evaluated by 2-wayANOVA, followed by the Fisher least-squares temporal-differencepost hoc test. For nonnumeric data (scoring data), Kruskal-WallisANOVA on Ranks was used for comparison among the segments forboth groups. A critical value of P�0.05 was considered to indicatesignificant treatment effect or between-groups difference.
The authors had full access to the data and take full responsibilityfor the integrity of the data. All authors have read and agree to themanuscript as written.
ResultsAll animals tolerated the stent implantation and angioscopicprocedures well, without any adverse cardiac or systemicevents. There were no complications of morbidity or mortal-ity until final euthanasia of the animals.
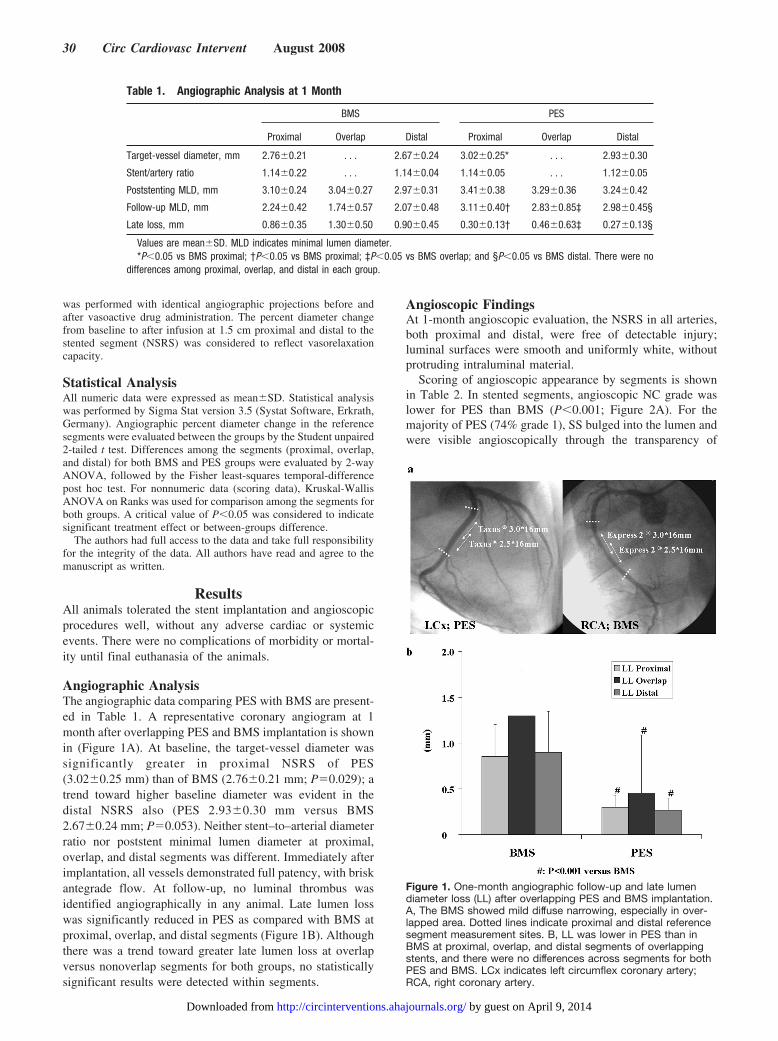
Angiographic AnalysisThe angiographic data comparing PES with BMS are present-ed in Table 1. A representative coronary angiogram at 1month after overlapping PES and BMS implantation is shownin (Figure 1A). At baseline, the target-vessel diameter wassignificantly greater in proximal NSRS of PES(3.02�0.25 mm) than of BMS (2.76�0.21 mm; P�0.029); atrend toward higher baseline diameter was evident in thedistal NSRS also (PES 2.93�0.30 mm versus BMS2.67�0.24 mm; P�0.053). Neither stent–to–arterial diameterratio nor poststent minimal lumen diameter at proximal,overlap, and distal segments was different. Immediately afterimplantation, all vessels demonstrated full patency, with briskantegrade flow. At follow-up, no luminal thrombus wasidentified angiographically in any animal. Late lumen losswas significantly reduced in PES as compared with BMS atproximal, overlap, and distal segments (Figure 1B). Althoughthere was a trend toward greater late lumen loss at overlapversus nonoverlap segments for both groups, no statisticallysignificant results were detected within segments.
Angioscopic FindingsAt 1-month angioscopic evaluation, the NSRS in all arteries,both proximal and distal, were free of detectable injury;luminal surfaces were smooth and uniformly white, withoutprotruding intraluminal material.
Scoring of angioscopic appearance by segments is shownin Table 2. In stented segments, angioscopic NC grade waslower for PES than BMS (P�0.001; Figure 2A). For themajority of PES (74% grade 1), SS bulged into the lumen andwere visible angioscopically through the transparency of
Table 1. Angiographic Analysis at 1 Month
BMS PES
Proximal Overlap Distal Proximal Overlap Distal
Target-vessel diameter, mm 2.76�0.21 . . . 2.67�0.24 3.02�0.25* . . . 2.93�0.30
Stent/artery ratio 1.14�0.22 . . . 1.14�0.04 1.14�0.05 . . . 1.12�0.05
Poststenting MLD, mm 3.10�0.24 3.04�0.27 2.97�0.31 3.41�0.38 3.29�0.36 3.24�0.42
Follow-up MLD, mm 2.24�0.42 1.74�0.57 2.07�0.48 3.11�0.40† 2.83�0.85‡ 2.98�0.45§
Late loss, mm 0.86�0.35 1.30�0.50 0.90�0.45 0.30�0.13† 0.46�0.63‡ 0.27�0.13§
Values are mean�SD. MLD indicates minimal lumen diameter.*P�0.05 vs BMS proximal; †P�0.05 vs BMS proximal; ‡P�0.05 vs BMS overlap; and §P�0.05 vs BMS distal. There were no
differences among proximal, overlap, and distal in each group.
Figure 1. One-month angiographic follow-up and late lumendiameter loss (LL) after overlapping PES and BMS implantation.A, The BMS showed mild diffuse narrowing, especially in over-lapped area. Dotted lines indicate proximal and distal referencesegment measurement sites. B, LL was lower in PES than inBMS at proximal, overlap, and distal segments of overlappingstents, and there were no differences across segments for bothPES and BMS. LCx indicates left circumflex coronary artery;RCA, right coronary artery.
30 Circ Cardiovasc Intervent August 2008
by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from
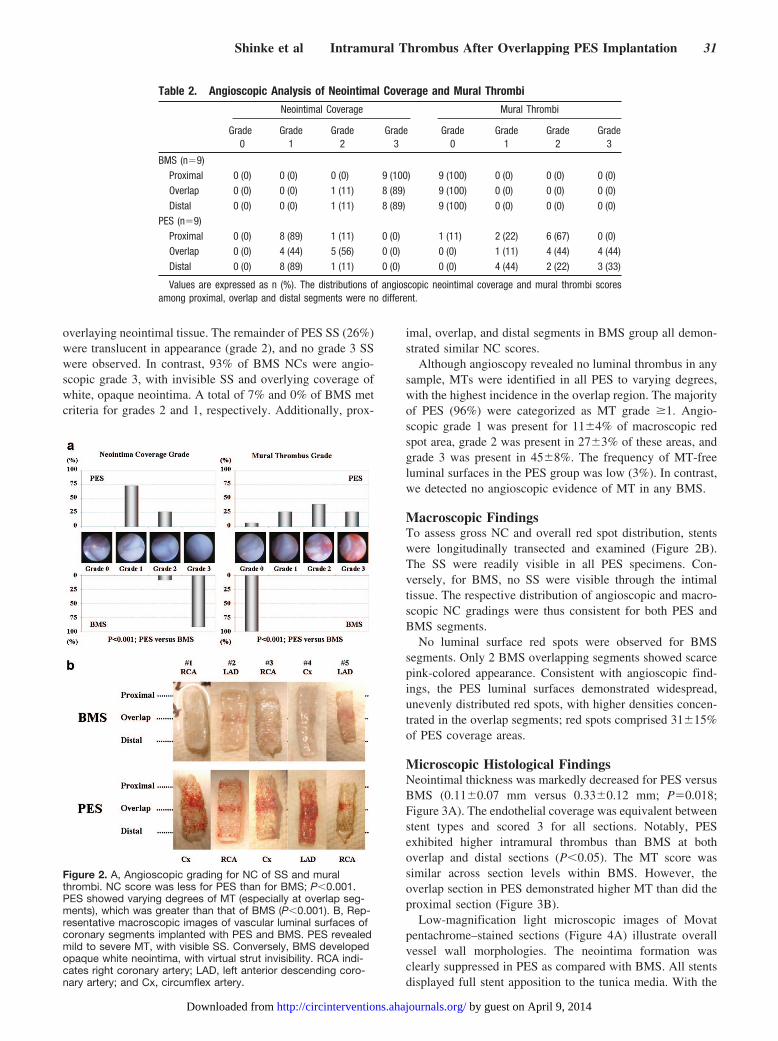
overlaying neointimal tissue. The remainder of PES SS (26%)were translucent in appearance (grade 2), and no grade 3 SSwere observed. In contrast, 93% of BMS NCs were angio-scopic grade 3, with invisible SS and overlying coverage ofwhite, opaque neointima. A total of 7% and 0% of BMS metcriteria for grades 2 and 1, respectively. Additionally, prox-
imal, overlap, and distal segments in BMS group all demon-strated similar NC scores.
Although angioscopy revealed no luminal thrombus in anysample, MTs were identified in all PES to varying degrees,with the highest incidence in the overlap region. The majorityof PES (96%) were categorized as MT grade �1. Angio-scopic grade 1 was present for 11�4% of macroscopic redspot area, grade 2 was present in 27�3% of these areas, andgrade 3 was present in 45�8%. The frequency of MT-freeluminal surfaces in the PES group was low (3%). In contrast,we detected no angioscopic evidence of MT in any BMS.
Macroscopic FindingsTo assess gross NC and overall red spot distribution, stentswere longitudinally transected and examined (Figure 2B).The SS were readily visible in all PES specimens. Con-versely, for BMS, no SS were visible through the intimaltissue. The respective distribution of angioscopic and macro-scopic NC gradings were thus consistent for both PES andBMS segments.
No luminal surface red spots were observed for BMSsegments. Only 2 BMS overlapping segments showed scarcepink-colored appearance. Consistent with angioscopic find-ings, the PES luminal surfaces demonstrated widespread,unevenly distributed red spots, with higher densities concen-trated in the overlap segments; red spots comprised 31�15%of PES coverage areas.
Microscopic Histological FindingsNeointimal thickness was markedly decreased for PES versusBMS (0.11�0.07 mm versus 0.33�0.12 mm; P�0.018;Figure 3A). The endothelial coverage was equivalent betweenstent types and scored 3 for all sections. Notably, PESexhibited higher intramural thrombus than BMS at bothoverlap and distal sections (P�0.05). The MT score wassimilar across section levels within BMS. However, theoverlap section in PES demonstrated higher MT than did theproximal section (Figure 3B).
Low-magnification light microscopic images of Movatpentachrome–stained sections (Figure 4A) illustrate overallvessel wall morphologies. The neointima formation wasclearly suppressed in PES as compared with BMS. All stentsdisplayed full stent apposition to the tunica media. With the
Figure 2. A, Angioscopic grading for NC of SS and muralthrombi. NC score was less for PES than for BMS; P�0.001.PES showed varying degrees of MT (especially at overlap seg-ments), which was greater than that of BMS (P�0.001). B, Rep-resentative macroscopic images of vascular luminal surfaces ofcoronary segments implanted with PES and BMS. PES revealedmild to severe MT, with visible SS. Conversely, BMS developedopaque white neointima, with virtual strut invisibility. RCA indi-cates right coronary artery; LAD, left anterior descending coro-nary artery; and Cx, circumflex artery.
Table 2. Angioscopic Analysis of Neointimal Coverage and Mural Thrombi
Neointimal Coverage Mural Thrombi
Grade0
Grade1
Grade2
Grade3
Grade0
Grade1
Grade2
Grade3
BMS (n�9)Proximal 0 (0) 0 (0) 0 (0) 9 (100) 9 (100) 0 (0) 0 (0) 0 (0)Overlap 0 (0) 0 (0) 1 (11) 8 (89) 9 (100) 0 (0) 0 (0) 0 (0)Distal 0 (0) 0 (0) 1 (11) 8 (89) 9 (100) 0 (0) 0 (0) 0 (0)
PES (n�9)Proximal 0 (0) 8 (89) 1 (11) 0 (0) 1 (11) 2 (22) 6 (67) 0 (0)Overlap 0 (0) 4 (44) 5 (56) 0 (0) 0 (0) 1 (11) 4 (44) 4 (44)Distal 0 (0) 8 (89) 1 (11) 0 (0) 0 (0) 4 (44) 2 (22) 3 (33)
Values are expressed as n (%). The distributions of angioscopic neointimal coverage and mural thrombi scoresamong proximal, overlap and distal segments were no different.
Shinke et al Intramural Thrombus After Overlapping PES Implantation 31
by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from
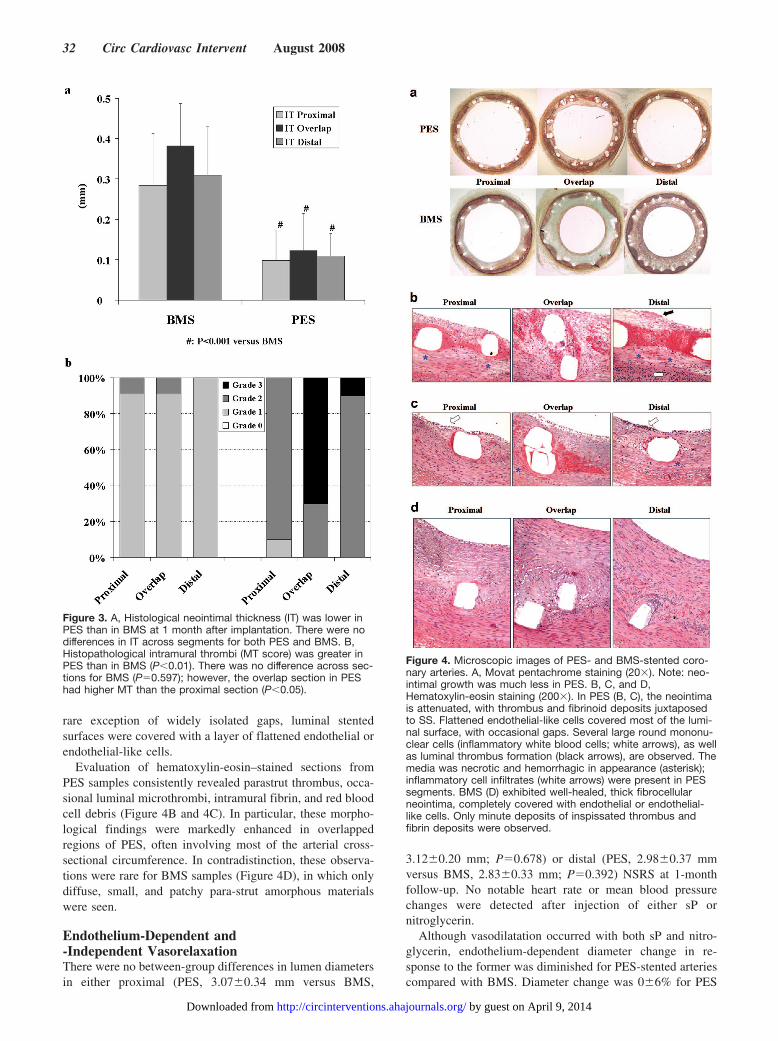
rare exception of widely isolated gaps, luminal stentedsurfaces were covered with a layer of flattened endothelial orendothelial-like cells.
Evaluation of hematoxylin-eosin–stained sections fromPES samples consistently revealed parastrut thrombus, occa-sional luminal microthrombi, intramural fibrin, and red bloodcell debris (Figure 4B and 4C). In particular, these morpho-logical findings were markedly enhanced in overlappedregions of PES, often involving most of the arterial cross-sectional circumference. In contradistinction, these observa-tions were rare for BMS samples (Figure 4D), in which onlydiffuse, small, and patchy para-strut amorphous materialswere seen.
Endothelium-Dependent and-Independent VasorelaxationThere were no between-group differences in lumen diametersin either proximal (PES, 3.07�0.34 mm versus BMS,
3.12�0.20 mm; P�0.678) or distal (PES, 2.98�0.37 mmversus BMS, 2.83�0.33 mm; P�0.392) NSRS at 1-monthfollow-up. No notable heart rate or mean blood pressurechanges were detected after injection of either sP ornitroglycerin.
Although vasodilatation occurred with both sP and nitro-glycerin, endothelium-dependent diameter change in re-sponse to the former was diminished for PES-stented arteriescompared with BMS. Diameter change was 0�6% for PES
Figure 3. A, Histological neointimal thickness (IT) was lower inPES than in BMS at 1 month after implantation. There were nodifferences in IT across segments for both PES and BMS. B,Histopathological intramural thrombi (MT score) was greater inPES than in BMS (P�0.01). There was no difference across sec-tions for BMS (P�0.597); however, the overlap section in PEShad higher MT than the proximal section (P�0.05).
Figure 4. Microscopic images of PES- and BMS-stented coro-nary arteries. A, Movat pentachrome staining (20�). Note: neo-intimal growth was much less in PES. B, C, and D,Hematoxylin-eosin staining (200�). In PES (B, C), the neointimais attenuated, with thrombus and fibrinoid deposits juxtaposedto SS. Flattened endothelial-like cells covered most of the lumi-nal surface, with occasional gaps. Several large round mononu-clear cells (inflammatory white blood cells; white arrows), as wellas luminal thrombus formation (black arrows), are observed. Themedia was necrotic and hemorrhagic in appearance (asterisk);inflammatory cell infiltrates (white arrows) were present in PESsegments. BMS (D) exhibited well-healed, thick fibrocellularneointima, completely covered with endothelial or endothelial-like cells. Only minute deposits of inspissated thrombus andfibrin deposits were observed.
32 Circ Cardiovasc Intervent August 2008
by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from
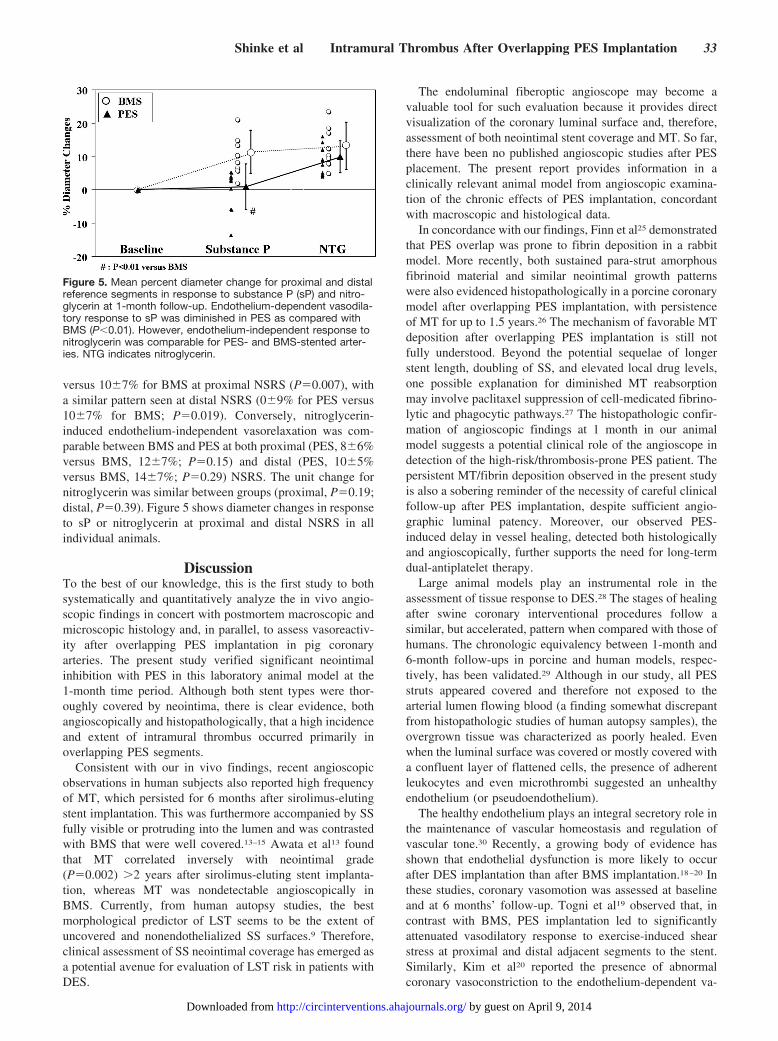
versus 10�7% for BMS at proximal NSRS (P�0.007), witha similar pattern seen at distal NSRS (0�9% for PES versus10�7% for BMS; P�0.019). Conversely, nitroglycerin-induced endothelium-independent vasorelaxation was com-parable between BMS and PES at both proximal (PES, 8�6%versus BMS, 12�7%; P�0.15) and distal (PES, 10�5%versus BMS, 14�7%; P�0.29) NSRS. The unit change fornitroglycerin was similar between groups (proximal, P�0.19;distal, P�0.39). Figure 5 shows diameter changes in responseto sP or nitroglycerin at proximal and distal NSRS in allindividual animals.
DiscussionTo the best of our knowledge, this is the first study to bothsystematically and quantitatively analyze the in vivo angio-scopic findings in concert with postmortem macroscopic andmicroscopic histology and, in parallel, to assess vasoreactiv-ity after overlapping PES implantation in pig coronaryarteries. The present study verified significant neointimalinhibition with PES in this laboratory animal model at the1-month time period. Although both stent types were thor-oughly covered by neointima, there is clear evidence, bothangioscopically and histopathologically, that a high incidenceand extent of intramural thrombus occurred primarily inoverlapping PES segments.
Consistent with our in vivo findings, recent angioscopicobservations in human subjects also reported high frequencyof MT, which persisted for 6 months after sirolimus-elutingstent implantation. This was furthermore accompanied by SSfully visible or protruding into the lumen and was contrastedwith BMS that were well covered.13–15 Awata et al13 foundthat MT correlated inversely with neointimal grade(P�0.002) �2 years after sirolimus-eluting stent implanta-tion, whereas MT was nondetectable angioscopically inBMS. Currently, from human autopsy studies, the bestmorphological predictor of LST seems to be the extent ofuncovered and nonendothelialized SS surfaces.9 Therefore,clinical assessment of SS neointimal coverage has emerged asa potential avenue for evaluation of LST risk in patients withDES.
The endoluminal fiberoptic angioscope may become avaluable tool for such evaluation because it provides directvisualization of the coronary luminal surface and, therefore,assessment of both neointimal stent coverage and MT. So far,there have been no published angioscopic studies after PESplacement. The present report provides information in aclinically relevant animal model from angioscopic examina-tion of the chronic effects of PES implantation, concordantwith macroscopic and histological data.
In concordance with our findings, Finn et al25 demonstratedthat PES overlap was prone to fibrin deposition in a rabbitmodel. More recently, both sustained para-strut amorphousfibrinoid material and similar neointimal growth patternswere also evidenced histopathologically in a porcine coronarymodel after overlapping PES implantation, with persistenceof MT for up to 1.5 years.26 The mechanism of favorable MTdeposition after overlapping PES implantation is still notfully understood. Beyond the potential sequelae of longerstent length, doubling of SS, and elevated local drug levels,one possible explanation for diminished MT reabsorptionmay involve paclitaxel suppression of cell-medicated fibrino-lytic and phagocytic pathways.27 The histopathologic confir-mation of angioscopic findings at 1 month in our animalmodel suggests a potential clinical role of the angioscope indetection of the high-risk/thrombosis-prone PES patient. Thepersistent MT/fibrin deposition observed in the present studyis also a sobering reminder of the necessity of careful clinicalfollow-up after PES implantation, despite sufficient angio-graphic luminal patency. Moreover, our observed PES-induced delay in vessel healing, detected both histologicallyand angioscopically, further supports the need for long-termdual-antiplatelet therapy.
Large animal models play an instrumental role in theassessment of tissue response to DES.28 The stages of healingafter swine coronary interventional procedures follow asimilar, but accelerated, pattern when compared with those ofhumans. The chronologic equivalency between 1-month and6-month follow-ups in porcine and human models, respec-tively, has been validated.29 Although in our study, all PESstruts appeared covered and therefore not exposed to thearterial lumen flowing blood (a finding somewhat discrepantfrom histopathologic studies of human autopsy samples), theovergrown tissue was characterized as poorly healed. Evenwhen the luminal surface was covered or mostly covered witha confluent layer of flattened cells, the presence of adherentleukocytes and even microthrombi suggested an unhealthyendothelium (or pseudoendothelium).
The healthy endothelium plays an integral secretory role inthe maintenance of vascular homeostasis and regulation ofvascular tone.30 Recently, a growing body of evidence hasshown that endothelial dysfunction is more likely to occurafter DES implantation than after BMS implantation.18–20 Inthese studies, coronary vasomotion was assessed at baselineand at 6 months’ follow-up. Togni et al19 observed that, incontrast with BMS, PES implantation led to significantlyattenuated vasodilatory response to exercise-induced shearstress at proximal and distal adjacent segments to the stent.Similarly, Kim et al20 reported the presence of abnormalcoronary vasoconstriction to the endothelium-dependent va-
Figure 5. Mean percent diameter change for proximal and distalreference segments in response to substance P (sP) and nitro-glycerin at 1-month follow-up. Endothelium-dependent vasodila-tory response to sP was diminished in PES as compared withBMS (P�0.01). However, endothelium-independent response tonitroglycerin was comparable for PES- and BMS-stented arter-ies. NTG indicates nitroglycerin.
Shinke et al Intramural Thrombus After Overlapping PES Implantation 33
by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from

sodilator acetylcholine more significantly in the distal epicar-dial segments of coronaries with PES than in those withBMS. This paradoxical pathophysiological vasoreactivitymay augment the vulnerability of DES-stented arteries toLST via exacerbation of flow stasis and turbulence andreduction of laminar flow and flow velocity.9,10 Such condi-tions would be expected to create a prothrombotic as well asproinflammatory vascular environment.
Our study is the first to evaluate endothelium-dependentand -independent vasorelaxation in combination with angio-scopic observation after overlapping PES implantation. Inter-estingly, despite normal luminal morphology of all targetedNSRS 1.5 cm proximal and distal to the SS, luminal diameterchange was significantly diminished in PES vessels as com-pared with BMS vessels. Although the exact mechanism forsuch vasomotor dysfunction in adjacent angioscopically nor-mal NSRS remains unclear, earlier studies have implicated adirect drug effect on endothelial repair.18–20 Drug diffusioninto the vessel wall may result in elution into the vasavasorum, thereby eventually reaching the adjacent arterialvessel wall, including the endothelium, beyond the stentedsegment. Further studies are needed to elucidate the mecha-nism of this mismatch phenomenon (normal angioscopic andhistological appearance with abnormal vasomotor function)in detail. Vasomotor function, as evaluated angiographicallyin response to vasodilator administration, may serve as animportant surrogate benchmark for vessel healing and func-tional recovery after DES in the clinical setting.
LimitationsFirst, the relatively small number of animal subjects shouldbe considered and the statistical data analysis interpretedaccordingly. Second, the current angioscope technology pro-vides a forward-viewing system only; complete circumferen-tial luminal surface visualization is limited. Conversely,optical coherence tomography provides high-resolutioncross-sectional imaging (at 10- to 20-�m pixel resolution) ofthe entire vasculature and may offer superior quantitativeevaluation of vascular responses to DES.31 However, differ-entiating thin neointimal growth from fibrin/thrombus depo-sition is not possible with optical coherence tomography atthe present time.
Biological results in normal porcine coronary arteries afterPES implantation may be not be representative of those in thediseased human coronary system, as the latter consists oflipid-rich atherosclerotic, and potentially thrombotic, stenoticlesions. In contrast to human postmortem findings, fullneointimal coverage was seen for both stent varieties in theporcine coronary model. Finally, serial long-term studies,with varying durations of angioscopic and histologicalfollow-up to evaluate neointimal coverage, thrombus burden,and vasomotor function, were not performed in the presentstudy; therefore, the later stages of structural and functionalrecovery after PES in this model remain unknown.
ConclusionsOur study demonstrated persistent MT and attenuated NC byfiberoptic angioscopy in porcine coronary arteries at sites ofoverlapping PES at 1 month after implantation. These in vivo
observations corresponded to macroscopic examination ofexcised, longitudinally transected stented coronary samplesand were furthermore related to histological findings ofpersistent MT and fibrinoid deposits in various layers of thevessel wall, including neointima and media. Furthermore,endothelium-dependent vasorelaxation was found to be im-paired in adjacent, angioscopically normal, proximal, anddistal NSRS. Our findings support the notion that toxiceffects of PES on the coronary endothelium and neointimaltissue exist, which may contribute to intractable vasospasmand, potentially by means of blood flow disturbance, to LSTclinically. The potential implications of these findings in thepathophysiology of human DES LST may be further eluci-dated in longer-term animal studies as well as in vivo humanangioscopic evaluation.
AcknowledgmentsThe authors express gratitude to Tetsuaki Li, MD, for his help inperforming angioscopy, Cynthia Baranowski and Lian Dorsey fortheir excellent technical assistance in preparation of histologicalsections, and Courtnye Billingsley for her assistance in managing thestudy execution.
Source of FundingThis study was funded by Saint Joseph’s Translational ResearchInstitute.
DisclosuresNone.
References1. Stettler C, Wandel S, Allemann S, Kastrati A, Morice MC, Schomig A,
Pfisterer ME, Stone GW, Leon MB, de Lezo JS, Goy JJ, Park SJ, SabateM, Suttorp MJ, Kelbaek H, Spaulding C, Menichelli M, Vermeersch P,Dirksen MT, Cervinka P, Petronio AS, Nordmann AJ, Diem P, Meier B,Zwahlen M, Reichenbach S, Trelle S, Windecker S, Juni P. Outcomesassociated with drug-eluting and bare-metal stents: a collaborativenetwork meta-analysis. Lancet. 2007;370:937–948.
2. Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice MC,Colombo A, Schampaert E, Grube E, Kirtane AJ, Cutlip DE, Fahy M,Pocock SJ, Mehran R, Leon MB. Safety and efficacy of sirolimus- andpaclitaxel-eluting coronary stents. N Engl J Med. 2007;356:998–1008.
3. Pendyala L, Jabara R, Shinke T, Chronos N, Robinson K, Li J, Hou D.Drug-eluting stents: present and future. Cardiovasc Hematol Agents MedChem. 2008;6:105–115.
4. Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G,Airoldi F, Chieffo A, Montorfano M, Carlino M, Michev I, Corvaja N,Briguori C, Gerckens U, Grube E, Colombo A. Incidence, predictors, andoutcome of thrombosis after successful implantation of drug-elutingstents. JAMA. 2005;293:2126–2130.
5. Pfisterer M, Brunner-La Rocca HP, Buser PT, Rickenbacher P, HunzikerP, Mueller C, Jeger R, Bader F, Osswald S, Kaiser C; BASKET-LATEInvestigators. Late clinical events after clopidogrel discontinuation maylimit the benefit of drug-eluting stents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol. 2006;48:2584–2591.
6. Kuchulakanti PK, Chu WW, Torguson R, Ohlmann P, Rha SW, ClavijoLC, Kim SW, Bui A, Gevorkian N, Xue Z, Smith K, Fournadjieva J,Suddath WO, Satler LF, Pichard AD, Kent KM, Waksman R. Correlatesand long-term outcomes of angiographically proven stent thrombosis withsirolimus- and paclitaxel-eluting stents. Circulation. 2006;113:1108–1113.
7. Daemen J, Wenaweser P, Tsuchida K, Abrecht L, Vaina S, Morger C,Kukreja N, Juni P, Sianos G, Hellige G, van Domburg RT, Hess OM,Boersma E, Meier B, Windecker S, Serruys PW. Early and late coronarystent thrombosis of sirolimus-eluting and paclitaxel-eluting stents inroutine clinical practice: data from a large two-institutional cohort study.Lancet. 2007;369:667–678.
34 Circ Cardiovasc Intervent August 2008
by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from
8. Joner M, Finn AV, Farb A, Mont EK, Kolodgie FD, Ladich E, Kutys R,Skorija K, Gold HK, Virmani R. Pathology of drug-eluting stents inhumans: delayed healing and late thrombotic risk. J Am Coll Cardiol.2006;48:193–202.
9. Finn AV, Joner M, Nakazawa G, Kolodgie F, Newell J, John MC, GoldHK, Virmani R. Pathological correlates of late drug-eluting stent throm-bosis: strut coverage as a marker of endothelialization. Circulation. 2007;115:2435–2441.
10. Finn AV, Nakazawa G, Joner M, Kolodgie FD, Mont EK, Gold HK,Virmani R. Vascular responses to drug eluting stents: importance ofdelayed healing. Arterioscler Thromb Vasc Biol. 2007;27:1500–1510.
11. Mauri L, Hsieh WH, Massaro JM, Ho KK, D’Agostino R, Cutlip DE.Stent thrombosis in randomized clinical trials of drug-eluting stents.N Engl J Med. 2007;356:1020–1029.
12. Uretsky BF, Denys BG, Counihan PC, Ragosta M. Angioscopic eval-uation of incompletely obstructing coronary intraluminal filling defects:comparison to angiography. Cathet Cardiovasc Diagn. 1994;33:323–329.
13. Awata M, Kotani J, Uematsu M, Morozumi T, Watanabe T, Onishi T,Iida O, Sera F, Nanto S, Hori M, Nagata S. Serial angioscopic evidenceof incomplete neointimal coverage after sirolimus-eluting stent implan-tation: comparison with bare-metal stents. Circulation. 2007;116:910–916.
14. Takano M, Yamamoto M, Xie Y, Murakami D, Inami S, Okamatsu K,Seimiya K, Ohba T, Seino Y, Mizuno K. Serial long-term evaluation ofneointimal stent coverage and thrombus after sirolimus-eluting stentimplantation by use of coronary angioscopy. Heart. 2007;93:1353–1356.
15. Kotani J, Awata M, Nanto S, Uematsu M, Oshima F, Minamiguchi H,Mintz GS, Nagata S. Incomplete neointimal coverage of sirolimus-elutingstents: angioscopic findings. J Am Coll Cardiol. 2006;47:2108–2111.
16. Ellis SG, Colombo A, Grube E, Popma J, Koglin J, Dawkins KD, StoneGW. Incidence, timing, and correlates of stent thrombosis with thepolymeric paclitaxel drug-eluting stent: a TAXUS II, IV, V, and VImeta-analysis of 3,445 patients followed for up to 3 years. J Am CollCardiol. 2007;49:1043–1051.
17. Weissman NJ, Ellis SG, Grube E, Dawkins KD, Greenberg JD, Mann T,Cannon LA, Cambier PA, Fernandez S, Mintz GS, Mandinov L, KoglinJ, Stone GW. Effect of the polymer-based, paclitaxel-eluting TAXUSExpress stent on vascular tissue responses: a volumetric intravascularultrasound integrated analysis from the TAXUS IV, V, and VI trials. EurHeart J. 2007;28:1574–1582.
18. Hofma SH, van der Giessen WJ, van Dalen BM, Lemos PA, McFaddenEP, Sianos G, Ligthart JM, van Essen D, de Feyter PJ, Serruys PW.Indication of long-term endothelial dysfunction after sirolimus-elutingstent implantation. Eur Heart J. 2006;27:166–170.
19. Togni M, Raber L, Cocchia R, Wenaweser P, Cook S, Windecker S,Meier B, Hess OM. Local vascular dysfunction after coronary paclitaxel-eluting stent implantation. Int J Cardiol. 2007;120:212–220.
20. Kim JW, Suh SY, Choi CU, Na JO, Kim EJ, Rha SW, Park CG, Seo HS,Oh DJ. Six-month comparison of coronary endothelial dysfunction asso-ciated with sirolimus-eluting stent versus paclitaxel-eluting stent. J AmColl Cardiol Intv. 2008;1:65–71.
21. Sakai S, Mizuno K, Yokoyama S, Tanabe J, Shinada T, Seimiya K,Takano M, Ohba T, Tomimura M, Uemura R, Imaizumi T. Morphologicchanges in infarct-related plaque after coronary stent placement: a serialangioscopy study. J Am Coll Cardiol. 2003;42:1558–1565.
22. den Heijer P, Foley DP, Hillege HL, Lablanche JM, van Dijk RB, FranzenD, Morice MC, Serra A, de Scheerder IK, Serruys PW. The “Erm-enonville” classification of observations at coronary angioscopy: eval-uation of intra- and inter-observer agreement: European Working Groupon Coronary Angioscopy. Eur Heart J. 1994;15:815–822.
23. Hong MK, Kornowski R, Bramwell O, Ragheb AO, Leon MB. Paclitaxel-coated Gianturco-Roubin II (GR II) stents reduce neointimal hyperplasiain a porcine coronary in-stent restenosis model. Coron Artery Dis. 2001;12:513–515.
24. Ohwada T, Saito T, Saitoh S, Osugi T, Ohtake A, Maehara K, IshibashiT, Maruyama Y. Specificity of vascular reactivity and remodeling afterrepeated endothelial injury in a swine model. Int Heart J. 2006;47:297–310.
25. Finn AV, Kolodgie FD, Harnek J, Guerrero LJ, Acampado E, Tefera K,Skorija K, Weber DK, Gold HK, Virmani R. Differential response ofdelayed healing and persistent inflammation at sites of overlappingsirolimus- or paclitaxel-eluting stents. Circulation. 2005;112:270–278.
26. Wilson GJ, Polovick JE, Huibregtse BA, Poff BC. Overlappingpaclitaxel-eluting stents: long-term effects in a porcine coronary arterymodel. Cardiovasc Res. 2007;76:361–372.
27. Seifert P, Huibregtse BA, Polovick J, Poff B. Early vascular response tooverlapped paclitaxel-eluting stents in swine coronary arteries. Car-diovasc Revasc Med. 2007;8:251–258.
28. Schwartz RS, Edelman ER, Carter A, Chronos N, Rogers C, RobinsonKA, Waksman R, Weinberger J, Wilensky RL, Jensen DN, ZuckermanBD, Virmani R; Consensus Committee. Drug-eluting stents in preclinicalstudies: recommended evaluation from a consensus group. Circulation.2002;106:1867–1873.
29. Suzuki T, Kopia G, Hayashi S, Bailey LR, Llanos G, Wilensky R,Klugherz BD, Papandreou G, Narayan P, Leon MB, Yeung AC, Tio F,Tsao PS, Falotico R, Carter AJ. Stent-based delivery of sirolimus reducesneointimal formation in a procine coronary model. Circulation. 2001;104:1188–1193.
30. Hou D, Narciso H, Kamdar K, Zhang P, Barclay B, March KL. Reducingneointimal proliferation by a stent-based delivery of nitric oxide in aporcine carotid overstretch injury model. Cardiovasc Intervent Radiol.2005;28:60–65.
31. Matsumoto D, Shite J, Shinke T, Otake H, Tanino Y, Ogasawara D,Sawada T, Paredes OL, Hirata K, Yokoyama M. Neointimal coverage ofsirolimus-eluting stents at 6-month follow-up: evaluated by opticalcoherence tomography. Eur Heart J. 2007;28:961–967.
CLINICAL PERSPECTIVEIn the current era of drug-eluting stent (DES) use for interventional cardiology, the importance of accurate and appropriateintravascular imaging for optimal patient monitoring, prognosis, and management has gained special prominence.Intravascular ultrasound is accepted as a standard clinical imaging modality, whereas optical coherence tomography andfiberoptic angioscopy are still considered research tools in many countries, including the United States. Although DES arehighly effective for in-stent restenosis suppression, they carry a small but real risk of late stent thrombosis (LST). Certainpatient and lesion characteristics appear to be associated with increased risk of LST for DES, yet there are currently noconsensus methods by which specific DES implantation sites may be identified as having high LST potential. Angioscopyallows direct visualization of the arterial luminal surface and thereby supplies image information that cannot be providedby intravascular ultrasound or optical coherence tomography. In this study, we have demonstrated that the angioscopicappearance of DES 1 month after implantation in porcine coronary arteries is distinct from the appearance of bare metalstents. In parallel, we have shown that DES are histologically identified as having less complete healing, with persistentintramural thrombus and poor endothelial functional recovery as compared with bare metal stents; such phenomena havebeen related to LST of DES in autopsy studies. Our findings support the use of the angioscope as a means to identify, withan intravascular imaging modality, those stent implants which may be predisposed to LST. Such information may bevaluable to the practicing clinician in managing patients with DES.
Shinke et al Intramural Thrombus After Overlapping PES Implantation 35
by guest on April 9, 2014http://circinterventions.ahajournals.org/Downloaded from




















