
Recombinative events of the T cell antigen receptor delta gene in peripheral T cell lymphomas
Upload
khangminh22Category
view
0download
0
Hematopathology / HISTOPATHOLOGIC FEATURES OF SPLENIC SMALL B-CELL LYMPHOMAS
Histopathologic Features of Splenic Small B-CellLymphomas
A Study of 42 Cases With a Definitive Diagnosis by the World Health Organization Classification
Rina Kansal, MD, Charles W. Ross, MD, Timothy P. Singleton, MD, William G. Finn, MD, and Bertram Schnitzer, MD
Key Words: Splenic lymphoma; Marginal zone; Small B-cell; Mantle cell lymphoma; Follicular lymphoma; Chronic lymphocytic leukemia;Small lymphocytic lymphoma; WHO classification
DOI: 10.1309/HWG084N3F3LRJ8XB
A b s t r a c t
We studied 42 cases of splenic small B-celllymphoma (SBL) (21 women, 21 men; aged 32-82 years;median, 65 years) with a definitive diagnosis by theWorld Health Organization classification: chroniclymphocytic leukemia (CLL), 8; mantle cell lymphoma(MCL), 9; follicular lymphoma (FL), 12; marginal zonelymphoma, 13 (splenic [SMZL], 12; extranodal[EMZL], 1). Splenectomy was performed for diagnosisor therapy; splenic weights were 0.2 to 3.8 kg (median,1.4 kg). In general, splenic SBLs showed white pulp(WP) expansion; morphologic features of the nodulesrecapitulated the corresponding lymph nodehistopathologic features. “Marginal zones” wereobserved commonly in SMZL and FL, may be present inMCL involving the spleen, and may be seen in hilarlymph nodes (HLNs) in SBLs other than SMZL. FL maysimulate SMZL and can be distinguished by the presenceof neoplastic follicles and HLN morphologic features.Extracellular hyaline deposits (EH) are common in FLand SMZL. MCL typically shows WP expansion by amonotonous small lymphocytic infiltrate, without diffusered pulp (RP) infiltration or EH; leukemic MCL mayshow RP infiltration. Splenic morphologic features inCLL vary in WP or RP dominance; marginal zonesusually are not observed in CLL.
Malignant lymphomas commonly involve the spleensecondarily as part of generalized disease.1,2 Occasionally,lymphomas manifest with prominent splenomegaly, with orwithout overt evidence of lymphadenopathy, and a splenec-tomy is performed for diagnostic purposes.3-7
Small B-lymphocytic neoplasms are conceptualized asclonal proliferations of mature small B-lymphocytes, withdifferent subtypes arising from various stages in the life ofa mature B cell.8 The differential diagnosis of small B-celllymphomas (SBLs) involving the spleen can be difficult,especially in cases with prominent splenomegaly only, inwhich no additional diagnostic interpretation can be madefrom a lymph node biopsy specimen. The significant differ-ences in therapy and prognosis within various subclasses ofSBLs mandate precise diagnostic subclassification.9 Whilea number of studies have focused on marginal zonelymphomas of the spleen, few studies have compared thedifferent subtypes of splenic SBL after the description ofsplenic marginal zone lymphomas.10-12 In the most recentstudy by Piris et al,12 the primary diagnosis in 11 of 33study cases was made by peripheral blood examinationalone, with no supportive flow cytometric immunopheno-typic or lymph node histopathologic evidence for the diag-noses of 9 chronic lymphocytic leukemias and 2 mantlecell lymphomas.
The objective of our study was to define the morphologicfeatures of SBL involving the spleen by studying the cases ofsplenic SBL in which a definitive diagnosis and subclassifica-tion was established according to the recent World HealthOrganization (WHO) classification, after integrating all avail-able clinical and pathologic information.
Am J Clin Pathol 2003;120:335-347 335335 DOI: 10.1309/HWG084N3F3LRJ8XB 335
© American Society for Clinical Pathology
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Kansal et al / HISTOPATHOLOGIC FEATURES OF SPLENIC SMALL B-CELL LYMPHOMAS
Materials and Methods
Case Selection
The surgical pathology laboratory information system atthe University of Michigan, Ann Arbor, was searched forlymphomas involving the spleen from January 1980 to May2001. Sections of all cases of splenic lymphomas retrieved inthe search were reviewed (R.K, B.S.) to exclude cases ofHodgkin lymphoma, diffuse large B-cell lymphoma, T-cellneoplasms, and follicular lymphoma, grade 3, involving thespleen. The case cohort reflects sequential patients withsplenic SBL who received treatment at the University ofMichigan. The diagnostic paraffin-embedded, B5- orformalin-fixed, H&E-stained sections of the spleen, lymphnode or bone marrow biopsies, immunohistochemical stains,peripheral blood smears, and corresponding flow cytometricdata and clinical information were reviewed. The diagnostichistologic sections in all cases were reviewed by at least 3pathologists (R.K., C.W.R., B.S.). The dot plots for all flowcytometric immunophenotypic analyses were reviewed by atleast 2 pathologists (R.K., C.W.R.). All cases included in thestudy were classified according to currently acceptedcriteria,13,14 with specific inclusion criteria as follows:
B-Cell Chronic Lymphocytic Leukemia/Small LymphocyticLymphoma
All patients with B-cell chronic lymphocytic leukemia(CLL) had absolute lymphocytosis and involvement ofperipheral blood and bone marrow at the time of diagnosis,with morphologic and flow cytometric immunophenotypicfeatures characteristic of CLL. By flow cytometry, featurestypical for CLL/small lymphocytic lymphoma (SLL)included expression of CD5, dim or absent CD11c, usuallydim CD20, dim or absent CD22, CD23, dim surfaceimmunoglobulin expression, and dim or absent FMC7 on theneoplastic cells.15 One case of CLL with increased (18%)prolymphocytes14,16,17 was included in this category. Casesclassified as SLL had a diagnostic lymph node biopsyshowing histologic features on H&E-stained sections diag-nostic of this subclassification.
Mantle Cell LymphomaAll cases had a peripheral or hilar lymph node (HLN)
biopsy specimen available for review, with features diagnosticof mantle cell lymphoma (MCL). The lymphoma cells werecyclin D1+ by immunohistochemical analysis in all cases.
Follicular LymphomaAll cases had a peripheral or HLN biopsy specimen
available for review, with histopathologic features diagnosticof follicular lymphoma (FL), grades 1 or 2.
Marginal Zone Lymphoma
Patients given a diagnosis of splenic marginal zonelymphoma (SMZL) underwent diagnostic splenectomy forextramedullary tissue diagnosis and subclassification andhad no involvement of extranodal sites, as determined byreview of all available information in the patients’ medicalrecords. One MZL case with previous involvement of extra-nodal sites was classified as extranodal MZL (EMZL) subse-quently involving the spleen. We did not find any case ofsplenectomy performed for a nodal MZL in our study.Splenic histopathologic features on H&E-stained sectionswere as described in the WHO classification.14 In addition,all cases had peripheral blood or HLN specimens availablefor review, with features consistent with or typical of MZL.In all selected cases, features specific for other subtypes ofSBL were absent, including neoplastic follicles or prolifera-tion centers in histologic sections, circulating cleavedlymphoma cells evident by peripheral blood smear morpho-logic examination, and bone marrow morphologic and clin-ical features typical for lymphoplasmacytic lymphoma/Waldenström macroglobulinemia. The neoplastic cells in allcases were negative for CD5 and for CD10 by immunoper-oxidase stains on paraffin-embedded sections or by multi-color flow cytometric immunophenotypic analysis. CD23positivity in cases with features otherwise consistent withMZL and with absence of features that would suggestCLL/SLL did not exclude the diagnosis of MZL; 2 suchcases with CD23 positivity by flow cytometry were included.In all cases with available sections, the lymphoma cells werenegative for cyclin D1 by immunohistochemical analysis; 3cases without available sections for a cyclin D1 stain wereincluded. We did not find any cyclin D1+ case in our studywith histologic features typical for MZL.
Excluded CasesOnly 1 patient with a definitive diagnosis of lympho-
plasmacytic lymphoma/Waldenström macroglobulinemiaunderwent splenectomy in our series of cases, and this diag-nostic category was, therefore, excluded. Cases with unavail-able or inadequate diagnostic material for review wereexcluded; these cases included 3 suspected FLs and 1suspected lymphoplasmacytic lymphoma. One SBL caseinvolving peripheral blood and bone marrow, with clinicaland pathologic features suggesting SMZL, was excludedbecause the resected spleen consisted predominantly ofnonviable tissue.
Pathologic Features and Immunohistochemical Analysis
The weight of the spleen and significant macroscopicfindings were recorded from the original pathology reports.Histopathologic features studied in the spleen included thepresence and extent of white pulp (WP) expansion, presence
336 Am J Clin Pathol 2003;120:335-347336 DOI: 10.1309/HWG084N3F3LRJ8XB
© American Society for Clinical Pathology
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Am J Clin Pathol 2003;120:335-347 337337 DOI: 10.1309/HWG084N3F3LRJ8XB 337
© American Society for Clinical Pathology
Hematopathology / ORIGINAL ARTICLE
or absence of residual germinal centers (GCs), extracellularhyaline deposits in the WP, presence of a “marginal zone”(MZ) pattern, presence of red pulp (RP) infiltration (nodularor diffuse), and the cytologic composition of the neoplasticcell population. Splenic HLN sections were reviewed, whenavailable, to assess nodal architecture, preservation ofsinuses, presence of a MZ pattern, and the cytologic featuresof neoplastic cells. In cases with involvement of the periph-eral blood or bone marrow, the available smears and sectionswere reviewed. The H&E- and immunohistochemicallystained sections of all diagnostic lymph node biopsies werereviewed to confirm the diagnoses.
Additional paraffin section immunoperoxidase stainswere performed, if necessary, to confirm the diagnoses. Acyclin D1 immunoperoxidase stain was performed in allcases of MCL and MZL with available sections. Allimmunostains used an automated stainer (Ventana, Tucson,AZ). The antibodies (clone, source) and antigen retrievalmethods used are listed in ❚Table 1❚. For antigen retrieval,sections were microwaved in a 10-mmol/L concentration ofcitrate buffer, pH 6.0, for 10 or 15 minutes or microwaved ina 0.25-mol/L tris(hydroxymethyl)aminomethane–0.1-mmol/L EDTA solution, pH 9.0, for 15 minutes, or digestedwith protease (Protease 1, Ventana) for 16 minutes.
Flow Cytometric Immunophenotyping
Flow cytometric immunophenotypic analysis oflymphoma cells was performed in 44 specimens from 32patients in the study. For 9 patients (CLL, 1; MCL, 3; FL, 1;SMZL, 4) more than 1 specimen source was analyzed byflow cytometry. The 44 specimens analyzed included 16peripheral blood samples (CLL, 5; SMZL, 5; MCL, 4; FL,2), 14 spleens (SMZL, 8; CLL, 2; MCL, 2; FL, 2), 11 bonemarrow aspirates (SMZL, 4; MCL, 3; CLL/SLL, 2; FL, 1;EMZL, 1), 2 lymph nodes (FL, 1; MCL, 1), and 1 pleuralfluid sample (FL).
The specimens were analyzed using an EPICS XL-MCLflow cytometer (Beckman Coulter, Miami, FL), using multi-color analysis and previously described methods15 for the
majority of cases in the study. Cells from lymph nodes andsplenic tissue were obtained by mechanical disaggregation.The antibodies with the directly conjugated fluorochromesused for flow cytometry included the following: CD5/phyco-erythrin (PE; Becton Dickinson, San Jose, CA), CD10/fluo-rescein isothiocyanate (FITC; Becton Dickinson), CD11c/PE(Immunotech, Miami, FL), CD19/PE (Immunotech),CD20/FITC (Becton Dickinson), CD22/FITC (Immunotech),CD23/PE (Becton Dickinson), CD25/FITC (Immunotech),CD45/ECD (Immunotech), CD103/PE (Immunotech),FMC7/FITC (Immunotech), κ/FITC (Becton Dickinson), andλ/PE (Becton Dickinson).
A surface antigen was considered positive if at least 20%of the neoplastic cells showed flow cytometric immunofluo-rescence in excess of an isotype-matched negative control.The flow cytometry dot plots were reviewed in all cases. Allcases had immunoglobulin light chain restriction diagnosticof lymphoma. For CD20 and surface immunoglobulins, theintensity of fluorescence was reported as dim if the meanfluorescence intensity was within the first positive loga-rithmic decade and as bright if the mean fluorescence inten-sity was in the second or third logarithmic decade.
Statistical Analysis
The Fisher exact probability test was applied to test forsignificant histologic differences in the SBL subtypes, usingSPSS for Windows, version 10.1 (SPSS, Chicago, IL). Thesubtypes analyzed were MZL vs CLL/SLL, MZL vs MCL,and MZL vs FL. For the purpose of statistical analysis, theEMZL case was combined with the 12 SMZL cases. Thehistologic variables were considered positive or negative;focal positivity, as in focally effaced HLN sinuses, and rarelyobserved histologic variables were considered positive. A Pvalue of less than .05 indicated a statistically significantdifference.
Clinical Information
Clinical information was obtained by medical chartreview in all cases. Patient age and sex, stage of disease,
❚Table 1❚Immunoperoxidase Stains
Antigen Antibody Clone Source Pretreatment
CD3ε Polyclonal DAKO, Carpinteria, CA 15 min, citrate, microwaveCD5 4C7 Novocastra, Burlingame, CA Tris-EDTA, microwaveCD10 56C6 Novocastra Tris-EDTA, microwaveCD20 L26 DAKO 15 min, citrate, microwaveCD23 BU38 The Binding Site, San Diego, CA 16 min, Protease 1 (Ventana, Tucson, AZ)CD43 L60 Becton Dickinson, San Jose, CA 15 min, citrate, microwaveCyclin D1 AM29 Zymed, South San Francisco, CA Tris-EDTA, microwaveκ Polyclonal DAKO 10 min, citrate, microwaveλ Polyclonal DAKO 10 min, citrate, microwave
Tris, tris(hydroxymethyl)aminomethane.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022
Kansal et al / HISTOPATHOLOGIC FEATURES OF SPLENIC SMALL B-CELL LYMPHOMAS
presence of involvement of lymph nodes and bone marrow,and the clinical indications for splenectomy were recorded inall cases, with the available follow-up information. “Diag-nostic” intent included splenectomies performed for specificsubclassification of lymphoma, following a suspected orconfirmed diagnosis of a lymphoproliferative disorder byperipheral blood or bone marrow examination.
Results
Pathologic Features
Forty-two cases that met the aforementioned criteriawere included. ❚Table 2❚ shows a summary of the pathologicfeatures, including the median spleen weights, numbers ofcases with the studied histologic features in the spleen andsplenic HLNs, and numbers of cases with a diagnostic lymphnode biopsy or supportive flow cytometric immunopheno-typic analysis, in the different lymphoma subtypes.
The splenic gross features were available for 31 cases.For all cases, the spleen weight range was 0.2 to 3.8 kg(median, 1.4 kg). For each subtype of lymphoma, the spleenweight ranges were as follows: CLL, 0.2 to 1.4 kg; MCL, 0.9to 3.8 kg; FL, 0.6 to 1.9 kg; and MZL, 0.6 to 3.1 kg. Bygross examination, prominence of the WP was reported in 28of 31 cases (CLL, 3/6; MCL, 7/7; FL, 8/8; MZL, 10/10). Amiliary pattern was reported in 23 cases (CLL, 3; MCL, 7;FL, 6; MZL, 7). Occasional WP nodules up to 0.6 cm indiameter were noted in 1 case of CLL. Multiple fleshynodules up to 2.5 cm in diameter were described in 2 cases
of MCL. WP nodules in MZL were reported to measure upto 0.5 cm in diameter. Prominent expansion of the RP wasreported in 3 cases of CLL.
Histopathologic Features
B-Cell Chronic Lymphocytic Leukemia/Small LymphocyticLymphoma (n = 8)
Microscopically, there was expansion of the WP ❚Image
1A❚ in all cases, primarily by small, mature-appearinglymphocytes admixed with scattered, larger cells with round,vesicular nuclei and distinct, central nucleoli (paraim-munoblasts) ❚Image 1B❚. In cases 1 and 5, these larger cellswere clustered into aggregates referred to as “proliferationcenters,” often highlighted by an immunohistochemical stainfor CD23. In case 4, the lymphoid infiltrate included a fewlymphocytes with angulated nuclei in addition to smalllymphocytes with round nuclear contours. Infiltration of theRP was present in all cases ❚Image 1C❚ and ❚Image 1D❚ andwas predominantly nodular in 1 case, predominantly diffusein 3 cases, and nodular and diffuse in 4 cases. A rare GC wasidentified in 1 case, with occasional GCs in 2 additionalcases. Extracellular hyaline deposition usually was absent.MZs were not observed in the spleen or splenic HLNs.
All available splenic HLNs showed at least partialeffacement of the nodal architecture, with completeeffacement in 4 cases, due to an infiltrate composedprimarily of small lymphocytes admixed with scatteredparaimmunoblasts. Proliferation centers were identified inHLNs from 2 cases, one of which also had the samefeature in the spleen.
338 Am J Clin Pathol 2003;120:335-347338 DOI: 10.1309/HWG084N3F3LRJ8XB
© American Society for Clinical Pathology
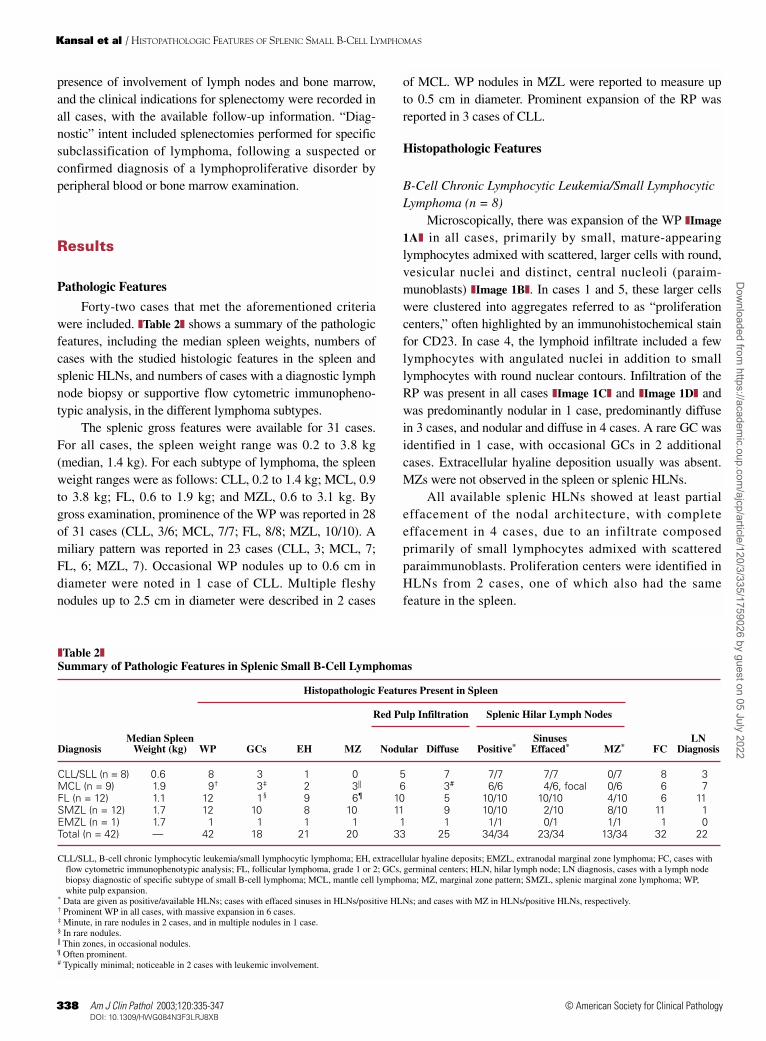
❚Table 2❚Summary of Pathologic Features in Splenic Small B-Cell Lymphomas
Histopathologic Features Present in Spleen
Red Pulp Infiltration Splenic Hilar Lymph Nodes
Median Spleen Sinuses LNDiagnosis Weight (kg) WP GCs EH MZ Nodular Diffuse Positive* Effaced* MZ* FC Diagnosis
CLL/SLL (n = 8) 0.6 8 3 1 0 5 7 7/7 7/7 0/7 8 3MCL (n = 9) 1.9 9† 3‡ 2 3|| 6 3# 6/6 4/6, focal 0/6 6 7FL (n = 12) 1.1 12 1§ 9 6¶ 10 5 10/10 10/10 4/10 6 11SMZL (n = 12) 1.7 12 10 8 10 11 9 10/10 2/10 8/10 11 1EMZL (n = 1) 1.7 1 1 1 1 1 1 1/1 0/1 1/1 1 0Total (n = 42) — 42 18 21 20 33 25 34/34 23/34 13/34 32 22
CLL/SLL, B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma; EH, extracellular hyaline deposits; EMZL, extranodal marginal zone lymphoma; FC, cases withflow cytometric immunophenotypic analysis; FL, follicular lymphoma, grade 1 or 2; GCs, germinal centers; HLN, hilar lymph node; LN diagnosis, cases with a lymph nodebiopsy diagnostic of specific subtype of small B-cell lymphoma; MCL, mantle cell lymphoma; MZ, marginal zone pattern; SMZL, splenic marginal zone lymphoma; WP,white pulp expansion.
* Data are given as positive/available HLNs; cases with effaced sinuses in HLNs/positive HLNs; and cases with MZ in HLNs/positive HLNs, respectively.† Prominent WP in all cases, with massive expansion in 6 cases.‡ Minute, in rare nodules in 2 cases, and in multiple nodules in 1 case.§ In rare nodules.|| Thin zones, in occasional nodules.¶ Often prominent.# Typically minimal; noticeable in 2 cases with leukemic involvement.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Hematopathology / ORIGINAL ARTICLE
Mantle Cell Lymphoma (n = 9)
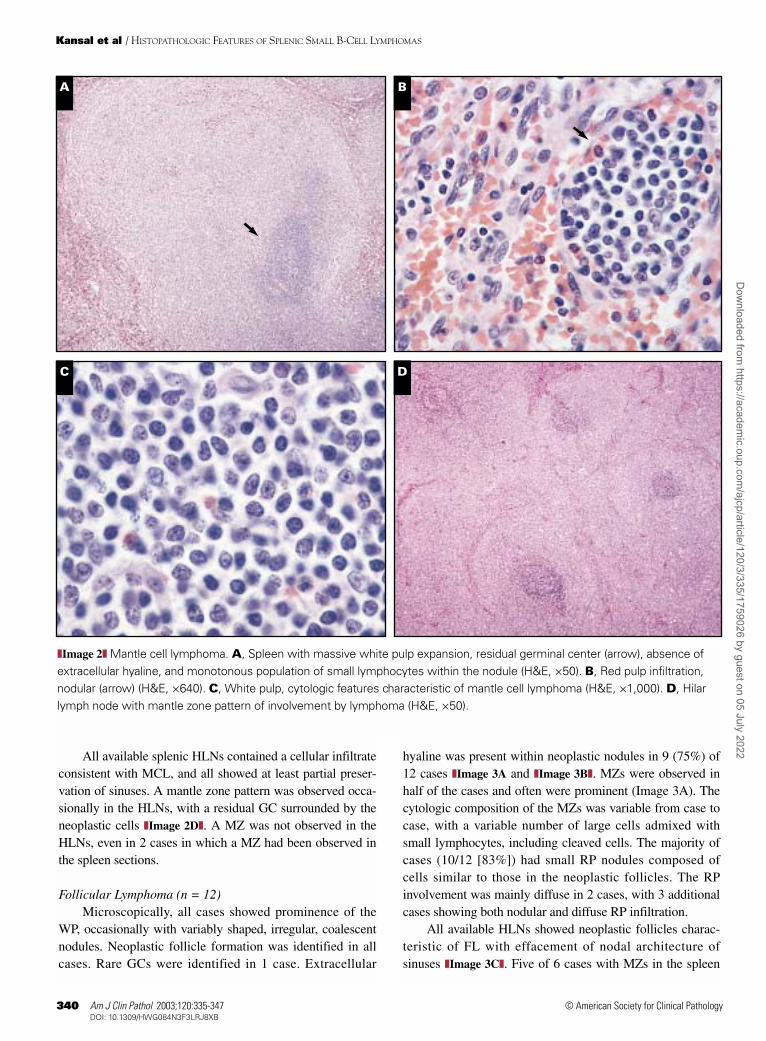
Microscopically, the WP was expanded in all cases, withmassive expansion in 6 cases ❚Image 2A❚ in the form of vari-ably sized, focally coalescent nodules. Near-total effacementof architecture by these massive nodules with minimal inter-vening RP corresponded to the macroscopic fleshy nodulesreported in 2 cases. Infiltration of the RP by lymphoma waspresent in the form of small nodules ❚Image 2B❚, typicallywith minimal diffuse infiltration. In cases 16 and 17, diffuseRP infiltration was noted; both of these cases had a moderateabsolute peripheral blood lymphocytosis as well. GCs werevery small (Image 2A) and rare in 2 cases and were presentin multiple nodules in 1 case. In this latter case, a triphasic
pattern was present with a central GC, an intermediate darkerzone of small lymphocytes, and an outer lighter MZ. Extra-cellular hyaline was noted within a GC in 1 case and within aneoplastic nodule in 1 case. Thin MZs were present in occa-sional nodules in the spleen in 3 cases. The neoplastic cellsin all cases included predominantly small lymphocytes withscant cytoplasm and variably irregular nuclear contours, rela-tively coarsely clumped chromatin, and indistinct nucleolicharacteristic of MCL ❚Image 2C❚. Scattered or clusteredpale histiocytes were present within the neoplastic infiltratein all cases. One case classified as the blastoid variant ofMCL had larger cells with more finely distributed nuclearchromatin and prominent mitotic activity.
Am J Clin Pathol 2003;120:335-347 339339 DOI: 10.1309/HWG084N3F3LRJ8XB 339
© American Society for Clinical Pathology
A B
C D
❚Image 1❚ B-cell chronic lymphocytic leukemia (CLL). A, Spleen with irregular white pulp expansion, absence of marginal zones(H&E, ×25). B, Splenic white pulp with scattered paraimmunoblasts (H&E, ×400). C, Red pulp infiltration, nodular (arrow), bysmall lymphocytes (H&E, ×400). D (Case 6), CLL with increased prolymphocytes. Spleen, red pulp infiltration, diffuse, by smalllymphocytes and paraimmunoblasts (H&E, ×640); inset, circulating prolymphocytes in the same case (Wright-Giemsa, ×1,000)
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022
340 Am J Clin Pathol 2003;120:335-347340 DOI: 10.1309/HWG084N3F3LRJ8XB
© American Society for Clinical Pathology
Kansal et al / HISTOPATHOLOGIC FEATURES OF SPLENIC SMALL B-CELL LYMPHOMAS
All available splenic HLNs contained a cellular infiltrateconsistent with MCL, and all showed at least partial preser-vation of sinuses. A mantle zone pattern was observed occa-sionally in the HLNs, with a residual GC surrounded by theneoplastic cells ❚Image 2D❚. A MZ was not observed in theHLNs, even in 2 cases in which a MZ had been observed inthe spleen sections.
Follicular Lymphoma (n = 12)Microscopically, all cases showed prominence of the
WP, occasionally with variably shaped, irregular, coalescentnodules. Neoplastic follicle formation was identified in allcases. Rare GCs were identified in 1 case. Extracellular
hyaline was present within neoplastic nodules in 9 (75%) of12 cases ❚Image 3A and ❚Image 3B❚. MZs were observed inhalf of the cases and often were prominent (Image 3A). Thecytologic composition of the MZs was variable from case tocase, with a variable number of large cells admixed withsmall lymphocytes, including cleaved cells. The majority ofcases (10/12 [83%]) had small RP nodules composed ofcells similar to those in the neoplastic follicles. The RPinvolvement was mainly diffuse in 2 cases, with 3 additionalcases showing both nodular and diffuse RP infiltration.
All available HLNs showed neoplastic follicles charac-teristic of FL with effacement of nodal architecture ofsinuses ❚Image 3C❚. Five of 6 cases with MZs in the spleen
A B
C D
❚Image 2❚ Mantle cell lymphoma. A, Spleen with massive white pulp expansion, residual germinal center (arrow), absence ofextracellular hyaline, and monotonous population of small lymphocytes within the nodule (H&E, ×50). B, Red pulp infiltration,nodular (arrow) (H&E, ×640). C, White pulp, cytologic features characteristic of mantle cell lymphoma (H&E, ×1,000). D, Hilarlymph node with mantle zone pattern of involvement by lymphoma (H&E, ×50).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Am J Clin Pathol 2003;120:335-347 341341 DOI: 10.1309/HWG084N3F3LRJ8XB 341
© American Society for Clinical Pathology
Hematopathology / ORIGINAL ARTICLE
had HLNs available for review, and 4 of these HLNs alsoshowed MZs ❚Image 3D❚.
Marginal Zone Lymphoma (n = 13)Twelve of 13 cases were classified as SMZL and 1 case
(case 35) as EMZL involving the orbit and breast, withsubsequent involvement of the spleen 14 years after theinitial diagnosis. One case (case 31) had a cervical lymphnode involved by MZL 10 years after the splenectomy. Clini-cally, 25% of patients with SMZL had a history of animmunologic disorder (cases 30, 36, and 42).
Microscopically, all cases showed WP expansion ❚Image
4A❚, usually in the form of round nodules and often with
numerous smaller nodules in the RP. Very uniform-sizednodules were noted in case 32. MZs were observed in thespleen in 11 of 13 cases. A biphasic pattern was identified inat least a few nodules in the majority of cases, ie, a centralvariably thick zone of small lymphocytes surrounded by avariably thick paler zone (MZ) of small lymphocytes withmore abundant cytoplasm ❚Image 4B❚. Small residual GCswithin these nodules, present in 11 of 13 cases, occasionallyimparted a triphasic appearance. The proportion of small andlarge lymphoid cells within the MZs was variable in differentcases. One case with limited sections for review (case 30)showed predominantly small nodules in the RP and fewenlarged WP nodules with MZs. Extracellular hyaline
A B
C D
❚Image 3❚ Follicular lymphoma. A, Spleen with uniform white pulp expansion, prominent marginal zones, and frequentextracellular hyaline deposits (H&E, ×25). B, White pulp with extracellular hyaline deposition between small cleaved cells, andsurrounding marginal zone at the corner of the photomicrograph (arrows) (H&E, ×400). C, Hilar lymph node with effaced sinuses(H&E, ×25). D, Hilar lymph node with a rim of marginal zone (outlined by arrows) surrounding the neoplastic follicle (H&E, ×400).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022
Kansal et al / HISTOPATHOLOGIC FEATURES OF SPLENIC SMALL B-CELL LYMPHOMAS
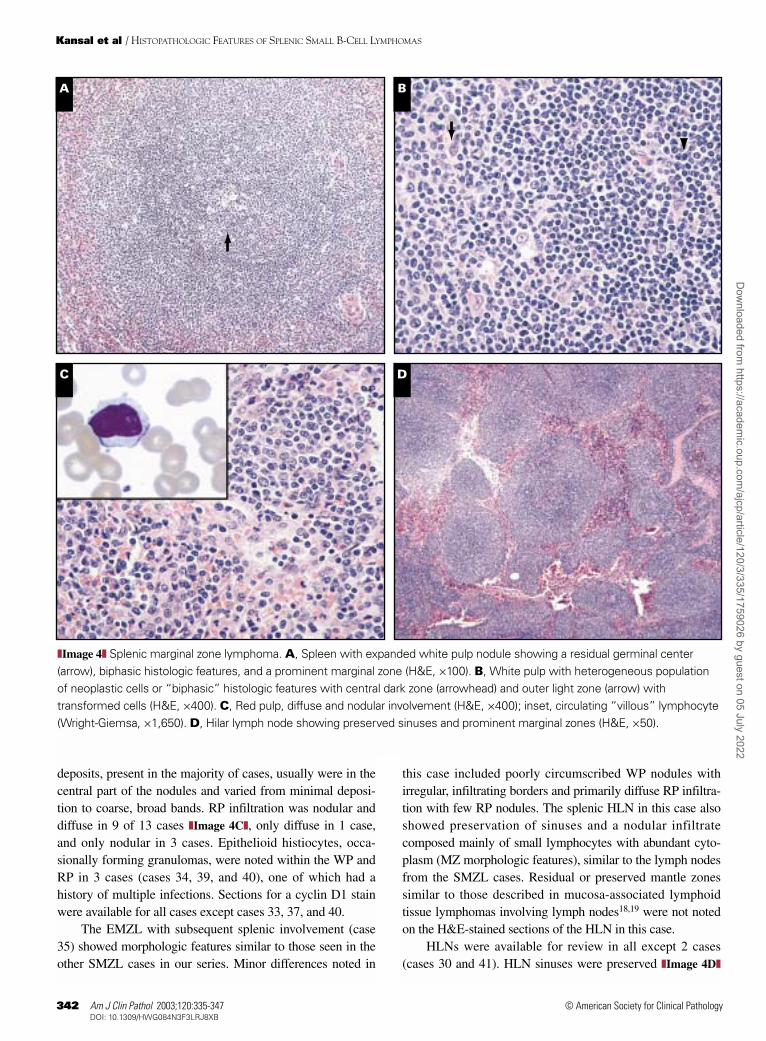
deposits, present in the majority of cases, usually were in thecentral part of the nodules and varied from minimal deposi-tion to coarse, broad bands. RP infiltration was nodular anddiffuse in 9 of 13 cases ❚Image 4C❚, only diffuse in 1 case,and only nodular in 3 cases. Epithelioid histiocytes, occa-sionally forming granulomas, were noted within the WP andRP in 3 cases (cases 34, 39, and 40), one of which had ahistory of multiple infections. Sections for a cyclin D1 stainwere available for all cases except cases 33, 37, and 40.
The EMZL with subsequent splenic involvement (case35) showed morphologic features similar to those seen in theother SMZL cases in our series. Minor differences noted in
this case included poorly circumscribed WP nodules withirregular, infiltrating borders and primarily diffuse RP infiltra-tion with few RP nodules. The splenic HLN in this case alsoshowed preservation of sinuses and a nodular infiltratecomposed mainly of small lymphocytes with abundant cyto-plasm (MZ morphologic features), similar to the lymph nodesfrom the SMZL cases. Residual or preserved mantle zonessimilar to those described in mucosa-associated lymphoidtissue lymphomas involving lymph nodes18,19 were not notedon the H&E-stained sections of the HLN in this case.
HLNs were available for review in all except 2 cases(cases 30 and 41). HLN sinuses were preserved ❚Image 4D❚
342 Am J Clin Pathol 2003;120:335-347342 DOI: 10.1309/HWG084N3F3LRJ8XB
© American Society for Clinical Pathology
A B
C D
❚Image 4❚ Splenic marginal zone lymphoma. A, Spleen with expanded white pulp nodule showing a residual germinal center(arrow), biphasic histologic features, and a prominent marginal zone (H&E, ×100). B, White pulp with heterogeneous populationof neoplastic cells or “biphasic” histologic features with central dark zone (arrowhead) and outer light zone (arrow) withtransformed cells (H&E, ×400). C, Red pulp, diffuse and nodular involvement (H&E, ×400); inset, circulating “villous” lymphocyte(Wright-Giemsa, ×1,650). D, Hilar lymph node showing preserved sinuses and prominent marginal zones (H&E, ×50).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Hematopathology / ORIGINAL ARTICLE
in all except 2 cases (cases 39 and 42). The HLN in case 39was small, with the architecture effaced by small lympho-cytic cells in the absence of a distinct nodular pattern. MZsin HLNs (Image 4D) were present in 7 (78%) of 9 cases withMZs in the splenic sections. When present, MZs in HLNstypically were observed within the larger nodules. Rareresidual GCs were identified in HLNs from 2 cases.
Peripheral blood smears with circulating lymphoma cellswere available for review in 7 cases (Image 4C, inset). Thelymphoma cells usually were intermediate or large, with lesscondensed nuclear chromatin (compared with maturelymphocytes), single or multiple small nucleoli, and moder-ately abundant, light basophilic cytoplasm with or withoutvillous cytoplasmic projections. Bone marrow morphology,available for review in 7 cases, usually showed a nodular andinterstitial lymphoid infiltrate.
Flow Cytometric Immunophenotyping
The immunophenotypic features for the CLL/SLL andMZL cases were as described in the inclusion criteria.Paraffin section immunohistochemical stains were availablein the MZL case without flow cytometric analysis (case 42).In MCL, the neoplastic cells showed a bright intensity ofCD20 and surface immunoglobulin expression in all exam-ined cases and were CD10–, CD23–, and FMC7+. Theneoplastic cells in all cases except the blastoid variant ofMCL (case 15) coexpressed CD5. The FL cells wereCD5–CD20+ in all cases examined by flow cytometry, withCD10+ neoplastic cells in 5 of 5 cases.
Immunophenotypic discordance in neoplastic cells wasnoted in 3 (33%) of 9 cases with more than 1 specimenanalyzed by flow cytometry. In case 8, a subset of the periph-eral blood lymphocytes was FMC7+ at the initial diagnosis ofCLL, and splenectomy performed 6 years later showed thesplenic lymphoma cells to be FMC7–. The FL case without a
previous LN biopsy (case 26) showed CD10– circulatinglymphoma cells and CD10+ splenic lymphoma cells by flowcytometry. One SMZL case (case 37) showed dim CD10expression in a small subset of the splenic cells by flowcytometry. However, the circulating lymphoma cells in thiscase were CD5–, CD10–, CD11c–, CD23–, CD25–, andCD103– by flow cytometry, with morphologic features quitetypical of SMZL and no circulating cleaved lymphocytes.
Statistical Comparisons
A summary of the results of statistical analyses is given in❚Table 3❚. In comparison with CLL/SLLs involving the spleen,MZLs involving the spleen are more likely to show MZs in thespleen, extracellular hyaline deposition in the splenic nodules,MZs in the HLNs, and preserved HLN sinuses. Residual GCs inthe spleen seem to be more common in MZL than in CLL/SLL;however, this trend did not achieve statistical significance.MZLs in the spleen also are more likely than MCL to manifestwith MZs in the HLNs, MZs in the spleen, residual GCs inneoplastic nodules in the spleen, and extracellular hyalinedeposits in the spleen. However, preservation of HLN sinuses isunlikely to be helpful in differentiating MZL from MCL. Incontrast, MZs in the spleen or in the splenic HLNs and extracel-lular hyaline deposits in the spleen are not helpful for discrimi-nating MZL from low-grade FL involving the spleen. MZLs inthe spleen are more likely than low-grade FLs to show residualGCs in the neoplastic nodules in the spleen and less likely thanFLs to show effaced HLN sinuses. The presence of RP infiltra-tion, either nodular or diffuse, is not helpful for discriminatingMZL from any of the other studied SBL subtypes.
Clinical Information
The patients included 21 women (CLL/SLL, 3; MCL, 4;FL, 7; MZL, 7) and 21 men (CLL, 5; MCL, 5; FL, 5; MZL,6), who underwent splenectomy at a median age of 65 years
Am J Clin Pathol 2003;120:335-347 343343 DOI: 10.1309/HWG084N3F3LRJ8XB 343
© American Society for Clinical Pathology
❚Table 3❚Summary of Statistical Comparisons
P* Values
Variable MZL vs CLL/SLL MZL vs MCL MZL vs FL
Splenic histologic featuresResidual germinal centers .056 .026 .000Extracellular hyaline .024 .044 1.000Marginal zones .000 .026 .097Red pulp infiltration
Nodular .253 .264 .593Diffuse 1.000 .079 .111
Splenic hilar lymph nodesMarginal zones .002 .002 .080Preserved sinuses .002 .109 .000
Sex .659 .693 1.000
CLL, B-cell chronic lymphocytic leukemia; FL, follicular lymphoma, grade 1 or 2; MCL, mantle cell lymphoma; MZL, marginal zone lymphoma.* P < .05 indicates a statistically significant difference between the lymphoma subtypes.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Kansal et al / HISTOPATHOLOGIC FEATURES OF SPLENIC SMALL B-CELL LYMPHOMAS
(range, 32-82 years). The age ranges (median age) of thepatients with each subtype of lymphoma were as follows:CLL/SLL, 43 to 82 years (69 years); MCL, 34 to 78 years(68 years); FL, 40 to 78 years (59 years); and MZL, 32 to 71years (60 years). The individual clinical features, includingstage of disease at splenectomy, presence of bone marrow
involvement, lymph node involvement and biopsy, indica-tions for splenectomy, and patient follow-up after splenec-tomy are given in ❚Table 4❚. Splenectomy was performedprimarily for diagnostic purposes in 23 patients (55%;SMZL, 12; FL, 6; MCL, 4; CLL with increased prolympho-cytes, 1), who also had clinically prominent splenomegaly.
344 Am J Clin Pathol 2003;120:335-347344 DOI: 10.1309/HWG084N3F3LRJ8XB
© American Society for Clinical Pathology
❚Table 4❚Clinical Features of 42 Patients With Splenic Small B-Cell Lymphoma*
Biopsy Sites
Case No./Sex/ Outcome After Age (y) Diagnosis Stage BM LN Indication for Splenectomy Splenectomy
1/F/77 SLL IV + + Thrombocytopenia; 4 y after diagnosis AWD2/M/69 CLL IV + + Thrombocytopenia; 5 y after diagnosis LFU3/F/69 CLL III NA No biopsy AIHA; 2 y after diagnosis LFU4/M/61 CLL IV + No biopsy Nondiagnostic; 1 y after BM biopsy DOD5/F/82 CLL IV + + Thrombocytopenia DOD, <1 y6/M/43 CLL/PL IV + No biopsy Diagnostic; thrombocytopenia, prominent splenomegaly, DOD, 3 mo
8 mo after BM biopsy7/M/75 CLL IV + No biopsy Thrombocytopenia; 6 y after diagnosis DOD, 22 mo8/M/64 CLL IV + No biopsy Pancytopenia, AIHA AWD, 4 wk9/M/43 MCL IV + + Therapeutic, prominent splenomegaly AWD, 20 mo10/F/68 MCL IV + + Thrombocytopenia AWD, 2 y11/M/65 MCL IV + + Therapeutic; 4 mo after LN and BM biopsy diagnosis LFU, 2 y12/F/59 MCL IV + + Therapeutic; within 6 mo of diagnosis NA13/F/69 MCL IV + No biopsy, + Diagnostic; thrombocytopenia, prominent splenomegaly, DOD
(by CT scan) 13 mo after BM biopsy14/M/78 MCL IV + + Diagnostic; anemia, thrombocytopenia; 1 wk after BM DOD, 4 wk
biopsy; LN biopsy 1 wk later15/F/34 MCL, blastoid IV + No biopsy Therapeutic; tissue diagnosis 1 y after PB examination BMT, 1 mo;
variant ANED, 39 mo16/M/68 MCL IV + NA No biopsy Diagnostic; prominent splenomegaly 3 mo after PB Alive, 14 mo
examination17/M/73 MCL IV + + Diagnostic; before BM and LN biopsies Alive, 6 y18/F/78 FL, grade 1 NA – + Trauma; 2 y after BM biopsy AWD, 2 y19/M/67 FL, grade 1 IV + + Relapse in spleen, thrombocytopenia, 14 mo after BM and CR, 4 y
LN biopsies20/F/62 FL, grade 1 IV + + Diagnostic; prominent splenomegaly AWD, 7 y21/F/68 FL, grade 1 IV + + Diagnostic; 1 mo after BM biopsy AWD, 3 y22/F/56 FL, grade 1 IV, liver + – + Symptomatic relief Died, 18 mo23/F/65 FL, grade 1 IV + + Nondiagnostic; 2 y after BM and LN biopsies Alive, 5 y24/F/41 FL, grade 1 IV + + Diagnostic; concurrent BM and LN biopsies Alive, 5 y25/M/53 FL, grade 1 IV + + Symptomatic relief; 3 y after LN biopsy Died, 16 mo26/M/75 FL, grade 2 NA – No biopsy Diagnostic; prominent splenomegaly, cytopenia Dead within 10 y27/M/40 FL, grade 2 IV + + Symptomatic relief; 7 y after LN and BM biopsies Died, 1 y28/M/55 FL, grade 2 IV + + Diagnostic; concurrent BM and abdominal LN biopsies Died, 6 mo29/F/50 FL, grade 1 IV + + Diagnostic; 1 mo after BM biopsy; LN biopsy 3 y later Alive, 16 y30/F/69 SMZL NA NA NA Diagnostic; AIHA NA31/F/50 SMZL IV + + Diagnostic; cervical LN biopsy 10 y later, MZL Alive, 17 y32/F/67 SMZL IV + No biopsy Diagnostic NA33/F/62 SMZL IV + No biopsy Diagnostic; 2 mo after BM biopsy; pancytopenia Alive, 7 y34/M/71 SMZL IV + – Diagnostic; 6-mo history of pyrexia, chest infection Died, 1 y35/F/56 EMZL IV + + Anemia; 14-y history of NHL in orbit and breast before AWD, 5 y
splenectomy36/M/41 SMZL IV + NA Diagnostic; 12-y history of splenomegaly and autoimmune Alive, 10 y
symptoms after BMT37/F/32 SMZL IV + No biopsy Diagnostic; 1 mo after PB examination Alive, 16 mo38/M/67 SMZL IV + No biopsy Diagnostic; 3 y after BM biopsy Alive, 20 mo39/M/51 SMZL IV + No biopsy Diagnostic; cytopenias; 1 y after BM biopsy Alive, 1 mo40/M/56 SMZL IV + No biopsy Diagnostic; 3 mo after BM biopsy Alive, 9 mo41/M/60 SMZL IV + No biopsy Diagnostic; 3 y after PB examination Alive, 1 mo42/F/70 SMZL IV + – Diagnostic; C1 esterase deficiency Alive, 11 mo
AIHA, autoimmune hemolytic anemia; ANED, alive with no evidence of disease; AWD, alive with disease; BM, bone marrow; BMT, bone marrow transplant; CLL, B-cellchronic lymphocytic leukemia; CLL/PL, “mixed” CLL16 or CLL with increased prolymphocytes14; CR, complete remission; CT, computed tomography; DOD, died of disease;EMZL, extranodal MZL; FL, follicular lymphoma (World Health Organization classification); LFU, lost to follow-up; LN, lymph node; MCL, mantle cell lymphoma; MZL,marginal zone lymphoma; NA, not available; NHL, non-Hodgkin lymphoma; PB, peripheral blood; SLL, small lymphocytic lymphoma; SMZL, splenic MZL; +, positive forlymphoma; –, negative for lymphoma.
* Age and stage at splenectomy.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Hematopathology / ORIGINAL ARTICLE
Splenectomy was performed primarily for therapeuticmanagement (persistent cytopenia or reduction of tumorburden) in 18 patients (43%).
Discussion
Primary splenic lymphomas have been defined aslymphomas confined to the spleen and splenic HLNs.4 Inmost instances, when an extensive search is made, thedisease is found to be widespread, often involving theretroperitoneal lymph nodes or bone marrow.6,7,20 Accordingto a recent report of unselected and sequential splenectomiesfrom 2 tertiary care centers, primary splenic lymphomasrepresent a clinical expression of a biologically heteroge-neous group of lymphomas.21 Our cases that underwentsplenectomy for diagnostic subclassification do not representstrictly defined primary splenic lymphomas as defined byKraus et al.21 Instead, according to their criteria, these casesin our study may be considered as examples of permissivelydefined primary splenic lymphomas that manifested withprominent splenomegaly.
Lymphomas manifesting with prominent splenomegalymay include SBLs such as SLL, FL, MCL, andMZL.2,5,6,10,11,22,23 Differential diagnosis can be difficultbecause SBLs involving the spleen preferentially involve theWP24,25 and may accentuate the normally present MZ struc-ture in the spleen, thus mimicking a SMZL. Our study casesof SBL have well-characterized clinical, histologic, andimmunophenotypic features and, thus, have a definitive diag-nostic subclassification according to WHO criteria.14 Ingeneral, we observed that the morphologic features ofsplenic WP nodules in well-characterized cases of SBL werea recapitulation of the histopathologic features of lymphnodes involved by the corresponding lymphoma. By grossexamination, there is involvement of the WP, often in amiliary pattern and without the large, coalescent nodules thatare characteristic of large cell lymphomas. MCL involvingthe spleen can lead to massive enlargement with largermacroscopic nodules than in other SBLs, correlating histo-logically with massive WP expansion and near-total oblitera-tion of splenic architecture, which we noted in two thirds ofour MCL cases. Diffuse RP infiltration was present in theleukemic phase of 2 MCL cases. Predominance of WPinvolvement, compared with that of RP involvement, waspresent in all cases. The splenic architecture was relativelypreserved in all cases of SBL except in the cases of MCLwith massive WP expansion. This architectural preservationmay reflect the tendency of low-grade B-cell neoplasms to“home” to compartments of the spleen where their normalcounterparts are found, in contrast with higher-grade B-celllymphomas that do not respect the compartmental boundaries.25
We observed residual GCs in WP nodules most frequently inSMZL cases and rarely in cases of MCL, FL, and CLL.Extracellular hyaline within WP nodules was common inboth FL and SMZL.
The MZ is a unique structure present around thelymphocytes of the mantle zone or primary follicles in thespleen and Peyer patches.26,27 Lymphomas now presumed toarise from the MZ originally were described by Neiman etal.28 The term splenic marginal zone lymphoma was coinedlater by Schmid et al.29 Prominence of MZs may be seen inlymphomas other than MZL,11,12,22 and we noted thisfrequently in our cases of FL. We also found that MCL canbe a mimicker of the MZ pattern in the spleen, as previouslydescribed.10,12 The differentiation of MCL from MZL oftenmay be straightforward by evaluation of histopathologic andimmunophenotypic features.10,22,23,30 The characteristichistopathologic features of MCL with a monotonous smalllymphocytic infiltrate contrast with those of MZL, whichalmost always has a polymorphous lymphoid populationwith scattered large lymphoid cells and is negative for cyclinD1 by immunohistochemical analysis.30
In contrast, we found that distinguishing FL fromSMZL can be difficult. One FL case in our series wasreported previously as a pitfall in the diagnosis of SMZL.31
At low magnification, FL involving the spleen can have ahistologic appearance similar to that of MZL, with promi-nent WP expansion, extracellular hyaline deposits, oftenprominent MZs, and multiple small RP nodules similar tothose described in MZL.12 In addition, we observed MZs inHLNs, as well as in the spleen, in 40% (4/10) of our FLcases, which may add to the diagnostic dilemma. The criticaldiagnostic feature is the identification of neoplastic follicleswithin the WP or in HLNs, or even within the small RPnodules, in FLs involving the spleen. If necessary, applyingthe bcl-2 immunohistochemical stain to demonstrateneoplastic follicles in FL is helpful for differentiating themfrom reactive GCs in MZL.22,23 Rarely, FLs involving thespleen also can have a few residual benign GCs, raising thedifferential diagnosis of reactive follicular hyperplasia.32 Wenoted this pitfall in 1 case of FL in our study.
The splenic morphologic features of the MZL cases inour study were similar to those described earlier.29,33-35 Themorphologic features of the circulating lymphoma cells weresimilar to those described earlier, with a subset of casesshowing “villous lymphocytes.”36 Clinically, we noted ahistory of an immunologic disorder in 25% of patients (3/12)with SMZL, unlike findings in a previous study in which nosuch history was found in 12 patients with SMZL37 andsimilar to findings in a later report.38 The morphologicfeatures of the neoplastic nodules in lymph nodes involvedby SMZL have been reported to resemble those of the WP inthat entity.18 Our findings in HLNs from 34 splenic SBL
Am J Clin Pathol 2003;120:335-347 345345 DOI: 10.1309/HWG084N3F3LRJ8XB 345
© American Society for Clinical Pathology
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Kansal et al / HISTOPATHOLOGIC FEATURES OF SPLENIC SMALL B-CELL LYMPHOMAS
cases confirm the similarity in morphologic features inHLNs and splenic nodules in all SBL subtypes. Furthermore,we found that unequivocal neoplastic follicles in HLNs witheffaced nodal sinuses is a most helpful feature in the diag-nosis of FL and for distinguishing FL from MZL, whichalmost always had preserved nodal sinuses. In the study byMollejo et al,18 HLNs from all cases of SMZL had preserva-tion of sinuses, similar to the findings in HLNs from most ofour MZL cases. We observed a MZ pattern on H&E-stainedsections in splenic HLNs from 80% (8/10) of our SMZLcases, compared with 1 of 14 HLN cases reported byMollejo et al.18
We did not detect a MZ pattern in our CLL/SLL cases.Evaluation of a splenectomy specimen in these cases usuallyis not difficult, since the diagnosis usually is establishedbefore splenectomy, which is most likely performed forimprovement of cytopenias. Furthermore, the cytologicfeatures of the larger WP nodules in spleens involved byCLL/SLL may be typical of lymph nodes involved byCLL/SLL, with the presence of proliferation centers or scat-tered paraimmunoblasts.
From our study, we conclude that well-characterizedcases of SBLs involving the spleen often have typicalmorphologic features, with the morphologic features of thesplenic WP and RP nodules reminiscent of the histopatho-logic features of lymph nodes involved by the correspondinglymphoma. Histopathologic evaluation of HLNs is invalu-able in differential diagnosis, since obliteration or effacementof architecture caused by SBL may be easier to interpret inlymph nodes than in the spleen. Therefore, a search forHLNs must always be performed in splenectomy specimens.MZs may be observed in the spleen and in splenic HLNsinvolved by SBLs other than SMZL. Nevertheless, preciseclassification of SBLs in a splenectomy specimen can beachieved by careful assessment of histopathologic features inmost cases. In comparison with FL, MZLs in the spleen aremore likely to show residual GCs in the neoplastic WPnodules in the spleen (P = .000) and less likely to showeffaced HLN sinuses (P = .000), while MZs in the spleen orin the HLNs are not significantly different in MZL and FL.MZL and MCL can be distinguished by the cytologiccomposition of the neoplastic infiltrate and cyclin D1immunohistochemical analysis. Furthermore, in comparisonwith MCL, MZLs are more likely to show MZs in splenicHLNs (P = .002), MZs in the spleen (P = .026), residual GCsin the spleen (P = .026), and extracellular hyaline deposits (P= .044), while preservation of HLN sinuses is not signifi-cantly different in MZL and MCL. In comparison withCLL/SLL, MZLs are more likely to show MZs in the spleen(P = .000), MZs in HLNs (P = .002), and preservation ofHLN sinuses (P = .002). RP infiltration, nodular or diffuse, isnot significantly different in MZL compared with CLL/SLL,
MCL, or low-grade FL. In difficult cases, overall assessmentand correlation of the histologic features with peripheralblood and bone marrow morphologic, immunophenotypic,and clinical features is most helpful and usually leads toprecise subclassification of SBLs involving the spleen.
From the Department of Pathology, University of Michigan, AnnArbor.
Address correspondence to Dr Kansal: Dept of Pathology, 7thFloor, Buffalo General Hospital, 100 High St, Buffalo, NY 14203.
References1. Kim H, Dorfman RF. Morphological studies of 84 untreated
patients subjected to laparotomy for the staging of non-Hodgkin’s lymphomas. Cancer. 1974;33:657-674.
2. Warnke RA, Weiss LM, Chan JKC, et al. Lymphomas of thespleen. In: Tumors of the Lymph Nodes and Spleen.Washington, DC: Armed Forces Institute of Pathology;1995:411-429. Rosai J, ed. Atlas of Tumor Pathology; Thirdseries, Fascicle 14.
3. Ahmann DL, Kiely JM, Harrison EG, et al. Malignantlymphoma of the spleen: a review of 49 cases in which thediagnosis was made at splenectomy. Cancer. 1966;19:461-469.
4. Brox A, Bishinsky JI, Berry G. Primary non-Hodgkinlymphoma of the spleen. Am J Hematol. 1991;38:95-100.
5. Kraemer BB, Osborne BM, Butler JJ. Primary splenicpresentation of malignant lymphomas and related disorders: astudy of 49 cases. Cancer. 1984;54:1606-1619.
6. Narang S, Wolf BC, Neiman RS. Malignant lymphomapresenting with prominent splenomegaly: a clinicopathologicstudy with special reference to intermediate cell lymphoma.Cancer. 1985;55:1948-1957.
7. Spier CM, Kjeldsberg CR, Eyre HJ, et al. Malignantlymphoma with primary presentation in the spleen: a study of20 patients. Arch Pathol Lab Med. 1985;109:1076-1080.
8. Jaffe ES, Raffeld M, Medeiros LJ. Histopathologic subtypes ofindolent lymphomas: caricatures of the mature B-cell system.Semin Oncol. 1993;20:3-30.
9. Mason DY, Harris NL, eds. Human Lymphoma: ClinicalImplications of the REAL Classification. London, England:Springer-Verlag; 1999:1.1-20.8.
10. Pittaluga S, Verhoef G, Criel A, et al. “Small” B-cell non-Hodgkin’s lymphomas with splenomegaly at presentation areeither mantle cell lymphoma or marginal zone celllymphoma: a study based on histology, cytology,immunohistochemistry, and cytogenetic analysis. Am J SurgPathol. 1996;20:211-223.
11. Arber DA, Rappaport H, Weiss LM. Non-Hodgkin’slymphoproliferative disorders involving the spleen. ModPathol. 1997;10:18-32.
12. Piris MA, Mollejo M, Campo E, et al. A marginal zonepattern may be found in different varieties of non-Hodgkin’slymphoma: the morphology and immunohistology of splenicinvolvement by B-cell lymphomas simulating splenicmarginal zone lymphoma. Histopathology. 1998;33:230-239.
13. Harris NL, Jaffe ES, Stein H, et al. A revised European-American classification of lymphoid neoplasms: a proposalfrom the International Lymphoma Study Group. Blood.1994;84:1361-1392.
346 Am J Clin Pathol 2003;120:335-347346 DOI: 10.1309/HWG084N3F3LRJ8XB
© American Society for Clinical Pathology
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022

Hematopathology / ORIGINAL ARTICLE
14. Jaffe ES, Harris NL, Stein H, et al, eds. Pathology and Geneticsof Tumours of Hematopoietic and Lymphoid Tissues. Lyon,France: IARC Press; 2001:119-187. World Health OrganizationClassification of Tumours.
15. Tworek JA, Singleton TP, Schnitzer B, et al. Flow cytometricand immunohistochemical analysis of small lymphocyticlymphoma, mantle cell lymphoma, and plasmacytoid smalllymphocytic lymphoma. Am J Clin Pathol. 1998;110:582-589.
16. Bennett JM, Catovsky D, Daniel M-T, et al. Proposals for theclassification of chronic (mature) B and T lymphoidleukemias. J Clin Pathol. 1989;42:567-584.
17. Melo JV, Catovsky D, Galton DA. The relationship betweenchronic lymphocytic leukaemia and prolymphocyticleukaemia. Br J Haematol. 1986;63:377-387.
18. Mollejo M, Lloret E, Menarguez J, et al. Lymph nodeinvolvement by splenic marginal zone lymphoma:morphological and immunohistochemical features. Am J SurgPathol. 1997;21:772-780.
19. Campo E, Miquel R, Krenacs L, et al. Primary nodal marginalzone lymphomas of splenic and MALT type. Am J Surg Pathol.1999;23:59-68.
20. Falk S, Stutte HJ. Primary malignant lymphomas of thespleen. Cancer. 1990;66:2612-2619.
21. Kraus MD, Fleming MD, Vonderheide RH. The spleen as adiagnostic specimen: a review of 10 years’ experience at twotertiary care institutions. Cancer. 2001;91:2001-2009.
22. Delsol G, Diebold J, Isaacson PG, et al. Pathology of thespleen: report on the workshop of the VIIIth meeting of theEuropean Association for Haematopathology, Paris 1996.Histopathology. 1998;32:172-179.
23. Isaacson PG. Malignant lymphomas with follicular growthpattern. Histopathology. 1996;28:487-495.
24. Van Krieken JHJM, Feller AC, te Velde J. The distribution ofnon-Hodgkin’s lymphoma in the lymphoid compartments ofthe human spleen. Am J Surg Pathol. 1989;13:757-765.
25. Van Krieken JHJM. Histopathology of the spleen in non-Hodgkin’s lymphoma. Histol Histopathol. 1990;5:113-122.
26. Van Krieken JHJM, te Velde J. Normal histology of thehuman spleen. Am J Surg Pathol. 1988;12:777-785.
27. Van Krieken JHJM, von Schilling C, Kluin M, et al. Splenicmarginal zone lymphocytes and related cells in the lymphnode: a morphologic and immunohistochemical study. HumPathol. 1989;20:320-325.
28. Neiman RS, Sullivan AL, Jaffe R. Malignant lymphomasimulating leukemic reticuloendotheliosis: a clinicopathologicstudy of ten cases. Cancer. 1979;43:329-342.
29. Schmid C, Kirkham N, Diss T, et al. Splenic marginal zonecell lymphoma. Am J Surg Pathol. 1992;16:455-466.
30. Savilo E, Campo E, Mollejo M, et al. Absence of cyclin D1protein expression in splenic marginal zone lymphoma. ModPathol. 1998;11:601-606.
31. Alkan S, Ross CW, Hanson CA, et al. Follicular lymphomawith involvement of the splenic marginal zone: a pitfall in thedifferential diagnosis of splenic marginal zone cell lymphoma.Hum Pathol. 1996;27:503-506.
32. Burke J. Surgical pathology of the spleen: an approach to thedifferential diagnosis of splenic lymphomas and leukemias.Am J Surg Pathol. 1981;5:551-563.
33. Hammer RD, Glick AD, Greer JP, et al. Splenic marginalzone lymphoma. Am J Surg Pathol. 1996;20:613-626.
34. Isaacson PG, Matutes E, Burke M, et al. The histopathologyof splenic lymphoma with villous lymphocytes. Blood.1994;84:3828-3834.
35. Mollejo M, Menarguez J, Lloret E, et al. Splenic marginal zonelymphoma: a distinctive type of low-grade B-cell lymphoma.Am J Surg Pathol. 1995;19:1146-1157.
36. Catovsky D, Matutes E. Splenic lymphoma with circulatingvillous lymphocytes/splenic marginal zone lymphoma. SeminHematol. 1999;36:148-154.
37. Dierlamm J, Pittaluga S, Wlodarska I, et al. Marginal zone B-cell lymphomas of different sites share similar cytogenetic andmorphologic features. Blood. 1996;87:299-307.
38. Murakami H, Irisawa H, Saitoh T, et al. Immunologicabnormalities in splenic marginal zone cell lymphoma. Am JHematol. 1997;56:173-178.
Am J Clin Pathol 2003;120:335-347 347347 DOI: 10.1309/HWG084N3F3LRJ8XB 347
© American Society for Clinical Pathology
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/120/3/335/1759026 by guest on 05 July 2022
Copyright © 2022 FDOKUMEN




















