
A novel P2Y12 adenosine diphosphate receptor antagonist that inhibits platelet aggregation and...
9
© 2007 Schattauer GmbH, Stuttgart 847 A novel P2Y 12 adenosine diphosphate receptor antagonist that inhibits platelet aggregation and thrombus formation in rat and dog models Yi-Xin Wang, JonVincelette,Valdeci da Cunha, Baby Martin-McNulty, Cornell Mallari, Richard M. Fitch, SereneAlexander, Imadul Islam, Brad O. Buckman, ShendongYuan, Joseph M. Post, Babu Subramanyam, RonaldVergona, Mark E. Sullivan,William P. Dole, John Morser, Judi Bryant Berlex Biosciences, Richmond, California, USA Summary Irreversible platelet inhibitors, such as aspirin and clopidogrel, have limited anti-thrombotic efficacy in the clinic due to their bleeding risk. We have developed an orally active reversible P2Y 12 receptor antagonist, BX 667.The aim of this study was to determine if the reversible antagonist BX 667 had a greater therapeutic index than the irreversible P2Y 12 receptor antagon- ist clopidogrel. Since BX 667 is rapidly converted to its active metabolite BX 048 in rats,we first injected BX 048 intravenously (iv) in a rat arterial venous (A-V) shunt model of thrombosis. BX 048 dose- and concentration-dependently attenuated thrombo- sis.When administered orally,BX 667 and clopidogrel had simi- lar efficacy, but BX 667 caused less bleeding than clopidogrel. In a rat model of a platelet-rich thrombus induced by vessel injury with FeCl 2 , both BX 667 and clopidogrel exhibited higher levels Keywords ADP, platelet aggregation, thrombosis, rat, dog, cyclic flow vari- ation of thrombus inhibition after oral administration compared to their potency in the A-V shunt model.Again, BX 667 caused less bleeding than clopidogrel. In a dog cyclic flow model, iv injection of either BX 667 or clopidogrel dose-dependently reduced thrombus formation with lower bleeding for BX 667 than clopi- dogrel. Inhibition of thrombosis was highly correlated with in- hibition of ADP-induced platelet aggregation in these animal models. In dogs pre-treated with aspirin, BX 667 maintained its wider therapeutic index, measured by inhibition of platelet ag- gregation over bleeding, compared to the aspirin-clopidogrel combination.These data demonstrate that the reversible P2Y 12 receptor antagonist, BX 667, has a wider therapeutic index than clopidogrel in experimental models of thrombosis. Thromb Haemost 2007; 97: 847–855 Animal Models Correspondence to: Yi-Xin (Jim) Wang Berlex Biosciences 2600 Hilltop Drive Richmond, CA 948047, USA Tel.: +1 510 669 4489, Fax: +1 510 669 4247 E-mail: [email protected] Received December 22, 2006 Accepted after revision March 1, 2007 Prepublished online April 4, 2007 doi:10.1160/TH06–12–0732 Introduction Antiplatelet therapy reduces mortality and non-fatal events in patients with atherothrombotic disease. Aspirin and clopidogrel have both emerged as critical therapies in the treatment of coron- ary artery disease, inhibiting platelet aggregation by two distinct mechanisms. Aspirin, which inhibits thromboxane-induced pla- telet aggregation by irreversibly blocking the enzyme cyclo- oxygenase (1), is modestly efficacious (25% risk reduction for the occurrence of myocardial infarction, stroke or vascular death) and relatively safe, thus, remaining the standard reference compound for oral antiplatelet treatment (2–4). Clopidogrel (Plavix ™ ) undergoes hepatic metabolism (5) to produce active metabolites (6, 7) that irreversibly inhibit ADP-induced platelet aggregation (8) through the platelet ADP receptor P2Y 12 (9). In the CAPRIE trial, clopidogrel was shown to be slightly more ef- fective than aspirin with five fewer thrombotic events per 1,000 patients (8.7% added benefit) (10, 11). When taken with aspirin, clopidogrel further reduced adverse coronary events by 19%, which, however, was accompanied by a 30% increase in major bleeding relative to aspirin treatment alone (12). Nearly half of the major bleeding events were defined as life-threatening, and six per 1,000 patients who were treated with clopidogrel in com- bination with aspirin required a blood transfusion. Despite the widespread use of these drugs and the obvious benefit of antipla- telet therapy, there are concerns about their use. Clopidogrel has a narrow therapeutic index with modest efficacy at 75 mg/day and higher doses causing unacceptable bleeding (13). Addition-
Transcript of A novel P2Y12 adenosine diphosphate receptor antagonist that inhibits platelet aggregation and...

© 2007 Schattauer GmbH, Stuttgart
847
A novel P2Y12 adenosine diphosphate receptor antagonist thatinhibits platelet aggregation and thrombus formation in rat anddog modelsYi-Xin Wang, JonVincelette,Valdeci da Cunha, Baby Martin-McNulty, Cornell Mallari, Richard M. Fitch,Serene Alexander, Imadul Islam, Brad O. Buckman, ShendongYuan, Joseph M. Post, Babu Subramanyam,RonaldVergona, Mark E. Sullivan, William P. Dole, John Morser, Judi BryantBerlex Biosciences, Richmond, California, USA
SummaryIrreversible platelet inhibitors, such as aspirin and clopidogrel,have limited anti-thrombotic efficacy in the clinic due to theirbleeding risk. We have developed an orally active reversibleP2Y12 receptor antagonist, BX 667.The aim of this study was todetermine if the reversible antagonist BX 667 had a greatertherapeutic index than the irreversible P2Y12 receptor antagon-ist clopidogrel. Since BX 667 is rapidly converted to its activemetabolite BX 048 in rats,we first injected BX 048 intravenously(iv) in a rat arterial venous (A-V) shunt model of thrombosis.BX048 dose- and concentration-dependently attenuated thrombo-sis.When administered orally, BX 667 and clopidogrel had simi-lar efficacy, but BX 667 caused less bleeding than clopidogrel. Ina rat model of a platelet-rich thrombus induced by vessel injurywith FeCl2, both BX 667 and clopidogrel exhibited higher levels
KeywordsADP, platelet aggregation, thrombosis, rat, dog, cyclic flow vari-ation
of thrombus inhibition after oral administration compared totheir potency in theA-V shunt model.Again,BX 667 caused lessbleeding than clopidogrel. In a dog cyclic flow model, iv injectionof either BX 667 or clopidogrel dose-dependently reducedthrombus formation with lower bleeding for BX 667 than clopi-dogrel. Inhibition of thrombosis was highly correlated with in-hibition of ADP-induced platelet aggregation in these animalmodels. In dogs pre-treated with aspirin, BX 667 maintained itswider therapeutic index, measured by inhibition of platelet ag-gregation over bleeding, compared to the aspirin-clopidogrelcombination.These data demonstrate that the reversible P2Y12receptor antagonist,BX 667,has a wider therapeutic index thanclopidogrel in experimental models of thrombosis.
Thromb Haemost 2007; 97: 847–855
Animal Models
Correspondence to:Yi-Xin (Jim) WangBerlex Biosciences2600 Hilltop DriveRichmond, CA 948047, USATel.: +1 510 669 4489, Fax: +1 510 669 4247E-mail: [email protected]
Received December 22, 2006Accepted after revision March 1, 2007
Prepublished online April 4, 2007doi:10.1160/TH06–12–0732
IntroductionAntiplatelet therapy reduces mortality and non-fatal events inpatients with atherothrombotic disease. Aspirin and clopidogrelhave both emerged as critical therapies in the treatment of coron-ary artery disease, inhibiting platelet aggregation by two distinctmechanisms. Aspirin, which inhibits thromboxane-induced pla-telet aggregation by irreversibly blocking the enzyme cyclo-oxygenase (1), is modestly efficacious (25% risk reduction forthe occurrence of myocardial infarction, stroke or vasculardeath) and relatively safe, thus, remaining the standard referencecompound for oral antiplatelet treatment (2–4). Clopidogrel(Plavix™) undergoes hepatic metabolism (5) to produce activemetabolites (6, 7) that irreversibly inhibit ADP-induced platelet
aggregation (8) through the platelet ADP receptor P2Y12 (9). Inthe CAPRIE trial, clopidogrel was shown to be slightly more ef-fective than aspirin with five fewer thrombotic events per 1,000patients (8.7% added benefit) (10, 11). When taken with aspirin,clopidogrel further reduced adverse coronary events by 19%,which, however, was accompanied by a 30% increase in majorbleeding relative to aspirin treatment alone (12). Nearly half ofthe major bleeding events were defined as life-threatening, andsix per 1,000 patients who were treated with clopidogrel in com-bination with aspirin required a blood transfusion. Despite thewidespread use of these drugs and the obvious benefit of antipla-telet therapy, there are concerns about their use. Clopidogrel hasa narrow therapeutic index with modest efficacy at 75 mg/dayand higher doses causing unacceptable bleeding (13). Addition-

Wang et al. Inhibition of thrombin by a reversible ADP antagonist
848
ally, clopidogrel has a slow onset of action, requiring more thanfour days to reach steady-state levels of inhibition of platelet ag-gregation (14–17). To counteract this deficiency, a 300-mg load-ing dose of clopidogrel is often used, although there seems to beno significant benefit to this loading dose compared to giving a75-mg dose only (18, 19). Conversely, clopidogrel irreversiblyinhibits platelet aggregation, requiring about five days to returnto pretreatment behavior after discontinuing the drug (8, 14–17).While this may be beneficial in terms of patient compliance, itcan lead to complications when clopidogrel-treated patientsrequire surgery or other procedures. Furthermore, clopidogrelwas reported to cause thrombotic thrombocytopenic purpura, aninfrequent but potentially fatal complication also associated withthe structurally related ticlopidine (20). In addition, clopidogrelis converted to its active metabolites in the liver by cytochromeP450 3A4, which potentially can cause drug-drug interactions(21, 22). Perhaps a greater concern is the emergence of aspirin
and clopidogrel resistance, which may put some patients at riskof therapeutic failure (23–26).
While the beneficial effects of oral antiplatelet compoundsare well established, the limitations of aspirin and clopidogrelunderscore the need for new agents with improved efficacy andsafety profiles. Both aspirin and clopidogrel are irreversible in-hibitors of platelet aggregation. We have discovered and devel-oped an orally active and reversible small-molecule ADP P2Y12
receptor antagonist, BX 667, which may overcome the deficien-cies of clopidogrel by exhibiting a wider therapeutic index,allowing higher levels of platelet inhibition, faster onset and off-set of action, and a low potential for drug-drug interaction. Theaim of the present study was to test whether a reversible ADP re-ceptor antagonist will have a wider therapeutic index than an ir-reversible antagonist by comparing the efficacy versus bleedingrisk of BX 667 to clopidogrel in combination with or without as-pirin in models of thrombosis.
Figure 2: Experimental illustration of the A-V shunt model ofthrombosis in anesthetized rats (A), dose- (B) and concen-tration- (C) response curves, and correlations (D) between in-hibition of thrombus formation and platelet aggregation fol-
Figure 1: Chemicalstructures of BX 667 andBX 048.
lowing intravenous bolus injection of BX 048. Number of animals(n) in each dosing group is indicated above the x-axis in panel B. Thedata in panel C and D are obtained from panel B.
Wang et al. Inhibition of thrombin by a reversible ADP antagonist
849
MethodsChemicalsBX 667, “(S)-4-({4-[1-(Ethoxycarbonyl)-1-methylethoxy]-7-methyl-2-quinolyl} Carbamoyl)-5-[4-(ethoxycarbonyl) piper-azin-1-yl]-5-oxopentanoic acid”, and BX 048, “(S)-4-({[4-(1-Carboxy-1-methylethoxy)-7-methylquinolin-2-yl]carbonyl}amino)-5-[4-(ethoxycarbonyl) piperazin-1-yl]-5-oxopentanoicacid”, were used in this study. BX 048 is the acid form of the esterBX 667 (Fig. 1). The details of chemical synthesis, as well as thepharmacological, chemical and physical properties of BX 667and BX 048 will be reported in separate publications. Plavix tab-lets (List No. 1171–40, NDC 63653–1171–4, Bristol-MyersSquibb/Sanofi Pharmaceuticals Partnership) were crushed into apowder using a pestle and mortar, from which clopidogrel wasextracted and purified.
Animal modelsAll animal experimental procedures were approved by the Insti-tutional Animal Care and Use Committee and were in accord-ance with the Guide for the Care and Use of Laboratory Animals(NIH).
Rat arterial venous shunt (A-V shunt) modelMale Sprague-Dawley rats (350–450 g, 7–18 animals/group)were anesthetized with an intraperitoneal injection of Nembutal
(65 –75 mg/kg). As illustrated in Figure 2A, the left carotid ar-tery and the right jugular vein were each cannulated with silicon-ized PE-50 tubing (8 cm). Fifty minutes (min) after anesthesia,when the animal’s condition was stabilized after surgery, the ar-terial and venous catheters were connected by a shunt tube(Tygon S-50-HL, 6 cm) containing a silk thread (6–0 silk suture,10 cm) coated with collagen (Horm, 100 µg/ml) to form an arter-ial venous (A-V) shunt. Blood was allowed to flow through theshunt for 10 min.At the end of the experiment, the shunt tube wasremoved and the amount of thrombus deposited on the silkthread was measured as dry weight after 24 hours (h) at roomtemperature. BX 048 (1, 3 and 10 mg/kg) or vehicle (15% di-methyl sulfoxide [DMSO] in saline, 1 ml/kg) was injected via thejugular vein catheter 5 min before the A-V shunt. Blood samples(1 ml) were taken immediately before dosing and at the end of theexperiment for measurements of ex-vivo platelet aggregation.The last blood sample was also used for measurement of plasmadrug levels.
In a separate experiment, BX 667, clopidogrel or vehicle(94% PEG 300, 4% ethanol and 2% water) was administered bygavage in conscious rats. The pharmacokinetic (PK)/phar-macodynamic (PD) profiles for BX 667 and clopidogrel arequite different. Our previous PK / PD studies in rats showed thatfollowing a single oral dose of BX 667, peak plasma drug con-centration of its metabolite BX 048 and platelet inhibition wereachieved in 30–60 min followed by a slow decline. In contrast,
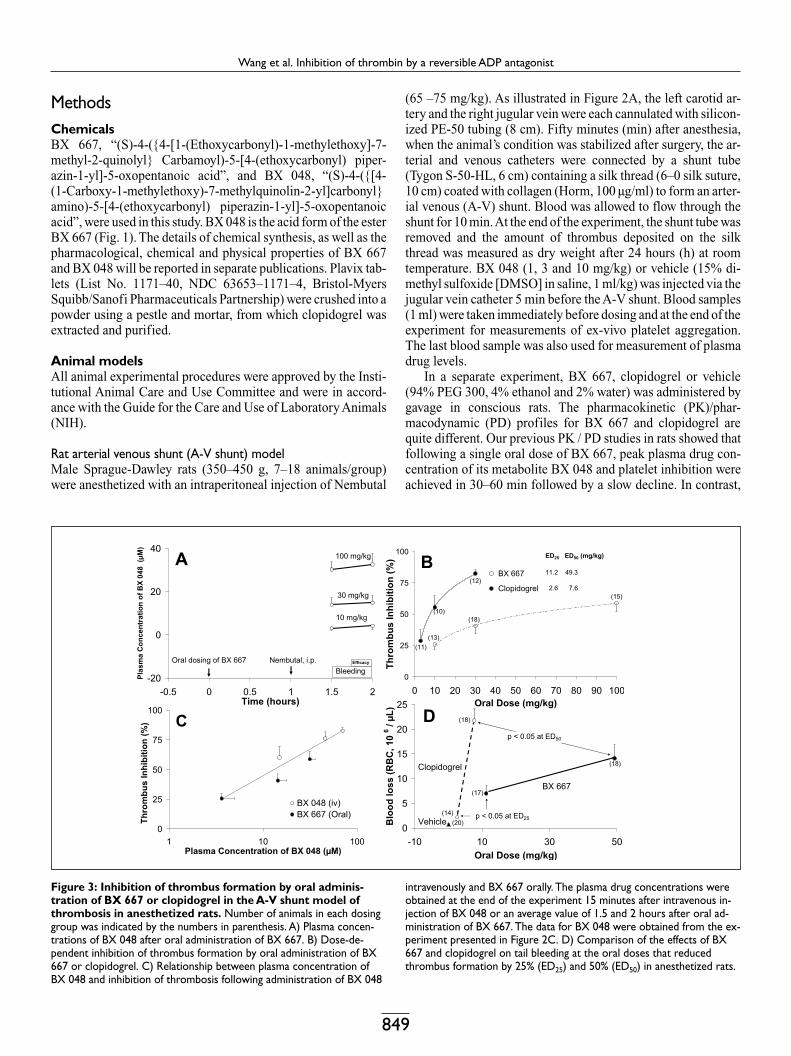
Figure 3: Inhibition of thrombus formation by oral adminis-tration of BX 667 or clopidogrel in the A-V shunt model ofthrombosis in anesthetized rats. Number of animals in each dosinggroup was indicated by the numbers in parenthesis. A) Plasma concen-trations of BX 048 after oral administration of BX 667. B) Dose-de-pendent inhibition of thrombus formation by oral administration of BX667 or clopidogrel. C) Relationship between plasma concentration ofBX 048 and inhibition of thrombosis following administration of BX 048
intravenously and BX 667 orally. The plasma drug concentrations wereobtained at the end of the experiment 15 minutes after intravenous in-jection of BX 048 or an average value of 1.5 and 2 hours after oral ad-ministration of BX 667. The data for BX 048 were obtained from the ex-periment presented in Figure 2C. D) Comparison of the effects of BX667 and clopidogrel on tail bleeding at the oral doses that reducedthrombus formation by 25% (ED25) and 50% (ED50) in anesthetized rats.

Wang et al. Inhibition of thrombin by a reversible ADP antagonist
850
oral administration of clopidogrel (10 mg/kg) required 2 to 4 h toreach maximum platelet inhibition, and this effect could persistfor several days (5, 8). Since clopidogrel undergoes a complexmetabolism to produce active metabolites that are unstable anddifficult to detect in plasma (6), inhibition of platelet aggregationis used as an indirect way of measuring clopidogrel’s effect. Toobviate such PK and metabolic differences and to compare thedrugs’ effects at a stable plasma level, BX 667 was given 1 h be-fore and clopidogrel 3 h before anesthesia as illustrated in Figure3A. Blood samples (0.5 ml) were taken 20 min before the A-Vshunt (0.5 h after anesthesia) and at the end of the experiment formeasurement of plasma levels of BX 048. Since the conversionof BX 667 to its active metabolite BX 048 is complete and im-mediate in rats, no BX 667 can be detected following oral dosing.Dose-response curves were constructed, and effective doses thatreduced thrombus weight by 25% (ED25) or 50% (ED50) werecalculated using the curve fitting method.
In order to compare the bleeding tendency between BX 667and clopidogrel at equivalent efficacy, ED25 or ED50 doses forboth compounds were given by gavage (n = 14 – 20/group) usingthe identical protocol described above (Fig. 3A). The tip of thetail was excised 1 mm from the end and immediately immersedin 25 ml of isotonic saline at 37°C. Bleeding was allowed to pro-ceed for 30 min. Clotting of the collected blood was prevented bycontinuous stirring during the experiment and by addition of 5ml of 5% EDTA in saline at the end of the experiment. Blood losswas quantified by counting the red blood cells (RBC, 106/µl)using a blood cell counter (Baker-9200+cp).
Rat carotid artery injury (FeCl2) modelThe arterial injury model has been well-characterized as a pla-telet-rich thrombosis model (27, 28) and was run as described indetail in our previous publication (29). The experimental proto-col used for drug application in the A-V shunt model was alsoused in this experiment (Fig. 4A).A bleeding test was carried outin the same animals simultaneously with efficacy study. Five minafter removal of FeCl2, a small incision was made on the back ofthe tongue using a standard cutting device (Surgicutt Jr., Inter-national Technidyne Corp., Edison, NJ, USA). The time requiredfor bleeding to stop was recorded as bleeding time, and the bloodloss was collected and weighed on a pre-weighed piece of blot-ting paper. Blood samples were also taken at the end of the ex-periment to measure plasma levels of BX 048.
Dog cyclic flow variation modelMale beagle dogs (8–12 kg) were anesthetized by inhalation ofisoflurane (1–3%) via an intubated tracheal tube before isolationof the femoral artery and placement of a flow probe (2.5SB,Transonic Systems, Ithaca, NY, USA) around the vessel(s). Athree-lumen catheter was inserted into the right jugular vein. AMillar pressure transducer (2 Fr.) was inserted into the right bra-chial artery to measure blood pressure and heart rate. After stabi-lization of the hemodynamic parameters, cyclic flow variationwas initiated in the femoral artery with mechanical injury of theendothelium by clamping the vessel six times with a pair of 8 mmwide hemostatic forceps whose teeth were covered with papertape to prevent vessel tears. Next, the mean femoral blood flowwas reduced to 20 ml/min by applying a constrictor around thevessel. After cyclic flow variation had been established, a blood
Figure 4: Oral administration of BX 667 or clopidogrel pre-vented carotid artery occlusion in a rat model of injury-in-duced thrombosis caused by exposure to FeCl2 on the carotidartery in anesthetized rats. A) Experimental protocol. B) Represen-tative original recordings of blood flow measured in the isolated carotidartery topically applied with FeCl2 in rats treated with vehicle (control)
or BX 667 at 3 mg/kg. C) Dose-response curves of carotid artery bloodflow at 30 minutes (min) (top) and time to occlusion (bottom) followingapplication of FeCl2 . Since the experimental duration was 30 min, whenthe time to occlusion reached 30 min, the treatment completely pre-vented FeCl2-induced occlusion. The data are obtained from the sameexperiment in Figure 5A.

Wang et al. Inhibition of thrombin by a reversible ADP antagonist
851
sample was taken for determining basal platelet activity in an ex-vivo platelet aggregation assay. Basal bleeding time was alsomeasured from the tongue using a standardized cutting device(Surgicutt Jr., International Technidyne Corp., Edison, NJ,USA). After 30 min of stable cyclic flow variations, BX 667,clopidogrel or phosphate buffered saline (PBS) was injected as abolus into the jugular vein. Subsequently, bleeding time was de-termined and blood samples were collected for measuring ex-vivo platelet aggregation and drug concentrations at 1, 30, 60,90, 120 and 180 min after drug or vehicle administration. Thetotal number of cyclic flow variations occurring in each 30-minperiod was counted.
Ex-vivo platelet aggregation and plasma drugconcentrationEx-vivo inhibition of ADP-induced platelet aggregation wasmeasured in rats and dogs undergoing efficacy studies using animpedance aggregometer (Model # 592, Chronolog Corpor-ation). Heparinized (10 U/ml) whole blood was diluted 1:1 with0.9% saline and incubated at 37oC in a cuvette, which was thentransferred to an impedance measuring well.A submaximal con-centration of 5 µMADP was added that had been shown in a pilotstudy to induce platelet aggregation at 90% of the maximal levelin control blood (EC90). The extent of platelet aggregation wascalculated by measuring the area under the curve (AUC) over 15min and expressing it as % inhibition compared to the baselinelevel in each animal determined in the blood obtained beforedrug treatment. Plasma concentrations of BX 667 and its activemetabolite BX 408 were measured by LC/MS/MS.
Data analysis and statisticsData are presented as mean and standard error of the mean unlessspecified otherwise. Statistical comparisons among the treat-ments were performed by Student t-test for two groups or analy-sis of variance (ANOVA) for more than two groups, followed, ifsignificant, by the Student-Newman-Keuls test. A p-value lessthan 0.05 was used to determine statistical significance.
ResultsRat A-V shunt modelIntravenous bolus injection of BX 048 dose-dependently in-hibited platelet aggregation and thrombus formation (Fig. 2).The responses nearly reached the plateau level of ~80% in-hibition of thrombus formation at 3 mg/kg but were not furtherincreased at 10 mg/kg (Fig. 2B). Both the inhibition of plateletaggregation and thrombus formation were dependent on plasmadrug concentration measured at the end of the experiment (Fig.2C). In addition, inhibition of thrombus formation also cor-related with inhibition of platelet aggregation (Fig. 2D).
Following oral administration of BX 667, plasma concen-tration of its active metabolite, BX 048, remained constant from1.5 to 2 h after administration (Fig. 3A), during which thrombusformation was dose-dependently reduced (Fig. 3B). Clopidogrelalso dose-dependently reduced thrombus formation, however,with a much steeper dose-response curve. The ED25 and ED50
were 11.2 and 49.3 mg/kg for BX 667, and 2.6 and 7.6 mg/kg forclopidogrel, respectively.The efficacy of BX 667 correlated withplasma concentrations of the active metabolite BX 048 with an
Figure 5: Oral administration of BX 667 or clopidogrel in-hibited thrombus formation and prolonged bleeding time ininjury-induced thrombosis caused by exposure of the carotidartery to FeCl2 in anesthetized rats. A) The therapeutic index cal-culated from the area under the curves between inhibition of thrombusweight (solid line with left y-axis) and bleeding time prolongation or
blood loss (dashed line with right y-axis). Number of animals (n) in eachdosing group is indicated below the x-axis in panel A. B) Pharmacody-namic relationship between inhibition of thrombus weight (top) orbleeding time (bottom) and average plasma concentrations of BX 048before thrombus formation and at the end of the experiment. The dataare obtained from the same experiment in panel A.
Wang et al. Inhibition of thrombin by a reversible ADP antagonist
852
EC50 value of 22 µM. The relationship between plasma concen-trations of BX 048 and thrombus inhibition is similar whether itwas administered intravenously as BX 048 or metabolized fol-lowing oral dosing with BX 667 (Fig. 3C).
In order to compare bleeding at the same efficacy betweenBX 667 and clopidogrel, ED25 and ED50 doses of BX 667 (11.2and 49.3 mg/kg) and clopidogrel (2.6 and 7.6 mg/kg) or vehiclewere given by gavage to separate groups of rats (n=14–20), fol-lowing an identical experimental protocol to that used in the ef-ficacy study (Fig. 3A). Both BX 667 and clopidogrel dose-de-pendently increased blood loss (Fig. 3D). However, clopidogrelresulted in a steeper dose-response curve compared to BX 667.Thus, a ~three-fold increase in the dose of clopidogrel (from 2.6to 7.6 mg/kg) resulted in a ~ten-fold increase in blood loss,whereas a ~4.4-fold increase in the dose of BX 667 (from 11.2 to49.3 mg/kg) only resulted in a ~two-fold increase in bleeding. Atthe ED50 dose clopidogrel resulted in significantly more bloodloss than BX 667 (Fig. 3D).
Rat carotid artery injury (FeCl2) modelFollowing topical application of FeCl2 on the outside of the iso-lated carotid artery, a thrombus gradually formed inside thevessel reducing carotid blood flow and eventually causing
thrombotic occlusion in all control rats treated with vehicle (Fig.4B). Pre-treatment with either BX 667 or clopidogrel dose-de-pendently increased carotid artery blood flow measured at 30min (Fig. 4C, top) and the time to vessel occlusion (Fig. 4C, bot-tom), as well as attenuated thrombus formation measured as clotweight (Fig. 5A). Although the ED50 of BX 667 (0.9 mg/kg) wascomparable to clopidogrel (0.6 mg/kg), the dose-response curvewas steeper for clopidogrel than for BX 667. In rats treated withBX 667, thrombus inhibition was correlated with the plasmaconcentrations of BX 048 with an EC50 value of 0.71 µM (Fig.5B, top). Although bleeding time (Fig. 5A, top) and blood loss(Fig. 5A, bottom) were also dose-dependently increased for bothcompounds, they were significantly less in rats treated with BX667 than with clopidogrel. In rats treated with BX 667, the bleed-ing time was not significantly prolonged until the plasma con-centration of BX 048 exceeded 10 µM, a level ten-fold higherthan the EC50 of the efficacious concentration (Fig. 5B, bottom).
The therapeutic index can be expressed as the area betweenthe dose response curve for efficacy and the dose responsecurves for either bleeding time (Fig. 5A, top) or blood loss (Fig.5A, bottom). When measured by bleeding time, BX 667 (AUC =5456) exhibited an over eight-fold greater therapeutic index thanclopidogrel (AUC=641). When measured by blood loss, BX 667
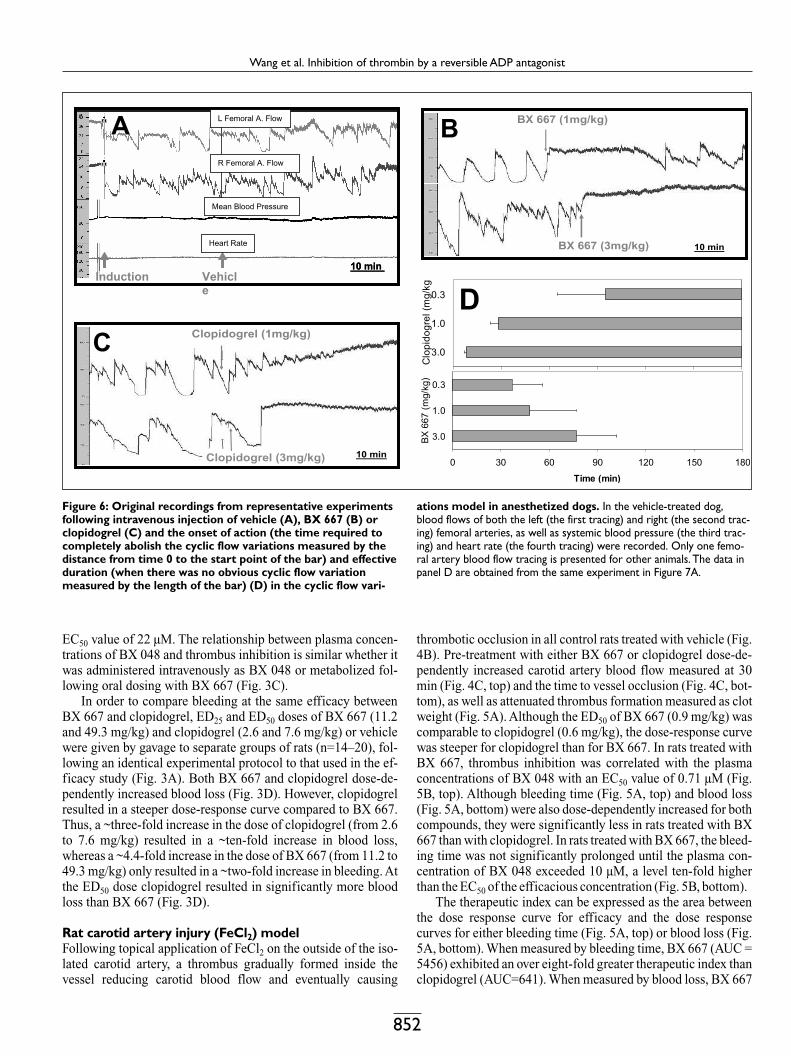
Figure 6: Original recordings from representative experimentsfollowing intravenous injection of vehicle (A), BX 667 (B) orclopidogrel (C) and the onset of action (the time required tocompletely abolish the cyclic flow variations measured by thedistance from time 0 to the start point of the bar) and effectiveduration (when there was no obvious cyclic flow variationmeasured by the length of the bar) (D) in the cyclic flow vari-
ations model in anesthetized dogs. In the vehicle-treated dog,blood flows of both the left (the first tracing) and right (the second trac-ing) femoral arteries, as well as systemic blood pressure (the third trac-ing) and heart rate (the fourth tracing) were recorded. Only one femo-ral artery blood flow tracing is presented for other animals. The data inpanel D are obtained from the same experiment in Figure 7A.

Wang et al. Inhibition of thrombin by a reversible ADP antagonist
853
(AUC = 7,500) exhibited an over six-fold greater therapeuticindex than clopidogrel (AUC = 1,275). Another way of calculat-ing the therapeutic index is to divide the effective dose that ex-tends bleeding time two-fold (ED2x) or three-fold (ED3x) by theefficacious dose at ED50. Thus, the ED2x / ED50 was 8 for BX 667and only 3 for clopidogrel. The ED3x / ED50 was 37 for BX 667and only 5 for clopidogrel. By this calculation the therapeuticindex is three- to seven-fold greater for BX 667 when comparedto clopidogrel.
Dog cyclic flow variation modelThe canine cyclic flow variation model has been widely used forcharacterization of antiplatelet compounds (30–35). In thismodel vascular injury and stenosis are employed to induce pla-telet-dependent thrombus formation resulting in intermittentthrombotic occlusion or cyclic blood flow variations character-ized by a transient reduction of flow to zero followed by sponta-neous resumption of blood flow (Fig. 6). The pattern of cyclicflow variations was stable for over 4 h and was not interrupted byintravenous injection of vehicle. In some experiments, we simul-taneously recorded blood flows in both of the femoral arteries. Avery similar pattern of cyclic flow variations was observed be-tween the left and right femoral arteries with no changes in bloodpressure and heart rate (Fig. 6A). There was also no obvious dif-ference in response to drug treatment between the two vessels.Therefore in subsequent experiments, we only used the data ob-tained from one femoral artery. Intravenous bolus injection ofBX 667 immediately abolished the cyclic flow variation, which
recurred later as plasma drug levels declined, demonstrating thatthe effect of BX 667 is reversible (Fig. 6B). The duration of ac-tion of BX 667 was dose-dependent (Fig. 6D). In contrast, theonset of the effect was much slower for clopidogrel (Fig. 6C), al-though faster at higher doses (Fig. 6D). In addition, the effects ofclopidogrel were irreversible. Once the cyclic flow variationswere abolished by clopidogrel, there was no recurrence duringthe remainder of the study (Fig. 6C, D).
Both BX 667 and clopidogrel dose-dependently inhibitedcyclic flow variations (Fig. 7A) and platelet aggregation (Fig.7B), with a similar potency measured by an ED50 of 0.21 and0.25 mg/kg, respectively, and dose-dependently prolongedtongue bleeding time (Fig. 7A, B). The bleeding time was sig-nificantly longer (p < 0.05) in the dogs treated with clopidogrel(5.5 ± 0.6 fold) than BX 667 (3.5 ± 0.7 fold) at 3 mg/kg, but notat 0.3 and 1 mg/kg where bleeding was minimal. Thus, the thera-peutic index was greater for BX 667 than clopidogrel. In separ-ate groups of dogs, 20 mg/kg aspirin was orally administered forthree days, which abolished arachidonic acid-, but not ADP-in-duced platelet aggregation, and prolonged the baseline bleedingtime 45% (from 2.21 ± 0.16 to 3.24 ± 0.32 min, p < 0.01). Furthertreatment with BX 667 or clopidogrel in these dogs led to an en-hanced inhibition of platelet aggregation and prolongation ofbleeding time in a dose-dependent manner (Fig. 7C). Yet, thetherapeutic index, measured as the ratio of bleeding time to pla-telet aggregation, was still greater with the aspirin-BX 667 thanwith the aspirin-clopidogrel combination.
Figure 7:Therapeutic index measured by inhibition of cyclicflow or platelet aggregation (solid line with left y-axis) andtongue bleeding time prolongation (dashed line with righty-axis) without (A, B) or with (C) pre-treatment with 20 mg/kgaspirin per day for three days with the number of animals (n)used in each group, and concentration-response curves of BX
667 (D) and correlation between inhibition of cyclic flow vari-ations and platelet aggregation (E) following intravenous ad-ministration of clopidogrel and BX 667 in the cyclic flow vari-ation model in anesthetized dogs. The data in panel D and E are ob-tained from the same animals in panel A and B.

Wang et al. Inhibition of thrombin by a reversible ADP antagonist
854
In studies with BX 667, there was a good correlation betweenplasma levels of drug (summation of BX 667 and BX 048 levels)and efficacy measured either by inhibition of cyclic flow vari-ation or by platelet aggregation with an EC50 of 0.17 and0.34 µM, respectively (Fig. 7D). In addition, there was also agood correlation between the inhibition of cyclic flow variationand platelet aggregation for both BX 667 and clopidogrel, de-monstrating that platelet aggregation is a good pharmacody-namic marker for predicting efficacy in this model of thrombosis(Fig. 7E).
DiscussionIn the present studies, we demonstrated that a novel orally activeand reversible small-molecule P2Y12 receptor antagonist, BX667, inhibited ADP-induced platelet aggregation and thrombusformation in three different animal models of thrombosis. Com-pared to the irreversible clopidogrel, BX 667 showed a greatertherapeutic index, rapid onset and reversibility of action. Evenwhen given with aspirin in the dog model, BX 667 still main-tained a wider therapeutic index than clopidogrel. These resultsare consistent with reports in a canine thrombosis model that areversible P2Y12 receptor antagonist inhibited thrombus withminimal bleeding prolongation (36–39).
The present data also showed that antithrombotic efficacywas highly correlated with inhibition of ADP-induced plateletaggregation, and at least 80% inhibition of platelet aggregationwas required to give near maximal antithrombotic efficacy inanimal models of thrombosis. In contrast, the current clinicaldose of clopidogrel of 75 mg/day only inhibits platelet aggre-gation by 40–50 % with higher doses causing excessive bleed-ing. Thus, the greater therapeutic index of BX 667 in animalmodels of thrombosis would allow dosing to achieve higher in-hibition of platelet aggregation without increasing bleeding risk,leading to greater therapeutic efficacy. Reversible P2Y12 recep-tor antagonists have been shown in humans to inhibit platelet ag-gregation by 80% with minimal effects on bleeding, demonstrat-ing a greater therapeutic index than either aspirin or clopidogrel(38, 40, 41). Furthermore, intravenous administration of cangre-lor, a reversible P2Y12 receptor antagonist, in patients under-going percutaneous coronary intervention achieved rapid, re-versible inhibition of platelet aggregation with less bleeding timeprolongation compared to the glycoprotein IIb/IIIa receptor an-tagonist, abciximab (42).
Pharmacokinetic and metabolic studies showed that in ani-mals, the ester form, BX 667, is hydrolyzed to the carboxylicacid form, BX 048, without a significant change in binding af-finity and platelet inhibitory potency. Such conversion is im-mediate and complete in rats; thus, only BX 048 but not BX 667can be measured in circulating blood. In the rat A-V shunt ex-periment, both intravenous BX 048 and oral BX 667 adminis-trations resulted in a similar efficacy with a similar pharmacody-namic relationship between the plasma concentration of BX 048and thrombus inhibition for both compounds even given by dif-ferent routes of administration (Fig. 3C). In dogs, both com-pounds can be measured in circulating blood as the conversionfrom BX 667 to BX 048 is gradual and incomplete. Since both
compounds have a similar biological activity and potency, thesummation of the plasma concentrations of both compounds wasused to construct concentration-response curves. In the dog cyc-lic flow variation model, the EC50 (0.34 µM) for thrombus in-hibition was comparable with the EC50 (0.71 µM) in the ratmodel of platelet-rich thrombosis.The slightly higher potency ofBX 048 and BX 667 in the dog than rat model is consistent withthe in-vitro potency in platelet aggregation assays (details will bepublished in separate publications).
The rat A-V shunt model produces a fibrin-rich thrombus,which is more sensitive to an anticoagulant than an antiplateletagent (43, 44). Alternative arterial injury models, such as the ratFeCl2 (27–29, 45) and dog cyclic flow variation (30–35) models,induce a platelet-rich thrombus, and thus are more sensitive toantiplatelet agents. This explains why the potency of both BX667 and clopidogrel was much higher in both rat and dog arterialinjury models compared to that in the rat A-V shunt model in thepresent study. In all these models, BX 667 had much shallowerdose-response curves for both antithrombotic efficacy andbleeding compared to clopidogrel. This feature of BX 667 issimilar to that of FPL-67085, both of which are reversible pla-telet ADP-receptor antagonists, suggesting that their reversibil-ity allows a wider safe range of dose or plasma concentration fora more predictable efficacy than the irreversible clopidogrel (37,41). Drug-target residence time is important for both the efficacyand potential side effects of a drug (46). In the case of P2Y12 an-tagonists efficacy and bleeding are both due to the blockade ofthe receptor. Thus, while a long drug-target residence time im-proves efficacy, it would also inevitably increase bleeding.Clopidogrel, being an irreversible inhibitor would exacerbate thebleeding side effects, especially in situations where the patientreceives a hemostatic challenge or needs surgery.
Although the combination of clopidogrel and aspirin showedan additional 20% relative risk reduction for future events (com-posite of death from cardiovascular causes, non-fatal myocardialinfarction, or stroke) in patients with acute coronary syndromes,it was associated with a 30% increase in major bleeding, com-pared to aspirin treatment alone (12). In the present study, pre-treatment with aspirin itself increased bleeding by 45%. Co-treatment of either BX 667 or clopidogrel together with aspirinfurther increased bleeding compared to that of either individualtreatment. However, the therapeutic index of the BX 667-aspirincombination was still wider than that of the clopidogrel-aspirincombination. This result further demonstrates the relative safetyof BX 667 compared with clopidogrel even when the bleedingrisk has already been increased by co-treatment with aspirin, andsuggests that a combination therapy consisting of the irreversibleinhibitor, aspirin, and a reversible P2Y12 inhibitor may be a bettertherapeutic option than the combination of two irreversible pla-telet inhibitors in the treatment of cardiovascular disease.
In summary, although currently used oral platelet inhibitors(aspirin, ticlopidine, clopidogrel) are relatively safe, they areonly modestly effective in preventing arterial thrombosis. Thepresent data provide strong evidence that an orally active and re-versible ADP-receptor antagonist could represent a new medicalentity for platelet inhibition with a wider therapeutic index thanother platelet inhibitors currently on the market.

Wang et al. Inhibition of thrombin by a reversible ADP antagonist
855
AbbreviationsADP, adenosine diphosphate; A-V shunt, arterial venous shunt; ED, ef-fective dose; EC, effective concentration; AUC, area under the curve;PBS, phosphate buffered saline; PK, pharmacokinetics; PD, phar-macodynamics; IV, intravenous; PO, oral.
17. Caplain H, Thebault JJ, Necciari J. Clopidogreldoes not affect the pharmacokinetics of theophylline.Semin Thromb Hemost 1999; 25 (Suppl 2): 65–68.18. Steinhubl SR, Berger PB, Brennan DM, et al. Opti-mal timing for the initiation of pre-treatment with 300mg clopidogrel before percutaneous coronary inter-vention. J Am Coll Cardiol 2006; 47: 939–943.19. Steinhubl SR, Berger PB, Mann JT, 3rd, et al. Earlyand sustained dual oral antiplatelet therapy followingpercutaneous coronary intervention: a randomizedcontrolled trial. J Am Med Assoc 2002; 288:2411–2420.20. Bennett CL, Connors JM, Carwile JM, et al.Thrombotic thrombocytopenic purpura associatedwith clopidogrel. N Engl J Med 2000; 342: 1773–1777.21. Lau WC, Gurbel PA. Antiplatelet drug resistanceand drug-drug interactions: Role of cytochrome P4503A4. Pharm Res 2006; 23: 2691–2708.22. Neubauer H, Mugge A. Thienopyridines and sta-tins: assessing a potential drug-drug interaction. CurrPharm Des 2006; 12: 1271–1280.23. Cattaneo M. Aspirin and clopidogrel: Efficacy,safety, and the issue of drug resistance. 2004; 1980–7.24. Cattaneo M, Gachet C. ADP receptors and clinicalbleeding disorders. Arterioscler Thromb Vasc Biol1999; 19: 2281–2285.25. Nguyen TA, Diodati JG, Pharand C. Resistance toclopidogrel: a review of the evidence. J Am Coll Car-diol 2005; 45: 1157–1164.26. WangTH, Bhatt DL,Topol EJ.Aspirin and clopido-grel resistance: an emerging clinical entity. Eur Heart J2006; 27: 647–654.27. Falati S, Gross P, Merrill-Skoloff G, et al. Real-timein vivo imaging of platelets, tissue factor and fibrinduring arterial thrombus formation in the mouse. NatMed 2002; 8: 1175–1181.28. Falati S, Gross PL, Merrill-Skoloff G, et al. In vivomodels of platelet function and thrombosis: study ofreal-time thrombus formation. Methods Mol Biol2004; 272: 187–197.29. Wang YX, Dong N, Wu C, et al. Lipopolysacchar-ide attenuates thrombolysis in batroxobin-induced lungvasculature fibrin deposition but not in ferrous chlor-ide-induced carotid artery thrombus in rats: role of en-dogenous PAI-1. Thromb Res 2003; 111: 381–387.30. Folts JD, Crowell EB, Jr., Rowe GG. Platelet aggre-gation in partially obstructed vessels and its elimin-ation with aspirin. Circulation 1976; 54: 365–370.31. Eidt JF, Ashton J, Golino P, et al. Thromboxane A2and serotonin mediate coronary blood flow reductionsin unsedated dogs.Am J Physiol 1989; 257: H873–882.32. Eidt JF, Ashton J, Golino P, et al. Treadmill exercisepromotes cyclic alterations in coronary blood flow indogs with coronary artery stenoses and endothelial in-jury. J Clin Invest 1989; 84: 517–527.33. Eidt JF, Allison P, Noble S, et al. Thrombin is an im-portant mediator of platelet aggregation in stenosed ca-nine coronary arteries with endothelial injury. J Clin In-vest 1989; 84: 18–27.34. Eidt JF, Allison P, Noble S, et al. Thrombin is an im-portant mediator of cyclic coronary blood flow vari-ations due to platelet aggregation in stenosed canine
coronary arteries. Trans Assoc Am Physicians 1988;101: 125–136.35. Willerson JT, Yao SK, McNatt J, et al. Frequencyand severity of cyclic flow alternations and platelet ag-gregation predict the severity of neointimal prolifer-ation following experimental coronary stenosis and en-dothelial injury. Proc Natl Acad Sci USA 1991; 88:10624–10628.36. Huang J, Driscoll EM, Gonzales ML, et al. Preven-tion of arterial thrombosis by intravenously adminis-tered platelet P2T receptor antagonist AR-C69931MXin a canine model. J Pharmacol Exp Ther 2000; 295:492–499.37. Robertson MJ, Humphries RG, Tomlinson W, et al.The effects of FPL 67085 on thrombosis and haemosta-sis in the anaesthetized dog: Comparison with aspirinand the GPIIb/IIIa antagonists, Ro 449883 and GR144053. Br J Pharmacol 1994; 113: 64P.38. van Giezen JJ, Humphries RG. Preclinical andclinical studies with selective reversible direct P2Y12antagonists. Semin Thromb Hemost 2005; 31:195–204.39. Wang K, Zhou X, Zhou Z, et al. Blockade of theplatelet P2Y12 receptor by AR-C69931MX sustainscoronary artery recanalization and improves the myo-cardial tissue perfusion in a canine thrombosis model.Arterioscler Thromb Vasc Biol 2003 2003; 23:357–362.40. Storey RF, Wilcox RG, Heptinstall S. Comparisonof the pharmacodynamic effects of the platelet ADP re-ceptor antagonists clopidogrel and AR-C69931MX inpatients with ischaemic heart disease. Platelets 2002;13: 407–413.41. Wyld PJ, Gardner JJ, Wilkinson D, et al. Dose-re-sponse relationship and elimination characteristics ofthe short-acting P2T-purinoceptor antagonist FPL67085 in man. Blood 1994; 84 (Suppl 1): 475a.42. Greenbaum AB, Grines CL, Bittl JA, et al. Initialexperience with an intravenous P2Y12 platelet receptorantagonist in patients undergoing percutaneous coron-ary intervention: results from a 2-part, phase II, multi-center, randomized, placebo- and active-controlledtrial. Am Heart J 2006; 151: 689.e1-.e10.43. Ono M, Nawa K, Marumoto Y. Antithrombotic ef-fects of recombinant human soluble thrombomodulinin a rat model of vascular shunt thrombosis. ThrombHaemost 1994; 72: 421–425.44. Berry CN, Girard D, Lochot S, et al. Antithrom-botic actions of argatroban in rat models of venous,'mixed' and arterial thrombosis, and its effects on thetail transection bleeding time. Br J Pharmacol 1994;113: 1209–1214.45. Dong N, Da CunhaV, CitkowiczA, et al. P-selectin-targeting of the fibrin selective thrombolytic Desmo-dus rotundus salivary plasminogen activator alpha1.Thromb Haemost 2004; 92: 956–965.46. Copeland RA, Pompliano DL, Meek TD. Drug-tar-get residence time and its implications for lead optimiz-ation. Nat Rev Drug Discov 2006; 5: 730–739.
References1. Roth GJ, Stanford N, Majerus PW. Acetylation ofprostaglandin synthase by aspirin. Proc Natl Acad SciUSA 1975; 72: 3073–3076.2. Antiplatelet-Trialists'-Collaboration-I. Collabor-ative overview of randomised trials of antiplatelet ther-apy--I: Prevention of death, myocardial infarction, andstroke by prolonged antiplatelet therapy in various cat-egories of patients. Br Med J 1994; 308: 81–106.3. Antiplatelet-Trialists'-Collaboration-II. Collabor-ative overview of randomised trials of antiplatelet ther-apy--II: Maintenance of vascular graft or arterial paten-cy by antiplatelet therapy. Br Med J 1994; 308:159–168.4. Antiplatelet-Trialists'-Collaboration-III. Collabor-ative overview of randomised trials of antiplatelet ther-apy--III: Reduction in venous thrombosis and pulmon-ary embolism by antiplatelet prophylaxis among surgi-cal and medical patients. Br Med J 1994; 308: 235–246.5. Savi P, Herbert JM, Pflieger AM, et al. Importanceof hepatic metabolism in the antiaggregating activity ofthe thienopyridine clopidogrel. Biochem Pharmacol1992; 44: 527–532.6. Pereillo JM, Maftouh M, Andrieu A, et al. Structureand stereochemistry of the active metabolite of clopi-dogrel. Drug Metab Dispos 2002; 30: 1288–1295.7. Savi P, Pereillo JM, Uzabiaga MF, et al. Identifica-tion and biological activity of the active metabolite ofclopidogrel. Thromb Haemost 2000; 84: 891–896.8. Savi P, Herbert JM. ADP receptors on platelets andADP-selective antiaggregating agents. Med Res Rev1996; 16: 159–179.9. Hollopeter G, Jantzen HM, Vincent D, et al. Identi-fication of the platelet ADP receptor targeted by anti-thrombotic drugs. Nature 2001; 409: 202–207.10. CAPRIE-Steering-Committee. A randomised,blinded, trial of clopidogrel versus aspirin in patients atrisk of ischaemic events (CAPRIE). Lancet 1996; 348:1329–1339.11. Harker LA, Boissel JP, Pilgrim AJ, et al. Com-parative safety and tolerability of clopidogrel and as-pirin: results from CAPRIE. CAPRIE Steering Com-mittee and Investigators. Clopidogrel versus aspirin inpatients at risk of ischaemic events. Drug Saf 1999; 21:325–335.12. CURE-Trial. The Clopidogrel in Unstable Anginato Prevent Recurrent Events Trial Investigators. Effectsof clopidogrel in addition to aspirin in patients withacute coronary syndromes without ST-segment elev-ation. N Engl J Med 2001, 2001; 345: 494–502.13. Thebault JJ, Kieffer G, Lowe GD, et al. Repeated-dose pharmacodynamics of clopidogrel in healthy sub-jects. SeminThromb Hemost 1999; 25 (Suppl 2): 9–14.14. Caplain H, Cariou R. Long-term activity of clopi-dogrel: a three-month appraisal in healthy volunteers.Semin Thromb Hemost 1999; 25 (Suppl 2): 21–24.15. Caplain H, D'Honneur G, Cariou R. Prolonged he-parin administration during clopidogrel treatment inhealthy subjects. Semin Thromb Hemost 1999; 25(Suppl 2): 61–64.16. Caplain H, Donat F, Gaud C, et al. Pharmacoki-netics of clopidogrel. Semin Thromb Hemost 1999; 25(Suppl 2): 25–28.
AcknowledgementsThe authors would like to thank Jeff Davis, Keith Place, Dave Smith, KarenMay, Roberta Hough, Lorraine Kent for their support of this work. This re-search was part of the discovery and development of ADP antagonists car-ried out in Berlex Biosciences, USA, an affiliation of Schering AG, Ger-many, by which all authors were employed.




















