Health status and the end-of-life stage
12
Author's personal copy Health status and the end-of-life stage Robert J. Johnson a,1 , Krysia N. Mossakowski b, *, Terrence D. Hill c,2 a Sociology Department, University of Miami, 5202 University Drive, 120 Merrick, Coral Gables, FL 33146, United States b Sociology Department, University of Hawaii at Manoa, Saunders Hall, Room 215, 2424 Maile Way, Honolulu, HI 96822, United States c Sociology Department, Florida State University, Bellamy 514, Tallahassee, FL 32306-2270, United States 1. Introduction Although there are subtle differences in the conceptuali- zation between earlier and later life stages, almost all life stages are closely linked to chronological age (Settersten & Mayer, 1997). Earlier stages of the life course are numerous and cover narrow age ranges (e.g., pre-natal, newborn, infant, child, adolescent, emerging adult, and young adult). Some life stages, such as young adulthood, have been defined by transitions into social roles rather than by specific ages (Billari & Liefbroer, 2010; Shanahan, 2000). Late life stages, however, have been stratified by age, such as ‘‘young old,’’ ‘‘old,’’ and ‘‘oldest old’’ (Suzman & Riley, 1985). Our study uses an underutilized approach that moves beyond chronological age. Instead of conceptualizing the life course as life stages delineated by specific ages, we identify the changes in self-rated health status and functional health limitations that occur when older adults pass from a vital stage of life into a stage where they are nearing ‘‘the-end-of-life (EOL) stage.’’ The major differ- ence is the reference point of the EOL stage. In lieu of referencing change in terms of differences between starting points and current time (e.g., birth and current age), or between earlier times and current time (e.g., changes in age or time), the EOL stage uses an end point of time (death) for the major reference point. Focusing on the number of years prior to death, with an emphasis on self- reported health problems and functional limitations, rather than age as a signal of demise, has important theoretical implications for how life course researchers can advance our understanding of late life. 2. Background Researchers interested in aging have used a variety of strategies to conceptualize and analyze different stages and experiences of older adults near the end of life. Some studies Advances in Life Course Research 16 (2011) 132–143 A R T I C L E I N F O Article history: Received 4 April 2011 Received in revised form 8 July 2011 Accepted 3 August 2011 Keywords: Life course End-of-life stage Self-rated health status Functional limitations A B S T R A C T Although numerous studies highlight the social, psychological, and physiological significance of life stages based on specific ages, little scholarly attention has been devoted to identifying factors that distinguish the stage prior to death. Instead of conceptualizing the life course as stages delineated by specific ages, our study explores the changes in self-rated health status and functional health limitations that occur when older adults pass from a vital stage of life into the end-of-life stage. Using data from the Longitudinal Study on Aging, we compare the health status of those at varying points near the end-of-life (died within 1–6 years from the initial interview) to vital survivors (survived beyond 6 years). Controlling for age, sex, race, education, and a host of diagnosed diseases and serious health conditions, those in the end-of-life stage have more lower and upper body limitations, greater difficulty with activities of daily living, and worse overall self-rated health than vital survivors. We conclude that the end-of-life stage should be considered a unique period in the life course that is irreducible to age. ß 2011 Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +1 808 956 8416; fax: +1 808 956 3707. E-mail addresses: [email protected] (R.J. Johnson), [email protected] (K.N. Mossakowski), [email protected] (T.D. Hill). 1 Tel.: +1 305 284 6768; fax: +1 305 284 5310. 2 Tel.: +1 850 644 6416; fax: +1 850 644 6208. Contents lists available at ScienceDirect Advances in Life Course Research jou r nal h o mep ag e: w ww .elsevier .co m /loc ate/alc r 1040-2608/$ – see front matter ß 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.alcr.2011.08.002
-
Upload
manoa-hawaii -
Category
Documents
-
view
2 -
download
0
Transcript of Health status and the end-of-life stage

Author's personal copy
Health status and the end-of-life stage
Robert J. Johnson a,1, Krysia N. Mossakowski b,*, Terrence D. Hill c,2
a Sociology Department, University of Miami, 5202 University Drive, 120 Merrick, Coral Gables, FL 33146, United Statesb Sociology Department, University of Hawaii at Manoa, Saunders Hall, Room 215, 2424 Maile Way, Honolulu, HI 96822, United Statesc Sociology Department, Florida State University, Bellamy 514, Tallahassee, FL 32306-2270, United States
1. Introduction
Although there are subtle differences in the conceptuali-zation between earlier and later life stages, almost all lifestages are closely linked to chronological age (Settersten &Mayer, 1997). Earlier stages of the life course are numerousand cover narrow age ranges (e.g., pre-natal, newborn,infant, child, adolescent, emerging adult, and young adult).Some life stages, such as young adulthood, have beendefined by transitions into social roles rather than byspecific ages (Billari & Liefbroer, 2010; Shanahan, 2000). Latelife stages, however, have been stratified by age, such as‘‘young old,’’ ‘‘old,’’ and ‘‘oldest old’’ (Suzman & Riley, 1985).
Our study uses an underutilized approach that movesbeyond chronological age. Instead of conceptualizing the
life course as life stages delineated by specific ages, weidentify the changes in self-rated health status andfunctional health limitations that occur when older adultspass from a vital stage of life into a stage where they arenearing ‘‘the-end-of-life (EOL) stage.’’ The major differ-ence is the reference point of the EOL stage. In lieu ofreferencing change in terms of differences betweenstarting points and current time (e.g., birth and currentage), or between earlier times and current time (e.g.,changes in age or time), the EOL stage uses an end point oftime (death) for the major reference point. Focusing on thenumber of years prior to death, with an emphasis on self-reported health problems and functional limitations,rather than age as a signal of demise, has importanttheoretical implications for how life course researcherscan advance our understanding of late life.
2. Background
Researchers interested in aging have used a variety ofstrategies to conceptualize and analyze different stages andexperiences of older adults near the end of life. Some studies
Advances in Life Course Research 16 (2011) 132–143
A R T I C L E I N F O
Article history:
Received 4 April 2011
Received in revised form 8 July 2011
Accepted 3 August 2011
Keywords:
Life course
End-of-life stage
Self-rated health status
Functional limitations
A B S T R A C T
Although numerous studies highlight the social, psychological, and physiological
significance of life stages based on specific ages, little scholarly attention has been
devoted to identifying factors that distinguish the stage prior to death. Instead of
conceptualizing the life course as stages delineated by specific ages, our study explores
the changes in self-rated health status and functional health limitations that occur when
older adults pass from a vital stage of life into the end-of-life stage. Using data from the
Longitudinal Study on Aging, we compare the health status of those at varying points near
the end-of-life (died within 1–6 years from the initial interview) to vital survivors
(survived beyond 6 years). Controlling for age, sex, race, education, and a host of
diagnosed diseases and serious health conditions, those in the end-of-life stage have more
lower and upper body limitations, greater difficulty with activities of daily living, and
worse overall self-rated health than vital survivors. We conclude that the end-of-life stage
should be considered a unique period in the life course that is irreducible to age.
� 2011 Elsevier Ltd. All rights reserved.
* Corresponding author. Tel.: +1 808 956 8416; fax: +1 808 956 3707.
E-mail addresses: [email protected] (R.J. Johnson),
[email protected] (K.N. Mossakowski), [email protected] (T.D. Hill).1 Tel.: +1 305 284 6768; fax: +1 305 284 5310.2 Tel.: +1 850 644 6416; fax: +1 850 644 6208.
Contents lists available at ScienceDirect
Advances in Life Course Research
jou r nal h o mep ag e: w ww .e lsev ier . co m / loc ate /a lc r
1040-2608/$ – see front matter � 2011 Elsevier Ltd. All rights reserved.
doi:10.1016/j.alcr.2011.08.002

Author's personal copy
examine mortality, death and dying, and age stratificationamong the oldest old (Suzman & Riley, 1985). Othersconsider attitudes toward death itself (Kastenbaum, 1985).Studies of the oldest old were introduced more than 25 yearsago (Suzman & Riley, 1985) and have since proliferated.Although mortality rates are higher among the oldest oldcompared to other age groups, many of the oldest old are notyet near the end of life. For example, in 2004, the CDC (2007)estimated that 83,114 out of 100,000 births would survive toage 65. The number declined to 66,605 out of 100,000 forthose at age 75 and to 38,321 out of 100,000 at age 85. Whilemany of these adults will remain alive and vital for severalyears to come, these survivors may be more vital than manyadults in younger age groups. Thus, while death and dying orthe oldest old may be considered to be in the final stage ofthe life course, the time just preceding death at any age maybe thought of as the penultimate stage of the life course.
The strategy for studying the stage near the end of lifethat has been underutilized is to stratify by proximity todeath. In the same way that the chronological method ofmeasuring age in terms of time elapsed since birth islargely a proxy for many life circumstances, attitudes, andnorms about aging, stratifying the older adult populationon time periods prior to death using longitudinal data canreflect distinct characteristics of life circumstances (e.g.,health status, quality of life), attitudes (e.g., religiousbeliefs, life satisfaction) and norms (e.g., health careutilization) about the EOL stage. For example, studieshave used the proximity to death approach to examinehealth care utilization (Roos, Montgomery, & Roos, 1987;Wolinsky, Stump, & Johnson, 1995) and the use of informalcare (Johnson, Gallagher, & Wolinsky, 2004). Research hasalso used this approach to consider religiosity, spirituality(Idler, Kasl, & Hayes, 1998), quality of life (Idler,McLaughlin, & Kasl, 2009), and life satisfaction (Gerstorf,Ram, Rocke, Lindenberger, & Smith, 2008). Regardinghealth status, Guralnik, LaCroix, Branch, Kasl, and Wallace’(1991) groundbreaking study documented that decedentshad more self-rated functional limitations in the 3 yearspreceding death than those who survived. Moreover, levelsof activities in daily living (ADL) disability and mobilitylimitations increased substantially prior to death, butchronic diseases did not show a consistent increase withage at death. Bernard and colleagues’ (1997) studyrevealed that when taking into account chronic diseases,a global measure of self-rated functional disabilitysignificantly predicted a shorter time until death amongolder adults. Lunney, Lynn, Foley, Lipson, and Guralnik’(2003) study found that those in the final month of lifewere substantially more disabled (ADL) than thoseinterviewed 12 months before death among those whodied of cancer, organ failure, or frailty. Cancer decedentshad relatively better functional status early in the last yearof life, but the steepest decline in functional status in thelast 3 months of life. Other research has similarly shownthat people who died of cancer often experienced aprecipitous functional decline in the last 5 months of life,whereas people with other diagnosed health conditions (4other leading causes of death) generally had morefunctional (ADL) limitations in the last year of life and amore gradual decline (Teno, Weitzen, Fennell, & Mor,
2001). A recent study by Keeler, Guralnik, Tian, Wallace,and Reuben (2010) showed that 75-year-old men andwomen without functional limitations had 5 more years tolive than those with ADL limitations and more than 1 yearlonger in life expectancy than those with limited walkingmobility. Therefore, more studies of functional limitationsand disability prior to death are needed, especially thoseadjusting for chronic health conditions. Overall, thisapproach of examining proximity to death has greatpotential for integration into the life course paradigm.
The present study uses this approach to focus on self-rated health status and functional limitations during thelast few years of life in an effort to determine how thosewho are near the end of life experience their health.Compared to the earlier study by Guralnik and colleagues(1991), we examine a longer time period before death andmore health outcomes, one of which includes a measure ofself-rated health.
Self-rated health is widely used to measure generalphysical health status. It is thought to capture a wide rangeof physical health problems, including diagnosed or knownconditions and symptoms of undiagnosed or unknownconditions (Idler & Benyamini, 1997). It is stronglycorrelated with more objective measures of physicalhealth, including physician diagnoses, and various mea-sures of morbidity (Blyth et al., 2001; Idler & Benyamini,1997; Manderbacka, Lundberg, & Martikainen, 1999;Mossey & Shapiro, 1982). Self-rated health is also apowerful predictor of mortality and life expectancy. Somestudies have found that among patients diagnosed with adisease, self-rated health status is a robust predictor ofsurvival time (Bosworth et al., 1999; Dasbach, Klein, Klein,& Moss, 1994). Research on general populations has alsodemonstrated that self-rated health is a significantpredictor of mortality (Benyamini, Leventhal, & Leventhal,1999; Bernard et al., 1997; Ferraro & Kelley-Moore, 2001;Idler & Benyamini, 1997; Wolinsky & Johnson, 1993), if nota better predictor than clinical diagnosis of disease (Ferraro& Farmer, 1999). Therefore, self-rated health status is animportant measure that can improve our understanding ofold age and the EOL stage.
Health status can also be measured with functionallimitations, which are restrictions regarding physicalstrength, mobility (e.g., upper and lower body), thehousehold (e.g., problems doing chores), and cognition(e.g., problems managing money and using the telephone) inour daily lives (Johnson & Wolinsky, 1994; Long & Pavalko,2004). Essentially, functional limitations shed light on thedisability process. An illuminating finding in the work ofLong and Pavalko (2004) is that self-rated functionallimitations do not depend on age. Thus, additional researchis needed to understand the extent to which functionallimitations signify the EOL stage – irrespective of age.
2.1. Aging and Health
It is commonly believed that health deteriorates as theolder adult ages, with the rate of deterioration increasingover the period before death. Observing the deteriorationin self-rated health status with age has been a dominantresearch agenda (see Idler, 1993). Billari (2009) has
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143 133

Author's personal copy
highlighted that life course researchers have made majoradvancements in recent years by examining health withlongitudinal data.
One thing we have learned is that aging and declines inself-rated health status, while related, are conceptuallyseparate processes. As a person grows older, health statusdeteriorates more or less rapidly, depending on individualbiological, psychological, and social characteristics. Forsome groups, the diversity in health status amongindividuals of the same age can be nearly as great as thediversity in health status among individuals across wideage ranges. In other words, it is certainly possible forpeople to have more in common because of their self-ratedhealth status than because of their age. Thus, health statusmay aptly represent a recognizable change that ischaracteristic of a unique stage of life.
Health status is increasingly recognized as a complex,multidimensional phenomenon (Clark, Stump & Wolinsky,1997; Johnson & Wolinsky, 1993, 1994; Lawrence, 1995;Leinonen, Heikkinen & Jylha, 1999; Pinquart, 2001; Stump,Clark, Johnson, & Wolinsky, 1997; Wilson & Cleary, 1995;Wolinsky, 1996). In order to deal with some of thecomplexities, some researchers have examined thechanges in individual indicators of self-rated health status(Long & Pavalko, 2004; Wolinsky, Stump, Callahan, &Johnson, 1996), advocated use of a single global disabilityindicator (Verbrugge, 1997; Verbrugge, Merrill, & Liu,1999), discussed strategies of measuring morbidity with asimple count of diseases or using binary variables (Ferraro& Wilmoth, 2000), analyzed trajectories of functionallimitations (Wolinsky, Armbrecht, & Wyrwich, 2000), orattempted to specify a process of disablement (Jette, 1997,1999; Jette, Assmann, Rooks, Harris, & Crawford, 1998;Lawrence & Jette, 1996; Leinonen, Heikkinen, & Jylha,2001; Verbrugge & Jette, 1994). Most of these researchefforts have one thing in common: they link health statuswith chronological aging.
2.2. Paradigms of aging
Previous paradigms concerning changes in healthstatus often relied on biological conceptualizations ofhealth based on chronological age. ‘‘Age is only a ‘roughindicator’ of an individual’s status along biological, social,or psychological dimensions’’ (Settersten & Mayer, 1997:240). Other paradigms have expressed aging in terms ofpsychological (childhood development to maturation andsenility) and social aging processes (childhood, adoles-cence, young adulthood, middle age, and old age) (seeSettersten & Mayer, 1997). The life-course paradigmemphasizes the consequences of the ‘‘timing’’ of normativelife events and transitions (Elder, Johnson, & Crosnoe,2004: 12). For example, the principle of timing has guidedresearch on the life consequences of the age at entry intomilitary service (Elder, 1999), health disparities based onthe ages when adult social roles are entered, whichrepresents the transition to adulthood (Billari & Liefbroer,2010; Shanahan, 2000), and the distinct mental healtheffects of the age at immigration (Mossakowski, 2007).However, periods of old ages are often neglected orunderstudied. Age stratification (young old, old, oldest old)
came closest to providing a paradigm for understandinglater life (Suzman & Riley, 1985). For instance, the ‘‘young–old’’ have been categorized as ages 65–74, or between ages65 and 84, and the ‘‘old–old’’ have been defined as thoseages 75 or older, or 85 and older (Settersten & Mayer,1997). This chronological approach usually compares agegroups to draw conclusions about the aging process,changes in health status, and risk factors for mortality.‘‘Although the prevalence rates of disease and disabilityincrease with age, there is no a priori reason to believe thatwithin older populations those dying at younger agesshould have less disability prior to death than those dyingat older ages’’ (Guralnik et al., 1991: 445)
2.3. End-of-life stage
Our study conceptualizes the EOL stage withoutemphasizing chronological age. According to ‘‘the life-stage principle’’ from the life-course paradigm, health canvary by life stage not only because of age, but in large partdue to personal histories, life events, social roles, andsocial-psychological resources (Elder, 1987). In contrast tochronological aging paradigms, the EOL stage is not simplydefined by specific years of age. It is characterized bytemporal proximity to death and changes in self-ratedhealth status and functional limitations
The EOL stage envisions older adults transitioning from avital stage in their lives to the penultimate stage of the lifecourse that is often defined by diminishing health andvitality. The vital stage of life is one in which a person canreasonably expect to survive for several years, remainingrelatively healthy and physically and socially functional (asopposed to those who have a closer proximity to death).These older adults are termed here as vital survivors (VS).The EOL stage begins when a person can no longerreasonably expect to be such a survivor, and health andvitality diminish in his or her life. It is at this stage thatdistinctive changes in life circumstances (e.g., health),behaviors (e.g., health care utilization), attitudes (e.g.,religious beliefs, life satisfaction), life events (e.g., retire-ment), and social roles (e.g., caregiver) may occur that willlikely render chronological paradigms of aging less relevantto their experiences during the transition to the end of life.Individuals and members of their social networks in the EOLstage may or may not recognize this as the EOL, but they willlikely be aware of the transition because of these changes intheir lives. In essence, our lifecourse study explores whetherpeople in the EOL stage share similar experiences withregard to their self-rated health and functional limitations,perhaps entirely independent of age.
We compare vital survivors (VS) with those in EOL stageby examining six dimensions of health status, which havebeen verified among different racial groups (Johnson &Wolinsky, 1993, 1994) and in a wider range of samples ofolder adults (Johnson et al., 2004; Long & Pavalko, 2004;Markides et al., 2001; Ng, Niti, Chiam, & Kua, 2006;Simonsick et al., 2001; Wolinsky et al., 2007). Morespecifically, the conceptual dimensions of health statusinclude two dimensions of physical limitations, threedimensions of limitations in activities of daily living, andself-rated health.
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143134

Author's personal copy
3. Methods
3.1. Data
This study uses detailed information on the health andfunctioning of older individuals in the United States whowere included in the Supplement on Aging (SOA) from theNational Health Interview Survey conducted in 1984(response rate = 92.3%). Used in this analysis is the subsetof 7527 noninstitutionalized persons who were part of theLongitudinal Study on Aging (LSOA), which was a follow-up of that 1984 survey. Subjects selected for the follow-upwere aged 70 years or older at the time of their interview inthe 1984 SOA. They were interviewed subsequently in1986, 1988, and 1990 for the LSOA. Face-to-face interviewsin the respondents’ households were conducted for thebaseline interview and then Computer Assisted TelephoneInterviews were used for the LSOA follow-up waves. All ofthe data used in the present analysis are based on self-reports given in the first interview in 1984, which involvedproxies in 8.6 percent of the cases, and date of deathinformation collected over the next six years throughmatching with the National Death Index. In this study, wereport results based on the unweighted data. The results ofsupplementary analyses using weighted data did notsubstantively differ. Findings of others confirm that thesampling design of the LSOA has little impact on varianceestimation (see Fitti & Kovar, 1987), and moreover, anyimpact is sufficiently attenuated by the inclusion of age(see Harris, Kovar, Suzman, Kleinman, & Feldman, 1989)and other covariates (see Johnson & Wolinsky, 1993) inmultivariate analyses. In our analyses, we adjust theregression models for age, race, gender, education, andproxy use. It should be noted that not all subjects providedcomplete information on all the variables, and thus list-wise deletion was used, accounting for small differences inthe sample sizes in our analyses (see Table 3).
The LSOA is distinctive in part because the lifeexperiences it measures occurred during recent decadesof mortality improvement and it documents life-courseprocesses in an early historical period of the aging of ourpopulation, among a group of older adults two generationsin advance of the baby boomers. Greater detail on thedesign and execution of the LSOA can be found elsewhere(Centers for Disease Control, 2011 http://www.cdc.gov/nchs/lsoa/lsoa1.htm; Fitti & Kovar, 1987).
3.2. Measures
3.2.1. Demographic, disease, and health condition variables
The demographic control variables include age (70–99+), sex (male = 1, female = 0), the number of years ofeducation, and race (white = 1, other = 0). The ‘‘other’’ racecategory includes Indian (Aleutian, American, Eskimo),Asian/Pacific Islander, Black, multiple race, or other. Thereare also 15 dichotomous indicators of self-reporteddiagnosis of disease including osteoporosis, hip fracture,atherosclerosis, rheumatic fever, rheumatic heart disease,coronary heart disease, angina, myocardial infarction,heart attack, stroke, Alzheimer’s disease, cancer, arthritisand diabetes. Another control variable dichotomously
measures whether a proxy (household or non-householdmember who provided answers for the respondent) wasused to report health conditions
3.3. Dependent variables: health outcomes
3.3.1. Physical limitations
The types of physical limitations are measureddichotomously with a value of ‘‘1’’ reflecting a ‘‘yes’’answer to having difficulty in that activity and a value of‘‘0’’ indicating a ‘‘no’’ response. Three items (range 0–3),which include the inability to walk a quarter of a mile,walk up ten steps, or stand, are summed to measure lowerbody limitation (LBL). Three summed items (range 0–3),which include the inability to reach up over your head,reach out as if to shake hands, and grasp objects with yourfingers, comprise the measure of upper body limitation(UBL).
3.3.2. Activity limitations
Dichotomous items also are used to measure limita-tions in activities of daily living (ADL). A value of ‘‘1’’reflects a ‘‘yes’’ answer to the question about having anydifficulty performing the activity because of a health orphysical problem. A value of ‘‘0’’ indicates a response of ‘‘nodifficulty’’ or ‘‘do not do that activity for reasons other thanhealth.’’ Four measures are summed for basic ADL (BADL),which include difficulties in bathing, dressing, getting inand out of bed or a chair, and toileting. Household ADL(HADL) is measured by summing the following threeitems: difficulties in shopping, meal preparation, and lighthousework. Cognitive ADL (CADL) is a summative measureassessing difficulties in managing money and using thetelephone (Johnson & Wolinsky, 1993, 1994)
3.3.3. Self-rated Health
An ordinal item is used as an indicator of self-ratedhealth status. The respondents were asked, ‘‘Would yousay your health in general is excellent, very good, good, fair,or poor?’’ Self-rated health is ordered from low to highwith responses ranging (1–5) from poor, fair, good, verygood, to excellent. The construct of self-rated health isessentially a psychosocial assessment of physical healthstatus (Idler & Benyamini, 1997)
3.3.4. Vital survivors and end-of-life stage
The data were stratified to show differences amongthose who died within 1–6 calendar years (1984–1989)from the initial interview referred to as the end-of-life(EOL) stage, and vital survivors (VS), those who survivedbeyond (1989) 6 calendar years. Those in the EOL stage areplaced into 6 groups to characterize their decedent statusin terms of the number of years of life remaining (YLR)based on the year in which their death was recorded by theNational Death Index (see Appendix B). Six dichotomousvariables (YLR 1 to YLR 6) were created for the followingEOL stage sub-groups: those who had less than 1 year oflife remaining and whose death occurred in 1984 (YLR 1),at least 1 year but less than 2 years of life remaining (YLR2), at least 2 years but less than 3 years of life remaining(YLR3), at least 3 years but less than 4 years of life
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143 135

Author's personal copy
remaining (YLR4), at least 4 years but less than 5 years of liferemaining (YLR 5), and at least 5 years but less than 6 yearsof life remaining (YLR 6). Vital survivors (VS) have more than6 years of life remaining and VS is the reference category inthe regression models examining the relationship betweenYLR and health status
3.4. Analysis
We first examine the descriptive statistics for the datastratified by two groups (EOL and VS) by testing forsignificant differences in the initial bivariate (t-test)analyses. We then analyze the mean differences in healthstatus for the six dependent variables across the multiplegroups, the six years of life remaining (YLR) groups duringthe EOL stage and the vital survivors (VS). We comparethese results to the analyses of age differences across sixstrata of old age to highlight differences or similaritiesbetween age and YLR. These comparisons are made usingthe F statistic derived from ANOVA analyses to detectsignificant differences between multiple means. ANOVA isa relatively robust test for multiple differences especiallywhen sample sizes are large. ANOVA results are reliablewhen distributional assumptions are violated (Zar, 1996).Finally, we provide the OLS multiple regression resultsshowing the effects of YLR (EOL stage indicators) on the 6outcomes of health status controlling for age, education,sex, race, proxy, and the 15 disease and health conditions.The measures of health status are examined in two ways.First, we introduce several control variables to examine
their associations with the health status indicators. Thecontrol variables examined are demographic and diagnos-tic variables known to influence mortality or be importantnear the end of life. Second, we examine the relationshipbetween YLR in the EOL stage and health status, comparedto those who are vital survivors (VS).
4. Findings
4.1. Descriptive statistics, t-tests, and ANOVA
Table 1 compares those in the EOL stage to VS focusingon the means and standard deviations or percentages forthe variables measuring demographics, functional limita-tions, and self-rated health. The results for the t-tests areshown in the last column of Table 1. In sum, vital survivorsare in significantly better health on every measure of self-reported health status compared to those in the EOL stage.In addition, the VS group (mean = 76 years of age) issignificantly younger than the EOL group (mean = 80.0years of age). A significantly smaller proportion of vitalsurvivors are male compared to those at the end of life.
ANOVA results also confirm that the years of liferemaining (YLR) are significantly related to the differenthealth status indicators, such that those dying closer to thefirst year of the interview had significantly worse self-rated health and more functional limitations and dis-abilities than those dying later or surviving. The numbersof observations in the 6 subgroups of YLR are reported inTable 2. Of the 7527 older adults interviewed, 163 (2.2%)
Table 1
Means/standard deviations or percent � 95% CI and t-tests for variables in the analyses comparing end of life (EOL) and vital survivor (VS) stages among older
adults.
Vital survivors EOL stage
Mean/% Std/CI Mean/% Std/CI t-Value
Demographics
Age 76.0 5.0 80.0 6.3 �19.5
Male 34.5% 2.4 46.8% 2.5 �9.6
White 91.5% 1.4 91.2% 1.4 0.5
Proxy 6.1% 1.4 14.7% 1.6 �10.3
Lower body limitations
Walk 27.0% 2.3 53.3% 2.4 �21.1
Steps 22.8% 2.2 44.5% 2.4 �17.6
Stand 32.8% 2.4 55.5% 2.5 �17.8
Stoop 38.3% 2.5 55.1% 2.5 �13.3
Lift 25 37.0% 2.5 56.8% 2.5 �15.5
Upper body limitation
Reach up 14.5% 1.9 25.3% 2.1 �10.2
Reach out 1.7% 0.8 4.9% 1.0 �6.4
Grasp 9.5% 1.6 16.3% 1.7 �7.6
Basics ADL
Bath 7.6% 1.6 23.5% 1.9 �16.2
Dress 4.5% 1.3 14.6% 1.6 �12.5
Bed/Chair 7.0% 1.5 16.0% 1.7 �10.4
Toilet 2.8% 1.1 12.2% 1.5 �12.7
Household ADL
House 4.9% 1.4 18.5% 1.7 �15.3
Meal 5.0% 1.4 18.5% 1.7 �15.1
Shop 9.0% 1.7 27.7% 1.2 �17.9
Cognitive ADL
Telephone 3.9% 1.2 11.7% 1.5 �10.5
Money 3.7% 1.2 14.0% 1.6 �13.0
Health
Self-rated 3.2 1.2 2.6 1.3 17.2
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143136

Author's personal copy
had less than 1 year of life remaining (YLR 1) because theydied at some point in 1984, 346 (4.6%) had less than 2 yearsof life remaining (YLR 2), 392 (5.2%) had less than 3 YLR,384 (5.1%) had less than 4 YLR, 372 (4.9%) had less than 5YLR, 400 (5.3%) had less than 6 YLR.2 The VS numbered
5150 (68.4%). The F-statistics show statistically significantdifferences for the associations among the categories ofYLR and each of the health indicators: lower bodylimitations (F = 16, 6 df, p < .001), upper body limitations(F = 6, 6 df, p < .001), basic ADLs (F = 38, 6 df, p < .001),household ADLs (F = 39, 6 df, p < .001), cognitive ADLs(F = 27, 6 df, p < .001), and self-rated health (F = 14, 6 df,p < .001). The F-statistics for the associations between ageand each of the dependent variables are as follows: lowerbody limitations (F = 25, 5 df, p < .001), upper bodylimitations (F = 5, 6 df, p < .001), basic ADLs (F = 30, 5 df,
Table 2
Means and CI of health status by age sextiles and years of life remaining (YRL vs. VS).
Years of life remaining YLR1 YLR2 YLR3 YLR4 YLR5 YLR6 VS
n = 163 n = 346 n = 392 n = 384 n = 372 n = 400 n = 5150
Mean � 95% CI Mean � 95% CI Mean � 95% CI Mean � 95% CI Mean � 95% CI Mean � 95% CI Mean � 95% CI
Self-rated health 2.28 0.19 2.40 0.13 2.68 0.13 2.77 0.12 2.81 0.12 2.92 0.13 3.23 0.03
Lower body limitations 1.80 0.20 1.85 0.14 1.54 0.13 1.51 0.13 1.39 0.13 1.31 0.13 0.82 0.03
Upper body limitations 0.48 0.12 0.58 0.09 0.49 0.08 0.47 0.08 0.40 0.07 0.38 0.07 0.25 0.02
Basic ADLs 0.80 0.18 0.66 0.11 0.55 0.10 0.46 0.09 0.38 0.08 0.34 0.07 0.15 0.01
Household ADLs 1.01 0.20 0.83 0.13 0.63 0.11 0.65 0.11 0.50 0.10 0.48 0.09 0.19 0.02
Cognitive ADLs 0.43 0.11 0.39 0.07 0.25 0.06 0.24 0.06 0.18 0.05 0.17 0.05 0.08 0.01
Age sextiles 70–74 75–79 80–84 85–89 90–94 95+
n = 3131 n = 2306 n = 1266 n = 608 n = 181 n = 35
Mean � 95% CI Mean � 95% CI Mean � 95% CI Mean � 95% CI Mean � 95% CI Mean � 95% CI
Lower body limitations 0.81 0.04 0.91 0.05 1.36 0.07 1.59 0.10 2.09 0.18 2.12 0.38
Upper body limitations 0.26 0.02 0.29 0.03 0.40 0.04 0.44 0.06 0.42 0.11 0.66 0.33
Basic ADLs 0.16 0.02 0.20 0.03 0.33 0.04 0.52 0.07 0.77 0.16 0.85 0.37
Household ADLs 0.17 0.02 0.25 0.03 0.44 0.05 0.74 0.09 1.20 0.19 1.60 0.45
Cognitive ADLs 0.06 0.01 0.10 0.02 0.15 0.02 0.34 0.05 0.62 0.11 0.80 0.31
Self-rated health 3.08 0.04 3.12 0.05 3.02 0.07 3.02 0.10 3.04 0.18 2.71 0.39
0
0.5
1
1.5
2
2.5
3
3.5
YLR1 YLR2 YLR3 YLR4 YLR5 YLR6 VS
HEALTH
&
DIFFICULTY
Years of Life Remaining
Self-rated Health Lowe r Body Limit a�ons Upp er Body Limit a�ons
Basic Ac �vi� es of Daily Li ving Household Ac� vi� es of Dai ly Living Cog ni� ve Ac �vi� es of D aily Li ving
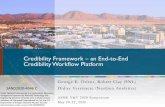
Fig. 1. Means of self-rated health, physical limitations, and difficulty with ADLs by years of life remaining (YLR).
2 The smaller sample and proportion of deaths for less than 1 YLR is
reflective of the fact that these subjects were not exposed to risk of death
for an entire calendar year as those whose deaths had less than 2 or 3–6
YLR.
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143 137

Author's personal copy
p < .001), household ADLs (F = 71, 5 df, p < .001), cognitiveADLs (F = 79, 5 df, p < .001), and self-rated health (F = 3, 5df, p < .01).
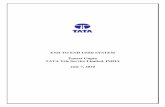
To illustrate the point, the chart appearing in Fig. 1demonstrates the mean differences for health status bycomparing those at various years in the EOL stage to VS.The comparisons across age in Fig. 2 show a pattern thatclearly distinguishes EOL from VS. The depiction of these
means over time with age shows a general pattern ofworsening self-rated health, functional limitations, andadditional difficulties (see Fig. 2). The older adults in eachlife stage, either VS or EOL show a gradual rise inlimitations and disabilities with age. In the cases oflimitations and disabilities, vital survivors always havelower levels of difficulty relative to those in the EOLstage. Those in the VS group also consistently report better
0
0.5
1
1.5
2
2.5
3
3.5
70-74 75-79 80-84 85-89 90-94 95+
Health
&
Difficulty
AGE
Lowe r Body Limita�ons Upp er Body Limita�ons Ba sic Ac�vi�es of D aily Living
Household Ac�vi�es of Dai ly Living Cogni�ve Ac�vi�es of D aily Living Self-rate d Heal th
Fig. 2. Means of self-rated health, physical limitations, and difficulty with ADLs by age category (70–95+).
Table 3
The unstandardized (b) and standardized (b) associations for demographics and EOL status with <1 to <6 years of life remaining (YLR) vs. VS on 6
dimensions of self-reported health status controlling for diagnoses of 15 diseases or conditions.
Lower body
limitations
Upper body
limitations
Basic ADLs Household ADLs Cognitive ADLs Self-rated
health
Independent variable b b b b b b b b b b b b
Age .03 .14*** .00 .02 .01 .07*** .02 .14*** .01 .13*** .02 .07***
Male �.20 �.08*** �.09 �.07*** �.08 �.06*** �.16 �.10*** �.01 �.01 �.03 �.01
White �.16 �.04*** �.06 �.03* �.05 �.02 �.12 �.04*** �.02 �.01 .16 .04***
Education �.09 �.08*** �.03 �.05*** .00 .00 �.01 �.01 �.01 �.03*** .17 .16***
Proxy .55 .12*** .22 .10*** .51 .21*** .70 .25*** .47 .32*** �.45 �.10***
YLR1 .56 .07*** .05 .01 .39 .09*** .51 .09*** .19 .07*** �.69 �.08***
YLR2 .66 .12*** .20 .07*** .28 .09*** .38 .11*** .15 .08*** �.60 �.11***
YLR3 .41 .08*** .17 .06*** .23 .08*** .21 .06*** .05 .03* �.35 �.06***
YLR4 .44 .08*** .11 .04*** .18 .06*** .28 .08*** .06 .03** �.36 �.07***
YLR5 .33 .06*** .05 .02 .12 .04*** .15 .04*** .02 .01 �.27 �.05***
YLR6 .27 .05*** .09 .03*** .11 .04*** .18 .05*** .02 .01 �.16 �.03**
R-square .29 .15 .23 .27 .27 .20
N 6581 6786 6827 6827 6827 6827
Note: Results presented above control for the diagnoses of osteoporosis, hip fracture, atherosclerosis, hypertension, rheumatic fever, rheumatic heart
disease, coronary heart disease, angina, myocardial infarction, heart attack, stroke, Alzheimer’s disease, cancer, arthritis, diabetes.* p < .05.** p < .01.*** p < .001.
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143138

Author's personal copy
self-rated health than those in the EOL stage. This suggeststhat vital survivors form a meaningful category of olderadults.
4.2. Multivariate results
The associations for the different EOL categories (YRL1 toYLR6 with VS as the reference category) with the 6dependent variables measuring health status are shownin Table 3, controlling for demographic variables (age, sex,race, education), proxy reporting of health status, anddiagnoses of 15 diseases and chronic conditions. Out of the36 coefficients for YLR during the EOL stage, 32 arestatistically significant and show a consistent trend ofweakening association (coefficient sizes moving closer tozero) with greater number of years of life remaining (YLR).For upper body limitations, having less than 1 year of liferemaining (YLR 1) or less than 5 years of life remaining (YLR5) were not statistically significant (Table 3). YLR 5 and YLR 6did not have significant associations with cognitive ADLs.Otherwise, there is a consistent trend of worse health statusfor those in the EOL stage compared to VS
To clarify this trend, the coefficients from the multi-variate analyses in Table 3 are charted in a bar graph (seeFig. 3). For BADL for example, the coefficients for YLR 1 toYLR 6, respectively, are b = .39, b = .28, b = .23, b = .18,b = .12, and b = .11. A similar pattern is repeated for theother functional disabilities. Likewise, self-rated health isworse for those with fewer years of life remaining(b = �.69; b = �.60; b = �.35; b = �.36; b = �.27; b = �.16).Overall, the bar graph (Fig. 3) shows a general trend of thecoefficients diminishing as the years of life remainingincrease. Thus, people in the EOL stage with more years oflife remaining generally have better health status.
5. Discussion
This study explored two interrelated issues in agingresearch, one conceptual and one methodological. First, we
examined the value of conceptualizing the EOL stage,which was inspired by the life course perspective and itsemphasis on studying transitions and life stages. This stageof life will necessarily overlap with other concepts such asterminal illness, dying, frail health, terminal drop, com-pression of morbidity, and old age (especially the oldest-old). It was expected, however, that the end of life wouldhave identifiable characteristics that, being distinct fromthese overlapping concepts, may have potential value forfuture gerontological, sociological, and life course researchon self-reported health and functional limitations. Thesecond issue involves the further specification of aretrospective research methodology using longitudinaldata. The methodology is best characterized as ‘‘countingage backwards’’ from the time of death.
Our findings partially replicate but also extend those ofthe first study by Guralnik and colleagues (1991) that usedthe proximity to death approach and highlighted theimportance of functional limitations. We used a differentand ideally suited data set (the LSOA) and a broader rangeof health indicators: (1) lower body limitations, (2) upperbody limitations, (3) cognitive disability, and (4) self-ratedhealth as being among the new dimensions examined.Guralnik et al. (1991) examined chronic health conditionsand ADL disability as outcomes. We also were able toinclude a broader range of chronic diseases and conditionsusing the LSOA, and we used these as control variables,rather than dependent variables. The relationship betweenproximity to death and functional status was adjusted forchronic disease and condition because chronic disease isinextricably linked to both functional status and mortality.We were also able to examine death within a 6 year period.Finally, our outcome measures reflected the level of healthstatus for each type of outcome, not the odds of having anyof one of several types. In our study, the operationalizationof this methodology provides a variable that represents the‘‘years of life remaining’’ (YLR). In previous efforts, thisvariable was used alternately as a dichotomous variablerepresenting the year of death or the number of years of life
Fig. 3. The pattern of associations between years of life remaining and health status in the multivariate analyses.
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143 139

Author's personal copy
remaining (Johnson et al., 2004; Wolinsky et al., 1995).Guralnik and colleagues’ (1991) study examined the 3years preceding death and compared a combined group ofdecedents in the 2nd and 3rd years to survivors. Theyfound that those who died at older ages had more (ADL)disability, but not disease, prior to death than those whodied at younger ages. We found similar bivariate results forour measures of ADLs, self-rated health, and functionallimitations across the age continuum and controlling forage in the multivariate models. Our findings indicated thatself-rated health status, functional limitations, and dis-abilities were significantly worse among those in the EOLstage compared to vital survivors. There was a decline inhealth status as one approaches death regardless of age.
Life course researchers should aim to capture the largerpicture of how life circumstances (e.g., quality of life),norms (e.g., retirement, caregiving), and attitudes (e.g.,religious beliefs, life satisfaction) change as self-ratedhealth and functional limitations worsen during the EOLstage. How these issues interconnect with increasingproximity to death, irrespective of age, requires greaterunderstanding to improve health care services andutilization. Roos and colleagues (1987: 247) concludedthat ‘‘dying has a greater impact on utilization thanaging. . ..’’ They found that decedents who were over theage of 84 did not spend as much time in the hospital ormake as many visits to physicians as those who died atyounger ages. This suggests that there was ‘‘compressionof morbidity,’’ which refers to health problems occurring ina shortened period of time at the end of life.
The usefulness of the concept of a stage at the end of lifewill depend, in part, on also having a reliable and validmodel of health status for both groups (EOL and VS). Futureresearch should ensure that this is the case. Such researchshould first examine whether EOL status has a moderatingeffect on the measurement properties of these dimensionsof health status and on the relationships among them. Asinterest in the growing number of older adults in ourpopulation increases, and the life course perspective isincreasingly applied to the end of life, these findingsprovide an important baseline for future studies so we candetermine if there is a trend or whether this is a stablephenomenon. Research examining other cohorts, such asthe Baby Boom Generation, can be compared to ourfindings to establish historical period effects. To advancethe growing end-of-life research literature, longitudinalstudies need to examine longer trajectories of dying fordifferent health conditions (George, 2002). Interestingly,recent research suggests that sudden functional declineacross different health conditions among those in pallia-tive care should be considered ‘‘a sentinel event’’ orwarning that death is near (Downing, Lesperance, Lau, &Yang, 2010: 555). According to our study, deficits infunctioning occurred as early as 6 years prior to death, andworsened closer to the end of life.
5.1. Limitations
Although the results of this study indicate that theconcept of the EOL stage shows promise, we would like tohighlight several limitations. The first deals with the
question of terminal disease and dying. Among the EOLgroup, and despite being asked specifically to reportseveral diseases, a subset of individuals undoubtedly hadan undiagnosed or unmeasured terminal illness. Whetherand how those EOL individuals with a certain diagnosiswill differ from those without remains unresolved untilone obtains such a measure. Nevertheless, the certain anddifferential diagnosis of a terminal illness may be seen as aspecial condition of the EOL stage, not necessarily analternative or distinct phase of it
Another limitation is a possible problem caused byincluding long-term chronically ill (those who survive past6 years) among vital survivors. On the one hand, a long-term chronic illness may seem at odds with the notion ofvitality. On the other hand, many long-term chronically illmay adapt well to their illness and remain vital andrelatively functional over long periods of time. And furtherseparating the ill survivors from healthy survivors wouldartificially enhance the expected distinctive patterns andcharacteristics of health status among those near the endof life. To the extent that ill survivors persist as members ofthe vital survivor group, such a condition provides aconservative test of the hypotheses of differences betweenthe ill at the EOL stage and VS. Nonetheless, furtherinvestigation of the ill survivors will likely help todetermine whether and how much bias exists as a resultof including them with vital survivors following the lastmeasurement of YLR.
Finally, there may be a need to make a distinctionbetween the clinical EOL and normative EOL. Although allof the subjects in the current study were living in thecommunity at the time of the interview, many may havespent the EOL in hospital or nursing home settings largelyinfluenced by clinical factors.3 The point is that the healthcare system should not only target helping people withdiagnosed diseases in a clinical setting or not, but alsothose struggling with functional limitations and disabil-ities living at home in the EOL stage at any age. Makingthese conceptual distinctions and measuring them willlikely be useful in future research and have importanthealth policy implications. One of the ways that policy-makers should address the EOL stage and the increasingcost of health care is by focusing on preventative care. Forexample, public health initiatives such as at-home careshould be made more affordable and available. Moreover,programs should be targeted to improve social, cognitive,and physical functioning, which would ultimately increaselife expectancy and benefit overall quality of life.
5.2. Prospects for future life course research
Future research should examine the EOL stage toexplore other lifecourse principles. For example, moreresearch is necessary that uses the principle of ‘‘linkedlives’’ by examining changes in social relationships near
3 Although all subjects who participated were living at home during the
time of the interview, some were subsequently hospitalized or placed in a
nursing home. The numbers and correlates of these occurrences have
been reported elsewhere (Wolinsky, Callahan, Fitzgerald, & Johnson,
1992; Wolinsky, Culler, Callahan, & Johnson, 1994).
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143140

Author's personal copy
the end of life and the effects on health, well-being,longevity, and both formal and informal health care (Elderet al., 2004; Johnson et al., 2004). Furthermore, researchersshould recognize the role of ‘‘human agency’’ during theEOL stage, which involves people’s choices and behaviorsthat shape the quality of their remaining years of life (Elderet al., 2004). The life-course principle of ‘‘time and place’’highlights the importance of researching different histori-cal and geographical locations. Thus, more longitudinalstudies are necessary to compare and contextualize theself-reported health for successive cohorts of EOL and VS,using different proximities to death and more recentcohorts than this study, and cohorts in other countries. Theresearch questions in these cases would be to determinehow many years of survival are necessary before the EOLstage differences disappear and whether this varies by
historical period and country. Finally, there is some recentevidence of a decline in life satisfaction in old age (Gerstorfet al., 2008). More research is also needed to explore therole of symptoms of depression, which is often a co-morbidcondition with chronic illness. A potentially useful area ofexploration might include examining the effects ofdepression on self-rated health status, functional limita-tions, and life satisfaction in the transition to later life(Penninx, Leveille, Ferrucci, van Eijk, & Guralnik, 1999;Schnittker, 2005). Symptoms of depression can be a majorhealth issue for the older population (Penninx et al., 1999;Schnittker, 2005). Therefore, more questions can be askedabout how different people experience changes in mentalhealth, physical health, and quality of life, how theyperceive these changes, and exactly what factors aredriving these changes near the end of life.
References
Benyamini, Y., Leventhal, E. A., & Leventhal, H. (1999). Self-assessments ofhealth—What do people know that predicts their mortality? Research onAging, 21(3), 477–550.
Bernard, S. L., Kincade, J. E., Konrad, T. R., Arcury, T. A., Rabiner, D. J.,Woomert, A., et al. (1997). Predicting mortality from community
surveys of older adults: The importance of self-rated functionalability social sciences. Journal of Gerontology, 52B, S155–S163.
Billari, F. C., & Liefbroer, A. C. (2010). Towards a new pattern of transition toadulthood? Advances in Life Course Research, 15, 59–75.
Billari, F. C. (2009). The life course is coming of age. Advances in Life CourseResearch, 14, 83–86.
Appendix A. Correlations among the six dependent variables in the analyses (n = 7124)
1 2 3 4 5 6
1. Self-rated health 1.00
2. Household ADL �0.32 1.00
3. Basic ADL �0.31 0.70 1.00
4. Cognitive ADL �0.23 0.62 0.51 1.00
5. LBL �0.46 0.52 0.50 0.31 1.00
6. UBL �0.31 0.40 0.44 0.30 0.47 1.00
Mean 3.09 0.32 0.25 0.13 1.02 0.31
Std. dev. 1.24 0.82 0.69 0.42 1.23 0.65
Appendix B
Coding scheme for the end of life variablesThe dichotomous variables defining years of life remaining (YLR) and vital survivors (VS) are depicted in the diagram below. All
subjects were initially interviewed in 1984. Those who did not survive beyond the end of the calendar year (CY) are defined by
YLR1. Those defined by YLR2, interviewed in 1984, survived that calendar year but did not survive CY 1985. This coding scheme
was repeated for YLR3–YLR6. Those who were interviewed in 1984 and survived through 1989 are defined as vital survivors
(VS).
Years of death are determined by the recorded dates in the National Death Index (NDI).
Dichotomous variables YLR1–YLR6 and VS defined by year of reported death.
1984 1985 1986 1987 1988 1989 1990+
YLR1
YLR2 Survive ‘84
YLR2 Survive ‘85
YLR4 Survive ‘86
YLR5 Survive ‘87
YLR6 Survive ‘88
VS Survive ‘89
A shaded block indicates the CY in which the death is recorded in the NDI.
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143 141

Author's personal copy
Blyth, F., March, L., Brnabic, A., Jorm, L., Williamson, M., & Cousins, M. (2001).Chronic pain in Australia: A prevalence study. Pain, 89, 151–165.
Bosworth, H. B., Siegler, I. C., Brummett, B., Barefoot, J. C., Williams, R. B.,Clapp-Channing, N., et al. (1999). The association between self-ratedhealth and mortality in a well-characterized sample of coronary arterydisease patients. Medical Care, 37, 1226–1236.
Centers for Disease Control (2007). United States life tables, (2004). NationalVital Statistics Report (NVSR), 56, 9.
Centers for Disease Control (2011). Longitudinal study on aging. http://www.cdc.gov/nchs/lsoa/lsoa1.htm (accessed 21.06.11).
Clark, D. O., Stump, T. E., & Wolinsky, F. D. (1997). A race- and gender-specificreplication of five dimensions of functional limitation and disability.Journal of Aging and Health, 9(1), 28–42.
Dasbach, E., Klein, R., Klein, B., & Moss, S. (1994). Self-rated health andmortality in people with diabetes. American Journal of Public Health, 84,1775–1779.
Downing, G. M., Lesperance, M., Lau, F., & Yang, J. (2010). Survival implica-tions of sudden. Functional decline as a sentinel event using thepalliative performance scale. Journal of Palliative Medicine, 13(5),549–557.
Elder, G. H., Jr. (1987). War mobilization and the life course: A cohort ofWorld War II veterans. Sociological Forum, 2(3), 449–472.
Elder, G. H., Jr. (1999). Children of the great depression: Social change in lifeexperience (25th anniversary ed.). Boulder, CO: Westview Press.
Elder, G., Jr., Johnson, M. K., & Crosnoe, R. (2004). The emergence anddevelopment of life course theory. In J. Mortimer & M. J. Shanahan(Eds.), Handbook of the life course (pp. 3–19). New York: Springer.
Ferraro, K. F., & Farmer, M. M. (1999). Utility of health data from socialsurveys: Is there a gold standard for measuring morbidity? AmericanSociological Review, 64, 303–315.
Ferraro, K. F., & Kelley-Moore, J. A. (2001). Self-rated health and mortalityamong black and white adults: Examining the dynamic evaluationthesis. Journals of Gerontology Series B-Psychological Sciences and SocialSciences, 56(4), S195–S205.
Ferraro, K. F., & Wilmoth, J. M. (2000). Measuring morbidity: Disease counts,binary variables, and statistical power. Journals of Gerontology Series B-Psychological Sciences and Social Sciences, 55(3), S173–S189.
Fitti, J. E., & Kovar, M. G. (1987). The Supplement on Aging to the 1984 NationalHealth Interview Survey. DHHS Publication 87-1323. Washington, DC: USGovernment Printing Office.
George, L. K. (2002). Research design in end-of-life research: State of science.The Gerontologist, 42(3), 86–98 (Special Issue).
Gerstorf, D., Ram, N., Rocke, C., Lindenberger, U., & Smith, J. (2008). Declineinlife satisfaction in old age: Longitudinal evidence for links to distance-to-death. Psychology and Aging, 23(1), 154–168.
Guralnik, J. M., LaCroix, A. Z., Branch, L. G., Kasl, S., & Wallace, R. B. (1991).Morbidity and disability in older persons in the years prior to death.American Journal of Public Health, 81, 443–447.
Harris, T., Kovar, M. G., Suzman, R., Kleinman, J. C., & Feldman, J. J. (1989).Longitudinal study of physical ability in the oldest-old. American Journalof Public Health, 79, 698–702.
Idler, E. L. (1993). Age differences in self-assessments of health: Age changes,cohort differences, or survivorship? Journal of Gerontology: SocialSciences, 48, S289–S300.
Idler, E. L., & Benyamini, Y. (1997). Self-rated health and mortality: A reviewof twenty seven community studies. Journal of Health and Social Behavior,38, 21–37.
Idler, E. L., McLaughlin, J., & Kasl, S. (2009). Religion and the quality of livein the last year of life. Journal of Gerontology: Social Sciences, 64(4),528–537.
Idler, E. L., Kasl, S. V., & Hayes, J. C. (1998). Patterns of religious practice andbelief in the last year of life. The Journals of Gerontology: Social Sciences,56B(6), S326–S334.
Jette, A. M. (1997). Disablement outcomes in geriatric rehabilitation. MedicalCare, 35(6), JS28–JS37.
Jette, A. M. (1999). Disentangling the process of disablement. Social Science &Medicine, 48(4), 471–472.
Jette, A. M., Assmann, S. F., Rooks, D., Harris, B. A., & Crawford, S. (1998).Interrelation-ships among disablement concepts. Journals of Geron-tology Series A-Biological Sciences and Medical Sciences, 53(5),M395–M404.
Johnson, R. J., & Wolinsky, F. D. (1993). The structure of health status amongolder adults: Disease, disability, functional limitation, and perceivedhealth. Journal of Health and Social Behavior, 34, 105–121.
Johnson, R. J., & Wolinsky, F. D. (1994). Gender, race, and health: Thestructure of health status among older adults. The Gerontologist, 34(1),24–35.
Johnson, R. J., Gallagher, T. J., & Wolinsky, F. D. (2004). The influence of theend of life on the extent of informal help received by older adults.Research on Aging, 26(2), 259–283.
Kastenbaum, R. (1985). Dying and death: A life-span approach. In J. E. Birren& K. W. Schaie (Eds.), Handbook of the psychology of aging. New York: VanNorstrand Reinhold.
Keeler, E., Guralnik, J. M., Tian, H., Wallace, R. B., & Reuben, D. B. (2010). Theimpact of functional status on life expectancy in older persons. Journal ofGerontology: Medical Sciences, 65(7), 727–733.
Lawrence, R. H. (1995). The structure of physical health-status—Comparingproxies and self-respondents. Journal of Aging and Health, 7(1), 74–98.
Lawrence, R. H., & Jette, A. M. (1996). Disentangling the disablement process.Journals of Gerontology Series B-Psychological Sciences and Social Sciences,51(4), S173–S182.
Leinonen, R., Heikkinen, E., & Jylha, M. (1999). A path analysis model of self-rated health among older people. Aging-Clinical and Experimental Re-search, 11(4), 209–220.
Leinonen, R., Heikkinen, E., & Jylha, M. (2001). Predictors of decline in self-assessments of health among older people—A 5-year longitudinal study.Social Science and Medicine, 52(9), 1329–1341.
Long, J. R., & Pavalko, E. (2004). The life course of activity limitations:Exploring functional limitations over time. Journal of Aging and Health,16, 490–516.
Lunney, J. R., Lynn, J., Foley, D. J., Lipson, S., & Guralnik, J. M. (2003). Patternsof functional decline at the end of life. Journal of the American MedicalAssociation, 289(18), 2387–2392.
Manderbacka, K., Lundberg, O., & Martikainen, P. (1999). Do risk factors andhealth behaviors contribute to self-ratings of health? Social Science &Medicine, 48, 1717–1720.
Markides, R. S., Black, S. A., Ostir, G. V., Angel, R. J., Guralnik, J. M., &Lichenstein, M. (2001). Lower body function and mortality in MexicanAmerican elderly people. Journals of Gerontology Series A-BiologicalSciences and Medical Sciences, 56(4), M243–M247.
Mossakowski, K. N. (2007). Are immigrants healthier? The case of depressionamong Filipino Americans. Social Psychology Quarterly, 70, 290–304.
Mossey, J. K., & Shapiro, E. (1982). Self-rated health: A predictor of mortalityamong the elderly. American Journal of Public Health, 72(2), 800–808.
Ng, T., Niti, M., Chiam, P., & Kua, E. (2006). Physical and cognitive domains ofthe instrumental activities of daily living: Validation in a multiethnicpopulation of Asian older adults. Journals of Gerontology Series A: Biolog-ical Sciences and Medical Sciences, 61(7), 726–735.
Penninx, B. W. J. H. , Leveille, S., Ferrucci, L., van Eijk, J. T., & Guralnik, M. J.M. (1999). Exploring the effect of depression on physical disability:Longitudinal evidence from the established populations for epidemi-ologic studies of the elderly. American Journal of Public Health, 89(9),1346–1352.
Pinquart, M. (2001). Correlates of subjective health in older adults: A meta-analysis. Psychology and Aging, 16(3), 414–426.
Roos, N. P., Montgomery, P. R., & Roos, L. L., Jr. (1987). Hospital utilization inthe years prior death. Milbank Quarterly, 65(2), 231–254.
Schnittker, J. (2005). When mental health becomes health: Age and theshifting meaning of self-evaluations of general health. The MilbankQuarterly, 83, 397–423.
Settersten, R. A., & Mayer, K. U. (1997). The measurement of age, agestructuring, and the life course. Annual Review of Sociology, 23, 233–261.
Simonsick, E. M., Kasper, J. D., Guralnik, J. M., Bandeen-Roche, K., Ferrucci, L.,Hirsch, R., et al. (2001). Severity of upper and lower extremity functionallimitation: Scale development and validation with self-report and per-formance-based measures of physical function. Journal of Gerontology B-Psychological Science Social Science, 56, S10–S19.
Shanahan, M. J. (2000). Pathways to adulthood in changing societies: Vari-ability and mechanisms of the life course perspective. Annual Review ofSociology, 26, 667–692.
Stump, T. E., Clark, D. O., Johnson, R. J., & Wolinsky, F. D. (1997). The structureof health status among Hispanic African American, and white olderadults. Journals of Gerontology Series B-Psychological Sciences and SocialSciences, 52, 49–56.
Suzman, R., & Riley, M. W. (1985). Introducing the oldest old. MilbankMemorial Fund Quarterly-Health and Society, 63(2), 177–186.
Teno, J. M., Weitzen, S., Fennell, M. L., & Mor, V. (2001). Dying trajectory in thelast year of life: Does cancer trajectory fit other diseases? Journal ofPalliative Medicine, 4(4), 457–464.
Verbrugge, L. M. (1997). A global disability indicator. Journal of Aging Studies,11(4), 337–362.
Verbrugge, L. M., & Jette, A. M. (1994). The disablement process. Social Science& Medicine, 38(1), 1–14.
Verbrugge, L. M., Merrill, S. S., & Liu, X. (1999). Measuring disability withparsimony. Disability and Rehabilitation, 21(5–6), 295–306.
Wilson, I. B., & Cleary, P. D. (1995). Linking clinical-variables with health-related quality of life—A conceptual model of patient outcomes. JAMA,273(1), 59–65.
Wolinsky, F. D. (1996). Advances in the measurement of health status—Introduction. Gerontologist, 36(5), 570–657.
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143142

Author's personal copy
Wolinsky, F. D., Armbrecht, E. S., & Wyrwich, K. W. (2000). Rethinkingfunctional limitation pathways. Gerontologist, 40(2), 137–146.
Wolinsky, F. D., Callahan, C. M., Fitzgerald, J. F., & Johnson, R. J. (1992). Therisk of nursing home placement and subsequent death among olderadults. Journal of Gerontology, 47(4), 173–183.
Wolinsky, F. D., Culler, S. D., Callahan, C. M., & Johnson, R. J. (1994). Hospitalresource consumption among older adults: A prospective analysis ofepisodes, length of stay, and charges over a 7 year period. Journal ofGerontology, 49(5), 240–252.
Wolinsky, F. D., & Johnson, R. J. (1993). Perceived health status andmortality among older men and women. Journal of Gerontology, 47,S304–S312.
Wolinsky, F. D., Miller, T. M., Malmstrom, T. K., Miller, J. P., Schoolman, M.,Andresen, E. A., et al. (2007). Four-year lower extremity disabilitytrajectories among African American men and women. Journals of Ger-ontology Series A-Biological Sciences and Medical Sciences, 62(5), 525–530.
Wolinsky, F. D., Stump, T. E., Callahan, C. M., & Johnson, R. J. (1996).Consistency and change in functional status among older adults overtime. Journal of Aging and Health, 8(2), 155–182.
Wolinsky, F. D., Stump, T. E., & Johnson, R. J. (1995). Hospital utilization profilesamong older adults over time: Consistency and volume among survivorsand decedents. Journal of Gerontology: Social Sciences, 50B(2), S88–S100.
Zar, J. H. (1996). Biostatistical analysis (3rd ed.). Upper Saddle River, NJ:Prentice-Hall. p. 128.
R.J. Johnson et al. / Advances in Life Course Research 16 (2011) 132–143 143