Chronic extra-aortic balloon counterpulsation: First-in-human pilot study in end-stage heart failure
6
INNOVATION Chronic extra-aortic balloon counterpulsation: First-in-human pilot study in end-stage heart failure Christopher S. Hayward, MD, FRACP, a William S. Peters, MD, b,c Alan F. Merry, FANZCA, FRCA, b,c Peter N. Ruygrok, MD, FRACP, b,c Paul Jansz, FRACS, PhD, a Gerry O’Driscoll, PhD, FRACP d , Robert I. Larbalestier, FRACS, d Julian A. Smith, FRACS, e Betty Ho, FRACP, f Malcolm E. Legget, MD, FRACP, b,c and F. Paget Milsom, FRACS b,c From the a Department of Cardiology, Heart Lung Transplant Unit, St. Vincent’s Hospital, Darlinghurst, New South Wales, Australia; b Department of Cardiology, Auckland City Hospital, Auckland, New Zealand; c University of Auckland, Auckland, New Zealand; d Advanced Heart Failure and Cardiac Transplant Services, Royal Perth Hospital, Perth, Western Australia, Australia; e Monash Medical Centre (Clayton) and Department of Surgery (MMC), Monash University, Melbourne, Victoria, Australia; f Department of Cardiology, Dandenong Hospital, Victoria, Australia. BACKGROUND: Some patients continue to have significant heart failure symptoms despite optimal medical therapy. METHODS: We describe a first-in-human experience with an implantable non– blood-contacting extra- ascending aortic counterpulsation heart assist system (C-Pulse) in 5 end-stage heart failure patients, aged 54 to 73 years. RESULTS: All patients improved by 1 NYHA class and improvements in invasive hemodynamics were documented in 3 patients. Three of 5 patients (60%) had infectious complications. Two patients were explanted at 5 and 7 weeks, respectively, as a result of mediastinal infection related to the implant procedure. One patient was successfully transplanted at 1 month and 1 remained hemodynamically improved on the device at 6 months but suffered infective complications. The device and protocol have been modified as a result of this pilot study with a further multicenter safety study underway. CONCLUSIONS: Although feasibility of this device is suggested by this pilot study, safety and efficacy will need to be examined in a larger cohort with longer follow-up. J Heart Lung Transplant 2010;29:1427–32 © 2010 International Society for Heart and Lung Transplantation. All rights reserved. KEYWORDS: counterpulsation; heart-assist devices; heart failure; aorta; histology; extra-aortic Ambulatory intra-aortic balloon pump (IABP) counterpul- sation provides extended diastolic augmentation and pre-sys- tolic unloading of the heart in chronic heart failure patients and may relieve symptoms, reverse volume overload, mitigate ischemia and potentially allow re-remodeling and recovery, 1 or may be used as a bridge to transplant. 2 We report the first-in- human experience with the C-Pulse heart assist system (Sun- shine Heart, Inc., Eden Prairie MN), a non– blood-contacting, implantable aortic counterpulsation device. Methods Investigational device The C-Pulse cuff consists of a polyurethane balloon and polyester wrap fitted to conform to the ascending aorta. The Reprint requests: Christopher S. Hayward, MD, FRACP, Department of Cardiology, Heart Failure and Transplant Unit, St. Vincent’s Hospital, Victoria Street, Darlinghurst NSW 2010, Australia. Telephone: 61-2- 8382-6880. Fax: 61-2-8382-6881. E-mail address: [email protected] http://www.jhltonline.org 1053-2498/$ -see front matter © 2010 International Society for Heart and Lung Transplantation. All rights reserved. doi:10.1016/j.healun.2010.06.014
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Chronic extra-aortic balloon counterpulsation: First-in-human pilot study in end-stage heart failure
I
CF
CAPRM
FWAWM
stmi
oV8
http://www.jhltonline.org
1d
NNOVATION
hronic extra-aortic balloon counterpulsation:irst-in-human pilot study in end-stage heart failure
hristopher S. Hayward, MD, FRACP,a William S. Peters, MD,b,c
lan F. Merry, FANZCA, FRCA,b,c Peter N. Ruygrok, MD, FRACP,b,c
aul Jansz, FRACS, PhD,a Gerry O’Driscoll, PhD, FRACPd,obert I. Larbalestier, FRACS,d Julian A. Smith, FRACS,e Betty Ho, FRACP,f
alcolm E. Legget, MD, FRACP,b,c and F. Paget Milsom, FRACSb,c
rom the aDepartment of Cardiology, Heart Lung Transplant Unit, St. Vincent’s Hospital, Darlinghurst, New Southales, Australia; bDepartment of Cardiology, Auckland City Hospital, Auckland, New Zealand; cUniversity of Auckland,uckland, New Zealand; dAdvanced Heart Failure and Cardiac Transplant Services, Royal Perth Hospital, Perth,estern Australia, Australia; eMonash Medical Centre (Clayton) and Department of Surgery (MMC), Monash University,
elbourne, Victoria, Australia; fDepartment of Cardiology, Dandenong Hospital, Victoria, Australia.BACKGROUND: Some patients continue to have significant heart failure symptoms despite optimalmedical therapy.METHODS: We describe a first-in-human experience with an implantable non–blood-contacting extra-ascending aortic counterpulsation heart assist system (C-Pulse) in 5 end-stage heart failure patients,aged 54 to 73 years.RESULTS: All patients improved by 1 NYHA class and improvements in invasive hemodynamics weredocumented in 3 patients. Three of 5 patients (60%) had infectious complications. Two patients were explantedat 5 and 7 weeks, respectively, as a result of mediastinal infection related to the implant procedure. One patientwas successfully transplanted at 1 month and 1 remained hemodynamically improved on the device at 6 monthsbut suffered infective complications. The device and protocol have been modified as a result of this pilot studywith a further multicenter safety study underway.CONCLUSIONS: Although feasibility of this device is suggested by this pilot study, safety and efficacywill need to be examined in a larger cohort with longer follow-up.J Heart Lung Transplant 2010;29:1427–32© 2010 International Society for Heart and Lung Transplantation. All rights reserved.
KEYWORDS:counterpulsation;heart-assist devices;heart failure;aorta;histology;extra-aortic
mhsi
M
I
T
Ambulatory intra-aortic balloon pump (IABP) counterpul-ation provides extended diastolic augmentation and pre-sys-olic unloading of the heart in chronic heart failure patients anday relieve symptoms, reverse volume overload, mitigate
schemia and potentially allow re-remodeling and recovery,1 or
Reprint requests: Christopher S. Hayward, MD, FRACP, Departmentf Cardiology, Heart Failure and Transplant Unit, St. Vincent’s Hospital,ictoria Street, Darlinghurst NSW 2010, Australia. Telephone: �61-2-382-6880. Fax: �61-2-8382-6881.
pE-mail address: [email protected]
053-2498/$ -see front matter © 2010 International Society for Heart and Lungoi:10.1016/j.healun.2010.06.014
ay be used as a bridge to transplant.2 We report the first-in-uman experience with the C-Pulse heart assist system (Sun-hine Heart, Inc., Eden Prairie MN), a non–blood-contacting,mplantable aortic counterpulsation device.
ethods
nvestigational device
he C-Pulse cuff consists of a polyurethane balloon and
olyester wrap fitted to conform to the ascending aorta. TheTransplantation. All rights reserved.
ctlaadc6rancvtbsttlmwt
S
TeshItiH1
otducaeavectcdfp
I
Iclsfuwgmavs
R
Ttqactmscta3iN0
R
O
AFo
1428 The Journal of Heart and Lung Transplantation, Vol 29, No 12, December 2010
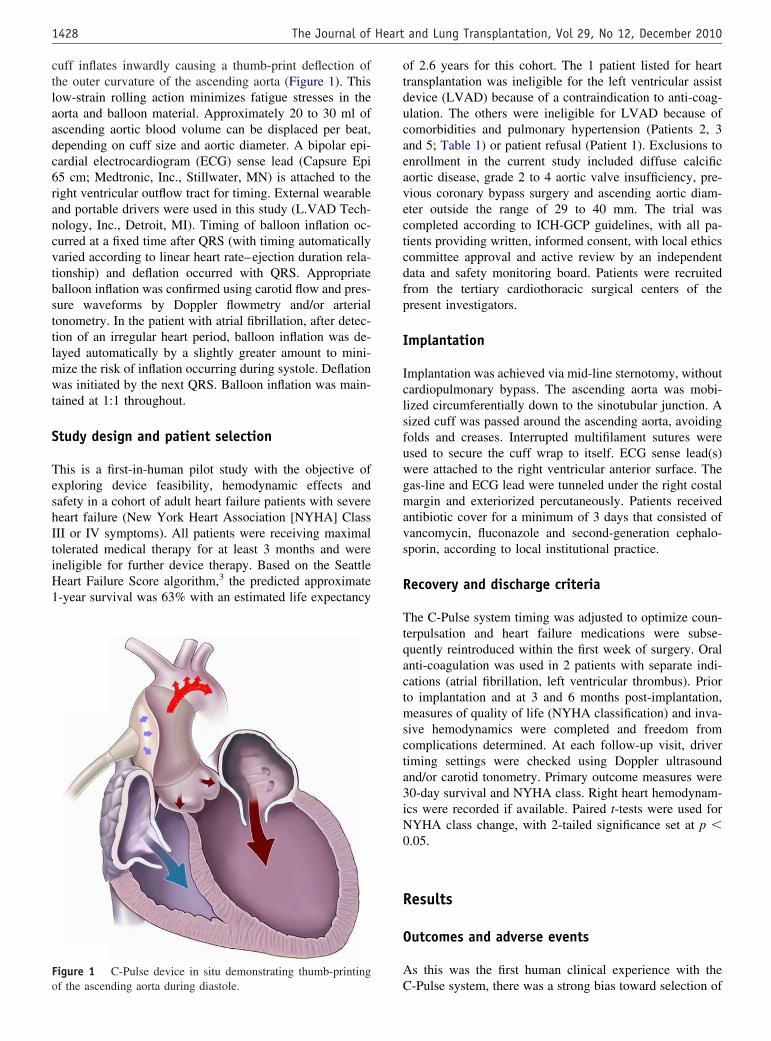
uff inflates inwardly causing a thumb-print deflection ofhe outer curvature of the ascending aorta (Figure 1). Thisow-strain rolling action minimizes fatigue stresses in theorta and balloon material. Approximately 20 to 30 ml ofscending aortic blood volume can be displaced per beat,epending on cuff size and aortic diameter. A bipolar epi-ardial electrocardiogram (ECG) sense lead (Capsure Epi5 cm; Medtronic, Inc., Stillwater, MN) is attached to theight ventricular outflow tract for timing. External wearablend portable drivers were used in this study (L.VAD Tech-ology, Inc., Detroit, MI). Timing of balloon inflation oc-urred at a fixed time after QRS (with timing automaticallyaried according to linear heart rate–ejection duration rela-ionship) and deflation occurred with QRS. Appropriatealloon inflation was confirmed using carotid flow and pres-ure waveforms by Doppler flowmetry and/or arterialonometry. In the patient with atrial fibrillation, after detec-ion of an irregular heart period, balloon inflation was de-ayed automatically by a slightly greater amount to mini-ize the risk of inflation occurring during systole. Deflationas initiated by the next QRS. Balloon inflation was main-
ained at 1:1 throughout.
tudy design and patient selection
his is a first-in-human pilot study with the objective ofxploring device feasibility, hemodynamic effects andafety in a cohort of adult heart failure patients with severeeart failure (New York Heart Association [NYHA] ClassII or IV symptoms). All patients were receiving maximalolerated medical therapy for at least 3 months and wereneligible for further device therapy. Based on the Seattleeart Failure Score algorithm,3 the predicted approximate-year survival was 63% with an estimated life expectancy
igure 1 C-Pulse device in situ demonstrating thumb-printing
Cf the ascending aorta during diastole.f 2.6 years for this cohort. The 1 patient listed for heartransplantation was ineligible for the left ventricular assistevice (LVAD) because of a contraindication to anti-coag-lation. The others were ineligible for LVAD because ofomorbidities and pulmonary hypertension (Patients 2, 3nd 5; Table 1) or patient refusal (Patient 1). Exclusions tonrollment in the current study included diffuse calcificortic disease, grade 2 to 4 aortic valve insufficiency, pre-ious coronary bypass surgery and ascending aortic diam-ter outside the range of 29 to 40 mm. The trial wasompleted according to ICH-GCP guidelines, with all pa-ients providing written, informed consent, with local ethicsommittee approval and active review by an independentata and safety monitoring board. Patients were recruitedrom the tertiary cardiothoracic surgical centers of theresent investigators.
mplantation
mplantation was achieved via mid-line sternotomy, withoutardiopulmonary bypass. The ascending aorta was mobi-ized circumferentially down to the sinotubular junction. Aized cuff was passed around the ascending aorta, avoidingolds and creases. Interrupted multifilament sutures weresed to secure the cuff wrap to itself. ECG sense lead(s)ere attached to the right ventricular anterior surface. Theas-line and ECG lead were tunneled under the right costalargin and exteriorized percutaneously. Patients received
ntibiotic cover for a minimum of 3 days that consisted ofancomycin, fluconazole and second-generation cephalo-porin, according to local institutional practice.
ecovery and discharge criteria
he C-Pulse system timing was adjusted to optimize coun-erpulsation and heart failure medications were subse-uently reintroduced within the first week of surgery. Oralnti-coagulation was used in 2 patients with separate indi-ations (atrial fibrillation, left ventricular thrombus). Prioro implantation and at 3 and 6 months post-implantation,easures of quality of life (NYHA classification) and inva-
ive hemodynamics were completed and freedom fromomplications determined. At each follow-up visit, driveriming settings were checked using Doppler ultrasoundnd/or carotid tonometry. Primary outcome measures were0-day survival and NYHA class. Right heart hemodynam-cs were recorded if available. Paired t-tests were used forYHA class change, with 2-tailed significance set at p �.05.
esults
utcomes and adverse events
s this was the first human clinical experience with the
-Pulse system, there was a strong bias toward selection of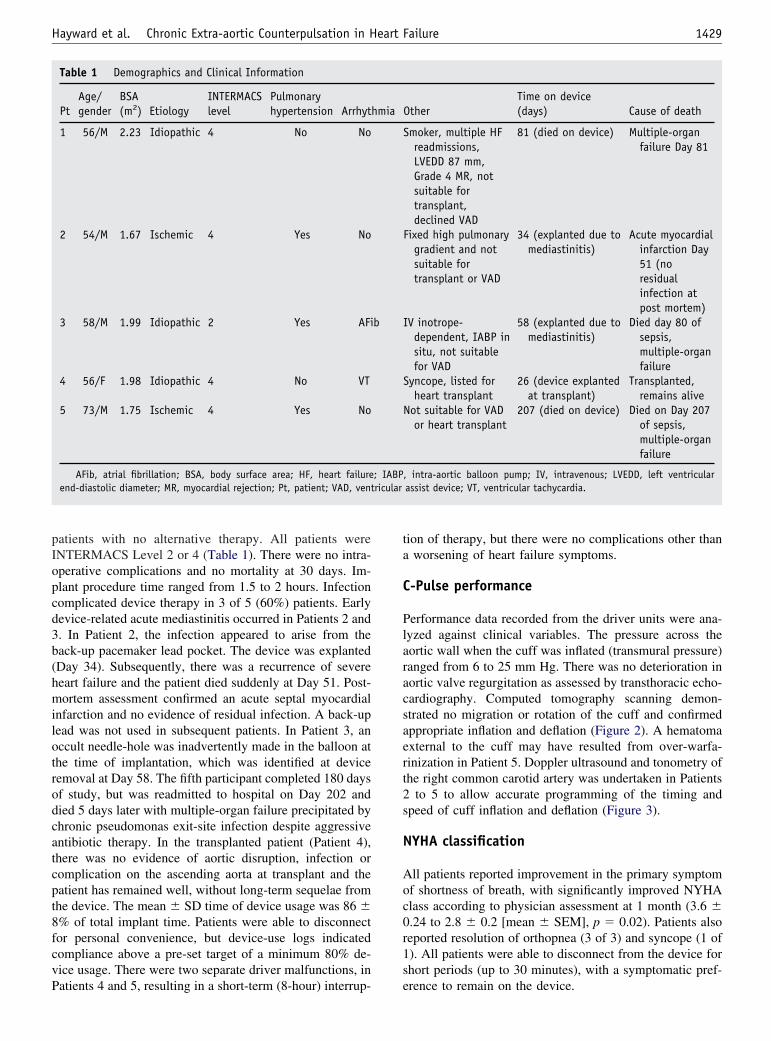
pIopcd3b(hmilotrodcatcpt8fcvP
ta
C
Plaracsaert2s
N
Aoc0r1s
1429Hayward et al. Chronic Extra-aortic Counterpulsation in Heart Failure
atients with no alternative therapy. All patients wereNTERMACS Level 2 or 4 (Table 1). There were no intra-perative complications and no mortality at 30 days. Im-lant procedure time ranged from 1.5 to 2 hours. Infectionomplicated device therapy in 3 of 5 (60%) patients. Earlyevice-related acute mediastinitis occurred in Patients 2 and. In Patient 2, the infection appeared to arise from theack-up pacemaker lead pocket. The device was explantedDay 34). Subsequently, there was a recurrence of severeeart failure and the patient died suddenly at Day 51. Post-ortem assessment confirmed an acute septal myocardial
nfarction and no evidence of residual infection. A back-upead was not used in subsequent patients. In Patient 3, anccult needle-hole was inadvertently made in the balloon athe time of implantation, which was identified at deviceemoval at Day 58. The fifth participant completed 180 daysf study, but was readmitted to hospital on Day 202 andied 5 days later with multiple-organ failure precipitated byhronic pseudomonas exit-site infection despite aggressiventibiotic therapy. In the transplanted patient (Patient 4),here was no evidence of aortic disruption, infection oromplication on the ascending aorta at transplant and theatient has remained well, without long-term sequelae fromhe device. The mean � SD time of device usage was 86 �% of total implant time. Patients were able to disconnector personal convenience, but device-use logs indicatedompliance above a pre-set target of a minimum 80% de-ice usage. There were two separate driver malfunctions, in
Table 1 Demographics and Clinical Information
PtAge/gender
BSA(m2) Etiology
INTERMACSlevel
Pulmonaryhypertension Arrhyt
1 56/M 2.23 Idiopathic 4 No No
2 54/M 1.67 Ischemic 4 Yes No
3 58/M 1.99 Idiopathic 2 Yes AFi
4 56/F 1.98 Idiopathic 4 No VT
5 73/M 1.75 Ischemic 4 Yes No
AFib, atrial fibrillation; BSA, body surface area; HF, heart failureend-diastolic diameter; MR, myocardial rejection; Pt, patient; VAD, vent
atients 4 and 5, resulting in a short-term (8-hour) interrup- e
ion of therapy, but there were no complications other thanworsening of heart failure symptoms.
-Pulse performance
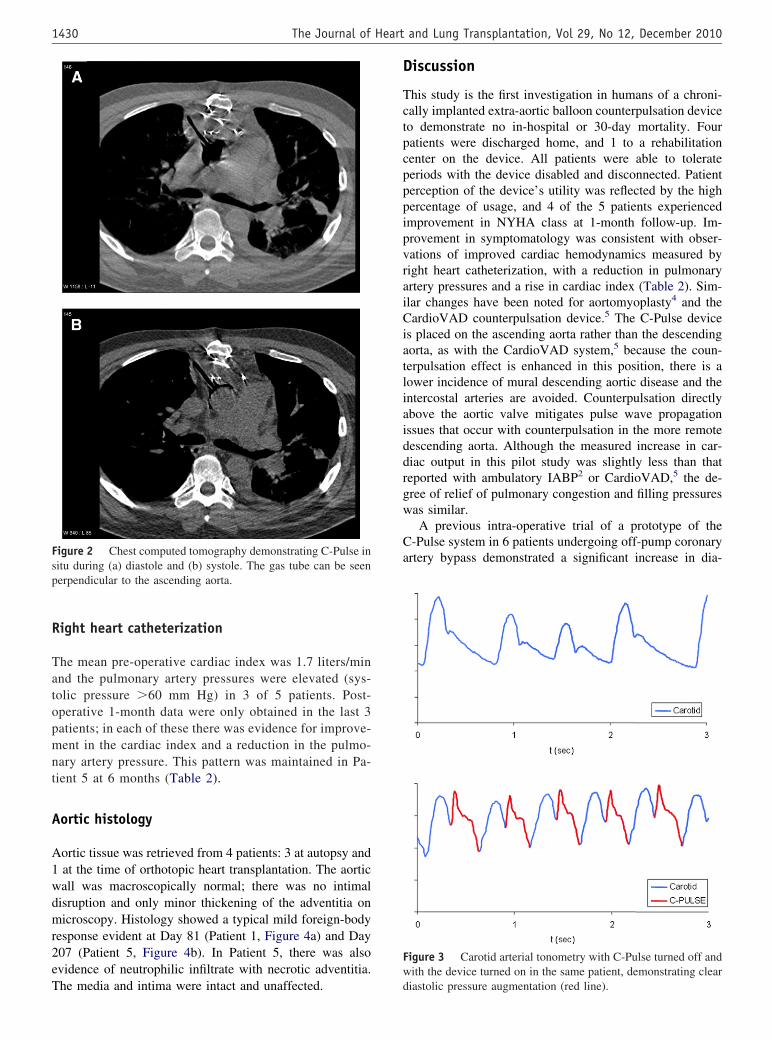
erformance data recorded from the driver units were ana-yzed against clinical variables. The pressure across theortic wall when the cuff was inflated (transmural pressure)anged from 6 to 25 mm Hg. There was no deterioration inortic valve regurgitation as assessed by transthoracic echo-ardiography. Computed tomography scanning demon-trated no migration or rotation of the cuff and confirmedppropriate inflation and deflation (Figure 2). A hematomaxternal to the cuff may have resulted from over-warfa-inization in Patient 5. Doppler ultrasound and tonometry ofhe right common carotid artery was undertaken in Patients
to 5 to allow accurate programming of the timing andpeed of cuff inflation and deflation (Figure 3).
YHA classification
ll patients reported improvement in the primary symptomf shortness of breath, with significantly improved NYHAlass according to physician assessment at 1 month (3.6 �.24 to 2.8 � 0.2 [mean � SEM], p � 0.02). Patients alsoeported resolution of orthopnea (3 of 3) and syncope (1 of). All patients were able to disconnect from the device forhort periods (up to 30 minutes), with a symptomatic pref-
OtherTime on device(days) Cause of death
Smoker, multiple HFreadmissions,LVEDD 87 mm,Grade 4 MR, notsuitable fortransplant,declined VAD
81 (died on device) Multiple-organfailure Day 81
Fixed high pulmonarygradient and notsuitable fortransplant or VAD
34 (explanted due tomediastinitis)
Acute myocardialinfarction Day51 (noresidualinfection atpost mortem)
IV inotrope-dependent, IABP insitu, not suitablefor VAD
58 (explanted due tomediastinitis)
Died day 80 ofsepsis,multiple-organfailure
Syncope, listed forheart transplant
26 (device explantedat transplant)
Transplanted,remains alive
Not suitable for VADor heart transplant
207 (died on device) Died on Day 207of sepsis,multiple-organfailure
, intra-aortic balloon pump; IV, intravenous; LVEDD, left ventricularassist device; VT, ventricular tachycardia.
hmia
b
; IABPricular
rence to remain on the device.
R
Tatopmnt
A
A1wdmr2eT
D
TctpcpppipvraiCiatliaiddrgw
Ca
Fw
Fsp
1430 The Journal of Heart and Lung Transplantation, Vol 29, No 12, December 2010
ight heart catheterization
he mean pre-operative cardiac index was 1.7 liters/minnd the pulmonary artery pressures were elevated (sys-olic pressure �60 mm Hg) in 3 of 5 patients. Post-perative 1-month data were only obtained in the last 3atients; in each of these there was evidence for improve-ent in the cardiac index and a reduction in the pulmo-
ary artery pressure. This pattern was maintained in Pa-ient 5 at 6 months (Table 2).
ortic histology
ortic tissue was retrieved from 4 patients: 3 at autopsy andat the time of orthotopic heart transplantation. The aorticall was macroscopically normal; there was no intimalisruption and only minor thickening of the adventitia onicroscopy. Histology showed a typical mild foreign-body
esponse evident at Day 81 (Patient 1, Figure 4a) and Day07 (Patient 5, Figure 4b). In Patient 5, there was alsovidence of neutrophilic infiltrate with necrotic adventitia.
igure 2 Chest computed tomography demonstrating C-Pulse initu during (a) diastole and (b) systole. The gas tube can be seenerpendicular to the ascending aorta.
he media and intima were intact and unaffected. d
iscussion
his study is the first investigation in humans of a chroni-ally implanted extra-aortic balloon counterpulsation deviceo demonstrate no in-hospital or 30-day mortality. Fouratients were discharged home, and 1 to a rehabilitationenter on the device. All patients were able to tolerateeriods with the device disabled and disconnected. Patienterception of the device’s utility was reflected by the highercentage of usage, and 4 of the 5 patients experiencedmprovement in NYHA class at 1-month follow-up. Im-rovement in symptomatology was consistent with obser-ations of improved cardiac hemodynamics measured byight heart catheterization, with a reduction in pulmonaryrtery pressures and a rise in cardiac index (Table 2). Sim-lar changes have been noted for aortomyoplasty4 and theardioVAD counterpulsation device.5 The C-Pulse device
s placed on the ascending aorta rather than the descendingorta, as with the CardioVAD system,5 because the coun-erpulsation effect is enhanced in this position, there is aower incidence of mural descending aortic disease and thentercostal arteries are avoided. Counterpulsation directlybove the aortic valve mitigates pulse wave propagationssues that occur with counterpulsation in the more remoteescending aorta. Although the measured increase in car-iac output in this pilot study was slightly less than thateported with ambulatory IABP2 or CardioVAD,5 the de-ree of relief of pulmonary congestion and filling pressuresas similar.A previous intra-operative trial of a prototype of the
-Pulse system in 6 patients undergoing off-pump coronaryrtery bypass demonstrated a significant increase in dia-
igure 3 Carotid arterial tonometry with C-Pulse turned off andith the device turned on in the same patient, demonstrating clear
iastolic pressure augmentation (red line).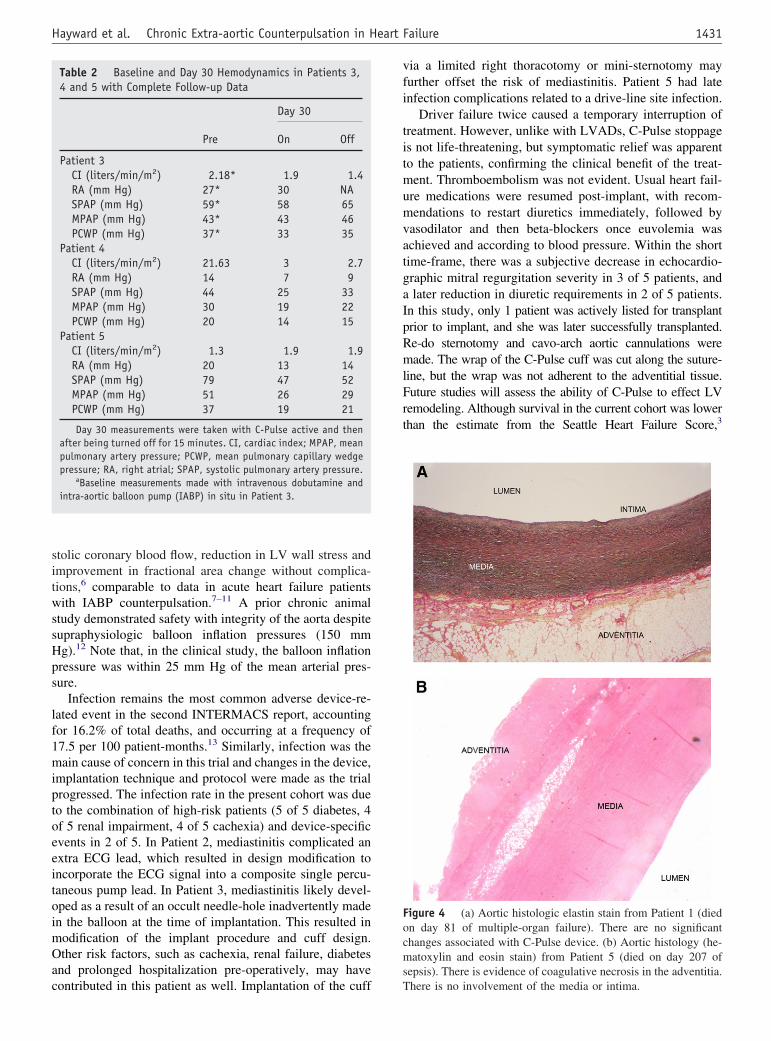
sitwssHps
lf1miptoeeitoimOac
vfi
titmumvatgaIpRmlFrt
Focms
1431Hayward et al. Chronic Extra-aortic Counterpulsation in Heart Failure
tolic coronary blood flow, reduction in LV wall stress andmprovement in fractional area change without complica-ions,6 comparable to data in acute heart failure patientsith IABP counterpulsation.7–11 A prior chronic animal
tudy demonstrated safety with integrity of the aorta despiteupraphysiologic balloon inflation pressures (150 mmg).12 Note that, in the clinical study, the balloon inflationressure was within 25 mm Hg of the mean arterial pres-ure.
Infection remains the most common adverse device-re-ated event in the second INTERMACS report, accountingor 16.2% of total deaths, and occurring at a frequency of7.5 per 100 patient-months.13 Similarly, infection was theain cause of concern in this trial and changes in the device,
mplantation technique and protocol were made as the trialrogressed. The infection rate in the present cohort was dueo the combination of high-risk patients (5 of 5 diabetes, 4f 5 renal impairment, 4 of 5 cachexia) and device-specificvents in 2 of 5. In Patient 2, mediastinitis complicated anxtra ECG lead, which resulted in design modification toncorporate the ECG signal into a composite single percu-aneous pump lead. In Patient 3, mediastinitis likely devel-ped as a result of an occult needle-hole inadvertently maden the balloon at the time of implantation. This resulted inodification of the implant procedure and cuff design.ther risk factors, such as cachexia, renal failure, diabetes
nd prolonged hospitalization pre-operatively, may have
Table 2 Baseline and Day 30 Hemodynamics in Patients 3,4 and 5 with Complete Follow-up Data
Day 30
Pre On Off
Patient 3CI (liters/min/m2) 2.18* 1.9 1.4RA (mm Hg) 27* 30 NASPAP (mm Hg) 59* 58 65MPAP (mm Hg) 43* 43 46PCWP (mm Hg) 37* 33 35
Patient 4CI (liters/min/m2) 21.63 3 2.7RA (mm Hg) 14 7 9SPAP (mm Hg) 44 25 33MPAP (mm Hg) 30 19 22PCWP (mm Hg) 20 14 15
Patient 5CI (liters/min/m2) 1.3 1.9 1.9RA (mm Hg) 20 13 14SPAP (mm Hg) 79 47 52MPAP (mm Hg) 51 26 29PCWP (mm Hg) 37 19 21
Day 30 measurements were taken with C-Pulse active and thenafter being turned off for 15 minutes. CI, cardiac index; MPAP, meanpulmonary artery pressure; PCWP, mean pulmonary capillary wedgepressure; RA, right atrial; SPAP, systolic pulmonary artery pressure.
aBaseline measurements made with intravenous dobutamine andintra-aortic balloon pump (IABP) in situ in Patient 3.
ontributed in this patient as well. Implantation of the cuff T
ia a limited right thoracotomy or mini-sternotomy mayurther offset the risk of mediastinitis. Patient 5 had latenfection complications related to a drive-line site infection.
Driver failure twice caused a temporary interruption ofreatment. However, unlike with LVADs, C-Pulse stoppages not life-threatening, but symptomatic relief was apparento the patients, confirming the clinical benefit of the treat-ent. Thromboembolism was not evident. Usual heart fail-
re medications were resumed post-implant, with recom-endations to restart diuretics immediately, followed by
asodilator and then beta-blockers once euvolemia waschieved and according to blood pressure. Within the shortime-frame, there was a subjective decrease in echocardio-raphic mitral regurgitation severity in 3 of 5 patients, andlater reduction in diuretic requirements in 2 of 5 patients.
n this study, only 1 patient was actively listed for transplantrior to implant, and she was later successfully transplanted.e-do sternotomy and cavo-arch aortic cannulations wereade. The wrap of the C-Pulse cuff was cut along the suture-
ine, but the wrap was not adherent to the adventitial tissue.uture studies will assess the ability of C-Pulse to effect LVemodeling. Although survival in the current cohort was lowerhan the estimate from the Seattle Heart Failure Score,3
igure 4 (a) Aortic histologic elastin stain from Patient 1 (diedn day 81 of multiple-organ failure). There are no significanthanges associated with C-Pulse device. (b) Aortic histology (he-atoxylin and eosin stain) from Patient 5 (died on day 207 of
epsis). There is evidence of coagulative necrosis in the adventitia.
here is no involvement of the media or intima.
wisbuTp
wasiPtvbe
D
Ttstp
Ih
R
1
1
1
1
1432 The Journal of Heart and Lung Transplantation, Vol 29, No 12, December 2010
hether this was due to underestimation by the SHFS (by notncorporating diabetic status, existence of pulmonary hyperten-ion or preceding mechanical support) or to the device has noteen answered in this pilot trial. A Phase I trial is currentlynderway in Class III or ambulant Class IV patients (Clinical-rials.gov identifier: NCT00815880), excluding patients withredicted poor short-term outcomes.
In conclusion, this is the first-in-human pilot trial fromhich significant device and procedural modifications have
risen. As a result of the experience reported herein, amaller C-Pulse driver has been developed, with designmprovements in the implanted cuff and percutaneous lead.atients reported in this cohort represented extreme cases of
herapy-intolerant heart failure, ineligible for alternate de-ice therapy. Although feasibility of this device is suggestedy this pilot study, safety and efficacy will need to bexamined in a larger cohort with longer follow-up.
isclosure statement
he authors acknowledge the considerable contributions ofhe clinical research coordinators and other investigativetaff, as well as the members of the data and safety moni-oring board (Chair: Professor Cliff Hughes, AO), in sup-orting this clinical trial.
W.S.P. and F.P.M. were consultants to Sunshine Heart,nc., at the time of this study. None of the remaining authorsave any conflicts of interest to disclose.
eferences
1. Buchanan SA, Langenburg SE, Mauney MC, et al. Ambulatory in-
traaortic balloon counterpulsation. Ann Thorac Surg 1994;58:1547-8.2. Cochran RP, Starkey TD, Panos AL, et al. Ambulatory intraaorticballoon pump use as bridge to heart transplant. Ann Thorac Surg2002;74:746-51.
3. Levy WC, Mozaffarian D, Linker DT, et al. The Seattle Heart FailureModel: prediction of survival in heart failure. Circulation 2006;113:1424-33.
4. Trainini J, Cabrera Fischer EI, Barisani J, et al. Dynamic aortomyo-plasty in treating end-stage heart failure. J Heart Lung Transplant2002;21:1068-73.
5. Jeevanandam V, Jayakar D, Anderson AS, et al. Circulatory assistancewith a permanent implantable IABP: initial human experience. Circu-lation 2002;106(suppl 1):I-183-8.
6. Legget ME, Peters WS, Milsom FP, et al. Extra-aortic balloon coun-terpulsation: an intraoperative feasibility study. Circulation 2005;112(suppl):I-26-31.
7. Cheung AT, Savino JS, Weiss SJ. Beat-to-beat augmentation of leftventricular function by intraaortic counterpulsation. Anesthesiology1996;84:545-54.
8. Hutchison SJ, Thaker KB, Chandraratna PA. Effects of intraaorticballoon counterpulsation on flow velocity in stenotic left main coro-nary arteries from transesophageal echocardiography. Am J Cardiol1994;74:1063-5.
9. Katz ES, Tunick PA, Kronzon I. Observations of coronary flow aug-mentation and balloon function during intraaortic balloon counterpul-sation using transesophageal echocardiography. Am J Cardiol 1992;69:1635-9.
0. Reichert CL, Koolen JJ, Visser CA. Transesophageal echocardiographicevaluation of left ventricular function during intraaortic balloon pumpcounterpulsation. J Am Soc Echocardiogr 1993;6:490-5.
1. Zehetgruber M, Mundigler G, Christ G, et al. Relation of hemody-namic variables to augmentation of left anterior descending coronaryflow by intraaortic balloon pulsation in coronary artery disease. Am JCardiol 1997;80:951-5.
2. Peters WS, Howlett CR, Power JM, et al. Aortic intimal integritymaintained following long-term extra-aortic balloon counterpulsationin sheep. Australian Society of Cardiothoracic Surgeons, November2004, Noosa, Australia.
3. Kirklin JK, Naftel DC, Kormos RL, et al. Second INTERMACSannual report: more than 1,000 primary left ventricular assist device
implants. J Heart Lung Transplant 2010;29:1-10.