Corticospinal excitability is specifically modulated by the social dimension of observed actions
Upload
independentCategory
view
1download
0
doi:10.1093/brain/awh558 Brain (2005) Page 1 of 11
Altered motor nerve excitability in end-stagekidney disease
Arun V. Krishnan,1,2 Richard K. S. Phoon,3 Bruce A. Pussell,3 John A. Charlesworth,3
Hugh Bostock4 and Matthew C. Kiernan1,2
1Institute of Neurological Sciences, Prince of Wales Hospital, Randwick, Sydney, Australia, 2Prince of Wales MedicalResearch Institute and Prince of Wales Clinical School, University of New South Wales, 3Department of Nephrology,Prince of Wales Hospital, Randwick, Sydney, Australia and 4Sobell Department of Neurophysiology, Institute of Neurology,Queen Square, London, UK
Correspondence to: Dr Matthew Kiernan, Prince of Wales Medical Research Institute, Barker Street, Randwick,Sydney, NSW 2031, AustraliaE-mail: [email protected]
Although multiple toxins have been implicated in the development of uraemic neuropathy, no causative agenthas been identified. In the present study, the excitability properties of lower limb motor nerves in patients withend-stage kidney disease treated with haemodialysis were measured before, during and after a standard 5 hhaemodialysis session, in an attempt to explore the pathophysiology of uraemic neuropathy. Compound muscleaction potentials were recorded from tibialis anterior and extensor digitorum brevis, following stimulationof the common peroneal nerve in 14 patients. Measures of excitability were assessed in relation to changesin serum levels of potential neurotoxins, including potassium, calcium, urea, uric acid, parathyroid hormoneand b-2-microglobulin. Before dialysis, measures of nerve excitability were significantly abnormal in thepatient group for axons innervating tibialis anterior and extensor digitorum brevis, consistent with axonaldepolarization: refractoriness was increased and superexcitability and depolarizing threshold electrotonuswere reduced. Pre-dialysis excitability abnormalities were strongly correlated with serum K+. Correlationwas also noted between the severity of symptoms and excitability abnormalities. Haemodialysis normalizedthe majority of nerve excitability parameters. In conclusion, lower limb motor axons in uraemic patientsare depolarized before dialysis. The correlation between serum K+ and excitability measures indicates thathyperkalaemia is primarily responsible for uraemic depolarization, and a likely contributing factor to thedevelopment of neuropathy.
Keywords: membrane potential; nerve excitability; potassium; threshold electrotonus; uraemic neuropathy
Abbreviations: b-2M = b-2-microglobulin; CMAP = compound muscle action potential; EDB = extensor digitorum brevis;ESKD = end-stage kidney disease; NCS = nerve conduction study; NSS = neuropathy symptom score; PTH = parathyroidhormone; SNAP = sensory nerve action potential; TA = tibialis anterior; TEd = depolarizing threshold electrotonus;TEh = hyperpolarizing threshold electrotonus; T-NSS = total neuropathy symptom score
Received February 24, 2005. Revised April 10, 2005. Accepted May 12, 2005
IntroductionPeripheral neuropathy in end-stage kidney disease (ESKD)
presents as a length-dependent, distal sensorimotor poly-
neuropathy with greater lower limb than upper limb
involvement (Bolton, 1980; Asbury, 1993). Previous studies
of neuropathy in ESKD have demonstrated prevalence rates
which vary from 60 to 100%, depending on the choice of
nerve segments, the indices measured and the number of
nerves studied (Nielsen, 1973; Bolton, 1980; Ackil et al.,
1981; Van den Neucker et al., 1998; Laaksonen et al., 2002).
The pathophysiology of uraemic neuropathy has not been
established. The finding that neurological complications of
renal failure may be improved by dialysis (Hegstrom et al.,
1962) and that patients receiving peritoneal dialysis had a
lower incidence of neuropathy than haemodialysis patients
gave rise to the ‘middle molecule hypothesis’ (Babb et al.,
1971). This hypothesis postulated that the higher rate of
neuropathy in patients on haemodialysis was secondary to
retention of toxic molecules in the middle molecular range
# The Author (2005). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: [email protected]
Brain Advance Access published June 10, 2005 by guest on July 18, 2016
http://brain.oxfordjournals.org/D
ownloaded from

of 300–12 000 Da (Vanholder et al., 1994), given that these
substances were poorly cleared by haemodialysis membranes.
Examples of such molecules include parathyroid hormone
(PTH) and b-2-microglobulin (b-2M), the levels of which
are elevated in patients with ESKD (Vanholder et al., 1994).
The hypothesis, however, remains unproven and the toxicity
of a number of these middle molecules remains contentious
(Vanholder et al., 1994; Bostock et al., 2004).
Measurements of nerve excitability, which provide infor-
mation about membrane potential and biophysical properties
of peripheral axons (Bostock et al., 1998; Burke et al., 2001),
have been used to study peripheral nerves in patients with
neuropathy and have provided information about disease
pathophysiology (Cappelen-Smith et al., 2001; Kiernan et al.,
2001a, 2002a, 2005; Kanai et al., 2003; Nodera et al., 2004).
A preliminary study of motor nerve excitability in the upper
limb of patients with ESKD demonstrated membrane poten-
tial changes—specifically membrane depolarization before
haemodialysis (Kiernan et al., 2002b)—with subsequent
improvement in nerve excitability after dialysis. Given the
length-dependent predisposition of uraemic neuropathy, typ-
ically worse in the legs than in the arms, the present study
has focused on lower limb motor nerve excitability. The aim
of the study was to expand the original study by investigating
the excitability properties of lower limb motor axons, before,
during and after haemodialysis in patients with ESKD.
In addition, correlations were explored between excitability
changes and the clinical severity of neuropathy, related to
changes in the serum levels of potential uraemic toxins and
the severity of neuropathic symptoms.
MethodsStudies were undertaken on 14 patients with ESKD (8 men, 6 women:
age range, 17–69 years; mean age, 50.3 years) receiving thrice-weekly
haemodialysis, using a biocompatible low-flux polysulfone mem-
brane (Fresenius, Bad Homburg, Germany). All patients were
dialysed against a K+ concentration of 2 mmol/l. None of the
patients had a history of other illnesses known to cause neuropathy
such as diabetes or amyloidosis and there was no history of exposure
to neurotoxic medications, including immunosuppressive therapy.
The causes of ESKD in this group were glomerulonephritis
(9 patients), polycystic kidney disease (1), medullary cystic kidney
disease (2) and hypertensive vascular disease (2).
Patients gave informed consent to the procedures, which were
approved by the South East Sydney Area Health Service Human
Research Ethics Committee (Eastern Section) and the Committee
on Experimental Procedures Involving Human Subjects of the Uni-
versity of New South Wales. The studies were performed in accord-
ance with the Declaration of Helsinki.
A neurological history and examination were initially undertaken
and symptoms were graded using the neuropathy symptom score
(NSS) (Dyck et al., 1980, 1987, 1992; Laaksonen et al., 2002). Patients
were asked about the presence of motor symptoms in the limbs
(subset IB) and sensory symptoms, both negative (subset IIA) and
positive (subset IIB). Each symptom received a score of 1 and the
number of symptoms present in each subset was added to give a
total neuropathy symptom score (T-NSS). The maximum possible
T-NSS was 9.
Routine nerve conduction studies were undertaken in all patients.
Neurophysiological indices which had previously been shown to be
sensitive markers of uraemic neuropathy were evaluated (Ackil et al.,
1981; Laaksonen et al., 2002). Studies were undertaken on the sural,
tibial, common peroneal and superficial radial nerves using a Mede-
lec Synergy system (Oxford Instruments, Surrey, UK) and conven-
tional nerve conduction techniques (Burke et al., 1974; Kimura,
1983). Nerve stimulation was performed at a frequency of 1 Hz
for motor nerves and 2 Hz for sensory nerves. Motor amplitudes
were measured peak to peak and sensory amplitudes were measured
as an average of the rising and falling phase amplitudes. Latency was
measured to the onset of the compound potential. For sensory stud-
ies, a bipolar recording electrode configuration was used with a
standard interelectrode distance of 4 cm (Eduardo and Burke,
1988). For tibial nerve F-wave studies, the latency was recorded as
the mean of 10 responses following supramaximal stimulation of the
nerve at the medial malleolus.
The excitability properties of lower limb motor nerves in patients
with ESKD treated with haemodialysis were measured before, during
and 1 h after a standard 5 h haemodialysis session using a previously
described protocol (Kiernan et al., 2000; Krishnan et al., 2004).
Recordings were obtained from tibialis anterior (TA) and extensor
digitorum brevis (EDB), following stimulation of the peroneal nerve
at the fibular neck. Skin temperature was monitored close to the site
of stimulation for the duration of each study.
Serum electrolytes, urea, creatinine, PTH and b-2M
were measured at the time of the excitability studies. Kt/V, a standard
and commonly accepted measure of dialysis adequacy (Daugirdas,
1995, 2000), was also calculated according to the following formula,
where K is the dialyser clearance, t is the length of the dialysis session
(hours) and V is the urea distribution volume (litres), U1 is pre-
dialysis urea (mmol/l); U2 is post-dialysis urea (mmol/l, 1 h after
dialysis), BW is body weight, DBW is the change in body weight
following dialysis.
Kt=V ¼ �ln U1=U2 � 0:008 · tð Þ þ 4 � 3:5 · U1=U2ð Þ · DBW=BW: ð1Þ
The current required to produce the desired CMAP (compound
muscle action potential) amplitude was determined using a compu-
terized threshold-tracking program (QTRAC version 5.2a, Institute
of Neurology, Queen Square, London, UK, with multiple excitability
protocol TRONDXM2) that was run on a Pentium computer
(Kiernan et al., 2000). Recordings were amplified (gain 1000,
bandwidth 5–10 kHz) and digitized using an analogue-to-digital
(A/D) board (DT2812, Data Translation, Marlboro, MA, USA),
with a sampling rate of 10 kHz. Stimulus waveforms were converted
to current using a purpose-built isolated linear bipolar constant-
current stimulator.
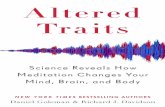
Stimulus–response curves were generated for test stimuli of 0.2
and 1 ms duration (Fig. 1). The slope of the 1 ms stimulus–response
curve and the magnitude of the tracking ‘error’ (i.e. the difference
between measured response and target response) were used to
optimize the subsequent threshold tracking. The peak 1 ms response
was also used to calculate the target response (40% of the supra-
maximal CMAP response). The ratio between the stimulus–response
curves for the two different stimulus durations was used to calculate
rheobase (Burke et al., 2001) and the strength–duration time con-
stant (tSD) of motor axons of different thresholds using Weiss’s
formula (Weiss, 1901; Mogyoros et al., 1996).
Page 2 of 11 Brain (2005) A. V. Krishnan et al.
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

The threshold changes that occur in response to subthreshold
depolarizing and hyperpolarizing pulses, referred to as threshold
electrotonus, were measured by altering nerve excitability using sub-
threshold polarizing currents of 100 ms duration, set to 40% of the
unconditioned threshold current (Bostock and Baker, 1988; Kiernan
et al., 2000; Burke et al., 2001). A current–threshold relationship,
analogous to the conventional current–voltage (I/V) relationship
(Kiernan et al., 2000), was obtained by tracking the changes in
threshold of 1 ms test pulses that occurred following subthreshold
polarizing currents of 200 ms duration. In the final part of the
Fig. 1 Six plots of excitability parameters recorded from TA for a single representative patient (continuous lines with circles) before dialysiswith 95% confidence intervals (broken lines) for a single subject (Krishnan et al., 2004). (A) Absolute stimulus–response relationship forstimuli of 0.2 ms duration (line without filled circle) and 1 ms duration (line with filled circle). The filled circle on the 1 ms response curvecorresponds to the threshold for a CMAP 50% of maximum and the broken ellipse corresponds to the 95% confidence limits for a singlesubject. (B) Normalized stimulus–response relationship. The responses in (A) are expressed as a percentage of maximum and the stimuli asa percentage of the stimulus for a response 50% of maximum. (C) Current–threshold relationship, reflecting rectifying properties of theaxon following polarizing currents, expressed as a percentage of resting threshold. Threshold changes to hyperpolarizing current arerepresented on the left and to depolarizing current on the right. (D) Distribution of strength–duration time constants of nine populations ofaxons, from 5 to 95% of maximal CMAP in groups of 10%. (E) Threshold electrotonus. Threshold changes to polarizing currents of 640%of the resting threshold. Changes are plotted as threshold reductions, with depolarization represented in an upward direction andhyperpolarization in a downward direction. (F) Recovery cycle, showing refractoriness superexcitability and late subexcitability.See text for further details.
Uraemic neuropathy Brain (2005) Page 3 of 11
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

protocol, the recovery cycle of excitability of motor axons was
assessed by tracking the changes in threshold that occurred following
a supramaximal conditioning stimulus of 1 ms duration.
Abnormalities of nerve conduction and excitability were estab-
lished by comparing the results with normative data from our unit
(Burke et al., 1974; Krishnan et al., 2004) and other centres (Ma et al.,
1981; Ma and Liveson, 1983; Buschbacher, 1999; Puksa et al., 2003).
Excitability results were corrected for age, temperature and gender
(Kiernan et al., 2001b). Single comparisons in excitability parameters
were analysed using Student’s unpaired t-test for comparisons with
normative data (n = 25; age range, 22–60 years; mean age, 31 years)
and Student’s paired t-test for comparisons before and after dialysis.
Logarithmic conversions were undertaken to normalize certain
variables. Correlations were analysed using Pearson’s correla-
tion coefficient. A probability value of <0.05 was considered statist-
ically significant. Results are expressed as mean 6 standard error of
the mean.
ResultsNerve conduction studies andneuropathy assessmentThe amplitude of sural nerve SNAP (sensory nerve action
potential) (Burke et al., 1974) was reduced in 71% of patients
(Table 1) and in the entire group as a whole (mean sural SNAP
amplitude, 5.8 6 1.1 mV; n = 14), with a minor reduction in
sural nerve conduction velocity (Table 1). Superficial radial
SNAP amplitude (Ma et al., 1981) was reduced in 50% of
patients (mean, 18.1 6 2.4 mV), although conduction velocity
was generally preserved (mean, 53.6 6 0.9 m/s).
Abnormalities of lower limb motor conduction were
also demonstrated in a number of patients with neuro-
pathy (Table 1). Tibial CMAP amplitudes (Buschbacher, 1999)
were reduced in 43% of patients and mean tibial CMAP
amplitude was mildly reduced (mean tibial CMAP amplitude,
3.6 6 0.7 mV). Tibial distal motor latency was prolonged in
38% of patients although mean latency was within the normal
range (mean tibial distal motor latency, 5.2 6 0.5 mV). Tibial
F-wave minimum latency (Puksa et al., 2003) was prolonged
in 43% of patients (Table 1) and persistence was reduced
in 43% of patients. Peroneal CMAP amplitudes (Ma and
Liveson, 1983) were reduced in 21% of patients and
there was a mild reduction in mean CMAP amplitude
(mean peroneal CMAP amplitude, 3.2 6 0.5 mV). These
changes were accompanied by a reduction in peroneal
nerve conduction velocity in 36% of patients, although the
mean value was within the normal range (mean peroneal
nerve conduction velocity, 43.4 6 1.6 m/s). Peroneal distal
motor latency was normal in all patients in whom a CMAP
response was evident.
All ESKD patients in the study reported symptoms of
neuropathy (Table 2), with an average of approximately
two symptoms per patient (mean NSS 1.9 6 0.2). The severity
of neuropathy in the present study (Table 2) was staged
as follows using a modified form of a previously devised
system (Dyck, 1988): Stage 0, no neuropathy [T-NSS < 2
with normal NCS (nerve conduction study)]; Stage 1, asymp-
tomatic neuropathy (T-NSS = 0 with abnormalities on NCS);
Stage 2, symptomatic neuropathy (T-NSS > 2 with normal
NCS or T-NSS � 1 with abnormal NCS; neuropathic symp-
toms non-disabling); Stage 3, disabling neuropathy (T-NSS �2 with normal NCS or T-NSS � 1 with abnormal NCS;
neuropathic symptoms reported to be disabling). Using
this scale, 1 patient had no neuropathy (stage 0), 10 had
Stage 2 neuropathy and 3 had Stage 3 neuropathy (Table 2).
Table 1 Nerve conduction parameters for each patient
Patient SuralSNAP (mV)
RadialSNAP (mV)
TibialCMAP (mV)
TibialDML (ms)
Tibial F-wave min.latency (ms)
Tibial F-wavepersistence (%)
PeronealCMAP (mV)
PeronealDML (ms)
1 6.0* 15.0* 4.4 7.7* 51.9 100 4.7 3.52 2.0* 11.0* 2.8* 6.9* 59.8* 90 2.1 3.43 3.1* 9.0* 1.8* 4.2 44.6 60* 2.5 3.54 1.5* 13.0* 1.6* 6.2* 61.8* 60* 1.8* 3.85 12.0 24.0 8.6 3.3 43.1 60* 1.5* 4.06 14.0 33.5 8.1 4.4 41.8 100 7.1 3.87 11.5 36.0 4.0 5.2 30.6 90 5.2 4.28 8.9 20.0 3.9 3.8 42.2 90 1.9 3.59 2.5* 17.4 4.8 3.5 54.2* 100 4.3 4.5
10 5.5* 13.0* 3.8 5.2 58.3* 90 3.4 3.411 4.3* 24.3 0.3* 7.9* 49.2 40* 4.0 3.712 4.3* 20.7 4.2 6.1* 48.9 90 2.6 3.113 Absent* 6.0* Absent* Absent Absent* Absent* Absent* Absent14 6.0* 11.0* 2.4* 3.0 57.9* 70* 3.0 3.7Mean (patients) 5.8 6 1.1 18.1 6 2.4 3.6 6 0.7 5.2 6 0.5 49.6 6 2.5 80 6 5 3.2 6 0.5 3.7 6 0.1Normal controls 13.6 6 7.5 42.4 6 14.9 12.9 6 4.5 4.5 6 0.8 45.9 6 4.4 100% 8.9 6 4.0 4.0 6 0.7
Group data expressed as mean 6 standard error of the mean for each parameter. Data include amplitudes for sensory nerve actionpotential (SNAP) and compound motor action potential (CMAP), distal motor latency (DML) and tibial F-wave minimum latency (min.latency). The patient number is the same as in Table 2. *Denotes an abnormal result. Normative data are shown as mean 6 standarddeviation and are taken from the sources referred to in the text. Normative data for sural SNAP amplitudes (Burke et al., 1974) and tibialCMAP amplitudes (Buschbacher, 1999) were age-matched and are shown in the table for the age groups 41–60 y and 30–59 y, respectively.
Page 4 of 11 Brain (2005) A. V. Krishnan et al.
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Nerve excitability abnormalitiesbefore dialysisMotor excitability studies were successfully obtained from
TA in all patients and from EDB in 13 out of 14 patients.
The recordings from a single, representative patient are com-
pared with normal limits in Fig. 1, and mean electrotonus and
recovery cycle data are illustrated in Fig. 2A and B. Patient 13
(Table 2) had no recordable response from EDB. Pre-dialysis
abnormalities in excitability were noted in 12 out of
14 patients in the study. Stimulus–response curves for the
group (e.g. Fig. 1A) were shifted to the right in pre-dialysis
recordings from both TA and EDB when compared with
previously established normative data (Krishnan et al.,
2004), indicating that their axons were of high threshold
before dialysis. The stimulus intensity needed to produce a
CMAP 50% of maximal was significantly greater in the renal
patients for both TA and EDB recordings (TA ESKD record-
ings, 10.0 6 1.7 mA; controls, 5.7 6 0.3 mA; P < 0.005; EDB
ESKD recordings, 12.9 6 1.4 mA; controls, 6.9 6 0.3 mA;
P < 0.0005). In keeping with the length-dependent nature
of uraemic neuropathy, maximal CMAP amplitude in renal
patients, measured from onset to negative peak, was similar to
that in controls for TA recordings but significantly reduced in
EDB recordings (TA ESKD recordings, 2.4 6 0.5 mV; con-
trols, 2.4 6 0.2 mV; EDB ESKD recordings, 1.3 6 0.2 mV;
controls, 2.5 6 0.2 mV; P < 0.0005).
There was a significant reduction in tSD for EDB in the
renal patients compared with controls, although tSD was sim-
ilar in both groups in TA recordings (TA ESKD recordings,
0.41 6 0.08 ms; controls 0.43 6 0.01 ms; EDB ESKD record-
ings, 0.33 6 0.05 ms; controls 0.46 6 0.01; P < 0.0005).
Rheobase, defined as the threshold current for a stimulus
of infinitely long duration (Bostock and Rothwell, 1997;
Bostock et al., 1998), was increased in ESKD patients in both
TA and EDB recordings before dialysis (TA ESKD recordings,
7.3 6 1.8 mA; controls, 3.8 6 0.2 mA; P < 0.005; EDB ESKD
recordings, 9.7 6 1.2 mA; controls 4.5 6 0.2 mA; P < 0.0005).
Reductions in threshold electrotonus (Figs 1E and 2A) were
noted in both the depolarizing and hyperpolarizing direc-
tions, leading to a ‘fanned in’ appearance (Kiernan and
Bostock, 2000; Kaji, 2003). Depolarizing threshold electroto-
nus (TEd) at the 90–100 ms interval (TEd 90–100 ms),
previously established as a sensitive indicator of resting
membrane potential (Kiernan and Bostock, 2000), was
lower in the ESKD patients in both TA and EDB recordings
(Table 3) than in the normal controls (TA, P < 0.005; EDB,
P < 0.0005). There were similar reductions in TEd 10–20 ms
(TA, P < 0.0005; EDB, P < 0.0005) and TEd 40–60 ms (TA,
P < 0.0005; EDB, P < 0.0005). Hyperpolarizing threshold
electrotonus (TEh) was also significantly reduced in the ESKD
patients at the 10–20 ms (TA, P < 0.005; EDB, P < 0.0005) and
90–100 ms intervals (TA, P < 0.005; EDB, P < 0.0005). With
respect to the current–threshold relationship (Fig. 1C),
although the resting and minimum current–threshold slopes
were not significantly different between renal patients and
controls, there was a significant change in the hyperpolarizing
current–threshold slope (TA ESKD recordings, 0.64 6 0.02;
controls 1.24 6 0.30; P < 0.01; EDB ESKD recordings,
0.60 6 0.03; controls 1.12 6 0.12; P < 0.0005).
With respect to the recovery cycle (Figs 1F, 2B and D),
refractoriness, owing to inactivation of voltage-gated
transient Na+ channels, was significantly increased in the
renal patients (TA, P < 0.05; EDB, P < 0.005). Superexcitab-
ility, related to the depolarizing afterpotential (Barrett and
Barrett, 1982; David et al., 1992), was reduced in the ESKD
patients (Table 3) before dialysis (TA, P < 0.0005; EDB,
P < 0.0005). Late subexcitability was also reduced in
pre-dialysis recordings (TA, P < 0.05; EDB, P < 0.05).
Table 2 Demographic and clinical data: neuropathy stage, T-NSS, neuropathic symptoms and Kt/V for each patient
Patient Age Stage T-NSS Clinical symptoms Kt/V
1 17 2 1 Lower limb paraesthesiae 1.672 64 3 4 Leg weakness, leg pain, numbness in hands and feet, unsteady gait 1.663 57 2 2 Leg weakness, numbness in feet 2.374 69 2 2 Leg weakness, upper limb paraesthesiae 1.335 22 2 2 Lower limb paraesthesiae, burning feet 1.526 28 0 1 Upper limb paraesthesiae 1.327 37 2 2 Lower limb paraesthesiae, leg weakness 1.438 62 2 2 Lower limb pain, paraesthesiae 1.629 52 2 1 Numbness in feet 1.69
10 55 2 2 Lower limb paraesthesiae, leg weakness 1.4811 62 2 1 Numbness in feet 1.6712 63 3 2 Lower limb paraesthesiae, pain in feet 2.7913 69 3 2 Leg weakness, hand weakness 1.4814 52 2 2 Pain in feet, lower limb numbness 2.31
Neuropathy staged according to the following scale: Stage 0, no neuropathy (T-NSS < 2 with normal NCS); Stage 1, asymptomaticneuropathy (T-NSS = 0 with abnormalities on NCS); Stage 2, symptomatic neuropathy (T-NSS > 2 with normal NCS or T-NSS � 1 withabnormal NCS; neuropathic symptoms non-disabling); Stage 3, disabling neuropathy (T-NSS � 2 with normal NCS or T-NSS � 1 withabnormal NCS; neuropathic symptoms reported to be disabling). The maximum possible T-NSS was nine.
Uraemic neuropathy Brain (2005) Page 5 of 11
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Nerve excitability changesfollowing dialysisThe ‘fanned-in’ appearance of threshold electrotonus and
the reduction in superexcitability noted before the com-
mencement of haemodialysis indicate axonal depolarization
(Kiernan and Bostock, 2000). In order to explore the hypo-
thesis that these changes may be caused by a dialysable toxin
(Bostock et al., 2004), excitability studies were repeated dur-
ing and 1 h following haemodialysis. These studies revealed
significant improvement in a number of excitability paramet-
ers (Figs 2 and 3). In particular, the original abnormalities in
parameters of threshold electrotonus largely resolved during
dialysis (Table 3). The initial pre-dialysis reduction in TEd
90–100 ms improved following dialysis in both TA and EDB
recordings (TA, P < 0.0005; EDB, P < 0.0005). Qualitatively
similar changes were also observed in TEd 40–60 ms (TA,
P < 0.005; EDB, P < 0.0005) and TEh 90–100 ms (TA, P < 0.05;
EDB, P < 0.0005).
Changes were also noted in parameters of the recovery cycle
(Table 3). There was a reduction in the degree of refractori-
ness (TA, P < 0.0005; EDB, P < 0.0005) following dialysis and
a shortening of the duration of the relative refractory period
(TA, P < 0.005; EDB, P = 0.06). These changes were accom-
panied by an increase in superexcitability following dialysis
(TA, P < 0.05; EDB, P < 0.005). An increase in late sub-
excitability following dialysis was also noted (TA, P < 0.0005;
EDB, P < 0.05).
Comparison of the post-dialysis recordings with normative
data (Krishnan et al., 2004) revealed complete resolution of
the depolarization changes noted in the pre-dialysis record-
ings in all parameters of the recovery cycle (Table 3). There
were, however, persistent abnormalities in TEd 10–20 ms (TA,
P < 0.005; EDB, P < 0.005), TEh 10–20 ms (TA, P < 0.0005;
EDB, P < 0.0005) and TEh 90–100 ms in TA recordings (TA,
P < 0.05), indicating that, although improvement occurred
with dialysis, some residual impairment persisted.
Fig. 2 Comparison of threshold electrotonus (A and C) and recovery cycle (B and D) in renal patients (continuous lines with circles)before and after dialysis, with 95% confidence intervals for normal controls (broken lines). Pre-dialysis traces demonstrate ‘fanning in’of threshold electrotonus, increased refractoriness and reduced superexcitability and late subexcitability. Abnormalities have largelyresolved 1 h after dialysis.
Page 6 of 11 Brain (2005) A. V. Krishnan et al.
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Correlation of symptoms,neurophysiological parametersand potential neurotoxinsThere was a close correlation between the stage of neuropathy
and nerve conduction parameters (Fig. 4A), both motor and
sensory (sural amplitude, r = 0.68; P < 0.01; superficial radial
amplitude, r = 0.59; P < 0.05; peroneal CMAP amplitude,
r = 0.74; P < 0.01; tibial CMAP amplitude, r = 0.54;
P < 0.05). Significant correlation was also noted between
T-NSS and both pre-dialysis refractoriness (r = 0.73;
P < 0.01) and pre-dialysis TEd 90–100 ms (r = �0.53;
P < 0.05) in TA recordings (Fig. 4B).
In order to further explore the basis of the pre-dialysis
excitability changes, excitability parameters were assessed in
relation to levels of potential neurotoxins, in addition to
Table 3 Mean excitability values before, during and after dialysis for recordings from TA and EDB, with normal controldata (Krishnan et al., 2004)
Before dialysis During dialysis After dialysis Normal controls
TEd 90–100 ms (TA) 33.6 6 3.1%*** 39.2 6 2.3%*** 41.9 6 2.2% 41.5 6 0.9%TEd 90–100 ms (EDB) 33.7 6 2.6%*** 40.0 6 2.3%*** 45.9 6 1.7% 46.0 6 0.9%TEd 40–60 ms (TA) 39.9% 6 3.2%** 46.6 6 2.6%** 51.3 6 2.0% 51.1 6 0.9%TEd 40–60 ms (EDB) 41.2 6 3.3%*** 47.1 6 2.9%*** 58.0 6 2.2% 55.8 6 0.9%TEh 90–100 ms (TA) �75.2 6 10.9%* �91.1 6 19.9%* �89.2 6 8.5% �108.3 6 4.3%TEh 90–100 ms (EDB) �75.2 6 11.8%*** �84.7 6 11.0%** �101.2 6 8.1% �115.2 6 3.7%Refractoriness (TA) 59.8 6 15.9%*** 55.6 6 13.6%*** 43.8 6 11.0% 31.9 6 3.5%Refractoriness (EDB) 64.7 6 17.9%*** 56.9 6 11.3%*** 33.1 6 7.5% 24.9 6 2.8%Relative refractory period (TA) 5.4 6 0.8 ms** 4.9 6 0.9 ms*** 3.8 6 0.5 ms 3.3 6 0.1 msRelative refractory period (EDB) 5.4 6 0.8 ms (NS) 4.4 6 0.6 ms*** 3.9 6 0.8 ns 3.1 6 0.07 msSuperexcitability (TA) �9.6 6 2.0%* �14.0 6 2.1% (NS) �21.2 6 2.2% �19.1 6 1.2%Superexcitability (EDB) �11.5 6 2.6%** �14.8 6 2.7%** �28.6 6 2.8% �27.6 6 1.4%Late subexcitability (TA) 5.0 6 1.7%*** 5.9 6 1.7%*** 9.4 6 3.0% 10.6 6 0.9%Late subexcitability (EDB) 4.9 6 1.6%* 7.0 6 1.7%** 13.5 6 3.5% 9.0 6 1.0%
Data are shown for depolarizing and hyperpolarizing threshold electrotonus (TEd and TEh, respectively) and recovery cycle parameters.Data are expressed as mean 6 standard error of the mean. Pre-dialysis and during dialysis measures were compared to post-dialysis valuesusing Student’s paired t-test. Significance levels are indicated as follows: *, P < 0.05; **, P < 0.005; ***, P < 0.0005.
Fig. 3 Comparison of excitability parameters recorded from TA and EDB before, during and after dialysis. (A) Depolarizing thresholdelectrotonus at 90–100 ms. (B) Superexcitability. (C) Late subexcitability. (D) Hyperpolarizing threshold electrotonus at 90–100 ms.Results are expressed as mean 6 standard error of the mean. Asterisks indicate significance (Student’s t-test: *, P < 0.05; **, P < 0.005;***, P < 0.0005; NS, not significant).
Uraemic neuropathy Brain (2005) Page 7 of 11
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

measures of dialysis adequacy (Table 4). With respect to
pre-dialysis excitability parameters, changes in threshold
electrotonus and superexcitability correlated strongly with
pre-dialysis serum K+ (Fig. 4C). The correlations between
these excitability parameters and K+ were far greater than
those for other substances, including creatinine, urea, cal-
cium, b-2M and PTH (Table 4). Recordings were also
obtained from one patient on five separate occasions before
dialysis and a similarly close correlation was noted between
TEd 90–100 ms and serum K+ (Fig. 4D). Correlation was also
noted between pre-dialysis PTH and superexcitability in EDB
recordings (r = 0.60; P < 0.05) and this correlation was further
strengthened after allowing for the effect of K+ (Table 4).
Although correlations were noted between excitability
measures and both urea and b-2M, these correlations were
not significant after allowing for K+ (Table 4). Kt/V, a mea-
sure of dialysis adequacy, correlated poorly with changes
in TEd 90–100 ms in recordings from both TA (r = 0.30)
and EDB (r = 0.37). It is noteworthy that all patients in the
present study had a Kt/V > 1.2 (Table 2), in keeping with
current guidelines on dialysis adequacy (National Kidney
Foundation, 2001).
Fig. 4 Relationship between (A) sural amplitude and neuropathy stage, (B) pre-dialysis TEd 90–100 ms from TA and T-NSS and(C) pre-dialysis TEd 90–100 ms from TA and serum K+. (D) Relationship between pre-dialysis TEd 90–100 ms from EDB and serum K+
in a single subject, tested on five separate occasions before dialysis. All correlations were significant at the 0.05 level. Dotted lines in(C) and (D) represent 95% confidence intervals for normal controls.
Table 4 Correlation coefficients for TEd 90–100 ms, TEh 90–100 ms and superexcitability against potential neurotoxinsbefore dialysis
Mean TEd 90–100 ms TEh 90–100 ms Superexcitability
TA EDB TA EDB TA EDB
K+ (3.6–5.1) 4.9 6 0.3 �0.87*** �0.85*** 0.90**** 0.89*** 0.85*** 0.69*Creatinine (60–110) 877 6 49.1 �0.26 �0.28 0.26 0.26 0.09 0.29
0.07 0.02 �0.13 �0.11 �0.41 0.07Urea (2.9–7.1) 24.2 6 2.3 �0.68** �0.55 0.62* 0.45 0.50 0.42
�0.24 �0.02 0.03 �0.33 �0.19 �0.04b-2M (0.7–1.8) 42.7 6 4.8 �0.42 �0.66* 0.55* 0.66 0.51 0.49
0.38 �0.18 �0.06 0.20 �0.06 0.09PTH (0.5–5.0) 28.4 6 10.2 �0.33 �0.36 0.37 0.45 0.14 0.60*
�0.18 �0.43 0.29 0.62* �0.19 0.65*Ca2+ (2.25–2.58) 2.4 6 0.06 �0.26 �0.36 0.18 0.28 0.11 �0.10
0.07 �0.05 �0.30 �0.18 �0.37 �0.57
Correlation coefficients after allowing for the effect of K+ are shown in bold font. Mean serum concentrations for the group are expressed asmean 6 standard error of the mean. Normal ranges for serum concentrations are displayed in parentheses. Serum levels are expressed inmmol/l except for creatinine (mmol/l), b-2M (mg/l) and PTH (pmol/l). Significance levels: *, P < 0.05; **, P < 0.01; ***, P < 0.001;****, P < 0.0001.
Page 8 of 11 Brain (2005) A. V. Krishnan et al.
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

DiscussionThe present study investigated the excitability properties of
lower limb motor axons in patients with ESKD. All patients
complained of neuropathic symptoms, and in most patients
nerve conduction studies revealed changes consistent with
peripheral neuropathy. Axonal excitability was abnormal
before dialysis, with reductions in TEd and TEh at multiple
intervals, leading to a ‘fanned in’ appearance, alteration
in the hyperpolarizing current–threshold slope and less
superexcitability and late subexcitability. There was marked
improvement in excitability parameters following dialysis,
and post-dialysis excitability recordings were either approach-
ing or were within the normal range.
Clinical symptoms and nerveconduction abnormalitiesThe rate of neuropathy in the present study was 93%,
in keeping with previous studies of uraemic neuropathy,
which have demonstrated similarly high rates of neuropathy
in patients with ESKD (Ackil et al., 1981; Angus-Leppan and
Burke, 1992; Van den Neucker et al., 1998; Laaksonen et al.,
2002). The most commonly affected parameter in the present
study was sural SNAP amplitude, which was abnormal in a
higher percentage of patients than radial SNAP amplitude,
consistent with the lower limb predisposition of neuropathy.
Previous studies have demonstrated that abnormalities in late
responses, namely F-waves and H-reflexes, may be a sensitive
marker of neuropathy in patients with uraemia (Halar et al.,
1979; Panayiotopoulos and Lagos, 1980; Van den Neucker
et al., 1998; Laaksonen et al., 2002). In the present study,
although tibial F-wave minimum latency was abnormal in
43% of patients, all but one of those patients had accompany-
ing abnormalities of sensory amplitudes, suggesting that sural
nerve SNAP amplitudes are a more sensitive neurophysio-
logical indicator of neuropathy in patients with uraemia
than lower limb F-wave parameters.
Excitability abnormalities in ESKDThere were significant abnormalities in peroneal nerve
excitability before dialysis. Maximal CMAP amplitude was
reduced in EDB recordings but maintained in TA recordings,
consistent with the length-dependent predisposition of
uraemic neuropathy. In addition, there were changes in
sensitive markers of membrane potential, including threshold
electrotonus and recovery cycle parameters, suggestive of
axonal depolarization. Threshold electrotonus refers to the
threshold changes that occur in response to subthreshold
depolarizing and hyperpolarizing pulses and is sensitive
to changes in resting membrane potential (Bostock et al.,
1998). Membrane depolarization causes a ‘fanning in’
of threshold curves (Kiernan and Bostock, 2000), as was
noted in the present study in pre-dialysis recordings from
both TA and EDB. Superexcitability, as a result of the depol-
arizing afterpotential, determined in part by the level of
activation of paranodal voltage-dependent K+ channels
(Barrett and Barrett, 1982; David et al., 1995), was signific-
antly reduced before dialysis, which is also consistent with
membrane depolarization (Kiernan and Bostock, 2000).
Although a reduction in tSD (limited to EDB recordings)
before dialysis would be unexpected for axonal depolariza-
tion, the inherent variability of this excitability measure,
and its potential to vary with metabolic change, particularly
acid-base disturbances, preclude further comment (Mogyoros
et al., 1997; Baker and Bostock, 1999).
The clear improvements in excitability parameters follow-
ing dialysis noted in the present study and in a previous study
of upper limb nerve excitability in uraemic patients (Kiernan
et al., 2002b) provide a sharp contrast to the conflicting results
of studies utilizing standard nerve conduction techniques.
Although some studies have documented post-dialysis
improvements in a number of neurophysiological parameters,
including sensory nerve conduction velocity (Nielsen, 1973;
Lang and Forsstrom, 1977) and sensory and motor action
potential amplitudes (Mansouri et al., 2001), others have
found no significant changes in neurophysiological para-
meters following a single haemodialysis session (Laaksonen
et al., 2002).
Contributing factors to pre-dialysisexcitability changesThe present study detected correlations between serum K+
and threshold electrotonus parameters and superexcitability.
There was also significant correlation between T-NSS and
both pre-dialysis refractoriness and TEd 90–100 ms, with
patients with a higher T-NSS manifesting greater excitability
changes (Fig. 4B). This is the first evidence that altered axonal
membrane potential, as recorded by nerve excitability testing,
is directly related to neuropathic symptoms. Abnormalities
of serum K+ will lead to changes in membrane potential as a
result of the dependence of resting membrane potential on
the concentration gradient for K+ (Bostock et al., 2004). The
alterations in late subexcitability provide further evidence for
the contribution of K+ to the excitability abnormalities, since
subexcitability depends on the difference between the resting
potential and the K+ equilibrium potential, and actually
increases with depolarization if extracellular K+ is unchanged
(Kiernan and Bostock, 2000). The reduction in late sub-
excitability in the pre-dialysis recordings from TA and EDB
in the present study mirrors the findings of a previous study
of median nerve excitability in patients with ESKD (Kiernan
et al., 2002b). In total, these studies suggest that pre-dialysis
axonal membrane depolarization in patients with ESKD is
more probably caused through effects mediated by serum
K+ than as a consequence of a reduction in Na+/K+ pump
function (Kiernan and Bostock, 2000; Kiernan et al., 2002b).
Studies of sensory nerve excitability in ESKD are currently
under way that may provide further insights into the role of
K+ in uraemic neuropathy, given the sensory predilection
of uraemic neuropathy and the differential effects of K+ on
sensory and motor axons (Neumcke et al., 1980).
Uraemic neuropathy Brain (2005) Page 9 of 11
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

How do the reversible changes demonstrated in the present
study lead to the more irreversible neurological changes that
characterize uraemic neuropathy? It may be argued that the
abnormalities of serum K+ noted constitute a transient
homeostatic disturbance that is rapidly corrected by dialysis
and therefore unlikely to play a major role in the development
of chronic irreversible neuropathy. Against such an argument,
prolonged exposure to hyperkalaemia in ESKD patients seems
likely, given that the post-dialysis rebound of K+ is a well-
recognized phenomenon (De Nicola et al., 2000; Ahmed
and Weisberg, 2001), with hyperkalaemia typically recurring
within 6 h of a dialysis session owing to re-equilibration
between intracellular and extracellular fluid compartments
(Blumberg et al., 1997). Such prolonged hyperkalaemia
may cause disruption of normal ionic gradients, which are
essential for axonal survival (see Bostock et al., 2004), activ-
ating damaging Ca++-mediated processes and leading to
axonal loss (Craner et al., 2004). Excitability studies focusing
on a more prolonged period between consecutive haemo-
dialysis sessions may shed further light on the duration for
which excitability remains truly ‘normal’ in ESKD patients.
It remains possible that K+ acts synergistically with another
toxin in mediating neurotoxicity, given that excitability
changes occurred even when K+ was in the upper limits
of the normal range, rather than outside normative values
(Fig. 4C). A possible candidate is PTH, which correlated
with pre-dialysis superexcitability in EDB (Table 4). A num-
ber of studies have suggested a link between PTH and neuro-
logical complications in ESKD (Slatopolsky et al., 1980;
Massry, 1987) and PTH has been shown to prolong motor
nerve conduction velocities in animal studies (Goldstein et al.,
1978). Human studies of the effect of PTH on peripheral
nerves have yielded conflicting results, with variable
changes in motor nerve conduction velocity in patients
with ESKD (Avram et al., 1978; Di Giulio et al., 1978; Schaefer
et al., 1980).
The correlation between pre-dialysis PTH and super-
excitability in EDB must be interpreted with caution for
the following reasons. First, there was no such correlation
with superexcitability in TA, or in the combined TA and
EDB data (whereas this combination strengthened the cor-
relation with K+). Second, there was no correlation between
PTH and superexcitability in EDB when pre-dialysis and post-
dialysis data were combined (whereas this combination again
strengthened the correlation with K+).
Apart from K+ and PTH, there was no evidence for an effect
on nerve excitability of the other potential toxins, including
urea and creatinine. Although these substances are easily dia-
lysed, they correlated poorly with excitability abnormalities,
after allowing for the effect of K+. The absence of any detect-
able neurotoxic effect of urea calls into question the suitability
of Kt/V, a measure based on urea (Mallick and Gokal, 1999;
Daugirdas, 2000), for determining the adequacy of a dialysis
regimen to prevent neurotoxicity. All patients in the present
study met the current guidelines for dialysis adequacy and
yet excitability was significantly abnormal before dialysis
in the majority, with all patients exhibiting symptoms of
neuropathy. Our data suggest that, at least as far as axons
are concerned, a better indication of adequate dialysis might
be the maintenance of serum K+ within normal limits between
periods of dialysis. This may require more attention to dietary
restriction of K+ intake in some patients.
AcknowledgementsA.V.K. was supported by the Australian Association of
Neurologists Research Fellowship. Grant support from the
Australian Brain Foundation, the Sylvia and Charles Viertel
Charitable Foundation and the Ramaciotti Foundation is
gratefully acknowledged.
References
Ackil AA, Shahani BT, Young RR, Rubin NE. Late response and sural
conduction studies. Usefulness in patients with chronic renal failure.
Arch Neurol 1981; 38: 482–5.
Ahmed J, Weisberg LS. Hyperkalemia in dialysis patients. Semin Dial 2001;
14: 348–56.
Angus-Leppan H, Burke D. The function of large and small nerve fibers in
renal failure. Muscle Nerve 1992; 15: 288–94.
Asbury AK. Neuropathies with chronic renal failure, hepatic disorders,
chronic respiratory insufficiency, and critical illness. In: Dyck PJ,
Thomas PK, Griffin JW, Low PA, Poduslo JF, editors. Peripheral
neuropathy. Philadelphia: WB Saunders; 1993.
Avram MM, Feinfeld DA, Huatuco AH. Search for the uremic toxin.
Decreased motor-nerve conduction velocity and elevated parathyroid
hormone in uremia. N Engl J Med 1978; 298: 1000–3.
Babb AL, Popovich RP, Christopher TG, Scribner BH. The genesis of
the square meter-hour hypothesis. Trans Am Soc Artif Intern Organs
1971; 17: 81–91.
Baker MD, Bostock H. The pH dependence of late sodium current in large
sensory neurons. Neuroscience 1999; 92: 1119–30.
Barrett EF, Barrett JN. Intracellular recording from vertebrate myelinated
axons: mechanism of the depolarizing afterpotential. J Physiol (Lond)
1982; 323: 117–44.
Blumberg A, Roser HW, Zehnder C, Muller-Brand J. Plasma potassium
in patients with terminal renal failure during and after haemodialysis;
relationship with dialytic potassium removal and total body potassium.
Nephrol Dial Transplant 1997; 12: 1629–34.
Bolton CF. Peripheral neuropathies associated with chronic renal failure.
Can J Neurol Sci 1980; 7: 89–96.
Bostock H, Baker M. Evidence for two types of potassium channel in human
motor axons in vivo. Brain Res 1988; 462: 354–8.
Bostock H, Rothwell JC. Latent addition in motor and sensory fibres of
human peripheral nerve. J Physiol (Lond) 1997; 498: 277–94.
Bostock H, Cikurel K, Burke D. Threshold tracking techniques in the study of
human peripheral nerve. Muscle Nerve 1998; 21: 137–58.
Bostock H, Walters RJ, Andersen KV, Murray NM, Taube D, Kiernan MC.
Has potassium been prematurely discarded as a contributing factor to the
development of uraemic neuropathy? Nephrol Dial Transplant 2004; 19:
1054–7.
Burke D, Skuse NF, Lethlean AK. Sensory conduction of the sural nerve
in polyneuropathy. J Neurol Neurosurg Psychiatry 1974; 37: 647–52.
Burke D, Kiernan MC, Bostock H. Excitability of human axons. Clin
Neurophysiol 2001; 112: 1575–85.
Buschbacher RM. Tibial nerve motor conduction to the abductor hallucis.
Am J Phys Med Rehabil 1999; 78: S15–20.
Cappelen-Smith C, Kuwabara S, Lin CS, Mogyoros I, Burke D. Membrane
properties in chronic inflammatory demyelinating polyneuropathy. Brain
2001; 124: 2439–47.
Page 10 of 11 Brain (2005) A. V. Krishnan et al.
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Craner MJ, Hains BC, Lo AC, Black JA, Waxman SG. Co-localization of
sodium channel Nav 1.6 and the sodium-calcium exchanger at sites of
axonal injury in the spinal cord in EAE. Brain 2004; 127: 294–303.
Daugirdas JT. Simplified equations for monitoring Kt/V, PCRn, eKt/V, and
ePCRn. Adv Ren Replace Ther 1995; 2: 295–304.
Daugirdas JT. Dialysis adequacy and kinetics. Curr Opin Nephrol Hypertens
2000; 9: 599–605.
David G, Barrett JN, Barrett EF. Evidence that action potentials activate an
internodal potassium conductance in lizard myelinated axons. J Physiol
(Lond) 1992; 445: 277–301.
David G, Modney B, Scappaticci KA, Barrett JN, Barrett EF. Electrical and
morphological factors influencing the depolarizing after-potential in rat
and lizard myelinated axons. J Physiol (Lond) 1995; 489: 141–57.
De Nicola L, Bellizzi V, Minutolo R, Cioffi M, Giannattasio P, Terracciano V,
et al. Effect of dialysate sodium concentration on interdialytic increase of
potassium. J Am Soc Nephrol 2000; 11: 2337–43.
Di Giulio S, Chkoff N, Lhoste F, Zingraff J, Drueke T. Parathormone as a
nerve poison in uremia. N Engl J Med 1978; 299: 1134–5.
Dyck PJ. Detection, characterization, and staging of polyneuropathy: assessed
in diabetics. Muscle Nerve 1988; 11: 21–32.
Dyck PJ, Sherman WR, Hallcher LM, Service FJ, O’Brien PC, Grina LA, et al.
Human diabetic endoneurial sorbitol, fructose, and myo-inositol related to
sural nerve morphometry. Ann Neurol 1980; 8: 590–6.
Dyck PJ, Bushek W, Spring EM, Karnes JL, Litchy WJ, O’Brien PC, et al.
Vibratory and cooling detection thresholds compared with other tests in
diagnosing and staging diabetic neuropathy. Diabetes Care 1987; 10:
432–40.
Dyck PJ, Karnes JL, O’Brien PC, Litchy WJ, Low PA, Melton LJ III. The
Rochester Diabetic Neuropathy Study: reassessment of tests and criteria for
diagnosis and staged severity. Neurology 1992; 42: 1164–70.
Eduardo E, Burke D. The optimal recording electrode configuration for
compound sensory action potentials. J Neurol Neurosurg Psychiatr 1988;
51: 684–7.
Goldstein DA, Chui LA, Massry SG. Effect of parathyroid hormone and
uremia on peripheral nerve calcium and motor nerve conduction velocity.
J Clin Invest 1978; 62: 88–93.
Halar EM, Brozovich FV, Milutinovic J, Inouye VL, Becker VM. H-reflex
latency in uremic neuropathy: correlation with NCV and clinical findings.
Arch Phys Med Rehabil 1979; 60: 174–7.
Hegstrom RM, Murray JS, Pendras JP, Burnell JM, Scribner BH. Two year’s
experience with periodic hemodialysis in the treatment of chronic uremia.
Trans Am Soc Artif Intern Organs 1962; 8: 266–80.
Kaji R. Physiology of conduction block in multifocal motor neuropathy and
other demyelinating neuropathies. Muscle Nerve 2003; 27: 285–96.
Kanai K, Kuwabara S, Arai K, Sung JY, Ogawara K, Hattori T. Muscle cramp
in Machado-Joseph disease: altered motor axonal excitability properties
and mexiletine treatment. Brain 2003; 126: 965–73.
Kiernan MC, Bostock H. Effects of membrane polarization and ischaemia
on the excitability properties of human motor axons. Brain 2000; 123:
2542–51.
Kiernan MC, Burke D, Andersen KV, Bostock H. Multiple measures of axonal
excitability: a new approach in clinical testing. Muscle Nerve 2000; 23:
399–409.
Kiernan MC, Hart IK, Bostock H. Excitability properties of motor axons
in patients with spontaneous motor unit activity. J Neurol Neurosurg
Psychiatr 2001a; 70: 56–64.
Kiernan MC, Cikurel K, Bostock H. Effects of temperature on the excitability
properties of human motor axons. Brain 2001b; 124: 816–25.
Kiernan MC, Guglielmi JM, Kaji R, Murray NM, Bostock H. Evidence for
axonal membrane hyperpolarization in multifocal motor neuropathy with
conduction block. Brain 2002a; 125: 664–75.
Kiernan MC, Walters RJ, Andersen KV, Taube D, Murray NM, Bostock H.
Nerve excitability changes in chronic renal failure indicate membrane
depolarization due to hyperkalaemia. Brain 2002b; 125: 1366–78.
Kiernan MC, Isbister GK, Lin CS-Y, Burke D, Bostock H. Acute tetrodotoxin-
induced neurotoxicity after ingestion of puffer fish. Ann Neurol 2005;
57: 339–348.
Kimura J. Electrodiagnosis in diseases of nerve and muscle. Philadelphia:
FA Davis; 1983.
Krishnan AV, Lin CS-Y, Kiernan MC. Nerve excitability properties in lower
limb motor axons: evidence for a length-dependent gradient. Muscle Nerve
2004; 29: 645–55.
Laaksonen S, Metsarinne K, Voipio-Pulkki LM, Falck B. Neurophysiologic
parameters and symptoms in chronic renal failure. Muscle Nerve 2002; 25:
884–90.
Lang AH, Forsstrom J. Transient changes of sensory nerve functions in
uraemia. Acta Med Scand 1977; 202: 495–500.
Ma DM, Liveson JA. Nerve conduction handbook. Philadelphia: FA Davis;
1983.
Ma DM, Kim SH, Spielholz N, Goodgold J. Sensory conduction study of distal
radial nerve. Arch Phys Med Rehabil 1981; 62: 562–4.
Mallick NP, Gokal R. Haemodialysis. Lancet 1999; 353: 737–42.
Mansouri B, Adybeig B, Rayegani M, Yasami S, Behshad V. Uremic neuro-
pathy and the analysis of electrophysiological changes. Electromyogr Clin
Neurophysiol 2001; 41: 107–15.
Massry SG. Parathyroid hormone: a uremic toxin. Adv Exp Med Biol 1987;
223: 1–17.
Mogyoros I, Kiernan MC, Burke D. Strength-duration properties of human
peripheral nerve. Brain 1996; 119: 439–47.
Mogyoros I, Kiernan MC, Burke D, Bostock H. Excitability changes in human
sensory and motor axons during hyperventilation and ischaemia. Brain
1997; 120: 317–25.
National Kidney Foundation. NKF-K/DOQI clinical practice guidelines
for hemodialysis adequacy: update 2000. Am J Kidney Dis 2001; 37:
S7–64.
Neumcke B, Schwarz W, Stampfli R. Differences between K channels in motor
and sensory nerve fibres of the frog as revealed by fluctuation analysis.
Pflugers Arch 1980; 387: 9–16.
Nielsen VK. The peripheral nerve function in chronic renal failure. V.
Sensory and motor conduction velocity. Acta Med Scand 1973; 194:
445–54.
Nodera H, Bostock H, Kuwabara S, Sakamoto T, Asanuma K, Jia-Ying S, et al.
Nerve excitability properties in Charcot-Marie-Tooth disease type 1A.
Brain 2004; 127: 203–11.
Panayiotopoulos CP, Lagos G. Tibial nerve H-reflex and F-wave studies in
patients with uremic neuropathy. Muscle Nerve 1980; 3: 423–26.
Puksa L, Stalberg E, Falck B. Reference values of F wave parameters in healthy
subjects. Clin Neurophysiol 2003; 114: 1079–90.
Schaefer K, Offermann G, von Herrath D, Schroter R, Stolzel R, Arntz HR.
Failure to show a correlation between serum parathyroid hormone,
nerve conduction velocity and serum lipids in hemodialysis patients.
Clin Nephrol 1980; 14: 81–8.
Slatopolsky E, Martin K, Hruska K. Parathyroid hormone metabolism and its
potential as a uremic toxin. Am J Physiol 1980; 239: F1–12.
Van den Neucker K, Vanderstraeten G, Vanholder R. Peripheral motor and
sensory nerve conduction studies in haemodialysis patients. A study of 54
patients. Electromyogr Clin Neurophysiol 1998; 38: 467–74.
Vanholder R, De Smet R, Hsu C, Vogeleere P, Ringoir S. Uremic
toxicity: the middle molecule hypothesis revisited. Semin Nephrol 1994;
14: 205–18.
Weiss G. Sur la possibilite de rendre comparables entre eux les appareils
servant l’excitation electrique. Arch Ital Biol 1901; 35: 413–46.
Uraemic neuropathy Brain (2005) Page 11 of 11
by guest on July 18, 2016http://brain.oxfordjournals.org/
Dow
nloaded from
Copyright © 2022 FDOKUMEN