
Development of novel fusogenic vesosomes for transcutaneous immunization
Upload
khangminh22Category
view
0download
0

Pain Reviews 2001; 8: 00–00
© Arnold 2001 10.1191/0968130201pr182ra
IntroductionTranscutaneous electrical nerve stimulation(TENS) is used by health care professionalsthroughout the world to provide pain relief for awide range of conditions, including postoperativepain, labour pain and chronic pain. During
TENS, electrical currents are generated by astimulating device and delivered across the intactsurface of the skin via conducting pads calledelectrodes (Figure 1). The popularity of TENShas grown because it is noninvasive, easy toadminister and has few side-effects or drug inter-actions. There is no potential for toxicity or over-dose and patients can administer TENSthemselves at home and titrate the dosage oftreatment as required. When compared withlong-term drug therapy, TENS treatment is con-siderably cheaper.1–3
Recently, systematic reviews have challenged
Address for correspondence: Mark I Johnson, School ofHealth Sciences, Faculty of Health and Environment, LeedsMetropolitan University, Calverley Street, Leeds LS1 3HE,UK. E-mail [email protected]
Transcutaneous Electrical NerveStimulation (TENS) and TENS-like devices: do they providepain relief?Mark I JohnsonSchool of Health Sciences, Faculty of Health and Environment,Leeds Metropolitan University, UK
The term ‘transcutaneous electrical nerve stimulation’ (TENS) is synonymous with a standard TENSdevice. Increasingly, nonstandard TENS-like devices are being marketed to health care professionals forpain relief. These include: interferential current therapy, microcurrent electrical therapy, high-voltagepulsed (galvanic) currents, TENS-pens, transcranial electrical stimulation and Limoge currents, Codetron,transcutaneous spinal electroanalgesia, action potential simulation, and H-wave therapy. This review eval-uates the effectiveness of TENS and TENS-like devices for pain relief, to inform health care profession-als about device selection. The results from systematic reviews suggest that TENS is not effective forpostoperative pain and labour pain, although volatile evaluation models may partly explain the findings.Evidence is inconclusive for chronic pain. Health care professionals should not dismiss the use of TENSfor any condition until the issues in clinical trial design and review methodology have been resolved. Thereis limited experimental evidence available for most TENS-like devices. Claims by manufacturers aboutthe specificity and extent of effects produced using TENS-like devices are overstated and could probablybe achieved by using a standard TENS device or a microcurrent electrical therapy device. When makingdecisions about device selection, health care professionals should consider the physiological intention ofcurrents and whether this can be achieved by using particular devices. Clinical trials that examine the rel-ative effectiveness of TENS-like devices with a standard TENS device are desperately needed.

8 MI Johnson
Pain Reviews 2001; 8: 00–00
claims that TENS is clinically effective.Bandolier, the journal for evidence-based healthcare that uses the findings of systematic reviewsto provide ‘clinical bottom lines’ states that:‘TENS is not effective in the relief of postopera-tive pain’4; ‘TENS does not alleviate labour painnor reduce the use of additional analgesics’5;‘There is a lack of evidence for the effectivenessof TENS [for chronic pain] at recommendedtreatment schedules’.6 Concerns about TENS’effectiveness have not reduced the variety ofTENS devices reaching the market, which seemto be fuelled in part by advances in electronictechnology and the need to gain a competitiveedge in the market-place. The aim of this articleis to review critically the clinical effectiveness ofTENS and TENS-like devices for pain relief inorder to inform decisions about device selection.For the purpose of this article TENS-like devices
include any stimulating device that delivers elec-trical currents across the intact surface of the skinand whose generic name differs from TENS. Thiswill include interferential current therapy (IFT),microcurrent electrical therapy (MET), high-voltage pulsed (galvanic) currents (HVPC),TENS-pens (in particular, high-voltage TENS-pens), transcranial electrical stimulation (TCES,in particular Limoge currents), Codetron, tran-scutaneous spinal electroanalgesia (TSE), actionpotential simulation (APS), and H-wave therapy(HWT). This list is not exhaustive. The reviewwill not address the potential use of TENS-likedevices for nonpainful conditions, although ref-erence to these uses will be made where deemedappropriate.
Figure 1 A standard TENS device. An electrical pulse generator delivers currents via conducting electrodesattached to the intact surface of the skin. Traditionally, carbon rubber electrodes smeared with conducting geland attached to the skin using self-adhesive tape were used to deliver the electrical currents. Nowadays, self-adhesive electrodes are used (modified from Figure 17.1 in: Johnson M. Transcutaneous electrical nervestimulation (TENS). In: Kitchen S ed. Electrotherapy: evidence-based practice. Edinburgh: ChurchillLivingstone, 2001: 259–862; with permission from Elsevier Science)

Efficacy of TENS and TENS-like devices in pain relief 9
Pain Reviews 2001; 8: 00–00
Defining TENSIn broad terms TENS is anything that deliverselectricity across the intact surface of the skin toactivate underlying nerves. This would includethe delivery of electric shocks by electrogenicfish, as was commonly used in early history, andthe harnessed and controlled delivery of currentswith specific characteristics as used in mostmodern-day TENS devices. A broad definition ofTENS would not take account of the electricalcharacteristics of the currents (i.e. the outputcharacteristics or technical specifications of thedevice). However, in health care the term TENSis commonly used to describe currents deliveredby a ‘standard TENS device’ (Figure 1).
The standard TENS deviceStandard TENS devices are distinguished bytheir output characteristics. They usually deliverbiphasic pulsed currents in a repetitive mannerwith a pulse duration between 50 µs and 1000 µsand pulse frequencies between 1 and 250 pulsesper second (pps).1,2,7–9 Pulses are usually deliv-ered in a continuous pattern, although mostmodern-day devices have other patterns availablesuch as burst and modulation (Table 1, Figure 2).The technical specifications and output charac-
teristics of standard TENS devices vary betweenmanufacturers, as they attempt to achieveuniqueness and a competitive edge in the market-place. However, these variations are minor andprobably have limited impact on the physiologi-cal effects produced by the devices. As TENS isa technique-based intervention, outcome will bedictated by the appropriateness of TENS proce-dures used to deliver currents as determined bythe end-user. A number of factors need to beconsidered when determining a TENS procedure,including the characteristics of the electrical cur-rents selected by the user (i.e. the output char-acteristics), the application procedure (i.e.electrode type and location) and the dosingregimen (Figure 3). The number of potentialTENS procedures is vast, even with a simpleTENS device, so it is important that the user hasbasic knowledge about the principles underpin-ning TENS techniques.
Principles of TENSThe purpose of TENS is to activate selectivelydifferent populations of nerve fibres in order toproduce particular physiological outcomes. The common types of TENS described in the literature are1,7,9:
Table 1 The technical specifications of a standard TENS device modified from Table 1 in: Johnson MI. Acritical review of the analgesic effects of TENS-like devices. Phys Ther Rev 2001; 6: 153–7310)
Weight Dimensions 50–250 g
6 × 5 × 2 cm (small device) 12 × 9 × 4 cm (large device)
Cost £30–150Pulse waveform (usually fixed) Monophasic
Symmetrical biphasicAsymmetrical biphasic
Pulse amplitude (usually adjustable) 1–50 mA into a 1 k Ω loadPulse duration (sometimes fixed, sometimes adjustable) 10–1000 µs Pulse frequency (usually adjustable) 1–250 pps Pulse pattern Continuous and burst
Some devices have random pulse frequencySome devices have modulated pulse amplitudes, frequencies and/or duration
Channels 1 or 2 Batteries PP3 (9V), rechargeableAdditional features Timer

10 MI Johnson
Pain Reviews 2001; 8: 00–00
• Conventional TENS;• Intense TENS;• Acupuncture-like TENS (AL-TENS)
(Table 2).
These types of TENS have evolved fromknowledge about the ability of various nervefibres to activate different analgesic mechanismsin the body. Evidence from axonal stimulationstudies in vitro suggests that excitability variesaccording to the characteristics of an externallyapplied electrical current. The different types ofTENS attempt to describe the most efficientcharacteristics of current to activate endogenousanalgesic mechanisms and they have been widelyaccepted in the health care profession.Unfortunately, the use of these ‘banner’ terms
oversimplifies TENS techniques and this hasresulted in TENS literature that tends to focus onthe output characteristics of TENS devices ratherthan the physiological intention of the currents.Evidence suggests that the theoretical relation-ship between output characteristics and nervefibre activation may break down in practiceowing to the nonhomogeneous nature of thetissue underlying the electrodes.11,12 It is impor-tant to clarify the physiological intention of dif-ferent types of TENS when delivered by astandard TENS device.
Conventional TENSThe purpose of conventional TENS is to acti-
vate selectively large diameter Aβ fibres without
AMPLITUDE
HIGH
LOW
DURATION
SHORT LONG
FREQUENCY
HIGH (250pps) LOW (1pps)
PATTERN
CBM
On
Off4
F7
6
9
10 1
5
2
38
2
3
46
8
9
10 1
7 5
I4
D7
6
9
10 1
5
2
38
CONTINUOUS
FREQUENCY MODULATED
RANDOM PULSES
Figure 2
BURST
Figure 2 Common output characteristics on standard TENS devices (topographic view). Most devices allowthe amplitude and frequency of electrical pulses to be controlled by the end-user. Pulse duration and pulsepattern options are also available on some standard TENS devices: (pps: pulses per second; I: intensity; F:frequency; D: duration; C: continuous; B: burst; M: modulation) (modified from Figure 17.1 in: Johnson M.Transcutaneous electrical nerve stimulation (TENS). In: Kitchen S ed. Electrotherapy: evidence-basedpractice. Edinburgh: Churchill Livingstone, 2001: 259–862; with permission from Elsevier Science)

Efficacy of TEN
S and TEN
S-like devices in pain relief 11
Pain R
eviews 2001; 8
: 00–00
Figure 3 Variables influencing the way in which TENS can be administered. Many possible combinations of TENS parameters can bechosen by the end-user
Pulse Pulse Pulse Electrode Prescribed Openfrequency intensity pattern Number Location Treatment Treatment As much as you like1–250 pps 1–50 mA Continuous Pen (point) Site of pain Time frequency Before pain
Paraesthesia Burst 2 electrodes Nerve bundle Seconds Per day During pain• barely perfceptible Random • single channel Acupuncture points Minutes Per week• comfortable (weak) Modulated 3 electrodes Trigger point Hours Per month• comfortable (strong) • amplitude • Limoge currents Dermatomal• painful • frequency 4 electrodes Myotomal• painful • duration • dual channel Transcranial
Muscle contraction > 4 electrodes Transpinal• yes/no • multichannel Other . . .• tetanic/phasic 6 active electrodes
• Codetron
Elecrical Application Dosagecharacteristics procedure regimen

12M
I Johnson
Pain R
eviews 2001; 8
: 00–00
Table 2 TENS techniques that can be achieved using a standard TENS device. The output (electrical) characteristics identified for eachTENS technique are based on the strength and duration of pulsed currents necessary to generate an action potential in different types ofaxon.7 In clinical practice, patients and practitioners use the sensation produced by TENS to determine the appropriate stimulating character-istics (modified from Table 2 in: JOhnson MI. A critical review of the analgesic effects of TENS-like devices. Phys Ther Rev 2001; 6:153–7310)
Purpose of Theoretical optimum Sensory experience Electrode position Analgesic profile Duration of Mechanism ofcurrents output characteristics during stimulation treatment analgesic action
(desired outcome)
Conventional Selective High frequency/low Strong but Site of pain Rapid onset <30 min Continuously Segmental TENS activation of intensity: comfortable Dermatomal after switch-on when in pain
nonnoxious cutaneous Amplitude = low electrical Rapid offset <30 minsafferents (e.g. Aß Duration = 100–200 µs paraesthesia after switch-offfibres from Frequency = 10–200 pps with minimalmechano receptors) Pattern = continuous muscle
contraction
AL-TENS Selective Low frequency/high Strong but Motor point/muscle Delayed onset >30 mins ~30 mins/session Extrasegmentalactivation of intensity: comfortable at site of pain after switch-on as muscle fatigue Segmentalmotor efferents to Amplitude = high muscle twitches Myotomal Delayed offset >1 h may occurgenerate a muscle Duration = 100–200 µs after switch-offtwitch and activity Frequency = 2 bps andin nonnoxious muscle 100 pps within burstafferents (i.e. GIII Pattern = burstfibres fromergoreceptors)
Intense TENS Activation of noxious High frequency/high Highest tolerable Site of pain or main Rapid onset <30 min ~15 mins/session Peripheralactivation of noxious intensity: level with nerve bundlel after switch-on as patients Extrasegmental‘pinprick’ cuntaneous Amplitude = high minimall proximal to delayed offset 1h experience Segmentalafferents (i.e. Aß fibres Duration = 1000 µs muscle pain after switch-off discomfortfrom nocipeptors Frequency = 200 pps contractionl
Pattern = continuous
bps: burst per second; pps: pulses per second
Efficacy of TENS and TENS-like devices in pain relief 13
Pain Reviews 2001; 8: 00–00
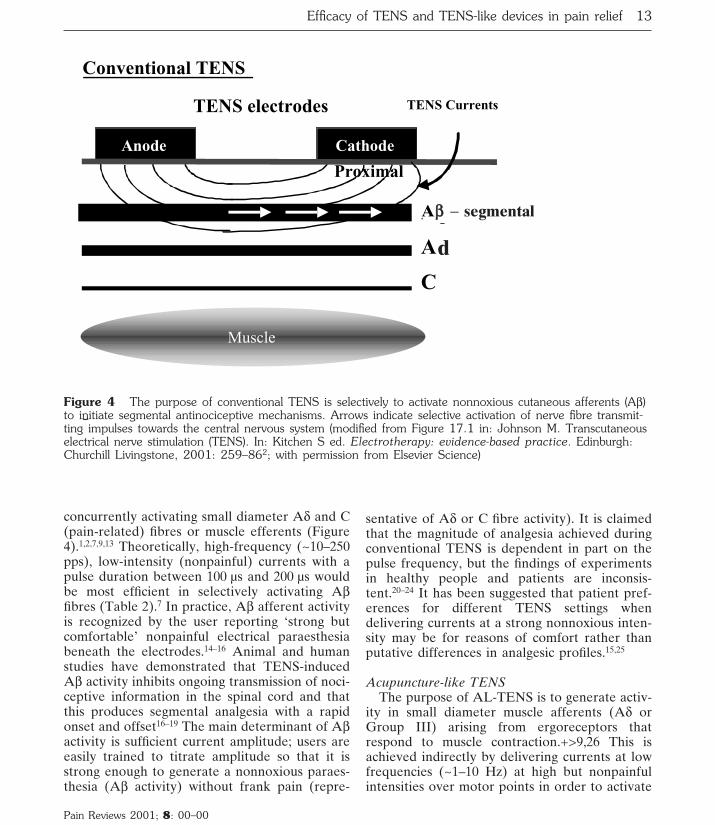
concurrently activating small diameter Aδ and C(pain-related) fibres or muscle efferents (Figure4).1,2,7,9,13 Theoretically, high-frequency (~10–250pps), low-intensity (nonpainful) currents with apulse duration between 100 µs and 200 µs wouldbe most efficient in selectively activating Aβfibres (Table 2).7 In practice, Aβ afferent activityis recognized by the user reporting ‘strong butcomfortable’ nonpainful electrical paraesthesiabeneath the electrodes.14–16 Animal and humanstudies have demonstrated that TENS-inducedAβ activity inhibits ongoing transmission of noci-ceptive information in the spinal cord and thatthis produces segmental analgesia with a rapidonset and offset16–19 The main determinant of Aβactivity is sufficient current amplitude; users areeasily trained to titrate amplitude so that it isstrong enough to generate a nonnoxious paraes-thesia (Aβ activity) without frank pain (repre-
sentative of Aδ or C fibre activity). It is claimedthat the magnitude of analgesia achieved duringconventional TENS is dependent in part on thepulse frequency, but the findings of experimentsin healthy people and patients are inconsis-tent.20–24 It has been suggested that patient pref-erences for different TENS settings whendelivering currents at a strong nonnoxious inten-sity may be for reasons of comfort rather thanputative differences in analgesic profiles.15,25
Acupuncture-like TENSThe purpose of AL-TENS is to generate activ-
ity in small diameter muscle afferents (Aδ orGroup III) arising from ergoreceptors thatrespond to muscle contraction.+>9,26 This isachieved indirectly by delivering currents at lowfrequencies (~1–10 Hz) at high but nonpainfulintensities over motor points in order to activate
Muscle
A§ - segmental
TENS electrodes TENS Currents
Anode Cathode
Ad
C
Conventional TENS
Figure 4
Proximal
Figure 4 The purpose of conventional TENS is selectively to activate nonnoxious cutaneous afferents (Aβ)to initiate segmental antinociceptive mechanisms. Arrows indicate selective activation of nerve fibre transmit-ting impulses towards the central nervous system (modified from Figure 17.1 in: Johnson M. Transcutaneouselectrical nerve stimulation (TENS). In: Kitchen S ed. Electrotherapy: evidence-based practice. Edinburgh:Churchill Livingstone, 2001: 259–862; with permission from Elsevier Science)
d
Aββ − segmental

14 MI Johnson
Pain Reviews 2001; 8: 00–00
Aα efferents resulting in a forceful but non-painful phasic muscle twitch27,28 The subsequentvolley of impulses from muscle afferents medi-ates an extrasegmental antinociceptive mecha-nism and the release of endogenous opioidpeptides in a manner similar to that suggested foracupuncture (Figure 5).7,29–32 Low frequencyburst patterns of pulse delivery were incorpo-rated in TENS devices because they were foundto be more comfortable than low-frequencysingle pulses in producing muscle twitches (Table2).28 It should be remembered that currents deliv-ered during AL-TENS will also activate Aβduring their passage through the skin, leading tosegmental analgesia. AL-TENS has also beendescribed as the delivery of TENS to acupunc-ture points without reference being made to the
presence of muscle contractions. The use of theterm in this way is not entirely appropriate.33
Intense TENSThe purpose of intense TENS is to activate
small diameter Aδ cutaneous afferents by deliv-ering TENS over peripheral nerves arising formthe site of pain at an intensity that is just tolera-ble to the patient (Figure 6).2,34–36 Currents areadministered at high frequencies (up to 150 pps)to prevent phasic muscle twitches that would betoo forceful for the patient to tolerate (Table 2).Cutaneous Aδ afferent activity has been shownto block transmission of nociceptive informationin peripheral nerves and to activate extraseg-mental antinociceptive mechanisms.37–40 IntenseTENS will also activate Aβ fibres, producing seg-
MUSCLE
Aß - segmental
TENS electrodes
CONTRACTION
GI
GIII - extrasegmental
Cathode Anode
MUSCLE
AL-TENS
Motor point
Figure 5
Proximal
TENS Currents
Figure 5 The purpose of AL-TENS is selectively to activate large diameter motor efferents to elicit anonpainful muscle twitch. This muscle twitch generates activity in ergoreceptors and small diameter muscleafferents to initiate extrasegmental antinociceptive mechanisms. In addition, Aβ afferents are also likely tobecome active. Arrows indicate direction of relevant impulse information (modified from Figure 17.1 in:Johnson M. Transcutaneous electrical nerve stimulation (TENS). In: Kitchen S ed. Electrotherapy: evidence-based practice. Edinburgh: Churchill Livingstone, 2001: 259–862; with permission from Elsevier Science)
Aββ − segmental

Efficacy of TENS and TENS-like devices in pain relief 15
Pain Reviews 2001; 8: 00–00
mental antinociceptive effects. As intense TENSacts in part as a counter-irritant, it can be deliv-ered only for a short time, but it may prove usefulpostoperatively and for minor surgical proce-dures and such as wound dressing and sutureremoval.13,41
In clinical practice in the UK, conventionalTENS is most commonly used. AL-TENS andintense TENS are used only in specific situations.Despite a large published literature on TENS,there is a lack of good quality and systematicexperimental work that has directly comparedthe clinical effectiveness and analgesic profiles ofthese types of TENS.
The clinical effectiveness ofTENSWhen assessing TENS’ effectiveness one needs toisolate the effects due to the currents from theeffects associated with the act of giving the cur-rents. Many early TENS trials lacked appropri-ate controls and therefore changes observed intrials could have been due to patients’ expecta-tion that TENS would reduce pain. In addition,many early trials lacked randomization, leadingto the overestimation of treatment effects. Thiswas elegantly demonstrated by Carroll et al., whofound that 17/19 controlled clinical trials thatwere not randomized reported that TENS wasbeneficial for postoperative pain, whereas 15/17trials that were randomized reported that it wasnot.42 Recently, a number of systematic reviewsand meta-analyses on TENS have challenged the
Muscle
A§ - segmental
TENS electrodes TENS Currents
Anode Cathode
Ad - extrasegmental
C
Intense TENS
Figure 6
Proximal
Figure 6 The purpose of intense TENS is to activate noxious cutaneous afferents (Aδ) to initiate extraseg-mental antinociceptive mechanisms and peripheral blockade of nociceptive impulses travelling in Aδ fibres. Inaddition, Aβ afferents are also likely to become active. Arrows indicate direction of relevant impulse informa-tion (modified from Figure 17.1 in: Johnson M. Transcutaneous electrical nerve stimulation (TENS). In:Kitchen S ed. Electrotherapy: evidence-based practice. Edinburgh: Churchill Livingstone, 2001: 259–862;with permission from Elsevier Science)
Aββ − segmental
Ad − extrasegmental

16 MI Johnson
Pain Reviews 2001; 8: 00–00
Table 3 A summary of systematic reviews and meta-analysis on the clinical effectiveness of TENS.(modifiedfrom Table 17.4 in: Johnson M. Trancutaneous electrical nerve stimulation (TENS). In Kitchen S ed.Electrotherapy: evidence-based practice. Edinburgh: Churchill Livingstone, 2001: 259–862; with permissionfrom Elsevier Science)
Condition Existing reviews
Acute Pain Reeve et al., 199646: SRMixed conditions (dysmenorrheoa, dental, cervical, orofacial)TENS > control in 7/14 RCTsReviewers’ conclusion: evidence inconclusive – poor RCT methodology
Postoperative pain Reeve et al., 199646: SRTENS > control in 12/20 RCTsReviewers’ conclusion: evidence inconclusive – poor RCT methodologyCarroll et al., 199642: SRTENS > control in 2/17 RCTsReviewers’ conclusion: evidence of no effectBjordal et al., in press.48 MATENS > sham for reducing analgesic consumption (MWD = 35.5%) Reviewers’ conclusion: evidence of effect – analgesic sparing
Labour Pain Reeve et al., 199646: SRTENS > control in 3/9 RCTsReviewers’ conclusion: evidence inconclusive – poor RCT methodologyCarroll et al., 1997511: SRTENS > control in 3/8 RCTsReviewers’ conclusion: evidence of no effectCarroll et al., 199750: update of Carroll et al.,51: SRTENS > control in 3/10 RCTsReviewers’ conclusion: evidence of no effect
Chronic pain Reeve et al., 199646: SRMixed conditions (low back, pancreatitis, arthritis, angina)TENS > control in 9/20 RCTsReviewers’ conclusion: evidence inconclusive – poor RCT methodologyMcQuay and Moore, 199856: SRMixed conditions (low back, pancreatitis, osteoarthritis, dysmenorrhoea)TENS > control in 10/24 RCTsReviewers’ conclusion: evidence inconclusive – inadequate TENS dosesCarroll et al., 200157: SRMixed conditions (19 RCTs, 652 patients)TENS > control in 10/15 RCTsReviewers’ conclusion: evidence inconclusive – inadequate TENS doses
Gadsby and Flowerdew, 200062; Flowerdew and Gadsby, 199763: MALow back pain (6 RCTs)TENS > sham for pain relief (OR = 2.11)Reviewers’ Conclusion: TENS effective – poor RCT methodologyMilne et al., 200160; Brosseau et al., 200261: MALow back pain (5 RCTs, 421 patients)TENS = sham for pain relief (SMD = –0.207)Reviewers’ conclusion: evidence of no effect

belief that its effects are clinically meaningfuland/or a result of the electrical currents them-selves (Table 3).
TENS and postoperative pain Early reports suggested that TENS reduced post-operative pain and opioid consumption.43–45
However, a health technology assessment byReeve et al.46 reported that TENS was demon-strated to be of benefit in only 12/20 randomizedcontrolled trials (RCTs). A systematic review byCarroll et al.42 reported that TENS did notproduce significant benefit when compared withplacebo in 15/17 RCTs. Both reviews used painrelief as the primary outcome measure, althoughpatients in some of the trials had access to addi-tional analgesic drugs so that those in sham andactive TENS groups could titrate analgesic con-sumption to achieve similar levels of pain relief.There were also minor inconsistencies in judge-ments of trial outcome between the reviewersbecause of the difficulty of dichotomizing multi-ple outcome measures in RCTs. TENS is knownto be less effective for severe pains, like thoseassociated with thoracic surgical procedures, anddetecting reductions in mild pain (i.e. against asmall pre-TENS baseline) requires large samplesizes to achieve statistical power.47 Some RCTsused sample sizes with insufficient statisticalpower to detect potential differences betweengroups. Recently, my colleagues and I have per-
formed a meta-analysis of 21 RCTs that accountsfor some of these issues.48 We found that themean reduction in analgesic consumption afterTENS was 26.5% (range –6% to +51%) betterthan placebo. It is important that a subgroupanalysis of 11 trials (964 patients) that met ourcriteria for optimal TENS dosage (i.e. a strong,subnoxious electrical stimulation) reported amean weighted reduction in analgesic consump-tion of 35.5% (range 14–51%) better thanplacebo. In the trials without explicit confirma-tion of optimal TENS dosage, the mean weightedanalgesic consumption was 4.1% (range –10% to+29%) in favour of active TENS. The differencein favour of adequate stimulation was highly sig-nificant (p = 0.0002). This suggests that adequateTENS technique is necessary in order to achievean effect.
TENS and labour painAugustinsson et al. pioneered the use of TENS inlabour pain by delivering currents to areas of thespinal cord that correspond to the input of noci-ceptive afferents associated with the first andsecond stages of labour (e.g. T10–L1 and S2–S4respectively).49 Early reports of TENS’ successresulted in the design of specialized obstetricTENS devices with dual channel output and‘boost’ controls for contraction pain. Despiteextensive use of TENS, systematic reviews con-clude that TENS provides little, if any, pain relief
Efficacy of TENS and TENS-like devices in pain relief 17
Pain Reviews 2001; 8: 00–00
Price and Pandyan, 200158: MAPost-stroke shoulder pain (4 RCTs, 170 patients); any surface ESES = sham/no treatment control for pain relief (WMD = 0.13)ES > sham/no treatment control for range of movement (WMD = 9.17)Reviewers’ conclusion: evidence inconclusive
Osiri et al., 200265: MAKnee osteoarthritis (7 RCTs, 294 patients)TENS > sham for pain relief (SMD = –0.448, although only 2/7 RCTs +ve)Reviewers’ conclusion: evidence of effect – pain relief
Proctor et al., 200264: MAPrimary dysmenorrhoea (8 RCTs, 213 patients)HF TENS > sham for pain relief (OR = 7.2)LF TENS = sham for pain relief (OR = 1.3)Reviewers’ conclusion: evidence of effect – pain relief for HF TENS only
SR: systematic review; RCT: randomized-controlled trial; MWD: mean weighted difference; MA: meta-analysis;OR: odds ratio; SMD, standardized mean difference; ES, electrical stimulation; WMD, weighted mean differ-ence (= MWD); HF, high-frequency; LF, low-frequency

18 MI Johnson
Pain Reviews 2001; 8: 00–00
Table 4 Common characteristics of ‘generic categories’ TENS-like devices (taken in part from Table 3 in:Johnson MI. A critical review of the analygesic effects of TENS-like devices. Phys Ther Rev 2001; 6:153–7310)
Typical Standard TENS IFT MET HVPCcharacteristics
Delivery system 1 channel Quadripolar = 2 1 channel 1 channel(2 electrodes) channels (4 (2 electrodes) (2 electrodes)
electrodes) Single pointBipolar = 1 channel pen electrode(2electrodes) Suction electrodes sometimes used
Pulse generator Hand-held Desktop and Desktop and Desktop andhand-held hand-held hand-held
Recommended Site of pain Site of pain Site of pain Site of painelectrode position Either side of Either side of
wound woundAcupuncture/ Motor point fortrigger points muscletranscranial stimulation
Recommended Self-administration Under Under supervision Under treatment regimen as required supervision supervision of therapist supervision of
Continuous of therapist and self-admistration therapist Intermittentstimulation whenever Intermittent Intermittent stimulation Intemittent stimulation in pain stimulation (e.g. (e.g. ~20–60 min (e.g. ~20–60 min
~30 mins during for 1–3 times a day) for 1–3 times visit to clinic) a day)
Waveform Monophasic Amplitude Modified Twin peak symmetrical biphasic modulated square direct monophasic Asymmetrical biphasic interference current with spiked pulse
wave generated monophasic orby 2 out-of-phase biphasic pulsesinusoidal currents changing polarity
at regular intervalsAmplitude + 1–60 mA 1–60mA 1–600 µA 1–2 Aintensity Non-noxious Non-noxious No paraesthesia Paraesthesia
paraesthesia paraesthesia (i.e. below sensorydetection threshold)
Pulse rate Adjustable Adjustable Adjustable Adjustable1–250 pps 1–250 Hz for 1–5000 pps 1–120 pps
amplitude-modulatedwave Carrier wave2000–4000 Hz
Pulse duration Fixed and/or Carrier waves = Fixed/adjustable <100 µsadjustable unknown adjustable50–1000 µs Range unknown
Pulse pattern Continuous Amplitude Continuous ContinuousBurst modulated BurstModulated frequency, wave can be Modulatedamplitude and pulse continuous or amplitudeduration modulated in
frequencyusing sweepsand swing patterns

Efficacy of TENS and TENS-like devices in pain relief 19
Pain Reviews 2001; 8: 00–00
during labour.46,50,51 Carroll et al.50reported that10/10 RCTs showed that pain relief scores pro-duced by TENS were no greater than shamTENS or a no treatment control. However, theself-report of pain relief may have been compro-mised by access to additional analgesics in someof the RCTs. The finding that analgesic inter-vention may be less likely with TENS, asreported in the original systematic review, wasnot confirmed in the updated review when datafrom an additional study was added.
These findings seem to conflict with clinicalexperience where midwives and patients reportsatisfaction with TENS’ effects.52 It is possiblethat pain relief ratings were influenced by fluctu-ating emotional and physical conditions duringlabour because one trial found that significantlymore women and midwives favoured activerather than sham TENS when recorded underdouble-blind conditions at the end of childbirth.53
After childbirth, women are more likely to berelaxed and perhaps better able to reflect on theeffects of the intervention. The systematicreviews also included RCTs that used unconven-tional TENS devices.54,55 These studies usedLimoge currents, which are administered tran-scranially and clearly differ from conventionalobstetric TENS (see section on TCES). It is inter-esting that both studies reported that Limogecurrents produced analgesic sparing effects whencompared with sham or no-treatment control.
TENS and chronic painA large number of clinical trials suggest thatTENS is useful for chronic pain. Three system-atic reviews have examined TENS’ effectivenesson mixed populations of chronic pain patients.Reeve et al. reported that TENS was more effec-tive than sham (n = 7) or no treatment (n = 2) in9/20 RCTs.46 McQuay and Moore stated thatTENS was better than sham TENS, placebo pills,or inappropriate electrode placements in 10/24RCTs.56 Carroll et al. reported that TENS pro-vided better pain relief than sham or no treat-ment in 10/15 RCTs. All reviewers concludedthat the evidence for TENS in chronic pain wasinconclusive.57
Reviews on specific populations of chronicpain patients are also inconclusive. A meta-analy-sis of any form of surface electrical stimulation
on 170 patients with post-stroke shoulder painfound no significant change in pain incidence(odds ratio = 0.64) or pain intensity (standardizedmean difference (SMD) = 0.13) after electricalstimulation compared with control.58,59 However,electrical stimulation improved the pain-freerange of passive humeral lateral rotation(weighted mean difference (WMD) = 9.17) andreduced the severity of glenohumeral subluxation(SMD = –1.13). For low back pain the findings ofreviews have been contradictory. A meta-analy-sis on 321 patients reported no statistically sig-nificant differences between active and shamTENS for pain relief.60,61 In contrast, a meta-analysis on 288 patients reported that TENSreduced pain and improved the range ofmotion.62,63 The overall odds ratio for pain reliefagainst placebo was only 2.11, although an oddsratio of 7.22 was reported in favour of AL-TENS.However, RCTs on AL-TENS did not state thatTENS generated muscle contractions, which isconsidered to be a prerequisite for AL-TENS. Ameta-analysis of the effect of TENS on pain asso-ciated with primary dysmenorrhoea reported thathigh-frequency but not low-frequency TENS wasmore effective for pain relief than sham.64 Ameta-analysis of 294 patients with kneeosteoarthritis reported that TENS produced sig-nificantly better pain relief and reductions inknee stiffness than placebo.65
All reviewers conclude that the low method-ological quality of TENS trials has contributed tothe uncertainty in the clinical evidence for effec-tive use in chronic pain. Underdosing of TENShas been recognized as a problem and some trialsmeasure outcome after a single TENS interven-tion or following a course of intermittent TENStreatments.57 This differs from clinical practice,where long-term users of TENS administer itover long periods of time because the effects ofTENS appear to be maximal when the device isswitched on.15 Nevertheless, the uncertaintyabout the clinical effectiveness of standard TENSdevices for pain relief has questioned it as aviable treatment option. Attempts to improveefficacy by searching for optimal stimulator set-tings have largely been unsuccessful. As a result,health care professionals are turning to commer-cially available TENS-like devices with noveltechnical specifications that have emerged from
20M
I Johnson
Pain R
eviews 2001; 8
: 00–00
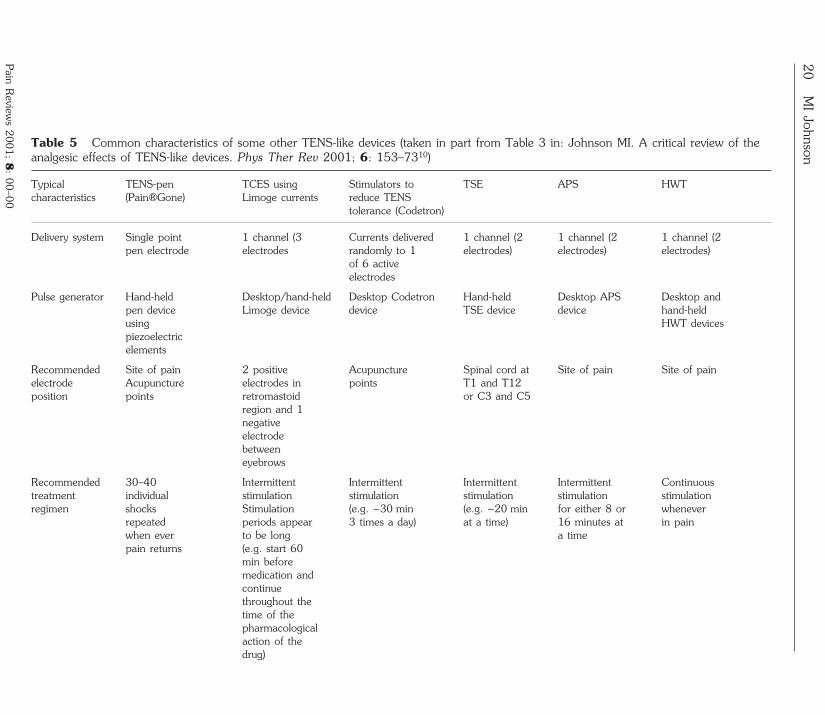
Table 5 Common characteristics of some other TENS-like devices (taken in part from Table 3 in: Johnson MI. A critical review of theanalgesic effects of TENS-like devices. Phys Ther Rev 2001; 6: 153–7310)
Typical TENS-pen TCES using Stimulators to TSE APS HWTcharacteristics (Pain®Gone) Limoge currents reduce TENS
tolerance (Codetron)
Delivery system Single point 1 channel (3 Currents delivered 1 channel (2 1 channel (2 1 channel (2 pen electrode electrodes randomly to 1 electrodes) electrodes) electrodes)
of 6 activeelectrodes
Pulse generator Hand-held Desktop/hand-held Desktop Codetron Hand-held Desktop APS Desktop and pen device Limoge device device TSE device device hand-held using HWT devicespiezoelectricelements
Recommended Site of pain 2 positive Acupuncture Spinal cord at Site of pain Site of painelectrode Acupuncture electrodes in points T1 and T12position points retromastoid or C3 and C5
region and 1negativeelectrodebetweeneyebrows
Recommended 30–40 Intermittent Intermittent Intermittent Intermittent Continuous treatment individual stimulation stimulation stimulation stimulation stimulation regimen shocks Stimulation (e.g. ~30 min (e.g. ~20 min for either 8 or whenever
repeated periods appear 3 times a day) at a time) 16 minutes at in painwhen ever to be long a time pain returns (e.g. start 60
min beforemedication andcontinuethroughout thetime of thepharmacologicalaction of thedrug)

Efficacy of TEN
S and TEN
S-like devices in pain relief 21
Pain R
eviews 2001; 8
: 00–00
Waveform Single Positive pulse Square wave Differentiated/ Monophasic Biphasic wave Monophasic (high intensity with DC rectangular square pulse with spiked pulse short duration) current of with exponential
followed by opposite exponential decaynegative pulse polarity decay and DC(low intensity following offset of 5 Vlong duration) each pulsedelivered intrains (bursts)
Amplitude + Low ampere ~2 mA/30 V Milliampere Low ampere Microampere Milliampere high voltage <60 m\A high voltage No <10 mA ‘low (e.g. 6 µA/ Non-noxious No paraesthesia output to 15,000 V) paraesthesia paraesthesia (i.e. below ‘reduce Non-noxious to pinprick (i.e. below sensory heating’ to mild pain sensory detection Non-noxious noxious pinprick detection threshold) paraesthesia sensation threshold)
Pulse rate Ad hoc: 125 kHz Presets Presets Fixed at Adjustable or depends on interrupted include include ~150 pps presets rate of button with an 1, 2, 4, 200 pps 600– between 2 andpress intermittent 10,000 pps 60 pps
current of83 Hz
Pulse duration Unknown but Positive phase Fixed preset Fixed preset Fixed preset Fixed preset atat fixed preset of pulse between between 1.5 between 800 16000 µs
1.7 µs, 1000–5000 µs and 4 µs and 6600 µsnegativephase ofpulse 6.3 µs
Pulse pattern Ad hoc: Trains of high- Continuous Continuous Continuous Continuous depends on frequency Burstpattern of pulsesbutton press interrupted by
low frequencypulses
22M
I Johnson
Pain R
eviews 2001; 8
: 00–00 Table 6 TENS-like device identity. Randomized controlled clinical trials that compare the analgesic effects of TENS-like devices with a standard TENSare needed for all categories (taken in part from Table 4 in: Johnson MI. A critical review of the analgesic effects of TENS-like devices. Phys Ther Rev2001; 6: 153–7310)
Standard IFT MET HVPC TENS-pen TCES Stimulators to TSE APS HWTTENS using Limoge reduce TENS
currents tolerance(Codetron)
Main Pain relief Pain relief Assist Muscle Pain relief Reduce Pain relief Pain relief Pain relief Pain reliefindications Muscle tissue stimulatio analgesic/
stimulation healing Assist anaestheticAnti- Pain relief tissue intakeinflammatory healing
Pain relief
Claims for Currents Currents Currents Currents Currents Currents Currents Currents Currents Currents uniqueness selectively excite deep- mimic pass easily activate directly reduce by-pass skin mimic more
activate seated ‘current of through body’s pain influence nervous and action comfortable different tissue injury’ to skin to relief brain system directly potentials than TENS nerve accelerate activate system function habituation excite Relationship fibres to healing motor and mimic central to H-reflex initiate nerves electro- nervous unclearpain selectively acupuncture systemmodulatory tissue tomechanisms reduce
centralsensitization
Principle of Proven Unclear Unclear Unclear Unclear Unclear Evidence Interesting Unclear Unclear action for Similar to may be due Similar to Could be Evidence supports but Similar to Similar topain relief standard to tissue standard noninvasive suggests reduction unproven MET standard
TENS? healing; TENS? acupuncture that central in TENSDifferent evidence nervous habituationanalgesic conflicting system but needseffects activity to beresulting

Efficacy of TEN
S and TEN
S-like devices in pain relief 23
Pain R
eviews 2001; 8
: 00–00
from and neuro shown thatdeep hormonal thisand levels translatessuperficial change intofibre clinicallyactivation meaningfulneed to be reductionsshown in the
incidenceof TENStolerance
Evidence Effects > Effects > ? effects = Unknown Unknown Unknown Effects > ? effects = Unknown ? effects > for placebo placebo placebo placebo placebo Effects = placeboanalgesic Analgesic Effects = standard Effects = effects in profiles conventional TENS and standard healthy types of TENS IFT TENSpeople TENS
needed
Evidence Large Little Little Very little No available Some Little Little Evidence Very little amount of evidence evidence evidence evidence evidence evidence evidence available evidence evidence available available, available available available available but available available and trials with on pain but ? effects > Effects = inappropriate Evidence but have conflicting outcomes conflicting placebo placebo in interpretation inconclusiveconflicting design outcomes Evidence findings ? effects > one of findingsand flaws ? effects > inconclusive ? effects > conventional unpublished ? effects =dependent ? effects = placebo in placebo in TENS study placeboon placebo initial trials sparing Evidence Effects > Evidencecondition Evidence Evidence analgesics inconclusive conventional inconclusivetreated inconclusive inconclusive for labour TENS in? effects > pain pilot studyplacebo if Evidence Evidenceadministered inconclusive inconclusivecorrectlyEvidenceinconclusive

24 MI Johnson
Pain Reviews 2001; 8: 00–00
other areas of health care. At present, informa-tion about the effectiveness of TENS-like devicesis limited and decisions about device selection arebeing based on unreliable sources such as manu-facturers’ material or hearsay from colleagues.An assessment of the merits of some of the com-mercially available TENS-like devices is needed.
Defining and categorizingTENS-like devicesFor the purpose of this review TENS-like devicesare defined as any stimulating device that deliv-ers electrical currents across the intact surface ofthe skin and whose generic name differs fromTENS. Potential TENS-like devices were identi-fied from a cursory search of published literature,coupled with discussions with colleagues in thefield. This was followed by searches ofMEDLINE (1966–2001) using device namesidentified from the cursory search and the keywords ‘transcutaneous electrical nerve stimula-tion’ and ‘electrical stimulation therapy’. Allpotential links to related articles were followed,as were manual searches of items given in refer-ence lists. Information from manufacturers andthe Internet was used wherever possible to helpto determine technical specifications, recom-mended treatment procedures, and establishclaims of effectiveness.
The search identified a variety of TENS-likedevices, although categorization according toformal criteria was impossible. Some devicescould be differentiated according to output char-acteristics (e.g. IFT, MET and HVPC; Table 4).Some devices could be differentiated accordingto the procedures used to deliver the currents(e.g. TENS-pens and TCES). Some could be dif-ferentiated according to novel principles ofaction (e.g. stimulators trying to overcome TENStolerance, TSE, APS and HWT; Table 5). Therewas much overlap between these divisions. Forexample, MET could be administered transcra-nially (e.g. as a type of TCES) or using a TENS-pen. Consequently, each TENS-like device isdiscussed separately for reasons of convenience(Table 6).
Interferential currenttherapyIFT was developed in the 1950s and has remainedfor the most part within the discipline of physio-therapy.66 Surveys have shown that IFT is usedthroughout the world67,68 and there appeared tobe more published information on IFT than anyof the other TENS-like device in this review.Three textbooks on IFT were found thatdescribed the clinical use of the modality basedon the personal experience of the authors.69–71
There was an absence of good-quality experi-mental work to support the claims made in thetextbooks.67,72,73 IFT is most commonly used forpain relief74 although advocates claim that it willalso reduce inflammation, assist tissue repair(including bone fractures) and re-educate muscle(especially for incontinence).69–71,75,76 IFT devicesare more expensive than standard TENS devicesand tend to reside in physiotherapy clinicsbecause they are relatively large. Recently, somebattery-operated hand-held IFT devices haveappeared on the market.
The purpose of IFT appears to be to delivercurrents to deep-seated structures. IFT stimula-tors are designed to generate an amplitude-mod-ulated interference wave, sometimes called theIFT ‘beat’. This wave is created by two out-of-phase currents that collide with each other togenerate an interference wave with a frequencyusually between 1 Hz and 200 Hz (Figure 7). Thetwo out-of-phase currents are delivered at fre-quencies between 2 Hz and 4 kHz because suchhigh-frequency short cycle duration waves willovercome skin impedance and penetrate deepbody structures.69–71,77–79 Advocates argue thatthese high-frequency kilohertz currents act asweak stimuli for nervous tissue, so a low fre-quency amplitude-modulated wave is created inorder to excite neurones.
Traditionally, the interference wave wascreated within the tissue by delivering two out-of-phase currents across the skin via four elec-trodes (termed quadripolar IFT), althoughnowadays the interference wave is often pre-modulated within the IFT device and deliveredvia two electrodes (bipolar IFT). IFT deviceshave an array of settings. The amplitude-modu-lated wave can be set at frequencies between 1
F

Efficacy of TENS and TENS-like devices in pain relief 25
Pain Reviews 2001; 8: 00–00
Hz and 200 Hz and can fluctuate between upperand lower preset boundaries (termed the sweep)over a set time duration (termed the swingpattern). For example, a 6 Λ 6 swing patterndelivers amplitude-modulated frequenciesbetween preset lower and upper frequencies overa 6-second time period. A 6 Λ 6 swing patterndelivers amplitude-modulated waves at the lowerfrequency for 6 s and then at its upper frequencyfor 6 s.
When used for pain relief, IFT is delivered togenerate a strong but comfortable electricalparaesthesia at the site of the pain. This approachis comparable with conventional TENS and islikely to generate Aβ activity and segmental anal-gesia. Similarities in administration proceduresfor IFT and conventional TENS have led some
commentators to challenge assumed differencesin analgesic profiles between the two modali-ties.66,73,80 Studies using healthy people havefound that IFT elevates an experimentallyinduced cold pain threshold and reduces experi-mentally induced ischaemic pain when comparedwith sham, although there were no differences inIFT effects when compared with conventionalTENS.19,81,82 It is claimed that different ampli-tude-modulated wave frequencies selectivelyactivate different populations of nerve fibres togenerate specific physiological outcomes. Forexample, Savage70 claims that frequencies of100–130 Hz are in the analgesic range and thesedative range, and that frequencies of 5–100 Hzactivate autonomic nerves. No evidence could befound to support such claims. Furthermore, the
Figure 7
Time
Channel A4000Hz
Channel B4100Hz
AMF100Hz
Cur
rent
Am
plit
ude
Amplitude-Modulated Wave within deep seated tissue
B
BA
A
Figure 7 Principles used to generate an amplitude-modulated interference wave within deep tissue. Darkshaded electrodes attached anterior and lighter shaded electrodes attached posterior (A: electrodes forchannel A; B: electrodes for channel B) (adapted from Figure 1 in: Johnson MI, Tabasam G. A double blindplacebo controlled investigation into the analgesic effecs of interferential currents (IFC) and transcutaneouselectrical nerve stimulation (TENS) on cold induced pain in healthy subjects. Physiother Theory Pract 1999;15: 217–3319)
26 MI Johnson
Pain Reviews 2001; 8: 00–00
Palmer et al.90 found no differences in psy-chophysiological outcomes when IFT was admin-istered in both the presence and the absence ofthe amplitude-modulated wave. Thus, it is possi-ble that any pain relieving effects of IFT are dueto the higher frequency current (i.e. 2–4 kHz)rather than to the amplitude-modulated wave.
Microcurrent electricaltherapyMET uses currents that are 1/1000th of anampere smaller than those delivered by standardTENS devices (milliamperes). Advocates claimthat MET devices can be used to accelerate tissuehealing and relieve pain, especially pain relatedto sporting injuries91–94 MET comes under arange of guises, including microcurrent electricalnerve stimulation, microamperage stimulation,low-intensity direct current, and pulsed low-intensity direct current. Definitions of MET arevaried, although the American Physical TherapyAssociation has defined it as a low-intensitydirect current that delivers monophasic or bipha-sic pulsed microamperage currents across theintact surface of the skin.8 Often, MET devicesutilize adjustable pulse frequencies between 0.5pps and 150 pps with periodic reversals in polar-ity. MET can be delivered using probe electrodes(sometimes in the form of a pen) or pad elec-trodes, which are applied to acupuncture points,trigger points or over the site of pain. Some METdevices have a point finder to detect areas of theskin with low resistance, which are believed tocorrespond to acupuncture points.95 MET canalso be administered on ear lobes and transcra-nially, where it is claimed that it will relievemigraine, headache, insomnia and stress.96
MET developed from the claim that tissuehealth is maintained by a direct current electricalsystem in the human body and that a shift in this‘normal current flow’ occurs when tissue isdamaged97–99 This direct current shift wasdescribed as the ‘current of injury’, with a mag-nitude in the microampere range. Advocatesclaim that MET simulates this current of injuryto assist tissue growth and healing, and that mil-liampere currents delivered by standard TENSdevices are detrimental to this process ofrepair.100,101 They also claim that MET provides
physiological rationale for including frequencysweeps and swing patterns in IFT device designis obscure. Systematic investigations into theeffects of different frequencies and swing pat-terns of IFT on experimentally induced pain inhealthy people has found that analgesia was notaffected by frequency or swing pattern when IFTwas administered at a strong but comfortableintensity without concurrent muscle contrac-tion.83–85
The majority of clinical reports on IFT effectsare anecdotal and lack appropriate controls.Taylor et al. reported no significant differencesbetween the effects of sham and active IFT onpain and dysfunction in 40 patients suffering fromjaw pain.86 Quirk et al. found no additional ben-efits from IFT when compared with exercise in38 patients suffering pain and dysfunction asso-ciated osteoarthrosis of the knee.87 An RCT on152 patients by Werners et al.87 reported thatthere were no significant differences in the mag-nitude of pain relief achieved using IFT whencompared with motorized lumbar traction withmassage management for low back pain. The lackof IFT effects in these controlled studies may bedue to underdosing of IFT because it is believedthat patients experience fatigue if stimulationlasts more than 30–40 min. Observations ofpatients using TENS at strong but comfortableintensities in a similar manner to that describedfor IFT suggest that this is not the case. Theacceptance of short duration IFT treatment maybe due to constraints of the clinical rota becausemost IFT treatment sessions take place in theclinical setting under the supervision of a thera-pist. Furthermore, applying IFT may not be themost appropriate approach; Hurley et al.88 haveshown that IFT delivered over the spinal nerveproduced greater reductions in functional dis-ability when compared with IFT administereddirectly over the painful area.
Explanations of how IFT produces pain reliefare at best vague and tend to focus on ‘pain gates’and ‘endorphins’. The justification for using anamplitude-modulated interference wave to stim-ulate neural tissue rather than a biphasic pulsedcurrent as generated by standard TENS devicesseems to be entirely speculative. Demmink11 hasreported that IFT modulation patterns could bereproduced in water but not in biological tissue,where current distribution was unpredictable.

Efficacy of TENS and TENS-like devices in pain relief 27
Pain Reviews 2001; 8: 00–00
pain relief, although it is unclear whether this isa primary effect through direct action on theantinociceptive system or a secondary effect fromtissue healing. Users do not perceive MET cur-rents, so it seem likely that the putative mecha-nism of action differs from conventional TENS.A relatively large body of published research wasfound for MET that could be divided into effectson pain and on tissue healing.
MET and pain reliefInvestigations into the effects of MET on exper-imentally induced pain in healthy prople haveproduced contradictory results. Weber et al.reported no significant differences betweenmassage, upper body ergometry, MET and a notreatment control on delayed-onset muscle sore-ness induced by high-intensity exercise in 40healthy volunteers.102 In contrast, Lambert et al.reported that MET reduced the severity ofdelayed-onset muscle soreness in 30 healthy menunder double-blind, placebo-controlled condi-tions.103 A study using cold-induced pain foundno significant differences between active andplacebo MET on experimentally-induced painthreshold and pain intensity rating in 36 healthyvolunteers using single-blind methodology.104
evidence available from clinical trials is alsoinconclusive. Clinical trials on MET often lackmethodological rigor. For example, a report of adouble-blind placebo-controlled trial claimedthat MET significantly reduced chronic back painin 40 patients, yet details about the statisticalanalysis were omitted from the report.105 METwas administered for two 6-second periods to 16points on the back, three times per week for twoweeks. No physiological rationale was given forsuch a prescriptive treatment regimen. Similarly,MET was given to the affected hands of 36patients with carpal tunnel syndrome for threetreatments per week for 4–5 weeks in combina-tion with low-level laser acupuncture and otheralternative therapies.106 Although it was claimedthat this treatment approach was successful inrelieving pain, it was not possible to determinethe exact contribution of MET. Clinical trialshave also found that MET effects are compara-ble to TENS in patients with migraine andchronic headaches,107but less effective than alaser for improving mobility and pain in patientswith degenerative joint disease.108
MET and tissue healingIt is possible that putative pain relief may be a by-product of the accelerated healing process. Initialreports of experiments in vitro suggested thatMET accelerates the healing of damaged tis-sue,109–112 possibly through increased protein syn-thesis100,101,113 or through antimicrobal effects114–116
However, two well-controlled animal studiesfound that MET did not accelerate the healing ofexperimentally induced wounds in rats andYucatan mini pigs.117,118 The editor of one journalconcluded that ‘the time has come to weigh theevidence and to face the accumulation of datafrom these and other reports indicating that thismodality [MET] does not assist in wound healingwhen used in the manner described.119
Clinical evidence is also inconclusive.Encouraging reports of MET accelerating thehealing of ulcers and wounds are often under-mined by the lack of appropriate controlgroups.109,120–122 Carley and Wainapel123 adminis-tered MET for two hours twice a day for sixweeks and found that it accelerated the healingof ulcers in 30 patients when compared with con-ventional wound dressings. However, the absenceof a placebo control group meant that observedeffects may have been due to the act of givingMET rather than the electrical currents gener-ated by MET. Randomized double-blind sham-controlled multicentre studies on the effects ofelectrical stimulation on ulcers and wounds doexist, although it is not certain whether the typesof electrical stimulation used were strictly MET.Mulder124 found that pulsed electrical stimulationdecreased wound size by 56% when comparedwith a 33% reduction with sham on 59 patientswith open wounds of pressure, vascular and sur-gical origin. A similar study on 47 patients withchronic dermal ulcers found differences in woundsize and healing rate in favour of electrical stim-ulation.125 Pulsed cathodal electrical stimulationwas delivered twice daily at a pulse frequency of128 pps, although the peak amplitude of 29.2 mAwas higher than that seen for MET. A meta-analysis of 15 trials on a variety of forms of elec-trical stimulation reported that the healing ratewas 22% per week compared with 9% for con-trols.126 Unfortunately, findings on the relativeeffectiveness of the different types of electricalstimulation devices used in the studies wereinconclusive.

28 MI Johnson
Pain Reviews 2001; 8: 00–00
Rebox devices also deliver microampere cur-rents and, as a consequence, could be classed asMET. They were developed in the 1970s and usecurrent trains of unipolar rectangular pulses viaa charged probe electrode using microampereamplitudes (1–300 µA), pulse frequenciesbetween 200 Hz and 5000 Hz, and a pulse dura-tion of 50–250 µs.127,128 Available evidence aboutthe pain relieving effects of Rebox is conflicting.Johannsen et al.129 reported that Rebox improvedboth pain and function in patients with chroniclateral epicondylitis. In contrast, Hatten et al.reported that Rebox did not provide significantpain relief in patients130 A placebo-controlledtrial by Nussbaum and Gabison showed no dif-ferences between active and placebo with dailytreatments of Rebox on experimentally-induceddelayed onset muscle soreness in 30 healthy vol-unteers.131
High-voltage pulsed currents HVPC, also known as high-voltage galvanic stim-ulation and high-voltage pulsed galvanic stimula-tion, have been used for muscle strengthening,wound healing and pain relief since the1940s.99,127, 128,132 Until recently HVPC deviceswere relatively large and resided in physiother-apy clinics, although, with advances in electronictechnology, modern HVPC devices can be similarin size to standard TENS devices and, as a con-sequence, are being marketed for pain andwound management. HVPC devices deliverdirect current with twin monophasic spikedpulses of 10–500 V (500 ohm load) with a shortpulse duration (microseconds) to increase pene-tration of tissue, leading to greater selectivity inrecruiting motor nerves in innervated muscle andimproved comfort for the patient. Pulses aredelivered at double pulse frequencies of between1 and 120 per second via a variety of types ofelectrodes including sponge, traditional carbonrubber and hand-held point electrodes.127,132
Much of the experimental work on HVPC hasfocused on claims that it assists wound healingand is out of the scope of this discussion.99,128 TwoRCTs of note have reported that HVPC assiststhe rate of healing of ulcers. Kloth and Feedar133
delivered HVPC to patients with decubitis ulcers
and reported that the healing rate was fasterwhen compared with sham. Griffin et al.134
reported that HVPC significantly increase thehealing rate of pressure ulcers in the pelvic regionwhen given at 100 pps and an intensity of 200 Vfor 1 h a day for 20 consecutive days.
Little experimental work on the effects ofHVPC on pain relief was found. A comparisonof the analgesic effects of HVPC with differenttypes of TENS on electrically induced painthreshold and tolerance in 14 healthy peoplefound no significant differences between thegroups.135 Morris and Newton136 investigated theeffects of HVPC on 28 patients with symptomsof pain and discomfort in the perirectal or rectalregion (levator ani syndrome). HVPC wereadministered using a rectal probe for 1 h at a fre-quency of 120 Hz and at the maximum intensitythat the patients could tolerate. They reportedthat 50% of these patients had pain or symptomrelief after an average of eight treatments,although the study lacked a control group.Clearly, more experimental work is needed.
TENS-pensA variety of hand-held pain relieving ‘pens’ areavailable on the market, which deliver electricalcurrents to the intact surface of the skin using asingle point electrode. TENS-pens are availableas stand-alone battery operated devices orattached to battery operated pulse generators viaa lead. The single point electrode used in TENS-pens encourages users to deliver currents to dis-crete points on the surface of the body.Acupuncture points are often used as sites forstimulation and some devices incorporate anacupuncture point finder that detects low resis-tance on the skin. However, advertizing materialrecommends that TENS-pens can also be used tostimulate trigger points or the site of pain. Theuser needs to hold the pen during stimulation, sotreatment times tend to be short and often lessthan a minute. It is therefore assumed that pain-relieving effects occur predominantly post-stimulation.
The technical specifications of TENS-pens varyconsiderably between manufacturers, with avail-able pens delivering currents in both milliampere(i.e. using a standard TENS pulse generator) and

Efficacy of TENS and TENS-like devices in pain relief 29
Pain Reviews 2001; 8: 00–00
microampere (i.e. using a standard MET genera-tor) ranges. Milliampere pens that deliver pulsedcurrents at strong but nonnoxious intensities arelikely to activate large diameter nerve fibres andmimic the actions of conventional TENS. It is notknown whether there are differences in outcomewhen conventional TENS currents are deliveredto acupuncture points rather than to the site ofpain because experimental evidence is lacking. Areview of studies that assessed the pain relievingeffects of TENS when delivered to acupuncturepoints using traditional electrode pads reportedconflicting results.33 Furthermore, it is not knownwhether delivering nonnoxious pulsed currentsvia a pen produces different outcomes to thoseobtained by using self-adhesive surface elec-trodes. Nevertheless, as the post-stimulationeffects of nonnoxious pulsed currents (i.e. con-ventional TENS) are short lived, the delivery ofcurrents intermittently would be of limitedbenefit. MET devices sometimes use pen elec-trodes to administer microampere currents.Whether this produces different treatment out-comes to those seen when MET is administeredusing pad electrodes is not known.
Recently, high-voltage single-pulse TENS-pens(e.g. Pain®Gone) have appeared on the UKmarket for treatment of minor ailments andpainful conditions such as arthritis, back pain,headache and sports injuries.137 High-voltageTENS-pens generate a single pulse when twocrystals (piezoelectric elements) are forcedtogether by a plunger. Each pulse has a highvoltage (claimed to be 15,000 V) and short pulseduration, resulting in a 6 µA ‘shock’. Advocatesclaim that the high-voltage TENS-pens delivercurrents in the microampere range, yet theiroutput characteristics clearly differ from METand are probably more akin to HVPC.
High-voltage TENS-pens are claimed to gen-erate low-frequency stimulation (1–2 pps),although the frequency of pulse delivery will bedependent on the rate of button pressing by theuser, and is more likely to be ad hoc and asyn-chronous. Manufacturers recommend thatpatients should click the stimulating button 30–40times over acupuncture points or over the site ofpain as this will result in effects that are similarto TENS and acupuncture. Descriptions of thismechanism of action are superficial and incom-
plete. The ‘shock’ produces a sensation thatresembles a pinprick and can be mildly painful,depending on the body site stimulated. This sug-gests that cutaneous Aδ fibres are active. Aδafferents are believed to have a role in acupunc-ture analgesia and are known to trigger diffusenoxious inhibitory controls and releaseendorphins. Thus, high-voltage TENS-pens mayinitiate acupuncture-like mechanisms (onacupuncture points) or counter-irritation (onremote body sites) or both. It is not knownwhether the effects of high-voltage TENS-pensare dependent on the site of application.
Information on the clinical effectiveness ofhigh-voltage TENS-pens is lacking. One unpub-lished manuscript of an open uncontrolled clini-cal trial on 25 patients was identified.137 Eachpatient received 25 clicks of the high-voltageTENS-pen once a day for 3–5 days, either overor just above the most painful area. Good toexcellent pain relief that occurred immediatelyafter treatment and lasted for ‘some hours’ wasreported by 76% of patients. Similar results wereobtained in an uncontrolled trial on 36 patientswith chronic musculoskeletal pain.138 There wasno placebo control group in either study, so it ispossible that the pain relieving effects were pro-duced by the act of giving the treatment ratherthan the electrical currents. Clearly, randomizedcontrolled clinical trials are needed.
Transcutaneous cranial electrical stimulationTCES has been used for over 30 years in reha-bilitation medicine in the USA for insomnia,anxiety, depression, drug withdrawal and painrelief, and to reduce consumption of analgesicsand anaesthetics.139,140 Other names for TCESinclude cranial electrotherapy stimulation, tran-scranial electrotherapy, neuroelectric therapy,transcranial electrostimulation, and electrosleep.Electrode positions for TCES give the techniqueits identity and include: (1) attaching an electrodeto each earlobe; or (2) attaching electrodes toeach temple; or (3) attaching two positive elec-trodes in the retromastoid region and a negativeelectrode between the eyebrows (Limoge cur-rents). TCES treatment usually lasts for 30–60minutes and is repeated once or twice daily. It

30 MI Johnson
Pain Reviews 2001; 8: 00–00
uses MET-like currents with current amplitudesbelow 1 mA. Pulse repetition rates of 100 pps arepopular, although they can range from 0.5 pps to15,000 pps, depending on the device.
There does not seem to be a general consen-sus about the specific mechanism by which TCEScould alleviate pain. Advocates claim that theoutput characteristics of TCES devices enablecurrents to reach the brain directly from the siteof stimulation and that the currents affect brain function through direct action on neuronalactivity and/or endogenous pharmacology.Animal and human studies have implicatedendorphins, serotonin, cortisol and many otheragents as potential mediators of TCESeffects.140–143 Experimental work suggests thatTCES may potentiate the effects of opiates, neuroleptics and anxiolytics, allowing reductionsin drug medication during anaesthetic proce-dures.144–153
The findings of clinical trials on TCES areencouraging. A multicentre double-blind RCT on100 patients with tension headache reported thatTCES significantly reduced pain intensity whencompared with placebo.154 RCTs have also foundpositive effects of TCES on stress-related symp-toms in people with closed head injury155 and inreducing anxiety during routine dental proce-dures,156 which may indirectly reduce pain.Recently, Scherder et al.157 reported that TCESproduced no improvements in cognition and(affective) behaviour in 18 patients withAlzheimer’s disease when compared withplacebo. One meta-analysis on the clinical effec-tiveness of TCES versus sham was found.158
Eighteen RCTS were identified, out of which 14had sufficient data to pool. TCES was signifi-cantly more effective than sham treatment foranxiety (eight trials) and headache (two trials),but not significant for brain dysfunction (twotrials) and insomnia (two trials).
TCES using Limoge currents has attractedattention for use in anaesthesic proceduresbecause it has been claimed to reduce con-sumption of analgesics and anaesthet-ics.140,144,145,148,149,153 One group claims to haveadministered TCES using Limoge currents inover 30,000 major interventions and also to aiddrug withdrawal in 4000 opioid addicted patients,without any adverse events.140. Limoge currents
are high-frequency pulses (166 kHz; on-time = 1ms) interrupted with a repetitive low-frequencypulse (83 Hz; on-time = 4 ms) and delivered atlow intensities of approximately 2 mA..159 Eachpulse has a high-amplitude, short duration (1.7µs) positive phase and this is followed by a low-amplitude, long duration negative phase (6.3 µs).These pulses are delivered in trains (bursts).Some Limoge devices deliver currents at 167kHz, interrupted with an intermittent current of77 Hz, 83 Hz or 100 Hz. Two studies included insystematic reviews on TENS and labour painfound that Limoge currents reduced additionalanalgesic intervention in women experiencinglabour pain when compared with a shamdevice.54,55
Stimulators to overcometolerance to TENSReports have suggested that some patientsbecome tolerant to the pain-relieving effects ofcurrents delivered by a standard TENS device,which may result from nervous system habitua-tion to repetitive monotonous stimuli.160–162 In anattempt to overcome nervous system habituationand the resultant TENS tolerance, some devicesnow have output characteristics that fluctuatebetween preset limits during stimulation.
One common approach to TENS tolerance hasbeen to fluctuate pulse frequency (i.e. frequencymodulation) between upper and lower bound-aries in a similar manner to that described forIFT. Frequency modulation on TENS devices hasproved popular with patients and has been shownto be effective in relieving pain.163–165 However,it is not known whether frequency modulationproduces clinically meaningful reductions in theincidence of TENS tolerance. Another approachhas been to deliver pulses randomly (i.e. randomfrequency). Random frequency TENS has beenshown to elevate the experimental pain thresholdin healthy people when compared with placebo,but the magnitude of the change was no differ-ent to that seen with other modes of TENS.14 Noclinical studies were found that had assessed theeffects of random frequency TENS on TENStolerance.
An alternative approach to overcome nervoussystem habituation has been to deliver TENS

Efficacy of TENS and TENS-like devices in pain relief 31
Pain Reviews 2001; 8: 00–00
pulses randomly to different body sites. Codetronis a TENS-like device that delivers low-frequency(2–4 pps) square waves with a pulse duration of1 ms in a random order to one of six active elec-trode pads, which are usually positioned onacupuncture points. A small direct current ofopposite polarity follows each pulse in order toavoid polarization of tissue. Codetron has beenshown to increase the amplitude of corticalevoked potentials, indicative of a reduction innervous system habituation, in healthy volunteerswhen compared with pulses delivered using con-ventional TENS.166 Manufacturers also claim thatCodetron mimics the effects of electroacupunc-ture and AL-TENS. Patients are advised toadminister Codetron currents at the highestintensity that they can tolerate, providing they donot produce frank pain.167–169 It is plausible,therefore, that Codetron generates activity insmall diameter nerve fibres, resulting in extraseg-mental analgesia, in a manner similar to elec-troacupuncture.
Clinical trials of Codetron have produced con-flicting results. It has been shown to provide over30% pain relief in 107 of 137 patients with avariety of painful conditions.168 A double-blindrandomized sham controlled trial in 37 patientswith osteoarthritis of the knee found thatCodetron significantly improved pain when com-pared with sham (low-intensity TENS).69 It hasalso been reported that Codetron reduces mus-culoskeletal pain to the same extent as elec-troacupuncture when delivered to acupuncturepoints at 4 pps and 200 pps at intensities justbelow pain.170 Patients were given 20-minutetreatment sessions, once or twice a week for amaximum of 12 treatments, depending on need.Telephone interviews 4–8 months after the endof the study showed that patients in the Codetrongroup reported greater improvement when com-pared with those in the electroacupuncturegroup. In contrast, a RCT that examined theeffect of adding Codetron to an exercise pro-gramme in 58 low back pain patients found nodifferences between actual or placebo (nocurrent) stimulation for disability or painscores.166 Patients did improve with exercise.
Transcutaneous spinal electroanalgesia TSE, which has attracted much attention in theUK since its introduction in 1995, is indicated forminor aches and pains, migraine and stress.171
Preliminary data suggest that TSE may help toreduce general practitioner consultation ratesand that patients are satisfied with its effects.172,173
TSE delivers pulsed currents with a high fre-quency (600–10,00 pps), high voltage and shortpulse duration (1.5–4 µs) via two pad electrodespositioned either at T1 and T12 or straddlingC3–C5. The intention of TSE is to activateexcitable tissue in the spinal cord in order toreduce central sensitization by ‘resetting’ centralnervous system neuronal activity back to its pre-sensitized state.171 Physiological studies suggestthat conventional TENS may reduce central sen-sitization,174–177 although there have so far beenno experiments investigating the effects of TSE.If proved, TSE could be useful in the manage-ment of hyperalgesia and allodynia.
The output characteristics of TSE devices aredesigned to overcome skin resistance so that cur-rents bypass the skin and directly affect spinalcord circuitry. Patients do not usually experienceelectrical paraesthesia during TSE, so it is likelythat cutaneous nerves are not activated to anyappreciable extent and therefore the mechanismof action is different from conventional TENSmechanisms (i.e. activation of Aβ afferents). It isalso claimed that, because peripheral nerve inputconverges at the spinal cord, TSE effects will bewidespread over the body.171
Studies on the effects of TSE are sparse. Theinitial promise of TSE was based on observationsthat it reduced pain by 60% in over two-thirds ofa sample of 100 pain patients.171 A preliminaryRCT on eight patients suffering musculoskeletalpain found that TSE produced significantlygreater reductions in pain measures than TENS.Each patient received one 20-minute treatmentof TSE (10 kHz, 1.5 µs) and one 20-minute treat-ment of TENS (100 pps, 200 µs) in a randomized,double-blind cross-over fashion. Both TSE andTENS were applied over T1 and T12. Theauthors recognized that this was not the normalway of administering TENS and that the studylacked power owing to the small sample size.

32 MI Johnson
Pain Reviews 2001; 8: 00–00
However, these initial findings suggested that theoutput characteristics of TSE produced morepain relief than those from a standard TENSdevice when administered at spinal sites.
Subsequent reports have been less encourag-ing. Towell et al.178conducted a study using 60healthy people to investigate the effects of TSEon mood and mechanical pain tolerance. Whenapplied to the spinal cord for 30 minutes, itreduced tolerance to mechanical pain when com-pared with sham TSE, suggesting that TSE hadmade the experimental pain worse. However,TSE was found significantly to elevate mood. Asecond experiment by the same group appliedTSE to the shoulder joint and found no differ-ences in mood or pain tolerance to experimentalpain in healthy people when compared withsham. Studies reported in conference proceed-ings confirm the lack of analgesic effect.Hilberstadt et al.179 reported that TSE did notalter pain when administered in 10-day periodsto two patients with low back pain. A series ofdouble-blind placebo controlled trials conductedby Heffernan and Rowbotham180 found that TSEdid not reduce pain or the need for additionalanalgesic interventions when compared withsham TSE in acute and chronic pain settings. Atleast one other RCT on the effects of TSE forpain after breast cancer treatment was found,although the current status of this trial isunknown.181
Action potential simulation It is claimed that APS provides pain relief,reduces inflammation and swelling, enhanceslocal blood circulation, increases mobility, regen-erates cell and bone growth, and generatesadenosine triphosphate (ATP).182–184. The term‘action potential simulation’ derives from claimsthat APS devices generate electrical currents thatare similar in shape to nerve action poten-tials.101,184 It is unclear whether APS currents aredesigned to trigger action potentials or whetherthey simulate changes in membrane potentialsresulting from neural activity.
APS delivers monophasic square waves withexponential decay and a DC offset that remainsat 5 V. APS uses a long pulse duration between800 µs and 6.6 ms, a pulse frequency fixed at ~150
pps and a pulse amplitude between 0 and 24.4mA into a 500 ohm load. It is claimed that APSis a unique type of MET, although most articleson APS do not make this explicit.101,113 In someexperiments APS was delivered using low-current amplitudes (e.g. between 0.70 mA and 1.7mA) with patients being unable to perceive cur-rents.182,185 However, it has also been delivered atdoses that appear to be ‘strong’ and producingelectrical paraesthesia.182,186 APS is administeredusing two electrodes attached close to the site ofpain and protocols used in some published trialsseem to focus on treatment times in multiples of8 min (e.g. 8 and 16 min) although the rationalefor this approach is vague.182,183
Descriptions of the hypothetical mechanism ofaction of APS are ambiguous, and general state-ments that APS leads to excitation of the centralnervous system and the release of neurohor-mones are common.184,187 It is claimed that theDC offset in the APS waveform increases pro-duction of ATP and also creates tissue polariza-tion, resulting in increased levels of oxygen andcatabolism and leading to the removal of wastesubstances of tissue damage.101,113,184 It is inter-esting that tissue polarization is seen as anadverse effect for Codetron but is considered tobe of benefit for APS.
The majority of experimental work on theeffects of APS originates in South Africa, wherethe device was originally designed. A double-blind placebo controlled study found that APSincreased plasma levels of L-enkephalin andmelatonin and reduced Beta-endorphin whencompared with sham APS (no current) inpatients suffering chronic low back pain.187 Nochanges in plasma serotonin or cortisol levelswere found and the authors speculated thatdecreasing plasma beta-endorphin would help toreduce inflammation, although this could not beproved within their experiment because they didnot record changes in inflammation directly.Experimental evidence on the effect of TENS onplasma opioids is conflicting.188–190 An open trialusing 285 patients with a variety of chronic painconditions found that APS improved pain andmobility, although the study lacked a controlgroup.183
Odendaal and Joubert185 examined the effectsof APS in a placebo controlled trial on 76

Efficacy of TENS and TENS-like devices in pain relief 33
Pain Reviews 2001; 8: 00–00
patients with chronic low back pain and claimedthat APS ‘may be an effective treatment’. Thedata suggested that there were no differencesbetween APS and sham APS groups, althoughthe authors argued that the trial population wastoo small to conduct a between-group analysis.Berger and Matzner182 examined the effects ofAPS, TENS and placebo on mobility and swellingin 99 patients suffering from osteoarthritis,reporting that APS, TENS and placebo improvedpain. However, no effects were found betweentreatment groups, suggesting that the act ofgiving APS, rather than the electrical currentsdelivered by APS, produced the reduction inpain. The authors argued that APS was a viabletreatment option because it was unacceptable toadminister placebos in clinical practice. A moreappropriate interpretation of these findingswould be that APS, TENS and placebo areequally ineffective in the treatment of patientswith osteoarthritis. Double-blind studies on theeffects of APS, TENS and IFT on skin tempera-ture and mechanical pain threshold in healthypeople have also failed to find any significant dif-ferences between groups.85,191
H-wave therapy Manufacturers claim that HWT is useful in thetreatment of soft tissue injuries by promotinghealing, reducing inflammation and oedema, andrelieving pain. It has been used to treat neuro-pathic pain associated with diabetes192 and fordental anaesthesia.193 It seems that HWT wasdeveloped to reproduce the H-reflex (Hoffmanreflex), hence the name, although a suitableexplanation of the relationship between theHoffman reflex, HWT and analgesia could not befound. Manufacturers state that HWT currentspass through the skin without causing discomfortand that the output characteristics mimic thosefound in the body, although how this relates tophysiological mechanisms is not clear.
HWT is administered by using two electrodesat the site of pain, over acupuncture points orover muscle bellies surrounding tissue. It deliversa biphasic exponentially decaying wave of longpulse duration (16 ms) with pulse frequencieslimited to either 2 pps or 60 pps. Marketing mate-rial argues that frequencies above 60 pps are not
needed because HWT uses a bipolar waveformand 60 pps equates to 120 pps monophasic wave-forms, although this rationale appears to be weakbecause most standard TENS devices deliveringbiphasic waveforms offer frequencies beyond 200pps. Manufacturers also recommend that high-frequency HWT (i.e. 60 pps) generating a strongbut comfortable electrical paraesthesia within thesite of pain will provide the best pain relief. Themechanism of action of this effect is likely to besimilar to that found for conventional TENS.Low-frequency HWT (i.e. 2 pps) generatingmuscle twitches is recommended for inflamma-tion and oedema because it will produce musclepumping actions that will compress surroundingcirculatory vessels and improve blood flow andfluid drainage.
Clinical studies on HWT are few. It was shownsignificantly to reduce pain associated withperipheral neuropathy in 31 patients with type 2diabetes when compared with sham stimula-tion.194 HWT was administered to the lowerextremities for 30 min daily for four weeks usingpulses with a frequency of 2 pps ‘or greater’ anda duration of 4 ms. A follow-up study reportedthat HWT improved neuropathic pain associatedwith diabetes in 76% of respondents to a postalquestionnaire, although this study failed toinclude a control group.195 Workers havereported that HWT increases the mechanicalpain threshold196 and reduces McGill PainQuestionnaire scores for experimentally-inducedischaemic pain in healthy people when comparedwith sham HWT,197 although this latter findingwas not confirmed in a follow-up study.198 HWTwas also shown to increase the latency of thecompound action potential in the superficialradial nerve of 32 healthy volunteers, suggestingthat it reduces nerve conduction in peripheralnerves.199 HWT delivered at 2 pps, but not 60pps, has also been shown to increase skin bloodflow and skin temperature when compared withplacebo, providing indirect evidence that it maybe useful in facilitating tissue repair throughimproved circulation.200

34 MI Johnson
Pain Reviews 2001; 8: 00–00
DiscussionIt is hardly surprising that confusion exists aboutthe effectiveness of TENS and TENS-like deviceswith such an array of available stimulators andclaims of efficacious treatment protocols. Thetheoretical principles underpinning many of theTENS-like devices described in this review havetheir traditional roots in physiotherapy and reha-bilitation medicine. Until recently, treatmentwith many TENS-like devices could be obtainedonly under the supervision of a trained therapistin a clinic setting and working under the con-straints of the clinical rota. Advances in elec-tronic technology have reduced the cost, size anddangers of TENS-like devices and companiesnow market to a broader section of health careprofessionals. Increasing numbers of cheap hand-held devices have placed greater emphasis onself-treatment and the general public can pur-chase many TENS-like devices directly frommanufacturers. It is important that the interestsof the public, patients and health care profes-sionals are protected by scrutinizing claims madeby manufacturers about the relative effectivenessof the different devices.
The findings of systematic reviews and meta-analyses on the effectiveness of TENS for painrelief can be summarized as follows: TENS willrelieve pain associated with knee osteoarthritis65
and primary dysmenorrhoea,64 but will notrelieve postoperative pain42 or labour pain.50,51
Evidence is inconclusive for post-stroke shoulderpain58 and chronic pain in general.57 Evidence forthe efficacy of TENS in chronic low back pain hasproduced conflicting results.60–63 These clinicalbottom lines are particularly attractive to practi-tioners when making decisions about treatmentinterventions. However, the term TENS encom-passes a range of output characteristics, applica-tion procedures and dosing regimens, and this hasresulted in the use of inconsistent and sometimesinappropriate criteria to differentiate types ofTENS, such as conventional TENS and AL-TENS.
Furthermore, the evaluation models used insome reviews have been challenged. Trials in theacute pain setting use pain scores as the primaryoutcome measure, despite patients having accessto additional analgesic drugs, which will compro-mise pain scores because patients in both sham
and active TENS groups will titrate analgesicconsumption to achieve effective relief andminimal pain. Analgesic consumption would bethe most clinically meaningful outcome in thesetrials, although this has been dismissed as beingof secondary importance by some authors.51 Thecorrect way to administer TENS is also con-tentious and some systematic reviews includeRCTs that used protocols that underdose or useTENS-like devices that differ from standardTENS devices. When these issues are taken intoaccount they can change the outcome of system-atic reviews.48
An evaluation of the literature on the effec-tiveness of TENS-like devices revealed that:
• Available experimental evidence is limited inboth quality and quantity.
• Controlled studies for different TENS-likedevices, when available, suggest that somehave absolute effectiveness resulting from theelectrical currents rather than from the act ofadministering the currents. However, this is farfrom proven and seems to depend on the typeof nerve fibre activated, irrespective of theoutput characteristics of the device.
• Available evidence suggests that there areminimal differences in the magnitude and timecourse of pain relief achieved with differenttypes of device. Any potential differences inoutcome appear to be linked to the type offibre activated rather than the output charac-teristics of the device.
• The specificity of effect of different TENS-likedevices is questioned.
The relationship between output char-acteristics and physiological intentionElectrical currents form the active ingredient ofTENS in much the same way as a chemical struc-ture forms the active ingredient of a drug. In thisreview, output characteristics were the main cri-teria used to differentiate standard TENS devicesfrom nonstandard TENS-like devices. Most ofthe broad categories of TENS-like devices usenovel electrical currents to gain identity in themarket-place. Current waveform is commonlyused in marketing literature to differentiate onetype of device from another and all broad cate-gories of devices (i.e. standard TENS, IFT, MET,HVPC) gain identity in part from their current

Efficacy of TENS and TENS-like devices in pain relief 35
Pain Reviews 2001; 8: 00–00
waveform (Figure 8). A more appropriate way todifferentiate devices would be according to thephysiological intention of the currents. Whenused to generate pain relief, two main intentionsdominate the literature: first, the use of currentsto assist physiological processes associated withtissue healing; and secondly, the use of currentsto stimulate nerve fibres in order to activate painmodulatory circuits.
The main intention of microampere currents isto activate cellular processes that assist tissuehealing. Experimental evidence suggests thatMET can alter ATP and other biochemicalmarkers of tissue healing in vitro.100,110–112
However, there is doubt about whether this
translates to meaningful changes in the rate oftissue healing in animals and humans.119 Theabsence of MET-induced sensations such as elec-trical paraesthesia during stimulation suggeststhat MET currents have insufficient energy toactivate cutaneous afferents to any appreciableextent. It is assumed that putative pain relieffrom MET is an indirect result of acceleratedtissue healing.
The main intention of milliampere currents isto stimulate neural circuitry directly to modulatenociceptive transmission at peripheral, segmentaland extrasegmental levels. Experimental evi-dence supports the view that recruitment of dif-ferent populations of fibres leads to different
Standard TENS
IFT
HVPC
HWT
APS
Codetron
(a) (b) (c) (d)
Figure 8
Limoge currents
+0-
+0-
+0-
+0-
+0-
+0-
+0-
Figure 8 Waveform characteristics commonly used by standard TENS and TENS-like devices. StandardTENS devices often use pulse waveforms that are monophasic (a), symmetrical biphasic (b), asymmetricalbiphasic (c), or spike-like biphasic (d). IFT uses an amplitude-modulated interference wave resulting from thecollision of two out-of-phase sinusoidal-like currents. HVPC uses high-voltage double spike pulses. Limogecurrents are wave trains of positive pulses of high intensity, short duration, followed by negative pulses ofweak intensity long duration. Codetron uses biphasic square pulses. APS uses a monophasic square pulsewith exponential decay. HWT uses bipolar exponentially decaying pulsed currents. No diagramatic representa-tion of MET or TSE could be found in the literature. Whether these subtle differences in waveform character-istics translate into clinically different outcomes is not known

36 MI Johnson
Pain Reviews 2001; 8: 00–00
modulatory mechanisms becoming active.Activation of large diameter cutaneous afferents(i.e. Aβ) is related to segmental analgesia.Activation of small diameter muscle afferents(i.e. Group III) through a phasic muscle twitch isrelated to extrasegmental analgesia. Activationof small diameter cutaneous afferents (i.e. Aδ) isrelated to counter-irritant effects and blockade oftransmission in peripheral nociceptive nerves.Whether these various mechanisms result in clin-ically meaningful differences in outcome remainscontentious. Theoretical models based onstrength-duration curves for axonal excitationprovides information about the relationshipbetween output characteristics and fibre recruit-ment. However, the simplest way to recruit dif-ferent fibre types is to raise current amplitudeand/or alter electrode positions. This raises ques-tions about the influence of other output charac-teristics in determining the magnitude and profileof segmental analgesia. The literature lacks pub-lished systematic investigations into the analgesiceffects of different output characteristics (such aspulse frequency, pattern and duration) whencurrent amplitude is kept constant. It has beensuggested that patients choose pulse frequenciesand patterns for reasons of comfort rather thanimproved analgesia.
The physiological justification for incorporat-ing novel output characteristics in many TENS-like devices is weak. Explanations of therelationship between output characteristics andphysiological effect are often general anddescriptions of ‘closing pain gates’ or ‘ increasinglevels of circulating endorphins’ are prevalent inmanufacturers’ literature. It was often difficult toascertain whether a TENS-like device was beingadministered with a view to activating nervefibres selectively or to aid the healing process, orboth. If the TENS-like devices are ‘closing thepain gate’, then it may be cheaper to use a stan-dard TENS device. Clearly, manufacturers needto demonstrate that TENS-like devices produceeffects that are clinically different to, or greaterin magnitude than, those achieved using a stan-dard TENS device. At present, many differencesin output characteristics between TENS-likedevices appear to be purely cosmetic.
The diversity of ways in which electrical cur-rents can be administered confounds categoriza-
tion and the synthesis of available evidence.Electrode sites may be similar to those proposedfor conventional TENS (i.e. around the site ofpain for IFT and HWT) or completely different(i.e. on the head for TCES or spinal cord place-ment for TSE). Treatment regimens varied con-siderably and some seem to defy logic. Forexample, in one trial, APS was administered for16 minutes followed by a 3-minute rest and afurther 16 minutes.185 Intermittent stimulation ofbetween 20 and 60 minutes repeated a few timesa day tended to predominate in published advicefor many TENS-like devices, especially for non-potable devices that reside in clinics. It is possi-ble that such dosing regimens have developedbecause they fit into the clinical rota.73
Patients who use conventional TENS areencouraged to administer treatment to produce astrong, comfortable electrical paraesthesia when-ever they are in pain because this reflects activ-ity in Aβ afferents. Evidence from animals,normal people and patients shows that the effectsof conventional TENS are maximal when thedevice is switched on and are usually short livedonce it is switched off.15,17–19 Intermittent dosingregimens for conventional TENS are known tolead to inadequate treatment and this has beenrecognized as a design flaw in many TENStrials.56,57 When TENS-like devices are used togenerate a strong but comfortable electricalparaesthesia within the site of pain (e.g. HWT,IFT) a continuous dosing regimen should beused. The intermittent dosing regimens recom-mended for TENS-like devices need to be justi-fied by demonstrating, through well-designedexperimental trials, that post-stimulatory effectsactually occur.
The relationship betweenoutput characteristics andclinical effectivenessFrom a practical perspective, health care profes-sionals need experimental evidence on absoluteeffectiveness (e.g. against a placebo control) andrelative effectiveness (e.g. against other existingtreatments) to inform clinical decisions. With anever-increasing number of TENS and TENS-likedevices available on the market, evidence about

Efficacy of TENS and TENS-like devices in pain relief 37
Pain Reviews 2001; 8: 00–00
relative effectiveness is particularly important toinform device selection. In essence, health careprofessionals want to know whether changing theoutput characteristics of TENS devices altersclinical effects. Cost-effectiveness should also beconsidered and whether putative treatmenteffects can be achieved by using a standard TENSdevice rather than a more expensive TENS-likedevice. At present, there are few comparativestudies between standard TENS and TENS-likedevices or between different types of TENS-likedevices. Those that exist suggest that the outputcharacteristics of TENS-like devices, which maydiffer from each other markedly, do not influenceclinical outcome to the extent inferred by theiradvocates. Clinical trials that examine the rela-tive effectiveness of TENS-like devices with astandard TENS device are desperately needed toinform therapists about device selection.
In conclusion, despite the technologicallyimpressive appearance of many TENS-likedevices, a standard TENS device probablyremains the best type of stimulator for pain relief.Standard TENS devices are predominantly usedto stimulate different populations of nerve fibres,with the potential to produce different analgesicoutcomes. Clinical evidence does suggest that astandard TENS device, if used appropriately, canprovide pain relief. The findings of systematicreviews suggesting that TENS is not effective forpostoperative and labour pain have recently beenchallenged. Health care professionals often turnto TENS-like devices when patients fail torespond to treatment with a standard TENSdevice. It is important that the causes of nonre-sponse to standard TENS have been fullyexplored before the switch is made to a moreexpensive TENS-like device. Patients can beinappropriately labelled as nonrespondersbecause they have been given unrealistic expec-tations of treatment outcome or insufficient infor-mation about the principles and practice ofTENS use. Experimenting with the electricalcharacteristics, electrode positions or dosingregimen and/or trials of the different types ofTENS, such as AL-TENS, can often overcomeproblems associated with treatment resistantpatients.
The driving force for the design of manyTENS-like devices has been the ability to incor-
porate technologically impressive output charac-teristics based on hypothetical and speculativephysiological rationale. At present there is a lackof good quality physiological and clinical evi-dence to justify so many different types of device.In future it would be more relevant to defineTENS and TENS-like devices according to thephysiological intention of the currents. Physio-logical justification for the inclusion of specificoutput characteristics in stimulator design shouldalso be provided by manufacturers and supportedby experimental evidence that demonstrateseffects over and above those seen with a standardTENS device. Describing and defining TENSeffects in relation to nerve activity will improveconsistency in reporting and will enable system-atic reviews to include and exclude trials accord-ing to the physiological consequences of currentsrather than output characteristics.
References1 Walsh D. TENS. Clinical applications and related
theory. New York: Churchill Livingstone, 1997.2 Johnson M. Transcutaneous electrical nerve
stimulation (TENS). In: Kitchen S ed.Electrotherapy: evidence-based practice. Edinburgh:Churchill Livingstone, 2001: 259–86.
3 Chabal C, Fishbain DA, Weaver M, Heine LW.Long-term transcutaneous electrical nervestimulation (TENS) use: impact on medicationutilization and physical therapy costs. Clin J Pain1998; 14: 66–73.
4 Bandolier. Transcutaneous electrical nervestimulation (TENS) in postoperative pain.Bandolier 1999; (July). Available from: URL:http://www.jr2.ox.ac.uk/bandolier/booth/painpag/Acutrev/Other/AP019.html [Accessed 16-Jan-03]
5 Bandolier. Transcutaneous electrical nervestimulation (TENS) in labour pain. Bandolier 1999;(July). Available from: URL:http://www.jr2.ox.ac.uk/bandolier/booth/painpag/Acutrev/labour/AP001.html [Accessed 16-Jan-03]
6 Bandolier. Transcutaneous electrical nervestimulation (TENS) in chronic pain. Bandolier 1999;(July). Available from: URL:http://www.jr2.ox.ac.uk/bandolier/booth/painpag/Chronrev/Other/CP074.html [Accessed 16-Jan-03]
7 Woolf C, Thompson J Segmental afferent fibre-induced analgesia: transcutaneous electrical nervestimulation (TENS) and vibration. In: Wall P,Melzack R eds. Textbook of pain. Edinburgh:Churchill Livingstone, 1994: 1191–208.
8 American Physical Therapy Association.Electrotherapeutic terminology in physical therapy:

38 MI Johnson
Pain Reviews 2001; 8: 00–00
Report by the Electrotherapy Standards Committeeof the Section on Clinical Electrophysiology of theAmerican Physical Therapy Association (APTA).Alexandria, VA: APTA, 1990.
9 Sjölund B, Eriksson M, Loeser J. Transcutaneousand implanted electric stimulation of peripheralnerves. In: Bonica J ed. The management of pain.Philadelphia, PA: Lea and Febiger, 1990: l852–61.
10 Johnson MI. A critical review of the analgesiceffects of TENS-like devices. Phys Ther Rev 2001;6: 153–73.
11 Demmink J. The effect of a biological conductingmedium on the pattern of modulation anddistribution in a two-circuit static interferential field[Abstract]. In: Abstracts of the Proceedings of the12th International Conference of the WorldConfederation for Physical Therapy; 1995;Washington DC; 583.
12 Demmink J. The degree of modulation ininterferential current stimulation as used inphysiotherapy. The effect of a biological conductingmedium on the pattern of modulation in a two-circuit static interferential field [Thesis]. Norway:University of Bergen; 1993.
13 Mannheimer J, Lampe G. Clinical transcutaneouselectrical nerve stimulation. Philadelphia, PA: FADavis, 1988.
14 Johnson MI, Ashton CH, Bousfield DR, ThompsonJW. Analgesic effects of different pulse patterns oftranscutaneous electrical nerve stimulation on cold-induced pain in normal subjects. J Psychosom Res1991; 35: 313–21.
15 Johnson MI, Ashton CH, Thompson JW. An in-depth study of long-term users of transcutaneouselectrical nerve stimulation (TENS). Implicationsfor clinical use of TENS. Pain 1991; 44: 221–29.
16 Johnson MI, Ashton CH, Thompson JW. Analgesiceffects of acupuncture-like TENS on cold pressorpain in normal subjects. Eur J Pain 1992; 13:101–108.
17 Garrison DW, Foreman RD. Decreased activity ofspontaneous and noxiously evoked dorsal horn cellsduring transcutaneous electrical nerve stimulation(TENS). Pain 1994; 58: 309–15.
18 Garrison DW, Foreman RD. Effects oftranscutaneous electrical nerve stimulation (TENS)on spontaneous and noxiously evoked dorsal horncell activity in cats with transected spinal cords.Neurosci Lett 1996; 216: 125–28.
19 Johnson MI, Tabasam G. A double blind placebocontrolled investigation into the analgesic effects ofinterferential currents (IFC) and transcutaneouselectrical nerve stimulation (TENS) on cold inducedpain in healthy subjects. Physiother Theory Pract1999; 15: 217–33.
20 Sjölund BH. Peripheral nerve stimulationsuppression of C-fiber-evoked flexion reflex in rats.Part 1: Parameters of continuous stimulation. J
Neurosurg 1985; 63: 612–16.21 Sjölund BH. Peripheral nerve stimulation
suppression of C-fiber-evoked flexion reflex in rats.Part 2: Parameters of low-rate train stimulation ofskin and muscle afferent nerves. J Neurosurg 1988;68: 279–83.
22 Johnson MI, Ashton CH, Bousfield DR, ThompsonJW. Analgesic effects of different frequencies oftranscutaneous electrical nerve stimulation on cold-induced pain in normal subjects. Pain 1989; 39:231–36.
23 Walsh D. TENS. Clinical applications and relatedtheory. New York: Churchill Livingstone, 1997:63–81.
24 Walsh D. TENS. Clinical applications and relatedtheory. New York: Churchill Livingstone, 1997:83–124.
25 Johnson MI, Ashton CH, Thompson JW. Theconsistency of pulse frequencies and pulse patternsof transcutaneous electrical nerve stimulation(TENS) used by chronic pain patients. Pain 1991;44: 231–34.
26 Johnson MI. The analgesic effects and clinical useof acupuncture-like TENS (AL-TENS). Phys TherRev 1998; 3: 73–93.
27 Andersson SA, Hansson G, Holmgren E, RenbergO. Evaluation of the pain suppressing effect ofdifferent frequencies of peripheral electricalstimulation in chronic pain conditions. Acta OrthoScand 1976; 47: 149–57.
28 Eriksson MB, Sjölund BH. Acupuncture-likeelectroanalgesia in TNS resistant chronic pain. In:Zotterman Y ed. Sensory functions of the skin.Oxford: Pergamon Press, 1976: 575–81.
29 Andersson SA, Ericson T, Holmgren E, Linquist G.Electroacupuncture. Effect of pain thresholdmeasured with electrical stimulation of teeth. BrainRes 1973; 63: 393–96.
30 Sjölund BH, Terenius L, Eriksson M. Increasedcerebrospinal fluid levels of endorphins afterelectro-acupuncture. Acta Physiol Scand 1977; 100:382–84.
31 Sjölund BH, Eriksson MB. The influence ofnaloxone on analgesia produced by peripheralconditioning stimulation. Brain Res 1979; 173:295–301.
32 Meyerson B. Electrostimulation procedures: effectspresumed rationale, and possible mechanisms. In:Bonica J, Lindblom U, Iggo A eds. Advances inpain research and therapy, vol. 5. New York: Raven,1983: 495–534.
33 Walsh DM. Transcutaneous electrical nervestimulation and acupuncture points. ComplementaryTher Med 1996; 4: 133–37.
34 Melzack R, Vetere P, Finch L. Transcutaneouselectrical nerve stimulation for low back pain. Acomparison of TENS and massage for pain andrange of motion. Phys Ther 1983; 63: 489–93.

Efficacy of TENS and TENS-like devices in pain relief 39
Pain Reviews 2001; 8: 00–00
35 Jeans M, Relief of chronic pain by brief, intensetranscutaneous electrical stimulation - a doubleblind study. In: Bonica J, Liebeskind J, Albe-Fessard D eds. Advances in pain research andtherapy, vol. 3. New York: Raven Press, 1979;601–606.
36 Levin M, Hui-Chan C. Conventional andacupuncture-like transcutaneous electrical nervestimulation excite similar afferent fibers. Arch PhysMed Rehabil 1993; 74: 54–60.
37 Ignelzi RJ, Nyquist JK. Direct effect of electricalstimulation on peripheral nerve evoked activity:implications in pain relief. J Neurosurg 1976; 45:159–65.
38 Ignelzi RJ, Nyquist JK. Excitability changes inperipheral nerve fibers after repetitive electricalstimulation. Implications in pain modulation. JNeurosurg 1979; 51: 824–33.
39 Chung JM, Fang ZR, Hori Y, Lee KH, Willis WD.Prolonged inhibition of primate spinothalamic tractcells by peripheral nerve stimulation. Pain 1984; 19:259–75.
40 Woolf CJ, Mitchell D, Barrett GD, Antinociceptiveeffect of peripheral segmental electrical stimulationin the rat. Pain 1980; 8: 237–52.
41 Carrol EN, Badura AS. Focal intense brieftranscutaneous electric nerve stimulation fortreatment of radicular and postthoracotomy pain.Arch Phys Med Rehabil 2001; 82: 262–64.
42 Carroll D, Tramer M, McQuay H, Nye B, MooreA. Randomization is important in studies with painoutcomes: systematic review of transcutaneouselectrical nerve stimulation in acute postoperativepain. Br J Anaesth 1996; 77: 798–803.
43 Hymes A, Raab D, Yonchiro E, Nelson G, PrintyA. Electrical surface stimulation for control of postoperative pain and prevention of ileus. Surg Forum1974; 65: 1517–20.
44 Schuster G, Infante M. Pain relief after low backsurgery: the efficacy of transcutaneous electricalnerve stimulation. Pain 1980; 8: 299–302.
45 Ali J, Yaffe C, Serrette C. The effect oftranscutaneous electric nerve stimulation onpostoperative pain and pulmonary function. Surgery1981; 89: 507–12.
46 Reeve J, Menon D, Corabian P. Transcutaneouselectrical nerve stimulation (TENS): a technologyassessment. Int J Technol Assess Health Care 1996;12: 299–324.
47 Benedetti F, Amanzio M, Casadio C et al. Controlof postoperative pain by transcutaneous electricalnerve stimulation after thoracic operations. AnnThorac Surg 1997; 63: 773–76.
48 Bjordal J, Johnson M, Ljunggren A.Transcutaneous electrical nerve stimulation (TENS)can reduce postoperative analgesic consumption. Ameta-analysis with assessment of optimal treatmentparameters for postoperative pain. Eur J Pain (in
press).49 Augustinsson L, Bohlin P, Bundsen P et al. Pain
relief during delivery by transcutaneous electricalnerve stimulation. Pain 1977; 4: 59–65.
50 Carroll D, Moore A, Tramer M, McQuay H.Transcutaneous electrical nerve stimulation doesnot relieve in labour pain: updated systematicreview. Contemp Rev Obstet Gynaecol 1997; 9:195–205.
51 Carroll D, Tramer M, McQuay H, Nye B, MooreA. Transcutaneous electrical nerve stimulation inlabour pain: a systematic review. Br J ObstetGynaecol 1997; 104: 169–75.
52 Johnson MI. Transcutaneous electrical nervestimulation (TENS) in the management of labourpain: the experience of over ten thousand women.Br J Midwifery 1997; 5: 400–405.
53 Harrison R, Woods T, Shore M, Mathews G,Unwin A. Pain relief in labour using transcutaneouselectrical nerve stimulation (TENS). ATENS/TENS placebo controlled study in two paritygroups. Br J Obstet Gynaecol 1986; 93: 739–46.
54 Champagne C, Papiernik E, Thierry JP, Noviant Y.[Transcutaneous cerebral electric stimulation byLimoge current during labor.] Ann Fr AnesthReanim 1984; 3: 405–13.
55 Wattrisse G, Leroy B, Dufossez F, Bui Huu Tai R.[Transcutaneous electric stimulation of the brain: acomparative study of the effects of its combinationwith peridural anesthesia using bupivacaine-fentanylduring obstetric analgesia.] Cah Anesthesiol 1993;41: 489–95.
56 McQuay H, Moore A. TENS in chronic pain. In:McQuay H, Moore A eds. An evidence-basedresource for pain relief. Oxford: Oxford UniversityPress, 1998: 207.
57 Carroll D, Moore RA, McQuay HJ, Fairman F,Tramer M, Leijon G. Transcutaneous electricalnerve stimulation (TENS) for chronic pain[Cochrane review]. In: The Cochrane Library, Issue4, 2001; Oxford: Update Software.
58 Price CI, Pandyan AD. Electrical stimulation forpreventing and treating post-stroke shoulder pain: asystematic Cochrane review. Clin Rehabil 2001; 15:5–19.
59 Price CI, Pandyan AD. Electrical stimulation forpreventing and treating post-stroke shoulder pain[Cochrane review]. In: The Cochrane Library, Issue4, 2001; Oxford: Update Software.
60 Milne S, Welch V, Brosseau L et al. Transcutaneouselectrical nerve stimulation (TENS) for chronic lowback pain [Cochrane Review]. In: The CochraneLibrary, Issue 4, 2001; Oxford: Update Software.
61 Brosseau L, Milne S, Robinson V et al. Efficacy ofthe transcutaneous electrical nerve stimulation forthe treatment of chronic low back pain: a meta-analysis. Spine 2002; 27: 596–603.
62 Gadsby JG, Flowerdew MW. Transcutaneous

40 MI Johnson
Pain Reviews 2001; 8: 00–00
electrical nerve stimulation and acupuncture-liketranscutaneous electrical nerve stimulation forchronic low back pain [Cochrane review]. In: TheCochrane Library, Issue 2, 2000; Oxford: UpdateSoftware.
63 Flowerdew M, Gadsby G, A review of thetreatment of chronic low back pain withacupuncture-like transcuatenous electrical nervestimulation and transcutaneous electrical nervestimulation. Comp Ther Med 1997; 5: 193-201.
64 Proctor ML, Smith CA, Farquhar CM, Stones RW,Transcutaneous electrical nerve stimulation andacupuncture for primary dysmenorrhoea (CochraneReview). In: The Cochrane Library, Issue 1, 2002;Oxford: Update Software.
65 Osiri M, Welch V, Brosseau L et al. Transcutaneouselectrical nerve stimulation for knee osteoarthritis.(Cochrane review). In: The Cochrane Library, Issue1, 2002; Oxford: Update Software.
66 Palmer ST, Martin DJ. Interferential current forpain control. In: Kitchen S ed. Electrotherapy:evidence based practice. Edinburgh: ChurchillLivingstone, 2001: 287–300.
67 Pope GD, Mockett SP, Wright JP. A survey ofelectrotherapeutic modalities: Ownership and use inthe NHS in England. Physiotherapy 1995; 81: 82–91.
68 Robertson VJ, Spurritt D. Electrophysical agents:implications of their availability and use inundergraduate clinical placements. Physiotherapy1998; 84: 335–44.
69 DeDomenico G. New dimensions in interferentialtherapy. A theoretical and clinical guide. Linfield:Reid Medical, 1987.
70 Savage B. Interferential therapy. London: Wolfe,1992.
71 Nikolova L. Treatment with interferential current.Edinburgh: Churchill Livingstone, 1987.
72 Martin D. Interferential for pain control. In:Kitchen S, Bazin S eds. Clayton’s Electrotherapy,tenth edition. London: Saunders, 1994: 306–15.
73 Johnson MI. The mystique of interferentialcurrents. Physiotherapy 1999; 85: 294–97.
74 Johnson MI, Tabasam G. A questionnaire surveyon the clinical use of interferential currents (IFC)by physiotherapists [Abstract]. In: Abstract of theProceedings of the Pain Society of Great BritainAnnual Conference; April 1998; Leicester; abstr 29.
75 Ganne J, Speculand B, Mayne L, Goss A.Inferential therapy to promote union of mandibularfractures. Aust N Z J Surg 1979; 49: 81–83.
76 Laycock J, Green R. Interferential therapy in thetreatment of incontinence. Physiotherapy 1988; 74:161–68.
77 Nelson B. Interferential therapy. Aust J Physiother1981; 27: 53–56.
78 Willie CD. Interferential therapy. Physiotherapy1969; 55: 503–505.
79 Kloth LC. Interference current. In: Nelson RM,
Currier DP eds. Clinical electrotherapy. EastNorwalk, CT: Appleton and Lange, 1991: 221–60.
80 Noble JG, Lowe AS, Walsh DM. Interferentialtherapy review: Part 1. Mechanism of analgesicaction and clinical use. Phys Ther Rev 2000; 5:239–45.
81 Tabasam G, Johnson MI. Electrotherapy for painrelief: does it work? A laboratory based study toexamine the analgesic effects of electrotherapy oncold-induced pain in healthy individuals. Clin EffectNurs 1999; 3: 14–24.
82 Johnson MI, Tabasam G. A single-blind placebo-controlled investigation into the analgesic effects ofinterferential currents on experimentally inducedischaemic pain in healthy subjects. Clin PhysiolFunct Imaging 2002; 22: 187–96.
83 Johnson MI, Tabasam G. A single-blindinvestigation into the hypoalgesic effects ofdifferent swing patterns of interference currents(IFC) on cold-induced pain in healthy volunteers.Arch Phys Med Rehabil (in press).
84 Johnson MI, Tabasam G. Differential analgesiceffects of amplitude modulated wave frequencies ofinterferential currents (IFC) on cold induced painin healthy subjects [Abstract]. In: Abstract of theProceedings of the IXth World Congress on Pain.1999 Aug 22–27; Vienna, Austria. Seattle: IASPPress, 1999: 453.
85 Noble JG. Interferential therapy: assessment ofhypoalgesic and neurophysiological effects [Thesis].Belfast: University of Ulster, 2000.
86 Taylor K, Newton RA, Personius WJ, Bush FM.Effects of interferential current stimulation fortreatment of subjects with recurrent jaw pain. PhysTher 1987; 67: 346–50.
87 Quirk A, Newman RJ, Newman KJ. An evaluationof interferential therapy, shortwave diathermy andexercise in the treatment of osteoarthrosis of theknee. Physiotherapy 1985; 71: 55–57.
88 Werners R, Pynsent PB, Bulstrode CJ. Randomizedtrial comparing interferential therapy withmotorized lumbar traction and massage in themanagement of low back pain in a primary caresetting. Spine 1999; 24: 1579–84.
89 Hurley DA, Minder PM, McDonough SM, WalshDM, Moore AP, Baxter DG. Interferential therapyelectrode placement technique in acute low backpain: a preliminary investigation. Arch Phys MedRehabil 2001; 82: 485–93.
90 Palmer ST, Martin DJ, Steedman WM, Ravey J,Alteration of interferential current andtranscutaneous electrical nerve stimulationfrequency: effects on nerve excitation. Arch PhysMed Rehabil 1999; 80: 1065–71.
91 Picker R, Micro electrical neuromuscularstimulation. Network-Electrix 1987; (March):S72–S74.
92 Picker R. Current trends: low volt pulsed microamp

Efficacy of TENS and TENS-like devices in pain relief 41
Pain Reviews 2001; 8: 00–00
stimulation parts 1 and 2. Clin Man Phys Ther 1988;9: 10–33.
93 Mercola JM, Kirsch DL. The basis for microcurrentelectrical therapy in conventional medical practice.J Adv Med 1995; 8(2). Available from: URL:http://www.harborside.com/naspenmed/page8.htm[Accessed 15-Jan-03]
94 Kirsch DL, Lerner FN. Electromedicine: The otherside of physiology. In: Weiner R ed. The Textbookof the America Academy of Pain Management,Innovations in pain management: a practical guidefor clinicians, vol. 4 update. Winter Park, FL: GRPress, 1995. Available from: URL:http://www.alternatives.com/raven/cpain/chap23-0.html [Accessed 15-Jan-03]
95 DuPont JS, Graham R, Tidwell JB. Trigger pointidentification and treatment with microcurrent.Cranio 1999; 17: 293–96.
96 Heffernan MS. Comparative effects of microcurrentstimulation on EEG spectrum and correlationdimension. Integrative Physiol Behav Sci 1996; 31:202–209.
97 Becker R, Selden G. The body electric. New York:Morrow, 1985.
98 Becker R, Murray D. Method for producing cellulardedifferentiation by means of very small electricalcurrents. Trans N Y Acad Sci 1967; 29: 606–15.
99 Watson T. Electrical stimulation for wound healing:a review of current knowledge. In: Kitchen S ed.Electrotherapy: evidence-based practice, eleventhedition. Edinburgh: Churchill Livingstone, 2002:313–34.
100 Cheng N, Hoof HV, Bockx E. The effects ofelectric current on ATP generation, proteinsynthesis, and membrane transport in rat skin. ClinOrthop Rel Res 1982; 171: 264–72.
101 Seegers JC, Engelbrecht CA, van Papendorp DH.Activation of signal-transduction mechanisms mayunderlie the therapeutic effects of an appliedelectric field. Med Hypotheses 2001; 57: 224–30.
102 Weber MD, Servedio FJ, Woodall WR. The effectsof three modalities on delayed onset musclesoreness. J Orthop Sports Phys Ther 1994; 20:236–42.
103 Lambert MI, Marcus P, Burgess T, Noakes TD.Electro-membrane microcurrent therapy reducessigns and symptoms of muscle damage. Med SciSports Exerc 2002; 34: 602–607.
104 Johnson MI, Penny P, Sajawal MA. Anexamination of the analgesic effects of microcurrentstimulation (MES) on cold-induced pain in healthysubjects. Physiother Theory Pract 1997; 13: 293–301.
105 Lerner F, Kirsch D. A double blind comparativestudy of micro-stimulation and placebo effect inshort term treatment of the chronic back painpatient. J Chiropract 1981; 15: 101–106.
106 Branco K, Naeser MA. Carpal tunnel syndrome:clinical outcome after low-level laser acupuncture,
microamps transcutaneous electrical nervestimulation, and other alternative therapies – anopen protocol study. J Altern Complement Med1999; 5: 5–26.
107 Annal N, Soundappan S, Palaniappan K,Chandrasekar S. Introduction of transcutaneous,low voltage, non-pulsatile direct current (DC)therapy for migrane and chronic headaches. Acomparison with transcutaneous electrical nervestimulation (TENS). Headache Q 1992; 3: 434–37.
108 Bertolucci LE, Grey T. Clinical comparative studyof microcurrent electrical stimulation to mid-laserand placebo treatment in degenerative joint diseaseof the temporomandibular joint. Cranio 1995; 13:116–20.
109 Wolcott L, Wheeler P, Hardwicke H, Rowley B.Accelerated healing of skin ulcers byelectrotherapy. South Med J 1969; 62: 795–801.
110 Nessler J, Mass D. Direct-current electricalstimulation of tendon healing in vitro. Clin OrthopRel Res 1987; 217: 303–12.
111 Oweye I, Spielholz N, Fetto J, Nelson J. Low-intensity pulsed galvanic current and the healing oftenotomized rat achilles tendons: preliminary reportusing load-to-breaking measurements. Arch PhysMed Rehabil 1987; 68: 415–18.
112 Richez J, Chamay A, Bieler L. Bone changes dueto pulses of direct electric microcurrent. VirchowsArch A Pathol Anat 1972; 357: 11–18.
113 Seegers JC, Lottering ML, Joubert AM et al. Apulsed DC electric field affects P2-purinergicreceptor functions by altering the ATP levels in invitro and in vivo systems. Med Hypotheses 2002; 58:171–76.
114 Rowley BA. Electrical current effects on E. coligrowth rates. Proc Soc Exp Biol Med 1972; 139:929–34.
115 Rowley BA, McKenna JM, Chase GR, Wolcott LE.The influence of electrical current on an infectingmicroorganism in wounds. Ann N Y Acad Sci 1974;238: 543–51.
116 Rowley BA, McKenna JM, Wolcott LE.Proceedings: The use of low level electrical currentfor enhancement of tissue healing. Biomed SciInstrum 1974; 10: 111–14.
117 Leffmann D, Arnall D, Holmgren P, Cornwall M.Effect of microamperage stimulation on the rate ofwound healing in rats. A histological study. PhysTher 1994; 74: 195–200.
118 Byl NN, McKenzie AL, West JM et al. Pulsedmicroamperage stimulation: a controlled study ofhealing of surgically induced wounds in Yucatanpigs. Phys Ther 1994; 74: 201–13.
119 Rothstein J. Microamperage: a lesson to be learned[editors note]. Phys Ther 1994; 74: 194.
120 Assimacopoulos D. Low intensity negative electriccurrent in the treatment of ulcers of the leg due tochronic venous insufficiency. Preliminary report of

42 MI Johnson
Pain Reviews 2001; 8: 00–00
three cases. Am J Surg 1968; 115: 683–87.121 Gault W, Gatens P. Use of low intensity direct
current in management of ischemic skin ulcers.Phys Ther 1976; 56: 265–69.
122 Sinitsyn L, Razvozva E. [Effects of electricalmicrocurrents on regeneration processes in skinwounds.] Ortop Travmatol Protez 1986; Feb (2):25–28 (Rus).
123 Carley P, Wainapel S. Electrotherapy foracceleration of wound healing: low intensity directcurrent. Arch Phys Med Rehabil 1985; 66: 443–46.
124 Mulder G. Treatment of open-skin wounds withelectric stimulation. Arch Phys Med Rehabil 1991;72: 375–77.
125 Feedar JA, Kloth LC, Gentzkow GD. Chronicdermal ulcer healing enhanced with monophasicpulsed electrical stimulation. Phys Ther 1991; 71:639–49.
126 Gardner SE, Frantz RA, Schmidt FL. Effect ofelectrical stimulation on chronic wound healing: ameta-analysis. Wound Repair Regen 1999; 7:495–503.
127 Low J, Reed A. Electrical stimulation of nerve andmuscle. In: Low J, Reed A eds. Electrotherapyexplained: principles and practice. Oxford:Butterworth-Heinemann, 1994: 39–116.
128 Bjordal JM. Electrical currents. In: Bjordal JM,Johnson MI, Couppe C eds. Clinical electrotherapy.Your guide to optimal treatment. Kristiansand:HoyskoleForlaget Norwegian Academic Press, 2001:102–16.
129 Johannsen F, Gam A, Hauschild B, Mathiesen B,Jensen L. Rebox: an adjunct in physical medicine?Arch Phys Med Rehabil 1993; 74: 438–40.
130 Hatten E, Hervik J, Kalheim T, Sundvor T. Paintreatment with Rebox. Fysioterapeuten 1990; 11:8–13.
131 Nussbaum EL, Gabison S. Rebox effect onexercise-induced acute inflammation in humanmuscle. Arch Phys Med Rehabil 1998; 79: 1258–63.
132 Khan J. Electrical stimulation. In: Khan J ed.Principles and practice of electrotherapy. New York:Churchill Livingstone, 1987: 95–125.
133 Kloth LC, Feedar JA. Acceleration of woundhealing with high voltage, monophasic, pulsedcurrent. Phys Ther 1988; 68: 503–508.
134 Griffin JW, Tooms RE, Mendius RA, Clifft JK,Vander Zwaag R, el-Zeky F. Efficacy of highvoltage pulsed current for healing of pressure ulcersin patients with spinal cord injury. Phys Ther 1991;71: 433–42.
135 Jette D. Effect of different forms of transcutaneouselectrical nerve stimulation on experimental pain.Phys Ther 1986; 66: 187–93.
136 Morris L, Newton RA. Use of high voltage pulsedgalvanic stimulation for patients with levator anisyndrome. Phys Ther 1987; 67: 1522–25.
137 Asbjorn O. Treatment of tennis elbow with
transcutaneous nerve stimulation (TNS). Availablefrom: URL: http://www.paingone.com/ 2000[Accessed 01-Jul-02]
138 Ivanova-Stoilova T, Howells D. The usefulness ofPainGone pain killing pen for self-treatment ofchronic musculoskeletal pain - a pilot study[Abstract]. In: The Pain Society of Great BritainAnnual Scientific Meeting Abstracts; 2002 Apr 9–12;Bournemouth, UK; abstr. 104.
139 Kirsch DL, Smith RB. The use of cranialelectrotherapy stimulation in the management ofchronic pain: a review. NeuroRehabilitation 2000;14: 85–94.
140 Limoge A, Robert C, Stanley TH. Transcutaneouscranial electrical stimulation (TCES): a review 1998.Neurosci Biobehav Rev 1999; 23: 529–38.
141 Southworth S. A study of the effects of cranialelectrical stimulation on attention andconcentration. Integrative Physiol Behav Sci 1999;34: 43–53.
142 Taylor D, Lee C, Katims J. Effects of cranialtranscutaneous electrical nerve stimulation innormal subjects at rest and during psychologicalstress. Acupunct Electrother Res 1991; 16: 65–74.
143 Schroeder MJ, Barr RE. Quantitative analysis ofthe electroencephalogram during cranialelectrotherapy stimulation. Clin Neurophysiol 2001;112: 2075–83.
144 Stinus L, Auriacombe M, Tignol J, Limoge A, LeMoal M. Transcranial electrical stimulation withhigh frequency intermittent current (Limoge’s)potentiates opiate-induced analgesia: blind studies.Pain 1990; 42: 351–63.
145 Robert C, Limoge A, Stinus L. Transcranialelectrical stimulation (Limoge’s currents)potentiates the inhibition of righting reflex inducedby droperidol in rats. Brain Res 1999; 822: 132–41.
146 Alantar A, Azerad J, Limoge A, Robert C, RokytaR, Pollin B. Potentiation of fentanyl suppression ofthe jaw-opening reflex by transcranial electricalstimulation. Brain Res 1997; 763: 14–20.
147 Malin DH, Lake JR, Hamilton RF, Skolnick MH.Augmented analgesic effects of enkephalinaseinhibitors combined with transcranialelectrostimulation. Life Sci 1989; 44: 1371–76.
148 Auriacombe M, Tignol J, Le Moal M, Stinus L.Transcutaneous electrical stimulation with Limogecurrent potentiates morphine analgesia andattenuates opiate abstinence syndrome. BiolPsychiatry 1990; 28: 650–56.
149 Mignon A, Laudenbach V, Guischard F, Limoge A,Desmonts JM, Mantz J. Transcutaneous cranialelectrical stimulation (Limoge’s currents) decreasesearly buprenorphine analgesic requirements afterabdominal surgery. Anesth Analg 1996; 83: 771–75.
150 Stanley TH, Cazalaa JA, Atinault A, Coeytaux R,Limoge A. Louville Y, Transcutaneous cranialelectrical stimulation decreases narcotic
Efficacy of TENS and TENS-like devices in pain relief 43
Pain Reviews 2001; 8: 00–00
requirements during neurolept anesthesia andoperation in man. Anesth Analg 1982; 61: 863–66.
151 Stanley TH, Cazalaa JA, Limoge A, Louville Y.Transcutaneous cranial electrical stimulationincreases the potency of nitrous oxide in humans.Anesthesiology 1982; 57: 293–97.
152 Svetlov V, Alisov A, Kozlov S, Tsibuliak V.[Central electroanalgesia as a component ofcombined anesthesia in reconstructivemicrosurgery]. Anesteziol Reanimatol 1994; 4: 46–50(Rus).
153 Mantz J, Azerad J, Limoge A, Desmonts JM.Transcranial electrical stimulation with Limoge’scurrents decreases halothane requirements in rats.Evidence for the involvement of endogenousopioids. Anesthesiology 1992; 76: 253–60.
154 Solomon S, Elkind A, Freitag F et al. Safety andeffectiveness of cranial electrotherapy in thetreatment of tension headache. Headache 1989; 29:445–50.
155 Smith RB, Tiberi A, Marshall J. The use of cranialelectrotherapy stimulation in the treatment ofclosed-head-injured patients. Brain Inj 1994; 8:357–61.
156 Winick RL. Cranial electrotherapy stimulation(CES): a safe and effective low cost means ofanxiety control in a dental practice. Gen Dent 1999;47: 50–55.
157 Scherder EJ, Deijen JB, Vreeswijk SH, SergeantJA, Swaab DF. Cranial electrostimulation (CES) inpatients with probable Alzheimer’s disease. BehavBrain Res 2002; 128: 215–17.
158 Klawansky S, Yeung A, Berkey C, Shah N, Phan H,Chalmers TC. Meta-analysis of randomizedcontrolled trials of cranial electrostimulation.Efficacy in treating selected psychological andphysiological conditions. J Nerv Ment Dis 1995; 183:478–84.
159 Limoge A. [Electricity in pain management.] PresseMedicale 1999; 28: 2197–203 [Fre].
160 Bates JA, Nathan PW. Transcutaneous electricalnerve stimulation for chronic pain. Anaesthesia1980; 35: 817–22.
161 Loeser J, Black R, Christman A. Relief of pain bytranscutaneous electrical nerve stimulation. JNeurosurg 1975; 42: 308–14.
162 Eriksson MB, Sjölund BH, Nielzen S. Long termresults of peripheral conditioning stimulation as ananalgesic measure in chronic pain. Pain 1979; 6:335–47.
163 Tulgar M, McGlone F, Bowsher D, Miles JB.Comparative effectiveness of different stimulationmodes in relieving pain. Part II. A double-blindcontrolled long-term clinical trial. Pain 1991; 47:157–62.
164 Tulgar M, McGlone F, Bowsher D, Miles JB.Comparative effectiveness of different stimulationmodes in relieving pain. Part I. A pilot study. Pain
1991; 47: 151–55.165 Ekstrom U, Sjölund B. Is modulation the way to
increase the efficacy of conventional TENS? Anexperimental study. In: Dubner R, Gebhart G,Bond MR eds. Proceedings of the Vth WorldCongress on Pain (Pain research and clinicalmanagement, vol. 3); 1987 Aug 2–7; Hamburg.Amsterdam: Elsevier, 1988: 583–89.
166 Pomeranz B, Niznick G. Codetron, a newelectrotherapy device overcomes the habituationproblems of conventional TENS devices. Am JElectromed 1987; (first quarter): 22–26.
167 Herman E, Williams R, Stratford P, Fargas-BabjakA, Trott M. A randomized controlled trial oftranscutaneous electrical nerve stimulation(CODETRON) to determine its benefits in arehabilitation program for acute occupational lowback pain. Spine 1994; 19: 561–68.
168 Fargas-Babjak A, Rooney P, Gerecz E.Randomized trial of Codetron for pain control inosteoarthritis of the hip/knee. Clin J Pain 1989; 5:137–41.
169 Fargas Babjak AM, Pomeranz B, Rooney PJ.Acupuncture-like stimulation with codetron forrehabilitation of patients with chronic painsyndrome and osteoarthritis. Acupunct ElectrotherRes 1992; 17: 95–105.
170 Cheng R, Pomeranz B. Electrotherapy of chronicmusculoskeletal pain; comparison ofelectroacupuncture and acupuncture-like TENS.Clin J Pain 1986; 2: 143–49.
171 Macdonald ARJ, Coates TW. The discovery oftranscutaneous spinal electroanalgesia and its reliefof chronic pain. Physiotherapy 1995; 81: 653–60.
172 Royle J. Transcutaneous spinal electroanalgesia(TSE) and its efficacy on GP consultation rates[Abstract]. In: The Pain Society of Great BritainAnnual Scientific Meeting Abstracts; Bournemouth,UK; 2002 Apr 9–12; abstr. 121.
173 Royle J. Transcutaneous spinal electroanalgesia(TSE) and its efficacy in the patient community: aqualitative assessment [Abstract]. In: The PainSociety of Great Britain Annual Scientific MeetingAbstracts; Bournemouth UK; 2002 Apr 9–12: abstr.122.
174 Leem J, Park E, Paik K. Electrophysiologicalevidence for the antinociceptive effect oftranscutaneous electrical stimulation onmechanically evoked responsiveness of dorsal hornneurons in neuropathic rats. Neurosci Lett 1995;192: 197–200.
175 Gopalkrishnan P, Sluka KA. Effect of varyingfrequency, intensity, and pulse duration oftranscutaneous electrical nerve stimulation onprimary hyperalgesia in inflamed rats. Arch PhysMed Rehabil 2000; 81: 984–90.
176 Sluka KA, Bailey K, Bogush J, Olson R, RickettsA. Treatment with either high or low frequency

44 MI Johnson
Pain Reviews 2001; 8: 00–00
TENS reduces the secondary hyperalgesia observedafter injection of kaolin and carrageenan into theknee joint. Pain 1998; 77: 97–102.
177 Sluka KA, Judge MA, McColley MM, Reveiz PM.Low frequency TENS is less effective than highfrequency TENS at reducing inflammation-inducedhyperalgesia in morphine-tolerant rats. Eur J Pain2000; 4: 185–93.
178 Towell A, Williams D, Boyd S. High frequencynon-invasive stimulation over the spine: effects onmood and mechanical pain tolerance in normalsubjects. Behav Neurol 1997; 10: 61–65.
179 Hilberstadt D, Barlas P, Foster N. The effect oftranscutaneous spinal electroanalgesia upon chronicpain: a single case study. Physiotherapy 2000; 86:150–51.
180 Heffernan A, Rowbotham D. Transcutaneous spinalelectroanalgesia: its effects in acute and chronicpain patients and healthy volunteers [Abstract]. In:The Pain Society of Great Britain Annual ScientificMeeting Abstracts; Bournemouth, UK; 2002 Apr9–12: abstr. 53.
181 Robb K. Pain after breast cancer treatment: arandomised, placebo controlled crossover trial tocompare two different stimulation analgesictechniques. In: The Pain Society of Great BritainAnnual Scientific Meeting Abstracts; Leicester, UK;1998 Apr: abstr. 45.
182 Berger P, Matzner L. Study on 99 patients withosteoarthritis (OA) of the knee to investigate theeffectiveness of low frequency electrical currents onmobility and pain: action potential simulationtherapy (APS) current compared withtranscutaneous electrical nerve stimulation (TENS)and placebo. South Afr J Anaesthesiol Analg 1999;5: 1–11.
183 Papendorp V, Krugere M, Maritz C, Dippenaar N.Action potential simulation therapy: self assessmentby 285 patients with chronic pain. Geneeskunde TheMedical Journal 2000; (Jan/Feb): 18–24.
184 Sandham J. Action potential simulation therapy.Eng Technol 2000; (July): 45–48.
185 Odendaal C, Joubert G. APS therapy – a new wayof treating chronic headache – a pilot study. SouthAfr J Anaesthesiol Analg 1999; 5: 1–3.
186 Noble JG. Interferential therapy: assessment ofhypoalgesic and neurophysiological effects. [Thesis].Belfast: University of Ulster, 2000: 166–87.
187 Wet ED, Oosthuizen J, Odendaal C, Shipton E.Neurochemical mechanisms that may underlie theclinical efficacy of ‘action potential simulation’(APSim) therapy in chronic pain management.South Afr J Anaesthesiol Analg 1999; 5: 1–5.
188 Facchinetti F, Sandrini G, Petraglia F, Alfonsi E,Nappi G, Genazzani AR. Concomitant increase in
nociceptive flexion reflex threshold and plasmaopioids following transcutaneous nerve stimulation.Pain 1984; 19: 295–303.
189 Facchinetti F, Sforza G, Amidei M et al. Centraland peripheral beta-endorphin response totranscutaneous electrical nerve stimulation. NIDARes Monogr 1986; 75: 555–58.
190 Johnson MI, Ashton CH, Thompson JW, WeddellA, Wright Honari S. The effect of transcutaneouselectrical nerve stimulation (TENS) andacupuncture on concentrations of beta endorphin,met enkephalin and 5 hydroxytryptamine in theperipheral circulation. Eur J Pain 1992; 13: 44–51.
191 Alves-Guerreiro J, Noble JG, Lowe AS, WalshDM. The effect of three electrotherapeuticmodalities upon peripheral nerve conduction andmechanical pain threshold. Clin Physiol 2001; 21:704–11.
192 Alvaro M, Kumar D, Julka IS. Transcutaneouselectrostimulation: emerging treatment for diabeticneuropathic pain. Diabetes Technol Ther 1999; 1:77–80.
193 Meizels P. Electronic anesthesia. H-wave and TMJtreatment. J California Dent Assoc 1987; 15: 42–44.
194 Kumar D, Marshall HJ. Diabetic peripheralneuropathy: amelioration of pain withtranscutaneous electrostimulation. Diabetes Care1997; 20: 1702–705.
195 Julka IS, Alvaro M, Kumar D. Beneficial effects ofelectrical stimulation on neuropathic symptoms indiabetes patients. J Foot Ankle Surg 1998; 37:191–94.
196 McDowell BC, McCormack K, Walsh DM, BaxterDG, Allen JM. Comparative analgesic effects of H-wave therapy and transcutaneous electrical nervestimulation on pain threshold in humans. Arch PhysMed Rehabil 1999; 80: 1001–1004.
197 Walsh DM, Baxter D, Allen JM, Bell AJ, MokhtarB. An assessment of the analgesic effects of H-wavetherapy upon experimentally-induced ischaemicpain [Abstract]. Ir J Med Sci 1992; 161: 472.
198 McDowell BC, Lowe AS, Walsh DM, Baxter GD,Allen JM. The lack of hypoalgesic efficacy of H-wave therapy on experimental ischaemic pain. Pain1995; 61: 27–32.
199 McDowell BC, Lowe AS, Walsh DM, Baxter GD,Allen JM. The effect of H-wave therapy uponconduction in the human superficial radial nerve invivo. Exp Physiol 1996; 81: 821–32.
200 McDowell BC, McElduff C, Lowe AS, Walsh DM,Baxter GD. The effect of high- and low-frequencyH-wave therapy upon skin blood perfusion:evidence of frequency-specific effects. Clin Physiol1999; 19: 450–57.

Copyright © 2022 FDOKUMEN




















