HAEMOSTATIC ACTIVATION AFTER SURGERY AND TRAUMA
36
HAEMOSTATIC ACTIVATION AFTER SURGERY AND TRAUMA Relationship to clinicopathological findings Jens V. Sørensen
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of HAEMOSTATIC ACTIVATION AFTER SURGERY AND TRAUMA

HAEMOSTATIC ACTIVATIONAFTER SURGERY AND TRAUMARelationship to clinicopathological findings
Jens V. Sørensen

Denne afhandling er i forbindelse med nedenstående publicere de afhandlinger af Det Sundhedsviden-skabelige Fakultet ved Aarhus Universitet antaget til offentlig at forsvares for den medicinske doktorgrad.
Aarhus Universitet, den 20. november 1995.
Arvid B. Maunsbachdekan
Forsvaret finder sted fredag den 26. april 1996,kl. 13.00 præcis i auditorium 424, Anatomisk Institut, Aarhus Universitet.

1
HAEMOSTATIC ACTIVATIONAFTER SURGERY AND TRAUMA
Relationship to clinicopathological findings
Jens V. Sørensen

This thesis is based on the following papers, which will be referred to in the text by their Roman numerals:
I. Sørensen JV, Borris LC, Lassen MR, Christi-ansen HM, Schøtt P, Olsen AD. Levels of thrombin-antithrombin III complex and factor VIII activity in relation to postoperative deep vein thrombosis and influence of proph ylaxis with a low mole cular weight hepa rin. Blood Coagul Fibrinol 1: 389-392, 1990.
II. Sørensen JV, Lassen MR, Borris LC, Rahr HB, Jensen HP, Hoppen steadt D, Walenga J, Fareed J. Reduction of plasma levels of proth rom bin fragment 1 and 2 during thrombo prophylaxis with a low molecular weight heparin. Blood Coagul Fibri nol 3: 55-59, 1992.
III. Sørensen JV, Rahr HB, Jensen HP, Borris LC, Lassen MR, Ejstrud P. Markers of coagulation and fibrino lysis after fractures of the lower extremities. Thromb Res 65: 479-486, 1992.
IV. Sørensen JV, Jensen HP, Rahr HB, Borris LC, Lassen MR, Knudsen F. F1+2 and FpA in urine from patients with multiple trauma and healthy individuals. A pilot study. Throm b Res 67: 429-434, 1992.
V. Sørensen JV, Jensen HP, Rahr HB, Borris LC, Lassen MR, Fedders O, Haase JP, Knudsen F. Fibrinogen and fibrin deriva tives in trauma tized patients: relation to injury severity and post-traumatic pulmonary dys function. Haemos tasis 23: 91-97, 1993.
VI. Sørensen JV, Jensen HP, Rahr HB, Borris LC, Lassen MR, Fedders O, Haase JP, Knudsen F. Haemostatic activation in patients with head injury with and without simultaneous multiple trauma. Scand J Clin Lab Invest 53: 659-665, 1993.
VII. Sørensen JV. Levels of fibrinolytic activators and inhibitors in plasma after severe trauma. Blood Coagul Fibrinol 5: 43-49, 1994.
2

PrefaceThe work on which this thesis is based was condu-cted in the period from 1989 to 1994. It was perfor-med while working with the Venous Thrombosis Group at the Depart ment of Orthopae dics at Aalborg Hospital.I am thankful to dr. Lars C. Borris and dr. Michael R. Lassen for providing excellent working conditions in the Venous Thrombosis Group and a never failing interest for this work. I am also most thankful to dr. Hans B. Rahr for being an inspired and enthusiatic co-worker, and for many good discussions and constructive criticism. I wish to thank dr. Hans Peter Jensen for including many of the patients in the studies. I am deeply thankful to laboratory technician Dorthe Refeldt Lund for her never ending enthusi-asm and her meticulous work in the laboratory. In addition I wish to express my grati tude towards Hanne M. Christiansen, Agnethe D. Olsen, Peter Schøtt, Debra A. Hoppen steadt, Jeanine M. Walenga, Jawed Fareed, Per Ejstrud, Ole Fedders, Jens P. Haase, Flemming Knudsen, the Depart ment of Ort-hopaedics, the Department of Neurosurgery and the Department of Anaesthesia at Aalborg Hospital. I also thank Lene Kraul, Chromoge nix AB, Hillerød, Denmark, who kindly provided the kits for the fibrino lytic assays in study VII. The study was suppor ted by research grants from Aalborg Stift-tidendes Julelotteri and Nordjyl lands Amtskommu-nes Forsk ningsfond.
3

Contents1 Introduction ....................................................... 5
2 Markers of haemostatic activation .................... 5 2.1 Introduction .............................................. 5 2.2 Prothrombin fragment 1+2 (F1+2)........... 5 2.3 Thrombin-antithrombin III complex (TAT) ........................................................ 6 2.4 Fibrinopeptide A (FpA)............................ 6 2.5 Fibrin monomers (FM)............................. 6 2.6 Fibrin/fibrinogen degradation products (FbDP, FgDP) ............................ 7 2.7 Tissue plasminogen activator (t-PA) ........ 7 2.8 Tissue plasminogen activator inhibitor type 1 (PAI-1)........................................... 7
3 Alterations in haemostatic tests after surgery and trauma.................................... 8 3.1 Introduction .............................................. 8 3.2 Intraoperative alterations in haemostatic tests .................................. 8 3.3 Postoperative coagulation tests ................ 9 3.4 Postoperative fibrinolytic tests................. 9 3.5 The effect of anaesthesia on haemostatic tests....................................... 10 3.6 Hae most atic tests after isolated fractures of the lower limbs ................................... 11 3.7 Haemostatic tests after multiple trau ma and after isolated closed head injury........ 12 3.8 Haemostatic tests after traumatic shock... 13 3.9 Haemostatic tests after burn injury .......... 13 3.10 Discussion ................................................ 13
4 Haemostatic activation and relationship to clinicopathological findings after surgery......... 13 4.1 Introduction .............................................. 13 4.2 The relationship between cardiopulmonary dysfunc tion during hip surgery and haemostatic activa tion.............................. 14 4.3 Haemostatic tests and relationship to postoperative ve nous thromboembolism . 14 4.3.1 Studies in general surgery............. 14 4.3.2 Studies in elective hip surgery...... 15 4.4 Conclusions .............................................. 16
5 Haemostatic activation and relationship to clinicopathological findings after trauma ......... 16 5.1 Introduction .............................................. 16 5.2 Experimental studies, autopsy studies, paraclinical studi es ................................... 16 5.3 Relationship between injury severity and hae mosta tic tests....................................... 17 5.4 Relationship between haemostatic tests and posttrauma tic mortali ty and disseminated intravascular coagulation ......................... 17 5.5 Relationship between haemostatic tests and develop ment of posttraumatic pulmonary dysfunc tion............................. 18 5.6 Conclusions .............................................. 19
6 Perspectives of haemostatic activation after tissue injury ................................................................. 19 6.1 Introduction .............................................. 19 6.2 Fibrin and wound healing ........................ 20 6.3 Fibrin/FDP and initiation of increased permeability and inflammation ................ 20 6.4 Haemostatic activation, wound healing, organ dysfunc tion, and venous throm- boembolism after surgery and trauma...... 20 6.5 Possible future implications ..................... 22
7 Summary ........................................................... 22
8 Summary in Danish........................................... 23
9 References ......................................................... 24
AbbreviationsAMCA Tranexamic acid (Trans- 4 aminome- thylcyclohexane carboxylic acid)APTT Activate Partial Thromboplastin TestARDS Adult Respiratory Distress SyndromeAT III Antithrombin IIIBAL Bronchoalveolar lavage fluidBß1-42 Fibrin/Fibrinogen degradation product derived
from the ß chain Bß15-42 Fibrin/Fibrinogen degradation product derived
from the ß chainCV Coefficient of VariationD-dimer Fibrin Degradation Product of cross-linked
fibrin (two D-domains) DIC Disseminated Intravascular CoagulationDVT Deep Vein ThrombosisEACA Epsilon-aminocaproic acidECLT Euglobulin Clot Lysis Time ELISA Enzyme-Linked Immunosorbent AssayEPI Extrinsic Pathway InhibitorFbDP Fibrin Degradation ProductsFDP Fibrin/Fibrinogen Degradation ProductsFgDP Fibrinogen Degradation ProductsFM Fibrin MonomersFpA Fibrinopeptide AF1+2 Prothrombin Fragment 1 and 2GCS Glasgow Coma ScaleHC II Heparin Cofactor IIISS Injury Severity ScorePAI Plasminogen Activator InhibitorPAI-1 Plasminogen Activator Inhibitor type 1PAI-1:ag Plasminogen Activator Inhibitor type 1 anti-
genPaO2 Arterial partial oxygen saturationPC Protein CPD Pulmonary DysfunctionRIA RadioimmunoassayRT Recalcification TimeTAT Thrombin/antithrombin III complexTDP Total Degradation Products of fibrin and fibri-
nogenTHR Total Hip Replacementt-PA Tissue Plasminogen Activatort-PA:ag Tissue Plasminogen Activator antigenXL-FDP Cross-linked Fibrin Degradation Pro ducts
4

1 IntroductionThe soluble fibrinogen molecule may, with adequate stimulus, become insoluble in the blood and aggregate into fibrin complexes, which may be incorporated into larger fibrin clots. The hae mostatic action of fibrinogen and platelets is an important factor in the preven tion of deleterious and life-threatening loss of blood after trauma. Apart from the indis pensable capacity to facilitate haemostasis, the fibrin network within the wound provides a physiolo gical frame-work on which the process of wound healing can begin (1). On the other hand, when fibrin is deposi-ted else where, potentially harmful injury may occur due either to vascular obstruction or to initiation of in flammation and repair. It has been suggested that the processes of the haemosta tic system are controlled in a dynamic balance with the capaci ty to initiate repair of vascular lesions without inter fering with the patency of the vascular tree (2,3). Events which activate the haemosta tic system may therefore affect this balan ce. Haemostatic imbalance may occur when one or more controlling systems are over whelmed or exhausted. The alteration of blood coagulabi lity in relation to haemorr hage was studied by William Hewson in 1772. He observed that “The blood taken later coagula ted in less and less time till the blood issued last coagulated first” (4). In 1914, Gray and Lunt observed that the coagulation time of the blood decreased after ex perimen tal haemorr hage (5). In 1945, Bergquist made similar observations on patients during the early postoperative phase. The fall in whole blood coagulation time returned to normal in 24 to 48 h after operation (6). On the other hand, Macfarlane and Biggs found alterations in blood clot lysis time in connection with operation (7). It became evident that opera tion and trauma influenced several clotting and clot lysis-based haemostatic assays, but Warren et al wrote in 1950 that “We are obliged to state that throughout this work we have been con scious of the inadequacies of the methods used due to the lack of ability to isolate, with the exception of fibrino gen and platelets, the substances in question” (8). Until very recently quantification of the activation in the haemostatic system has been attempted by measure-ments of zymo gens of the coagulation cascade (factors X, VIII, V, prothrombin, and fibrinogen). But they proved to be rather insensitive in the detection of haemostatic activation, possibly due to the fact that they are present in plasma in excess and only a minor fraction is ac tivated or consumed during the haemostatic activation (9,10). The recent development of immuno chemical methods has made it possible to construct assays that can quantify the ac tivities of various steps of the haemostatic system (9,10). The present study attempts to describe the influence of sur gery, frac tures of the ex tremities, neurotrauma, and multiple trauma on the generation of specific
molecular markers of coagulation and fibrinolysis by newly developed immunochemical assays. Furthermore, it attempts to evalua te possible rela-tions hips between clinicopatho logical findings after surgery and trauma and the haemostatic activation.
2 Markers of haemostatic activation
2.1 IntroductionThe enzymes generated during the coagulation and fibrinolysis cascades are not directly available for quantification. Several molecules that are released as a consequence of the enzymatic activation of thrombin and its action on fibrinogen can be quantified by immunological methods. Furthermore, the activa tion pathway for plasmino gen, as well as the enzymatic reaction of plasmin on fibrin and fibrinogen, can be quantified. The processes that take place immediately before the formation of fibrin, and the processes that take place when fibrin is degraded, may then be characterized. Figure 1 presents a simplified scheme of the central actions in the formation and degradation of fibrin.
2.2 Prothrombin fragment 1+2 (F1+2)Several pathways have been suggested for the conversion of prothrombin to thrombin, but under physiolo gical conditions this process occurs in the presence of factor Xa, Va, and calcium ions, facilitating cleavage of prothrombin and libera tion of thrombin and F1+2, which is a polypeptide of 273 amino acids (11) (Fig. 1). A double-antibody liquid-phase ra dioimmu noassay (RIA) for the determi na tion of F1+2 was descri bed in 1979 by Lau et al (12). Later, the same group evaluated the assay on clinical samples (13, 15). The plasma half-life of F1+2 was calculated as approximate ly 90 min in healthy individuals (14). Plasma levels of F1+2 increase with age (15). A two-site solid-phase immunoen zymatic assay is now available (16). In this assay the first antibody directed against F1+2 is immunoaffinity purified, while the second tagging peroxidase-conjugated antibody is polyclo nal and directed against proth rombin. The enzyme activity on a chromogenic substrate is determined photometri cally. In the original assay for F1+2 a special anti coagulant solution with protease inhibitors was recommended in order to prevent in vitro formation of F1+2 (12,13). Citrated plasma is recommended for the commercially available assay (16). The use of the thrombin inhibitor D-Phe-Pro-Arg-Chlorometyhylketo ne (p-pack) in clinical samples did not result in a reduction in levels of F1+2, TAT, FgDP, or FbDP, compared with levels in citrated plasma (17). The ELISA test was used in the present study for the
5

determi na tion of F1+2 (Behring, Marburg, Germany) (16). The referen ce range given by the manufac turer is 0.44 - 1.11 nM between the 5th - 95th per centile. For 10-fold determina tion in one assay at two levels, the CV was 5.4% for 0.89 nM and 10.5% for 8.2 nM. The CV between series on test plasma was 14% for 0.51 nM on 5 occasions. Median (total range) in a group of 10 healthy in dividuals was 0.7 (0.3-1.8) nM.
2.3 Thrombin-antithrombin III complex (TAT)Thrombin is inactivated by its main physiological inhibitor, antithrombin III, by irreversible complex formation (Fig. 1). In an experimental study, data indicated that TAT is cleared from plasma by a receptor-mediated mechanism on hepatocytes (18). The plasma half-life of TAT in animals is reported to vary between a few minutes to 11 h, depending on the ex perimental model used (18). In 1980, Lau et al introduced a RIA for the determina-tion of TAT, based on the double-antibody method in liquid-phase, as for F1+2 (19). A solid-phase two-site immunoenzymatic method is now available. A polyclonal antibody specific for thrombin binds the complex, and a second enzyme-labelled antibody against antithrombin is used to quantify the complex (20). The assay was evaluated on clinical samples; raised levels were observed in patients with thromboembolism and disseminated intravascular coagulation (DIC) (21). In the present study, TAT was determined by the ELISA test (Behring, Marburg, Germany) (20). The reference range given by the manufac turer is 1.0 - 4.1 ng/ml between the 5th - 95th percentile. For 10-fold determina tion in one assay at two levels, the CV was 10.5% for 3.4 ng/ml and 10.7% for 43.7 ng/ml. The CV between series on test plasma was 9% for 10 ng/ml on 11 occa sions. Median (total range) in a group of 10 healthy individu als was 1.7 (1.2-2.6) ng/ml.
2.4 Fibrinopeptide A (FpA)In 1971, a RIA was introduced by Nossel and co-workers for the determination of FpA (22). FpA is a peptide of 16 amino acids cleaved from the Aα chain of the fibrinogen molecule by thrombin action (Fig. 1). The assay was later evaluated on clinical blood samples, and the disappearance rate from plasma in normal individuals was estimated to correspond to a plasma half-life of 3-5 min (23). Several patient groups had increased levels of FpA in plasma, and it was observed that the in vitro generation of FpA was increased in certain patients, suggesting increased intravascular coagulation (24). To counteract erroneously raised levels of FpA due to in vitro generation, samples were processed in an anticoagulant solution of trasylol and heparin (23,24). Since the antibodies used in the assay were not totally specific for FpA, depletion of fibrinogen prior to assay was necessary (23).
The FpA assay has been widely adopted as a very sensitive marker of coagulation activation, and very many studies concerning FpA have been published (25). However, the assay has not gained widespread clinical applicability due to cumbersome sampling technique and time-consuming assay procedures. It has been suggested that determination of FpA in the urine is a valid and sensitive method for the detection of the cumulative effect of thrombin action on fibrinogen. The recovery, stability, and accuracy have been reported as adequate (26-28). Increased urinary FpA immunoreactivity has been observed after myocardial infarction, ischaemic heart disease, peripheral artery disease, aortic aneurysm, malignancy, burn injury, and pulmonary embolism (26,27,29,30).An ELISA test for the detection of FpA in fibrinogen depleted plasma was developed in 1980 (31). Polyclonal FpA antibodies are incubated in excess with the fibrinogen depleted plasma, and the incubation mixture is transferred to FpA-coated vessels. For further incubation, a second peroxidase conjugated anti-IgG antibody is added. The peroxidase reaction through (H2O2) on ortho-phenylenediamine is measured spectrophotometrically at 492 nm. In the present study, FpA assay was performed with the ELISA test (31) (Boehringer Mannheim, GmbH, Diagnostica, Germany) on plasma depleted of fibrinogen by bentonite. The plasma was processed in an anticoagulant solution of citrate, trasylol, and heparin. The reference range given by the manufac-turer was <3 ng/ml. For 10-fold determination in one assay at two levels the CV was 8.6% for 2.1 ng/ml and 19.4% for 20.9 ng/ml. All levels in a group of 10 healthy individuals were below 3 ng/ml.
2.5 Fibrin monomers (FM)Thrombin action on the fibrinogen molecule results in the formation of FpA, fibrinopeptide B, and solu-ble fibrin monomers (FM) (Fig. 1). Fibrin monomers may polymerize in plasma, and activated factor XIII catalyzes the cross-linking of fibrin polymers, resulting in precipitation from plasma of an insoluble network of fibrin. Assays for the detection of soluble fibrin monomers have been available for more than 2 decades. They are qualitative tests based on gelatination of fibrin monomers by either ethanol or protamine sulphate (32,33). These tests are quickly and easily performed and have become widespread in clinical laboratories. A new assay for the determination of soluble FM was introduced by Wiman and Rånby in 1986 (34). This assay is based on the stimulatory effect of soluble fibrin on tissue plasminogen activator activation of plasminogen. The formed plasmin is quantified with a chrominogenic substrate. The assay has been evaluated in laboratory and clinical studies by Halvorsen et al (35-37). They found good agreement between the FM test and other qualitative FM tests, but correlation between the FM test and the FpA
6

assay was poor, and it was suggested that fibrinogen interfered with the assay (35-37). FM was determined by this test (Diagnostica Kabi, Stockholm, Sweden). The sensitivity of the FM assay was 30 nmol/l, but it was improved by following the time-course of the increase of absorbance at 405nm and then plotting the second time derivative of A405 (d2A/dt2) against the linear-phase reaction (0.1<A405<1.0) (34). By this modification the sensitivity of the assay was 3nmol/l.For 10-fold determination in one assay at two levels the CV was 25% for 8 nmol/l and 3.7% for 131 nmol/l. Median (range) in a group of 10 healthy individuals was 4 (<3-19) nmol/l.
2.6 Fibrin/fibrinogen degradation products (FbDP, FgDP)The degradation by plasmin of fibrinogen, soluble fibrin, and cross-linked fibrin results in a variety of degradation products, of which some can be further cleaved into smaller fragments (38). Semi-quantita tive agglutination tests for the determination FbDP/FgDP appeared in the 1960s, and a polyclo-nal-based enzyme immunoassay for the detection of fibrinogen fragment E was developed in 1973 (39-41). Since the antibodies used in these assays cross-react virtually completely with fibrinogen, only serum samples could be used. However, artefactual results on serum samples have been demonstrated in samples containing heparin or anticoagulating fibrinogen degradation fragments, resulting in inade-quate depletion of fibrinogen and leading to false positive results. During serum preparation, FDPs can be absorbed in the clot, leading to false negative results (42-44). The development of the monoclonal antibody preparation technique has made it possible to construct assays which can be performed on plasma samples (45-48). The FgDP assay consists of two different monoclonal antibodies. The first is a solid-phase capturing antibody, which forms complexes exclusively with E domain containing degradation products. It reacts with FgDP and FbDP, but not with fibrinogen or fibrin. The tagging antibody conjugated with horse-radish peroxidase reacts with fibrinogen and fibri-nopeptide A, comprising fibrinogen fragments, but not with free FpA (46). The kit used for the FgDP assay was from Organon Teknika, Turnhout, Belgium, the reference range given by the manufacturer is <0.25 µgFE/ml (FE = Fibrinogen Equivalent units).
The FbDP assay has the same capturing antibody as the FgDP assay, but the conjugated monoclonal antibody is virtually specific for FbDP (47). The commercially available kit used for FbDP assay was from Organon Teknika, Turnhout, Belgium. The reference range given by the manufacturer is < 0.31 µgFE/ml. The CV was 9.2% for 9.9 µgFE/ml for 6-fold determination in one assay. In a group of 10 healthy
individuals all levels were equal to or below0.3 µgFE/ml. In the assay for total degradation products (TDP), the capturing antibody is also the same as for the FgDP assay, and the conjugated antibodies consist of a mixture of the conjugated antibodies from the FgDP and FbDP assays (45). The commercially available kit used for the TDP assay was from Organon Teknika, Durham NC, USA, reference range <0.22 nmolFE/l.
2.7 Tissue plasminogen activator (t-PA)Tissue plasminogen activator t-PA is a single-chain glycoprotein of 530 amino acids, which is synthesi-zed by the endothelial cells. In the presence of fibrin the active t-PA converts plasminogen to plasmin. Since the formation of plasmin is virtually restricted to the fibrin surface, other plasma proteins are less exposed for plasmin degradation (49). Global fibrino-lytic assays, measuring the time required for lysis of clots made from diluted plasma, diluted blood, or the euglobulin fraction of plasma, have previously been used for the quantification of the profibrinolytic activity. The euglobulin clot lysis time is believed to measure the tissue plasminogen activity in the absence of antiplasmins (50). During the last 10 years, several immunoassays have been developed for the determination of t-PA antigen (t-PA:ag) (51). The t-PA:ag ELISA used in the present study consists of an anti-t-PA monoclonal antibody for both the solid-phase reaction and the reaction with the conjugated antibody (52). The kit was supplied by Chromogenix AB, Sweden. In 51 healthy individuals the manufacturer gives the median (range) as 6.0 ng/ml (1.7-18.4). In the present study, median (total range) in 10 healthy individuals was 4 ng/ml (1-8 ng/ml). For 9-fold determination in one assay at two levels, the CV was 4.7% for 4.6 ng/ml and 5.4% for 14 ng/ml.
2.8 Tissue plasminogen activator inhibitor type 1 (PAI-1)Plasminogen activator inhibitor type 1 (PAI-1) is the principal inhibitor of t-PA. In the blood PAI-1 occurs in an active form, a latent form or bound to plasminogen activators. Platelets and plasma are distinct compartments for PAI-1 (53). As a consequence of considerable diurnal variation of PAI activity, the blood collection time should be standardized. Assays for the quantification of PAI activity are performed in principle by incubating samples with t-PA in excess. In the next step and in the presence of a stimulator (fibrinogen fragments), the residual t-PA activity activates plasminogen to plasmin, which is quantified by reaction on a chromogenic substrate (54). The PAI activity kit was supplied from Chromogenix AB, Sweden (CoatestR PAI-1). In 44 healthy individuals, the manufacturer gives the median (range) as 3.9 AU/mL (0-71 AU/ml). For 10-fold
7

determination in one assay, the CV was 7.2% for 9 AU/ml. Median (range) in 10 healthy individuals was 7 AU/ml (4-10 AU/ml). A solid-phase enzyme immunoassay was used for the quantification of immunoreactive PAI-1. A monoclonal antibody directed against PAI-1 was used in the solid phase as well as the conjugated antibody. PAI-1 antigen was assayed by an ELISA from Chromogenix AB, Sweden (CoalizaR PAI-1). In 51 healthy individuals, the manufacturer gives the median (range) as 22.9 ng/ml (5-140 ng/ml). For 10-fold determination in one assay at two levels, the CV were 6.0% for 38 ng/ml and 5.3% for 73 ng/ml, and median (range) in 10 healthy individuals was 19 ng/ml (8-38 ng/ml).
3 Alterations in haemostatic tests after surgery and trauma
3.1 IntroductionTissue injury after trauma differs from that after surgery
with respect to the absence of anaesthesia, often severe haemorrhage and traumatic shock or closed wounds, such as closed fractures, closed head injuries, and major soft tissue injury. Studies of haemosta tic tests on surgical and trauma patients have been performed in the past. This chapter includes a survey of the literature and a presentation of the author's experience concerning alterations in haemostatic tests after surgery and trauma.
3.2 Intraoperative alterations in haemostatic testsShortening of clotting time, as determined by various clotting assays, has been observed during operations (55-58), but prolongation of the activated partial thromboplastin time assay (APTT) has been observed at the end of surgery (59). In hip surgery, Modig and Malmberg observed that the decrease in clotting time was most pronounced during insertion of the femoral component (60). Shortening of various global fibrinolytic tests has also been seen during surgery (57,61-63). Giercksky et al studied circulating tissue thromboplastin in 7 patients during hip surgery.
8
FIGURE 1. The key processes involved in the final common pathway for both coagulation and fibrinolysis.F1+2: Prothrombin fragment 1 and 2. TAT: Thrombin/Antithrombin III-Complex. FpA: Fibrinopeptide A. FM: Fibrin Monomer. FgDP: Fibrinogen Degradation Product. FbDP: Fibrin Degradation Product. PAI-1: Plasminogen Activator Inhibitor type 1. t-PA: Tissue Plasminogen Activator.

Samples taken during the operation contained measurable levels of tissue thromboplastin, whereas preoperative samples did not (64). A significant fall in antithrombin III (ATIII) activity has been observed under different surgical procedures (65,66). Sandset et al measured the activity levels of extrinsic pathway inhibitor (EPI), ATIII, heparin cofactor II (HCII), and protein C (PC) in hip surgery and cholecystectomy. Levels of all the coagulation inhibitors decreased during surgery. The underlying mechanisms were probably haemodilution, since plasma levels of albumin decrea-sed accordingly (67). In two studies on hip surgery, levels of FpA increased significantly at the time of inserting the femoral component (68,69). In the latter study a similar increase in levels of XL-FDP (cross-linked fibrin degradation products) was observed. In two other studies on hip surgery patients, levels of TAT increased by a factor of 10 during bone manipulation (70), and levels of F1+2 increased by a factor of 2 at the time of implementation of the acetabular component (71). Increased haemostatic activation, as indicated by high levels of FpA, Bß15-42 (fibrinogen fragment), D-dimer (cross-linked fibrin degradation product), and TAT has been observed during gastric and hepatic surgery (72,73). Increased levels of t-PA activity, PAI activity, and PAI antigen have been found during hip surgery (71,74).
3.3 Postoperative coagulation testsShortening of coagulation time of the blood has been observed in the immediate postoperative period (6,56). A prolongation of the APTT has been reported in the postoperative period after abdominal surgery (75), but this was not seen in another study on general surgery patients (57). Decreased levels of factor VII, prothrombin, fibrinogen, and platelets are usually seen in the immediate postoperative period after major surgery. From the first postoperative day a continuing rise is observed in levels of prothrombin, fibrinogen, platelets, factor VIII activity (VIII:C), and factor V activity. Levels become significantly higher than preoperative levels between the 3th and 5th postoperative days (8,76-78) (I). The exact duration of this phase is at present un clear, but levels are still raised on the 10th postoperative day after major surgery. Observations have been made that AT III levels after major surgery return to preoperative levels within the 5th and 7th postoperative day (67,79) (Fig. 2). Similar observations have been made for EPI, HC II, and PC after hip surgery (67). Increased levels of FpA have been reported after major abdominal surgery (80-82) and after major neurosurgical operations (83,84), but levels of FpA were not increased in the postoperative period after abdominal surgery in another study (75).On the first postoperative day after hip surgery, levels of FpA were not increased over preoperative levels
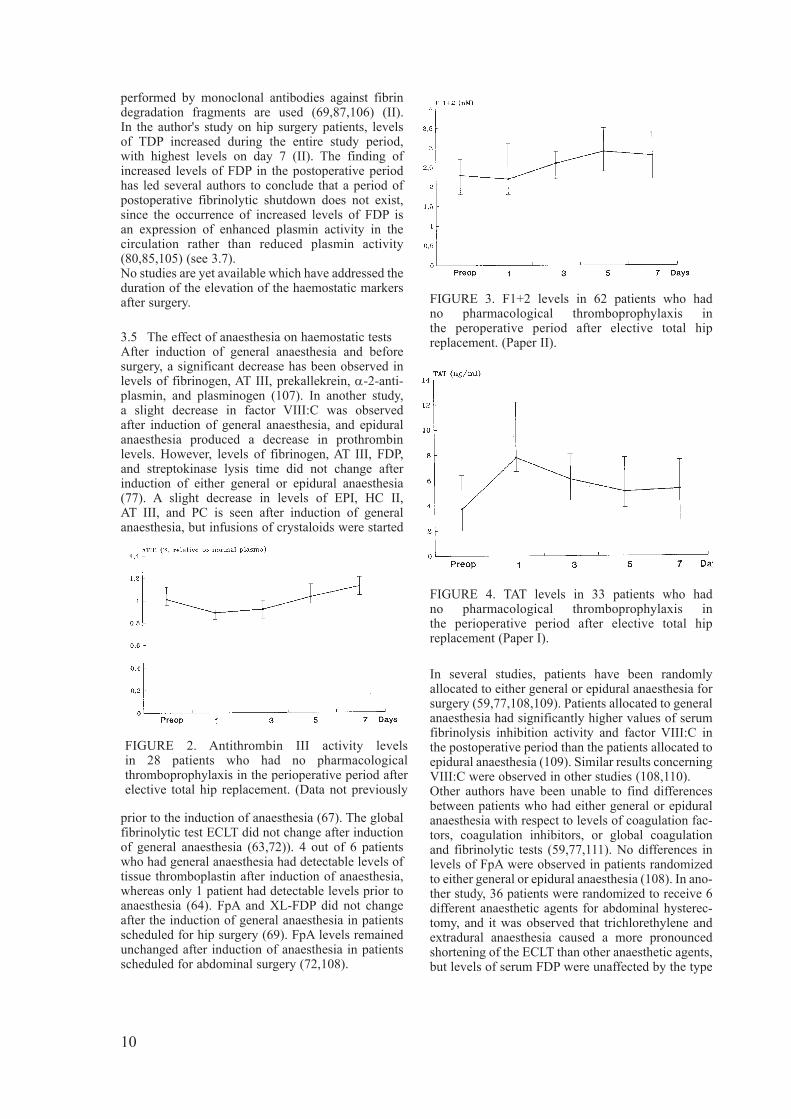
(69,85). However, on the 7th postoperative day FpA levels were significantly higher than preoperative levels (85). These observations on FpA levels are similar to the observations on F1+2 levels after hip surgery (II). In patients not receiving anticoagulants for thromboprophylaxis, postoperative levels of F1+2 were significantly higher than preoperative levels on days 3,5, and 7, but not on day 1 (II) (Fig.3). These observations on FpA and F1+2 may suggest a delayed reactivation of coagulation in the postoperative period. On the other hand, levels of TAT are highest on the first postoperative day and decrease gradually towards lower levels in the postoperative period (86-88) (I) (Fig.4). Similar observations on TAT were made after lung cancer surgery and upper abdominal surgery (82,89). These apparently contradictory observations may suggest that the plasma half-life of F1+2 and FpA is considerably shorter than the plasma half-life of TAT in the postoperative/traumatic period (see 3.6 and 3.7).
3.4 Postoperative fibrinolytic testsPostoperative prolongation of global fibrinolytic tests has been observed (57,62,77,90-94). Conflicting results were observed in different patient groups, since global fibrinolytic tests indicated fibrinolytic shut down in cancer patients undergoing surgery, but not in patients undergoing surgery for benign diseases (95). In a study using the euglobulin faction on a fibrin plate, a decrease in activity from the first to the 7th postoperative day was observed (76). Other authors who used global fibrinolytic tests depending on fibrin digestion methods did not observe a post-operative fibrinolytic shutdown (96,97). It was later suggested that the apparent postoperative reduction in fibrinolysis, as determined in the euglobulin fraction, was due to reduced t-PA activity, possibly as a consequence of increased PAI activity in the circulation (94,98-103). t-PA activity 24 h post-operative was significantly lower than preoperative activity. The t-PA activity increases on the following days, and it is significantly higher than preoperative levels on day 7. t-PA:ag levels were significantly higher than preoperative levels on the first, 5th, and 7th postoperative days (103). In accordance with these observations it is found that PAI-1 activity and PAI antigen are significantly higher than preoperative values on the first postoperative day. On the following days the PAI activity declines towards pre operative values, whereas PAI antigen levels remain higher than preoperative levels (102). Levels of fibrinogen/fibrin degradation products are an indication of previous plasmin activity (104). Bß1-
42 or Bß15-42 are such peptides released from plasmin action on fibrinogen and fibrin. These peptides, which have been quantified in several studies in the postoperative period, are reported to be significantly raised on the first postoperative day, followed by a continuing rise during the first 7 postoperative days (80,85,105). Similar results are obtained when tests
9
performed by monoclonal antibodies against fibrin de gra dation fragments are used (69,87,106) (II). In the author's study on hip surgery patients, levels of TDP increased during the entire study period, with highest levels on day 7 (II). The finding of increased levels of FDP in the postoperative period has led several authors to conclude that a period of postoperative fibrinolytic shutdown does not exist, since the occurrence of increased levels of FDP is an expression of enhanced plasmin activity in the circulation rather than reduced plasmin activity (80,85,105) (see 3.7). No studies are yet available which have addressed the duration of the elevation of the haemostatic markers after surgery.
3.5 The effect of anaesthesia on haemostatic testsAfter induction of general anaesthesia and before surgery, a significant decrease has been observed in levels of fibrinogen, AT III, prekallekrein, α-2-anti-plasmin, and plasminogen (107). In another study, a slight decrease in factor VIII:C was observed after induction of general anaesthesia, and epidural anaesthesia produced a decrease in prothrombin levels. However, levels of fibrinogen, AT III, FDP, and streptokinase lysis time did not change after induction of either general or epidural anaesthesia (77). A slight decrease in levels of EPI, HC II, AT III, and PC is seen after induction of general anaesthesia, but infusions of crystaloids were started
prior to the induction of anaesthesia (67). The global fibrinolytic test ECLT did not change after induction of general anaesthesia (63,72)). 4 out of 6 patients who had general anaesthesia had detectable levels of tissue thromboplastin after induction of anaesthesia, whereas only 1 patient had detectable levels prior to anaesthesia (64). FpA and XL-FDP did not change after the induction of general anaesthesia in patients scheduled for hip surgery (69). FpA levels remained unchanged after induction of anaesthesia in patients scheduled for abdominal surgery (72,108).
In several studies, patients have been randomly allocated to either general or epidural anaesthesia for surgery (59,77,108,109). Patients allocated to general anaesthesia had significantly higher values of serum fibrinolysis inhibition activity and factor VIII:C in the postoperative period than the patients allocated to epidural anaesthesia (109). Similar results concerning VIII:C were observed in other studies (108,110).Other authors have been unable to find differences between patients who had either general or epidural anaesthesia with respect to levels of coagulation fac-tors, coagulation inhibitors, or global coagulation and fibrinolytic tests (59,77,111). No differences in levels of FpA were observed in patients randomized to either general or epidural anaesthesia (108). In ano-ther study, 36 patients were randomized to receive 6 different anaesthetic agents for abdominal hysterec-tomy, and it was observed that trichlorethylene and extradural anaesthesia caused a more pronounced shortening of the ECLT than other anaesthetic agents, but levels of serum FDP were unaffected by the type
10
FIGURE 2. Antithrombin III activity levels in 28 patients who had no pharmacological thromboprophylaxis in the perioperative period after elective total hip replacement. (Data not previously
FIGURE 3. F1+2 levels in 62 patients who had no pharmacological thromboprophylaxis in the peroperative period after elective total hip replacement. (Paper II).
FIGURE 4. TAT levels in 33 patients who had no pharmacological thromboprophylaxis in the perioperative period after elective total hip replacement (Paper I).

of anaesthesia (110).
3.6 Haemostatic tests after isolated fractures of the lower limbs
Several earlier studies have attempted to estimate coagulation changes in patients with fractures of the lower limbs. However, it is not easy to derive much useful information from them (112,113). One study concluded that trauma which caused isolated frac-tures did not affect coagulation activity (114). Innes and Sevitt gave no specific information about coagu-lation changes in patients with isolated fractures of the lower limbs, but they stated that the changes were less pronounced than in patients with severe trauma (115). In the author's study on patients with an isolated lower limb fracture (III), substantial haemostatic
activation was observed, as indicated by high levels of F1+2, TAT, FM, FbDP, and FgDP shortly after trauma. At admission the correlations between the different coagulation markers were relatively strong, but on day 1 the correlations were weak or absent. An explanation for this observation could be that admission plasma levels reflect an equally increased production of the different markers, whereas on day 1 the plasma levels are the result of different degradation and excretion rates (III). The plasma levels of TAT, FbDP, and FgDP during the first week in patients with hip fractures are shown in figure 5. TAT levels decreased gradually in this period. Levels of FbDP and FgDP decreased from admission to day 3, but an increase between days 3 and 6 was observed, which was significant at the 5% level for both markers.
11
FIGURE 5. Levels of TAT, FbDP and FgDP in 28 patients with hip fractures on admission (26 samples) and on days 1 (25 samples), 2 (23 samples), 3 (16 samples) and 6 (11 samples).
The curves represent median and the bars represent the interquatile range.
Levels of TAT decreased significatly from admission to day 1 (p<0.001)*, and from day 1 to day 6 (p<0.05)*.
Levels of FbDP and FgDP decreased significantly from admission to day 1 (p<0.001)*, and the increase from day 3 to day 6 was significant for both markers (p<0.05)*.
Details concerning the patients are given in paper III.(Data from days 2, 3 and 6 not previously published)

3.7 Haemostatic tests after multiple trauma and after isolated closed head injury
In the study performed by Innes and Sevitt in 1964, serial blood samples were taken from trauma victims in the posttraumatic period (115). Minor haemostatic disturbances were seen in patients who had isolated fractures of the extremities, whereas patients with multiple trauma had shortening of clot lysis time and clotting time in the first hours after trauma. Prolongation of the clot lysis time, together with a normal clotting time, occurred during the first posttraumatic day. Prolongation of both global tests continued on the following posttraumatic days. Coagulation fac tors, such as factor VII, factor V, prothrombin, and fibrinogen, were low shortly after trauma, but they increased to normal levels during the early posttraumatic period. Platelet count declined during the first 1-3 posttraumatic days, followed by thrombocytosis, which remained for more than a week. These findings were later confirmed by other authors who furthermore found raised levels of serum FDP in patients with multiple trauma or isolated head injury (114,116-120). High levels of FpA have been observed in admission blood samples from patients with multiple trauma or head injury (121-123) (V). On the following days levels reach near normal (122) (V). In the study by the author, levels of F1+2 were greatly increased at admission, but decreased towards normal on the following days (VI).The FM test performed on plasma from the same patients showed very high levels at admission. The levels declined during the following days, but they did not become normal during the first week after admission (V). Another study showed highly raised levels of TAT immediately after severe trauma (20 min) (124) and at admission to the emergency unit. In the study by the author, TAT levels were also higher on admission, declining on the following days but remaining considerably above normal in the first 7 days after trauma (VI).The urinary excretion of FpA in trauma patients is about 50-fold higher than in healthy controls with normal plasma levels of FpA (IV). This observation may suggest that FpA generation was highly increased in spite of only marginally raised plasma levels in the posttraumatic period. The posttraumatic plasma fluctuation in levels of F1+2 seems to be similar to that of FpA; likewise, F1+2 immunoreactivity is detected in the urine from trauma patients. The urinary immunoreactivity of F1+2 was higher than the corresponding plasma levels, and the excretion was almost 100 times that of healthy controls. On the other hand, TAT immunoreactivity was virtually not detected in the urine from the trauma patients, which may suggest that the larger TAT molecule is not excreted in the urine. It is possible that the urinary levels of FpA and F1+2 are more sensitive indicators of the coagulation turnover than measurement of the plasma levels of these peptides. But the observations
on urinary FpA and F1+2 in trauma patients are at present preliminary and need further investigation. Alterations in renal excretion and handling may occur in the posttraumatic period, and the antigenic properties of the molecules may change in the urine (IV).Assays for D-dimers, FbDP, TDP, or FgDP, which use monoclonal antibodies, have been used to detect haemostatic activation in plasma samples from trauma patients. Lampl et al measured these 4 markers in samples taken from trauma victims within the first 30 min after the incident (125). All the markers were about 20 to 50 times above normal levels. The next sample was taken within 58 to 98 min after the incident, at which time levels of FgDP and fibrinogen were significantly decreased. The other markers, virtually reflecting fibrin derived degradation products, did not change between the two samples (125). Plasma and serum levels of FDP decrease to near normal from day 1 to day 3 after trauma, but a second rise in levels of FDP has been observed by the author and other investigators at the end of the first week after trauma (122,126) (V). These findings were not confirmed in another study (123). However, compari-sons are difficult, since the most traumatized patients in the last named study were given gabexate mesilate (a protease inhibitor with high affinity for thrombin). This secondary increase in plasma levels of FbDP, occurring between the 3th and 7th day after surgery and trauma (II,V), may reflect wound healing associated fibrin degradation and dissolution of other extravascular or intravascular fibrin clots. But it may also be a response that opposes the possible secondary increased fibrin production in the post ope-ra tive/traumatic period (see 3.4). High levels of t-PA:ag and t-PA activity were observed immediately after severe trauma, but within the next 11/2 h a 10-fold fall occurred for both measures of t-PA. PAI activity levels rose significantly during the same period (125). PAI activity levels were measured in serially taken blood samples from trauma patients who were admitted within 1 h after the incident (127). The normal admission levels of PAI activity rose to peak levels 12 h after admission. A steady fall towards normal PAI activity levels then occurred within 24 h after trauma. No further increase was seen within the first 4 posttraumatic days. Levels of t-PA:ag, PAI-1:ag, and PAI-1 activity were increased in 19 patients with multiple trauma, and levels of α-2-antiplasmin were low at admission (1/2 to 7 h after trauma) (VII). Levels of t-PA:ag normalized during the first week, whereas PAI-1:ag levels decreased gradually from day 1 to day 3, after which a secon dary increase was observed. A similar trend occurred in levels of PAI activity. Levels of α-2-antiplasmin increased to above normal levels (VII). The general assumption is that the fall in plasma profibrinolytic activity (decreased t-PA activity/increased PAI activity) is due to increased liberation of PAI, which subsequently inactivates free t-PA, leading to decreased or impaired
12

fibrinolysis. On the other hand, fibrin degradation is accomplished when the active t-PA molecule is adsorbed on the fibrin surface activating the adsorbed plasminogen (49). The postoperative/-traumatic fall in t-PA activity could therefore be an indication of increased t-PA adsorption on fibrin. This would result in increased rather than decreased fibrinolysis. The concept that low plasma levels of t-PA activity are an indication of reduced fibrinolysis after surgery and trauma may then be challenged (VII).
3.8 Haemostatic tests after traumatic shockTraumatic haemorrhagic shock may be defined as a significant loss of blood volume due to trauma, which during resuscitation necessitates multiple blood trans-fusions in order to maintain adequate tissue per-fusion. Clinical studies concerning the influence of traumatic haemorrhagic shock on coagulation tests are sparse. However, the influence of massive transfusions on conventional coagulation tests has been studied in trauma patients. Prolongation of partial thromboplastin time, prothrombin time, and APTT has been observed shortly after multiple transfusions, but 15 h later the values were near normal. After day 2 the test results were normal. Levels of fibrinogen, factor V, and factor VIII are initially low, but they increase during the post-traumatic period; raised values have been seen on day 2 (128,129). Raised levels of serum FDP were observed in a majority of patients during an obser-vation period of 25 days after haemorrhagic shock (129).
3.9 Haemostatic activation after burn injury Severe burn injury is also associated with consi-derable alterations in haemostatic tests, and the response pattern is similar to that in trauma patients (130,131).
3.10 Discussion Brain, lung, and epithelium of the skin possess large amounts of tissue factor (132). Most authors find it plausible that tissue thromboplastin released from the wound activates the extrinsic coagulation pathway, which stimulates fibrin formation. It has been suggested that the release of vasopressin from the posterior pituitary may mediate haemostatic activation during operations, since a close temporal relationship exists between the rise in plasma vasopressin levels and the rise in FpA levels during operation (72). Other neurophysiological mechanisms may contribute to the haemostatic activation during and after surgery and trauma, since the global coagulation time decreases during experimental haemorrhage (133) and levels of FpA increase in dogs after infusion of adrenaline (134). Nygaard et al demonstrated increased thromboplastin activity in systemic circulating blood monocytes after total hip replacement, and suggested that this might play a part in the induction of a post operative prethrombotic state (135).
For the different markers of coagulation and fibrinolysis, several reservations must be considered when interpretations of the plasma levels are made. 1) Measurement of the haemostatic markers in
plasma does not distinguish whether the plasma levels are the result of local activation, local release, or systemic haemostatic activation.
2) Differences in plasma half-life may exist between the different haemostatic markers, and the plasma half-life may change due to alterations in the metabolic and excretion behaviour.
3) A wide inter-individual range of the markers was observed in the investigated patients.
It is suggested from the author's studies (I-VII) that the immediate effect on the haemostatic system of hip replacement surgery, isolated fractures of the hip, femur, and leg, isolated head injury, and multiple trauma is activation of both fibrin formation and fibrin degradation pathways. This could be due to the release of procoagulant activity from the wound and the release of profibrinolytic activity, which may originate from the endothelium.A temporary fall towards lower levels of the coagu-lation markers occurs during the first postoperative and the posttraumatic days, but levels are above normal in the first week, suggesting continuing activation of coagulation. This may possibly reflect a secondary activation of the haemostatic system, promoted by the inflammatory processes in the wound healing sequence and procoagulant activity released when the haemostatic plugs are degraded. As indicated by increased levels of fibrin/fibrinogen degradation products, a secondary increase in fibrin degradation is observed between the 3rd and 7th day. This may reflect increased degradation of fibrin as a response to the increased fibrin formation in this period, degradation of fibrin in the wound, and degradation of intravascular fibrin. The work by the author does not reject the hypothesis that the changes in the blood after surgery and trauma, as determined by the haemostatic markers, are a consequence of a dynamic haemostatic balance, and that this may be considered as a normal physio-logical response to tissue injury and repair.
4 Haemostatic activation and relationship to clinicopathological findings after surgery
4.1 IntroductionA variety of complications which occur after elective surgery and trauma have been attributed to the haemostatic system. They include cardiopulmonary impairment during hip surgery, postoperative/traumatic deep vein thrombosis and pulmonary emboli, posttraumatic pulmonary dysfunction, and posttraumatic disseminated intravascular coagulation. This chapter surveys the literature and presents the author's experience concerning the
13

relationship between complications after surgery and the haemostatic system.
4.2 The relationship between cardiopulmonary dysfunction during hip surgery and haemo static activation
Cardiopulmonary changes during total hip replacement (THR) using cemented components include hypoxaemia, hypotension, cardiac arrest, and sudden death. The intraoperative mortality ranges from 0.02% to 6.6% (136). A transient fall in arterial partial oxygen saturation (PaO2) occurs immediately after the insertion of the cemented femoral component (60,137). Several pathogenetic factors have been suggested (138). Orsini et al demonstrated that the pressurizing effect of bone cement on producing high intramedullary pressure caused pulmonary micro emboli in dogs (138). The pulmonary microemboli contain fat, a variety of bone marrow cells, platelet aggregations, and small fibrin plugs, which are released from the intramedullary cavity during instrumentation and insertion of the femoral component (58,138,139). Infusion of bone cement (monomethylmethacrylate) into dogs did not affect clotting tests or produce pulmonary trapping of fibrin and platelets, and no change in pulmonary function was recorded (140). A marked increase in circulating FpA, F1+2, and TAT levels, and a reduction in plasma coagulation time, when recalcified, are observed at the time of instrumentation and insertion of the femoral component, suggesting that thromboplastic containing material is released (58,68-71). Patients undergoing THR were given 51Cr labelled platelets and 125I labelled fibrinogen the day before operation (141). A transient accumulation in the lungs of 51Cr radioactivity and 125I radioactivity was recorded during femoral bone manipulation and after impaction of the femoral component. When the tourniquet used for bloodless field during total knee replacement was deflated, transoesophageal echocardiography revealed showers of echogenic material crossing the right atrium and ventricle and the pulmonary artery (142). Conclusive evidence has not yet been established for a causal relationship between cardiopulmonary impairment and activation of the haemostatic system during hip surgery.
4.3 Haemostatic tests and relationship to post-operative venous thromboembolism
Patients who undergo major surgery are exposed to a risk of venous thromboembolism, which accounts for a significant part of the morbidity and mortality after surgery (143). The frequency of non-symptomatic postoperative thromboembolism depends on the diag nostic method used. A variety of methods have been used for the detection of non-symptomatic postoperative deep vein thrombosis (DVT); bilateral phlebography, I-125-fibrinogen scanning, impedance plethysmography, and doppler or real-time B-mode ultrasound. Very poor agreement between the different
methods has been reported when they are used for screening of postoperative DVT (144-146). At present, bilateral phlebography is considered to be the reference standard for screening of non-symptomatic postoperative DVT. However, the interpretation of bilateral phlebograms obtained from postoperative patients seems to be highly dependent on the observer, since interobserver variation is pronounced (147). Many attempts have been made to relate different coagulation and fibrinolytic tests to the occurrence of postoperative venous thromboembolism, but conflicting results have often been reported.
4.3.1 Studies in general surgerySeveral studies on patients undergoing elective abdominal, urological, and gynaecological surgery for benign or malignant diseases have observed lower preoperative fibrinolytic activity, as measured by global fibrinolytic tests, in patients in whom postoperative DVT developed (90,94,148-151). Other authors have not found differences in preoperative global fibrinolytic tests between patients with and without postoperative DVT (63,95-97,152-155). Aranda et al reported that preoperative PAI activity levels were significantly higher in patients in whom DVT developed, but levels of t-PA activity and t-PA antigen were not different (94). Other studies measured the preoperative t-PA inhibition activity, but no differences were seen between patients with or without DVT (98,151,156). Likewise, no significant differences in preoperative levels of t-PA activity and antigen levels have been observed between patients with and without postoperative DVT (151,156). Significantly lower preoperative levels of plasmin- α-2-antiplasmin complex have been reported in patients who developed postoperative DVT (157). The findings of preoperative differences in the fibrinolytic tests cannot be interpreted as proof of a causal relationship between impaired preoperative fibrinolytic activity and the development of postoperative DVT. Clearly, other significant differences existed between the patients who developed DVT and those who did not. DVT patients are older (148,150,151) and their operations are more often for malignant diseases, which may require more extensive surgery (148,150,158). The possibility that the preoperative fibrinolytic tests were confounded by high age and malignancy has been given very little attention.The above-mentioned assays have also been performed on postoperative plasma samples. In a study on 28 patients, the fibrinolytic activity, determined by a 125-I-fibrin digestion technique, was higher 48 h after the operation in the 9 patients who developed postoperative DVT (97). As determined by the dilute blood clot lysis test and the fibrin plate lysis area, patients with postoperative DVT had a higher reduc-tion of fibrinolytic activity on the first postoperative day (95). The fibrinolytic activity, as determined by a timed fibrin digestion technique,
14

revealed that the DVT patients had significantly lower fibrinolytic activity on the first postoperative day. However, on the following postoperative days, no differences in fibrinolytic activity existed between the patients (96). Similar observations were made by others, who found that the dilute blood clot lysis time and the ECLT were significantly longer on the 1st postoperative day in DVT patients (90,154). Other studies found no differences in the ECLT or in fibrin plate activity when patients with and without DVT were compared (63,94,153). In a study on orthopaedic and urological patients, using whole blood dilute clot lysis assay, patients who had normal test results in pre- and postoperative samples had a 1% risk of postoperative DVT, whereas the incidence of DVT was 28% in patients who had one abnormal assay, and 56% in patients with three abnormal assays (159). In another study t-PA activity and antigen levels were not different in the postoperative period when patients with and without DVT were compared (94). Individual increases in t-PA inhibition from pre- to postoperative days were significantly higher in patients with DVT (98). It has also been reported that t-PA antigen levels decreased from preoperative to postoperative in patients who developed DVT, whereas patients without DVT showed an increase in t-PA antigen levels from preoperative to postoperative (160). In a study comprising 36 patients, postoperative levels of serum FDP were significantly higher in patients who had either DVT or PE than in patients without thromboembolism (161). This finding was not confirmed in another study (153).A study on patients who underwent major gastrointestinal surgery for malignant or benign diseases measured levels of FpA and fibrinogen fragment Bß15-42 in pre- and postoperative samples (80). 14 of the 32 patients developed postoperative DVT. The DVT patients had higher levels of FpA on the 7th postoperative day and higher Bß15-42 on the first post operative day than the patients without DVT.
4.3.2 Studies in elective hip surgeryThe relationship between haemostatic tests and the development of non-symptomatic thromboembolism after THR has been investigated during the past 10 years. In contrast to the studies on general surgery patients, the group of elective hip surgery patients is more uniform with respect to the preoperative disease status, undergoing a standard operation (trauma) and following a standard rehabilitation programme. The use of elective hip surgery patients may partly overcome the difficulties and considerations concerning possible confounding linkages between concurrent disease, age, type of operation, and the haemostatic tests.In five studies, the observation was made that preoperative PAI-1 activity levels were significantly higher in patients in whom postoperative non-symptomatic thromboembolism developed than in patients without (101,102,162-164). In another study
no such difference was observed (165). However, significantly lower preoperative levels of t-PA activity have been found in patients with postoperative DVT (103). Levels of PAI activity, PAI antigen, and t-PA antigen were higher 15 min after surgery and on day 1 in patients who later developed thromboembolism (102). PAI activity and t-PA antigen levels on day 7 were also higher in patients with thromboembolism (101,102). However, the other studies did not find these differences in the postoperative period (103,162,164,165). This survey suggests that low plasma profibrinolytic activity is associated with the development of post-operative thromboembolism. A causal relationship has not been demonstrated, and it remains to be established whether a preoperative or a postoperative modulation of the plasma profibrinolytic activity may influence the occurrence of postoperative thromboembolism after THR. Postoperative levels of FDP seem to be significantly higher in patients with DVT (87,106). In the study by the author in patients who had no pharmacological thromboprophylactic medication, levels of TDP were significantly higher on day 7 in patients who had DVT. But due to a wide overlap between groups with and without DVT, levels of TDP were without predic-tive power for the identification of patients with DVT. In patients who had low molecular weight heparin (LMW-heparin) for prophylaxis, no significant difference was observed between groups with and without DVT (II).FpA levels did not differ between patients with and without DVT in a rather small study (85). In the author's study, the F1+2 levels postoperatively were significantly higher in patients with DVT, who received no anticoagulants, than in patients without DVT, who received no anticoagulants (II). Levels of F1+2 were without predictive power for DVT. In the group who had LMW-heparin for prophylaxis, no differences in levels of F1+2 were observed between patients with and without DVT. Postoperative levels of TAT have also been observed to be higher in patients with DVT (86,87,106). A trend towards such differences was seen in the study by the author, but it was not statistically significant (I).The prophylactic use of low molecular weight heparin (LMW-heparin) reduces the incidence of non-symptomatic DVT after elective hip surgery (166). The mechanisms by which this is accomplished are not yet fully understood. In studies by the author and others, no influence of prophylactic dosages of LMW-heparin on levels of t-PA and PAI has been observed (102,103,165). In the study by the author (I), postoperative levels of TAT did not differ significantly between patients who had LMW-heparin and patients who had placebo (I). On the other hand, in the larger study (II), levels of F1+2 were significantly lower in patients who had LMW-heparin, and day 7 levels of TDP were significantly lower in the LMW-heparin group (II). The results may support the hypothesis
15

that the prophylactic administration of LMW-heparin reduces thrombin turnover, which possibly reduces the amount of fibrin available for plasmin degradation in the postoperative period. A further discussion of suggested and postulated mechanisms is beyond the scope of this presenta-tion.
4.4 ConclusionsNo haemostatic test has so far provided a satis-factory predictive power for the discrimination bet-ween patients with and without non-symptomatic postopera-tive DVT. The following factors presu-mably contribute to the conflicting findings concer-ning the relationship between postoperative DVT and haemostatic tests: differences in the haemostatic tests used, heterogeneous patient groups, patients undergoing differ-ent types of operation, patients receiving different kinds of thromboprophylaxis, and, as mentioned, differences in and difficulties with the diagnostic methods used for the detection of non-symptomatic thromboembolism. It is possible that thrombotic events may not be restricted to the deep veins of the lower extremities (see 6.4).The clinical significance of the detection by phlebo-graphy of non-symptomatic DVT on a particular day in the postoperative period seems to be unclear. To elucidate a possible clinical usefulness of the haemostatic markers, It is suggested that studies should be performed concerning the relationship between haemostatic markers and clinical events, such as symptomatic postoperative cardiopulmonary disease and postoperative mortality. However, lack of methods for proper quantitation of cardiopulmo-nary symptoms may complicate such studies.
5 Haemostatic activation and rela-tionship to clinicopathological findings after trauma
5.1 IntroductionThe capacity to increase fibrin formation after trauma may, as previously mentioned, be an important factor in wound haemostasis. However, several observations suggest that fibrin formation after trauma is not restricted to the wound only. Experimental studies, autopsy studies, and paraclinical studies suggest that intravascular fibrin deposition is common after haemorrhage and trauma. This chapter presents such studies, and studies on the relationship between haemostatic tests and clinicopathological findings in patients after trauma.
5.2 Experimental studies, autopsy studies, paraclinical studies Turpini and Stefanini observed intravascular deposition of fibrin and platelets in the lung, kidney, and liver in rabbits after severe haemorrhage, though
not in previously splenectomized animals (167). These observations, which suggest that the spleen is an important mediator of haemostatic activation after haemorrhage, were reported several decades earlier by McClintock and Magers, who noted shortening of the clotting time in dogs after haemorrhage, but not when the dogs were splenectomized (168). Their study was based on the classical study by Gray and Lunt, who found that exclusion of the abdominal circulation increased clotting time, and that severe haemorrhage did not decrease clotting time when the abdominal circulation was excluded (5). The experimental studies on haemorrhagic shock were later continued by Hardaway in 1963. In the first study (169), 28 dogs were subjected to haemorrhagic shock for 21/2 h, after which the blood was retransfused. 14 of the dogs were additionally given streptokinase, the rest acting as controls. 11 dogs in the streptokinase group survived, whereas only 3 survived in the control group. In the second study (170), dogs were divided into 3 groups. 15 dogs were controls as in the first study. Another 15 were treated with streptokinase. The third group of 9 dogs was not bled, but received streptokinase. Within 24 h, 11 control dogs died, while 4 in the treated group died. All the dogs survived which received streptokinase only. In experimental closed minor head injury in rats, pretreated with epsilonaminocarproic acid (EACA), which inhibits plasminogen binding to fibrin, fibrin deposition in the pulmonary vessels was seen shortly after the injury. These changes were not seen in animals which under went the same treatment, except for the head injury (171).Using radiolabelled platelets and fibrinogen for external detection of pulmonary deposition of radioactivity, pulmonary microembolism was observed after musculoskeletal trauma of a hind limb in pigs (172). In another study, anaesthetized pigs were subjected to major soft tissue injury of the outer thigh (173). 9 untreated animals died within 48 h, whereas 5 animals treated with streptokinase and 5 animals treated with tissue plasminogen activator survived, treatment having started 4 h after trauma (173).The relative importance of the lung fibrinolytic capacity was demonstrated by Saldeen, who injected thrombin intravenously into rats (174). After 5 to 10 min fibrin deposits were found regularly in small lung vessels, but less often after 15 to 30 min, and only in a few isolated vessels after 60 min. When rats were pretreated with EACA, the fibrin deposits were not eliminated from the lungs. The injection of human tissue thromboplastin into rats gave virtually the same response as seen for thrombin (175). After injection, the rats developed marked dyspnoea, which lasted from 5 to 15 min. When the dosage was increased, the animals died in respiratory distress. Defibrinogenation of animals prior to treatment with thrombin and tranexamic acid (AMCA), which inhibit plasminogen binding to fibrin, prevented
16

pulmonary insufficiency, whereas isolated leucopenia or thrombocytopenia did not (176).In the classical study by Sevitt and Gallagher on the prevention of pulmonary embolism in patients with hip fracture, autopsy studies were performed in patients who died during the study period (177). The incidence of lethal pulmonary emboli was 2% in patients who were given phenindione, while it was 14% in the control group. In the autopsy study on burned and injured patients by the same authors, deep vein thrombosis was demonstrated in 65% and pulmonary embolism in 16% (178). Later, Eeles and Sevitt found that lung microthrombosis was a frequent pathological finding in patients who died from trauma (179). Pulmonary microthrombosis was most often seen in patients who died within 3 h after trauma and in patients in whom injury and haemorrhage were severe. Microthrombi were less frequent in patients who died 2 or more days after injury, but in some cases, when microthrombi appeared, signs of organization were seen. Pulmonary arterial microthrombi and macro thrombi were found in 20% of patients who survived for more than a week (179). Lindquist et al performed autopsy studies on 28 patients who had sustained severe trauma, excluding patients with head injury and patients who died within 24 hours after trauma (180). They found pulmonary fibrin deposition in all the patients, and in 20 this was considered to be responsible for the fatal outcome. In the autopsy study by Kaufman et al on patients with severe head injury who died within the first 2 days after admission, microthrombi were frequently found in the brain, liver, and lungs (181). Blaisdell et al, in their autopsy study on patients who died after major vascular surgery, found that pulmonary microembolism was a common causative factor in postoperative mortality and morbidity (182). Trapping of radiolabelled fibrinogen in the lungs, determined by external detection of radioactivity, was demonstrated in patients who developed pulmo-nary insufficiency after trauma (183,184). The incidence of posttraumatic deep vein thrombosis, as determined by phlebography, is reported to range from 18% to 90%, with the highest risk in elderly patients and in patients with spinal injury (185). The risk of pulmonary embolism ranged from 4% to 22% (185). In a one-year retrospective review of 1316 patients who were admitted to a trauma centre, 30 cases of symptomatic pulmonary emboli, diagnosed by pulmonary angiography, were found, and 7 died from this complication (186). The experimental animal studies, the autopsy studies, and the clinical studies using paraclinical methods suggest that intravascular fibrin deposition in the form of macrothromboemboli or microthromboemboli is common after trauma, and the possibility that intravascular fibrin deposition may play a pathogenetic role in the development of posttraumatic organ dysfunction is likely. Consequently, an attractive approach would be to search for haemostatic tests which could identify
patients in whom posttraumatic organ dysfunction would develop, and predict a fatal outcome.
5.3 Relationship between injury severity and haemostatic testsHaemostatic abnormalities, as determined by con-ventional coagulation tests, are reported to be more pronounced in patients with severe head injury than in patients with less severe head injury, as quantified by the Glasgow Coma Score (GCS) or Cranial computer tomography scans (120,187,188). Virtually no statistical differences were observed in the posttraumatic levels of F1+2, TAT, FpA, FM, and FbDP when patients with isolated head injury were compared with patients with multiple trauma, al though the latter group showed a trend towards higher levels of all markers, and levels of TAT were significantly higher in the multiple trauma group (V, VI). Weak, but significant correlations were seen between admission levels of F1+2, TAT, FpA and the anatomically based Injury Severity Score (ISS) (189), whereas admission levels of fibrinogen were inversely correlated to the ISS. A correlation between the markers and the coma score, assessed by the GCS (190), was not detected, but this may be due to too few observations since only 14 patients had isolated head injury. In other studies, levels of D-dimer in the posttraumatic period were correlated to the ISS (126,191). In study VII, the plasma profibrinolytic and antifibri-nolytic factors, t-PA:ag, PAI-1:ag or PAI-1 activity, were not correlated to the ISS on any day, but levels of α-2-antiplasmin showed a weak correlation to the ISS on day 7. Levels of F1+2, TAT, FpA, FM, and FbDP were not significantly different in patients who received or did not receive blood transfusions (V,VI). On the other hand, posttraumatic levels of tPA:ag and PAI-1:ag were higher in patients who had 6 or more units of blood transfused during resuscitation (VII). Whether the observed differences are a consequence of haemorrhage or of multiple blood transfusions is at present not clear (VII).
5.4 Relationship between haemostatic tests and posttraumatic mortality and disseminated intravascular coagulation
Attar et al, in 1969, performed serial haemostatic analyses on 54 trauma patients during the initial hours after admission (192). In 15 patients who died, the silicone clotting time, prothrombin time, and partial thromboplastin time were significantly prolonged, compared with values in the surviving group. Levels of fibrinogen, platelets, VIII, IX, X, and plasminogen were significantly lower in the fatal cases. Thrombin time, antithrombin titre, plasminogen activator activity, and plasmin activity did not differ between survivors and fatal cases. The incidence of shock (arterial blood pressure below 90 mmHg) did not influence the haemostatic tests. No information was given concerning trauma score
17

or death from posttraumatic organ failure. Similar differences between survivors and nonsurvivors, using similar haemostatic tests, were observed in 18 American servicemen wounded in the Vietnam war (193). In a study on 15 trauma patients using serial chromogenic peptide substrate assays, plasma levels of prekallikrein, plasma Hageman factor, ATIII, and prothrombin were significantly lower in 6 patients who died from sepsis and/or posttraumatic adult respiratory distress syndrome (ARDS) (194); the fatal cases had raised serum FDP, whereas levels were within normal range in the survivors (195). Risberg et al studied 20 patients with multiple trauma, of whom 5 developed DIC (122). DIC was diagnosed by raised serum FDP, reduced platelet count, and a positive ethanol gelation test, in addition to the presence of clinical signs of diffuse bleeding or organ failure. 3 DIC patients died from multiple organ failure, and 4 non-DIC patients died, 3 from brain injury and one from pulmonary embolism. Early studies on patients with head injury suggested that the occurrence of DIC was a common phenomenon associated with a high mortality rate (116,196-198). Sande et al performed coagulation studies on 150 patients who were admitted after blunt head injury, of whom 10 died (114). Serum FDP levels were 80 µg/ml or more in 13 patients, eight of whom died. Miner et al studied 87 children with head injury, of whom 22 died (199). DIC was defined as the presence of 3 or more abnormal clotting tests among the prothrombin time, APTT, platelet counts, fibrinogen level, and serum FDP in samples taken within 2 h after admission. According to these criteria, 32% had DIC, and in these the mortality was 54%, compared with 12% in the patients without DIC. Even after correction for the severity of the injury, a clear relationship between 3 abnormal coagulation tests and mortality existed. Kumura et al used a similar definition of DIC in their study on 100 patients with head injury (200). 24 had DIC by these criteria, of whom 14 died, whereas only 5 of 76 patients without DIC died. A multivariate analysis showed that the levels of the APTT assay and the GCS were most closely correlated with the prognosis. Olson et al, in a study of 269 patients with isolated head injuries, registered admission GCS, platelet counts, prothrombin time, APTT, thrombin clotting assay, fibrinogen, serum FDP, and a DIC score based on these assays (187). No specific information was given concerning the cause of death of 96 patients. A stepwise logistic regression analysis demonstrated that the GCS, serum FDP levels, and DIC score had predictive value for mortality.
5.5 Relationship between haemostatic tests and the development of posttraumatic pulmonary
dysfunction Impairment of pulmonary function in patients who suffer trauma remote from the lungs has been known for many years, and the syndrome has been given
many names, including fat emboli syndrome, white lung syndrome, shock lung syndrome, traumatic wet lung, and pulmonary microembolism. The term Respiratory Distress Syndrome in Adults (ARDS) was introduced by Ashbaugh et al (201), who noted that the postmortem findings in trauma patients who died from respiratory failure were similar to those seen in infants who died from respiratory distress. The term ARDS was later widely adopted, but various clinical definitions have been used. The incidence of posttraumatic pulmonary dysfunction (PD) is between 6% and 20%, depending on the type of trauma and the definition used (172,202-204).In studies on patients with fractures of the lower limbs, it was noted that many patients had abnor-mally low levels of PaO2, which was interpreted as subclinical fat embolism (112,113). A connection between the fat embolism syndrome and the coagu-lation system was suggested, but this could not be established by measurement of platelets and fibrinogen. In the study by the author on patients with fractures of the lower extremities, the post-traumatic lung function was not quantified (III). Car-diopulmonary symptoms are very common after hip fracture in older patients, and the symptoms are often interpreted as pneumonia, myocardial infarction, or congestive heart failure. In the study by String et al, 40 patients with multiple trauma were divided into three groups according to the degree of posttraumatic PD (205). The first group consisted of 13 patients who needed ventilatory support for more than 3 days, and who had bilateral diffuse reticular infiltrates on chest X-ray. Many of these patients developed multiple organ failure. The second group consisted of 16 patients who developed only moderate degrees of PD, and respiratory support was limited to less than 3 days. The third group consisted of 11 patients with little or no evidence of PD. Coagulation changes were most severe in the first group, with low levels of coagulation factors I, II, V, VII, VIII, and IX, low thrombocyte counts, and high levels of FDP. Coagulation changes were less severe in the second and third groups. In that study, however, it was not stated when the blood samples were taken, and the severity of injuries was not quantified. Crone et al studied 33 patients with severe closed head injury with GCS less than 8 (206). Nine of 11 patients who had admission levels of serum FDP > 6 µg/ml developed ARDS during the first 2 days, compared with only 1 of 22 patients with serum FDP < 64 µg/ml. Schramm el al studied 52 polytrauma patients, of whom 24 developed ARDS (no definition was given) (207). PAI activity levels were significantly higher in patients with than without ARDS. The AT III levels were significantly lower in the ARDS group at 6 h, 12 h, and 24 h after the trauma. Levels of D-dimers were reported to be higher in the ARDS group, but this was not statistically significant. In another study the authors suggested that a secondary elevation of D-dimer levels was indicative of pathological
18

thrombosis since a patient with pulmonary embolism, another with ARDS, and a third with sepsis syndrome had highly raised levels 7 days after trauma, whereas patients without these complications had less raised levels (126).Seeger et al studied 25 multiple trauma patients by serial determinations of recalcification time (RT) in the presence or absence of phosphatidylethanoamine in bronchoalveolar lavage (BAL) fluid (208). 11 patients had a high ARDS score, and 14 a low score. With respect to age and ISS no significant difference existed between the 2 groups. The RT was lower in the patients than in healthy controls. Patients with a high ARDS score had significantly lower RT from day 4 to day 12 after trauma than patients with a low ARDS score. However, no such difference was seen during the initial 3 posttraumatic days. In another study on 8 patients with established ARDS (2 cases due to trauma), BAL fluid contained decreased urokinase activity, presumably due to inhibition by PAI-1, since urokinase antigen level was normal (209). In a similar study, plasminogen activator activity in the BAL fluid was depressed in 14 ARDS patients (6 cases due to trauma) and plasmin mediated fibrinolysis was low, but levels of plasminogen and α-2-antiplasmin were higher in the ARDS group (210). Both extrinsic pathway inhibitor activity and tissue factor procoagulant activity were higher in patients with ARDS compared with patients at risk of ARDS. In both these last named studies it was concluded that increased antifibrinolytic activity predisposed to alveolar fibrin deposition in ARDS. However, in these studies it is difficult to tell whether the reduced fibrinolytic capacity of BAL fluid had a pathophysiological role in the development of ARDS or was simply a consequence of ARDS. In the study by the author, admission plasma levels of F1+2, TAT, FpA, FM, or FbDP were highly raised, but no differences were observed in patients who later had PD compared with patients without PD (V,VI). Consumption and loss of coagulation zymogens during the initial minutes after trauma may have been more pronounced in the patients who later had PD, resulting in lower levels of coagulation zymogens. Therefore the possibility remains that a more marked activation of coagulation and fibrinolysis was overlooked in the patients with PD, since blood sampling in many cases was delayed 3-4 h after the trauma. Four patients who developed PD had significantly lower levels of F1+2 and FbDP on the day after admission than patients without PD. On the following days no difference was observed in levels of the markers when patients with and without PD were compared. Due to the low number of patients with PD, the statistical evaluation must be considered with reservation. However, the observations may suggest lower thrombin and plasmin activity in the patients with PD on the day after admission. On the other hand, since levels of TAT, FpA, and FM were
not lower in patients with PD, the finding of lower F1+2 levels in these patients seems unclear. The trend towards lower FbDP levels in patients with PD seems to be in accordance with previous observations, which suggest that the pulmonary fibrinolytic capacity is critical in the prevention of pulmonary fibrin deposition. On the other hand, consumption and loss of coagulation zymogens may have been more marked in these patients, resulting in a lower generation rate of F1+2 and FbDP. Further investigations concerning plasma levels of t-PA and PAI-1 and α-2-antiplasmin were performed on 19 patients who had sustained multiple trauma and of whom 4 developed PD. Levels of PAI-1 antigen, PAI-1 activity, t-PA antigen, and α-2-antiplasmin did not differ between patients with or without PD. The definition used for PD was based on an arbitrarily chosen level of a functional index for the respiratory function, which was used in a similar study (206). It is the author's experience that the majority of the trauma patients had considerable impairment of the respiratory function especially on day 1, as determined by the functional respiratory index; however, only 4 patients fulfilled the chosen criteria for PD.
5.6 ConclusionsPlasma levels of the different markers of coagulation and fibrinolysis seem to be correlated to some extent to the severity of the injury.The author's findings do not reject the hypothesis that the haemostatic system plays an important pathophysiological role in the development of PD after trauma. On the other hand, the haemostatic tests used in this study were unable to identify patients in whom PD developed. Any clinical relevance of these haemostatic tests in trauma patients has so far not been provided.
6 Perspectives of the haemostatic activation after tissue injury
6.1 IntroductionThe hypothesis of the previous chapters was that part of the fibrin that is generated after injury may be deposited in the wound, facilitating haemostasis, that a second part may immediately be degraded, resulting in FDP, and that a third part may be deposited somewhere in the vascular system, for a longer or a shorter period, as micro- or macrothromboemboli, causing more or less obstruction of blood flow. This chapter includes a presentation of the possible physiological reactions of fibrin/FDP located in the wound and possible pathophysiological reactions of fibrin/FDP in the vascular system. Based on these considerations, the author suggests a model for the interpretation of the possible linkages between
19

the haemostatic system, wound healing, organ dysfunction, and thromboembolism after surgery and trauma.
6.2 Fibrin and wound healing Fibrin deposition in wounds may be interpreted as a major defence mechanism against exsanguination, and may provide a physical framework on which inflammation and angiogenesis can occur, leading to repair and healing. The antigenic properties of fibrin and fibrin degradation products seem to be important (1,211), as well as the composition and concentration of the fibrin gel, which are determinative factors for cellular infiltration (212,213). The haemostatic activation process after trauma may therefore be the initial step in a cascade of inflammatory reactions, which leads to healing of the wound. However, inflammatory cells, including fibroblasts and macr-ophages, may aggregate on fibrin matrices which are not situated in a wound (212,213).
6.3 Fibrin/FDP and initiation of increased permeability and inflammationThe possible relationship between fibrin microemboli/FDP and increased endothelial permeability has been the object of several studies.Experimental observations suggest that pulmonary oedema following pulmonary thromboembolization with glass beads is due to secondary fibrin formation and not mechanical obstruction, since animals pre-trea ted with heparin did not develop pulmonary oedema (214). Increased pulmonary vascular permeability and increased leakage of protein in the pulmonary interstitial spaces were seen in dogs which were given thrombin and AMCA. Ultrastructural studies showed that the leakage occurred across the endothelial cells (215).It was observed in other experimental studies that fibrinogen degradation product D, when injected intravenously into rabbits, produced progressive PD and interstitial pulmonary oedema (216,217). A permeability increasing pentapeptide and an undecapeptide derived from fibrin and fibrinogen have been isolated (218). Oedema in the alveolar and interstitial spaces in the lungs is a common autopsy finding in patients who die from trauma (172). Damage to the alveolarcapillary membrane and aggregation of polymorphonuclear leucocytes are early morphological findings in trauma patients (219). In patients who have suffered ARDS for more than four days, fibroblast proliferation and deposits of collagen are superimposed (172). The possible effects of fibrin are illustrated in Fig. 6.
6.4 Haemostatic activation, wound healing, organ dysfunction, and thromboembolism after surgery and trauma
Immediately after trauma, procoagulant activity from wounds, and possibly from the spleen, may be released directly into the venous circulation,
promoting fibrin formation. It may be anticipated that most of the fibrin aggregates that are formed in the venous circulation will be trapped in the pulmonary microvascular system. When the blood then enters the arterial system it circulates for only a few seconds before it reaches a peripheral microvascular system, in which possible fibrin aggregates, formed during the passage from the lungs, are entrapped and lysed by the fibrinolytic system. On the other hand, when the blood returns to the venous system, the blood flow velocity is considerably lower than in the arterial system, about 5 cm/s (220). Relatively more fibrin may be generated during the blood passage from the peripheral veins to the pulmonary microvascular system than during the passage from the pulmonary circulation to the peripheral microvascular system. The lungs may thereby act as the organ of major importance in the clearance of intravascularly formed fibrin. Depending on the capacity of the fibrinolytic system in the lungs, the fibrin aggregates are quickly dissolved. If they are not quickly dissolved, the sequence of acute inflammatory reactions may ensue. These reactions may be a consequence of fibrin/FDP damage to the endothelial cells or of local activation and degranulation of polymorphonuclear leucocytes, macrophages, and platelets, including liberation of histamine, bradykinin, serotonin, and prostaglandins. This may result in increased capillary permeability with subsequent exudation and congestion of the pulmonary parenchyma. These changes may later be followed by reparative proliferation by leucocytes and fibroblasts, resembling the processes of wound healing. These processes may be reversible for a period, but if they last long enough they may become irreversible, leading to fibrosis and organ damage. These pathophysiological reactions may progress to involve other organs such as the kidneys, gastrointestinal tract, heart, and brain.The initial or early signs of PD after trauma may reflect both mechanical obstruction and acute pulmonary oedema due to the presence of fibrin and platelet plugs, whereas the later signs of organ dysfunction would be a consequence of progressive cellular inflammatory reactions. The fibrin, which primarily initiated the process, may be dissolved during the inflammatory steps. On the other hand, the inflammatory process may stimulate secondary coagulation activation, with fibrin formation and deposition. The initial hyperactivation of fibrin formation may be followed in the postoperative/traumatic period by a period of lowgrade increased fibrin formation, which may be a secondary phenomenon of the wound healing processes. Possible fibrin aggregates, formed in the leg veins and systemic veins in the postoperati-ve/traumatic period, may not adhere to the vein wall, but may be transferred directly to the pulmonary circulation as pulmonary microemboli or fibrin aggregates, where they may be cleared by the pulmonary fibrinolytic system. However, in individuals with a low potential to resist fibrin
20

deposition in the lungs, the continuing increased stimulation of fibrin formation may overwhelm the local capacity to degrade fibrin, leading to the pathophysiological reactions of acute inflammation. Fibrin aggregates may also be able to adhere to the vein wall, if the local defence mechanisms are unable to oppose fibrin and platelet deposition, and propagation to larger vein thrombi may then take place. The vein thrombus may break up into larger or smaller fragments giving rise to pulmonary emboli, or it may remain attached to the vein wall undergoing lysis or organization and superimposed inflammation, which may lead to vein fibrosis. As a consequence of impaired venous drainage of the extremity, the postthrombotic syndrome may later develop. Indeed, many pathogenetic mechanisms have been incriminated in the pathophysiology in ARDS and multiple organ failure (221-224). The suggested mechanisms include mediators of inflammation such as complement activation, neutrophil proteases, cyclooxygenase pathway products, oxygen radicals, lipoxygenase pathway products, and cytokines. After trauma and surgery, many patients suffer from cardiopulmonary symptoms, which are often considered to be pneumonia, myocardial infarction, or congestive heart failure. For the clinician it may be a very common experience that these patients do not improve when treated with antibiotics or diuretics. In many cases the symptoms disappear
during the postoperative period, but in others the cardiopulmonary function continues to deteriorate, and they remain unresponsive to treatment. Havig, studying a mixed population of hospital autopsies, noted that, in 70% of patients who died from a pulmonary embolus or multiple pulmonary emboli, the preceding symptoms were undramatically dominated by dyspnoea, tachycardia, cerebral symptoms, and often fever (225). The symptoms were incorrectly attributed to cardiac disease, pneumonia or cerebrovascular disease in 90% of these patients. These symptoms often occur in patients with a fractured hip in the posttraumatic/operative period. These patients are often older, and they often suffer from cardiopulmonary disease with only a marginal cardiopulmonary reserve capacity. Consequently, even a minor reduction of the pulmonary capacity would lead to a catastrophic impairment of oxygenation. In conclusion, the author finds it possible that the haemostatic activation followed by fibrin deposition in wounds should be considered as a major defence mechanism against bleeding after trauma. Furthermore, the author finds it possible that fibrin deposition in the wound initiates the wound healing processes by activation of the inflammatory reactions, which take over in the process of repair, proliferation, and angiogenesis in the wound. Deleterious effects may occur if the haemostatic activation becomes unbalanced, resulting in either an increased bleeding
21
FIGURE 6.Possible effects of fibrin after tissue injury (See text).

tendency or intravascular fibrin deposition such as micro- or macrothromboemboli. Intravascularly situated fibrin may as a direct consequence impair blood circulation or damage the endothelium and initiate the acute inflammatory cascade reactions, leading to accumulation of interstitial fluid with subsequent congestion and oedema of the involved organ. It is suggested that the majority of the intravascularly formed fibrin is normally cleared in the pulmonary microcirculation by the fibrinolytic system. If the fibrin aggregates trapped in the lungs are not dissolved shortly after their appearance, the sequence of acute inflammation and interstitial fluid accumulation may supervene. Later, the processes of cellular proliferation and tissue repair may take place. The organ in which the intravascular fibrin clots are situated is mistaken for a wound by the inflammatory systems.
6.5 Possible future implicationsThe treatment of trauma patients has improved during the past 20 years. The initial resuscitation with ventilatory support and stabilization of the circulation in order to obtain adequate tissue perfusion and avoid prolonged periods of hypoxaemia are considered to be of major importance (226). Early stabilization of fractures of the lower extremities in multiple trauma patients may reduce the risk of pulmonary and other complications in the posttraumatic period (227).Much attention has been given to the occurrence of non-symptomatic DVT after operations. Particularly in the past 15 years, an immense number of studies have been performed in order to prove that the incidence of non-symptomatic deep vein thrombosis can be reduced by anticoagulant drugs, and that some of these drugs are better and safer than others.The object of clinical trials should be improved care of the patients. In order to obtain this when testing a new treatment, variables such as morbidity and mortality should be the end point in clinical trials.The triggering mechanisms for PD after sepsis, pancreatitis, aspiration, and cancer may not be the same as for the development of PD after trauma. This may have to be considered when treatment or prophylaxis is directed against supposed causative factors. Trials for the investigation of potentially beneficial drugs should therefore include only welldefined patient groups with the same underlying disorder. Otherwise any potentially beneficial effect of the treatment under investigation could easily disappear.The suggested interactions between the haemostatic system and the system of inflammation and repair, which on one side lead to beneficial reactions and on the other side may lead to deleterious organ dys-function, give, at least theoretically, several options for interventions. Anticoagulants may moderate fibrin formation, and administration of fibrinolytic drugs may increase the capacity to dissolve fibrin. Pharmacological treatment by corticosteroids, prostaglandins, and N-acetylcysteine may moderate
the acute inflammation processes. Common to these drugs, when they are administrated to trauma patients, is that the potentially adverse effects may surpass the potentially beneficial effects. It is hoped that future studies will be able to elucidate whether trauma patients may benefit from treatment or prophylaxis by one or more of these drug categories.
7 SummaryThe recent development of immunochemical methods has made it possible to construct assays which can quantitate the activities of various steps of the haemostatic system by measurements of split products and enzyme inhibitor complexes. It has been suggested that these methods may provide more sensitive and accurate information about the existing coagulation and fibrinolytic status than conventional haemostatic tests. The present study is an attempt to describe the influence of surgery, fractures of the extremities, neurotrauma, and multiple trauma on the generation of specific molecular markers of coagulation and fibrinolysis by newly developed immunochemical assays. Furthermore, it attempts to evaluate possible relationships between clinicopathological findings after surgery and trauma and haemostatic activation. The development and principles of the different coagulation and fibrinolytic assays are briefly reviewed. Values for normal individuals and the assay reproducibility are given.The immediate effect of hip replacement surgery, isolated fractures of the hip, femur, and leg, isolated head injury, and multiple trauma on the haemostatic system is activation of both fibrinforming and fibrindegrading pathways, as measured by high levels of coagulation and fibrinolytic markers. This may be due to release of procoagulant activity from the wound and release of profibrinolytic activity, which may originate from the endothelium.At admission, patients with fractures of the lower extremities showed relatively strong correlations betwe en the different haemostatic markers, but on day 1 the correlations between the markers were weak or absent. This may suggest that the plasma half-lives of the markers are different.A temporary fall towards lower levels of the coagulation markers occurs during the first postoperative and posttraumatic days, but levels are above normal in the first week, suggesting continuing activation of coagulation. This may possibly reflect a secondary activation of the haemostatic system, promoted by the inflammatory processes in the wound healing sequence and procoagulant activity released when the haemostatic plugs are degraded. As indicated by increased levels of fibrin/fibrinogen degradation products, a secondary increase in fibrin degradation is observed between the 3rd and 7th days. This may reflect increased degradation of fibrin
22

as a response to oppose the increased fibrin formation in this period, degradation of fibrin in the wound, and degradation of intravascular fibrin. In the posttraumatic period the urinary excretion of fibrinopeptide A (FpA) is about 50-fold higher than in healthy controls with normal plasma levels of FpA. Likewise, prothrombin fragment 1+2 (F1+2) immunoreactivity is detected in the urine of trauma patients. The urinary immunoreactivity of F1+2 was higher than the corresponding plasma levels, and the excretion was almost 100 times that of healthy controls. This observation may suggest that the rate of fibrin formation was considerably higher than that indicated by plasma concentrations, which were only twice as high as normal.The fall in plasma profibrinolytic activity (decreased t-PA activity/increased PAI activity) has previously been interpreted as decreased or impaired fibrinolysis after surgery and trauma. However, the author suggests that the fall in plasma profibrinolytic activity may be due to activation of plasmin by increased t-PA adsorption onto fibrin, resulting in increased fibrin degradation and lower plasma levels of t-PA. The relationship between the occurrence of nonsymptomatic deep vein thrombosis (DVT) after surgery and haemostatic tests has been given much attention in the past. In the study by the author, levels of F1+2 and fibrin/fibrinogen degradation products were increased to a greater extent in patients in whom non-symptomatic DVT developed, as diagnosed by bilateral phlebography, than in patients without DVT.In the study on trauma patients, a weak correlation was observed between the trauma score, assessed by the Injury Severity Score, and levels of the haemostatic markers, with the exception of the profibrinolytic markers (t-PA and PAI).Levels of the haemostatic markers were not different when trauma patients who had received blood transfusions were compared with trauma patients who had no transfusions. On the other hand, posttraumatic levels of t-PA:ag and PAI-1:ag were higher in patients who had been transfused with 6 or more units of blood during resuscitation. It was observed that 4 patients who developed posttraumatic pulmonary dysfunction (PD) had significantly lower levels of F1+2 and FbDP on the day after admission than patients without PD.No clinical relevance of the haemostatic markers in surgery and trauma patients has yet been provided. On the other hand, the work by the author does not reject the hypothesis that the changes in the blood after surgery and trauma, as determined by the haemostatic markers, are a consequence of a dynamic haemostatic balance which is not only a local phenomenon, but is possibly a systemically activated condition with a subtle balance between intravascular formation and degradation of fibrin.Previous experimental studies, autopsy studies, and paraclinical studies suggest that the pulmonary microvascular system clears the surplus production
of fibrin microthromboemboli which follow after trauma and injections of tissue thromboplastin or thrombin. These fibrin thromboemboli may not promote tissue injury if they are cleared rapidly by the fibrinolytic system.Both fibrin and fibrin degradation products have a potent permeability increasing effect on the pulmonary endothelial cells, and, in accordance with this, the early signs of posttraumatic pulmonary dysfunction are characterized by alveolar and interstitial oedema. Fibrin in the wound may activate the woundhealing sequence by activating the inflammatory system. It is suggested that intravascular fibrin deposition may result in a reaction similar to wound healing. The organ in which the intravascular fibrin clots are situated is mistaken for a wound by the inflammatory systems; this may lead to irreversible wound healinglike reactions and organ damage. Thus it may be suggested that the haemostatic balance after surgery and trauma is of significance for the balance between localized inflammation (wound healing) and disseminated inflammation (organ damage).
8 Summary in DanishI de seneste år har udviklingen i immunologiske metoder gjort det muligt at konstruere analysemetoder, der er i stand til at måle spaltningsprodukter og enzyminhibitorkomplekser dannet ved aktivering af det hæmostatiske system. Det er foreslået, at metoderne kan kvantitere de forskellige enzymatiske reaktioner i det hæmostatiske system, og derved give et mere præcist billede af den aktuelle koagulations- og fibrinolysestatus end konventionelle koagulations- og fibrinolyseanalysemetoder.Formålet med forfatterens arbejde har været at undersøge, hvorledes hoftealloplastikkirurgi, underekstremitetsfrakturer, kranietraumer og multitraumer påvirker koagulations- og fibrinolysesystemet. Herudover er det forsøgt at finde mulige sammenhænge mellem det hæmostatiske system og kliniske fund og komplikationer efter kirurgi og traumer.Udviklingen af og principperne for de forskellige koagulations- og fibrinolyseanalyse metoder gennemgås kort, og de af forfatteren fundne værdier hos raske personer samt analysereproducerbarhed indenfor de enkelte analyser angives. Umiddelbart efter hoftealloplastikkirurgi, underekstremitetsfrakturer, kranietraumer og multitraumer ses et betydeligt øget plasmaindhold af såvel koagulations- og fibrinolysemarkører. Disse fund tyder på en systemisk forøgelse af koagulations- og fibrinolyseaktiviteten med en betydelig øget fibrinomsætning. Udløsende årsag er formentlig frigivelse af vævstromboplastin fra de traumatiserede områder og afgivelse af profibrinolytiske faktorer fra karvæggen.Kort efter et vævstraume ses en god korrelation mellem de forskellige markører, men i løbet af det næste døgn ses en dårlig eller manglende korrelation
23

mellem de forskellige markører. Dette kunne tyde på, at halveringstiden for markørerne er forskellige efter traume.I de efterfølgende 2-3 dage falder plasmaindholdet af koagulationsmarkører, men forbliver over normalområdet i den første uge, hvilket tyder på en kontinuerlig koagulationsaktivering i den post opera-tive/posttraumatiske fase.Fra tredje til syvende dag ses en sekundær stigning af fibrinolysemarkører målt som degraderingsprodukter af fibrin og fibrinogen. Dette kunne tyde på en sekundær degradering af fibrin, hvilket kan være et udtryk for øget dannelse af fibrin i denne periode, nedbrydning af fibrin lokaliseret i såret samt nedbrydning af intravaskulært lokaliseret fibrin.Efter multitraume falder plasmakoncentrationen af protrombin fragment 1+2 (F1+2) og fibrinopeptid A (FpA) til ca. det dobbelte af plasmakoncentrationen hos normale, hvorimod urinudskillelsen af F1+2 og FpA er 50 til 100 gange højere hos traumepatienter end hos normale raske personer. Der fandtes en god korrelation mellem urinudskillelsen og plasmakoncentrationen af F1+2. Disse resultater kunne tyde på, at koagulationsomsætningen er betydelig større hos disse patienter end hvad plasmakoncentrationer umiddelbart afslører.Den profibrinolytiske aktivitet i plasma falder i løbet af det første døgn efter kirurgi og traumer (faldende t-PA aktivitet/stigende PAI aktivitet). Dette er konventionelt opfattet som udtryk for, at fibrinolysen er nedsat i det postoperative/posttraumatiske forløb. Forfatteren foreslår, at den lave profibrinolytiske aktivitet i plasma kunne skyldes, at profibrinolytiske faktorer (t-PA) i plasma binder sig til fibrin og aktiverer plasmin, hvorved fibrinnedbrydningen øges, men plasmaindholdet af profibrinolytiske faktorer falder.Sammenhængen mellem forekomsten af dyb venøs trombose efter kirurgi og hæmostatiske test har gennem tiderne været genstand for stor interesse. I forfatterens undersøgelser sås en tendens til højere plasmakoncentrationer af F1+2 og fibrin/fibrinogen degraderingsprodukter hos patienter, som fik diagnosticeret ikke symptomgivende DVT ved flebografi sammenlignet med patienter med negativ flebografi.I forfatterens undersøgelser på traumepatienter sås en svag korrelation mellem koagulations- og fibrinolysemarkører og traumestørrelsen beregnet med "The Injury Severity Score" (ISS), hvorimod de profibrinolytiske aktivatorer og inhibitorer ikke var korreleret til ISS. Koagulations- og fibrinolysemarkørerne var ikke forskellige hos traumepatienter, som fik blodtransfusioner sammenlignet med traumepatienter, der ikke fik blodtransfusioner. Patienter, der under den primære behandling fik 6 eller flere blodtransfusioner, havde i den posttraumatiske fase højere plasmakoncentrationer af profibrinolytiske aktivatorer og inhibitorer (t-PA/PAI).Hos patienter, der udviklede posttraumatisk
lungedysfunktion fandtes signifikant lavere værdier af F1+2 og fibrin degraderingsprodukter dagen efter traumet. Herudover fandtes ingen forskelle i plasmakoncentrationer af de forskellige markører ved sammenligningen mellem patienter med og uden posttraumatisk lungedysfunktion. Forfatterens undersøgelser tyder på, at de hæmostatiske reaktioner efter vævslæsion er i en dynamisk og aktiveret tilstand, som ikke kun er et lokalt fænomen i området ved vævslæsionen, men formentlig en systemisk aktiveret reaktion med en hårfin balance mellem intravaskulær dannelse og nedbrydning af fibrin. Herudover har forfatterens undersøgelser ikke afsløret nogen klinisk anvendelighed af de hæmostatiske markører. Tidligere eksperimentelle studier, autopsi studier og parakliniske studier tyder på, at lungekredsløbet fjerner "overskudsproduktionen" af mikrotromboembolier, som umiddelbart efter traumer eller efter indgift af vævstromboplastin eller trombin føres til lungekredsløbet. Mikrotromboembolierne når formentlig ikke at gøre nogen skade, hvis det fibrinolytiske system er i stand til hurtigt at opløse dem.Både mikrotromber og fibrin degraderingsprodukter har en betydelig permeabilitets øgende effekt på endotelcellerne i lungekredsløbet og i overensstemmelse hermed er det primære billede på posttraumatisk lungedysfunktion præget af alveolært og interstitielt lungeødem.Fibrin i såret aktiverer det inflammatoriske system og starter formentlig sårhelingsreaktionen. Det foreslås, at fibrinmikrotromboembolier lokaliseret i det mikrovaskulære kredsløb også er i stand til at aktivere sårhelingsreaktionen. D.v.s. at organismen fejlkender dette mikrovaskulære kredsløb som et sår (f.eks. lungekredsløbet), og følgen kan i værste fald være en irreversibel sårhelingsreaktion og organskade. Derfor foreslås det, at den dynamiske hæmostatiske balance efter kirurgi og traumer har betydning for balancen mellem lokaliseret inflammation (sårhelingsreaktion) og dissemineret inflammation (organskade).
9 References1. Thompson WD, Harvey JA, Kazmi MA, Stout
AJ. Fibrinolysis and angiogenesis in wound healing. J Pathol 165:311-318; 1991.
2. Astrup T. Fibrinolysis of the organism. Blood
11:781-806; 1956.
3. Marder VJ, Francis CW. Physiological balance of haemostasis and bleeding. Drugs 33 Suppl 3:13-21; 1987.
4. Hewson, W. The works of William Hewson,
London:Sydenham Society, 1846. 5. Gray H, Lunt LK. Factors affecting the
24

coagulation time of blood. Am J Physiol 34:332-351; 1914.
6. Bergquist G. Changes in blood in connection
with thromboembolism, An investigation regarding operation and delivery (Thesis). Acta Chir Scand Suppl (101) 92:1-132; 1945.
7. Macfarlane RG, Biggs R. Observations on fibri-
nolysis spontaneous activity associated with surgical operations, trauma. Lancet ii:862-864; 1946.
8. Warren R, Amdur MO, Belko J, Baker DV.
Postoperative alterations in the coagulation mechanism of the blood. Observations on circulating thromboplastin. Arch Surg 61:419-432; 1950.
9. Bauer KA, Rosenberg RD. The pathophysiology
of the prethrombotic state in humans: insights gained from studies using markers of the hemostatic system activation. Blood 70:343-350; 1987.
10. Mannucci PM, Giangrande PLF. Detection of
the prethrombotic state due to procoagulant imbalance. Eur J Haematol 48:65-69; 1992.
11. Aronson DL, Stevan L, Ball AP, Franza BRJ, Finlayson JS. Generation of the combined prothrombin activation peptide (F1+2) during the clotting of blood and plasma. J Clin Invest 60:1410-1418; 1977.
12. Lau HK, Rosenberg JS, Beeler DL, Rosenberg
RD. The isolation and characterization of a specific antibody population directed against the prothrombin activation fragments F2 and F1 + 2. J Biol Chem 254:8751-8761; 1979.
13. Teitel JM, Bauer KA, Lau HK, Rosenberg RD.
Studies of the prothrombin activation pathway utilizing radioimmunoassays for the F2/F1 + 2 fragment and thrombin/antithrombin complex. Blood 59:1086-1097; 1982.
14. Bauer KA, Goodman TL, Kass BL, Rosenberg
RD. Elevated factor Xa activity in the blood of asymptomatic patients with congenital antithrombin deficiency. J Clin Invest 76:826-836; 1985.
15. Bauer KA, Weiss LM, Sparrow D, Vokonas PS,
Rosenberg RD. Aging associated changes in indices of thrombin generation and protein C activation in humans. Normative Aging Study. J Clin Invest 80:1527-1534; 1987.
16. Pelzer H, Schwarz A, Stuber W. Determination
of human prothrombin activation fragment 1 + 2 in plasma with an antibody against a synthetic peptide. Thromb Haemost 65:153-159; 1991.
17. Rahr HB, Sørensen JV, Danielsen D.
Haemostatic activation products in blood samples drawn into citrate with and without D-Phe-Pro-Arg-Chloromethylketone (PPACK). Thromb Res 73:279-284; 1994.
18. Shifman MA, Pizzo SV. The in vivo metabo-
lism of antithrombin III and antithrombin III complexes. J Biol Chem 257:3243-3248; 1982.
19. Lau HK, Rosenberg RD. The isolation
and characterization of a specific antibody population directed against the thrombin antithrombin complex. J Biol Chem 255:5885-5893; 1980.
20. Pelzer H, Schwarz A, Heimburger N.
Determination of human thrombinantithrombin III complex in plasma with an enzymelinked immunosorbent assay. Thromb Haemost 59:101-106; 1988.
21. Hoek JA, Sturk A, ten Cate JW, Lamping RJ,
Berends F, Borm JJ. Laboratory and clinical evaluation of an assay of thrombin/antithrombin III complexes in plasma. Clin Chem 34:2058-2062; 1988.
22. Nossel HL, Younger LR, Wilner GD, Procupez
T, Canfield RE, Butler VPJ. Radioimmunoassay of human fibrinopeptide A. Proc Natl Acad Sci U S A 68:2350-2353; 1971.
23. Nossel HL, Yudelman I, Canfield RE, Butler
VPJ, Spanondis K, Wilner GD, Qureshi GD. Measurement of fibrinopeptide A in human blood. J Clin Invest 54:43-53; 1974.
24. Nossel HL, Ti M, Kaplan KL, Spanondis
K, Soland T, Butler VPJ. The generation of fibrinopeptide A in clinical blood samples: evidence for thrombin activity. J Clin Invest 58:1136-1144; 1976.
25. Haeberli, A. Fibrinopeptide A (FPA). In: ECAT
Assay Procedures, A manual of laboratory techniques, edited by Jespersen, J., Bertina, R.M. and Haverkate, F. Dordrecht, Boston, London: Kluwer Academic Publishers, 1992, p. 109-116.
26. Alkjaersig N, Fletcher AP. Catabolism and
excretion of fibrinopeptide-A. Blood 60:148-156; 1982.
25

27. Gallino A, Haeberli A, Straub PW. Fibrinopeptide A excretion in urine in patients with atherosclerotic artery disease. Thromb Res 39:237-244; 1985.
28. Leeksma OC, Meijer Huizinga F, Stoepman
van Dalen EA, van Aken WG, van Mourik JA. Fibrinopeptide A in urine from patients with venous thromboembolism, disseminated intravascular coagulation and rheumatoid arthritis evidence for dephosphorylation and carboxyterminal degradation of the peptide by the kidney. Thromb Haemost 54:792-798; 1985.
29. Wilensky RL, Zeller JA, Wish M, Tulchinsky
M. Urinary fibrinopeptide A levels in ischemic heart disease. J Am Coll Cardiol 14:597-603; 1989.
30. Tulchinsky M, Zeller JA, Reba RC. Urinary
fibrinopeptide A in evaluation of patients with suspected acute pulmonary embolism. A prospective pilot study. Chest 100:394-398; 1991.
31. Soria J, Soria C, Ryckewaert JJ. A solid
phase immuno enzymological assay for the measurement of human fibrinopeptide A. Thromb Res 20:425-435; 1980.
32. Godal HC, Abildgaard U. Gelation of soluble
fibrin in plasma by ethanol. Scand J Haematol 3:342-350; 1966.
33. Seaman AJ. The recognition of intravascular
clotting. The plasma protamine paracoagulation test. Arch Intern Med 125:1016-1021; 1970.
34. Wiman B, Rånby M. Determination of soluble
fibrin in plasma by a rapid and quantitative spectrophotometric assay. Thromb Haemost 55:189-193; 1986.
35. Halvorsen S, Skjonsberg OH, Ruyter R, Godal
HC. Comparison of methods for detecting soluble fibrin in plasma. An in vitro study. Thromb Res 57:489-497; 1990.
36. Halvorsen S, Skjonsberg OH, Godal HC.
The stimulatory effect of soluble fibrin on plasminogen activation by tissue plasminogen activator as studied by the Coaset Fibrin Monomer test. Thromb Res 61:453-461; 1991.
37. Halvorsen S, Skjonsberg OH, Godal HC.
Comparison of methods for detecting soluble fibrin in plasma from patients with venous thromboembolism. Thromb Res 61:341-348; 1991.
38. Francis CW, Marder VJ, Barlow GH.
Plasmic degradation of crosslinked fibrin.
Characterization of new macromolecular soluble complexes and a model of their structure. J Clin Invest 66:1033-1043; 1980.
39. Allington MJ. Fibrinogen and fibrin degradation
products and the clumping of staphylococci by serum. Br J Haematol 13:550-567; 1967.
40. Merskey C, Lalezari P, Johnson AJ. A rapid,
simple, sensitive method for measuring fibrino-lytic split products in human serum. Proc Soc Exp Biol Med 131:871-875; 1969.
41. Gordon YB, Martin MJ, McNeile AT, Chard
T. Specific and sensitive determination of fibrinogen degradation products by radioimmunoassay. Lancet ii:1168-1170; 1973.
42. Gaffney PJ, Perry MJ. Unreliability of current
serum fibrin degradation product (FDP) assays. Thromb Haemost 53:301-302; 1985.
43. Nieuwenhuizen, W. Quantitative enzyme
immunoassays for degradation products of fibrinogen (FgDP), fibrin (FbDP) and total of FgDP and FbDP (TDP). In: ECAT Assay Procedures, A manual of laboratory techniques, edited by Jespersen, J., Bertina, R.M. and Haverkate, F. Dordrect, Boston, London: Kluwer Academic Publishers, 1992, p. 191-203.
44. Boisclair MD, Ireland H, Lane DA. Assessment of hypercoagulable states by measurement of activation fragments and peptides. Blood Rev 4:25-40; 1990.
45. Koopman J, Haverkate F, Koppert P,
Nieuwenhuizen W, Brommer EJ, Van der Werf WG. New enzyme immunoassay of fibrinfibrinogen degradation products in plasma using a monoclonal antibody. J Lab Clin Med 109:75-84; 1987.
46. Koppert PW, Kuipers W, Hoegee de Nobel B,
Brommer EJ, Koopman J, Nieuwenhuizen W. A quantitative enzyme immunoassay for primary fibrinogenolysis products in plasma. Thromb Haemost 57:25-28; 1987.
47. Koppert PW, Hoegee de Nobel E, Nieuwenhuizen
W. A monoclonal antibody based enzyme immunoassay for fibrin degradation products in plasma. Thromb Haemost 59:310-315; 1988.
48. Rylatt DB, Blake AS, Cottis LE, Massingham
DA, Fletcher WA, Masci PP, Whitaker AN, Elms M, Bunce I, Webber AJ, et al . An immunoassay for human D dimer using monoclonal antibodies. Thromb Res 31:767-778; 1983.
49. Wiman B, Collen D. Molecular mechanism of
physiological fibrinolysis. Nature 272:549-550; 1978.
26
50. Chakrabarti R, Bielawiec M, Evans JF, Fearnley
GR. Methodological study and a recommended technique for determining the euglobulin lysis time. J Clin Pathol 21:698-701; 1968.
51. Juhan-Vauge, I. and Alessi, M.C. Tissue type
plasminogen activator antigen (t-PA Ag). In: ECAT Assay Procedures, A manual of laboratory techniques, edited by Jespersen, J., Bertina, R.M. and Haverkate, F. Dordrect, Boston, London: Kluwer Academic Publishers, 1992, p. 131-138.
52. Holvoet P, Cleemput H, Collen D. Assay of
human tissue-type plasminogen activator (t-PA) with an enzymelinked immunosorbent assay (ELISA) based on three murine monoclonal antibodies to t-PA. Thromb Haemost 54:684-687; 1985.
53. Declerck PJ, Alessi MC, Verstreken M, Kruithof
KO, Juhan-Vauge I, Collen D. Measurement of plasminogen activator inhibitor 1 in biological fluids with a murine monoclonal antibody based enzyme linked immunosorbent assay. Blood 71:220-225; 1988.
54. Chmielewska J, Wiman B. Determination of
tissue plasminogen activator and its "fast" inhibitor in plasma. Clin Chem 32:482-485; 1986.
55. Starup U. Undersøgelser over blodets
koagulationstid i tilslutning til operationer. Nord Med 16:2876-2881; 1942.
56. Sharnoff JG, Bagg JF, Breen SR, Rogliano AG,
Walsh AR, Scardino V. The possible indication of postoperative thromboembolism by platelet counts and blood coagulation studies in the patient undergoing extensive surgery. Surg Gynecol Obstet 111:469; 1960.
57. Melissari E, Scully MF, Paes T, Ellis V, Kakkar
VV. The influence of DDAVP infusion on the coagulation and fibrinolytic response to surgery. Thromb Haemost 55:54-57; 1986.
58. Modig J, Busch C, Olerud S, Saldeen T,
Waernbaum G. Arterial hypotension and hypoxaemia during total hip replacement: the importance of thromboplastic products, fat embolism and acrylic monomers. Acta Anaesthesiol Scand 19:28-43; 1975.
59. Donadoni R, Baele G, Devulder J, Rolly G.
Coagulation and fibrinolytic parameters in patients undergoing total hip replacement: influence of the anaesthesia technique. Acta Anaesthesiol Scand 33:588-592; 1989.
60. Modig J, Malmberg P. Pulmonary and circulatory reactions during total hip replacement surgery. Acta Anaesthesiol Scand 19:219-237; 1975.
61. Andersson L, Nilsson IM, Olow B. Fibrinolytic
activity in man during surgery. Thromb Diath Haemorrhag 7:391-403; 1962.
62. Griffiths NJ, Woodford M, Irving MH. Plasma
fibrinolytic inhibitors after operation. Surg Gynecol Obstet 144:673-676; 1977.
63. Macintyre IM, Webber RG, Crispin JR, Jones
DR, Wood JK, Allan NC, Prescott RJ, Ruckley CV. Plasma fibrinolysis and postoperative deep vein thrombosis. Br J Surg 63:694-697; 1976.
64. Giercksky KE, Bjorklid E, Prydz H, Renck H.
Circulating tissue thromboplastin during hip surgery. Eur Surg Res 11:296-300; 1979.
65. Gitel SN, Salvati EA, Wessler S, Robinson HJJ,
Worth MHJ. The effect of total hip replacement and general surgery on antithrombin III in relation to venous thrombosis. J Bone Joint Surg Am 61:653-656; 1979.
66. Seyfer AE, Seaber AV, Dombrose FA, Urbaniak
JRU. Coagulation changes in elective surgery and trauma. Ann Surg 193:210-213; 1981.
67. Sandset PM, Hogevold HE, Lyberg T, Andersson
TR, Abildgaard U. Extrinsic pathway inhibitor in elective surgery: a comparison with other coagulation inhibitors. Thromb Haemost 62:856-860; 1989.
68. Dahl OE, Molnar I, Vinje A, Ro JS, Kierulf
P, Andersen AB, Dalaker K, Prydz H. Studies on coagulation, fibrinolysis, kallikreinkinin and complement activation in systemic and pulmonary circulation during hip arthroplasty with acrylic cement. Thromb Res 50:875-884; 1988.
69. Wilson J, Grant PJ, Davies JA, Boothby M, Gaffney PJ, Prentice CR. The relationship between plasma vasopressin and changes in coagulation and fibrinolysis during hip surgery. Thromb Res 51:439-445; 1988.
70. Dahl OE, Johnsen H, Kierulf P, Molnar I, Ro
JS, Vinje A, Mowinckel P. Intrapulmonary thrombin generation and its relation to monomethylmethacrylate plasma levels during hip arthroplasty. Acta Anaesthesiol Scand 36:331-335; 1992.
71. Dahl OE, Pedersen T, Kierulf P, Westvik B, Lund
P, Arnesen H, Sjeleflot I, Abdelnoor M, Lyberg T. Sequential intrapulmonary and systemic activation of coagulation and fibrinolysis during
27

and after total hip replacement surgery. Thromb Res 70:451-458; 1993.
72. Grant PJ, Tate GM, Davies JA, Williams
NS, Prentice CR. Intraoperative activation of coagulation a stimulus to thrombosis mediated by vasopressin? Thromb Haemost 55:104-107; 1986.
73. Kambayashi J, Sakon M, Yokota M, Shiba E,
Kawasaki T, Mori T. Activation of coagulation and fibrinolysis during surgery, analyzed by molecular markers. Thromb Res 60:157-167; 1990.
74. Eriksson BI, Hultman E, Martinell S, Eriksson
E, Tengborn L, Risberg B. Regional fibrinolysis following total hip replacement. Thromb Res 62:441-447; 1991.
75. Kang J, Kambayashi J, Sakon M, Tsujinaka T,
Mori T. Postoperative changes in hemostasis analyzed by the serial determination of fibrinopeptides and D-dimer. Jpn J Surg 19:262-268; 1989.
76. Ygge J. Changes in blood coagulation and
fibrinolysis during the postoperative period. Am J Surg 119:225-232; 1970.
77. Rem J, Feddersen C, Brandt MR, Kehlet H.
Postoperative changes in coagulation and fibrinolysis independent of neurogenic stimuli and adrenal hormones. Br J Surg 68:229-233; 1981.
78. Hawkey CJ, Stirling Y, Chakrabarti R, Brozovic
M, Cox AG, Meade TW. Haemostatic changes following surgery. Thromb Res 32:223-227; 1983.
79. Fredin H, Nilsson B, Rosberg B, Tengborn L.
Pre- and postoperative levels of antithrombin III with special reference to thromboembolism after total hip replacement. Thromb Haemost 49:158-161; 1983.
80. Douglas JT, Blamey SL, Lowe GD, Carter
DC, Forbes CD. Plasma betathromboglobulin, fibrinopeptide A and B beta 15-42 antigen in relation to postoperative DVT, malignancy and stanozolol treatment. Thromb Haemost 53:235-238; 1985.
81. Torngren S, Noren I, Savidge G. The effect of
lowdose heparin on fibrinopeptide A, platelets, fibrinogen degradation products and other haemostatic parameters measured in connection with intestinal surgery. Thromb Res 14:871-879; 1979.
82. Rahr HB, Sørensen JV, Larsen JF, Jensen FS,
Bredahl C, Nieuwenhuizen W. Haemostatic activation before and after surgery in patients with and without gastric malignancy. Thromb Haemost 71:713-718; 1994.
83. Bostrom S, Holmgren E, Jonsson O, Lindstrom
B, Stigendal L. Fibrinopeptide A and fibrinogen fragment B beta 15-42 and their relation to the operative trauma and postoperative thromboembolism in neurosurgical patients. Acta Neurochir Wien 88:49-55; 1987.
84. Owen J, Kvam D, Nossel HL, Kaplan KL,
Kernoff PB. Thrombin and plasmin activity and platelet activation in the development of venous thrombosis. Blood 61:476-482; 1983.
85. Lane DA, Ireland H, Wolff S, Grant R, Jennings
S, Allen Mersh T. Plasma concentrations of fibrinopeptide A, fibrinogen fragment B beta 1-42 and betathromboglobulin following total hip replacement. Thromb Res 26:111-118; 1982.
86. Hoek JA, Nurmohamed MT, ten Cate JW, Buller
HR, Knipscheer HC, Hamelynck KJ, Marti RK, Sturk A. Thrombinantithrombin III complexes in the prediction of deep vein thrombosis following total hip replacement. Thromb Haemost 62:1050-1052; 1989.
87. Jørgensen LN, Lind B, Hauch O, Leffers
A, Albrecht Beste E, Konradsen LA. Thrombinantithrombin III-complex & fibrin degradation products in plasma: surgery and postoperative deep venous thrombosis. Thromb Res 59:69-76; 1990.
88. Ofosu FA, Levine M, Craven S, Dewar L, Shafai
S, Blajchman MA. Prophylactically equivalent doses of Enoxaparin and unfractionated heparin inhibit in vivo coagulation to the same extent. Br J Haematol 82:400-405; 1992.
89. Bogaty Yver J, Samama M. Throm-
binantithrombin III complexes for the detection of postoperative hypercoagulable state in surgical patients receiving heparin prophylaxis [letter]. Thromb Haemost 61:538; 1989.
90. Mansfield AO. Alteration in fibrinolysis
associated with surgery and venous thrombosis. Br J Surg 59:754-757; 1972.
91. Chakrabarti R, Hocking ED, Fearnley GR.
Reaction pattern to three stresses-electroplexy, surgery, and myocardial infarction-of fibrinolysis and plasma fibrinogen. J Clin Pathol 22:659-662; 1969.
92. Sautter RD, Myers WO, Ray JF, Wenzel
28

FJ. Relationship of fibrinolytic system to postoperative thrombotic phenomena. Arch Surg 107:292-296; 1973.
93. Paramo JA, Rocha E. Changes in coagulation
and fibrinolysis after total hip replacement and their relations with deep vein thrombosis. Haemostasis 15:345-352; 1985.
94. Aranda A, Paramo JA, Rocha E. Fibrinolytic
activity in plasma after gynecological and urological surgery. Haemostasis 18:129-134; 1988.
95. Browse NL, Gray L, Morland M. Changes in
the blood fibrinolytic activity after surgery (the effect of deep vein thrombosis and malignant disease). Br J Surg 64:23-27; 1977.
96. Gordon Smith IC, Hickman JA, Le Quesne LP.
Postoperative fibrinolytic activity and deep vein thrombosis. Br J Surg 61:213-218; 1974.
97. Reilly DT, Burden AC, Fossard DP. Fibrinolysis
and the prediction of postoperative deep vein thrombosis. Br J Surg 67:66-68; 1980.
98. Kluft C, Jie AF, Lowe GD, Blamey SL,
Forbes CD. Association between postoperative hyperresponse in t-PA inhibition and deep vein thrombosis [letter]. Thromb Haemost 56:107; 1986.
99. Kluft C, Verheijen JH, Jie AF, Rijken DC,
Preston FE, Sue Ling HM, Jespersen J, Aasen AO. The postoperative fibrinolytic shutdown: a rapidly reverting acute phase pattern for the fastacting inhibitor of tissue-type plasminogen activator after trauma. Scand J Clin Lab Invest 45:605-610; 1985.
100. Paramo JA, de Boer A, Colucci M, Jonker JJ,
Collen D. Plasminogen activator inhibitor (PA-inhibitor) activity in the blood of patients with deep vein thrombosis [letter]. Thromb Haemost 54:725; 1985.
101. Eriksson BI, Eriksson E, Gyzander E, Teger
Nilsson AC, Risberg B. Thrombosis after hip replacement. Relationship to the fibrinolytic system. Acta Orthop Scand 60:159-163; 1989.
102. Eriksson BI, Eriksson E, Risberg B. Impaired
fibrinolysis and postoperative thromboembolism in orthopedic patients. Thromb Res 62:55-64; 1991.
103. Sørensen JV, Borris LC, Lassen MR, Christiansen
HM, Schøtt P, Olsen AD, Neerstrand HS. Association between plasma levels of tissue plasminogen activator and postoperative deep vein thrombosis-influence of prophylaxis with a
low molecular weight heparin. Thromb Res 59:131-138; 1990.
104. Francis CW, Alkjaersig N, Galanakis DK, Graeff
H, Owen J, Gaffney P, Marder VJ. Terminology for macromolecular plasmic derivatives of crosslinked fibrin. Thromb Haemost 57:110-111; 1987.
105. Rowbotham BJ, Whitaker AN, Harrison
J, Murtaugh P, Reasbeck P, Bowie EJ. Measurement of crosslinked fibrin derivatives in patients undergoing abdominal surgery: use in the diagnosis of postoperative venous thrombosis. Blood Coagul Fibrinoly 3:25-31; 1992.
106. Borris LC, Sørensen JV, Lassen MR, Walenga
JM, Fareed J, Jørgensen LN, Hauch O, Wille Jørgensen P. Components of coagulation and fibrinolysis during thrombosis prophylaxis with a low molecular weight heparin (Enoxaparin) versus Dextran 70 in hip arthroplasty. Thromb Res 63:21-28; 1991.
107. Melissari E, Scully MF, Paes T, Kakkar VV. The
influence of LMW heparin on the coagulation and fibrinolytic response to surgery. Thromb Res 37:115-126; 1985.
108. Bredbacka S, Blomback M, Hagnevik K, Irestedt
L, Raabe N. Per- and postoperative changes in coagulation and fibrinolytic variables during abdominal hysterectomy under epidural or general anaesthesia. Acta Anaesthesiol Scand 30:204-210; 1986.
109. Modig J, Borg T, Bagge L, Saldeen T. Role
of extradural and of general anaesthesia in fibrinolysis and coagulation after total hip replacement. Br J Anaesth 55:625-629; 1983.
110. Simpson PJ, Radford SG, Forster SJ, Cooper
GM, Hughes AO. The fibrinolytic effects of anaesthesia. Anaesthesia 37:3-8; 1982.
111. Richard LC, Buller HR, Bovilland J, ten Cate
JW. Influence of anaesthesia on coagulation and fibrinolytic proteins. Br J Anaesth 55:869-872; 1983.
112. Wilson RF, McCarthy B, LeBlanc LP, Mammen
E. Respiratory and coagulation changes after uncomplicated fractures. Arch Surg 106:395-399; 1973.
113. Riseborough EJ, Herndon JH. Alterations
in pulmonary function, coagulation and fat metabolism in patients with fractures of the lower limbs. Clin Orthop 248-267; 1976.
114. van der Sande JJ, Veltkamp JJ, Boekhout Mussert RJ, Bouwhuis Hoogerwerf ML. Head
29

injury and coagulation disorders. J Neurosurg 49:357-365; 1978.
115. Innes D, Sevitt S. Coagulation and fibrinolysis
in injured patients. J Clin Pathol 17:1-13; 1964. 116. Goodnight SH, Kenoyer G, Rapaport SI, Patch
MJ, Lee JA, Kurze T. Defibrination after braintissue destruction: a serious complication of head injury. N Engl J Med 290:1043-1047; 1974.
117. Borowiecki B, Sharp AA. Trauma and
fibrinolysis. J Trauma 9:522-536; 1969. 118. Sefrin P, Brunswig D, Seyboldt A. Dynamics
of blood coagulation disorders in traumatic hemorrhagic shock. Chirurg 48:227-231; 1977.
119. Kapsch DN, Metzler M, Harrington M, Mitchell
FL, Silver D. Fibrinolytic response to trauma. Surgery 95:473-478; 1984.
120. Ueda S, Fujitsu K, Fujino H, Sekino T, Kuwabara T. Correlation between plasma fibrinfibrinogen degradation product values and CT findings in head injury. J Neurol Neurosurg Psychiatry 48:58-60; 1985.
121. Touho H, Hirakawa K, Hino A, Karasawa J,
Ohno Y. Relationship between abnormalities of coagulation and fibrinolysis and postoperative intracranial hemorrhage in head injury. Neurosurgery 19:523-531; 1986.
122. Risberg B, Medegard A, Heideman M, Gyzander
E, Bundsen P, Oden M, Teger Nilsson AC. Early activation of humoral proteolytic systems in patients with multiple trauma. Crit Care Med 14:917-925; 1986.
123. Gando S, Tedo I, Kubota M. Posttrauma
coagulation and fibrinolysis. Crit Care Med 20:594-600; 1992.
124. Lampl L, Seifried E, Tisch M, Helm M,
Maier B, Bock KH. Hemostatic disorders following polytrauma - the role of physiologic coagulation inhibitors during the preclinical phase. Anasthesiol Intensivmed Notfallmed Schmerzther 27:31-36; 1992.
125. Lampl L, Bock KH, Hartel W, Helm M,
Tisch M, Seifried E. Disorders of hemostasis after polytrauma. On the extent of intrinsic fibrinolytic activity in the preclinical phase. Chirurg 63:305-309; 1992.
126. Schmidt U, Enderson BL, Chen JP, Maull KI. D-dimer levels correlate with pathologic thrombosis in trauma patients. J Trauma 33:
312-319; 1992. 127. Kluft C, de Bart CWW, Barthels M, Sturm
J, Moller W. Short term extreme increases in plasminogen activator inhibitor 1 (PAI-1) in plasma of polytrauma patients. Fibrinolysis 2:223-226; 1988.
128. Counts RB, Haisch C, Simon TL, Maxwell
NG, Heimbach DM, Carrico CJ. Hemostasis in massively transfused trauma patients. Ann Surg 190:91-99; 1979.
129. Harrigan C, Lucas CE, Ledgerwood AM. The
effect of hemorrhagic shock on the clotting cascade in injured patients. J Trauma 29:1416-1421; 1989.
130. Alkjaersig N, Fletcher AP, Peden JCJ, Monafo
WW. Fibrinogen catabolism in burned patients. J Trauma 20:154-159; 1980.
131. Kowal Vern A, Gamelli RL, Walenga JM,
Hoppensteadt D, Sharp Pucci M, Schumacher HR. The effect of burn wound size on hemostasis: a correlation of the hemostatic changes to the clinical state. J Trauma 33:50-56; 1992.
132. Fleck RA, Rao LV, Rapaport SI, Varki N.
Localization of human tissue factor antigen by immunostaining with monospecific, polyclonal anti-human tissue factor antibody. Thromb Res 59:421-437; 1990.
133. Cannon WB, Gray H. Factors affecting the
coagulation time of blood. The hastening or retarding of coagulation by adrenalin injections. Am J Physiol 34:232-250; 1914.
134. Swedenborg J, Olsson P. Activation of plasma
coagulation in vivo by epinephrine and platelet release reaction. An experimental study in the dog. Thromb Res 13:37-45; 1978.
135. Nygaard OP, Unneberg K, Reikeras O, Osterud
B. Thromboplastin activity of blood monocytes after total hip replacement. Scand J Clin Lab Invest 50:183-186; 1990.
136. Rinecker H. New clinicopathophysiologic
al studies on the bone cement implantation syndrome. Arch Orthop Trauma Surg 97:263-274; 1980.
137. Kallos T. Impaired arterial oxygenation
associated with use of bone cement in the femoral shaft. Anesthesiology 42:210-215; 1975.
138. Orsini EC, Byrick RJ, Mullen JB, Kay JC,
30
Waddell JP. Cardiopulmonary function and pulmonary microemboli during arthroplasty using cemented or noncemented components. The role of intramedullary pressure. J Bone Joint Surg Am 69:822-832; 1987.
139. Sharnoff JG. Results in the prophylaxis of
postoperative thromboembolism. Surg Gynecol Obstet 123:303-307; 1966.
140. Modig J, Busch C, Waernbaum G. Effects of
graded infusions of monomethylmethacrylate on coagulation, blood lipids, respiration and circulation. An experimental study in dogs. Clin Orthop 187-197; 1975.
141. Modig J, Busch C, Olerud S, Saldeen
T. Pulmonary microembolism during intramedullary orthopaedic trauma. Acta Anaesthesiol Scand 18:133-143; 1974.
142. Parmet JL, Berman AT, Horrow JC, Harding
S, Rosenberg H. Thromboembolism coincident with tourniquet deflation during total knee arthroplasty. Lancet 341:1057-1058; 1993.
143. Bergqvist, D. Postoperative thromboembolism;
Frequency, Etiology, Prophylaxis, Berlin, Heidelberg, New York:Springer-Verlag, 1983.
144. Faunø P, Suomalainen O, Bergqvist D, Fredin
H, Kettunen K, Soimakallio S, Cederholm C, Karjalainen P, Vissinger H, Justesen T. The use of fibrinogen uptake test in screening for deep vein thrombosis in patients with hip fracture. Thromb Res 60:185-190; 1990.
145. Harris WH, Athanasoulis C, Waltman AC,
Salzman EW. Cuff impedance phlebography and 125I fibrinogen scanning versus roentgenographic phlebography for diagnosis of thrombophlebitis following hip surgery. A preliminary report. J Bone Joint Surg Am 58:939-944; 1976.
146. Borris LC, Christiansen HM, Lassen MR,
Olsen AD, Schøtt P. Comparison of realtime B-mode ultrasonography and bilateral ascending phlebography for detection of postoperative deep vein thrombosis following elective hip surgery. Thromb Haemost 61:363-365; 1989.
147. Wille-Jørgensen P, Borris LC, Lassen MR,
Jørgensen LN, Hauch O, Nehen AM, Kjær L, Jensen R. Potential influence of observer variation in thromboprophylactic trials. Haemostasis 22:211-215; 1992.
148. Clayton JK, Anderson JA, McNicol GP.
Preoperative prediction of postoperative deep
vein thrombosis. Br Med J ii:910-912; 1976. 149. Rakoczi I, Chamone D, Verstraete M, Collen
D. The relevance of clinical and hemostasis parameters for the prediction of postoperative thrombosis of the deep veins of the lower extremity in gynecologic patients. Surg Gynecol Obstet 151:225-231; 1980.
150. Sue Ling HM, Johnston D, McMahon MJ, Philips
PR, Davies JA. Preoperative identification of patients at high risk of deep venous thrombosis after elective major abdominal surgery. Lancet i:1173-1176; 1986.
151. Sue Ling HM, Johnston D, Verheijen JH,
Kluft C, Philips PR, Davies JA. Indicators of depressed fibrinolytic activity in preoperative prediction of deep venous thrombosis. Br J Surg 74:275-278; 1987.
152. Becker J. Postoperative venous thrombosis. A
clinical and experimental study with special reference to early diagnosis, prophylaxis, course and some haematological findings. Acta Chir Scand Suppl 431:1-38; 1972.
153. Korvald E, Abildgaard U, Fagerhol MK. Major
operations, hemostatic parameters and venous thrombosis. Thromb Res 4:147-154; 1974.
154. Knight MT, Dawson R, Melrose DG. Fibrinolytic
response to surgery. Labile and stable patterns and their relevance to postoperative deep venous thrombosis. Lancet ii:370-373; 1977.
155. Lowe GD, Carter DC, Prentice CR. Preoperative
prediction of postoperative deepvein thrombosis [letter]. Lancet i:1474; 1982.
156. Mellbring G, Dahlgren S, Wiman B, Sunnegårdh
O. Relationship between preoperative status of the fibrinolytic system and occurrence of deep vein thrombosis after major abdominal surgery. Thromb Res 39:157-163; 1985.
157. Mellbring G, Dahlgren S, Wiman B. Prediction
of deep vein thrombosis after extensive abdominal operations by the quotient between plasmin alpha-2-antiplasmin complex and fibrinogen concentration in plasma. Surg Gynecol Obstet 161:339-342; 1985.
158. Rahr HB, Sørensen JV. Venous thromboembolism
and cancer. Blood Coagul Fibrinoly 3:451-460; 1992.
159. Comp PC, Jacocks RM, Taylor FBJ. The dilute
whole blood clot lysis assay: a screening method for identifying postoperative patients with a high incidence of deep venous thrombosis. J Lab Clin
31
Med 93:120-127; 1979. 160. Summaria L, Caprini JA, McMillan R,
Sandesara J, Axelrod CA, Mueller ME, Vagher JP, Walenga J, Fareed J. Relationship between postsurgical fibrinolytic parameters and deep vein thrombosis in surgical patients treated with compression devices. Am Surg 54:156-160; 1988.
161. Ruckly CV, Das PC, Leitch AG, Donaldson AA,
Copland WA, Redpath AT, Scott P, Cash JD. Serum fibrin/fibrinogen degradation products associated with postoperative pulmonary embolus and venous thrombosis. BMJ 4:395-398; 1970.
162. Paramo JA, Alfaro MJ, Rocha E. Postoperative
changes in the plasmatic levels of tissue type plasminogen activator and its fast acting inhibitor relationship to deep vein thrombosis and influence of prophylaxis. Thromb Haemost 54:713-716; 1985.
163. Rocha E, Alfaro MJ, Paramo JA, Canadell
JM. Preoperative identification of patients at high risk of deep venous thrombosis despite prophylaxis in total hip replacement. Thromb Haemost 59:93-95; 1988.
164. Grimaudo V, Kruithof EKO, Stiekema JCJ,
Bachmann F. High preoperative plasminogen activator inhibitor levels are correlated with postoperative deep vein thrombosis in total hip replacement. Thromb Haemost 62:96; 1989.(Abstract)
165. Sørensen JV, Lassen MR, Borris LC, Jørgensen
PS, Schøtt P, Weber S, Murphy R, Walenga J. Postoperative deep vein thrombosis and plasma levels of tissue plasminogen activator inhibitor. Thromb Res 60:247-251; 1990.
166. Lassen MR, Borris LC, Christiansen HM, Schøtt
P, Olsen AD, Sørensen JV, Rahr H, Jensen HP. Clinical trials with low molecular weight heparins in the prevention of postoperative thromboembolic complications: a metaanalysis. Semin Thromb Hemost 17 Suppl 3:284-290; 1991.
167. Turpini R, Stefanini M. The nature and
mechanism of the hemostatic breakdown in the course of experimental hemorrhagic shock. J Clin Invest 38:53-65; 1959.
168. McClintock JT, Magers E. Coagulation time
following hemorrhage after splenectomy. Proc Soc Exp Biol Med 24:203-204; 1926.
169. Hardaway RM, Drake DC. Prevention of ireversible hemorrhagic shock with fibrinolysin. Am Surg 157:39-47; 1963.
170. Hardaway RM, Burns JW. Mechanism of action
of fibrinolysin in the prevention of irreversible hemorrhagic shock. Am Surg 157:305-309; 1963.
171. van der Sande JJ, Emeis JJ, Lindeman
J. Intravascular coagulation: a common phenomenon in minor experimental head injury. J Neurosurg 54:21-25; 1981.
172. Jansson I. Posttraumatic pulmonary
microembolism; a clinical and experimental study (Thesis). Acta Chir Scand Suppl 523:1-80; 1984.
173. Hardaway RM, Adams WH. Blood clotting
problems in acute care. Acute Care 14-15:138-207; 1988.
174. Saldeen T. Quantiative determination of
intravascular coagulation in the lungs of experimental animals. Scand J Haematol 6:205-215; 1969.
175. Giercksky KE, Bjorklid E, Prydz H. The effect
of intravenous injection of purified human tissue thromboplastin in rats. Scand J Haematol 16:300-310; 1976.
176. Busch C, Lindquist O, Saldeen T. Respiratory
insufficiency in the dog induced by pulmonary microembolism and inhibition of fibrinolysis. Effect of defibrinogenation, leucopenia and thrombocytopenia. Acta Chir Scand 140:255-266; 1974.
177. Sevitt S, Gallagher NG. Prevention of venous
thrombosis and pulmonary embolism in injuried patients. Lancet ii:981-989; 1959.
178. Sevitt S, Gallagher N. Venous thrombosis and
pulmonary embolism; a clinicopathological study in injured and burned patients. Br J Surg 47:475-489; 1961.
179. Eeles GH, Sevitt S. Microthrombosis in injured
and burned patients. J Pathol Bacteriol 93:275-293; 1967.
180. Lindquist O, Rammer L, Saldeen T. Pulmonary
insufficiency, microembolism and fibrinolysis inhibition in a posttraumatic autopsy material. Acta Chir Scand 138:545-549; 1972.
181. Kaufman HH, Hui KS, Mattson JC, Borit
A, Childs TL, Hoots WK, Bernstein DP, Makela ME, Wagner KA, Kahan BD, et al .
32
Clinicopathological correlations of disseminated intravascular coagulation in patients with head injury. Neurosurgery 15:34-42; 1984.
182. Blaisdell FW, Lim RCJ, Amberg JR, Choy
SH, Hall AD, Thomas AN. Pulmonary microembolism. A cause of morbidity and death after major vascular surgery. Arch Surg 93:776-786; 1966.
183. Busch C, Dahlgren S, Jacobsson S, Jung B,
Modig J, Saldeen T. Determination of fibrin trapping in the lungs of patients developing the microembolism syndrome. A preliminary report. Acta Chir Scand 137:599-601; 1971.
184. Busch C. Quantitative determination of
pulmonary microembolism in the dog. Comparison of in vivo and in vitro methods. Ups J Med Sci 79:72-83; 1974.
185. Shackford SR, Davis JW, Hollingsworth
Fridlund P, Brewer NS, Hoyt DB, Mackersie RC. Venous thromboembolism in patients with major trauma. Am J Surg 159:365-369; 1990.
186. O'Malley KF, Ross SE. Pulmonary embolism in major trauma patients. J Trauma 30:748-750; 1990.
187. Olson JD, Kaufman HH, Moake J, O'Gorman
TW, Hoots K, Wagner K, Brown CK, Gildenberg PL. The incidence and significance of hemostatic abnormalities in patients with head injuries. Neurosurgery 24:825-832; 1989.
188. van der Sande JJ, Veltkamp JJ, Boekhout
Mussert RJ, Vielvoye GJ. Hemostasis and computerized tomography in head injury. Their relationship to clinical features. J Neurosurg 55:718-724; 1981.
189. Civil ID, Schwab CW. The Abbreviated Injury
Scale, 1985 revision: a condensed chart for clinical use. J Trauma 28:87-90; 1988.
190. Teasdale G, Jennett B. Assessment of coma
and impaired consciousness. A practical scale. Lancet ii:81-84; 1974.
191. Enderson BL, Chen JP, Robinson R, Maull KI. Fibrinolysis in multisystem trauma patients. J Trauma 31:1240-1246; 1991.
192. Attar S, Boyd D, Layne E, McLaughlin J,
Mansberger AR, Cowley RA. Alterations in coagulation and fibrinolytic mechanisms in acute trauma. J Trauma 9:939-965; 1969.
193. Hirsch EF, Fletcher JR, Moquin R, Dostalek R, Lucas S. Coagulation changes after combat
trauma and sepsis. Surg Gynecol Obstet 133:393-396; 1971.
194. Kierulf P, Aasen AO, Aune S, Godal HC, Ruud
TE, Vaage J. Chromogenic peptide substrate assays in patients with multiple trauma. Acta Chir Scand Suppl 509:69-72; 1982.
195. Aasen AO, Kierulf P, Vaage J, Godal HC, Aune
S. Determination of components of the plasma proteolytic enzyme systems gives information of prognostic value in patients with multiple trauma. Adv Exp Med Biol 156:1037-1047; 1983.
196. Keimowitz RM, Annis BL. Disseminated
intravascular coagulation associated with massive brain injury. J Neurosurg 39:178-180; 1973.
197. Preston FE, Malia RG, Sworn MJ, Timperley
WR, Blackburn EK. Disseminated intravascular coagulation as a consequence of cerebral damage. J Neurol Neurosurg Psychiatry 37:241-248; 1974.
198. Strinchini A, Baudo F, Nosari AM, Panzacchi G, de Cataldo F. Letter: Defibrination and head injury. Lancet ii:957; 1974.
199. Miner ME, Kaufman HH, Graham SH, Haar
FH, Gildenberg PL. Disseminated intravascular coagulation fibrinolytic syndrome following head injury in children: frequency and prognostic implications. J Pediatr 100:687-691; 1982.
200. Kumura E, Sato M, Fukuda Y, Takemoto Y,
Tanaka Sh, Kohama A. Coagulation disorders following acute head injury. Acta Neurochir 85:23-28; 1987.
201. Ashbaugh DG, Bigelow DB, Petty TL, Levine
BE. Acute respiratory distress in adults. Lancet 2:319-323; 1967.
202. Fulton RL, Jones CE. The cause of posttraumatic
pulmonary insufficiency in man. Surg Gynecol Obstet 140:179-186; 1975.
203. Laghi F, Siegel JH, Rivkind AI, Chiarla C,
DeGaetano A, Blevins S, Stoklosa JC, Borg UR, Belzberg H. Respiratory index/pulmonary shunt relationship: quantification of severity and prognosis in the posttraumatic adult respiratory distress syndrome. Crit Care Med 17:1121-1128; 1989.
204. Dalal SA, Burgess AR, Siegel JH, Young JW,
Brumback RJ, Poka A, Dunham CM, Gens D, Bathon H. Pelvic fracture in multiple trauma:
33

classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma 29:981-1000; 1989.
205. String T, Robinson AJ, Blaisdell FW. Massive
trauma. Effect of intravascular coagulation on prognosis. Arch Surg 102:406-411; 1971.
206. Crone KR, Lee KS, Kelly DLJ. Correlation
of admission fibrin degradation products with outcome and respiratory failure in patients with severe head injury. Neurosurgery 21:532-536; 1987.
207. Schramm W, Spannagel M, Joka T, Sturm J.
Follow up of hemostatic and fibrinolytic factors in polytraumatized patients. Blut 58:114; 1989. (Abstract)
208. Seeger W, Hubel J, Klapettek K, Pison U,
Obertacke U, Joka T, Roka L. Procoagulant activity in bronchoalveolar lavage of severely traumatized patients-relation to the development of acute respiratory distress. Thromb Res 61:53-64; 1991.
209. Bertozzi P, Astedt B, Zenzius L, Lynch K,
LeMaire F, Zapol W, Chapman HAJ. Depressed bronchoalveolar urokinase activity in patients with adult respiratory distress syndrome. N Engl J Med 322:890-897; 1990.
210. Idell S, James KK, Levin EG, Schwartz BS,
Manchanda N, Maunder RJ, Martin TR, McLarty J, Fair DS. Local abnormalities in coagulation and fibrinolytic pathways predispose to alveolar fibrin deposition in the adult respiratory distress syndrome. J Clin Invest 84:695-705; 1989.
211. Knighton DR, Hunt TK, Thakral KK, Goodson
WH. Role of platelets and fibrin in the healing sequence: an in vivo study of angiogenesis and collagen synthesis. Ann Surg 196:379-388; 1982.
212. Ciano PS, Colvin RB, Dvorak AM, McDonagh
J, Dvorak HF. Macrophage migration in fibrin gel matrices. Lab Invest 54:62-70; 1986.
213.Colvin RB, Gardner PI, Roblin RO, Verderber EL, Lanigan JM, Mosesson MW. Cell surface fibrinogenfibrin receptors on cultured human fibroblasts. Association with fibronectin (cold insoluble globulin, LETS protein) and loss in SV40 transformed cells. Lab Invest 41:464-473; 1979.
214. Malik AB, van der Zee H. Lung vascular
permeability following progressive pulmonary embolization. J Appl Physiol 45:590-597;
1978. 215. Costabella PMo, Lindquist O, Kapanci Y,
Saldeen T. Increased vascular permeability in the delayed microembolism syndrome. Microvasc Res 15:275-286; 1978.
216. Luterman A, Manwaring D, Curreri PW. The
role of fibrinogen degradation products in the pathogenesis of the respiratory distress syndrome. Surgery 82:703-709; 1977.
217. Manwaring D, Thorning D, Curreri PW.
Mechanisms of acute pulmonary dysfunction induced by fibrinogen degradation product D. Surgery 84:45-53; 1978.
218. Belew M, Gerdin B, Porath J, Saldeen T.
Isolation of vasoactive peptides from human fibrin and fibrinogen degraded by plasmin. Thromb Res 13:983-994; 1978.
219. Schlag G, Redl H. Lung in shock-posttraumatic
lung failure (organ failure)-MOFS. Prog Clin Biol Res 308:3-16; 1989.
220. Wright HP, Osborn SB, Edmonds DG. Effect of
postoperative bed rest and early ambulation on the rate of venous bloodflow. Lancet i:22-25; 1951.
221. DeCamp MM, Demling RH. Posttraumatic
multisystem organ failure. JAMA 260:530-534; 1988.
222. Demling RH. Current concepts on the adult
respiratory distress syndrome. Circ Shock 30:297-309; 1990.
223. Barton R, Cerra FB. The hypermetabolism.
Multiple organ failure syndrome. Chest 96:1153-1160; 1989.
224. Repine JE. Scientific perspectives on adult
respiratory distress syndrome. Lancet 339:466-469; 1992.
225. Havig O. Deep vein thrombosis and pulmonary
embolism (Thesis). Acta Chir Scand Suppl 478:1-120; 1977.
226. Border JR, Allgøver M, Hansen ST, Ruedi TP.
Blunt Multiple Trauma, New York:Dekker, 1990.
227. Ejstrud P, Sørensen JV. Tidlig osteosyntese af und
erekstremitetsfrakturer hos multitraumatiserede. Ugeskr Laeger 155:1202-1206; 1993.
34