
Glassy cell carcinoma of the cervix
9
GLASSY CELL CARCINOMA OF THE CERVIX PHILIP LITTMAN, MD, PHILIP B. CLEMENT, MD, BIRCIT HENRIKSEN, MD, C. C. WANC, MD, STANLEY J. ROBBOY, MD, PRISCILLA D. TAFT, MD, HOWARD ULFELDER, MD, AND ROBERT E. SCULLY, MD A clinicopathologic analysis of 13 c a m of glassy cell carcinoma of the uterine cervix is presented. T h e glassy cell carcinoma is considered to be a poorly dif- ferentiated mixed adenosquamous carcinoma. Its histologic appearance is dis- tinctive, being characterized by cells with a moderate amount of cytoplasm having a ground glass or finely granular appearance, a distinct cell wall that stains with eosin and PAS, and enlarged nuclei with prominent nucleoli. In the present study this tumor was associated with extrapelvic spread in 6/13 cases at diagnosis. Results were p r with either surgery and/or radiotherapy. Only four of I3 patients survived 5 years. The glassy cell carcinoma appears to be a distinct clinicopathologic entity which warrants a place in the classification of carcinoma of the cervix. Cancer 37:225&2246, 1976. N ADDITION TO SQUAMOUS CELL CARCINOMA I and adenocarcinoma of the cervix, a mixed form composed of both squamous and glan- dular elements has been recognized for many years. In 1956, Glucksmann and Cherry sub- divided mixed carcinomas of the cervix into well-differentiated and p r l y differentiated categories.5 The latter included the signet-cell carcinoma and an undifferentiated form, which these authors designated glassy cell car- cinoma. T h e diagnostic features of the glassy cell were stated to be a moderate amount of cytoplasm of ground-glass appearance, a dis- tinct cell wall, and a large nucleus containing a prominent nucleolus. The glassy cell carci- noma proved to be highly malignant, being refractory to both radiation and surgical ther- apy. After this report and subsequent articles by the same authors in 19574 and 19612 this type of tumor has been ignored in the litera- ture. At the Massachusetts General Hospital, the glassy cell carcinoma has been recognized since 1957. Because its prognosis has been poor in contrast to that of the nonkeratinizing large-cell squamous cell carcinomae with From the Departments of Radiation Medicine, Gyne- cology, and Pathology, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 021 14. Address for reprints: Robert E. Scully, MD, Depart- ment of Pathology, Masaachusetts General Hospital, Boston, MA 02114. The authors thank Anne Annuziato for her help In the prepartion of this manuscript. Received for publication July 28, 1975. which it may easily be confused, the 13 cases treated at this institution have been analyzed from a clinicopathological viewpoint. PRETREATMENT CLINICAL DATA (TABLE 1) The 13 patients were Caucasian and ranged in age from 33 to 63 years with a mean of 46 years. The most common presenting symptoms were vaginal staining, bleeding, and discharge for an average of 4 months' duration. Most of the tumors appeared bulky and exophytic on pelvic examination. According to the cri- teria of the International Federation of Gynecology and Obstetrics, three patients had Stage I; nine, Stage 11; and one, Stage I11 tu- mors. Four patients had lymphangiograms as part of their initial evaluation, and three of them were positive for metastatic carcinoma. CYTOLOGY Although no case was discovered by cytol- ogy, pretreatment cytologic smears had been obtained from eight of the patients. One smear initially called negative was found on review to contain a few cells resembling those of squamous cell carcinoma in situ. In the other seven cases, the smear was interpreted as positive for malignant cells. In three cases the cells suggested invasive squamous cell car- cinoma, while in four the diagnosis of undif- 2238
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Glassy cell carcinoma of the cervix

GLASSY CELL CARCINOMA OF THE CERVIX PHILIP LITTMAN, MD, PHILIP B. CLEMENT, MD, BIRCIT HENRIKSEN, MD,
C. C. WANC, MD, STANLEY J. ROBBOY, MD, PRISCILLA D. TAFT, MD, HOWARD ULFELDER, MD, AND ROBERT E. SCULLY, MD
A clinicopathologic analysis of 13 c a m of glassy cell carcinoma of the uterine cervix is presented. T h e glassy cell carcinoma is considered to be a poorly dif- ferentiated mixed adenosquamous carcinoma. Its histologic appearance is dis- tinctive, being characterized by cells with a moderate amount of cytoplasm having a ground glass or finely granular appearance, a distinct cell wall that stains with eosin and PAS, and enlarged nuclei with prominent nucleoli. I n the present study this tumor was associated with extrapelvic spread in 6/13 cases at diagnosis. Results were p r with either surgery and/or radiotherapy. Only four of I3 patients survived 5 years. The glassy cell carcinoma appears to be a distinct clinicopathologic entity which warrants a place in the classification of carcinoma of the cervix.
Cancer 37:225&2246, 1976.
N ADDITION TO SQUAMOUS CELL CARCINOMA I and adenocarcinoma of the cervix, a mixed form composed of both squamous and glan- dular elements has been recognized for many years. In 1956, Glucksmann and Cherry sub- divided mixed carcinomas of the cervix into well-differentiated and p r l y differentiated categories.5 The latter included the signet-cell carcinoma and an undifferentiated form, which these authors designated glassy cell car- cinoma. T h e diagnostic features of the glassy cell were stated to be a moderate amount of cytoplasm of ground-glass appearance, a dis- tinct cell wall, and a large nucleus containing a prominent nucleolus. The glassy cell carci- noma proved to be highly malignant, being refractory to both radiation and surgical ther- apy. After this report and subsequent articles by the same authors in 19574 and 19612 this type of tumor has been ignored in the litera- ture. At the Massachusetts General Hospital, the glassy cell carcinoma has been recognized since 1957. Because its prognosis has been poor in contrast to that of the nonkeratinizing large-cell squamous cell carcinomae with
From the Departments of Radiation Medicine, Gyne- cology, and Pathology, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 021 14.
Address for reprints: Robert E. Scully, MD, Depart- ment of Pathology, Masaachusetts General Hospital, Boston, MA 02114.
The authors thank Anne Annuziato for her help In the prepartion of this manuscript.
Received for publication July 28, 1975.
which i t may easily be confused, the 13 cases treated at this institution have been analyzed from a clinicopathological viewpoint.
PRETREATMENT CLINICAL DATA (TABLE 1)
The 13 patients were Caucasian and ranged in age from 33 to 63 years with a mean of 46 years.
The most common presenting symptoms were vaginal staining, bleeding, and discharge for an average of 4 months' duration. Most of the tumors appeared bulky and exophytic on pelvic examination. According to the cri- teria of the International Federation of Gynecology and Obstetrics, three patients had Stage I; nine, Stage 11; and one, Stage I11 tu- mors. Four patients had lymphangiograms as part of their initial evaluation, and three of them were positive for metastatic carcinoma.
CYTOLOGY
Although no case was discovered by cytol- ogy, pretreatment cytologic smears had been obtained from eight of the patients. One smear initially called negative was found on review to contain a few cells resembling those of squamous cell carcinoma in situ. In the other seven cases, the smear was interpreted as positive for malignant cells. In three cases the cells suggested invasive squamous cell car- cinoma, while in four the diagnosis of undif-
2238

No. 5 GLASSY CELL CARCINOMA * Littman et a1. 2239
TABLE 1 .
Clinical appearance Lympho- Therapy and lymph-node Case Age Stage of tumor gram findings at operation Followup
1
2
3
4
5
6
7
8
9
10
1 1
12
1 3
35
48
54
42
57
6 3
3 3
61
47
46
35
41
35
1B fungating mass, post. lip pelvic & expl. lap., para-aortic nodes para-aortic pos.; 7200 mghr Ra., nodes pos. 4500 rad pelvic walls,
4800 rad para-aortic nodes
resid. tumor, nodes neg. 1B fungating mass a t 0 s no 4320 mghr, Wertheim,
1B ulcer endocx. no expl. lap., pelvic and para-aortic nodes pos., 6000 rad pelvis, 3600 mghr
supracl. node, hilar mass, and vag. recur.; died 23 mo.; no pm.
diffuse met. to bone & 1ungs;died 12 mo.;no pni.
died 6 mo. ; no pm.
2A tumor replacing cx. & no 2000 rad whole pelvis, upper 1/3 vag. 7680 mghr, 2200 rad pelvic
walls
(5/ 1 1 nodes pos.)
2800 mghr; treatment not completed
7194 mghr, 2000 rad pelvic
2R ulcer of endocx. & post. no 7920 mghr, 1500 rad whole
2X tumor replacing most of no 3600 mghr, Wertheim
2B mass replacing cx. & upper no 3000 rad whole pelvis,
cx. and vag. fornix
vag. extend. into paramet.
2B fungating mass replacing no 2500 rad whole pelvis, cx. with minimal paramet. extens. walls
lip with extens. into both paramet.
fornices, & paramet.
pelvis, 2000 rad pelvic walls
2B extens. tumor of cx., vag. neg. 4000 rad whole pelvis, 4800 mghr, 1000 rad pelvic walls
2B ulcer. tumor of cx. with no 4000 rad pelvis, 4800 mghr, 1000 rad pelvic walls
2B necrotic tumor of post. lip no Wertheim, nodes neg.
paramet. extens.
with extens. into paramet.
2B bulk;y tumor replacing cx. pelvic & expl. lap., para-aortic nodes para-aortic pos.; 3000 rad whole pelvis, nodes pos. 3600 mghr;
with paramet. extens.
3000 rad pelvic wall, 4400 rad para-aortic nodes
3 large fungating tumor pelvic & 4000 rad pelvis, 4300 mghr; replace. cx; pelvic wall para-aortic 1000 rad pelvic walls, mass nodes pos. 4400 rad para-aortic nodes
alive and well 5 yr.
died 15 mo.; pm. revealed pelvic and retrop. met.
died 13 mo. with chest met.; no pm.
alive and well 5 yr.
alive and well 11 yr.
died 1 1 mo. with pelvic mass and local recur.; no pm.
died 6 mo. with pelvic mass; no pm.
lived 15 yr. with no evi- dence of disease, died of myoc. infarct; no pm.
died 6 mo. with recur. a t vag. apex; no pm.
died 1 yr. with pelvic tumor: no pm.
ferentiated carcinoma was made because of scanty, poorly defined cytoplasm surrounding malignant appearing nuclei. One smear, in- terpreted as undifferentiated carcinoma (Fig. l), contained nuclei with delicate borders, ir- regular chromatin and large, occasionally multiple nucleoli, but in the other three such cases the nucleoli were not as prominent and the nuclear chromatin was coarser, possibly due to degeneration. In summary, these tu- mors did not have a distinctive cytologic ap- pearance.
TREATMENT
A Wertheim hysterectomy with pelvic node dissection was the treatment in three cases (Cases 2, 5, and 11); in two (Cases 2 and 5) radium had been administered preoperatively. None of these patients received postoperative irradiation.
An exploratory laparotomy was performed in three cases (Cases 1, 3, and 12) with the intention of doing a radical hysterectomy, but the lymph nodes were found to be involved,

2240 'CANCER May 1976 VOl. 37
FIG. 1. Case 5. Cyto- logic preparation from Papanicolaou smear. Clusters of malignant cells have large nuclei, irregular nuclear chro- matin, large nucleoli, a n d a moderate amount of cytoplasm (Papanicolaou stain, X600).
surgical therapy was abandoned, and the pa- tients were given definitive radiation therapy. Seven patients (Cases 4, 6-10, 13) received radiation therapy without prior laparotomy. All the therapy was done at the Massachuetts General Hospital. T h e basic regime consisted of one or two radium applications employing
a modified Stockholm technique plus external irradiation with the 2 MeV Van de Graaff generator. A final dosage of 7000-8000 rad to the paracervical triangle (Point A) and 6000 rads to the pelvic walls was accomplished for most of the patients receiving primary radia- tion therapy. One patient (Case 6) failed to
FIG. 2. Case 2. Nests of uniform anaplastic tumor cells are sep- arated by thin bands of fibrous stroma in- filtrated with inflam- matory cells (H & E, X210).
No. 5 GLASSY CELL CARCINOMA * Littman et al. 224 1
complete her treatment and consequently re- ceived an inadequate dose. Three patients (Cases 1, 12, and 13) with para-aortic lymph node metastases, diagnosed by lymphangio- gram, received 4400 to 4800 rad to the para- aortic area through anterior and posterior portals on the 2 MEV Van de Graaff generator.
OUTCOME
All the patients have been followed to death or from 5 to 15 years after treatment. Only four patients, all with Stage I1 tumors, sur- vived for 5 years or longer; three (Cases 4, 7, 8) had been treated by radiation therapy and the third (Case 11) by Wertheim hysterectomy.
Nine patients died. Seven had been treated by radiation therapy alone and two by pre- operative irradiation followed by Wertheim hysterectomy. Of the seven patients in whom radiation therapy failed six died with local recurrence. One of the patients who had pre- operative radiation therapy also died with local recurrence.
GROSS PATHOLOGY OF HYSTERECTOMY SPECIMENS
The tumors in the three hysterectomy speci- mens had no specific gross morphologic fea-
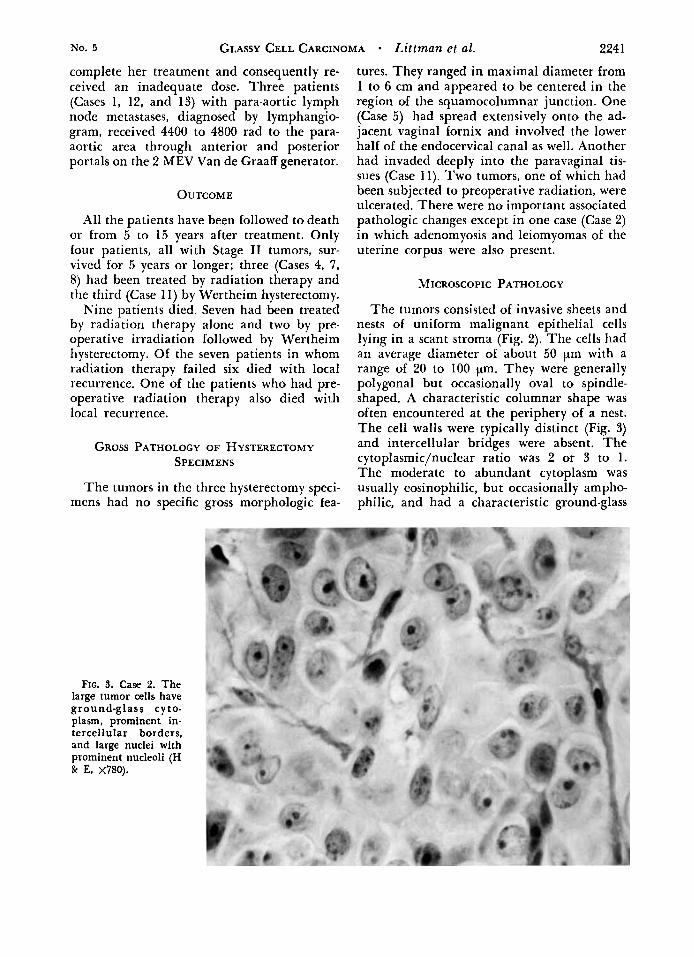
FIG. 3. Case 2. The large tumor cells have ground-glass cyto- plasm, prominent in- tercellular borders, and large nuclei with prominent nucleoli (H & E, ~780).
tures. They ranged in maximal diameter from 1 to 6 cm and appeared to be centered in the region of the squamocolumnar junction. One (Case 5) had spread extensively onto the ad- jacent vaginal fornix and involved the lower half of the endocervical canal as well. Another had invaded deeply into the paravaginal tis- sues (Case 11). Two tumors, one of which had been subjected to preoperative radiation, were ulcerated. There were no important associated pathologic changes except in one case (Case 2) in which adenomyosis and leiomyomas of the uterine corpus were also present.
MICROSCOPIC PATHOLOGY
The tumors consisted of invasive sheets and nests of uniform malignant epithelial cells lying in a scant stroma (Fig. 2). The cells had an average diameter of about 50 pm with a range of 20 to 100 'pm. They were generally polygonal but occasionally oval to spindle- shaped. A characteristic columnar shape was often encountered at the periphery of a nest. The cell walls were typically distinct (Fig. 3) and intercellular bridges were absent. The cytoplasmic/nuclear ratio was 2 or 3 to 1. The moderate to abundant cytoplasm was usually eosinophilic, but occasionally ampho- philic, and had a characteristic ground-glass
2242 CANCER May 1976 VOl. 37
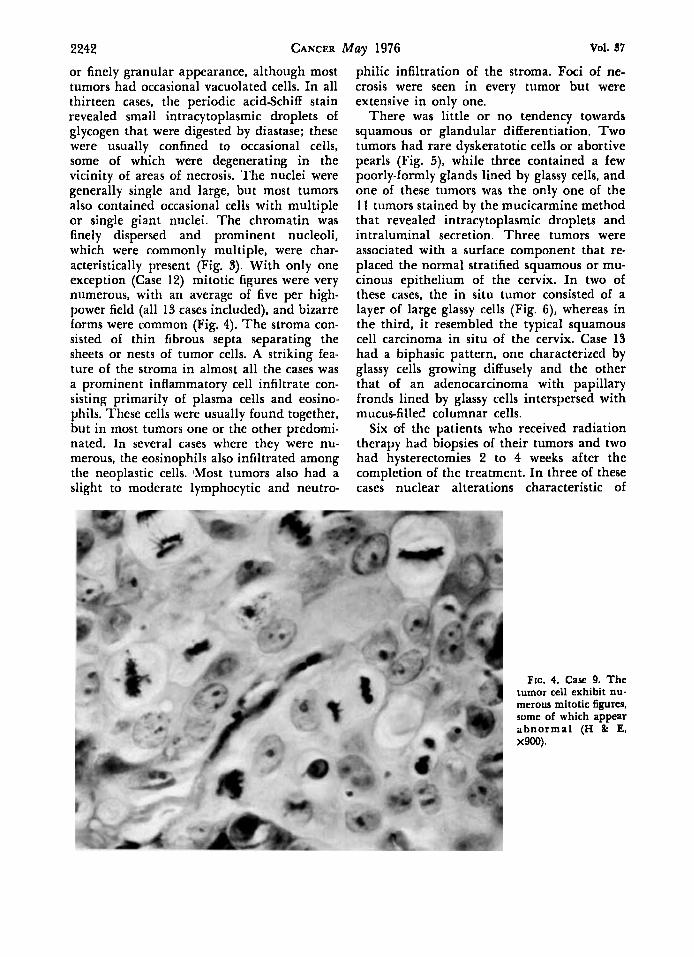
or finely granular appearance, although most tumors had occasional vacuolated cells. In all thirteen cases, the periodic acidSchiff stain revealed small intracytoplasmic droplets of glycogen that were digested by diastase; these were usually confined to occasional cells, some of which were degenerating in the vicinity of areas of necrosis. The nuclei were generally single and large, but most tumors also contained occasional cells with multiple or single giant nuclei. The chromatin was finely dispersed and prominent nucleoli, which were commonly multiple, were char- acteristically present (Fig. 3). With only one exception (Case 12) mitotic figures were very numerous, with an average of five per high- power field (all 13 cases included), and bizarre forms were common (Fig. 4). The stroma con- sisted of thin fibrous septa separating the sheets or nests of tumor cells. A striking fea- ture of the stroma in almost all the cases was a prominent inflammatory cell infiltrate con- sisting primarily of plasma cells and eosino- phils. These cells were usually found together, but in most tumors one or the other predomi- nated. In several cases where they were nu- merous, the eosinophils also infiltrated among the neoplastic cells. IMost tumors also had a slight to moderate lymphocytic and neutro-
philic infiltration of the stroma. Foci of ne- crosis were seen in every tumor but were extensive in only one.
There was little or no tendency towards squamous or glandular differentiation. Two tumors had rare dyskeratotic cells or abortive pearls (Fig. 5), while three contained a few poorly-formly glands lined by glassy cells, and one of these tumors was the only one of the 11 tumors stained by the mucicarmine method that revealed intracytoplasmic droplets and intraluminal secretion. Three tumors were associated with a surface component that re- placed the normal stratified squamous or mu- cinous epithelium of the cervix. In two of these cases, the in situ tumor consisted of a layer of large glassy cells (Fig. 6), whereas in the third, it resembled the typical squamous cell carcinoma in situ of the cervix. Case 13 had a biphasic pattern, one characterized by glassy cells growing diffusely and the other that of an adenocarcinoma with papillary fronds lined by glassy cells interspersed with mucus-filled columnar cells.
Six of the patients who received radiation therapy had biopsies of their tumors and two had hysterectomies 2 to 4 weeks after the completion of the treatment. In three of these cases nuclear alterations characteristic of
FIG. 4. Case 9. The tumor cell exhibit nu- merous mitotic figures. some of which appear abnormal (H & E, x900).

No. 5 GLASSY CELL CARCINOMA Littrnan et al. 2243
FIG 5. Case 12. Poorly developed qua- mous pearls are sur- rounded by glassy car- cinoma cells (H & E, x290).
radiation effect were observed, but in only Otherwise the tumors appeared little altered, one were these changes marked and was with only mild cytoplasmic vacuolation and a keratinization of the neoplastic cells observed. slight increase in the stroma and neutrophilic
FIG. 6. Case 9. A focus of glassy cell car- cinoma in situ is shown with glassy cells replacing the full thickness of the sur- face epithelium (H & E, %440).
2244 CANCER May 1976 Vol. 37
infiltration. Most of the irradiated tumors retained an appearance similar enough to that of the pretreatment specimens that they could be identified easily as glassy cell carcinomas.
In three of the four cases in which lymph node metastases were available for micro- scopical examination the tumor was identical to the primary tumor, while in the fourth the cells were smaller and undifferentiated. Only one vaginal recurrence was biopsied and it closely resembled the primary tumor. One patient (Case 5 ) had a postmortem examina- tion, which revealed widespread pelvic and retroperitoneal metastases, but material was not available for microscopic review.
DISCUSSION
Although this series of 13 cases is small, the data presented confirm the conclusion of Glucksmann and Cherry that the glassy cell carcinoma is an unusually malignant form of cervical cancer that can be recognized on microscopical examination. In their series of cervical carcinomas, 8% were of the mixed type, and of these, 20% were glassy cell carci- nomas, for an incidence of 1.6% of all cervical carcinomas. From the years 1957 to 1973, 991 cervical carcinomas were diagnosed at the Massachusetts General Hospital, and of these, 13 were of the glassy cell variety, resulting in an incidence of 1.3%.
The three major criteria of Glucksmann and Cherry for the microscopical diagnosis of glassy cell carcinoma were adopted in the present investigation: cells with a moderate amount of cytoplasm having a ground-glass or finely granular appearance, a distinct cell wall that stains with eosin and PAS, and large nuclei with prominent nucleoli. Also observed in the present study were several ancillary diagnostic features mentioned by the previous authors: a failure of the tumor cells to stain with mucicarmine or PAS after dia- stase digestion (although they may contain small amounts of glycogen), absent or rare squamous or glandular differentiation, and frequently little or no cytologic change after radiation therapy. Glucksmann and Cherry noted that after irradiation the glassy cells en- larged and occasionally showed some para- keratosis, but typically they exhibited no in- creased differentiation in the form of keratini- zation or mucin production. We observed marked radiation changes in only one of eight
cases in which posttreatment biopsy specimens were available for examination. Other dis- tinctive features of the glassy cell carcinoma include a large cell size (average diameter of 50 p), a high mitotic rate with frequent abnormal forms, and a dense inflammatory infiltrate of plasma cells, eosinophils, or both. Although Glucksmann and Cherry noted that some of their tumors contained signet cells, we did not find them in the present series.
Several types of cervical carcinoma may be easily confused with the glassy cell carcinoma on microscopical examination. The most com- mon of these is the large-cell non-keratinizing squamous cell carcinoma, which is important to distinguish because of its reported radio- sensitivity.aJ’ Histologic features that are often seen in this type of tumor, but very rarely in the glassy cell carcinoma, include intercel- lular bridges, abundant intracellular glycogen, and squamous differentiation in the form of dyskeratotic cells. In addition, this variety of squamodi cell carcinoma usually lacks the prominent cell walls and large nucleoli that are characteristic of the glassy cell carcinoma. Other poorly differentiated and possibly closely related cervical carcinomas have some but not all the characteristics of the glassy cell carcinoma, and still other cervical carcinomas contain minor components of glassy cell car- cinoma; tumors in both these groups should be excluded from the category of glassy cell carcinoma as originally defined.
In addition to their distinct pathologic ap- pearance the tumors in the present series were associated with clinical features different from those of other types of cervical carcinoma. Figure 7, which shows the age distribution of our patients compared to that expected for all patients with carcinoma of the cervix, sug- gests that glassy cell carcinoma occurs in a somewhat younger age group than that of cervical carcinoma in general. Although the average clinical stage (Fig. 8) of the tumors in this series was lower than that of all cervical cancers, the 5-year survival was only 31% compared to an expected survival rate of approximately 50% for cervical carcinomas as a group.6
Two major factors seemed to contribute to the poor survival in this disease. The first was the difficulty of controlling the primary tumor with radiation therapy. Of the ten patients treated by radical radiation therapy alone six had local recurrence. The second factor was

No. 5 GLASSY CELL CARCINOMA Littmtln et al. 2245
FIG. 7. Age distribution of I3 glassy cell carcinomas compared with that of all cervical car- cinomas.
40
30
20 %
10
0
All Carcinomas8
the high rate of metastases outside of the pelvis. Because lymphangiograms. laparot- omies, and postmortem examinations were not performed on all the patients the actual number of cases with distant metastases is not known. Nevertheless, extrapelvic spread was evident in 6/13 of the patients. In contrast the frequency of extrapelvic extension in 2200 patients with squamous cell carcinoma of the cervix who were similarly evaluated was only 15%.’
That a new approach to the management of glassy cell carcinoma is indicated seems evident from the data presented in this paper. The high rate of distant metastases demands i1 very tliorougli evaluation of the possible spread of the tumor before definitive treat- ment is undertaken. A bipedal lymphogram should be performed when ;I patient is con- sidered for curative therapy, and if possible ii laparotomy should also be done to confirm the findings of the lymphogram since the ac- curacy of that technique has not been fully established and the treatment of the para- aortic area by radiation therapy is not without hazards.7 The high rate of local recurrence suggests that some form of combination of both radiation therapy and surgery may be considered, but clearcut recommendations can- not be made at the present time because the 5-year survival rate has heen poor regardless of the various therapelltic approaches in the
20 30 4 0 50 60 70 80
A G E
present series of cases. Owing to the propen- sity of the disease to distant metastases, one should also consider aggressive chemotherapy for this disease even when the lesion may appear to be localized.
In summary, the glassy cell carcinoma war- rants a place in the classification of carcinoma of the cervix. I t is hoped that with analysis of a greater number of cases optimal therapy may be more clearly defined and the poor prognosis of this tumor improved.
% ‘O I ’ 30 I
STAGE
FIG. 8. Stage distribution of 13 glassy cell carcinomas compared with that of all cervical carcinomas.
2246 CANCER May 1976
REFERENCES
VOl. 31
1. Carlson, V.. Delclos. L.. and Fletcher, G. H.: Distant metastases in squamous cell carcinoma of the uterine cervix. Radiology 88:961-966, 1967.
2. Cherry, C. P., and Gliicksmann. A.: Histology of carcinomas of the uterine cervix and survival rates in pregnant and non-pregnant patients. Surg. Gynecol. Obstet. 112763476, 1961.
3. Finck, F. M., and Denk. M.: Cervical carcinoma- Relationship between histology and survival following radiation therapy. Obstet. Gynecol. 35:339-343, 1970.
4. Cliicksmann. A.: Relationships between hormonal changes in pregnancy and the development of “mixed carcinoma” of the uterine cervix. Cancer 10:831-837, 1957.
5. Gliicksmann, A., and Cherry, C. P.: Incidence,
histology, and response to radiation of mixed carci- nomas (adenocanthomas) of the uterine cervix. Cancer
6. International Federation of Gynecology and Obstetrics: Annual Report on the Results of Treat- ment in Carcinoma of the Uterus, Vagina, and Ovary, Volume 15, 1973.
7. Lepanto, P., Littman, P.. Mikuta, J.. Davis, L., and Celebre, J.: Treatment of para-aortic nodes in carcinoma of the cervix. Cancer 35: 1510-1513, 1975.
8. Sadugor, M. G., and Palmer, J. P.: Age, incidence, and distribution of 4,652 cases of carcinoma of the cervix. A m . J . Obstet. Gynecol. 5668M86, 1948.
9. Wentz, W. B.. and Reagan, J. W.: Survival in cer- vical cancer with respect Lo cell type. Cancer 12:384- 388, 1959.
9~971-979, 1956.




















