
Functional training in the management of chronic facial paralysis.
11
doi: 10.2522/ptj.20100404 Originally published online December 22, 2011 2012; 92:605-613. PHYS THER. Thangjam Bindiya V. Prakash, K. Hariohm, P. Vijayakumar and D. Facial Paralysis Functional Training in the Management of Chronic http://ptjournal.apta.org/content/92/4/605 found online at: The online version of this article, along with updated information and services, can be Collections Therapeutic Exercise Self-Care and Home Management Psychosocial: Other Patient/Client-Related Instruction Neurology/Neuromuscular System: Other Case Reports in the following collection(s): This article, along with others on similar topics, appears e-Letters "Responses" in the online version of this article. "Submit a response" in the right-hand menu under or click on here To submit an e-Letter on this article, click E-mail alerts to receive free e-mail alerts here Sign up by guest on May 23, 2014 http://ptjournal.apta.org/ Downloaded from by guest on May 23, 2014 http://ptjournal.apta.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Functional training in the management of chronic facial paralysis.

doi: 10.2522/ptj.20100404Originally published online December 22, 2011
2012; 92:605-613.PHYS THER. Thangjam BindiyaV. Prakash, K. Hariohm, P. Vijayakumar and D.Facial ParalysisFunctional Training in the Management of Chronic
http://ptjournal.apta.org/content/92/4/605found online at: The online version of this article, along with updated information and services, can be
Collections
Therapeutic Exercise Self-Care and Home Management
Psychosocial: Other Patient/Client-Related Instruction
Neurology/Neuromuscular System: Other Case Reports
in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from

Functional Training in theManagement of Chronic FacialParalysisV. Prakash, K. Hariohm, P. Vijayakumar, D. Thangjam Bindiya
Background and Purpose. Disability in patients with facial paralysis is theresult of impairment or loss of complex and multidimensional functions of the face,including expression of emotions, facial identity, and communication. However, themajority of interventions for facial paralysis are unidimensional and impairmentoriented. Thus, a functional training program intended to address various dimensionsof disability caused by facial paralysis was devised. This patient-centered, multi-dimensional approach to the rehabilitation of people with facial paralysis consists ofpatient education, functional training, and complementary exercises. This approachis focused on various dimensions of disability, including the physical, emotional, andsocial dimensions, by encouraging context-specific facial functions, positive copingstrategies, and social interaction skills.
Case Description. The patient was a 25-year-old woman with chronic completeright facial paralysis caused by a postoperative complication of ear surgery. Thepatient’s problems were evaluated with the Facial Disability Index (physical functionsubscale score�45/100, social/well-being function subscale score�28/100) and aninformal interview exploring her experiences and priorities.
Outcomes. After 8 weeks of functional training, the patient showed considerableimprovement in facial functions (physical function subscale score�95/100, social/well-being function subscale score�100/100) and reported positive changes in socialinteractions and interpersonal relationships.
Discussion. The use of a functional training program was associated with positivechanges in emotional expression, psychosocial function, and social integration, thuscontributing to reduced disability of a person with chronic facial paralysis.
V. Prakash, MPT, Charotar Instituteof Physiotherapy, Charotar Univer-sity of Science and Technology,CHARUSAT Campus, Changa, Pet-lad, Anand 388421, Gujarat, India.Address all correspondence to MrPrakash at: [email protected].
K. Hariohm, MPT, MohamedSathak AJ College of Physiother-apy, Chennai, Tamilnadu, India.
P. Vijayakumar, MPT, NavodayaCollege of Physiotherapy, Raichur,Karnataka, India.
D. Thangjam Bindiya, BPT,Department of Physiotherapy,Navodaya Medical College Hospi-tal and Research Centre, Raichur,Karnataka, India.
[Prakash V, Hariohm K, Vijayaku-mar P, Thangjam Bindiya D. Func-tional training in the managementof chronic facial paralysis. PhysTher. 2012;92:605–613.]
© 2012 American Physical TherapyAssociation
Published Ahead of Print:December 22, 2011
Accepted: December 12, 2011Submitted: November 23, 2010
Case Report
Post a Rapid Response tothis article at:ptjournal.apta.org
April 2012 Volume 92 Number 4 Physical Therapy f 605 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from

Facial functions are multidimen-sional, serving emotional, social,and physical aspects of a per-
son’s health. The primary functionsof the face include displaying affec-tive emotions and identifying andcommunicating with other humanbeings.1 Different portions of theface also play a major role in eyeprotection, eating, drinking, andspeech.2 In addition, facial recogni-tion and the perception of facialattractiveness facilitate communica-tion among people by influencinginterpersonal attraction.3 Thesehuman attributes are necessary toestablish and maintain intimate inter-personal relationships and to pre-serve affective social interactions.
Therefore, when a person experi-ences facial paralysis, the concernsencountered also are multidimen-sional. These concerns can rangefrom emotional distress to physicalproblems, such as leaking of foodfrom the mouth, difficulty in commu-nication, and consequent attenua-tion of social interactions.1,2 Animpaired ability to express context-specific emotions can be detrimentalto a person’s sense of emotionalwell-being and the ability to establishand maintain interpersonal relation-ships.1 Such impairments can createa sense of shame and a fear of rejec-tion and being misunderstood ormisjudged by others.4 Condescend-ing reactions by others to the resul-tant facial unattractiveness fromfacial asymmetry can lead to low self-esteem and an unfavorable bodyimage for people with facial paraly-sis.5 In addition, pain or irritationof the eye, unanticipated pronuncia-tion errors while speaking, leakingof fluid and food while drinking andeating—especially in a social con-text—may significantly interferewith daily activities and cause con-siderable physical and psychologicaldistress to people with facial paraly-sis. Consequently, people with facialparalysis may experience over-
whelming negative emotions (eg,social anxiety) and adopt avoidancestrategies, which can lead to adecline in social interactions.6,7
This view is exemplified by the highreported incidence of symptoms ofdepression in people with facial neu-romotor disorders—an incidence 3to 5 times that in the general popu-lation.8 Specifically, impairment ofsmiling was found to be a key pre-dictor of depression in patients withfacial neuromuscular disorders.9
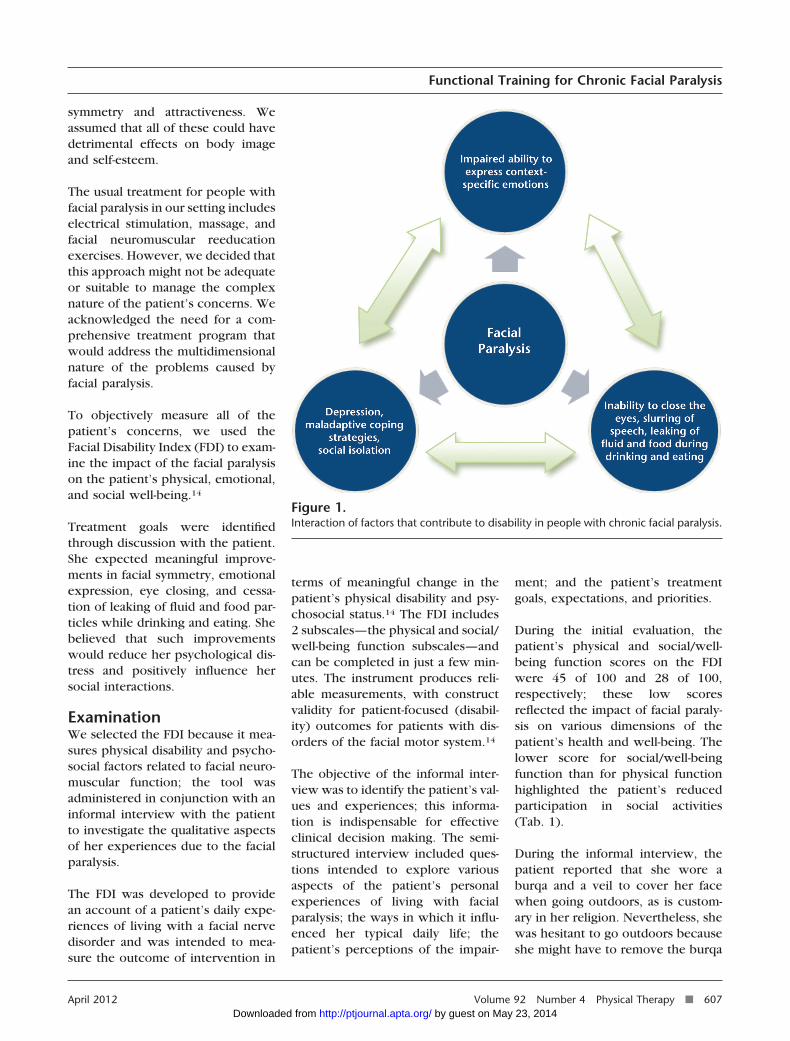
In summary, facial functions arecomplex and multidimensional.Hence, the disability caused by paral-ysis of the facial muscles results froma complex interaction of the afore-mentioned factors (Fig. 1).
However, the majority of existingphysical therapy interventions forfacial paralysis are unidimensional(impairment oriented), and theirclinical effectiveness in improving apatient’s function is limited.10,11 Tra-ditional interventions place moreemphasis on eliciting isolatedactions of facial muscles, such as rais-ing the eyebrows or puckering thelips; these interventions involveeither passive treatments, such aselectrical stimulation,10 or activeexercises, such as facial neuromus-cular reeducation.12 The aim ofmime therapy, a relatively recentintervention in the rehabilitation ofpeople with facial paralysis, is todevelop a conscious connectionbetween the use of certain musclesand facial emotional expression.13
However, this approach addressesonly part of the problem because itis focused on producing volitionalemotional characteristics withoutincorporating the spontaneousexpression of emotions.
The basic assumption underlying allof these intervention strategies isthat improvement in one dimensionof facial dysfunction will automati-
cally lead to overall improvement inothers. Because facial functions arecomplex, any intervention strategyaimed at having a profound impacton the recovery of people with facialparalysis must address the multidi-mensional nature of the disability.Therefore, we developed a func-tional training program that isfocused on the physical, emotional,and psychosocial dimensions of thisdisorder.
The purposes of this case report are:(1) to describe the development ofthe functional training program and(2) to demonstrate the use of thisintervention in the management ofchronic facial paralysis.
Patient History and Reviewof SystemsThe patient was a 25-year-old Indianfemale homemaker who developedchronic complete right facial paraly-sis after ear surgery that occurred 8years earlier. Two years after the sur-gery, she developed severe pain inthe right eye because of constant irri-tation; she consulted an ophthalmol-ogist, who advised her to regularlyuse safety glasses and eyedrops.After 3 to 4 weeks, her pain sub-sided, but she continued to usesafety glasses for about 2 years. Shedid not have any problems related tohearing or taste. As part of her reli-gious practice, she wore a burqa anda veil when going outdoors. Whenshe visited our facility, she had notundergone any physical therapy andhad no active medical problemsother than the facial paralysis.
Her major concerns included inap-propriate facial expressions duringconversations (eg, deviation of themouth to one side while talking orlaughing), inability to close the eyescompletely, leaking of fluid andfood particles while drinking andeating, slurring of speech while talk-ing (especially when angry), andher perception of her altered facial
Functional Training for Chronic Facial Paralysis
606 f Physical Therapy Volume 92 Number 4 April 2012 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from
symmetry and attractiveness. Weassumed that all of these could havedetrimental effects on body imageand self-esteem.
The usual treatment for people withfacial paralysis in our setting includeselectrical stimulation, massage, andfacial neuromuscular reeducationexercises. However, we decided thatthis approach might not be adequateor suitable to manage the complexnature of the patient’s concerns. Weacknowledged the need for a com-prehensive treatment program thatwould address the multidimensionalnature of the problems caused byfacial paralysis.
To objectively measure all of thepatient’s concerns, we used theFacial Disability Index (FDI) to exam-ine the impact of the facial paralysison the patient’s physical, emotional,and social well-being.14
Treatment goals were identifiedthrough discussion with the patient.She expected meaningful improve-ments in facial symmetry, emotionalexpression, eye closing, and cessa-tion of leaking of fluid and food par-ticles while drinking and eating. Shebelieved that such improvementswould reduce her psychological dis-tress and positively influence hersocial interactions.
ExaminationWe selected the FDI because it mea-sures physical disability and psycho-social factors related to facial neuro-muscular function; the tool wasadministered in conjunction with aninformal interview with the patientto investigate the qualitative aspectsof her experiences due to the facialparalysis.
The FDI was developed to providean account of a patient’s daily expe-riences of living with a facial nervedisorder and was intended to mea-sure the outcome of intervention in
terms of meaningful change in thepatient’s physical disability and psy-chosocial status.14 The FDI includes2 subscales—the physical and social/well-being function subscales—andcan be completed in just a few min-utes. The instrument produces reli-able measurements, with constructvalidity for patient-focused (disabil-ity) outcomes for patients with dis-orders of the facial motor system.14
The objective of the informal inter-view was to identify the patient’s val-ues and experiences; this informa-tion is indispensable for effectiveclinical decision making. The semi-structured interview included ques-tions intended to explore variousaspects of the patient’s personalexperiences of living with facialparalysis; the ways in which it influ-enced her typical daily life; thepatient’s perceptions of the impair-
ment; and the patient’s treatmentgoals, expectations, and priorities.
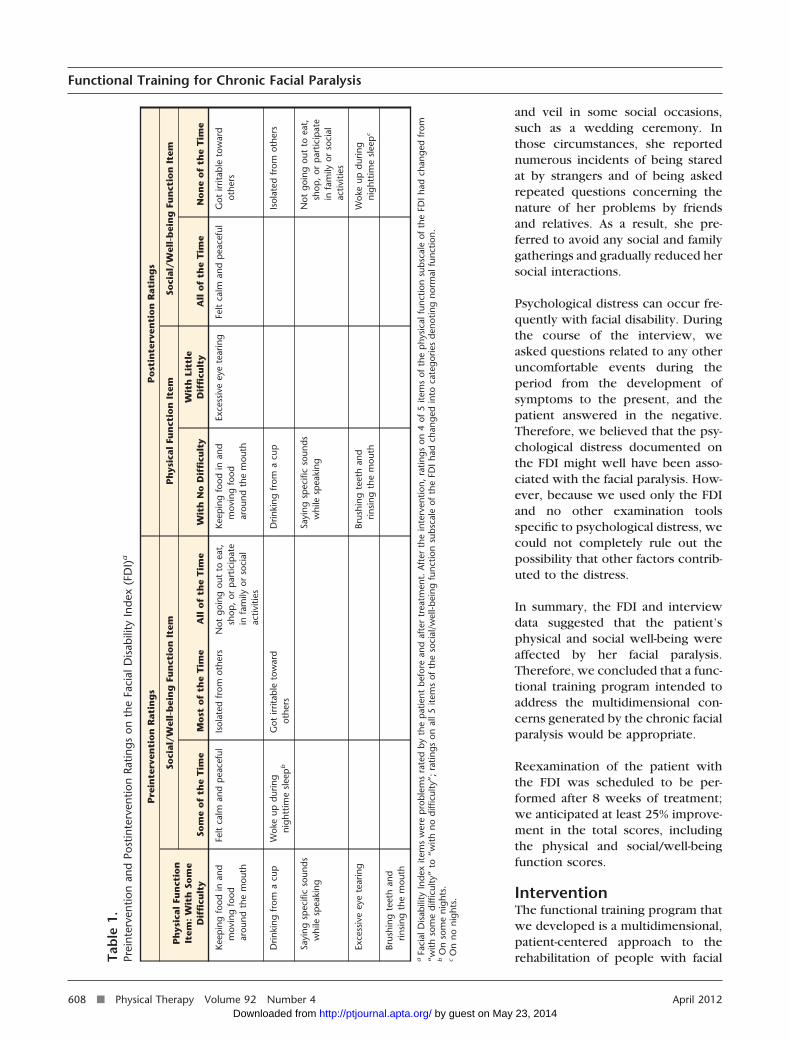
During the initial evaluation, thepatient’s physical and social/well-being function scores on the FDIwere 45 of 100 and 28 of 100,respectively; these low scoresreflected the impact of facial paraly-sis on various dimensions of thepatient’s health and well-being. Thelower score for social/well-beingfunction than for physical functionhighlighted the patient’s reducedparticipation in social activities(Tab. 1).
During the informal interview, thepatient reported that she wore aburqa and a veil to cover her facewhen going outdoors, as is custom-ary in her religion. Nevertheless, shewas hesitant to go outdoors becauseshe might have to remove the burqa
Figure 1.Interaction of factors that contribute to disability in people with chronic facial paralysis.
Functional Training for Chronic Facial Paralysis
April 2012 Volume 92 Number 4 Physical Therapy f 607 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from
and veil in some social occasions,such as a wedding ceremony. Inthose circumstances, she reportednumerous incidents of being staredat by strangers and of being askedrepeated questions concerning thenature of her problems by friendsand relatives. As a result, she pre-ferred to avoid any social and familygatherings and gradually reduced hersocial interactions.
Psychological distress can occur fre-quently with facial disability. Duringthe course of the interview, weasked questions related to any otheruncomfortable events during theperiod from the development ofsymptoms to the present, and thepatient answered in the negative.Therefore, we believed that the psy-chological distress documented onthe FDI might well have been asso-ciated with the facial paralysis. How-ever, because we used only the FDIand no other examination toolsspecific to psychological distress, wecould not completely rule out thepossibility that other factors contrib-uted to the distress.
In summary, the FDI and interviewdata suggested that the patient’sphysical and social well-being wereaffected by her facial paralysis.Therefore, we concluded that a func-tional training program intended toaddress the multidimensional con-cerns generated by the chronic facialparalysis would be appropriate.
Reexamination of the patient withthe FDI was scheduled to be per-formed after 8 weeks of treatment;we anticipated at least 25% improve-ment in the total scores, includingthe physical and social/well-beingfunction scores.
InterventionThe functional training program thatwe developed is a multidimensional,patient-centered approach to therehabilitation of people with facialTa
ble
1.Pr
eint
erve
ntio
nan
dPo
stin
terv
entio
nRa
tings
onth
eFa
cial
Dis
abili
tyIn
dex
(FD
I)a
Pre
inte
rven
tio
nR
atin
gs
Po
stin
terv
enti
on
Rat
ing
s
Ph
ysic
alFu
nct
ion
Item
:W
ith
Som
eD
iffi
cult
y
Soci
al/W
ell-
bei
ng
Fun
ctio
nIt
emP
hys
ical
Fun
ctio
nIt
emSo
cial
/Wel
l-b
ein
gFu
nct
ion
Item
Som
eo
fth
eT
ime
Mo
sto
fth
eT
ime
All
of
the
Tim
eW
ith
No
Dif
ficu
lty
Wit
hLi
ttle
Dif
ficu
lty
All
of
the
Tim
eN
on
eo
fth
eT
ime
Keep
ing
food
inan
dm
ovin
gfo
odar
ound
the
mou
th
Felt
calm
and
pea
cefu
lIs
olat
edfr
omot
hers
Not
goin
gou
tto
eat,
shop
,or
par
ticip
ate
infa
mily
orso
cial
activ
ities
Keep
ing
food
inan
dm
ovin
gfo
odar
ound
the
mou
th
Exce
ssiv
eey
ete
arin
gFe
ltca
lman
dp
eace
ful
Got
irrita
ble
tow
ard
othe
rs
Drin
king
from
acu
pW
oke
updu
ring
nigh
ttim
esl
eep
bG
otirr
itabl
eto
war
dot
hers
Drin
king
from
acu
pIs
olat
edfr
omot
hers
Sayi
ngsp
ecifi
cso
unds
whi
lesp
eaki
ngSa
ying
spec
ific
soun
dsw
hile
spea
king
Not
goin
gou
tto
eat,
shop
,or
par
ticip
ate
infa
mily
orso
cial
activ
ities
Exce
ssiv
eey
ete
arin
gBr
ushi
ngte
eth
and
rinsi
ngth
em
outh
Wok
eup
durin
gni
ghtt
ime
slee
pc
Brus
hing
teet
han
drin
sing
the
mou
th
aFa
cial
Dis
abili
tyIn
dex
item
sw
ere
pro
blem
sra
ted
byth
ep
atie
ntbe
fore
and
afte
rtr
eatm
ent.
Aft
erth
ein
terv
entio
n,ra
tings
on4
of5
item
sof
the
phy
sica
lfun
ctio
nsu
bsca
leof
the
FDI
had
chan
ged
from
“with
som
edi
fficu
lty”
to“w
ithno
diffi
culty
”;ra
tings
onal
l5ite
ms
ofth
eso
cial
/wel
l-bei
ngfu
nctio
nsu
bsca
leof
the
FDI
had
chan
ged
into
cate
gorie
sde
notin
gno
rmal
func
tion.
bO
nso
me
nigh
ts.
cO
nno
nigh
ts.
Functional Training for Chronic Facial Paralysis
608 f Physical Therapy Volume 92 Number 4 April 2012 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from

paralysis. The program encompassesmajor facial functions, integrates therole of contextual factors, and pro-motes positive coping strategies andsocial interaction skills to deal withvarious dimensions of disability,including the physical, emotional,and social well-being dimensions(Fig. 2). The program includespatient education, functional train-ing, and complementary exercises.
Patient EducationThe patient education component ofthe functional training program isbased on principles of cognitive-behavioral training.15,16 The aim ofthis component is to change thebehavior of the patient, rather thanthe physical appearance alone, by
optimizing coping strategies andsocial interaction skills. The educa-tion component has 2 objectives.One objective is to change the wayin which the patient thinks so thathe or she will feel or act better evenif the situation does not change. Theother objective is to reconstruct thepatient’s thoughts and perceptionsof problems, such as negative self-perceptions of facial attractiveness(body image) and interpretations ofothers’ or society’s views toward thepatient’s disability. The contents ofthe patient education componentare shown in Table 2. Patient educa-tion was not provided within a dis-crete treatment session but wasinterwoven with the other compo-
nents of the functional trainingprogram.
Functional TrainingThe aim of functional training is toincorporate the primary movementfunctions of the face, including theexpression of emotions and othermotor functions, into the patient’sdaily activities. In real-life situations,people spontaneously express emo-tions with rapid variations. Emotionsare significantly influenced by thecontext,17,18 such that in somesituations people may feel a mix-ture of emotions, with varyinglevels of intensity, which they tryto hide, alter, or dampen to influencea viewer’s perception. Such sce-narios require both spontaneous
Figure 2.Multidimensional functional training program.
Functional Training for Chronic Facial Paralysis
April 2012 Volume 92 Number 4 Physical Therapy f 609 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from

expression and deliberate expres-sion of emotions, involving differentcombinations of muscle actions thatcannot be easily reproduced by acti-vation outside the context.19,20
Therefore, our training consisted ofactivities such as watching movies,television programs, or humorousvideos and narrating them to thephysical therapist and augmentedperiods of conversation during thetreatment sessions and at home toencourage the expression of emo-tions in a real-life context. Table 3
shows a complete list of theactivities.
We also encouraged the patient to bemore animated during her story nar-rations to enhance her attempts toexpress emotions deliberately andspontaneously. The goal was to pro-vide more opportunities for thepatient to express emotions in con-texts that were relevant to her dailyactivities.
A female physical therapist wasassigned to provide the training to
try to alleviate any reservation thatthe patient might have had about tak-ing part in a free conversation. Treat-ment was provided in a closed andisolated room to avoid outside inter-ruptions during the conversationand to provide adequate privacy totry to alleviate any inhibition that thepatient might have had aboutexpressing herself freely.
Complementary ExercisesThe primary objective of the comple-mentary exercises was to enhancethe level of activity of the facial
Table 2.Patient Education
Objective Education Strategy
To change the way in which the patient thinks to feel or act better even ifthe situation does not change
Only initial encounters may be difficult, and even those can be managedwith positive interaction skills.
Staring by strangers may be more out of curiosity than dislike oraversion and can be effectively managed by smiling, staring back, orignoring them.
Remain calm and politely but assertively confront others with negativereactions.
To reconstruct the patient’s thoughts and perceptions of problems, suchas negative self-perceptions of facial attractiveness and interpretations ofothers’ or society’s views toward the patient’s disability
Challenge the patient’s assumptions about being “defective” and modifyperceptions or apprehensions concerning facial attractiveness byquestioning the functional “cost” of these assumptions.
Constantly reassure the patient that she is cared for and loved by herfamily and friends (as they would look at her beyond physicalappearance) and urge her family to provide frequent encouragementand helpful comments.
Encourage the patient to adopt a positive self-image and be optimisticabout recovery.
Educate family members and friends about the nature of the patient’scondition.
Table 3.Functional Training
Rationale/Objective Functional Training Activity
To facilitate context-specific spontaneous and voluntary expressionof emotions
Watch movies, television programs, and humorous videos.
Narrate stories during treatment sessions in the clinic.
Think about funny incidents that have happened in your life or jokesthat you have heard or read recently and share them with friends orfamily members.
To facilitate motor functions of facial muscles around the eyes,lips, and mouth
Hum or sing songs that you like as often as possible.
Play games such as peek-a-boo or blowing bubbles with children.
Rinse your mouth and spit out the water slowly.
Blow a pipe while imagining that you are cooking in the kitchen andthat the fire in the wood stove suddenly goes out; you have toblow the pipe to start the fire again.
Functional Training for Chronic Facial Paralysis
610 f Physical Therapy Volume 92 Number 4 April 2012 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from

muscles to complement the overalleffort of the patient in achieving theexpression of emotions and othermotor functions of the face. In addi-tion, we believed that a regular exer-cise schedule would motivate thepatient to achieve her own treat-ment goals and might enhance heradherence to the treatment. Theexercises were based on treatmentssuggested by VanSwearingen.12 Thecomplementary exercises were asfollows: suck the cheeks betweenthe teeth; wrap the lips over theteeth; pucker the lips; make thespeech sounds “sh,” “p,” “b,” and “f”with the teeth clenched; and lookdown, close the eyes, and continueto look down with the eyes closed(eye-closing exercise).
DosageFor patient education and functionaltraining, the treating physical thera-pist provided 20- to 30-minute ses-sions to the patient, once per day, 6days per week, for 8 weeks. For com-plementary exercises, the patientwas asked to perform each exercise5 to 10 times, 3 times per day (oncein the clinic and twice at home), 6days per week, for 8 weeks. Theintervention dosage was modified inaccordance with observed changesin the patient’s ability to perform andcope with the exercises.
OutcomeThe patient showed significantimprovements with regard to the ini-tial treatment goals, as measured 8weeks after the commencement oftreatment. Final FDI scores were 95 of100 on the physical function subscaleand 100 of 100 on the social/well-being function subscale, represent-ing postintervention improvementsof 50 and 72 points, respectively(Tab. 1).
Physical functions of the patient’sface that were affected, including dif-ficulty with eye closing, leaking offluid and food while drinking and
eating, and slurring of speech,improved considerably. This improve-ment was manifested as a 50-pointincrease in the score on the physicalfunction subscale of the FDI relativeto the pretreatment score. The rat-ings for 4 of the 5 items on thissubscale improved from “with somedifficulty” to “with no difficulty”(Tab. 1).
During our clinical observations ofthe patient, we noted no apparentchanges in some actions, such as vol-untary smiling and the ability to raisethe eyebrows. However, we notedobvious improvements in her facialsymmetry at rest, which wererevealed in our comparison of stillphotographs taken during variousstages of treatment. In line with ourobservations, the patient alsoreported positive changes in her per-ception of her facial attractiveness,which may have been due to thechanges in facial symmetry at rest.We believe that such changes werereflected in her renewed interest inwearing jewelry and makeup.
We observed substantial progress inthe patient’s social functions as well.During the posttreatment interview,she reported that her family mem-bers were happy with the results ofthe treatment and appreciated herefforts. She felt more confidentgoing outdoors and provided a fewexamples of social gatherings thatshe previously had avoided but nowattended without inhibition or feel-ings of stigma. In addition, shereported marked improvements inher interpersonal relationships andsocial interactions. These observa-tions may explain the changesrecorded in the postinterventionscore on the social/well-being func-tion subscale of the FDI, with normalfunction being recorded for all 5items at the end of the intervention.
DiscussionThe purpose of this case report were2-fold: first, to describe the develop-ment of our functional training pro-gram, and second, to demonstrate itsuse for the management of chronicfacial paralysis. After the 8-weekfunctional training program, thepatient showed substantial improve-ments in physical, psychological,and social functions affected by herfacial paralysis.
In the rehabilitation of people withfacial paralysis, patient educationtypically includes information aboutthe anatomy of the facial nerves,facial musculature, and synkinesis12
as well as the recovery process.21
Such an approach may be inade-quate when a patient’s primary con-cern arises from the disabling psy-chosocial consequences of facialparalysis, including low self-esteem,social isolation, and altered emo-tional well-being. Therefore, wedevised a patient education programthat is specifically focused on thedevelopment of positive copingstrategies and social interactionskills.
During the posttreatment interview,the patient reported that her familymembers had identified noticeableimprovement in her face. As men-tioned previously, she spoke ofseveral social occasions that sheattended without hesitation or feel-ings of rejection. In Indian culture, itis customary for a woman to wearjewelry, especially during socialoccasions, as an important indicatorthat she is feeling good about herself.The patient’s renewed interest inwearing jewelry and makeup helpedreassure us that her perception ofher facial attractiveness and bodyimage had improved. In addition, wenoted that she started removing herveil after entering our clinic, some-thing she previously had been reluc-tant to do. When asked about thisnew behavior, she replied that she
Functional Training for Chronic Facial Paralysis
April 2012 Volume 92 Number 4 Physical Therapy f 611 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from

removed her veil more frequentlynow. Such behavioral transforma-tions clearly indicate improved socialinteraction skills, self-perceptionof body image, self-esteem, andconfidence.
Similar findings were reported instudies investigating the effective-ness of cognitive-behavioral trainingin people with facial disfigurement;these findings included positive out-comes in terms of self-esteem, devel-opment of positive coping strategies,reduction in social anxiety, andimprovement in social skills.22,23
The functional training componentof our program encourages and pro-vides opportunities to expresscontext-specific, variable emotionswithin a patient’s natural environ-ment and involves tasks that facili-tate other facial motor functionswithin that environment, such asrinsing the mouth and spitting outthe water or playing games such asblowing bubbles with children.Intervention strategies such aswatching movies, television pro-grams, or humorous videos, discuss-ing them during treatment sessions,and sharing funny incidents or jokeswith friends provide more opportu-nities to express felt emotions withina real-world context. While watch-ing movies, people tend to mimic(emotional contagion) or react to theemotions displayed in the scenebeing watched, and this behaviormay facilitate the spontaneousexpression of emotions.24
During narrative discussions, weobserved that the patient was able toexpress a variety and a mixture ofemotions and switch from theexpression of one emotion toanother more easily than before. Herexpressions involved movements ofthe corners of the lips and wrinklingof the skin at the outer edge of theaffected eye, movements that shehad been unable to produce volun-
tarily. These observations could havebeen due to the involvement of dif-ferent neural pathways25,26 for spon-taneous expression and voluntaryexpression of emotions. In addition,spontaneous expression involvescombinations of muscle actions thatcannot be easily reproduced by vol-untary effort.19,20
Complementary exercises also mighthave contributed to the changesobserved on the physical functionsubscale of the FDI, such as improve-ments in the ability to drink and eatwithout leaking of fluid and foodfrom the mouth and in the ability toclose the eyes. Thus, we believe thatthe effects of the components of thefunctional treatment program weresynergistic, leading to improvementsin multiple aspects of function(Fig. 2).
In patients with facial paralysis,there may be a gap between “capac-ity” (what they can do at their best)and “performance” (the execution ofthat activity in the real world); thisgap may be mediated by the psycho-logical distress experienced bypatients.9 In other words, patientsmay underperform because of theadoption of negative coping strate-gies. These circumstances furtherworsen their condition, eventuallycausing further decline in their exist-ing capacity. We hoped to narrowthe gap between capacity and per-formance by encouraging positivecoping strategies and social interac-tions to deal with psychologicaldistress and social isolation whilesimultaneously creating moreopportunities to express emotionsand perform other facial motor func-tions. Although there was relativelyless improvement in the patient’sability to voluntarily activate individ-ual muscles, the positive changes inthe patient’s expression of emotionsand coping strategies resulted in con-siderable achievement of social inte-
gration, the ultimate goal of any reha-bilitation strategy.
In summary, we believe that themultidimensional approach of ourfunctional training program foraddressing the expression of emo-tions, altered body image and self-esteem, and negative coping strate-gies would be an appropriateintervention strategy for the com-plex problems experienced by peo-ple with chronic facial paralysis. Theinterventions need not be limited tothose described in this report. Usingthe conceptual framework of thefunctional training program, clini-cians can develop specific strategiesthat are relevant to their patients’contextual factors (including per-sonal, social, and cultural factors).Examination of the effects of thefunctional training program withmore rigorous, controlled researchdesigns or a series of single-subjectexperimental designs could serve tovalidate the observations of this casereport.
All authors provided concept/idea/researchdesign and consultation (including review ofmanuscript before submission). Mr Prakashand Mr Hariohm provided writing. MsThangjam Bindiya provided data collection.Mr Prakash, Mr Hariohm, and Ms ThangjamBindiya provided data analysis. Mr Vijaya-kumar provided the participant andfacilities/equipment.
Ms Thangjam Bindiya was participating in aninternship during data collection.
The authors thank Dr Susan R. Harris and MrR. Vasanthan for their assistance in editing anearlier version of this article.
DOI: 10.2522/ptj.20100404
References1 Twerski AJ, Twerski B. The emotional
impact of facial paralysis. In: May M, ed.The Facial Nerve. New York, NY: ThiemeInc; 1986:788–794.
2 de Swart BJ, Verheij JC, Beurskens CHG.Problems with eating and drinking inpatients with unilateral peripheral facialparalysis. Dysphagia. 2003;18:267–273.
Functional Training for Chronic Facial Paralysis
612 f Physical Therapy Volume 92 Number 4 April 2012 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from

3 Fink B, Penton-Voak I. Evolutionary psy-chology of facial attractiveness. Curr DirPsychol Sci. 2002;11:154–158.
4 Brown WM, Moore C. Smile asymmetriesand reputation as reliable indicators oflikelihood to cooperate: an evolutionaryanalysis. Adv Psychol Res. 2002;11:59–78.
5 Rumsey N, Harcourt D. Body image anddisfigurement: issues and interventions.Body Image. 2004;1:83–97.
6 Coulson SE, O’Dwyer NJ, Adams RD, Crox-son GR. Expression of emotion and qualityof life after facial nerve paralysis. Otol Neu-rotol. 2004;25:1014–1019.
7 Ekman P. Psychosocial aspects of facialparalysis. In: May M, ed. The Facial Nerve.New York, NY: Thieme Inc; 1986:781–787.
8 VanSwearingen JM, Cohn JF, Turnbull J,et al. Psychological distress: linkingimpairment with disability in facial neuro-muscular disorders. Otolaryngol HeadNeck Surg. 1998;118:790–796.
9 VanSwearingen JM, Cohn JF, Bajaj-LuthraA. Specific impairment of smilingincreases the severity of depressive symp-toms in patients with facial neuromusculardisorders. Aesthetic Plast Surg. 1999;23:416–423.
10 Teixeira LJ, Soares BG, Vieira VP, PradoGF. Physical therapy for Bell’s palsy (idio-pathic facial paralysis). Cochrane Data-base Syst Rev. 2008;3:CD006283.
11 Cardoso JR, Teixeira EC, Moreira MD,et al. Effects of exercises on Bell’s palsy:systematic review of randomized con-trolled trials. Otol Neurotol. 2008;29:557–560.
12 VanSwearingen JM. Facial rehabilitation: aneuromuscular reeducation, patient-centered approach. Facial Plast Surg.2008;24:250–259.
13 Buerskens CHG, Heymans PG. Mime ther-apy improves facial symmetry in peoplewith long-term facial nerve paresis: a ran-domised controlled trial. Aust J Phys-iother. 2006;52:177–183.
14 VanSwearingen JM, Brach JS. The FacialDisability Index: reliability and validity of afunctional assessment instrument for dis-orders of the facial neuromuscular system.Phys Ther. 1996;76:1288–1300.
15 Partridge J. Changing Faces: The Chal-lenge of Facial Disfigurement. London,United Kingdom: Penguin Books; 1994.
16 Clarke A. Psychosocial aspects of facial dis-figurement: problems, management andthe role of a lay-led organization. PsycholHealth Med. 1999;4:127–142.
17 Barrett LF. Variety is the spice of life: apsychological construction approach tounderstanding variability in emotion.Cogn Emot. 2009;23:1284–1306.
18 Barrett LF, Kensinger EA. Context is rou-tinely encoded during emotion percep-tion. Psychol Sci. 2010;21:595–599.
19 Cohn JF, Schmidt KL. The timing of facialmotion in posed and spontaneous smiles.International Journal of Wavelets, Multi-resolution, and Information Processing.2004;2:1–12.
20 Schmidt KL, Ambadar Z, Cohn JF, Reed LI.Movement differences between deliberateand spontaneous facial expressions: zygo-maticus major action in smiling. J Nonver-bal Behav. 2006;30:37–52.
21 Brach JS, VanSwearingen JM. Physical ther-apy for facial paralysis: a tailored treatmentapproach. Phys Ther. 1999;79:397–404.
22 Robinson E, Rumsey N, Partridge J. Anevaluation of the impact of social interac-tion skills training for facially disfiguredpeople. Br J Plast Surg. 1996:1:281–289.
23 Veale D, Gournay K, Dryden W, et al. Bodydysmorphic disorder: a cognitive behav-ioural model and pilot randomised con-trolled trial. Behav Res Ther. 1996;34:717–729.
24 Lundqvist LO, Dimberg U. Facial expres-sions are contagious. Int J Psychophysiol.1995;9:203–211.
25 Wild B, Rodden FA, Grodd W, Ruch W.Neural correlates of laughter and humour.Brain. 2003;126:2121–2138.
26 Berkman ET, Lieberman MD. Using neuro-science to broaden emotion regulation:theoretical and methodological consider-ations. Soc Personal Psychol Compass.2009;3:475–493.
Functional Training for Chronic Facial Paralysis
April 2012 Volume 92 Number 4 Physical Therapy f 613 by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from
doi: 10.2522/ptj.20100404Originally published online December 22, 2011
2012; 92:605-613.PHYS THER. Thangjam BindiyaV. Prakash, K. Hariohm, P. Vijayakumar and D.Facial ParalysisFunctional Training in the Management of Chronic
References
http://ptjournal.apta.org/content/92/4/605#BIBLfor free at: This article cites 22 articles, 6 of which you can access
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on May 23, 2014http://ptjournal.apta.org/Downloaded from




















