Facial motion analysis of acid burn victims—Development of a new facial motion impairment index
10
Facial motion analysis of acid burn victims—Development of a new facial motion impairment index Samuel Ghani a, *, Ashim Mannan a , Ahmed Kaucer a , Samanta Lal Sen b , Alex Clarke c , Peter Butler c , Annabel Cartwright d a Thikhana House, Acid Survivors Foundation, Dhaka, Bangladesh b Dhaka Medical College Hospital, Dhaka, Bangladesh c Department of Plastic Surgery, Royal Free Hospital, London, UK d Department of Astrophysics, University of Cardiff, Cardiff, UK 1. Introduction The need for an accurate and reproducible method of assessing facial function, and planning surgical reconstruc- tion, has long been recognised by clinicians. Most efforts focussed on patients suffering congenital and/or acquired facial paralysis [1–15]. Traditional assessments of facial movement and the degree of facial dysfunction relied on the subjective judgement of a trained observer. Numerous subjective facial functional grading scales have been proposed. Most notable of these include the House– Brackman grading scale (HBGS), Toronto (Sunnybrook) facial burns xxx (2007) xxx–xxx article info Article history: Accepted 5 August 2006 Keywords: Acid assault Facial burns Facial motion analysis Facial motion impairment index abstract Objectives: Evaluation of facial movement is necessary for the assessment of motor deficits and planning reconstructive surgery in facial burns. Clinicians recognise the need for an accurate and reproducible method of functional assessment. We propose a new facial functional impairment index (FFII) for assessing facial motor dysfunction due to severe burn injury and provide inter/intra-patient comparison for documenting rehabilitation. Methods: The maximal static response assay (MSRA) was used to compare facial movement in 20 acid burn victims with 20 control subjects. Data compiled from 12 soft tissue landmarks was used to quantify rest and dynamic asymmetry, anatomic and non-anatomic motion and calculate the FMII. The Katz score, Nottingham index and number of affected aesthetic units provided insight into FFII efficacy. Results: Patients with greater aesthetic disfigurement demonstrated significantly poorer anatomic function (c = 0.62; p = 0.03) as well as larger global facial functional impairment (c = 0.52; p = 0.08). Conclusion: Acid burns caused severe asymmetry and functional impairment. The FFII is a composite score of global function based on a reproducible method of data collection and it differentiated between acid burn victims and provided objective comparative measures. Software automation, integration of video and 3D data, appropriate graphical and pictorial depiction of variables and measurements, and further research into the accuracy of FFII as a marker of clinical recovery and assessment of function in facial burns, will enhance future clinical applications and potentially aid surgical reconstruction. # 2006 Elsevier Ltd and ISBI. All rights reserved. * Corresponding author at: 34 Miles Drive, Thamesmead, London SE28 0JA, UK. E-mail address: [email protected] (S. Ghani). JBUR-2422; No of Pages 10 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/burns 0305-4179/$30.00 # 2006 Elsevier Ltd and ISBI. All rights reserved. doi:10.1016/j.burns.2006.08.024 Please cite this article in press as: Ghani S, et al., Facial motion analysis of acid burn victims—Development of a new facial motion impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
Transcript of Facial motion analysis of acid burn victims—Development of a new facial motion impairment index

JBUR-2422; No of Pages 10
Facial motion analysis of acid burn victims—Developmentof a new facial motion impairment index
Samuel Ghani a,*, Ashim Mannan a, Ahmed Kaucer a, Samanta Lal Sen b, Alex Clarke c,Peter Butler c, Annabel Cartwright d
aThikhana House, Acid Survivors Foundation, Dhaka, BangladeshbDhaka Medical College Hospital, Dhaka, BangladeshcDepartment of Plastic Surgery, Royal Free Hospital, London, UKdDepartment of Astrophysics, University of Cardiff, Cardiff, UK
b u r n s x x x ( 2 0 0 7 ) x x x – x x x
a r t i c l e i n f o
Article history:
Accepted 5 August 2006
Keywords:
Acid assault
Facial burns
Facial motion analysis
Facial motion impairment index
a b s t r a c t
Objectives: Evaluation of facial movement is necessary for the assessment of motor deficits
and planning reconstructive surgery in facial burns. Clinicians recognise the need for an
accurate and reproducible method of functional assessment. We propose a new facial
functional impairment index (FFII) for assessing facial motor dysfunction due to severe
burn injury and provide inter/intra-patient comparison for documenting rehabilitation.
Methods: The maximal static response assay (MSRA) was used to compare facial movement
in 20 acid burn victims with 20 control subjects. Data compiled from 12 soft tissue landmarks
was used to quantify rest and dynamic asymmetry, anatomic and non-anatomic motion
and calculate the FMII. The Katz score, Nottingham index and number of affected aesthetic
units provided insight into FFII efficacy.
Results: Patients with greater aesthetic disfigurement demonstrated significantly poorer
anatomic function (c = 0.62; p = 0.03) as well as larger global facial functional impairment
(c = 0.52; p = 0.08).
Conclusion: Acid burns caused severe asymmetry and functional impairment. The FFII is a
composite score of global function based on a reproducible method of data collection and it
differentiated between acid burn victims and provided objective comparative measures.
Software automation, integration of video and 3D data, appropriate graphical and pictorial
depiction of variables and measurements, and further research into the accuracy of FFII as a
marker of clinical recovery and assessment of function in facial burns, will enhance future
clinical applications and potentially aid surgical reconstruction.
# 2006 Elsevier Ltd and ISBI. All rights reserved.
avai lab le at www.sc iencedi rec t .com
journal homepage: www.e lsev ier .com/ locate /burns
1. Introduction
The need for an accurate and reproducible method of
assessing facial function, and planning surgical reconstruc-
tion, has long been recognised by clinicians. Most efforts
focussed on patients suffering congenital and/or acquired
* Corresponding author at: 34 Miles Drive, Thamesmead, London SE28E-mail address: [email protected] (S. Ghani).
0305-4179/$30.00 # 2006 Elsevier Ltd and ISBI. All rights reserved.doi:10.1016/j.burns.2006.08.024
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
facial paralysis [1–15]. Traditional assessments of facial
movement and the degree of facial dysfunction relied on
the subjective judgement of a trained observer.
Numerous subjective facial functional grading scales have
been proposed. Most notable of these include the House–
Brackman grading scale (HBGS), Toronto (Sunnybrook) facial
0JA, UK.
lysis of acid burn victims—Development of a new facial motion

b u r n s x x x ( 2 0 0 7 ) x x x – x x x2
JBUR-2422; No of Pages 10
grading system and the facial clinimetric evaluation scale
(FACE) [5,16,17]. The HBGS is regarded as the gold standard.
However, recent advances in objective grading systems,
using photographic and video analysis of the mimic muscle
system, have rendered subjective assessments unsuitable for
detecting clinically important change over the course of time
and/or treatment [15]. Most objective grading systems are
based on measuring displacement of pre-defined soft tissue
landmarks [7–9,13]. Photographic analysis yielding displace-
ment vectors, following a series of voluntary facial anima-
tions, is defined as the maximal static response assay (MSRA).
Recently emphasis has shifted to perfecting the measurement
of mimic movements in three dimensions as opposed to two
[18–20].
Despite new methods of objective measurement of facial
motion, authors found it difficult to integrate these into an
objective ‘facial functional impairment index’. Murty et al.
[13] proposed the Nottingham system for scoring unilateral
facial paralysis—an objective facial functional grading tool
measuring inter-landmark distances during eyebrow raise,
maximal eye closure and closed lip smile and expressing
them as a ratio of affected side to unaffected. However,
Linstrom demonstrated flaws in this approach. He showed
that unilateral facial paralysis patients with synkinesis move
not only remote regions of the face on the affected side, but
also remote regions on the normal side in an attempt to
compensate for the loss of function on the affected side [21].
Hence, the Nottingham index, reliant on comparison between
both sides of the face, is inherently compromised by this
overcompensation. In addition this scale is not applicable in
bilateral facial pathology.
The vast majority of functional assessment has been
within the context of facial paralysis with little attention to
facial trauma. The concept of developing a facial functional
analysis protocol for reliable assessment of facial pathology
ranging from paralysis to trauma and their associated
complications has not been actively considered.
House defined the requirements of an effective facial
grading system as follows: scoring should differentiate
between patients who are different; should represent some-
thing meaningful and defined; and should measure secondary
defects—for example synkinesis, crocodile tears, eye dryness
and taste disturbances in facial paralysis. Facial dysfunction
should also be measured on a continuum, to effectively
measure intermediate levels and differentiate subtle differ-
ences in facial function [22,23]. This was reinforced by
Linstrom’s suggestion of an international facial nerve grading
system, emphasising the importance of a composite score of
several different observations yielding both a total picture
(Gestalt) of the whole and regional pictures of facial expression
[18]. The aim of this study was to develop a new facial
functional impairment index (FFII) to allow effective inter-
patient comparison and objective quantification of facial
function.
2. Materials and methods
We conducted this study in Bangladesh and performed facial
functional analysis of acid burn victims using MSRA. Acid
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
attacks are a unique form of vicious violence resulting in
permanent physical stigmata including devastating facial
scarring, visual impairment and blindness [24,25]. Bangladesh
has the highest reported incidence of acid attacks in the world
constituting 9% of all burns [25,26]. Perpetrators normally
target the face, although burns to the scalp, neck and arms are
frequent. Ethical approval was obtained from the Royal Free
Hospital, London.
2.1. Patient group
Twenty female acid burn victims were recruited from the
Acid Survivors Foundation—a non-government organisation
set up to cater for the medical, surgical and psychological
needs of acid burn survivors. Patients ranged from 16 to 25
years of age. All were of Bangladeshi origin and had been
attacked with sulphuric acid. All burns were due to refusal of
sexual advances or marriage proposals from male perpe-
trators. A lack of first aid knowledge resulted in none of
these patients receiving immediate irrigation of wounds and
mean time of presentation to a tertiary care centre was 4.5
days. All patients underwent a minimum of two full
thickness skin grafts and prior to our assessment had not
been subjected to any surgical intervention for at least 2
years. Scarring ranged from mild to severe hypertrophic
scarring. Patients with keloids were excluded from this
assessment.
2.2. Control group
Twenty females with no history of facial disfigurement or
facial pathology were selected. They ranged from 16 to 21
years of age and were all of Bangladeshi origin and similar
socio-economic status.
2.3. Aesthetic assessments
Digital AP photographs (SONY DSC-L1) of the control and
patients groups were taken at rest. The inner canthal–lateral
oral commissure, outer canthal–lateral oral commissure and
alar–lateral oral commissure distances were measured and
expressed as a ratio of right to left. Individual patient ratios
were statistically compared to mean control group measures.
z-Scores were calculated based on control group mean and
standard deviations. For patients with z-scores greater than 2,
cumulative probability scores were used to devise a contin-
uous asymmetry index from 0 to 1. All those with z-scores less
than 2 (i.e. within 95% confidence interval) had an asymmetry
index of 0.
Mean control facial shape was calculated and expressed as
the ratio of bizygomatic width to face height (nasion to most
inferior midpoint on the chin). Subsequently the facial shape
index was calculated for each patient and statistically
compared to the control group [27].
Patient group facial disfigurement was assessed using the
Katz score and the number of affected aesthetic units based on
Gonzales–Ulloas’s original regional classification [28,29]. The
presence and magnitude of scleral show was noted in acid
burn patients as well as ectropion, corneal scarring and
presence/absence of complete loss of the auricle.
lysis of acid burn victims—Development of a new facial motion

b u r n s x x x ( 2 0 0 7 ) x x x – x x x 3
JBUR-2422; No of Pages 10
2.4. Functional assessment
A MSRA analysis of the control and patient groups was
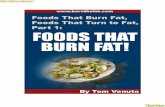
conducted. Twelve soft tissue landmarks were highlighted on
all subjects using a surgical marker pen (Fig. 1):
1. Below lower lip at the midpoint of the left and right lateral
oral commissures.
2. Right lateral oral commissure.
3. Left lateral oral commissure.
4. Above upper lip at the midpoint of the left and right lateral
oral commissures.
5. Right infraorbit.
6. Rhinion (bony-cartilaginous junction along the nasal
dorsum).
7. Left infraorbit.
8. Right lateral canthus.
9. Right superiority.
10. Point directly above the rhinion in line with the left and
right supraorbit.
11. Left superiority.
12. Left lateral canthus.
Patients were asked to stand to their full height and place
their head within a fixed space frame measuring
30 cm � 30 cm. They rested their chin on a chin rest and head
was secured using the head clamp. A series of digital
photographs were taken of the following facial animations:
Fig. 1 – Facial motif illustrating soft tissue landmarks
highlighted for maximal static response assay
measurement.
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
1. Neutral pose (Rest).
2. Eyebrow raise (ER).
3. Maximum eye closure—eyes closed as tightly as possible
(MEC).
4. Minimum smile—smile without opening the mouth (MINS).
5. Maximum smile—smile showing the teeth (MAXS).
6. Purse lip (PL).
Each patient repeated these facial animations three times.
Images were downloaded and edited on Adobe Photoshop
5.5ME (Adobe Systems Inc., Mountain View, CA). All twelve
points marked on the face at rest, were given a (x, y) coordinate
based on an origin sited at the midpoint of the inter-tragal
distance [21,30]. Following each facial expression the new
positions of each of the 12 points were measured and resultant
vectors relative to neutral pose, were calculated.
Soft tissue displacement was subdivided into anatomic and
non-anatomic components. Anatomic motion is termed the
motion of specific facial points studied by the MSRA that can
be attributed solely to the pull of the regional facial muscles
that govern the movement of these points [31]. Non-anatomic
motion is described as movement at points elsewhere on the
face. Designation of anatomic and non-anatomic motion was
standardised based on the facial action coding sequence
(FACS). This is a database consisting of breakdown of facial
expressions into action units that correspond to specific facial
muscles responsible for the facial expression under consid-
eration [32,33] (Table 1).
For each facial expression, markers within the ‘active’
regions of the face demonstrated activity of specific muscle
groups defined by the FACS. Movement at all other landmarks
was considered non-anatomic. This classification was carried
out for each facial expression enabling functional analysis of
the upper, mid and lower thirds of the face. In addition the
Nottingham score was also calculated for all patients.
2.5. Facial functional impairment index (FFII)
Statistical comparison of patient derived vectors for each soft
tissue landmark for each facial expression with corresponding
mean control group vectors was carried out. z-Scores of
greater than 2 were regarded as being significantly abnormal.
Cumulative probability scores for significantly abnormal
vectors were used to calculate a continuous impairment
index, ranging from 0 to 1, for a variety of parameters
consisting of: (1) x-directional movement; (2) y-directional
movement; (3) total magnitude; (4) bearing. These were
totalled to produce the facial functional impairment index
(FFII). The FFII was subsequently broken down into anatomic
and non-anatomic components based on soft tissue designa-
tions described above. The complete method for FFII calcula-
tion was reviewed by a mathematician and found to be sound.
2.6. Statistical analysis
Rest asymmetry, facial shape index, Katz score, affected
aesthetic units, Nottingham score and facial functional impair-
ment index were all measured and calculated for the patient
group.Statistical analysis of relationship between aesthetic and
functional measures of disfigurement was conducted.
lysis of acid burn victims—Development of a new facial motion

Table 1 – Table listing the action units and muscles actively involved in each facial expression assessed
Facial expression (AU: action unit) Anatomic (blue) and non-anatomic (red)
Eyebrow raise (ER)
AU 1: frontalis, pars medialis
AU 2: frontalis, pars lateralis
Maximum eye closure (MEC)
AU 4: corrugator supercilli, depressor supercilli
AU 43: orbicularis oris, pars palpebralis
Minimum smile (MINS)
AU 6: orbicularis oculi, pars orbitalis
AU 12: zygomaticus major
AU 14: buccinator
AU 24: orbicularis oris (lips pressed together)
Maximum smile (MAXS)
AU 6: orbicularis oculi, pars orbitalis
AU 12: zygomaticus major
AU 20: risorius with platysma
AU 25: depressor labii inferioris
Purselip (PL)
AU 18: incisive labii superioris, incisive labii inferioris
Adjacent facial motifs showing designated anatomic and non-anatomic soft tissue landmarks. This designation is later used to derive
anatomic and non-anatomic facial functional impairment scores.
b u r n s x x x ( 2 0 0 7 ) x x x – x x x4
JBUR-2422; No of Pages 10
3. Results
3.1. Aesthetic assessments
Control subjects were of poor socioeconomic status and had
no history of facial trauma, otologic or neurotologic
disorders, facial plastic or otologic surgery; and no known
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
lesion which would predispose the individual to facial
paralysis [21]. Patient group consisted of 10 individuals with
unilateral burns and 10 with bilateral. Facial lesions involved
both skin and muscle. Contractures and hypertrophic scars
were widespread and all injuries were full thickness. Specific
facial injuries included scalp burns (45%), ear injuries and/or
complete loss of the auricle (55%), nose injuries (85%), lips
lysis of acid burn victims—Development of a new facial motion

Fig. 2 – Graph showing excellent positive correlation
between Katz score and the number of affected aesthetic
units.
b u r n s x x x ( 2 0 0 7 ) x x x – x x x 5
JBUR-2422; No of Pages 10
(55%) and neck involvement (40%). Ophthalmic injuries
consisted of scleral show (65%), eyelid injuries (75%),
ectropion (25%) and corneal scarring (30%). They were
initially treated in Bangladesh and received localised
pressure therapy and steroid injections in addition to basic
surgical scar treatments.
3.2. Asymmetry index
The control group demonstrated level horizontal inner canthi,
outer canthi and lateral oral commissures with no scleral
show. There was no significant rest asymmetry. The mean left
outer canthal–lateral oral commissure distance was slightly
greater than the right (t-test: p = 0.56, p > 0.05). Mean right
inner canthal–lateral oral commissure and alar–lateral oral
commissure distances were greater than the left (t-test:
p = 0.09 and p = 0.069). Mean total difference between right
and left measures was 0.37 cm with a standard deviation of
0.21 cm.
Most patients complained of significant tightening of the
skin, pruritis, pain, and muscle spasm. Ten acid burn victims
demonstrated significant canthal asymmetry. These
patients had widespread unilateral or bilateral burns and
resultant abnormal displacement of the canthi was the
net result of contractual forces acting from above and/or
below.
Amongst the patient group, the inner canthi, outer canthi
and lateral oral commissures were found to be asymmetric in
the horizontal plane. Mean right left measure differences were
significantly greater for patients than control group (p = 0.003;
p < 0.05). Unilateral and bilateral burns, individually, had
significantly greater asymmetry than control group (p = 0.006
and p = 0.005, respectively). There was no significant differ-
ence in asymmetry between patients with unilateral and
bilateral burns.
3.3. Facial shape
There was no significant difference between patient and
control bizygomatic ( p = 0.53), facial height (p = 0.29) and
subsequent facial shape index (p = 0.14).
Fig. 3 – Total, anatomic and non-anatomic marker displacemen
maximum eye closure; MINS: minimum smile; MAXS: maximu
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
3.4. Katz score and aesthetic units
The mean Katz score was 6.9 (range = 6) with five patients
scoring � 8 (maximum score = 9). Standard deviation was 1.5.
The mean number of burn affected aesthetic units was 5.4
units with a standard deviation of 2.6. The Katz score and
number of affected aesthetic units are both markers of
aesthetic disfigurement and correlated well. A correlation
coefficient of 0.86 was achieved with a p-value of <0.01 for
ANOVA single factor analysis (Fig. 2).
3.5. Functional assessment
All normal subjects were able to carry out each facial
animation. Acid burn victims demonstrated reduced mean
total marker displacement (sum of vector magnitude for each
soft tissue marker) for each facial expression, except eyebrow
raise (ER), relative to control group. Total displacement was
subdivided into anatomic and non-anatomic components for
each facial expression. Total patient mean anatomic displace-
ment was reduced in maximum eye closure (MEC), maximum
smile (MAXS), and significantly in minimum smile (MINS).
t for patients and controls. ER: eyebrow raise; MEC:
m smile; PL: purse lip.
lysis of acid burn victims—Development of a new facial motion

Table 2 – Two tailed t-test p values for mean totaldisplacement (cm) for control subjects and acid burnpatients
Facial animation Two tailed t-test p values
Total Anatomic Non-anatomic
Eyebrow raise 0.42 0.38 0.57
Max eye closure 0.15 0.12 0.86
Min smile 0.20 0.01 0.43
Max smile 0.20 0.08 0.78
Purse lip 0.65 0.63 0.19
There was no significant difference in total displacement between
controls and patients for any expression.
Fig. 4 – Graph showing global FFII scores for each patient
with global anatomic FFII (blue) and global non-anatomic
FFII (red) components. (For interpretation of the references
to colour in this figure legend, the reader is referred to the
web version of the article.)
b u r n s x x x ( 2 0 0 7 ) x x x – x x x6
JBUR-2422; No of Pages 10
Conversely total patient mean non-anatomic displacement
was greater in ER, MINS and MAXS. However, this was not
statistically significant. There was no significant difference in
total displacement between controls and patients for any
facial expression. These findings are summarised in Fig. 3 and
Table 2.
3.6. Facial functional impairment index
The Nottingham score and facial functional impairment index
(FFII) were calculated for each patient. ‘Global’ FFII scores were
subdivided into anatomic and non-anatomic components.
The FFII scores are based on a continuous scale with a
maximum possible impairment score of 100. Hence, impair-
ment scores are expressed as percentages and listed in Table 3,
as well as corresponding affected aesthetic units, Katz and
Nottingham scores. The global FFII score is the sum of the
anatomic and non-anatomic error components and is pre-
sented in the bar chart in Fig. 4.
Table 3 – Table presenting all error indices used to assess fac
Patient Unilateralbilateral burn
Katzscore
Aestheticunits
Notts
1 Unilateral 6 4 N
2 Bilateral 7 5 5
3 Bilateral 7 3.5 5
4 Unilateral 6 3.5 9
5 Unilateral 7 4.5 7
6 Bilateral 9 8 8
7 Bilateral 8 10 4
8 Bilateral 9 9.5 7
9 Unilateral 6 3.5 6
10 Bilateral 7 3.5 8
11 Unilateral 6 5.5 7
12 Unilateral 4 0.5 9
13 Unilateral 6 4.5 6
14 Unilateral 7 5.5 9
15 Bilateral 9 7.5 7
16 Unilateral 3 0.5 9
17 Bilateral 7 5.5 5
18 Bilateral 7 6.5 9
19 Bilateral 9 9 7
20 Unilateral 8 4.5 7
Patients highlighted in bold were unable to carry out satisfactorily all fa
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
All measures of facial function were statistically com-
pared to the area of facial injury (i.e. number of burn affected
aesthetic units score). Correlation coefficients and the
results of ANOVA analysis are presented in Table 4 and
Fig. 5.
Nottingham score was negatively correlated with burn area
and not significant (coefficient = �0.43/�0.31; p-values = 0.064/
0.327). On categorising patients into unilateral and bilateral
burns the number of affected aesthetic units for bilateral
ial function for 20 acid burn patients
inghamcore
Facial motion impairment index
Anatomicerror (%)
Non-anatomicerror (%)
Combinederror (%)
/A N/A N/A 12.42354
4 7.35547 6.817455 14.17293
9.65 7.654775 8.276555 15.93133
5.86 7.02042 7.603165 14.62358
7.42 5.341415 5.01655 10.35797
0.80 8.32016 10.1482 18.46836
4.44 5.63272 7.54895 13.18167
9.73 10.26859 9.438335 19.70692
7.86 6.192495 7.350405 13.54289
0.43 4.656638 6.202345 10.85898
8.08 2.423861 7.547545 9.971406
5.52 4.507253 5.62656 10.13381
4.11 6.39942 11.84373 18.24314
8.92 3.278456 3.259306 6.537762
0.97 5.719715 5.12563 10.84535
3.64 4.598169 7.244425 11.84259
5.27 1.979135 10.56925 12.54838
7.14 5.82001 7.542485 13.3625
9.10 7.235915 5.69976 12.93568
5.49 6.71591 5.97117 12.68708
cial expressions.
lysis of acid burn victims—Development of a new facial motion

Table 4 – Correlation coefficients and F p-values for ANOVA analysis comparing measures of facial motion impairmentwith burn affected aesthetic units
Measures of facial motion impairmentcompared to correspondingaesthetic units score
Twenty acid burns patientsa Twelve acid burns patientsb
Correlationcoefficient
ANOVA F:p-value
Correlationcoefficient
ANOVA F:p-value
Katz score 0.86 6.55ES07 0.91 3.29ES05
Nottingham score �0.43 0.063961 �0.31 0.326796
Global FMII 0.38 0.101599 0.52 0.082273
Anatomic FMII 0.39 0.101912 0.62 0.032389
Non-Anatomic FMII 0.13 0.573347 0.38 0.223339
Global FMII + rest asymmetry index 0.41 0.071649 0.52 0.081146
Anatomic FMII + rest asymmetry index 0.42 0.073641 0.57 0.052568
5% significance level was used. There was a significant positive correlation between anatomic FMII and aesthetic units affected (amongst
patients able to perform all facial expressions). Graphs displaying important correlations are presented below.a Twenty acid burns victims assessed by MSRA for facial function.b Twelve acid burns victims were able to complete all facial expressions satisfactorily for complete MSRA analysis.
b u r n s x x x ( 2 0 0 7 ) x x x – x x x 7
JBUR-2422; No of Pages 10
burns was significantly greater than unilateral (t-test p = 0.004,
p < 0.05). However, based on the Nottingham index, there was
poorer correlation between facial function and burn area for
bilateral burns (c = �0.05; F significance = 0.89, p > 0.05) than
for unilateral (c = �0.40; F significance = 0.29, p > 0.05). Indeed,
bilateral burn Nottingham scores were significantly less than
unilateral (p = 0.04).
Global FFII scores increased with increasing burn area. This
correlation improved with incorporation of the rest asymme-
try index (20 patients: coefficient = 0.38–0.41; p-value = 0.102–
0.072; 12 patients: coefficient = 0.5212–0.5228; p-value = 0.082–
0.081). There was a significant positive correlation between
anatomic FFII and burn area (coefficient = 0.62; p-value = 0.032;
p < 0.05). However, the anatomic FFII was not influenced by
the rest asymmetry index. Global and anatomic FFII scores
were significantly greater for bilateral burn victims than
unilateral (global FFII: t-test p = 0.041; anatomic FFII: t-test
p = 0.046). There was a poor correlation between the Notting-
ham score and global FFII (0.062).
There was no significant correlation between non-
anatomic FFII scores and number of affected aesthetic
Fig. 5 – Graph showing correlation between affected
aesthetic units and global FFII, anatomic FFII, non-
anatomic FFII.
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
units. There was also no significant difference between
non-anatomic FFII scores for unilateral and bilateral
burns.
4. Discussion
Facial expression reproduction has been shown to be a
justified and accurate means of functional assessment [34].
Johnson et al. [14] used the MSRA, to evaluate the success of
functional free muscle transfer in patients with chronic facial
paralysis and concluded it could be used to objectively assess
the results of facial reanimation. We used the MSRA for the
objective assessment of 20 control subjects and 20 female
patients with devastating facial burns following attacks with
sulphuric acid [25].
4.1. Control group
The control group consisted of 20 females matched for age,
facial shape index and ethnicity. Weedan demonstrated
significant positive correlation between facial shape index –
objective assessment of facial size – and facial motion.
Weedan et al. also demonstrated that males and females
showed differences in maximum facial movements after
adjusting for differences in facial size with males having
greater movement than females [27]. Tzou et al. demonstrated
the influence of ethnicity with significant differences in facial
motion between normal Asian and European faces, conclud-
ing that they were generally the result of differences in facial
size. Hence, Asians (with smaller faces) demonstrated smaller
facial excursion than Europeans [35]. Giovanoli [20] demon-
strated significant increase in facial motion with increasing
age.
These variables were all taken into consideration with
regards to control group selection. There were no significant
differences in facial shape between our control and patient
groups (bizygomatic distance: p = 0.53; face height: p = 0.29;
and facial shape index: p = 0.14) and all control subjects and
patients were female and of Bangladeshi origin, enabling valid
comparison for the purposes of calculating the facial func-
tional impairment index.
lysis of acid burn victims—Development of a new facial motion

b u r n s x x x ( 2 0 0 7 ) x x x – x x x8
JBUR-2422; No of Pages 10
4.2. Patient group
The patient group consisted of 20 females sustaining acid
burns from sulphuric acid with no surgical intervention for at
least 2 years. The majority of patients had widespread facial
hypertrophic scars. Patients with keloid scars were not
included in this study. Based on Magliacani et al.’s [36]
classification of burn scars, hypertrophic scars can be
described as short or medium-term evolution and achieve
normalisation within 2 years. Hence, the patient group can be
described as homogenous and their respective scars being in
complete remission at time of assessment.
4.3. Facial functional impairment index (FFII)
We propose the ‘facial functional impairment index’ (FFII).
This consists of 7 separate measures of facial functional
impairment based on excursion at 12 soft tissue landmarks for
5 facial expressions. Linear displacement, vectors and bear-
ings were measured in acid burn victims and statistically
compared to mean normal values obtained from MSRA
analysis of a group of volunteers matched for age, sex, facial
shape and ethnicity—all factors shown to significantly
influence facial motion. The FFII accounts for abnormalities
in absolute displacement, proportional displacement and
absolute direction. The mathematical calculations involved
in derivation of the FFII were formally checked by a
mathematician based at the University of Cardiff.
For each facial expression, soft tissue landmarks were
designated as anatomic or non-anatomic based on the facial
action coding sequence (Table 1). As a result the FFII score for
each facial expression can be subdivided into anatomic and
non-anatomic components. As defined earlier, anatomic
motion is termed the motion of specific facial points studied
by the MSRA that can be attributed solely to the pull of the
regional facial muscles that govern the movement of these
points and hence non-anatomic motion is movement at points
elsewhere on the face. If we define the total of all FFII scores for
each facial expression as the global FFII, corresponding global
anatomic and global non-anatomic scores can be derived.
The Katz score and distribution of affected aesthetic units
provided aesthetic measures of disfigurement. They were
consistent with a significant positive correlation (c = 0.86;
p < 0.01). The FFII was calculated for all patients and correlated
well with corresponding aesthetic measures. Larger burns and
more disfigurement resulted in worse facial function (c = 0.52;
p = 0.08, p > 0.05).
In particular, larger facial burns resulted in significantly
worse anatomic function (c = 62; p = 0.03, p < 0.05). Within the
context of facial paralysis, poor anatomic function is judged to
be the result of defective motor nerve innervation. Abnormal
non-anatomic motion was defined by Linstrom as synkinesis
[21] and by Bajaj-Luthra, as secondary to the pull of the
unaffected contralateral muscles, transmitted to the paral-
yzed hemiface [31].
In acid burn victims, all injuries are full thickness and
damage generally extends beyond dermal and epidermal
layers. Assuming intact motor nerve function, normal
anatomic motion is restricted by overlying, tight, scar tissue
as well as muscle necrosis, particularly at points of origin and
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
insertion. Hypertrophic scar tissue extending from anatomic
to non-anatomic regions may thus transmit anatomic move-
ment to non-anatomic landmarks, and hence represent
abnormal non-anatomic displacements.
4.4. Rest asymmetry index
Such was the severity of burns in some patients, hypertrophic
scars and grafts resulted in contractures pulling and displa-
cing certain soft tissue landmarks, at rest. The FFII is a
dynamic measure of functional impairment but does not take
into account static disfigurement that may potentially con-
found any active comparison. In other words certain soft
tissue landmarks and their surrounding relations in patients
may not relate accurately to the control group and hence
comparison of like with like is not quite accurate.
The rest asymmetry index was calculated prior to the FFII
and based on comparison of control and patient neutral pose.
Various inter-soft tissue landmark distances, on either side of
the face, were measured and expressed as a ratio of left to
right. Significant differences in ratios between patients and
the normogram, represent the effects of contractures produ-
cing a significantly asymmetric facial profile at rest. Anatomic
function was not significantly affected by any static facial
asymmetry. However, non-anatomic motion was significantly
affected with increased non-anatomic FFII scores ( p = 0.04).
The rest asymmetry index was factored into the FFII for
further accuracy.
4.5. FFII—advantages
Critical assessment of the FFII reveals several advantages, as
well as drawbacks, that bode well for its effective clinical
application. The FFII is able to differentiate between patients
and is not based on an exponential scale. It takes into account
five facial expressions representing active movement in the
upper third, tragal third (middle) and gonion (lower third)
region of the face. The FFII is a composite score of regional and
global function. Scores for specific facial animations represent
measures of regional function. Individual soft tissue landmark
scores provide geographical details of global and regional
facial functional deficit with specific areas of abnormal motion
relating to specific muscle groups based on the facial action
coding sequence.
The FFII accounts for movement in the x- and y-direction
and hence addresses angular direction indirectly but also
directly addresses absolute direction with the inclusion of a
bearing component. Earlier grading systems were based on
the assumption that abnormal displacement due to facial
dysfunction manifests as abnormally decreased excursion
and/or inter-landmark distances. Acid burn injuries are
capable of reshaping the normal soft tissue profile of the
face and hence, potentially compromising sites of origin and
insertion of facial muscles without necessarily directly
damaging muscle tissue. Hence, it is possible that resultant
anatomic excursions maybe of normal magnitude but have
radically altered bearing. Furthermore, the need for direc-
tional and proportional measures is emphasised with the
recognition of overcompensation and synkinesis in facial
paralysis. Linstrom’s and Frey’s objective measurement of
lysis of acid burn victims—Development of a new facial motion

b u r n s x x x ( 2 0 0 7 ) x x x – x x x 9
JBUR-2422; No of Pages 10
movement in the x- and y-planes is not enough to account for
bearing, and the Nottingham index and HBGS do not consider
directional change at all [11,13,18].
Kahn noted that current facial grading systems work by
compartmentalizing facial movement. However, this is not a
true reflection of real facial function. Within a given
individual, separate facial zones’ movements, both ipsilateral
and contralateral, impact on adjoining zones [19]. The FFII
standardises normal impaction of movement across ipsilat-
eral and contralateral zones and hence is able to define and
quantify pathological non-anatomic, as well as anatomic,
motion.
The FFII is based on deliberate facial action tasks. Directed
facial action tasks may differ in appearance and timing from
spontaneously occurring expressions [33]. Deliberate and
spontaneous facial behaviour are mediated by separate motor
pathways—the pyramidal and extra pyramidal motor tracts
[33]. As a consequence fine motor control of deliberate facial
actions is often inferior and less symmetric to that which
occurs spontaneously. All normal subjects and patients were
asked to perform directed facial expressions and patients were
well trained beforehand.
4.6. FFII—disadvantages
The FFII still has significant drawbacks. The calculation of this
index is extremely labour intensive and at this stage remains a
clinical research tool at best. The FFII does not take into
account neck excursion. Neck burns and contractions can
have significant effects on facial function and further
refinement of the FFII will require incorporation of neck
excursion as a facial expression.
The FFII works on the assumption that expressions are
singular and begin and end from a neutral position. Mimetic
movement is in fact multi-vectored and the range of move-
ment is on a continuum from a relaxed state to a fully
contracted [37–39]. Unfortunately FFII and MSRA consider only
neutral and final maximally contracted states and are
restricted to two dimensions.
The incorporation of video and dynamic study of facial
motion accounts for multi-vectored movements. Video
motion analysis enables measurement of velocity and accel-
eration of facial excursion throughout the duration of move-
ment. Peak Motus Motion Measurement System, 3D Expert
Vision Hi Res motion analysis system, Facialis and FaciShow
have proved to be successful motion capture software in facial
functional assessment, but extremely expensive [18,21–
23,30,37–44].
The significance of velocity and acceleration in the
evaluation of facial function has not been definitively
elucidated. Linstrom showed that the presentation of accel-
eration and velocity in the form of time plots for normal versus
pathological facial nerve function clearly demonstrates
degrees of postoperative facial nerve recovery [21]. In the
context of facial nerve paralysis, loss of facial nerve function
appears to result in reduced acceleration. In the context of acid
burn victims, assuming no facial nerve damage, normal and
pathological excursion would be expected to accelerate at the
same rate until the effects of scar damage limit the maximum
possible displacement of the burn affected side and radically
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
reduce velocity. If this is the case this sort of analysis may help
to decide the borders of potential grafts.
Recently there has also been a shift towards three-
dimensional assessments of facial function and asymmetry
[18,21,23,30,41–43]. Comparisons of 2D and 3D measurements
of facial excursion in normal individuals by Lin et al. [30]
demonstrated that a 3D analysis may be more appropriate for
detecting clinical differences in facial function. According to
Frey et al. [18], important information is lost and accuracy of
measurement is sacrificed by projecting 3D data into 2D. Lin
et al. [30] found significant differences (p < 0.001) between 2D
and 3D excursion despite high correlation between the two
(r > 0.69) with 2D measurements underestimating 3D.
The FFII is a 2D based impairment index and hence may
underestimate facial functional impairment in acid burn
victims. The future incorporation of 3D data may improve the
accuracy of the FFII. Automation of FFII calculation is
necessary to allow routine clinical use. This automation
requires the development of software to work side by side with
affordable video based motion capture.
The degrees of movement as well as facial coordination
normally differ from person to person. Some people have
more expressive faces with larger smiles and greater eyebrow
excursion than others [43]. Also it might be expected that
subjects with larger faces would have greater displacements.
Hence, Lin accounted for this by normalising differences with
anthropometric measurements. The calculation of the FFII is
based on a normogram database for each facial expression.
Assuming a normal distribution for varying degrees of facial
expressiveness and facial size, there is a need for more
exhaustive normogram databases.
5. Conclusion
MSRA analysis of 20 acid burn victims was successfully
conducted. A normogram database enabled the develop-
ment of the facial functional impairment index (FFII)—a
composite score of global and regional measures of facial
function; able to differentiate patients; define anatomic and
non anatomic functional impairment and; correlate sig-
nificantly with aesthetic measures of disfigurement. Our
analysis of 20 female acid burn victims revealed some
significant findings. Anatomic facial function was signifi-
cantly compromised by larger burn injuries. Abnormal non-
anatomic motion was significantly increased in the presence
of rest asymmetry. Global facial function worsened with
increasing burn area.
Introduction of the FFII into clinical practice requires
automation, the integration of video, appropriate graphical
and pictorial depiction of variables and measurements, and
further research into the accuracy of FFII as a marker of
clinical recovery and assessment of facial function.
r e f e r e n c e s
[1] May M. Facial paralysis, peripheral type: a proposedmethod of reporting. Laryngoscope 1970;80:331–90.
lysis of acid burn victims—Development of a new facial motion

b u r n s x x x ( 2 0 0 7 ) x x x – x x x10
JBUR-2422; No of Pages 10
[2] Adour KK, Swanson Jr PJ. Facial paralysis in 403 consecutivepatients: emphasis on treatment response in patients withBell’s palsy. Trans Am Acad Ophthalmol Otolaryngol1971;75:1284–301.
[3] Stennert E. Facial nerve paralysis scoring system. In: FischU, editor. Facial nerve surgery. Proceedings of the ThirdInternational Symposium on Facial Nerve Surgery.Amstelveen, The Netherlands: Kugler Medical Publications;1977. p. 543–7.
[4] Smith M. Cited in House JW. Facial nerve grading systems.Laryngoscope 1983;93:1056–69.
[5] House JW, Brackmann DE. Facial nerve grading system.Otolaryngol Head Neck Surg 1985;93:146–7.
[6] Evans RA, Harries ML, Baguley DM, Moffat DA. Reliability ofthe House and Brackmann grading system for facial palsy. JLaryngol Otol 1989;103:1045–6.
[7] Burres SA. Facial biomechanics: the standards of normal.Laryngoscope 1985;95:708–14.
[8] Burres SA. Objective grading of facial paralysis. AnnOtolaryngol Rhinol Laryngol 1986;95:238–41.
[9] Burres S, Fisch U. The comparison of facial gradingsystems. Arch Otolaryngol Head Neck Surg 1986;112:755–8.
[10] Smith IM, Murray JA, Cull RE, Slattery J. A comparison offacial grading systems. Clin Otolaryngol 1992;17(4):303–7.
[11] Lewis BL, Adour KK. An analysis of the Adour–Swanson andHouse–Brackmann grading systems for facial nerverecovery. Eur Arch Otorhinolaryngol 1995;252:265–9.
[12] Neely JG, Cheung JY, Wood M, Byers J, Rogerson A.Computerized quantitative dynamic analysis of facialmotion in the paralyzed and synkinetic face. Am J Otol1992;13:97–107.
[13] Murty GE, Diver JP, Kelly PJ, et al. The Nottingham system:objective assessment of facial nerve function in the clinic.Otolaryngol Head Neck Surg 1994;110:156–61.
[14] Johnson. et al. Quantitative facial motion analysis afterfunctional free muscle reanimation procedures. PlastReconstruct Surg 1997;100(7):1710–9.
[15] Bajaj-Luthra A, Mueller T, Johnson P. Quantitative analysisof facial motion components: anatomic and nonanatomicmotion in normal persons and in patients with completefacial paralysis. Plast Reconstr Surg 1997;7:1894–902.
[16] Kahn JB, Gliklich RE, Boyev KP, Stewart MG, Metson RB,McKenna MJ. Validation of a patient-graded instrument forfacial nerve paralysis: the FaCE scale. Laryngoscope2001;111:387–98.
[17] House JW. Facial nerve grading systems. Laryngoscope1983;93:1056–69.
[18] Frey. et al. Three-dimensional video analysis of facialmovements: a new method to assess the quantity andquality of the smile. Plast Reconstruct Surg1999;104(7):2032–9.
[19] Kahn JB, Gliklich RE, Boyev KP, Stewart MG, Metson RB,McKenna MJ. Validation of a patient-graded instrument forfacial nerve paralysis: the FACE scale. Laryngoscope2001;111:387–98.
[20] Giovanoli P, et al. Three-dimensional video-analysis offacial movements in healthy volunteers. Br J Plast Surg2003;56(7):644–52.
[21] Linstrom, Christopher JMD. Objective facial motionanalysis in patients with facial nerve dysfunction.Laryngoscope 2002;112(7):1129–47.
[22] Ferrario VF, Sforza C, Poggio CE, Tartaglia G. Distance fromsymmetry: a three-dimensional evaluation of facialasymmetry. J Oral Maxillofac Surg 1994;52(11):1126–32.
Please cite this article in press as: Ghani S, et al., Facial motion ana
impairment index, Burns (2007), doi:10.1016/j.burns.2006.08.024
[23] Ross BG, Fradet G, Nedzelski JM. Development of a sensitiveclinical facial grading system. Otolaryngol Head Neck Surg1996;114(3):380–6.
[24] Faga A, Scevola D, Mezzetti MG, Scevola S. Sulphuric acidburned women in Bangladesh: a social and medicalproblem. Burns 2000;26:701–9.
[25] Mannan A, Ghani S, Sen SL, Clarke A, Butler PEM. Acidburns in Bangladesh. J Surg 2004;1(2).
[26] Bari MS, Choudhury M, Mahmud I. Acid burns inBangladesh. Ann Burns Fire Disasters 2001;14:115–8.
[27] Weeden JC, Trotman CA, Faraway JJ. Three dimensionalanalysis of facial movement in normal adults: influence offacial shape and sex. Angle Orthod 2000;71(2):132–40.
[28] Fattabi TT. An overview of facial aesthetic units. Journal ofOral Maxillofacial Surgery 2003;61:1207–11.
[29] Katz MR, Irish JC, Devins GM, Rodin GM, Gullane PJ.Reliability and validity of an observer-rated disfigurementscale for head and neck cancer patients. Head Neck2000;22(2):132–41.
[30] Lin S-C, et al. Comparison of two-dimensional and three-dimensional techniques for determination of facialmotion—absolute movement in a local face frame. JFormos Med Assoc 2000;99(5).
[31] Bajaj-Luthra A, Mueller T, Johnson PC. Quantitativeanalysis of facial motion components: anatomic and nonanatomic motion in normal persons and in patients withcomplete facial paralysis. Plast Reconstr Surg1997;99(7):1894–902 [discussion 1903–4].
[32] Kanade T, Cohn JF, Tian Y. Comprehensive database forfacial expression analysis. Unpublished manuscript. TheRobotics Institute & Department of Psychology, CarnegieMellon University, Pittsburgh, USA; 2003.
[33] Zlochower AJ. Deciphering emotion from the face. Anevaluation of FACS, EMG, and computer-vision basedapproaches to facial expression analysis. Unpublishedmanuscript. University of Pittsburgh; 1997.
[34] Johnston DJ, Millett DT, Ayoub AF, Bock M. Are facialexpressions reproducible? Cleft Palate Craniofac J2003;40(3):291–6.
[35] Tzou CHJ, Giovanoli P, Ploner M, Frey M. Are there ethnicdifferences of facial movements between Europeans andAsians? Br J Plast Surg 2005;58:183–95.
[36] Magliacani G, Stella M, Castagnoli C. Classification ofpathological burn scars. Ann Burns Fire Disasters 1999;12(1).
[37] Koff E, Borod JC, White B. Asymmetries for hemiface sizeand mobility. Neuropsychologica 1981;9:825–30.
[38] Farkas LG, Cheung G. Facial asymmetry in healthy NorthAmerican Caucasian. Angle Orthod 1981;51:70–7.
[39] Niparko JK. The acute facial palsies. In: Jackler RK,Brackmann DE, editors. Neurotology. St. Louis: Mosby-YearBook; 1994. p. 1291–313.
[40] Flowers RS, Caputy GG, Flowers SS. The biomechanics ofbrow and frontalis function and its effect onblepharoplasty. Clin Plast Surg 1993;20:255–68.
[41] Coulson SE, Croxson GR, Gilleard WL. Three-dimensionalquantification of the symmetry of normal facial movement.Otol Neurotol 2002;23(6):999–1002.
[42] Coulson SE, Croxson GR, Gilleard WL. Three-dimensionalquantification of ‘‘still’’ points during normal facialmovement. Ann Otol Rhinol Laryngol 1999;108(3):265–8.
[43] Linstrom CJ, Silverman CA, Susman WM. Facial-motionanalysis with a video and computer system: a preliminaryreport. Am J Otol 2000;21(1):123–9.
[44] Shah SM, Joshi R. An assessment of asymmetry in thenormal craniofacial complex. Angle Orthod 1978;48:141–8.
lysis of acid burn victims—Development of a new facial motion