
Context processing during irony comprehension in right frontal ...
Upload
independentCategory
view
0download
0
Brain (1996), 119, 2105-2120
Frontal lobe dysfunction in amyotrophic lateralsclerosisA PET study
S. Abrahams,1 L. H. Goldstein,1 J. J. M. Kew,3 D. J. Brooks,3 C. M. Lloyd,2 C. D. Frith34 andP. N. Leigh2
1 Department of Psychology, Institute of Psychiatry, the2Department of Clinical Neurosciences, Institute ofPsychiatry and King's College Hospital Medical School,the 3MRC Cyclotron Unit, Hammersmith Hospital and the^Wellcome Department of Cognitive Neurology, Institute ofNeurology, London, UK
Correspondence to: Dr Sharon Abrahams, Department ofPsychology, Institute of Psychiatry, De Crespigny Park,London SE5 8AF, UK
SummaryPET measurements of regional cerebral blood flow (rCBF)were used to explore frontal lobe dysfunction in amyotrophiclateral sclerosis (ALS). An activation paradigm of executivefrontal lobe function (verbal fluency), which contrasted rCBFduring word generation and word repetition, was used. Twogroups of ALS patients, defined by the presence orabsence of cognitive impairment (ALSi) (impaired, n = 6;ALSu, unimpaired, n = 6) were compared with healthyage-matched controls (n = 6). Patient selection was basedon prior performance on a written test of verbal fluency.Additional neuropsychological assessment of the patientsrevealed evidence of executive and memory dysfunctionin the ALSi group only, with marked deficits in tests ofintrinsic generation. The ALSi patients displayed significantly
(P < 0.001) impaired activation in cortical and subcorticalregions including the dorsolateral prefrontal cortex (DLPFC;areas 46 and 9), lateral premotor cortex (areas 8 and 6),medial prefrontal and premotor cortices (areas 8 and 9),insular cortex bilaterally and the anterior thalamic nuclearcomplex. Although the three groups showed matched wordgeneration performance on the scanning paradigm, the ALSugroup displayed a relatively unimpaired pattern of activation.These results support the presence of extra-motor neuronalinvolvement, particularly along a thalamo-frontal associationpathway, in some non-demented ALS patients. In addition,this study suggests dysfunction of DLPFC in some ALSpatients with associated cognitive impairments.
Keywords: frontal lobes; cognitive impairment; ALS; PET; verbal fluency
Abbreviations: ALS = amyotrophic lateral sclerosis; ALSi = cognitively impaired ALS patients; ALSu, = cognitivelyunimpaired ALS patients; DLPFC = dorsolateral prefrontal cortex; rCBF = regional cerebral blood flow; RMJT = randommovement joystick task; SPM = statistical parametric mapping; VFI = Verbal Fluency Index; WCST = Wisconsin CardSorting Test
IntroductionAmyotrophic lateral sclerosis is a progressive disordercharacterized by degeneration of the corticospinal tract andlower motor neurons of the brainstem and spinal cord. Hencemost research on the mechanisms of neurodegeneration inALS has focused on the motor system. There is, however,increasing evidence that ALS should be regarded as amultisystem disorder and that cortical involvement extendsbeyond the confines of the primary motor areas (Smith, 1960;Kew et al., 1993a, b; Leigh et al., 1994; Talbot et al., 1995).
© Oxford University Press 1996
Dementia occurs in - 3 % of patients with sporadic ALS(Kew and Leigh, 1992, 1994), and such patients displaycognitive and behavioural changes characteristic of frontallobe dysfunction (Neary et al., 1990; Peavy et al., 1992). Theunderlying pathology in these cases consists of spongiformneuronal degeneration in layers 2 and 3 of the prefrontal andtemporal cortex (Hudson, 1981; Wikstrom etal., 1982; Moritaet al., 1987; Neary et al., 1990; Wightman et al, 1992) withadditional involvement of regions within the limbic system
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

2106 S. Abrahams et al.
(the hippocampal formation, subiculum and amygdala)(Okamoto et al., 1991; Wightman et al., 1992; Kato et al.,1994).
In non-demented patients with sporadic ALS cognitivechanges have been reported in a number of neuropsycho-logical investigations (Gallassi et al., 1985, 1989; David andGillham, 1986; Ludolph et al., 1992; Kew et al., 1993b).These studies have revealed a pattern of frontal lobe (execut-ive) and memory deficits, clearly suggestive of corticalinvolvement extending beyond the motor system. Executivedysfunction has been demonstrated using tests of verbalreasoning, visual attention, picture sequencing and categoryformation on the Wisconsin Card Sorting Test (WCST)(Gallassi et al., 1985, 1989; David and Gillham, 1986; Talbotet al., 1995). However, the most striking and consistentimpairment is found using tests of verbal fluency, whichrequire rapid word generation, typically involving ortho-graphic or category-based procedures (Gallassi et al., 1985,1989; Ludolph et al., 1992; Kew et al., 1993*). Memory andlearning impairments have also been reported using tests ofprose recall, word list and verbal paired associate learning,and picture recall (Gallassi et al., 1985, 1989; David andGillham, 1986; Iwasaki et al., 1990; Kew et al., \993b).
Further insight into the neural basis of the cognitivechanges in ALS has been provided by a PET study (Kewet al., 1993a, b). This was conducted using a motor paradigmwhich compared paced joystick movements in a freely chosen(random) direction to movements only in a forward direction(stereotyped). The study showed impaired activation ofmedial prefrontal cortex (Brodmann areas 10 and 32), anteriorcingulate gyrus, parahippocampal gyrus and anterior thalamicnuclear complex, in ALS subjects selected on the basis ofabnormal verbal fluency scores (Kew et al., 1993£>). Suchdysfunction was less marked in patients with unimpairedverbal fluency. This study therefore revealed clear evidenceof medial prefrontal cortex dysfunction, in non-demented
Table 1 Clinical characteristics of 12 ALS patients
ALS patients with cognitive impairment, and alsodemonstrated that verbal fluency appears to be a sensitiveindicator of such cortical dysfunction.
In the present investigation, we used PET to further explorefrontal lobe functions in ALS using a verbal fluency activationparadigm. The task was based closely on a study by Frithet al. (1991a) and contrasts rCBF increases during twoconditions, orthographically based word generation and wordrepetition. Word generation is known to produce relativeactivation of the DLPFC (Frith et al., 1991a). The purposeof this study was to identify the neural basis of the markedabnormalities of verbal fluency detected in some ALS subjectsand to test the hypothesis that such subjects show impairedactivation of prefrontal and subcortical areas, previouslyshown to be implicated in ALS (Kew et al., 1993a).
Material and methodsAmyotrophic lateral sclerosis patientsTwelve patients with sporadic ALS, recruited from theMaudsley/King's College Hospital, London MND Care andResearch Centre, were studied. All patients had clinical andelectrophysiological evidence of combined upper and lowermotor neuron involvement and were classified as 'definite'or 'probable' ALS according to the El Escorial criteria(Swash and Leigh, 1992; World Federation of NeurologyResearch Group, 1994). The clinical characteristics of thepatients are presented in Table 1. No patient had a historyof cerebrovascular disease, hypertension or diabetes, andnone was taking psychoactive drugs or any medication thatmight influence CBF. All patients were right handed. Patientswere excluded if severity of speech, swallowing or respiratorysymptoms would have hindered their task performance(speaking whilst lying supine in the PET scanner). Prior tothe investigation, the patients underwent a pilot of the test
Patient(group)
1 (ALSu)2 (ALSu)3 (ALSu)4 (ALSu)5 (ALSu)6 (ALSu)7 (ALSi)8 (ALSi)9 (ALSi)
10 (ALSi)11 (ALSi)12 (ALSi)
Pseudo-bulbarPalsy(UMN)
—-+------+++
Bulbarinvolvement(LMN)
+++-----++++
WastingUL
++++++++-+-+
WastingLL
++---++++--+
Fasciculations(UL and LL)
++++++++++++
SpasticityUL
—+++-----+-+
SpasticityLL
—-+-+-+--+++
Hyper-reflexia
++++++++++++
Babinskisign
—++++-+-+++-
Pseudobulbar palsy evidence: brisk jaw jerk, spasticity of factila and or tongue muscles, spastic dysarthria. Bulbar involvement evidencenasal speech, fasciculations, wasting of tongue and weak cough. UMN = upper motor neuron; LMN = lower motor neuron.UL = upper limb; LL = Lower Limb. + = present/positive; - = absent/negative; ALSu = ALS unimpaired; ALSi = ALS impaired.
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from
Frontal lobe activation in ALS 2107
Table 2 Subject characteristics
ALSu(n = 6)
ALSi(» = 6)
Controls(« = 6)
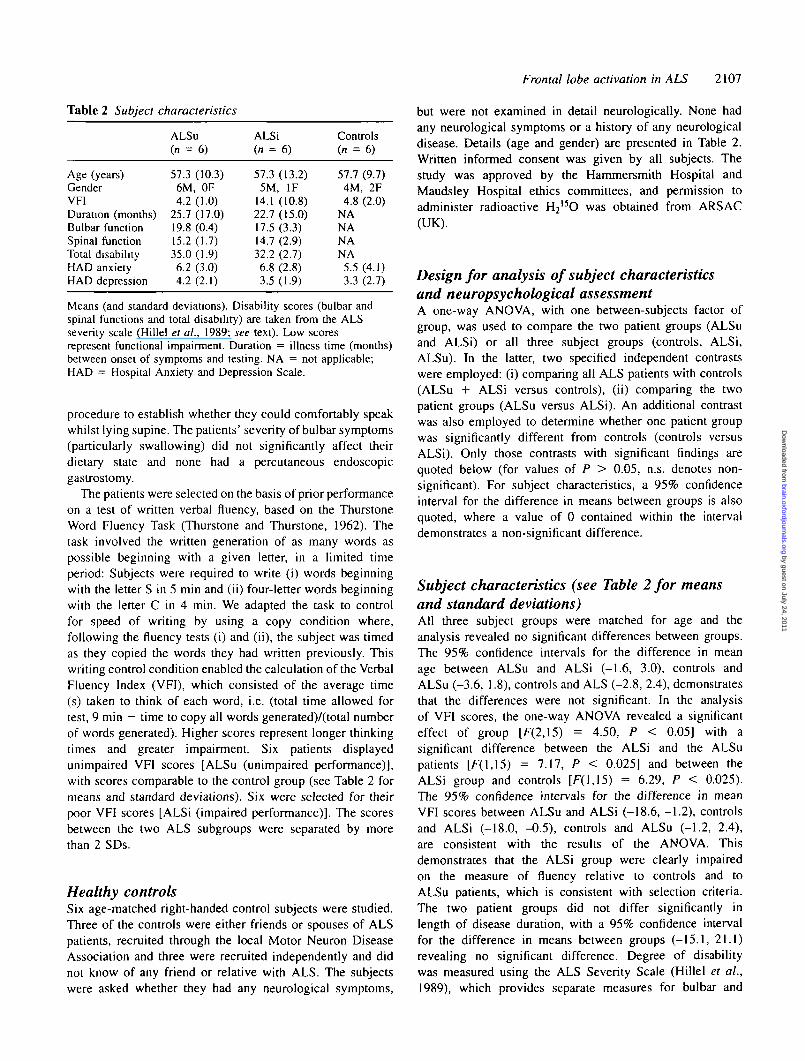
Age (years)GenderVFIDuration (months)Bulbar functionSpinal functionTotal disabilityHAD anxietyHAD depression
57.36M4.2
25.719.815.235.06.24.2
(10.3), OF(10)(17.0)(0.4)(1.7)(1.9)(3.0)(2.1)
57.35M
14.122.717.514.732.26.83.5
(13.2), IF(10.8)(15.0)(3.3)(2.9)(2.7)(2.8)(1.9)
57.74M4.8
NANANANA5.53.3
(9.7), 2F(2.0)
(4.1)(2.7)
Means (and standard deviations). Disability scores (bulbar andspinal functions and total disability) are taken from the ALSseverity scale (Hillel et al., 1989; see text). Low scoresrepresent functional impairment. Duration = illness time (months)between onset of symptoms and testing. NA = not applicable;HAD = Hospital Anxiety and Depression Scale.
procedure to establish whether they could comfortably speakwhilst lying supine. The patients' severity of bulbar symptoms(particularly swallowing) did not significantly affect theirdietary state and none had a percutaneous endoscopicgastrostomy.
The patients were selected on the basis of prior performanceon a test of written verbal fluency, based on the ThurstoneWord Fluency Task (Thurstone and Thurstone, 1962). Thetask involved the written generation of as many words aspossible beginning with a given letter, in a limited timeperiod: Subjects were required to write (i) words beginningwith the letter S in 5 min and (ii) four-letter words beginningwith the letter C in 4 min. We adapted the task to controlfor speed of writing by using a copy condition where,following the fluency tests (i) and (ii), the subject was timedas they copied the words they had written previously. Thiswriting control condition enabled the calculation of the VerbalFluency Index (VFI), which consisted of the average time(s) taken to think of each word, i.e. (total time allowed fortest, 9 min - time to copy all words generated)/(total numberof words generated). Higher scores represent longer thinkingtimes and greater impairment. Six patients displayedunimpaired VFI scores [ALSu (unimpaired performance)],with scores comparable to the control group (see Table 2 formeans and standard deviations). Six were selected for theirpoor VFI scores [ALSi (impaired performance)]. The scoresbetween the two ALS subgroups were separated by morethan 2 SDs.
Healthy controlsSix age-matched right-handed control subjects were studied.Three of the controls were either friends or spouses of ALSpatients, recruited through the local Motor Neuron DiseaseAssociation and three were recruited independently and didnot know of any friend or relative with ALS. The subjectswere asked whether they had any neurological symptoms,
but were not examined in detail neurologically. None hadany neurological symptoms or a history of any neurologicaldisease. Details (age and gender) are presented in Table 2.Written informed consent was given by all subjects. Thestudy was approved by the Hammersmith Hospital andMaudsley Hospital ethics committees, and permission toadminister radioactive H2
I5O was obtained from ARSAC(UK).
Design for analysis of subject characteristicsand neuropsychological assessmentA one-way ANOVA, with one between-subjects factor ofgroup, was used to compare the two patient groups (ALSuand ALSi) or all three subject groups (controls, ALSi,ALSu). In the latter, two specified independent contrastswere employed: (i) comparing all ALS patients with controls(ALSu + ALSi versus controls), (ii) comparing the twopatient groups (ALSu versus ALSi). An additional contrastwas also employed to determine whether one patient groupwas significantly different from controls (controls versusALSi). Only those contrasts with significant findings arequoted below (for values of P > 0.05, n.s. denotes non-significant). For subject characteristics, a 95% confidenceinterval for the difference in means between groups is alsoquoted, where a value of 0 contained within the intervaldemonstrates a non-significant difference.
Subject characteristics (see Table 2 for meansand standard deviations)All three subject groups were matched for age and theanalysis revealed no significant differences between groups.The 95% confidence intervals for the difference in meanage between ALSu and ALSi (-1.6, 3.0), controls andALSu (-3.6, 1.8), controls and ALS (-2.8, 2.4), demonstratesthat the differences were not significant. In the analysisof VFI scores, the one-way ANOVA revealed a significanteffect of group [F(2,15) = 4.50, P < 0.05] with asignificant difference between the ALSi and the ALSupatients [F(l,15) = 7.17, P < 0.025] and between theALSi group and controls [F(l,15) = 6.29, P < 0.025).The 95% confidence intervals for the difference in meanVFI scores between ALSu and ALSi (-18.6, -1.2), controlsand ALSi (-18.0, -0.5), controls and ALSu (-1.2, 2.4),are consistent with the results of the ANOVA. Thisdemonstrates that the ALSi group were clearly impairedon the measure of fluency relative to controls and toALSu patients, which is consistent with selection criteria.The two patient groups did not differ significantly inlength of disease duration, with a 95% confidence intervalfor the difference in means between groups (-15.1, 21.1)revealing no significant difference. Degree of disabilitywas measured using the ALS Severity Scale (Hillel et al.,1989), which provides separate measures for bulbar and
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

2108 S. Abrahams et al.
spinal function (see Table 2, lower scores represent greaterfunctional impairment). There was no significant differencebetween the two patient groups in the separate bulbar andspinal function disability scores, although a non-significanttrend emerged for the comparison of total disability scores[F(l,lO) =4.39, P = 0.06] which was significant using a95% confidence interval (0.2, 5.4), with the ALSi grouptending to show greater disability than the ALSu patients.This difference was more apparent on mean scores ofbulbar function; however, the scores are computed from amaximum of 20, demonstrating that the ALSi groupdisplayed some slight bulbar functional impairment, whilethe ALSu group was virtually unimpaired.
A measurement of anxiety and depression was alsoobtained in order to exclude the possibility that abnormalitiesin blood flow may be associated with such psychologicalfactors. This was obtained using the Hospital Anxiety andDepression Scale (Zigmond and Snaith, 1983), which weadapted for use with both patients and controls. This alterationconsisted of the removal of one statement ('I feel as if I amslowed down'), used to calculate depression scores, andwhich we felt would falsely exaggerate the measure ofdepression in ALS patients.
The analysis of the Hospital Anxiety and Depression Scalequestionnaire scores (see Table 2) demonstrated no significantdifferences between the three groups on anxiety (P > 0.05),with a 95% confidence interval for the difference in meansbetween ALSu and ALSi (-3.9, 2.7), controls and ALSu(-4.8, 3.4) and controls and ALSi (-5.3, 2.7). This wasalso the case for the modified depression scores (P >0.05), with a 95% confidence interval for the differencein means between ALSu and ALSi (-1.6, 3.0), controlsand ALSu (-3.6, 1.8), and controls and ALSi (-2.8, 2.4).This demonstrates that the three groups were matched interms of anxiety and depression.
Neuropsychological assessmentA neuropsychological assessment was conducted on bothpatients and controls to determine whether the three groupsdiffered in terms of neuropsychological profile. Theassessment consisted of standard and experimental tests offrontal lobe and memory function. The tests included theNational Adult Reading Test—Revised, to estimate premorbidfull scale IQ (Nelson and Willison, 1991). In addition to thewritten verbal fluency procedure (see above), frontal lobetests measuring executive functions included a computerizedWisconsin Card Sorting Test (Grant and Berg, 1990) and arandom movement joystick task (RMJT) (Deiber et al., 1991)where subjects have to generate random sequences of 50movements with a four-way directional joystick. Memorytests included verbal Paired Associate Learning (Wechsler,1987), the Recognition Memory Test (Warrington, 1984)using both words and faces, and the Kendrick Object LearningTest (Kendrick, 1985), in which a subject has to remember
pictorial representations of common objects, printed on acard and presented to the subject for a limited time period.
Structural imagingWherever possible, patients underwent either an MRI scan,or a CT scan of the brain to exclude any significant cerebralatrophy or ventricular dilation, which may have affected thestereotactic normalization of the PET scans (see below). MRIimages were acquired using a Picker 1.0 Tesla HPQ VistaMRI system. The scans consisted of a Trweighted 3D RFspoiled scan (TR = 21, TE = 6, flip angle 35%). The CTscans consisted of a series of axial images with a 10 mminter-plane distance using a CT9800 whole body scanner(IGE Medical Systems Ltd, Slough, UK). Four of the patientsstudied underwent MRI and one CT, none of which showedany evidence of atrophy. In addition, an autopsy on a furtherpatient was found to be normal. Of these six patients, fourwere from the ALSi cognitively impaired group.
An MRI scan was performed on one control subject forthe purposes of co-registration with his PET image. This wasconducted in order to identify clearly and display optimallythe regions of significant rCBF change produced by thisword generation paradigm in a healthy individual. Co-registration of the PET and MRI was conducted usingmethods described previously (Watson et al., 1993; Woodset al, 1993).
PET imagingExperimental designThe PET activation paradigm was based on that developedby Frith et al. (1991a) and contrasted rCBF during twoconditions: word generation and word repetition. In thepresent study, modifications to the procedure were requiredto accommodate an older patient group with possible speechimpairment. The subjects had eight PET measurements ofrCBF during a scanning session. Four measurements weremade during each condition using an ABAB design. TherCBF measurements were performed with the subjects' eyesclosed in a darkened room. During the word generationcondition the subject was required to say aloud any wordbeginning with a given letter in response to the word 'next'presented aurally every 5 s. (The optimum rate of presentationwas established prior to the scanning investigation in arigorous pilot study of paced verbal fluency in a separategroup of ALS patients, some with bulbar symptoms.) Thesubject was given a different letter (S, C, F, T) for each ofthe four word generation scans. On failure to generate anappropriate word, the subject was required to respond withthe word 'pass', within the 5 s response time. This enabledthe amount of speech output to be matched between the twoconditions. During the four word repetition scans, randomwords (see Frith et al., 1991a) were presented verbally tothe subject every 5 s and the subject was required to respond
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from
Frontal lobe activation in ALS 2109
by repeating the words aloud. Prior to the scanning session,all subjects underwent up to five practice word generationtrials (with different letters), to familiarize them with theprotocol.
Data acquisitionPET scans were performed using a Siemens 935b PETScanner allowing 31 planes of data acquisition (CTI,Knoxville, Tenn., USA), whose physical characteristics havebeen described previously (Spinks et al., 1988). Scanning isperformed in 3D mode with the septa retracted. At the startof each scanning session, a transmission scan was performedwith an external ^Ge/^Ga ring source to correct for tissueattenuation of "/-irradiation. Regional cerebral blood flowmeasurements were obtained by recording regional levels ofcerebral 15O activity following repeated infusions 15 mCi ofH2
15O, administered through an antecubital vein, at a flowrate of 10 ml min~'. Prior to each rCBF measurement, abackground scan lasting 30 s was performed. The rCBF scanlasted 165 s and followed the background scan. Five secondsbefore the start of the rCBF scan the subjects beganperforming the activating task, the entry of the radioactivewater into the brain coinciding with performance of theactivating task. A 10-min interscan interval was used to allow15O activity to decay to background levels. Each image wasreconstructed in 31 axial planes, using a Hanning filter witha cut-off frequency of 0.5, giving an image resolution of8.5X8.5X4 mm, full width at half maximum.
Data analysisData analysis was performed on a SUN Sparc2 workstation(Sun Microsystems Europe Inc., Surrey, UK) using displaysoftware (ANALYZE 6.0: Robb and Hanson, 1991). Imagematrix calculations were performed using PRO MATLAB(Mathworks Inc., Sherborn, Mass., USA), and images wereanalysed using Statistical Parametric Mapping (SPM)software (MRC Cyclotron Unit, London, UK). The 31 planesin each image were initially interpolated to 43 planes toproduce images with ~2 mm3 voxels. Correction for headmovement between scans was conducted using a automatedrealignment program (Woods et al., 1992). The images werethen standardized by resizing into stereotactic space, usingthe intercommissural line (AC-PC) as a reference plane forreslicing and reorientation (Friston et al., 1989). The imageswere smoothed using a Gaussian filter (10X10x6 mm, fullwidth half maximum), to improve signal to noise ratio andaccommodate variability in functional anatomy. This processgenerated a normalized set of 26 image planes, parallel tothe AC-PC line, with an interplane distance of 4 mmcorresponding to the axial brain sections of the atlas ofTalairach and Tournoux (1988).
Statistical image analysisVariations in global CBF between subjects and conditions wereremoved using a voxel based ANCOVA with global blood flow
as the covariate (Friston et al, 1990). This process normalizedglobal CBF to a value of 50 ml/100 g/min and produced a meanrCBF value and adjusted error variance for each voxel foreach condition (word repetition and word generation). Thenormalized mean rCBF values for the two conditions innormals and patients were then compared with a within-groupanalysis using the t statistic for each voxel, and significantdifferences were displayed in three orthogonal projections asa statistical parametric map (SPM{f}; Friston et al., 1991a).The between-group analysis differences in mean rCBFdistribution were first assessed with y} statistic using anomnibus threshold of P < 0.001 to avoid false positives dueto multiple comparisons. Normalized mean rCBF differenceswere then again compared with the t statistic.
ResultsVerbal fluency during scanningThe number of different words produced (excluding passes)during each word generation scan was recorded as a measureof task performance. All subjects were clearly capable ofconducting the word generation task successfully, followingup to five practice trials, and, on average, produced fivepasses in 35 responses during scanning. A comparison of thescores between subject groups (ALSu, ALSi and controls)revealed no significant differences (group, P > 0.35; contrastsP > 0.15). The 95% confidence intervals for the differencein means between ALSu and ALSi (-5.3, 7.3), controls andALSu (-1.4, 7.2) and controls and ALSi (-1.4, 9.3) areconsistent with the results of the ANOVA revealing nosignificant differences between groups. This analysisdemonstrates that the three subject groups were matched interms of performance during scanning, and excludes thepossibility that differences in rCBF between groups can beassociated with this factor.
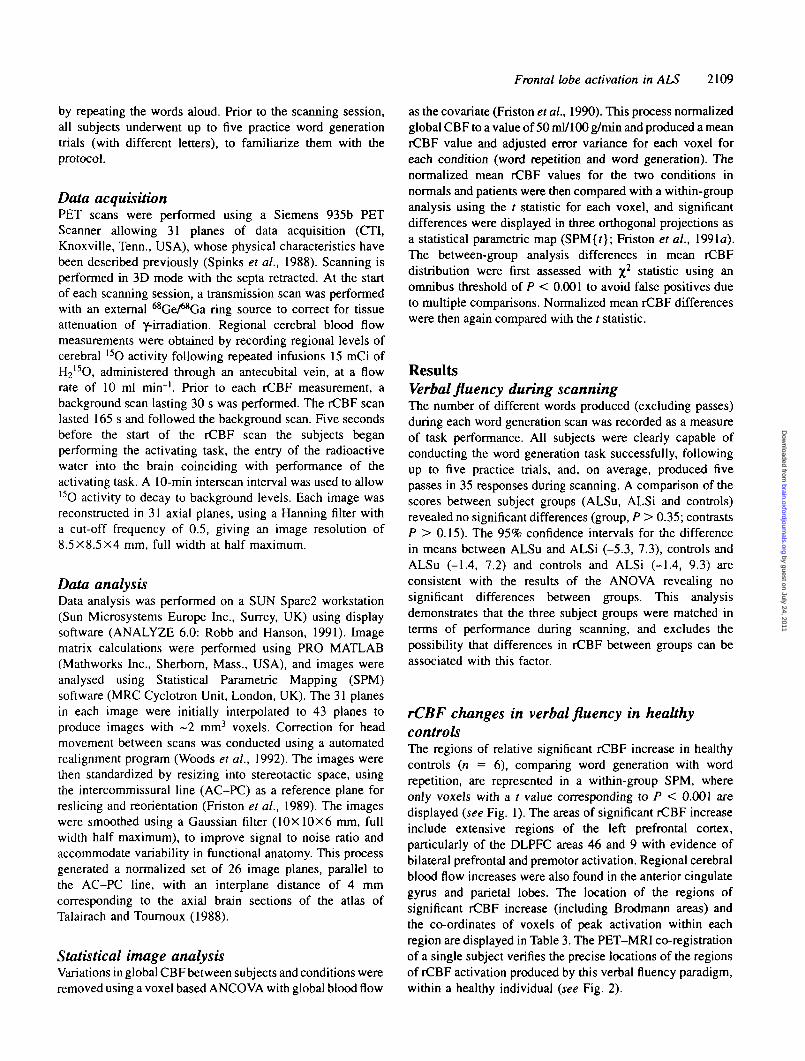
rCBF changes in verbal fluency in healthycontrolsThe regions of relative significant rCBF increase in healthycontrols {n — 6), comparing word generation with wordrepetition, are represented in a within-group SPM, whereonly voxels with a t value corresponding to P < 0.001 aredisplayed (see Fig. 1). The areas of significant rCBF increaseinclude extensive regions of the left prefrontal cortex,particularly of the DLPFC areas 46 and 9 with evidence ofbilateral prefrontal and premotor activation. Regional cerebralblood flow increases were also found in the anterior cingulategyrus and parietal lobes. The location of the regions ofsignificant rCBF increase (including Brodmann areas) andthe co-ordinates of voxels of peak activation within eachregion are displayed in Table 3. The PET-MRI co-registrationof a single subject verifies the precise locations of the regionsof rCBF activation produced by this verbal fluency paradigm,within a healthy individual (see Fig. 2).
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

2110 S. Abrahams et al.
sogitfbl coronal
IV 1
1 V
HJL VAC
- 1 0 * 68VPC VAC
0
P IPL
n\}
SPMprojections
transverse
Fig. 1 Statistical parametric map (SPM) representing increases in rCBF produced in the comparison of word repetition and wordgeneration in healthy controls (n = 6). Cortical and subcortical regions of significant (P < 0.001) rCBF increase are displayed in black.Left: sagittal, coronal and transverse projections of SPM displayed on a grid representing the stereotactic co-ordinate system of Talairachand Tournoux (1988). VAC and VPC are orientation lines transecting the anterior and posterior commissures. Right: medial and lateralview of left hemisphere (above); medial and lateral views of right hemisphere (below). The location of regions of significant change aredisplayed in Table 3.
Table 3 Cortical regions of significant rCBF increase (P < 0.001) in controls, produced in the comparison of wordgeneration with word repetition
Region Region (mmabove AC-PC)
Coordinates Z score
z)
Left dorsal prefrontal cortex (areas 9 and 46) 16-36Right dorsal prefrontal cortex (area 9) 24-36Left inferior frontal gyms (areas 44 and 45) 20-28Left anterior prefrontal cortex (area 10) 20-24Right lateral premotor cortex (areas 6 and 8) 40-64Left lateral premotor cortex (areas 6 and 8) 40-64Left medial premotor cortex (area 6) 44-60Left anterior cingulate gyms (areas 32 and 24) 24-44Left insular cortex 8-12Right insular cortex 4-20Left inferior and superior parietal lobe (areas 40 and 7) 40-48Right inferior and superior parietal lobe (areas 40 and 7) 36-48Left precuneus (area 7) 44-52Right precuneus (area 7) 36-44Left cuneus (area 19) 36Left supramarginal gyms (area 40) 36Left superior occipital gyms (area 19) 28-32Left anterior thalamus (na and dm) 18Left posterior thalamus 8Right anterior thalamus (va) 8
-3830
-40-28
18-24
0- 6
-3028
-4632
-146
- 6-34-24- 6
012
24321244
02
16142012
-42-64-68-74-78-46-66-14-30- 6
2832242460524440128
444448403636321688
5.675.934.625.734.825.505.306.125.404.434.624.384.223.643.964.453.793.123.404.03
Talairach and Tournoux coordinates of the most significant voxel within each region are displayed. AC-PC refers to the intercommissuralline; 'area' refers to the cytoarchitectonic (Brodmann) area in which significant voxels were located. Z score refers to the specifiedcoordinate, va = ventral anterior nucleus; na = anterior nucleus; dm = dorsal medial nucleus; p = pulvinar.
The comparison of verbal fluency with repetition alsoshowed relative decreases in rCBF in healthy controls. Theseregions of significant (P < 0.001) rCBF reduction (fromword repetition to word generation) were found in posteriorcingulate gyrus (areas 31, 23 and 30) and temporal lobesbilaterally; the left and right middle and inferior temporalgyri (areas 39, 21 and 37), and the left and right superior
temporal gyri (areas 22 and 38). This is consistent withfindings reported by Frith et al. (1991a).
Comparison of rCBF activation between groupsThe ALSi group versus controlsThe ALSi group displayed significantly (P < 0.001) impairedactivation in the DLPFC (areas 46 and 9), premotor cortex
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

Frontal lobe activation in ALS 2111
"Fig. 2 Increases in rCBF in a single healthy control subject. Co-registered PET and MRI images. Left: transverse section 4 mm aboveAC-PC line, areas of rCBF increase include left dorsolateral prefrontal cortex (DLPFC; areas 46 and 45) Middle: transverse section38 mm above AC-PC line, areas of rCBF increase include left and right DLPFC (area 9) anterior cingulate (area 32), left inferiorparietal lobe (areas 40 and 19). Right: transverse section 55 mm above AC-PC line, areas of rCBF increase include left premotor cortex(areas 8 and 6) and right premotor cortex (area 8).
sagittal coronal
Ai
= •
n
^v -"C VAC- 1 0 *
VPCVAC6B
SPMprojections
transverse
Fig. 3 Between-group SPM comparing the pattern of activation in ALSi and control groups. Cortical and subcortical regions showingsignificantly (P < 0.001) impaired activation in the ALSi group compared with controls, are displayed in black. Left: sagittal, coronaland transverse projections. Right: medial and lateral views of left hemisphere (above): medial and lateral views of right hemisphere{below). The location of the regions displayed are described in Table 4.
(8 and 6), insular cortex (see Fig. 3.) and thalamus (see Table4). Differences in activation arose as a result of increases inrCBF in controls relative to ALSi patients comparing wordgeneration with word repetition.
The ALSu group versus controlsA comparison of the ALSu group with controls at an omnibussignificance level of P < 0.001 revealed minor differencesin rCBF activation between the two groups (see Fig. 4).Areas of impaired activation included right dorsal prefrontalcortex (area 9), the left and right inferior parietal lobule (area
40) and the left middle and superior temporal gyri (areas 39and 22).
The ALSi group versus the ALSu groupThe comparison of the two patient groups (ALSi versusALSu) produced a similar pattern of rCBF activationdifferences as found in the comparison of the ALSi groupwith controls (see Fig. 5). The regions of significant (P< 0.001) difference included prefrontal cortex, lateral andmedial premotor cortex, bilateral insular cortex, andthalamus (see Table 5). In general, these differences were
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

2112 S. Abrahams et al.
Table 4 Regions of significant difference (P < 0.001) in activation in the comparison between the control and the ALSi(ALS impaired) groups
Region Region(mm above —AC-PC) (x
Coordinates % Changesin rCBF
z) controls/ALSi
Z score
Left dorsal prefrontal cortex (areas 46 and 9) 24-32Left anterior prefrontal cortex (area 10) 24Right medial prefrontal cortex (area 9) 36-44Right lateral prefrontal cortex (area 9) 28-36Right anterior medial prefrontal cortex (area 10) 20Left medial premotor cortex (area8) 36—44Left lateral premotor cortex (areas 6 and 8) 44-52Right lateral premotor cortex (area 8) 40-48Right primary motor cortex (area 4) 52-56Left primary motor cortex (area 4) 44Left anterior cingulate gyrus (area 24) 24Left posterior cingulate gyrus (area 23) 28Left insular cortex 16Right insular cortex 8-16Left precuneus (area 7) 48-52Left cuneus (area 19) 32-36Right cuneus (area 18) 24Left anterior thalamus (na and dm) 12-16Right anterior thalamus (va) 16Left posterior thalamus 8-12
- 3 4- 2 2
42812
- 1 0- 3 6
2636
- 4 4- 8
- 1 0- 630
- 8- 1 2
10- 2 6
10- 4
385248325044
23012
- 21634144
6680
•8210
- 432
282436362036524052442428168
5232241688
+3.4/-3.5+2.11-2.1—1.1/—6.6+5.0/-0.4+0.5/-2.6+2.27-5.6+2.8/-4.5+4.3/-0.2+ 1.9/-3.0+2.2/-3.3+5.1/-0.5+2.4/-3.5+ 1.9/-4.2+2.3/-2.1+3.1/-3.4+2.9/-2.5+ 1.9/-2.8+ 1.7/-2.1+ 3.3/-2.8+3.2/-2.2
3.833.183.334.173.183.254.353.253.303.703.213.173.123.763.753.463.113.384.033.31
% Changes in rCBF denotes the change in rCBF from word repetition to word generation (a positive sign denotes a relative activationand a negative sign a relative deactivation). Talairach and Tournoux coordinates (and corresponding Z score) of the most significantvoxel within the region are displayed. See Table 3 legend for abbreviations.
/
V
- • -
BOgrttd
1 i— \\
72
n
32J
i
Lil
a an\
f
al
1 '
r 1-104 66
VPC VAC
0
64
\
\s
*
f
\\
yJ
SPMprojections
iransvans
Fig. 4 Between-group SPM comparing the pattern of activation in ALSu and control groups. Cortical and subcortical regions showingsignificantly (P < 0.001) impaired activation in the ALSu group in comparison with controls are displayed in black. Left: sagittal,coronal and transverse projections. Right: medial and lateral views of left hemisphere {above); medial and lateral views of righthemisphere {below).
due to increases in rCBF in the ALSu group relative tothe ALSi group comparing word generation with wordrepetition {see Table 5).
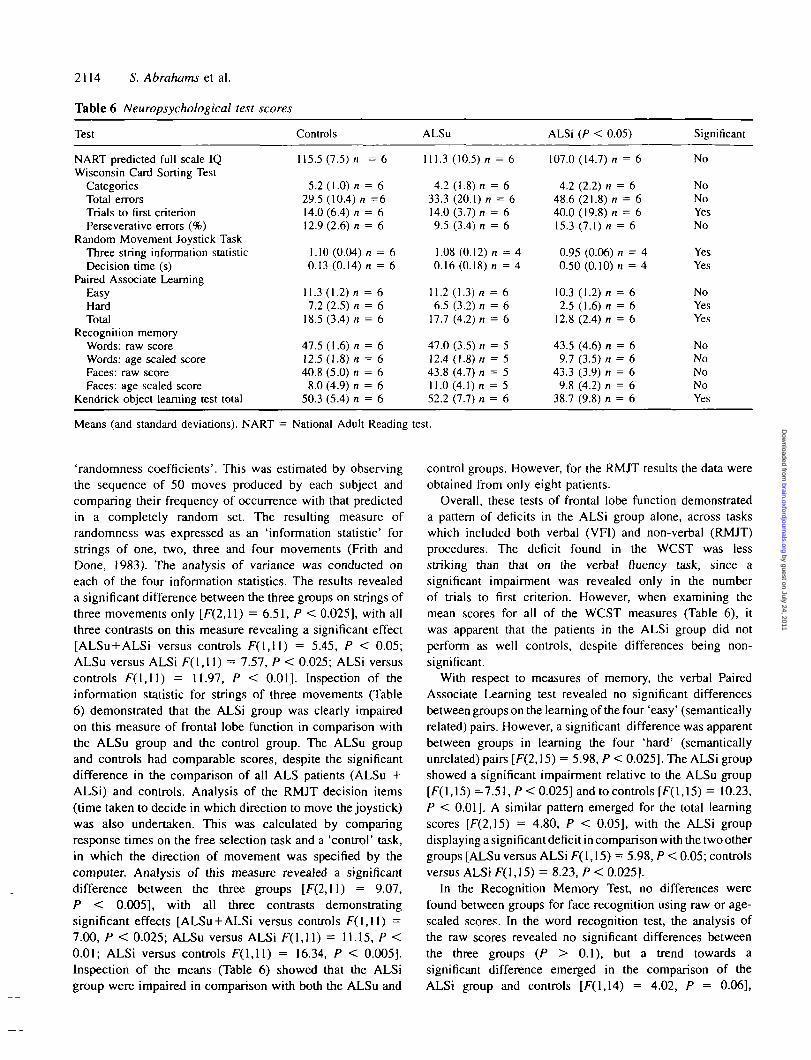
Neuropsychological testsThe mean scores (and standard deviations) for theneuropsychological tests are reported in Table 6. The analysisof variance on National Adult Reading Test—Revised, IQ
scores revealed no significant differences between the groups{P > 0.05). The 95% confidence intervals for the differencein means between ALSu and ALSi (-8.2, 20.8), controls andALSu (-8.1, 12.5), controls and ALSi (-5.4, 21.7) areconsistent with the results of the ANOVA, demonstratingthat the three groups were matched in premorbid IQ.
The WCST was measured in terms of four scores: numberof categories achieved (maximum of six), total number oferrors, trials to first criterion (number of trials taken to
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

Frontal lobe activation in ALS 2113
- t ( M
1
V•L V J.
*—<i
\s n
I f-4
-T
f-f
1
T
i--*
-
VPCVAC
fi4
/
\
**
yjtransverse
SPMprojections
Fig. 5 Between-group SPM comparing the pattern of activation in ALSi and ALSu. Cortical and subcortical regions of significantly(P < 0.001) impaired activation in the ALSi group in comparison with the ALSu group are displayed in black. Left: sagittal, coronal andtransverse projections. Right: left hemisphere (above); right hemisphere (below). The locations of the regions displayed are described inTable 5.
Table 5 Regions of significant difference (P < 0.001) in activation in the comparison between the ALSu (ALS unimpaired)and ALSi (ALS impaired) groups
Region Region(mm aboveAC-PC)
Coordinates
v) •r)
% ChangesinrCBFALSu/ALS
Z score
Left DPFC (area 46)Left DPFC (area 46)Right DPFC (areas 44 and 45)Right medial prefrontal cortex (area 9)Right lateral prefrontal cortex (area9)Right premotor cortex (area 8)Left medial premotor cortex (area 8)Left lateral premotor cortex (area 8)Left anterior medial premotor cortex (area 8)Right medial premotor cortex (area 8)Left paracentral lobuleLeft SMA (paracentral lobule)Right primary motor cortex (area 4)Left primary motor cortex (area 4)Left primary motor cortex (area 4)Right cingulate gyms (area 24)Left anterior cingulate gyrus (area 24)Right insular cortexLeft insular cortexLeft anterior thalamus (na and dm)Right posterior thaJamus (p)
24-281616-202824-2852-565244-484036-444844-485244-4832-3636^401216-20161612
- 3 6- 3 4
44241512
- 8- 4 6- 812
- 1 6- 1 2
34- 4 6- 5 0- 1 0- 826
-22- 412
3646146502632-64440•3414-4-6-8123216814•26
281620282856524440404844524432401220161612
+2.6/-4.I+5.5/-1.1+0.1/—3.9+0.2/-4.0+ 1.0/-3.1-0.4/-6.7-2.0/-7.9-0.1/-4.8-2.0/-7.3-0.5/-4.9+ I.3/-3.5+ 3Z7/-2.6+ 1.1/-4.0+ 3.7/-2.7+3.0/-1.6+3.0/-4.1+2.5/-2.5+ 1.4/-4.0+ 1.9/-3.I+ 1.5/-4.7+ 2.6/-3.0
3.523.443.223.133.203.293.103.453.233.263.183.183.173.743.184.023.103.103.113.073.10
SMA = supplementary motor area; DPFC = dorsal prefrontal cortex. See Table 3 legend for abbreviations.
complete the first category) and perseverative errors (wherethe subject continues to use a previous and irrelevant rule).No significant differences emerged between groups on thecategory scores or on the total number of errors. The analysisof perseverative errors revealed a trend towards a significantdifference in the comparison of the two patient groups[F(1,I3) = 3.84, P = 0.07], with the ALSi patientsshowing greater perseveration than the ALSu group.However, there was no overall difference between thethree groups and the ALSi group were not significantly
impaired relative to controls. In the analysis of the numberof trials taken to reach the first criterion, a significantdifference emerged between the three groups, [F(2,14) =9.09, P < 0.005], with a clearly significant impairment inthe ALSi patients as compared with the ALSu group[F( 1,14) = 14.04, P < 0.005] and controls [ALSi versuscontrols, F( 1,14) = 14.04, P < 0.005]. This resultdemonstrated a deficit in the ALSi group in the speed atwhich they learned to sort the cards and deduce the first rule.
Performance on the RMJT was measured in terms of
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from
2114 S. Abrahams et al.
Table 6 Neuropsychological test scores
Test
NART predicted full scale IQWisconsin Card Sorting Test
CategoriesTotal errorsTrials to first criterionPerseverative errors (%)
Random Movement Joystick TaskThree string information statisticDecision time (s)
Paired Associate LearningEasyHardTotal
Recognition memoryWords: raw scoreWords: age scaled scoreFaces: raw scoreFaces: age scaled score
Kendrick object learning test total
Controls
U5.5(7.5)/i = 6
5.2 (1.0) n = 629.5 (10.4) n =614.0 (6.4) n = 612.9 (2.6) n = 6
1.10(0.04)/i = 60.13 (0.14) n = 6
11.3(1.2) n = 67.2 (2.5) n = 6
18.5 (3.4) n = 6
47.5(1.6) n = 612.5(1.8) n = 640.8 (5.0) n = 6
8.0 (4.9) n = 650.3 (5.4) n = 6
ALSu
111.3 (10.5)/i = 6
4.2(1.8)/i = 633.3 (20.1)/i = 614.0 (3.7) n = 69.5 (3.4) n = 6
1.08 (0.12)/i = 40.16(0.18)/! = 4
11.2(1.3)/! = 66.5 (3.2) n = 6
17.7 (4.2)/i = 6
47.0 (3.5) n = 512.4(1.8)/i = 543.8 (4.7) n = 511.0 (4.1) n = 552.2 (7.7) n = 6
ALSi (/> < 0.05)
107.0 (14.7) n = 6
4.2 (2.2) n = 648.6(21.8)/! = 640.0(19.8)/! = 615.3 (7.1)/i = 6
0.95 (0.06) /i = 40.50(0.10)/! = 4
10.3 (1.2)/i = 62.5 (1.6)/i = 6
12.8 (2.4)/i = 6
43.5 (4.6) /i = 69.7 (3.5) /i = 6
43.3 (3.9) /i = 69.8 (4.2) /i = 6
38.7 (9.8) n = 6
Significant
No
NoNoYesNo
YesYes
NoYesYes
NoNoNoNoYes
Means (and standard deviations). NART = National Adult Reading test.
'randomness coefficients'. This was estimated by observingthe sequence of 50 moves produced by each subject andcomparing their frequency of occurrence with that predictedin a completely random set. The resulting measure ofrandomness was expressed as an 'information statistic' forstrings of one, two, three and four movements (Frith andDone, 1983). The analysis of variance was conducted oneach of the four information statistics. The results revealeda significant difference between the three groups on strings ofthree movements only [F(2,ll) = 6.51, P < 0.O25], with allthree contrasts on this measure revealing a significant effect[ALSu + ALSi versus controls F(l , l l ) = 5.45, P < 0.05;ALSu versus ALSi F(l , l l ) = 7.57, P < 0.025; ALSi versuscontrols F(l , l l ) = 11.97, P < 0.01]. Inspection of theinformation statistic for strings of three movements (Table6) demonstrated that the ALSi group was clearly impairedon this measure of frontal lobe function in comparison withthe ALSu group and the control group. The ALSu groupand controls had comparable scores, despite the significantdifference in the comparison of all ALS patients (ALSu +ALSi) and controls. Analysis of the RMJT decision items(time taken to decide in which direction to move the joystick)was also undertaken. This was calculated by comparingresponse times on the free selection task and a 'control' task,in which the direction of movement was specified by thecomputer. Analysis of this measure revealed a significantdifference between the three groups [F(2,ll) = 9.07,P < 0.005], with all three contrasts demonstratingsignificant effects [ALSu + ALSi versus controls / r(l , l l) =7.00, P < 0.025; ALSu versus ALSi F(l , l l ) = 11.15, P <0.01; ALSi versus controls F(l , l l ) = 16.34, P < 0.005].Inspection of the means (Table 6) showed that the ALSigroup were impaired in comparison with both the ALSu and
control groups. However, for the RMJT results the data wereobtained from only eight patients.
Overall, these tests of frontal lobe function demonstrateda pattern of deficits in the ALSi group alone, across taskswhich included both verbal (VFI) and non-verbal (RMJT)procedures. The deficit found in the WCST was lessstriking than that on the verbal fluency task, since asignificant impairment was revealed only in the numberof trials to first criterion. However, when examining themean scores for all of the WCST measures (Table 6), itwas apparent that the patients in the ALSi group did notperform as well controls, despite differences being non-significant.
With respect to measures of memory, the verbal PairedAssociate Learning test revealed no significant differencesbetween groups on the learning of the four 'easy' (semanticallyrelated) pairs. However, a significant difference was apparentbetween groups in learning the four 'hard' (semanticallyunrelated) pairs [F(2,15) = 5.98, P < 0.025]. The ALSi groupshowed a significant impairment relative to the ALSu group[F(l,15) =7.51, P < 0.025] and to controls [F(l,15) = 10.23,P < 0.01]. A similar pattern emerged for the total learningscores [F(2,15) = 4.80, P < 0.05], with the ALSi groupdisplaying a significant deficit in comparison with the two othergroups [ALSu versus ALSi F(l,15) = 5.98, P < 0.05; controlsversus ALSi F(l, 15) = 8.23, P < 0.025].
In the Recognition Memory Test, no differences werefound between groups for face recognition using raw or age-scaled scores. In the word recognition test, the analysis ofthe raw scores revealed no significant differences betweenthe three groups (P > 0.1), but a trend towards asignificant difference emerged in the comparison of theALSi group and controls [F(l,14) = 4.02, P = 0.06],
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

Frontal lobe activation in ALS 2115
with the ALSi group displaying lower scores. For agescaled scores, a similar pattern was revealed with noevidence of an effect of group although contrastsdemonstrated a trend towards a significant differencebetween the ALSi group and controls [F(l,14) = 3.74,P = 0.07].
The analysis of performance on the Kendrick objectlearning test was conducted on total scores, as the threegroups were closely age-matched. The ANOVA revealed asignificant group effect 17(2,15) = 5.21, P < 0.025] withthe contrasts demonstrating a significant differencebetween ALSu and ALSi groups [F(l,15) = 8.86, P < 0.01]and between ALSi patients and controls [F(l,15) = 6.62,P < 0.025], in each case, with poorer performance by theALSi group. Therefore the above tests revealed evidence ofmemory impairments in the ALSi group only, with significantdeficits on the Kendrick object learning test and PairedAssociate Learning Task.
Overall, the findings of the neuropsychological assessmentrevealed a profile of cognitive dysfunction in the ALSigroup, with deficits on frontal lobe and memory tasks, whilecognitive functions in the ALSu patients appeared to berelatively unaffected.
DiscussionThe findings of this study clearly illustrate that regional brainactivation abnormalities, particularly in the frontal associationareas, can be detected in a subgroup of ALS subjects, usinga paced verbal fluency PET paradigm. Cognitively impairedALS patients showed impaired activation in DLPFC (leftareas 46, 9 and 10; right area 9), lateral and medial premotorcortex (areas 6 and 8) and frontal cortex (areas 8 and 9).They also displayed bilateral impaired activation of theinsulae and anterior thalamic nuclei. In contrast, rCBFactivation in ALS patients who performed normally on thewritten verbal fluency task (ALSu) was similar to healthycontrols. This pattern of results was revealed despite matchedperformance between the three groups on the scanningparadigm, hence differences in rCBF activation cannot beassociated with verbal output during scanning.
Cerebral regions activated by verbal fluencyparadigmThe task, adapted from Frith et al. (1991a), activated regionsof the frontal cortex, particularly the left DLPFC; areas 46and 9, in a group of healthy subjects. The location of thisregion of activation was verified in a control subject, throughthe direct co-registration of rCBF increases onto the MRIscan. Activation of the left DLPFC is consistent with rCBFincreases reported in previous studies of internal wordgeneration (Friston et al., 1991; Frith etal., 1991a, b; Cantor-Graae et al., 1993). In contrast to the study by Frith et al.(1991a), the regions of cerebral activation revealed in the
current task extended beyond the left DLPFC, as bilateralprefrontal rCBF increases were revealed. Such bilateralprefrontal activity has also been demonstrated in other tasksrequiring volitional output such as internal generation ofpaced joystick movements, in freely chosen directions(Deiber et al., 1991) and freely chosen finger movements(Frith et al., 1991a). These nonverbal procedures are similarto verbal fluency in that responses are not wholly specifiedby the immediate situation and so decision making is centralto the tasks. Our current study also revealed rCBF increasesin the anterior cingulate gyms (areas 32 and 24) during wordgeneration consistent with previous reports. This region isprobably concerned with processes of response selection andattention (Petersen et al, 1988; Frith et al, 1991a).
The regions of rCBF increase seen in healthy controlsduring word generation also encompassed areas known to beinvolved in language production, including regions of Broca'sarea (areas 44 and 45 and lateral premotor cortex 6; seeMesulam, 1990). The task was designed to ensure that diespeech components of the word repetition and wordgeneration conditions were matched, using a paced procedurein which the subject responded to every stimulus. However,differences may have occurred in the amount of subvocalspeech each condition generated. Verbal fluency not onlyinvolves intrinsic generation, but also working memory.Letter-based fluency paradigms encourage the processingand manipulation of phonological information, which (inBaddeley's working memory model), is rehearsed throughsubvocalization within the articulatory loop (Baddeley, 1986).Functional studies have associated subvocal rehearsal andthe covert retrieval of words with regions involved in theproduction of speech sounds, i.e. Broca's area (Wise et al,1991; Demonet et al, 1992; Hinke et al, 1993; Paulesuet al, 1993). In the word repetition condition, fewer demandsare placed on working memory and subvocalization isunnecessary, as the response is fully specified by the stimulusand generated immediately after the stimulus presentation.
The paced verbal fluency paradigm employed alsoproduced activation within the superior, inferior and medialaspects of the parietal lobes (areas 7 and 40). Connectionsbetween the prefrontal cortex (area 46) and superior parietallobe have been described by Pandya and Barnes (1987). Inaddition, activation of the inferior parietal lobe was reportedin covert word retrieval paradigms using verb generation(Warburton et al, 1996). Reports have also associated suchregions of the parietal cortex to the processing of phonologicalinformation (Demonet et al, 1992, 1994; Zatorre et al,1992). In neuropsychological investigations of brain-damagedpatients (Shallice and Vallar, 1990), the left inferior parietallobule was shown to be associated with the short-termphonological store. This was recently supported by thedemonstartion of activation of the supramarginal gyms in aphonological short-term memory task (Paulesu et al. 1993)and is consistent with the intensive connectivity which isfound between parietotemporal cortex and Broca's area(Mesulam, 1990). Paulesu et al, (1993) also showed
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from
2116 S. Abrahams et al.
association of bilateral increases in the insulae with suchphonological processes. A similar pattern of activation wasfound in the current study.
Hence, in the current paradigm, the pattern of rCBF changein healthy controls (in regions other than the DLPFC) maybe related to demands on working memory. In orthographicverbal fluency, subvocal rehearsal and the short-term memoryof phonological information is required to help cue word-retrieval and keep track of recent responses to avoid repetition(Jones-Gotman and Milner, 1977; Miller, 1984). The presentparadigm may more reliably detect such areas of activationassociated with verbal fluency, as a greater number of rCBFmeasurements were acquired (four measurements of eachcondition, in six subjects) than in previous studies.
Cortical and subcortical dysfunction in ALSThe results of the current investigation revealed frontalassociation area dysfunction in those ALS patients withcognitive impairment. Dysfunction of the DLPFC inALS is consistent with reports from neuropsychologicalinvestigations of frontal lobe (executive) type cognitivedeficits (Gallassi et al., 1985, 1989; David and Gillham,1986; Ludolph et al., 1992; Kew et al, 1993ft). Verbalfluency deficits have been frequently related to lesions of theleft prefrontal cortex (Benton, 1968; Miceli et al., 1981;Pendleton et al., 1982; Miller, 1984; Bornstein, 1986) andsuch impairments are repeatedly found in ALS using verbaland non-verbal tasks of the fluency-type (Gallassi et al.,1985, 1989; Ludolph et al., 1992; Kew et al., 1993ft). Inaddition, the results of our neuropsychological assessment ofALSi patients revealed evidence of executive dysfunction onverbal and nonverbal frontal lobe tests, with deficits on theRMJT and one measure of WCST, i.e. trials to first criterion.The RMJT was based on an activation paradigm reported byDeiber et al. (1991) which was associated with bilaterallyincreased rCBF in the DLPFC (as described above). Thetask involves the production of freely chosen sequencesof movements and is similar to verbal fluency in terms ofintrinsic generation; the ALSi subgroup was impaired interms of its ability to generate a random string of movements.The neuropsychological profile displayed by the ALSi patientsis therefore characterized by deficits in tests of verbal andnon-verbal willed actions. Several studies have also reportedan association between deficits on the WCST and damageof the DLPFC (Milner, 1963, 1971). The WCST has beenemployed as a functionally activating task and is alsoassociated with rCBF increases in this region of the prefrontalcortex (Weinberger et al., 1986). Hence, the results of thisneuropsychological investigation are in accordance with thepattern of rCBF abnormalities, in that ALS patients withfrontal lobe executive-type deficits display correspondingdysfunction of the DLPFC.
Cortical abnormalities in non-demented ALS patients have,until recently, not been well documented. However, thefinding of frontal lobe involvement is supported by some brain
imaging investigations. Ludolph et al. (1992) demonstratedreduced cortical glucose utilization in a group of 18 ALSpatients. Neuropsychological assessment, conducted on someof these patients, revealed deficits in verbal and non-verbalfluency tests; however, no impairment was found on theWCST. Talbot et al. (1995) demonstrated pronouncedreductions in rCBF in frontal and anterior temporal corticesin non-demented patients with classical ALS using singlephoton emission computed tomography. These patientsshowed evidence of subtle frontal lobe dysfunction with asignificant deficit on a picture sequencing task, and trendstowards reduced verbal fluency and category formation onthe WCST. Structural imaging studies have typically shownatrophy restricted to the motor cortex and cortico-spinal tractsin non-demented ALS patients, using CT (Poloni et al., 1986;Gallassi et al., 1989) and MRI (Goodin et al., 1988; Luiset al., 1990; Abe et al., 1993; Ishikawa et al., 1993), withfrontal lobe atrophy limited to ALS patients with dementia(Abe et al., 1993). Recently more sensitive analysistechniques using volumetric measurements have revealedatrophy of the underlying subcortical white matter in theanterior frontal cortex, but with no significant frontal corticalatrophy. In addition, in a longitudinal investigation of ALSpatients, progressive atrophy of the frontal and temporalregions with serial CT and MRI was reported (Kato et al.,1993). This study demonstrated atrophy involving initiallythe frontal and anterior temporal lobes and progressing topre- and then post-central gyrus, anterior cingulate and corpuscallosum. Three of the patients studied were also demented;however, the fronto-temporal degeneration was not restrictedto these patients. Unfortunately in neither of these structuralimaging investigations were the findings related toneuropsychological status.
The findings of our current investigation suggest that thedeficit in verbal fluency revealed in several neuro-psychological investigations is predominantly a result ofdysfunction of the DLPFC. The pattern of impaired activationin the ALSi group did not include other regions which maybe associated with the working memory component of thetask (Broca's area and area 40 of the parietal cortex; seePaulesu et al., 1993). Bilateral abnormalities in rCBF werealso revealed in lateral and medial premotor areas whencomparing ALSi patients with controls. These regions, how-ever, were located dorsal to those associated with Broca'sarea. In addition, the comparison of the two patient groupsrevealed a significant impairment of activation of the supple-mentary motor area in ALSi patients. In the study of short-term memory and phonological processing conducted byPaulesu et al. (1993), activation of the supplementary motorarea was demonstrated, even though the task was conductedusing covert speech. This region may be involved in themotor aspect of vocal or subvocal speech preparation andexecution, hence dysfunction could exaggerate the verbalfluency deficit. This pattern of rCBF abnormalities is sup-ported by our previous findings of reduced rCBF in the lateralpremotor cortex (area 6) bilaterally and in the supplementary
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

Frontal lobe activation in ALS 2117
motor area in resting state scans of ALS patients (Kewet al, 1993a).
The comparison of ALSi patients with controls alsorevealed impaired activation bilaterally in the anterior insularcortex. Unilateral dysfunction in this region has been reportedpreviously in ALS patients, with reduced rCBF at rest,but increased activation during upper limb movement, ascompared with healthy controls (Kew et al., 1993a). In theworking memory task conducted by Paulesu et al. (1993),the insular cortex was bilaterally activated in control subjects,suggesting that this region is involved in phonologicalprocessing. In addition, the insulae also possess specificconnections to areas 45 and 46 of the prefrontal cortex(Mesulam and Mufson, 1985). Hence dysfunction of theinsular cortex could also contribute to the production offluency-type deficits in ALS.
The results of this investigation also support our previousfindings of subcortical involvement in ALS patients withcognitive impairment. In our earlier investigations,impaired activation was revealed in some ALS patients,involving the medial prefrontal cortex, anterior cingulategyrus, parahippocampal gyrus and anterior thalamic nuclearcomplex (Kew et al., 1993a, b). Attenuation of rCBF alongthis pathway was associated with the presence of impairedwritten verbal fluency. This is supported by the presentcomparison of ALSi patients and controls which revealedreduced rCBF bilaterally in predominantly anterior, butalso posterior thalamus. Fibres running through the anteriorthalamic nuclei project to the medial prefrontal areas and tothe lateral premotor cortices (Aggleton et al., 1986;Bachevalier and Mishkin, 1986; Walsh, 1994). Our findingsalso suggest impairment of activation of the dorsomedialthalamic nucleus which projects to the prefrontal cortex(Walsh, 1994). However, resolution using PET is not sufficientto determine involvement of specific nuclei.
Thalamic degeneration has been shown to be associatedwith motor neuron disease in a number of investigations.Brownell et al. (1970) reported thalamic gliosis in 53% of36 cases of non-demented patients with ALS. In addition,subcortical involvement in ALS is corroborated by Ludolphet al. (1992), who noted reduced resting glucose metabolismin the thalamus, although this reduction was not significant.Ludolph et al. (1992) suggested that the findings of cognitivedeficits in ALS may be related to degeneration of subcorticalstructures. Thalamic abnormalities have been associated withsevere cognitive changes resulting in dementia in a numberof studies (Cambier and Graveleau, 1985; Moossy et al.,1987). Unilateral thalamic damage has been associated withmemory loss and frontal signs (Speedie and Heilman, 1982,1983). Thalamic dysphasia has also been observed with anaccompanying verbal adynamia (see Walsh, 1994). This ischaracterized by a lack of spontaneous speech and is clearlyassociated with processes of intrinsic generation related tothe DLPFC. The reduced thalamic activation and glucosemetabolism currently seen may, however, simply reflectreduced afferent input and not intrinsic degeneration of this
nucleus. Indeed, in view of the evidence for extra-motorcortical damage in ALS (Smith, 1960; Okamoto et al, 1992;Kato et al, 1993; Kiernan and Hudson, 1994; Leigh et al,1994), subcortical degeneration is unlikely to be the dominantcause of neuropsychological impairments, although it isalmost certainly contributory.
Involvement of the hippocampal system in ALS reportedin our previous investigation could not be verified in thisstudy, since the verbal fluency paradigm employed doesnot activate this region in healthy controls. However, theneuropsychological profile of the ALSi patients also revealedevidence of memory impairments, which is consistent withdysfunction of the limbic system. Deficits were found on theKendrick Object Learning Test and Paired Associate Learningtest, supporting previous reports of impairments on visualrecall (Gallassi et al, 1985, 1989; Kew et al, 1993/?) andverbal memory (Gallasi et al, 1985; David and Gillham,1986; Iwasaki et al, 1990a, b). Pathological changes inlimbic structures consisting of ubiquitin immunoreactiveinclusions in the dentate gyrus of the hippocampus andassociated entorhinal cortex and in the amygdala are presentin some non-demented ALS subjects (Okamoto et al, 1991;Wightman et al, 1992; Leigh et al, 1994; Anderson et al,1996).
Altered function in extra-motor cortex in non-dementedpatients with cognitive impairment, closely parallels theregions most affected in patients with ALS with dementia(Neary et al, 1990; Kew and Leigh, 1992; Wightman et al,1992; Talbot et al, 1995). The neuropsychological profileof ALS patients with dementia is also characterized bybehavioural and cognitive problems reflecting gross frontallobe dysfunction, with relative preservation of functionsof the posterior association cortices (Neary et al, 1990).Behavioural features include disinhibition, apathy, and per-sonality changes (Kew and Leigh, 1992). Neuro-psychological test results are difficult to obtain. However,some studies have demonstrated gross deficits in verbalfluency, attention, and tests requiring the ability to shift fromone line of thinking to another, similar to the WCST (Peavyet al, 1992; Kato et al, 1994; Talbot et al, 1995). Hencethe findings of the current and earlier investigations demon-strates that some non-demented ALS patients display a lesserdegree of the cognitive dysfunction found in ALS-dementiapatients. This has led to the suggestion that a spectrum ofextra-motor cortical and subcortical involvement exists inALS (Leigh et al, 1994), although an alternative hypothesisis that an ALS subgroup exists, characterized by cognitiveimpairment. Interestingly ALS-related dementia frequentlyoccurs in conjunction with bulbar pathology, which may bepresent in up to 85% of cases (Wikstrom et al, 1982;Mitsuyama, 1984; Kew and Leigh, 1992; Talbot et al, 1995).In this study, clinical features were similar in cognitivelyimpaired and unimpaired groups, but there was a tendencyfor the ALSi group to show greater bulbar involvement thanthe ALSu patients. In addition there was a slightly higherincidence of pseudobulbar involvement in patients with
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

2118 S. Abrahams et al.
cognitive impairment, suggesting the possibility of a subtleassociation. Only longitudinal studies will indicate whetherthe two groups are dissimilar from the outset, or whethersubjects in the ALSu group progress to show the samecognitive impairments identified in the ALSi patients.
In summary, this investigation has demonstrated that PETactivation studies are an effective technique for detectingfrontal lobe dysfunction in ALS subjects and has revealedevidence of impaired function in the prefrontal cortex insome non-demented patients with ALS, associated withselective cognitive deficits. It has also provided evidence thatdorsolateral and not just medial prefrontal cortex may beimpaired in some ALS patients. The PET findings areconsistent with dysfunction of thalamo-cortical pathways, assuggested in our previous studies using a motor paradigm(Kew et al., 1993&). Future studies will need to define thetemporal sequence of cognitive changes and the pathologicalcorrelates of frontal lobe involvement in ALS subjects.These observations will help to identify important phenotypicvariations in ALS.
AcknowledgementsThis project was supported by the Medical Research Councilof Great Britain, and additional assistance was provided bythe Tregaskis Bequest (University of London), the WellcomeTrust and the Guarantors of Brain.
ReferencesAbe K, Fujimura H, Toyooka K, Hazama T, Hirono N, Yorifuji S,et al. Single-photon emission computed tomographic investigationof patients with motor neuron disease [see comments]. Neurology1993; 43: 1569-73. Comment in: Neurology 1994; 44: 1186-7.
Aggleton JP, Desimone R, Mishkin M. The origin, course, andtermination of the hippocampothalamic projections in the macaque.J Comp Neurol 1986; 243: 409-21.
Anderson VER, Caims N, Leigh PN. Involvement of the amygdalain motor neurone disease. J Neurol Sci 1996. In press.
Bachevalier J, Mishkin M. Visual recognition impairment followsventromedial but not dorsolateral prefrontal lesions in monkeys.Behav Brain Res 1986; 20: 249-61.
Baddeley A. Working memory. Oxford' Clarendon Press, 1986.
Benton AL. Differential behavioral effects in frontal lobe disease.Neuropsychologia 1968; 6: 53-60.
Bornstein RA. Contributions of various neuropsychologicalmeasures to detection of frontal lobe impairment. Int J ClinNeuropsychol 1986; 3: 18-22.
Brownell B, Oppenheimer DR, Hughes JT. The central nervoussystem in motor neurone disease. J Neurol Neurosurg Psychiatry1970; 33: 338-57.
Cambier J, Graveleau T. Thalamic syndromes. In: Vinken PJ, BruynGW, Klawans HL, editors. Handbook of clinical neurology, Vol.45. Amsterdam: Elsevier, 1985: 87-98.
Cantor-Graae E, Warkentin S, Franzen G, Risberg J. Frontal lobechallenge: a comparison of activation procedures during rCBFmeasurements in normal subjects Neuropsychiat NeuropsycholBehav Neurol 1993; 6: 83-92.
David AS, Gillham RA. Neuropsychological study of motor neurondisease. Psychosomatics 1986; 27: 441-5.
Deiber M-P, Passingham RE, Colebatch JG, Friston KJ, Nixon PD,Frackowiak RSJ. Cortical areas and the selection of movement: astudy with positron emission tomography. Exp Brain Res 1991; 84:393-402.
Demonet J-F, Chollet F, Ramsay S, Cardebat D, Nespoulous JL,Wise R, et al. The anatomy of phonological and semantic processingin normal subjects. Brain 1992; 115: 1753-68.
Demonet J-F, Price C, Wise R, Frackowiak RSJ. Differentialactivation of right and left posterior sylvian regions by semanticand phonological tasks: a positron-emission tomography study innormal human subjects. Neurosci Lett 1994; 182: 25-8.
Friston KJ, Passingham RE, Nutt JG, Heather JD, Sawle GV,Frackowiak RSJ. Localisation in PET images: direct fitting of theintercommissural (AC-PC) line. J Cereb Blood Flow Metab 1989;9: 690-5.
Friston KJ, Frith CD, Liddle PF, Dolan RJ, Lammertsma AA,Frackowiak RSJ. The relationship between global and local changesin PET scans. J Cereb Blood Flow Metab 1990; 10: 458-66.
Friston KJ, Frith CD, Liddle PF, Frackowiak RSJ. Comparingfunctional (PET) images: the assessment of significant change. JCereb Blood Flow Metab 1991; 11: 690-9.
Frith CD, Done DJ. Stereotyped responding by schizophrenicpatients on a two-choice guessing task. Psychol Med 1983; 13:779-86.
Frith CD, Fnston K, Liddle PF, Frackowiak RSJ. Willed action andthe prefrontal cortex in man: a study with PET. Proc R Soc LondB Biol Sci 1991a; 244: 241-6.
Fnth CD, Friston KJ, Liddle PF, Frackowiak RSJ. A PET study ofword finding. Neuropsychologia 1991b; 29: 1137-48.
GaJlassi R, Montagna P, Ciardulli C, Lorusso S, Mussuto V,Stracciari A. Cognitive impairment in motor neuron disease. ActaNeurol Scand 1985; 71: 480-4.
Gallassi R, Montagna P, Morreale A, Lorusso S, Tinuper P, DaidoneR, et al. Neuropsychological, electroencephalogram and braincomputed tomography findings in motor neuron disease. Eur Neurol1989; 29: 115-20.
Goodin DS, Rowley HA, Olney RK. Magnetic resonance imagingin amyotrophic lateral sclerosis. Ann Neurol 1988; 23: 418-20.
Grant DA. Berg ED. Winconsin Card Sorting Test. Odessa (FL):Psychological Assessment Resources. 1990.
Hillel AD, Miller RM, Yorkston K, McDonald E. Norris FH,Konikow N. Amyotrophic lateral sclerosis severity scale.Neuroepidemiology 1989; 8: 142-50.
Hinke RM, Hu X, Stillman AE, Kim S-G, Merkle H, Salmi R,et al. Functional magnetic resonance imaging of Broca's area duringinternal speech. Neuroreport 1993; 4: 675-8.
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from

Frontal lobe activation in ALS 2119
Hudson AJ. Amyotrophic lateral sclerosis and its association withdementia, parkinsonism and other neurological disorders: a review.[Review]. Brain 1981; 104: 217-47.
Ishikawa K, Nagura H, Yokota T, Yamanouchi H. Signal loss inthe motor cortex on magnetic resonance images in amyotrophiclateral sclerosis. Ann Neurol 1993; 33: 218-22.
Iwasaki Y, Kinoshita M, Oceda K, Takamiya K, ShiojimaT. Cognitiveimpairment in amyotrophic lateral sclerosis and its relation to motordisabilities. Acta Neurol Scand 1990; 81: 141-3.
Jones-Gotman M, Milner B. Design fluency: the invention ofnonsense drawings after focal cortical lesions. Neuropsychologia1977; 15: 653-74.
Kato S, Hayashi H, Yagishita A. Involvement of the frontotemporallobe and limbic system in amyotrophic lateral sclerosis: as assessedby serial computed tomography and magnetic resonance imaging.J Neurol Sci 1993; 116: 52-8.
Kato S, Oda M, Hayashi H, Kawato A, Shimizu T. Participation ofthe limbic system and its associated areas in the dementia ofamyotrophic lateral sclerosis. J Neurol Sci 1994; 126: 62-9.
Kendrick D. Cognitive Tests for the Elderly. Windsor: NFER-Nelson, 1985.
Kew J, Leigh N. Dementia with motor neuron disease. In: RosserMN, editor. Unusual dementias. Bailliere's clinical neurology, Vol.1, No. 3. London: Bailhere Tindall, 1992: 611-26.
Kew JJM, Leigh PN. Unusual forms of dementia. In: Burns A,Levy R, editors. Dementia. London: Chapman and Hall, 1994:789-811.
Kew JJM, Leigh PN, Playford ED, Passingham RE, Goldstein LH,Frackowiak RSJ, et al. Cortical function in amyotrophic lateralsclerosis: a positron emission tomography study. Brain 1993a; 116:655-80.
Kew JJM, Goldstein LH, Leigh PN, Abrahams S, Cosgrave N,Passingham RE, et al. The relationship between abnormalities ofcognitive function and cerebral activation in amyotrophic lateralsclerosis: a neuropsychological and positron emission tomographystudy. Brain 1993b; 116: 1399^423.
Kiernan JA, Hudson AJ. Frontal lobe atrophy in motor neurondiseases. Brain 1994; 117: 747-57.
Leigh PN, Kew JJM, Goldstein LH, Brooks DJ. The cerebral lesionsin amyotrophic lateral sclerosis: new insights from pathology andfunctional brain imaging. In: Clifford Rose F, editor. Amyotrophiclateral sclerosis from Charcot to the present and into the future.London: Smith-Gordon, 1994: 191-209.
Ludolph AC, Langen KJ, Regard M, Herzog H, Kemper B, KuwertT, et al. Fronta] lobe function in amyotrophic lateral sclerosis: aneuropsychological and positron emission tomography study. ActaNeurol Scand 1992; 85: 81-9.
Luis ML, Hormigo A, Mauricio C, Alves MM, Serrao R. Magneticresonance imaging in motor neuron disease [see comments]. JNeurol 1990; 237: 471^1. Comment in: J Neurol 1992; 239: 112-13.
Mesulam MM. Large-scale neurocognitive networks and distributedprocessing for attention, language, and memory. [Review], AnnNeurol 1990; 28: 597-613.
Mesulam MM, Mufson EJ. The insula of Reil in man and monkey:architectonics, connectivity and function. In: Cerebral cortex,Peters A and Jones EG, editors. New York Press; 1985: 179-226.
Miceli G, Caltagirone C, Gainotti G, Masullo C, Silveri MC.Neuropsychological correlates of localized cerebral lesions in non-aphasic brain-damaged patients. J Clin Neuropsychol 1981; 3: 53-63.
Miller E. Verbal fluency as a function of a measure of verbalintelligence and in relation to different types of cerebral pathology.Br J Clin Psychol 1984; 23: 53-7.
Milner B. Effects of different brain lesions on card sorting. ArchNeurol 1963; 9: 90-100.
Milner B. Interhemispheric differences in the localization ofpsychological processes in man. [Review]. Br Med Bull 1971; 27:272-7.
Mitsuyama Y. Presenile dementia with motor neuron disease inJapan: clinico-pathological review of 26 cases. J Neurol NeurosurgPsychiatry 1984; 47: 953-9.
Moossy J, Martinez AJ, Hanin I, Rao G, Yonas H, Boiler F.Thalamic and subcortical gliosis with dementia. Arch Neurol 1987;44: 510-13.
Morita K, Kaiya H, Ikeda T, Namba M. Presenile dementia combinedwith amyotrophy: a review of 34 Japanese cases. [Review]. ArchGerontol Geriatr 1987; 6: 263-77.
Neary D, Snowden JS, Mann DMA, Northen B, Goulding PJ,Macdermott N. Frontal lobe dementia and motor neuron disease. JNeurol Neurosurg Psychiatry 1990; 53: 23-32.
Nelson HE, Willison JR. Restandardisation of the NART againstthe WAIS-R. Windsor NFER-Nelson, 1991.
Okamoto K, Hirai S, Yamazaki T, Sun XY, Nakazato Y. Newubiquitin-positive intraneuronal inclusions in the extra-motorcortices in patients with amyotrophic lateral sclerosis. Neurosci Lett1991; 129: 233-6.
Okamoto K, Murakami N, Kusaka H, Yoshida M, Hashizume Y,Nakazato Y, et al. Ubiquitin-positive transneural inclusions in theextramotor cortices of presenile dementia patients with motor neurondisease. J Neurol 1992; 239: 426-30.
Pandya DN, Barnes CL. Architecture and connections of the frontallobes. In: Perecman E, editor. The frontal lobes revisited. NewYork: IRBN Press, 1987: 41-71.
Paulesu E, Frith CD, Frackowiak RSJ. The neural correlates of theverbal component of working memory [see comments]. Nature1993; 362: 342-5. Comment in: Nature 1993; 363: 583—4.
Peavy GM, Herzog AG, Rubin NP, ' Mesulam M-M.Neuropsychological aspects of dementia of motor neuron disease:a report of two cases. Neurology 1992; 42: 1004-8.
Pendleton MG, Heaton RK, Lehman RAW, Hulihan D. Diagnosticutility of the Thurstone Word Fluency Test in neuropsychologicalevaluations. J Clin Neuropsychol 1982; 4: 307-17.
Petersen SE, Fox PT, Posner MI, Mintun M, Raichle ME. Positronemission tomographic studies of the cortical anatomy of single-word processing. Nature 1988; 331: 585-9.
Poloni M, Capitani E, Mazzini L, Ceroni M. Neuropsychological
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from
2120 S. Abrahams et al.
measures in amyotrophic lateral sclerosis and their relationship withCT scan-assessed cerebral atrophy. Acta Neurol Scand 1986; 74:257-60.
Robb RA, Hanson DP. A software system for interactive andquantitative visualization of multidimensional biomedical images.Australas Phys Eng Sci Med 1991; 14: 9-30.
Shallice T, Vallar G. In: Vallar G, Shallice T, editors,Neuropsychological impairments of short-term memory. Cambridge:Cambridge University Press, 1990: 11-53.
Smith MC. Nerve fibre degeneration in the brain in amyotrophiclateral sclerosis. J Neurol Neurosurg Psychiatry 1960; 23: 269-82.
Speedie LJ, Heilman KM. Amnesic disturbance following infarctionof the left dorsomedial nucleus of the thalamus. Neuropsychologia1982; 20: 597-604.
Speedie LJ, Heilman KM. Anterograde memory deficits forvisuospatial material after infarction of the right thalamus. ArchNeurol 1983; 40: 183-6.
Spinks TJ, Jones T, Gilardi MC, Heather JD. Physical performanceof the latest generation of commercial positron scanner. IEEE TransNucl Sci 1988; 35: 721-5.
Swash M, Leigh N. Criteria for diagnosis of familial amyotrophiclateral sclerosis. [Review]. Neuromuscul Disord 1992; 2: 7-9.
Talairach J, Tournoux P. Co-planar stereotaxic atlas of the humanbrain. Stuttgart: Thieme, 1988.
Talbot PR, Goulding PJ, Lloyd JJ, Snowden JS, Neary D, TestaHJ. Inter-relation between 'classic' motor neuron disease andfrontotemporal dementia: neuropsychological and single photonemission computed tomography study. J Neurol NeurosurgPsychiatry 1995; 58: 541-7.
Thurstone LL, Thurstone TG. Primary mental abilities. Chicago:Science Research Associates, 1962.
Walsh KW. Neuropsychology: a clinical approach. 3rd ed.Edinburgh: Churchill Livingstone, 1994.
Warburton E, Wise RJS, Price CJ, Weiller C, Hadar U, Ramsay S,et al. Studies wiuS positron emission tomography of noun and verbretrieval by normal subjects. Brain 1996; 119: 159-79.
Warrington EK. Recognition Memory Test. Windsor: NFER-Nelson, 1984.
Watson JDG, Myers R, Frackowiak RSK, Hajnal JV, Woods RP,Mazziotta JC, et al. Area V5 of the human brain: evidence from acombined study using positron emission tomography and magneticresonance imaging. Cereb Cortex 1993; 3: 79-94.
Wechsler D. Wechsler Memory Scale—Revised. San Antonio:Psychological Corporation, 1987.
Weinberger DR, Berman KF, Zee RF. Physiologic dysfunction ofdorsolateral prefrontal cortex in schizophrenia [see comments]. ArchGen Psychiatry 1986; 43: 114-24. Comment in: Arch Gen Psychiatry1991; 48: 282-3.
Wightman G, Anderson VER, Martin J, Swash M, Anderton BH,Neary D, et al. Hippocampal and neocortical ubiquitin-immunoreactive inclusions in amyotrophic lateral sclerosis withdementia. Neurosci Lett 1992; 139: 269-74.
Wikstrom J, Paetau A, Palo J, Sulkava R, Haltia M. Classicamyotrophic lateral sclerosis with dementia. Arch Neurol 1982; 39:681-3.
Wise R, Chollet F, Hadar U, Fnston K, Hoffner E, FrackowiakR. Distribution of cortical neural networks involved in wordcomprehension and word retrieval. Brain 1991; 114: 1803-17.
Woods RP, Cherry SR, Mazziotta JC. Rapid automated algorithmfor aligning and reslicing PET images. J Comput Assist Tomogr1992; 16: 620-33.
Woods RP, Mazziotta JC, Cherry SR. MRI-PET registration withautomated alogrithm. J Comput Assist Tomogr 1993; 17: 536-46.
World Federation of Neurology Research Group on Neuromusculardiseases. El Escorial World Federation of Neurology Criteria forthe diagnosis of ALS. J Neurol Sci 1994: 124(Suppl): 96-107.
Zatorre RJ, Evans AC, Meyer E, Gjedde A. Lateralization ofphonetic and pitch discrimination in speech processing. Science1992; 256: 846-9.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale.Acta Psychiatr Scand 1983; 67: 361-70.
Received August 14, 1996. Revised June 24, 1996.Accepted July 24, 1996
by guest on July 24, 2011brain.oxfordjournals.org
Dow
nloaded from
Copyright © 2022 FDOKUMEN




















