
The effect of age on frontal lobe related cognitive functions of unmedicated depressed patients
6
Brief report The effect of age on frontal lobe related cognitive functions of unmedicated depressed patients Yoram Braw a,b , Shai Aviram a , Yuval Bloch a,c , Yechiel Levkovitz a,c,d, ⁎ a The Emotion-Cognition Research Center, Shalvata Mental Health Care Center (affiliated with the Sackler Faculty of Medicine, Tel-Aviv University), Hod-Hasharon, Israel b Department of Behavioral Sciences, Ariel University Center of Samaria, Israel c Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel d Department of Psychiatry, Massachusetts General Hospital (affiliated with Harvard Medical School), Boston, Massachusetts, USA article info abstract Article history: Received 28 February 2010 Received in revised form 26 July 2010 Accepted 26 July 2010 Background: Aging is associated with a decline in frontal lobe related cognitive functioning of healthy subjects (i.e., executive functioning and higher-order cognition). Unipolar depression is associated with dysfunctions in similar cognitive domains — deficits that impact the functioning and quality of life of these patients. The effect of age on frontal lobe related cognitive functions of depressed patients, however, has not been adequately studied. The current study therefore assessed a wide age range of depressed patients and compared their frontal lobe related cognitive functions to that of matched healthy controls. Recruitment of unmedicated patients minimized the confounding effect of psychiatric medications. Method: Depressed patients and healthy controls were divided into three age groups (b 25, 25– 45, and 46–65 years of age) and matched in gender, age and education level (N total = 170). Cognition was assessed using the Cambridge Neuropsychological Test Automated Battery (CANTAB). Results: The depressed patients had deficits in cognitive planning/organization, working memory, and sustained attention compared to the healthy controls. Aging was associated with a decrease in frontal lobe related functioning. Except for working memory, no significant interactions were found between the age groups and the study group (depressed/healthy). Conclusions: Depressed patients are impaired in most domains of frontal lobe related cognitive functions. These deficits are already evident at an early age and persist in older age cohorts (despite an overall age related decline). These findings may help clarify the profile and course of cognitive deficits among depressed patients while providing tentative support for a developmental model of cognitive impairment in depression. © 2010 Elsevier B.V. All rights reserved. Keywords: Depression Age Cognition Executive functions Higher-order cognition 1. Introduction Healthy subjects show an age related decline in executive functioning (Jurado and Rosselli, 2007; van Hooren et al., 2007) as well as in higher-order cognitive functions (e.g., fluid intelligence; Bugg et al., 2006). These findings were interpreted to support the frontal lobe aging hypothesis, according to which this cognitive decline parallels changes in the frontal lobe and its related neural circuits (Rodriguez- Aranda and Sundet, 2006; West, 2000). Depression is characterized by cognitive impairments, with frontal lobe related cognitive functions prominent among them (Gualtieri et al., 2006; Nakano et al., 2008; Paelecke-Habermann et al., 2005). Earlier studies of depressed patients, however, investigated either a single age cohort (primarily of middle or old age) or aggregated different age cohorts together (see; Castaneda et al., 2008). As a consequence it is not clear Journal of Affective Disorders 129 (2011) 342–347 ⁎ Corresponding author. Department of Psychiatry, Massachusetts General Hospital, Harvard Medical School, 50 Staniford Street, Suite 401, Boston, MA 02114, USA. Tel.: +1 617 794 2505; fax: +1 617 726 7541. E-mail address: [email protected] (Y. Levkovitz). 0165-0327/$ – see front matter © 2010 Elsevier B.V. All rights reserved. doi:10.1016/j.jad.2010.07.032 Contents lists available at ScienceDirect Journal of Affective Disorders journal homepage: www.elsevier.com/locate/jad
Transcript of The effect of age on frontal lobe related cognitive functions of unmedicated depressed patients

Journal of Affective Disorders 129 (2011) 342–347
Contents lists available at ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r.com/ locate / j ad
Brief report
The effect of age on frontal lobe related cognitive functions of unmedicateddepressed patients
Yoram Braw a,b, Shai Aviram a, Yuval Bloch a,c, Yechiel Levkovitz a,c,d,⁎a The Emotion-Cognition Research Center, Shalvata Mental Health Care Center (affiliated with the Sackler Faculty of Medicine, Tel-Aviv University), Hod-Hasharon, Israelb Department of Behavioral Sciences, Ariel University Center of Samaria, Israelc Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israeld Department of Psychiatry, Massachusetts General Hospital (affiliated with Harvard Medical School), Boston, Massachusetts, USA
a r t i c l e i n f o
⁎ Corresponding author. Department of Psychiatry, MHospital, Harvard Medical School, 50 Staniford Street,02114, USA. Tel.: +1 617 794 2505; fax: +1 617 726
E-mail address: [email protected] (Y. Levkovitz).
0165-0327/$ – see front matter © 2010 Elsevier B.V.doi:10.1016/j.jad.2010.07.032
a b s t r a c t
Article history:Received 28 February 2010Received in revised form 26 July 2010Accepted 26 July 2010
Background: Aging is associated with a decline in frontal lobe related cognitive functioning ofhealthy subjects (i.e., executive functioning and higher-order cognition). Unipolar depressionis associated with dysfunctions in similar cognitive domains — deficits that impact thefunctioning and quality of life of these patients. The effect of age on frontal lobe relatedcognitive functions of depressed patients, however, has not been adequately studied. Thecurrent study therefore assessed a wide age range of depressed patients and compared theirfrontal lobe related cognitive functions to that of matched healthy controls. Recruitment ofunmedicated patients minimized the confounding effect of psychiatric medications.Method: Depressed patients and healthy controls were divided into three age groups (b25, 25–45, and 46–65 years of age) and matched in gender, age and education level (N total=170).Cognition was assessed using the Cambridge Neuropsychological Test Automated Battery(CANTAB).Results: The depressed patients had deficits in cognitive planning/organization, workingmemory, and sustained attention compared to the healthy controls. Aging was associated witha decrease in frontal lobe related functioning. Except for working memory, no significantinteractions were found between the age groups and the study group (depressed/healthy).Conclusions: Depressed patients are impaired in most domains of frontal lobe related cognitivefunctions. These deficits are already evident at an early age and persist in older age cohorts(despite an overall age related decline). These findings may help clarify the profile and courseof cognitive deficits among depressed patients while providing tentative support for adevelopmental model of cognitive impairment in depression.
© 2010 Elsevier B.V. All rights reserved.
Keywords:DepressionAgeCognitionExecutive functionsHigher-order cognition
1. Introduction
Healthy subjects show an age related decline in executivefunctioning (Jurado and Rosselli, 2007; van Hooren et al.,2007) as well as in higher-order cognitive functions (e.g.,fluid intelligence; Bugg et al., 2006). These findings were
assachusetts GeneraSuite 401, Boston, MA7541.
All rights reserved.
l
interpreted to support the frontal lobe aging hypothesis,according to which this cognitive decline parallels changesin the frontal lobe and its related neural circuits (Rodriguez-Aranda and Sundet, 2006; West, 2000). Depression ischaracterized by cognitive impairments, with frontal loberelated cognitive functions prominent among them (Gualtieriet al., 2006; Nakano et al., 2008; Paelecke-Habermann et al.,2005). Earlier studies of depressed patients, however,investigated either a single age cohort (primarily of middleor old age) or aggregated different age cohorts together (see;Castaneda et al., 2008). As a consequence it is not clear

343Y. Braw et al. / Journal of Affective Disorders 129 (2011) 342–347
whether aging is associated with a different cognitivetrajectory among depressed patients (compared to healthycontrols). The current study therefore assessed the frontallobe related cognitive functions (i.e., cognitive planning/organization, cognitive flexibility and response inhibition) ofunmedicated depressed patients from different age cohorts.Sustained attention and workingmemory were also assessed.These cognitive functions can be conceptualized as executivefunctions or as higher-order cognitive functions that supportexecutive functioning (Baddeley, 1992; McCabe et al., 2010;Silver and Feldman, 2005). The sole inclusion of unmedicatedpatients prevented the possible confounding effect of psychi-atricmedications and is in keepingwith the need for studies ofmedication-free depressed patients (see; Reppermund et al.,2009). A cognitive assessment was conducted using theCambridge Neuropsychological Test Automated Battery, pre-viously used to study the cognitive functioning of a wide agerange of healthy subjects (De Luca et al., 2003; Luciana, 2003).We hypothesized that the depressed patients would exhibitcognitive deficits compared to the matched controls and thatthese impairments would already be discernible at an earlyage. These hypotheses are in line with earlier findings thatutilized the CANTAB to study depressed patients duringadolescence (Matthews et al., 2008), adulthood (Reppermundet al., 2009; Weiland-Fiedler et al., 2004) and old age (Beatset al., 1996). In light of inconsistencies in findings, we did nothave a priori hypotheses with regard to specific cognitivedomains in which the depressed patients would exhibitimpairments (see; Rogers et al., 2004). No hypothesis wasmade with regard to possible interactions between age andstudy group on the subjects' cognitive functioning. It should benoted that all the cognitive functions that were assessed in thecurrent study involved not only the frontal lobes, but also acomplex network of frontal-cortical and subcortical circuitries(Alvarez and Emory, 2006). The term “frontal lobe relatedcognitive functions” is therefore used to conveniently delineatethe assessment of both executive functions and supportinghigher-order cognitive functions.
2. Method
Retrospective data of depressed outpatients and healthycontrols (N=122 and N=129, respectively) was extractedfrom the archives of the Shalvata Mental Health Center. Aspart of their original studies, depressed patients wereinterviewed by a trained clinician who performed theStructured Clinical Interview for DSM-IV (SCID; Spitzer et al.,1992), assessed depressive symptoms and scored the ClinicalGlobal Impression scale (CGI; Haro et al., 2003). The patientscompleted the Beck Depression Inventory (BDI-II). Healthycontrols underwent a clinical interview and completed theBrief Symptom Inventory (BSI; Derogatis and Melisaratos,1983). Next, the subjects performed the following CANTABtasks in a semi-randomized fashion: (a) Tower of London (ToL;CANTAB's Stockings of Cambridge): assessed cognitive planningand organization. (b) Intra-Dimensional–Extra-Dimensionalshift (ID/ED): a computerized analog of the Wisconsin CardSorting Task (Heaton et al., 1993) that assessed cognitiveflexibility. (c) Rapid Visual Information Processing (RVIP): A′(ability to detect the target sequence) assessed sustainedattention. ‘Probability of false alarms’ (responding to a non-
target sequence) was tentatively interpreted as representingresponse inhibition. (d) Spatial Working Memory (SWM):assessed working memory. All subjects signed an informedconsent form and were free to withdraw at any time fromtheir original studies. The study received local InstitutionalReview Board (IRB) committee approval.
Inclusion criteria were: (a) b65 years of age. (b) Fordepressed patients: DSM-IV diagnosis of depression, no changein psychiatric diagnosis ≤six months following cognitiveassessment, depressed at the time of assessment [HDRS-17total score N14 for subjects older than 18 years, or CDRS-R totalscore≥40 for subjects younger than 18 years (Hamilton, 1960;Poznanski and Mokros, 1995)], and unmedicated during themonth prior to cognitive assessment. (b) For healthy controls:no life-time axis-I psychopathology. Exclusion criteria were:any significant, unstable, or untreated medical illness (with anemphasis on neurological disorders), mental retardation orborderline intelligence (b80 full scale I.Q., according to thepatients' medical records or attendance in special educationprograms), and drug/alcohol abuse or dependency problem.
Next, the depressed patients and healthy controls werematched in gender, age (±2 years) and education level(±1 year). Twenty six depressed patients and 35 healthycontrols did not have a matched subject, and their data wasdiscarded. Data on the cognitive assessments of eightdepressed patients was incomplete and was thereforediscarded (as well as the data of their matched controls).Overall, the data of 170 subjects was utilized and divided intothree age groups: (a) ‘Adolescence and young adulthood’ (YA)defined as age b25 years (N=30). (b) ‘Middle adulthood’(MA) defined as 25–45 years (N=30). (c) ‘Late adulthood’(LA) defined as 46–65 years (N=25). We defined age groupsin the same way Tombaugh (2004) defined them, whilecombining the older age groups in order to increase the samplesize of each age group. Differences between the groups inparametric variables were assessed using analyses of variance(ANOVA) with between-subject factors of ‘group’ (depressed/healthy) and ‘age’ (YA/MA/LA). Analyses of clinical variableswere conducted using ANOVAs with a between-subject factorof ‘age’. Chi-square analyses were conducted separately foreach age group for non-parametric variables. Hierarchicallinear regressions assessed possible predictors of depressedpatients' cognitive functioning. Cognitive variables inwhich thedepressedpatients haddeficitswereusedasoutcomevariables.Possible predictors were entered in three blocks: demographicvariables, disorder-related variables (illness duration), anddepression severity. Similar regression analyses were con-ducted for the healthy controls (note that the clinical variableswere not applicable to the healthy controls). A Bonferronicorrection was employed for tasks in which more than onemeasure was assessed (ANOVA analyses: pb .0167 for Tower ofLondon task, pb .025 for RVIP and ID/ED; Regression analyses:pb0.025 set for overall significance in the Tower of Londontask). This correction was made in order to keep the totalchance of erroneously reporting a difference below .05α(Bonferroni, 1936).
3. Results
Significant effects were evident in the following CANTABtasks: (a) Tower of London (cognitive planning/organization):
344 Y. Braw et al. / Journal of Affective Disorders 129 (2011) 342–347
depressedpatients solved fewer problems inminimummovesand were slower to solve the task after moving the first ballthan healthy controls were (subsequent thinking time in 5-move problems) (pb .001 for both main-effects). An ‘age’main-effect was also evident (pb .01 for the number ofproblems solved in minimum moves and pb .001 for subse-quent thinking time in 5-move problems). Follow-up analysesindicated that LA solved fewer problems in minimum movesthan did YA, and LA had slower thinking after moving the firstball than did both YA and MA. (b) SWM (working memory):there were ‘group’, ‘age’ and ‘group’× ‘age’ effects for thenumber of errors committed (pb .05, pb .001, and pb .05,respectively). Follow-up analyses indicated that an age effectwas evident only among the healthy controls (pb .001); LAmade more errors than both YA and MA. Depressed patientsmademore errors than thehealthy controls in the YA age group(pb .01) with a near-significant effect in the MA age group(depressed patients tended tomakemore errors than controls;pb .1). (c) RVIP (attention): depressed patients had a lowerprobability of detecting targets (A′) in the task compared to thehealthy controls (‘group’ main-effect; pb .001). There was an‘age’ main-effect (pb .01); LA had a lower probability ofdetecting a target than YA and MA.
In the first stage of three regression analyses, the demo-graphic variables significantly predicted the cognitive func-tioning of the depressed patients [ToL problem solved inminimum moves; ToL subsequent thinking time in 5-moveproblems; SWM between errors; pb .05 for all analyses]. Theyshowed a near-significant effect in the fourth regression(RVIP A′; p=.052). In all analyses, age was the strongestpredictor among the demographic variables, while illnessduration did not add a significant contribution to theexplained variance (beyond the demographic variables).Depression severity (BDI-II) added a significant contributionto the explained variance of only one outcome measure, theToL number of problem solved in minimum moves (pb .05).The regression model for ToL subsequent thinking time in 5-move problems was non-significant in the final stage of theregression (all other analyses were significant in the laststage). The regression analyses for the healthy controlsindicated that the demographic variables significantly pre-dicted the cognitive functioning of the healthy controls (notpresented). Age was found to be the strongest predictor in allanalyses (for example, RVIP A′; β=−.449, pb .001). SeeTables 1 and 2.
4. Discussion
Depressed patients had deficits in most of the cognitivedomains that were assessed (see also; Gualtieri et al., 2006;Paelecke-Habermann et al., 2005). The depressed patientshad deficits in cognitive planning and organization, solvingfewer problems in minimum moves in the Tower of Londontask, and requiring more time to complete the task aftermoving the first ball. They also had deficits in the domains ofworkingmemory and sustained attention. From a perspectiveof daily functioning, these deficits are likely to interfere withtheir ability to carry out multi-step activities, conductcomplex mental manipulations, and sustain a high level offunctioning over time. The findings however cannot rule outthe possibility that the depressed patients have a broader,
non-specific profile of cognitive impairment (Reppermund etal., 2009). This possibility is supported by a closer inspectionof the findings, suggesting that additional cognitive deficitsmay have gone undetected. For example, cognitive inflexi-bility may have been masked due to the use of CANTAB's ID/ED task. While studies found differences between depressedand healthy subjects when utilizing the Wisconsin CardSorting Task (WCST), an established task of cognitiveflexibility (Elderkin-Thompson et al., 2006; Fossati et al.,2002), these findings were not replicated by most studiesemploying the ID/ED task (including studies utilizing bothtasks; Grant et al., 2001).
The current study indicates an age related decline infrontal lobe related cognitive functions, evident in bothdepressed and healthy controls (as found earlier; De Luca etal., 2003). The lack of significant group×age interactions inmost of the cognitive domains indicates that the deficitsdisplayed by the depressed patients were manifested at anearly age and continued throughout adulthood (i.e., theywere evident regardless of the age related cognitive declineseen in both groups). The findings tentatively support aneurodevelopmental model of cognitive impairment indepression. Such a model suggests that after the onset ofpsychopathology there are no further changes in cognitionbeyond those that occur with normal aging. These conclu-sions are strengthened by the regression analyses that foundillness duration to have a limited predictive power on thecognitive functioning of the depressed patients. It wassomewhat unexpected to find no significant differences inworking memory capacity between the different age groupsof depressed patients. This finding may be due to a “flooreffect” in CANTAB's SWM task (i.e., it was not sensitiveenough to detect an age related decrease in functioning).While this finding necessitates further research, it does notseem to alter the overall conclusions of the current study.
It can be argued that a cross-sectional study design canonly serve as an indirect, confirmatory approach to assesschanges in cognitive functioning over time (with a longitu-dinal approach being better suited to directly explore thisissue). The basis for this argument is the possibility of a biasedsample selection (i.e., differences in characteristics betweenage sub-groups). Indeed, certain differences – which may actas confounders (e.g., education level) – can be found betweenthe age groups in our analyses. We attempted to eliminate atleast some of these possible confounders (e.g., participantswere given practice trials with the computer tasks in order toreduce age cohort – versus true age – effects, which mayresult from certain age groups having less experience withperforming computer tasks). It should also be noted that alongitudinal research design entails limitations as well,including short follow-up periods, effects of practice, lowerpsychopathology scores at follow-up, drop-out at re-test,changes in medication regimens, etc. It seems therefore thatboth approaches have shortcomings and should be regardedas complementary methods. Additional, prospective longitu-dinal studies will be needed in order to assess the possibledifferential contributions of age, illness duration, and otherrelated variables (i.e., investigating developmental and neu-rodegenerative models of cognitive impairment in depres-sion). These studies should take into consideration severaladditional limitations of the current study; first, only non-
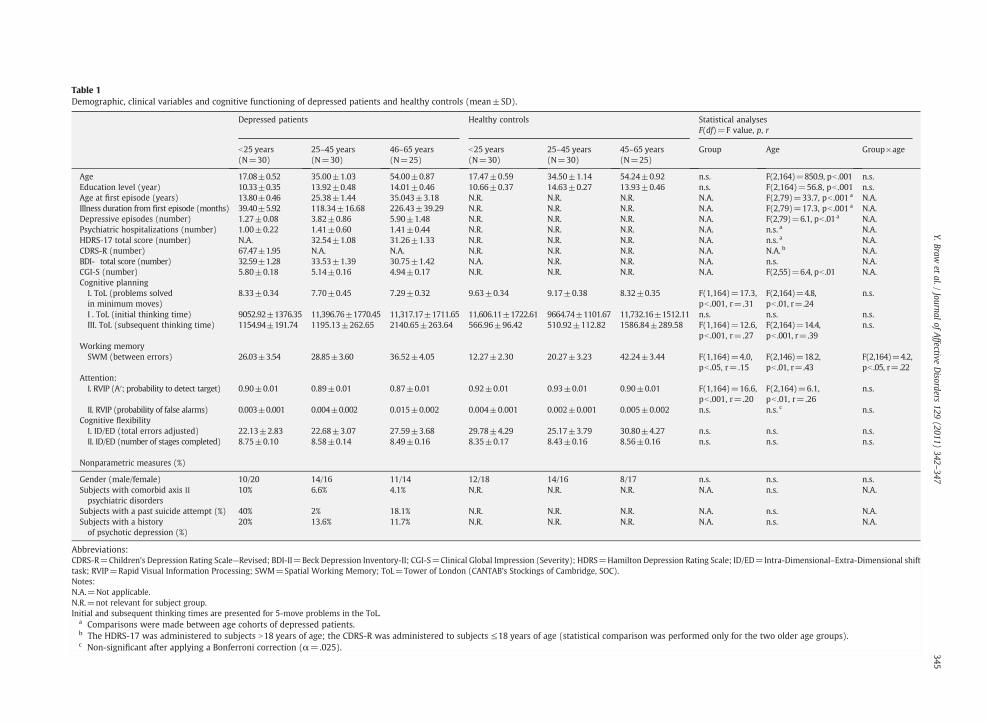
Table 1Demographic, clinical variables and cognitive functioning of depressed patients and healthy controls (mean±SD).
Depressed patients Healthy controls Statistical analysesF(df)=F value, p, r
b25 years(N=30)
25–45 years(N=30)
46–65 years(N=25)
b25 years(N=30)
25–45 years(N=30)
45–65 years(N=25)
Group Age Group×age
Age 17.08±0.52 35.00±1.03 54.00±0.87 17.47±0.59 34.50±1.14 54.24±0.92 n.s. F(2,164)=850.9, pb .001 n.s.Education level (year) 10.33±0.35 13.92±0.48 14.01±0.46 10.66±0.37 14.63±0.27 13.93±0.46 n.s. F(2,164)=56.8, pb .001 n.s.Age at first episode (years) 13.80±0.46 25.38±1.44 35.043±3.18 N.R. N.R. N.R. N.A. F(2,79)=33.7, pb .001 a N.A.Illness duration from first episode (months) 39.40±5.92 118.34±16.68 226.43±39.29 N.R. N.R. N.R. N.A. F(2,79)=17.3, pb .001 a N.A.Depressive episodes (number) 1.27±0.08 3.82±0.86 5.90±1.48 N.R. N.R. N.R. N.A. F(2,79)=6.1, pb .01a N.A.Psychiatric hospitalizations (number) 1.00±0.22 1.41±0.60 1.41±0.44 N.R. N.R. N.R. N.A. n.s. a N.A.HDRS-17 total score (number) N.A. 32.54±1.08 31.26±1.33 N.R. N.R. N.R. N.A. n.s. a N.A.CDRS-R (number) 67.47±1.95 N.A. N.A. N.R. N.R. N.R. N.A. N.A. b N.A.BDI- total score (number) 32.59±1.28 33.53±1.39 30.75±1.42 N.A. N.R. N.R. N.A. n.s. N.A.CGI-S (number) 5.80±0.18 5.14±0.16 4.94±0.17 N.R. N.R. N.R. N.A. F(2,55)=6.4, pb .01 N.A.Cognitive planningI. ToL (problems solvedin minimum moves)
8.33±0.34 7.70±0.45 7.29±0.32 9.63±0.34 9.17±0.38 8.32±0.35 F(1,164)=17.3,pb .001, r=.31
F(2,164)=4.8,pb .01, r=.24
n.s.
I . ToL (initial thinking time) 9052.92±1376.35 11,396.76±1770.45 11,317.17±1711.65 11,606.11±1722.61 9664.74±1101.67 11,732.16±1512.11 n.s. n.s. n.s.III. ToL (subsequent thinking time) 1154.94±191.74 1195.13±262.65 2140.65±263.64 566.96±96.42 510.92±112.82 1586.84±289.58 F(1,164)=12.6,
pb .001, r=.27F(2,164)=14.4,pb .001, r=.39
n.s.
Working memorySWM (between errors) 26.03±3.54 28.85±3.60 36.52±4.05 12.27±2.30 20.27±3.23 42.24±3.44 F(1,164)=4.0,
pb .05, r=.15F(2,146)=18.2,pb .01, r=.43
F(2,164)=4.2,pb .05, r=.22
Attention:I. RVIP (A′; probability to detect target) 0.90±0.01 0.89±0.01 0.87±0.01 0.92±0.01 0.93±0.01 0.90±0.01 F(1,164)=16.6,
pb .001, r=.20F(2,164)=6.1,pb .01, r=.26
n.s.
II. RVIP (probability of false alarms) 0.003±0.001 0.004±0.002 0.015±0.002 0.004±0.001 0.002±0.001 0.005±0.002 n.s. n.s. c n.s.Cognitive flexibilityI. ID/ED (total errors adjusted) 22.13±2.83 22.68±3.07 27.59±3.68 29.78±4.29 25.17±3.79 30.80±4.27 n.s. n.s. n.s.II. ID/ED (number of stages completed) 8.75±0.10 8.58±0.14 8.49±0.16 8.35±0.17 8.43±0.16 8.56±0.16 n.s. n.s. n.s.
Nonparametric measures (%)
Gender (male/female) 10/20 14/16 11/14 12/18 14/16 8/17 n.s. n.s. n.s.Subjects with comorbid axis IIpsychiatric disorders
10% 6.6% 4.1% N.R. N.R. N.R. N.A. n.s. N.A.
Subjects with a past suicide attempt (%) 40% 2% 18.1% N.R. N.R. N.R. N.A. n.s. N.A.Subjects with a historyof psychotic depression (%)
20% 13.6% 11.7% N.R. N.R. N.R. N.A. n.s. N.A.
Abbreviations:CDRS-R=Children's Depression Rating Scale—Revised; BDI-ΙΙ=Beck Depression Inventory-ΙΙ; CGI-S=Clinical Global Impression (Severity); HDRS=Hamilton Depression Rating Scale; ID/ED=Intra-Dimensional–Extra-Dimensional shifttask; RVIP=Rapid Visual Information Processing; SWM=Spatial Working Memory; ToL=Tower of London (CANTAB's Stockings of Cambridge, SOC).Notes:N.A.=Not applicable.N.R.=not relevant for subject group.Initial and subsequent thinking times are presented for 5-move problems in the ToL.
a Comparisons were made between age cohorts of depressed patients.b The HDRS-17 was administered to subjects N18 years of age; the CDRS-R was administered to subjects ≤18 years of age (statistical comparison was performed only for the two older age groups).c Non-significant after applying a Bonferroni correction (α=.025). 345
Y.Brawet
al./Journal
ofAffective
Disorders
129(2011)
342–347
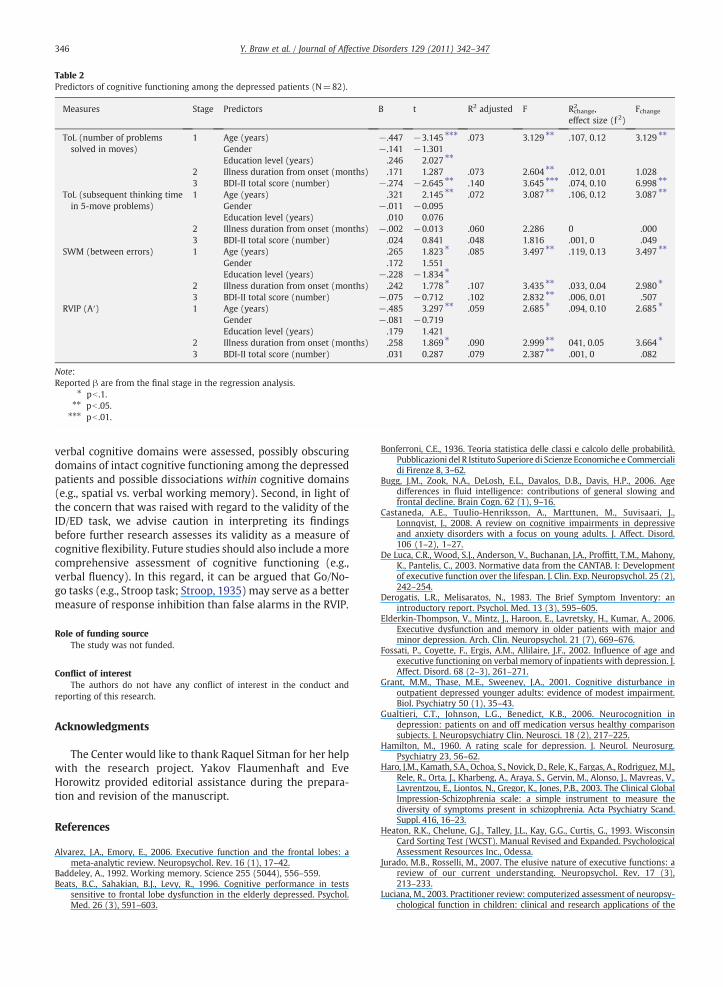
Table 2Predictors of cognitive functioning among the depressed patients (N=82).
Measures Stage Predictors B t R2 adjusted F R2change,
effect size (f 2)Fchange
ToL (number of problemssolved in moves)
1 Age (years) −.447 −3.145 ⁎⁎⁎ .073 3.129 ⁎⁎ .107, 0.12 3.129 ⁎⁎
Gender −.141 −1.301Education level (years) .246 2.027 ⁎⁎
2 Illness duration from onset (months) .171 1.287 .073 2.604 ⁎⁎ .012, 0.01 1.0283 BDI-II total score (number) −.274 −2.645 ⁎⁎ .140 3.645 ⁎⁎⁎ .074, 0.10 6.998 ⁎⁎
ToL (subsequent thinking timein 5-move problems)
1 Age (years) .321 2.145 ⁎⁎ .072 3.087 ⁎⁎ .106, 0.12 3.087 ⁎⁎
Gender −.011 −0.095Education level (years) .010 0.076
2 Illness duration from onset (months) −.002 −0.013 .060 2.286 0 .0003 BDI-II total score (number) .024 0.841 .048 1.816 .001, 0 .049
SWM (between errors) 1 Age (years) .265 1.823 ⁎ .085 3.497 ⁎⁎ .119, 0.13 3.497 ⁎⁎
Gender .172 1.551Education level (years) −.228 −1.834 ⁎
2 Illness duration from onset (months) .242 1.778 ⁎ .107 3.435 ⁎⁎ .033, 0.04 2.980 ⁎
3 BDI-II total score (number) −.075 −0.712 .102 2.832 ⁎⁎ .006, 0.01 .507RVIP (A′) 1 Age (years) −.485 3.297 ⁎⁎ .059 2.685 ⁎ .094, 0.10 2.685 ⁎
Gender −.081 −0.719Education level (years) .179 1.421
2 Illness duration from onset (months) .258 1.869 ⁎ .090 2.999 ⁎⁎ 041, 0.05 3.664 ⁎
3 BDI-II total score (number) .031 0.287 .079 2.387 ⁎⁎ .001, 0 .082
Note:Reported β are from the final stage in the regression analysis.
⁎ pb .1.⁎⁎ pb .05.⁎⁎⁎ pb .01.
346 Y. Braw et al. / Journal of Affective Disorders 129 (2011) 342–347
verbal cognitive domains were assessed, possibly obscuringdomains of intact cognitive functioning among the depressedpatients and possible dissociations within cognitive domains(e.g., spatial vs. verbal working memory). Second, in light ofthe concern that was raised with regard to the validity of theID/ED task, we advise caution in interpreting its findingsbefore further research assesses its validity as a measure ofcognitive flexibility. Future studies should also include amorecomprehensive assessment of cognitive functioning (e.g.,verbal fluency). In this regard, it can be argued that Go/No-go tasks (e.g., Stroop task; Stroop, 1935) may serve as a bettermeasure of response inhibition than false alarms in the RVIP.
Role of funding sourceThe study was not funded.
Conflict of interestThe authors do not have any conflict of interest in the conduct and
reporting of this research.
Acknowledgments
The Center would like to thank Raquel Sitman for her helpwith the research project. Yakov Flaumenhaft and EveHorowitz provided editorial assistance during the prepara-tion and revision of the manuscript.
References
Alvarez, J.A., Emory, E., 2006. Executive function and the frontal lobes: ameta-analytic review. Neuropsychol. Rev. 16 (1), 17–42.
Baddeley, A., 1992. Working memory. Science 255 (5044), 556–559.Beats, B.C., Sahakian, B.J., Levy, R., 1996. Cognitive performance in tests
sensitive to frontal lobe dysfunction in the elderly depressed. Psychol.Med. 26 (3), 591–603.
Bonferroni, C.E., 1936. Teoria statistica delle classi e calcolo delle probabilità.Pubblicazioni del R Istituto Superiore di Scienze Economiche e Commercialidi Firenze 8, 3–62.
Bugg, J.M., Zook, N.A., DeLosh, E.L., Davalos, D.B., Davis, H.P., 2006. Agedifferences in fluid intelligence: contributions of general slowing andfrontal decline. Brain Cogn. 62 (1), 9–16.
Castaneda, A.E., Tuulio-Henriksson, A., Marttunen, M., Suvisaari, J.,Lonnqvist, J., 2008. A review on cognitive impairments in depressiveand anxiety disorders with a focus on young adults. J. Affect. Disord.106 (1–2), 1–27.
De Luca, C.R., Wood, S.J., Anderson, V., Buchanan, J.A., Proffitt, T.M., Mahony,K., Pantelis, C., 2003. Normative data from the CANTAB. I: Developmentof executive function over the lifespan. J. Clin. Exp. Neuropsychol. 25 (2),242–254.
Derogatis, L.R., Melisaratos, N., 1983. The Brief Symptom Inventory: anintroductory report. Psychol. Med. 13 (3), 595–605.
Elderkin-Thompson, V., Mintz, J., Haroon, E., Lavretsky, H., Kumar, A., 2006.Executive dysfunction and memory in older patients with major andminor depression. Arch. Clin. Neuropsychol. 21 (7), 669–676.
Fossati, P., Coyette, F., Ergis, A.M., Allilaire, J.F., 2002. Influence of age andexecutive functioning on verbal memory of inpatients with depression. J.Affect. Disord. 68 (2–3), 261–271.
Grant, M.M., Thase, M.E., Sweeney, J.A., 2001. Cognitive disturbance inoutpatient depressed younger adults: evidence of modest impairment.Biol. Psychiatry 50 (1), 35–43.
Gualtieri, C.T., Johnson, L.G., Benedict, K.B., 2006. Neurocognition indepression: patients on and off medication versus healthy comparisonsubjects. J. Neuropsychiatry Clin. Neurosci. 18 (2), 217–225.
Hamilton, M., 1960. A rating scale for depression. J. Neurol. Neurosurg.Psychiatry 23, 56–62.
Haro, J.M., Kamath, S.A., Ochoa, S., Novick, D., Rele, K., Fargas, A., Rodriguez, M.J.,Rele, R., Orta, J., Kharbeng, A., Araya, S., Gervin, M., Alonso, J., Mavreas, V.,Lavrentzou, E., Liontos, N., Gregor, K., Jones, P.B., 2003. The Clinical GlobalImpression-Schizophrenia scale: a simple instrument to measure thediversity of symptoms present in schizophrenia. Acta Psychiatry Scand.Suppl. 416, 16–23.
Heaton, R.K., Chelune, G.J., Talley, J.L., Kay, G.G., Curtis, G., 1993. WisconsinCard Sorting Test (WCST). Manual Revised and Expanded. PsychologicalAssessment Resources Inc., Odessa.
Jurado, M.B., Rosselli, M., 2007. The elusive nature of executive functions: areview of our current understanding. Neuropsychol. Rev. 17 (3),213–233.
Luciana, M., 2003. Practitioner review: computerized assessment of neuropsy-chological function in children: clinical and research applications of the

347Y. Braw et al. / Journal of Affective Disorders 129 (2011) 342–347
Cambridge Neuropsychological Testing Automated Battery (CANTAB). J.Child. Psychol. Psychiatry 44 (5), 649–663.
Matthews, K., Coghill, D., Rhodes, S., 2008. Neuropsychological functioning indepressed adolescent girls. J. Affect. Disord. 111 (1), 113–118.
McCabe, D.P., Roediger, H.L., McDaniel, M.A., Balota, D.A., Hambrick, D.Z.,2010. The relationship between workingmemory capacity and executivefunctioning: evidence for a common executive attention construct.Neuropsychology 24 (2), 222–243.
Nakano, Y., Baba, H., Maeshima, H., Kitajima, A., Sakai, Y., Baba, K., Suzuki, T.,Mimura, M., Arai, H., 2008. Executive dysfunction in medicated, remittedstate of major depression. J. Affect. Disord. 111 (1), 46–51.
Paelecke-Habermann, Y., Pohl, J., Leplow, B., 2005. Attention and executivefunctions in remitted major depression patients. J. Affect. Disord. 89 (1–3), 125–135.
Poznanski, E.O., Mokros, H.B., 1995. Children's Depression Rating Scale,Revised (CDRS-R) Manual Los Angeles, Calif: Western PsychologicalServices.
Reppermund, S., Ising, M., Lucae, S., Zihl, J., 2009. Cognitive impairment inunipolar depression is persistent and non-specific: further evidence forthe final common pathway disorder hypothesis. Psychol. Med. 39 (4),603–614.
Rodriguez-Aranda, C., Sundet, K., 2006. The frontal hypothesis of cognitiveaging: factor structure and age effects on four frontal tests amonghealthy individuals. J. Genet. Psychol. 167 (3), 269–287.
Rogers, M.A., Kasai, K., Koji, M., Fukuda, R., Iwanami, A., Nakagome, K.,Fukuda, M., Kato, N., 2004. Executive and prefrontal dysfunction inunipolar depression: a review of neuropsychological and imagingevidence. Neurosci. Res. 50 (1), 1–11.
Silver, H., Feldman, P., 2005. Evidence for sustained attention and workingmemory in schizophrenia sharing a common mechanism. J. Neuropsy-chiatry Clin. Neurosci. 17 (3), 391–398.
Spitzer, R.L., Williams, J.B., Gibbon, M., First, M.B., 1992. The StructuredClinical Interview for DSM-III-R (SCID). I: History, rationale, anddescription. Arch. Gen. Psychiatry 49 (8), 624–629.
Stroop, J.R., 1935. Studies of interference in serial verbal reactions. J. Exp.Psychol. Gen. 18, 643–662.
Tombaugh, T.N., 2004. Trail Making Test A and B: normative data stratified byage and education. Arch. Clin. Neuropsychol. 19 (2), 203–214.
van Hooren, S.A., Valentijn, A.M., Bosma, H., Ponds, R.W., van Boxtel, M.P.,Jolles, J., 2007. Cognitive functioning in healthy older adults aged 64–81:a cohort study into the effects of age, sex, and education. Neuropsychol.Dev. Cogn. B Aging Neuropsychol. Cogn. 14 (1), 40–54.
Weiland-Fiedler, P., Erickson, K., Waldeck, T., Luckenbaugh, D.A., Pike, D.,Bonne, O., Charney, D.S., Neumeister, A., 2004. Evidence for continuingneuropsychological impairments in depression. J. Affect. Disord. 82 (2),253–258.
West, R., 2000. In defense of the frontal lobe hypothesis of cognitive aging. JInt Neuropsychol Soc, 6(6), 727–729; discussion 730.




















