From theoretical model to practical use: an example of knowledge translation
12
DISCUSSION PAPER From theoretical model to practical use: an example of knowledge translation Ida Torunn Bjørk, Kirsten Lomborg, Carsten Munch Nielsen, Grethe Brynildsen, Anne-Marie Skovsgaard Frederiksen, Karin Larsen, Inger A ˚ se Reierson, Irene Sommer & Britta Stenholt Accepted for publication 22 December 2012 Correspondence to I.T. Bjørk: e-mail: [email protected] Ida Torunn Bjørk MNS PhD RN Professor Department of Nursing Science, Institute of Health and Society, University of Oslo, Norway Kirsten Lomborg MNS PhD RN Associate Professor Department of Public Health, Aarhus University, Denmark Carsten Munch Nielsen MEd RN Curriculum Coordinator VIA University College, Aarhus, Denmark Grethe Brynildsen MNS RN Assistant Professor Lovisenberg Diaconal University College, Oslo, Norway Anne-Marie Skovsgaard Frederiksen MLP RN Lecturer VIA University College, Aarhus, Denmark Karin Larsen MLP RN Educational Coordinator Department of Endocrinology and Internal Medicine, Aarhus University Hospital, Denmark BJØRK I.T., LOMBORG K., NIELSEN C.M., BRYNILDSEN G., FREDERIKSEN A.-M.S., LARSEN K., REIERSON I.A ˚ ., SOMMER I. & STENHOLT B. (2013) From theoretical model to practical use: an example of knowledge translation. Journal of Advanced Nursing 00(0), 000–000. doi: 10.1111/jan.12091 Abstract Aim. To present a case of knowledge translation in nursing education and practice and discusses mechanisms relevant to bringing knowledge into action. Background. The process of knowledge translation aspires to close the gap between theory and practice. Knowledge translation is a cyclic process involving both the creation and application of knowledge in several phases. The case presented in this paper is the translation of the Model of Practical Skill Performance into education and practice. Advantages and problems with the use of this model and its adaptation and tailoring to local contexts illustrate the cyclic and iterative process of knowledge translation. Discussion. The cultivation of a three-sided relationship between researchers, educators, and clinical nurses was a major asset in driving the process of knowledge translation. The knowledge translation process gained momentum by replacing passive diffusion strategies with interaction and teamwork between stakeholders. The use of knowledge creates feedback that might have consequences for the refinement and tailoring of that same knowledge itself. With end-users in mind, several heuristics were used by the research group to increase clarity of the model and to tailor the implementation of knowledge to the users. Implications for nursing. This article illustrates the need for enduring collaboration between stakeholders to promote the process of knowledge translation. Translation of research knowledge into practice is a time-consuming process that is enhanced when appropriate support is given by leaders in the involved facilities. Conclusion. Knowledge translation is a time-consuming and collaborative endeavour. On the basis of our experience we advocate the implementation and use of a conceptual framework for the entire process of knowledge translation. More descriptions of knowledge translation in the nursing discipline are needed to inspire and advise in this process. © 2013 Blackwell Publishing Ltd 1 continued on page 2 JAN JOURNAL OF ADVANCED NURSING
Transcript of From theoretical model to practical use: an example of knowledge translation

DISCUSSION PAPER
From theoretical model to practical use: an example of knowledge
translation
Ida Torunn Bjørk, Kirsten Lomborg, Carsten Munch Nielsen, Grethe Brynildsen,
Anne-Marie Skovsgaard Frederiksen, Karin Larsen, Inger Ase Reierson, Irene Sommer &
Britta Stenholt
Accepted for publication 22 December 2012
Correspondence to I.T. Bjørk:
e-mail: [email protected]
Ida Torunn Bjørk MNS PhD RN
Professor
Department of Nursing Science,
Institute of Health and Society,
University of Oslo, Norway
Kirsten Lomborg MNS PhD RN
Associate Professor
Department of Public Health,
Aarhus University, Denmark
Carsten Munch Nielsen MEd RN
Curriculum Coordinator
VIA University College, Aarhus,
Denmark
Grethe Brynildsen MNS RN
Assistant Professor
Lovisenberg Diaconal
University College, Oslo, Norway
Anne-Marie Skovsgaard Frederiksen MLP
RN
Lecturer
VIA University College, Aarhus, Denmark
Karin Larsen MLP RN
Educational Coordinator
Department of Endocrinology and Internal
Medicine, Aarhus University Hospital,
Denmark
B JØRK I .T . , LOMBORG K . , N IEL SEN C .M . , BRYN ILDSEN G . , FREDER IKSEN
A . -M . S . , LARSEN K . , RE I ERSON I . A . , SOMMER I . & STENHOLT B . ( 2 0 1 3 )
From theoretical model to practical use: an example of knowledge translation.
Journal of Advanced Nursing 00(0), 000–000. doi: 10.1111/jan.12091
AbstractAim. To present a case of knowledge translation in nursing education and practice
and discusses mechanisms relevant to bringing knowledge into action.
Background. The process of knowledge translation aspires to close the gap
between theory and practice. Knowledge translation is a cyclic process involving
both the creation and application of knowledge in several phases. The case
presented in this paper is the translation of the Model of Practical Skill
Performance into education and practice. Advantages and problems with the use
of this model and its adaptation and tailoring to local contexts illustrate the
cyclic and iterative process of knowledge translation.
Discussion. The cultivation of a three-sided relationship between researchers,
educators, and clinical nurses was a major asset in driving the process of
knowledge translation. The knowledge translation process gained momentum by
replacing passive diffusion strategies with interaction and teamwork between
stakeholders. The use of knowledge creates feedback that might have
consequences for the refinement and tailoring of that same knowledge itself. With
end-users in mind, several heuristics were used by the research group to increase
clarity of the model and to tailor the implementation of knowledge to the users.
Implications for nursing. This article illustrates the need for enduring
collaboration between stakeholders to promote the process of knowledge
translation. Translation of research knowledge into practice is a time-consuming
process that is enhanced when appropriate support is given by leaders in the
involved facilities.
Conclusion. Knowledge translation is a time-consuming and collaborative
endeavour. On the basis of our experience we advocate the implementation and
use of a conceptual framework for the entire process of knowledge translation.
More descriptions of knowledge translation in the nursing discipline are needed
to inspire and advise in this process.
© 2013 Blackwell Publishing Ltd 1
continued on page 2
JAN JOURNAL OF ADVANCED NURSING

Inger Ase Reierson MNS RN
Assistant Professor
Telemark University College, Porsgrunn,
Norway
Irene Sommer MCN RN
Education and Development Nurse
Department of Cardiology, Aarhus
University Hospital, Skejby, Denmark
Britta Stenholt MNS RN
Lecturer
VIA University College, Silkeborg, Denmark
Introduction
Nursing is a practice discipline and one major purpose of
research in nursing is to develop knowledge that can be
applied in nursing practice or in the education of nurses.
This simple statement refers to a large and problematic gap
between science and practice that is evident in all the
healthcare disciplines. Research knowledge is produced and
published at an increasing rate, but changes in clinical prac-
tice and education are quite slow (Kitson 2008, Benner
et al. 2010).
Several terms are used in the literature to characterize
the efforts to move scientific results or other kinds of
knowledge into practical use. As literature on such efforts
is produced in many different disciplines, concepts are used
differently and with great variations in their definitions
(Thompson et al. 2006). An often-cited definition published
by the Canadian Institutes of Health Research (CIHR)
(2010) states that knowledge translation is: ‘A dynamic
and iterative process that includes synthesis, dissemination,
exchange and ethically sound application of knowledge
[…] within a complex system of interactions between
researchers and knowledge users which may vary in inten-
sity, complexity and level of engagement depending on the
nature of the research and the findings as well as the needs
of the particular knowledge user’. Although debates in
nursing focus on epistemological aspects of knowledge, dis-
cussions on the mechanisms underlying knowledge transfer
processes are almost non-existent in the nursing literature
(Aita et al. 2007). More attention is therefore urgently
needed.
In this article, we present a case of knowledge translation
in a Nordic context. The endeavour was not planned
according to a knowledge translation model from the out-
set. We cannot therefore present our translation efforts as a
theoretically structured case of knowledge translation. Our
purpose is to demonstrate the translation of the theoretical
and normative Model of Practical Skill Performance (Bjørk
& Kirkevold 2000) into nursing practice and education and
to use an existing knowledge translation framework to dis-
cuss our experiences of mechanisms relevant to knowledge
translation. We first exemplify the translation of the model
into nursing practice and education and then discuss how
interaction and teamwork between stakeholders from
research, education, and practice in nursing drove the pro-
cess of knowledge translation. Most articles that discuss
knowledge translation focus on moving knowledge into
clinical practice. We found that the issues are quite similar
in efforts to translate new knowledge into the educational
setting in nursing. Drawing on our experiences, we high-
light the value of ‘three-sided thinking’ to expedite and
strengthen translational processes and results. Knowledge
translation may involve knowledge for conceptual use,
direct use, or policy use (Ward et al. 2009). In our efforts
to move the Model of Practical Skill Performance into edu-
cation and practice, the target was both conceptual and
practical use.
Background
Moving knowledge into practice is complex. It is a process
with many facets (Rycroft-Malone 2010) and a great vari-
ety of terminology, frameworks and models have been used
to represent this process (Estabrooks et al. 2006, Graham
and Tetroe 2007, Mitton et al. 2007, Sudsawad 2007,
Pentland et al. 2011). In the USA, several models and pro-
grammes were launched during the 1970s to support
nurses’ research utilization in clinical settings. Initiatives
such as the Stetler/Marram model (Stetler & Marram
1976), later adjusted by Stetler and named the Stetler
(2001) model and Conduct and Utilization of Research in
Nursing (CURN) (Horsley et al. 1983) were developed to
enhance nurses’ use of research knowledge in practice. A
more recent framework for the implementation of research,
Promoting Action on Research Implementation in Health
Services, was first published by Kitson et al. (1998) and
further developed by Rycroft-Malone and colleagues
(Rycroft-Malone et al. 2002, Rycroft-Malone 2004).
Promoting Action on Research Implementation in Health
Services is a conceptual model that presents research imple-
mentation as the interplay between three core elements: the
level and nature of the evidence used, the context or envi-
ronment where the research is to be placed, and the method
by which the implementation process is to be facilitated
(Sudsawad 2007). The framework is focused on the imple-
mentation process of knowledge, not the creation of knowl-
2 © 2013 Blackwell Publishing Ltd
I.T. Bjørk et al.

edge. It is not a model to guide actual implementation. It
delineates the core elements so that researchers and knowl-
edge users can work together towards creating the best
environment for structured change and development in
practice (Rycroft-Malone 2004).
In this article, we use the term ‘knowledge translation’.
Knowledge can mean more than research knowledge. The
CIHR makes it clear that their definition of knowledge
translation involves interactions between researchers, who
predominantly produce research knowledge and users. The
CIHR refers to users as key stakeholders who have the
intention to improve both health outcomes and the health-
care system and state that the interaction in knowledge
translation is collaborative and two-way. The gap between
science and practice has recently been addressed by the
European Union through a presidency status report promot-
ing The European Research Area (ERA) vision for 2020
(Council of the European Union 2008). This report suggests
that the views on collaboration in knowledge translation
must be expanded by including education as a corner stone.
Special attention is given to the so-called Triangle of
Knowledge, which articulates a three-sided relationship in
knowledge translation between research, practice, and edu-
cation. The report also suggests that education has an equal
and parallel role to research and practice in the effort to
promote the use of knowledge. The report states that ‘A
wide range of activities are taking place in individual parts
of this triangle without systematic consideration of interac-
tions with the remaining two, which leads to non system-
atic policies’ (p. 13). It also suggests that ‘a better
functioning knowledge triangle has the potential to reduce
bureaucracy and increase transparency in transforming
knowledge into innovative products and services’ (p. 14).
We interpret this part of the ERA vision to mean that
knowledge translation will be strengthened by expanding
the two-way collaboration promoted by CIHR to include
education in the knowledge-to-action equation. Involving
education and the clinical learning milieu in this equation
may ultimately result in the education of students who are
qualified in knowledge-to-action activities and thereby
better qualified as stakeholders when they move into
practice as professionals.
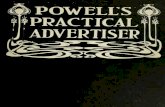
Knowledge translation is identified as either a linear,
cyclic, or dynamic multidirectional process (Ward et al.
2009). A cyclic knowledge-to-action framework was
published by Graham et al. (2006) (Figure 1) on the basis
of a review of planned-action theories and frameworks. As
opposed to many other frameworks for knowledge transla-
tion, this framework has been tested. It was used as a
model for planning and evaluating knowledge translation
strategies for developing a mentorship strategy in contin-
uing education (Straus et al. 2008). The framework
described by Graham et al. (2006) depicts the process of
knowledge translation as ‘an iterative, dynamic and
complex process concerning the creation and application
(action cycle) of knowledge’ (Straus et al. 2009, p. 166).
The process of knowledge creation contains three phases
(Figure 1): (1) knowledge inquiry, representing primary
research; (2) knowledge synthesis, representing the aggrega-
tion of existing knowledge; and (3) knowledge tools and
Monitorknowledge
use
Sustainknowledge
Tailo
ring
know
ledg
e
use
Evaluateoutcomes
Adaptknowledge
to local context
Assess barriers/supports to
knowledge use
Select, tailor,implement
Interventions
Identify problem
Identify, Review,Select knowledge
Products/tools
Synthesis
Knowledge inquiry
KNOWLEDGE CREATION
Figure 1 The Knowledge-to-Action
Process by Graham et al. (2006), used
with permission. The Alliance for Contin-
uing Medical Education, The Society for
Academic Continuing Medical Education,
and The Association for Hospital
Medical Education.
© 2013 Blackwell Publishing Ltd 3
JAN: DISCUSSION PAPER Knowledge translation

products, representing the distillation of concise and user-
friendly formats of knowledge, such as guidelines or deci-
sion aids. Researchers involved in the process of knowledge
creation can tailor their activities in response to the prob-
lems identified by knowledge users (Graham et al. 2006).
The process of knowledge application includes seven phases
(Figure 1), from identifying a problem and identifying,
reviewing and selecting knowledge (phase 1), to sustaining
knowledge use (phase 7). These phases are based on com-
mon aspects in theories of planned action for change in
healthcare systems and groups (Graham & Tetroe 2007).
Graham et al. (2006) present these phases as a circle. They
emphasize that the phases can influence each other or be
influenced by the knowledge creation phases in a dynamic
way and thereby move back and forth between phases. This
dynamic movement depends on the cultivation of relation-
ships between stakeholders as a necessary premise in devel-
oping a common understanding of knowledge translation
and actual exchange of knowledge. In the following, we
will present the motivation to develop the Model of Practi-
cal Skill Performance and give a short description of its
intention and significance.
Knowledge creation: developing the Model of Practical
Skill Performance
The Model of Practical Skill Performance was developed as
part of a doctoral dissertation and published internationally
in three articles (Bjørk 1999, Bjørk & Kirkevold 1999,
2000). Sources of data that were combined to inform the
development of the model were both theoretical and empiri-
cal. The impetus to develop this model was based on the
repeatedly communicated worries in the literature and in
practice, about lack of proficiency in practical nursing skills
in newly graduated nurses. The model aspired to assert
practical skills in nursing as complex actions in contrast
with former renditions of practical nursing skills as simple
and technically focused motor or psychomotor skills. This
complexity would in turn have consequences for skill teach-
ing and learning, both in the skills centre and in clinical
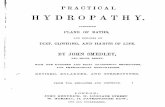
placements. The model is generic (for practical nursing
skills) and normative, and suggests that six categories or
elements comprise and express what must be realized in a
good practical skill performance (Figure 2).
The model is visualized as a circle symbolizing unity,
wholeness, and integration. The stippled lines between the
categories suggest their interrelatedness. There is no hierar-
chical relationship between the layers, nor is any one layer
more important than the others, because all categories
should be present when a practical skill is performed. The
arrows symbolize that caring behaviour is fundamental to
acting professionally as a nurse and therefore permeates all
elements of practical skill performance (for more details
see, e.g. Bjørk & Kirkevold 2000).
Moving the model into research, practice, and education
Since first published in scientific journals at the turn of the
21st century, the model has spread to the Nordic audience
by what Thompson et al. (2006, p. 692) refer to as ‘passive
diffusion’. Through articles, books, and book chapters
aimed at nursing practice and education (Bjørk 2002, 2003,
2006, Bjørk & Breievne 2005), the model has been pre-
sented and discussed, aiming to influence nurses’, students’,
and nursing educators’ views of the constitution of practical
skills in nursing. In a more active transfer pathway, the
development and relevant use of the model have been
taught in classes with masters students and presented at
national and international conferences. It has also been the
topic of seminars with nurse educators in Norway and Den-
mark. Such activities are common among most scholars,
but there is no guarantee of use merely because information
is timely, relevant and objective and disseminated to the
right people in usable form (Rich 1979). Diffusion of
knowledge by researchers is often termed the ‘push forces’
of knowledge translation. This means that researchers ‘push
information, hoping…that someone, somewhere, will find
the fruits of our well-intended work ripe for consumption’
(Dearing & Kreuter 2010, p,. S102). The ‘pull forces’, on
the other hand, denote what potential adopters want. These
adopters may be individuals, teams, or organizations, and
they pull what they value, prefer, or pay attention to
(Dearing & Kreuter 2010).
The result of these push forces was that some Norwegian
and Danish doctoral students, masters students, and nursing
education faculties, quite independently of one another,
found that the model addressed analytical and practical
problems related to teaching and learning of practical skills
in nursing. Lomborg (2004), in her doctoral dissertation,
used the categories in the model as an inspiration in her
analysis of assisted personal body care in patients with
chronic obstructive pulmonary disease. The findings were
organized under the headings Caring conduct, Accuracy,
Fluency (and pace), and Integration. Two masters students
used the model. One as a tool to analyse the development
of students’ skills in assisting with personal body care
during clinical placement in nursing homes (Brynildsen
2007), and the other as a standard to evaluate the quality
of students’ practical skill learning in the skills centre
(Blig�ard 2007).
4 © 2013 Blackwell Publishing Ltd
I.T. Bjørk et al.

Through independent initiatives of the nursing faculty,
the model was included in the curriculum at a university
college in Norway in 2002 and at two nursing education
sites in one university college in Denmark in 2006. In these
plans, the model was presented as a norm for well-
performed practical skills and students were encouraged to
use the model during practical skill learning in the skills
centre and during clinical studies. The formalization of the
model in the curriculum inspired nurse educators at the
Norwegian university college to study students’ acquisition
of substance, sequence, and accuracy in the skills centre
during skill learning (Solli & Reierson 2006).
The faculty at the university college in Denmark had
launched a study investigating the development in practical
skills during an 8-week clinical placement period. They com-
pared the progress of students in dedicated educational units
with students in ordinary nursing units (Nielsen et al. 2005).
The researchers had come across the model while searching
for literature and decided to use it as a tool to guide analysis
of videos of the students’ skill development. Struggling with
several methodological questions pertaining to the use of the
model, they contacted the creator of the model. This was in
2004, so the diffusion period had lasted four years. At the
same time, an educational nurse working in the clinical set-
ting in a Danish hospital contacted the faculty group and
instigated a project to incorporate the model as a teaching
tool for clinical nurses in their supervision of student nurses
during clinical placements in medical units (Larsen & Nielsen
2006). One spin-off from this study was educational material
in the form of pocketsize laminated pamphlets presenting the
model. Another spin- off was a theoretical article in a Danish
nursing journal presenting and discussing the model as a rele-
vant tool for supervision and self-evaluation during practical
skill learning in the clinical setting (Nielsen et al. 2007,
2009). Skovsgaard et al. (2008) studied the relevance of
using nursing homes as clinical placements. They used the
model as an analytical tool to gauge whether students man-
aged to develop their practical skill performance sufficiently
at this type of placement.
This overview of projects shows that the model has been
used in hospitals, nursing homes, skills centres, and as a nor-
mative basis in educational curricula. Although also used as a
tool in analysis of empirical data, the model’s use in actual
education and practice is the focus in the rest of this article.
Substance
&
Sequence
Accuracy
Integration
Fluency
Caring comportment
© Ida Torunn Bjørk 1999
Model of Practical Skill Performance
Substance refers to the inclusion of relevant content in the form of movement steps, instruction and information.
Sequence reflects if movement steps, instruction andinformation come in a logical order.
Accuracy refers to exactness in each movementstep and the correctness of instruction and information included. E.g. opening bandages andequipment without contaminating the contens, giving the correct information about the purpose of the ambulation, or giving precise instructions on how to get out of bed.
Fluency is when each element of performance give an impression of ease and smoothness, whenthey seem ”finished” and without hesitation.
Integration reflects ability to harmonize and time theparallel aspects of an action such as movement steps, physical support and verbal interaction. Integration alsoincludes being attentive to what the patient in total needs whiletaking care of the specifics of the ongoing action.
Caring comportment relates to how the nurse createsan atmosphere that is respectful, accepting and encouraging.It includes concern of the whole person by relating to the patients’feelings and reactions to the instrumental steps of the action, and to the total experience of being a patient. Caring permeates all the elements of performance.
Figure 2 The Model of Practical Skill Performance.
© 2013 Blackwell Publishing Ltd 5
JAN: DISCUSSION PAPER Knowledge translation

Advantages and challenges in the use of the model
Experiences common to users of the model was that it gave
an overview of elements involved in practical skills in
nursing, functioned as a tool for supervision and evaluation
during practical skill performance and learning and used a
common, specific language that replaced former more vague
terms such as routine and handiness (Fransson 2009). A com-
mon experience was also that by using the model in discus-
sions, both students and nurses became more attuned to the
quality of performance than to the number of skills practised.
The categories in the model were also a starting point for
delving deeper into specifics of performance and stimulating
students to transfer theoretical and practical knowledge
across contexts and different nursing procedures.
Some challenges also emerged. Each category in the model
was defined and exemplified. However, masters students,
nurses, faculty and baccalaureate nursing students experi-
enced difficulties in specifying aspects of their actions in the
categories, often unable to decide between categories. The
category of ‘integration’ was especially difficult. Being able to
integrate a specific skill into the patient’s situation relies on
the ability to theorize and analyse one’s own actions during
the activity itself (Fransson 2009) and this is certainly difficult
for inexperienced students. To remedy this, the Danish fac-
ulty suggested adding two categories (Nielsen et al. 2007). In
retrospect, this was seen as an interpretation and reorganiza-
tion that undermined the theoretical consistency and the
common understanding of the model.
Adapting and tailoring the model to local contexts
While the model was being tried out in different settings
and for different purposes, in 2006, the creator of the
model gathered the people involved into the research group
Research in Nursing Skills (RiNS). The group immediately
organized their work through twice-yearly 3-day seminars.
The aim of the research group is defined on their homepage
as: ‘To develop a comprehensive understanding of practical
skills in nursing and how these skills are learned. By means
of systematic research and developmental projects we
propose to gain insight and develop knowledge that can
play a role in strengthening the performance of practical
skills in nursing. This will contribute to the delivery of
hands-on nursing at a high professional level to patients
and clients in need of nursing’ (www.rins.dk).
The problems with the model resulted in a communal
effort to further develop the model. To overcome language
and cultural barriers, the concepts in the model were pre-
cisely defined and translations into all languages concerned
were made. Educational materials and illustrative examples
from clinical practice were developed. In several workshops
during 2008–2009, the research group worked through
models of different practical skills in nursing to confirm the
appropriateness of the original six categories of the model.
They discussed ideas for development, read literature on
the development of models, and invited a researcher experi-
enced in the use of economic models to elaborate on the
development of models. Finally, the group developed a
more detailed instrumental supplement to guide students,
teachers, and nurses in the supervision, formative evalua-
tion, and self-evaluation of practical skill performance
(Figure 3). This is a supplement to – and not a replacement
for – the model. Definitions of categories are more precise
in the instrumental supplement (Figure 3) than in the
original model (Figure 2); aspects that denote quality in
performance are specified in relation to the defined
categories.
Implementing the instrumental supplement and
evaluating its use
The instrumental supplement of the model is now presented
on the RiNS website www.rins.dk in English, Danish, and
Norwegian. It has been incorporated into the curriculum
plans at the two university colleges together with the original
model and used in new projects in both countries. Members
of the research group have involved other educators at the
university colleges in action-research studies. The aims are to
improve teaching and learning at the skill centres by active
incorporation of the instrumental supplement of the model
during teaching and supervision and to supervise the
students while they use it during planning, self-study, and
self-evaluation of learning. Baseline and follow-up data were
gathered using video recordings. The primary investigators
collected detailed minutes of meetings and written logs and
plans developed in the action groups. Several members of
the research group are collaborating with supervisors and
teachers to use the model during clinical placements in hos-
pitals and nursing homes. At present, these implementation
efforts are being evaluated through focus group interviews,
written logs and surveys. Data are presently being analysed.
Questions to be answered are related to the participants
understanding of underlying values of the model and the
concepts used to describe quality performance, ease of use of
the instrumental supplement and other tools developed by
the research group, and barriers and facilitators to their use
in education and practice. These questions are related to
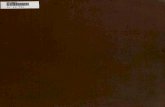
both conceptual and direct use of knowledge. To facilitate
the reader’s understanding of our knowledge translation
6 © 2013 Blackwell Publishing Ltd
I.T. Bjørk et al.

activities described above, we show our progression in
relation to the Knowledge-to-Action Process described by
Graham et al. (2006) (Figure 4).
Discussion
A major drive to knowledge translation is the potential and
need for improvement in clinical care (Wallin 2009). The
efforts to improve knowledge translation described in this
article were driven by the conviction of several people that
practical skill learning can and should be enhanced in both
the educational and clinical setting. At the outset, no theory
or model of knowledge translation was used to guide the
diffusion of the Model of Practical Skill Performance into
practice and education. The diffusion activities described in
this article are best portrayed as a ‘natural’ consequence of
perceiving one’s own work as important for nursing and
trying to disseminate this knowledge out into the world.
Although the many projects designed to use the model are
examples of efforts in knowledge translation, it is fair to say
that use of the model really first took off through the com-
bined efforts of the members in the research group RiNS.
The problem that needed addressing – ‘How to improve
practical skill-learning in nursing students’ – was already
Instrumental supplement
Model of Practical Skill Performance © RiNS 2009
Definition of categories in the model Characteristics of quality performance
SUBSTANCE AND SEQUENCE are the core aspects of a practical skill. Necessary steps in the skill are included and performed in a logical order
Substance and sequences are determined on the basis of content in clinical guidelines, professional standards and principles. Substance and sequence is adapted to the patient and the situation where the skill is being performed
ACCURACY refers to exactness of each movement step, instruction and information. Accuracy is important in order to ensure security of patient, nurse and environment
Accuracy implies to act: - correctly - precisely
Accuracy implies to inform and instruct: - what is necessary and sufficient - distinctly - understandably
FLUENCY signifies that tempo and rhythm is adjusted to both the patient and the type of practical skill being performed and that the practical skill is performed with smoothness
Fluency implies to act, inform and instruct: - without hesitancy - without unnecessary breaks - with ease
INTEGRATION signifies that all parallel aspects within the practical skill are harmonized.
Integration also implies that the skill as such is adjusted to the patient’s current condition and situation.
Integration implies to: - time and coordinate the elements of
action
Integration related to adjustment implies to: - be attentive - have an overview - be flexible
CARING COMPORTMENT signifies to create an atmosphere where the patient’s dignity is upheld, self-determination is ensured according to the patient’s current condition and situation and well-being is warranted
Caring comportment implies to: - acknowledge - show respect - ensure patient participation - be empathic - use appropriate touch - be engaged - use appropriate communication - work aesthetically
Figure 3 Instrumental supplement of the Model of Practical Skill Performance.
© 2013 Blackwell Publishing Ltd 7
JAN: DISCUSSION PAPER Knowledge translation

acknowledged by the group members. All members brought
with them experiences of the different ways they had tried
to solve this problem. According to Corcoran (2006), the
process of knowledge translation requires a multilevel
approach that involves prolonged interactions with a range
of individuals. By organizing the work in the research group
in a seminar format, we promoted extended interactions
among stakeholders representing all sides of the ‘knowledge
triangle’ (Council of the European Union 2008).
The primary research and systematic aggregation of
knowledge required to develop the Model of Practical Skill
Performance were done by one researcher before the
research group was established. However, the necessary
process of producing knowledge tools and tailoring the
developed model for use in practice and education occurred
as an iterative process over several years. In addition to
members of the research group, it involved students, teach-
ers, and nurses who reacted to and commented on the
model when using it or being supervised by it. This might
indicate that the knowledge we put into action was prema-
ture. It might also highlight the unfinished state of theory
and show that the use of knowledge creates feedback that
Knowledge creation and tailoring
Doctoral work resulting in the original Model of
Practical Skill Performance
Tailoring knowledge through cooperation with
stakeholders
1. Identify problem and review knowledge
• Problem of qualifying nursing students in practical skill acknowledged by educators, researchers and students
2. Adapt knowledge to local context
• Foundation of RiNS • Refinement of The Model
• Development and validation of a supplement
• Development of heuristic devices
3. Assess barriers to knowledge use
• Translation from English into Nowegian and Danish
• Examples provided in articles and folders to promote understanding
4. Select, tailor and implement interventions
• Implementation in skills centres and clinical practice
• Involvement of students, teachers and clinical supervisors
5. Monitor knowledge use
• Local monitoring as part of the defined projects
6. Evaluate outcomes
• Process and utcome evaluation of using the model in on-going studies
7. Sustain knowledge use
• To be addressed in ongoing and future evaluation
Figure 4 Activities in translating the Model of Practical Skill Performance illustrated with the phases of the Knowledge-to-Action Process
by Graham et al. (2006). The arrows symbolize the iterative process between knowledge application and knowledge tailoring.
8 © 2013 Blackwell Publishing Ltd
I.T. Bjørk et al.

might impinge on the refinement and tailoring of that same
knowledge itself. This back-and-forth process in the
development of appropriate knowledge illustrates the cyclic
nature of knowledge translation as described by Graham
et al. (2006).
The collaboration between researchers, educators, and
clinical nurses has been a major asset in the knowledge
translation endeavour. We think that our collaboration is
an example of the relevance of thinking in a ‘three-sided’
manner about knowledge translation (Council of the Euro-
pean Union 2008). In effect, education is both an end-user
of the model and acts as a co-researcher in knowledge
translation targeted at the clinical setting. The knowledge
triangle implies three equal partners in knowledge transla-
tion. Our experience is that the often-illustrated progres-
sion of knowledge translation as a linear process – with
knowledge being ‘moved’ by the researcher into clinical
practice – is far too simple. It does not match the reality of
our experience where, in fact, the active actions of end-
users, i.e. clinical nurses and educators, instigated the pro-
cess of active collaboration with the researcher in translat-
ing the model into practice.
The model was originally developed and presented in
research journals in the English language. The end-users of
the model in our knowledge translation efforts were
Norwegian and Danish nursing students and their teachers
and nurses in the clinical setting, not international fellow
researchers. As it is imperative to analyse the needs of end
users to inform the implementation planning process
(Graham & Tetroe 2007), we saw the necessity to address
barriers to knowledge use among our stakeholders. Barriers
to knowledge use in nursing have been extensively exam-
ined (see, e.g. Hutchinson & Johnston 2004) and lack of
readability and conceptual clarity in the research literature
are common barriers. Several heuristics were used by the
research group to increase the clarity of the model and to
tailor the implementation of knowledge to the users. We
also made sure that the language used in the Norwegian
and Danish versions of the model and the subsequent
instrumental supplement was properly validated.
Both push and pull strategies were used in our efforts to
move the model into education and practice. These are con-
trasting strategies brought about by cultural differences.
Roux et al. (2006) suggest that researchers should involve
end-users in the knowledge creation process to ensure that
the knowledge they develop will be received with more
enthusiasm. This may not always be possible when the
knowledge developed is the result of an unstructured
inquiry into underresearched areas and not the answer to a
recognized problem. We experienced that the push efforts
by the creator of the model were very important because
they managed to sensitize interested parties to the fact that
the theory developed could be of benefit to them in solving
problems they faced. We also experienced that the pull
forces came strongly into play when prolonged social inter-
action (Williams et al. 2008) was possible between
researchers, educators, and educational nurses in the RiNS
group. These pull forces have clearly contributed to the
knowledge-tailoring efforts during the knowledge transla-
tion process. The members of RiNS brought in valuable
experiences from students’, nurses’, teachers’, and their
own use of the model. Research into knowledge translation
is demanding and time-consuming (Rycraft-Malone 2004).
A major help in this work has been the financial support
and time provided by educational and research institutions.
Nursing facilities that support collaboration across national
borders and publication efforts have also been helpful.
The implementation process of knowledge translation
efforts must be examined (Wallin 2009). The different
What is already known about this topic
● Research knowledge is produced and published at an
increasing rate, but changes in clinical practice and
education are quite slow.
● Discussions on the mechanisms underlying knowledge
transfer processes are almost non-existent in the nurs-
ing literature.
● Passive diffusion of knowledge is no guarantee that it
will be used.
What this paper adds
● Three-sided collaboration that includes educators,
researchers, and clinical nurses is a major asset in
knowledge translation.
● A multilevel approach with prolonged interactions
between all stakeholders is necessary to gain momen-
tum in a knowledge-to-action process.
● A cyclic and not linear knowledge-to-action frame-
work, matched the actual process of knowledge trans-
lation.
Implications for practice and/or policy
● A theoretical framework of knowledge translation
should be used from the outset when knowledge trans-
lation projects are planned.
● More descriptions of knowledge translation efforts
should be published in the nursing literature.
© 2013 Blackwell Publishing Ltd 9
JAN: DISCUSSION PAPER Knowledge translation

studies published so far by members of the RiNS group
only touch on this process. We acknowledge the need to
investigate this process in detail and have chosen action-
research approaches including video-recorded observa-
tions, focus group interviews with stakeholders, and ques-
tionnaire surveys to gauge the implementation process in
our ongoing studies. By evaluating our efforts in knowl-
edge translation, we found that the phases of the cyclic
knowledge-to-action model (Graham & Tetroe 2007)
actually matched the collaborative efforts of the RiNS
members quite well. Whilst this is a very pleasing finding,
we regret that we did not actively discuss and choose a
knowledge translation framework from the outset. A
more structured approach to our translation efforts might
have reduced the resources we expended on the ‘complex,
messy, and demanding’ (Rycraft-Malone 2004) task it has
been to translate the model into education and practice.
We agree with Estabrooks et al. (2006) who suggest that
finding a fit between the context where knowledge trans-
lation is aimed and theory that can underpin these efforts
is important for knowledge translation initiatives to suc-
ceed.
Implications for nursing
This article illustrates that enduring collaboration between
stakeholders promotes the process of knowledge transla-
tion. Translation of research knowledge into practice is a
time-consuming process that is enhanced when appropriate
support is given by leaders in the involved facilities.
Limitations
This article has described and discussed how a theoretical
model in nursing has been moved into practice and
education in the Nordic countries. We acknowledge that
the scope of this endeavour may be viewed as small, but as
an example of the knowledge-to-action process, it may still
inspire and illuminate the challenges inherent in moving
research into practice.
Conclusion
We described a case of knowledge translation in a Nordic
context in this article. Although the case presented might
be viewed as a small-scale translation endeavour, it involves
many of the central phases described in a cyclic knowledge-
to-action process. A lesson to be learnt from our process is
that passive – and even active – diffusion activities are
limited in their effect. The combined effort of stakeholders
in research, clinical practice, and education in prolonged
interaction and teamwork was a necessary condition for the
knowledge translation process. More descriptions of knowl-
edge translation in the nursing discipline are needed and to
document these properly, a recognized knowledge transla-
tion framework must be implemented at the inception of
such research.
Funding
No funding for this work.
Conflict of interest
No conflict of interest has been declared by the authors.
Author contributions
All authors have agreed on the final version and meet at
least one of the following criteria [recommended by the
ICMJE (http://www.icmje.org/ethical_1author.html)]:
● substantial contributions to conception and design, acqui-
sition of data, or analysis and interpretation of data;
● drafting the article or revising it critically for important
intellectual content.
References
Aita M., Richer M.-C. & H�eon M. (2007) Illuminating the
processes of knowledge transfer in nursing. Worldviews on
Evidence-Based Nursing 4(3), 146–155.
Benner P., Sutphen M., Leonard V. & Day L. (2010) Educating
Nurses: A Call for Radical Transformation. Jossey-Bass, San
Francisco, CA.
Bjørk I.T. (1999) Practical skill development in new nurses.
Nursing Inquiry 6(1), 34–47.
Bjørk I.T. (2002) Kroppen i møtet mellom pasient og sykepleier
[The body in encounters between patient and nurse]. In Møte
mellom pasient og sykepleier [Encounters Between Patient and
Nurse] (Bjørk I.T., Helseth S. & Nortvedt F., eds), Gyldendal
Akademisk, Oslo, Norway, pp. 223–236 (Norwegian).
Bjørk I.T. (2003) �A lære praktiske ferdigheter i sykepleie [Learning
practical skills in nursing]. In �A lære i praksis [Learning in
Clinical Practice] (Bjørk I.T. & Bjerknes M.S., eds), Univer-
sitetsforlaget, Oslo, Norway, pp. 88–109 (Norwegian).
Bjørk I.T. (2006) Nyutdannede sykepleieres manglende praktiske
sykepleieferdigheter [New nurses’ lack of practical skills in
nursing]. Klinisk Sygepleje 20(4), 23–30 (Norwegian).
Bjørk I.T. & Breievne G. (2005) Kropp og velvære i sykepleien
[Body and well-being in Nursing]. In Grunnleggende sykepleie,
Bind 1 [Fundamental Nursing,Volume 1] (Kristoffersen N.J.,
Nortvedt , F. & Skaug E-A., eds), Gyldendal Akademisk, Oslo,
Norway, pp.106–136 (Norwegian).
10 © 2013 Blackwell Publishing Ltd
I.T. Bjørk et al.

Bjørk I.T. & Kirkevold M. (1999) Issues in nurses’ practical skill
development in the clinical setting. Journal of Nursing Care
Quality 14(1), 72–84.
Bjørk I.T. & Kirkevold M. (2000) From simplicity to complexity:
developing a model of practical skill performance. Journal of
Clinical Nursing 9(4), 620–631.
Blig�ard D. (2007) Formativ evaluering i det tredje læringsrum -
færdighedslaboratoriet. En kulturpsykologisk undersøgelse
[Formative evaluation in the third learning environment – the
skills centre. A cultural-psychological study]. Master’s thesis, The
Pedagogical University of Denmark, �Arhus, Denmark (Danish).
Brynildsen G. (2007) ‘Ikke bare enkle prosedyrer’. Læring og
utvikling av praktiske ferdigheter i en naturlig setting [‘Not just
simple procedures’. Learning and development of practical skills
in a natural setting]. Master’s thesis, Institute of Nursing and
Health Sciences, University of Oslo, Norway (Norwegian).
Canadian Institutes of Health Research (CIHR)(2010). Retrieved
from http://www.cihr-irsc.gc.ca/e/29418.html on April 2011.
Corcoran M. (2006) Dissemination or knowledge translation.
American Journal of Occupational Therapy 60(5), 487–488.
Council of the European Union (2008) 2020 Vision for The
European Research Area (ERA). Retrieved from http://register.
consilium.europa.eu/pdf/en/08/st16/st16767.en08.pdf on April
2011
Dearing J.W. & Kreuter M.W. (2010) Designing for diffusion: how
can we increase uptake of cancer communication innovations?.
Patient Education and Counseling 81(Suppl.), S100–S110.
Estabrooks C.A., Thompson D.S., Lovely J.E. & Hofmeyer A.
(2006) A guide to knowledge translation theory. The Journal of
Continuing Education in the Health Professionals 26(1), 25–36.
Fransson E. (2009) Modellen for Praktisk Ferdighetsutøvelse
i Sykepleie. En evaluering av bruken av Bjørks modell
i undervisning og forskning. [The Model of Practical Skill
Performance in nursing. An evaluation of its use in education
and research], Norwegian Report. Institute of Nursing and
Health Sciences, University of Oslo, Norway.
Graham I.D., Tetroe J. & the KT Theories Research Group (2007)
Some theoretical underpinnings of knowledge translation.
Academic Emergency Medicine 14(4S), 936–941.
Graham I.D., Logan J., Harrison M.B., Harrison M.B., Straus S.E.,
Tetroe J., Caswell W. & Robinson N. (2006) Lost in knowledge
translation: time for a map?. Journal of Continuing Education in
the Health Professions 26(1), 13–24.
Horsley J.A., Crane J., Crabtree M.K & Wood D.J. (1983) Using
Research to Improve Nursing Practice: A Guide. Grune
& Stratton, San Francisco.
Hutchinson A.M. & Johnston L. (2004) Bridging the divide: a
survey of nurses opinions of barriers to and facilitators of,
research utilization in the practice setting. Journal of Clinical
Nursing 13(3), 304–315.
Kitson A.L. (2008) The need for systems change: reflections on
knowledge translation and organizational change. Journal of
Advanced Nursing 65(1), 217–228.
Kitson A., Harvey G. & McCormack B. (1998) Enabling the
implementation of evidence based practice: a conceptual
framework. Quality in Health Care 7, 149–158.
Larsen K. & Nielsen C.M. (2006) Grundlæggende sygepleje/
kropspleje. Afprøving af model om kliniske færdigheder i forhold
til klinisk vejledning og bedømmelse [Fundamental nursing/body
care. Testing a model of practical skill in relation to clinical
supervision and evaluation]. Danish Report. VIA University
College, �Arhus, Denmark.
Lomborg K. (2004) Nurse-patient interactions in assisted personal
body care. A qualitative study in people hospitalized with severe
chronic obstructive pulmonary disease (COPD). PhD thesis,
Aarhus University, Denmark.
Mitton C.M., Adair C.E., McKenzie E., Pattern S.B. & Perry B.W.
(2007) Knowledge transfer and exchange: review and synthesis
of the literature. Milbank Quarterly 85(4), 729–768.
Nielsen CM, Skovsgaard AMF & Stenholt B. (2005) Studieunits
[Dedicated educational units]. Danish Report nr. 4,
Udviklingsinitiativet for Sygeplejerkeuddannelsen i �Arhus Amt,�Arhus, Denmark.
Nielsen C.M., Larsen K., Skovsgaard A.M.F. & Stenholt B. (2007)
Model for at lære praktisk Sygepleje [Model for learning
practical nursing]. Sygeplejersken 107(17), 60–64 (Danish).
Nielsen C., Larsen K., Skovsgaard A.M., Stenholt B. & Lomborg K.
(2009) Brug for fokus p�a kliniske færdigheder. [A need to focus on
clinical skills]. Sygeplejersken 109(16), 48–52 (Danish).
Pentland D., Forsyth K., Maciver D., Walsh M., Murry R., Irvine
L. & Sikora S. (2011) Key characteristics of knowledge transfer
and exchange in health care: integrative literature review. Journal
of Advanced Nursing 67(7), 1408–1425.
Rich R.F. (1979) The pursuit of knowledge. Knowledge: Creation,
Diffusion, Utilization 1(1), 6–30.
Roux D.J., Rogers K.H., Biggs H.C., Ashton P.J. & Sergeant A. (2006)
Bridging the science- management divide: moving from unidirectional
knowledge transfer to knowledge interfacing and sharing. Ecology and
Society 11(1), Art.4.
Rycroft-Malone J. (2004) The PARIHS framework – a framework
for guiding the implementation of evidence-based practice.
Journal of Nursing Care Quality 4, 297–304.
Rycroft-Malone J. (2010) Using theory and frameworks to
facilitate the implementation of evidence into practice.
Worldviews on Evidence-based Nursing 7(2), 57–58.
Rycroft-Malone J., Kitson A., Harvey G., McCormack B., Seers K.,
Titchen A. & Estabrooks C.A. (2002) Ingredients for change:
revisiting a conceptual framework. Quality & Safety in Health
Care 11, 174–180.
Skovsgaard A.M.F., Stenholt B., Nielsen C.M. & Sørensen D. (2008)
Læring af grundlæggende sygepleje i primær sunnhedstjeneste
[Learning fundamental nursing in primary health care settings].
Danish Report. Via University College, �Arhus, Denmark.
Solli H. & Reierson I-�A. (2006) Fra mesterlære til selvstudium
[From apprenticeship to self- study]. Norsk Tidsskrift for
Sykepleieforskning 8(4), 35–50 (Norwegian).
Stetler C.B. (2001) Updating the Stetler model of research utilization
to facilitate evidence-based practice.Nursing Outlook 49, 272–279.
Stetler C.B. & Marram G. (1976) Evaluating research findings for
applicability in practice. Nursing Outlook 24(9), 559–563.
Straus S.E., Graham I.D., Taylor M. & Lockyer J. (2008) Development
of a mentorship strategy: a knowledge translation case study. Journal
of Continuing Education in the Health Professions 28(3), 117–122.
Straus S.E., Tetroe J. & Graham I. (2009) Defining knowledge
translation. Canadian Medical Association Journal 181(3–4), 165–
168.
© 2013 Blackwell Publishing Ltd 11
JAN: DISCUSSION PAPER Knowledge translation

Sudsawad P. (2007) Knowledge Translation: Introduction to
Models, Strategies and Measures. Southwest Educational Devel-
opment Laboratory, The National Center for the Dissemination
of Disability Research, Austin, TX.
Thompson G.N., Estabrooks C.A. & Degner L.F. (2006) Clarifying
the concepts in knowledge transfer: a literature review. Journal
of Advanced Nursing 53(6), 691–701.
Wallin L. (2009) Knowledge translation and implementation
research in nursing. International Journal of Nursing Studies 46
(4), 576–587.
Ward V., House A. & Hamer S. (2009) Developing a framework
for transferring knowledge into action: a thematic analysis of the
literature. Journal of Health Services Research & Policy 14(3),
156–164.
Williams C.L., Kothari A., Leipert B., Ward-Griffin C., Forbes D.,
King M.L., Kloseck M., Ferguson K. & Oudshoorn A. (2008)
Accelerating client-driven care: pilot study for a social interaction
approach to knowledge translation. Canadian Journal of Nursing
Research 40(2), 58–74.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the advancement of
evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance
and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original
research reports and methodological and theoretical papers.
For further information, please visit JAN on the Wiley Online Library website: www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work in JAN:
• High-impact forum: the world’s most cited nursing journal, with an Impact Factor of 1·477 – ranked 11th of 95 in the 2011 ISI
Journal Citation Reports (Social Science – Nursing).
• Most read nursing journal in the world: over 3 million articles downloaded online per year and accessible in over 10,000 libraries
worldwide (including over 3,500 in developing countries with free or low cost access).
• Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jan.
• Positive publishing experience: rapid double-blind peer review with constructive feedback.
• Rapid online publication in five weeks: average time from final manuscript arriving in production to online publication.
• Online Open: the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley
Online Library, as well as the option to deposit the article in your own or your funding agency’s preferred archive (e.g. PubMed).
12 © 2013 Blackwell Publishing Ltd
I.T. Bjørk et al.