
Frequency, severity, and evolution of split family alliances: How observable are they
11
COUPLES AND FAMILIES Frequency, severity, and evolution of split family alliances: How observable are they? CRISTINA MUN ˜ IZ DE LA PEN ˜ A 1 , MYRNA FRIEDLANDER 1 , & VALENTI ´ N ESCUDERO 2 1 Department of Educational and Counseling Psychology, University at Albany, State University of New York, Albany, NY, USA & 2 Department of Psychology, Universidad de La Corun ˜a, La Corun ˜a, Spain. (Received 7 April 2008; revised 3 September 2008; accepted 6 September 2008) Abstract Split alliances (within-family differences in the emotional bond with the therapist) were studied in 19 U.S. and 21 Spanish families using the System for Observing Family Therapy Alliances (SOFTA; Friedlander, Escudero, & Heatherington, 2006). Examining individual family members’ scores on the corresponding self-report and observational Emotional Connection to the Therapist SOFTA scales, the authors identified mild, moderate, and severe split alliances. In both samples, self-reported splits occurred frequently and with almost all of the therapists. Although clients’ observed interactions with the therapist often mirrored their self-reports, family members’ perceptions of the therapeutic bond were generally more discrepant than their behavior suggested. The majority of families that dropped out had a moderately or severely split alliance in at least one session. Keywords: couples and family systems therapy; psychotherapist training/supervision/development It is not uncommon for clients to feel like ‘‘therapy hostages’’ (Friedlander, Escudero, & Heatherington, 2006, p. 201) when family members make threats, implicit or explicit, about their participation in therapy: ‘‘If you don’t go to therapy, I’ll leave you/ divorce you/send you to a group home/bring charges against you/expel you from school/cut off all finan- cial support’’ and so on. Not surprisingly, such behind-the-scenes negotiations do not bode well for forming a strong working alliance. The conflict over the need for treatment can easily turn into an argument about the therapist’s style, personality, or competence. For this reason, it is challenging to create strong bonds with families in conflict when one or more people attend the sessions under duress. Little is known, however, about whether differences in family members’ emotional investments can reliably be observed and whether these differences are mean- ingful indicators of a therapy in trouble. Compared with the abundant literature in indivi- dual therapy, there has been relatively little research on the working alliance in conjoint couple and family therapy. As Pinsof and Catherall (1986) first noted, there is no ‘‘single’’ family alliance. Each person has a unique relationship with the therapist and also observes every other family member interacting with the therapist. To complicate matters further, there are also two kinds of within-system alliances (Pinsof, 1994, 1995): (a) the alliance between and among family members with regard to the therapy and (b) alliances within the institution (e.g., between cotherapists, between therapist and supervisor, within therapy teams). As Pinsof (1995) pointed out, ‘‘Each alliance level influences, through mutual causality, every other level and locus ... [and] differential causality asserts that some levels of the alliance may play a more critical role than others’’ (p. 67). To study the strength of multiple alliances, Pinsof and Catherall (1986) developed the Couple and Correspondence concerning this article should be addressed to Myrna Friedlander, Department of Educational and Counseling Psychology, ED220, University at Albany, State University of New York, Albany, NY 12203, USA. E-mail: mfriedlander@uamail. albany.edu Psychotherapy Research, March 2009; 19(2): 133142 ISSN 1050-3307 print/ISSN 1468-4381 online # 2009 Society for Psychotherapy Research DOI: 10.1080/10503300802460050
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Frequency, severity, and evolution of split family alliances: How observable are they

COUPLES AND FAMILIES
Frequency, severity, and evolution of split family alliances: Howobservable are they?
CRISTINA MUNIZ DE LA PENA1, MYRNA FRIEDLANDER1, & VALENTIN ESCUDERO2
1Department of Educational and Counseling Psychology, University at Albany, State University of New York, Albany, NY,
USA & 2Department of Psychology, Universidad de La Coruna, La Coruna, Spain.
(Received 7 April 2008; revised 3 September 2008; accepted 6 September 2008)
AbstractSplit alliances (within-family differences in the emotional bond with the therapist) were studied in 19 U.S. and 21 Spanishfamilies using the System for Observing Family Therapy Alliances (SOFTA; Friedlander, Escudero, & Heatherington,2006). Examining individual family members’ scores on the corresponding self-report and observational EmotionalConnection to the Therapist SOFTA scales, the authors identified mild, moderate, and severe split alliances. In bothsamples, self-reported splits occurred frequently and with almost all of the therapists. Although clients’ observedinteractions with the therapist often mirrored their self-reports, family members’ perceptions of the therapeutic bond weregenerally more discrepant than their behavior suggested. The majority of families that dropped out had a moderately orseverely split alliance in at least one session.
Keywords: couples and family systems therapy; psychotherapist training/supervision/development
It is not uncommon for clients to feel like ‘‘therapy
hostages’’ (Friedlander, Escudero, & Heatherington,
2006, p. 201) when family members make threats,
implicit or explicit, about their participation in
therapy: ‘‘If you don’t go to therapy, I’ll leave you/
divorce you/send you to a group home/bring charges
against you/expel you from school/cut off all finan-
cial support’’ and so on. Not surprisingly, such
behind-the-scenes negotiations do not bode well
for forming a strong working alliance. The conflict
over the need for treatment can easily turn into an
argument about the therapist’s style, personality, or
competence.
For this reason, it is challenging to create strong
bonds with families in conflict when one or more
people attend the sessions under duress. Little is
known, however, about whether differences in family
members’ emotional investments can reliably be
observed and whether these differences are mean-
ingful indicators of a therapy in trouble.
Compared with the abundant literature in indivi-
dual therapy, there has been relatively little research
on the working alliance in conjoint couple and family
therapy. As Pinsof and Catherall (1986) first noted,
there is no ‘‘single’’ family alliance. Each person has a
unique relationship with the therapist and also
observes every other family member interacting
with the therapist. To complicate matters further,
there are also two kinds of within-system alliances
(Pinsof, 1994, 1995): (a) the alliance between and
among family members with regard to the therapy and
(b) alliances within the institution (e.g., between
cotherapists, between therapist and supervisor, within
therapy teams). As Pinsof (1995) pointed out, ‘‘Each
alliance level influences, through mutual causality,
every other level and locus . . . [and] differential
causality asserts that some levels of the alliance may
play a more critical role than others’’ (p. 67).
To study the strength of multiple alliances, Pinsof
and Catherall (1986) developed the Couple and
Correspondence concerning this article should be addressed to Myrna Friedlander, Department of Educational and Counseling
Psychology, ED220, University at Albany, State University of New York, Albany, NY 12203, USA. E-mail: mfriedlander@uamail.
albany.edu
Psychotherapy Research, March 2009; 19(2): 133�142
ISSN 1050-3307 print/ISSN 1468-4381 online # 2009 Society for Psychotherapy Research
DOI: 10.1080/10503300802460050
Family Therapy Alliance Scales (CTAS and FTAS),
which ask clients to evaluate their own alliance with
the therapist in terms of goals, tasks, and bonds as
well as the alliances of other family members and the
family as a group in relation to the therapist. The
revised versions of the measures (CTAS-R and
FTAS-R; Pinsof, 1999; Pinsof, Zinbarg, & Kno-
bloch-Fedders, 2008) include a fourth dimension,
the within-system alliance, which asks clients to
report on the alliance among family members (i.e.,
apart from the therapist).
Research with the CTAS and FTAS, as well as
with other measures and methods (Beck, Friedlan-
der, & Escudero, 2006; Bennun, 1989; Bourgeois,
Sabourin, & Wright, 1990; Knobloch-Fedders, Pin-
sof, & Mann, 2004; Robbins, Turner, Alexander, &
Perez, 2003; Robbins et al., 2006, 2008; Symonds &
Horvath, 2004), has consistently found that the
relationship between self-reported alliances and
therapeutic outcome is not straightforward. Family
members often perceive the therapy process quite
differently, and differences in perceptions have con-
sequences for treatment completion. Results have
shown, for example, that discrepancies in parents’
and adolescents’ alliances put families at greater risk
for dropout than either family member’s alliance
with the therapist considered in isolation (Robbins
et al., 2003). In one study of couples (Quinn,
Dotson, & Jordan, 1997), therapy was most success-
ful when wives’ perceptions of the alliance with the
therapist exceeded those of their husbands, whereas
another couples study (Symonds & Horvath, 2004)
found the opposite pattern. To complicate matters
further, in the latter study similarity in the partners’
alliances with the therapist, whether favorable or
unfavorable, was more predictive of treatment
success than either partner’s rating of the alliance
alone.
How, then, can we best capture the alliance
empirically? Arguably, adding or averaging family
members’ alliance scores to arrive at a ‘‘total’’ family
score is misleading because doing so obscures in-
dividual clients’ scores. Yet how much of a discre-
pancy in family members’ scores is meaningful?
Addressing this question, Heatherington and Fried-
lander (1990) estimated the frequency of what Pinsof
and Catherall (1986) called split alliances by defining
a split in terms of standard deviation units on one
subscale (Self with Therapist) of the CTAS or FTAS.
When the split was defined as family members having
scores that were 1 SD apart, 43% of couples and 75%
of families seen in a U.S. hospital clinic had a split
alliance. Based on a more conservative decision rule
(i.e., a 2 SD difference in scores), 14% of the couples
and 42% of the families had split alliances. More
recently, Mamodhoussen, Wright, Tremblay, and
Poitras-Wright (2005) reported that 32% of couples
in a French-speaking university clinic in Quebec had
a 1 SD split alliance and 13.3% had a 2 SD split.
Similarly, Knobloch-Fedders et al. (2004) found that
roughly 40% of couples in a large outpatient agency
had a split alliance in either Session 1 or Session 8.
Despite differences in the three samples and settings,
it is reasonable to conclude that split alliances are
common occurrences.
With few exceptions, the assessment of split
alliances has relied solely on clients’ self-reported
perceptions. Robbins et al. used selected items from
the observational Vanderbilt Therapeutic Alliance
Scale-Revised (VTAS-R; Diamond, Liddle, Hogan,
& Dakof, 1999) to estimate the therapeutic alliance
in functional family therapy (FFT) for adolescent
behavior problems (Robbins et al., 2003) and in
multidimensional family therapy (MDFT; Robbins
et al., 2006) and brief strategic family therapy
(BSFT; Robbins et al., 2008) for adolescent drug
use. Compared with completer families, families
that dropped out of FFT and BSFT demonstrated
more ‘‘unbalanced’’ alliances (Robbins et al., 2003,
2008). In the MDFT study (Robbins et al., 2006),
mothers exhibited significantly better working rela-
tionships with the therapist than did their sons, and
when both clients’ alliance scores decreased from
Session 1 to Session 2, the family was likely to
terminate prematurely.
Although significant correlations have been re-
ported between family members’ perceptions of the
alliance and their in-session behavior (Escudero,
Friedlander, Varela, & Abascal, 2008; Friedlander,
Escudero, Horvath, et al., 2006), these group studies
have little to say about whether, within a given
family, split alliances can be detected behaviorally.
To date, only one study has considered the degree to
which discrepancies in family members’ self-re-
ported alliances are reflected in observable behavior.
Beck et al. (2006) analyzed four family therapy cases
seen at a university clinic in Spain. Behavioral
manifestations of clients’ emotional bonds with
therapists were rated using the Spanish version of
the System for Observing Family Therapy Alliances
(SOFTA; Escudero & Friedlander, 2003). Results
showed that two of the four families had mildly split
alliances in their postsession perceptions (i.e.,
FTAS-R Self-with Therapist scores), but the splits
were minimally reflected in the behavioral ratings.
These findings suggest that mildly split alliances may
not be readily observable.
The correspondence, or lack thereof, of observers’
and clients’ scores has long been of interest to
psychotherapy researchers (e.g., Tichenor & Hill,
1989), and it is generally agreed that clients’ scores are
more predictive of treatment success (e.g., Horvath &
134 C. M. de la Pena et al.
Bedi, 2002). More so than in individual therapy,
clients in conjoint therapy may be unwilling to show
their private feelings in session, when other family
members are closely observing their behavior. Some
clients hide their reactions because of the power
differential in the family or because they cannot risk
showing their true feelings in a therapy context. A
reluctant adolescent, for example, may simply pay lip
service to the therapist in order to appease his parents.
In other words, because what happens, or does not
happen, in couple and family therapy can have
immediate interpersonal consequences, many clients
feel compelled to disguise their true responses (posi-
tive as well as negative) to the therapist.
In the present study, we began by examining the
frequency and severity of split alliance sessions. Our
primary question was, can observers detect split
alliances? That is, how often are discrepancies in
family members’ perceptions of the therapist re-
flected in their observable, in-session behaviors?
Are only severe splits readily observable? A second-
ary question was how split alliances evolve over
time in terms of severity and whether families with
severe splits are likely to drop out of treatment
prematurely.
These research questions were studied in two
existing data sets with (a) low-income families in a
nonprofit community clinic in the United States
and (b) middle-income families in a Spanish uni-
versity training clinic. We anticipated that our
results, if consistent across these diverse samples,
would have implications not only for future family
process research but also for practice. Because
mildly split alliances seem to be commonplace
(Beck et al., 2006; Heatherington & Friedlander,
1990; Knobloch-Fedders et al., 2004; Mamodhous-
sen et al., 2005), it may be easy for a therapist to
miss the signs of a poorly developing relationship
with a quiet family member. If only severely split
alliances can be detected in client behavior, it may
be too late for the therapist, who needs to rely on
observable behavior, to repair the split before the
family drops out. To build theory about how split
alliances can effectively be corrected, we first need
to know whether they can be observed, that is,
whether discrepancies in family members’ self-
reported feelings toward the therapist match their
behavior and, if so, whether the observed within-
family discrepancies are more or less extreme than
the self-reported ones. We also need to know how
often splits remain unchanged, improve, or deterio-
rate over time in treatment and how often they
result in premature termination.
Method
Participants
U.S. sample. Data for this study were drawn from
an existing data set of 29 low-income families who
volunteered to participate in a study on the effec-
tiveness of family therapy (Friedlander, Lambert, &
Muniz de la Pena, 2008). Clients were seen for a
maximum of 10 free conjoint sessions (M�8.8,
SD�2.1). All families had at least one school-age
child at risk, and presenting concerns included
family conflict; children’s conduct problems, poor
school performance, or sexual abuse; and parental
death, separation/divorce, substance abuse, or in-
carceration. The majority of families were headed by
single parents, and most families had fairly young
children (mean age�10.2 years, SD�3.69). For the
present study, we used data from 19 of the 29
families (i.e., all those that were seen for at least
three sessions in which two or more family members
completed the self-report alliance measure). (Chil-
dren younger than 12 years did not provide self-
report data.) Participating clients ranged in age from
12 to 58 years (M�28.02, SD�12.80).
The 10 therapists in the full sample (seven White
women, one Latina, two White men) had a wide age
range (23�59 years, M�41.3, SD�11.39) and
range of clinical experience (9 months to 23 years;
M�6.8, SD�6.64). Nine of these 10 therapists saw
families in the present subsample; four therapists
were graduate students, and the remainder were
either master’s-level (n�4) or doctorate-level (n�1)
clinicians. Various theoretical approaches were re-
presented, including family systems (n�4), eclectic
(n�2), psychodynamic (n�1), client centered (n�1), and cognitive�behavioral (n�1).
Spanish sample. Data from a sample of 37
mostly middle-income couples (n�16) and families
(n�21), seen for an average of 7.6 sessions (SD�3.1), came from a recent study of the relationship of
alliance to therapeutic progress (Escudero et al.,
2008). Only the 21 families (i.e., none of the
couples) were included in the present study. Pre-
senting problems included family conflict, problems
with communication, parenting concerns, separa-
tion/divorce, and parental death. All of the partici-
pating clients were White Spaniards, aged 12 to 72
years (M�35.3, SD�17.53).
The families were seen by six White therapists
(three women, three men) ranging in age from 30 to
50 years (M�40, SD�7.57) and in experience
ranging 4 to 20 years (M�11.2, SD�7.26). Two
therapists were doctorate-level and four were mas-
ter’s-level psychologists. The predominant theoreti-
cal orientation was an integrative model of brief
Split alliances 135

systemic therapy that included structural, strategic,
and solution-focused elements.
System for Observing Family Therapy
Alliances
SOFTA-o. The transtheoretical SOFTA-o was
created simultaneously in English (Friedlander
et al., 2004; Friedlander, Escudero, & Heathering-
ton, 2006; Friedlander, Escudero, Horvath, et al.,
2006) and Spanish (Sistema de Observacıon de
la Alianza Terapeutica en Intervencıon Familiar;
Escudero & Friedlander, 2003) to assess four
behavioral aspects of the therapeutic alliance in the
context of couple and family therapy. Two dimen-
sions reflect Bordin’s (1979) goals, tasks, and bonds:
Engagement in the Therapeutic Process and Emo-
tional Connection to the Therapist (EC). The other
two dimensions, Safety Within the Therapeutic
System and Shared Sense of Purpose Within the
Family, reflect aspects of the alliance that are unique
to conjoint treatment.
In the present study, only the clients’ EC dimen-
sion was of interest because, according to authors of
the SOFTA (Friedlander, Escudero, & Heathering-
ton, 2006), this dimension best captures ruptures in
clients’ individual relationships with the therapist.
Moreover, the EC dimension is the one most similar
to the FTAS self with therapist alliance, which was
used in previous research on split alliances (e.g.,
Beck et al., 2006; Heatherington & Friedlander,
1990). In the SOFTA, the emotional connection is
operationally defined as
Viewing the therapist as an important person in
the client’s life, almost like a family member; a
sense that the relationship is based on affiliation,
trust, caring, and concern; that the therapist
genuinely cares and ‘‘is there’’ for the client, that
he or she is on the same wavelength with the
therapist (e.g., similar life perspectives, values)
and that the therapist’s wisdom and expertise are
valuable. (Friedlander, Escudero, & Heathering-
ton, 2006, p. 88)
Using the SOFTA-o, trained observers make
inferences about clients’ perceptions of the alliance
from their observed interactions in either videotaped
or live couple and family therapy sessions. To use
this rating system, trained judges observe a session
and tally the frequencies of specific, operationally
defined positive and negative alliance-related beha-
viors (see later examples) in each of the four
dimensions as they occur. Based on these tallies,
each dimension is then rated from �3 (extremely
problematic) to 3 (extremely strong; with 0�unremark-
able or neutral). To go from the tallies to the global
ratings, judges consult the operational definitions
and rating guidelines in the training manual (Fried-
lander et al., 2004) and consider the valence
(positive or negative), frequency, intensity, and
clinical meaningfulness of the observed behaviors.
According to the guidelines, the rating must be
between 1 and 3 when only positive behaviors are
exhibited and between �1 and �3 when only
negative behaviors are exhibited; ratings must be
between �1 and 1 when a client exhibits both
positive and negative behaviors. In the EC dimen-
sion, 10 verbal and nonverbal behaviors are repre-
sented, including ‘‘Client expresses interest in the
therapist’s personal life,’’ ‘‘Client shares a joke or
lighthearted moment with the therapist,’’ and ‘‘Cli-
ent mirrors the therapist’s body posture.’’ The
negative behaviors include ‘‘Client avoids eye con-
tact with the therapist,’’ ‘‘Client is reluctant or
refuses to answer the therapist,’’ and ‘‘Client has
hostile or sarcastic interactions with the therapist.’’
The authors of the SOFTA-o (Friedlander, Escu-
dero, & Heatherington, 2006) reported intraclass
reliabilities ranging from .72 to .95 across several
studies.
SOFTA-s. The self-report SOFTA-s (Friedlander,
Escudero, & Heatherington, 2006) has four subscales
that correspond closely to the operationally defined
SOFTA-o dimensions. The 16 items, both positively
and negatively worded, are rated on 5-point Likert
scales (1�not at all and 5�very much). The four
items on the EC scale are ‘‘The therapist understands
me,’’ ‘‘The therapist is doing everything possible to
help me,’’ ‘‘The therapist has become an important
person in my life,’’ and ‘‘The therapist lacks the
knowledge and skills to help me.’’ With the last item
reverse scored, high EC scores indicate a strong
personal bond with the therapist (range�4�20).
In previous research, the SOFTA-s has been reli-
able (Cronbach alphas�.62�.87) and significantly
associated with SOFTA-o behavioral ratings (Fried-
lander, Escudero, & Heatherington, 2006). In the
present samples, the EC internal consistency reliabil-
ities were .76 (United States) and .67 (Spanish).
Dropout. The U.S. families were offered a max-
imum of 10 conjoint family sessions, and the
Spanish families were offered eight sessions, with
the option to continue for an additional eight
sessions on the therapist’s recommendation. We
defined dropout in both samples as premature
termination (i.e., when a family unilaterally chose
to discontinue treatment for any reason, usually by
failing a scheduled appointment and not returning).
136 C. M. de la Pena et al.

Procedure
Adult clients and adolescents older than age 12
completed the SOFTA-s immediately after Sessions
3, 6, and 9 in the U.S. sample. In the Spanish
sample, the measure was administered only after
Sessions 3 and 6 because very few Spanish families
had nine or more sessions.
Four graduate students in the United States (two
doctoral and two master’s students in counseling
psychology), all White women, and three research
assistants in Spain were trained in the SOFTA-o for
more than 20 hr using practice videotapes until 90%
of their ratings varied by 1 point or less. The U.S.
judges were then split into two teams, each person
independently rating half the final sample from
videotapes. All three Spanish raters independently
rated a randomly selected subsample (30%) of
sessions, and the remaining sessions were rated by
a single judge. Both teams negotiated discrepancies
to consensus.
As is usual with the SOFTA-o, the judges rated
the behavior of all members of the family simulta-
neously. The judges were aware of the session
numbers (3, 6, or 9) but not the present research
questions, because the ratings were completed be-
fore this study was devised. In the larger U.S. sample
from which the present data were drawn, the judges
achieved a mean intraclass correlation (ICC) of .86
on the EC dimension. In the Spanish sample, the
judges achieved a mean ICC of .76.
Results
To begin, we calculated the EC means and standard
deviations for both the SOFTA-s and the SOFTA-o
separately for each sample and for each session (see
Table I). The distributions of self-reported EC scores
showed that clients in both samples perceived the
emotional bonds with their therapists quite favorably.
Notably, the Spanish sample scored significantly
higher and reported less variability than the U.S.
sample in both Session 3, t(97)�3.96, pB.0001,
and Session 6, t(68)�4.22, pB.0001.
The observational EC ratings were similar in the
two samples (see Table I), with means close to 0,
which indicates that, on average, the clients exhib-
ited unremarkable to moderately positive emotional
connections with their therapists. However, compar-
isons showed that, in Session 6, the Spanish clients
demonstrated relatively more positive and less vari-
able emotional connection behavior (M�0.42,
SD�0.67) than did the U.S. clients (M��0.04,
SD�1.01), t(83)�2.33, pB.02.
Self-Reported Splits
Identification. Split alliances were defined as ses-
sions in which two or more family members had
notably discrepant SOFTA-s scores. Forty-nine ses-
sions from the U.S. sample and 31 sessions from the
Spanish sample were examined for splits. (Because
of missing self-report data and because a number of
the U.S. children were too young to complete the
postsession members, some sessions could not be
examined for split alliances.)
As was done in other split alliance studies, we
identified split alliances based on standard deviation
units. However, going beyond the prior research, we
also took into account the sample means, which
allowed us to assess the degree of severity in the
families’ split EC scores. Mild splits were operation-
ally defined as occurring when two or more family
members’ self-reported EC scores differed by at least
1 SD and all clients scored at or above the respective
sample mean. Moderate splits occurred when two
family members’ EC scores differed by 1 SD and at
least one client scored below the sample mean.
Severe splits occurred when there was a difference
in standard deviation of 2 or more between or among
family members, with at least one client below the
sample mean.
Table I. Means and Standard Deviations of Self-Reported and Observed Emotional Connection Scores
U.S. sample Spanish sample
Variable M SD M SD p
SOFTA-s
Session 3 14.94 3.13 17.16 2.40 .0001
Session 6 14.82 4.20 18.27 1.72 .0001
Session 9 15.09 3.39 * * *
SOFTA-o
Session 3 0.27 1.03 0.22 0.71 �.05
Session 6 �0.04 1.01 0.42 0.66 .022
Session 9 0.35 1.07 * * *
Note. None of the Spanish families had nine sessions. SOFTA�System for Observing Family Therapy Alliances; s�self-report; o�observed. SOFTA-s range: 4�20; SOFTA-o range��3 to 3.
Split alliances 137

Because most clients completed the SOFTA-s at
least twice, we avoided redundancy in the data by
using separate sample means and standard devia-
tions for each session. Thus, by rounding to the
nearest whole numbers, we used M�15 as a
decision rule for all three sessions with the U.S.
sample, but we used SD�3 for Sessions 3 and 9 and
SD�4 for Session 6 (see Table I). For the Spanish
sample, we used SD�2 for both sessions but M�17
for Session 3 and M�18 for Session 6.
Frequency and severity. As operationalized by the
self-report data, eight of the nine (89%) U.S.
therapists and five of the six (83%) Spanish thera-
pists had one or more families with a split alliance
session. At least one self-reported split session was
reported by 14 of the 19 (73.6%) U.S. families and
by 14 of the 21 (66.67%) Spanish families. Adoles-
cents’ scores were lower than their parents’ in 50%
of the U.S. families and 35.7% of the Spanish
families. In both samples, a parent occasionally had
the lower score; in several cases, the family member
reporting the lower score varied from one session to
another.
The self-reported splits occurred most often in
Session 3 (in 52.6% of U.S. families and 57.1% of
Spanish families). In the U.S. sample, four families
(21%) had one split session, eight (42%) had two
split sessions, and two (10.5%) had three split
sessions. In the Spanish sample, eight families
(38.1%) had one split session and six (28.57%)
had two split sessions.
Table II shows the frequencies of split alliances by
level of severity. For the U.S. sample, 26 sessions had
self-reported splits; six (23%) were mild, eight
(31%) were moderate, and 12 (46%) were severe.
Twenty (45%) of the Spanish family sessions had
self-reported splits, of which five (25%) were mild,
eight (40%) were moderate, and seven (35%) were
severe.
Consistency and Congruence of Observer
Ratings
Consistency. After identifying sessions in which
either a mild, moderate, or severe split was present
in the self-reported EC scores, we examined the
observers’ EC ratings of those same sessions. First,
we examined the consistency of the SOFTA-o
ratings of the family members who had self-reported
splits. To consider the observer ratings to be a
consistent reflection of the split reported by the
clients, the same two (or more) family members
needed to have at least mildly discrepant observer
ratings (as defined later) in the same direction. For
example, if the mother’s self-reported SOFTA-s
score were 2 SDs higher than her daughter’s, for
the observed split to be considered consistent the
mother’s SOFTA-o behavioral rating needed to be at
least 1 SD higher than the daughter’s. If the mother’s
and daughter’s SOFTA-o ratings were identical, or if
the daughter’s behavior was rated higher than the
mother’s, the session was not counted as a consistent
observational split. In other words, we were only
interested in observational splits that matched the
self-reported splits.
As shown in Table II, most of the self-reported
splits in the U.S. sample (62%) were consistently
detected by the SOFTA-o, particularly those that
were moderate or severe. For the Spanish families,
40% of the self-reported splits were consistent with
behavior, predominantly those that were moderate
or severe.
Severity congruence. Corresponding to the opera-
tionalization of severity in SOFTA-s scores, we used
the SOFTA-o sample mean (0) and standard devia-
tion (1) to identify the degree of severity in the
observed splits. Thus, observed splits were consid-
ered mild when there was at least a 1-point difference
in two or more family members’ SOFTA-o ratings,
with no ratings below 0. Moderate splits were defined
Table II. Consistency and Congruence of Self-Reported and Observed Split Alliances
U.S. families Spanish families
Variable Self-report
Consistent
w/self-reporta
Congruent
in severityb Self-report
Consistent
w/self-reporta
Congruent
in severityb
Mild 6 .33 .17 5 .20 .20
Moderate 8 .63 .13 8 .50 .13
Severe 12 .75 .42 7 .43 .29
Total 26 .62 .27 20 .40 .20
Note. There were 49 total sessions (from 19 families) in the U.S. sample, 31 total sessions (from 21 families) in the Spanish sample, in which
at least two family members provided self-reported alliance ratings on the System for Observing Family Therapy Alliances�self-report
(SOFTA-s). Self-reported splits were defined based on clients’ SOFTA-s Emotional Connection scores.aProportions of self-reported split sessions that matched the observational (SOFTA-o) ratings in terms of which family members had higher
or lower Emotional Connection scores. bProportions of self-reported split sessions that were not only consistent but were also at the same
level of severity (i.e., mild, moderate, or severe) on the SOFTA-o.
138 C. M. de la Pena et al.
as a 1-point difference in SOFTA-o ratings, with at
least one family member below 0. Severe splits
required a difference of at least 2 points in family
members’ ratings, with at least one family member
below 0.
For all of the ‘‘consistent’’ sessions (those in which
the same family members had at least a mildly split
alliance on both measures), we determined the
degree of severity congruence. In other words, a
congruent split was defined as occurring when the
observed split was at the same level of severity as the
self-reported split (i.e., a mild self-reported split was
also observed as mild, a moderate split was observed
as moderate, and a severe split was observed as
severe). Thus, for example, if a mother and daughter
had SOFTA-o behavioral ratings that were 2 points
apart (mother�1, daughter��1), with one rating
below 0, this severe observed split would be con-
gruent with the severe self-reported split (SOFTA-s
scores: mother�18, daughter�10). On the other
hand, the observed split would be considered non-
congruent if the discrepancy in SOFTA-o ratings
was either mild (mother�1 and daughter�0) or
moderate (mother�0, daughter��1) rather than
severe.
Table II shows the severity congruence of self-
reported and observed splits. Congruence was gen-
erally poor in both the Spanish (20% of sessions)
and the U.S. (27%) samples. However, in both
samples, congruence was most likely for the severe
splits (42% of the severe U.S. sessions and 29% of
the severe Spanish sessions).
We also examined the noncongruent splits (not
tabled) to determine in what way the observed splits
differed in severity from the self-reported splits.
Notably, 75% of the noncongruent observed splits
in both samples were less severe than the self-
reports. In other words, when the observer ratings
were not congruent with the self-reported alliance
scores in level of severity, family members’ self-
reported alliances were generally more discrepant
than their behavior indicated.
Evolution of Self-Reported Splits
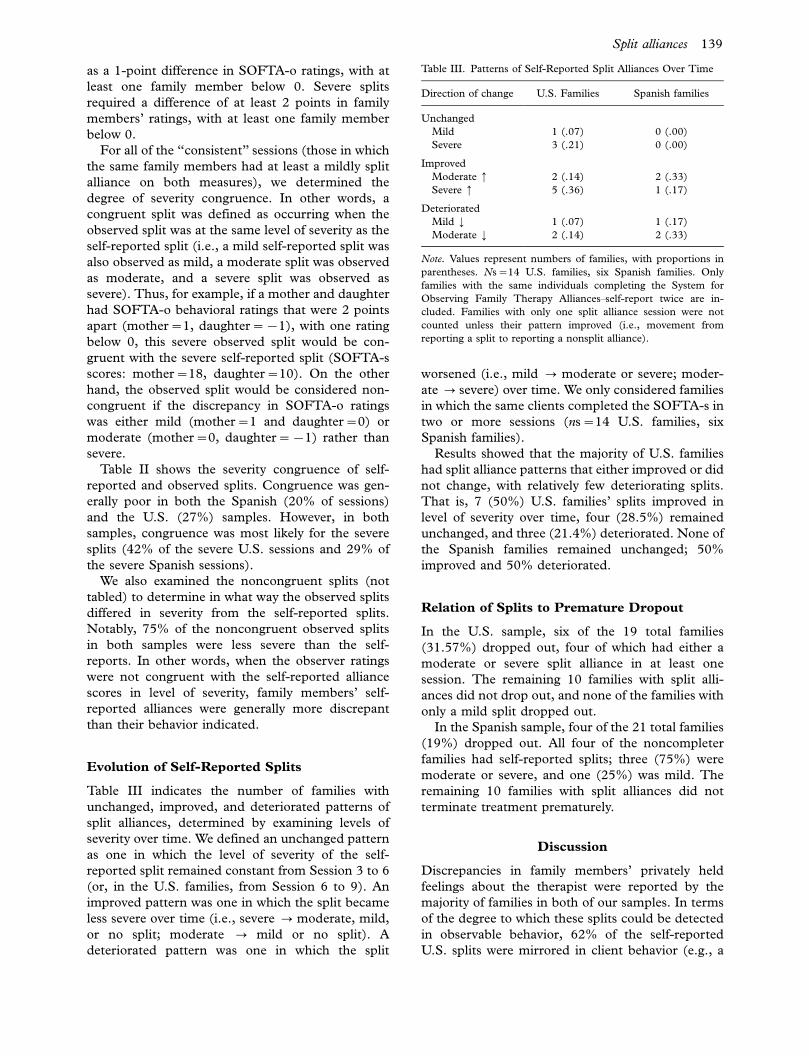
Table III indicates the number of families with
unchanged, improved, and deteriorated patterns of
split alliances, determined by examining levels of
severity over time. We defined an unchanged pattern
as one in which the level of severity of the self-
reported split remained constant from Session 3 to 6
(or, in the U.S. families, from Session 6 to 9). An
improved pattern was one in which the split became
less severe over time (i.e., severe 0 moderate, mild,
or no split; moderate 0 mild or no split). A
deteriorated pattern was one in which the split
worsened (i.e., mild 0 moderate or severe; moder-
ate 0 severe) over time. We only considered families
in which the same clients completed the SOFTA-s in
two or more sessions (ns�14 U.S. families, six
Spanish families).
Results showed that the majority of U.S. families
had split alliance patterns that either improved or did
not change, with relatively few deteriorating splits.
That is, 7 (50%) U.S. families’ splits improved in
level of severity over time, four (28.5%) remained
unchanged, and three (21.4%) deteriorated. None of
the Spanish families remained unchanged; 50%
improved and 50% deteriorated.
Relation of Splits to Premature Dropout
In the U.S. sample, six of the 19 total families
(31.57%) dropped out, four of which had either a
moderate or severe split alliance in at least one
session. The remaining 10 families with split alli-
ances did not drop out, and none of the families with
only a mild split dropped out.
In the Spanish sample, four of the 21 total families
(19%) dropped out. All four of the noncompleter
families had self-reported splits; three (75%) were
moderate or severe, and one (25%) was mild. The
remaining 10 families with split alliances did not
terminate treatment prematurely.
Discussion
Discrepancies in family members’ privately held
feelings about the therapist were reported by the
majority of families in both of our samples. In terms
of the degree to which these splits could be detected
in observable behavior, 62% of the self-reported
U.S. splits were mirrored in client behavior (e.g., a
Table III. Patterns of Self-Reported Split Alliances Over Time
Direction of change U.S. Families Spanish families
Unchanged
Mild 1 (.07) 0 (.00)
Severe 3 (.21) 0 (.00)
Improved
Moderate � 2 (.14) 2 (.33)
Severe � 5 (.36) 1 (.17)
Deteriorated
Mild ¡ 1 (.07) 1 (.17)
Moderate ¡ 2 (.14) 2 (.33)
Note. Values represent numbers of families, with proportions in
parentheses. Ns�14 U.S. families, six Spanish families. Only
families with the same individuals completing the System for
Observing Family Therapy Alliances�self-report twice are in-
cluded. Families with only one split alliance session were not
counted unless their pattern improved (i.e., movement from
reporting a split to reporting a nonsplit alliance).
Split alliances 139

mother’s score at least 1 SD higher than her
daughter’s score on both the self-report and obser-
vational measures). However, only 27% of the
observed splits were congruent in terms of severity
with the self-reported splits. The majority of the
congruent splits were severe, indicating that family
members who felt very differently about the therapist
often showed this extreme difference in their beha-
vior. Results were somewhat more modest in the
Spanish sample, however, in which only 40% of the
splits matched the in-session behavior, with only
20% of the splits congruent in severity. Importantly,
in both samples the noncongruent splits occurred
generally because individual family members’ self-
reported bonds with the therapist were more dis-
crepant (i.e., severe) than their in-session behavior
suggested. These results, which are consistent with
Beck et al.’s (2006) case studies, suggest that, in a
given session, differences in the quality of family
members’ bonds with the therapist may be detect-
able but the extremity of clients’ feelings tends not to
be readily apparent.
Looking at where the splits occurred, we found
that the majority of split alliances took place early in
therapy (i.e., the third session, when the quality of
the therapeutic relationship is still developing).
Notably, it was not consistently either the adolescent
or the parent(s) whose EC score was the lowest in
the family. In terms of changes over time, only three
families with mild splits in Session 3 had a deterior-
ating pattern, and a fair proportion of the moderate
and severe splits improved with time (43% of U.S.
families, 50% of Spanish families). Consistent with
this finding, split alliances did not invariably lead to
dropout; in both samples, the majority of families
with split alliances did not terminate treatment
prematurely. Notably, though, dropout occurred
most often in families whose splits were relatively
more severe.
Consistent with alliance research in general, the
present clients’ self-reported emotional connections
to their therapist were, on average, fairly (U.S.
sample) to very (Spanish sample) strong, whereas
the average observed (behavioral) EC ratings in both
samples were only moderate. These results are
consistent with previous findings (Shelef, Diamond,
Diamond, & Little, 2005) that clients reported
feeling more positively about their personal relation-
ships with the therapist than their behavior indi-
cated. It may be that in session some clients do not
want to show how much they like the therapist,
especially if they were coerced into treatment by
other family members. Alternately, it is possible that
self-reported alliances are inflated as a result of social
desirability (Shelef et al., 2005), although our clients
knew that their therapists would not have access to
the questionnaire data.
The relatively more positive mean scores on the
SOFTA-s tell only a part of the story, however.
Without examining each family individually, we
might overlook the fact that a fair number of families
in both samples had moderately or severely split
alliances in at least one session. This finding, which is
consistent with three prior studies (Beck et al., 2006;
Heatherington & Friedlander, 1990; Mamodhoussen
et al., 1995), is notable given the cultural, linguistic,
contextual, and demographic differences across sam-
ples. The present U.S. families, all low income, were
seen in a not-for-profit community clinic, whereas the
Spanish clients, seen in a university training center,
tended to be middle class and somewhat older. The
Spanish therapists had relatively more experience and
consistently used a brief systemic approach, whereas
the U.S. therapists were less experienced and notably
more eclectic in orientation. Whether the somewhat
larger proportion of severe splits in the U.S. sample
was due to any of these differences is not possible to
discern. Nonetheless, the similar results across sam-
ples are of importance both theoretically and
practically.
In general, our results are consistent with previous
reports, suggesting that variability in family mem-
bers’ alliance perceptions is commonplace. How-
ever, the present study improved on the earlier
investigations in several ways. This was the first
research to assess the degree of consistency between
self-reported and behavioral split alliances. Like
prior researchers (Beck et al., 2006; Heatherington
& Friedlander, 1990; Knobloch-Fedders et al.,
2004; Mamodhoussen et al., 2005), we operationally
defined a split in terms of standard deviation units,
but we also took into account the relative strength of
clients’ perceived bonds with the therapist (i.e.,
where each family member’s SOFTA-s score was in
relation to the sample mean). This methodology
allowed us to determine congruence in level of
severity, a characteristic that seems to be meaningful
for comparing self-reported and observed splits and
for identifying patterns of split alliances over time.
Use of our methods in future research can permit a
close examination of what actually takes place in
sessions when moderate and severe splits improve or
when they result in premature dropout. We also need
to consider clients’ ratings on all four SOFTA
dimensions in order to determine whether emotional
connection to the therapist is a unique predictor of
outcome. It may well be that, despite having a split
alliance with the therapist, families that stay in
treatment are highly engaged in problem solving,
find the therapeutic setting to be a safe environment,
and share a common vision for family change.
140 C. M. de la Pena et al.

There are at least three explanations for the fair
number of self-reported split alliances that were not
detected by the behavioral ratings. First, there is an
important methodological difference between self-
reported and observed alliances: When asked to
complete an alliance questionnaire, clients consider
their cumulative experience of the therapist, whereas
observers only rate what they see in a single session.
Second, the items in these two measurement formats
differ, despite being based on the same operational
definitions. Whereas clients report on their global
impressions of the therapist, the observational ratings
are more conservative estimates of the alliance. That
is, to maximize interrater reliability, only clearly
evident behavioral manifestations of the alliance are
recorded, and subtle signs of positive and negative
emotional connection are not tallied. Third, clients’
feelings about the therapist may well be the result of
covert processes that could not be captured by any
behavioral rating system. That is, emotional bonds
are not always created through direct communication
but rather through more complex, indirect interac-
tion. Because each family member observes the
therapist interacting with all the other family mem-
bers, a mother may feel a bond with the therapist not
because of how the therapist treats her but because
she sees the therapist showing support and concern
for her troubled child.
Another limitation has to do with the fact that
although EC scores estimate each client’s individual
bond with the therapist, in any family context,
individuals’ thoughts, emotions, and behaviors are
interdependent (Bolger & Shrout, 2007). To avoid
this problem, it would be preferable to analyze data
from individual clients within families, within ses-
sions, and within therapists, but finding large enough
samples for a hierarchical linear analysis can be
problematic. The modest overlap between self-re-
port and observer scores suggests that researchers
need both sources of information on the alliance to
fully understand what is taking place in conjoint
couple and family therapy. One implication for
future research has to do with the problem of
designating an appropriate unit of analysis. Our
findings indicate that it is worthwhile to define a
family-level variable (e.g., mild, moderate, or severe
split) by comparing the behaviors or responses of
individual family members. Future research that
compares families in their development and patterns
of split alliances is the one possible next step in this
line of inquiry.
Another important next step is to examine the
extent to which therapists can detect split alliances.
Therapists and external judges may see the alliance
similarly because they must both rely on observable
behavior to assess family members’ levels of emo-
tional connection. However, given their direct and
subjective involvement with the family, therapists’
perceptions may be more similar to the clients’
experience. On the other hand, therapists’ percep-
tions may not be accurate if they have strong
personal reactions to the family that interfere with
their ability to discern their clients’ feelings correctly.
Finally, what about individual therapist effects? All
but one therapist in each sample experienced a split
session. With future research, we may discover
whether split sessions have more to do with therapist
behavior or with preexisting differences within fa-
milies (e.g., varying motivation levels, relational
capacities). Given the frequency of therapists with
split sessions, we suspect that splits have more to do
with what each family brings to treatment, especially
because previous researchers found that splits could
be predicted from couples’ levels of marital (Kno-
bloch-Fedders et al., 2004; Mamodhoussen et al.,
2005), individual (Mamodhoussen et al., 2005), or
family-of-origin (Knobloch-Fedders et al., 2004)
distress.
When we consider all the reasons why clients’
feelings toward their therapists may not be reflected
in behavior, it is important to know that a fair
number of split alliances can be detected from in-
session behavior. When becoming aware of a split,
therapists should not lose sight of two points. First,
the level of severity may not be apparent. It is likely
that some family members privately feel more
extremely positive or negative than they appear.
Second, the reason for clients’ discrepant feelings is
likely to be different for every family. In one case, the
therapist may be favoring one client over another,
leading the latter to feel resentful; in another case,
there may be a ‘‘hostage’’ who is merely paying lip
service to the therapist to avoid recrimination from
other family members. Discerning the cause of a
split alliance may shed light on hidden family
patterns that, if attended to within the therapy,
may well also improve the family’s private life.
Acknowledgements
This article was presented at the 2008 Annual
Conference of the Society for Psychotherapy Re-
search in Barcelona. We are grateful to the many
research assistants who rated videotapes and to
Shaina Bernardi and Laurie Heatherington for their
helpful comments on a previous version of this
article.
References
Beck, M., Friedlander, M. L., & Escudero, V. (2006). Three
perspectives on clients’ experiences of the therapeutic alliance:
Split alliances 141

A discovery-oriented investigation. Journal of Marital and
Family Therapy, 32, 355�368.
Bennun, I. (1989). Perceptions of the therapist in family therapy.
Journal of Family Therapy, 11, 243�255.
Bolger, N., & Shrout, P. N. (2007). Accounting for dependency in
longitudinal data on dyads. In T. D. Little, D. Todd, J. A.
Bovaird & N. A. Card (Eds), Modeling contextual effects in
longitudinal studies (pp. 285�298). Mahwah, NJ: Erlbaum.
Bordin, E. S. (1979). The generalizability of the psychoanalytic
concept of the working alliance. Psychotherapy, 16, 252�260.
Bourgeois, L., Sabourin, S., & Wright, J. (1990). Predictive
validity of therapeutic alliance in group marital therapy. Journal
of Consulting and Clinical Psychology, 58, 608�613.
Diamond, G. M., Liddle, H. A., Hogue, A., & Dakof, G. A.
(1999). Alliance-building interventions with adolescents in
family therapy: A process study. Psychotherapy: Theory, Re-
search, Practice, Training, 36, 355�368.
Escudero, V., & Friedlander, M. L. (2003). El sistema de
observacion de la alianza terapeutica en intervencion familiar
(SOATIF): Desarrollo trans-cultural, fiabilidad, y aplicaciones
del instrumento [The observation system for the therapeutic
alliance in family intervention (SOATIF): Developing cross-
cultural, reliability, and applications of the instrument]. Mo-
saico (Journal of the Spanish Federation of Family Therapy
Associations), 25, 32�36.
Escudero, V., Friedlander, M. L., Varela, N., & Abascal, A.
(2008). Observing the therapeutic alliance in family therapy:
Associations with participants’ perceptions and therapeutic
outcomes. Journal of Family Therapy, 30, 194�204.
Friedlander, M. L., Escudero, V., & Heatherington, L. (2006).
Therapeutic alliances with couples and families: An empirically-
informed guide to practice. Washington, DC: American Psycho-
logical Association.
Friedlander, M. L., Escudero, V., Heatherington, L., Deihl, L.,
Field, N., Lehman, P., et al. (2004). System for Observing Family
Therapy Alliances (SOFTA-o) training manual-revised. Retrieved
September 22, 2008, from www.softa-soatif.net
Friedlander, M. L., Escudero, V., Horvath, A. O., Heatherington,
L., Cabero, A., & Martens, M. P. (2006). System for Observing
Family Therapy Alliances: A tool for research and practice.
Journal of Counseling Psychology, 53, 214�225.
Friedlander, M. L., Lambert, J. E., & Muniz de la Pena, C.
(2008). A step toward disentangling the alliance/improvement
cycle in family therapy. Journal of Counseling Psychology, 55,
118�124.
Heatherington, L., & Friedlander, M. L. (1990). Couple and
family therapy alliance scales: Empirical considerations. Journal
of Marital and Family Therapy, 16, 299�306.
Horvath, A. O., & Bedi, R. P. (2002). The alliance. In J. C.
Norcross (Ed.), Psychotherapy relationships that work: Therapist
contributions and responsiveness to patients (pp. 37�69). New
York: Oxford University Press.
Knobloch-Fedders, L. M., Pinsof, W., & Mann, B. J. (2004). The
formation of the therapeutic alliance in couple therapy. Family
Process, 43, 425�442.
Mamodhoussen, S., Wright, J., Tremblay, N., & Poitras-Wright,
H. (2005). Impact of marital and psychological distress on
therapeutic alliance in couples undergoing couple therapy.
Journal of Marital and Family Therapy, 31, 159�169.
Pinsof, W. M. (1994). An integrative systems perspective on the
therapeutic alliance: Theoretical, clinical, and research implica-
tions. In A. O. Horvath & L. S. Greenberg (Eds), The working
alliance: Theory, research, and practice (pp. 173�195). New York:
Wiley.
Pinsof, W. M. (1995). Integrative problem-centered therapy. New
York: Basic Books.
Pinsof, W. M. (1999). Family Therapy Alliance Scale-Revised.
Evanston, IL: The Family Institute.
Pinsof, W. M., & Catherall, D. (1986). The integrative psy-
chotherapy alliance: Family, couple, and individual therapy
scales. Journal of Marital and Family Therapy, 12, 137�151.
Pinsof, W. M., Zinbarg, R., & Knobloch-Fedders, L. M. (2008).
Factorial and construct validity of the Revised Short Form
Integrative Psychotherapy Alliance Scales for family, couple,
and individual therapy. Family Process, 47, 281�301.
Quinn, W. H., Dotson, D., & Jordan, K. (1997). Dimensions of
therapeutic alliance and their associations with outcome in
family therapy. Psychotherapy Research, 7, 429�438.
Robbins, M. S., Liddle, H. A., Turner, C. W., Dakof, G. A.,
Alexander, J. F., & Kogan, S. M. (2006). Adolescent and
parent therapeutic alliances as predictors of dropout in multi-
dimensional family therapy. Journal of Family Psychology, 20,
108�116.
Robbins, M. S., Mayorga, C. C., Mitrani, V. B., Szapocznik, J.,
Turner, C. W., & Alexander, J. F. (2008). Adolescent and
parent alliances with therapists in brief strategic family therapy
with drug-using Hispanic adolescents. Journal of Marital and
Family Therapy, 34, 316�328.
Robbins, M. S., Turner, C. W., Alexander, J. F., & Perez, G. A.
(2003). Alliance and dropout in family therapy for adolescents
with behavior problems: Individual and systemic effects.
Journal of Family Psychology, 17, 534�544.
Shelef, K., Diamond, G. M., Diamond, G. S., & Liddle, H. A.
(2005). Adolescent and parent alliance and treatment outcome
in multidimensional family therapy. Journal of Consulting and
Clinical Psychology, 73, 689�698.
Symonds, D., & Horvath, A. O. (2004). Optimizing the alliance in
couples therapy. Family Process, 43, 443�455.
Tichenor, V., & Hill, C. E. (1989). A comparison of six measures
of working alliance. Psychotherapy: Theory, Research, Prac-
tice. Training, 26, 195�199.
142 C. M. de la Pena et al.





















