
Fractionated endocardial electrograms are associated with slow conduction in humans: Evidence from...
8
JACC Vol. 13. No. 2 February IYR9:369-76 369 ELECTROPHYSIOLOGIC STUDIES Fractionated Endocardial Electrograms Are Associated Conduction in Humans: Evidence From Pace-Mapping WILLIAM G. STEVENSON, MD, FACC, JAMES N. WEISS, MD, FACC, ISAAC WIENER, MD, FACC, S. MITCHELL RIVITZ, MD, FACC, With Slow KOONLAWEE NADEMANEE, MD, THOMAS KLITZNER. MD, LAWRENCE YEATMAN, MD, MARTIN JOSEPHSON, MD, DANIEL WOHLGELERNTER, MD, FACC Los Angeks, C~~l~f~~rnicr Fractionated ventricular electrograms recorded during catheter mapping may arise from areas of asynchronous depolarization associated with slow conduction, the sub- strate for reentrant ventricular tachycardia, but can also be a nonspecific abnormality or even artifact. To determine whether fractionated sinus rhythm electrograms are asso- ciated with slow conduction in humans, the results of endocardial catheter mapping and pacing at 133 endocar- dial sites in 13 patients were analyzed. Eleven patients had sustained monomorphic ventricular tachycardia and two patients had old myocardial infarction without ventricular tachycardia. Functional evidence of slow conduction at the recording site was assessed by pacing at that site and measuring the interval between the stimulus artifact (S) and the onset of the QRS complex in the 12 lead electrocardiogram (ECG). During pacing at 89 of 90 sites without fractionated sinus rhythm electrograms, the S-QRS interval was ~40 ms, a value consistent with rapid propagation of the stimulated wave front away from the pacing site. During pacing at 21 (49%) of 43 sites with fractionated sinus rhythm electro- grams, the S-QRS interval was MO ms (range 40 to 140), consistent with slow conduction at the pacing site (p < 0.001 versus nonfractionated sites). In 9 of the 11 patients with ventricular tachycardia analysis of the paced QRS configuration, electrograms during induced ventricular tachycardia or programmed stimulation during tachycardia suggested that a site with a long S-QRS interval during pacing was located at or near a ventricular tachycardia circuit. Therefore, fractionated si- nus rhythm electrograms are often associated with slow conduction, which may be the substrate for reentrant ventricular tachycardia. Endocardial pacing at these sites can be used to provide functional evidence of slow conduc- tion in humans. (J Am CONCardiol1989;13:369-76) Fractionated ventricular electrograms are frequently re- corded from patients with ventricular tachycardia late after a myocardial infarction (I-IO). Studies (I l-13) in animal mod- els of myocardial infarction have shown that fractionated electrograms can result from asynchronous activation of muscle fibers at the recording site associated with slow propagation of the activation wave front through that area. In humans, fractionated sinus rhythm electrograms are often recorded over a relatively wide area around an infarct (6.7). From the Division of Cardiology. Department of Internal Medicine. University of California at Los Angeles School of Medicine, Center for Health Sciences. Los Angeles. California. Manuscript received June 13. 1988: revised manuscript received Septem- ber 7. 1988. accepted September 25. 1988. Address for reorints: William G. Stevenson. MD. Division of Cardiology. University of California at Los Angeles. CHS 47-123. Los Angeles. California 90024. cc 1989 by the .4merican College of Cxddogy 0735.l097189153.50 These areas of slow conduction may be the substrate for intraventricular reentry causing ventricular tachycardia. However, fractionated electrical activity can result from motion of the recording catheter or activation of areas at a distance from the recording site (14-17). It is not possible in humans to directly measure myocardial conduction velocity in vivo. However, functional evidence of slow conduction during endocardial pacing, manifested as a delay between the pacing stimulus and the onset of the paced QRS com- plex, has been anecdotally reported in patients with right ventricular dysplasia (l&19), ventricular tachycardia after myocardial infarction (20), antiarrhythmic drug toxicity (21- 23) and hyperkalemia (24). The use of this technique to demonstrate slow intramyocardial conduction could poten- tially allow identification of sites where fractionated electro- grams are due to slow conduction. The purpose of this study was to systematically evaluate
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Fractionated endocardial electrograms are associated with slow conduction in humans: Evidence from...

JACC Vol. 13. No. 2 February IYR9:369-76
369
ELECTROPHYSIOLOGIC STUDIES
Fractionated Endocardial Electrograms Are Associated Conduction in Humans: Evidence From Pace-Mapping
WILLIAM G. STEVENSON, MD, FACC, JAMES N. WEISS, MD, FACC,
ISAAC WIENER, MD, FACC, S. MITCHELL RIVITZ, MD, FACC,
With Slow
KOONLAWEE NADEMANEE, MD, THOMAS KLITZNER. MD, LAWRENCE YEATMAN, MD,
MARTIN JOSEPHSON, MD, DANIEL WOHLGELERNTER, MD, FACC
Los Angeks, C~~l~f~~rnicr
Fractionated ventricular electrograms recorded during catheter mapping may arise from areas of asynchronous depolarization associated with slow conduction, the sub- strate for reentrant ventricular tachycardia, but can also be a nonspecific abnormality or even artifact. To determine whether fractionated sinus rhythm electrograms are asso- ciated with slow conduction in humans, the results of endocardial catheter mapping and pacing at 133 endocar- dial sites in 13 patients were analyzed. Eleven patients had sustained monomorphic ventricular tachycardia and two patients had old myocardial infarction without ventricular tachycardia.
Functional evidence of slow conduction at the recording site was assessed by pacing at that site and measuring the interval between the stimulus artifact (S) and the onset of the QRS complex in the 12 lead electrocardiogram (ECG). During pacing at 89 of 90 sites without fractionated sinus rhythm electrograms, the S-QRS interval was ~40 ms, a
value consistent with rapid propagation of the stimulated wave front away from the pacing site. During pacing at 21 (49%) of 43 sites with fractionated sinus rhythm electro- grams, the S-QRS interval was MO ms (range 40 to 140), consistent with slow conduction at the pacing site (p < 0.001 versus nonfractionated sites).
In 9 of the 11 patients with ventricular tachycardia analysis of the paced QRS configuration, electrograms during induced ventricular tachycardia or programmed stimulation during tachycardia suggested that a site with a long S-QRS interval during pacing was located at or near a ventricular tachycardia circuit. Therefore, fractionated si- nus rhythm electrograms are often associated with slow conduction, which may be the substrate for reentrant ventricular tachycardia. Endocardial pacing at these sites can be used to provide functional evidence of slow conduc- tion in humans.
(J Am CON Cardiol1989;13:369-76)
Fractionated ventricular electrograms are frequently re- corded from patients with ventricular tachycardia late after a myocardial infarction (I-IO). Studies (I l-13) in animal mod- els of myocardial infarction have shown that fractionated electrograms can result from asynchronous activation of muscle fibers at the recording site associated with slow propagation of the activation wave front through that area. In humans, fractionated sinus rhythm electrograms are often recorded over a relatively wide area around an infarct (6.7).
From the Division of Cardiology. Department of Internal Medicine. University of California at Los Angeles School of Medicine, Center for Health Sciences. Los Angeles. California.
Manuscript received June 13. 1988: revised manuscript received Septem- ber 7. 1988. accepted September 25. 1988.
Address for reorints: William G. Stevenson. MD. Division of Cardiology. University of California at Los Angeles. CHS 47-123. Los Angeles. California 90024.
cc 1989 by the .4merican College of Cxddogy 0735.l097189153.50
These areas of slow conduction may be the substrate for intraventricular reentry causing ventricular tachycardia. However, fractionated electrical activity can result from motion of the recording catheter or activation of areas at a distance from the recording site (14-17). It is not possible in humans to directly measure myocardial conduction velocity in vivo. However, functional evidence of slow conduction during endocardial pacing, manifested as a delay between the pacing stimulus and the onset of the paced QRS com- plex, has been anecdotally reported in patients with right ventricular dysplasia (l&19), ventricular tachycardia after myocardial infarction (20), antiarrhythmic drug toxicity (21- 23) and hyperkalemia (24). The use of this technique to demonstrate slow intramyocardial conduction could poten- tially allow identification of sites where fractionated electro- grams are due to slow conduction.
The purpose of this study was to systematically evaluate

370 STEVENSON ET AL. JACC Vol. 13, No. 2 SLOW CONDUCTION February 1989:369-76
Table 1. Clinical Characteristics of 13 Patients
Case Age (yr)/ Heart No. of VT Antiarrhythmic No. Gender Disease VT Configurations Drug at Study
I 74F Inf MI t 4 Amiod 2 63M Inf Ml t 4 Sotalol 3 54M Ant Ml t 2 Amiod 4 5OM Ant MI t 2 -
5 63F Ant MI t 4 Amiod t Mex 6 56M Inf MI t 2 -
7 48M Ant MI t 4 Amiod 8 55M Ant MI t I Proc 9 86M IDCM + 2 Amiod
10 8F Myocarditis t 2 - II 20F MVP t I - 12 46M Inf MI - - - I3 44M Inf MI - - -
I A
AVF
VI ---v--- 1 In”
LV 5-7 luFc
Figure 1. Recordings from Patient 1. From the top are 50 ms time (T) lines, surface ECG leads I, aVF and V, and intracardiac recordings from left ventricular site 5-7 (LV 5-7) and the right ventricular apex (RVAp). The electrogram at site 5-7 is markedly fractionated and has a duration of 240 ms.
Amiod = amiodarone; Ant = anterior: F = female: IDCM = idiopathic dilated cardiomyopathy; Inf = inferior; M = male: Mex = mexiletine; MI = myocardial infarction; MVP = mitral valve prolapse: Proc = procainamide: VT = ventricular tachycardia; t = present: - = absent.
the use of endocardial pacing for identifying areas of slow conduction during catheter mapping and to determine whether fractionated sinus rhythm electrograms are associ- ated with functional evidence of slow conduction in humans. As areas of slow conduction are the likely substrate for ventricular tachycardia, the relation of these areas to cath- eter mapping data in patients with ventricular tachycardia was also analyzed.
Methods Study patients. Thirteen patients undergoing endocardial
catheter mapping and programmed electrical stimulation were studied. Selected patient characteristics are listed in Table 1. Eight patients (Cases I to 8) had had multiple spontaneous episodes of sustained ventricular tachycardia late after a myocardial infarction and were referred for attempted surgical or catheter ablation of the arrhythmo- genie focus. Patient 9 had idiopathic dilated cardiomyopathy and recurrent ventricular tachycardia. Patient 10 had sus- tained ventricular tachycardia arising in an inferobasal left ventricular aneurysm resulting from an episode of myocar- ditis. Patient 11 had exercise- and isoproterenol-induced ventricular tachycardia and mitral valve prolapse with nor- mal ventricular wall motion. The remaining two patients had inferior wall myocardial infarction without spontaneous sus- tained ventricular tachycardia and were participating in a study of left ventricular catheter mapping approved by the Human Subject Protection Committee of this institution.
Electrophysiologic study. After informed consent was ob- tained, multipolar electrode catheters were inserted percu- taneously into femoral veins and a femoral artery. Catheters were positioned at the right ventricular apex, His bundle
position and in the left ventricle. Three to five surface electrocardiographic (ECG) leads were recorded simulta- neously with intracardiac electrograms at paper speeds of 100 to 150 mm/s on an Electronics for Medicine VR-12 chart recorder. Intracardiac electrograms were filtered at 30 to 500 Hz and recorded at a gain of 1 to 3 cm/mV. Full standard 12 lead ECGs were recorded at a paper speed of 25 mm/s (Marquette, Inc.) during stable induced ventricular tachycar- dias and ventricular pacing.
Progrrrmmed electrical stimulation was performed from the distal electrode pair of the desired catheter and during stimulation a bipolar electrogram was recorded from the proximal electrode pair of the pacing catheter. Ventricular stimuli with a pulse width of 2 ms were delivered by a programmable stimulator (Bloom Ltd.). The stimulation protocol for tachycardia initiation consisted of one, two and three extrastimuli delivered during sinus rhythm and paced ventricular drives at cycle lengths of 600, 500 and 400 ms from the right ventricular apex. The stimulus strength was twice the late diastolic threshold. One patient (case 8) required an intravenous isoproterenol infusion for tachycar- dia initiation.
Ventricular mapping. Endocardial mapping was per- formed with a 6F quadripolar catheter with I cm interelec- trode distances (USC& Catheter positions were verified by fluoroscopy in two planes and designated by the endocardial coordinates of Josephson et al. (25). Bipolar electrograms were recorded from the distal electrode pair and the proxi- mal electrode pair of the mapping catheter during sinus rhythm. Fractionated electrograms were defined as those having a duration >60 ms und multiple rapid low amplitude (co.5 mV) deflections (Fig. I). Immediately after the sinus rhythm electrogram was recorded and without repositioning the mapping catheter, bipolar ventricular pacing was begun with use of the distal electrode pair of the mapping catheter for stimulation. Pacing stimuli had an amplitude of IO mA and a pulse width of 2 ms. During pacing at a cycle length as

JACC Vol. 13, No. 2 STEVENSON ET AL. 371 February lYXY:36%7h SLOW CONDUCTION
close as possible to 600 ms, a 12 lead ECG was recorded. At sites where the paced ECG was concordant in QRS config- uration with an inducible or spontaneous sustained mono- morphic ventricular tachycardia, ventricular tachycardia was initiated by programmed stimulation before the mapping catheter was repositioned. We attempted to first evaluate several sites from areas with normal wall motion. To mini- mize the time required for mapping and limit repeated attempts to initiate and terminate ventricular tachycardia, we then concentrated on evaluating sites that had abnormal electrograms during sinus rhythm or ventricular tachycardia. To avoid repeated sampling from the same site. sites within approximately 2 cm of each other were not designated as separate sites and only one site from each such area was included in the analysis.
Assessing slow conduction. Evidence of slow conduction during pacing at the recording site was sought by measuring the interval between the stimulus artifact (S) and the earliest onset of the QRS complex on the surface ECG during continuous pacing at a cycle length as close as possible to 600 ms. The shortest S-QRS interval recorded from any of the 12 surface leads was measured to avoid the potential error introduced when the initial portion of the QRS complex was isoelectric in some leads. Only ECGs recorded at the 25 mm/s paper speed were analyzed because the QRS onset became more difficult to identify at faster paper speeds. The pacing cycle length of 600 ms was chosen to attempt to avoid obscuring the QRS onset by superimposition of the T wave from the preceding paced beat. Paced QRS complexes were considered concordant with a ventricular tachycardia QRS complex when the mean frontal plane and horizontal plane axis of the paced QRS differed by ~45” from that of ventricular tachycardia (26).
Statistics. Statistical comparisons were made with use of Student’s t test and chi-square tests. Bonferroni’s adjusr- ment for multiple comparisons was used as noted.
Results Fractionated electrograms. A total of 133 endocardial
sites were evaluated in the 13 patients (Table 2). A fraction- ated sinus rhythm electrogram was observed at 43 sites in 12 patients. No fractionated sinus rhythm electrogram was observed in Patient 11, whose only structural cardiac abnor- mality was mitral valve prolapse. Table 3 shows the number of sites according to the S-QRS interval during pacing. This interval was >40 ms (Fig. 2A) during pacing at 2 1 (49%) of 43 sites with but at only 1 of the 90 sites without a fractionated sinus rhythm electrogram (p < 0.001). The duration of the sinus rhythm electrograms increased with increasing S-QRS intervals although there was a great deal of overlap in electrogram duration between groups (Fig. 3).
Observations during ventricular tachycardia. In the I I patients with sustained ventricular tachycardia, electro-
Table 2. Characteristics of Endocardial Sites in 13 Patients
Sites With S-QRS Interval (ms)
Case Site5 Fractionated 40 to x0 10
No. Analyzed Electrogram <40 >40 79 II9 >I?0
I Y 4 7 2 0 I I 2 II IO 3 8 3 s 0 3 I 0 I 9 I 0 0 I 4 15 2 I’ 0 0 0 0
s 4 I 3 I 0 I 0 6 5 ? 3 7 I I 0
7 I7 7 I6 0 I 0 0
8 I2 5 Y 0 3 0 0
Y 17 6 IS 0 2 0 0
IO Y I 7 2 2 0 0
II I3 0 I3 0 0 0 II
I:! 6 I 6 0 0 0 0
I3 5 3 5 0 0 0 0
grams during induced monomorphic ventricular tachycardia were recorded at 58 of the pacing sites (mean of 6 + 3 sites in each patient) (Table 3). Sites with an S-QRS interval of 40 to 79. 80 to 119 and >I20 ms did not differ statistically from each other in the characteristics listed in Table 3. Therefore, all sites with an S-QRS interval >40 ms were combined for statistical comparison with sites having a paced S-QRS interval ~40 ms. During ventricular tachycardia presystolic electrical activity, occurring between the end of the QRS complex and the onset of the following QRS, or continuous electrical activity (8) spanning systole and diastole, was recorded at 86% of sites with an S-QRS interval >40 ms and at 32% of sites with an S-QRS interval ~40 ms (p = 0.001).
Concordance of the paced QRS configuration with the QRS configuration of inducible ventricular tachycardia (Fig. 2) was more frequent during pacing at sites with an S-QRS interval >40 ms (64%) than at sites with a shorter S-QRS interval (16%, p < 0.001).
During sustuined ventriurlur tuchycardia, programmed electrical stimulation was performed at 24 of the pace- mapping sites to attempt to assess the participation of the pacing site in the tachycardia circuit (20,271. Specifically, scanning premature stimuli or trains of stimuli, or both were delivered to the site to determine whether local capture at the pacing site could reset, entrain or terminate ventricular tachycardia without propagating widely to myocardium dis- tant from the pacing site. At three (38%) of eight sites that had a paced S-QRS interval >40 ms, electrical stimuli reset or entrained the ventricular tachycardia without altering the surface ECG QRS complex. After the stimulus, the QRS onset of the advanced tachycardia beat occurred after a delay of 80 to 400 ms, suggesting that the stimulation site was in or near an area of slow conduction that was participating in the reentrant circuit (20,27). Similar findings occurred during stimulation at only I of the 16 sites with a short paced

372 STEVENSON ET AL. JACC Vol. 13, No. 2 SLOW CONDUCTION February 1989:369-76
Table 3. Number of Endocardial Sites According to the S-QRS Interval During Pace-Mapping of Ventricular Tachycardia
<40
S-QRS Interval (ms)
40 to 80 to
>40 79 119 >I20 p Value*
Total sites III 22 I? 8 2
Electrogram
Fractionated 22 ?I II 8 2 <O.Ool Nonfractionated 89 I I 0 0
Concordance of VT and paced QRS I8 14 7 5 2 <O.Ool
Electrogram during VT Sites evaluated 44 I4 4 8 2 Continuous 2 6 0 4 2 0.02 Presystolic or continuous I4 I2 2 8 2 0.001
*p values are for comparison of column I (sites <40 ms) with column 2 (all sites >40 ms). With use of the
Bonferroni adjustment for multiple comparisons. a value of 0.0125 indicates a 0.05 significance level (alpha).
S-QRS interval during pace mapping (p = 0.17 compared with sites with an S-QRS interval >40 ms).
Discussion Mechanism of fractionated electrograms. The mechanism
and significance of fractionated electrograms recorded dur- ing catheter mapping in humans have not been fully eluci- dated. Ideker et al. (14) demonstrated that high gain record- ing from a sponge on the surface of the heart could produce fractionated electrograms. Waxman and Sung (16) found that the interelectrode distance and filter settings influenced the presence of fragmented electrograms, which appeared to be unrelated to induced ventricular tachycardia. Although frac- tionated electrograms can be artifacts of the recording tech- nique, a well established association exists between the presence of fractionated electrograms recorded during cath- eter and intraoperative mapping and the occurrence of spontaneous and inducible sustained ventricular tachycardia in patients surviving a myocardial infarction (l-7). These electrograms are the likely source of the low amplitude, high frequency late potentials that can be recorded with high gain surface ECG techniques and are also associated with the occurrence of ventricular tachycardia (28-31). In canine models of myocardial infarction, several investigators (I l- 13) have provided evidence that fractionated electrograms are due to asynchronous activation of myocardial fibers at the recording site and are associated with slow conduction through these areas. Because slow conduction is critical for the occurrence of intraventricular reentry, fractionated elec- trograms may identify areas of slow conduction that give rise to reentrant ventricular tachycardia in humans (2-4,8). However, several investigators (16,32-34) have shown that fractionated electrograms and continuous electrical activity recorded during ventricular tachycardia can be independent of the tachycardia; apparently they arise from sites separate from the tachycardia circuit or are due to artifact.
Fractionated electrograms and areas of slow conduction. Our study provides evidence that fractionated electrograms are associated with areas of slow conduction in humans. Because it is not possible to measure myocardial conduction velocity with current catheter techniques, we relied on the functional demonstration of slow conduction during ventric- ular pacing. In both animal models and humans, fractionated electrograms are generally of very low amplitude. Pacing from within these areas gives rise to a wave front of depolarization, which propagates away from the pacing site but is not detectable on the surface ECG until it reaches myocardial tissue that generates a signal of greater amplitude due to the more rapid depolarization of a larger mass of myocardium. Therefore, the interval between the pacing stimulus artifact and the onset of the QRS complex is a crude indication of conduction velocity away from the pacing site. Our findings support this hypothesis. During pacing in nor- mal ventricular myocardium, the onset of the paced QRS complex immediately followed the stimulus artifact. In con- trast to normal sites, a distinct interval of 40 to 140 ms was observed between the stimulus artifact and the QRS onset during pacing at 49% of endocardial sites that had fraction- ated sinus rhythm electrograms. These long S-QRS intervals are not due to an initial isoelectric component of the QRS complex, which can occur when the initial QRS forces are oriented perpendicular to the axis of the recording elec- trodes, because all 12 ECG leads were recorded during stable continuous pacing. Latency between the stimulus and depolarization at the stimulation site is also an unlikely explanation as delays of up to 140 ms between the stimulus artifact and the QRS onset were observed. Similar findings have been obtained in the presence of high levels of anti- arrhythmic drugs (21-23) and hyperkalemia (24), both of which slow myocardial conduction.
Slow conduction and ventricular tachycardia. Slow con- duction is the likely substrate for reentrant ventricular
JACC Vol. 13. No. 2 February 1989:369-76
STEVENSON ET AL. 373 SLOW CONDUCTION
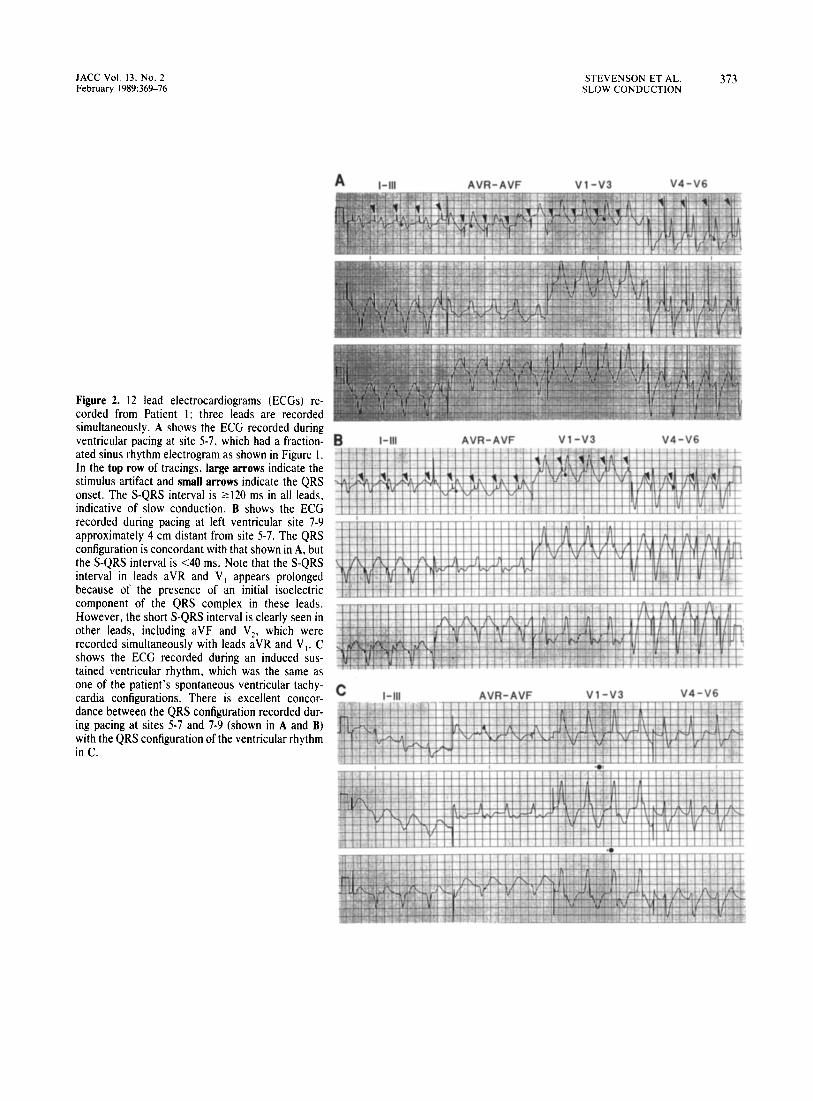
Figure 2. 12 lead electrocardiograms (ECGs) re- corded from Patient 1; three leads are recorded simultaneously. A shows the ECG recorded during ventricular pacing at site 5-7, which had a fraction- ated sinus rhythm electrogram as shown in Figure I. In the top row of tracings, large arrows indicate the stimulus artifact and small arrows indicate the QRS onset. The S-QRS interval is ~120 ms in all leads, indicative of slow conduction. B shows the ECG recorded during pacing at left ventricular site 7-9 approximately 4 cm distant from site 5-7. The QRS configuration is concordant with that shown in A, but the S-QRS interval is ~40 ms. Note that the S-QRS interval in leads aVR and V, appears prolonged because of the presence of an initial isoelectric component of the QRS complex in these leads. However, the short S-QRS interval is clearly seen in other leads, including aVF and VI, which were recorded simultaneously with leads aVR and V,. C shows the ECG recorded during an induced sus- tained ventricular rhythm, which was the same as one of the patient’s spontaneous ventricular tachy- cardia configurations. There is excellent concor- dance between the QRS configuration recorded dur- ing pacing at sites 5-7 and 7-9 (shown in A and B) with the QRS configuration of the ventricular rhythm in C.
A I-111 AVR-AVF Vl-v3 V4-V6
B I-III AVR-AVF Vl -v3 V4-V6
C I-111 AVR-AVF Vl-v3 V4-V6

374 STEVENSON ET AL. JACC Vol. 13, No. 2 SLOW CONDUCTION February 1989:369-76
Figure 3. Graph of the S-QRS interval during pacing (abscissa) versus the sinus rhythm (SR) electrogram (EG) duration (ordinate). All measurements are in milliseconds. Linear regression demon- strated a relation between the electrogram duration and the S-QRS interval during pacing at the recording site (r = 0.61, p < 0.01).
tachycardia (l-8,11-13). Catheter techniques are limited in their ability to precisely localize reentrant circuits and intraoperative mapping with electrode arrays, which allow simultaneous recording from multiple sites, will likely be required to firmly establish whether areas of slow conduc- tion identified by pacing participate in ventricular reentrant circuits. However, we observed several findings suggesting that some of the areas of slow conduction identified by pacing were involved in ventricular reentrant circuits. Sites with a long S-QRS interval more frequently had presystolic electrical activity and continuous electrical activity (8,17) recorded during ventricular tachycardia as compared with sites with a short S-QRS interval. The QRS configuration recorded during pacing at sites with a long S-QRS interval was frequently concordant with a ventricular tachycardia QRS configuration. At three sites with a long paced S-QRS interval, electrical stimuli were able to reset or entrain the tachycardia without propagating widely to the surrounding myocardium, suggesting that the site was in or near the tachycardia circuit (20,27). However, it should be recog- nized that some areas of slow conduction detected during pacing may not participate in a reentrant circuit. Such “bystander” areas of slow conduction have been hypothe- sized to be responsible for fractionated early diastolic elec- trograms and continuous electrical activity recorded during ventricular tachycardia, which appeared to be independent of the tachycardia circuit (32-34). At five of eight sites with a long S-QRS interval during pace-mapping, pacing during ventricular tachycardia failed to alter the tachycardia, sug- gesting that the site did not participate in the tachycardia circuit (20,27). Although at some sites this could be due to failure of premature stimuli to capture during tachycardia, it is also consistent with the presence of “bystander” areas of slow conduction.
Previous studies (35-37) of pace-mapping for localizing ventricular tachycardia foci have focused on comparing the paced QRS configuration to the QRS configuration during
ventricular tachycardia (35-37). Although the S-QRS inter- val was not mentioned, examples of long S-QRS intervals were shown in some of these reports (Fig. 10 in reference 35 and Fig. 3 in reference 37). Comparing the results of pace- mapping with the analysis of electrograms recorded during ventricular tachycardia, Josephson et al. (35) observed that these two mapping techniques often suggested disparate sites of tachycardia origin in the same patient. It is likely that combining analysis of the paced QRS configuration with the assessment of slow conduction from the S-QRS interval may improve the utility of pace-mapping for localizing reentrant circuits.
Limitations. Although the number of patients studied was small, the relation of fractionated electrograms to long S-QRS intervals was striking. Antiarrhythmic drugs could not be withdrawn before study in seven of our patients because of the refractory nature of their ventricular tachy- cardia. These drugs (amiodarone, sotalol and mexiletine) do not have prominent effects on conduction velocity in normal ventricular myocardium during slow heart rates (38-40). We cannot exclude the possibility that they contributed to slow- ing of conduction in abnormal areas. However, long S-QRS intervals of 40 to 80 ms were observed in two patients with ventricular tachycardia (Patients 6 and 10) who were studied in the drug-free state. Also, 89 of 90 sites that did not have a fractionated electrogram during sinus rhythm had a short S-QRS interval during pacing regardless of the presence or absence of antiarrhythmic drugs.
The ECG did not demonstrate evidence of slow conduc- tion during pacing at 51% of sites that had a fractionated sinus rhythm elecrrogram. Although these fractionated elec- trograms may be due to artifact or asynchronous ventricular activation without associated slow conduction, it is likely that our methods do not exclude the presence of slow conduction at these sites. Pacing at an area of slow conduc- tion could theoretically produce a short S-QRS interval if the area of slow conduction were relatively small or the pacing site were located at the edge of the abnormal area. The stimulated wave front may then propagate slowly, but traverse only a short distance before reaching more normal myocardium. We used pacing stimuli with an amplitude of 10 mA to facilitate identification of the stimulus artifact on the surface ECG and to reduce the time required for perform- ance of the study. It is possible that these stimuli depolarized a larger area than would have occurred with lower amplitude stimuli, shortening the S-QRS interval at some sites. How- ever, a preliminary report (41) examining the effect of stimulus strength on intraventricular conduction times dur- ing pacing at normal and abnormal endocardial sites found no decrease in conduction time until stimulus strength was increased to >lO mA. Finally, it is also possible that slow conduction at some sites occurs only at fast heart rates or in response to a premature stimulus (18,42). Pacing at the relatively slow cycle length of 600 ms may fail to identify

JACC Vol. 13. No. 2 STEVENSON ET AL. 375 February 1989:36%X SLOW CONDUCTION
some areas in which conduction is slow during ventricular tachycardia.
Implications. Areas of slow conduction may be the crit- ical substrate for reentrant ventricular tachycardia. Analysis of the stimulus to QRS interval during endocardial electrical pacing can provide functional evidence of slow conduction at sites that have a fractionated sinus rhythm electrogram and can be easily performed during catheter mapping. This information may be a useful adjunct to analysis of sinus rhythm electrograms and the paced QRS configuration for rapidly assessing the probability that a site could be involved in a tachycardia circuit without initiating ventricular tachy- cardia. As catheter mapping can be a difficult, lengthy procedure, these methods may assist in quickly focusing attention on the sites most likely to participate in the tachycardia circuit. These sites can then be more extensively evaluated during induced ventricular tachycardia. Whether this result will facilitate localization of sites for successful catheter ablation remains to be determined (20).
I.
2.
3.
4.
5.
6
7.
8.
9.
IO.
References Wiener 1. Mindich B. Pitchon R. Determinants of ventricular tachycardia in patients with ventricular aneurysms: results of intraoperative epicardial and endocardial mapping. Circulation 1982:65:856-661.
Klein H, Karp RB. Kouchoukos NT. Zorn CL. James TN. Waldo AL. lntraoperative electrophysiologic mapping of the ventricles during sinus rhythm in patients with a previous myocardial infarction: identification of the electrophysiologic substrate of ventricular arrhythmias. Circulation 1982:66:847-53.
Wiener 1. Mindich B. Pitchon R. Fragmented endocardial electrical activity in patients with ventricular tachycardia: a new guide to surgical therapy. Am Heart J 1984:107:8690.
Kienzle MG, Miller J. Falcone RA, Harken A, Josephson ME. Intraop- erative endocardial mapping during sinus rhythm: relationship to site of origin of ventricular tachycardia. Circulation 1984;70:957-65.
Josephson ME, Simson MB. Harken AH. Horowitz LN. Falcone RA. The incidence and clinical significance of epicardial late potentials in patients with recurrent sustained ventricular tachycardia and coronary artery disease. Circulation 1982:66: 1199-204.
Cassidy DM, Vassallo JA. Buxton AE. Doherty JU. Marchlinski FE. Josephson ME. The value of catheter mapping during sinus rhythm to localize site of origin of ventricular tachycardia. Circulation 1984:69: 1103-10.
Cassidy DM, Vassallo JA, Miller JM, et al. Endocardial catheter mapping in patients in sinus rhythm: relationship to underlying heart disease and ventricular arrhythmias. Circulation 1986;73:645-52.
Josephson ME, Horowitz LN, Farshidi A. Continuous local electrical activity: a mechanism of recurrent ventricular tachycardia. Circulation 1978;57:65%5.
Untereker WJ. Spielman SR. Waxman HL. Horowitz LN. Josephson ME. Ventricular activation in normal sinus rhythm: abnormalities with recurrent sustained tachycardia and a history of myocardial infarction. Am J Cardiol 1985;55:974-9.
Fontaine G. Guiraudon G, Frank R. lntramyocardial conduction defect5 in patients prone to ventricular tachycardia. 111. The post-excitation syndrome in ventricular tachycardia. In: Sandoe E, Julian DG. Bell JW. eds. Management of Ventricular Tachycardia: Role of Mexilitine. Am- sterdam: Excerpta Medica. 1978:67-79.
I I. Gardher PJ. Ursell PC, Fenoglio JJ, Wit AL. Electrophysiologic and anatomic basis for fractionated electrograms recorded from healed myo- cardial infarcts. Circulation 1985:72:596-661 I.
12. Richards DA. Blake GJ, Spear JF. Moore EN. Electrophysiologic sub- strate for ventricular tachycardia: correlation of properties in vivo and in vitro. Circulation 1984:69:369-8 I.
13. Kienzle MG. Tan RC. Ramza BM. Young ML, Joyner RW. Alterations in endocardial activation of the canine papillary muscle early and late after myocardial infarction. Circulation 1987:76:86&74.
14. Ideker RE. Lofland GK. Bardy GH. et al. Late fractionated potentials and continuous electrical activity caused by electrode motion. PACE 198316: 980-94.
15. Gallagher JJ. Kasell JH, Cox JL, Smith WM. ldeker RE. Smith WM. Techniques of intraoperative electrophysiologic mapping. Am J Cardiol 1982:49:X1-40.
16. Waxman HL. Sung RJ. Significance of fragmented ventricular electro- grams observed using intracardiac recording techniques in man. Circula- tion 1980162: 1349-56.
17. Josephson ME. Wit AL. Fractionated electrical activity and continuous electrical activity: fact or artifact. Circulation 1984:70:529-32.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32
Fontaine G. Guiraudon G. Frank R. Intrdmyocardial conduction defects in patients prone to ventricular tachycardia. 111. A dynamic study of the post-excitation syndrome. In: Ref. IO: 56.66.
Frank R. Fontaine G. Vedel J. et al. Electrocardiologie de 4 cas de dysplasie ventriculaire droite arythmogene. Arch Mal Coeur 1978:71:963- 71.
Stevenson WG. Weiss J. Wiener 1. Wohlgelernter D, Yeatman L. Localization of slow conduction in a ventricular tachycardia circuit: implications for catheter ablation. Am Heart J 1987:114:1253-8.
Gay RJ. Brown DF. Pacemaker failure due to procainamide toxicity. Am J Cardiol 1974:34:728-32.
Mehta J. Khan AH. Pacemaker Wenckebach phenomenon due to anti- arrhythmic drug toxicity. Cardiology 1976:61:189-94.
Moss AJ. Goldstein S. Clinical and pharmacological factors associated with pacemaker latency and incomplete pacemaker capture. Br Heart J 1969:31:112-7.
Varriale P. Manolis A. Pacemaker Wenckebach secondary to variable latency: an unusual form of hyperkalemic pacemaker exit block. Am Heart J 1987:114:189-92.
Josephson ME, Horowitz LN, Spielman SR. Waxman HL, Greenspan AM. Role of catheter mapping in the preopertive evaluation of ventricular tachycardia. Am J Cardiol 1982:49:207-20.
Wilber DJ. Davis MJ, Rosenbaum M. Ruskin JN, Garan H. Incidence and determinants of multiple morphologically distinct sustained ventricular tachycardias. J Am Coll Cardiol 1987:10:583-91.
Stevenson WG. Weiss JN. Wiener I. et al. Resetting of ventricular tachycardia: implications for localizing the area of slow conduction. J Am Coll Cardiol 1988: I I :522-9.
Rozanski JJ, Mortara D. Myerburg RJ. Castellanos A. Body surface detection of delayed depolarizations in patients with recurrent ventricular tachycardia and left ventricular aneurysm. Circulation 1981:63: 1172-8.
Simson MB. Use of signal in the terminal QRS complex to identify patients with ventricular tachycardia after myocardial infarction. Circu- lation 1981:64:235-42.
Vassallo JA. Cassidy D, Simson MB, Buxton AE, Marchlinski FE, Josephson ME. Relation of late potentials to site of origin of ventricular tachycardia associated with coronary heart disease. Am J Cardiol 1985:55:985-9.
Simson MB, Untereker WJ, Spielman SR. et al. Relation between late potentials on the body surface and directly recorded fragmented electro- grams in patients with ventricular tachycardia. Am J Cardiol 1983:51: IOS- 12.
Brugada P, Abdollah H, Wellens HJJ. Continuous electrical activity during sustained monomorphic ventricular tachycardia. Observations on

376 STEVENSONETAL. SLOWCONDUCTION
JACC Vol. 13. No. 2 February 1989:369-76
its dynamic behavior during the arrhythmia. Am J Cardiol 1985:55:402- ventricular tachycardia with intracardiac shocks: results in 33 patients. II. Circulation 1987:75:1037-49.
33. Miller JM. Vassallo JA. Hargrove WC, Josephson ME. Intermittent failure of local conduction during ventricular tachycardia. Circulation 1985;72:1286-92.
34. Gessman LJ, Agarwal JB, Helfant RH. Specificity of continuous electri- cal activity in locating the site of reentry in ventricular tachycardia (abstr). Am J Cardiol 1982;49:956.
38. Singh BN. Amiodarone: historical development and pharmacological profile. Am Heart J 1983:106:788-97.
39. Rosen RM, Wit A. Electropharmacology of antiarrhythmic drugs. Am Heart J 1983:106:829-39.
35. Josephson ME. Waxman HL. Cain ME. Gardner MJ. Buxton AE. Ventricular activation during ventricular endocardial pacing. Role of pace-mapping to localize origin of ventricular tachycardia. Am J Cardiol 1982;50: I l-22.
40. Singh BN, Vaughn-Williams EM. A third class of antiarrhythmic action: effects on atrial and ventricular intra-cellular potentials, and other phar- macologic actions on cardiac muscle of MJ 1999 and AH 3474. Br J Pharmacol 1970;39:675-85.
36. Waxman HL. Josephson ME. Ventricular activation during ventricular endocardial pacing. 1. Electrocardiographic patterns related to the site of pacing. Am J Cardiol 1982;50: I-IO.
41. Meesman M, Marchlinski FE. Effect of pacing site and current strength on indices of ventricular activation in man (abstr). Circulation 1987;76: (suppl IV):IV-281.
37. Morady F, Scheinman MM. Di Carlo L. et al. Catheter ablation of
42. El-Sherif N, Scherlag BJ, Lazzara R, Hope RR. Re-entrant ventricular arrhythmias in the late myocardial infarction period. 1. Conduction characteristics in the infarction zone. Circulation 1977;55:686-702.


















