Offset femoral en los resultados clínicos y funcionales de los ...
Upload
independentCategory
view
2download
0
Single Center Experience with FemoralExtraction of Permanent EndocardialPacing Leads
MOUSTAPHA JARWE, DIDIER KLUG, JEAN PAUL BEREGI, PIERRE LE ERANG,DOMINIQUE LAGROIX, GLAUDE KOUAKAM, LAURENGE GUEDON-MOREAU,NAZIH ZGHAL, and SALEM KAGET
From theiLille University Hospital, Lille^France]
JARWE, M., ET AL.: Single Center Experience with Femoral Extraction of Permanent Endocardial PacingLeads..Between March 1995 and June 1997, 128 leads were extracted from the hearts of 28 women and 50men, 69 ± 15 years of age (mean ± SD, range 22-92 years). The indications for the procedure were: Ac-cufixleadsin 18 patients (14%), dysfunction or incompatibility with ICD in 16(12%), endocarditis on thelead in 41 (32%), pulse generator pocket infection in 28 (22%), and pulse generator and/or lead erosionin 25 patients (19%). The extraction was performed with a snare (lasso), via a femora! vein as a first ap-proach in 116 leads, and as an alternate approach, after extraction from the original site of implantationhad failed, in 12 leads. The leads had been implanted for 62 ± 48 months (range 1-205 months). A Cooksheath was used in 7, and a femoral approach traction in 20 instances. Of the 128 leads, 122 (95%) werecompletely extracted, and 2 (2%) were partially extracted (the distal electrode remaining attached to themyocardium), and 4 (3%) could not be removed. Four complications occurred: 2 tears of the tricuspidvalve without clinical consequences, one separation of the lead's distal electrode which migrated into thehypogastric vein, and one hemorrhage at the femoral puncture site. There was no death or serious com-plication caused by lead extraction in this series. (PACE 1999; 22:1202-12091
pacemaker, lead extraction, pacing complications
Introduction
Pacing lead extraction is a technically chal-lenging and risky procedure, to which cliniciansare increasingly exposed, as a result of infectiouscomplications, growing number of leads im-planted per patient, and lead aging.^ Percutaneouslead extraction from the implant vein (upper ap-proach), or from the femoral vein (femoral ap-proach) is used most frequently.^'^ The successand complications rates of the upper approachhave been reported in several puhlications,*"^while those of the femoral approach are less wellknown.^ The aim of this study was to examine theresults of a consecutive series of pacemaker lead
Address for reprints: Moustapha |arwe. M.D., Service de Car-diologie A, Hopital cardioiogique de Lille, Boulevard du PrLeclercq, CHR-U 59037 Lille, France. Fax: (33) 3 20 44 68 98.
Received March 5, 1998; revised October 26, 1998; acceptedNovember 13, 1998,
extractions performed via the femoral approach ata single medical center. We hypothesized that anassessment of the success rate of this extractiontechnique and, perhaps more importantly, of therate and seriousness of its complications would fa-cilitate an estimation of its risk-benefit ratio andhelp to hetter define its indications.
Materials and Methods
Between March 1995 and June 1997. 128 leadextractions were performed at the Lille UniversityMedical Center. The procedure was performed viaa femoral vein as a first approach in 116 leads and,as an alternate approach after extraction from theoriginal site of implantation had failed, in 12leads.
Twenty-eight women and 50 men, 69 ± 15years of age (range 22-92 years), referred fromother hospitals to our tertiary center for lead ex-traction or management of lead infection, under-went the procedure. Twenty-nine patients had 1
1202 August 1999 PACE, Vol. 22

FEMORAL EXTRACTION OF PACING LEADS
Table 1.
Indications for Pacemaker Lead Extraction
Indications
Ctass 1~ Lead endocarditis- Accufix lead
Class tt
- PG pocket infection- PG and/or iead erosion- Lead dysfunction or IGD incompatibiiity
and> 2 ieads across the TV
N (%)
41 (32)18(14)
28 (22)25(19)
16(13)
ICD = implantabie cardioverler defibrillator; N = number ofleads; PG = pulse generator; TV = tricuspid valve.
previously implanted lead, 33 had 2, and 11 had 3leads.
Procedural Indications
The indications for lead extraction, pre-sented in Tahle I, fell into two classes. Class Iindications included endocarditis on the leadand Accufix (Telectronics Inc., Englewood, CO,USA) lead fracture with or without wire protru-sion, where all percutaneous, and, if necessary,surgical extraction methods, including car-diopulmonary hypass, were considered. Class IIindications included pulse generator pocket in-fection, pulse generator, and/or lead erosion, andlead dysfunction in presence of more than twoleads across the tricuspid valve, where the pro-cedure was limited to percutaneous extractionattempts.
This series included 41 Class I, and 87 Class IIindications.
Indications for Extraction Via the FemoralApproach
The femoral approach was the technique offirst choice:
1. in cases of septic complications at thepulse generator site, to allow bacteriological testsof the lead tip without contaminating it by itswithdrawal through the pulse generator pocket
2. to remove Accufix leads3. to extract leads which had migrated into
the venous system, the proximal end of whichcould not he reached
4. at the physician's discretion, to circum-vent scar tissue, often responsihle for failures toextract the lead via the implant vein
In the remaining cases, the femoral approachwas chosen after failure of lead extraction hy theupper approach.
Lead Characteristics
The average lead implantation time was 62 ±48 months (range 1-205 months); 16% had beenimplanted for < 12 months, 8% between 13 and 24mouths, 33% between 25 and 36 months, and 43%had been implanted for > 60 months. The charac-teristics of the leads are presented in Tahle II. Thevessel used as the original access was the left sub-clavian vein in 32 leads, right suhclavian in 17, leftcephalic in 9, right cephalic in 16, left external jugu-lar in 1, right external jugular in 6, left internal jugu-lar in 1, and right internal jugular vein in 3 leads.
Instrumentation
The following instruments were used to per-form the procedures: (1) Snare extractor {lasso,
Site
RVRA
n
7157
Active
10 ieads55 ieads
Leads
Passive
61 ieads2 ieads
Table II.
Gharacteristics
Unipolar
26 leads7 leads
Bipolar
45 leads50 ieads
3.2 mm
58 ieads53 ieads
5-6 mm
13 leads4 leads
Site ^ site of iead impiantation; n = number of ieads; active versus passive = type of fixation; unipolar versusbipolar = iead polarity; 3.2 versus 5-6 mm = pacemaker connector size; RV = Right ventrioie; RA = Rightatrium.
PACE, Vol, 22 August 1999 1203

JARWE, ETAL.
PM lead
Snare
ig Tai
Figure 1. Example of femoral approach traction. Apigtail is introduced in tbe left femoral vein tbrougb a 7Fr introducer, and a snare is introduced in the rightfemoral vein through a 14 Fr introducer. While thepigtail forms a loop wif/i tbe lead body at tbe level of tberigbt atrium, the distal tip of tbe pigtail is seized witbthe snare sucb tbat the pigtail-snare assembly forms abridge above the body of tbe lead. Wbile retaining tbelead at tbe implant site to prevent its movement at tbatlevel, traction is applied downward until tbe lead isdetacbed from its endocardial fixation site.
TFE Catheter. Cook Corp., Leechburg, PA, USA);(2) 6 Fr 110-cm Pigtail (Cordis Johnson & JohnsonCorp., Leechburg. PA, USA); and (3) Cook dilationsheaths (Byrd Dilator Sheath Set, Cook Corp.)
Definitions
A femoral approach defines any lead extrac-tion using the insertion of a 14 Fr introducer intoa femoral vein in order to recover the lead with asnare, once it has heen separated from its point offixation.
A femoral approach traction defines any tech-nique using tools introduced into the femoral in-troducer in order to separate the lead from its fix-ation point or from adhesions when simpletraction was not sufficient (Fig. 1).
Surgical Procedure
Before any extraction procedure, the lead lo-calization, type, and fixation system were noted.
A chest radiograph and a transthoracic or trans-esophageal echocardiogram, depending on the ex-traction indication, were performed, as well as anupper limh venogram to verify the patency of theimplant vein. The patient's chest and femoral areawere prepped. The procedure was performed un-der local anesthesia, in an operating roomequipped with standard cardiopulmonary resusci-tation equipment.
Temporary pacing was prepared for the inter-vention in pacemaker dependent patients only,identified on the basis of the original pacing indi-cation, and after several days of monitoring duringVVI pacing programmed at a backup rate of 40beats/min. In case of lead infection, an epicardialpacing system was implanted via subxiphoid ap-proach hefore the extraction procedure. In theother cases, pacing was ensured by a temporary 6Fr bipolar endocardial lead introduced via afemoral sheath.
The procedure consisted of four consecutivesteps.
Step 1
Introduction of a 14 Fr introducer with hemo-static valve into the right femoral vein and injec-tion of heparinized saline solution through thevalve to prevent thrombus formation within thesheath.
Step 2
Proximal liberation of the lead. The pulsegenerator pocket was surgically explored and thelead disconnected from the pulse generator, thenliberated from its extravascular adhesions. A rigidnonlocking stylet supplied by the lead manufac-turer, of appropriate length for the lead, was intro-duced into the lead body in order to stiffen it. Inseven lead extractions, in the beginning of our ex-perience, a Cook dilating set was used in presenceof endovenous fibrotic tissue or venous thrombuspreventing proximal freeing of the lead. There-after, the femoral approach traction was used as afirst maneuver instead of Cook dilating sheaths.
Step 3
Distal detachment: detachment of the leadfrom its distal fixation site was performed by ex-erting constant and gradual traction on the proxi-
1204 August 1999 PACE. VoL 22

FEMORAL EXTRACTION OF PACING LEADS
mal end of the lead. If this maneuver remainedunsuccessful, traction was applied from thefemoral approach.
Step 4
Lead recovery: once the lead was detachedfrom the endocardium, its distal tip was posi-tioned in the upper half of the right atrium and en-trapped by the snare loop; the proximal lead seg-ment was severed at the implant vein, and theremaining portion was extracted through thefemoral vein (Fig. 2). The proximal and distal ends
ofthe leads were then sent for microbiological ex-aminations.
In situations where the proximal end of a cutlead had migrated into the venous system, a pig-tail and snare were used to bring the proximal endof the lead down to the level of the inferior venacava. The lead was then freed from its distal fixa-tion hy traction on its proximal end with thesnare.
Fotlow-Up
Chest radiographs and transthoracic echocar-diography were performed within 24 hours after
Snare Snare
PM lead
Figure 2. Steps of lead recovery witb a snare duringextraction by the femora! approach. (A) Tbe distal tip oftbe lead is positioned in tha upper half of the rightatrium; tbe snare is tben opened to grasp tbe lead. (B)Tbe lead is caugbt by tbe snare. (C) Tbe lead is pulledtbrougb tbe inferior vena cava (left), then tbrougb tbefemora! vein, to be finally recovered tlirougb a 14 Frfemoral sheath (rigbt).
PACE, Vol. 22 August 1999 1205

lARWE, ET AL.
extractions of the leads, and the patients wereseen in the outpatient clinic 6—8 weeks after theirdischarge from the hospital. Particular attentionwas paid to the possible presence of physical find-ings of venous thrombosis. Venography was notperformed systematically.
Statistical Analysis
Data were analyzed by Student's paired f-test for continuous variables, and the chi-squaretest and Fischer's exact test for discontin-uous variables. A P value < 0.05 was consideredsignificant.
Results
One hundred and twenty-eight leads wereextracted from 78 patients. The average proce-dure time was 101 ± 56 minutes (range 30-300min), with an average fluoroscopy time of 25 ±19 minutes/lead (range 3-98 min). On 20 occa-sions (16 ventricular leads and 4 atrial leads)traction from the femoral approach was used tofree the leads from surrounding fibrotic tissue.The Cook instrumentation, consisting of two di-lation sheaths, was used for six ventricular andone atrial lead. This technique was used in theheginning of our experience in presence oftightly stenotic or thrombotic suhclavian veins.Passage through these obstacles was not possibleand associated with unacceptable patient dis-comfort. Inferior traction was performed as an al-ternate maneuver in these patients, and weresucccessful in six cases and unsuccessful inone. From then on, extraction via the femoralapproach became the technique of first choice,whenever simple proximal traction had failed
Table Ml.
Additional Instrumentation Used According to the LeadImplantation Site
SiteTraction from the CookFemoral Approach Sheath
Ventricular (71 leads)Atrial (57 leads)
164
(Table III). The leads for which a femoral ap-proach traction (as first or second choice) wasnecessary had been implanted for 93 ± 59months compared with 59 ± 44 months for theleads which required no special instrumenta-tion (P - 0.001, Table IV).
Ultimately, 122 leads were extracted, repre-senting a complete success rate of 95%. Successwas considered partial for two leads (2%), the dis-tal electrode of which was left attached to the en-docardium after removal of the entire remainderof the lead. Four leads (3%) could not be ex-tracted despite the use of femoral traction in eachcase, preceded, in 1 case, by the use of dilationsheaths. It is noteworthy that among these fourfailures, three patients had a subclavian veinthrombosis.
The lead characteristics, in relation to the ex-traction results, are summarized in Table V. Itshould be noted that all failures occurred withpassive fixation ventricular leads, and the twopartial successes with active fixation atrial leads.However, differences with respect to lead implan-tation site or fixation type were not statisticallysignificant (P = 0.055).
Table IV.
Additional Instrumentation Used According to Duration ol
NonePigtailCook sheath
Number(n)
10120
7
Polarityf Lead Implantation, Type of Fixation, and
Average Lead Age Active Fixation Passive(months)
59 ± 4 493 ± 5 969 ±25
(n) Fixation (n)
58 435 152 5
Unipolar(n)
3030
1206 August 1999 PACE, Vol. 22
FEMORAL EXTRACTION OF PACING LEADS
Ventricular leads
Atrial leads
Complications
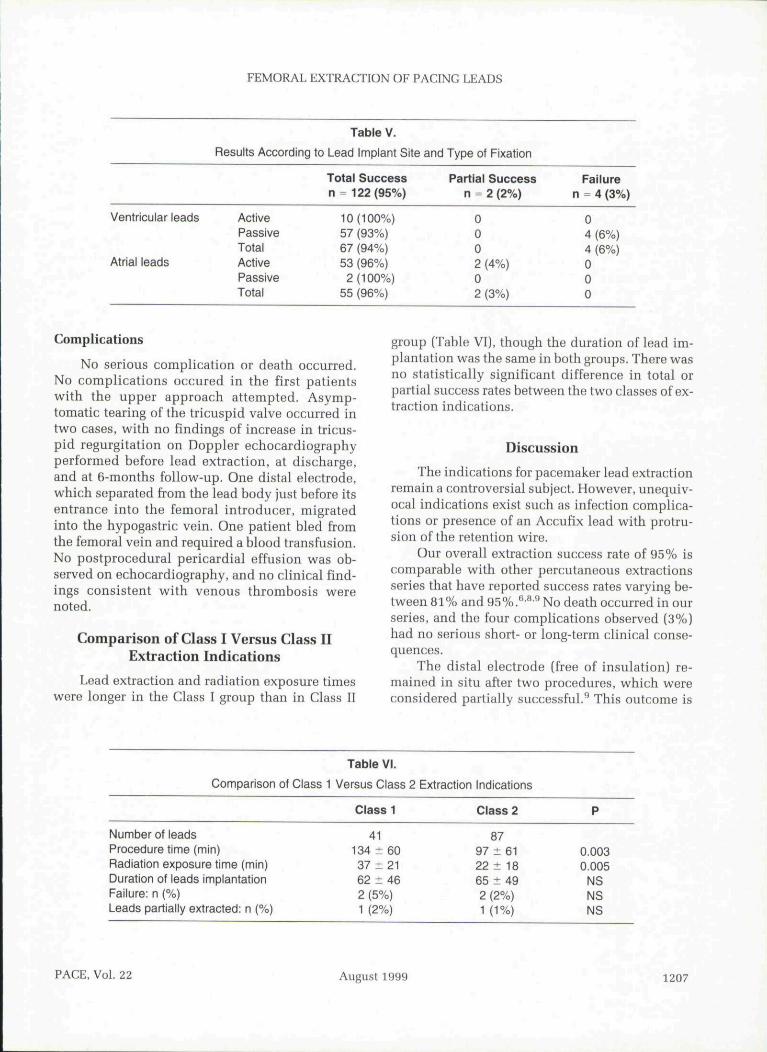
Results According
ActivePassiveTotalActivePassiveTotal
Table V.
to Lead Implant Site
Total Successn = 122(95%)
10(100%)57 (93%)67 (94%)53 (96%)2(100%)
55 (96%)
sroui
and Type of Fixation
Partial Successn = 2 (2%)
0,002 (4%)02 (3%)
3 (Table VII. thoueh the
Failuren - 4 (3%)
04 (6%)4 (6%)000
duration o
No serious complication or death occurred.No complications occured in the first patientswith the upper approach attempted. Asymp-tomatic tearing of the tricuspid valve occurred intwo cases, with no findings of increase in tricus-pid regurgitation on Doppler echocardiographyperformed hefore lead extraction, at discharge,and at 6-months foUow-up. One distal electrode,which separated from the lead body just before itsentrance into the femoral introducer, migratedinto the hypogastric vein. One patient bled fromthe femoral vein and required a blood transfusion.No postprocedural pericardial effusion was oh-served on echocardiography, and no clinical find-ings consistent with venous thromhosis werenoted.
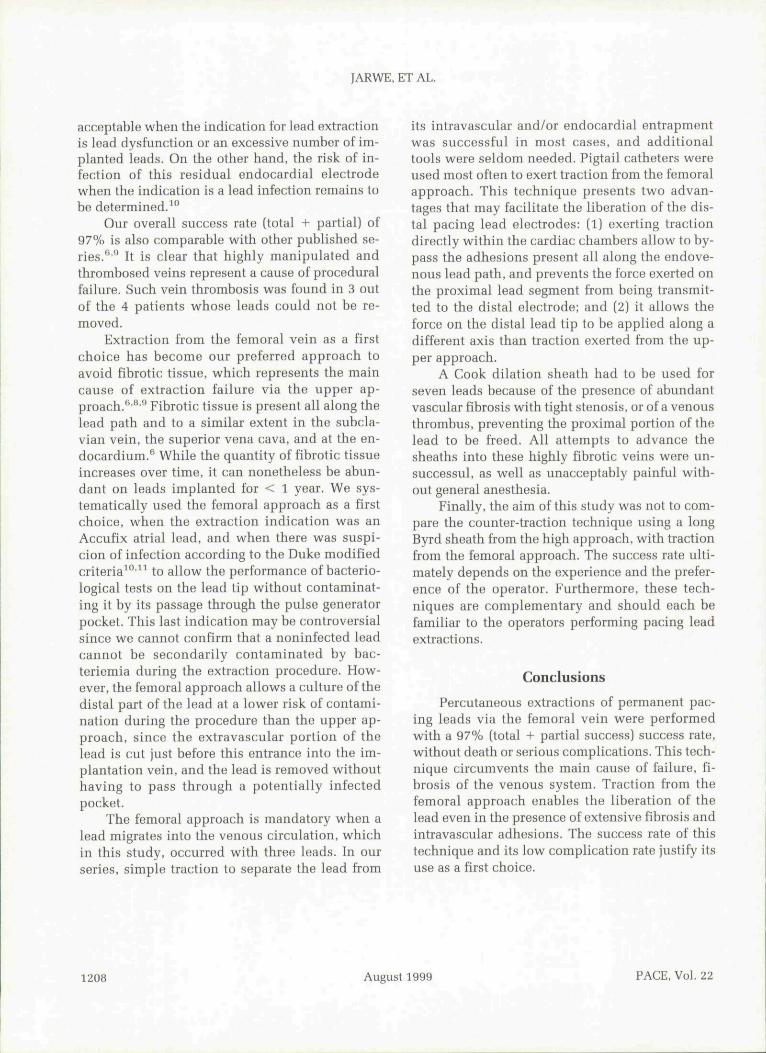
Comparison of Class I Versus Class IIExtraction Indications
Lead extraction and radiation exposure timeswere longer in the Class I group than in Class II
plantation was the same in both groups. There wasno statistically significant difference in total orpartial success rates between the two classes of ex-traction indications.
DiscussionThe indications for pacemaker lead extraction
remain a controversial subject. However, unequiv-ocal indications exist such as infection complica-tions or presence of an Accufix lead with protru-sion ofthe retention wire.
Our overall extraction success rate of 95% iscomparable with other percutaneous extractionsseries that have reported success rates varying he-tween 81% and95%.^'*"No death occurred in ourseries, and the four complications observed (3%)had no serious short- or long-term clinical conse-quences.
The distal electrode [free of insulation) re-mained in situ after two procedures, which wereconsidered partially successful.^ This outcome is
Comparison of Class 1
Number of leadsProcedure time (min)Radiation exposure time (min)Duration of leads implantationFailure: n (%)Leads partially extracted: n (%)
Table VI.
Versus Class 2
Class 1
41134 ± 6037 ±2162 ± 462 (5%)1 (2%)
Extraction Indications
Class 2
8797 ± 6122 ± 1865 ± 492 (2%)1 (1%)
P
0.0030.005
NSNSNS
PACE, Vol. 22 August 1999 1207
JARWE, ET AL.
acceptable when the indication for lead extractionis lead dysfunction or an excessive number of im-planted leads. On the other band, the risk of in-fection of this residual endocardial electrodewhen the indication is a lead infection remains tobe determined.^"
Our overall success rate (total + partial) of97% is also comparable with other published se-ries." '̂̂ It is clear that highly manipulated andthromhosed veins represent a cause of proceduralfailure. Such vein thrombosis was found in 3 outof the 4 patients whose leads could not be re-moved.
Extraction from the femoral vein as a firstchoice has become our preferred approach toavoid fibrotic tissue, which represents the maincause of extraction failure via the upper ap-proach.'** '̂* Fibrotic tissue is present all along thelead path and to a similar extent in the suhcla-vian vein, the superior vena cava, and at the en-docardium.^ While the quantity of fibrotic tissueincreases over time, it can nonetheless be abun-dant on leads implanted for < 1 year. We sys-tematically used the femoral approach as a firstchoice, wben the extraction indication was anAccufix atrial lead, and when there was suspi-cion of infection according to the Duke modifiedcriteria^°'^^ to allow the performance of bacterio-logical tests on the lead tip witbout contaminat-ing it by its passage through the pulse generatorpocket. This last indication may be controversialsince we cannot confirm that a noninfected leadcannot be secondarily contaminated by bac-teriemia during the extraction procedure. How-ever, the femoral approach allows a culture ofthedistal part of the lead at a lower risk of contami-nation during the procedure than the upper ap-proach, since the extravascular portion of thelead is cut just before this entrance into the im-plantation vein, and the lead is removed withouthaving to pass through a potentially infectedpocket.
The femoral approach is mandatory when alead migrates into the venous circulation, whicbin this study, occurred with three leads. In ourseries, simple traction to separate the lead from
its intravascular and/or endocardial entrapmentwas successful in most cases, and additionaltools were seldom needed. Pigtail catheters wereused most often to exert traction from the femoralapproach. This technique presents two advan-tages that may facilitate the liberation of tbe dis-tal pacing lead electrodes: (1) exerting tractiondirectly within tbe cardiac chambers allow to by-pass the adhesions present all along the endove-nous lead path, and prevents the force exerted onthe proximal lead segment from being transmit-ted to the distal electrode; and (2] it allows theforce on the distal lead tip to be applied along adifferent axis than traction exerted from the up-per approach.
A Cook dilation sheath bad to be used forseven leads because of the presence of abundantvascular fihrosis with tight stenosis, or of a venousthrombus, preventing the proximal portion ofthelead to be freed. All attempts to advance thesheaths into these highly fibrotic veins were un-successul, as well as unacceptably painful witb-out general anesthesia.
Finally, the aim of this stndy was not to com-pare the counter-traction technique using a longByrd sheath from the high approach, with tractionfrom the femoral approach. The success rate ulti-mately depends on the experience and the prefer-ence of the operator. Furthermore, these tech-niques are complementary and should each befamiliar to the operators performing pacing leadextractions.
Conclusions
Percutaneous extractions of permanent pac-ing leads via the femoral vein were performedwith a 97% (total + partial success) success rate,without death or serious complications. This tech-nique circumvents the main cause of failure, fi-brosis of the venous system. Traction from thefemoral approach enables the liberation of tbelead even in tbe presence of extensive fibrosis andintravascular adhesions. Tbe success rate of tbistechnique and its low complication rate justify itsuse as a first choice.
1208 August 1999 PACE, Vol. 22
FEMORAL EXTRACTION OF PACING LEADS
References
Madigan NP, Curtis JJ, Sanfelippo JF, et al. Diffi-culty of extraction of chronically implanted tinedventricular endocardial leads. J Am Coll Cardiol1984; 3:725-731.Byrd CL, Schvv'artz SJ, Hedin N. Intravascular tech-niques for extraction of permanent pacemakerleads. J Thorac Cardiovasc Surg 1991: 101:989-997.Byrd CL, Schwartz SJ, Hedin N. Lead extraction.Indications and techniques. Cardiol Clin 1992;10:735-748.Frandsen F, Oxhoj H, Hielsen B. Entrapment of atined pacemaker electrode in the tricuspid valve.A case report. PACE 1990: 13:1082-1083.Myers MR, Parsonnet V, Bernstein AD. Extractionof implanted transvenous pacing leads: A reviewof persistent clinical problem. Am Heart J 1991;3:881-888.Smith HJ, Fearnot NE. Byrd CL, et al., for the U.S.Lead Extraction Database. Five-years experience
10.
11.
with intravascular lead extraction. PACE 1994;17:2016-2020.Espinosa RE. Hayes DL, Vlietstra RE, et al. The dot-ter retriever and pigtail catheter: Efficacy in ex-traction of chronic transvenous pacemaker leads.PACE 1993; 16:2337-2342.Smith CW, Messenger JC, Schaner SP, et al. Car-diac pacemaker electrodes: Improved methods ofextraction. Radiology 1994; 193:739-742Alt E, Neuzner J, Binner L, et al. Three-year expe-rience with a stylet for lead extraction: A multi-center study. PACE 1996; 19:18-25.Klug D, Lacroix D, Savoye C, et al. Systemic infec-tion related to endocarditis on pacemaker leads:Clinical presentation and management. Circula-tion 1997; 95:2098-Z107.Bayer A, Ward JL Ginzton LE, et a l Evaluationof new clinical criteria for the diagnosis of in-fective endocarditis. Am J Med. 1994: 96:211-219.
PACE, Vol. 22 August 1999 1209

Copyright © 2022 FDOKUMEN