
Early right atrial pacing after myocardial infarction
7
Stern D Tzivoni, A Keren, S Gottlieb, C Granot, J Benhorin, E Gazala, JO Golhman and S Right atrial pacing soon after myocardial infarction ISSN: 1524-4539 Copyright © 1982 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online 72514 Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX 1982, 65:330-335 Circulation http://circ.ahajournals.org/content/65/2/330.citation located on the World Wide Web at: The online version of this article, along with updated information and services, is http://www.lww.com/reprints Reprints: Information about reprints can be found online at [email protected] Fax: 410-528-8550. E-mail: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://circ.ahajournals.org//subscriptions/ Subscriptions: Information about subscribing to Circulation is online at by guest on July 12, 2011 http://circ.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Early right atrial pacing after myocardial infarction

SternD Tzivoni, A Keren, S Gottlieb, C Granot, J Benhorin, E Gazala, JO Golhman and S
Right atrial pacing soon after myocardial infarction
ISSN: 1524-4539 Copyright © 1982 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online
72514Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
1982, 65:330-335Circulation
http://circ.ahajournals.org/content/65/2/330.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at [email protected]: 410-528-8550. E-mail: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://circ.ahajournals.org//subscriptions/Subscriptions: Information about subscribing to Circulation is online at
by guest on July 12, 2011http://circ.ahajournals.org/Downloaded from

Right Atrial Pacing Soon After Myocardial InfarctionDAN TZIVONI, M.D., ANDRE KEREN, M.D., SHMUEL GOTTLIEB, M.D., CHAIM GRANOT, M.D.,
JESAIA BENHORIN, M.D., ELIAHU GAZALA, M.D., JOSE 0. GOLHMAN, M.D.,AND SHLOMO STERN, M.D.
SUMMARY To assess the presence of residual myocardial ischemia and its prognostic significance soonafter an acute myocardial infarction (MI), right atrial pacing (RAP) was performed in 85 consecutive patients1 day before hospital discharge. No patient was excluded from the study because of his clinical condition. Themean age of the patients was 61.2 years (range 29-85 years). The study was performed at the bedside 10-28days (mean 14.2 days) after the MI. No complications occurred during or after the test. RAP was consideredpositive if I mm or more of horizontal ST depression developed.The mean maximal pacing rate achieved was 147 beats/min (range 100-160 beats/min). There were 46 pa-
tients (54%) with negative and 39 patients (46%) with positive RAP. Of the 30 patients with anterior MI, 17%had positive RAP, compared with 61% of the 23 with inferior MI and 63% of the 32 patients with subendo-cardial MI. The average follow-up period was 5.8 months. Among the 46 patients with a negative RAP, therewas one sudden death; no reinfarction occurred, but eight patients required cardiac hospitalization and five pa-tients suffered chest pain. Among the 39 patients with a positive RAP, three died (one suddenly and two afterreinfarction); four additional patients had reinfarction. There were 20 cardiac hospitalizations in this group.Eighteen patients suffered from chest pain. A treadmill test was performed 6 months after MI in 37 patients.Seventeen of the 21 patients with negative RAP had a negative test, whereas 13 of the 16 with positive RAPhad a positive treadmill test 6 months later.We conclude that RAP can be performed safely in patients after MI. Forty-six percent of all post-MI pa-
tients had residual areas of stress-induced myocardial ischemia. RAP was sensitive in predicting subsequentreinfarction, cardiac death, cardiac rehospitalization, angina pectoris and the response to a treadmill test 6months after MI.
PATIENTS recovering from acute myocardial infarc-tion (MI) are at high risk for reinfarction and cardiacdeath, especially during the first year after infarc-tion.1-7 Early identification of patients at risk may leadto a more intensive medical or surgical therapy andreduction of reinfarction and cardiac death rate.Several investigators have reported that exercise test-ing soon after MI can identify a large proportion ofthis high-risk group.8 13 However, many of the patientsin these reports such as those with persistent chestpain or signs of left ventricular failure at the time ofdischarge or those older than 70 years, were excludedfrom the studies because of the potential hazard ofstress testing, although such patients consitute thehigh-risk subset. Further, many patients could notperform even the modified exercise test.
In this study we used right atrial pacing (RAP) toassess the presence of residual myocardial ischemia inpost-MI patients. This method permits a controlled,stepwise increase in heart rate and consequently inmyocardial oxygen demand;14-'6 RAP is not depen-dent on the patient's physical fitness and if ischemicchanges develop they can be reversed immediately bycessation of pacing. These factors make RAP moresuitable than exercise testing in post-MI patients.
From the Heiden Department of Cardiology, Bikur CholimHospital and Hebrew University-Hadassah Medical School,Jerusalem, Israel.
Supported in part by the Joint Research Fund of the HebrewUniversity and Hadassah and by the American PhysiciansFellowship.
Address for correspondence: Dan Tzivoni, M.D., Bikur CholimHospital, P.O.B. 492, Jerusalem, Israel.
Received January 19, 1981; revision accepted May 28, 1981.Circulation 65, No. 2, 1982.
MethodsIn our service, 91 consecutive patients survived an
acute MI during a 12-month period commencing inSeptember 1979. RAP was performed successfully in85; three patients refused the test, and the electrodecould not be advanced to the right atrium in threeothers.There were 66 males and 19 females, ages 29-85
years (mean 61.2 years). Sixty-three of the patientshad suffered their first infarct, 20 their second, andtwo their third. The site of the infarct was anterior in30, inferior in 23 and subendocardial in 32. No patientwas excluded from the study because of clinical condi-tion, age or physical disability. All patients continuedto take their medication on the day of RAP. All pa-tients gave informed consent.Acute MI was diagnosed when two of the following
criteria were met: ischemic chest pain that lasted formore than 30 minutes; elevation of two of the threecardiac enzymes - creatine kinase, aspartate aminotransferase or lactic dehydrogenase; and characteristicECG changes. Transmural MI was diagnosed when anew Q wave appeared, and subendocardial infarctionwas diagnosed when characteristic ST-T changesappeared in the ECG.RAP was performed at bedside 10-28 days (mean
14.2 days) after the acute infarction and the patientwas discharged from hospital the next day. An armvein was punctured and a #5F bipolar electrode wasadvanced through a #14 needle or through an in-troducing sheath to the right atrium. The electrodeposition was verified by the appearance of a largenegative P wave in the intraatrial recording. A 12-leadECG was recorded at rest, and atrial pacing wasstarted at a rate of 10 beats/min above the patient's
330 by guest on July 12, 2011http://circ.ahajournals.org/Downloaded from

ATRIAL PACING SOON AFTER MI/Tzivoni et al.
resting heart rate. Pacing rate was increased by 10beats every 2 minutes, until a rate of 160 beats/minwas achieved.
During pacing, the patients were continuouslymonitored. Leads V,, V5 and V6 were recorded everyminute. Blood pressure was measured every 2minutes. A 12-lead ECG was recorded during everysecond pacing rate and at the maximal pacing rate.After each pacing period, pacing was stopped and theECG was recorded continuously for about 30 seconds;then, the pacing rate was increased. RAP was ter-minated if more than 3 mm of ST depressiondeveloped in any of the leads, if the patient com-plained of severe chest pain, if frequent ventricularpremature complexes or atrial fibrillation occurred orif blood pressure decreased more than 15 mm Hgbelow resting blood pressure. Ten patients developedMobitz type 1 second-degree atrioventricular block;they were given 0.5-1.5 mg of atropine and pacing wascontinued. RAP was regarded positive if 1 mm ormore of horizontal ST depression was observed, com-pared with the prepacing ECG, which persisted for atleast three postpacing beats. RAP was consideredstrongly positive if more than 2 mm of ST depressionwas observed, or if ST depression developed at a pac-ing rate of 120 beats/min or less. There were no ECGor enzyme changes in any of the patients within 24hours after the RAP. In no patient did the RAPresults influence the therapeutic approach at dis-charge.No patient was lost to follow-up. The patients were
examined in our cardiac outpatient clinic 1, 3, 6, 9 and12 months after the MI. A physical examination wasperformed and the clinical history and a 12-lead ECGwere obtained. The follow-up ranged from 0-12months (mean 5.8 months). Six months after dis-charge, 37 patients performed a treadmill test (Bruceprotocol). Seven additional patients were excludedfrom the treadmill test at 6 months because of recentinfarct, unstable angina pectoris, congestive heartfailure or physical disability.
ResultsRAP was performed without complications in all
85 patients. Table 1 lists the maximal heart ratesachieved. Fifty-five patients (65%) achieved a heartrate of 150 beats/min or greater, while 71 patients
TABLE 1. Maximal Pacing Rate in 85 Patients
Pacing rate(beats/min) No. of pts
100 1
110 2120 6130 5
140 16150 12160 43
Mean 147 beats/min
(84%) achieved a heart rate of 140 beats/min orgreater. The mean maximal pacing rate was 147beats/min. Thirty patients did not achieve a heart rateof 150 beats/min because the exercise test was stoppedfor one of the following reasons: ST depression in 22,atrial fibrillation in two, atrioventricular block in four(atropine was only partially effective or was contrain-dicated) and multiple ventricular premature complex-es in two patients. In no patient was the test in-terrupted because of a decrease in blood pressure orsevere chest pain.The mean systolic blood pressure at rest was 133.1
± 17.1 mm Hg (SD) (table 2). At peak pacing rate thisvalue was 137 mm Hg ± 21.5 (NS). The mean doubleproduct at rest was 10355 ± 2245 mm Hg.min, and atmaximal pacing rate it was 20177 ± 3578 mm Hg*min(p < 0.001).
Table 3 details the results of the RAP test. Thirty-nine of the 85 patients (46%) had a negative test; in 15of them the test was strongly positive. Examples ofpositive tests are shown in figures 1 and 2. Separationof the patients according to infarct site reveals thatonly 17% of those with anterior infarct had a positivetest, compared with 61% of the inferior and 63% of thesubendocardial infarcts.Of the 39 patients with positive RAP, chest pain ac-
companied the ischemic ST depression in only nine.Four other patients had nontypical chest pain withoutST-T changes, but continued despite pain; no STdepression developed and the pain did not increase inintensity. Three patients had multiple ventricularpremature complexes, associated with ST depressionin two. Three other patients had atrial fibrillation, twoat a pacing rate of 140 beats/min and one at 150beats/min. Pacing was therefore terminated, andsinus rhythm returned spontaneously.ST elevation occurred in nine patients during pac-
TABLE 2. Mean Systolic Blood Pressure and Double Prod-uct in 85 PatientsMean systolic blood pressure (mm Hg)
Before RAP 133.1 ± 17.1At peak pacing 137.0 ± 21.5
Mean double product (mm Hg-min)Before RAP 10355 ± 2245At peak pacing 20177 ± 3578
Values are mean ± SD.
TABLE 3. Results ofRight Atrial Pacing in 85 PatientsType of Nega- Posi- % posi-infarct n tive tive* tive
Anterior 30 25 5 (2) 17Inferior 23 9 14 (5) 61Subendocardial 32 12 20 (8) 63Total 85 46 39% of total 54 46*Numbers in parentheses indicate number of strongly
positive tests.
331
by guest on July 12, 2011http://circ.ahajournals.org/Downloaded from
VOL 65, No 2, FEBRUARY 1982
4,
RESTneM
t0o0
L U,~~~~
t. Sligh_t STdepre...s-
n
I 1 z|E z
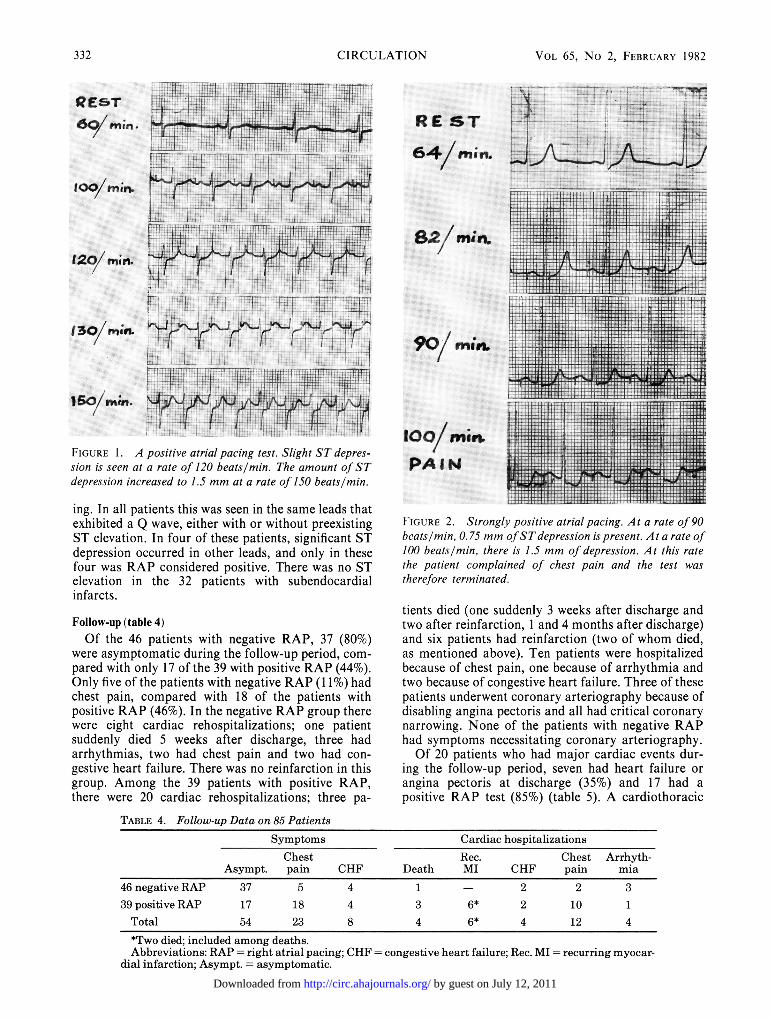
FIGURE A postivSe atra pain test .Slight ST deprs -+ o>
dersso inrae to015 mm at a rat of0 beatlmin
ing.~~-In al patens ti wa se9en in th sam ledsthat
exhibited a Q wave, either with or without preexistingST elevation. In four of these patients, significant ST
depression occurred in other leads, and only in these
four was RAP considered positive. There was no STelevation in the 32 patients with subendocardialinfarcts.
Follow-up (table 4)
Of the 46 patients with negative RAP, 37 (80%)were asymptomatic daring the follow-up period, com-
pared with only 17 of the 39 with positive RAP (44%).
Only five of the patients with negative RAP(1s1%) had
chest pain, compared with 18 of the patients with
positive RAP (46%). In the negative RAP group there
were eight cardiac rehospitalizations; one patientsuddenly died 5 weeks after discharge, three had
arrhythmias, two had chest pain and two had con-
gestive heart failure. There was no reinfarction in this
group. Among the 39 patients with positive RAP,there were 20 cardiac rehospitalizations; three pa-
RE ST
64/nun.
8/Minun
90, mitt
100/mitt
PA I
<< f s S b w . A . . > . . . - x .p < g 4 4 * e e 4t e F t i > . i i - .\ . i. . s - 8 st.. _ .: t a x> - V * T i * s > * E * * *} j S
R s {D 55S s. . .. . Se * £ B st fi § *S- Ss S3?TA i > s _ t s s 4 x s _ s s S i } e i aN .$' | , t k + z - 2 S: i e fit- ''- i: f ;s S;s SiaN' \ 71 s s s \ AN bF>|Ex s--N -ENs sss 5 ssNiN e : D: ,' 8X | x <-o o A $ S ' \ E , g P : - Et * ^ | > i; A A v > 5 Lz E 5#R )t ^ ' ^ ' 5 [i - Sf -+ w .. . .. -. + 9 ... s.&+ te --eFE o 5--- 4 t .
z/ -.__v-- w P B . 5 E b.:-
ti
WH}e 2eA
.34WFq?v.t > M
F 4 . Fti4 i4. 4i .4 4 T .4 . -
-t¢t hS 44- 5{6
-L IH- ti .... .*-- i+
ITl~4
=r,. ,i-e i
II'It:+.7. .1.7. ntS -erF+4
-7TFT1
4+ +T A -]'TT AtP-TFl
.I+ _ 4 4 it a > 4 t* -. '7 _ *. . ..: ^ >- =; .> ti t z X | :tX ; W; 4 t i . W r .s K . ; . X 5 S j X X t; . > f tS _ 4 t t!+ " t * e : K e E ; _ z N + W q h _ + + h b * hES + t kFR 5 b * w i S k .. +.-t * o vAX >+ _ + @n' 2' w . ,4S'SS'Sq Am m t.a' +e4 t: > tt +Ht tS t 4 42- 42 Ae; pS h* S It M_ _* 1 1 SmW7X;t; tH-X+XH44H
U4M=S T_ ?T 7 =_r__ __k_U.2;W_
X;2i_WHM[
e4g X t < t' Tq 44Xi;+ + °4t t-X25t tq$;4 t 4+.+; T4_2ttti,.j44' *+4.'4vX4094 *S44->X4'W''f'F'&'>F-FS _rE
4++ w+Ff Hei+>t''ttf'+S:1
'Nm 14
f'IGURE 2. Strongly positive atrial pacing. At a rate of 90beats/min, 0.75 mm ofSTdepression is present. At a rate of100 beats/min, there is 1.5 mm of depression. At this rate
the patient complained of chest pain and the test was
therefore terminated.
tients died (one suddenly 3 weeks after discharge andtwo after reinfarction, I and 4 months after discharge)and six patients had reinfarction (two of whom died,as mentioned above). Ten patients were hospitalizedbecause of chest pain, one because of arrhythmia andtwo because of congestive heart failure. Three of thesepatients underwent coronary arteriography because ofdisabling angina pectoris and all had critical coronarynarrowing. None of the patients with negative RAPhad symptoms necessitating coronary arteriography.Of 20 patients who had major cardiac events dur-
ing the follow-up period, seven had heart failure or
angina pectoris at discharge (35%) and 17 had a
positive RAP test (85%) (table 5). A cardiothoracic
TABLE 4. Follow-up Data on 85 PatientsSymptoms Cardiac hospitalizations
Chest Rec. Chest Arrhyth-Asympt. pain CHF Death MI CHF pain mia
46 negative RAP 37 5 4 1 - 2 2 339 positive RAP 17 18 4 3 6* 2 10 1
Total 54 23 8 4 6* 4 12 4
*Two died; included among deaths.Abbreviations: RAP - right atrial pacing; CHF - congestive heart failure; Rec. MI = recurring myocar-
dial infarction; Asympt. asymptomatic.
-F4+4 4.74
la
prr'.
t ..t ..
332 CIRCULATION
04';
by guest on July 12, 2011http://circ.ahajournals.org/Downloaded from

ATRIAL PACING SOON AFTER MI/Tzivoni et al.
TABLE 5. Comparison of Clinical Symptoms and Right Atrial Pacing at Discharge with Subsequent Major Cardiac EventsMajor cardiac events No major
Symptoms at No. of Results of RAP Unstable Recurrent cardiacdischarge pts Negative Positive AP MI Death Total event
32 - - - - 38Asymptomatic 62
30 7 5 3 13 179 - - 1 1 8
Heart failure 134 1 - - 1 3
5 2 - - 2 3Angina pectoris 10
5 2 1 - 3 2Total 85 46 39 12 6 4 20 65Abbreviations: AP = angina pectoris; MI = myocardial infarction.
ratio greater than 0.55 was present in 18 patients, butonly four (22%) had subsequently a major cardiacevent (two unstable angina pectoris, one recurrent MIand one death).
Thirty-seven patients performed a treadmill test(Bruce protocol) 6 months after MI. Of the 21 pa-tients with negative RAP, 17 (80%) had a negativetreadmill test. Of the 16 with positive RAP, only three(19%) had a negative test; all others (81%) had a posi-tive treadmill test (table 6).
DiscussionRight atrial pacing was introduced by Sowton et
al.14 in 1967 as a myocardial stressing method forassessing the presence and severity of coronary arterydisease. RAP has been used extensively to inducemyocardial ischemia.'7-23 Kelemen and co-workers24and Piessens and co-workers26 found that RAP had asomewhat lower sensitivity and higher specificity thanexercise stress testing. However, these studies showthat in patients with advanced coronary disease, thesensitivity of RAP increases to about 85%. All of ourpatients had unequivocal advanced coronary disease,and therefore the diagnostic accuracy of RAP in thisgroup of patients is not in doubt.
In this study we used RAP to identify stress-inducedresidual myocardial ischemia in patients recoveringfrom acute MI. Because a preliminary study of 31 pa-tients showed25 that RAP is safe even soon after MI,no patient was excluded from the present studybecause of clinical condition. In similar studies, usingtreadmill testing, many high-risk patients, i.e., thosewith angina pectoris, congestive heart failure, associ-
TABLE 6. Comparison of Right Atrial Pacing Soon afterMyocardial Infarct and Treadmill Test 6 Months Later in37 Patients
Treadmill testNegative Positive
Negative RAP 21 17 4Positive RAP 16 3 13Total 37 20 17Abbreviation: RAP = right atrial pacing.
ated valvular or pulmonary disease, or hypertension,were not included.12' 18 RAP could easily be applied atthe bedside; all patients tolerated the study well andthere were no complications. The three patients whohad atrial fibrillation reverted spontaneously to sinusrhythm. The mean maximal heart rate during RAPwas 147 beats/min, a rate much higher than thatachieved during the "modified" post-MI exercisetests.'2' 18Of the 85 patients studied, 47% had ischemic ECG
changes during RAP. In previous studies on post-MIpatients, Theroux and co-Workers'2 found only 30%positives and Davidson and co-workers'8 only 18%positives during treadmill testing. Our explanation ofthe higher ischemic response to RAP than to treadmilltesting is the faster heart rate during RAP and theconsequently higher myocardial work load. Further,our patient population differs from the others, as nopatient was excluded from our study, compared with a50% exclusion rate in studies using treadmill testing;therefore, our results probably better represent thetrue prevalence of residual ischemia in post-MIpatients.Only 17% of the patients with anterior MI had a
positive RAP test, compared with 61% of those withinferior and 63% of those with anterior MI. Theseresults suggest that patients with subendocardial MIfrequently have critical coronary narrowing, and aretherefore at higher risk for reinfarction. This clinicalobservation seems to be well known to cardiologistsand internists, but has been evaluated in only fewstudies.27-29 The higher frequency of ischemic responseto pacing among patients with inferior MI thanamong patients with anterior MI is consistent with re-cent reports on the higher incidence of two- and three-vessel disease in patients with inferior infarction.830 1
Castellanet and co-workers82 performed stress tests inpatients with prior MI and found a significantly higherrate of ischemic response among patients who had in-ferior MI than among those who had anterior MI(84% vs 52.1%).
Chest pain accompanied ST depression in only nineof the 35 patients with positive RAP (26%). This is inaccordance with the prevailing concept that chest painis an insensitive index of mycocardial ischemia.U. 84
333
by guest on July 12, 2011http://circ.ahajournals.org/Downloaded from

VOL 65, No 2, FEBRUARY 1982
Ventricular arrhythmias occurred in only three pa-tients during atrial pacing (4%), in striking contrast toexercise testing soon after MI, which evoked ventric-ular arrhythmias in 20-38% of the patients.12 13, 36
Four patients died during the relatively shortfollow-up period of this study (mean 5.8 months). Onehad a negative RAP, a massive anterior MI and severecongestive heart failure and died suddenly. Threeother patients had a positive RAP; two died after rein-farction and one died suddenly. Six patients had rein-farction (including the two who died); all had positiveRAP. Thus, RAP seems to be a better predictor forlater reinfarction than for cardiac death. Reinfarctionseems to be related to the presence of critical coronarystenosis, whereas cardiac death is influenced by otherimportant factors, such as infarct size, congestiveheart failure, and serious ventricular arrhyth-mias. -6, 36-39There were 20 cardiac hospitalizations among the
39 patients with positive RAP, compared with eightamong the 46 with negative RAP. Most hospitaliza-tions among patients with positive RAP were due tochest pain or reinfarction, whereas among those with anegative RAP, the presence of arrhythmias was themain cause of hospitalization. Three patients un-derwent coronary arteriography because of disablingangina pectoris; in all three, severe coronary narrow-ing requiring cardiac surgery was found. No patientwith negative RAP required coronary angiography.The clinical symptoms at discharge (angina pectoris,congestive heart failure or an increased cardio-thoracic ratio) were less indicative of subsequent un-stable angina pectoris, recurrent MI or death than wasthe RAP test.RAP was sensitive in predicting the presence of an
ischemic response to the treadmill test performed 6months after the infarct. Of the 21 patients in thegroup with negative RAP, 17 (80%) had negativetreadmill test, and of the 16 with positive RAP, 13(81%) had a positive treadmill test. Thus, ischemicchanges present immediately after the infarct tend topersist. In the small group of patients who had positiveRAP and 6 months later had a negative treadmill test,it is possible that effective collateral circulation haddeveloped, whereas in the small group with negativeRAP who had positive treadmill test 6 months later, itis possible that coronary disease had progressed toproduce critical narrowing.RAP could be performed at the bedside in all pa-
tients. Although the test is invasive, it involves an in-convenience similar to that of inserting an i.v. line.The test does not require the patient's cooperation,and is not dependent on physical fitness, which is ex-tremely poor in many post-MI patients. Thus, mostpatients find this test easier and less tiring than a testthat requires physical effort. RAP has the advantageover treadmill testing that the heart rate increases un-der a strict control and if ischemic changes develop,they can be reversed immediately by cessation of pac-ing. For these reasons, RAP is safer and thereforemore suitable than exercise testing for post-MI pa-tients. We did not exclude any patient from the study,
in contrast to exercise testing where in some studiesmore than 50% of the patients, including many whocarry a high risk, were excluded. This difference inpopulation material and the faster heart rate achievedduring RAP explain the higher percentage of ischemicresponses to RAP (46%) than to exercise testing. Thedifference in population may explain also the higherincidence of death in our population (four deaths dur-ing a follow-up period of 5.8 months), compared witha less than 2% annual mortality found by Davidsonand co-workers.13We conclude that RAP can be performed safely
soon after MI in all patients. This test provides impor-tant information about cardiac morbidity and mor-tality. Further studies are required before changes inthe therapeutic approach can be based on the result ofthe RAP in the individual patient.
References1. Moss AJ: Profile of high risk in people known to have coronary
heart disease: a review. Circulation 52 (suppl III): 111-147, 19752. Gazes PJ, Kitchell JR, Meltzer LE, Rosenblatt WH, Roth 0:
Death rate among 795 patients in first year after myocardial in-farction. JAMA 197: 906, 1966
3. Kannel WB, Solie P: Prognosis after initial myocardial infarc-tion: the Framingham Study. Cardiology 44: 53, 1979
4. Norris RM, Canghey DE, Deeming LW, Mercer CJ, Scott PJ:Coronary prognostic index for predicting survival afterrecovery from acute myocardial infarction. Lancet 2: 485, 1970
5. Vedin JA, Wilhelmson C, Elmfeldt D: Sudden death: identifica-tion of high-risk groups. Am Heart J 86: 124, 1973
6. Moss AJ, DeCamilla J, Engstrom F, Hoffman W, Odoroff C,Davis H: The post-hospital phase of myocardial infarction.Identification of patients with increased mortality risk. Circula-tion 49: 460, 1974
7. Killip T: Arrhythmia, sudden death and coronary artery dis-ease. (editorial) Am J Cardiol 28: 614, 1971
8. Ibsen H, Kjoller E, Styperek J, Pedersen A: Routine exerciseECG three weeks after acute myocardial infarction. Acta MedScand 198: 463, 1975
9. Markiewicz H, Houston N, DeBusk RF: Exercise testing soonafter myocardial infarction. Circulation 56: 26, 1977
10. Sami M, Kraemer H, DeBusk RF: The prognostic significanceof serial exercise testing after myocardial infarction. Circula-tion 60: 1238, 1979
11. DeBusk RF, Houston N, Haskell W, Fry C, Parker M: Exer-cise training soon after myocardial infarction. Am J Cardiol 44:1223, 1979
12. Theroux P, Waters DD, Halphen C, Debaisieux JC, MizgalaHT: Prognostic value of exercise testing soon after myocardialinfarction. N Engl J Med 301: 341, 1979
13. Davidson DM, DeBusk RF: Prognostic value of a single exer-cise test 3 weeks after uncomplicated myocardial infarction.Circulation 61: 236, 1979
14. Sowton GE, Balcon R, Gross G, Frick MH: Measurement ofthe angina threshold using atrial pacing. Cardiovasc Res 1: 301,1967
15. Balcon R, Maloy WC, Sowton E: Clinical use of atrial pacingtest in angina pectoris. Br Med J 3: 91, 1968
16. Parker JO, Ledwich JR, Case RB: Reversible cardiac failureduring angina pectoris. Hemodynamic effects of atrial pacing incoronary artery disease. Circulation 39: 745, 1969
17. Linhart JH, Hildne FJ, Barold SS, Lister JW, Samet P: Leftheart hemodynamics during angina pectoris induced by atrialpacing. Circulation 40: 483, 1969
18. Balcon R, Sowton E: The hemodynamic effects of atrial pacingin patients with ischemic heart disease. Acta Med Scand 188:199, 1970
19. Helfant RH, Forrester JS, Hampton JR: Coronary heart dis-ease. Differential hemodynamic, metabolic and electrocardio-graphic effects in subjects with and without angina pectoris dur-
334 CIRCULATION
by guest on July 12, 2011http://circ.ahajournals.org/Downloaded from

ATRIAL PACING SOON AFTER MI/Tzivoni et al.
ing atrial pacing. Circulation 42: 601, 197020. Forrester JS, Helfant RH, Pasternac A: Atrial pacing in cor-
onary circulation. Am J Cardiol' 27: 237, 197121. Parker JD, Chiong MA, West RO, Case RB: Sequential
alterations in myocardial lactate metabolism, S-T segments,and left ventricular function during angina induced by atrialpacing. Circulation 40: 113, 1969
22. Armstrong PW, Chiong MA, Parker JO: Effects of propranololon the= hemodynamic, coronary sinus blood flow and myocar-dial metabolic response to atrial pacing. Am J Cardiol 40: 83,1977
23. Linhart JW: Atrial pacing in coronary artery disease. Am JMed 53: 64, 1972
24. Kelemen MH, Gillilan RE, Bouchard RJ, Heppner RL, War-basse JR: Diagnosis of obstructive coronary disease by max-imal exercise and atrial pacing. Circulation 48: 1227, 1973
25. Piessens J, van Mieghem W, Kesteloot H, de Geest H:Diagnostic value of clinical history, exercise testing and atrialpacing in patients with chest pain. Am J Cardiol 33: 351, 1974
26. Tzivoni D, Gazala E, Keren A, Golhman JO, Stern S: Rightatrial pacing soon after myocardial infarction for assessment ofresidual myocardial ischemia. Israel J Med Sci 16: 594, 1980
27. Cannon D, Levy W, Cohen L: The short and long termprognosis of patients with transmural and nontransmural in-farction. Am J Med 61: 452, 1976
28. Genovese M, Salaki J, Kennedy R: Subendocardial infarction:what happens later? Am Heart J 92: 542, 1976
29. Kossowsky W, Mohr B, Raffi S: Superimposition of transmuralinfarction following acute subendocardial infarction. Chest 69:758, 1976
30. Miller RR, DeMaria AN, Vismara LA, Salel AF, MaxwellKS, Amsterdam EA, Mason DT: Chronic stable inferiormyocardial infarction: unsuspected harbinger of high-risk prox-imal left coronary arterial obstruction' amenable to surgicalrevascularization. Am J Cardiol 39: 954, 1977
31. Tubau JF, Chaitman BR, Bourassa MG, Waters DD: Detec-tion of multivessel coronary disease after myocardial infarc-tion using exercise stress testing and multiple ECG leadsystems. Circulation 61: 44, 1980
32. Castellanet MJ, Greenberg PS, Ellestad MH: Comparison ofS-T segment changes on exercise testing with angiographic find-ings in patients with prior myocardial infarction. Am J Cardiol42: 29, 1978
33. Allen RD, Gettes LS, Phalen C, Avington MD: Painless S-Tsegment depression in patients with angina pectoris. Chest 69:467, 1976
34. Stern S, Tzivoni D: The dynamic nature of the ST-T segment inischemic heart disease. Am, Heart J 91: 820, 1976
35. Ericson M, Granath A, Ohlsen P, Sodermark T, Volpe U:Arrhythmias and symptoms during' treadmill testing threeweeks after myocardial infarction in 100 patients. Br Heart J35: 787, 1973
36. Kotler MN, Tabatznik B, Mower B, Tominaga S: Prognosticsignificance of ventricular ectopic beats with respect to suddendeath in the late post infarction period. Circulation 47: 959,1973
37. The Coronary Drug Project Research Group: Prognostic im-portance of premature beats following myocardial infarction:experience in the Coronary Drug Project. JAMA 223: 1116,1973
38. Moss AJ, DeCamille J, Mietlowsky W, Greene WA, GoldstienS, Locksley R: Prognostic grading and significance of ventric-ular premature beats after recovery from myocardial infarc-tion. Circulation 52 (suppl III): III-204, 1975
39. Borer JS, Rosing DR, Miller RH, Stark RM, Kent KM,Bacharach SL, Green MU, Lake CR, Cohen H, Holmes D,Donohue D, Baker W, Epstein SE: Natural history of left ven-tricular function during I year after acute myocardial infarc-tion: comparison with clinical, electrocardiographic andbiochemical determinations. Am J Cardiol 46: 1, 1980
335
by guest on July 12, 2011http://circ.ahajournals.org/Downloaded from




















