
Permanent direct his bundle pacing does not induce ventricular dyssynchrony unlike conventional...
12
Permanent direct his bundle pacing does not induce ventricular dyssynchrony unlike conventional right ventricular apical pacing An intrapatient acute comparison study Domenico Catanzariti & Massimiliano Maines & Claudio Cemin & Gianpaolo Broso & Tiziana Marotta & Giuseppe Vergara Received: 8 June 2006 / Accepted: 10 July 2006 / Published online: 18 November 2006 # Springer Science + Business Media, LLC 2006 Abstract Background Benefits of A-V synchrony during right ventric- ular apical pacing are neutralized by induction of ventricular dyssynchrony. Only a few data are reported about direct His bundle pacing influence on ventricular synchronism. Aim Was to assess the capability of direct His bundle pacing to prevent pacing-induced ventricular dyssynchrony comparing DDD- (or VVI- in case of Atrial Fibrillation) right ventricular apical pacing with DDD- (or VVI-) direct His bundle pacing in the same patients cohort. Methods 23 of 24 patients (mean age 75.1± 6.4 years) with narrow QRS (HV< 65 ms) underwent permanent direct His bundle pacing for “brady–tachy syndrome” (11) or supra- Hisian II/III-degree AV Block (permanent atrial fibrillation 7, AV Node ablation 1). A 4.1 F screw-in lead was fixed in His position, guided by endocardial pacemapping and unipolar recordings. Additional permanent (13 patients) or temporary right ventricular apical pacing leads were also positioned. Inter- and left intra-ventricular dyssynchrony, mitral regurgitation and left systolic ventricular function Tei index were assessed during either direct His bundle pacing or right ventricular apical pacing. Results Permanent direct His bundle pacing was obtained in 23 of 24 patients. Indexes of ventricular dyssynchrony were drastically reduced, mitral regurgitation decreased and left systolic ventricular function Tei index improved during direct His bundle pacing (or His bundle and septum pacing) in comparison to apical pacing (p < 0.05). No statistically significant differences were observed between direct His bundle pacing and combined His bundle and septum pacing. Conclusion Direct His bundle pacing (also fused with adjacent septum capture) prevents pacing-induced ventric- ular dyssynchrony. Keywords His bundle pacing . His bundle . Brady . Tachy sick sinus syndrome . SupraHisian AV block . Cardiac pacing . Ventricular dyssynchrony Abbreviations RVAP right ventricular apical pacing HP His bundle pacing Hb His bundle PHP para-Hisian pacing H+SP combined pacing of both Hb and adjacent ventricular septum AV atrio-ventricular RV right ventricular LV left ventricular PM pacemaker AVB atrioventricular block ICD implantable cardioverter defibrillator CRT cardiac resynchronization pacing therapy LBBB left bundle branch block J Interv Card Electrophysiol (2006) 16:81–92 DOI 10.1007/s10840-006-9033-5 Mrs. Tiziana Marotta is an employee of Medtronic inc. who gave her assistance during the implantation procedure. D. Catanzariti (*) : M. Maines : C. Cemin : G. Broso : G. Vergara Divisione di Cardiologia, Ospedale S. Maria del Carmine, Corso Verona, n. 4, 38068, Rovereto, TN, Italy e-mail: [email protected] T. Marotta Medtronic Italy, Inc., Milan, Italy
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Permanent direct his bundle pacing does not induce ventricular dyssynchrony unlike conventional...

Permanent direct his bundle pacing does not induceventricular dyssynchrony unlike conventionalright ventricular apical pacingAn intrapatient acute comparison study
Domenico Catanzariti & Massimiliano Maines & Claudio Cemin &
Gianpaolo Broso & Tiziana Marotta & Giuseppe Vergara
Received: 8 June 2006 / Accepted: 10 July 2006 / Published online: 18 November 2006# Springer Science + Business Media, LLC 2006
AbstractBackground Benefits of A-V synchrony during right ventric-ular apical pacing are neutralized by induction of ventriculardyssynchrony. Only a few data are reported about direct Hisbundle pacing influence on ventricular synchronism.Aim Was to assess the capability of direct His bundlepacing to prevent pacing-induced ventricular dyssynchronycomparing DDD- (or VVI- in case of Atrial Fibrillation)right ventricular apical pacing with DDD- (or VVI-) directHis bundle pacing in the same patients cohort.Methods 23 of 24 patients (mean age 75.1± 6.4 years) withnarrow QRS (HV< 65 ms) underwent permanent direct Hisbundle pacing for “brady–tachy syndrome” (11) or supra-Hisian II/III-degree AV Block (permanent atrial fibrillation7, AV Node ablation 1). A 4.1 F screw-in lead was fixed inHis position, guided by endocardial pacemapping andunipolar recordings. Additional permanent (13 patients) ortemporary right ventricular apical pacing leads were alsopositioned. Inter- and left intra-ventricular dyssynchrony,mitral regurgitation and left systolic ventricular function Teiindex were assessed during either direct His bundle pacingor right ventricular apical pacing.
Results Permanent direct His bundle pacing was obtainedin 23 of 24 patients. Indexes of ventricular dyssynchronywere drastically reduced, mitral regurgitation decreased andleft systolic ventricular function Tei index improved duringdirect His bundle pacing (or His bundle and septum pacing)in comparison to apical pacing (p < 0.05). No statisticallysignificant differences were observed between direct Hisbundle pacing and combined His bundle and septumpacing.Conclusion Direct His bundle pacing (also fused withadjacent septum capture) prevents pacing-induced ventric-ular dyssynchrony.
Keywords His bundle pacing . His bundle . Brady . Tachysick sinus syndrome . SupraHisian AV block . Cardiacpacing . Ventricular dyssynchrony
AbbreviationsRVAP right ventricular apical pacingHP His bundle pacingHb His bundlePHP para-Hisian pacingH+SP combined pacing of both Hb and adjacent
ventricular septumAV atrio-ventricularRV right ventricularLV left ventricularPM pacemakerAVB atrioventricular blockICD implantable cardioverter defibrillatorCRT cardiac resynchronization pacing therapyLBBB left bundle branch block
J Interv Card Electrophysiol (2006) 16:81–92DOI 10.1007/s10840-006-9033-5
Mrs. Tiziana Marotta is an employee of Medtronic inc. who gaveher assistance during the implantation procedure.
D. Catanzariti (*) :M. Maines :C. Cemin :G. Broso :G. VergaraDivisione di Cardiologia, Ospedale S. Maria del Carmine,Corso Verona, n. 4, 38068, Rovereto, TN, Italye-mail: [email protected]
T. MarottaMedtronic Italy, Inc.,Milan, Italy

PW Pulsed-waveTDI Tissue Doppler imagingIVD interventricular electromechanical delaySPD septal to left posterior wall motion delayTDId maximal difference between TDI systolic
velocities of basal LV segmentsMR mitral regurgitation flowEROA effective regurgitant orifice areaPISA proximal isovelocity surface areaMPI myocardial performance indexICT sovolumetric contraction timeIRT isovolumetric relaxation timeLVET left ventricular ejection time
1 Introduction
A large body of evidence from several pacemaker or ICDtrials has emerged on the long-term detrimental effects ofright ventricular apical pacing (RVAP) on left ventricular(LV) function [1–7].
Experimental data have reported diastolic and systolicLV dysfunction, remodeling and dilatation of the leftventricle, asymmetrical LV wall hypertrophy, workloadand metabolic regional heterogeneity after RVAP [8–13].
Unphysiologic LV depolarization, and in turn mechan-ical LV dyssynchrony due to RVAP, may underlie theseharmful effects, counteracting the beneficial hemodynamiceffects of atrio-ventricular (AV) synchrony provided bydual-chamber cardiac pacing.
For this purpose, among the emerging strategies, in apioneering work, Deshmukh et al. proposed permanent Hisbundle pacing (HP), and documented clinical and echocar-diographic benefits during follow-up [14, 15].
However, few data are currently available on thefeasibility of permanent HP [14–16] and its electromechan-ical effects in comparison with those of RVAP. We thereforeprospectively examined the effects of pacing at thesedifferent sites on ventricular synchronism, mitral regurgita-tion and LV systolic performance in the same group ofpatients undergoing permanent direct HP.
2 Materials and methods
2.1 Patients
Patients were eligible for enrollment if they had preservedinfra-Hisian conduction and an indication for conventionalpacemaker (PM) implantation according to ACC/AHA/NASPE guidelines [17] including “brady–tachy” sick sinussyndrome, permanent atrial fibrillation with low ventricularresponse and supra-Hisian permanent second- or third-
degree AV block (AVB). Patients with concomitant indica-tions for implantable cardioverter defibrillator (ICD) werealso included.
Hb conduction was considered to be preserved whenQRS duration was < 120 ms and HV interval was < 65 ms.
Patients with indication for cardiac resynchronizationpacing therapy (CRT) [18], who refused a potentially time-demanding implantation procedure or who could benefit bynew pacing algorithms of minimal ventricular pacing wereexcluded.
All patients provided written informed consent beforeimplantation. The study complies with the Declaration ofHelsinki and institutional ethical committee approved theresearch protocol.
Eligible patients underwent the following baselineassessments: NYHA class, M-mode and 2D-Dopplerechocardiography and measurement of QRS interval by12-lead ECG recordings.
After this initial evaluation, study participants underwentan electrophysiologic study and then an implantationattempt of permanent HP.
Patients with an effective permanent HP implant wereenrolled in the study.
2.2 Electrophysiological study
The purpose of the electrophysiological study was to assessthe status of AV conduction and to identify the sitesselected for the following permanent HP implantationattempt.
The patient was brought to the electrophysiologylaboratory in the fasting, unsedated state. Satisfactoryconscious sedation were achieved during the procedure bymeans of intravenous infusion of midazolam and fentanyl.Two 4-polar fixed-curve or deflectable diagnostic electrodecatheters were inserted through the femoral venous accessand placed in the Hb region and RV apex or high lateralright atrium.
The Hb diagnostic catheter was positioned at the apicalpart of the Koch’s triangle to record the sites with optimalHb potential recordings and adequate Hb pace-mapping.These dots were marked on the screen by means of a 20°RAO view projection so that they could be easily relocatedduring permanent HP implantation. Frequently (12 patients),this micrometric mapping was assisted by a nonfluoroscopicmapping system (Localisa, Medtronic, Inc.).
Direct HP was defined as Hb-mediated ventricularcapture with QRS-T wave morphology identical to sinusrhythm and an isoelectric tract (> 25 ms) between thepacing stimulus artifact and the beginning of the QRScomplex (similar to HV interval ± 3 ms) (Fig. 1). At higherpacing output levels the basal RV septum was alsofrequently captured with a slight widening of the QRS
82 J Interv Card Electrophysiol (2006) 16:81–92

duration and an early slurred “delta wave-like” segment ofthe QRS complex (Fig. 1).
Para-Hisian pacing (PHP) was defined when, at lowerpacing output, anterobasal RV septum capture was obtainedin the presence of wide QRS complexes, left bundle branchblock (LBBB) pattern and “normal” axis, while at higheroutput, narrowing of QRS with ventricular fused beats andshortening of concomitant retrograde atrial conductionindicated the indirect capture of the Hb/proximal rightbundle branch [19].
2.3 Implantation of permanent Hb pacing lead
Subclavian venipuncture was used to insert a coronarysinus diagnostic quadripolar electrode catheter (to betterdisplay the three-dimensional configuration of the Koch’striangle) and, subsequently, a permanent HP lead.
A 4.1 Fr active fixation lead with a 2-mm long non-retractable screw at the tip (Select Secure, model 3830;Medtronic, Inc.) was positioned by using a 9 Fr steerablecatheter as an introducer tool (Select Site, model 10634 or10635, Medtronic, Inc.) in the target region.
Screw-in lead fixation was guided by direct endocardialpace-mapping (at output level < 3 V at 0.5 ms pulse width),after marking on the Rx screen the supra-tricuspidal site ofKoch’s triangle with the lowest Hb pacing threshold andhighest amplitude of Hb potential recordings.
Fluoroscopy and procedural times were calculated.
2.4 Selection and programming of devices
Patients in sinus rhythm with sick sinus syndrome receivedEnrhythm (model P1501DR) or Enpulse (model E2DR03)dual-chamber pacemakers (Medtronic, Inc.). Right atrialappendage (model 4574, Medtronic, Inc.) and HP leadswere then connected to the atrial and ventricular channelsof the device, respectively.
Patients with sinus rhythm and associated permanent AVblock received an additional back-up RVAP lead and wereimplanted with an Insync III pacemaker (model 8042,Medtronic Inc.), in which the HP lead was connected to the“LV port” of the device and the RVAP lead to its “RV port.”An 80 ms delay was programmed between the two stimuli,with the HP channel as the first pacing site, followed by anon-capturing RVAP stimulus delivered during the non-excitable period of the ventricle.
The RVAP lead not only provides back-up pacing in theevent of HP lead exit block or the development of infra-Hisianconduction block, above all, it ensures adequate RV sensing.
In patients with permanent atrial fibrillation and low ven-tricular response (due to associated AV nodal conductiondefect), a two-lead (HP lead and RVAP lead as a back-up)arrangement was used; in this latter configuration, dual-chamber pacemakers were implanted, with the Hb leadconnected to the “atrial port” of the device and with theshortest interval (i.e., 80 ms) between the HP and the RVAPchannels.
Fig. 1 Surface ECG recordingsin the same patient during SR(left), during HP(center) andduring H+SP (right). SR: Sinusrhythm; HP: direct His bundlepacing; H+SP: His bundle andadjacent ventricular septumpacing. LL: Limb leads.PL: Precordial leads
J Interv Card Electrophysiol (2006) 16:81–92 83

In all patients with sinus rhythm, the paced AV intervalwas programmed according to Doppler echocardiographyto obtain the best diastolic filling pattern (according to theiterative method) and resulting in the greatest stroke volume[20].
All patients with a concomitant indication for an ICDreceived a three-lead system, the defibrillation lead beingused as both RVAP and sensing lead.
2.5 Comparative pacing protocols
In patients with sinus rhythm, sequential activation of theright atrium and Hb was performed at a fixed heart rateranging from 70 to 90 bpm, after optimizing the “AV”interval delay on the basis of mitral valve Doppler flowpattern. This pacing mode was then compared with dual-chamber DDD RVAP.
In patients without a back-up RVAP lead, dual-chamberDDD RVAP was obtained by using a temporary RVAP leadinserted through a transvenous femoral route. In the eventof preserved nodal AV conduction, the AV paced intervalwas shortened to maximize the aberrancy of QRS mor-phology on the 12-lead surface electrocardiogram and theamount of ventricular activation due to the RVAP lead eventhough mitral diastolic flow pattern was suboptimal.
In patients with permanent atrial fibrillation, the RVapical VVI pacing mode was compared with HP pacing atthe same pacing rate of 70–90 bpm.
During HP, low energy output was used to ensureisolated capture of the Hb, while high output pacingensured the combined capture of both the Hb andventricular septum (H+SP). Patients with PHP and indirectcapture of the Hb/proximal right bundle branch wereassigned to the H+SP group for the purposes of analysis.
In order to compare site-specific effects, each pacingmodality (right ventricular apical pacing, His bundle pacingand combined His bundle and septum pacing) was main-tained for at least 15 min. Subsequently, the echocardio-graphic measurements described below, were assessed foreach pacing site.
2.6 Echocardiographic evaluation of ventriculardyssynchrony and function
The m-mode echocardiographic tracings and the Dopplerand Tissue Doppler imaging (TDI) waveforms wererecorded at a paper speed of 100 mm/s on a videotape forlater analysis.
The echocardiographic exam was performed sequentiallyby a single sonographer during HP, H + SP and RVAP onthe same day as the implantation procedure (after closure ofsurgical wound) or the following day.
Echocardiographic images of the LV chamber wereacquired in the standard views as recommended by theAmerican Society of Echocardiographic Committee [21].
The Doppler sample volume was placed at the tips of themitral leaflets, and the LV inflow waveforms were obtainedfrom the apical 4-chamber view, to optimize the paced AVinterval.
Aortic and pulmonary systolic flows were sampled justbelow the valve from the apical 4-chamber view andparasternal short-axis view, respectively, to assess the inter-ventricular activation delay.
TDI waveforms were recorded to assess the left intra-ventricular activation delay.
LV (or RV) electromechanical delay was defined as thetime from the beginning of the QRS interval to the onset ofaortic (or pulmonary) outflow.
Interventricular electromechanical delay (IVD) wasassessed as the difference between the LV electromechan-ical delay and the RV electromechanical delay [22].
Regional electro-mechanical delay time was defined asthe time from the beginning of the QRS (or pacing artifactstimulus) and the onset (or early peak) of TDI systoliccontraction velocity of the four basal LV segments.
Septal to left posterior wall motion delay (SPD) wasdefined as the shortest time interval between the maximalexcursion of the LV septum and that of the LV posteriorwall, as determined by m-mode echocardiography in theparasternal short-axis view at the papillary muscle level[23].
Maximal difference between TDI systolic velocities(TDId) of two of the four basal LV segments was definedas the difference between the maximum and minimumvalue of each regional electro-mechanical delay (using thefirst peak or alternatively, in the event of not straightfor-ward evaluation, the onset of systolic contraction velocity)for all basal LV segments [24, 25].
Mitral regurgitation flow (MR) was assessed by de-termining the effective regurgitant orifice area (EROA)using standard formulae (EROA= regurgitant flow/maxi-mal mitral regurgitant velocity) by means of the proximalisovelocity surface area (PISA) method, as previously de-scribed. Color flow imaging of MR was optimized with asmall color angle from the apical window. The color flowat zero baseline was shifted downward to increase hemi-spheric PISA. The negative aliasing velocity was generallyadjusted from 20 to 40 cm/s to obtain satisfactory hemi-spheric PISA [26].
Myocardial performance index (MPI) was calculated,only in patients with sinus rhythm, as the ratio between thesum of isovolumetric contraction (ICT) and relaxationtimes (IRT) divided by the left ventricular ejection time(LVET), according to the standard formula: MPI ¼LVET=ICTþ IRT [27].
84 J Interv Card Electrophysiol (2006) 16:81–92

IVD was evaluated as an index of interventriculardyssynchrony; SPD and TDId were evaluated as indexesof left intraventricular dyssynchrony and MR and Tei indexas correlated functional parameters of the left ventricle.
For all standard echocardiographic, Doppler and TDImeasurements, reported values are the mean of measure-ments taken from three cardiac cycles.
In our laboratory, the values of intra-observer variabilityin repeated measures of time to onset of systolic flow byPulsed-wave (PW) Doppler recordings and electromechan-ical systolic delay by TDI Doppler exam were 5 and 6%,respectively. In the core laboratory, the values of inter-observer variability in assessing TDI septal and lateralregional electromechanical delay were 3 ± 3 and 3 ± 2 ms,respectively.
2.7 Electrocardiographic pattern and follow-up
Twelve-lead ECGs were recorded with the patient at rest ina supine position. Recordings were calibrated at 0.1 mV/mm at a paper speed of 50 mm/s. QRS width was measuredfrom either the onset of the native QRS interval or theartifact of the pacing stimulus.
All patients underwent clinical assessment by means of a12-lead electrocardiogram, standard 2D echocardiogramand telemetric check of implanted devices, 24 h, 2, 6 and12 months after implantation. RVAP, HP and H+SP pacingthresholds, impedances, and ventricular sensing weremeasured during periodical follow-up visits.
2.8 Statistical analysis
Continuous data were expressed as mean ± standard devi-ation. Differences between continuous variables wereassessed by using a Student t-test, and comparisons amonggroups were carried out by the GLM Repeated Measuresprocedure; the statistical significance level was defined as pvalue < 0.05. Analyses were performed with SPSS 12.0software for Windows.
3 Results
3.1 Patients’ baseline characteristics
Between July 2004 and November 2005, 24 of 45 screenedpatients were eligible and underwent an HP implantationattempt. One patient was not enrolled because of failure ofthe HP implant. Of the 23 enrolled patients undergoingeffective permanent HP implantation (11 women, mean age75.1 ± 6.4 years), 11 were affected by “brady–tachy” sicksinus syndrome, seven by permanent atrial fibrillation withlow ventricular response, five by supra-Hisian second- or
third-degree AVB (one complete AVB was due to trans-catheter AV node ablation). Main etiologies of cardiacdisease were arterial hypertension (9) or myocardialischemia (2). Seven patients had no structural heart disease.Mean left ventricular ejection fraction was 43.2 ± 8.9%.
Two of 23 patients, who also had either recurrentsustained ventricular tachycardias or idiopathic dilatedcardiomiopathy with severe left ventricular dysfunctionand absence of dyssynchrony, underwent a concomitantimplantation of a cardioverter defibrillator lead.
Baseline clinical characteristics of study patients aresummarized in Table 1.
Of the 23 study patients, SPD analysis, TDI analysis,IVD analysis, MR and Tei index evaluation were effective-ly performed in 21, 21, 20, 21 and 16 patients, respectively.In the remaining cases, adequate echocardiographic win-dow, absence of MR or atrial fibrillation (Tei index) limitedthe echocardiographic assessment.
3.2 Implant and electrical data
Of 23 patients with permanent HP, direct HP was obtainedin 17 patients and PHP in six patients.
HP was obtained by maneuvering the deflectablecatheter from above the tricuspid valve, while PHP wasobtained by fixing the lead across or just beneath thetricuspid valve annulus. In one patient Hb capture was notobtained even at high pacing outputs (5V/1 ms) either fromthe diagnostic or from the permanent Hb lead. Since only
Table 1 Patients’ clinical characteristics and demographics
Baseline clinical characteristics
Number of patients 23Age (years) 75.1 ± 6.4Male 12NYHA functional class I 15
II 3III 1
Structural heart disease IHD 2HHD 9VHD 1DCM 1CPD 3
Ejection fraction (%) 43.2 ± 8.9Cardiac pacing indications PAF 7
SSS 11AVB 5
Baseline QRS duration (ms) 108 ± 24
IHD: Ischemic heart disease; HHD: hypertensive heart disease; VHD:valvular heart disease; DCM: dilated cardiomyopathy; CPD: chronicpulmonary disease; PAF: permanent atrial fibrillation with lowventricular response; SSS: sick sinus syndrome (brady–tachy); AVB:sinus rhythm and second or third-degree supra-Hisian atrioventricularblock
J Interv Card Electrophysiol (2006) 16:81–92 85
high right ventricular septal pacing was obtained in thiscase, the patient was not enrolled in the study.
A median number of two attempts (range 1–5) wereneeded to adequately fix the Hb screw-in lead.
Mean procedural and fluoroscopy exposure times were135.7 ± 18.1 min (range 106 –147) and 10.2 ± 4.1 min,respectively (in addition, 2.3 ± 1.6 min were needed for theelectrophysiology study performed before the pacemaker orICD implantation).
Pacing thresholds, impedance and sensed potentials of theHb lead, recorded 30–60 min after lead fixation and at thelast follow-up examination, were 1.61 ± 0.55 V and 1.71 ±0.92 V at a pulse width of 0.5 ms, 552 ± 89 and 525 ±101 ohm, 4.32 ± 2.77 and 4.17 ± 3.63 mV, respectively.
There were no adverse events during the procedure.All HP leads were positioned at the time of first
implantation procedure.
Mean follow-up time of pts was 225 ± 87 days (range85–687).
3.3 Echocardiographic parameters of ventricularsynchronism
Mean values ( ± SD) of echocardiographic parameters,including inter- and intra-ventricular synchronism are listedin Table 2.
3.3.1 Interventricular dyssynchrony
The mean value of IVD was 41.2 ± 12.6 ms during RVAP,vs 4.7 ± 16.8 ms during HP (p < 0.05) and 4.6 ± 5.1 msduring H+ SP (p < 0.05).
IVD, which is the relative difference between the onsetof aortic and pulmonary systolic flow onset, was shortened
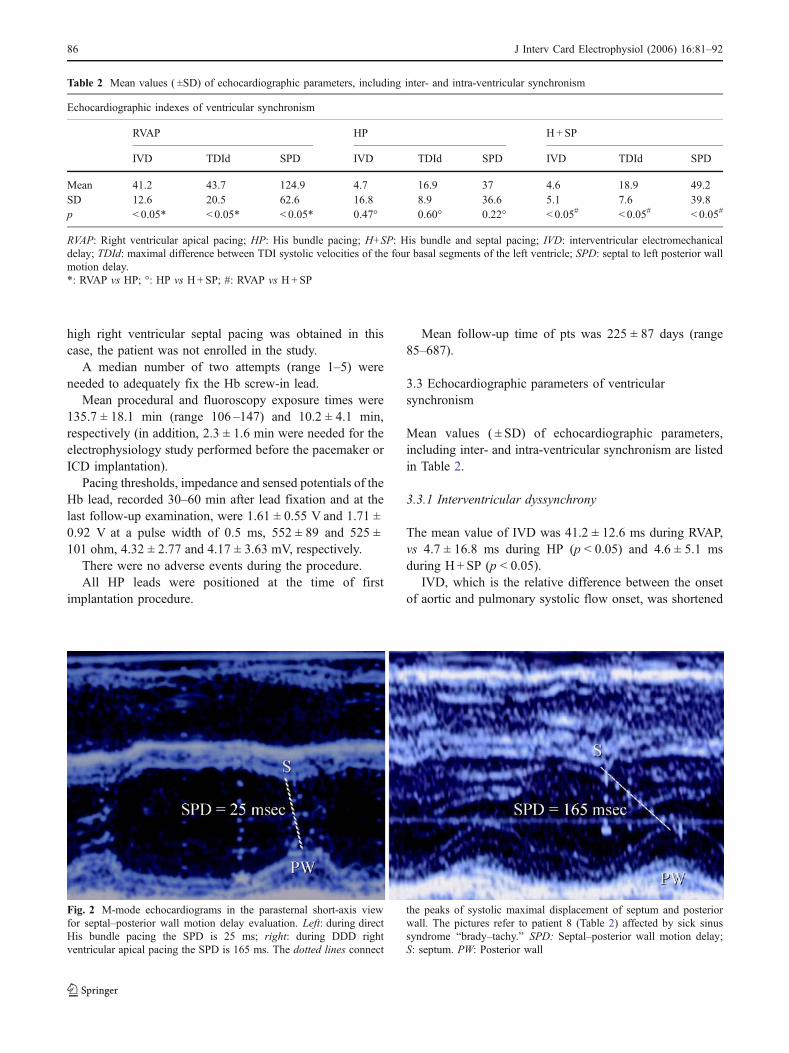
Fig. 2 M-mode echocardiograms in the parasternal short-axis viewfor septal–posterior wall motion delay evaluation. Left: during directHis bundle pacing the SPD is 25 ms; right: during DDD rightventricular apical pacing the SPD is 165 ms. The dotted lines connect
the peaks of systolic maximal displacement of septum and posteriorwall. The pictures refer to patient 8 (Table 2) affected by sick sinussyndrome “brady–tachy.” SPD: Septal–posterior wall motion delay;S: septum. PW: Posterior wall
Table 2 Mean values ( ±SD) of echocardiographic parameters, including inter- and intra-ventricular synchronism
Echocardiographic indexes of ventricular synchronism
RVAP HP H+SP
IVD TDId SPD IVD TDId SPD IVD TDId SPD
Mean 41.2 43.7 124.9 4.7 16.9 37 4.6 18.9 49.2SD 12.6 20.5 62.6 16.8 8.9 36.6 5.1 7.6 39.8p < 0.05* < 0.05* < 0.05* 0.47° 0.60° 0.22° < 0.05# < 0.05# < 0.05#
RVAP: Right ventricular apical pacing; HP: His bundle pacing; H+SP: His bundle and septal pacing; IVD: interventricular electromechanicaldelay; TDId: maximal difference between TDI systolic velocities of the four basal segments of the left ventricle; SPD: septal to left posterior wallmotion delay.*: RVAP vs HP; °: HP vs H+SP; #: RVAP vs H+SP
86 J Interv Card Electrophysiol (2006) 16:81–92

by a mean value of 35.4 ± 16.3 ms during HP and of 36.2 ±15.6 ms during H+SP in comparison with RVAP.
3.3.2 Intraventricular dyssynchrony (Fig. 2)
The mean value of SPD was 124.9 ± 62.6 ms during RVAP,vs 37 ± 36.6 ms during HP (p < 0.05) and 49.2 ± 39.8 msduring H+ SP (p < 0.05).
The mean value of TDId was 43.7 ± 20.5 ms duringRVAP, vs 16.9 ± 8.9 ms during HP (p < 0.05) and 18.9 ±7.6 ms during H+SP (p < 0.05).
Indexes of left intraventricular electromechanical delaysignificantly improved during HP and H+SP, with a meandecrease in SPD of 87.9 ± 42.7 during HP and of 93.6 ±36.5 during H+SP and a mean decrease in the TDId indexof 26.8 ± 22.4 during HP and 24 ± 10.2 ms during H + SP.
Cut-off values of 30 ms for IVD, 110 ms for SPD and25 ms for TDId adequately separated the two groups ofdata: on RVAP, 91%, 89% and 95% of the values of IVD,SPD and TDId, respectively, were equal to or higher thanthe cut-off values, while 100%, 100% and 95% of thecorresponding values on HP pacing were lower than thesereference values, as shown in figures (Fig. 3).
3.3.3 Mitral valve regurgitation
MR was observed and adequately quantified in 21 patients.During HP and H+ SP, mitral regurgitation, as assessed
by EROA area calculation, was 15.9 ± 8.3 and 15.7 ± 5.2(15.8 ± 7.3 on combining the two groups), while duringRVAP it was 19.1 ± 8.3 (p < 0.05). No statistical differenceswere observed between the HP and H+SP groups (p =0.95, n.s.).
3.3.4 Myocardial performance index
During RVAP, systolic function, assessed by echocardio-graphic Tei index, deteriorated from a mean value of 0.53 ±0.04 during HP (p < 0.005) and 0.59 ± 0.08 during H+SP(p = 0.01) to a mean value of 0.85 ± 0.14 (p = 0.0004 and0.01, respectively). No statistical differences were observedbetween the HP and H+SP groups (p = 0.11, n.s.).
In summary, asynchrony echocardiographic indexes ofinter- and intra-ventricular delay were significantly reducedduring both HP and H+SP in comparison with RVAP.
Moreover, no statistically significant differences wereobserved between HP and H+SP.
4040
8080
120120
160160
200200
240240
124,9124,9
373749.249.2
SPDSPD
RVAPRVAP HPHP H+SPH+SP
P < 0.05P < 0.05
P > 0.05P > 0.05
P < 0.05P < 0.05
**
**********
1010
2020
3030
4040
5050
6060
41.241.2
4.74.7 4.64.6
IVDIVD
RVAPRVAP HPHP H+SPH+SP
P < 0.05P < 0.05
P > 0.05P > 0.05
P < 0.05P < 0.05
**
**********
1010
2020
3030
4040
5050
6060
43.743.7
16.916.918.918.9
TDIdTDId
RVAPRVAP HPHP H+SPH+SP
P < 0.05P < 0.05
P> 0.05P> 0.05
P < 0.05P < 0.05
**
**********
* = comparison between HP and H+SP. ** = comparison between RVAP and H+SP. *** = comparison between RVAP and HP.
Fig. 3 Distribution of interventricular electromechanical delay (left),maximal difference between TDI systolic velocities (center) and septalto left posterior wall motion delay (right) values during rightventricular apical pacing, His bundle pacing and combined pacing ofHis bundle and adjacent ventricular septum. Data are reported as meanvalue ± standard deviation, indicated by horizontal bars. Individualvalues are plotted as black dots. Cut-off values for interventricularelectromechanical delay of 25 ms, for maximal difference between
TDI systolic velocities of 30 ms and for septal to left posterior wallmotion delay of 110 ms discriminate right ventricular apical pacingfrom the other two pacing sites. IVD: Interventricular electromechan-ical delay. TDId: Maximal difference between TDI regional systolicvelocities (TDId). SPD: Septal to left posterior wall motion delay(SPD). RVAP: Right ventricular apical pacing. HP: His bundle pacing;H+SP: ventricular septum and His bundle pacing
J Interv Card Electrophysiol (2006) 16:81–92 87

3.4 ECG pattern
The mean paced QRS duration was 112 ± 27 ms on HPimplantation, and 109 ± 26 ms at the last follow-upexamination. These values are similar to the baseline meanvalue of the native QRS width of 108 ± 24 ms (p = n.s.).
3.5 Follow-up and troubleshooting
No lead dislodgment, exit block or significant changes inpacing threshold were observed during follow-up in ourstudy patients.
In three patients with sinus rhythm and 2-lead configu-ration (atrial and HP leads connected to a dual-chamberdevice), sensing-related problems (ventricular undersensingor atrial oversensing with cross-talking inhibition) wereobserved, one on implantation and the remaining twoduring follow-up.
In the first patient, who had ventricular undersensing ofthe Hb lead, an RVAP lead was added and connected to theLV port of a CRT device.
In the second patient, who had a remote myocardial in-farction, ventricular undersensing developed after 6 monthsof follow-up both during bigeminal ventricular extrasystolic
Fig. 4 Surface ECG recording(precordial leads) of a patientwith brady–tachy syndrome andpost-myocardial infarction car-diomyopathy (with moderateventricular dilation but withoutbasal dyssynchrony): after 6-month from the atrio-Hisianpacemaker implantation, occur-rence of a concomitant episodeof atrial fibrillation and sus-tained ventricular tachycardia.Automatic mode switch wasactivated. Note the undersensingof ventricular activity by the Hisbundle lead with asynchronousineffective His-bundle pacingand the fusion beat induced bythe fourth pacing stimulus. Ven-tricular undersensing defect wassolved by inserting a third rightventricular apical defibrillatorlead during upgrading of pace-maker to an atrio-Hisianimplantable cardioverter-defibrillator
88 J Interv Card Electrophysiol (2006) 16:81–92

rhythm and during syncopal episodes of sustained ventric-ular tachycardias (not related to lead malfunction) due tothe low amplitude and slew rate of ventricular intrinsic de-flection recorded by the HP lead. A back-up sensing/pacingand defibrillator RVA lead was then added to up-grade thedevice from “atrio-Hisian” pacemaker to dual-chamber“atrio-Hisian” implantable cardioverter-defibrillator withadequate ventricular sensing ensured by the defibrillatorlead (Fig. 4).
In the last patient, oversensing of atrial activity inhibitedHP during transient atrial fibrillation episodes, althoughduring sinus rhythm the device worked properly. Also inthis case, after 2 months of follow-up, an RVAP lead wasinserted and connected to the “RV port” of a biventriculardevice, which replaced the originally implanted dual-chamber device to avoid cross-talking effects.
4 Discussion
In recent years, growing evidence has suggested thatdyssynchrony has a considerable clinical impact on thedeterioration of ventricular function and the progression ofheart failure. Indeed, many randomized clinical trials haveshown that CRT induces a significant benefit by reducingspontaneous dyssynchrony due to left bundle branch blockin patients with dilated cardiomyopathy. Moreover, recentstudies have shown that RVAP is associated with pooreroutcomes, inducing depression of systolic and diastolicventricular function [8–13].
By comparing AAI(R) and either VVI or DDDR modesof pacing, the Danish trials have clearly documented thelong-term detrimental effects of non-physiologic RVAP[1,4]. In contrast, studies comparing DDD (DDDR) with VVI(VVIR) modes of pacing have yielded neutral and some-what unexpected results [2, 3, 5–7]. DAVID trial revealed amore marked depressant role of RVAP in patients withbasal ventricular dysfunction [7].
Ventricular desynchronization induced by RVAP mayunderlie these unfavorable effects.
Minimizing RVAP can be done either by using dedicatedpacing algorithms [28] or by pacing via alternative ventric-ular sites.
Direct HP could be the ideal way to avoid ventriculardyssynchrony, in that it provides rapid, synchronized, electri-cal activation through the specialized conduction system.Vassallo et al. authors previously demonstrated that the tem-poral dispersion of left intraventricular segmental contractionis minimized during sinus rhythm, mainly owing to the rapidelectrical recruitment of the remote basal regions of the LV.This proved clearly different from the dispersion of theelectromechanical activation induced by RVAP, with slowerconduction to the basal segments of the LV free wall [29].
After preliminary experimental data reporting successfulHP [30], Deshmukh et al. recently applied the HP techniqueto humans[14, 15]. Hemodynamical improvements due toHP were seen during mid-term follow-up in candidates for“ablate and pace” therapy affected by dilated cardiomyop-athy and atrial fibrillation with high ventricular response,although positive effects of direct HP reported by the authorscould also have been due to ventricular rate control.
Although some data are available on high right ventric-ular septum pacing [31, 32], no data have yet been reportedon the effects of HP on ventricular synchronism in com-parison with those of RVAP. The present study showed thatthe HP technique can prevent the left ventricular dyssyn-chrony acutely induced by RVAP and its consequenceson mitral valve competence and global systolic ventricularperformance.
Favorable effects of HP were observed in our patientpopulation, both on interventricular and on left intraven-tricular synchronism. More than 80% of our patients had atleast one asynchrony criterion induced by RVAP, incomparison with only 9% of patients when either HP orH+SP was implemented. The asynchrony-related effectswere more marked in patients with some degree of basalventricular dysfunction, which could represent substratesthat are more vulnerable to dyssynchrony [7].
The echocardiographic dyssynchrony indexes used in thepresent study have been largely adopted in the literature toassess baseline asynchrony in patients candidates to CRT,because of their high reliability. In particular, SPD analysis,although of limited value in cases of septal or inferiormyocardial infarction, is indicative of circumferential LVdyssynchrony. Moreover, the TDI echocardiographic anal-ysis of LV basal segments is generally related to longitu-dinal left intraventricular dyssynchrony.
In our patient population, systolic asynchrony betweenseptal and lateral apical segments of the left ventricle wereobserved only during RVAP, although low TDI systolicvelocity precluded a reliable quantitative evaluation of mid-apical regions of the ventricle.
Mitral regurgitation and the Tei index, which is a reliableechocardiographic index of global systolic performance ofthe left ventricle, were also more favorably influenced byHP than by RVAP.
The data from the present study are the first to confirmthe theoretical assumption that HP, because it creates anelectrical ventricular activation that spreads through thespecific conduction system, does not induce ventricularmechanical dyssynchrony.
Our study examined both para-Hisian pacing andcombined pacing of the Hb and adjacent septum. Owingto our supravalvular approach to HP implantation, a highdegree of discrimination between the thresholds of Hb andof the adjacent ventricular myocardium was observed—
J Interv Card Electrophysiol (2006) 16:81–92 89
higher than that obtained by means of an infravalvular and/or para-Hisian approach, which is more frequently associ-ated with a marginal difference. Therefore, the effects ofisolated HP, in comparison with those of RVAP, could bedistinguished from the effects of combined capture of theHb and septum, which was obtained at higher levels ofoutput in HP group patients.
Beneficial effects on synchronism and ventricular func-tion were also observed with this “hybrid” pacing. This wasprobably because rapid activation of the ventricles due tothe specialized conduction system predominated over theconcomitant slower activation of the adjacent myocardiuminduced by associated septal pacing.
No differences were observed between HP and H+ SP,although we cannot rule out the possibility that small dif-ferences might have gone undetected owing to the limitedsample size of the para-Hisian group. Both direct and indi-rect HP can therefore be regarded as ideal and physiologicpacing modalities in patients with permanent atrial fibrilla-tion with low ventricular response, sick sinus syndrome and/or supra-Hisian AVB, without associated infra-Hisian andintraventricular conduction delay.
HP, in fact, could be more physiologic than biventricularpacing namely in the absence of basal asynchrony or ad-vanced LV dysfunction since, unlike biventricular pacing, itcan restore the natural septal twisting motion [33], as re-cently shown by Saleh et al.
4.1 Can we afford to rely on the His bundle pacingtechnique as an effective therapeutic option?
As recent technological refinements have made the proce-dure of HP lead implantation more feasible and moreflexible, we had an implant success rate of 95% in ourpatient population [16].
Even though HP sometimes offers some technicalchallenges compared to conventional RVAP, mean implan-tation time resulted similar to that of a biventricular pacing.Nevertheless, it is still unclear if HP can be proposed as aprimary approach to lead placement or as an upgradingprocedure, should haemodynamic deterioration develop.
The supravalvular (atrial) approach to HP was thepreferred technique of implantation used in this study.
Some concerns remain about ventricular sensing duringHP, particularly with regard to ventricular extrasystoles ortachycardias or the oversensing of atrial activity during atrialtachyarrhythmias. These concerns stem from the proximityof the HP site to right atrial chamber, in particular usinga supravalvular approach. For these reasons, an RV apicalsensing back-up lead was inserted in all the patients in ourseries in whom this approach was adopted. With this ap-proach, only the back-up RVAP lead was effectively insertedinto the right ventricle; this avoided the insertion of two leadswithin the tricuspid annulus, which is one of the potentiallimitations to bifocal right ventricular pacing.
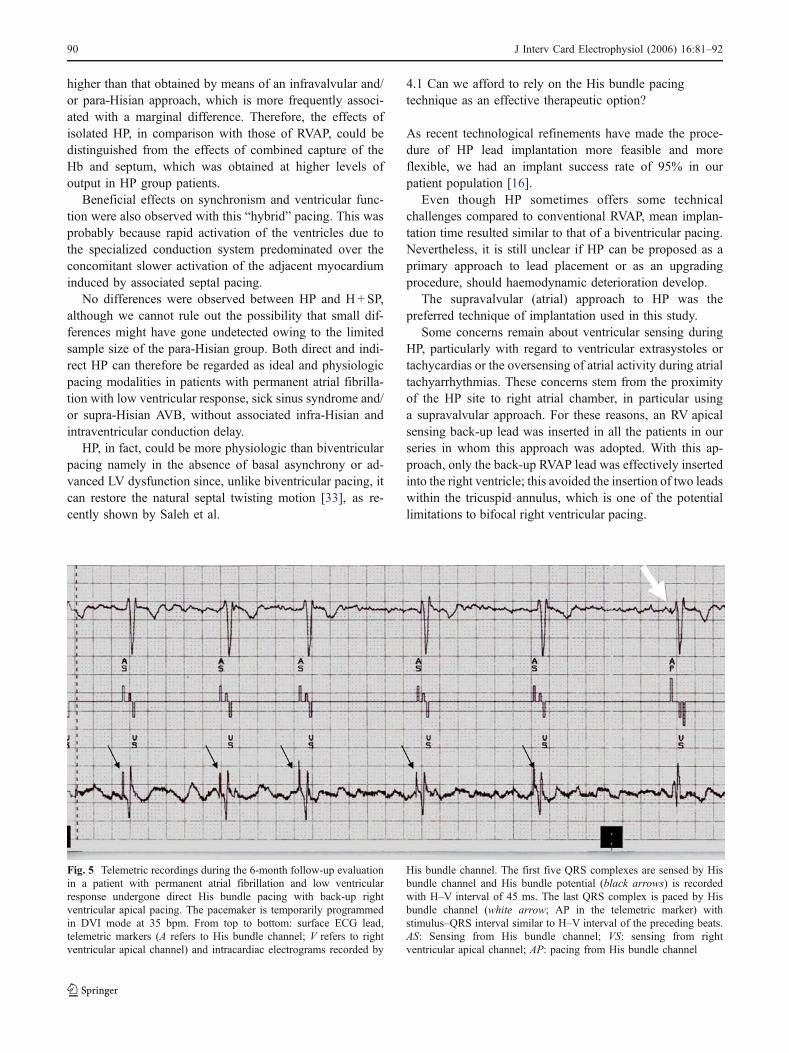
Fig. 5 Telemetric recordings during the 6-month follow-up evaluationin a patient with permanent atrial fibrillation and low ventricularresponse undergone direct His bundle pacing with back-up rightventricular apical pacing. The pacemaker is temporarily programmedin DVI mode at 35 bpm. From top to bottom: surface ECG lead,telemetric markers (A refers to His bundle channel; V refers to rightventricular apical channel) and intracardiac electrograms recorded by
His bundle channel. The first five QRS complexes are sensed by Hisbundle channel and His bundle potential (black arrows) is recordedwith H–V interval of 45 ms. The last QRS complex is paced by Hisbundle channel (white arrow; AP in the telemetric marker) withstimulus–QRS interval similar to H–V interval of the preceding beats.AS: Sensing from His bundle channel; VS: sensing from rightventricular apical channel; AP: pacing from His bundle channel
90 J Interv Card Electrophysiol (2006) 16:81–92

No lead dislodgment(or exit block) was observed onshort–medium-term follow-up.
However, the mean Hisian pacing threshold was higherthan the RVAP; this was probably due to the fibroticisolation of the conducting tissue of the Hb within themembranous septum. Despite its protective role, thisenvelope increases the distance between the electrode tipand the excitable target tissue and the pacing threshold.However, technical progress in the design of electrode tips(longer helix, porous or inert electrical interface) couldincrease the active pacing surface area, thereby reducing theelectrical polarization impedance.
QRS width and pattern remained narrow and stableduring follow-up. Monitoring of the QRS width andmorphology and of the pacing stimulus–QRS interval maybe useful in assessing the status of the distal conductionsystem (Fig. 5). Moreover in some patients the telemetricrecording of Hb potential can be obtained and the directassessment of H–V interval can be no invasively per-formed. However, in our patients no intraventricularconduction disorder or progression of distal conductiondisease was observed.
Although these preliminary data suggest that this pacingsite is reliable, longer periods of follow-up are needed toassess its long-term reliability and electrical stability ofpacing thresholds.
5 Study limitations
In this study, only acute variations in ventricular synchro-nism and systolic function were evaluated. Acute responsesmay be related to chronic beneficial responses, although itis as yet unclear whether acute effects predict long-termclinical benefit and prevent the induction of unfavorable LVremodeling. In any case, the clinical status of patients wasameliorated or at least unchanged during follow-up.
The indexes of asynchrony used in the present studyrefer to the analysis of left intraventricular basal segments,although basal dyssynchrony of contraction (and relaxation)may not reflect the degree of asynchrony in all patients. Onthe other hand, in LBBB or CRT studies, these indexes arecommonly used to correlate either deterioration or im-provement of dyssynchrony and ventricular function. Insome patients, non-basal regions may be the sites ofasynchrony, which is best detected by a three-dimensionalimaging technique. However, m-mode and TDI Doppleranalysis of basal dyssynchrony might actually underesti-mate the benefits of HP.
In spite of these limitations, the data were statisticallysignificant and demonstrated the differences between theregional timings of LV contraction induced by conventionalpacing in comparison with HP.
6 Conclusions
Hisian and para-Hisian pacing techniques are feasible andsafe, and require a relatively low radiological exposure andlimited implantation time. They do not induce ventriculardyssynchrony, which is common during conventionalRVAP. Although long-term follow-up is necessary in orderto assess the effective and safe performance of this pacingmodality and its efficacy on chronic ventricular synchro-nism and function, our data are rather encouraging.
Acknowledgments The authors thank Dr. Chiara Salgarello, Ph.D.,who is an employee of Medtronic, Inc., and the technical staff of ourelectrophysiology laboratory (Coletti M., Pangrazzi C., Simoncelli M.,Tomasi G. and Marisa M.), for their technical assistance and supportboth during the implantation procedure and the follow-up analysis.
Conflict of interest statement There is no conflict of interest inconnection with the submitted article for the other authors. Nofinancial support was given to the study.
References
1. Andersen, H. R., Nielsen, J. C., Thomsen, P. E., et al. (1997).Long-term follow-up of patients from a randomised trial of atrialversus ventricular pacing for sick-sinus syndrome. Lancet, 350(9086), 1210–1216.
2. Connolly, S. J., Kerr, C. R., Gent, M., et al. (2000). Effects ofphysiologic pacing versus ventricular pacing on the risk of strokeand death due to cardiovascular causes. Canadian trial ofphysiologic pacing investigators. New England Journal ofMedicine, 342(19), 1385–1391.
3. Lamas, G. A., Lee, K. L., Sweeney, M. O., et al. (2002). Modeselection trial in sinus-node dysfunction. Ventricular pacing ordual-chamber pacing for sinus-node dysfunction. New EnglandJournal of Medicine, 346(24), 1854–1862.
4. Nielsen, J. C., Kristensen, L., Andersen, H. R., Mortensen, P. T.,Pedersen, O. L., & Pedersen, A. K. (2003). A randomizedcomparison of atrial and dual-chamber pacing in 177 consecutivepatients with sick sinus syndrome: Echocardiographic and clinicaloutcome. Journal of the American College of Cardiology, 42(4),614–623.
5. Sweeney, M. O., Hellkamp, A. S., Ellenbogen, K. A., et al.(2003). Mode selection trial investigators. Adverse effect ofventricular pacing on heart failure and atrial fibrillation amongpatients with normal baseline QRS duration in a clinical trial ofpacemaker therapy for sinus node dysfunction. Circulation, 107(23), 2932–2937.
6. Kerr, C. R., Connolly, S. J., Abdollah, H., et al. (2004). Canadiantrial of physiological pacing: Effects of physiological pacingduring long-term follow-up. Circulation, 109(3), 357–362, 27.
7. Sharma, A. D., Rizo-Patron, C., Hallstrom, A. P., et al. (2005).Percent right ventricular pacing predicts outcomes in the DAVIDtrial. Heart Rhythm, 2(8), 830–834.
8. van Oosterhout, M. F., Prinzen, F. W., & Arts, T., et al. (1998).Asynchronous electrical activation induces asymmetrical hyper-trophy of the left ventricular wall. Circulation, 98, 588–595.
9. Rosenqvist, M., Isaaz, K., Botvinick, E. H., et al. (1991). Theimportance of activation sequence compared to atrioventricular
J Interv Card Electrophysiol (2006) 16:81–92 91

synchrony in left ventricular function. American Journal ofCardiology, 67, 148–156.
10. Tse, H. F., Yu, C., Wong, K. K., et al. (2002). Functionalabnormalities in patients with permanent right ventricular pacing:The effect of sites of electrical stimulation. Journal of theAmerican College of Cardiology, 40, 1451–1458.
11. Barold, S. S., & Ovsyshcher, I. E. (2005). Pacemaker-inducedmitral regurgitation. Pacing and Clinical Electrophysiology, 28,357–359.
12. Nahlawi, M., Waligora, M., Spies, S. M., Bonow, R. O., Kadish,A. H., & Goldberger, J. J. (2004). Left ventricular function duringand after right ventricular pacing. Journal of the AmericanCollege of Cardiology, 44(9), 1883–1888.
13. Barold, S. S., & Herweg, B. (2005). Right ventricular outflowtract pacing: Not ready for prime-time. Journal of InterventionalCardiac Electrophysiology, 13, 39–46.
14. Deshmukh, P., Casavant, D., Romanyshyn, M., et al. (2000).Permanent, direct His-bundle pacing. A novel approach to cardiacpacing in patients with normal His–Purkinje activation. Circula-tion, 101, 869–877.
15. Deshmukh, P. M., & Romanyshyn, M. (2004). Direct His-bundlepacing: Present and future. Pacing and Clinical Electrophysiology,27(6 Pt 2), 862–870.
16. Zanon, F., Baracca, E., Aggio, S., et al. (2006). A feasibleapproach for direct His-bundle pacing using a new steerablecatheter to facilitate precise lead placement. Journal of Cardio-vascular Electrophysiology, 17(1), 29–33.
17. Gregoratos, G., Abrams, J., Epstein, A. E., et al. (2002). ACC/AHA/NASPE 2002 guideline update for implantation of cardiacpacemakers and antiarrhythmia devices: Summary article. Areport of the ACC/AHA task force on practice guidelines.Circulation, 106, 2145–2161.
18. Hunt, S. A., Abraham, W. T., Chin, M. H., et al. (2005). ACC/AHA 2005 Guideline update for the diagnosis and management ofchronic heart failure in the adult. Circulation, 112(12), e154–e235.
19. Hirao, K., Otano, K., Wang, X., et al. (1996). Para Hisian pacing.Circulation, 94, 1027–1035.
20. Dubin, J., Wallerson, D. C., Cody, R. J., et al. (1990). Comparativeaccuracy of Doppler echocardiography methods for clinical strokevolume determination. American Heart Journal, 120, 116–123.
21. Schiller, N. B., Shah, P. M., Crawford, M., et al. (1989).Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. Journal of American Society ofEchocardiography, 2, 358–367.
22. Bordachar, P., Lafitte, S., Reuter, S., et al. (2004). Echocardio-graphic parameters of ventricular dyssynchrony validation inpatients with heart failure using sequential biventricular pacing.Journal of the American College of Cardiology, 44, 2157–2165.
23. Pitzalis, M. V., Iacoviello, M., Romito, R., et al. (2002). Cardiacresynchronization therapy tailored by echocardiographic evalua-tion of ventricular asynchrony. Journal of the American College ofCardiology, 40, 1615–1622.
24. Bax, J. J., Bleeker, G. B., Marwick, T. H., et al. (2004). Leftventricular dyssynchrony predicts response and prognosis aftercardiac resynchronization therapy. Journal of the AmericanCollege of Cardiology, 44, 1834–1840.
25. Bader, H., Garrigue, S., Lafitte, S., et al. (2004). Intra-leftventricular electromechanical asynchrony. A new independentpredictor of severe cardiac events in heart failure patients. Journalof the American College of Cardiology, 43, 248–256.
26. Enriquez-Sarano, M., Seward, J. B., Bailey, K. R., et al. (1994).Effective regurgitant orifice area: A non invasive Dopplerdevelopment of an old hemodynamic concept. Journal of theAmerican College of Cardiology, 23, 443–451.
27. Tei, C., Nishimura, R. A., Seward, J. B., & Tajik, A. J. (1997).Noninvasive doppler-derived myocardial performance index:Correlation with simultaneous measurements of cardiac catheter-isation measurements. Journal of the American Society ofEchocardiography, 10(2), 169–178.
28. Sweeney, M. O., Ellenbogen, K. A., Casavant, D., et al. (2005).Multicenter, prospective, randomized safety and efficacy study ofa new atrial-based managed ventricular pacing mode (MVP) indual chamber ICDs. Journal of Cardiovascular Electrophysiology,16, 1–7.
29. Vassallo, J. A., Cassidy, D. M., Miller, J. M., Buxton, A. E.,Marchlinski, F. E., & Josephson, M. E. (1986). Left ventricularendocardial activation during right ventricular pacing: Effect ofunderlying heart disease. Journal of the American College ofCardiology, 7(6), 1228–1233.
30. Karpawich, P., Gates, J., & Stokes, P. (1992). Septal His–Purkinjeventricular pacing in canines: A new endocardial electrodeapproach. Pacing and Clinical Electrophysiology, 5, 2011–2015.
31. Yu, C. C., Lin, L. C., Lu, Y. B., Lin, M. S., Wang, J. Y., & Lin,J. L. (2005). Preservation of left ventricular contractile synchro-nism and diastolic function by right ventricular septal pacing:Implications from tissue Doppler imaging analysis. Circulation,112(17), II-594 (abstr 2812).
32. Occhetta, E., Bortnik, M., Magnani, A., et al. (2006). Preventionof ventricular desynchronization by permanent para-Hisian pacingafter atrioventricular node ablation in chronic atrial fibrillation. Acrossover, blinded, randomized study versus apical right ventric-ular pacing. Journal of the American College of Cardiology, 47,1938–1945.
33. Saleh, S., Liakopoulos, O. J., & Buckberg, G. D. (2006). Theseptal motor of biventricular function. European Journal ofCardio-thoracic Surgery, 29S, S126–S138.
92 J Interv Card Electrophysiol (2006) 16:81–92




















