
Malposition of Transvenous Pacing Lead in the Left Ventricle
9
Malposition of Transvenous Pacing Lead in the Left Ventricle MANSURA GHANI, RANJAN K. THAKUR. DEREK BOUGHNER. CARLOS A. MORILLO, RAYMOND YEE, and GEORGE J. KLEIN From The Department of Medicine, University of Western Ontario, London, Canada GHANI, M., ET AL.: Malposition of Transvenous Pacing Lead in the Left Ventricle. MaJposition 0/pace- maker leads has been described in several locations but rarely in the left ventricle. The incidence and clinical course of this pacemaker complicadon are unknown. We describe clinical, electrocardiographic, chest X ray, and echocardiographic findings in four patients in whom the transvenous pacing lead was inadvertendy placed through the interatriaJ septum and milraJ valve into the left ventricle, in these patients, lead misplacement was not recognized at the time of implantation and lead malposition was diagnosed a mean of 2 years later. All four patients had right bundle branch block configuration paced complexes. In retrospect, chest X rays suggested afypicaJ Jead position in all, but the initial posterior- anterior and lateral chest X rays were misinlerpreled and contributed to the delay in diagnosis. When lead misplacement in (he left ventricle was considered it was confirmed by two-dimensionaJ echocardiog- raphy. One patienf subsequently presented with a stroke and the remainder were diagnosed when they presented with other unrelated problems. Pacing thresholds were normal at the time o/implan(ation and behaved normally during follow-up. The patient presenting with stroke was anticoagulated and the other three have been managed expectantly without anticoagulafion. Diagnosis of left ventricular lead malposition is not difficuh but requires a high index of suspicion. A 12-lead ECC and posterior-anterior and lateral chest X rays after implantation can be diagnostic. Patients with pacing lead in the left ventricle may remain asymptomatic with normal lead function during long-term follow-up. Anticoagulation should be considered when this problem comes to attention for the first time during follow-up (PACE Vol. W, September 1993} pacemaker, lead malposition, pacemaker complication, echocardiography Introduction Malposition of pacemaker lead in the left ven- tricle is an unusual complication.^ This article de- scribes four cases of pacemaker lead malposition in the left ventricle, among patients followed in our pacemaker clinic over the last decade. Lead malposition was not suspected intraoperatively This study was supported by the Heart and Stroke Foundation of Ontario, Toronto, C:anada. Dr. Klein is a Distinguished Re- search Professor of Ihe Heart and Stroke Foundation, Address for reprints: R.K. Thakur, M.D,, University Hospital, 339 Windermere Rd., Box 5339, London, Ontario, Canada N6A 5A5. Fax: (519) 434-3278. Received February 25, 1993; revision March 18, 1993; revision April 20, 1993; accepted April 22, 1993. and on the immediate postoperative chest X rays neither the operators nor the radiologists sus- pected lead malposition. In retrospect, posterior- anterior (PA) and lateral chest X rays and 12-lead EGG were diagnostic of left ventricular lead posi- tion. Two-dimensional echocardiography was confirmatory. This problem can be avoided by a high index of suspicion at the time of implant and confirmed by simple noninvasive techniques. Case 1 In June 1989, a 76-year-old woman presented with a sudden onset of recurrent lightheadedness and one episode of syncope lasting a few seconds. The EGG showed a Mobitz II block with 2:1 and 3:1 conduction. Two-dimensional echocardiogra- 1800 September 1993 PACE, Vol. 16
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Malposition of Transvenous Pacing Lead in the Left Ventricle

Malposition of Transvenous Pacing Lead in theLeft Ventricle
MANSURA GHANI, RANJAN K. THAKUR. DEREK BOUGHNER.
CARLOS A. MORILLO, RAYMOND YEE, and GEORGE J. KLEIN
From The Department of Medicine, University of Western Ontario, London, Canada
GHANI, M., ET AL.: Malposition of Transvenous Pacing Lead in the Left Ventricle. MaJposition 0/pace-maker leads has been described in several locations but rarely in the left ventricle. The incidence andclinical course of this pacemaker complicadon are unknown. We describe clinical, electrocardiographic,chest X ray, and echocardiographic findings in four patients in whom the transvenous pacing lead wasinadvertendy placed through the interatriaJ septum and milraJ valve into the left ventricle, in thesepatients, lead misplacement was not recognized at the time of implantation and lead malposition wasdiagnosed a mean of 2 years later. All four patients had right bundle branch block configuration pacedcomplexes. In retrospect, chest X rays suggested afypicaJ Jead position in all, but the initial posterior-anterior and lateral chest X rays were misinlerpreled and contributed to the delay in diagnosis. Whenlead misplacement in (he left ventricle was considered it was confirmed by two-dimensionaJ echocardiog-raphy. One patienf subsequently presented with a stroke and the remainder were diagnosed when theypresented with other unrelated problems. Pacing thresholds were normal at the time o/implan(ation andbehaved normally during follow-up. The patient presenting with stroke was anticoagulated and theother three have been managed expectantly without anticoagulafion. Diagnosis of left ventricular leadmalposition is not difficuh but requires a high index of suspicion. A 12-lead ECC and posterior-anteriorand lateral chest X rays after implantation can be diagnostic. Patients with pacing lead in the left ventriclemay remain asymptomatic with normal lead function during long-term follow-up. Anticoagulationshould be considered when this problem comes to attention for the first time during follow-up (PACEVol. W, September 1993}
pacemaker, lead malposition, pacemaker complication, echocardiography
Introduction
Malposition of pacemaker lead in the left ven-tricle is an unusual complication.^ This article de-scribes four cases of pacemaker lead malpositionin the left ventricle, among patients followed inour pacemaker clinic over the last decade. Leadmalposition was not suspected intraoperatively
This study was supported by the Heart and Stroke Foundationof Ontario, Toronto, C:anada. Dr. Klein is a Distinguished Re-search Professor of Ihe Heart and Stroke Foundation,
Address for reprints: R.K. Thakur, M.D,, University Hospital,339 Windermere Rd., Box 5339, London, Ontario, Canada N6A5A5. Fax: (519) 434-3278.
Received February 25, 1993; revision March 18, 1993; revisionApril 20, 1993; accepted April 22, 1993.
and on the immediate postoperative chest X raysneither the operators nor the radiologists sus-pected lead malposition. In retrospect, posterior-anterior (PA) and lateral chest X rays and 12-leadEGG were diagnostic of left ventricular lead posi-tion. Two-dimensional echocardiography wasconfirmatory. This problem can be avoided by ahigh index of suspicion at the time of implant andconfirmed by simple noninvasive techniques.
Case 1
In June 1989, a 76-year-old woman presentedwith a sudden onset of recurrent lightheadednessand one episode of syncope lasting a few seconds.The EGG showed a Mobitz II block with 2:1 and3:1 conduction. Two-dimensional echocardiogra-
1800 September 1993 PACE, Vol. 16
PACING LEAD IN THE LEFT VENTRICLE
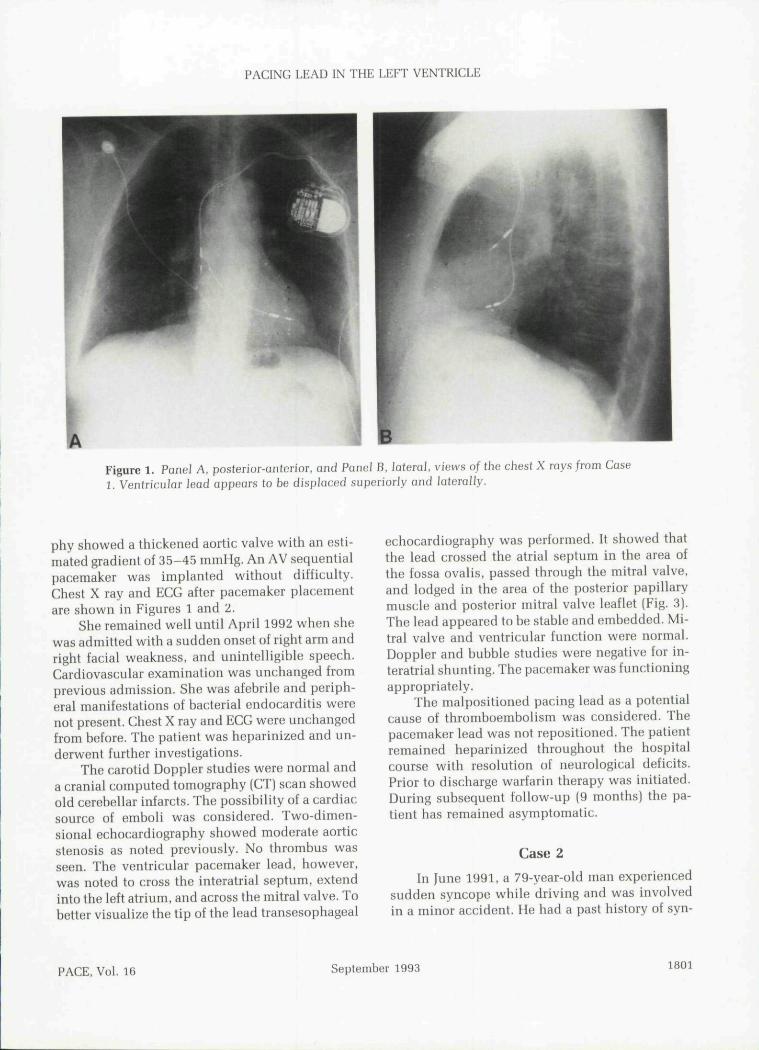
Figure 1. Panel A, posterior-anterior, and Panel B, lateral, views of the chest X rays from Case1. Ventricular lead appears to be displaced superiorly and Itilerally,
phy showed a thickened aortic valve with an esti-mated gradient of 35-45 mmHg. An AV sequentialpacemaker was implanted without difficulty.Chest X ray and ECC after pacemaker placementare shown in Figures 1 and 2.
She remained well until April 1992 when shewas admitted with a sudden onset of right arm andright facial weakness, and unintelligible speech.Cardiovascular examination was unchanged fromprevious admission. She was afebrile and periph-eral manifestations of bacterial endocarditis werenot present. Chest X ray and ECG were unchangedfrom before. The patient was heparinized and un-derwent further investigations.
The carotid Doppler studies were normal anda cranial computed tomography (CT) scan showedold cerebellar infarcts. The possihility of a cardiacsource of emboli was considered. Two-dimen-sional echocardiography showed moderate aorticstenosis as noted previously. No thrombus wasseen. The ventricular pacemaker lead, however,was noted to cross the interatrial septum, extendinto tbe left atrium, and across the mitral valve. Tobetter visualize the tip of the lead transesophageal
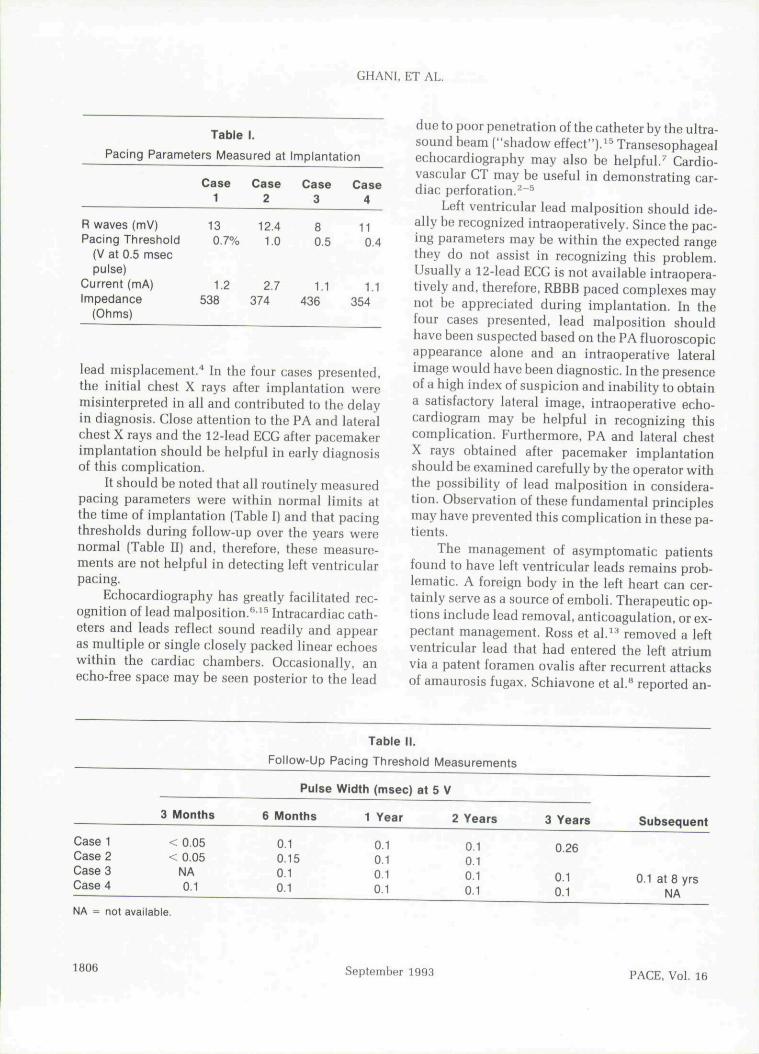
echocardiography was performed. It showed thatthe lead crossed the atrial septum in the area ofthe fossa ovalis. passed through the mitral valve,and lodged in the area of the posterior papillarymuscle and posterior mitral valve leaflet [Fig. 3).The lead appeared to be stable and embedded. Mi-tral valve and ventricular function were normal.Doppler and bubble studies were negative for in-teratrial shunting. The pacemaker was functioningappropriately.
The malpositioned pacing lead as a potentialcause of thromboembolism was considered. Thepacemaker lead was not repositioned. The patientremained heparinized throughout the hospitalcourse with resolution of neurological deficits.Prior to discharge warfarin therapy was initiated.During subsequent follow-up (9 months) the pa-tient has remained asymptomatic.
Case 2
In June 1991. a 79-year-old man experiencedsudden syncope while driving and was involvedin a minor accident. He had a past history of syn-
PACE, Vol. 16 September 1993 1801

GHANI. ET AL.
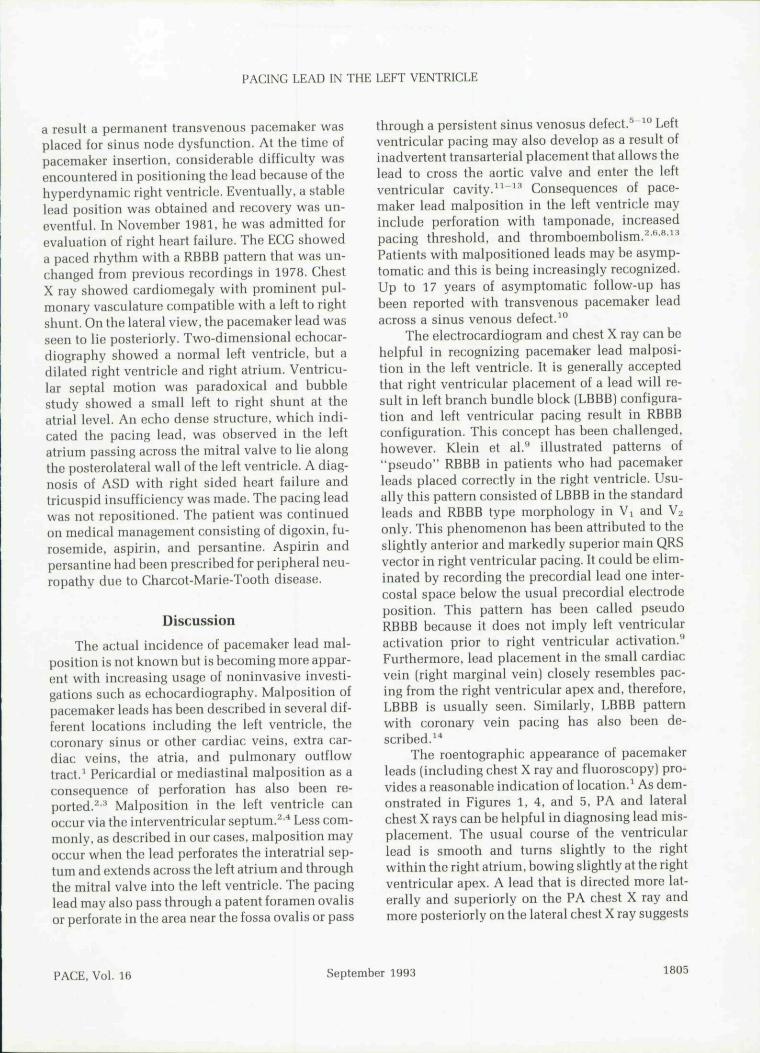
Figure 2. A 12-iead ECG with paced complexes demonstrating right bundle branch block pattern.
cope that had been fully investigated in 1990 anda diagnosis of sick sinus syndrome bad been madeat anotber center. As a result, a DDD pacemakerwas implanted witbout difficulty. Tbereafter hewas also placed on propafenone 150-mg po tid forthe prevention of atrial fibrillation.
Tbe ECG showed AV soqtiential pacing withrigbt bundle branch block (RBBB) morphology.The PA and lateral chest X rays are shown in Fig-ure 4. The possibility of pacemaker lead malposi-tion was considered, given the RBBB morpbologyand chest X ray findings. Two-dimensional echo-cardiography showed that the ventricular lead hadcrossed tbe interatrial septum in tbe area of tbefossa ovalis anterolaterally, extending into tbe loftatrium, across tbe mitral valve, and into tbe distalaspect of the left ventricle. Pacemaker evaluationrevealed an intrinsic sinus bradycardia at 40-45beats/min. Further investigations, including bead-up tilt table testing with isuprel, signal-averagedelectrocardiogram, Holter monitoring, and brainCT were unremarkable.
Propafenone was discontinued. Gardiogenicemboli causing syncope seemed unlikely and.
therefore, be was not anticoagulated. He has re-mained asymptomatic on subsequent follow-up(18 months).
Case 3
A 70-year-old woman witb a long-standingbistory of exertional angina and bypertension pre-sented witb polymorphic ventricular tachycardiaand torsade do pointes in August 1984. This wasinitially attributed to the use of prenylanine forangina, but arrhythmia still occurred after discon-tinuation of this medication. As a result, an AVsequential pacemaker was placed.
In Octobor 1985, she was admitted for inves-tigation of frequent episodes of presyncope.Medications at that time were propranolol andhydralazine. Tbe patient admitted drinkingbeavily. Cardiac and neurological examinationwore unremarkable.
Serum etbanol was 46.1 mg/dL. Completeblood count was normal apart from macrocytosis(mean corpuscular volume was 108 fL]. Tbe liverprofile was mildly abnormal witb an increased
1802 September 1993 PAGE, Vol. 16

PAGING LEAD IN THE LEFT VENTRIGLE
Figure 3. Image taken from the transesophageal echocardiogram demonstrates the pacing lead(arrows) in Ihe righl atrium, crossing the inleratrial septum into the left atrium and through themitral valve into the left ventricle.
Figure 4. Panel A, poslerior-onterior, and Panel B. lateral, views of the chest X rays from Case 2.
PAGE, Vol. 16 September 1993 1803

GHANI, ET AL.
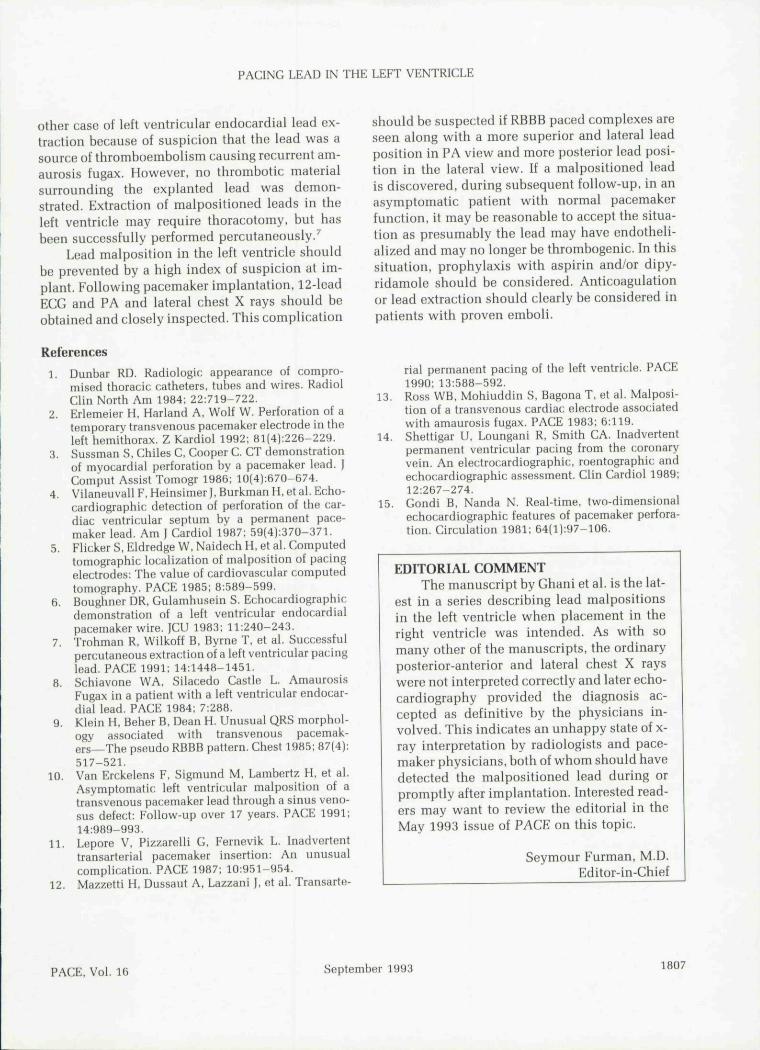
Figure 5. Panel A, posterior-anterior, and Panel B, lateral, views of the chest X rays from Case 3.
SGOT/SGPT ratio compatible with chronicethanol intake.
The ECG showed AV sequential pacing withRBBB complexes. Ghest X ray is shown in Figure5. Holter, carotid, Doppler examination, and thecranial GT were within normal limits. Two-dimen-sional echocardiography showed that the ventric-ular lead crossed the interatrial septum and mitralvalve and was located in the left ventricle,
Several causes of presyncope were consid-ered. The malpositioned lead was of concern as apossible source of cardiogenic thromboembolism.However, the lead appeared stable without vegeta-tions on echocardiography and it was felt to beunlikely that embolic phenomenon would presentas isolated episodes of presyncope. Therefore, pac-ing lead was not repositioned and she was not anti-coagulated. Presyncope was attributed to a combi-nation of ethanol excess and possible orthostaticeffects of hydralazine. Hydralazine was discontin-ued and nifedipine was substituted. She was dis-charged in stable condition and followed regularlyon an outpatient basis. The episodes of presyn-cope became less frequent and eventually quite
rare. Annual Holter evaluations have shownmainly a paced rhythm with short runs of asymp-tomatic atrial fibrillation/flutter.
The pacemaker malfunctioned in 1991 and re-quired replacement. The pacemaker generator wasreplaced uneventfully.
Case 4
A 72-year-old man with a history of cardiacmurmur and Charcot-Marie-Tooth syndrome pre-sented with symptoms of transient dizziness inNovember 1977. A diagnosis of paroxysmal atrialfibrillation was made and noninvasive studiesconfirmed the presence of a secundum atrial sep-tal defect (ASD). Physical findings were compati-ble with the diagnosis of an ASD and the EGGshowed an incomplete RBBB. Medical manage-ment with digoxin was recommended and symp-toms of transient dizziness improved.
By June 1978, symptoms of dizziness re-turned. Holter monitoring showed brief runs ofparoxysmal atrial tachycardia often followed byperiods of sinns arrest lasting up to 5 seconds. As
1804 September 1993 PACE, Vol. 16
PACINC LEAD IN THE LEFT VENTRICLE
a result a permanent transvenous pacemaker wasplaced for sinus node dysfunction. At the time ofpacemaker insertion, considerable difficulty wasencountered in positioning the lead because of thehyperdynamic right ventricle. Eventually, a stablelead position was obtained and recovery was un-eventful. In November 1981, he was admitted forevaluation of right heart failure. The ECG showeda paced rhythm with a RBBB pattern that was un-changed from previous recordings in 1978. ChestX ray showed cardiomegaly with prominent pul-monary vasculature compatible with a left to rightshunt. On the lateral view, the pacemaker lead wasseen to lie posteriorly. Two-dimensional echocar-diography showed a normal left ventricle, but adilated right ventricle and right atrium. Ventricu-lar soptal motion was paradoxical and bubblestudy showed a small left to right shunt at theatrial level. An echo dense structure, which indi-cated the pacing lead, was observed in the leftatrium passing across the mitral valve to lie alongthe posterolateral wall of the left ventricle. A diag-nosis of ASD with right sided heart failure andtricuspid insufficiency was made. The pacing leadwas not repositioned. The patient was continuedon medical management consisting of digoxin, fu-rosemide, aspirin, and persantine. Aspirin andpersantine had been prescribed for peripheral neu-ropathy due to Charcot-Marie-Tooth disease.
Discussion
The actual incidence of pacemaker lead mal-position is not known but is becoming more appar-ent with increasing usage of noninvasive investi-gations such as echocardiography. Malposition ofpacemaker leads has been described in several dif-ferent locations including the left ventricle, thecoronary sinus or other cardiac veins, extra car-diac veins, the atria, and pulmonary outflowtract.^ Pericardial or mediastinal malposition as aconsequence of perforation has also been re-ported.^-' Malposition in the left ventricle canoccur via the interventricular septum.^'* Less com-monly, as described in our cases, malposition mayoccur when the lead perforates the interatrial sep-tum and extends across the left atrium and throughthe mitral valve into the left ventricle. The pacinglead may also pass through a patent foramen ovalisor perforate in the area near the fossa ovalis or pass
through a persistent sinus venosus defect.^ ^" Leftventricular pacing may also develop as a result ofinadvertent transarterial placement that allows thelead to cross the aortic valve and enter the leftventricular cavity.^^"^^ Consequences of pace-maker lead malposition in the left ventricle mayinclude perforation with tamponade, increasedpacing threshold, and thromboembolism.^''"'^^Patients with malpositioned leads may be asymp-tomatic and this is being increasingly recognized.Up to 17 years of asymptomatic follow-up hasbeen reported with transvenous pacemaker leadacross a sinus venous defect.^°
The electrocardiogram and chest X ray can behelpful in recognizing pacemaker lead malposi-tion in the left ventricle. It is generally acceptedthat right ventricular placement of a lead will re-sult in left branch bundle block (LBBB) configura-tion and left ventricular pacing result in RBBBconfiguration. This concept has been challenged,however. Klein et al." illustrated patterns of"pseudo" RBBB in patients who had pacemakerleads placed correctly in the right ventricle. Usu-ally this pattern consisted of LBBB in the standardleads and RBBB type morphology in Vi and V2only. This phenomenon has been attributed to theslightly anterior and markedly superior main QRSvector in right ventricular pacing. It could be elim-inated by recording the precordial lead one inter-costal space below the usual precordial electrodeposition. This pattern has been called pseudoRBBB because it does not imply left ventricularactivation prior to right ventricular activation."Furthermore, lead placement in the small cardiacvein (right marginal vein) closely resembles pac-ing from the right ventricular apex and, therefore,LBBB is usually seen. Similarly, LBBB patternwith coronary vein pacing has also been de-scribed.̂ "*
The roentographic appearance of pacemakerloads (including chest X ray and fluoroscopy} pro-vides a reasonable Indication of location.^ As dem-onstrated in Figures 1, 4, and 5, PA and lateralchest X rays can be helpful in diagnosing lead mis-placement. The usual course of the ventricularlead is smooth and turns slightly to the rightwithin the right atrium, bowing slightly at the rightventricular apex. A lead that is directed more lat-erally and superiorly on the PA chest X ray andmore posteriorly on the lateral chest X ray suggests
PACE, Vol. 16 September 1993 1805
GHANI, ET AL.
Table 1.
Pacing Parameters Measured at
R waves (mV)Pacing Threshold
(V at 0.5 msecpulse)
Current (mA)Impedance
(Ohms)
Case1
130.7%
1.2538
Case2
12.41.0
2.7374
Implantation
Case3
80.5
1.1436
Case4
110.4
1.1354
lead misplacement." In tbo four cases prosentod,tho initial chest X rays after implantation weremisinterpreted in all and contributed to tbe delayin diagnosis. Close attontion to tbe PA and lateralchest X rays and tho 12-lead ECG after pacemakerimplantation should be helpful in early diagnosisof this complication.
It should be noted that all routinely measurodpacing parameters were within normal limits atthe time of implantation (Tablo I) and that pacingtbrosbolds during follow-up over tbe years worenormal (Table II) and, therefore, these measuro-monts are not helpful in detecting left ventricularpacing.
Echocardiograpby has greatly facilitated rec-ognition of lead malposition."'^^ Intracardiac cath-eters and leads reflect sound roadily and appearas multiple or single closely packed linear echoeswithin tbe cardiac cbambers. Occasionally, anecbo-froe space may be seen posterior to tho lead
due to poor penetration of tbe catbeter by the ultra-sound beam ("sbadow effect").i'^ Transesopbagealechocardiograpby may also be helpful.^ Cardio-vascular CT may be useful in demonstrating car-diac perforation.^"^
Left ventricular lead malposition should ide-ally be recognized intraoperatively. Since tbe pac-ing parameters may be within tho expected rangothey do not assist in recognizing tbis problem.Usually a 12-load EGC is not available intraopora-tively and. therefore, RBBB paced complexes maynot be appreciated during implantation. In thofour casos presented, lead malposition shouldhave boon suspected based on tbe PA fluoroscopicappearance alone and an intraoporativo latoralimago would bavo been diagnostic. In tho presenceof a high indox of suspicion and inability to obtaina satisfactory latoral imago, intraoperative ecbo-cardiogram may be belpful in recognizing thiscomplication. Furthermore, PA and lateral cbestX rays obtained aftor pacemaker implantationshould be examined carefully by the operator withtbe possibility of load malposition in considera-tion. Observation of tbese fundamental principlesmay have prevented this complication in these pa-tients.
Tbe management of asymptomatic patientsfound to have left ventricular loads remains prob-lematic. A foreign body in tho left heart can cer-tainly serve as a source of omboli. Therapeutic op-tions include lead removal, anticoagulation, or ex-pectant management. Ross ot al.^^ removed a leftventricular lead that had entered tbe left atriumvia a patent foramen ovalis after recurrent attacksof amaurosis fugax. Schiavono et al.^ reported an-
Case 1Case 2Case 3Case 4
NA = not
3 Months
<0.05< 0.05
NA0.1
available.
Table M.
Follow-Up Pacing Threshold
Pulse Width (msec) at
6 Months 1 Year
0.1 0.10.15 0.10,1 0.10.1 0.1
Measurements
5 V
2 Years
0.10.10.10.1
3 Years
0.26
0.10.1
Subsequent
0.1 at 8 yrsNA
1806 September 1993 PAGE, Vol. 16
PACING LEAD IN THE LEFT VENTRICLE
other case of left ventricular endocardial lead ex-traction because of suspicion that the lead was asource of thromboembolism causing recurrent am-aurosis fugax. However, no thrombotic materialsurrounding the explanted lead was demon-strated. Extraction of malpositioned leads in theleft ventricle may require thoracotomy, but hasbeen successfully performed percutaneously.'
Lead malposition in the left ventricle shouldbe prevented by a high index of suspicion at im-plant. Following pacemaker implantation, 12-leadECG and PA and lateral chest X rays should beobtained and closely inspected. This complication
References
1. Dunbar RD. Radiologic appearance of compro-mised thoracic catheters, tubes and wires. RadiolClin North Am 1984; 22:719-722.
2. Eriemeier H, Hariand A, Wolf W. Perforation of atemporary transvenous pacemaker electrode in theleft hemithorax. Z Kardiol 1992; 81(4):226-229.
3. Sussman S, Chiles C, Cooper C. CT demonstrationof myocardial perforation hy a pacemaker lead. JComput Assist Tomogr 1986; 10(4):670-674.
4. Vilaneuvall F, Heinsimer J, Burkman H, et al. Echo-cardiographic detection of perforation of the car-diac ventricular septum hy a permanent pace-maker lead. Am ] Cardiol 1987; 59[4l:370-371.
5. Flicker S, Eldredge W, Naidech H, et al. Computedtomographic localization of malposition of pacingelectrodes: The value of cardiovascular computedtomography. PACE 1985; 8:589-599.
6. Boughner DR, Gulamhnsein S. Echocardiographicdemonstration of a left ventricular endocardia!pacemaker wire. ]CU 1983; 11:240-243.
7. Trohman R, Wilkoff B, Byrne T, et al. Successfulpercutaneous extraction of a left ventricular pacinglead. PACE 1991; 14:1448-1451.
8. Schiavone WA, Silacedo Castle L. AmaurosisFugax in a patient with a left ventricular endocar-dial lead. PACE 1984; 7:288.
9. Klein H, Beher B, Dean H. Unusual QRS morphol-ogy associated with transvenous pacemak-ers^The pseudo RBBB pattern. Chest 1985; 87(4);517-521.
10. Van Erckelens F, Sigmund M, Lamhertz H, et al.Asymptomatic left ventricular malposition of atransvenous pacemaker lead through a sinus veno-sus defect: Follow-up over 17 years. PACE 1991:14:989-993.
11. Lepore V, Pizzarelli G, Fernevik L. Inadvertenttransarterial pacemaker insertion: An unusualcomplication. PACE 1987; 10:951-954.
12. Mazzetti H, Dussaut A, Lazzani f, et al. Transarte-
should be suspected if RBBB paced complexes areseen along with a more superior and lateral leadposition in PA view and more posterior lead posi-tion in the lateral view. If a malpositioned leadis discovered, during subsequent follow-up, in anasymptomatic patient with normal pacemakerfunction, it may he reasonable to accept the situa-tion as presumably the lead may have endotheli-alized and may no longer be thrombogenic. In thissituation, prophylaxis with aspirin and/or dipy-ridamole should be considered. Anticoagulationor lead extraction should clearly be considered inpatients with proven emboli.
rial permanent pacing of the left ventricle. PACE1990; 13:588-592.
13. Ross WB, Mohiuddin S, Bagona T. et al. Malposi-tion of a transvenous cardiac electrode associatedwith amaurosis fugax. PACE 1983; 6:119.
14. Shettigar LI, Loungani R, Smith CA. Inadvertentpermanent ventricular pacing from the coronaryvein. An electrocardiographic, roentographic andechocardiographic assessment. Clin Cardiol 1989;12:267-274.
15. Gondi B, Nanda N. Real-time, two-dimensionalechocardiographic features of pacemaker perfora-tion. Circulation 1981; 64(l):97-106.
EDITORIAL COMMENTThe manuscript hy Ghani et al. is the lat-
est in a series describing lead malpositionsin the left ventricle when placement in theright ventricle was intended. As with somany other of the manuscripts, the ordinaryposterior-anterior and lateral chest X rayswere not interpreted correctly and later echo-cardiography provided the diagnosis ac-cepted as definitive by the physicians in-volved. This indicates an unhappy state of x-ray interpretation by radiologists and pace-maker physicians, both of whom should havedetected the malpositioned lead during orpromptly after implantation. Interested read-ers may want to review the editorial in theMay 1993 issue of PACE on this topic.
Seymour Furman, M.D.Editor-in-Ghief
PACE, Vol. 16 September 1993 1807





















