Fluid structure interaction (FSI) of the left ventricle (LV) in ...
374
Fluid Structure Interaction (FSI) of the Left Ventricle (LV) in Developing the Next Generation Ventricular Assist Device (VAD) System A thesis submitted in fulfilments of the requirements for the degree of Doctor of Philosophy By MD. SHAMSUL AREFIN Faculty of Science, Engineering and Technology Bio-mechanical and Tissue Engineering Group Swinburne University of Technology 2015
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Fluid structure interaction (FSI) of the left ventricle (LV) in ...

Fluid Structure Interaction (FSI) of the
Left Ventricle (LV) in Developing the
Next Generation Ventricular Assist
Device (VAD) System
A thesis submitted in fulfilments of the requirements for
the degree of
Doctor of Philosophy
By
MD. SHAMSUL AREFIN
Faculty of Science, Engineering and Technology
Bio-mechanical and Tissue Engineering Group
Swinburne University of Technology
2015


II
ABSTRACT
This thesis represents the formal documentation for a Doctoral research program
undertaken at the Swinburne University of Technology in Melbourne Australia,
between the years of 2011 and 2014. The broad objective of the Doctoral research was
to apply innovative engineering approaches to analyze the Left Ventricle (LV) of the
human heart in order to provide the underpinning knowledge required to develop a
"next generation" Ventricular Assist Device (VAD). Also, it was possible to gain better
understanding of the dynamics of the LV (filling phase) for the first time by numerical
modelling based on general conditions, by varying the angles between the aortic and
mitral orifices and by applying the elastic modulus and friction co-efficient.
It was well established that a lack of natural blood circulation resulted in various cardiac
diseases. These diseases indisputably influenced the overall functionalities of the
cardiac structure and were a primary factor in cardiac related mortality. The LV of the
heart is its most significant compartment which helps circulate blood to the end organs
of the body. However, the natural performance of the LV decays due to aging and/or
weakened heart muscles and hence, various cardiac diseases can arise. In general, in
these circumstances the treatments in common use at the time this research commenced
were based on the use of ventricular assist devices (VADs), which were implanted
within patients. Over the years, research had demonstrated significant improvements in
VADs but various limitations still resulted in developing diseases/infections inside
patients. The literature review undertaken in this Doctoral program uncovered no
evidence of VADs that could prevent infections from arising.
In this Doctoral research, the long term focus was on providing the underlying
engineering analysis that would facilitate the development of a “next generation VAD”
which would be highly flexible and be able minimize potential complications -
specifically diseases and infections. In order to develop a next generation VAD, it was
critically important to determine the hemodynamic forces and structural
deformation/displacement of the LV during various physiological conditions. Moreover,
to achieve this, the reviewed research literature indicated that the utilization of a
numerical technique could provide an ideal tool to determine these properties. Hence,

III
the prime focus of this Doctoral research was eyed on the numerical investigations
required to determine hemodynamic parameters and the structural changes in a
"physiologically correct" LV model.
The Fluid Structure Interaction (FSI) scheme was determined to be an appropriate
means of investigating and determining the functionalities of the LV during various
physiological conditions. Hemodynamic features, such as:
• The flow pattern, including the vortex characteristics
• Changes in the intraventricular pressure (Ip)
• Wall Shear Stress (WSS) distributions
• Structural changes, using Total Mesh Displacement (TMD)
could be determined readily via this numerical technique, and in a cost-effective
manner. Once these values are determined they can then be incorporated into a
prototype of a next generation VAD. This prototype can successfully impersonate the
synchronization of the natural heartbeat.
In order to gain a greater understanding of the analysis prior to application into an LV
model, the numerical technique was initially applied to:
• The Internal Thoracic Artery- Left Anterior Descending (ITA-LAD) bypass
graft by varying the degrees of LAD-stenosis (0%, 30%, 50% and 75%)
• An Abdominal Aortic Aneurysm (AAA)
The application of the FSI technique in these two models (ITA-LAD and AAA)
generated substantial knowledge on the utilization of grid independency testing; suitable
boundary conditions, and different flow properties. This knowledge and data were then
applied on the LV model.
The FSI technique was then applied to an anatomically correct 3D LV model during the
filling phase. In doing so, Navier-Stoke’s equations and Arbitrary Lagrangian Eulerian

IV
(ALE) methods were coupled for the fluid and solid domains of the ventricle model.
Subsequently, hemodynamic parameters, such as:
• Velocity mapping including the vortex characteristics
• WSS distributions
• Ip distributions
• TMD distributions
were investigated and determined. In this thesis, the results are then presented, including
a discussion on how these parameters can influence the LV during diastole. Also, these
substantial findings were effective in understanding the natural rhythm of the LV and
would be important to the development of a next generation VAD device.
Simulations were also executed on the LV model by varying the angles between the
mitral and aortic orifices (50°, 55° and 60°) during the filling phase. Similar boundary
conditions and mathematical approaches were utilized to investigate and determine the
hemodynamic parameters and structural changes of the LV. These findings from this
thesis are novel and have not been investigated before, would be particularly useful in
the development of a next generation VAD.
The influences of the friction co-efficient and elastic modulus of the 3D LV model
during diastole were also investigated. Additionally, required mathematical approaches
and computational procedures were applied to study the hemodynamics and
physiological variations of the structure. Also, by varying the friction co-efficient and
elastic modulus for the first time to the best of our knowledge, Dilated Cardiomyopathy
(DCM) - a critical heart disease - could potentially be identified. Knowledge of this
disease condition would provide valuable data in developing a VAD device.
Overall, all the simulations were analyzed in detail and validated against previously
published research. Finally, overall conclusions are presented in this thesis, together
with potential future research directions.

V
ACKNOWLEDGEMENTS
I would like to express my gratitude to my principal co-ordinating supervisor Professor
Yosry Morsi, for his encouragement, inspiration, guidance and advice during the entire
research project. It would have been impossible to complete the work without his clear
supervision. Also, it has been my honour to work beside him and I am very grateful for
his support throughout the research. I would also like to thank my co-supervisor
Associate Professor Richard Manasseh for his valuable suggestions during my research.
Special thanks to two undergraduate group students, composed of students Wajid
Baryalai, Yining Wang, Abdul A. AlMalki, Majid B. Masoud, Ahmed S. Alrashdi,
Abdulhakim S. Almutarrid, Ahmed A. Aldhahri and Khaled A. Alenezi for their efforts
and help in developing a model/prototype of the next generation VAD device.
I am extremely thankful to Swinburne University of Technology for supporting me
financially by means of scholarship during my research.
Also, I would like to convey my gratitude to my colleagues, especially Himani
Mazumder and Arafat Ahmed for their assistance in technical knowledge and software
proficiency throughout the research.
Last but not the least, I would like to convey my gratitude to all my friends in the
biomechanical and tissue engineering group researchers whose friendship and assistance
alleviated my work and made my time enjoyable.
Finally, I also wish to convey my perpetual gratitude to my mother, father, brothers and
other family members for their everlasting support and belief during my research
program.

VI
This Thesis is Dedicated to
My Beloved Parents & Brothers
VII
DECLARATION
I declare that this thesis represents my own work and contains no material which has
been accepted for the award of any other degree, diploma or qualification in any
university except where due reference has been made in the text of the dissertation. To
the best of my knowledge and belief this thesis contains no material published or
written by other person except where due acknowledgement has been made.
Signed: …………………………… Date:
MD. SHAMSUL AREFIN

VIII
TABLE OF CONTENTS
ABSTRACT ..................................................................................................................... II
ACKNOWLEDGEMENTS ............................................................................................. V
DECLARATION .......................................................................................................... VII
TABLE OF CONTENTS ............................................................................................. VIII
LIST OF FIGURES ...................................................................................................... XV
LIST OF TABLES .................................................................................................... XVIII
LIST OF ABBREVIATIONS ....................................................................................... XX
Chapter 1 ........................................................................................................................... 1
Introduction ................................................................................................................... 1
1.1 Objectives of the Thesis ...................................................................................... 2
1.2 Detailed Background Study ................................................................................ 3
1.2.1 General .................................................................................................... 3
1.2.2 Overview of Cardiac Structure ................................................................ 3
1.2.3 Overview of Blood Flow ......................................................................... 5
1.2.4 Overview of Cardiac Cycle ..................................................................... 7
1.2.4.1 General ............................................................................................... 7
1.2.4.2 First Diastole Phase ............................................................................ 8
1.2.4.3 First Systole Phase .............................................................................. 8
1.2.4.4 Second Diastole Phase ........................................................................ 9
1.2.4.5 Second Systole Phase ......................................................................... 9
1.2.5 Synopsis of Heart Valves and its Diseases ............................................ 12
1.2.6 Synopsis of Arterial System .................................................................. 16
1.2.7 Overview of Cardiovascular Diseases (CVD) ....................................... 17
1.2.7.1 General Discussion ........................................................................... 17
1.2.7.2 Heart Failure ..................................................................................... 18
1.2.7.3 Coronary Heart Disease (CHD) ........................................................ 20
1.2.8 Current Treatments for Heart Diseases ................................................. 21
1.2.9 Overview of Ventricular Assist Devices (VADs) ................................. 23
1.2.10 Limitations of the Existing VAD System Technologies ................... 25

IX
1.2.11 Recent Advancements of the VAD Devices and the Need for A "Next
Generation" VAD System ................................................................................... 26
1.3 Specific Objectives of the Research.................................................................. 30
1.4 Overview of Methodology and Experimentation Methods .............................. 32
1.5 Specific Contributions of Research Program .................................................... 34
1.6 Structure of Thesis ............................................................................................ 35
Chapter 2 ......................................................................................................................... 37
Literature Review into the Left Ventricle: Experimental and Computational Approaches .................................................................................................................. 37
2.1 Overview ........................................................................................................... 38
2.2 Introduction ....................................................................................................... 40
2.3 Analysis on the Experimental Approaches of LV ............................................ 43
2.4 Analysis of Numerical Approaches using CFD/FSI for an Ideal LV ............... 55
2.5 Analysis of Experimental and Computational Approaches of the Diseased LV:
Dilated Cardiomyopathy (DCM) ............................................................................ 73
2.6 Summary ........................................................................................................... 82
Chapter 3 ......................................................................................................................... 84
Numerical Experimentation of Coronary Artery Bypass Graft and Abdominal Aortic Aneurysm Model ......................................................................................................... 84
3.1 Overview ........................................................................................................... 85
3.2 Review of Literature pertaining to the Bypass Graft ........................................ 86
3.3 Mathematical Procedure, Solver and Output Settings ...................................... 90
3.4 Case Study I: ITA-LAD Bypass Graft .............................................................. 94
3.4.1 Geometry ............................................................................................... 94
3.4.2 Meshing Configurations and Mesh Independency Testing ................... 96
3.4.3 Required Boundary Conditions ............................................................. 97
3.4.4 Simulation Results ............................................................................... 100
3.4.4.1 Velocity Distributions .................................................................... 100
3.4.4.2 Wall Shear Stress (WSS) Distributions .......................................... 107
3.4.4.3 Spatial Wall Shear Stress (WSS) Distributions .............................. 113
3.4.4.4 Structure Simulation using Total Mesh Displacement (TMD) ...... 119
3.4.5 Discussions on ITA-LAD for different degree of LAD-stenosis ........ 124

X
3.4.5.1 Variations of the hemodynamics inside the bypass graft using
velocity mapping ........................................................................................... 124
3.4.5.2 The effects of Wall Shear Stress (WSS) inside the bypass graft using
WSS distributions.......................................................................................... 126
3.4.5.3 The effects of the wall shear stress (WSS) inside the bypass graft
using spatial wall shear stress (WSS) distributions....................................... 127
3.4.5.4 Structure simulation of the bypass graft for different degree of LAD-
stenosis using total mesh displacement (TMD) ............................................ 128
3.5 Abdominal Aortic Aneurysm (AAA) ............................................................. 130
3.6 Literature Review of Abdominal Aortic Aneurysm (AAA) ........................... 132
3.7 Case Study II: abdominal aortic aneurysm (AAA) ......................................... 136
3.7.1 Geometry ............................................................................................. 136
3.7.2 Meshing Configurations and Mesh Independency Testing ................. 138
3.7.3 Required Boundary Conditions ........................................................... 139
3.7.4 Simulation Results ............................................................................... 141
3.7.4.1 Velocity Mapping ........................................................................... 141
3.7.4.2 Wall shear stress (WSS) distributions ............................................ 144
3.7.4.3 Total mesh displacement (TMD) distributions............................... 146
3.7.5 Discussion ........................................................................................... 149
3.7.5.1 Influence of flow dynamics of the AAA using velocity vectors .... 149
3.7.5.2 Influence of wall shear stress (WSS) of the AAA using WSS
distributions ................................................................................................... 150
3.7.5.3 Influence of the structral displacement of the AAA using total mesh
displacemnt (TMD) distributions .................................................................. 152
3.8 Summary of Results and Conclusions ............................................................ 154
Chapter 4 ....................................................................................................................... 156
Numerical Studies of the Left Ventricle during Diastole Phase: General Conditions ................................................................................................................................... 156
4.1 Overview ......................................................................................................... 157
4.2 Introduction ..................................................................................................... 158
4.3 Computational Approaches ............................................................................. 159
4.3.1 Overview ............................................................................................. 159

XI
4.3.2 Geometry ............................................................................................. 159
4.3.3 Meshing Information and Mesh Independency Trials ........................ 162
4.3.4 Required Boundary Conditions ........................................................... 163
4.4 Simulation Results and Discussions ............................................................... 165
4.4.1 Overview ............................................................................................. 165
4.4.2 Distributions of Pressure ..................................................................... 165
4.4.3 Distributions of Wall Shear Stress (WSS) .......................................... 172
4.4.4 Distributions of Velocity ..................................................................... 177
4.4.5 Structure Simulation using Total Mesh Displacement (TMD) ........... 186
4.5 Summary ......................................................................................................... 192
Chapter 5 ....................................................................................................................... 194
Numerical Analysis of the Left Ventricle during Diastole Phase: Angular Variations between the Mitral and Aortic Orifice ...................................................................... 194
5.1 Overview ......................................................................................................... 195
5.2 Introduction ..................................................................................................... 196
5.3 Computational Approaches ............................................................................. 197
5.3.1 Overview ............................................................................................. 197
5.3.2 Geometry Extraction ........................................................................... 197
5.3.3 Meshing Statistics and Mesh Independency Trials ............................. 199
5.3.3 Boundary Conditions ........................................................................... 201
5.4 Simulation Results .......................................................................................... 202
5.4.1 Overview ............................................................................................. 202
5.4.2 Distributions of Velocity ..................................................................... 202
5.4.2.1 Angular Difference of 50° .............................................................. 202
5.4.2.2 Angular Difference of 55° .............................................................. 207
5.4.2.3 Angular Difference of 60° .............................................................. 211
5.4.3 Wall Shear Stress (WSS) Distributions ............................................... 216
5.4.3.1 Angular Difference of 50° .............................................................. 216
5.4.3.2 Angular Difference of 55° .............................................................. 220
5.4.3.3 Angular Difference of 60° .............................................................. 224

XII
5.4.4 Distributions of Pressure ..................................................................... 228
5.4.4.1 Angular Difference of 50° .............................................................. 228
5.4.4.2 Angular Difference of 55° .............................................................. 233
5.4.4.3 Angular Difference of 60° .............................................................. 237
5.4.5 Structure Simulations using Total Mesh Displacement (TMD) .......... 242
5.4.5.1 Angular Difference of 50° .............................................................. 242
5.4.5.2 Angular Difference of 55° .............................................................. 247
5.4.5.3 Angular Difference of 60° .............................................................. 251
5.5 Discussion ....................................................................................................... 257
5.5.1 Influence of flow dynamics for 50°, 55° and 60° between the mitral and
aortic orifice using velocity mapping ................................................................ 257
5.5.2 Influence of intra-ventricular wall shear stress (WSS) for 50°, 55° and
60° between the mitral and aortic orifice using WSS distributions .................. 258
5.5.3 Influence of intra-ventricular pressure (Ip) for 50°, 55° and 60° between
the mitral and aortic orifice using pressure distributions .................................. 260
5.5.4 Influence of structure simulation for 50°, 55° and 60° between the
mitral and aortic orifice using total mesh displacement (TMD) ....................... 261
5.6 Summary ......................................................................................................... 263
Chapter 6 ....................................................................................................................... 265
Numerical Analysis of the Left Ventricle during Diastole Phase: The Influence of Friction Co-efficient and Elastic Modulus ................................................................ 265
6.1 Overview ......................................................................................................... 266
6.2 Introduction ..................................................................................................... 267
6.3 Computational Approaches ............................................................................. 268
6.3.1 Geometry Extraction ........................................................................... 268
6.3.2 Meshing Statistics and Mesh Independency Trials ............................. 268
6.3.3 Boundary Conditions ........................................................................... 270
6.4 Simulation Results .......................................................................................... 273
6.4.1 Overview ............................................................................................. 273
6.4.2 The influence of friction coefficient and elastic modulus of the LV
using wall shear stress (WSS) distributions ...................................................... 273

XIII
6.4.2.1 Elastic modulus of 0.35 MPa ......................................................... 273
6.4.2.2 Elastic modulus of 0.7 MPa ........................................................... 276
6.4.2.3 Elastic modulus of 1.4 MPa ........................................................... 279
6.4.3 The influence of friction coefficient and elastic modulus using
intraventricular pressure (Ip) distributions ........................................................ 281
6.4.3.1 Elastic modulus of 0.35 MPa ......................................................... 281
6.4.3.2 Elastic modulus of 0.7 MPa ........................................................... 284
6.4.3.3 Elastic modulus of 1.4 MPa ........................................................... 286
6.4.4 The influence of friction coefficient and elastic modulus using velocity
mapping ............................................................................................................. 289
6.4.4.1 Elastic modulus of 0.35 MPa ......................................................... 289
6.4.4.2 Elastic modulus of 0.7MPa ............................................................ 292
6.4.4.3 Elastic modulus of 1.4 MPa ........................................................... 294
6.4.5 The influence of friction coefficient and elastic modulus structure
simulation using total mesh displacement (TMD) ............................................ 297
6.4.5.1 Elastic modulus of 0.35MPa .......................................................... 297
6.4.5.2 Elastic modulus of 0.7MPa ............................................................ 299
6.4.5.3 Elastic modulus of 1.4 MPa ........................................................... 301
6.5 Discussion ....................................................................................................... 303
6.5.1 The influence of Cf and elastic modulus on the LV using WSS
distributions ....................................................................................................... 303
6.5.2 The influence of Cf and elastic modulus on the LV using Ip
distributions ....................................................................................................... 305
6.5.3 The influence of Cf and elastic modulus on the LV using velocity
mapping ............................................................................................................. 306
6.5.4 The influence of Cf and elastic modulus on the LV structure simulation
using total mesh displacement (TMD) .............................................................. 308
6.6 Summary ......................................................................................................... 310
Chapter 7 ....................................................................................................................... 312
Conclusions and Future Directions ........................................................................... 312
7.1 Overall Conclusions of the Dissertation ......................................................... 313
7.2 Clinical Implications ....................................................................................... 318

XIV
7.2.1 Overview ............................................................................................. 318
7.2.2 Significance of the next generation VAD system ............................... 318
7.2.3 Significance of the CABG and aortic aneurysm models ..................... 319
7.2.4 Significance of the LV model.............................................................. 320
7.3 Future Directions and Recommendations ....................................................... 323
7.3.1 Overview ............................................................................................. 323
7.3.2 Experimental Requirements for VAD Prototype [including the works
from two undergraduate groups] ....................................................................... 323
7.3.3 Experimental Requirements of the LV Model .................................... 324
7.3.4 Computational and Experimental Requirements of the CABG and
Aortic Aneurysm Model ................................................................................... 325
7.3.5 Computational Requirements of the LV Model .................................. 327
Appendix ....................................................................................................................... 329
1. Variations in the velocity distributions of AAA ............................................... 329
2. Variations in the WSS of AAA ......................................................................... 330
3. Variations in the structural displacement using TMD of AAA ........................ 331
4. Experimental VAD prototype design – using DC motor and wireless technology
............................................................................................................................... 332
5. Experimental VAD prototype design – using steel wings and wireless
technology ............................................................................................................. 333
List of Publications ....................................................................................................... 335

XV
LIST OF FIGURES
Figure 1.1 Major elements of the human heart (Bianco, 2000) .................................... 4
Figure 1.2 Human heart (Medic, 2011) .......................................................................... 5
Figure 1.3 Cross-section of the heart for different pressure values (Laizzo, 2009,
Dreamstime, 2013) ........................................................................................................... 6
Figure 1.4 Blood flow pattern (Bailey, 2011).................................................................. 8
Figure 1.5 Cardiac cycles (Physiology, 2013) ............................................................... 10
Figure 1.6 Left ventricle volume and pressure (Klabunde, 2011)................................ 11
Figure 1.7 Illustration of heart valves (Sentara, 2014) ................................................ 13
Figure 1.8 Illustration of the main layers of the coronary artery (Do, 2012) ............. 17
Figure 1.9 Illustration of heart failure (Mattox, 2013) ................................................ 19
Figure 1.10 Coronary disease (Health, 2012) ............................................................... 21
Figure 1.11 Illustration of heart transplant (Staff, 2012) ............................................ 22
Figure 1.12 Left Ventricular Assist Device (Bouthillet, 2011) ..................................... 23
Figure 1.13 The MYO-VAD (Ostrovsky, 2006)............................................................. 28
Figure 3.1 Illustration of the flow chart utilized during the entire simulation
procedure (Arefin and Morsi, 2014, Owida et al., 2012) .............................................. 93
Figure 3.2 Cross sectional view of the ITA-LAD bypass graft (75% LAD-stenosis) (a):
Ideal 3D model (SolidWorks 2012) (b): The model utilized in simulations (SolidWorks
2012) ............................................................................................................................... 95
Figure 3.3 Meshing independency testing .................................................................... 97
Figure 3.4 Inlet velocities for the ITA-LAD bypass graft (Ding et al., 2012) .............. 98
Figure 3.5 Velocity mapping of the ITA-LAD bypass graft for the (a) 0%, (b) 30%, (c)
50% and (d) 75%LAD-stenosis .................................................................................... 105
Figure 3.6 Distributions of WSS for different degrees of LAD-stenosis (0%, 30%, 50%
and 75%) ....................................................................................................................... 111
Figure 3.7 Spatial WSS distributions using Line A, Line B and line C .................... 113
Figure 3.8 Spatial WSS distributions of Line A, Line B and Line C for (a) 0% (b) 30%
(c) 50% and (d) 75% LAD-stenosis ............................................................................. 117
Figure 3.9 Structure simulation using total mesh displacement (TMD) for (a) 0% (b)
30% (c) 50% and (d) 75% LAD-stenosis ..................................................................... 122
Figure 3.10 Location of abdominal aortic aneurysm (AAA) (Stern) ......................... 131

XVI
Figure 3.11 (a) Cross-sectional geometry of an axisymmetric AAA (using SolidWorks
2012) (b) Detailed dimensions of the AAA (using SolidWorks 2012) (Li, 2005) ....... 137
Figure 3.12 Mesh independency testing using line control properties ...................... 139
Figure 3.13 Inlet velocity waveform (Li, 2005) ........................................................... 140
Figure 3.14 Actual outlet pressure waveform (Li, 2005) ............................................ 140
Figure 3.15 Simplified outlet pressure waveform utilized in the simulations ........... 140
Figure 3.16 Velocity distributions of the AAA in different time steps ....................... 143
Figure 3.17 WSS distributions of the AAA in different time steps ............................. 145
Figure 3.18 Structural displacement using total mesh displacement (TMD)
distributions .................................................................................................................. 148
Figure 4.1 (a) Dimensions of the LV used for the simulations (SolidWorks 2010) (b)
Geometric construction of the LV model (SolidWorks 2010) (Arefin and Morsi, 2014)
....................................................................................................................................... 161
Figure 4.2 Mesh independency trials (Arefin and Morsi, 2014) ................................ 163
Figure 4.3 Transmitral flow velocity (U) against time (t) waveform, implemented in
the inlet region (Arefin and Morsi, 2014) ................................................................... 164
Figure 4.4 Changes in the Ip for various time steps during diastolic flow conditions
(Arefin and Morsi, 2014) ............................................................................................. 169
Figure 4.5 Distributions of WSS during the filling phase .......................................... 175
Figure 4.6 Illustration of velocity distributions during diastolic flow conditions
(Arefin and Morsi, 2014) ............................................................................................. 184
Figure 4.7 Illustration of total mesh displacement (TMD) during diastolic flow
conditions (Arefin and Morsi, 2014) ........................................................................... 190
Figure 5.1 LV Model with the angular differences of (a) 50°, (b) 55° and (c) 60°
between the inlet and outlet (SolidWorks 2012) .......................................................... 199
Figure 5.2 Mesh independency trial using fluid flow velocity ................................... 200
Figure 5.3 Velocity mapping for the angular difference of 50° ................................. 206
Figure 5.4 Velocity mapping for the angular difference of 55° ................................. 210
Figure 5.5 Velocity mapping for the angular difference of 60° ................................. 215
Figure 5.6 Wall shear stress (WSS) distributions for the angular difference of 50° 219
Figure 5.7 Wall shear stress (WSS) distributions for the angular difference of 55° 223
Figure 5.8 Wall shear stress (WSS) distributions for the angular difference of 60° 227

XVII
Figure 5.9 Intra-ventricular pressure (Ip) distributions for the angular difference of
50° ................................................................................................................................. 231
Figure 5.10 Intra-ventricular pressure (Ip) distributions for the angular difference of
55° ................................................................................................................................. 236
Figure 5.11 Intra-ventricular pressure (Ip) distributions for the angular difference of
60° ................................................................................................................................. 241
Figure 5.12 Total mesh displacement (TMD) distributions for the angular difference
of 50° ............................................................................................................................. 246
Figure 5.13 Total mesh displacement (TMD) distributions for the angular difference
of 55° ............................................................................................................................. 250
Figure 5.14 Total mesh displacement (TMD) distributions for the angular difference
of 60° ............................................................................................................................. 255
Figure 6.1 Mesh independency trial by using fluid velocity....................................... 269
Figure 6.2 WSS distributions for 0.35 MPa ................................................................ 275
Figure 6.3 WSS distributions for 0.7 MPa .................................................................. 278
Figure 6.4 WSS distributions for 1.4 MPa .................................................................. 280
Figure 6.5 Ip distributions for the elastic modulus of 0.35MPa ................................ 283
Figure 6.6 Ip distributions for the elastic modulus of 0.7MPa .................................. 285
Figure 6.7 Ip distributions for the elastic modulus of 1.4MPa .................................. 288
Figure 6.8 Velocity distributions for the elastic modulus of 0.35MPa ...................... 291
Figure 6.9 Velocity distributions for the elastic modulus of 0.7MPa ........................ 293
Figure 6.10 Velocity distributions for the elastic modulus of 1.4MPa ...................... 296
Figure 6.11 TMD distributions for the elastic modulus of 0.35MPa ......................... 298
Figure 6.12 TMD distributions for the elastic modulus of 0.7MPa ........................... 300
Figure 6.13 TMD distributions for the elastic modulus of 1.4MPa ........................... 302

XVIII
LIST OF TABLES
Table 1.1 Overall status of the chambers of the heart (Bronzino, 2006) ....................... 7
Table 1.2 LV volume and pressure in different phase-conditions (Klabunde, 2011) .. 11
Table 1.3 Summary of heart valve diseases and medications ....................................... 13
Table 2.1 Primary investigations on LV flow dynamics (experimental) ...................... 50
Table 2.2 Left Ventricle researches and its configurations .......................................... 67
Table 2.3 Primary investigations on DCM .................................................................... 78
Table 3.1 Observations pertaining to figure 3.5 .......................................................... 105
Table 3.2 Observations pertaining to figure 3.6 .......................................................... 111
Table 3.3 Observations pertaining to figure 3.8 .......................................................... 118
Table 3.4 Observations pertaining to figure 3.9 .......................................................... 123
Table 3.5 Time step observations ................................................................................. 124
Table 3.6 Time step observations ................................................................................. 126
Table 3.7 Summary of the whole work (CABG and AAA) ......................................... 154
Table 4.1 Sequence of events pertaining to figure 4.4 ................................................ 169
Table 4.2 Summary of time-step observations relating to figure 4.5.......................... 176
Table 4.3 Time-step observations pertaining to figure 4.6 ......................................... 184
Table 5.1 Observations pertaining to figure 5.3 .......................................................... 206
Table 5.2 Observations pertaining to figure 5.4 .......................................................... 211
Table 5.3 Observations pertaining to figure 5.5 .......................................................... 215
Table 5.4 Observations pertaining to figure 5.6 .......................................................... 219
Table 5.5 Observations pertaining to figure 5.7 .......................................................... 223
Table 5.6 Observations pertaining to figure 5.8 .......................................................... 227
Table 5.7 Observations pertaining to figure 5.9 .......................................................... 232
Table 5.8 Observations pertaining to figure 5.10 ........................................................ 236
Table 5.9 Observations pertaining to figure 5.11 ........................................................ 241
Table 5.10 Observations pertaining to figure 5.12 ...................................................... 246
Table 5.11 Observations pertaining to figure 5.13 ...................................................... 251
Table 5.12 Observations pertaining to figure 5.14 ...................................................... 255
Table 6.1 Computations of Cf ...................................................................................... 271
Table 6.2 Observations pertaining to figure 6.2 .......................................................... 275
Table 6.3 Observations pertaining to figure 6.3 .......................................................... 278

XIX
Table 6.4 Observations pertaining to figure 6.4.......................................................... 281
Table 6.5 Observations pertaining to figure 6.5.......................................................... 283
Table 6.6 Observations pertaining to figure 6.6.......................................................... 286
Table 6.7 Observations pertaining to figure 6.7.......................................................... 288
Table 6.8 Observations pertaining to figure 6.8.......................................................... 291
Table 6.9 Observations pertaining to figure 6.9.......................................................... 294
Table 6.10 Observations pertaining to figure 6.10...................................................... 296
Table 6.11 Observations pertaining to figure 6.11...................................................... 299
Table 6.12 Observations pertaining to figure 6.12...................................................... 301
Table 6.13 Observations pertaining to figure 6.13...................................................... 303
Table 7.1 Overall features of the simulated models .................................................... 322

XX
LIST OF ABBREVIATIONS
AAA = Abdominal Aortic Aneurysm
AV = Aortic Valve
CABG = Coronary Artery Bypass Graft
BSM = Bjork-ShileyMonostrut
EDV = End-diastolic Volume
EDP = End-diastolic Pressure
ESPVR = End-systolic Pressure-Volume Relationship
FSI = Fluid Structure Interaction
ITA = Internal Thoracic Artery
MV = Mitral Valve
LA = Left Atrium
LAD = Left Anterior Descending
LV = Left Ventricle
PA = Pulmonary Artery
RV = Right Ventricle
RA = Right Atrium
VAD = Ventricular Assist Device

1
Chapter 1
Introduction

2
1.1 Objectives of the Thesis
The objective of this thesis is to document a Doctoral research program that was
undertaken between 2011 and 2014 in the Faculty of Science, Engineering and
Technology (FSET) at Swinburne University of Technology in Melbourne, Australia.
The primary purpose of the research program was to investigate engineering issues
associated with the development of a "next generation" Ventricular Assist Device
(VAD) system driven by a wireless controller. The key elements of this Doctoral
research program involved a detailed analysis of the hemodynamic forces and the
structure deformation of the Left Ventricle (LV) during different physiological
conditions.
More specifically, the primary focus of this research was to determine precisely the:
• Flow dynamics
• Shear stress
• Pressure
exerted on the ventricle endocardium and the degree of structural displacement of the
left ventricle. This knowledge would subsequently assist in the design of a next
generation VAD.
At the time this research commenced, there were many VADs available for patients but
a number of complications relating to their use had been uncovered. These are
documented in this thesis. The broader objective of this research was to create a
knowledge foundation that would enable a next generation VAD to be developed to
assist people who have a weak heart muscle and/or a cardiac structure with insufficient
strength to circulate the required amount of blood to the entire body.

3
1.2 Detailed Background Study
1.2.1 General
This section provides general background information on the research work, as well as
the impetus for the research that was undertaken and the need to develop a next
generation VAD system. Firstly, overviews of the cardiac structure and its components;
cardiac diseases; current treatments and VAD system are presented. Subsequently,
limitations of existing technologies (VADs) are highlighted and finally, recent
advancements and the need for a next generation VAD are documented.
1.2.2 Overview of Cardiac Structure
The human cardiovascular system is composed of a conically-formed pumping-organ
(the heart); blood and blood vessels which act as a branching network throughout the
whole body. The heart weighs approximately 0.33 kilogram for an adult male and 0.28
kilogram for adult female. In a given day, a healthy heart beats approximately a hundred
thousand times and pumps/drives around two thousand gallons of blood every day
(Bronzino 1999, Bronzino, 2006, Morsi, 2011, Bender, 1992).
Precisely, the heart is located between the 3rd and 6th ribs, inside the centre of the
thoracic cavity; it is suspended by its links to the great vessels and surrounded by a
rubbery sac - the pericardium (Laizzo, 2009, Bronzino 1999, Bronzino, 2006). See
Figure 1.1, which shows an overview diagram of the relevant elements.

4
Figure 1.1 Major elements of the human heart (Bianco, 2000)
Humans have a comparatively thick-walled pericardium compared to general
mammalian animals (e.g., canine, porcine or bovine) (Laizzo, 2009). A very small
quantity of fluid can be found inside the sac. This is referred to as pericardial fluid and
lubricates the outer part of the heart and allows it to move fluidly during a heartbeat.
The muscle tissue inside the ventricle walls is referred to as the myocardium, and the
inner layer and outer layer of the myocardium is known as the endocardium and
epicardium accordingly (Laizzo, 2009, Li, 2011).
Consequently, the heart is separated by a hard muscular wall, namely the interatrial-
interventricular septum, into a semi-circular shaped right part and cylindrically shaped
left part. Both parts function as a pump except that they are joined in series (Bronzino,
2006, Bronzino 1999). These two parts are separated into two main chambers, atriums
(upper portion) and ventricles (lower portions). Both of these are further separated into
two more chambers right atrium (upper chamber), left atrium (lower chamber) and right
ventricle, left ventricle. Figure 1.2 shows the construction of the human heart (Medic,
2011, Bronzino 1999, Bronzino, 2006, Bender, 1992, Morsi, 2011, Li, 2011).

5
Figure 1.2 Human heart (Medic, 2011)
The left atrium and left ventricle are accountable for the whole-body/systemic
circulation and the right atrium and right ventricle are accountable for the pulmonary
blood circulation. The primary task for the atriums is to gather the blood while the
ventricles are responsible for driving that blood through the heart valves. The blood
flow inside the heart is kept unidirectional by the four valves which always open and
close synchronously. Entering from the veins, the blood move into the heart via the
right atrium and then the heart begins its function cycle. However, the entering blood
transports a large amount of carbon dioxide, whereas the quantity of oxygen is
relatively low as the body tissue engross it completely (Li, 2011, Bender, 1992, Morsi,
2011).
1.2.3 Overview of Blood Flow
As noted in Section 1.2.2, the left part of the heart, including left atrium and left
ventricle push oxygen enriched blood via the semilunar aortic valve into systemic blood
circulation. The blood is then carried out through various areas of the cells throughout
the body and then comes back to the right side of the heart, where the amount of oxygen

6
in the blood is very low but enriched in carbon dioxide. The right atrium and the right
ventricle of the heart push the deoxygenated blood, via the pulmonary heart valve, to the
pulmonary blood circulation that drives the carbon dioxide enriched blood into the
lungs. The various elements are shown in Figure 1.3. In the lungs, the deoxygenated
blood is purified into the oxygenated blood and then this oxygen enriched blood is
driven to the left part of the heart again. Due to the physiological proximity of the heart
to the lungs, both the right atrium and right ventricle do not need to function very
strongly to pump the blood throughout the pulmonary blood circulation (Bronzino,
2006, Laizzo, 2009).
When the pressure of the ventricles is high and when it surpasses the pressure of the
pulmonary artery and/or aorta, then the blood is pushed out from the ventricle. This
functional cardiac phase is represented as systole. Now, when the myocytes in the
ventricle are at rest, (i.e., the ventricle pressure drops lower than that of the atria) the
atrioventricular valves open and then the ventricles replenish. This cardiac phase is
represented as diastole (Laizzo, 2009). The various status parameters associated with
the heart are listed in Table 1.1, abstracted from Bronzino (2006).
Figure 1.3 Cross-section of the heart for different pressure values (Laizzo, 2009,
Dreamstime, 2013)

7
Table 1.1 Overall status of the chambers of the heart (Bronzino, 2006) Chambers of the heart Wall thickness
(centimetre)
Volume of blood
(litres)
Pressure
(kilopascals)
Left atrium 0.3 0.045 0-3.33
Right atrium 0.2 0.063 0-1.33
Left ventricle Inconsistent,
maximum 1.2
0.1 18.67
Right ventricle 0.4 0.13 5.33
1.2.4 Overview of Cardiac Cycle
1.2.4.1 General
The cardiac cycle demonstrates consecutive events, which appear for a single cycle of a
heartbeat. This is the result of the sequence of events having occurred as the heart beats.
The cardiac cycle consists of two phases, identified as the Diastole and Systole phases
(Morsi, 2011, Bailey, 2011, Bijlani and Manjunatha, 2011).
Figure 1.4 demonstrates the total blood flow pattern, which shows the path of the blood
when it arrives into the heart and is squeezed out to the lungs. Subsequently, this blood
goes back to the heart and is squeezed out again to the whole body. The first and second
diastole phases always happen together and it is similar for the first and second systole
phases (Bailey, 2011).

8
Figure 1.4 Blood flow pattern (Bailey, 2011)
1.2.4.2 First Diastole Phase
During this phase, the atria and ventricles are relaxed/rested and the atrioventricular
valves (AV) (tricuspid and mitral) are opened. Superior and the inferior vena cava
contain de-oxygenated blood. This blood drifts into the right atrium. The blood then
flows through to the ventricles by the open atrioventricular valves. The Sinuatrial Node
(SA) starts pushing the atria to contract. Then, the right ventricle is filled up with blood
from the right atrium, and the tricuspid valve prevents backflow into the right atrium
(Bailey, 2011).
1.2.4.3 First Systole Phase
In the first systole phase, the Purkinje fibres provide stimulation to the right ventricle
and cause it to contract. In this phase, the atrioventricular and the semilunar valves
(aortic and pulmonary) are open and closed respectively. The pulmonary artery then
contains the deoxygenated blood and the pulmonary valve precludes the backflow into

9
the right ventricle. After that, the blood is passed to the lungs by the pulmonary artery.
In the lungs, the blood is purified with the oxygen and is then carried back to the left
atrium. This process is conducted by the pulmonary veins (Bailey, 2011).
1.2.4.4 Second Diastole Phase
During the second diastole phase, the semilunar and the atrioventricular valves are
closed and opened accordingly. The left atrium is gaining blood from the pulmonary
veins and at the same time, right atrium gains the blood form the vena cava. Then the
SA node again starts signalling the atria to contract. As a result, the left ventricle is
filled with blood from the left atrium. In this phase, the mitral valve averts the blood
from coming back into the left atrium (Bailey, 2011).
1.2.4.5 Second Systole Phase
During this phase, the atrioventricular and the semilunar valves are closed and opened
accordingly. The Purkinje fibres trigger the left ventricle, and it begins to contract. The
aorta receives the oxygenated blood and the backflow is prevented by the aortic valve
into the left ventricle. The aorta then spreads the oxygenated blood to the whole body
and the deoxygenated blood flows back to the heart via the vena cava (Bailey, 2011).
The various pressures for each phase are shown in Figure 1.5.

10
Figure 1.5 Cardiac cycles (Physiology, 2013)
Depending on a person’s age, the heart can contract 60-140 times a minute, each time it
is stimulated by an electrical impulse. Each contraction of the ventricles is referred to as
a single heartbeat. The ventricles start contracting a fraction of a second later than the
atria. As a result, the ventricles gain the blood from the atria before the ventricles can
start contracting. However, if any abnormal functioning occurs in the conduction system
of the heart, it can cause the heart to beat too slow or too fast, and can result in an
asymmetrical heart rate, referred to as arrhythmia (Pitigalaarachchi, 2011).
Subsequently, in the case of the Left Ventricle (LV), volume and pressure can be
summarized as per Table 1.2, (derived from Figure 1.6) (Klabunde, 2011).

11
(a) (b)
Figure 1.6 Left ventricle volume and pressure (Klabunde, 2011)
Table 1.2 LV volume and pressure in different phase-conditions (Klabunde, 2011)
Phases Situation of LV Pressure Situation of LV volume Ventricular
Filling (D)
(Phase a)
Point 1, where the mitral valve starts
closing, defines the pressure at the
completion of ventricular filling.
This point indicates the End Diastolic
Pressure (EDP).
At this point, the pressure is
approximately 10 mmHg.
Point 1, same as the EDP, also
indicates volume at the
completion of ventricular filling
and referred to as End Diastolic
Volume (EDV).
Here the volume is around 120
ml.
Isovolumetric
Contraction
(S) (Phase b)
When the ventricles start the
isovolumetric-contraction, then the
mitral valves close completely and
the pressure rises.
It can be examined at point 2, where
the aortic valve starts to open.
The pressure at this point is just
below 100 mmHg.
It can be also seen at point 2,
where there is no effect on the
volume, because all the valves
are closed.
So the volume would be same
as point 1 of around 120 ml.
Ejection (S)
(Phase c)
Aortic valve opens (point 2), when
the LV pressure surpasses the aortic
diastolic pressure and as a result,
ejection (phase c) starts.
Throughout this phase the LV
pressure rises to its highest rate (peak
Comparing to the same situation
of this phase in case of volume;
the volume starts dropping at
point 2 to point 3.
The lowest volume can be

12
systolic pressure) and then drops due
to the relaxation of the ventricle
(point 3).
The maximum pressure can be
obtained around 120 mmHg.
obtained around 50 ml.
Isovolumetric
Relaxation
(D) (Phase d)
At point 3, aortic valve starts to close
and that is why the ejection phase
stops.
The ventricle rests isovolumetrically
and as a result, the pressure falls.
The pressure at this stage is just
above 100 mmHg (point 3).
When the pressure drops lower than
the left atrial pressure (point 4),
ventricle starts to fill.
At the beginning, pressure starts to
drop due to the filling of ventricle
and when it is complete, then the
pressure and volume rises steadily.
When the ventricle rests
isovolumetrically, then the
volume stays unaffected, as all
valves are closed.
The volume at this stage is
known as End Systolic Volume
(ESV). The volume is around
50 ml.
1.2.5 Synopsis of Heart Valves and its Diseases
When the RA contracts/squeezes blood is then pushed inside the RV via the tricuspid
valve. At the same time as the right atrium contracts, blood is driven through the
pulmonary valve and passed to the lungs. In the lungs, the blood is purified and then the
oxygen-enriched blood containing low level of carbon dioxide comes back into the LA.
Next, this oxygen enriched blood is driven through the MV into the left ventricle after
the contraction of the LA. Coming from the left atrium, the blood is then propelled
through the aortic valve out to the rest of the body. The primary principle of these four
valves is to assist the blood flow normally in the heart. Naturally, humans have two
types of valves, bicuspid and tricuspid, which possess the number of leaflets inside the
valve. The key features of these valves are that they are unidirectional, and prevent
blood going back (this process is known as regurgitation) from one section to another
within the heart (Bender, 1992, Morsi, 2011).

13
There are four valves all total inside the human heart (Figure 1.7); two of these are
semilunar valves and the other two are atrioventricular valves. The semilunar heart
valves are further divided into the pulmonary and aortic valve and the atrioventricular
valves are divided into the tricuspid and mitral valves (Lanza et al., 2007).
Figure 1.7 Illustration of heart valves (Sentara, 2014)
Table 1.3 summarizes the various diseases and remedies as abstracted from various
references.
Table 1.3 Summary of heart valve diseases and medications Valve
Diseases
Causes and Effects Disease Indications Medications/Remedy References
Aortic
Regurgitati
on (AR)
1. Affects the aortic root,
valve leaflets and the
valve outlets; due to
annular
widening/prolapse of the
valve.
2. Increased
hypertension, higher
blood pressure and
elevated after-load.
Acute tiredness, briefness
in breathes, chest pain,
weakness, inflamed
feet/ankle and so on.
Using medicine, such as:
diuretics and blood
pressure medicine and
also the repair and
replacement of the
valve.
(Drugs, 2012,
Morsi, 2011,
Shipton and
Wahba, 2001,
Disease,
HealthCentral,
2014, Pick,
2012a)

14
Aortic
Stenosis
(AS)
The left ventricular free
wall and the inter-
ventricular septum are
hardened.
Briefness in breathe,
dizziness, coughing,
inflamed feet/ankle, heart
murmurs, extreme
urination and many more.
1. Replacement of aortic
valve is used after the
symptoms are matured.
2. Balloon vulvoplasty is
used if the patient is
unable for surgery
Mitral
Regurgitati
on (MR)
1. The LV, LA, PA and
RV are expanded.
2. Mitral valve prolapse
is the most frequent
anatomical defects,
responsible for this.
3. Severe regurgitation is
generally initiated by
myocardial infraction
Breathing complications,
exhaustion (mostly while
performing exercise),
cough, palpitations of the
heart, inflamed feet/ankle,
extreme urination and
various disorders.
1. It can be an
asymptomatic disease,
which might recover
rapidly for some
patients.
2. Echocardiogram helps
to determine the
acuteness of this disease.
3. Transesophageal
echocardiogram, MRI,
stress echo or cardiac
catheterization are also
useful to identify the
valve dysfunction,
cardiac injury and
suggested
medication/surgery.
(HealthCentral,
2013a, Shipton
and Wahba,
2001, Disease,
Pick, 2012b,
MeDIndia,
2014)
Mitral
Stenosis
(MS)
1. The LA, PA and RV
are expanded.
2. Overflow of blood in
PA and RV.
3. Rheumatic fever.
High pressure, lungs-
hardening and breathing-
complications, fatigue,
palpitations and many
more.
1. Mostly depends on
patient’s conditions.
2. Catheterization
techniques,
Percutaneous balloon
valvuloplasty and Mitral
balloon valvuloplasty
techniques are used
depending on the
patient’s conditions.
Tricuspid
Regurgitati
on (TR)
1. RA expands and the
blood pressure inside
RA also elevates.
2. Right part of the heart
carrying contagious
endocarditis triggers the
TR.
1. TR might not produce
any indications if the
patients do not have
pulmonary hypertension.
2. If the pulmonary
hypertension and medium-
acute TR be present all
1. Treatments might not
be required if there are
few or no indications,
but for acute indications,
hospitalization might be
necessary.
2.
(HealthCentral,
2010, Pick,
2007, Wang
and Bashore,
2009, Roberts
and
Buchbinder,

15
3. Bulge of RV, MS and
MR elevate the risk of
TR.
4. Rheumatic fever,
carcinoid tumours,
marfan disorder,
rheumatoid arthritis,
heart valve infections
and so on.
along then, exhaustion,
feebleness, reduced
urination, inflamed
feet/ankle and abdomen
and other indications
might take place.
Swelling/inflammation
can be cured by
diuretics.
3. Some patients might
require the rare
operation to
substitute/repair the
diseased valve and it is
performed only when
another heart valve (e.g.
mitral valve
replacement) needs to be
substituted.
1972, Barbour
and Roberts,
1986,
HealthCentral,
2013b,
HeartValveSurg
ery, 2012,
Roberts and
Sjoerdsma,
1964,
Shmookler et
al., 1977)
Tricuspid
Stenosis
(TS)
1. RA expands, but RV
does not acquire
sufficient blood and
remains small. So, the
cardiac output of the
blood reduces.
2. Rheumatic
fever/disease, carcinoid
heart disease, tumour or
connective tissue
diseases and others.
Drowsiness, tenderness,
trembling feeling in the
neck, palpitation, ache in
the right part (upper) of
the abdomen and many
more.
1. Basically TS does not
need any treatment, but
it mostly depends on the
acuteness of the disease.
2. General treatment
could be monitoring the
condition of patients,
medications and surgery
(if needed).
3. Chest X-ray,
electrocardiogram and
an echocardiogram are
useful to diagnose.
Moreover, cardiac
catheterization can be
used to carry out the
surgery.
Pulmonic
Regurgitati
on (PR)
1. Iatrogenic sources,
pulmonary hypertension
or the dilation of the
core PA, distorted or
stiffened pulmonary
valve.
2. Rarely, it can occur
due to endocarditis or
carcinoid heart disease.
Exhaustion, breathing
complications, chest ache,
palpation, expanded liver,
inflamed legs/feet,
cyanosis and so on.
Echocardiogram and
MRI are very useful to
diagnose and to decide
the requirement and
timing of the
operation/substitution.
(Shmookler et
al., 1977, Wang
and Bashore,
2009, Hospital,
2013, PSC,
2008, Virginia,
2013)
Pulmonic 1. Congenital heart Hurried/speedy breathing, 1. Chest X-ray,

16
Stenosis
(PS)
disease itself or
accumulated with
cardiovascular
congenital deficiency.
2. Irregular enhancement
of the pulmonary valve
during the first 8 weeks
of the fetal development.
3. Bacterial endocarditis
could occur.
breathing complications,
exhaustion, palpations,
inflamed feet, ankles, face,
eyelids, abdomen etc.
electrocardiogram,
echocardiogram, and
cardiac catheterization
could be used for the
diagnosis purpose.
2. Mild stenosis
generally does not need
any medication but the
medium-critical stenosis
is cured with the repair
of the diseased valve
(which includes
valvuplasty, valvotomy,
patch enlargement,
pulmonary valve
replacement).
1.2.6 Synopsis of Arterial System
The circulatory system of the human body contains the heart and blood vessels. The
blood vessels encompass the arteries, veins and capillaries. The heart helps circulating
the blood through the vessels, which contain the oxygenated blood, essential nutrients
for different organs, tissues and cells inside the body (Do, 2012).
A nutrition-bearing artery is made up of three distinct layers (Figure 1.8):
• The Intima
• The Media
• The Adventitia
These individual layers contain an exclusive constituent of cells and matrix (Do, 2012).

17
Figure 1.8 Illustration of the main layers of the coronary artery (Do, 2012)
The innermost layer is known as the tunica intima, which is a monolayer made up of
endothelial cells (EC). A sub-endothelium layer (where the matrix is enriched with
protein), consists of proteoglycan and the collagen that is located under the
endothelium. The mid layer is known as the media or tunica media, which largely
contains the smooth muscle cells and some scattered elastic connective tissue of varying
quantity. Finally, the outer/external wall encompassing the tunica media is known as the
adventitia (Do, 2012). Diseases related to coronary artery disease/coronary heart disease
are briefly described in the Section 1.2.7.
1.2.7 Overview of Cardiovascular Diseases (CVD)
1.2.7.1 General Discussion
Cardiovascular disease (CVD) is an expression that relates to every possible syndrome
and disorder of the heart and blood vessel system. It mostly causes damage to the veins
and arteries which pass to and from the heart. The National Health and Medical
Research Council (NHMRC) in Australia spent $439.5 million for research into CVD
between the years of 2000 to 2007 (Council, 2014).

18
CVD encompasses all the diseases as well as the stipulations of the cardiac structure
and blood vessels system. By far, it is the primary cause of mortality in Australia
including 45,600 deaths during the year of 2011. Overall CVD afflicts over 3.7 million
Australian inhabitants and precludes 1.4 million Australians from leading a normal life
(Council, 2014). Moreover, in underdeveloped countries the mortality rate from CVD is
found to be approximately 80% and the rate is rapidly rising. In developed countries, on
the other hand, age-related CVD-deaths reduced by 50% between the years 1960 to
2010 (Emeto et al., 2011).
Also, CVD is often diagnosed in advanced stages, which is why it can be dangerous.
For this reason alone, where detected early, suitable drug therapies are implemented at
the onset, to block the disease’s progression (Emeto et al., 2011).
Another issue with CVD is that it is a primary source of mortality for the Hemodialysis
(HD) patients. This is due to a combination of blood pressure, disturbed lipid
metabolism, oxidative stress, micro inflammation, hyperhomocysteinemia, anaemia,
secondary hyperparathyroidism and vascular shunt flow (Petrovi et al., 2011).
Additionally, when the high blood pressure is found to be the cause of the heart disease,
it is termed as hypertensive heart disease (Badii, 2012).
1.2.7.2 Heart Failure
Heart Failure (Figure 1.9) is a common disease which occurs due to lack of proper
physical functioning as the balance within the body is hindered, causing the patient to
expire. Heart failure generally represents the disorder which can occur due to any
functional dysfunction, which damages the capability and/or natural rhythms of the
ventricle to expand and contract. As a result, heart failure causes a lack of blood
circulation, increases lung pressure, decreases the level of enriched oxygenated blood
and death results (Hunt et al., 2009, Baryalai et al., 2011). In Australia alone, more than
380,000 people are susceptible to a heart attack at any time and each year approximately
55,000 people actually experience a heart attack (Foundation).

19
Figure 1.9 Illustration of heart failure (Mattox, 2013)
There are a number of different types of heart failure:
(i) Dilated Cardiomyopathy
The leading and most significant kind heart failure is Dilated
Cardiomyopathy. This causes the heart ventricles to become soft and
widened, resulting in a weakened heart. In addition, because of this
condition, the heart rate will try to facilitate the required cardiac output
as the stroke volume falls down (Peschar et al., 2004, Baryalai et al.,
2011).
If the necessary output is not met, the body will become starved of
nutrient enriched arterial blood, essential for vital organs. On the other
hand, the same symptoms of dilated cardiomyopathy can be observed;
that is, the pressure levels in the heart and lungs are increased, and is

20
identified as Congestive Herat Failure (Hunt et al., 2009, Baryalai et al.,
2011).
(ii) Hypertrophic Cardiomyopathy
When the heart muscle becomes thick, it causes the ventricles to solidify,
and is identified as Hypertrophic Cardiomyopathy. The solidifying of the
cardiac muscles can also responsible for the impediment of the left
ventricle, similar to the Aortic Stenosis (Fogoros, 2014a, Baryalai et al.,
2011).
(iii) Diastolic Dysfunction
The third most common kind of heart failure is Diastolic Dysfunction,
which is due to the irregular thickening of the ventricles and aberrant
filling of the ventricle during the filling phase. Higher blood pressure,
hypertrophic cardiomyopathy, coronary artery diseases, obesity and
many other causes can instigate this disease (Fogoros, 2014b, Baryalai et
al., 2011).
1.2.7.3 Coronary Heart Disease (CHD)
When the coronary arteries (which deliver blood and oxygen to the heart muscle) are
blocked with an oily substance known as ‘plaque’ or ‘atheroma’, this is identified as
Coronary Heart Disease (CHD) - see Figure 1.10. Plaque builds up along the
inner/internal wall of the arteries, affecting them to become thin, thus resulting in the
blood’s inability to pass properly within the arteries. This problem is known as
‘atherosclerosis’(Channel, 2014). CHD is one of the leading causes of deaths in the
world and one of the crucial factors for CHD is atherosclerosis (Basçiftçi and Incekara,
2011). Approximately 1.4 million Australian people suffer CHD and this disease is
responsible for the death of approximately 59 people per day (Foundation).

21
Figure 1.10 Coronary disease (Health, 2012)
1.2.8 Current Treatments for Heart Diseases
Heart failure itself is a serious issue which can be mitigated as time goes by. Some of
these diseases can be prevented by following a recommended course of treatment. In
addition, when the heart muscle becomes weakened, there are numerous treatments
available which can alleviate the symptoms and halt or decelerate the slow decline of
the situation (Center, 2014).
Xu et al. (2011) showed that the quantification of coronary arterial stenosis is effective
in the diagnosis of coronary heart disease (Xu et al., 2011). In another study, Petrovi et
al. (2011) noted that the process for lowering the cardiovascular death rate for
Hemodialysis (HD) patients must contain initial recognition of very high-risk patients;
permanent assessment dialysis suitability, and electrolyte stability (Petrovi et al., 2011).
Also, Lavu et al. (2011) reported that gene therapy could be an ideal treatment for
ischemic heart disease in humans in the near future (Lavu et al., 2011). Moreover,
related to the valvular diseases, Morsi, 2011 observed that the treatment lies in either

22
the valve replacement or substitution of the valve using mechanical or tissue valves
(Morsi, 2011).
The term Heart Transplant (See Figure 1.11), refers to a surgical procedure for replacing
a patient’s unhealthy heart with a healthy one from a deceased donor. It is the final stage
in saving a patient’s life, and it is done only when medical options and other serious
surgeries are unsuccessful. Patients must undergo a rigorous selection procedure, as the
number of donor hearts available for transplant are limited (National Heart, 2012).
Figure 1.11 Illustration of heart transplant (Staff, 2012)
There are of course numerous problems with heart transplants. Boucek et al. 2008 noted
that children and infants receiving an orthotropic heart transplant possess a higher risk
of death at the time of the procedure (Boucek et al., 2008). More pragmatically,
however, the perpetual scarcity of available donors for transplantation beckons a greater
focus on the implantation/insertion of Left Ventricular Assist Devices (LVADs)
(Agarwal and High, 2012).
Moreover, stem cell technologies could also be the basis of next generation tools to
assist heart failure patients. Mozes, 2011 reported that by utilizing stem cells, it was

23
possible to reduce the size of the expanded cardiac structure, but that more work was
required in this field (Mozes, 2011).
1.2.9 Overview of Ventricular Assist Devices (VADs)
A Ventricular Assist Device (VAD) is a type of mechanical pump that acts as a
ventricle and returns general hemodynamic and end-organ blood flow - see Figure 1.12.
The left ventricle of the heart is the targeted region for artificial assistance, as the left
ventricle plays a significant role in the provision of oxygen-rich blood to the body and is
also more prone to degradation from various diseases. Between 1998 and 2001, Left
Ventricular Assist Devices (LVADs) were accepted as a replacement therapy or bridge
to transplantation therapy (BTT). However, there are three important factors that create
peri-operative difficulties: (Goldstein et al., 1998, Rose et al., 2001, Awad et al., 2010).
• Native heart failure containing inferior organ impairment
• The implanted devices, having an enduring effect
• Surgical Procedures, comprising cardiopulmonary bypass (CPB)
Figure 1.12 Left Ventricular Assist Device (Bouthillet, 2011)

24
Subsequently, the primary goal of the VAD system is to help carrying the blood from
the lower chamber (ventricles) and then assist in pumping blood into the whole body,
including the vital organs. The VAD is effective when the ventricles of the human heart
do not work appropriately.
The fundamental components of a VAD system include:
• A small tube, which takes the blood from the heart to the pump
• Another tube, which removes the blood from the pump to the recipient’s body
• A power source
The power source is attached to a control unit, which mainly supervises the VAD’s
operation system. When the power is minimal or if the device is not functioning
properly, then this control unit also provides warnings or alarms (Institute, 2012).
Recent improvements in LVAD technologies, including refinements in patient selection
and management have vastly improved the survival rate (Moazami, 2011). These
modern VAD systems, being smaller in size and equipped with many options, deliver a
suitable replacement and, at the same time, also decrease the death rate for the patients
who are on the transplant waiting list (Garbade et al., 2011).
There are various kinds of VADs. Some of them generate the pulsating flow like the
heart, while others can provide a consistent flow of blood. It is possible that, when the
blood movement is consistent, then the recipients might not feel the usual pulse.
However, their body will still be receiving the blood which is necessary for the body to
function (Institute, 2012).
There are essentially two types of VADs:
• Left ventricular assist devices (LVADs)
• Right ventricular assist devices (RVADs)

25
When these two VADs are utilized together, then the resulting technology is referred to
as a biventricular assist device (BIVAD) (Institute, 2012).
The LVADs are the most popular type of VADs and their main function is to aid the
pumping of blood from the left ventricle to the aorta. RVADs are utilized to aid
pumping the blood from the right ventricle into the pulmonary artery. Finally, a BIVAD
might be employed when the two ventricles do not function properly to meet the general
requirements for the body. When the patient is in this kind of situation, then one other
treatment is considered, a total artificial heart (TAH), which substitutes the ventricles
(Institute, 2012).
1.2.10 Limitations of the Existing VAD System Technologies
While VADs offer a lifeline for some patients, they are also responsible for causing
various complicating issues. These issues relate to (Goldstein et al., 1998, Friedman et
al., 2011, Pamboukian, 2011):
• Device size
• Device durability
• Driveline infections
• Open chest surgery
• Right sided heart failure
• Thromboembolism
• Thrombotic and bleeding complications
Moreover for the implantation of LVADs, haemolysis has been an issue containing the
centrifugal and axial-flow for the LVADs. However, in patients, it did not show
evidence of any medical problem when the LVADs were implanted (Goldstein et al.,
1998). The problems with VADs can therefore be significant when these devices are
implanted inside the human body.

26
The broad objectives of this Doctoral research are to undertake engineering analysis and
developments that may reduce the risks associated with VAD systems and to enable
them operate more safely. In order to do that, FSI of the LV have been utilized during
the filling phase for different physiological conditions, which are analyzed and
discussed extensively in Chapter 4, Chapter 5 and Chapter 6.
1.2.11 Recent Advancements of the VAD Devices and the Need for A "Next Generation"
VAD System
At the time this Doctoral research commenced, significant developments in mechanical
VADs had been achieved, especially for the patients with severe heart failure.
Specifically, a high degree of stability in the VADs; simple pumping mechanisms
without bearings (or, at least, with few bearings), and continually improving valves
have been the prime developments in this field. At the time of compiling this
dissertation, various devices, such as (Molina and Boyce, 2013):
• HeartMate II
• HeartWare HVAD
• Jarvik 2000
• Micromed CardioVascular HeartAssist 5
• Synergy LVAD
were available and operational for heart failure patients.
Moreover, a range of different LVADs, such as (Molina and Boyce, 2013):
• HeartMate III
• HeartMateX
• HeartWare MVAD

27
were in the pipeline for the acute heart failure patients.
All the current devices offered flexibility but further improvements in LVAD
technologies, including much smaller and more robust pumps, will aid patients
extensively. Additionally, the removal of driveline wires, combined with upgraded
VAD pumps, less invasive surgical procedures and inclusion of wireless technology
will enhance the advancements of these devices in upcoming years (Molina and Boyce,
2013). Also, three different generations of LVAD devices have been obtained (Garbade
et al., 2011, Rodriguez et al., 2013):
First Generation: Uses pulsatile pump to generate the blood flow. These generation
VAD devices contain several moving parts. Examples are: HeartMate I, HeartMate
XVE etc.
Second Generation: Uses continuous blood pumping (axial pumps). Examples are:
HeartMate II, jarvik 2000 etc.
Third Generation: Contains non-contacting bearings and continuous flow pumps
(centrifugal pumps). Examples are: HeartWare LVAD, HeartMate III etc.
Detailed discussion concerning the different generation and improvement of VADs can
be found in (Goldstein et al., 1998, Farrar et al., 2007, Frazier et al., 1998, Burke et al.,
2001, Slaughter, 2010, Partyka and Taylor, 2014, Nguyen and Thourani, 2010, Hoshi et
al., 2006, Timms, 2011).
In relation to the improvement of VAD devices, it was reported by Ostrovsky, 2006 that
the New York-based Myotech Cardiovascular was testing devices with an enclosure/cup
around the heart to assist it in expanding/contracting synchronously with the natural
rhythm of the human body - see Figure 1.13. This device contains a smaller exterior
drive unit and stretchable polymer enclosure which can be implanted outside the heart
within three minutes. However, the developments did not discuss the use of wireless
technology (Ostrovsky, 2006).

28
Figure 1.13 The MYO-VAD (Ostrovsky, 2006)
More recently, Miller (2012) reported that with the aid of a "next generation" wireless-
power transfer system, it would be possible to facilitate improved VADs and artificial-
heart-development (Miller, 2012). However, wireless technology had been introduced
by Leviticus Cardio (Cardio, 2014) where they developed the wireless coplanar energy
transfer (CET) system which provided the daily requirements of energy for VADs. They
noted that their pioneering CET would be particularly useful for patients because it is
minimally sensitive to body movement; had minimal risk involved in skin heating and
was straightforward to implant (Cardio, 2014).
In another study, Waters et al. (2011) introduced the Free-Range Resonant Electrical
Energy Delivery (FREE-D) System, and experimented with the axial VAD and
VentrAssist VAD. They demonstrated that these VADs could be operated wirelessly
using the FREE-D system (Waters et al., 2012). However, for further utilization with
the VADs, the FREE-D system needed to incorporate single frequency operation and
advanced resonators which could be implanted efficiently and effectively (Waters et al.,
2013).

29
Subsequently, Kim et al. 2012 investigated the wireless power transmission between a
source and connected cardiac implant (Kim et al., 2012). Moreover, Ho et al. 2013
discussed the concept of midfield wireless powering and demonstrated it for a heart-
implant (Ho et al., 2013).
The introduction of wireless electricity (Glass and Ponsford, 2014) as the energy source;
wireless technology for the medical devices/implants (HospiMedica, 2012, Hartford,
2013) and even wireless charging (Sahota, 2013) will play a vital role in the
advancement of the different medical devices/implants in the future.
The detailed literature review in this thesis will show that although many researchers are
working on VADs to reduce mortality rates, a great deal of additional research, over a
number of fields, will be required in order to make a successful "next generation" VAD
device that provides a quantum leap over the currently available devices.

30
1.3 Specific Objectives of the Research
In Section 1.1, it was noted that the basic objectives of this Doctoral research program
were to investigate engineering issues associated with the development of a "next
generation" Ventricular Assist Device (VAD) system driven by a wireless controller.
Pursuant to this, a number of specific research objectives were identified, that is:
The development of a numerical analysis technique to model the
physiologically correct left ventricle and determine the hemodynamic forces
and the structural displacement.
The definition of the correct geometry of the left ventricle.
The determination of the required boundary conditions and heart cycle
(transmitral velocity) to calculate the required hemodynamic and structural
properties.
To verify and validate the results either by physical observations or
comparisons with existing published information.
To conduct numerical analysis of the Internal Thoracic Artery (ITA)-Left
Anterior Descending (LAD) bypass graft using fluid structure interaction
(FSI) to study the variations of the hemodynamics and structural properties.
To perform the FSI procedure for the Abdominal Aortic Aneurysm (AAA) to
identify the variations in the flow pattern and structural displacements.
To determine the hemodynamic and physiological effects by varying the
angles between the mitral and aortic orifices of the left ventricle using FSI.
To determine the significance of the friction coefficient and elastic modulus
on the left ventricle using FSI.

31
Finally, the objective was to determine the benefits and limitations of the work that was
conducted in this Doctoral research.

32
1.4 Overview of Methodology and Experimentation Methods
The long term goal for this research is to provide analysis to facilitate the development
of a "next generation" VAD system which can be controlled using wireless
technologies. However, in order to construct such a device it is necessary to obtain
engineering data on
• Velocity profile
• The shear stress
• Intraventricular pressure
• Degree of deformation of the cardiac structure
Therefore during the course of this Doctoral research, computational approaches using
the FSI were utilized on left ventricle (LV) to determine the flow dynamics,
intraventricular pressure distributions, wall shear and the deformation of the structure
during different heart cycles. In doing so, as mentioned in the objectives, a
physiologically correct geometry of the LV had to be identified. After that, required
boundary conditions had to be provided and required parameters were simulated.
However, before performing the numerical investigations on the LV, computational
studies using FSI had to be performed on the ITA-LAD (Internal Thoracic Artery- Left
Anterior Descending) and the results then verified. This study focused on the flow
pattern, changes in the wall shear and the structural displacement/deformation by
varying the degree of LAD-stenosis (0%, 30%, 50% and 75%). This investigation
provided an overall understanding related to the coronary artery diseases/coronary heart
diseases.
Similarly, numerical investigations were employed using FSI on the Abdominal Aortic
Aneurysm (AAA) to understand and determine the flow pattern, variations in the wall
shear and the deformation/displacement of the AAA-structure during different cardiac
cycles. As noted earlier, for both cases, physiologically correct geometries were
defined, required boundary conditions were provided and the simulations performed.

33
Moreover, simulations were performed on the flow dynamics, intraventricular pressure
distributions, changes in the wall shear and structural displacement of the LV, by
varying the angles between the mitral and aortic orifices of the LV during different
cardiac cycles. Once again, the geometry of the LV was defined, required boundary
conditions were applied and the simulations performed.
Furthermore, the friction co-efficient and elastic modulus of the LV during different
cardiac conditions, were analyzed. In doing so, similar approaches were undertaken to
determine the complete nature and physiological characteristics of the LV. By changing
the friction co-efficient and elastic modulus of the LV, the conditions for the dilated
cardiomyopathy (DCM) of the LV could be identified.
It also needs to be noted that different experimental approaches were undertaken by
involving undergraduate students from Swinburne University to construct a prototype of
the next generation VAD device. Therefore, a brief description of this is provided in
chapter 7.
All these numerical investigations provide useful insights on the LV in various
conditions and the data will be helpful in developing a next generation VAD model.

34
1.5 Specific Contributions of Research Program
It is believed that this Doctoral research program has made a number of specific
contributions of knowledge to the field. These include:
• A comprehensive review of literature into the fields of experimental and
computational studies both for the general LV and diseased LV (dilated
cardiomyopathy).
• The development of detailed models pertaining to the LV (general conditions,
by varying the angles and by changing the friction co-efficient and elastic
modulus), ITA-LAD bypass graft and AAA.
• Determination of benefits and limitations of the models and testing regimes
outlined in this thesis.
• Based on the end point and limitations of the research documented herein, an
identification of new areas of research to further the field.

35
1.6 Structure of Thesis
This thesis has seven chapters, six of which follow on from this introduction.
Specifically, these chapters are summarized as follows:
• Chapter 2 provides detailed discussions on the experimental and numerical
approaches (fluid structure interaction/computational fluid dynamics) of the left
ventricle and dilated cardiomyopathy that have been presented.
• Chapter 3 represents the numerical investigations of the ITA-LAD bypass graft
and AAA using FSI in terms of hemodynamic optimizations and structural
displacements. Using the available literatures, different boundary conditions and
assumptions have been utilized and the effects have been analysed. Also, this
chapter is helpful to build up more confidences on the FSI scheme.
• Chapter 4 contains the computational procedure of the left ventricle using FSI in
general conditions during the filling phase. Hemodynamic data and structural
displacements have been determined and analysed.
• Chapter 5 documents the computational procedures using FSI that were carried
out to determine the effects of the hemodynamics and physiological properties
of the left ventricle by varying the angles between the mitral and aortic orifices.
The results were discussed and analyzed during the diastolic wave conditions.
This numerical data would be useful in developing a wireless VAD even if the
angular variations exist.
• Chapter 6 determines and analyses the effects of the friction coefficient and
elastic modulus on the left ventricle during the filling phase. This chapter
provides the information for the diseased LV (dilated cardiomyopathy).
• Chapter 7 provides a synopsis of the whole work along with the clinical
implications, limitations and future directions. One should note that, four
different experimental approaches for developing the wireless VAD have been

36
enlisted in this chapter where two initial approaches have been conducted for the
demonstration purpose only and the other two with the assistance of the
undergraduate students.

37
Chapter 2
Literature Review into the Left Ventricle:
Experimental and Computational Approaches

38
2.1 Overview
The primary objective of this literature review was to determine the current state of
research in the fields of:
• Disease conditions (Dilated Cardiomyopathy (DCM)) of the left ventricle
• Experimental approaches
• Computational approaches
Based on previously published research outcomes and future directions identified from
learned researchers in the field, this literature review also provided the impetus for the
research directions in this Doctoral program. Specifically, the following areas were
investigated in the review and are documented herein:
(i) Historical perspective and overview of the Left Ventricle– this was
undertaken to get an insight into the significance of this research in the
overall totality of research that had been conducted to date.
(ii) Literature into Left Ventricle based on general conditions (experimental and
computational methods). Publications in this field were carefully analyzed in
order to determine the current state of research and to obtain related
hemodynamic and structural detail.
(iii) Literature related to the Left Ventricle based on the diseased condition
(Dilated Cardiomyopathy (DCM)). Publications related to this field were
thoroughly investigated in order to determine the significance of this
research and to obtain related hemodynamical and structural information for
the LV.
In Chapter 1, the cardiac structure and its components; related diseases and available
treatments were documented but some of the reviews related to general background
were included in order to provide a basic insight into the area.

39
More specifically, in relation to this Doctoral research, detailed analyses of past
research efforts were beneficial to executing fluid structure integration (FSI)
simulations, because the geometry and required boundary conditions had to be obtained
from the previous research studies.
Finally, limitations from earlier published research are highlighted herein and attempts
were made to address these during the simulation procedures. These review components
are documented in Sections 2.3 - 2.5. At the end of each section, tables (2.1, 2.2, and
2.3) are provided to get a clear view of the previous studies and their limitations.

40
2.2 Introduction
The human heart is a multifaceted, three dimensional (3D) structure which provides
circulation to the entire body (Watanabe et al., 2004). Heart diseases are self-evidently
major factors in human morbidity and hence research into the field is extensive.
Specifically, a substantial knowledge, based on cardiac models, for both normal and
diseased hearts was required to accomplish suitable outcomes in basic and clinical
cardiac investigations (Vadakkumpadan et al., 2010).
Various experimental and numerical simulations had been conducted before this
Doctoral research commenced but many vital challenges remained. Firstly, these related
to the incorporation of simulation insights into devices which could assist cardiac
patients having weaker heart muscles. Secondly, challenges remained in achieving an
entire hemodynamic analysis inside an anatomically correct left ventricle (LV) of the
heart.
Although ventricular assist devices (VADs) were utilized for the heart failure but in
Chapter 1 it was noted that these devices had numerous complications. At the time this
Doctoral research commenced, no comprehensive device had been completed and made
available to minimize the risk of driveline infection in the VAD. This Doctoral research
therefore aimed to conduct engineering analysis that would facilitate development of a
wireless cardiac assist device which would benefit patients having weaker heart muscle
and other cardiac related diseases - for example, dilated cardiomyopathy (DCM).
Moreover, to develop the engineering models it was essential to identify/collect and
collate real data in terms of:
• Amount of wall shear on exerted endocardium
• Correct physiological properties - fluid flow velocity including the formation of
vortices, pressure inside the ventricle and their influence on physiological
properties of the heart muscle
• Structural variations of the ventricle

41
The physiological conditions of dilated cardiomyopathy (DCM) were particularly
severe for aged persons. Therefore, real data also had to be acquired for the total
hemodynamic and physiological properties of the LV during DCM. In this context,
computational approaches using computational fluid dynamics (CFD)/FSI could assess
these numerical investigations and become effective in determining and understanding
the correct physiological functioning of the cardiac model (Vadakkumpadan et al.,
2010).
The development of the cardiac assist model and the need for this device could be
divided into three sections, specifically:
• Experimental
• Numerical
• DCM investigations for the left ventricle
Detailed investigations, based on general experimental approaches, were examined in
the course of the literature review. In most cases, general qualitative hemodynamic
analyses had been performed by various researchers but, at the time of conducting this
Doctoral research, they were yet to develop a complete wireless cardiac assist device.
In order to understand hemodynamic features correctly, computational fluid dynamics
(CFD) and fluid structure integration (FSI) were alternative approaches needed to
examine the detailed functionalities of the LV. The entire geometry of the LV, together
with various physiological effects and coupling between the blood flow and the
structure deformation, were computed inside virtual surroundings. The flow pattern,
generation of vortices and changes in the intraventricular pressure and wall shear were
analysed using both simplified geometry and by obtaining actual geometry by using
various imaging tools, such as magnetic resonance imaging (MRI), echocardiography.
Earlier researchers had proved that applying ideal/simplified geometry could produce
realistic results and hence, the primary focus was to determine the:

42
• Flow pattern
• Intraventricular pressure changes
• Displacement/deformation of the LV
under various physiological conditions.
The sections which follow, review the developments and achievements in LV
hemodynamic analysis in three main areas:
• Experimental approaches
• Uses of computational approaches on an ideal LV
• Uses of computational approaches on the diseased LV, DCM

43
2.3 Analysis on the Experimental Approaches of LV
A novel approach (flow-pulse method) to determine the ventricular functionalities
inside the LV chamber was demonstrated by Hunter et al., 1979, using 11 individual
canine LVs during the systolic condition. A latex balloon was placed inside the LV
through the mitral annulus and the balloon was also attached to a hydraulic servo
system. Authors noted that by using this method it was possible to determine the
variation in the intraventricular pressure during systole. Therefore, the flow-pulse
method was very effective in investigating intraventricular pressure during the ejection
phase. Though this study was based on isovolumetric conditions, other physiological
conditions needed to be assessed thoroughly (Hunter et al., 1979).
In the same year, Suga et al., 1979, investigated the influence of pressure and volume
during systole on the end-systolic pressure and permanent end-systolic volume in the
LV of canine hearts. 25 trials were conducted on individual canine LVs and a thin latex
balloon was positioned inside the LV during the experiments. After the completion of
systole, stroke volume (SV) by end-diastolic volume (EDV) could be evaluated more
precisely by end-systolic pressure than systolic volume and pressure (Suga et al., 1979).
Instantaneous pressure (P) inside the dog LV was evaluated by instantaneous volume
(V) of the ventricle-lumen. Also, in order to determine the supplementary causes of P at
specific V, a fixed volume was assigned to the ventricle at specific time during the heart
cycle while the end-diastolic volume (EDV) and ejection velocity were varied. During
the experiment, the LV was fitted with a thin latex balloon and a tiny pressure gauge
was positioned in the apical region of the ventricle. Results demonstrated that any given
time and volume, pressure was found decreasing with a rise in ejection velocity (Suga et
al., 1980).
Sunagawa et al., 1982(a), subsequently investigated the end-systolic pressure-volume
relationship (ESPVR) with a variation in the coronary arterial pressure (CAP) in 10
excised canine LVs. A laboratory setup was established by using servo-pumps acting as
a feed-back loop, oxygenator for support dogs. The results from this study indicated that
ESPVR was moderately linear within the physiological load-range and non-linear in the

44
low load-range. However, authors noted that precise physiological boundary conditions
needed to be included on the coronary feedback loop on ESPVR (Sunagawa et al.,
1982b).
In the same year, Sunagawa et al., 1982(b), introduced a microprocessor based system
to investigate the pressure-volume relationship, where the servo-pump was regulated by
microprocessor oriented end-device which was able to generate infinite volume
waveforms unlike the analog control unit (Sunagawa et al., 1982a). Again, this group
also investigated and demonstrated the effect of LV-interaction with arterial load in
excised canine hearts. This proposed model was only applicable when the LV was
functioning as usual (Sunagawa et al., 1983).
Later, the same group examined ESPVR based on the influence of canine heart rate. A
similar laboratory setup was established and a water filled latex balloon was positioned
inside the canine LV through a metal ring in the mitral orifice. Results demonstrated
that the dissimilarity in the response of ESPVR to altering of the rate of heart could be
very effective to add to diagnostic data for patients. However, researchers restricted
controlled conditions to analysis of undamaged animal hearts. Various controlled
factors such as, reflex action and variation in CAP could also alter the heart rate
(Maughan et al., 1985).
A flow-clamp study using excised rabbit hearts based on the influence of LV internal
resistance and the flow properties including flow duration, initial volume,
ejected/systolic volume and total volume at a specified time was conducted by Vaartjes
and Boom, 1987. 15 rabbits were used for this experiment where the left atrium was
ajar, mitral valve (MV) leaflets were removed and LV was directly used excised from
the rabbit heart. Results demonstrated that ejection flow evaluated from the LV
pressure-continuous flow relation did not depend on the magnitude of pressure (P),
volume (V) and time (t). However, data based on the pressure-flow relation was
considered only for continuous flow. If the flow was not continuous, the characteristics
would have been different (Vaartjes and Boom, 1987).

45
Later, Nikolic et al., 1990, studied the influence of early diastolic filling during the
myocardial relaxation inside a raw canine LV. During their investigations LV diastolic
volume was adjusted by using a remote-controlled, customized, prosthetic mitral valve,
and a controller was placed outside the ventricle to input the correct physiological
signal. Authors noted that myocardial relaxation was influenced by diastole condition
and because of that, the time period elevated. So this condition represented as a function
of ventricle volume and time and it was a critical factor in adjusting the pressure-
volume relationship (Nikolic et al., 1990).
Mouret et al., 2000, developed a dual activation simulator (DAS) in order to investigate
the flow dynamics inside the LV. The design incorporated the LV, left atrium and the
aorta which were made from silicon. Bjork-Shiley valves were used both for the mitral
and aortic orifice. Researchers indicated that their experimental trials could implement
in vivo investigations clinically (Mouret et al., 2000).
Consequently, a new mechanical heart valve (MHV) (Triflow) was used to study the
flow pattern in the aortic opening of the LV using digital particle image velocitmetry
(DPIV). This new MHV contained three leaflets arranged in symmetric positions, and
the LV was constructed as a straight-tube and transparent. From the analysis, it was
seen that the new MHV demonstrated excellent compliance, similar to the aortic heart
valve, and small vortex wakes were found in the LV chamber behind the valve leaflets.
However LV was considered as a translucent pipe/tube and its physiological properties
were neglected during the experiment (Brucker et al., 2002). The same group previously
worked on Bjork-ShileyMonostrut (BSM) and Sorin-Bicarbon (SB) heart valves using
video-oriented DPIV technique, but the experimental approach also lacked proper LV
data (Brücker, 1997).
Pantalos et al., 2004, developed the mock circulation system which incorporated the left
atrium, left ventricle and systemic and coronary compliances to examine ventricular
assist devices (VADs). This mock circulatory system was also utilized to determine the
capability of the mock left ventricle to imitate the Frank-Starling response/effect of the
ideal, dysfunctional heart and cardiac recovery states. During the tests, the left atrium
was made of flexible polyurethane, left ventricle with flexible, segmented polyurethane

46
sac and customized tri-leaflet polyurethane valves were placed in the outflow tract.
Authors noted that the mock vasculature could be formed to imitate the physiological
properties of the general vasculature, but this system would not be able to perform trials
with in vivo models (Pantalos et al., 2004). Also:
• Testing of mono and biventricular assist devices using Computer controlled
mock circulatory system (Ferrari et al., 1998)
• Electrical circuit of 3-component LV model (WIJKSTRA and BOOM, 1989)
• Hemodynamics and P-V relation for the continuous and pulsatile VADs using
mock circulatory system (Koenig et al., 2004)
• Elastance mock ventricle system (Colacino et al., 2008, Baloa et al., 2001)
• In vitro mock cardiovascular system with LV(Furusato et al., 2007)
• Color M mode Doppler with experimental setup (Steen and Steen, 1994)
• Mock circulatory loop for the left atrium, left ventricle and pulmonary
circulation (Tanné et al., 2010).
Pierrakos et al., 2005, examined the hemodynamics of two different valves, namely:
• Anatomical and anti-anatomical position/design of the St. Jude Medical (SJM)
bi-leaflet valve
• SJM biocor porcine valve inside the flexible and transparent LV by employing
time-resolved digital particle image velocimetry (TRDPIV)
Development and merging of vortices mainly affected the contraction and extraction of
the LV. From the analysis it was determined that the anatomical structure demonstrated
slower filling phenomena whereas the anti-anatomical and porcine structures had
quicker development times (Pierrakos et al., 2005).
Subsequently, Cenedese et al., 2005 analyzed the flow dynamics experimentally in the
LV including the effect of the tilting-disk valve in the mitral orifice during the whole
cardiac cycle. For the experiment, a Plexiglas compartment, filled with water and
transparent silicon rubber LV, was submerged. The flow pattern was studied by varying
the heart rate and stroke volume. Results from this experimental study were very
47
effective in categorizing the primary characteristics of the flow dynamics in the LV.
Results demonstrated that two vortices were seen to be formed, and were propagating
diagonally inside the LV chamber, near the apical region. In the ventricle model, wall
motion was enforced outwardly and the ratio between the diameter of the LV and the
dimension of the mitral valve was higher than the actual values (Cenedese et al., 2005).
After that, Domenichini et al., 2007 investigated the flow dynamics both experimentally
and numerically in the LV during the whole cardiac cycle. The flow pattern was
analyzed based on the vortex pattern by using 3D numerical approach. For the
experimental setup a model LV was made using transparent silicon rubber, positioned
within a Plexiglas compartment, which was attached with a piston-cylinder mechanism-
the compartment was filled with water. Results between the numerical and experimental
approaches were inline, and it was found that the ring shaped vortex intermixed with the
adjacent ventricle wall. However, the shape of the LV was slightly different as used in
simulation and experimental studies. A few key parameters were neglected in the LV, as
the mitral valve was considered fixed and fully opened (Domenichini et al., 2007).
A mock circulatory system was also utilized by Gregory et al., 2009 to investigate and
assess the functionalities of the cardiac assist device of a dilated cardiomyopathy-heart.
A CT scan was used to develop the image and then mould of the LV with dilated
cardiomyopathy. The LV sac was semi-transparent and compressible (made from
silicon) and used in experimental and simulation approaches. Results indicated that the
inclusion of pulmonary blood flow into the mock system was required to imitate the
flow dynamics of the LV. However, intraventricular pressure was found negative during
the end-systolic condition of the simulation with the flow rate of 5 l/min (Gregory et al.,
2009).
In another study, Querzoli et al., 2010 assessed the flow distribution by implementing
three different valves in the mitral opening during the whole cardiac cycle. At first, the
mitral opening was set with a fuse valve (top hat inflow) which was fully opened and
without modeling the leaflets and chordate tendinae. Subsequently, mono-leaflet and bi-
leaflet mechanical valves were positioned in the mitral opening respectively. Results
demonstrated that from the investigation of turbulence data, the mono-leaflet valve

48
provided much higher turbulence concentration compared to the bi-leaflet valve, but in
the case of the fuse valve, no complete transition of turbulence was found. Also,
analysis of the flow distribution showed that the variations in the inflow velocity highly
influenced the coherent structures in the LV chamber- which were formed during the
initial diastolic phase and the inflow wave due to the atrial contraction at the end
diastolic phase (Querzoli et al., 2010). A similar study was also conducted by this group
(Fortini et al., 2008).
Yokoyama et al., 2010, developed a new pulse duplicator to examine the functionalities
of the ventricular assist devices (which could be either pulsatile or continuous) by
utilizing the pressure-volume (p-v) curve of the general heart. The tests were performed
using the LV which was made of soft latex rubber and a mono-leaflet tilting disk valve
was placed in the mitral orifice and a bi-leaflet SJM valve was positioned in the aortic
orifice during the entire heart cycle. The trials of this pulse duplicator were very
effective and useful (Yokoyama et al., 2010).
In another study, Fortini et al., 2010 examined the 3D velocity pattern throughout the
ventricle filling wave and investigated the flow pattern which was achieved from the
velocity measurement in the LV model. This velocity measurement was executed by a
feature tracking algorithm. The same LV model, with flexible and transparent silicon
rubber, was used for the tests. Results showed that an enlarged vortex in the posterior
side of the LV wall shifted towards the apical region and the flow distribution was
found to be asymmetric during the filling wave, similar to some LV disease states
(Fortini et al., 2010).
Adib et al., 2012, briefly reviewed the flow dynamics through the valve leaflets inside
the LV. Authors noted that the experimental models had limitations mostly based on the
physical setups and the outcomes. For instance, lack of ability to influence the system
pressure and continuous flow pattern was one of the critical complications. Therefore,
further investigations were still required for the experimental approaches (Adib et al.,
2012).

49
Moreover, Espa et al., 2012, experimentally investigated the flow dynamics of the LV
during the entire heart cycle. The ventricle sac was silicon made and transparent and
two check-valves were positioned in both the mitral and aortic opening. Velocity
distributions were determined both in the Lagrangian and Eulerian methods by using
image analysis. From this investigation, authors reported that by using these methods
the complex phenomenon of the intraventricular flow pattern could be easily clarified.
Also, different cross-sectional planes were taken to analyze the 3D characteristics of the
flow pattern completely. However during the study, valve leaflets were not considered
(Espa et al., 2012).
In another study, (Vukićević et al., 2012) designed an asymmetric mechanical heart
valve (MHV) model including the asymmetrical leaflets and extended central orifice.
The same configurations for the LV model were used, along with the asymmetric MHV
leaflets during the subsequent experiment. The Feature Tracking imaging tool was
utilized to analyze the flow pattern and the influence of the inlet (mitral) and outlet
(aortic) valves. It was found that the existence of leaflets, which were not symmetrically
placed in the mitral opening, elevated the propagation of the inflow jet which matched
closely with the general flow dynamics. However, the primary limitations were the poor
quality manufacturing of the valve models and the fact that a considerable analysis
between the symmetric and asymmetric MHV was required (Vukićević et al., 2012).
The hemodynamics of the LV, during the entire heart cycle, using an experimental
approach were investigated by the same group (Espa et al., 2013). This heart cycle was
generated by using a linear motor; the LV sac was constructed using transparent silicon
rubber and a one-way hydraulic valve was placed in the mitral opening. The transparent
sac was very effective in capturing the flow pattern inside the LV by using an image
processing tool, Feature Tracking. The particle displacement and the changes in the
velocity vectors, including the evaluation and merging of vortices, were observed.
Results demonstrated that for every filling wave a ring-shaped vortex was developed,
and this vortex ring was correlated to two vorticity-peaks on the measured plane. These
vortices were found propagating towards the apical region of the LV. The viscous shear
stress was also determined, as it was expected to be a critical factor for destroying the
blood cells (Espa et al., 2013).

50
Various conditions for the LV flow dynamics using experimental approaches are listed
in Table 2.1, abstracted from various references (as cited therein).
Table 2.1 Primary investigations on LV flow dynamics (experimental) References LV
Conditions
Valve
Conditions
Test Trials
(LVs)
Findings Limitations
Hunter et al.
1979
Latex balloon Chordae
tendineae was
cut off from
MV
Canine Determined
intraventricular
pressure during
ejection
Only based on
isovolumetric
conditions
Suga et al. 1979 Thin/slim
latex balloon
Canine Stroke volume
evaluated with a
fixed EDV
EDP value not more
than 25 mm Hg
Suga et al. 1980 Thin/slim
latex balloon
Canine Pressure
decreased with
the rise in
ejection velocity
LV volume was
fixed at certain time,
but EDV and
ejection velocity
varied
Sunagawa et al.
1982 (a)
Thin balloon Canine ESPVR was
determined
Only in isovolumic
contractions
Sunagawa et al.
1982 (b)
Latex balloon Canine Servo-pump
controlled by
microprocessor
based computer
Sunagawa et al.
1983
Thin balloon
attached to a
plastic adaptor
Canine To determine
the influence of
LV-interaction
with arterial
load
Only suitable when
LV was functioning
naturally
Maughan et al.
1985
Latex balloon Metal ring in
mitral orifice
Canine Evaluated data
could be useful
to add
diagnostic
information
Restricted controlled
conditions
Vaartjes and
Boom, 1987
Rabbit LV Valve leaflets
were removed
Rabbit LV pressure-
flow relation did
Only continuous
flow was considered

51
from MV not depend on
P, V and t
Wijkstra and
Boom, 1989
Rabbit LV Aortic valve Rabbit With small
propagation of
flows, P could
surpass
isovolumic P
Continuation of
super-activation
mechanism was not
thoroughly
investigated
Nikolic et al.
1990
Canine LV Customized
prosthetic MV
Canine Myocardial
relaxation
varied due to
diastole
More precise
structures of
relaxation-state
should be
experimented
Steen and Steen,
1994
Rubber
balloon
Experimental
setup
The size of the
mitral orifice
was evaluated,
which phase
was
manipulated the
flow dynamics
during diastole
Brucker, 1997 Axial-
symmetric
flow conduit
Tested BSM
and SB heart
valves
Mock-circuit
loop
Using phase-
shifted DPIV,
flow
propagation was
studied
Proper LV data
needed
Ferrari et al.
1998
Mock-circuit
system
Computer-
controlled mono
and bi-VAD
investigations
The influence of
system control unit
on ventricle needed
to be improved
Mouret et al.
2000
Silicon LV
structure
Bjork-Shiley
valves for MV
and AV
Mock loop
system
DAS was very
effective to
determine the
effect of flow
dynamics in LV
Simplified
physiological
structures
Baloa et al.
2001
Single
chamber fluid
circuit
Polyurethane
tri-leaflet
valve and
resistance
needle valve
Mock circuit
system
(elastance)
Elastance-
oriented system
mimicked the
functionalities
of natural heart
Simplified fluid
dynamic
characteristics was
considered

52
Brucker et al.
2002
Clear, straight
tube
Triflo AV Mock circuit
system
Triflo
demonstrated
good agreement
with natural
aortic valve and
its properties
Correct LV cavity
and its physiological
properties were
neglected
Pantalos et al.
2004
Flexible,
segmented
polyurethane
cavity
customized
tri-leaflet
polyurethane
AV
Mock
circulation
procedure
system
Mock
circulatory
system
developed and
verified to
assess VAD
functionalities
Not planned for in
vivo trials
Koenig et al.
2004
Flexible,
polymer
cavity
Prosthetic MV
and AV
Mock
circulation
Significance of
the dissimilarity
between
continuous and
pulsatile assist
devices
Mock system,
unable to imitate
nurohemoral
reaction, tissular
characteristics or
genetic
characteristics
Pierrakos et al.
2005
Flexible,
transparent
silicone LV
St. Jude
Medical
(SJM) bi-
leaflet valve,
SJM biocor
porcine valve
Mock
circulatory
loop
Anatomical
valve
demonstrated
slower filling
phenomena than
anti-anatomical
valve
Velocity vectors
were restricted to a
plane
Cenedese et al.
2005
Transparent,
silicon rubber
LV
Tilting-disk
valve in mitral
position
Laboratory
setup
Two vortices
were
propagating
diagonally
Physiological
properties of the LV
wall was somewhat
restricted
Furusato et al.
2007
Silicon LV Mock
circulatory
system
Peak flow rate
was observed
during lower
systolic fraction
No information
regarding valves
Domenichini et
al. 2007
Transparent
silicon rubber
LV
Two, one-way
valves in
mitral and
aortic orifices
Experimental
setup
Ring shaped
vortex
intermixed with
the ventricle
MV was considered
fixed and open

53
wall
Colacino et al.
2008
Screw driven
piston-
cylinder LV
Passive
spring-plate
MV and AV
Mock
circulatory
system
Capable of
imitating
elastance
physiology of
LV
Conditions of the
valves needed to be
upgraded
Fortini et al.
2008
Flexible, clear
and silicone
rubber LV
One-way AV
and check
valve, BSM
and Bicarbon
MV
Laboratory
model
Generation of
vortices is an
important
characteristics
in diastole
Gregory et al.
2009
Semi-
transparent
compressible,
silicon LV
Mock
circulatory
system
Could help
reducing
stagnation and
thrombosis of
VAD cannula
Lower shore
hardness silicone
and LV wall
thickness decreased
Tanne et al.
2010
Deformable,
silicon mold
LV
MV, AV Mock
circulatory
system
Ventricle can
atrial volume
can be
manipulated
Shape of the left
atrium was slightly
modified and mitral
conduit was
considered circular
Querzoli et al.
2010
Flexible,
transparent
and conical
LV from
silicone
rubber
Check valve
(AV), check
valve, BSM
and bicarbon
valves (MV)
Experimental
model
Differences in
the inflow
velocity
substantially
influenced the
coherent
structures in LV
Simplified LV
cavity was
considered
Yokoyama et al.
2010
Soft latex
rubber LV
mono-leaflet
tilting disk
valve (MV),
bi-leaflet SJM
valve (AV)
Pulse
duplicator
To assess
cardiac
dynamics/functi
onalities
Fortini et al.
2010
Deformable,
clear silicon
rubber LV
cavity
One-way MV
and AV
Laboratory
model
Generation of
vortex shedding
and its influence
Simplified LV
structure
Adib et al. 2012 Concisely reviewed the flow dynamics through
the valve leaflets inside the LV
Lack of ability to influence the system
pressure and continuous flow pattern

54
are one of the critical complications
which needs to be highlighted
Espa et al. 2012 Flexible,
transparent
silicone LV
Check valves
for AV and
MV
Laboratory
model
Complex
phenomenon of
the
intraventricular
flow pattern
could be easily
explain
No valve leaflets
were considered
Vukicevic et al.
2012
Flexible,
transparent
silicone LV
Mono and bi-
leaflet MHV
Experimental
model
Valve leaflets
elevated the
propagation of
the inflow jet
Poor quality
manufacturing of the
valve models
Espa et al. 2013 Transparent
silicon rubber
One-way
hydraulic
valve
Experimental
setup
Viscous shear
stress was
determined

55
2.4 Analysis of Numerical Approaches using CFD/FSI for an Ideal LV
The flow dynamics inside the LV were investigated by Bellhouse, 1972, where in the
development and merging of vortices during the filling wave were analysed. He noted
that because of the shape of his LV-model, the vortex was not symmetrical and
expansion of the model LV eradicated the vortex pattern (Bellhouse, 1972). In 1981,
Reul and his team examined the flow pattern in the LV by initiating a resilient pressure
gradient during the flow deceleration (Reul et al., 1981). Later, these findings were
verified by using colour Doppler mapping and Magnetic Resonance Imaging (MRI)
(Kim et al., 1994, Kim et al., 1995, Firstenberg et al., 2000, Tonti et al., 2001, Baccani
et al., 2003).
In 1993, Owen examined the effect of variation in the LV pressure during the filling
wave, where it was found that minimum pressure at the ventricle-base was higher than
the ventricle-apex. In doing so, a numerical model was developed including the atrium
and ventricle, which were represented as distensible cylinder/container during the early
diastolic filling. Owen noted that this model was not aimed to obtain results
quantitatively but to gain comprehensive knowledge on the functional behaviour of the
LV filling. Results indicated that the observation could be justified as the inflow
velocity wave moved from the basal region to the apical region of the ventricle. After
reaching the ventricle apex, the flow was reflected back to the base. Although Owen
clarified the findings, based on the intraventricular pressure change, he used a
cylindrical structure for the atrium and ventricle. Moreover, the effect of LV wall
properties and the coupling procedure were excluded (Owen, 1993).
In order to perform a 3D simulation during the ejection of the LV, Taylor et al. 1994
developed a LV model by using computational fluid mechanics. A spherical LV model
was utilized to determine the 3D flow pattern and the pressure distribution. Although
they computed the simulation during the ejection phase, they did not report any detailed
investigation in terms of formation of vortices. Moreover, the required physiological
properties of the LV wall were omitted (Taylor et al., 1994).

56
In the following year, the same group improved on their previous work by taking a
realistic human LV model which was cast from a canine heart. The authors presented a
casting technique in order to develop a LV model and also 3D simulation of the flow
dynamics and variations in the pressure distribution during systole. However, they noted
that future investigations would be to determine the influence of myocardial infracted
zones in the cardiac wall and to simulate the flow pattern (Taylor and Yamaguchi,
1995).
Jones and Metaxas (1998), using CFD solver, examined the blood flow pattern into the
ventricle chamber (LV). They used MRI-SPAMM (Spatial Modulation of the
Magnetization) to extract the wall motion of the LV and then this was used as the
boundary condition in the simulation. It was the first time that an exact boundary
condition had been utilized in a patient-specific case (Jones and Metaxas, 1998).
In 1999, Vierendeels and his group developed a 2D computer model of a canine left
ventricle and simulated the flow dynamics during the filling wave. The influence on the
flow pattern, including the formation of vortices and the changes in the intraventricular
pressure, were reported in the study. Results demonstrated the F-wave generated due to
the reflection of the intraventricular pressure at the apical region. Moreover, the flow
velocities were found to be much higher compared to the wave propagation velocity.
However, during the simulation, mitral valve annulus was considered immovable, so the
subsequent nodes were fixed and the apical motion was restricted as well (Vierendeels
et al., 1999).
McQueen and Peskin, 2000, were famous for their development of the “Immersed
Boundary Method”, a numerical method which concurrently calculated the fluid/blood
motion and the elastic-boundary motion (or wall) submerged in and creating an effect
while interacting with the fluid. They were mainly focused on the behaviour of the
blood flow inside the human heart and to develop a method, which utilized the forces
evolving from a submerged boundary. However they noted that a lack of effective
interactive visualisations turned out to be their main problem. In addition, illustrating a
complete velocity distribution was found arduous and while demonstrating a small area
of a velocity field it was also complicated to compute vector components in the

57
direction, for the display monitor. Their medium-term aims were to examine some
disease conditions and to construct some prosthetic devices, specifically prosthetic
valves. The long term objectives were to calculate the flow behaviour inside the heart in
real time and, at the same time, to be capable of modifying the structure and functioning
properties of the model. McQueen and Peskin concluded that once they completed their
goals, this approach/method would then be very helpful to diagnose and to assist in
medical treatment, but it would require noteworthy advancements in end device power,
computing algorithms and higher imaging quality (McQueen and Peskin, 2000).
Utilizing the immersed boundary technique, Lemmon and Yoganathan, 2000, made a
computational model and deployed it into the thin-walled human left heart model under
appropriate flow conditions in order to investigate physiological flow conditions by
considering irregular diastolic dysfunctions. The authors considered changes in
ventricle stiffness and the volume of blood flow inside the LV and from the simulations,
they noted that the amount of blood flow reduced with an increase in ventricular
dysfunction and increase in ventricle stiffness (Lemmon and Yoganathan, 2000).
Vierendeels et al., 2000, improved their own previous study (Vierendeels et al., 1999)
by utilising the Immersed Boundary technique which was acquired from a study of
McQueen and Peskin, 2000. The authors investigated the intraventricular flow and
pressure gradients during diastole, based on a 2D axisymmetric simplified CAD model.
They stated that the generation of vortices were evident during the acceleration phases
of the diastolic wave and while it was in the diastasis phase, the vortices were enlarged
inside the ventricle. Although they demonstrated the pressure distribution and flow
dynamics in the LV but they did not consider the regional dissimilarities in the Young’s
modulus and thickness of the LV. Moreover, the effect in the flow dynamic with the
change in the angle between the mitral and aortic orifice were not computed
(Vierendeels et al., 2000).
In another study, Kilner and his team, 2000 investigated the axisymmetrical blood flow
directions inside the atria and ventricular cavities, obtained from the magnetic resonance
velocity mapping. They concluded that asymmetries in the ventricular cavity hold
fluidic and dynamic advantages (Kilner et al., 2000).

58
Saber et al., 2001, developed a methodology to simulate the flow pattern inside the LV
by using the combination of CFD and magnetic resonance imaging (MRI). In order to
perform CFD, the geometry of the LV was developed by employing an MRI of the
heart. Authors demonstrated the physiological changes in the LV, including the
contraction and expansion and flow dynamics inside the ventricle, incorporating the
formation of vortices and swirling features. Although the results were in line,
qualitatively, with previous research, the simulation of the velocity distribution was
restricted due to a lack of anatomical data related to the valve orifices (Saber et al.,
2001).
Watanabe et al., 2002, simulated the pumping characteristics of the human LV by using
the FSI finite element (FE) scheme, adding the dissemination of the excitation and
excitation-contraction (E-C) coupling method for discrete cardiac myocytes in the
subcellular level. The authors presumed that the inertia between the model wall and the
fluid were minimal. FSI was limited on the model boundary and because of this, the
kinematics of the fluid were eradicated from the FSI scheme. Also, a finite element
method (FEM) code was built to characterize the cardiac muscles (Watanabe et al.,
2002).
In 2000, a 3D in vivo flow pattern/characteristics and pressure distribution inside the
human LV using the combination of velocity field measurements and the computational
fluid dynamics was demonstrated by the Ebbers et al. They noted that the velocity and
pressure distributions offered substantial insights into ideal cardiac pressure dynamics.
Also, the in vivo measurement and visualization of these 3D velocity and pressure fields
could prove very useful in order to establish the total functionalities of the heart both for
the normal and diseased persons (Ebbers et al., 2002).
In 2002, Verdnock and Vierendeels observed the hydrodynamical mechanism inside a
simplified canine LV flow pattern was the propagation of the vortex during the 3D
filling cycle. They also investigated the correlation between the centre of the vortex and
location of the maximum flow velocity during diastole. However, the position of the

59
mitral annulus was considered stationary during the simulation (Verdonck and
Vierendeels, 2002).
Using CFD, the hemodynamics of the 3D LV model, including the formation of vortices
and the intraventricular pressure distribution during early diastole, was examined by
Nakamura et al., 2002. The authors confirmed that the transmitral velocity was
responsible for developing a vortex ring which elongated from the anterior side to the
posterior side in the ventricle chamber. Also, the vortices kept the flow pattern linear to
the apical region of the ventricle. However, during their investigation they assumed that
the ventricle-wall movement was not dependent on its flow pattern inside the chamber
(Nakamura et al., 2002). This work was further modified and updated by Nakamura et
al., 2003, to determine the primary features of the interaventricular pressure distribution
and the flow pattern during the filling wave. They demonstrated that the annular vortex
caused the inflow fluid path to be narrowed and thus the velocity of the fluid elevated
while flowing through this annular vortex. An echocardiographic test was conducted to
compare/match the results due to the transmitral fluid flow and the generation of the
vortices. Once again, they assumed an ideal LV geometry and the physiological
properties of the LV, including the twisting motion of the LV, were restricted
(Nakamura et al., 2003).
Subsequently, it was observed that a non-parallel/asynchronous electrical trigger could
lead to different irregularities in perfusion and pumping operations. For this reason,
Usyk and McCulloch, 2003, employed an electromechanical model in order to examine
the functioning effects of the distorted cardiac series by using a 3D canine ventricular
wall model. The authors found significant differences in delay times which were due to
numerous issues including discrepancy in local anatomy and end-diastolic strain and
stress. They concluded that these essential 3D ventricular features were responsible for
producing a series of fibre shortening, which yielded erratic replacement for regional
depolarization or electromechanical activation inside the undamaged ventricle (Usyk
and McCulloch, 2003).
In 2003, Kerckhoffs and his team, using a simplified canine model for pacing at the left
ventricle free wall and right ventricle apex, simulated using myofiber alignments the

60
depolarization time and shortening in the LV. The results demonstrated that early
shortening was evident during the isovolumic contraction/systole period and during the
late depolarization areas, myofibers were found lengthened. However, with the
exclusion of the right ventricle in the left ventricle free wall pacing, the depolarization
timing results were affected (Kerckhoffs et al., 2003).
After improving the work from (Saber et al., 2001), Saber et al., 2003 demonstrated the
flow dynamics of the LV, including the generation of vortices during the entire cardiac
cycle, using a combination of CFD and magnetic resonance imaging (MRI) scan of the
LV. The results showed that the development of the coherent vortex was identified near
the mitral orifice and, during the end-diastolic phase, an elongated vortex was formed in
the anterior region of the LV. Although they verified the results with MR data and other
experimental studies, due to the limitations of the MR data, especially for the valves,
they did not incorporate the detail physiological properties of the LV (Saber et al.,
2003).
In other work, Long et al., 2003, studied the influence of various boundary conditions
for the LV flow. They also developed a new hybrid approach in the inlet region in order
to examine different operational inlet boundary conditions. This approach amalgamated
the required velocity profile in the majority of the inlet region and required pressure
distribution to the rest of the inlet area in order to accomplish global mass conservation.
Simulations were employed with their projected approach and using the pure pressure
boundary approach. Based on comparisons and investigations on optimal and prime
areas, the authors noted that CFD simulations were very sensitive to imposed boundary
conditions in the filling phase inside the LV. With the change in the inlet area, however,
the flow pattern and the inflow profiles varied inconsistently (Long et al., 2003).
In 2004, Watanabe and his team developed their earlier work (Watanabe et al., 2002)
further in order to associate the sub-cellular molecular actions in the functioning
procedure of the heart. They prepared a 3D simulation technique where the objective
was to integrate the combination of contraction and expansion mechanisms along with
their proliferation in the cellular level physiology where they had conducted simulations
using the FSI scheme on the human LV using the FE (Finite Element) procedure. The

61
behaviour of the fluid flow inside the cavity, along with the effects on the cavity wall,
were simulated by using an electrical analogue to characterize the pulmonary
circulation. The left atrium (LA) was employed as a preload and the Windkessel model
utilized as afterload. They effectively imitated the biphasic filling flow and atrial
contraction allied to earlier research and other clinical findings. Wave propagation
velocity was investigated further using the FSI scheme and the authors noted that this
scheme could be an ideal source for correlating molecular disorders and clinical
irregularities. Conversely, due to the lack of computational power at the time the
research was conducted, LA was developed using electrical circuit which would
definitely limit the proper physiological conditions (Watanabe et al., 2004).
Verhey and Nathan, 2004, discussed a technique regarding the transfer of data of a LV
obtained from the transesophageal echocardiography (TEE) into a finite element
analysis software package, namely ABAQUS. The authors demonstrated the direction
of pressure exerted from the LV wall for both the filling wave and systole (Verhey and
Nathan, 2004).
In 2004, McCulloch also reviewed examples of computational biology in terms of:
• Computational models which were effective for different interacting features
within biochemical systems.
• Structurally detailed models which were valuable for interacting within
biological organizations, including molecules to organisms and assimilation of
data in clinical and laboratory works.
These types of features were described utilizing cardiac E-C coupling and the
electromechanics of the complete heart, both in ideal and disease stages (McCulloch,
2004).
Subsequently, an electromechanical model of the heart was deployed by Sermesant et
al., 2005, where they represented the MRI imaging method in vivo to:

62
• Examine the heart
• Develop a standard cardiac structure
• Develop mathematical equations to perform the simulation of electromechanical
characteristics of the model
• Match the general cardiac structure with the patient-cardiac model and the data
assimilation techniques to determine the contraction of the cardiac structure
However they noted that the long term goal would be to investigate the cardiac structure
of a patient experiencing electrophysiology studies (Sermesant et al., 2005).
The findings from previous studies were utilised by Cheng et al., 2005, where they
investigated the flow dynamics during the filling phase of a simplified LV structure.
During the computational approach, they analysed the variation in the pressure
distribution and velocity distribution, including the development and merging of
vortices. It was noted that flow patterns during the late diastole were inconsistent in
different computational and experimental approaches. Inclusion of real LV wall
properties and changes in angle between the inlet and outlet of the LV were neglected
(Cheng et al., 2005).
In another study, Domenichini et al., 2005 examined the numerical approach of the 3D
flow dynamics inside the simplified LV model using a prolate spheroid structure during
the filling phase. To identify and understand the primary fluid phenomena and
physiological characteristics inside the enlarging LV of healthy young adults, they
analysed the values of the geometrical and flow pattern parameters, including
generation and evolution of vortices. Results indicated that when the value of the
Strouhal Number was minimal, weak turbulence was seen developed by the flow
dynamics. However, they considered the quiescent flow as a preliminary boundary
condition during the computational approach and also they did not consider the
variation in angles between the mitral and aortic orifice in the LV (Domenichini et al.,
2005).
Pedrizzetti and Domenichini, 2005 investigated the intraventricular blood flow inside
the human LV by utilizing prolate spheroid geometry, where the model wall could be

63
"moved along" with time. The authors also analysed the flow patterns including the
evolution of vortices and they verified the findings, similar to the physiological
structure of the ventricle. Additionally they noted that, because of cardiac diseases
and/or due to substitution of valves, pumping efficiency could decrease more than 10%
and therefore that cardiac muscles were essential to supplement the functioning
efficiency (Pedrizzetti and Domenichini, 2005).
Although their primary work was basically focusing on physiological properties and
fluid flow inside the ventricle cavity, in 2006, Formaggia and others documented a
unique methodology, simulating the arterial network with minimal computational costs.
Their primary interest was in the coupling mechanisms between the LV and the arterial
network due to their significance in physio-pathology. However, the authors noted that
their future work would be highlighting different pathological cases, defining the wave
reflections provoked by the existing endoprosthesis, or by means of implementing
bypass in a surgery. Additionally, they noted that representing the detailed
functionalities of the heart (encompassing the venous system) and aging consequences
as well as triggering the electrical initiation of myocardium would need to be taken into
account as well (Formaggia et al., 2006).
Lee et al., 2009 reviewed the advancements and applications of the coupling
mechanisms within the entire heart, including the ventricle contraction, expansion,
excitation and the flow dynamics in the coronary artery. The authors investigated the
influence of the coupling mechanics in order to determine the entire cardiac
functionalities, but they noted that further investigation was required:
• On the hemodynamics
• To construct a physiological model of a cardiac anatomy
• To improve the additional coupling methods
so that these schemes could become more robust and efficient to deliver the necessary
insights of cardiac physiology (Lee et al., 2009).

64
Vadakkummpadan et al., 2010, reviewed earlier investigations into developing
computational models of the whole heart and then illustrated a processing pipeline
which was utilized to form the:
• Normal mouse, rabbit, canine, human hearts
• Weakened canine heart, infracted/diseased rabbit and canine cardiac structures
They generated these models from high resolution 3D structural magnetic resonance
(MR) and diffusion tensor magnetic resonance (DTMR) image tools ex vivo. They
concluded that although their generated models offered substantial structural features it
would take a significant amount of time to develop (Vadakkumpadan et al., 2010).
A 3D electromechanical model for the LV was constructed by Keldermann et al., 2010,
where the authors studied the influence of the effects of the electrical wave and
mechanical contraction. However, they used limited experimental results in order to
characterize desired mechanical feedback and also ignored the variation in the angles
between the mitral and aortic orifice (Keldermann et al., 2010).
In 2011, Gurev and his researchers presented an innovative method in order to produce
a precise anatomical model of the heart using imaging tools such as, higher MR
(Magnetic Resonance) resolution and DTMR (diffusion tensor magnetic resonance)
cardiac images. By using their methodology, they were able to produce the finite
element models consisting of normal canine, deteriorated canine and human ventricles,
but the normal canine model was further utilized to reproduce and analyse physiological
behaviour, signifying the effectiveness of their electromechanical model. Although they
generated the electromechanical model of the canine ventricle, in order to reduce the
computational effort, weak coupling was used. Also, they did not consider any angular
variation in the mitral and aortic orifice where the change in the hemodynamic
behaviour might affect or change the total physiological properties (Gurev et al., 2011).
Nordsletten et al., 2011, reviewed the entire mathematical framework in order to
characterize the contraction and expansion of the heart ventricles and the correlation
behind these mechanics, including the functionalities of the ventricle; 3D flow

65
dynamics; coronary blood flow; electrical activation, and in clinical applications. The
authors noted that further investigation and research were still required based on the
physiological characteristics - for example, detection of ischemia; advancements in
diagnosis tools and to characterize influences after cardiac surgery and/or ventricle
pacing (Nordsletten et al., 2011).
Mihalef et al., 2011 demonstrated a patient-specific model which included the entire
human heart. The cardiac structured incorporated all four chambers and the associated
valves; the aorta, and the pulmonary artery. The authors performed a CFD simulation
based on the hemodynamics flow pattern during the complete cardiac cycle. Later, the
simulation results were matched with the 4D flow pattern, which was acquired from the
phase contrast MRI (Mihalef et al., 2011). A 4D velocity distribution in the ventricle
chamber and the great vessels was reviewed and examined by Markl et al. 2011 (Markl
et al., 2011).
Sugiura et al., 2012 reviewed and analyzed the fundamental mechanisms and
characteristics to determine not only the multi-scale properties but also the significance
of the multi-physics properties of cardiac simulation, including the effect of molecular
and cellular features along with the characterization of the required electrophysiology
and the flow dynamics. The authors noted that it would be highly costly to construct a
heart model with all these features but they had developed a sample model. However,
the required characteristics, such as metabolism, would be included in a future model
which might be an ideal tool for clinical applications. Also, because of the restrictions
in computational power, almost every cardiac structure deployed the lumped parameter
structure in the case of cellular models. Although the capability of advanced-computer
systems was progressing rapidly, it was still very complicated to model the entire
cardiac structure including the features of the myocyte. This will require a large number
of degrees of freedom and was under development (Sugiura et al., 2012).
In another study, Lassila et al., 2012 implemented a novel method for a computational
approach and data assimilation inside the 3D LV during an entire heartbeat. Also, they
linked the LV with a 1D interaction of the arterial model in order to determine the flow
dynamics and pressure distribution, both in the LV and the arterial system and therefore

66
achieving a multi-scale structure. It was noted that his model could be effective for
clinical applications using patient-specific data and also by incorporating other multi-
scale and multi-physics properties (Lassila et al., 2012).
Lee and Sotiropoulos, 2013, presented an innovative cell-activation oriented structure in
order to simulate the physiological effect of the LV during the entire cardiac cycle.
Using FSI, the physiological characteristics of the LV wall motion were utilized to
simulate between the flow pattern and the influence of the bi-leaflet mechanical heart
valve (BMHV) inserted into the aortic orifice. They demonstrated that the model was
efficient in determining the influence of fibre deformation characteristics. However,
during the study, the mitral valve was considered fully open as the researchers did not
consider the influence of the mitral valve (Le and Sotiropoulos, 2013).
Consequently, Adib et al., 2013 examined the flow behaviour and the mitral valve
leaflet in the LV, during the diastolic condition, by considering simplified 2D heart
valve leaflets using FSI. They simulated the displacement and velocity pattern for four
different shapes of the valve leaflets and concluded that the triangle-leaflet
demonstrated maximum displacement and change in the velocity. The generation of
vortex was also evident under the valve leaflets. Even though these researchers
performed the FSI on the valve leaflets, they did not consider the effect of the ventricle
wall during the flow dynamics and a highly simplified LV geometry was adopted (Adib
et al., 2013).
In another study, Arefin and Morsi, 2014 studied the hemodynamics features by using
FSI during the diastolic flow conditions. Changes in the flow dynamics including the
overall characteristics of the vortices, wall shear stress (WSS) and intraventricular
pressure along with the deformation of the ventricle were simulated and determined
(Arefin and Morsi, 2014).
Table 2.2 encapsulates different LV flow conditions using computational approaches as
summarized and tabulated from various references.

67
Table 2.2 Left Ventricle researches and its configurations
References Fluid
State
Viscosity Limitations and
Challenges
Findings
Bellhouse,
1972
Expansion of LV eradicated
the vortex
Reul et al.
1981
3.6 cp LV wall properties were
not fully described
Developed vortices might
not affect the valve closure
procedure
Owen, 1993 Cylindrical LV model and
required LV wall
properties were excluded
Flow propagation inside the
LV due to change in
intraventricular pressure
Taylor et al.
1994
Newtonian,
homogeneou
s and
incompressi
ble
Formation of vortices and
LV wall properties were
not discussed
To compare simulation data
with different imaging
techniques
Kim et al.
1994
Doppler echocardiography Anaesthesia affected the
non-physiological
variables, as flow velocity,
heart rate and blood
pressure
Filling pattern inside the LV
during diastole were
affected by LV flow
dynamics
Kim et al.
1995
Magnetic resonance velocity
mapping
Vortex movement was
only measured in x-y plane
Sizeable counter clockwise
vortex inside LV was
reported
Taylor and
Yamaguchi,
1995
Newtonian,
homogeneou
s and
incompressi
ble
LV was considered hollow Formation of 3-D vortices
Jones and
Metaxas,
1998
Newtonian Vortex-phenomenon was
not discussed
Patient-specific LV flow
dynamics was simulated
Vierendeels et
al. 1999
Newtonian Mitral annulus was
inflexible and LV apical
movement was restricted
Generation of F-wave and
the influence of slower
relaxation and elevated
stiffness
Firstenberg et
al. 2000
Colour Doppler LV inflow wave was
considered laminar
Combination of complex
image processing method
and Eulerian equation to

68
investigate diastolic
pressure gradient
Vierendeels et
al. 2000
Newtonian 2.5431026
m2/s
Required LV wall
properties were neglected
including the variation in
wall thickness
Vortices developed during
the acceleration phases of
the diastolic wave and it
enlarged during diastasis
Lemmon and
Yoganathan,
2000
Physiological detail was
not fully included by these
coupled models (Lee et al.
2009)
The amount of blood flow
reduced with the rise in
ventricular dysfunction and
increase in ventricle
stiffness
Kilner et al.
2000
Different functional data
would be required to build
a reliable model (Lee et al.
2009)
Twisting and asymmetries
of the cardiac structure
provided substantial
functional advantages
McQueen and
Peskin, 2000
Newtonian
fluid
Interaction between the
fluid and leaflet motion of
the valves were highly
complicated to simulate
and lack of quality
graphics made it harder to
analyze
Flow pattern inside the
cardiac structure of human
Saber et al.
2001
Newtonian fluid; MRI Simulation of the velocity
distribution was restricted
Successfully generated 3D
systole and diastole
conditions of LV
Watanabe et
al. 2002
Viscosity 4.71 E-3 Pa Inertias between the model
wall and the fluid were
minimal and FSI was
limited on the model
boundary
To simulate the LV
contraction and the flow
dynamics inside LV FSI
code has been generated
Ebbers et al.
2002
Newtonian
fluid
0.004
Ns/m2
Spatial resolution was
somewhat restricted and
inadequate to evaluate
viscous resistance
Velocity and the pressure
distributions offered
considerable details in an
ideal cardiac structure
Verdnock and
Vierendeels,
2002
Color M-mode Doppler
echocardiograms
Location of the mitral
annulus was considered
inflexible
Hydrodynamical procedure
inside the canine LV flow
pattern is similar to the
propagation of the vortex in
the LV

69
Nakamura et
al. 2002
Newtonian,
homogeneous
and
incompressibl
e
3.5 E-3 Pa.s LV wall movement was
not dependent on its flow
dynamics inside the cavity
Transmitral velocity was
responsible for the
generation of vortex ring
and the vortices followed
linear flow pattern towards
apex
Nakamura et
al. 2003
Newtonian,
homogeneous
and
incompressibl
e
0.035
g/(cm.s)
Simplified LV model and
proper physiological
properties were neglected
Annular vortex inside LV
was responsible for the
inflow fluid path to be
narrowed and thus the
velocity of the fluid
elevated
Baccani et al.
2003
Newtonian, M-mode
representation
Axisymmetric assumption
of the geometry could not
illustrate 3D flow
dynamics
Multifaceted adhesive
vortices were found to be
developed due to the
moving/flexible valve
Usyk and
McCulloch,
2003
Considered a constant
interval in between
electrical initiation and
contraction
Validation of numerical
results and evaluation of LV
depolarization developing
in 40 to 55 msec
Long et al.
2003
Incompressibl
e Newtonian
0.004 Pa s Due to the change in the
inlet orifice, flow
dynamics varied
inconstantly
Pressure-regions were
affected by flow dynamics
in the hybrid boundary
states
Kerckhoffs et
al. 2003
Depolarization timing was
affected due to the
exclusion of RV in left
ventricle free wall pacing
Early shortening was
evident during the
isovolumic contraction
period and in late
depolarization areas,
myofibers were found
lengthened
Saber et al.
2003
Homogeneous
and
Newtonian
4
E-3 Pa.s
Detailed physiological
properties of the LV were
not considered
Development of the vortex
was located near the mitral
orifice and during the end-
diastolic phase an elongated
vortex was developed in the
anterior section of the LV
Watanabe et
al. 2004
Newtonian 4.71*10-3
Pa.s
LA model was developed
using electrical circuit
A finite element (FE) code
was developed and

70
because of lack of
computational power
implemented to simulate the
systole and diastole of the
LV, incorporated with LA
electrical analog and
pulmonary flow dynamics
McCulloch,
2004
[Review]
Verhey and
Nathan, 2004
3D transesophagealecho
cardiography (TEE)
Required substantial
validation procedure
including the pre, post and
bypass surgery using MRI
and compare between
them
For detailed intraoperative
investigation in LV, 3
factors namely, realistic
model data, LV pressure
and tissue elastance data
were required
Sermesant et
al. 2005
MRI Highly challenging to
investigate the invertibility
properties using data
assimilation method
Using data assimilation
technique, it was possible to
evaluate the contractility
from particular
displacements
Pedrizzetti
and
Domenichini,
2005
Newtonian 3*10-6 m2/s
(kinematic)
Mitral valve was
considered circular,
stationary and open
Flow energy dissipation
was seen decreasing related
to the anatomical
conditions
Domenichini
et al. 2005
Quiescent flow was
considered at the
beginning of the
simulation
Weak turbulence was seen
developed at low Strouhal
number
Cheng et al.
2005
Newtonian 0.00316
Pa·s
Simplified LV geometry
and uniform transmitral
flow velocity
Changes in the
intraventricular pressure
and velocity was obtained
and demonstrated in LV
cavity during ventricular
expansion
Formaggia et
al. 2006
Newtonian Movement of the vessel in
the arterial network was
restricted only in radial
direction and the flow was
considered axi-symmetric
Coupling between LV and
the arterial network have
been simulated due to its
significance in patho-
physiology with lower
computational expense
J. Lee et al. [Review]

71
2009
Vadakkummp
adan et al.
2010
Magnetic resonance (MR)
and diffusion tensor magnetic
resonance (DTMR)
Higher time required to
produce the models
Different animal models
were used to characterize
substantial structural
features for simulation of
the cardiac
electromechanical models
Keldermann
et al. 2010
Limited experimental data
was taken to characterize
electromechanical
feedback and only fibre
orientations was
considered in the model
3D electromehcanical
model of LV was developed
to investigate the electrical
proliferation and
physiological/mechanical
contraction
Gurev et al.
2011
Higher MR (Magnetic
Resonance) resolution and
DTMR (diffusion tensor
magnetic resonance)
No strong coupling
between electrical and
mechanical components
Cardiac cell membrane,
myofilament dynamics,
electrical wave, ventricle
shortening and
hemodynamics were
included in the
electromehanical model to
simulate the electrical and
physiological/mechanical
actions of the ventricles
Nordsletten et
al. 2011
[Review]
Mihalef et al.
2011
Newtonian 4m Pa.s Patient oriented heart model
was utilized to as an input
to 3D Navier-Stokes solver,
which provided realistic
flow pattern
Markl et al.
2011
4D Phase contrast
cardiovascular magnetic
resonance (CMR)
Substantial amount of time
was required to obtain and
investigate 4D velocity
components
Non-invasive 4D
measurements of
hemodynamics inside the
heart and great vessels
demonstrated substantial
insights over 2D and 3D
techniques
Sugiura et al.
2012
Required higher
computational power and
Constructed an electro-
mechano-hemodynamic

72
degrees of freedom cardiac structure prototype
Lassil aet al.
2012
Newtonian 0.035
g/cm/s
More precise data on LV
structure and accurate
calibration were required
Development and
investigation
ofhemodynamics using
mathematical multi-scale
structure by including 3D
LV model and 1D arterial
network
Lee and
Sotiropoulos,
2013
Incompressibl
e, Newtonian
3.33 E-6
m2/w
Influence of mitral valve
was not considered
To simulate hemodynamics
and the influence of the bi-
leaflet mechanical heart
valve (BMHV) positioned
into the aortic orifice
Adib et al.
2013
Incompressibl
e, Newtonian
2.70 E-3
Pa.s
LV wall effect was
neglected
Triangular leaflet
demonstrated maximum
velocity distribution and
displacement variation
Arefin et al.
2014
Newtonian 0.0035 Pa.s No valvular effects have
been included and only
filling phase has been
considered
Magnitude of the WSS,
intraventricular pressure,
flow pattern and structural
displacement have been
determined

73
2.5 Analysis of Experimental and Computational Approaches of the Diseased LV:
Dilated Cardiomyopathy (DCM)
Dilated heart failure generally characterises the LV diastolic pressure to increase
because of the lack of supply of blood to the whole body during systole. Grossman et
al., 1979, investigated other parameters, such as LV relaxation rate and diastolic
compliance, on eight people who were affected by cardiomyopathy in order to observe
whether these parameters could cause the diastolic pressure to elevate inside the LV.
Results indicated that LV relaxation in the early diastolic period reduced in
cardiomyopathy and this deficiency was due to a reduction in LV compliance
(Grossman et al., 1979).
Takenaka et al., 1986 also determined the significance of the LV filling with DCM
using pulse Doppler echocardiography. This study involved:
• 21 patients having DCM and mitral regurgitation (MR)
• 12 patients having only DCM without MR
• 19 healthy patients
Irregularities in the peak inflow velocity wave were identified from the investigation in
DCM patients with no MR. However, these irregularities were not found in the patients
containing both DCM and MR. So, it was concluded that MR substantially affected the
LV diastolic irregularities in DCM patients (Takenaka et al., 1986).
Jacobs et al., 1990 examined the pulsed-wave and colour Doppler measurement in 48
patients having DCM - 14 additional patients (in healthy condition) were utilized as a
reference. The results indicated that quick transmitral flow propagation starting from the
base to the apex of LV was observed in the healthy subjects. However, DCM-patients
lacked this phenomenon and delayed flow propagation was found in DCM conditions.
Also, the time differences of the inflow velocity in DCM patients were found to be
higher than the normal subjects. Moreover, in DCM cases, the apical velocities were
substantially elevated and the outflow velocity was decelerated (Jacobs et al., 1990).
Echocardiographic measurement was also utilized by various authors to determine the
74
functional behaviour and mitral regurgitation of the LV during the cardiac cycle
(Vanoverschelde et al., 1990, Kŭtova et al., 1981, Cioffi et al., 2005, Zhang et al., 2013,
Levisman, 1977 ).
Levin et al., 1996 reported that a 19 year old patient having heart failure, due to DCM,
was being assisted with the left ventricular assist device (LVAD) for approximately 183
days. However, when heart transplantation was planned for that patient, it was observed
that the patient’s heart came back to normal size and shape, general ejection fraction
and other functionalities. Therefore, that LVAD was explanted and the transplantation
was not executed. However, at a later stage, the heart enlarged, the ejection fraction was
abnormal and the patient died because of the heart failure intensified deeply by a
systemic viral illness infection. Because of this, the authors noted that these findings
might become useful in terms of the treatment procedure (Levin et al., 1996).
Loebe et al., 1997 reported that LVAD had assisted in a 36 year patient having DCM
for approximately 795 days. Throughout this period, functional repossession of the
cardiac structure was observed. When a donor was found for the heart transplantation,
LVAD was explanted from the patient and the surgery was performed. Following
surgery, the physical condition of the patient was found satisfactory and he was
discharged afterwards (Loebe et al., 1997).
Hetzer et al., 1999 investigated the significance of the ventricular assist device and/or
replacement of VAD pumps after an "assisting time" of 26 months on 19 patients
containing uncontrollable end-stage DCM. During their analysis
• 7 patients were found rebuilding their cardiac functionalities beyond 8 months
• 5 patients fewer than 5 months’ time.
• 5 patients died because of heart failure within 4-8 months’ time
• 2 patients died from other than cardiac related complications
The authors concluded that long-term retrieval can be achieved by ventricle-unloading
in a group of patients containing acute dilated cardiomyopathy (Hetzer et al., 1999).

75
Baccani et al., 2002, demonstrated a comprehensive analysis of the flow dynamics
inside the simplified LV model during the filling phase. The flow pattern had been
examined for both the normal and dilated ventricle. However, during the numerical
simulation, the flow pattern was considered axisymmetric and the mitral valve was
assumed fixed. For the normal case, the formation of a wake vortex during the early
filling wave was identified. During the simulation of the dilated ventricle, the thickness
of the LV wall increased, which resulted in a delayed separation of the wake vortex; the
flow velocity decreased and the vortex stagnated for a longer period of time close to the
apical region of the ventricle (Baccani et al., 2002).
Yotti et al., 2005 studied the influence of diastolic suction in patients with DCM by
using colour M-mode Doppler images. Diastolic suction is known to be a key factor in
animal trials for the early diastolic wave in the LV and it was related to the development
of a diastolic intraventricular pressure gradient (DIVPG) between the apical and basal
region of the LV during the early filling wave. Initially, authors performed and
validated this method on animals to evaluate the spatio-temporal distribution of DIVPG
using Doppler images. Subsequently, the authors used 40 patients with DCM and 20
healthy people for this study. Results demonstrated that the maximum DIVPD (diastolic
intraventricular pressure gradient and difference) was below 0.5 in the DCM patients
relative to the healthy people. Also, DCM patients displayed uncharacteristically
reduced diastolic suction. However, for acute DCM, the percentage of error, due to 1-D
Doppler image simplification, might be significant (Yotti et al., 2005).
Liden et al. (2007) studied the effect of LVAD device-weaning in 18 patients as a
bridge-to-transplantation. A four months follow-up was conducted and the patients were
frequently monitored with right heart catheterization and Doppler echocardiography. It
was found that three patients were able to accomplish the conditions required for
cardiac retrieval and the LVADs were explanted, but the process was unsuccessful as
the diseases reoccurred or they needed transplantation. Therefore, the authors claimed
that patients having acute heart failure were unlikely to demonstrate substantial
recovery of cardiac functionalities following the use of LVAD (Liden et al., 2007).

76
In another study, the effect of the formation of vortex using the left ventricle assist
device (LVAD) in a dysfunctional ventricle had been investigated by Loerakker et al.,
2008. An axisymmetric flow pattern of the LV model was considered and it was linked
with a lumped parameter model to accomplish the flow circulation. Computational
simulations were executed both in ideal and dilated conditions (DCM). It was found that
the magnitude of the primary vortex was significantly lower in the DCM ventricle than
the ideal case. Also, the LVAD was responsible for elevating the magnitude of the
vortex and was also responsible for diminishing the vortex much more quickly. The
authors used a simplified LV cavity for the computational approaches (Loerakker et al.,
2008).
Thomas et al., 2009 discussed the critical features of echocardiography in the
assessment and management of cardiomyopathy. The authors suggested that the people
who are presumed to have heart failure should undergo complete echocardiographic
assessment in order to diagnose DCM and other cardiac diseases including valve
diseases. By using the standard echocardiographic and ultrasound technique along with
the usage of modern technologies, such as:
• Tissue-Doppler imaging
• Strain analysis
• 3D echocardiographic assessment
greater insights could be obtained for pathological reports which might be effective for
cardiomyopathy patients (Thomas et al., 2009).
Jefferies and Towbin, 2010 discussed the fundamental characterization of the DCM and
its influence in heart failure. Although the outcomes in DCM had enhanced, the general
consequences still needed to be improved, especially for patients having non-ischemia
diseases. Because of this, gene-based therapies, including the gene-therapy, stem cell
treatment and other targeted therapies were in progress (Jefferies and Towbin, 2010).
DCM and its categories and the influence of myocardial collagen in the development of
DCM were further discussed by (Maron et al., 2006, Elliott et al., 2007, Hershberger
and Morales, 2013, Gunja-Smith et al., 1996).

77
Chan et al., 2012 examined the influence of size and shape of the simplified left
ventricle model in terms of the formation of vortices and the variation in the
intraventricular pressure gradient (IVPG) during the entire cardiac cycle. They used two
different methods namely:
• Geometry-prescribed
• FSI
in the normal and dilated ventricle. Results demonstrated that the magnitude of the
vortices and IVPG were greatly reduced inside the dilated LV which, in turn, elevated
the possibility of thrombus development and weakened flow propagation. Also, they
suggested that the FSI technique is the best possible option in order to investigate
dysfunction and certain predictive features of the LV. However, a simplified LV model
with DCM was considered for all the simulations (B. T. Chan et al., 2012).
The same group, Chan et al., 2013 further investigated sensitivity analysis in a dilated
(DCM) LV by using the FSI. During the work they examined the influence of the
idiopathic and ischemic DCM inside the LV in terms of the flow pattern and the
variation in the myocardial wall stress. Additionally, key factors which were responsible
for DCM were also examined, including the velocity of the peak E-wave, variation on
the myocardial-wall features and so on. The flow dynamics inside the ventricle and the
twisting of the myocardial wall were highly reduced compared to a healthy case. Also,
from the sensitivity analysis, it was demonstrated that flow velocity significantly
reduced with the rise in the ventricle stiffness. The analysis might provide
comprehensive data but by using an axisymmetrical model of the LV, intraventricular
flow dynamics and the formation of vortices might be influenced. Future studies would
need to use an asymmetrical LV model or any other patient-specific geometry (Chan et
al., 2013a).
Once again, the same group, Chan et al., 2013 reviewed computational approaches
(CFD/FSI) inside the heart with DCM. They noted that because of the limitations on the
imaging tools, CFD provides a better option for investigating and determining the entire

78
functionalities of the heart and its disease conditions. Moreover, from their discussions,
they noted that initial recognition of the diseases; enhancement of the assisting devices,
and other restorative features can be accelerated by using CFD analysis (Chan et al.,
2013b).
Mangual et al., 2013 studied the DCM affected LV flow pattern numerically compared
to the LV in the ideal condition. The computational approach was conducted by
combining the 3D echocardiographic technique and the equations for the flow
movement inside the LV. Results indicated that the flow pattern for the DCM-LV was
significantly different to that of the healthy LV in terms of the formation of vortices,
because those developed vortices were very weak in the enlarged DCM ventricle. Also,
the DCM and the healthy LV flow dynamics had differences in vortex-formation time
and energy dissipation. However, valvular effect, as well as the mitral and aortic valve
were neglected, and a limited frame rate for the 3D echocardiographic imaging was
utilized during the investigation (Mangual et al., 2013).
Table 2.3 summarizes the DCM conditions for the LV using both the experimental and
numerical approaches as enlisted from various references.
Table 2.3 Primary investigations on DCM Authors Methods Features Findings Limitations
Levisman,
1977
Echocardiography
and cardiac
catheterization
Observed the LV
conditions
including mitral
regurgitation (MR)
of 18 patients
6 patients were found
with minor or no
regurgitation and 12
patients with medium
or acute
Septal motion with
higher MR were not
visible using
echocardiography
Grossman et
al. 1979
Echocardiogram 8 patients with
severe congestive
heart failure due to
cardiomyopathy
LV relaxation rate in
the early diastolic
period decreased
Kutova et
al. 1981
Echocardiography 25 patients with
congestive
cardiomyopathy
and MR
Differences were
observed compared to
the usual
echocardiographic
results
Difficult to
discriminate between
the rheumatic mitral
deficiency and mitral
deficiency
Takenaka et Pulse Doppler 21 patients with LV diastolic Doppler LV indicators

79
al. 1986 echocardiography DCM and MR, 12
patients only with
DCM and 19
normal people
irregularities were
affected by MR in
DCM patients
were yet to be
determined clinically
Jacobs et al.
1990
Pulsed-wave and
colour Doppler
measurement
48 DCM patients
and 14 healthy
people
Delayed flow
propagation, from base
to apex was observed
in DCM patients
Vanoversch
elde et al.
1990
Pulsed wave
Doppler and M-
mode
echocardiography
34 patients with
DCM
LV filling was
influenced by left atrial
pressure (LAP) and
MR
Lack of invasive
assessment of LAP
Levin et al.
1996
Assisted with
LVAD for 183
days
19-year old patient
with DCM
LVAD was explanted
as the patient was
recovering
Patient died because of
heart failure
Gunja-Smith
et al. 1996
Human tissue
from the DCM-
hearts
Significance of
DCM in abundance
of collagen
Collagen increased two
times in ventricle wall
and four times overall
in amount
Coronary artery
dysfunction and other
infracted areas were
debarred
Loebe et al.
1997
Assisted with
LVAD
36 years-old DCM
patient
LVAD was explanted
when a donor was
found for heart-
transplantation
Hetzer et al.
1999
Observation of
VAD and/or
change of VAD
pumps after 26
months
19 patients (23-65
years) with end-
stage DCM
Overall 12 patients
were found recovering
and 7 patients died
To characterize the
patients who could be
able to recover their
normal functionalities
Baccani et
al. 2002
Numerical
simulation of
Navier-Stokes
equation
Flow pattern for the
normal and DCM
LV
thickness of the LV
wall increased, inflow
velocity decreased,
vortex stagnated much
longer
Flow pattern was
considered
axisymmetric and
mitral valve was
assumed fixed
Yotti et al.
2005
Colour Doppler
M-mode
recordings
40 DCM patients
and 20 healthy
people
Maximum DIVPD
(diastolic
intraventricular
pressure gradient and
difference) < 0.5 in
DCM patients
1-D Doppler trajectory
was assumed in Euler’s
equation and the error
was much higher

80
Cioffi et al.
2005
Colour Doppler 175 patients, aged >
70 years with
chronic heart failure
(CHF)
Negative correlation
between
MR and hospitalization
for deteriorating CHF
Patients with heart
valve diseases, severe
myocarditis and other
related diseases were
not considered
Maron et al.
2006
Detailed definitions and classifications of
primary and secondary cardiomyopathies
Correlation and
development molecular
genetics including the
ion channelopathies in
primary
cardiomyopathies
However,
channelopathies might
not provide suitable
explanation as
cardiomyopathies
(Elliott et al. 2007)
Elliott et al.
2007
Classified into morphological and
functional phenotypes and each of them
was sub-grouped into
familial and non-familial forms
Leaving and directing
the differences between
primary and secondary
cardiomyopathies into
more specific reasons
Limited to document
the causes of various
cardiomyopathies due
to similar genetic
metamorphosis genetic
Liden et al.
2007
Doppler
echocardio
graphy and
right heart
catheteriza
tion
15 patients with HeratMate
VE and 3 patients with
Jarvik 2000
Patients with acute
heart failure doubtful to
demonstrate substantial
cardiac recovery using
LVADs
The functionalities of
bridge to recovery for
the mechanical aiding
devices are unclassified
Loerakker et
al. 2008
Lumped
parameter
model and
a
computatio
nal model
of LV
Effect of LVAD on
vortices in normal and
DCM
Strength of primary
vortex in DCM is
lower than normal LV
Simplified LV chamber
Thomas et
al. 2009
Role of echocardiography in assessment
of DCM
Precise
pathophysiological data
can be obtained using
tissue-Doppler, strain
analysis and 3D
echocardiography
Capability and
reproducibility might
be a limiting factor for
tissue Doppler
Jefferies
and Towbin,
2010
Primary characteristics of DCM and its
effect in heart failure
Clinical characteristics,
genetics
and contributing
Stem-cell treatment for
end-stage DCM
resulted some

81
mechanisms,
diagnostic approaches,
treatments of
primary and secondary
DCM
controversies but it
was still in research
Chan et al.
2012
Geometry-
prescribed
and fluid
structure
interaction
(FSI)
simulation
To examine the flow
dynamics in DCM LV
during filling wave
Magnitude of the
intraventricular
vortices and
intraventricular
pressure gradient
reduced
Simplified LV
geometry
Chan et al.
2013
FSI
simulation
Sensitivity analysis
including the effect of
DCM inside the LV in
terms of the
intraventricular flow
pattern and change in wall
stress
Flow velocity notably
decreased with the rise
in the ventricle
stiffness
Simplified LV model
Chan et al.
2013
Review on the current diagnostic
approaches including the computational
simulations in DCM heart during diastole
and entire heart cycle
Computational
methods could play a
significant role to
detect early-stage
diseases
Generally assumptions
were considered during
computational
simulations
Zhang et al.
2013
Echocardio
graphy,
vector flow
mapping
51 patients having
coronary artery disease and
ejection fraction (EF)>
50%, 70 patients with 13
coronary disease and 57
DCM and EF< 50% and
62 normal people
Evolution of vortices
strongly correlated
with LV dimensions
and functionalities/
characteristics
3D intraventricular
flow data was taken
from the long axis due
to the effect of mitral
and aortic openings
Mangual et
al. 2013
3D
echocardio
graphy and
computatio
nal
approaches
20 normal people and 8
DCM patients
Generated vortices
were very weak in
DCM LV than normal
LV
Data was taken from
very few inhabitants
and the data on heart
valves were neglected
Hershberger
and
DCM characteristics and classifications,
primary reasons, diagnosis processes and

82
Morales,
2013
treatments
2.6 Summary
From the literature review it became evident that precise hemodynamic characteristics,
as well as the coupling between the fluid forces and the anatomical deformation of the
left ventricle, were imperative in the investigation of the cardiac diseases. However, the
literature revealed that evaluating and detecting such information in vivo had proven to
be highly complex. Moreover, no such research work was uncovered which could assist
patients having problems with an enlarged heart; driveline infections of VADs or other
cardiac diseases (e.g., dilated cardiomyopathy).
Hence, in this Doctoral research, an experimental work program was developed, based
on a cardiac assist device, which may ultimately be able to assist cardiomyopathy
patients and other patients whose heart muscles were weak and did not expand and
contract properly. At the time of compiling this dissertation, this assist device
development work was still in progress. However, with the assistance of undergraduate
students, it was possible to successfully demonstrate wireless expansion and contraction
(this is briefly documented in Chapter 7 and appendix).
In order to successfully complete the entire features of this cardiac assist device,
detailed numerical investigations, with realistic anatomical details, and complete
simulations of the left ventricle were espoused to evaluate the real data on the
hemodynamic forces including:
• Fluid and structural forces
• Wall shear
• Flow dynamics and vortex pattern
• Changes in the intraventricular pressure pattern inside the LV cavity
during the diastole condition.

83
The reviewed literature clearly suggested that numerous research efforts had been made
into the hemodynamic characteristics of the LV but a complete hemodynamic analysis
was still missing, both for the normal and diseased LV.
Therefore, this research aimed to simulate the hemodynamic forces by changing the
friction co-efficient and ventricular wall thickness during diastole. Also, the flow
patterns, changes in the intraventricular pressure, and the deformation of the LV wall,
were computed by varying the angles between the mitral and aortic orifice of the left
ventricle. This analysis provided substantial insights into the flow dynamics of the LV,
due to differences in cardiac structures and diseases. Also, the data arising from this
analysis would facilitate a greater focus in terms of a cardiac assist device.
It can be seen from the literature and the Tables 2.1, 2.2 and 2.3 that a simplified
geometry of the LV models was able to produce realistic results. One therefore
concludes that physiologically correct waveforms and realistic structures are the nuts
and bolts for effectively determining hemodynamic forces and flow dynamics inside the
LV. Moreover, a Fluid structure Interaction (FSI) tool had been utilized to analyse the
deformation and hemodynamic forces in many cases reported in the literature. Hence, in
this Doctoral research, during the numerical simulations, simplified and anatomically
correct LV geometry was used and the results were investigated and determined
accordingly using Fluid Structure Interaction (FSI) scheme. This is documented
throughout the remainder of this thesis.

84
Chapter 3
Numerical Experimentation of Coronary Artery
Bypass Graft and Abdominal Aortic Aneurysm
Model

85
3.1 Overview
The primary objective of the research processes documented in this chapter was to
become familiar with applications of the Fluid Structure Interaction (FSI) scheme.
Hence, two case studies were undertaken to develop knowledge in the field of FSI. The
case studies were performed by using three dimensional (3D) models of the:
• Coronary Artery Bypass Graft (CABG) with four different degree of stenosis:
o 0%
o 30%
o 50%
o 75%
• Abdominal Aortic Aneurysm (AAA)
During the case studies, the results were tabulated and analysed in terms of:
• Flow dynamics
• Wall shear stress (WSS)
• Deformation of the solid domain
In doing so, the results were compared and discussed in relation to previously published
results. During the simulations, suitable boundary conditions for both the solid domains
and fluid domains for both models were applied. Also, the Navier-Stokes equations and
the Arbitrary Lagrangian Eulerian (ALE) formulation were utilized to couple the fluid
and solid regions of the simulated models.
The work documented in this chapter was effective in developing knowledge in the
utilization of numerical techniques and also for quantitative and qualitative research in
the field of cardiology. Specifically, in relation to the objectives of this Doctoral
research, the analysis and discussion of these case studies proved to be highly useful in
performing the required FSI simulations on the Left Ventricle (LV) model, detailed in
Chapter 4 of this thesis.
Finally, this chapter concludes by specifying the significance and the utilization of FSI
and the lessons learned throughout the simulations.

86
3.2 Review of Literature pertaining to the Bypass Graft
The utilization of the Internal Thoracic Artery (ITA)/Internal Mammary Artery (IMA),
containing the Left Internal Thoracic Artery (LITA) - Left Anterior Descending (LAD)
anastomosis, elevates the rate of survival of patients in bypass surgery. The LITA in
Coronary Artery Bypass Grafting (CABG) is also extensively recognised due to its
exceptional and enduring patency rate (Ochi, 2006). The CABG procedure proved to be
very effective for re-establishing blood flow inside moderately or fully blocked arteries
(Kouhi, 2011).
The CABG procedure utilizes an autologous vein or any prosthetic channel/pipe
inserted into the closest/ proximal and remote/distal diseased segment of the artery, with
the target of restoring hemodynamics because of myocardial infarction. The parameters
for hemodynamic forces, such as wall shear stress (WSS), applied on the endothelial
cells, oscillatory shear index (OSI) and temporal and spatial wall shear stress gradients
(WSSG) are the most significant elements that can influence the patency rate of the
CABG. Nowadays, the most common operative approach for myocardial
revascularization involves an ITA connected with one or more Saphenous Vein Grafts
(SVG). To elevate the rate of survival of patients, an unobstructed LAD coronary artery,
including ITA, is required for surgery (Mohr and Kramer, 2006, Otaki et al., 1994,
Swillens et al., 2012, Kouhi, 2011, Kouhi et al., 2008).
Hemodynamic investigations of the CABG had been studied by using Computational
Fluid Dynamics (CFD) methods and also by utilizing experimental and imaging
techniques (Freshwater IJ, 2006, Owida et al., 2010, Zhang et al., 2008). These
methods/techniques require successful detections of various features, such as:
• Blood flow fields
• Wall shear stress and gradients
• Deformation of the artery and graft junction incorporating the degree of
compliance divergence
87
All these features were broadly investigated and analysed by (Kouhi et al., 2008,
Freshwater IJ, 2006, Do, 2012).
The CFD technique was also used by Ethier et al., 1998 and the authors concluded that
low and oscillatory WSS areas were the most crucial positions for Intimal Hyperplasia
(IH) and were repeatedly seen in distal anastomosis (Ethier et al., 1998). Also,
Goubertis et al., 2001 determined the impact of the lower WSS area in graft-failure
inside a saphenous vein, including varicose saphenous veins by employing CFD
(Goubergrits et al., 2001).
In another study, Freshwater et al., 2006, studied the significance of anastomotic angles
(20˚, 40˚ and 60˚) on flow dynamics and WSS distribution of the LIMA-LAD bypass
graft. The CFD method was used for the simulations and the authors concluded that
both the 60˚ (high) and 20˚ (low) anatomosis angles were linked to elevate flow
disturbance which might be responsible for crucial development of IH (Freshwater IJ,
2006). Moreover, Sankarnarayan et al., 2006, studied the flow dynamics inside a CABG
(out-of-plane) by utilizing CFD and they found a substantial effect which could affect
the graft patency. However, during the simulation, elasticity/flexibility of the wall and
the non-Newtonian flow properties, were neglected (Sankaranarayanan et al., 2006).
Siddique et al., 2009, examined the influence of the non-Newtonian characteristics of
the blood and pulsatality on the flow pattern of an artery comprising stenosis (Siddiqui
et al., 2009).
Subsequently, a large volume of numerical and experimental investigations of CABG
have been documented, mainly in the flow dynamics and the inflexible arterial wall, due
to the complexity of coupled fluid-structure deformation (Zarins et al., 1983, Taylor et
al., 1998, Deplano and Siouffi, 1999, Bertolotti and Deplano, 2000, Bertolotti et al.,
2001, Cole et al., 2002, Politis et al., 2008). However, this postulation was only suitable
for those states where the deformation of the structure did not affect the flow dynamics
(Kouhi, 2011, Perktold and Rappitsch, 1995). Moreover, the flow pattern and wall shear
stress in the end-to-side and side-to-side anastomosis of the CABG were studied by
Frauenfelder et al., 2007. Although the authors considered patient-specific data, the
simulations were carried out only for two patients, which somewhat restricted the

88
impact of clinical outcomes (Frauenfelder et al., 2007). Later, Nordgaard et al., 2010,
analyzed the influence of the competitive flow on WSS inside the LIMA-LAD porcine
model. They concluded that the flow pattern in the graft was particularly reliant/
dependent on the degree/scale of competitive flow. However, they utilized a simplified
geometry and boundary conditions for the simulations (Nordgaard et al., 2010).
Swillens et al., 2012, in a similar LIMA-LAD model, which was extracted from a pig,
studied hemodynamic influences, including the WSS and pressure at the distal area of
the LAD by varying the degree of LAD-stenosis. Although they concluded that a lower
degree of LAD-stenosis was connected with higher competitive flow and lower WSS in
the LIMA, they only considered simplified boundary conditions during the simulations
(Swillens et al., 2012). Also, Berger et al., 2004, studied the influence of lifelong
patency of the IMA tubes with clinical and angiographic data/statistics. There were
some limitations on obtaining related patient data but the findings indicated that the
lifelong patency rate of IMA grafts was minimum when the patient’s vessel/tube was
somewhat stenosed (Berger et al., 2004). Moreover, Sankaran et al., 2012, simulated the
flow pattern of a patient-specific CABG model using an implicitly coupled multiscale
structure to execute CFD simulations. During the simulations, the inflexible walls of the
structure were considered (Sankaran et al., 2012).
In another study, Morsi et al., 2012, demonstrated the directional movement of the
arterial wall of the CABG, along with its maximum deformation, by using FSI during
one cardiac cycle. For the simulations the authors considered the CABG with 20˚
anatomosis angle and graft-artery ratio of 1.6. The findings suggested that the simulated
data could be very effective for graft designers and/or surgeons/doctors, including the
selection of different bio-materials for the grafts. For the simulation, the authors
emphasized the use of FSI to determine the deformation of the structure, which could
influence the overall results (Morsi et al., 2012). In the same year, Kabinejadian and
Ghista, 2012, introduced an innovative design for the CABG which comprises the
coupled end-to-side and side-to-side anastomoses. The design offered effective flow
dynamics and WSS distributions when compared with the regular end-to-side
anatomosis. For the simulation, a two-way FSI technique had been utilized. However,

89
during the simulation, cardiac motion was not considered (Kabinejadian and Ghista,
2012).
Consequently Ding et al., 2012 investigated the influence of the flow dynamics in an
ITA-LAD bypass graft comprising various degree of LAD-stenosis using CFD. From
the analysis, the authors demonstrated that a bypass graft surgery might be required
when the degree of LAD-stenosis was found to be more than 75%. However during the
simulation, proper physiological and hemodynamic parameters were discarded (Ding et
al., 2012). Subsequently, Lassila et al., 2013, examined the inverse complications which
arose in the flow dynamics of a bypass graft (Lassila et al., 2013). Also, Sabik et al.,
2013, investigated the influence of the re-operative CABG of the LITA-LAD graft and
they stated that re-operative LITA-LAD bypass grafting was low risk. However, during
the study they did not incorporated angiographic patency data (Sabik et al., 2013).
The above mentioned investigations focused on the general flow dynamics inside the
CABG with varying degree of success. However, a complete analysis of the
hemodynamic forces and physiological variations of the model, which also
encompasses the relationship between the degrees of LAD-stenosis (0% or no stenosis,
30%, 50% and 75% stenosis) in the ITA-LAD bypass graft, was not thoroughly
covered.
For these reasons, in Section 3.3, the hemodynamic forces are described in terms of:
• Velocity distributions
• WSS distributions
• Structural displacement of the bypass graft model
with the correlation between the various degrees of LAD-stenosis in the ITA-LAD
bypass graft under different physiological conditions. In doing so, Arbitrary Lagrangian
Eulerian (ALE) equations were utilized for the FSI analysis of the 3D non-linear,
realistic bypass graft model.

90
3.3 Mathematical Procedure, Solver and Output Settings
The ANSYS software system was deployed to derive the fundamental solutions of the
3D time-dependent equations, which were based on the finite volume method and
various coupled iterative solver equations. The general conditions of the flow related
problems were computed by the exploitation of the principles of the conservation of
mass equations, momentum equations and energy equations. All the primary/governing
equations were mathematically discreted based on finite element methods. Also, during
the simulation, the Navier-Stokes equations were utilized in the simulation for the time-
dependent and incompressible viscous fluids, which were coupled with the continuity
equation, as per (Temam, 2001, Arefin and Morsi, 2014, Do, 2012, de Vecchi et al.,
2014, Pierrakos and Vlachos, 2006):
(3.1)
Equation of momentum:
(3.2)
Subsequently, the kinetic energy (Ek(t)), at an instant time (t):
( ) ( ) ( ) d 2
tk Ω⋅= ∫Ω
tvtvE ρ (3.3)
Viscous energy (Ev(t)), at an instant time (t):
( ) (3.4) dt d : t xT
v Ω∇∇= ∫∫Ω
ννµ xE
Where:
• ρ is the density of the fluid density.
0ˆ =∇⋅−⋅∇+∂∂ ρρ uU
t
( ) gSUuUut
U ρ+⋅∇=∇⋅−⊗⋅∇+∂∂ ˆ

91
• U and S denote the momentum and the Cauchy stress tensor respectively.
• g represents the gravity vector, u denotes the velocity vector; is the mesh
velocity vector.
• µ denotes the viscosity, v represents the velocity of the blood and Ω denotes the
antisymmetric sections of the velocity gradient tensor for the centre of the
vortex.
More details can be found in (Krittian et al., 2010, Tay et al., 2011). Moreover, the
energy transfer characteristics of the flow dynamics inside the cavity can be determined
further by utilizing work-energy equation, which were comprehensively analysed in
(Khalafvand, 2013, Hung et al., 2008). Consequently, the equation of motion for
displacement, utilized for elastics in the solid domain (Fluent, 2013, Arefin and Morsi,
2014):
(3.5) 0 f =+⋅∇ σ
Where, σ and f represent the stress tensor and the body force respectively.
Subsequently, by assuming insignificant deformation, the stress tensor equation is
characterized as (Fluent, 2013, Arefin and Morsi, 2014):
(3.6) I )T-(T 2-1
E - )I ) tr(2-1v(
1E 0α
υεε
υυσ +
+=
Where
• E represents the Young’s modulus.
• υ denotes the Poisson’s ratio.
• T is the temperature.
• T0 represents the reference temperature and T=T0.
• I denotes the unit tensor.
In this investigation, the Arbitrary Lagrangian Eulerian (ALE) finite element based
approach was adapted for the viscous fluid, which is non-linear, on a large surface wave
function. Subsequently, when the ALE method was compared to its Eulerian
u

92
equivalents it provided complete solution correctness for structures which could deform
and contain fluid. The detailed description on ALE, based on the Navier-Stoke equation,
was based on the information provided in (Huerta and Liu, 1998, Donea et al., 2004,
Temam, 2001, Souli et al., 2000, Arefin and Morsi, 2014).
The flow chart of Figure 3.1 shows that convergence occurs for the unidirectional FSI
approach for the conditions provided in the simulation. The algorithm of Semi-Implicit
Method of Pressure Linked Equations (SIMPLE) was used here to determine the
equations of mass and momentum. This flow chart was applicable until convergence of
the simulation occurred (Lemmon and Yoganathan, 2000, Patankar and Spalding, 1972,
Arefin and Morsi, 2014, Owida et al., 2012).

93
Structure Displacement
Forces
No
Yes
No
Yes
Figure 3.1 Illustration of the flow chart utilized during the entire simulation
procedure (Arefin and Morsi, 2014, Owida et al., 2012)
ANSYS 14.5 was utilized for the entire simulation, where the following approaches
were followed:
• Initially, all the required boundary conditions were provided.
• Subsequently, suitable meshing was employed.
• A coupling procedure was selected.
Start
FSI Simulation
ANSYS Structural
Solver
ANSYS Fluid
Solver
Solution
Converged?
Solution Complete?
Result Analysis

94
3.4 Case Study I: ITA-LAD Bypass Graft
3.4.1 Geometry
The 3D cross-sectional model of the ITA-LAD bypass graft, created using SolidWorks
2012, is demonstrated in Figure 3.2 (a), which characterizes the ideal human
anastomosis of the bypass graft. Figure 3.2 (b) demonstrates the detailed measurements
of the bypass graft using similar CAD (Computer-Aided Design) software. The
following parameters were used in modelling:
• The length of the native stenosed LAD coronary artery was taken to be 134 mm
with a diameter of 4 mm.
• The anastomosis angle was taken to be 45°, and the stenosis was assumed to be
located at 25.67 mm from the anastomosis angle.
• The length of the anastomosed ITA was considered to be 67.59 mm on the
longer side of the ITA, rear to the anastomosis angle and 61.19 mm close to the
anastomosis angle.
• The diameter of the ITA was taken to be 4.40 mm.
• The length of the stenosed LAD, starting from the diameter to the anastomosis
region, was taken to be 38.47 mm.
• The vessel thickness of the bypass graft was considered to be 1mm.
All the parameters closely matched those in the models of (Ding et al., 2012, Kouhi,
2011).

95
(a)
(b)
Figure 3.2 Cross sectional view of the ITA-LAD bypass graft (75% LAD-stenosis) (a):
Ideal 3D model (SolidWorks 2012) (b): The model utilized in simulations (SolidWorks
2012)

96
3.4.2 Meshing Configurations and Mesh Independency Testing
The CAD model of the bypass graft was imported/ transferred to ANSYS 14.5, where
the meshing was executed and the obligatory boundary conditions were applied. For the
meshing, "Mapped Face Meshing" was performed separately for both the solid and fluid
regions of the structure. Also, line control properties were utilized to determine the
discrepancies in the fluid velocity. Subsequently, a mesh independency test was
executed by utilizing these line control properties, where the differences in the flow
velocity were compared for successive nodes and elements (Kouhi, 2011). The changes
in the flow velocity were determined until convergence.
Figure 3.3 demonstrates the mesh independency test based on the variations in the fluid
velocity. Four different mesh types (coarse, medium and fine and coarse refinement)
were selected and changed during the simulations. It was validated that 22289 nodes
and 11546 elements were considered to be suitable for the solid region, and 18355
nodes and 85966 elements for the fluid region. Also, during the simulation, all these
nodes and elements were obtained from the medium mesh type. Moreover, the
convergence criterion for the fluid flow was considered to be 10-4 and 10-2 for the
coupling data transfer.

97
Figure 3.3 Meshing independency testing
3.4.3 Required Boundary Conditions
Boundary conditions are one of the preliminary conditions for executing the desired
simulations. Therefore, for this simulation, initially the flow velocity was provided at
the inlet region of the ITA and LAD. These blood flow velocity profiles were obtained
from in vivo trials/testing of 18 pigs, as reported in (Ding et al., 2012).The flow profiles
were categorized into four different inlet velocities according to various levels of LAD-
stenosis, specifically:
• 0%
• 30%
• 50%
• 75%.
Figure 3.4 demonstrates the flow profiles for various degrees of stenosis in the ITA-
LAD bypass graft. For the four different types of inlet velocities, the X-axis represents
the time (t) in seconds and Y-axis represents the velocity in m/s. A curve-fitting
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0 0.05 0.1 0.15
Velo
city
[m/s
]
Z [m]
Mesh Type-Coarse
Mesh Type-Medium
Mesh Type-Fine
Mesh Type-CoarseRefinement

98
technique was utilized to obtain these inlet velocities from the velocities provided in
(Ding et al., 2012). All the velocities were in line with the reported velocities from Ding
et al., 2012, except for the LAD 50%, due to the variations in the original one. The total
time duration for the simulation was taken to be 0.8 s (Ding et al., 2012).
Figure 3.4 Inlet velocities for the ITA-LAD bypass graft (Ding et al., 2012)

99
Subsequently (Ding et al., 2012, Lassila et al., 2012, Kouhi, 2011),
• Once the inlet velocities were provided in the bypass graft, the density and the
viscosity of the fluid were provided with the value of 1050 kg/m3 and 0.0035
Pa•s respectively.
• The arterial wall was considered to be isotropic and homogeneous with a
Poisson’s ratio of 0.49.
• Newtonian fluid flow was considered during the simulations, including the no-
slip boundary conditions.
• The flow was considered to be laminar.
• Relative pressure in the outlet was set to 0 Pa and the circumferential faces in
the inlets and outlet were fixed.
• For the coupling data transfer control, under relaxation factor was set to 0.75.
• A Cylindrical Support on the CABG (except the toe and heel) was employed,
where only the tangential direction was considered fixed and the radial and
axial directions were considered free. This was due to higher variations in the
inlet velocities.
Young’s Modulus, was obtained from the following equation (Olufsen, 1999, Kouhi,
2011):
𝐸ℎ𝑟0
= 𝑘1 × 𝑒𝑥𝑝(𝑘2𝑟0) + 𝑘3 (3.7)
Where,
• r0 denoted the diameter of the artery (distal area)
• h denoted the wall thickness
• 𝑘1 = 2 × 107 𝑔 𝑠2. 𝑐𝑚⁄
• 𝑘2 = −22.53 𝑐𝑚−1
• 𝑘3 = 8.652 × 105 𝑔 𝑠2. 𝑐𝑚⁄

100
Moreover, it is to be noted that blood’s rheological model usually differ from person to
person and therefore it is not possible to incorporate all the required parameters which
are associated in a model. Reynolds number is one such parameter which is generally
utilized in determining the influence of the turbulence of the flow dynamics. Reynolds
number can be determined using (Do, 2012, Vimmr and Jonášová, 2010):
𝑅𝑒 = 𝜌𝑉𝐷𝐻𝜇
(3.8)
Where,
• Re denoted the Reynolds number
• ρ denoted the density (kg/m3) of the fluid
• μ represented the dynamic viscosity (kg/m.s) of the fluid
• DH was the hydraulic diameter (m2)
• V denoted the mean velocity of the fluid (m/s)
3.4.4 Simulation Results
3.4.4.1 Velocity Distributions
The results are presented in terms of velocity distributions, including:
• The generation of vortices inside the artery
• Wall shear stress (WSS) distributions
• Structural displacement by using total mesh displacement (TMD)
for four different degree of LAD-stenosis in the ITA-LAD bypass graft.
Figures in 3.5 demonstrate the flow dynamics inside the ITA-LAD bypass for different
flow patterns of the LAD-stenosis (0%, 30%, 50% and 75%) in four different time

101
steps. Velocity mapping was utilized to characterize the discrepancies in the flow
distributions, which were mapped on the YZ cross-sectional plane of the bypass graft.
This cross-sectional plane was employed in the middle of the bypass graft structure,
where the plane contained the inlet regions of the ITA and the LAD, incorporating the
anastomosis and the distal LAD (Ding et al., 2012).
Apparently, because of various inlet flow velocities for different degree of LAD-
stenosis, discrepancies in the flow pattern were observed inside the bypass graft.
Subsequently, with the elevation in the degree of LAD-stenosis, the magnitude of the
inflow wave decelerated in the proximal area of the LAD but increased in the ITA
(Ding et al., 2012). Table 3.1 summarizes the observations from the results.
0.05s
0.3 s

102
0.55 s
0.75 s
(a) 0% LAD-stenosis
0.05 s
0.3 s
LAD-stenosis
LAD-stenosis

103
0.55 s
0.75 s
(b) 30% LAD-stenosis
0.05 s
0.3 s
LAD-stenosis
LAD-stenosis
LAD-stenosis
LAD-stenosis

104
0.55 s
0.75 s
(c) 50% LAD-stenosis
0.05 s
0.3 s
LAD-stenosis
Stagnation
LAD-stenosis Stagnation
LAD-stenosis
LAD-stenosis

105
0.55 s
0.75 s
(d) 75% LAD-stenosis Figure 3.5 Velocity mapping of the ITA-LAD bypass graft for the (a) 0%, (b) 30%, (c)
50% and (d) 75%LAD-stenosis
Table 3.1 Observations pertaining to figure 3.5
% Stenosis Observations 0% Reverse-flow/flow separation into the graft artery was evident during the flow pattern.
During the time step of t= 0.05 s, the magnitudes of the velocity through the ITA and
LAD region are 0 m/s and around 0.23 m/s respectively. During this time step, a
reverse flow was observed through the ITA region. Subsequently, the rate of flow
through the ITA and LAD was found to be in the forward direction during the time step
of 0.3 s. With the progression of the time step, t= 0.55 s the magnitude of the velocity
for the ITA increased to approximately 0.19 m/s and with the incoming jet from the
proximal LAD, maximum magnitude of velocity around 6.69E-1 m/s was found to be
close to the anastomosis angle in the distal LAD region. Once again, with the
deceleration in the inlet velocity through the ITA (around -0.18 m/s) and LAD region
(around 0.22 m/s), a reverse flow is observed in the ITA region. Consequently, the
magnitude of the flow velocity reduces through the distal LAD region of the host
artery.
LAD-stenosis
Stagnation
LAD-stenosis
Stagnation

106
30% During the time step of t= 0.05 s the magnitudes of the inlet jet velocity were found to
be around 0.15 m/s and 0.13 m/s through the ITA and LAD region accordingly. Due to
the stenosis in the proximal LAD of the host artery, a slight disturbance in the general
flow pattern was observed near the anatomosis region close to the heel but the direction
of the flow pattern was found to be forward. A disturbance in the flow was also
observed close to the heel during the time step of t= 0.3 s. During the time step of t=
0.55 s the magnitude of the inlet velocity through the ITA increased to approximately
0.225 m/s and maximum flow velocity of around 6.69E-1 m/s was found to be just
beside the anastomosis region of the distal LAD region. During the time step of t= 0.75
s the magnitude of the velocity of the ITA, with a value of around 0.22 m/s, was found
to be higher than the velocity of the LAD, with a value of around 0.12 m/s. Hence, the
magnitude of the velocity was found to be slightly higher close to the arterial wall of
the host artery with a value of around 4.46E-1 m/s, but the magnitude was lower
compared to the previous time step (t= 0.55 s).
50% The magnitude of the velocity through the ITA and LAD were found to be around 0.13
m/s and 0.031 m/s accordingly during the time step of t= 0.05 s. With the increase in
the degree of the stenosis in the proximal LAD region, the magnitude of the flow
velocity through the LAD region decreased and a disturbance in the anastomosis angle
of the bypass was observed with the time step of t= 0.05 s. Also, with the time step t=
0.3 s, the rate of flow somewhat increased through the ITA and decelerated through the
LAD region. Therefore, the rate of flow was found to be forward through the inlet of
the ITA region. Again, with the elevation in the inlet velocity through the ITA
(approximately 0.42 m/s) compared to the LAD velocity of around 0.04 m/s during the
time step of t= 0.55 s, maximum magnitude of the flow velocity was found to be
around 7.33E-1 m/s close to the arterial wall of the distal LAD region. However, with
the deceleration in the ITA velocity (around 0.2 m/s) during the time step of t= 0.75 s,
a disturbance in the flow pattern near the anastomosis angle was observed,
incorporating the re-circulation/ formation of ring shaped vortex close to the vicinity of
the anatomosis region of the arterial wall.
75% An inlet velocity of around 0.021 m/s for the 75% LAD-stenosis and a very weak ring
shaped vortex was seen developed near the vicinity of the anastomosis region of the
artery wall. Simultaneously, a higher flow rate was observed through the ITA region
and through the distal LAD region of the host artery. Also, due to the higher flow rate
through the ITA region, the direction of the rate of flow was found to be forward
towards the outlet region. Moreover, a small ring-shaped and clockwise (CW) vortex
was found to be developed close to the arterial wall in the anastomosis region.

107
Subsequently, with a rise in the inflow velocity through the ITA, with a magnitude of
around 0.52 m/s, maximum flow velocity with a value of approximately 8.92E-1 m/s
was found to be close to the arterial wall of the distal LAD. Later, with the time step t=
0.75 s, the magnitude of the inlet velocity through the ITA decelerated (approximately
0.25 m/s) and hence, a disturbance in the flow pattern near the anastomosis angle was
observed, where a strong ring shaped vortex was formed in the vicinity of the artery
wall in the anastomosis region.
3.4.4.2 Wall Shear Stress (WSS) Distributions
Figure 3.6 illustrates the variations of the wall shear stress (WSS) inside the bypass
graft for different levels of LAD-stenosis (0%, 30%, 50% and 75%) during a cardiac
cycle. It was decided that the effect of the wall motion, during a cardiac cycle for
various LAD-stenosis levels should be investigated. In so doing, WSS was considered
on the outer surface of the bypass graft. Also, the required boundary conditions were
implemented and the inlet velocities through the ITA and LAD were provided (Figure
3.4). Additionally, spatial WSS distributions are documented in Section 3.4.4.3. Table
3.2 summarizes the observations.
0.05 s

108
0.3 s
0.55 s
0.75 s
(a) 0% LAD-stenosis
0.05 s

109
0.3 s
0.55 s
0.75 s
(b) 30% LAD-stenosis
0.05 s

110
0.3 s
0.55 s
0.75 s
(c) 50% LAD-stenosis
0.05 s

111
0.3 s
0.55 s
0.75 s
(d) 75% LAD-stenosis Figure 3.6 Distributions of WSS for different degrees of LAD-stenosis (0%, 30%, 50%
and 75%)
Table 3.2 Observations pertaining to figure 3.6
% Stenosis Observations 0% The magnitude of the WSS was found to be slightly higher close to the inlet region of
the proximal LAD and close to the toe (t= 0.05 s). This can be explained with the higher
magnitude of inlet velocity through the LAD region compared to its ITA region, hence a
somewhat higher magnitude of WSS could be found in the LAD region. Later, during
the time step of t= 0.3 s, a slightly higher magnitude of WSS was found in the distal

112
LAD but comparatively lower magnitude of WSS both in the ITA and LAD region.
Once again, during the time step of t= 0.55 s, the magnitude of the inlet velocity through
the ITA elevated and hence higher magnitude of WSS with the value of around 7.9 Pa
could be found in the distal LAD region. Afterwards with the time step of t= 0.75 s, the
magnitude of the inlet velocities through the ITA and LAD regions decreased and hence
the influence of the WSS was found to be lower again compared with the previous time
step of t= 0.55 s.
30% A lower magnitude of inlet velocity entered through the ITA and LAD region during the
time step of t= 0.05 s. At that time, a slightly higher magnitude of WSS was found to be
near the toe of the bypass graft. Once again, during the time step of t= 0.3 s, the
magnitude of the inlet velocity decelerated and hence a lower magnitude of the WSS was
seen on the bypass graft. Later during the time step t= 0.55 s, the magnitude of the WSS
was found to be moderately higher on the distal LAD due to higher inlet velocity
through the ITA and LAD region. Also, a maximum magnitude of around 6.32 Pa was
found to be close to the toe of the bypass graft. After that with the progression in the
time step to t= 0.75 s, a higher magnitude of WSS was still found to be near the toe due
to the inlet velocity through the ITA region.
50% Due to the minimal inlet velocity through the inlet regions of the ITA and LAD during
the time step of t= 0.05 s, a lower magnitude of WSS was found to be both on the ITA
and proximal LAD, but slightly higher magnitude of WSS was found to be on the distal
LAD. During the time step of t= 0.3 s, the magnitude of the inlet velocity through the
ITA accelerated and through LAD it decelerated. Hence, the magnitude of the WSS was
found to be moderately higher in the ITA region compared to its LAD region. Later on,
the magnitude of the WSS was found to be much higher on the ITA, anastomosis region
and on the distal LAD during the time step of t=0.55 s. This could be attributed to the
fact that due to a much higher inlet velocity through the ITA, the magnitude of the WSS
elevated and simultaneously, it increased on the anastomosis region and on host artery. It
is noteworthy that the maximum magnitude of WSS was found to be around 1.58E1 Pa
on the toe close to the anastomosis region. During the time step of t= 0.75 s, the
magnitude of the WSS on the inlet region of the ITA and distal LAD decreased due to
much lower input velocity wave from the ITA region compared to its previous time step
of t= 0.55 s.
75% During the time step of t= 0.05 s, the magnitude of the WSS on the ITA was moderately
higher than its proximal LAD, due to a lower magnitude of the inlet velocity. Later, with
the increase in velocity of the ITA and decrease in the LAD region (t= 0.3 s), the
magnitude of the WSS on the ITA region was somewhat higher compared to its LAD
region. With the time step of t= 0.55 s, the flow rate through the ITA region increased

113
even more, which resulted the elevation in the magnitude of the WSS on the ITA region,
anastomosis region and on the distal LAD. Specifically, maximum magnitude of around
1.42E1 Pa was found to be near the anastomosis region on the distal LAD. Also, at the
same time step, the magnitude of the inflow velocity through the LAD region increased
but it was minimal. Once again, during the time step of t= 0.75 s, the magnitude of the
inlet velocity through the ITA and LAD region decelerated and therefore the magnitude
of the WSS on the graft artery and on the distal LAD including the anastomosis region
also decreased.
3.4.4.3 Spatial Wall Shear Stress (WSS) Distributions
In addition to the variations of the WSS distributions during different time steps of a
cardiac cycle, as reported in Section 3.4.4.2, three specific locations of the bypass graft
were considered to further analyse the discrepancies of the WSS distributions. In order
to characterize the spatial WSS distributions of the bypass graft for different degrees of
LAD-stenosis, three lines (line A, line B and line C) were chosen to investigate the
significance of the WSS during a cardiac cycle. Figure 3.7 represents the lines on the
bypass graft for spatial WSS distributions and Figure 3.8 demonstrates the variations of
WSS using Line A (toe), Line B (heel) and Line C (bed) for all stenosis levels (30%,
50% and 75%) and the no stenosis cases. The observations are summarized in Table 3.3.
Figure 3.7 Spatial WSS distributions using Line A, Line B and line C

114
(i) Line A
(ii) Line B
(iii) Line C
0
1
2
3
4
5
6
7
8
0.07 0.075 0.08 0.085 0.09
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0.09 0.095 0.1 0.105 0.11
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s
0
0.5
1
1.5
2
2.5
3
3.5
4
0 0.05 0.1 0.15
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s

115
(a) 0% LAD-stenosis
(i) Line A (30%)
(ii) Line B (30%)
(iii) Line C (30%)
(b) 30% LAD-stenosis
0
1
2
3
4
5
6
0.07 0.075 0.08 0.085 0.09
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s
0
0.5
1
1.5
2
2.5
0.09 0.095 0.1 0.105 0.11
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s
0
0.5
1
1.5
2
2.5
3
3.5
0 0.05 0.1 0.15
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s

116
(i) Line A (50%)
(ii) Line B (50%)
(iii) Line C (50%)
(c) 50% LAD-stenosis
-2
0
2
4
6
8
10
0.07 0.075 0.08 0.085 0.09
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s
0
0.1
0.2
0.3
0.4
0.5
0.6
0.09 0.095 0.1 0.105 0.11
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s
-2
0
2
4
6
8
10
12
0 0.05 0.1 0.15
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s

117
(i) Line A (75%)
(ii) Line B (75%)
(iii) Line C (75%)
(d) 75% LAD-stenosis
Figure 3.8 Spatial WSS distributions of Line A, Line B and Line C for (a) 0% (b) 30%
(c) 50% and (d) 75% LAD-stenosis
-2
0
2
4
6
8
10
12
0.07 0.075 0.08 0.085 0.09
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s
00.05
0.10.15
0.20.25
0.30.35
0.40.45
0.09 0.095 0.1 0.105 0.11
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s
-2
0
2
4
6
8
10
12
0 0.05 0.1 0.15
WSS
[Pa]
Z [m]
0.05 s
0.3 s
0.55 s
0.75 s

118
Table 3.3 Observations pertaining to figure 3.8
% Stenosis Observations 0% A maximum magnitude of approximately 6.8 Pa, during the time step of t= 0.55 s, was
obtained from the line A or toe of the bypass graft. Once again, this was due to the
higher inlet flow velocity through the ITA and LAD. Specifically for this no-stenosis
case during this time step, a higher flow rate entered through the proximal LAD and with
the mixture of the flow velocity coming from the ITA. Overall, from the graphical
representation of line A, due to the variations in the inlet velocities through the ITA and
LAD region, a higher magnitude of WSS was found to be on the toe of the bypass graft.
Subsequently, due to lower inlet velocity, WSS decreased. Similarly, from line B, a
maximum magnitude of 4.1 Pa was found to be on the heel of the bypass graft during the
time step of t= 0.55 s due to the higher flow rate from the inlets. However, during the
time step of t= 0.3 s, a much lower magnitude of WSS could be found on line B. From
line C, a maximum magnitude of the WSS of approximately 3.75 Pa (t= 0.55 s) was
found to be near the anastomosis region on the bed of the bypass graft. Also, during the
time step of t= 0.75 s the WSS was found to be lowest near the anastomosis region of the
bed.
30% A maximum magnitude of approximately 5.4 Pa during the time step of t= 0.55 s was
found to be on the toe (line A) of the bypass graft. Once more, higher magnitudes of
inlet flow velocities elevated the magnitude of the WSS on the toe. Also during the time
step of t= 0.3 s, with minimal inlet velocity, the magnitude of the WSS decreased (line
A). Likewise for line B, a maximum magnitude of WSS was found to be around 2 Pa
during the time step of t= 0.55 s on the heel of the bypass graft. This was due to the
higher inflow velocity through the inlets. Conversely, with the decrease in the inlet wave
WSS decelerated. Moreover, due to the higher inlet flow velocity during the time step of
t= 0.55 s, a maximum magnitude of 3.1 Pa was found to be near the anastomosis region
of the bed (line C). Also from line C it was evident that due to the 30% stenosis inside
the proximal LAD, the inlet flow velocity was hindered and specifically, during the time
step of t= 0.3 s, a lower magnitude of WSS was observed on the bed due to minimal inlet
flow velocity.
50% From line A, a much higher magnitude of the WSS with a value of approximately 9 Pa
could be found during the time step of t= 0.55 s on the toe of the bypass graft. With the
increased degree of stenosis, the overall flow rate through the LAD region minimized
and due to higher inlet flow velocity through the ITA region, maximum magnitude was
obtained on the toe of the artery. Similarly, from line B, a maximum magnitude of WSS
(0.55 Pa) was found to be on the heel during the time step of t= 0.55 s due to higher

119
inflow velocity. Also, from line C, during the time step of t= 0.55 s, a significant
elevation in the magnitude of the WSS with a value of around 11 Pa was found to be on
the bed of the artery near the anastomosis region. This can be ascribed to the fact that,
because of much higher inlet flow velocity during this time step, a maximum magnitude
of WSS was found to be on the anastomosis region. Also, due to lower inflow velocity
(t= 0.05 s) the magnitude of the WSS was found to be lowest.
75% Once again, a maximum magnitude of approximately 10 Pa (t= 0.55 s) was found to be
on the toe (line A) because of the higher inlet flow velocity, especially from ITA region.
Also, with the deceleration in the inlet flow velocity the magnitude of the WSS
decreased. Likewise, from line B, a maximum magnitude of approximately 0.41 Pa was
found to be near the heel of the proximal LAD during the time step of t= 0.55 s. Once
more, on the bed of the artery, a maximum magnitude of around 10.8 Pa was found
during the time step of t= 0.55 s. Also, with the deceleration in the inlet wave and due to
the stenosis inside the proximal LAD, the lowest magnitude of WSS was found to be on
the bed during the time step of t= 0.05 s.
3.4.4.4 Structure Simulation using Total Mesh Displacement (TMD)
The images in Figure 3.9 demonstrate the changes in the displacement of the bypass
graft for different degrees of LAD-stenosis (0%, 30%, 50% and 75%) for three different
time steps. Table 3.4 summarizes the observations. Variations in the displacement of the
structure for different degrees of LAD-stenosis were determined using TMD. Similar
boundary conditions and inlet waveforms (Figure 3.4), which are primarily employed
for the velocity mapping and WSS distributions were used. The changes in the
magnitude of the TMD were observed on the outer surface of the bypass graft. Also, an
XY plane was selected with a distance of 0.0913175 m in the Z-direction of the
anastomosis region, so that the discrepancies due to different inlet velocity waveforms
were mapped on this plane.

120
0.3 s
0.55 s
0.75 s
(a) 0% LAD-stenosis
0.3 s

121
0.55 s
0.75 s
(b) 30% LAD-stenosis
0.3 s
0.55 s

122
0.75 s
(c) 50% LAD-stenosis
0.3 s
0.55 s
0.75 s
(d) 75% LAD-stenosis Figure 3.9 Structure simulation using total mesh displacement (TMD) for (a) 0% (b)
30% (c) 50% and (d) 75% LAD-stenosis

123
Table 3.4 Observations pertaining to figure 3.9
% Stenosis Observations 0% With the propagation of the fluid inside the bypass graft through the ITA and proximal
LAD, the magnitude of the displacement varied accordingly. During the time step of t=
0.3 s for 0% or no-stenosis, a much higher magnitude of displacement could be found on
the distal LAD. However, the changes in the displacement of the ITA and proximal LAD
were minimal due to minimal inlet flow velocity. During the time step of t= 0.55 s a
maximum magnitude of around 6.25E-6 m could be found on the distal LAD close to the
outlet region. From the XY plane, a slightly higher magnitude of displacement could be
found on the LAD region compared to its ITA. During the time step of t= 0.75 s the
magnitude of the displacement on the bypass graft was found to be minimal because of
lower inflow velocity through the inlets.
30% A much higher magnitude of displacement was found to be on the distal LAD and heel
of the bypass graft during the time step of t= 0.3 s. Moreover, with the time step of t=
0.55 s the magnitude of the inlet velocity rose both through the ITA and LAD region.
With this higher flow propagation, a maximum magnitude of around 3.75E-6 m could be
found on the anastomosis region close to the heel of the bypass graft. Also, from the XY
plane, a slightly higher magnitude of displacement was observed near the anastomosis
region. During the time step of t= 0. 75 s the magnitude of the displacement was
observed to be lower both in the ITA and LAD region. This was once again due to
minimal flow velocity through the inlet region. However, a slightly higher magnitude of
the displacement could be found on the arterial wall of the distal LAD close to the outlet
region.
50% During the time step of t= 0.3 s, a somewhat higher magnitude of displacement was
found to be on the heel compared to its inlets (ITA and proximal LAD). Due to the
higher flow velocity though the ITA region, a slightly higher magnitude of displacement
was found on the ITA region/ heel (XY-plane). Consequently, during the time step of t=
0.55 s, due to higher inlet flow velocity maximum magnitude of around 1.25E-5 m was
found near the heel of the bypass graft. Also, a much higher magnitude of displacement
was found on the ITA region compared to its proximal LAD. Again, with the time step
of t= 0.75 s a much higher magnitude of displacement was found on the arterial wall of
the distal LAD close to the outlet region. At the same time step, displacement of the ITA
was moderately higher compared to its LAD (XY-plane).
75% During the time step of t= 0.3 s, a much higher magnitude of the displacement was found
to be around the outlet region. During the time step of t= 0.55 s a much higher
magnitude of displacement was found to be on the heel and on the ITA region. During

124
this time step, a much higher flow velocity entered through the ITA compared to its
stenosed LAD. With the time step of t= 0.75 s, a maximum magnitude of around 1.25E-5
m was found to be on the distal LAD and around the outlet region. Also from the XY
plane, a much lower magnitude of displacement was found to be on the anastomosis
region as the magnitude of the inlet waveform decelerated through the ITA and LAD
region.
3.4.5 Discussions on ITA-LAD for different degree of LAD-stenosis
3.4.5.1 Variations of the hemodynamics inside the bypass graft using velocity mapping
The changes in the flow pattern, including the generation, development, merging and
shifting of vortices during a complete heart cycle in the ITA-LAD bypass graft were
demonstrated and determined using velocity vectors. During the simulations, different
rates of flow through the ITA-LAD bypass graft were implemented for different degrees
of LAD-stenosis in order to understand and determine the hemodynamical conditions of
the bypass grafts. Hence, due to different inlet flow rates, variations in the flow patterns
are observed through the ITA and LAD region and, as a result, separation of flow,
formation of vortices and other phenomena are also observed. Moreover, from the
simulations it became evident that higher degree of LAD-stenosis decreased the flow
dynamics through the proximal LAD (Ding et al., 2012). The observations are
summarized in Table 3.5.
Table 3.5 Time step observations
Time Step Observations t= 0.05 s The flow direction through the ITA region was found to be reversed for the 0% LAD-
stenosis. This phenomenon can be explained in that, with the higher inlet velocity of the
proximal LAD compared to its ITA and also the negative velocity gradient for the ITA,
there was a separation of the flow and reverse directional flow was found at the ITA
region. However during the same time step, the direction of the flow was found to be
forward for the 30%, 50% and 75% LAD-stenosis levels. It needs to be noted that
disturbance in the flow pattern was observed close to the heel near the anastomosis
region, both for the 50% and 75% LAD-stenosis.

125
t= 0.3 s The direction of the flow was found to be forward for all four LAD-stenosis. With the
increase in the degree of LAD-stenosis, the rate of flow through the proximal LAD
decelerated. Therefore:
• A deceleration in the flow pattern (30%, 50% and 75%)
• Dominance of the flow through the ITA region (30%, 50% and 75%)
• Disturbance of flow near the heel in the anastomosis region (50% and 75%)
• Generation of a weak ring shaped and CW vortex in the anastomosis region of
the proximal LAD (75%)
were observed during this time step.
t= 0.55 s The direction of the flow pattern was found to be forward once again for all cases of
LAD-stenosis. With the elevation in the rate of flow through the ITA region and due to
the increase in the degree of LAD stenosis, a much higher flow velocity was found in
the distal LAD. Precisely, a much higher velocity was observed for the 75% LAD-
stenosis compared to 50%, 30% and 0% LAD-stenosis. Although a smooth flow profile
was observed in the bypass graft for the 0% and 30% LAD-stenosis, but for the 50%
and 75% LAD-stenosis, a fluid stagnation was found just beside the toe close to the
arterial wall of the distal LAD. This could be attributed to the fact that, due to higher
flow velocity through the ITA region, the rate of flow was found to be higher through
the distal LAD and hence, due to the anastomosis angle of the ITA, stagnation was
found close to the arterial wall. Also, because of the dominance of the flow rate through
the ITA region, a slight disturbance/hindrance in the flow pattern was observed near the
anastomosis region for the 75% LAD-stenosis, though the rate of flow through the
proximal LAD was minimal. Also, for the similar LAD-stenosis, the previous weak
vortex slightly merged with the inlet velocity through the LAD region.
t= 0.75 s A reverse-direction flow pattern was obtained once again for the 0% LAD-stenosis.
This could be ascribed to the fact that due to negative flow velocity through the ITA
and much higher flow rate through the proximal LAD, a reverse direction in the flow
pattern was observed through the ITA region. However, the direction of flow was
found to be forward in the bypass graft for all the stenosed cases. Once more, a smooth
flow profile was observed in the bypass graft of the 30% LAD-stenosis. Also, similar to
the previous time step (t= 0.55 s) a stagnation was found to be near the arterial wall of
the distal LAD, both for the 50% and 75% LAD-stenosis. Moreover, because of
minimal flow velocity through the LAD region, the weak ring shaped CW vortex was
seen once again near the arterial wall of the anastomosis region, but the location of the
vortex is shifted slightly towards the distal LAD region.

126
From Table 3.5, it can be noted that the general trend for the flow pattern, including:
• The disturbance of the flow
• Generation, merging and shifting of vortices
• Changes in the direction of the flow pattern inside the bypass graft
for the different degrees of LAD-stenosis coincided well with previously documented
investigations (Ding et al., 2012, Kouhi, 2011, Freshwater IJ, 2006).
3.4.5.2 The effects of Wall Shear Stress (WSS) inside the bypass graft using WSS
distributions
The variations in the WSS during different time steps are provided in table 3.6.
Table 3.6 Time step observations
Time Step Observations t= 0.05 s At the onset of the simulation (t= 0.05 s), the magnitude of the WSS was mostly
observed on:
• The LAD (0% stenosis)
• Toe (30% and 50% stenosis)
• ITA (75% stenosis)
Due to the variations in the inlet velocities through the ITA and LAD region for
different degrees of LAD-stenosis, the magnitude of the WSS varied accordingly.
Specifically, for the 0% stenosis in the proximal LAD, higher magnitudes of WSS were
found on the host artery. However, with the rise in the degree of stenosis inside the host
artery (LAD), much lower magnitudes of WSS were found on the LAD wall.
Moreover, for the 30% and 50% stenosis, WSS was found to be moderately higher on
the toe compared to its inlets, but for the 75% stenosis slightly higher WSS can be
found on the ITA and near the toe region of the bypass graft. So, with the rise in the
degree of LAD-stenosis during this time step, higher magnitudes of WSS were found
on the ITA region (75% LAD-stenosis).
t= 0.3 s During this time step, moderately higher magnitudes of WSS were found on the outlet
region/distal LAD of the bypass artery for the 0%ALD-stenosis. This can be explained
127
by the fact that fluid enters through the ITA and LAD region without any hindrance and
the flow pattern inflicts the magnitude of the WSS on the distal LAD. Moreover, this
slightly higher magnitude of the WSS on the outlet region was also seen for the 50%
LAD-stenosis and 75% LAD-stenosis. This was due to the variations in the inlet
velocity, but because of the higher flow rate through the ITA compared to its LAD
region, a somewhat higher magnitude of WSS was found on the ITA for these two
cases. However for the 30% LAD-stenosis, lower magnitudes of WSS were found on
the entire bypass graft due to minimal inflow velocity through the ITA and LAD
region.
t= 0.55 s The much higher inflow velocity through the LAD region for the 0% stenosis meant
that a higher magnitude of WSS was found on the host artery (both on proximal and
distal LAD) compared to its ITA. For the 30% LAD-stenosis, a higher magnitude of
WSS was found on the distal LAD and on the toe, but the magnitude on the distal LAD
was lower compared to 0% LAD-stenosis. Once again, the variations in the inlet
velocity were responsible for the discrepancies on the WSS. For the 50% and 75%
LAD-stenosis, due to higher inlet flow velocity through the ITA region, a much higher
magnitude of the WSS was found on the ITA, toe and on the distal LAD. Precisely,
much higher magnitude of WSS can be found on the toe (50% and 75% stenosis) and
just beside the anastomosis region on the distal LAD (75% stenosis). This was ascribed
to the fact that, with a higher degree of LAD-stenosis and higher inlet velocity through
the ITA, the WSS was seen to be much higher on the toe and near the anstomosis
region of the distal LAD.
t= 0.75 s During this time step, inlet flow velocity minimized through both the ITA and LAD
region for all cases and therefore, the magnitude of the WSS on the bypass graft for all
cases decreased relative to its previous time step (t= 0.55 s).
Consequently, from the simulation results and the analysis it was determined that the
general phenomena on the variations of the wall shear stress (WSS) were in line with
previously published researches (Kouhi, 2011, Ding et al., 2012).
3.4.5.3 The effects of the wall shear stress (WSS) inside the bypass graft using spatial
wall shear stress (WSS) distributions
128
From the graphical representations of the line A (toe), line B (heel) and line C (bed), the
variations in the WSS in different time steps were obtained for different inlet velocities
through the ITA and proximal LAD, for different degrees of stenosis. In general, for all
cases of line A, the maximum magnitude was found to be near the toe of the artery
during the time step of t= 0.55 s. This could be explained by the fact that a much higher
magnitude of inlet velocity was found to be entering through the ITA and LAD region
during this time step. However, due to the LAD-stenosis, the propagation of the flow
was obstructed inside the proximal LAD, but with higher inflow velocity through the
ITA region (for different degrees of LAD-stenosis), a much higher magnitude was
obtained on the toe of the bypass graft. Conversely, with a lower magnitude of inlet
velocity WSS decreased.
Subsequently, similar phenomena were observed for line B for different LAD-stenosis
levels. Once again, with the aid of higher inflow velocity (t= 0.55 s), a maximum
magnitude of WSS was found to be on the heel of the proximal LAD. Although higher
magnitude of WSS was found during this time step, but it needs to be noted that with
the increase in the degree of LAD-stenosis, the magnitude of the WSS on the heel
decreased.
Likewise, a maximum magnitude of WSS was found to be on the bed (line C) during
the time step of t= 0.55 s. Once again this was due to the higher inlet flow velocity,
which helped elevate the magnitude of WSS. Also, with lower inflow velocity, the
magnitude minimized.
So, the general trends of the variations of the spatial WSS distributions were in line with
the investigations from (Kouhi, 2011).
3.4.5.4 Structure simulation of the bypass graft for different degree of LAD-stenosis
using total mesh displacement (TMD)

129
During the time step of t= 0.3 s, due to minimal inlet flow velocity for all cases, the
magnitude of the displacement on the ITA and LAD were found to be minimal.
However, moderately higher magnitudes of displacement were found to be on the distal
LAD for all cases and around the outlet region (75%) during this time step. This can be
ascribed to the fact that, due to the propagation velocity through the inlet region,
volume inside the bypass graft rose and in turn, the magnitude of the displacement on
the distal LAD elevated.
Subsequently, with the time step of t= 0.55 s, much higher inlet flow velocities entered
through the ITA and LAD region. A maximum magnitude of displacement was found to
be on the distal LAD (0%), but from the simulated results it was observed that the
increase in the degree of the maximum magnitude of displacement was found to be on
the heel (30%, 50% and 75%). Also, due to higher inlet flow velocity (ITA and LAD),
the volume inside the inlets increased. Hence, during this time step, maximum
displacements on the ITA and proximal LAD were obtained for 50% LAD-stenosis.
At a time step of t= 0.75 s, magnitudes of the inlet velocities became minimal for all
cases compared to the previous time step of t= 0.55 s. During this time step, a much
lower magnitude on the entire bypass graft was found for the no-stenosis case.
However, for the stenosed cases, a slightly higher magnitude on the distal LAD (30%),
both on the ITA and distal LAD (55%) and maximum magnitude of displacement
around the outlet region and on the distal LAD (75%) were found. These phenomena
can be attributed to the fact that due to the minimal inlet velocity through the ITA and
LAD, magnitude of the displacement decreased (0%) as the volume inside the graft
provided very little displacement on the arterial wall. Also, for the stenosed cases,
because of the variations of the inlet velocities through the ITA and LAD, the volume
inside the ITA (55% and 75%) and on the distal LAD (30%, 55% and 75%) rose and
this consecutively increased the magnitude of the displacements.

130
3.5 Abdominal Aortic Aneurysm (AAA)
In general, an aneurysm indicates the ballooning/swelling of a local blood vessel above
half of its nominal diameter leading to a risk of unexpected rupture. There are various
factors responsible for producing aneurysms such as:
• Blood vessel deterioration
• Diseases
• Unexpected/sudden injuries
• Birth driven factors
Even though aneurysms can be developed in any blood vessels, four different types of
aneurysms can create critical risks (Li, 2005), specifically:
• Brain aneurysms
• Thoracic aortic aneurysms
• Dissecting aortic aneurysms
• Abdominal aortic aneurysms (AAA)
AAA is located in the abdominal aorta, which is below the renal arteries and above the
iliac bifurcation (Figure 3.10). Aged people (60 years or more) are much prone to AAA
diseases. Also, 90% of AAA are found to be between the renal arteries and iliac
bifurcation (Li, 2005).

131
Figure 3.10 Location of abdominal aortic aneurysm (AAA) (Stern)

132
3.6 Literature Review of Abdominal Aortic Aneurysm (AAA)
Various computational approaches had been conducted which focused on the
hemodynamics and wall shear stress analysis of the AAA models - both clinically and
laboratory-based - along with different computational approaches (Li, 2005). For
instance, Peattie et al., 1994, examined the steady flow through some polyvinyl chloride
models of aneurysms and the flow dynamics were determined by using colour Doppler
imaging. They noted that for lower flow rates, smooth and laminar flow patterns were
observed. Also, for higher rates of flow, the flow pattern was found to be intermittent,
fluctuating/random and turbulent (Peattie et al., 1994).
In another study, Yamada et al., 1994, investigated the mechanical features of the
expansion and rupture of the AAA. The researchers noted that intrinsic (maximum
diameter and wall thickness) and external (blood pressure) factors highly influenced the
deformation and stress distributions in the AAA. The results stated that the rise in the
intrinsic and external factors requirements elevated the wall stress because of the
expansion of the aneurysm (Yamada et al., 1994).
In the year 2000, Raghavan and Vorp (2000), constructed the finite strain structure of
the AAA by utilizing experimental results. They noted that their model was suitable for
the AAA stress analysis and it could also be effective for developing a biomechanical
tool which could clinically assist AAA affected patients. However during this
investigation, a simplified model of AAA was utilized (Raghavan and Vorp, 2000). The
same research group Raghavan et al., 2000 non-invasively examined the wall stress
distributions of a 3D model of the AAA during systolic blood pressure. Data was
obtained from six patients with AAA and one patient with non-aneurysmal aorta using
spiral CT images. However, during their analysis, the wall thickness was considered
uniform and invariable (Raghavan et al., 2000).
Hua et al., 2001, noted that simple geometric features were not reliable in estimating
AAA wall stresses (Hua and Mower, 2001). Subsequently, Elger et al., 1996, also
worked on the wall stresses of the AAA and determined the correlation between the
variations of stresses exerted on the wall and the shape of AAA (Elger et al., 1996).

133
Thubrikar et al., 2001, noted that in order to determine the rupture of an AAA, it was
essential to identify the primary features responsible for this. In doing so, the authors
examined the wall stresses in a clinical model of AAA and they concluded that the
rupture of the AAA was presumably to take place inside the internal surface of the wall
(Thubrikar et al., 2001a). In another study Thubrikar et al., 2001, examined the
mechanical properties/characteristics of aneurysms in various sections of the AAA.
From the results they identified the various yield stress, yield strains and other
mechanical features possessed in various sections of the AAA (Thubrikar et al., 2001b).
Sonesson et al., 1997, also studied the mechanical features of the aneurysm aorta and
they concluded that the AAA was the simplified process of a vasculature with
significant symptoms in the abdominal aorta (Sonesson et al., 1997).
Fillinger et al., 2002, determined the in vivo AAA wall stresses for ruptured and
symptomatic cases, and concluded that this stress analysis was viable. This might play a
significant role in detecting an AAA rupture-threat (Fillinger et al., 2002). The same
group extended their research and investigated the rupture-threat over time where the
patients were being monitored (Fillinger et al., 2003).
In 2005, Li and Kleinstreuer (2005) worked on AAA wall stresses and proposed a new
wall stress equation for the aneurysm-rupture (Li and Kleinstreuer, 2005). The same
group utilized FSI on AAA structure including variable neck and bifurcation angle to
investigate the effects of hemodynamics and wall stress (Li and Kleinstreuer, 2006) -
similarly with (Pelerin et al., 2006). The influence of the asymmetry and wall thickness
of the AAA were studied by Scotti et al., 2005 (Scotti et al., 2005). Moreover,
investigations on wall stresses and hemodynamics inside the AAA were also conducted
by the same research group (Scotti et al., 2008). Xenos et al., 2010, once again utilized
the FSI technique to study the development of aneurismal disease by considering the
iliac bifurcation and AAA neck angle (Xenos, 2010).
In another study, Georgakarakos et al., 2011, noted that the conventional norm of
maximum diameter was not enough to distinguish a small AAA, which may be likely to
rupture or expand quickly, but wall stress might play a significant role in such cases.

134
Hence, these researchers reviewed the significance of geometric-characteristics in
possible rupture or expansion, and the necessity for further assessment and validation of
geometric features (Georgakarakos et al., 2011).
Maksymowicz et al., 2011, noted that with the existing medical knowledge it was not
possible to avert the formation and progression of AAA since the pathogenesis of this
disease was unidentified. Therefore, the authors reviewed the three crucial factors which
were related with the development of AAA, such as (Sonesson et al., 1997, Shteinberg
et al., 2000, Maksymowicz et al., 2011):
• Maximum diameter
• Growth/ expansion rate
• Mural thrombus existence
They also stated that there could be multiple causes for the generation of AAA which
include (Sonesson et al., 1997, Shteinberg et al., 2000, Maksymowicz et al., 2011):
• Genetic
• Anatomic
• Hemodynamical
• Biomechanical
• Environmental issues such as smoking,
• Inflammatory/provocative
• Atherosclerotic
Martufi and Gasser, 2013, reviewed the functionalities of the biomechanical modelling
in the rupture-threat-evaluation for the AAA and they noted that the evaluation was
effective for patients as it aspired to preclude aneurysms from being ruptured, not
including a needless number of repair intercessions (Martufi and Gasser, 2013).
Another review was conducted by Kleinstreuer et al., 2013 based on the rupture risk-
threat-evaluation and surgical restoration of AAA. However, during their investigations
they noted that the Fluid Structure Interaction (FSI) for patient-specific AAA cases

135
vastly enhanced the accuracy of rupture occurrences (Kleinstreuer et al., 2013).
Subsequently, Soudah et al., 2013 exploited the computational fluid dynamics
modelling (CFD) of a 3D AAA model using hemodynamic loads. The authors noted
that AAA rupture was a multifaceted condition-which relied on the:
• Maximum diameter
• Internal pressure
• Wall stress
• Asymmetry
• Saccular manifestation
and so on (Soudah et al., 2013). Also, Giuma et al., 2013, employed FSI of the AAA
and highlighted the significance of geometric parameters in predicting the maximum
wall stresses (Giuma et al., 2013).
Svensjo et al., 2014, reported a population-oriented group-study where people had been
asked for the aortic ultrasound test at the age 65 and asked to be monitored once again
at the age of 70. They stated that the development of AAA was quite usual among
people incorporating an aortic diameter less than 30 mm (Svensjö et al., 2014).
In summary, researchers had studied the general flow pattern and wall stresses of an
AAA with different degrees of accomplishment. However, a complete investigation,
based on the hemodynamic and structural displacement of an AAA model needed to be
assessed thoroughly. In so doing, the hemodynamic forces inside the AAA were
analysed and demonstrated by utilizing velocity mapping and WSS distributions.
Structural displacements were demonstrated by employing total mesh displacement
(TMD) under different physiological conditions. Moreover, during the computational
approaches, Arbitrary Lagrangian Eulerian (ALE) equations were implemented for FSI-
analysis of the 3D axisymmetric AAA model.

136
3.7 Case Study II: abdominal aortic aneurysm (AAA)
3.7.1 Geometry
Figure 3.11 (a) represents a 3D axisymmetric model of the AAA, created using
SolidWorks 2012. This illustrates the ideal aortic aneurysm in the abdomen (AAA) of a
human body. Also, Figure 3.11 (b) demonstrates the detailed dimensions of the AAA by
utilizing the similar CAD software. For the following figures
• The diameter of the proximal neck was considered to be 20 mm.
• The iliac bifurcation artery 12 mm.
• The aneurysm wall 60 mm.
• The length of the neck aorta (proximal neck) was 20 mm.
• The aneurysm wall was 80 mm.
• The iliac bifurcation artery (distal neck) was 41 mm.
• The wall thickness of the neck aorta and aneurysm wall was considered to be
1.50 mm each.
• The iliac bifurcation artery was 1 mm.
• The iliac bifurcation artery angle was assumed to be 60°.
All the geometric parameters match closely with the models of (Li, 2005, Xenos, 2010,
Li and Kleinstreuer, 2006, Thubrikar et al., 2001a).

137
(a)
(b)
Figure 3.11 (a) Cross-sectional geometry of an axisymmetric AAA (using SolidWorks
2012) (b) Detailed dimensions of the AAA (using SolidWorks 2012) (Li, 2005)

138
3.7.2 Meshing Configurations and Mesh Independency Testing
In a similar approach to that deployed for the bypass graft model, after constructing the
3D AAA model in the CAD software, it was then imported to ANSYS 14.5, where a
suitable meshing was implemented and mandatory boundary conditions were provided.
Once again, “Mapped Face Meshing” was executed individually for both the solid and
fluid domain. Moreover, line control properties were applied in order to find the
variations in the velocity of the fluid. Subsequently, by implementing these line control
properties, mesh independency testing was carried out to determine and compare the
discrepancies in the fluid velocity for consecutive nodes and elements, until the velocity
converged (Kouhi, 2011).
The mesh independency testing is demonstrated in Figure 3.12 which was obtained
from the discrepancies in the fluid velocity. Moreover, three different mesh types
(coarse, medium and fine) were chosen and varied during the simulations. It should be
noted that, 28205 nodes and 15291 elements were considered to be apposite and
validated for the solid region, and 12706 nodes and 46557 elements, for the fluid region.
Also, for the solid domain refinement of the distal neck of the iliac bifurcation was
employed. Furthermore, from the simulations all these nodes and elements were
selected from the coarse mesh type. Once more, the convergence conditions for the fluid
flow were considered to be 10-4 and 10-2 for the coupling data transfer.

139
Figure 3.12 Mesh independency testing using line control properties
3.7.3 Required Boundary Conditions
Once again, similar to the simulations of the bypass graft, compulsory boundary
conditions had to be assigned to perform the desired simulations. During the simulation,
the inlet flow velocity was provided through the neck aorta (proximal neck) and the
outlet pressure waveform was provided through the iliac bifurcation arteries (and/or
distal neck) of the AAA. Figure 3.13 and figure 3.14 represent the velocity and pressure
waveforms through the inlet and outlet accordingly and the waveforms closely matched
with the previous investigations of (Li and Kleinstreuer, 2006, Li, 2005, Xenos, 2010).
For the inlet velocity waveform, the X-axis represents the time (t) in seconds and the Y-
axis represents the velocity (V) in m/s. Also, for the outlet waveform, the X-axis
represents the time (t) in seconds and the Y-axis represents the pressure (P) in mmHg.
In order to simplify the simulation and to avoid geometric inflation (Xenos, 2010), the
outlet pressure waveform was modified and is illustrated in Figure 3.15.
0
0.2
0.4
0.6
0.8
1
1.2
1.4
5.20E-055.30E-055.40E-055.50E-055.60E-055.70E-05
Velo
city
, V [m
/s]
Z [m]
Coarse refinementmesh
Medium mesh
Fine mesh

140
Figure 3.13 Inlet velocity waveform (Li, 2005)
Figure 3.14 Actual outlet pressure waveform (Li, 2005)
Figure 3.15 Simplified outlet pressure waveform utilized in the simulations
-0.1
0
0.1
0.2
0.3
0.4
0.5
0 0.5 1 1.5
Velo
city
, V (m
/s)
t (s)
Inlet velocity
0
20
40
60
80
100
120
140
0 0.5 1 1.5
Pres
sure
, P (m
mHg
)
t (s)
Outlet…
0
20
40
60
80
100
120
140
0 0.5 1 1.5
Pres
sure
, P (m
mHg
)
t (s)
Simplified outletpressure

141
After providing the required inlet and outlet waveforms, the density and viscosity of the
liquid/fluid were assigned with the value of 1050 kg/m3 and 0.0035 Pa•s accordingly.
Li, 2005, reported that experimental information suggested that the elastic modulus for
the aneurysm was much higher than that of a healthy artery (neck and iliac bifurcation).
Therefore, the elastic modulus for the aneurysm was considered to be 4.66 MPa and for
the healthy artery it was 1.2 MPa. Also, Poisson’s ratio for the aneurysm wall and
healthy artery were considered to be 0.45 and 0.49 respectively. Also, the
circumferential faces of the inlet and the outlet were considered fixed during the
simulation. Similar to the bypass simulations, the AAA wall was assumed to be
isotropic and homogeneous. Moreover, Newtonian fluid flow was considered during the
simulations including the no-slip boundary conditions. Also, the flow was assumed to
be laminar (Li, 2005, Xenos, 2010, Di Martino et al., 2001, Li and Kleinstreuer, 2006,
Soudah et al., 2013, Pelerin et al., 2006). Once again, for coupling data transfer control,
under relaxation, the factor had been set to 0.75.
3.7.4 Simulation Results
3.7.4.1 Velocity Mapping
Simulation results are illustrated by utilizing velocity mapping, which incorporates:
• The generation, development, shifting and merging of vortices inside the
aneurysm
• Distributions of wall shear stress (WSS)
• Structural displacement in terms of total mesh displacement (TMD)
during a complete cardiac cycle.
Figures in 3.16 illustrate the flow pattern inside the aneurysm in ten different time steps.
Velocity vectors were utilized to characterize the variations in the flow dynamics, which

142
were mapped on the XY cross-sectional plane of the AAA. This plane was set in the
middle of the AAA where the plane consisted of inlet, outlets and the aneurysm.
0.025 s 0.05 s
0.1 s
0.15 s 0.2s

143
0.275 s
0.5 s
Figure 3.16 Velocity distributions of the AAA in different time steps
At the beginning of the simulation, the jet started to enter through the distal neck of the
outlet regions inside the aneurysm body (t= 0.025 s). This was due to higher outlet
velocity compared to the inlet. With an increase in the time step (t= 0.05 s) the
exit/outlet velocity rose and therefore, a higher magnitude of velocity entered through
the distal neck. During this time step, two ring shaped vortices started to develop close
to the distal neck of the aneurysm wall. Subsequently, this clockwise (CW) ring shaped
vortex on the right-side and counter clockwise (CCW) ring shaped vortex on the left-
side were found to be elongating close to the distal neck (t= 0.1 s). During this exact

144
time step, the magnitude of the outlet velocity was still found to be higher than that of
inlet.
During the time step of t= 0.15 s the inlet velocity started to rise and the fluid entered
through the proximal neck of the aneurysm. At the same time step, the magnitude of the
velocity through the iliac bifurcation was found to be slightly decelerating compared to
the previous time step. Simultaneously, the primary vortices shifted their location and
moved towards the centre of the aneurysm body. Later, with the time step of t= 0.2 s, a
maximum magnitude of velocity, around 1.4 m/s, was found to be entering through the
distal neck. The inlet velocity with a magnitude of around 0.42 m/s (from Figure 3.13)
started to enter through the proximal neck. During this time step, the vortices slightly
expanded and reached toward the core of the aneurysm.
Consequently, with a higher magnitude of the inlet velocity through the proximal neck
(t= 0.275 s), a CCW ring shaped vortex developed on the right-side and a CW ring
shaped vortex on the left side, close to the proximal neck of the aneurysm. However,
with the progression in the time step, the magnitudes of the inlet and outlet start to
decrease. Precisely, during the time step of t= 0.5 s, with lower inlet and outlet velocity,
the secondary vortices expanded slightly but the primary vortices shifted their locations
once again close to the wall and started to merge. Later, with lower magnitudes of inlet
and outlet velocities (t= 0.7 s, 0.9 s and 1 s; please see in Appendix, Figure A-1), both
the primary and secondary vortices (all four) started to amalgamate with the progression
of the time steps.
3.7.4.2 Wall shear stress (WSS) distributions
All the illustrations in Figures 3.17 demonstrate the wall shear stress (WSS) inside the
aneurysm during a cardiac cycle. The wall motion during this cardiac cycle had to be
determined and in doing so, WSS was considered on the exterior surface of the
aneurysm wall for ten different time steps.

145
0.025 s 0.05 s
0.1 s 0.15 s
0.2 s 0.275 s
Figure 3.17 WSS distributions of the AAA in different time steps

146
As demonstrated in the Section 4.7.3.1, at the beginning of the simulation (t= 0.025 s),
the magnitude of the inflow velocity through the distal neck was much higher than at
the proximal neck. During this time step, a much higher magnitude of WSS was found
on the distal neck compared to its proximal neck. After that, with a rise in the inflow
velocity through the bifurcation (t= 0.05 s), the magnitude of the WSS on the distal neck
elevated and also the WSS of the iliac arteries/outlet regions rose compared to the
previous time step. During the time step of t= 0.1 s, the magnitude of the WSS was
found to be almost identical with the previous time step (t= 0.05 s). At the same time
step, a much higher magnitude of WSS was found on the distal neck compared to its
iliac arteries. With further progression of the time step, t= 0.15 s, the inlet jet started to
enter through the proximal neck and hence slight variations of the WSS were found on
the neck artery. Also, during this time step the magnitude of the WSS on the distal neck
was found to be decreasing compared to the previous time step (t= 0.1 s).
During the time step of t= 0.2 s, a maximum magnitude of WSS, approximately 1.2 E1
Pa was found to be on the distal neck of the aneurysm. Simultaneously, the magnitude
of the WSS on the proximal neck was found to be moderately higher when compared to
its previous time step, but this magnitude was much lower than that of the distal neck.
During the time step of t= 0.275 s, both the magnitude of the WSS on the proximal neck
and distal neck started to decline. During the time steps of t= 0.5 s, 0.7 s, 0.9 s and 1 s,
no significant variations of the WSS were identified on the AAA (Please see in
Appendix, Figure A-2).
3.7.4.3 Total mesh displacement (TMD) distributions
Figure 3.18 illustrates the variations of the structural displacement of the aneurysm
during a cardiac cycle in ten different time steps. Changes in the displacement of the
aneurysm-model during the cardiac cycle were determined using total mesh

147
displacement (TMD) distributions. In doing so, TMD had been considered on the outer
surface of the aneurysm body.
0.025 s 0.05 s
0.1 s 0.15 s
0.2 s 0.275 s

148
0.5 s
Figure 3.18 Structural displacement using total mesh displacement (TMD)
distributions
At the onset of the simulation (t= 0.025 s), the change in the displacement was found to
be minimal in the vicinity of the iliac bifurcation arteries, due to lower inflow waveform
through the iliac bifurcation arteries. With a rise in the inflow velocity through the distal
neck, variations in the magnitude of the displacement were evident on the aneurysm
wall and on the distal neck. Later, during the time step of t= 0.1 s, the magnitude of the
displacement on the aneurysm wall close to the distal neck was found to be increasing
and simultaneously, a higher magnitude of displacement was evident in the vicinity of
the bifurcation arteries.
During the time step of t= 0.15 s, the rate of flow through the proximal neck accelerated
and the magnitude of the displacement tended to increase on the aneurysm wall close to
the neck artery. However, the magnitude of the displacement close to the distal neck
was found to be increasing.
At the time step of t= 0.2 s the flow rate through the distal and proximal neck
accelerated and the magnitude of the displacement was still found to be moderately
higher close to the distal neck of the aneurysm. When the inflow velocity through the
proximal and distal neck decelerated (t= 0.275 s), a higher magnitude of displacement

149
was still found to be on the aneurysm wall close to the distal neck. Moreover, during the
time step of t= 0.5 s, a maximum displacement of approximately 2.3E-3 m was found
on the aneurysm wall close to the distal neck. Similarly, during the time steps of t= 0.7
s, 0.9 s and 1 s, a much higher magnitude of the displacement was found to be on the
aneurysm wall near the distal neck (please see in Appendix, Figure A-3).
3.7.5 Discussion
3.7.5.1 Influence of flow dynamics of the AAA using velocity vectors
At the onset of the simulation, a much higher magnitude of velocity flow started to enter
through the bifurcation towards the centre of the aneurysm. During the time step of t=
0.05 s, two ring shaped symmetric vortices (CW vortex on right-side and CCW vortex
on left side) developed close to the distal neck. With a rise in the inflow velocity
through the iliac artery (t= 0.1 s), the primary vortices were expanded and shifted their
position slightly upwards. It should be noted that, during this time step, the generation
of the CW vortex on the right-side and CCW vortex on the left-side contradicted with
the findings from (Li, 2005) who found that a CW vortex originated on the left-side and
CCW on the right-side. This can be attributed to the fact that due to the smaller diameter
of the distal neck and because of a much higher flow velocity through the bifurcation
CW and CCW, symmetric vortices originated and elongated on the right-side and left-
side accordingly. At the same time step, minimal inflow velocity starts to enter through
the inlet region of the aneurysm.
During the time step of t= 0.15 s, the inlet velocity started to rise but the inflow velocity
through the distal neck was much higher than its inlet. At the same time, the primary
symmetric vortices expanded longitudinally and shifted their position towards the centre
of the aneurysm. With further progression in the time step (t= 0.2 s), both the inflow
velocity through the proximal neck (inlet region) and distal neck (iliac
artery/bifurcation) rose. Simultaneously, the primary vortices were found to be at the
core of the aneurysm body. However, due to different parameters of the inlet and outlet

150
waveform, two vortices still existed during this particular time step - this was different
to the findings from (Li, 2005).
After reaching a peak of the inlet velocity (through proximal neck), flow started to
decelerate and during the time step of t= 0. 275 s another pair of symmetric ring shaped
vortices, which were CCW on the right-side and CW on the left-side, were seen
originating close to the proximal neck. The generation and direction of the vortices was
in line with the results from (Li, 2005). This can be attributed to the fact that, with the
higher inlet diameter (proximal neck) and higher magnitude of the inlet jet, the direction
of these two symmetric vortices also completely matched with the findings from (Li,
2005).
The magnitude of the inflow velocity through the inlet and outlet region started to
decelerate in subsequent time steps (t= 0.5 s, 0.7 s, 0.9 s and 1 s). Specifically, during
the time step of 0.5 s, the secondary vortices close to the proximal neck elongated
slightly and shifted their location downwards. The primary vortices changed their
position once again and moved closer to the wall. Later, during the time steps of t= 0.7
s, 0.9 s and 1 s, the primary vortex started to amalgamate, and the secondary vortex
(only right-side) merged also.
Although there were some discrepancies inside the flow dynamics of the aneurysm
during a cardiac cycle, the general trend of the flow dynamics, including the generation,
development, merging and shifting of vortices was in line with the findings from (Li,
2005, Xenos, 2010).
3.7.5.2 Influence of wall shear stress (WSS) of the AAA using WSS distributions
Once again because of the higher inflow velocity through the distal neck during the time
step of t= 0.025 s, a much higher magnitude of the WSS was found on the distal neck of
the aneurysm. Also, due to negative inlet velocity through the proximal neck, no
significant variations of the WSS were found on the neck artery. Subsequently, the

151
magnitude of the WSS on the distal neck was found to be increasing during the time
step of t= 0.05 s, due to the rise in the inflow velocity through the iliac artery. Hence,
the magnitudes of the WSS on the iliac arteries were also found to be elevating during
this exact time step.
During the time step of t= 0.1 s, a higher magnitude of WSS was found on the distal
neck but still due to the negative inflow velocity through the proximal neck, no
variations in the WSS on the proximal neck were found. However, due to higher flow
waves through the iliac arteries, the effect of WSS was found on the bifurcation artery.
Moreover, with the time step of t= 0.15 s, the magnitude of the inflow velocity through
the proximal neck started to rise and hence the discrepancy of the WSS could be found
on the proximal neck. Concurrently, due to a lower inflow wave through the distal neck,
the magnitude of the WSS on the distal neck was found to be decelerating, compared to
the previous time step, but the magnitude was still higher than that of proximal neck.
Also, the effects of the WSS on the iliac arteries are found to be minimizing during this
time step.
Once again, with the rise in the inflow velocity through the proximal and distal neck (t=
0.2 s) of the aneurysm, the magnitudes of the WSS on both the proximal and distal neck
were found to be elevating compared to the previous time steps. Also, the effect of the
WSS was found once more on the iliac bifurcation arteries. However, during the time
step of t= 0.275 s, the magnitude of the inflow wave through the inlet and iliac artery
started to decelerate and because of that, the magnitude of the WSS on both the neck
artery and distal neck were found to be decelerating. Additionally, the effects of the
WSS on the iliac arteries decelerated due to lower inflow waves through the outlet
region. Moreover, during the time steps of t= 0.5 s, 0.7 s, 0.9 s and 1 s the magnitude of
the WSS was found to be minimal because of the lower inflow wave through the
proximal and distal neck.

152
3.7.5.3 Influence of the structral displacement of the AAA using total mesh displacemnt
(TMD) distributions
At the beginning of the simulation (t= 0.025 s), the inflow wave started to enter through
the iliac arteries and therefore the magnitude of the displacement tended to be slightly
higher in the vicinity of the bifurcation arteries. With the progression of the time step
(t= 0.05 s), the inflow wave through the bifurcation arteries rose and a higher magnitude
of displacement was found on the aneurysm wall. This can be attributed to the fact that
due to the rise in the inflow wave through the iliac arteries, the jet started to propagate
from the distal neck towards the proximal neck. Hence, the volume inside the aneurysm
increased, which consecutively increased the magnitude of the displacement inside the
AAA.
During the time step of t= 0.1 s, a much higher magnitude of inflow wave started to
enter through the distal neck and the volume inside the aneurysm increased. Later, with
the time step of t= 0.15 s, the inflow wave through the proximal neck started to enter
and the volume inside the aneurysm increased. With the jet entering both the proximal
and distal neck, the volume inside the aneurysm rose and a higher magnitude of
displacement was found on the aneurysm wall close to the distal neck.
Once again, with the time step of t= 0.2 s the magnitude of the inflow jet both the
proximal and distal neck increased and therefore the volume increased. Also, a much
higher magnitude of displacement was still found to be on the aneurysm wall near the
distal neck. After that, the magnitude of the inflow wave started to decelerate (t= 0.275
s and 0.5 s) through the proximal and distal neck but, due to the increased volume inside
the aneurysm, a much higher magnitude of displacement was found on the aneurysm
wall. Precisely, during the time step of t= 0.5 s, a maximum magnitude of displacement
was found to be around 0.0023 m which was close to the value of 0.0016 m for the
symmetric aneurysm as reported by (Li, 2005).
Due to the variations in the outlet waveform and variations in the geometric parameters
of the AAA, the magnitude of the displacement varied. Once more, with lower inflow
velocity through the proximal and distal neck and increased volume inside the

153
aneurysm, a higher magnitude of displacement was still evident on the aneurysm wall,
near the distal neck.
It should be noted from the simulation results that, during all the assigned time steps,
the magnitude of the displacement was found to be higher in the vicinity of the
bifurcation arteries. This could be ascribed to the fact that, because of higher inflow
wave through the iliac arteries, with the bifurcation angle (β) inflow wave entered
through the arteries and combined in the vicinity of the bifurcation arteries. Hence, the
magnitudes of the displacement during all time steps were found to be much higher.

154
3.8 Summary of Results and Conclusions
Table 3.7 summarizes the whole work (CABG and AAA), as presented in this chapter.
Table 3.7 Summary of the whole work (CABG and AAA) Case
Studies
Mesh
Independ
ency
Testing
Boundary
Conditions
Simulations Findings
CABG
with0%,
30%, 50%
and 75%
LAD-
stenosis
Yes (i) Inlet
velocities
obtained from
pigs (Ding et al.,
2012)
(ii) Laminar;
fluid density
and the
viscosity of
1050 kg/m3 and
0.0035 Pa•s
accordingly
(i) Flow
dynamics
(ii) WSS
analysis
including
spatial WSS
distributions
(iii)
Deformation
of the solid
domain
using TMD
(i) Reverse flow direction for the 0% LAD-
stenosis but forward for the stenosed cases (30%,
50% and 75%) during t= 0.05 s
(ii) Disturbance of the flow and generation of
vortices were mostly observed in the anstomosis
region
(iii) Higher WSS were found near the
anastomosis region, toe and on the arterial wall
close to the anastomosis region
(iv) Maximum magnitude of WSS were found
mainly on the anatomosis region (Line C)
(v) With rise in the inlet flow velocity magnitude
of WSS tends to rise
(vi) For the 75% LAD-stenosis maximum
magnitude of displacement was found to be on
the distal LAD and close to the outlet region (t=
0.75 s)
AAA Yes (i) Outlet
pressure
waveform
(ii) Laminar;
fluid density
and the
viscosity of
1050 kg/m3 and
0.0035 Pa•s
respectively
(i) Flow
dynamics
(ii) WSS
analysis
(iii)
Deformation
of the
structure
using TMD
(i) Due to smaller diameter of the distal neck
than its proximal neck and higher magnitude of
inflow jet entering through the iliac arteries, CW
and CCW symmetric primary vortices were seen
developed and elongated on the right-side and
left-side of the aneurysm accordingly
(ii) With the rise in the inflow waveform, the
magnitude of the WSS elevated. However, with
minimal inflow waveform through the proximal
and distal neck, no significant variations in the
wall shear were seen on the AAA
(iii) The magnitude of displacement is always
found to be higher on the vicinity of the iliac

155
arteries even though the magnitudes varied with
different time steps
From the comprehensive investigations and simulation results detailed in this chapter,
the importance and applications of the FSI scheme were achieved. Specifically, the
necessity for:
• Grid independency testing
• Required physiological parameters/ boundary conditions for the solid and
fluid domains
• Physiologically correct pulsatile flow conditions through the inlet and outlet
regions
were learned. The manner in which these factors could change the general outcomes of
simulations (case studies) were analysed and discussed. The applications of different
numerical methods (Navier-Stokes equations and ALE); the variations in the simulations
using the under-relaxation factors and the extractions of the inlet and outlet flow
patterns, along with the appropriate boundary conditions were noted. The obtained
results and detailed analysis from the case studies, in terms of flow dynamics, WSS
analysis and the deformation of the solid domain, provided substantial insights into the
hemodynamics and structural changes of the coupled models.
In conclusion, during the numerical simulations (CABG and AAA), simplified and
anatomically correct geometries were deployed and the results were studied and
analyzed accordingly by employing a Fluid Structure Interaction (FSI) scheme. After
gathering the required information on the FSI and the applications of this scheme, the
approach was then utilized on a realistic model of the Left Ventricle (LV), presented in
Chapter 4.

156
Chapter 4
Numerical Studies of the Left Ventricle during
Diastole Phase: General Conditions

157
4.1 Overview
The primary objective of the research, documented in this chapter, was to determine and
analyze the hemodynamic characteristics and structural variations of the anatomically
correct 3D model of the left ventricle (LV) during diastolic flow conditions. The entire
simulations for the LV were computed using the Fluid Structure Interaction (FSI)
technique. During the simulations, the results were analyzed and are discussed, herein,
in terms of:
• Flow dynamics
• Intraventricular pressure (Ip) distributions
• Wall shear stress (WSS) distributions
• Deformation of the solid domain
Throughout the simulations, the required boundary conditions were applied. More
precisely, the transmitral flow velocity (U) in the inlet region was provided and in a
similar approach to that documented in Chapter 3, the Navier-Stokes equations and the
Arbitrary Lagrangian Eulerian (ALE) methods were used in order to couple the fluid
and solid domains of the LV model. The results were then studied and compared with
previously published results.
This chapter concludes by providing the findings from the simulations, which could be
particularly useful in the development of a next generation ventricular assist device
(VAD) system. Moreover, these numerical simulations provided a clear view of
hemodynamic features and structural changes which could be beneficial for future,
ongoing research, as presented in Chapter 5 and Chapter 6.
The research work documented in this chapter was extracted from the following
publication:
M. S. Arefin and Y. Morsi, Fluid structure interaction (FSI) simulation of the left
ventricle (LV) during the early filling wave (E-wave), diastasis and atrial
contraction wave (A-wave), Australas Phys Eng Sci Med, 37(2), 2014. DOI:
10.1007/s13246-014-0250-4

158
4.2 Introduction
As noted in the literature review of Chapter 2, a computational approach, using a
Computational Fluid dynamics (CFD)/Fluid Structure Interaction (FSI) scheme could be
utilized for computing the hemodynamic and physiological variations of the LV. It was
also evident from the literature that this simulation method was well established in
terms of understanding and determining the flow dynamics and physiological variations
of a simulated structure (Reul et al., 1981, McQueen and Peskin, 2000, Lemmon and
Yoganathan, 2000).
Earlier researchers had generally placed emphasis on the general flow dynamics of the
LV model, with varying degrees of accomplishment, but a comprehensive analysis of
the flow dynamics and physiological variations of the simulated model was not
thoroughly explained. In this regard, this chapter documents the utilization of the fluid
structure interaction (FSI) scheme in order to understand and determine the
hemodynamic forces and structural variations of a realistic, 3D model of the LV during
the diastolic conditions/filling phase under different physiological states. Therefore:
• Changes in the Ip
• Variations in the flow pattern, including the changing, shifting and merging of
vortices
• Differences in the wall shear stress (WSS)
under various physiological conditions are documented and discussed. Additionally, the
structural displacement of the LV model is also explained, using the total mesh
displacement during the filling phase. Conclusions are presented at the end of this
chapter, where the hemodynamic and physiological states are thoroughly explained
during diastolic flow conditions.

159
4.3 Computational Approaches
4.3.1 Overview
In this section, the details of the LV geometry are described and the various
measurement parameters are presented. Subsequently, the required boundary conditions
and inlet velocity waveform are executed. Once all the required features are provided,
the:
• Distributions of intraventricular pressure (Ip)
• Velocity pattern
• WSS distributions
• Variations in structural displacement
are observed and documented.
4.3.2 Geometry
A three dimensional (3D), physiologically realistic left ventricle model of the heart was
developed using CAD software (SolidWorks 2010) (figure 4.1). This structure was
modelled by considering the entire physiological characteristics/measurements of the
LV, with the aid of magnetic resonance imaging (MRI) data and additional required
information that was extracted from medical textbooks. These recommended
measurements/dimensions matched closely with the practical LV models, as stated in
(Arefin and Morsi, 2014, Bronzino 1999, Bronzino, 2006, Zheng et al., 2012, Saber et
al., 2001).
A simplified LV structure was utilized for the simulations. However, the literature
suggested that if the essential physiological and hemodynamic boundary conditions
were assigned properly, then a simplified model could still produce valid results, which
could be readily related to the physical behaviour of a real LV (Cheng et al., 2005,

160
Nakamura et al., 2002, Zheng et al., 2012, Watanabe et al., 2004, Arefin and Morsi,
2014).
The shape of the employed LV model was an ellipsoidal, which is exhibited in Figure
4.1, with the values of (Arefin and Morsi, 2014, Cheng et al., 2005):
• 0.7 cm starting from the topmost part of the LV (inlet/mitral orifice) to the
lowermost part of the model.
• 3.6 cm from the right-side of the LV to the left-side.
Moreover, in a similar approach to LV geometry as Cheng et al., 2005 (Arefin and
Morsi, 2014, Cheng et al., 2005):
• The diameter of the mitral valve was taken to be 2.5 cm in the inlet region, by
assuming the mitral valve completely open.
• The diameter of aortic valve was set to 2.1 cm in the outlet region, which was
considered completely closed during the total simulations.
• The wall of the LV model was presumed to comprise a uniform wall thickness,
where the magnitude of the wall thickness was 0.1 cm.

161
(a)
(b)
Figure 4.1 (a) Dimensions of the LV used for the simulations (SolidWorks 2010) (b)
Geometric construction of the LV model (SolidWorks 2010) (Arefin and Morsi, 2014)

162
4.3.3 Meshing Information and Mesh Independency Trials
In a similar approach to the meshing technique documented in Chapter 4, a CAD model
of the LV was introduced into ANSYS 15.0 and after importing, the required meshing
was performed and the essential boundary conditions were assigned. For these LV
simulations, “Mapped Face Meshing” was implemented separately, both for the solid
and the fluid regions of the LV. Once again, line control properties were applied and the
discrepancies in the fluid velocity were observed and determined. Hence, mesh
independency trials were executed by utilizing the changes in the flow velocity for
consequent nodes and elements (Kouhi, 2011, Arefin and Morsi, 2014). These changes
were determined until the flow velocities converged.
Figure 4.2 demonstrates the mesh independency trials using flow velocity. During the
testing, three different mesh categories were selected:
• Coarse
• Medium
• Fine
From testing, it was determined that, for the structural domain:
• 19706 nodes
• 10058 elements
were required for accuracy. For the fluid domain:
• 138311 nodes
• 746829 elements
were considered for accuracy purposes. Subsequent nodes and elements were selected
for the medium mesh type for the entire simulations. Moreover, the convergence
criterion for the fluid was considered to be 10-4 and for the coupling data transfer, it was
considered to be 10-2 (Arefin and Morsi, 2014).

163
Figure 4.2 Mesh independency trials (Arefin and Morsi, 2014)
4.3.4 Required Boundary Conditions
The flow velocity for the inlet region was ascertained using a lumped parameter model.
This data was clinically extracted from a young and healthy person. Also, the acquired
data was customized further, using the model of Waite et al. 2000 (Arefin and Morsi,
2014, Cheng et al., 2005, Waite et al., 2000).
Figure 4.3 shows the transmitral flow velocity, U (in m/s) on the X-axis and the time, t
(in seconds) on the Y-axis. This transmitral flow velocity was provided at the inlet of
the model during the simulation. However, in order to implement the velocity
waveform, a curve-fitting procedure was used and the extracted waveform matched
96% with the actual curve, which was acquired from (Arefin and Morsi, 2014, Cheng et
al., 2005, Waite et al., 2000).
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0 0.02 0.04 0.06 0.08
Velo
city
, V [m
/s]
Axial Position, Y [m]
Mesh Type-Coarse
Mesh Type-Medium
Mesh Type-Fine

164
Figure 4.3 Transmitral flow velocity (U) against time (t) waveform, implemented in
the inlet region (Arefin and Morsi, 2014)
The LV wall was considered to be isotropic and homogeneous, including the density of
the LV wall, which was set to be 1.2 g/cm3 and having an elastic modulus of 0.7 MPa
and a Poisson’s Ratio of 0.4. Newtonian fluid flow was considered for the entire
simulation, including:
• A density of 1050 kg/m3
• A viscosity of 0.0035 Pa.s
incorporating no-slip boundary conditions and the flow property was considered to be
laminar. Also, the outlet section and the circumferential face of the inlet were
considered fixed during the whole simulations. Entire simulations were executed on an
Intel® Xeon® processor of 3.07 GHz (Arefin and Morsi, 2014, Cheng et al., 2005,
Lassila et al., 2012, Vierendeels et al., 1999, Saber et al., 2003). For coupling data
transfer control, the under relaxation factor was fixed to 0.75.

165
4.4 Simulation Results and Discussions
4.4.1 Overview
The results and discussions are presented in this section, using
• Intraventricular pressure distribution (Ip)
• Wall Shear Stress (WSS)
• Flow dynamics, including the generation, development, merging and shifting of
vortices during the filling phase
Additionally, variations to the LV structure using total mesh displacement (TMD) were
also considered during the diastolic flow conditions (Arefin and Morsi, 2014).
4.4.2 Distributions of Pressure
It can be observed from Figure 4.3, that the transmitral flow profile (U) is composed of
two peaks, which are:
• At time t= 0.08s, where the flow velocity U is around 0.8 m/s.
• At time t= 0.44s, where the flow profile U is nearly 0.4 m/s.
The first peak was recognized as the early filling wave (E-wave), which resulted from
the resting-period of the LV, due to the flow of blood entering from the left atrium to
the ventricle and the latter peak was known as the atrial contraction wave (A-wave),
which was responsible for applying pressure on the atria. Subsequently, in-between
these two peaks, the middle phase of the flow profile (around 0.22<t<0.3s) was
recognized as the diastasis or slow filling or relaxed filling period (Arefin and Morsi,
2014, Cheng et al., 2005).

166
Figure 4.4 shows the pressure distribution into the interior section of the LV, where the
changes in the intraventricular pressure (Ip) were differentiated by implementing an XY
cross-sectional plane throughout the diastolic flow conditions. These variations in the Ip
were demonstrated for fourteen different states of the transmitral waveform. During the
simulation, the inlet was considered fully open and the outlet was considered fully-
closed, as noted in Section 4.3.2 (Cheng et al., 2005, Arefin and Morsi, 2014).
(a) t= 0.025s (b) t= 0.05s
(c) t=0.075 s (d) t= 0.125 s

167
(e) t= 0.15s (f) t= 0.2 s
(g) t= 0.225s (h) t= 0.275 s

168
(i) t= 0.35 s (j) t=0.375s
(k) t= 0.425 s (l) t= 0.45 s

169
(m) t= 0.475s (n) t=0.5s
Figure 4.4 Changes in the Ip for various time steps during diastolic flow conditions
(Arefin and Morsi, 2014)
From the images in Figure 4.4, from the initiation of the diastolic flow conditions, Table
4.1 summarizes the sequence of events that took place.
Table 4.1 Sequence of events pertaining to figure 4.4 Time Observations
t= 0.025 s Fluid starts to move into the cavity of the LV through the inlet/ mitral orifice. After
starting to fill the cavity; when t= 0.025s, the inlet velocity was determined to be
approximately 0.3 m/s and the basal pressure (which was close to the inlet region) was
observed to be much higher in magnitude relative to the apical pressure of the LV. At
this period of time, a negative pressure gradient was developed in the ventricle apex
and this occurred because the inlet velocity/flow velocity had not yet reached the apical
region of the LV.
t=0.05 s The chamber started to fill with the rise in the inlet velocity waveform and the negative
pressure gradient in the ventricle apex began to disappear.
t= 0.075 s When the inlet velocity (when U= 0.8 m/s) reached its first peak (with the time t=

170
0.075s, Peak of the E-wave) the intraventricular pressure elevated in the LV cavity and
the resultant Ip was found to approximately 5.4E2 Pa in the apical region of the LV.
Additionally, it was also observed that during the peak of the E-wave, the ventricle
apex had higher intraventricular pressure than the base of the LV. Moreover, a small
vortex was detected near the outlet region of the LV (Arefin and Morsi, 2014).
t= 0.125 s Once the inflow velocity reached the peak E-wave, it started to decline and a vortex
was seen formed close to the outlet tract. During the same time step, Ip in the apical
region was found to be much higher relatively than its basal region.
t= 0.15 s With a deceleration in the inflow velocity, around 0.5 m/s when t= 0.15 s, the changes
in the intraventricular pressure were still much higher in the apical region of the
ventricle compared to its basal region. At this time the vortex, which was located
previously close to the outlet region, started to expand its shape and size and changed
its position into the centre of the cavity. Also, when the Ip reached the ventricle apex,
the tip of the LV wall produced a non-negative reflection back to its inlet velocity
wave. Hence, the intermingling of these two waves raised the apical pressure, which
was recognized as the F-wave (Arefin and Morsi, 2014, Cheng et al., 2005, Vierendeels
et al., 1999).
t= 0.2 s With further decrease in the inlet velocity (around 2 m/s, t= 0.2 s) the primary vortex
reached almost to the core of the cavity and a small vortex was seen formed near the
dead-end of the outlet region. Although the magnitude of the Ip tends to be higher in
the ventricle apex and base but the magnitude minimized compared with the previous
time step, as the inflow velocity enters into the diastasis period.
t= 0.225 s When it came into the diastasis phase, the magnitude of the transmitral flow velocity
decreased and therefore, the variations in the intraventricular pressure were apparent
inside the LV chamber. At 0.225 s, the magnitude of the inflow wave was 0.1 m/s and
during this time step, higher intraventricular pressure in the cavity was found compared
to the basal pressure.
t= 0.275 s The development of the vortex was evident and was located in the core of the LV
chamber. At the same time, the small vortex began to merge inside the cavity. As the
inflow waveform was still low, the primary vortex tended to enlarge in the centre of the
cavity.
t= 0.35 s Initially, with the elevation in the inlet velocity, the primary vortex tended to merge
with the propagation of the flow. At this time step, basal pressure was found to be

171
somewhat higher than the apical pressure.
t= 0.375 s
t= 0.425 s
t= 0.45 s
With the elevation in the inlet velocity, the magnitude of the Ip at the base of the LV
started to rise again more than that of the LV apex. A second vortex was seen appearing
close to the outlet region and the core vortex began to amalgamate with the inlet wave.
Thus, when the inlet velocity elevated, the vortex began to merge in the ventricle cavity
(Arefin and Morsi, 2014). Consequently, at the beginning of the A-wave, the
magnitude of the pressure at the ventricle base started to increase again when compared
with the apical pressure, but when it touched the pinnacle of the A-wave, the magnitude
of the apical pressure became higher when compared with the pressure at the base of
the LV.
t= 0.475 s The inflow wave decelerated again and the basal pressure decreased simultaneously.
t= 0.5 s At the end of the inflow velocity the magnitude of the Ip at the base was found to be
somewhat higher but the magnitude was still much lower compared to the pressure at
the ventricle apex (Arefin and Morsi, 2014).
All these findings and the general trends of the Ip pressure distributions (with the
variations in the magnitude of Ip starting from the ventricle base to the apex),
generation, development and merging of vortices during the diastolic flow wave inside
the LV chamber, matched closely with the findings from previously published research
(Arefin and Morsi, 2014, Cheng et al., 2005, Vierendeels et al., 1999, Nakamura et al.,
2002).
Additionally, it was noted that the Ip could be determined during the diastolic flow
conditions by three different approaches:
• Using mean pulmonary wedge pressure (MPWP)/ mean left atrial (LA) pressure.
• End-diastolic pressure of the LV (LEDP), which occurs after the onset of A-
wave.
• Pre-A LV diastolic pressure.

172
The transmitral waveform played a significant role for the LV diastolic flow
propagations and changes in the Ip (Arefin and Morsi, 2014, Courtois et al., 1988,
Nagueh et al., 2009).
4.4.3 Distributions of Wall Shear Stress (WSS)
Wall Shear Stress (WSS) was determined in order to investigate its influence on the
motion of the ventricle wall. WSS was observed on the outer surface of the ventricle
wall, demonstrated in Figure 4.5 for the filling phase. Similar to the intraventricular
pressure distribution, fourteen different time steps were chosen for the variations in the
WSS distributions.
(a) t= 0.025 s (b) t= 0.05 s

173
(c) t=0.075 s (d) t= 0.125 s
(e) t= 0.15s (f) t= 0.2 s

174
(g) t= 0.225s (h) t= 0.275 s
(i) t= 0.35 s (j) t=0.375s

175
(k) t= 0.425 s (l) t= 0.45 s
(m) t= 0.475s (n) t=0.5s
Figure 4.5 Distributions of WSS during the filling phase
The images in Figure 4.5 represent the variations in the WSS during the changes in the
transmitral flow velocity. The sequence of events is summarized in Table 4.2.

176
Table 4.2 Summary of time-step observations relating to figure 4.5 Time Observations
t= 0.025 s As the transmitral flow wave entered through the inlet region, the magnitude of the wall
shear in ventricle base started to increase. At the same time, the wall shear in the apical
region of the ventricle varied very little as the inlet velocity had not yet reached its
apex. At the side of the inlet tract, WSS tended to be much higher due to the
propagation of the inflow jet.
t= 0.05 s The WSS rose in the side of the inlet tract with the elevation in the transmitral velocity.
During the exact time step, the magnitude of the wall shear in the basal region
increased with the rise in the inflow waveform.
t= 0.075 s When the inflow velocity reached the pinnacle of the E-wave, the maximum jet flowed
through the inlet region and therefore the magnitude of WSS in the basal region
elevated once again. Also, the magnitude slightly increased in the apical region, but
maximum WSS could be found at the side of the inlet region.
t= 0.125 s After reaching the peak of the E-wave, transmitral flow velocity decelerated and
simultaneously, WSS decreased both in the basal region and apical region of the LV.
Also, the shear stress effect at the side of the inlet wall tended to decrease. At the same
time step, the magnitude of the wall shear was much higher near the dead-end of the
outlet tract. This could be attributed to the fact that the fluid which existed inside the
LV cavity which created pressure on the ventricle wall and also the development of
vortex (as reported in Section 4.4.2), which could contribute to elevating the WSS near
the outlet region.
t= 0.15 s With further decrease in the inflow velocity, the magnitudes of the WSS in the ventricle
base and apex reduced.
t= 0.2 s As the inlet velocity was very low, WSS in the apical region reduced significantly
compared to its previous time step. WSS in the basal region reduced as well but the rate
was found to be minimal.
t= 0.225 s
t= 0.275 s
As the inlet waveform entered into the diastasis phase; the magnitude of the WSS in the
ventricle base reduced slightly but the magnitude in the ventricle apex increased. This
can be ascribed to the fact that, during the diastasis period, the fluid inside the chamber
tended to be in the centre and the apex of the ventricle and, therefore, WSS in the apical
region elevated. However, with the progression in the diastasis period, WSS tended to
rise in the basal region of the LV due to the inflow velocity waveform (Figure 4.3).

177
t= 0.35 s
t= 0.375 s
Once again, elevation in the inflow jet increased the magnitude of the WSS in the basal
region compared to its apical region. As the transmitral velocity increased, WSS in the
basal region decreased. This could be attributed to the inflow jet creating pressure
directly on the inlet region and hence, the reduction of the WSS in the basal region was
observed. Conversely, the maximum magnitude of the WSS was located at the side of
the inlet region.
t= 0.425 s
t= 0.45 s
t= 0.475 s
A much higher magnitude in the inlet was observed at the peak of the A-wave. After
reaching the peak of the A-wave, the inflow jet decelerated once more and the
magnitude of the WSS decreased in the inlet region.
t= 0.5 s At the end of the filling phase, WSS in the apical region and the basal region was found
slightly increasing relative to previous time steps.
The magnitudes of the WSS during the peak E-wave, diastasis and A-wave were
obtained in the ventricle apex and were approximately 4 Pa, 1.38 Pa and 1.63 Pa
respectively. In the ventricle base they were 5.7 Pa, 1.4 Pa and 2 Pa respectively
(Arefin and Morsi, 2014).
4.4.4 Distributions of Velocity
The primary features of the velocity mapping inside the cavity are demonstrated in
figure 4.6. The XY cross-sectional plane was set in the LV model and by using the
velocity vectors during the diastolic flow conditions, the variations in the flow pattern
were determined. Similar to the distribution of pressure, the flow pattern is also
illustrated for fourteen different time steps by considering the inlet, which is fully open,
and the outlet, which is completely closed, during the diastolic flow conditions (Arefin
and Morsi, 2014).

178
(a) t= 0.025 s (b) t= 0.05 s
(c) t=0.075s (d) t= 0.1s

179
(d) t= 0.125 s
(e) t= 0.15s
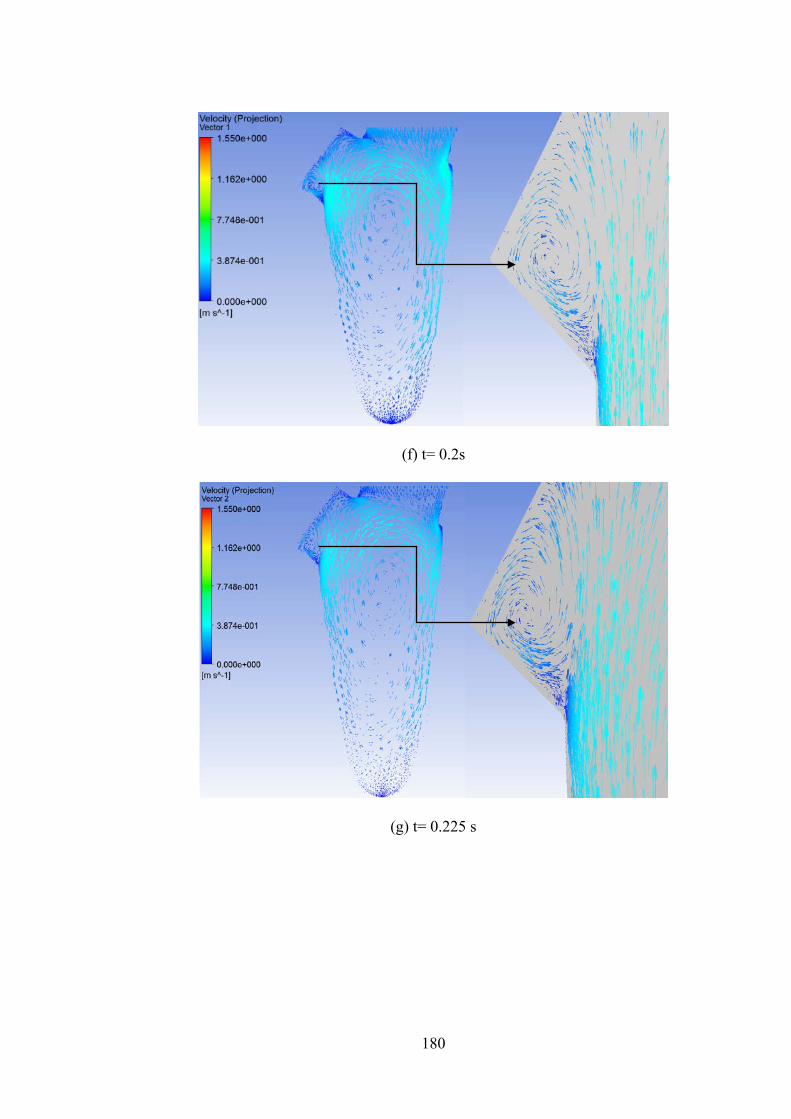
180
(f) t= 0.2s
(g) t= 0.225 s

181
(h) t= 0.275 s
(i) t= 0.3s

182
(j) t= 0.375 s
(k) t= 0.4s

183
(l) t= 0.45 s
(m) t= 0.475s

184
(n) t= 0.5s
Figure 4.6 Illustration of velocity distributions during diastolic flow conditions
(Arefin and Morsi, 2014)
The time-step observations pertaining to Figure 4.6 are contained in Table 4.3.
Table 4.3 Time-step observations pertaining to figure 4.6 Time Observations
t= 0.025 s At the initiation of the diastolic phase (Figure 4.6), the fluid started to enter the LV
chamber and it began to fill.
t= 0.05 s Due to the rise in the inflow jet a clockwise (CW) ring shaped vortex was seen forming
near the outlet tract.
t= 0.075 s The inlet velocity reached the pinnacle of the E-wave with a magnitude of approximately
0.8 m/s. At this time, maximum inflow velocity entered through the mitral orifice/ inlet
and the jet maintained its flow from the basal region of the LV to the apical region. Due to
this flow of E-wave, the ring shaped, CW vortex changed its location/ shifted its position
slightly downwards but still remained near the outlet tract. Also, the magnitude of flow
velocity was found to be higher in the anterior section of the LV cavity compared to its
posterior region from the mitral orifice. Once the inflow velocity reached the peak of the

185
E-wave it started to decelerate. Because of this, the adherence vortex, which was
developed previously, changed its place a little from the dead-end of the outflow tract and
started to expand simultaneously (Arefin and Morsi, 2014).
t= 0.125 s After reaching the pinnacle of the E-wave, inflow velocity minimized and the vortex
moved towards the core of the LV chamber.
t= 0.15 s The primary ring shaped, CW vortex shifted once more and elongated into the mid of the
LV but a second vortex, which was ring shaped but counter clockwise (CCW), developed
near the dead-end of the outlet region.
t= 0.2 s The inlet flow velocity of 0.2 m/s decelerated further and, as shown in Figure 4.6 (f), the
shape of the vortex enlarged and changed its position to the core of the cavity.
t= 0.225 s The primary vortex was found at the core of the chamber and the secondary/CCW vortex
tended to increase in size and shape.
t= 0.275 s
t= 0.3 s
The primary vortex slightly moved in the anterior direction as the inflow velocity was
minimal and the secondary vortex elongated but stayed close to the outlet tract.
Subsequently, at the end of the diastasis, this ring shaped vortex began to elongate once
more but, at the same time step, an additional counter-clockwise (CCW) vortex originated
at the anterior position of the outlet region, which also enlarged simultaneously (Arefin
and Morsi, 2014).
t= 0.375 s With the rise in the inflow jet, the primary vortex shifted its position again in the core of
the chamber and the CCW vortex was slightly enlarged near the outlet region.
t= 0.4 s
t= 0.45 s
A third vortex, which was ring shaped and CW, developed in the vicinity of the mitral
orifice and the aortic orifice. At the pinnacle of the A-wave, the inlet flow velocity began
to rise once more and because of this, the fundamental/primary vortex began to
amalgamate in the LV cavity. Simultaneously, the third vortex started to enlarge and shift
its position towards the centre of the LV and the second vortex tended to reduce its size
and shape.
t= 0.475 s After touching the peak of the A-wave, the inflow velocity started to decelerates again and
the second vortex stayed in the close outlet tract. However, the ineffective/weak third
vortex once again moved its position slightly to the core of the LV.
t=0.5 s At the end of the A-wave the feeble third vortex completely amalgamated with the

186
propagation of the inlet flow velocity but a primary ring-shaped vortex was formulated
once again at the core of the cavity. The magnitude of the maximum flow velocity of 1.55
m/s was acquired during the filling cycle (Arefin and Morsi, 2014).
The general trends concerning the flow characteristics, formation and/or evolution,
shifting, amalgamation/merging of vortices once again matched closely with previously
published research (Arefin and Morsi, 2014, Cheng et al., 2005, Watanabe et al., 2004,
Nakamura et al., 2002, Vierendeels et al., 1999, Lassila et al., 2012, Verdonck and
Vierendeels, 2002).
Although, the evolution of vortices from the simulations were in line with the results
observed from Cheng et al., 2005, the simulated results here did not directly coincide
with the developments of the vortices reported from the same group. This can be
ascribed to the fact that, in the late diastolic phase, the flow pattern could be altered
because of the utilization of different computational/simulation methods (Arefin and
Morsi, 2014, Cheng et al., 2005).
4.4.5 Structure Simulation using Total Mesh Displacement (TMD)
Similar to the pressure and the velocity distributions of the LV cavity, TMD was also
determined by considering the XY cross sectional plane inside the chamber. Figure 4.7
illustrates the variations in the TMD by taking the wide-open inlet/ mitral orifice and
fully closed outlet/ aortic orifice during the filling phase (Arefin and Morsi, 2014).

187
(a) t= 0.025 s (b) t= 0.05 s
(c) t= 0.075s (d) t= 0.125 s
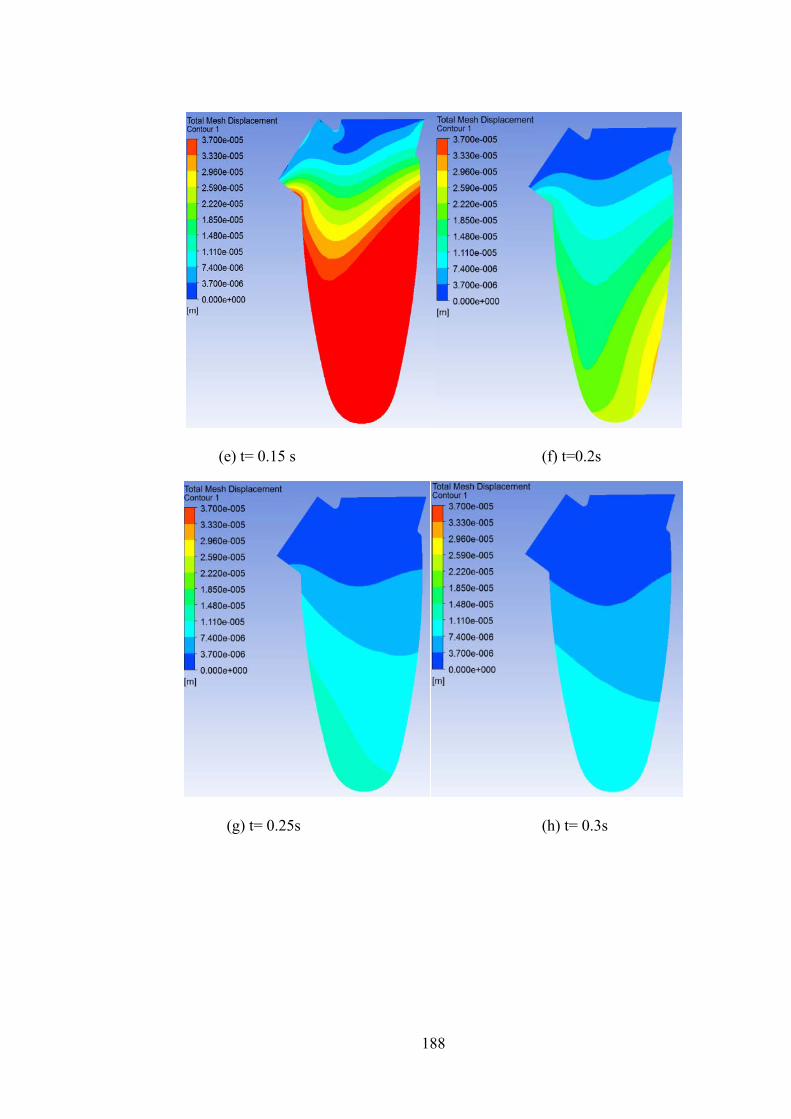
188
(e) t= 0.15 s (f) t=0.2s
(g) t= 0.25s (h) t= 0.3s

189
(i) t= 0.325 s (j) t= 0.375 s
(k) t=0.4s (l) t= 0.45 s

190
(m) t= 0.475s (n) t=0.5s
Figure 4.7 Illustration of total mesh displacement (TMD) during diastolic flow
conditions (Arefin and Morsi, 2014)
From the images in Figure 4.7; at the beginning of the filling phase, the volume in the
LV cavity started to increase with the progression of the flow propagation. For instance,
at the onset of the filling wave, the LV chamber was empty and with the rise in the
inflow velocity, the cavity started to fill. During the pinnacle of the E-wave, the jet
progressed through the inlet of the LV with maximum flow velocity and because of this,
a much higher magnitude of displacement was obtained in the ventricle apex compared
to the ventricle base. The magnitude in the apical region of the LV remained higher due
to the intraventricular pressure developed on the LV wall.
As soon as the inflow velocity wave entered into the diastasis phase, the value of the
TMD decreased in the tip of the ventricle, compared to its previous time steps (t= 0.2 s).
During the time step t= 0.25 s the displacement changed from the posterior section of
the LV to the anterior section in the ventricle apex, as shown in the ventricle-contour
(Figure 4.7 (g)) (Arefin and Morsi, 2014). At the end of the diastasis stage, the
magnitude of the displacement was found to be minimal due to the lower inlet velocity.
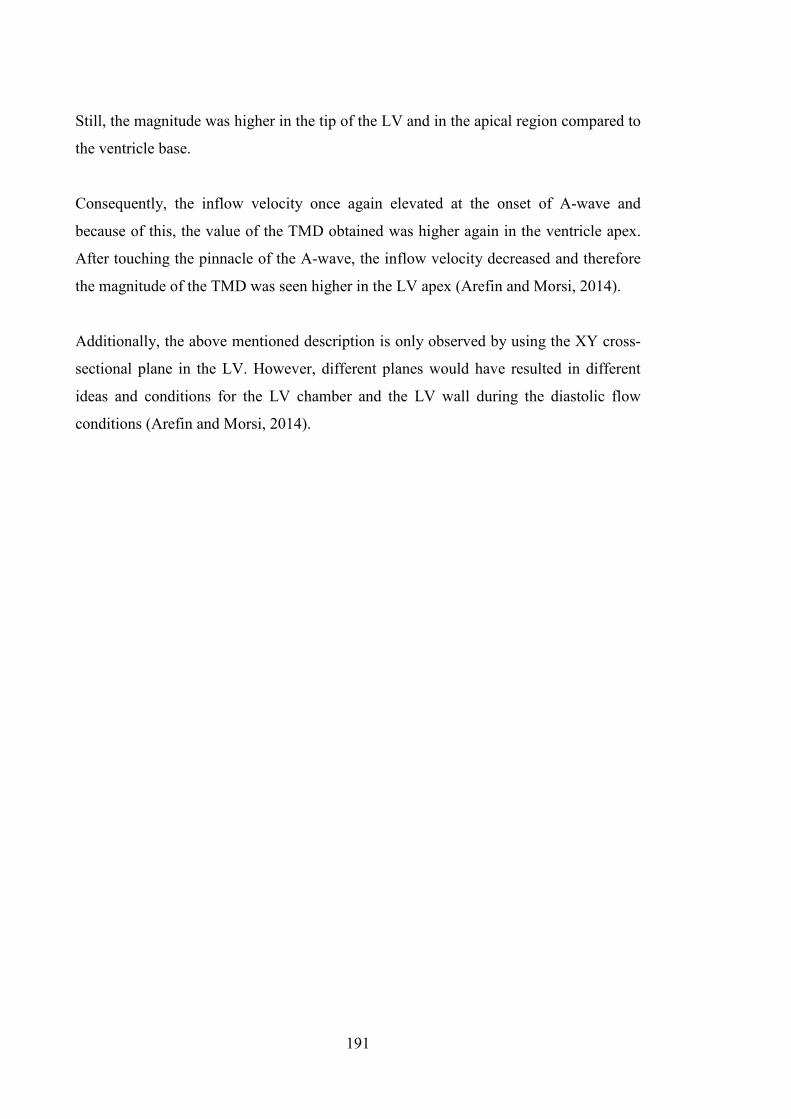
191
Still, the magnitude was higher in the tip of the LV and in the apical region compared to
the ventricle base.
Consequently, the inflow velocity once again elevated at the onset of A-wave and
because of this, the value of the TMD obtained was higher again in the ventricle apex.
After touching the pinnacle of the A-wave, the inflow velocity decreased and therefore
the magnitude of the TMD was seen higher in the LV apex (Arefin and Morsi, 2014).
Additionally, the above mentioned description is only observed by using the XY cross-
sectional plane in the LV. However, different planes would have resulted in different
ideas and conditions for the LV chamber and the LV wall during the diastolic flow
conditions (Arefin and Morsi, 2014).

192
4.5 Summary
The simulations indicated that the variations in the Ip within the chamber of the LV
occurred due to the changes in the LV wall during the E-wave and the A-wave. Also,
the value of the Ip in the ventricle apex was much higher compared to the Ip in the
ventricle base during the pinnacle of the early filling wave; atrial contraction wave, and
the diastasis. The basal pressure was higher at the onset of the early filling wave and the
atrial contraction wave. The development and merging of vortices were evident during
the filling phase inside the cavity of the LV (Arefin and Morsi, 2014).
WSS increased with the rise in the inflow velocity of the early filling wave and atrial
contraction phase, but vice-versa during the slow filling phase/diastasis (Arefin and
Morsi, 2014). During the filling phase, the fluid inside the ventricle chamber was
thought to be responsible for developing WSS. Moreover, similar effects had also been
found in the structure simulations of the LV where, with the rise in the inlet waveform
elevated and during the deceleration of the inflow velocity, the magnitudes of the
displacement were observed to be reduced.
The evolution of vortices, including the development, shifting and amalgamation, were
observed inside the LV cavity during various time steps of the inlet flow propagation.
However, it was determined that by using different simulation/ computational
approaches the results could vary during the late-diastolic period (Arefin and Morsi,
2014).
All these cardiac conditions were generally in line with previously published research
and clinical results. Also the outcomes of this simulation provided useful insights into
physiological and hemodynamical variations, which included (Arefin and Morsi, 2014):
• The flow pattern
• Distribution of Ip
• Distribution of WSS
• The structural displacement during the filling conditions

193
From these investigations, it was determined that (Arefin and Morsi, 2014):
• The maximum value of the intraventricular pressure (Ip) was 5.4E2 Pa
• The magnitude of WSS was 5.7 Pa
• The flow velocity was 1.55 m/s
• The maximum amount of displacement in the LV apex was found to be 3.7E-5
m during the pinnacle of the early filling wave
This investigation and the magnitudes of various parameters during the diastolic
conditions will be helpful in developing next generation VAD system.

194
Chapter 5
Numerical Analysis of the Left Ventricle during
Diastole Phase: Angular Variations between the
Mitral and Aortic Orifice

195
5.1 Overview
The main objective of the research documented in this chapter was to determine the
significance of the hemodynamic characteristics and the physiological alterations of the
left ventricle (LV), by varying the angles between the aortic and the mitral orifice
during the filling phase. During the simulations, three different angles were considered
and varied, as:
• 50°
• 55°
• 60°
Once again, similar to the simulations in Chapter 3 and Chapter 4, Fluid Structure
Interaction (FSI) was utilized and the results were also exhibited and analyzed in terms
of:
• Flow pattern
• Intraventricular pressure (Ip) distributions
• Wall shear stress (WSS) distributions
• Deformation of the structure
The 3D LV model and the required boundary conditions used here were similar to
Chapter 4. Again, similar to Chapter 3 and Chapter 4, the Navier-Stokes equations and
the Arbitrary Lagrangian Eulerian (ALE) methods were utilized to couple the fluid and
solid domains of the geometry. Subsequently, the simulated results were analyzed and
compared with previously published research work.
This chapter concludes by providing the findings from the simulations, which highlight
the significance of the hemodynamic features and structural changes brought about by
changing the degree of mitral and aortic orifices. As with previous analyses, these
would be useful for the development of a next generation VAD device.

196
5.2 Introduction
It was well-known that a small variation in the LV structure could change the overall
hemodynamic performance. Even though there were various imaging tools available
which could specify the qualitative differences in the flow dynamics inside the cavity of
the LV, the hemodynamic features achieved by varying the angles between the mitral
and aortic orifice still had to be investigated. In this research, the angles between the
mitral and aortic orifice were varied to 50°, 55° and 60° and the overall changes in the
structural and hemodynamic changes are described.
From the previous investigations in Chapter 3 and Chapter 4, it was evident that the
utilization of the FSI method was well established and offered significant features that
would enable researchers to determine and understand various physiological and clinical
aspects of the simulated models. The FSI technique was employed here in order to
determine the physiological and clinical significance of different angular variations in
the inlet and outlet region of the 3D, physiologically correct LV during filling
conditions.
During the application of these numerical approaches, an analysis of:
• The flow dynamics, including the evolution, merging and shifting of vortices
• Pressure distributions
• Wall Shear Stress (WSS) distributions
• Structural variations using Total Mesh Displacement (TMD) characteristics
was undertaken and documented. The primary features of the hemodynamic behaviour
and physiological displacement during diastolic conditions are subsequently
highlighted.

197
5.3 Computational Approaches
5.3.1 Overview
The LV geometry deployed here for all the simulations was similar to the one
documented in Chapter 4 but here the angles between the mitral and aortic orifices were
varied (50°, 55° and 60°). Once the required geometry was selected, boundary
conditions and inlet velocity wave/transmitral velocity profile (U) parameters similar to
those in Chapter 4 were implemented on the LV model. Subsequently, pressure
distributions, velocity distributions, WSS distributions and structural displacement were
investigated and determined.
5.3.2 Geometry Extraction
As noted above, a similar geometry of the LV to that illustrated in Chapter 4 [Figure 4.1
(a) and Figure 4.1 (b)], was utilized here for the simulations. Also, it was already proven
that by providing suitable boundary conditions and physiological parameters, a
simplified geometry could produce accurate results (Arefin and Morsi, 2014, Nakamura
et al., 2002, Watanabe et al., 2004, Cheng et al., 2005, Zheng et al., 2012). This
geometry was varied angularly between the mitral and the aortic orifices (50°, 55° and
60°) using SolidWorks 2012. Figure 5.1 demonstrates the LV model with the angular
discrepancies of 50°, 55° and 60° between the inlet and outlet.

198
(a)
(b)

199
(c)
Figure 5.1 LV Model with the angular differences of (a) 50°, (b) 55° and (c) 60°
between the inlet and outlet (SolidWorks 2012)
5.3.3 Meshing Statistics and Mesh Independency Trials
Once again, after a model was developed using SolidWorks 2012, it was then
introduced into ANSYS 14.5. Suitable meshing was then implemented and required
boundary conditions were allotted. For the current simulations, the “Tetrahedrons
Method using Patch Conforming Algorithm” was implemented for the solid and fluid
domains separately. Again, line control properties were utilized, similar to the research
documented in Chapter 4, to observe the differences in the flow velocity (Arefin and
Morsi, 2014, Kouhi, 2011).
Consequently, a mesh independency trial was executed using these line control
parameters and the variations in the fluid velocity were determined for successive nodes
and elements, both for the solid and fluid domains until convergence was achieved.
Figure 5.2 demonstrates the mesh independency trials by implementing the fluid

200
velocity. In this trial, three different meshing categories (coarse, medium and fine) were
chosen. After implementing these categories it was verified that:
• 5436 nodes
• 2743 elements
were assumed to be ideal for the solid region and:
• 2467 nodes
• 1331 elements
were considered to be ideal for the fluid domain. These nodes and elements were chosen
for the medium type of mesh. Also, the convergence criterion for the fluid was taken to
be 10-4 and for the coupling data transfer it was assumed to be 10-2, similar to the
simulations documented in Chapter 4 (Arefin and Morsi, 2014).
Figure 5.2 Mesh independency trial using fluid flow velocity
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0 0.02 0.04 0.06 0.08
Mesh Type-Coarse
Mesh Type-Fine
Mesh Type-Medium

201
5.3.3 Boundary Conditions
Transmitral flow velocity (U in m/s) was provided through the inlet region for all three
geometries. Moreover, the boundary conditions for the solid and fluid region remained
similar, as reported in Chapter4 (Figure 4.3), for the simulations (Arefin and Morsi,
2014). Moreover, with the inlet velocity profile, three states of the filling phase were
identified, as described in Chapter 4. These comprised:
• Two peaks, being the early filling wave (E-wave, at t= 0.08 s) and atrial
contraction wave (A-wave, at t= 0.44 s) with the velocity of 0.8 m/s and 0.4 m/s
correspondingly.
• In between the two peaks, the middle phase was recognized as the diastasis/slow
filling phase (0.22<t<0.3s) (Vierendeels et al., 1999, Cheng et al., 2005, Arefin
and Morsi, 2014).
As per the boundary details utilized in Chapter 4, the ventricle wall was considered to
be homogeneous and isotropic, with:
• A density of 1.2 g/cm3
• Elastic modulus of 0.7 MPa
• Poisson’s Ratio with the magnitude of 0.4
Also, during the simulations, Newtonian fluid flow was considered incorporating:
• Fluid density of 1050 kg/m3
• Viscosity of 0.0035 Pa.s
which also comprised no-slip boundary conditions. The flow property was assumed to
be laminar (Vierendeels et al., 1999, Cheng et al., 2005, Lassila et al., 2012, Arefin and
Morsi, 2014, Saber et al., 2003). Once again, for the coupling data transfer control, the
under relaxation factor was fixed to 0.75.

202
5.4 Simulation Results
5.4.1 Overview
The results are shown here in the form of velocity distributions incorporating:
• The evolution, merging and shifting of vortices
• Intraventricular pressure distributions (Ip)
• Distribution of wall Shear Stress (WSS)
• Variations in the structural displacement using total mesh displacement (TMD)
during the filling phase
5.4.2 Distributions of Velocity
5.4.2.1 Angular Difference of 50°
The images in Figure 5.3 illustrate the flow/hemodynamic characteristics inside the
chamber of the LV during the diastolic flow conditions. Velocity mapping was utilized
to epitomize the variations in the flow pattern, where the velocity vectors were plotted
on the XY cross-sectional plane of the LV, for the angular difference of 50°. The flow
profiles are illustrated by taking the mitral orifice wide open and the outlet region
completely closed. Fourteen different time steps are presented here, which were
obtained from the alterations in the inlet velocity waveform (U). Table 5.1 presents the
summary of the results during three states.

203
0.025s 0.05 s
0.075s 0.125s

204
0.175s 0.2s
0.25 s 0.275 s

205
0.3 s 0.35 s
0.4 s 0.45 s

206
0.475 s 0.5 s
Figure 5.3 Velocity mapping for the angular difference of 50°
Table 5.1 Observations pertaining to figure 5.3 Conditions Observations
E-wave During the initiation of the filling cycle, fluid began to flow concurrently through the
inlet into the LV cavity. Initially, the inflow velocity was minimal and when it reached
the pinnacle of the E-wave the maximum inflow velocity flowed through the wide open
inlet and the fluid rapidly started to flow from the basal region to the apical region of the
LV. During this time step, the flow velocity magnitude was higher relative to the
posterior position from the inlet region of the LV. Once it touched the pinnacle of the E-
wave, the inflow velocity began to decrease and during that time, fluid inside the
chamber started to develop a wake vortex near the vicinity of the mitral and aortic
orifice. A maximum velocity of 8.96E-1 m/s was found to be at the basal region of the
LV during the time step of t= 0.075s (close to peak E-wave). After touching the pinnacle
of the E-wave, the velocity of the inflow jet started to decrease and hence the magnitude
in the basal region started to decrease as well. The vortex was found to be enlarging and
shifting its position slightly towards the middle of the cavity (t= 0.125 s). With a further
decrease in the inlet velocity (when t= 0.175 s and t= 0.2 s) the primary vortex was still
found to be elongating and moving towards the centre of the chamber.
Diastasis When the inlet velocity entered into the diastasis period, inflow velocity was minimal
and therefore a change in the vortex location was observed inside the cavity. During that

207
time (t= 0.25 s), the vortex changes its location from the basal region into the core of the
chamber. The maximum velocity was found to be approximately 3E-1 m/s around the
core of the vortex.
A-wave At the onset of the A-wave (t= 0.3 s), the inflow velocity started to increase and
subsequently, with the rise in the inflow velocity (t= 0.35 s), due to the atrial contraction
wave, this vortex slowly amalgamated with the fluid which entered through the inlet
region. Inflow velocity decreased when it reached the peak of the A-wave but, once
again, the flow velocity decreased after reaching the peak. At the end of the filling
phase, a vortex developed again in the centre of the LV chamber. A maximum velocity
of approximately 4.48E-1 m/s was obtained during the time step, t= 0.045 s.
5.4.2.2 Angular Difference of 55°
Figure 5.4 illustrates the velocity distributions inside the cavity during the filling period
with the angular variation of 55° between the inlet and outlet region. It should be noted
that a similar approach and inlet velocity propagation were implemented to obtain the
changes in the hemodynamic characteristics inside the LV. Table 5.2 presents the
summary of the results.
0.025 s 0.05 s

208
0.075 s 0.125 s
0.175 s 0.2 s

209
0.25 s 0.275 s
0.3 s 0.35 s

210
0.4 s 0.45 s
0.475 s 0.5 s
Figure 5.4 Velocity mapping for the angular difference of 55°

211
Table 5.2 Observations pertaining to figure 5.4 Conditions Observations
E-wave At the onset of the simulation, fluid began to flow through the inlet region. Primarily, the
inflow velocity was minimum but with the rise in the inlet velocity (for example, t=
0.075 s, peak E-wave) the inflow jet got driven from the basal region of the LV towards
the apical region. During that time, a weak vortex originated close to the outlet region.
After touching the pinnacle of the E-wave, the inflow velocity decreased and
simultaneously, the weak vortex slightly elongated and shifted its position close to the
outlet tract. The maximum magnitude of the inflow velocity was found to be
approximately 1.02 m/s during the pinnacle of the E-wave.
Diastasis When the inlet velocity reached its diastasis period, an adherence vortex originated in
the core of the cavity. This weak vortex enlarged slightly during the diastasis period, but
the maximum velocity was approximately 2.55E-1 m/s around the centre of the vortex,
during the time step of (t= 0.25 s and t= 0.275 s).
A-wave Again, with the rise in the inlet velocity, the resultant adherence vortex began to
weaken/merge, but a ring shaped vortex developed close to the outlet region. At the end
of the diastolic period, this newly developed vortex enlarged once more and changed its
location towards the centre of the LV chamber. Also, during the peak of the A-wave, the
maximum magnitude of the inflow velocity was approximately 5.1E-1 m/s with the time
step of t= 0.45 s.
5.4.2.3 Angular Difference of 60°
A similar range of incidents were observed from the investigation of the angular
difference of 60° between the mitral and aortic region. Figure 5.5 demonstrates velocity
mapping of the LV chamber during the diastolic phase for the angular difference of 60°
between inlet and outlet tract. Also, a similar method and inlet waveform were utilized
to observe the primary discrepancies in the hemodynamic features for fourteen differnet
time steps inside the LV cavity. Table 5.3 demonstrates the summary of the results.

212
0.025 s 0.05 s
0.075 s 0.125 s

213
0.175 s 0.2 s
0.25 s 0.275 s

214
0.3 s 0.35 s
0.4 s 0.45 s

215
0.475 s 0.5 s
Figure 5.5 Velocity mapping for the angular difference of 60°
Table 5.3 Observations pertaining to figure 5.5 Conditions Observations
E-wave Fluid started to flow inside the cavity at the beginning of the filling phase. As the inlet
velocity increased, the flow velocity increased inside the LV chamber and the jet started
to move from the basal region to the apical region. At the peak of the E-wave (t= 0.075
s) a maximum flow velocity of 9.39E-1 m/s was observed in the mitral orifice area.
Also, during that time period, a vortex developed near the outlet tract. After reaching the
peak of the E-wave, the flow velocity started to decrease and simultaneously the vortex
slightly elongated and shifted its position towards the core of the chamber.
Diastasis When the inlet waveform entered into the diastasis phase, the adherence vortex in the
core of the cavity tended to enlarge with the increase in the time steps (t= 0.25 s and t=
0.275 s). A maximum of approximately 2.35E-1 m/s was found around the vortex with
the time step of t= 0.25 s.
A-wave After the diastais period, fluid flow increased and with the rise in the inlet velocity, the
vortex started to merge with the flow propagation. When the inlet velocity reached the
peak of the A-wave, the vortex merged with the fluid inside the cavity. After reaching
the peak of the A-wave, flow velocity decelerated and at the end of the filling phase, the
vortex developed and enlarged once again at the centre of the LV chamber. During the

216
time step of t= 0.45 s a maximum velocity of approximately 5E-1 m/s was noted in the
inlet region at the peak of the A-wave.
5.4.3 Wall Shear Stress (WSS) Distributions
5.4.3.1 Angular Difference of 50°
The images in Figures in 5.6 demonstrate the variations in the wall shear stress (WSS)
of the LV during diastolic flow conditions in twelve different time steps. The WSS was
examined in order to understand the influence it exerts on the motion of the LV wall. In
doing so, the exterior surface of the LV wall was considered for the demonstration of
the WSS effect. Initially, the effect was demonstrated for an angular difference of 50°
between the inlet and outlet region. Also, the boundary conditions and inlet velocity
profile that were implemented in the inlet orifice were similar to those in velocity
mapping. Table 5.4 provides the summary of the results.
0.025 s 0.075 s

217
0.1 s 0.15 s
0.2 s 0.25 s

218
0.3 s 0.35 s
0.4 s 0.45 s

219
0.475 s 0.5 s
Figure 5.6 Wall shear stress (WSS) distributions for the angular difference of 50°
Table 5.4 Observations pertaining to figure 5.6 Conditions Observations
E-wave When the inlet waveform entered the mitral orifice of the LV, magnitudes in the
ventricle base started to elevate and with a further rise in the inlet velocity, the WSS
elevated in the inlet tract and in the basal region of the ventricle. Subsequently, when the
inflow waveform reached the peak of the E-wave, maximum, WSS was found to be in
the basal region of the LV. After reaching the peak of the E-wave (t= 0.075 s), the
inflow waveform started to decelerate and simultaneously, the WSS in the inlet tract
began to decrease. At the same time, the WSS in the basal region tended to reduce as
well. The maximum magnitude of the WSS was around 3 Pa in the basal region with the
time steps of t= 0.075 s and t= 0.1 s.
Diastasis When the inlet waveform reached its diastasis phase, the flow velocity decreased and the
effect of the WSS significantly reduced in the basal region and in the inlet tract.
Although the magnitude of the WSS substantially reduced in the diastasis region, the
maximum magnitude of the WSS was approximately 6E-1 Pa in the basal region of the
LV wall with the time step of t= 0.25 s.
A-wave The flow velocity elevated once again and hence the effect of the WSS elevated. It was
also evident that with the rise in the inlet velocity the magnitude of the WSS rose once

220
again in the inlet tract and in the basal region of the LV wall. When the inflow velocity
reached the peak of the A-wave, maximum WSS was found to be approximately 1.8 Pa
in the base, with the time step of t= 0.45 s. At the end of the filling wave, the influence
of the WSS reduced once again in the inlet region of the LV.
5.4.3.2 Angular Difference of 55°
WSS distributions for the angular variation of 55° between the aortic and mitral orifices
of the LV wall during the diastolic flow conditions are illustrated in Figure 5.7. Once
again, similar boundary conditions and inlet waveform were employed on the LV to
obtain the WSS effect on the ventricle wall. Table 5.5 provides the summary of the
results.
0.025 s 0.075 s

221
0.1 s 0.15 s
0.2 s 0.25 s

222
0.3 s 0.35 s
0.4 s 0.45 s

223
0.475 s 0.5 s
Figure 5.7 Wall shear stress (WSS) distributions for the angular difference of 55°
Table 5.5 Observations pertaining to figure 5.7 Conditions Observations
E-wave With the rise in the inlet waveform, the influence of the WSS was much higher on the
basal region of the LV wall. When the inlet velocity reached the peak of the E-wave (t=
0.075 s), maximum WSS was on the base of the LV wall. Moreover, after reaching the
peak of the E-wave, with the deceleration in the inlet waveform, the effect of the WSS
also decreased (t= 0.1 s, t= 0.15 s and t= 0.2 s). On the other hand, with the time step of
t= 0.075s and t= 0.1 s, the maximum magnitude of WSS was approximately 3 Pa on the
basal region of the LV wall.
Diastasis When the inlet velocity entered into the diastasis phase, the effect of the WSS was
reducing on the centre of the LV wall and on the inlet tract. Also, the magnitude dropped
in the basal region of the LV wall. With the time step t= 0.25 s, the maximum magnitude
of WSS was approximately 6E-1 Pa on the centre of the LV wall.
A-wave With the rise in the inlet waveform, for example, during the initiation of A-wave, flow
velocity started to elevate in the beginning and, hence, the WSS effect on the ventricle
base started to rise once again. At the same time, the influence of the WSS was
increasing on the centre of the LV wall and close to the apical region of the LV. The
maximum magnitude of the WSS was approximately 3 Pa once again, close to the basal

224
region of the LV wall. At the end of the diastolic conditions, the effect of WSS
minimized but was somewhat apparent on the centre of the LV wall.
5.4.3.3 Angular Difference of 60°
The images in Figure 5.8 demonstrate the WSS distibutions on the LV wall in twelve
different time steps during the diastolic flow conditions. Similar boundary conditions
and inlet velocity were employed for the angular difference of 60° between the inlet and
outlet regions. Table 5.6 presents the summary of the results.
0.025 s 0.075 s

225
0.1 s 0.15 s
0.2 s 0.25 s

226
0.3 s 0.35 s
0.4 s 0.45 s

227
0.475 s 0.5 s
Figure 5.8 Wall shear stress (WSS) distributions for the angular difference of 60°
Table 5.6 Observations pertaining to figure 5.8 Conditions Observations
E-wave At the beginning of the diastolic condition, inflow velocity was minimal and with the
rise in the transmitral velocity, the influence of WSS on the LV wall rose and was
increasing mainly on the inlet tract and on the base of the LV wall. When the inlet
waveform reached the peak of the E-wave (t= 0.075 s), maximum WSS was near the
basal region of the LV wall. After touching the peak of the E-wave, inflow jet velocity
started to decelerate and influence of the WSS on the inlet tract and on the centre of the
cavity of the LV wall tended to reduce. However, maximum WSS was approximately 3
Pa close to the basal region of the LV wall with the time steps of t= 0.075 s and t= 0.1 s.
Diastasis Once the inflow velocity reached into the diastasis period, minimal inflow velocity
entered through the mitral orifice. As a result, the effect of the WSS reduced mainly on
the inlet tract and on the centre of the LV wall. Once again, 6E-1 Pa of maximum WSS
was found near the basal region of the LV wall.
A-wave When the inflow wave entered into the A-wave, the inlet velocity rose once again and
therefore, the effect of the WSS started to elevate again. Variations in the WSS
distributions were again on the inlet tract and on the basal region of the LV wall. The
maximum magnitude of WSS was approximately 1.8 Pa near the basal region of the LV

228
wall (t= 0.45 s). With further decrease in the inlet velocity, the magnitude of the WSS
was decreasing as well mainly on the inlet tract and on the basal region of the LV wall.
5.4.4 Distributions of Pressure
5.4.4.1 Angular Difference of 50°
The images in Figure 5.9 illustrate the variation in the intraventricular pressure (Ip)
inside the LV cavity during the filling phase in fourteen different time steps. Similar to
the velocity mapping in Section 5.4.2, an XY cross-sectional plane was taken inside the
ventricle for the angular difference of 50° to determine the changes in the Ip. Once
again, the variations in the Ip were obtained by considering the mitral/inlet orifice
completely open and the outlet/aortic orifice fully closed. Table 5.7 presents the
summary of the results.
0.025s 0.05 s

229
0.075 s 0.125 s
0.15 s 0.2 s
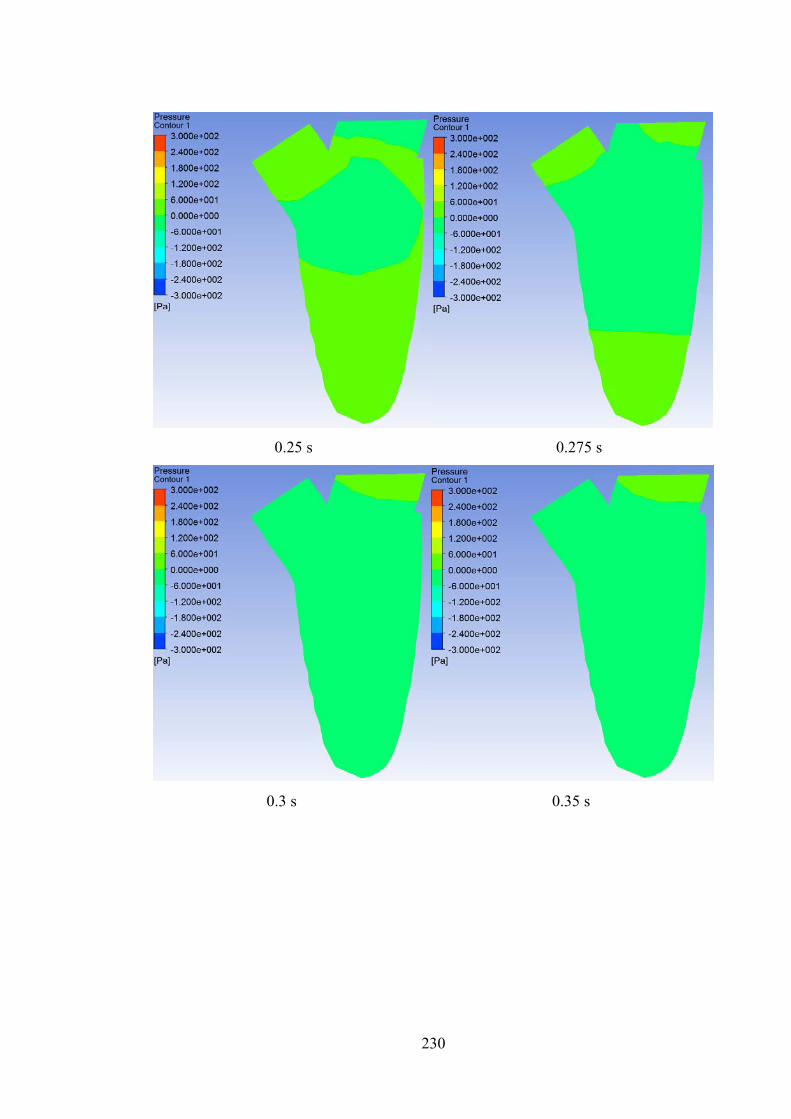
230
0.25 s 0.275 s
0.3 s 0.35 s

231
0.4 s 0.45 s
0.475 s 0.5 s
Figure 5.9 Intra-ventricular pressure (Ip) distributions for the angular difference of
50°

232
Table 5.7 Observations pertaining to figure 5.9 Conditions Observations
E-wave At the onset of the filling phase, the jet started to enter through the inlet and during the
time step of t= 0.025 s, the pressure inside the ventricle started to rise in the mitral
orifice. With further rise in the inflow velocity, the Ip pressure elevated in the basal
region of the ventricle and the jet started to move towards the apical region. The
magnitude of the Ip started to elevate in the apical region as well (t= 0.05 s). When the
inlet velocity touched the pinnacle of the E-wave, maximum jet entered through the inlet
(t= 0.075 s). Simultaneously, changes in the Ip in the ventricle apex also increased but
much higher Ip was obtained in the apical region, with a magnitude of approximately
2.4E2 Pa. After reaching the peak of the E-wave, inflow velocity started to decelerate
and hence, the magnitude of the Ip in the basal region began to decrease as well.
However, the magnitude of the Ip in the apical region was increasing with a value of
approximately 3E2 Pa (t= 0.125 s). Subsequently, with further decrease in the E-wave
velocity, the magnitude in the basal and the apical region started to decrease as well (t=
0.15 s and t= 0.2 s).
Diastasis When the transmitral velocity (U) reached the diastasis region, Ip in the apical region
was much higher compared to its basal region (t= 0.25 s). This comparison was noticed
due to the minimal inlet flow velocity. Also, a vortex developed in the centre of the
ventricle. During the time step of t= 0.275 s, the magnitude of the apical and basal
pressure was found to be decreasing but the magnitude of the apical pressure was still
higher compared to the Ip in the ventricle base. A maximum magnitude of the Ip was
obtained as approximately 6E1 Pa in the apical region (t= 0.25 s).
A-wave At the onset of the A-wave, the magnitude of the inflow velocity started to elevate and
simultaneously the Ip in the ventricle base began to increase (t= 0.3 s). However, at the
pinnacle of the A-wave, Ip in the apical region was much higher once again than the
basal pressure. After reaching the peak of the A-wave, the inlet flow velocity started to
decelerate and the Ip in the basal region decreased as well (t= 0.45 s). Although with
further deceleration in the A-wave, Ip in the ventricle base started to elevate slightly but
the magnitude was still much lower compared to the Ip in the ventricle apex. At the end
of the filling phase, a much higher magnitude of Ip was at the tip of the ventricle apex
with a value of approximately 3E2 Pa (t= 0.5 s).
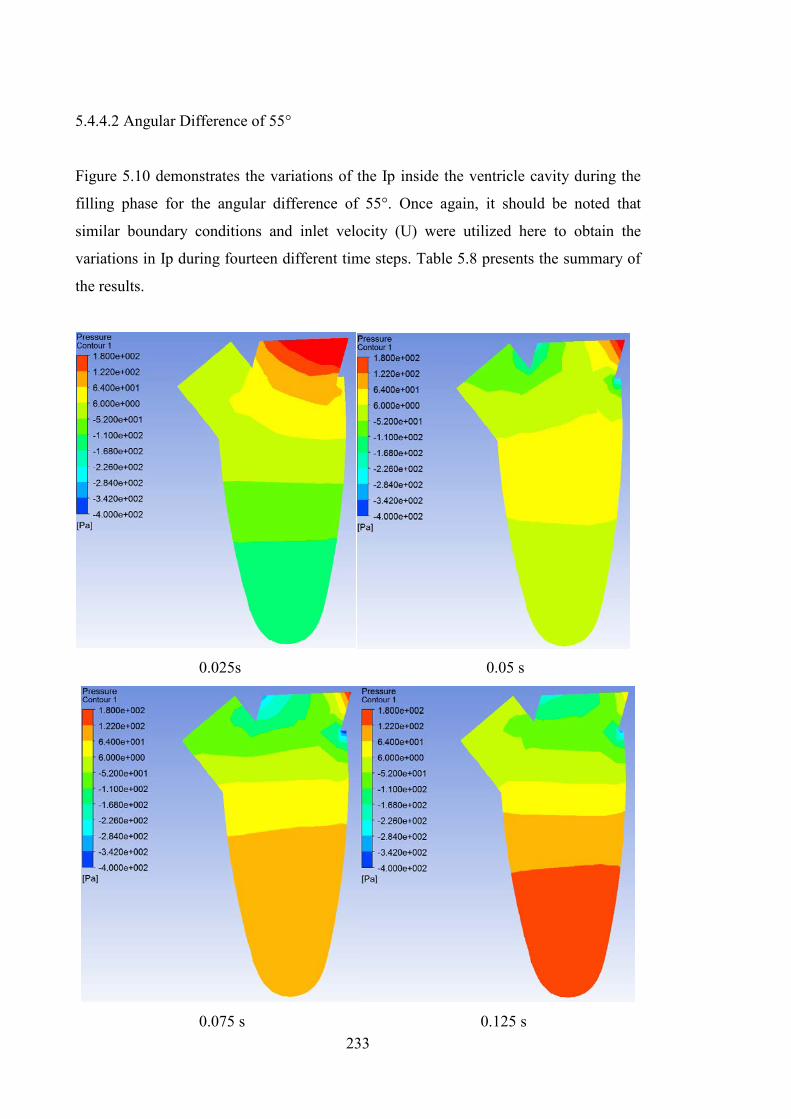
233
5.4.4.2 Angular Difference of 55°
Figure 5.10 demonstrates the variations of the Ip inside the ventricle cavity during the
filling phase for the angular difference of 55°. Once again, it should be noted that
similar boundary conditions and inlet velocity (U) were utilized here to obtain the
variations in Ip during fourteen different time steps. Table 5.8 presents the summary of
the results.
0.025s 0.05 s
0.075 s 0.125 s

234
0.15 s 0.2 s
0.25 s 0.275 s

235
0.3 s 0.35 s
0.4 s 0.45 s

236
0.475 s 0.5 s
Figure 5.10 Intra-ventricular pressure (Ip) distributions for the angular difference of
55°
Table 5.8 Observations pertaining to figure 5.10 Conditions Observations
E-wave At the initiation of the E-wave, minimal inflow velocity entered through the mitral
orifice and during that time step (t= 0.025 s) the magnitude of Ip in the basal region
started to rise and was much higher compared to the apical region. Unlike the angular
difference of 50°, a maximum magnitude of approximately 1.8E2 Pa was found to be in
the ventricle base with the time step of t= 0.025 s. Once more, with the advancement in
the E-wave, apical pressure inside the LV started to elevate and when the inlet velocity
reached the pinnacle of the E-wave (t= 0.075 s), Ip in the apical region was still found to
be increasing compared to its basal section. However, during this exact time step, the
magnitude of the Ip in the basal region was very low. This could be attributed to the fact
that, due to the variation in the ventricle geometry, the transmitral wave could not
directly enter through the mitral orifice and also it may be hindered with the wall of the
inlet region. Consequently, after reaching the pinnacle of the E-wave, inlet velocity
started to decelerate but the Ip in the ventricle apex increased and maximum magnitude
of Ip was approximately 1.8E2 Pa (t= 0.125 s and 0.15 s). At the end of the E-wave,
apical pressure was found to be much higher than the basal pressure (t= 0.2 s).
Diastasis During the diastasis phase, minimal inflow velocity entered through the mitral orifice.

237
During this phase, the magnitude of the Ip in the ventricle apex was decreasing but the Ip
in the basal region elevated slightly. The maximum magnitude of Ip was approximately
6.4E1 Pa in the apical region with the time step t= 0.25 s.
A-wave When the transmitral velocity (U) entered into the A-wave, inflow velocity started to rise
once again and the magnitude of the basal pressure started to elevate simultaneously (t=
0.3 s, t= 0.35 s and t= 0.4 s). At these exact time steps, the magnitude of the Ip in the
basal region was comparatively higher than the Ip in the ventricle apex. After reaching
the pinnacle of the A-wave, inflow velocity once again started to decrease (t= 0.45 s and
t= 0.475 s). During that time, Ip in the ventricle apex was much higher again compared
to the magnitude of Ip in the ventricle base. Also, the magnitude of the Ip in the apical
region of the chamber tended to increase with the deceleration in the A-wave. At the end
of the filling phase (t= 0.5 s) maximum Ip was at the tip of the LV apex with a
magnitude of around 1.8E2 Pa.
5.4.4.3 Angular Difference of 60°
All the images in Figure 5.11 illustrate the changes in the magnitudes of Ip inside the
LV chamber during the diastolic wave for the angular difference of 60°, in fourteen
different time steps. The boundary conditions and inlet velocity waveform (U) were
similar to those employed for the angular differences of 50° and 55°. Table 5.9 provides
the summary of the results.

238
0.025s 0.05 s
0.075 s 0.125 s

239
0.15 s 0.2 s
0.25 s 0.275 s

240
0.3 s 0.35 s
0.4 s 0.45 s
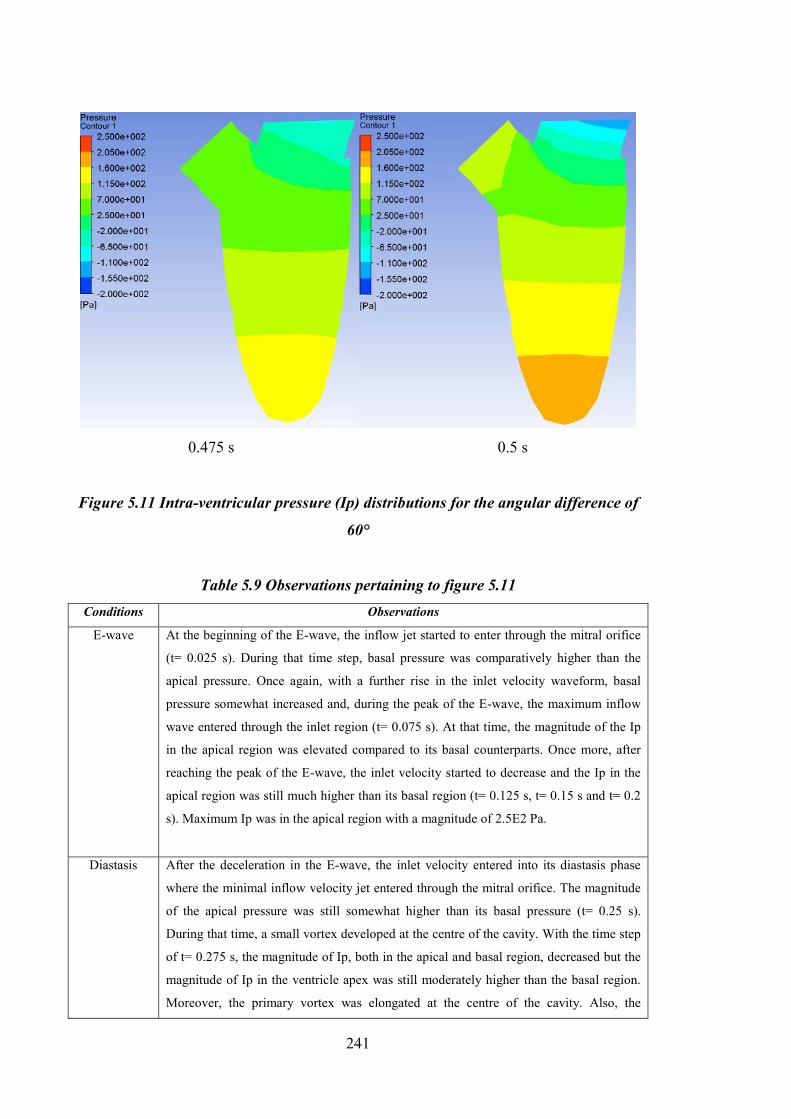
241
0.475 s 0.5 s
Figure 5.11 Intra-ventricular pressure (Ip) distributions for the angular difference of
60°
Table 5.9 Observations pertaining to figure 5.11 Conditions Observations
E-wave At the beginning of the E-wave, the inflow jet started to enter through the mitral orifice
(t= 0.025 s). During that time step, basal pressure was comparatively higher than the
apical pressure. Once again, with a further rise in the inlet velocity waveform, basal
pressure somewhat increased and, during the peak of the E-wave, the maximum inflow
wave entered through the inlet region (t= 0.075 s). At that time, the magnitude of the Ip
in the apical region was elevated compared to its basal counterparts. Once more, after
reaching the peak of the E-wave, the inlet velocity started to decrease and the Ip in the
apical region was still much higher than its basal region (t= 0.125 s, t= 0.15 s and t= 0.2
s). Maximum Ip was in the apical region with a magnitude of 2.5E2 Pa.
Diastasis After the deceleration in the E-wave, the inlet velocity entered into its diastasis phase
where the minimal inflow velocity jet entered through the mitral orifice. The magnitude
of the apical pressure was still somewhat higher than its basal pressure (t= 0.25 s).
During that time, a small vortex developed at the centre of the cavity. With the time step
of t= 0.275 s, the magnitude of Ip, both in the apical and basal region, decreased but the
magnitude of Ip in the ventricle apex was still moderately higher than the basal region.
Moreover, the primary vortex was elongated at the centre of the cavity. Also, the

242
maximum magnitude of Ip during the diastasis stage was approximately 7E1 Pa in the
apical region of the ventricle (t= 0.25 s).
A-wave With the initiation of the A-wave, inflow velocity started to elevate once again through
the mitral orifice. The basal pressure tended to increase with the elevation in the A-wave
and simultaneously the apical pressure was also rising (t= 0.3 s, t= 0.35 s and t= 0.4 s).
After reaching the peak of the A-wave, the inflow velocity started to decrease and during
the time steps of t= 0.45 s and t= 0.475 s, the magnitude of Ip in the ventricle apex
started to elevate once again compared to its basal pressure. At the end of the filling
phase (t= 0.5 s), a much higher magnitude of Ip was in the ventricle apex with a value of
approximately 2.05E2 Pa.
5.4.5 Structure Simulations using Total Mesh Displacement (TMD)
5.4.5.1 Angular Difference of 50°
The images in Figure 5.12 demonstrate the variations obtained in the ventricle
displacement during the diastolic wave propagation for thirteen different time steps.
Once again, boundary conditions and inlet velocity wavform (U) were similar to those
previously utilized for the velocity mapping, WSS and pressure distributions. Also, an
XY cross-sectional plane was taken inside the LV cavity to obtain the variations in the
mesh dispalcement of the structure. Moreover, the inlet was considerd fully opened and
the outlet was considered completely closed during the filling phase. Table 5.10
presents the summary of the results.

243
0.05 s
0.075 s 0.125 s

244
0.15 s 0.2 s
0.25 s 0.325 s

245
0.35 s 0.4 s
0.425 s 0.45 s

246
0.475 s 0.5 s
Figure 5.12 Total mesh displacement (TMD) distributions for the angular difference
of 50°
Table 5.10 Observations pertaining to figure 5.12 Conditions Observations
E-wave The volume inside the LV chamber started to increase with the flow propagation of the
filling wave. For example, at the beginning of the filling wave, the LV cavity was empty
and with the rise in the inlet velocity waveform, the volume of this chamber started to
elevate. When the inflow velocity touched the pinnacle of the E-wave (t= 0.075 s), a
comparatively higher magnitude of displacement was observed at the apical region of
the ventricle than its basal region. Once again, after touching the peak of the E-wave, the
inlet velocity decreased and hence the magnitude of the displacement increased at the
posterior side of the LV in the apical region, with a value of approximately 3.8E-5 m (t=
0.125 s). Moreover, with further deceleration in the E-wave, the magnitude of the TMD
in the apical region was decreasing.
Diastasis Once the inlet waveform reached its diastasis phase, the magnitude of the displacement
decreased but was still somewhat higher in the apical region than the basal region. The
maximum magnitude of the displacement was approximately 6.7E-6 m in the apical
region with the time step of t= 0.25 s.
A-wave After the minimal inflow velocity in the diastasis phase, the rate increased and entered

247
into the A-wave. With the rise in the A-wave velocity through the mitral orifice, the
magnitude of the displacement started to increase in the ventricle apex and this
magnitude increased even more with a further rise in the A-wave (t= 0.35 s, t= 0.4 s and
t= 0.425 s). After reaching the pinnacle of the A-wave, the inflow velocity once again
started to decrease and the magnitude in the apical region was still rising (t= 0.45 s and
t= 0.5 s). At the end of the filling phase (t= 0.5 s), the maximum magnitude in the
structure displacement was approximately 3.04E-5 m in the posterior LV wall in the
apical region.
5.4.5.2 Angular Difference of 55°
All the images in Figure 5.13 show the changes in the structure displacement of the LV
during the filling phase, in thirteen various time steps. Again, similar boundary
conditions and the inlet velocity waveform (U) were implementd during the
simulations. Table 5.11 represents the summary of the results.
0.05 s

248
0.075 s 0.125 s
0.15 s 0.2 s

249
0.25 s 0.325 s
0.35 s 0.4 s

250
0.425 s 0.45 s
0.475 s 0.5 s
Figure 5.13 Total mesh displacement (TMD) distributions for the angular difference
of 55°

251
Table 5.11 Observations pertaining to figure 5.13 Conditions Observations
E-wave At the initiation of the filling phase, the inlet jet started to enter the LV chamber and
with the rise in the inlet velocity, the magnitude of the displacement in the apical region
of the LV increased (t= 0.05 s). When the inlet velocity reached the peak of the E-wave
(t= 0.075 s), the magnitude of the displacement elevated even further in the ventricle
apex. After reaching the peak of the E-wave, the inflow velocity started to decline but
the maximum magnitude of displacement was in the ventricle apex with a value of
approximately 2.5E-5 m. Moreover, with further deceleration in the E-wave, TMD was
decreasing in the ventricle apex.
Diastasis When the inflow velocity entered into its diastasis phase, a minimal inflow jet entered
through the inlet region. However, the magnitude of the displacement was slightly
higher in the apical region compared to its basal region. The maximum magnitude of
displacement was still obtained at the posterior side of the LV wall in the apical region
with a value of around 7.5E-6 m (t= 0.25 s).
A-wave The inlet flow velocity entered into the atrial contraction wave (A-wave) and with the
rise in the A-wave, once again accelerated the magnitude of the displacement in the
apical region of the ventricle. After touching the pinnacle of the A-wave, it started to
decline again but the magnitude of the displacement in the apical region was increasing
(t= 0.45 s and t= 0.475 s). At the end of the filling phase (t= 0.5 s) the maximum
displacement was in the anterior side of the LV in the ventricle apex with a magnitude of
approximately 2E-5 m.
5.4.5.3 Angular Difference of 60°
Figure 5.14 demonstrates the variations in the displacement of the left ventricle during
the diastolic flow propagation. The inlet waveform (U) and the boundary conditons are
considered to be similar to those noted previosuly. Thirteen different time steps were
chosen to demonstare the variations in the displacement of the structure. Table 5.12
presents the summary of the results.

252
0.05 s
0.075 s 0.125 s

253
0.15 s 0.2 s
0.25 s 0.325 s

254
0.35 s 0.4 s
0.425 s 0.45 s

255
0.475 s 0.5 s
Figure 5.14 Total mesh displacement (TMD) distributions for the angular difference
of 60°
Table 5.12 Observations pertaining to figure 5.14 Conditions Observations
E-wave The rate of flow started to increase at the onset of the E-wave through the mitral orifice
into the LV chamber. With a further rise in the inlet velocity, the magnitude of the
displacement in the ventricle apex started to elevate (t= 0.05 s). After reaching the peak
of the E-wave (t= 0.075 s), the inflow velocity started to decrease and the maximum
magnitude of displacement was at the posterior side of the LV wall in the apical region,
with a value of approximately 3.5E-5 m (t= 0.125 s). Subsequently, with further
deceleration in the E-wave, the magnitude of the displacement in the apical region
decreased but it is still higher compared to the basal region.
Diastasis Once the inflow velocity entered into the diastasis phase, a minimal inlet velocity
entered through the inlet region. Although the magnitude of the displacement in the
ventricle apex decreased it was still higher compared to the basal region. Maximum
displacement was in the apical region of the ventricle with a magnitude of 7E-6 m (t=
0.25 s).
A-wave When the inlet velocity entered into the atrial contraction phase (A-wave), the inflow
velocity started to rise once again and with the rise in the A-wave, the magnitude of the

256
displacement in the apical region of the ventricle elevated once again (t= 0.35 s, t= 0.4 s
and t= 0.425 s). After touching the pinnacle of the A-wave, the inlet velocity started to
decrease but the TMD in the posterior side of the ventricle was higher in the ventricle
apex during the time step t= 0.45 s. At the end of the filling phase (t= 0.5 s), a higher
displacement was in the anterior region of the LV in the apex with a magnitude around
2.45E-5 m.

257
5.5 Discussion
5.5.1 Influence of flow dynamics for 50°, 55° and 60° between the mitral and aortic
orifice using velocity mapping
The variations in the flow distributions during the filling phase inside the LV, with
angular differences of:
• 50°
• 55°
• 60°
between the inlet and outlet regions were determined using velocity vectors. From the
simualtions it was evident that, at the onset of the filling wave, a minimal jet entered
through the inlet region. Consequently, with the elevation in the inlet velocity, the
magnitude of the velocity in the basal region of the LV was found to be much higher
compared to the apical region.
When the inlet velocity reached its pinnacle of the E-wave (approximately t= 0.075 s),
the LV geometry, with angular variations of 55° and 60°, developed a weaker vortex
close to the outlet region. This vortex, in both cases, was ring shaped and clockwise
(CW). The development of these vortices primarily depended on the angular variations
of the structure. However, the locations of these vortices were in similar places inside
the chamber. Subsequently, after touching the pinnacle of the E-wave, the inflow jet
started to decelerate and the magnitudes in the basal region of the ventricle began to
decrease. With the time step t= 0.125 s, the ring shaped and CW vortex was in the
vicinty of the inlet and outlet orifices for the 50° case but, for the 55° and 60° cases, the
vortices tended to elongate and shfit towards the core of the chamber. With further
deceleration in the E-wave (t= 0.175 s and t= 0.2 s) a similar kind of behaviour of the
vortices inside the cavity was observed for 50°, 55° and 60°. During these time periods,
the vortices were enlarging and heading into the central region of the LV cavity.

258
Once the inflow velocity entered into the diastasis period, the magnitude of the inflow
velocity decreased and the magnitudes in the ventricle base reduced. During this phase,
the adherence vortices for 50°, 55° and 60° were elongating and moved slightly towards
the core of the cavity. This was attributed to the fact that the primary vortex changed its
location towards the core of the cavity, where the posterior section of the vortex moved
marginally forward and the anterior/frontal section moved in opposite direction to the
posterior section, which in turn generated the adherence vortex. However, for the 55°
case, the location of the vortex was slightly upwards from the core of the LV, compared
to its counterparts (50° and 60°).
When the transmitral velocity entered into the A-wave, the inflow velocity started to
rise once again, as seen earlier. During this period, the adherence vortex in the ventricle
cavity began to merge with the rise in the inflow jet. This incident was apparent for the
50°and 60° cases, but in the 55° case, the the adherence vortex almost amalgamated
with the inflow jet and after touching the pinnacle of the A-wave (approximately t= 0.45
s), a clear, second ring-shaped and CW vortex originated near the outflow tract.
However, for 50° and 60° cases, this second vortex was obscure. This was ascribed to
the fact that, with the rise in the inflow velocity (peak A-wave), a vortex tended to
develop in the vicinity of the outlet tract due to variations of the anguar differences in
the LV geometry. Apparently, at the end of the filling phase, a ring shaped vortex
developed once again at the centre of the cavity.
Once again, the general trends of the flow behaviour, generation, development, shifting
and amalgamation of vortices were in line with the investigations from previously
published research (Arefin and Morsi, 2014, Vierendeels et al., 1999, Nakamura et al.,
2002, Watanabe et al., 2004, Cheng et al., 2005, Lassila et al., 2012).
5.5.2 Influence of intra-ventricular wall shear stress (WSS) for 50°, 55° and 60°
between the mitral and aortic orifice using WSS distributions

259
At the onset of the diastolic wave flow, the influence of the WSS was seen on the inlet
tract. With the elevation in the inlet velocity waveform, the magnitude of the WSS
increased on the inlet region and was also seen on the basal region of the LV wall.
During the pinnacle of the E-wave (t= 0.075 s), the maximum effect of the WSS was
observed on the anterior side of the basal region of the LV. However, a much higher
effect was seen on the basal region for the angular difference of 55° compared to 50°
and 60°. Moreover, for the 55° case, the influecne of WSS was higher close to the
anterior side of the apical region. For 50° and 60° cases, this effect was only observed
close to the anterior section of the ventricle core. With the deceleration of the E-wave,
the effect of the WSS on the inlet tract reduced simultaneously for 50°, 55° and 60°.
Also, during this period of time, the WSS effect minimized and remained on the basal
region for the 50° and 60° cases, but its effect was still evident on the core of the cavity
for 55°.
When the inlet waveform reached into the diastasis phase, the influence of the WSS
significantly reduced for the 50° and 60° cases. Precisely, the effect was minimal only
on the basal region of the LV. However, for the 55° case, this effect was still apparent
around the anterior section of the LV core but the effect was almost negligible on the
inlet tract.
Once again, at the onset of the A-wave, the effect of the WSS started to rise again, both
on the inlet tract and on the anterior position of the basal region for 50°, 55° and 60°.
Additionally, for the 55° case, this effect once again almost reached on the anterior
position of the apical region. With the rise in the A-wave, it accelerated the magnitude
of the WSS but with the deceleration in the A-wave, the WSS on the inlet tract began to
reduce once more for all cases. It also reduces on the basal region (for 50°and 60° cases)
and in the apical region and around the core of the LV (for 55°).
At the end of the filling phase, the WSS effect became negligible for the LV, especially
for the 50° and 60° cases, but was somewhat observed for the 55°. It should be noted
that, during the A-wave, the WSS effect was found to be sightly sideways/just beside
the basal region and on the centre of the LV compared to the effects originating during
the A-wave and the diastasis. This was attributed to the fact that, during the A-wave, the

260
elevation in the flow velocity did not rise much compared to the E-wave and hence, the
WSS effect could move slightly sideways on the LV wall.
5.5.3 Influence of intra-ventricular pressure (Ip) for 50°, 55° and 60° between the
mitral and aortic orifice using pressure distributions
At the begining of the filling wave, the magnitude of the Ip started to rise more in the
ventricle base than its apical region. Also, a negetive pressure gradient was observed at
the ventricle apex, as the propagation of the inflow jet was yet to reach in the apical
region of the cavity. So, the Ip in the basal region was found to be much higher than its
apical region. The magnitude of Ip in the basal region started to increase with the rise in
the early filling wave (E-wave) and the magnitude of Ip also increased in the apical
region of the ventricle. When the inlet velocity waveform reached the pinnacle of the
early filling wave (t= 0.075 s), a maximum inflow velocity entered through the mitral
orifice, which in turn also elevated the magnitude of the Ip in the apical region than the
basal pressure. During this exact time step, the maximum Ip was approximately 2.4E2
Pa for the 50° case, compared with a magnitude of 1.6E2 Pa for 60° and 1.22E2 Pa for
55°.
After reaching the pinnacle of the early filling wave, the inlet velcoity began to dip
down and the propagation of the jet reached to the end of the cavity (apical region) at
that time. Once it reached the apical region of the ventricle, the LV wall produced a
positive reflection back to the propagation of the inflow jet. This
superposition/amalgamation of the propagation of the flow with the reflected-wave from
the ventricle apex was responsible for elevating the magnitude of the Ip in the apical
region, which was generally termed as an "F-wave" (Cheng et al., 2005, Arefin and
Morsi, 2014). From the simulation results, it can be noted that a much higher magnitude
of Ip was found for the 50° and 60° cases compared to 55° for the ventricle apex. At the
end of the E-wave (t= 0.2 s), Ip in the apical region was still found to be moderately
higher for the 50° and 60° compared with 55°.

261
At the onset of the slow filling wave, a minimal inlet velocity entered through the mitral
region and the basal pressure tended to decrease. During this diastasis phase, a
maximum magnitude of Ip was in the apical region of the ventricle for all cases (50°,
55° and 60°). However, the discrepancies in the generation of vortex were found to be
somehwat different during the diastasis phase for the three cases. For the 60° case,
initally a very small vortex originated and then the vortex elongated. For the 50° case, a
much larger vortex (size and shape) was found compared to the 55° case during the time
step of t= 0.25 s. At a time step t= 0.275 s, a much larger vortex was observed for the
55° case compared to the 50° and 60° cases. It should be noted that, for the 50° case, the
primary vortex somewhat merged with fluid inside the chamber (t= 0.275 s).
Subsequently, the inlet velocity started to increase once again and with the rise in the
inlet velocity, the primary vortex started to merge with the propagation of the flow.
During the onset of the atrial contraction wave (A-wave), the magnitude of the Ip in the
ventricle base started to elevate once again compared to its basal pressure. After
reaching the peak of the A-wave, the inflow velocity dipped down once again and
during that time, the magnitude of Ip in the ventricle apex was much higher compared
to its basal pressure. At the end of the filling phase, the maximum magnitude of Ip is
found to be at the tip of the ventricle (apical region) for the 50° case with a magnitude
of approximately 3E2 Pa.
Consequently, the general phenomena of differences in the Ip, inside the ventricle
during the filling phase, were in line with previously published research (Vierendeels et
al., 1999, Nakamura et al., 2002, Cheng et al., 2005, Arefin and Morsi, 2014).
5.5.4 Influence of structure simulation for 50°, 55° and 60° between the mitral and
aortic orifice using total mesh displacement (TMD)
At the intiation of the filling wave, the inlet velocity jet started to enter the chamber,
which also increased the volume inside the cavity. With the rise in the inlet velocity, the
volume rose and, after touching the peak of the early filling wave, the inlet velocity

262
starts to decline. The superposiiton of the F-wave inside the LV; the increase in volume
inside the ventricle, and the intraventricular pressure changes meant that maximum
displacement was found in the apical region (t= 0.125 s) for all three cases. However,
for the 50° and 60° maximum TMD was observed in the posterior side of the LV wall in
the apical region compared to the 55°, where maximum TMD was at the ventricle apex.
With further deceleration in the E-wave, the magnitude of the displacement inside the
ventricle apex was found to be decreasing.
Once the inflow velocity entered into the diastasis phase, the rate of the inflow velocity
was minimal and the magnitude of the displacement in the apical region was decreasing.
However, the magnitude in the ventricle apex was still slightly higher compared to its
basal region for all three cases. This was attributed to the fact that, with minimal inlet
jet volume inside the chamber the variations in the displacement of the structure were
observed to be minimal during the diastasis phase.
When the inlet velocity entered into the A-wave, the flow rate through the inlet region
increased and the magnitude of the displacement started to rise once again. With further
rise in the inlet velocity, volume inside the chamber started to increase again which, in
turn, elevated the magnitude of the dispalcement in the apical region of the ventricle.
After touching the pinancle of the A-wave, the inlet velocity again started to dip down
and with the volume increased inside the cavity, the magnitude of the displacement in
the apical region started to elevate once more. At the end of the filling phase, because of
this increased volume inside the LV chamber, for all three cases, the magnitude of the
displacement in the apical region increased. Specifically, for the 50° case, the maximum
displacement was in the posterior side of the LV wall in the apical region but, for the
55° and 60° cases, it was found to be somewhat in the anterior side of the LV wall in the
ventricle apex.

263
5.6 Summary
From the above discussions and the simulated results, in general, it was evident that the
LV structure with an angular difference of 55° demonstrated different outcomes to the
50° and 60° geometry cases in terms of
• Velocity mapping
• WSS distributions
• Intraventricular Pressure distributions
• The structure simulations
during the filling phase.
For the velocity mapping, the flow dynamics including the:
• Generation
• Development
• Amalgamation
• Shifting
of vortices inside the LV chamber, for all three geometry cases were investigated and
determined. It was discovered that for the 55° case, the location of the vortex inside the
cavity was moderately upwards relative to the 50° and 60° cases, during the slow filling
phase. Also, during the atrial contraction phase, a second ring-shaped and CW vortex
was observed close to the outlet region for the 55° case, but for 50° and 60° cases, the
second vortex was somewhat obscured. However, after touching the pinnacle of the E-
wave for 50°, a ring shaped and CW vortex was seen developed in the vicinity of the
mitral and aortic orifice but for the 55° and 60° cases, this vortex was found to be
moderately elongating and changed its location towards the centre of the cavity.
The variations in the WSS of the LV wall were observed and it was determined that,
during the peak of the E-wave, the maximum WSS was seen on the anterior position of
the ventricle apex for all three cases. Specifically, a much higher magnitude of WSS

264
was found to be developed on the basal region of the LV for the 55° case than for 50°
and 60° cases. Also, a higher effect of WSS was seen developed near the anterior
position of the ventricle apex for the 55° case compared to 50° and 60° cases, where the
effect was only found near the anterior position of the centre of the LV. Moreover,
during the diastasis phase, the effect of WSS was still evident close to the anterior
position of the ventricle core for the 55° case, whereas for the 50° and 60° cases, very
little effect could be identified at the basal region. With the rise in the A-wave, the
effect of the WSS was increasing for all cases but, at the end of the diastolic wave, the
influence of the WSS became minimal for the 50° and 60° cases, but moderately
observed for the 55° case. Therefore, in general, with the rise in the inlet velocity, the
effect of the WSS increased (E-wave and A-wave) but for minimal inflow velocity this
effect decreased (slow filling phase) (Arefin and Morsi, 2014).
Subsequently, the magnitude of the Ip was also observed for all three cases during the
filling phase and it was noted that, at the end of the E-wave, the magnitude of Ip in the
ventricle apex was still slightly higher for the 50° and 60° cases than for the 55°. Also,
during the slow filling phase, dissimilarities in the generation and merging of the
primary vortex inside the cavity was observed for all cases. Specifically, for the angular
difference of 50°, the principle vortex was observed moderately amalgated with the
fluid inside the cavity (t= 0.275 s). Moreover, at the end of the filling wave, the
maximum magnitude of Ip was found to be at the tip of the ventricle apex for the 50°
case compared to 55° and 60° cases.
Finally, variations in the structural displacement were also observed during the filling
phase for all three cases. After touching the pinnacle of the E-wave, inflow velocity
decreased and at that time, the maximum magnitude of displacement was seen in the
posterior position of the LV wall in the ventricle apex for both the 50° and 60° cases
but, for the 55° cases, it was found to be in the apical region of the ventricle. During the
diastasis phase, for all three cases, the magnitude in the apical region of the LV was still
somewhat higher than its basal region. Consequently, at the end of the filling phase, the
maximum magnitude of displacement was observed in the posterior position of the
ventricle wall in the apical region for the 50° case, but it was observed slightly in the
anterior section of the ventricle wall in the apical region for the 55° and 60° cases.

265
Chapter 6
Numerical Analysis of the Left Ventricle during
Diastole Phase: The Influence of Friction Co-
efficient and Elastic Modulus

266
6.1 Overview
This chapter documents the research that highlighted the hemodynamic characteristics
and structural displacements of the LV during the diastolic phase by implementing the
effects of the:
• Friction co-efficient (Cf)
• Elastic modulus
Similar to the research documented in previous chapters, the Fluid Structure Interaction
(FSI) scheme was utilized for computing the simulations. The Cf and elastic modulus
were determined and implemented during the simulations to observe the influence in
terms of:
• Flow dynamics
• Intraventricular pressure (Ip) distributions
• Wall shear stress (WSS) distributions
• Structural variations
Once again, as reported in Chapter 4 the geometry of a 3D physiologically correct LV
model and required boundary conditions were used during the simulations. Once more,
similar to Chapter 3, Chapter 4 and Chapter 5, the Navier-Stokes equations and the
Arbitrary Lagrangian Eulerian (ALE) methods were employed to couple the solid and
fluid regions of the ventricle model. Subsequently, the results were compared, discussed
and analyzed with previously published research work.
Importantly, the implementation Cf and elastic modulus provided substantial insights
specifically into dilated cardiomyopathy (DCM) disease conditions, which were also
examined.
Finally, this chapter summarizes the findings from the above named simulations which,
as with previous analyses, would be useful for the development of a next generation
VAD system.

267
6.2 Introduction
Diastolic features of the LV are affected by the influence of the friction co-efficient (Cf)
and the elastic modulus, which primarily sway the hemodynamic and physiological
characteristics of the ventricle model. In order to determine and understand the
influence of the Cf and elastic modulus, the FSI method was implemented.
Using the FSI approach, many earlier investigations had been conducted based on the
variations of the flow pattern and the physiological features of the LV, but the
utilization of the Cf was neglected (Taylor et al., 1994, Jones and Metaxas, 1998,
Keldermann et al., 2010). Although in an experimental investigation Cope, 1963,
observed the frictional resistance of the septum but this was based on the insertion of
the transeptal catheter inside the LV (Cope, 1963). However, precise physiological
features were still required in order to simulate the complete functionalities of the
ventricle model (Lee et al., 2009, Nordsletten et al., 2011, Khalafvand et al., 2011).
The literature in Chapter 2 suggested that the FSI scheme was useful in determining the
physiological and hemodynamical characteristics for both the general and diseased
conditions. Hence, the research documented in this chapter once again utilized the FSI
method to determine and understand the structural and hemodynamic properties of the
LV model by implementing the effects of the friction co-efficient (Cf) and elastic
modulus during the filling phase. Moreover, the correlation of these effects with the
DCM was also determined during the diastolic flow conditions. Results are presented
in terms of the:
• Velocity mapping
• Ip distributions
• WSS distributions
• Structural variations of the LV model

268
6.3 Computational Approaches
6.3.1 Geometry Extraction
This section provides the details of the LV model and the boundary conditions,
including the effects of Cf and elastic modulus. Similar to the previous approaches,
documented in Chapter 4 and Chapter 5, after selecting the LV model, the transmitral
flow velocity (U) was implemented through the inlet/mitral orifice. Moreover, the
computed Cf and the elastic modulus were varied and implemented during the filling
phase.
For the simulations, the geometry of the LV was considered similar to the model used in
Chapter 4. Therefore, the detailed description of the LV model is not presented here.
For modelling the geometry, SolidWorks 2012 were utilized.
6.3.2 Meshing Statistics and Mesh Independency Trials
Similar to the previous approaches stated in Chapter 4 and Chapter 5, the LV model was
introduced once again into ANSYS 14.5 after being modelled using SolidWorks 2012.
Subsequently, the required meshing was performed and the mandatory boundary
conditions, which also included the varied Cf and the elastic modulus, were
implemented. For this simulation, “Mapped Face Meshing” was executed for the solid
and fluid region independently. Once again, similar to Chapter 3, Chapter 4 and Chapter
5, line control properties were implemented to study the discrepancies in the flow
velocity during the filling phase (Kouhi, 2011, Arefin and Morsi, 2014).
A mesh independency trial was carried out by using this line control properties and the
changes in the velocity of the fluid was computed for consecutive nodes and elements,
both for the solid region and fluid region till the velocity converged. Figure 6.1
illustrates the mesh independency trials by utilizing the fluid velocity. Once more,

269
during this test, three different meshing groups are chosen (coarse, medium and fine).
After utilizing these, it was confirmed that:
• 4507 nodes
• 2362 elements
acceptable for the solid region and:
• 34881 nodes
• 190377 elements
were considered to be accurate for the fluid region respectively. These elements and
nodes were selected for the medium mesh type. Furthermore, similar to the previous
simulations, the convergence criterion for the fluid was considered to be 10-4, and for
the coupling data transfer it is taken to be 10-2, as documented in Chapter 4 and Chapter
5 (Arefin and Morsi, 2014).
Figure 6.1 Mesh independency trial by using fluid velocity
0
0.2
0.4
0.6
0.8
1
1.2
1.4
0 0.02 0.04 0.06 0.08
Velo
city
[m/s
]
Y [m]
Mesh Type-MediumMesh Type-CoarseMesh Type-Fine

270
6.3.3 Boundary Conditions
Once again, similar to Chapter 4, the transmitral flow waveform (U in m/s) was
implemented through the inlet/mitral region and the primary boundary conditions were
also considered to be similar (Arefin and Morsi, 2014).
Subsequently, from the velocity waveform (U), it was recognized that three different
conditions existed, as explained in Chapter 4 and Chapter 5. In brief, the waveform
included:
• Two peaks termed the early filling wave (E-wave) and the atrial contraction
wave (A-wave) with the flow velocity of 0.8 m/s and 0.4 m/s in that order.
• Between these two peaks, the middle phase was recognized as the diastasis/slow
filling phase (0.22<t<0.3s) (Arefin and Morsi, 2014, Vierendeels et al., 1999,
Cheng et al., 2005).
Once more, similar to the Chapter 4 and Chapter 5, the ventricle wall was assumed to be
isotropic and homogeneous, which encompassed:
• The density of the ventricle wall with the value of 1.2 g/cm3
• Elastic modulus of 0.7 MPa
• Poisson’s ratio of 0.4
Consequently, Newtonian fluid flow was assumed for the entire simulation, including
the fluid density with a value of 1050 kg/m3 and a viscosity of 0.0035 Pa.s, which also
included no-slip boundary conditions. The flow property was considered to be laminar
(Cheng et al., 2005, Lassila et al., 2012, Vierendeels et al., 1999, Arefin and Morsi,
2014, Saber et al., 2003).
Moreover, the effect of the friction co-efficient (Cf) was determined by using the
following formula (Online, 2011, Young, 1939, Nash, 1966, Monaghan, 1953):

271
Cf= 2τmax / (ρU2peak) (6.1)
where:
• τmax denotes the maximum wall shear stress
• ρ is the density of the fluid
• U2 peak represents the peak velocity (diastole)
As mentioned above, there are two different peaks and one slow filling phase in the
diastolic phase. The computed Cf for each phase is provided in the following table
(Table 6.1):
Table 6.1 Computations of Cf
Conditions Time (t) Upeak (m/s) Cf
Peak E-wave 0.075s 0.75 0.125
Diastasis/ Slow
Filling Phase 0.275s 0.04 16.679
Peak A-wave 0.425s 0.4 0.193
Initially, the simulations were carried out without implementing the effects of the
friction co-efficient during the entire diastolic wave phase. From the simulations, the
magnitudes of τmax were determined. Subsequently, elastic modulus have been varied
considered as (Lassila et al., 2012):
• 0.35 MPa
• 0.7MPa
• 1.4 MPa

272
The entire simulation was executed for all three values of elastic modulus and the Cf.
Firstly, the magnitudes of the computed Cf for peak E-wave was considered fixed and
the magnitudes of the elastic modulus were then changed throughout the diastolic phase.
Subsequently, this step was employed again for the remaining magnitudes of the elastic
modulus and Cf. Finally, the findings were compared and the results offered substantial
insights in the physiological and hemodynamic influences including the disease factors
for DCM of the LV (Dellimore et al., 2013).

273
6.4 Simulation Results
6.4.1 Overview
The estimation of the Cf was mainly emphasized on the three imperative phases of the
diastolic wave, hence the results for varying the Cf and elastic modulus for the peak E-
wave, diastasis and peak A-wave were presented in terms of:
• WSS distributions
• Ip distributions
• Velocity mapping
• Structure simulations using TMD
6.4.2 The influence of friction coefficient and elastic modulus of the LV using wall
shear stress (WSS) distributions
The wall shear stress (WSS) of the LV during the filling phase was demonstrated for
three different time steps in the following figures. Once again, WSS was determined to
examine the influence of the Cf and elastic modulus, implemented on the ventricle wall
motion. Subsequently, the influence of the WSS was observed on the outer surface of
the LV wall. Similar to Chapter 4 and Chapter 5, the outlet region is considered
completely closed and the inlet region was considered fully open during the diastolic
wave conditions. Moreover, the required boundary conditions and the inlet velocity
waveform (U) were employed for this simulation (through the mitral region).
6.4.2.1 Elastic modulus of 0.35 MPa
The images in Figure 6.2 demonstrate the changes in the WSS of the ventricle wall in
three imperative phases in the filling phase. The influences of the Cf and the elastic

274
modulus (0.35 MPa) were added during the simulation for three different time steps. All
the required boundary conditions, including the velocity waveform (U) of the filling
phase, were implemented through the inlet orifice.
0.075 s
0.275 s

275
0.425 s
Figure 6.2 WSS distributions for 0.35 MPa
For this simulation (with a value of 0.35 MPa), initially the elastic modulus was
considered fixed and the Cf was varied during the filling phase. This simulation
therefore provided a better understanding on the effect of the Cf and Wt on LV wall
shear. Table 6.2 provides the summary of the results.
Table 6.2 Observations pertaining to figure 6.2 Conditions Observations
E-wave In general, at the onset of the filling phase, inlet velocity started to enter the LV chamber
and the magnitude of the WSS on the inlet wall and ventricle base started to increase.
However, with the added friction co-efficient (0.125) for the peak E-wave (t= 0.075 s),
the maximum magnitude of WSS of 3.68E1 Pa was observed almost on the whole
ventricle wall. During the peak E-wave, a maximum flow rate of around 0.75 m/s
entered through the inlet orifice. Also, just beside the centre of the ventricle chamber, the
magnitude of the WSS started to decrease up to the apical region. A similar effect could
be found in the inlet and outlet region. This could be attributed to the maximum flow
velocity WSS on the ventricle wall being much higher, thereby providing the added
magnitudes of Cf.
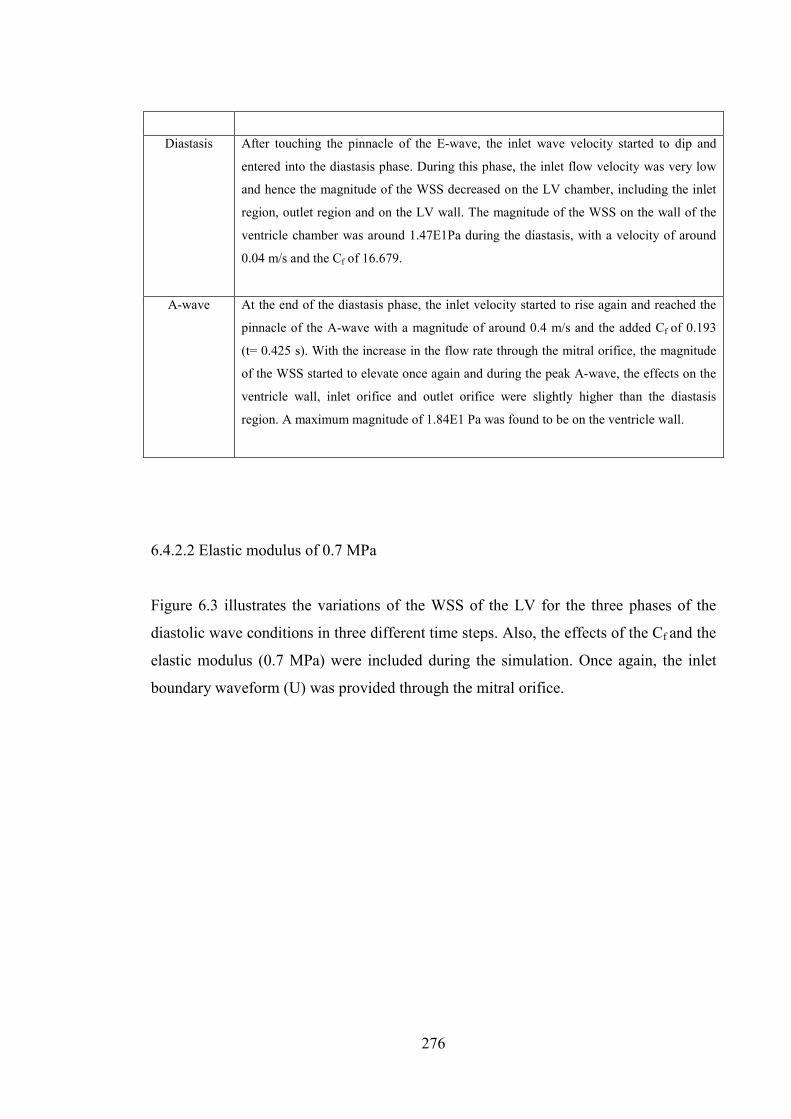
276
Diastasis After touching the pinnacle of the E-wave, the inlet wave velocity started to dip and
entered into the diastasis phase. During this phase, the inlet flow velocity was very low
and hence the magnitude of the WSS decreased on the LV chamber, including the inlet
region, outlet region and on the LV wall. The magnitude of the WSS on the wall of the
ventricle chamber was around 1.47E1Pa during the diastasis, with a velocity of around
0.04 m/s and the Cf of 16.679.
A-wave At the end of the diastasis phase, the inlet velocity started to rise again and reached the
pinnacle of the A-wave with a magnitude of around 0.4 m/s and the added Cf of 0.193
(t= 0.425 s). With the increase in the flow rate through the mitral orifice, the magnitude
of the WSS started to elevate once again and during the peak A-wave, the effects on the
ventricle wall, inlet orifice and outlet orifice were slightly higher than the diastasis
region. A maximum magnitude of 1.84E1 Pa was found to be on the ventricle wall.
6.4.2.2 Elastic modulus of 0.7 MPa
Figure 6.3 illustrates the variations of the WSS of the LV for the three phases of the
diastolic wave conditions in three different time steps. Also, the effects of the Cf and the
elastic modulus (0.7 MPa) were included during the simulation. Once again, the inlet
boundary waveform (U) was provided through the mitral orifice.

277
0.075 s
0.275 s
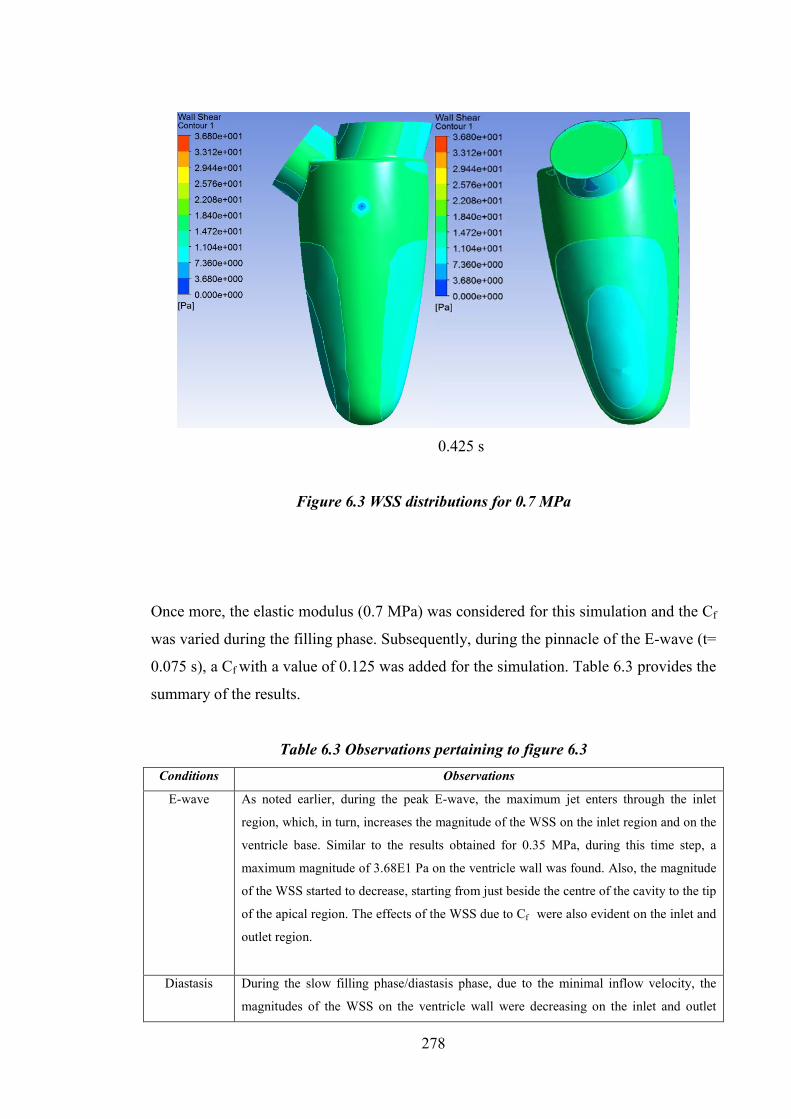
278
0.425 s
Figure 6.3 WSS distributions for 0.7 MPa
Once more, the elastic modulus (0.7 MPa) was considered for this simulation and the Cf
was varied during the filling phase. Subsequently, during the pinnacle of the E-wave (t=
0.075 s), a Cf with a value of 0.125 was added for the simulation. Table 6.3 provides the
summary of the results.
Table 6.3 Observations pertaining to figure 6.3 Conditions Observations
E-wave As noted earlier, during the peak E-wave, the maximum jet enters through the inlet
region, which, in turn, increases the magnitude of the WSS on the inlet region and on the
ventricle base. Similar to the results obtained for 0.35 MPa, during this time step, a
maximum magnitude of 3.68E1 Pa on the ventricle wall was found. Also, the magnitude
of the WSS started to decrease, starting from just beside the centre of the cavity to the tip
of the apical region. The effects of the WSS due to Cf were also evident on the inlet and
outlet region.
Diastasis During the slow filling phase/diastasis phase, due to the minimal inflow velocity, the
magnitudes of the WSS on the ventricle wall were decreasing on the inlet and outlet

279
tract. Once more, a maximum magnitude of around 1.47E1 Pa was found to be on the
LV wall. Simultaneously, the magnitudes of the WSS near the centre of the LV wall and
on the ventricle apex were found to be decreasing.
A-wave After the end of the diastasis period, the magnitude of the inlet velocity started to rise
and reached the pinnacle of the A-wave. Once again, due to the added Cf of 0.193 and
with the rise in the inlet velocity, the magnitude of the WSS was slightly higher
compared to the diastasis phase, but much lower than that of its peak E-wave. A
maximum magnitude of the WSS was approximately 1.84E1 Pa was found on the
ventricle wall.
6.4.2.3 Elastic modulus of 1.4 MPa
From the images in Figure 6.4, the variations of the WSS on the LV wall of three phases
of the filling phase were investigated. Once more, the effects of the Cf and the elastic
modulus (1.4 MPa) were combined for this simulation. Similar to the previous
simulations, boundary conditions were kept identical. This simulation is presented for
three different time steps. Table 6.4 provides the summary of the results.
0.075 s

280
0.275 s
0.425 s
Figure 6.4 WSS distributions for 1.4 MPa

281
Table 6.4 Observations pertaining to figure 6.4 Conditions Observations
E-wave During the peak of the E-wave, the maximum inflow jet starts to enter through the mitral
orifice and, for the included Cf with a value of 0.125, the maximum magnitude of WSS
was observed - similar to the findings for the 0.35 MPa and 0.7 MPa of elastic modules.
Once again, the influence of the WSS was mostly observed on the ventricle wall with a
magnitude of around 3.68E1 Pa. Higher magnitudes of WSS were also found on the inlet
orifice and outlet orifice. Furthermore, a similar phenomenon was observed with the
magnitude of the WSS - found to be decreasing, just beside the centre to the cavity to the
ventricle apex.
Diastasis After the end of the E-wave, the inlet velocity enters the diastasis phase where the inflow
velocity was minimal. Again, similar effects were observed on the variations of the WSS
for the discrepancies on the elastic modulus (0.35 MPa and 0.7 MPa). During the time
step of t= 0.275 s, in the slow filling phase, the magnitudes of the WSS were declining
and the maximum WSS was observed to be approximately 1.47E1 Pa on the ventricle
wall. Concurrently, magnitudes of the WSS (just beside the core of the ventricle wall to
the ventricle apex) were found to be decreasing as well.
A-wave As the inlet velocity entered into the A-wave, the inflow velocity started to increase and
then reached the peak A-wave. Due to the incline in the inlet velocity jet, the WSS on
the ventricle wall increased and the maximum magnitude of the WSS was approximately
1.84E1 Pa on the ventricle wall. It was noted that similar magnitudes and variations in
the WSS were observed (of 1.4 MPa) for the elastic modulus of 0.35 MPa and 0.7 MPa.
6.4.3 The influence of friction coefficient and elastic modulus using intraventricular
pressure (Ip) distributions
6.4.3.1 Elastic modulus of 0.35 MPa
The variations in the Ip pressure distributions during the diastolic wave conditions were
determined for three different time steps, as illustrated in the following figures. Also,
the effects of the Cf and elastic modulus were employed in order to determine the
variations in the Ip. By using similar boundary conditions as stated in Section 6.4.2,

282
discrepancies in the Ip distributions were demonstrated and are presented below. Ip
distributions during three phases are demonstrated using an XY cross-sectional plane
and the outer surface of the LV.
All the images in Figure 6.5 demonstrate the variations in the Ip distributions in three
different time steps during the filling cycle. Also, the effects of the Cf and elastic
modulus (0.35 MPa) are included in determining the changes in the Ip. Table 6.5
provides the summary of the results.
0.075 s
0.275 s

283
0.425 s
Figure 6.5 Ip distributions for the elastic modulus of 0.35MPa
Table 6.5 Observations pertaining to figure 6.5 Conditions Observations
E-wave During the simulation presented in Figure 6.5, the magnitude of the elastic modulus was
considered fixed and the Cf was varied in three different time steps. As noted earlier,
during the pinnacle of the E-wave, the maximum jet entered through the mitral orifice.
As seen in Chapter 4 and Chapter 5, the magnitudes of the intraventricular pressure
started to rise in the apical region during this time period. However, with the added Cf
the maximum magnitude of the WSS was approximately 7.46E2 Pa close to the tip of
the ventricle apex. Also, the Ip in the basal region, inlet and outlet tract was much lower
compared to the apical pressure. Moreover, a ring shaped vortex developed close to the
outlet region.
Diastasis Once again, after reaching the peak of the E-wave, the rate of flow declined and entered
into the diastasis phase. With the increased Cf during this phase, a much higher
magnitude of the Ip was found in the apical region of the LV with a value of around
1.23E2 Pa compared to its basal region. Also, just beside the tip of the ventricle apex, a
higher magnitude of Ip was found with a value of around 3.72E2 Pa. However, the value
of the Ip in the ventricle apex was still much lower compared to the magnitude of the
peak E-wave. As the inlet velocity was minimal during this phase, a lower magnitude of
the Ip in the centre of the ventricle was also observed. Additionally, the previously

284
formed ring shaped vortex changed its position towards the centre of the ventricle and
enlarged slightly.
A-wave At the beginning of the A-wave, the inlet velocity started to elevate once again and when
it reached the peak of the A-wave, a higher velocity of inlet jet entered through the
mitral region. Due to the added Cf of 0.193 the magnitude of the Ip in the apical region
(close to the tip of the LV apex) with a value of around 3.72E2 Pa, was still much higher
compared to its basal region. However, this magnitude was still lower than the peak E-
wave but higher than the diastasis phase. Once again, the vortex was enlarging during
this time step.
6.4.3.2 Elastic modulus of 0.7 MPa
The images in Figure 6.6 illustrate the changes in the Ip distributions for three important
phases of the diastolic flow conditions. Once again, the effects of the Cf and elastic
modulus (0.7 MPa) were added during the simulation. Table 6.6 provides the summary
of the results.
0.075 s

285
0.275 s
0.425 s
Figure 6.6 Ip distributions for the elastic modulus of 0.7MPa

286
Table 6.6 Observations pertaining to figure 6.6 Conditions Observations
E-wave Similar to the elastic modulus of 0.7 MPa; during the peak E-wave, the maximum flow
velocity entered through the inlet region. Once again, a higher magnitude of Ip was
obtained in the ventricle apex compared to its basal pressure. Precisely, the maximum
magnitude was found to be near the tip of the LV in the apical region with a value of
approximately 7.46E2 Pa. Once more, the magnitudes of the Ip in the inlet and outlet
region were much lower than that of its apical region. Also, a ring shaped vortex
developed near the outlet region.
Diastasis After the end of the E-wave, the inlet velocity entered into the diastasis phase, where the
flow velocity was minimal. During this time step (t= 0.275 s) the magnitude of the Ip in
the ventricle apex was still much higher compared to its basal region. A maximum
magnitude of around 1.23E2 Pa is found to be in the ventricle apex. Moreover, just
beside the tip of the apical region, a much higher magnitude was found with a value of
approximately 3.72E2 Pa. Once again, it was seen that, with the increased Cf during this
phase, the magnitude of the Ip reduced when compared with the peak E-wave. Also at
the core of the LV chamber and in the basal region, the magnitude of Ip was found to be
much lower. Again, the previously formed vortex changed its position towards the core
of the cavity.
A-wave During the peak of the A-wave, the rate of the inlet velocity elevated once again. Once
more, with the reduced magnitude of the Cf (0.193) compared to the diastasis phase, the
magnitude of the Ip in the ventricle apex (near the tip of the apex) was somewhat higher
with a value of approximately 3.72E2 Pa. Simultaneously, at the core of the ventricle,
the inlet and outlet regions, the magnitude of the Ip was much lower when compared
with its apical region. Once more, the previously formed ring shaped vortex was seen
elongated during this time step, at the core of the ventricle.
6.4.3.3 Elastic modulus of 1.4 MPa
Ip distributions of the LV, using the effects of the Cf and elastic modulus (1.4 MPa) are
demonstrated in Figure 6.7 during the three phases of the filling wave. Table 6.7
provides the summary of the results.

287
0.075 s
0.275 s
288
0.425 s
Figure 6.7 Ip distributions for the elastic modulus of 1.4MPa
Table 6.7 Observations pertaining to figure 6.7 Conditions Observations
E-wave In general, similar results were obtained during the peak E-wave, diastasis and peak A-
wave. Specifically, during the peak E-wave, the magnitude of the Ip in the ventricle apex
was much higher compared to its basal region. A maximum magnitude of approximately
7.46E2 Pa was found to be in the ventricle apex close to the tip of the apex. Once again,
the magnitude of the basal pressure was much lower compared to its apical region. At
the same time, a ring shaped vortex, similar to the previous elastic modulus (0.35 MPa
and 0.7 MPa) developed near the outlet region.
Diastasis Once again, after the end of the E-wave, the inlet velocity entered into the diastasis
phase and, during this phase, the flow velocity decreased and the primary vortex was
seen changing its position towards the core of the cavity. Even with the decelerated inlet
velocity, the magnitude of the Ip in the mitral region was still much higher compared to
its apical region. A maximum magnitude of 1.23E2 Pa was found in the apical region of
the ventricle during this phase. Also, a maximum magnitude of approximately 3.72E2 Pa
was in the ventricle apex near the tip of the LV. However, with the increased Cf during
this phase, the magnitude of the Ip in the apical region was found to be comparatively
lower than the peak E-wave.

289
A-wave After the diastasis phase, the inlet velocity wave came to the peak of the A-wave and the
magnitude of the inlet velocity rose once more. During this phase, similar effects were
found with the elastic modulus of 0.35 MPa and 0.7 MPa. Consequently, the magnitude
of the Ip in the apical region (close to the tip of the LV apex) was higher again with a
value of approximately 3.72E2 Pa compared to the ventricle base. Also, the vortex was
enlarged during this time step.
6.4.4 The influence of friction coefficient and elastic modulus using velocity mapping
6.4.4.1 Elastic modulus of 0.35 MPa
The changes in the velocity pattern during the peak E-wave, slow filling phase and the
peak A-wave are demonstrated in the following sections. Additionally, the effects of the
Cf and the elastic modulus were incorporated to observe and determine the influence on
the velocity distributions, including the formation, shifting and merging of vortices
during these three phases. In so doing, the required boundary conditions and transmitral
velocity wave (U) were implemented, as reported in Section 6.4.2. Also, an XY cross-
sectional plane was selected to observe the changes in the velocity pattern.
The images in Figure 6.8 demonstrate the discrepancies in the velocity distributions
during the three phases, including the effects of the Cf and elastic modulus (0.35 MPa).
Table 6.8 provides the summary of the results.

290
0.075 s
0.275 s

291
0.425 s
Figure 6.8 Velocity distributions for the elastic modulus of 0.35MPa
Table 6.8 Observations pertaining to figure 6.8 Conditions Observations
E-wave As stated earlier, during the peak E-wave, the inlet velocity was maximum entering
through the mitral orifice and propagated towards the ventricle apex. During the time
step, the elastic modulus was considered fixed (0.35 MPa) and the magnitude of the Cf
was varied. Because of the added Cf a ring shaped, clockwise (CW) vortex developed
close to the outlet region. Also, at the apical region of the ventricle, the flow pattern
appeared to be twisting and moving upwards. During this period, a maximum flow
velocity is obtained as approximately 1.25 m/s in the ventricle base.
Diastasis During the slow filling phase, the magnitude of the inlet flow velocity minimized and the
primary vortex was somewhat elongated and changed its positions towards the centre of
the cavity. Simultaneously, a weak vortex, which was also ring shaped and clockwise,
started to develop near the outlet tract. At the same time, because of the increased Cf a
twisting of the flow pattern was evident in apical region of the ventricle. Moreover, the
maximum velocity of approximately 6.25E-1 m/s was found to be in the basal region.
A-wave When the inlet waveform reached the pinnacle of the A-wave, the inlet velocity
increased and because of that, the primary vortex slowly began to merge with the
propagation of the inlet jet. Also, the weaker vortex amalgamated with the inflow wave,

292
but was still evident close to dead-end of the outlet tract. Additionally, a maximum
magnitude of the velocity of approximately 6.25E-1m/s existed close to the inlet region.
6.4.4.2 Elastic modulus of 0.7MPa
Once again, the velocity pattern for the elastic modulus was varied (0.7 MPa), and the
flow pattern was determined. This is illustrated in the images in Figure 6.9. Table 6.9
provides the summary of the results.
0.075 s

293
0.275 s
0.425 s
Figure 6.9 Velocity distributions for the elastic modulus of 0.7MPa

294
Table 6.9 Observations pertaining to figure 6.9 Conditions Observations
E-wave Similar to the elastic modulus of 0.35 MPa, the flow pattern was also determined for the
elastic modulus of 0.7 MPa by including the effects of the Cf (0.125) in three different
phases. During the peak of the E-wave, the flow rate elevated and a twisting in the flow
appeared at the ventricle apex. At the same time, a ring shaped, CW vortex formed near
the outlet region. During this time period, a maximum flow velocity of approximately
1.25m/s was in the ventricle base.
Diastasis When the inlet velocity entered into the slow filling phase, the inlet velocity became
minimal and the effect of the Cf (16.679) increased. During this time period, the primary
adherence vortex enlarged and shifted its position towards the centre of the cavity. At the
same time, a weak ring shaped CW vortex formed close to the aortic orifice of the
ventricle. Simultaneously, the twisting in the flow pattern in the ventricle apex was
observed, which was found to be moving towards the core of the chamber. During this
time period in the ventricle base, a maximum flow velocity of 6.25E-1 m/s was found.
A-wave During the pinnacle of the A-wave, the rate of flow increased once again, and the flow
dynamics were observed, including the effect of the Cf (0.193), which slightly decreased
compared to the diastasis. Subsequently, with the elevation in the flow rate, the primary
vortex slowly began to merge with the incoming jet from the inlet region and also the
secondary weak vortex started to amalgamate. However, the weaker vortex was still
evident close to the dead-end of the aortic orifice. Simultaneously, the twisting in the
flow dynamics in the apical region was seen amalgamated with the propagation of the
inlet jet. During this time period, the maximum magnitude of the velocity was found to
be approximately 6.25E-1 m/s close to the inlet region.
6.4.4.3 Elastic modulus of 1.4 MPa
Similar to the previous elastic modules, the flow dynamics, including the development,
shifting and merging of vortices are shown in Figure 6.10. Table 6.10 provides the
summary of the results.

295
0.075 s
0.275 s

296
0.425 s
Figure 6.10 Velocity distributions for the elastic modulus of 1.4MPa
Table 6.10 Observations pertaining to figure 6.10 Conditions Observations
E-wave Once again, similar effects were found for the flow pattern during the peak of the E-
wave, diastasis and peak of the A-wave, including the added effect of Cf. With higher
flow velocity during the peak E-wave, a wake vortex developed close to the outlet
region. Simultaneously, twisting of the flow was evident in the apical region of the
ventricle. Also, a maximum magnitude of flow velocity was approximately 1.25 m/s in
the basal region of the ventricle.
Diastasis When the inflow velocity entered into the diastasis phase, the rate of flow was minimal
and during this time period, the magnitude of the Cf increased. Hence, the primary
vortex, which was ring shaped and CW, elongated and changed its location to the core of
the chamber. Once again a weak second vortex, which was ring shaped and CW,
developed near the outlet tract. Concurrently, the twisting in the flow pattern in the
ventricle apex was also noticeable and was found to be moving upwards to the centre of
the ventricle. During this time period, a maximum magnitude of the velocity was
obtained to be approximately 6.25E-1 m/s in the basal region of the ventricle.
A-wave During the pinnacle of the A-wave, with the added effect of the Cf and with the rise in
the inflow jet, the primary vortex started to merge with the inflow wave inside the

297
ventricle. Also, the second weak vortex, which was ring shaped and CW was seen
merging but it was still visible near the cul-de-sac of the outlet tract. Moreover, the
twisting was also amalgamated with the propagation of the inlet jet. Subsequently, the
maximum magnitude of the flow velocity was acquired at approximately 6.25E-1 m/s,
close to the inlet tract.
6.4.5 The influence of friction coefficient and elastic modulus structure simulation
using total mesh displacement (TMD)
6.4.5.1 Elastic modulus of 0.35MPa
Structure simulation of the LV during the above mentioned phases was performed and
is illustrated in the following sections. Once again, the variations in the elastic modulus
and the effect of Cf were considered and varied. Similar to the previous boundary
conditions, reported in Section 6.4.2, all the required boundary details were included.
Also, an XY cross-sectional plane was taken to determine the variations in the mesh
displacement of the structure.
Total mesh displacement for the elastic modulus of 0.35 MPa is displayed in Figure
6.11. Table 6.11 provides the summary of the results.

298
0.075 s 0.275 s
0.425 s
Figure 6.11 TMD distributions for the elastic modulus of 0.35MPa

299
Table 6.11 Observations pertaining to figure 6.11 Conditions Observations
E-wave Similar to the previous simulations, initially the elastic modulus was fixed (0.35 MPa)
and the Cf was varied for the three different phases. During the peak of the E-wave,
when the flow velocity was maximum through the inlet region, a much higher
displacement was in the apical region compared to its basal region. A maximum
magnitude of 7.5E-6 m was in the ventricle apex.
Diastasis During the diastasis phase, the flow velocity minimized and the magnitude of the Cf
increased. During this time period, the maximum displacement is still found to be in the
apical region of the ventricle with a value of around 7.5E-6 m. Simultaneously, a much
lower magnitude of displacement was observed in the basal region and in the core of the
cavity.
A-wave Later, during the peak A-wave, the maximum magnitude was still found to be in the
apical region of the ventricle with a value of 7.5E-6 m compared to its basal region. At
the same time, the magnitude of the displacement in the basal region and at the centre of
the ventricle was elevated compared with its diastasis phase, but the magnitude was still
lower than that of its apex.
6.4.5.2 Elastic modulus of 0.7MPa
Once again, the elastic modulus was considered fixed and the magnitudes of the Cf were
varied to determine the variations in the displacement during three different phases.
Table 6.12 provides the summary of the results.

300
0.075 s 0.275 s
0.425 s
Figure 6.12 TMD distributions for the elastic modulus of 0.7MPa

301
Table 6.12 Observations pertaining to figure 6.12 Conditions Observations
E-wave During the pinnacle of the E-wave, the maximum flow velocity enters through the inlet
region and at the same time, the elastic modulus was fixed to 0.7 MPa. During this time
period, the maximum magnitude of displacement with a value of 7.5E-6 m was in the
ventricle apex and the magnitude was slightly higher compared to its basal region.
Diastasis When the inlet waveform reached its diastasis phase, the inflow velocity became
minimal and the magnitude of the Cf increased. During this period, the maximum
magnitude of the displacement was still in the apical region but the magnitude with the
value of around 6.75E-6 m decreased compared to its peak E-wave. Also, a lower
magnitude of displacement was in the ventricle base and in the centre of the chamber.
A-wave During the peak of the A-wave, the inlet velocity rose once again and the magnitude of
the Cf decreased relative to the diastasis phase. During this time step, a higher magnitude
of the displacement was still evident in the apical region with a magnitude of around 6E-
6 m, but in the tip of the ventricle apex the magnitude was approximately 6.75E-6 m. At
the same time, the magnitude of the displacement in the basal region increased slightly
when compared with its diastasis region but it was still lower compared with its peak E-
wave.
6.4.5.3 Elastic modulus of 1.4 MPa
Images in Figure 6.13 show the variations in the displacement of the LV during three
different phases including the effects of the Cf and elastic modulus (1.4 MPa). Table
6.13 provides the summary of the results.

302
0.075 s 0.275 s
0.425 s
Figure 6.13 TMD distributions for the elastic modulus of 1.4MPa

303
Table 6.13 Observations pertaining to figure 6.13 Conditions Observations
E-wave During the peak E-wave, the flow rate increased through the mitral region and, during
this time step, the effects of elastic modulus and Cf were incorporated. With the time step
of 0.075 s, a much higher magnitude of 7.5E-6 was obtained in the apical region
compared to its basal region.
Diastasis During the slow filling phase, a maximum magnitude of the displacement with a value of
approximately 3E-6 m was obtained in the apical region of the LV. It should be noted
that, once again at the tip of the ventricle apex, a slightly higher magnitude of the
displacement with a value of around 3.75E-6 m was observed. Moreover the magnitude
of the Cf increased during this phase. Also, the magnitude of the displacement in the
basal region was much lower compared to its apical region.
A-wave During the peak A-wave, inflow velocity rose once again and with the added effect of
the Cf , the maximum magnitude was in the ventricle apex with a value of approximately
2.25E-6 m. Moreover, in the tip of the LV, a maximum value of around 3.75E-6 m was
found. Once again, a lower magnitude of displacement was in the basal region of the
ventricle but it was slightly higher when compared with its diastasis phase.
6.5 Discussion
6.5.1 The influence of Cf and elastic modulus on the LV using WSS distributions
From the simulations of the LV, including the effects of the Cf, it was evident that
almost identical results were obtained in three phases, after varying the magnitudes of
the elastic modulus. Subsequently, at the peak of the E-wave, a maximum magnitude of
WSS was obtained for all elastic modules. During this time step, the maximum
magnitude of the inflow jet entered through the inlet region and hence the influence of
the WSS was observed mostly on the ventricle wall incorporating the effects of the Cf
for all cases of elastic modulus. This could be attributed to the fact that the variations of
the wall shear depended on the discrepancies of the Cf. Because of minimal Cf (for
example, 0.125) on the LV wall, WSS was much higher, mostly during the peak of the
E-wave, for all elastic modulus.

304
As the inlet jet entered into the diastasis phase, the rate of inlet velocity jet was minimal
and entered through the mitral orifice. During this time (for example, t= 0.275 s) the
magnitude of the Cf increased and this added magnitude results in lower wall shear on
the ventricle wall. This could be ascribed to the fact that, due to the rise in the Cf on the
ventricle wall, resistance increased (Dellimore et al., 2013) which, in due course,
impeded the natural motion of the LV wall and hemodynamic system of the ventricle.
Once again, at the onset of the A-wave, the flow velocity started to accelerate and when
it reached the pinnacle of the A-wave, the inlet velocity rose and the jet entered through
the inlet region with increased velocity. During the peak A-wave, the magnitude of the
Cf was found to be much lower compared to the diastsasis phase but slightly higher than
the peak E-wave. Subsequently, from the simulations it was evident that with the
decrease in the magnitude of the Cf, wall shear elevated compared to the diastasis phase.
Hence, it can be stated, from the simulations that with a rise in the Cf the magnitude of
the wall shear decreased. Also, almost identical WSS distributions were found after
varying the magnitudes of the elastic modulus (Figure 6.2, Figure 6.3 and Figure 6.4).
Moreover, the deceleration in the ventricle wall motion also implied the functional
deficiencies for Dilated Cardiomyopathy (DCM) which severely influenced the natural
hemodynamics of the LV (B. T. Chan et al., 2012). Furthermore, the physiological
property of the ventricle changed due to the inadequacy of the required WSS, which
successively indicated the primary feature of the DCM disease conditions.
From the experimental investigations of (W et al., 1974, Hayashida et al., 1990),
moderately higher WSS was found for the DCM conditions compared to the natural LV.
However, using FSI simulations, Chan et al. 2012 (B. T. Chan et al., 2012) illustrated
that higher WSS could be found in the general LV compared to the dilated ventricle, but
they noted that similar wall thicknesses/elastic modulus had been utilized during the
simulations. On the other hand, the influence of the friction co-efficient was not
included in their investigations.
Varying the elastic modulus generated negligible influences on the WSS distributions
but changing the Cf during the simulations, meant that a clear idea for detecting and

305
determining the DCM condition could be achieved. Also, the findings from the
simulations using these parameters coincided well with the previously published
research.
Subsequently, it was well documented that cardiomyopathies are accountable for the
cardiac muscle dysfunction, which often develops the Congestive Heart Failure (CHF)
(Maisch et al., 2002). Therefore, from this viewpoint, it can be noted that the effects of
friction co-efficient and elastic modulus could also play a noteworthy role in identifying
CHF.
6.5.2 The influence of Cf and elastic modulus on the LV using Ip distributions
Once again, similar effects were found during the investigations of Ip distributions for
three phases of the diastolic flow cycle. During the pinnacle of the E-wave, for all three
elastic modulus, a maximum magnitude was found to be in the apical region of the LV,
close to the tip of the LV apex. During this E-wave, the maximum flow velocity entered
through the mitral region and propagated from the basal region to the apical region
inside the LV cavity. Hence, the maximum magnitude of Ip was found to be in the
ventricle apex compared to its basal region. Moreover, a ring shaped vortex was formed
for all cases, near the outlet tract during this time step. This could be attributed to the
fact that, because the Cf developed higher flow resistance (Dellimore et al., 2013),
hence a vortex formed during this time step.
When the flow velocity came to the diastasis phase, the magnitude of the Ip was still
found to be slightly higher in the apical region of the ventricle compared to its basal
region for all three phases. During this time step, the magnitude of the Cf increased and
because of that, the value of the overall Ip decelerated, even though the magnitude was
still higher in the ventricle apex. Once again, the primary vortex which was formed
earlier changed its location towards the core of the chamber and was moderately
elongated.

306
During the pinnacle of the A-wave, the flow rate increased and entered through the inlet
region. During this time, the magnitude of the Ip in the ventricle apex was
comparatively higher than the basal region. With the incoming jet through the mitral
region, the jet mixed and propagated with the fluid inside the cavity and because of this,
the apical pressure was higher compared to its basal region. It should be noted that,
during this time, the magnitude of the Cf reduced, which also resulted in a slightly
higher magnitude of the Ip in the ventricle apex. Also, the previously formed primary
vortex was seen enlarged in the centre of the cavity.
From the above discussions, it is evident that, a higher magnitude of Cf resulted in a
comparatively lower magnitude of Ip and vice-versa. Also, the variations in the Wt of
the LV had negligible effects on the Ip distributions. Moreover, the general trend in the
variations of the Ip, between the apical and basal region of the LV, during the peak E-
wave, diastasis and peak A-wave were in line with previously published investigations
(Arefin and Morsi, 2014, Cheng et al., 2005, Vierendeels et al., 1999). However it was
discovered that, during the peak E-wave, diastasis and peak A-wave, a vortex originated
and this could be attributed to the implied Cf where higher flow resistance was
generated and hence the vortex became evident during these time periods.
6.5.3 The influence of Cf and elastic modulus on the LV using velocity mapping
During the peak E-wave for all three phases, the maximum inlet velocity started to enter
through the inlet region. Also, the added effects of the Cf variations in the flow pattern
were determined. For all three elastic modulus during the pinnacle of the E-wave, a ring
shaped CW vortex developed near the outlet region. Simultaneously, twisting in the
flow pattern was observed in the ventricle apex. These phenomena could be attributed to
the added Cf , which developed higher flow resistance (Dellimore et al., 2013) and
helped generate the twisting in the flow pattern and concurrently develop an adherence
vortex close to the outlet region.

307
When the inlet velocity entered into the diastasis phase, the magnitude of the inlet
velocity minimized and during this phase, the magnitude of the Cf increased. Because of
these, a twisting of the flow pattern inside the ventricle was evident and it started to
move towards the core of the ventricle. With the deceleration in the inlet velocity
waveform the primary adherence vortex somewhat elongated and travelled towards the
centre of the ventricle. Simultaneously, a second weak vortex developed close to the
aortic orifice.
During the pinnacle of the A-wave, the inlet velocity elevated once again and with the
added effect of the Cf, changes in the flow dynamics were observed. During this time
period, the primary vortex started to merge with the propagation of the inlet jet. Also,
the secondary vortex was also seen somewhat merging with the fluid inside the
ventricle. However, it was still evident as it shifted its position close to the cul-de-sac of
the outlet region. It should be noted that this vortex was ring shaped and CW.
Moreover, no twisting in the flow pattern in the apical region was found and it could be
ascribed to the fact that the fluid inside the cavity (during the E-wave and diastasis),
along with the incoming fluid from the inlet region, mixed and merged together and
hence the fluid circulated normally during this time step.
Once again, from the simulation results it was determined that the Cf influenced the
flow pattern during these three phases. A much higher magnitude of velocity could be
found during the peak of the E-wave but, during the diastasis and the peak A-wave, the
magnitude of the velocity tended to be similar in the basal region. Also, the elastic
modulus did not directly alter the flow pattern during these three phases.
The general trends of the flow pattern, including the development, shifting and merging
of vortices were in line with previously published research (Arefin and Morsi, 2014,
Nakamura et al., 2002, Cheng et al., 2005). However, it should be noted that, with the
added effect of the Cf, variations in the flow pattern, including the generation of vortices
and twisting in the flow pattern were observed.

308
6.5.4 The influence of Cf and elastic modulus on the LV structure simulation using
total mesh displacement (TMD)
During the peak of the E-wave, maximum flow velocity entered through the inlet tract
and with the added effect of the elastic modulus and Cf, the variations in the
displacement of the structure were determined. From the simulation results, during the
peak E-wave, the maximum magnitude of the displacement was found in the apical
region for all thickness. However, with the rise in the elastic modules, the magnitude of
the displacement in the basal region started to decelerate. This could be attributed to the
fact that a higher elastic modulus provided stiffness to the ventricle wall and with the
added effect of Cf, a lower magnitude of displacement was found in the basal region.
Also, due to the maximum flow rate, during the E-wave, the jet started to propagate
from the inlet to the apical region and hence the magnitude of the displacement in the
apical region tended to be higher than the basal region.
During the diastasis phase, similar incidents were noted from the simulations. With a
rise in the elastic modules and the added effect of the Cf, the magnitudes of the
displacement in the ventricle apex started to decelerate. Precisely, higher elastic
modulus resulted in lower magnitude of the displacement. This could be ascribed to the
fact that, with the added effect of the Cf and minimal inlet velocity, due to diastasis, the
volume of the fluid inside the chamber tended to affect the displacement of the
structure. Specially, if the ventricle became stiffer, a lower magnitude of displacement
was found. Also, from the simulation results, a higher magnitude of displacement could
be found in the ventricle apex compared to its basal region for all elastic modulus
during this phase.
Later, during the peak A-wave, the inlet velocity started to rise once again and with the
added effect of the Cf, a much higher magnitude of the displacement was found to be in
the ventricle apex. Once more, with the rise in the elastic modules, the magnitudes of
the displacement in the ventricle apex decreased. Similarly, the magnitudes of the
displacement in the basal region decreased with the elevation in the elastic modules.

309
Therefore, from the results, it was evident that with the rise in the magnitude of the
elastic modulus and its added Cf the magnitudes of the displacement decreased. It is to
be noted that, because of the added friction co-efficient and elastic modulus of the LV
(DCM condition), total displacement of the LV was expected and found to be minimal.

310
6.6 Summary
From the above discussion and the simulation results, it was evident that the effect of
the elastic modulus and Cf certainly influenced the WSS distributions, Ip distributions,
velocity mapping and the structure simulations during the three phases of the diastolic
cycle. Specifically:
(i) WSS Distributions - It was determined that, with the increase in the Cf, the
magnitude of the wall shear decreased. Also, similar WSSs were found by
varying the magnitudes of the elastic modulus. Moreover, the effects of the Cf
provided a better basis for determining DCM disease conditions.
(ii) Ip Distributions - The effect of the Cf was also evident during the three phases.
Results suggested that, with the rise in the magnitude of the Cf, a lower Ip could
be found and vice-versa. However, changing the magnitudes of the elastic
modulus provided negligible effect on the Ip distributions. Moreover, for all
elastic modulus, maximum magnitudes of the Ip were found to be in the
ventricle apex.
(iii) Velocity Distributions - It was noted that the effect of the Cf changed the flow
pattern during these three phases. Precisely, during the peak E-wave, a much
higher magnitude of velocity was found in the basal region, but the velocity was
almost identical during the diastasis and the peak A-wave in the LV base. Once
again, the variations in the elastic modulus were found to have negligible effect
on the flow pattern during the peak E-wave, slow filling phase and the peak A-
wave. Also, the generation, shifting and merging of vortices were evident for all
elastic modulus during these three phases. Additionally, twisting in the flow
pattern was also noticeable during the peak E-wave and diastasis.
(iv) Structural Displacement - The results indicated that the magnitudes of the
displacement depended on both the Cf and elastic modulus. Specifically, the
increase in the elastic modulus and its added Cf resulted in a decrease in the
magnitudes of the displacement. Also, for all elastic modules, higher magnitudes

311
of the displacement were found in the apical region of the ventricle compared to
its basal region during these three phases. Moreover, due to the friction co-
efficient and co-efficient and elastic modulus of the LV (DCM) total magnitude
of the LV deformation was obtained to be minimal.

312
Chapter 7
Conclusions and Future Directions

313
7.1 Overall Conclusions of the Dissertation
The primary purpose of this Doctoral research program was to investigate engineering
issues associated with the development of a "next generation" Ventricular Assist Device
(VAD) system driven by a wireless controller. In order to determine the required
hemodynamic and physiological variations of the LV, FSI simulations were utilized for
different cardiac conditions during the filling phase.
As stated previously, the human heart is a complex 3D structure which functions as a
pump that circulates blood throughout the body. Cardiovascular diseases (CVD) arise
whenever natural blood circulation is hindered for any reason. These diseases greatly
affect morbidity and mortality (Vadakkumpadan et al., 2010) and thus, are a major area
of research at many levels. In this Doctoral research, the focus has been on the
engineering analysis elements that relate to CVD.
One of the critical and leading causes of death from CVD relates to heart failure (HF).
A particular problem of interest relates to Dilated Cardiomyopathy (DCM) or, more
specifically, a weakened heart muscle. Those who are afflicted with a weakened heart
muscle and/or hearts which are otherwise functioning efficiently - generally due to age
and a range of other causative factors - usually require a special device to assist the
functioning of their cardiac muscles effectively. To this end, ventricular assist devices
(VADs) are commonly utilized to aid cardiac structures to circulate blood throughout
the body.
VADs are frequently utilized to support various hemodynamic conditions inside the
human body but these devices have various limitations. One of the most frequent
complications relates to driveline infections which can actually lead to deterioration of
physical and hemodynamic conditions in the human body in the long run. Moreover:
• The size of the device
• Thromboembolism
• Requirements for special maintenance

314
and other issues also hinder the normal process of blood circulation (Pamboukian, 2011,
Friedman et al., 2011, Goldstein et al., 1998). Considering the particular complications
of driveline infections, along with other conditions of VAD systems, this Doctoral
research sought to provide critical, underlying engineering analysis that could be used in
order to develop a next generation VAD system using wireless technology.
In doing so, both experimental and computational approaches were deployed in order to
form the basis of a next generation VAD system. For the computational approaches, it
was challenging to simulate the hemodynamic conditions of the whole heart. Therefore,
the left ventricle (LV) of the heart was considered for the purpose of simulating the
hemodynamic and physiological conditions in different circumstances, namely:
• Examination of general flow dynamics
• Angular variations of the mitral and aortic orifice of the LV
• By varying the elastic modulus and friction co-efficient
The data generated from the simulations could then be used to make a VAD more
effective and efficient. Prior to the execution of a fully-coupled Fluid Structure
Interaction (FSI) scheme in the left ventricle of the heart, a realistic 3D model of the
• Coronary artery bypass graft (CABG)
• Abdominal aortic aneurysm (AAA)
were simulated. The execution of FSI on the CABG and aneurysm model provided
significant knowledge and insights both for both hemodynamics and physiological
properties. Subsequently, and in a similar way, simulations were conducted for the LV
of the heart where changes in both physiological and hemodynamic characteristics were
emphasized.
In Chapter 1, the details of CVDs were described along with various treatments. VADs
were also introduced and the usefulness and the inadequacies of these devices were
highlighted. The needs for enhanced (next generation) VADs were highlighted,
particularly where the existing VADs provided some serious clinical complications.
315
However, a detailed literature review was required to fully understand the problem at
hand and to find a suitable way to develop such a next generation VAD.
For these reasons, Chapter 2 described the physiological and hemodynamic
characteristics of the cardiac structure and its related components - specifically, heart
valves and the arterial system, as well as diseases and suitable treatments. Additionally,
this chapter also contained a discussion of earlier published research based on the
physiological and hemodynamic characteristics of the left ventricle, in terms of
experimental and computational approaches. Earlier investigations and analysis were
also reviewed in relation to dilated cardiomyopathy (DCM), both for experimental and
numerical approaches. This information was beneficial in gaining insights into the
limitations of existing systems and to utilize this data as a basis for constructing the next
generation VAD system.
In Chapter 3, FSI was initiated and utilized to investigate the flow dynamics and the
physiological characteristics of an anatomically correct CABG as well as aortic
aneurysm models. This numerical approach provided a basic understanding of the
hemodynamic and anatomical characteristics of the cardiovascular components. The
outcomes of these numerical simulations helped to facilitate the overall Doctoral
research work, as the primary objective was to simulate the physiological and
hemodynamic characteristics of the LV.
Chapter 4 described the detailed analysis of the hemodynamics and anatomical features
of the LV during the filling phase using FSI. The results were demonstrated in terms of:
• The intraventricular pressure (Ip) distributions
• Velocity profiles
• Wall shear stress (WSS)
• Maximum displacement of the structure
Even though the results were in line with earlier published investigations, these
computational approaches could define the complications related to the hemodynamics
and physiological physiognomies at any particular point of interest.

316
Subsequently, using FSI, variations in the hemodynamic and anatomical features were
computed by changing the angles between the mitral and aortic orifice during the
diastolic phase of the LV in the next chapter. Three different angles:
• 50°
• 55°
• 60°
were chosen between the mitral and aortic orifice to investigate the significance of the
flow dynamics and the structural variations of the LV. The results were also in
agreement with the previous findings. To the best of our knowledge, the variations in
the hemodynamic and physiological conditions of the LV by changing the aortic and
mitral orifices have not been presented till now. Moreover, this data would be very
effective in developing the wireless VAD even if there are angular differences.
In chapter 6, FSI was employed once again to perform simulations of the LV by
effectively varying the changes in the friction co-efficient and elastic modulus during
the filling phase. The results were investigated in terms of
• Wall Shear Stress WSS distributions
• Structural variations
• Ip distributions
• Velocity mapping
This investigation also provided the knowledge of DCM related to the LV in order to
determine the variations in the hemodynamic and anatomical features. Simulation
results stated that it is possible to identify the conditions of DCM by varying the elastic
modulus and friction co-efficient of the LV. Once more, to the best of our knowledge,
these significant findings have not been documented to date and this information, in
identifying DCM would be very effective as well in developing wireless VAD for the
DCM patients.

317
Moreover, it is to be noted that even though the computational fluid dynamics (CFD)
were extensively utilized by many researchers and engineers for a long time, but
different phenomena such as, turbulence, combustion and multi-phase flow were either
cannot be solved entirely using CFD or unable to characterize the real-time situations.
All these problems ultimately produce many errors and limitations in using different
numerical analysis (Do, 2012). These errors could be related to software, numerical
techniques, and generation of mesh/meshing, user and application errors. Though it is
possible to lessen these errors by many different ways, but substantial amount of time
and cost would be required to obtain the desired solution. In general, engineers and
researchers should equalize/balance between the time and cost and satisfactory
numerical simulation errors. Also, experiment validations were frequently conducted to
boost the confidence of the numerical results (Do, 2012, Do et al., 2011, Owida et al.,
2010, Owida et al., 2012).

318
7.2 Clinical Implications
7.2.1 Overview
In this section, clinical implications are presented for the effects of experimental devices
and the effects of flow dynamics and physiological features. Also, the significance of
the CABG graft and the aneurysm model are described clinically.
7.2.2 Significance of the next generation VAD system
As part of this overall Doctoral research program, and following on from the analytical
research documented herein, four different experimental designs of a new VAD system
were developed. Two experimental designs were developed individually and another
two experimental designs were developed by two undergraduate student groups from
Swinburne University of Technology using wireless technology. These VAD prototypes
were modelled using:
• A DC motor (self)
• Linear actuators and switching circuitry (self)
• Motor driver (Wajid Baryalai, Yining Wang, Abdul Aziz AlMalki and Majid Bin
Masoud) [Please see Appendix Figure A-4]
• Steel wings (Ahmed Salem Alrashdi, Abdulhakim Saud Almutarrid, Ahmed
Awad Aldhahri and Khaled Abdulhadi Alenezi) [Please see Appendix Figure A-
5]
These four approaches offered ideas and substantial insights into new VAD models.
Brief description is provided in Table A-1.
It was well known that the driveline infections from existing VADs posed major threats
to users in the long run and hence the application of wireless technology could provide
both flexibility and risk-reduced operating conditions to the users. From a clinical point

319
of consideration, this next generation wireless VAD device could assist patients affected
by heart failure and/or weakened heart muscle.
7.2.3 Significance of the CABG and aortic aneurysm models
Hemodynamic and structural displacement were investigated in the CABG graft model
and the results were optimized for the bypass graft artery model which was varied with
the degree of stenosis (0%, 30%, 50% and 75%) in the LAD (Left Anterior Descending)
region. More precisely, a correlation was established with the LAD-stenosis and the
WSS distribution including the spatial WSS, velocity mapping and the structural
displacement. Results indicated that a separation of the flow pattern could be identified
near the anatomosis region of the graft. With an increase in the degree of LAD-stenosis
(0%, 30%, 50% and 75%), variations in the hemodynamic features could also be
observed. Reverse-flow conditions were also found near the anatomosis angle and with
an increase in the LAD-stenosis, this flow condition receded accordingly.
Moreover, the findings from the WSS, incorporating the spatial distribution, indicated
that a much higher WSS was found in the anatomosis angle of the graft artery and the
WSS rose with the elevation in the inlet flow velocity. Maximum WSS was near the toe
of the artery, with a magnitude of 12.6 Pa for the 75% LAD-stenosis. Generally, the
effects of the WSS and the flow dynamics could alter considerably with a change in the
inlet flow velocity (Do, 2012). All these findings, including the flow dynamics and the
WSS, were in line with earlier published results (Do, 2012, Ding et al., 2012, Kouhi,
2011). Also, the maximum magnitude of the structural displacement was found to be
2.6 E-06 m which is close to the anatomosis angle for the 75% stenosis.
From a clinical point of view, the findings provided substantial insights for both
structural and hemodynamic features. Moreover, these qualitative and quantitative
findings were effective and could enable different degrees of LAD-stenosis to be re-
vascularized.

320
Similarly, from the aortic aneurysm model, the numerical approach provided substantial
insights and required data, based on physiological and hemodynamic features.
Clinically, this information could be useful in enabling an aneurysm to be re-
vascularized.
7.2.4 Significance of the LV model
A realistic, 3D model of the LV model was simulated in terms of general physiological
and hemodynamic features, by varying the inlet (mitral) and outlet (aortic) angles of the
LV and for the diseased condition, DCM, by changing the friction co-efficient and
elastic modulus of the LV. For all three cases, hemodynamics and the structural
displacement were investigated during the filling phase. Hemodynamics, which
included:
• The flow pattern including the development, merging and shifting of vortices
• Distribution of Ip
• WSS distribution
were computed numerically during the diastolic flow condition.
For the general condition of the LV, results demonstrated that variation in the pressure
inside the ventricle occurred due to the ventricle wall, during the filling flow condition.
The maximum magnitude of the Ip was 5.4E2 Pa. Also, the magnitude of the WSS was
increasing with the rise in the early filling wave (E-wave) and atrial filling wave (A-
wave) but the magnitude of the WSS was decreasing during the diastasis phase. The
maximum magnitude of WSS was 5.7 Pa. Moreover, generation, merging and shifting
of vortices were observed during the transmitral flow propagation but it was determined
that the flow dynamics could change during the late-diastolic phase. The maximum
magnitude of the velocity was 1.55 m/s. These results were in line with earlier
published results (Cheng et al., 2005, Watanabe et al., 2004, Nakamura et al., 2002).

321
The maximum magnitude of the structural displacement is found to be 3.7E-5 m in the
LV apex during the peak E-wave.
A similar approach was undertaken, using the angles of 50°, 55° and 60° respectively
between the mitral and aortic orifices of the LV, during the diastolic phase. To the best
of our knowledge, previous studies did not investigate the variations in the flow pattern
by changing the angles between the mitral and aortic orifices. Hence, the changes in the
Ip, flow propagation and the structural displacement were investigated for the first time.
Results demonstrated that, for the angular difference of 55°, the flow propagation and
shifting of vortices were somewhat different to the 50° and 60° cases. Also, for the
intraventricular pressure, after reaching the peak E-wave, when the flow propagation
was directing towards the diastais phase, a higher Ip was found in the apical region of
the LV for the 50° angular difference. The findings from the simulations matched and
agree well with the previous research (Vierendeels et al., 1999, Lassila et al., 2012).
Subsequently, WSS, Ip and the flow velocity of the LV were determined by varying the
friction co-efficient and the elastic modulus of the LV during the filling wave. Once
again, to the best of our knowledge no one incorporated the friction co-efficient and
elastic modulus to determine the DCM and therefore, for the first time these properties
were coupled together in determining the conditions of DCM. The findings proved that
with the rise in the friction co-efficient, the viscosity of the fluid increased which, in
turn, decreased the magnitude of the WSS, Ip and the velocity. Due to the decrease in
the WSS, Ip and the velocity, LV-wall motion subsided as well. This stipulation led to
the physiological inequity of the LV which suggested the primary condition of the DCM
and chronic heart failure (CHF). The changes in elastic modulus had minimal influence
on the friction co-efficient. However, varying the friction co-efficient and corresponding
elastic modulus effects helped identifying the functional behaviour of the LV
hemodynamics, DCM and CHF conditions.
Table 7.1 generalizes the primary features of the modelling performed in the doctoral
research.
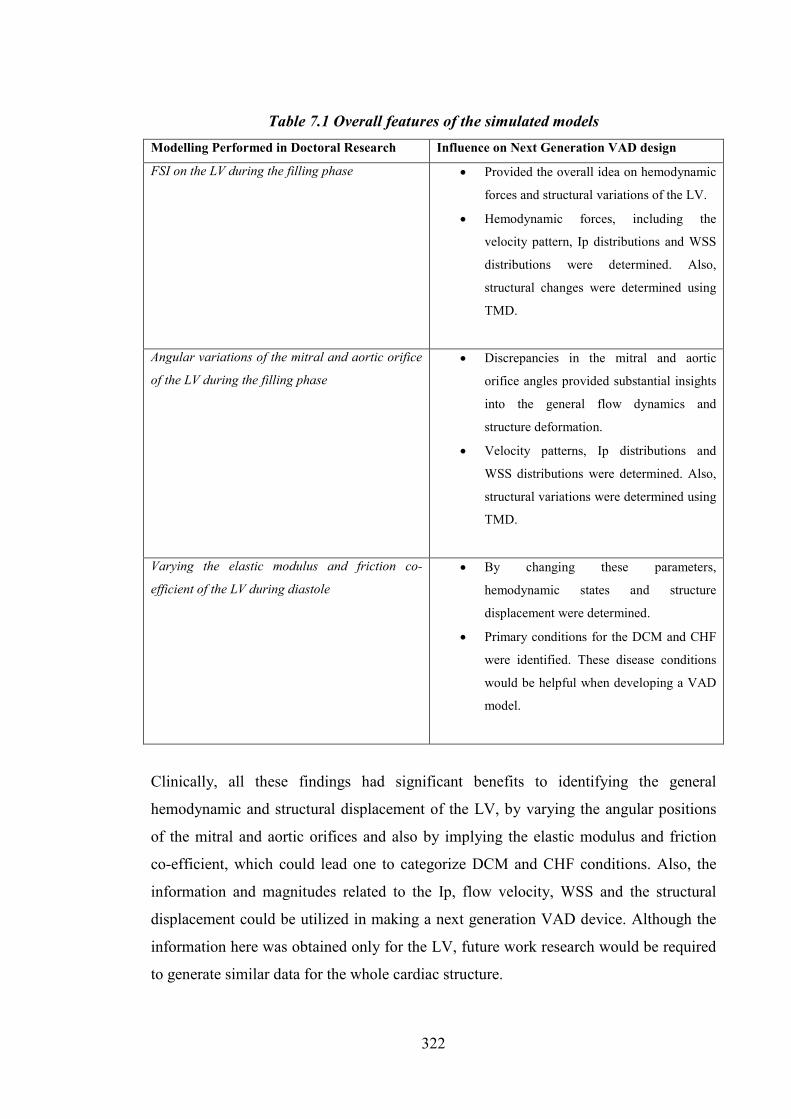
322
Table 7.1 Overall features of the simulated models Modelling Performed in Doctoral Research Influence on Next Generation VAD design
FSI on the LV during the filling phase • Provided the overall idea on hemodynamic
forces and structural variations of the LV.
• Hemodynamic forces, including the
velocity pattern, Ip distributions and WSS
distributions were determined. Also,
structural changes were determined using
TMD.
Angular variations of the mitral and aortic orifice
of the LV during the filling phase
• Discrepancies in the mitral and aortic
orifice angles provided substantial insights
into the general flow dynamics and
structure deformation.
• Velocity patterns, Ip distributions and
WSS distributions were determined. Also,
structural variations were determined using
TMD.
Varying the elastic modulus and friction co-
efficient of the LV during diastole
• By changing these parameters,
hemodynamic states and structure
displacement were determined.
• Primary conditions for the DCM and CHF
were identified. These disease conditions
would be helpful when developing a VAD
model.
Clinically, all these findings had significant benefits to identifying the general
hemodynamic and structural displacement of the LV, by varying the angular positions
of the mitral and aortic orifices and also by implying the elastic modulus and friction
co-efficient, which could lead one to categorize DCM and CHF conditions. Also, the
information and magnitudes related to the Ip, flow velocity, WSS and the structural
displacement could be utilized in making a next generation VAD device. Although the
information here was obtained only for the LV, future work research would be required
to generate similar data for the whole cardiac structure.

323
7.3 Future Directions and Recommendations
7.3.1 Overview
From the analysis documented in this dissertation, it is self-evident that further
investigations are required, involving both experimental and computational approaches.
The remaining future research needs are described here.
7.3.2 Experimental Requirements for VAD Prototype [including the works from two
undergraduate groups]
In general, to improve the next generation VAD model a range of investigations are
required. Specifically:
• It is necessary to determine the pressure exerted by the device on the cardiac
surface. This pressure can be calculated by determining the pressure exerted
from the connecting motors.
• An enclosure, made from polymers, needs to be wrapped around the device
to help expanding and contracting the whole cardiac structure precisely with
the heart beat (HB). Also, once the enclosure is attached, the required
pressure for the expansion and contraction of the cardiac structure needs to
be calculated and matched with the synchronization of the natural HB.
• Biocompatibility for the polymer and the VAD device needs to be assured.
• The power supply needs still needs a special attention. A wireless battery
charger may be an option for preventing surgery required for changing
existing power supplies.
• The total weight of the device needs to be reduced.

324
• Primarily, the VAD prototype was designed without considering any
attachment with the heart but, in the long run, this VAD prototype needs to
be connected effectively with the whole heart.
• This device needs to be tested in both in vitro and in vivo conditions to
ensure its dependability. Animal trials are required for the experiment
initially and this also will require FDA (Food and Drug Administration)
approval before installing the devices into human body.
• Alternatively, a neural classifier of the HB motion could be designed, which
could provide a fuzzy logic controller with precise information of the heart
rate. The fuzzy logic controller could be designed incorporating the HB
motion as an input which could then adaptively control the VAD prototype.
Moreover, an algorithm could be developed for diagnosing the critical
warning signals of the CHF and if this state is found, the necessary HB
motion pattern could be fed into the controller via the neural classifier.
7.3.3 Experimental Requirements of the LV Model
The following elements would be required in order to create the LV model:
• An exact shape of the LV would need to be obtained from MRI (Magnetic
Resonance Imaging) imaging.
• After getting the required values, an LV mould would need to be developed
in the conventional way and the Silicon (Si) rubber would be poured in the
mould to get a transparent Si-rubber LV model. This LV model would be
utilized for different testing using LDA (Laser Doppler Anemometers) and
PIV (Particle Image Velocimetry) measurements.

325
• Once the rubber model of LV was developed, colour liquid would be
decanted into the LV model. It should be noted that, the LV model would be
placed inside a bioreactor or suitable experimental setup where the liquid
would be given into the LV during the systole. Consequently, the LV would
be pushed by a piston, which is placed inside the bioreactor during the
diastolic phase where liquid would come back from the LV sac.
• Two mechanical valves, mitral and aortic, would be used for this
experiment. Therefore, the changes in the hemodynamic structure, including
the merging and shifting of vortices, Ip and the WSS would be defined along
with the structural displacement of the LV model. Moreover, tissue valves
could be implanted instead of mechanical valves and the flow pattern and
anatomical features for the LV could also be compared and determined.
• This result would then be matched with the simulated data to determine the
proper hemodynamic and anatomical data for the LV, which would be very
useful for developing the VAD prototype.
7.3.4 Computational and Experimental Requirements of the CABG and Aortic
Aneurysm Model
The following requirements need to be considered:
• In this research, only the general boundary conditions were applied in order to
investigate the flow dynamics and the anatomical features of these models.
Therefore, in vitro and in vivo boundary conditions need to be applied and
simulated. These would provide a better idea on the hemodynamic behaviour
and structural displacement by applying these boundary conditions. Also,
computational simulation codes could be very useful in order to improve the
accuracy of the whole simulations. These would assist in removing the

326
assumptions made during the simulations (Do, 2012). Moreover, in vivo
pulsatile flow analysis was required to determine the influence of the WSS.
• Although the validation of the numerical investigations here were shown to be
largely in line with other published computational research, but the results still
possessed a few discrepancies (Do, 2012) related to the study. Also, the findings
need to be matched with various experimental studies. Moreover, detailed
analysis on the WSS, flow dynamics and other parameters for the Newtonian
and non-Newtonian models and turbulent and laminar flows would be
determined at the location of the stenosis.
• The geometry utilized in the simulations is drawn using CAD (Computer Aided
Design) software. Therefore, CT-scan (Computed Tomography) or MRI images
can be segmented and utilized for further simulations. In doing so, geometric
complications could be minimized and the results can be made more accurate.
• Only a few selected degrees of LAD-stenosis (Ding et al., 2012) were applied
for the CABG model. Hence, research still needs to be carried out for various
degrees of stenosis and also the anastomosis angle should be varied.
• Moreover, the influence of the bypass graft, using different biomaterials, needs
to be carried out. Additionally, both the flow pattern and the structural
displacement need to be determined as well.
• Similarly, various investigations need to be carried out while changing the
bifurcations angle (β), neck angle (α) and by implying different asymmetry (Li,
2005) in the aneurysm main-body (AAA). Both the structural and hemodynamic
behaviour need to be investigated and determined.
• For both models, experimental studies are required. Moulds can be produced
similar to the LV model and by using the PIV and LDA techniques, the flow
pattern and physiological characteristics of the graft model could be determined.
Bioreactors could also be used for design and experimental purposes. Moreover,

327
an aneurysm model could be developed using the mould and similar
experimental approaches could be utilized for various investigations.
7.3.5 Computational Requirements of the LV Model
The following requirements need to be considered:
• Similar to the previous simulation approaches, in vitro and in vivo boundary
conditions, computational simulation codes and MRI images for the simulations
should be utilized.
• During the simulations, described herein, no valvular effects (mitral and aortic)
were considered. Therefore, both the aortic and mitral valves should be placed
and the related parameters should be determined. Also, systolic flow waveform
needs to be included during the simulations. Moreover, valvular diseases for the
mitral and aortic would be considered.
• More precisely, the myocardial contractility, including the structure-based strain
energy function and the stress tensor of the LV need to be evaluated. For
suitable mathematical formulas and details (Wang et al., 2013). Structure-based
strain energy function (Wang et al., 2013):
𝑊𝐼1, 𝐼4𝑓 , 𝐼4𝑠, 𝐼8𝑓𝑠 = 𝑎2𝑏
exp[𝑏(𝐼1 − 3)] + ∑ 𝑎𝑖2𝑏𝑖𝑖=𝑓,𝑠 exp[𝑏𝑖(𝐼4𝑖 − 1)2] − 1 +
𝑎𝑓𝑠2𝑏𝑓𝑠
exp 𝑏𝑓𝑠𝐼8𝑓𝑠2 − 1 𝑣𝑠 (7.1)
Where, a, b, ai, bi (i= f, s, fs) are eight positive-value material parameters. The
first term is denoted as the Fung-type expression, which resembles to the strain
energy of an isotropic matrix material. The other terms relates to the families of
collagen fibres entrenched inside the tissue. Also, it is presumed that the

328
collagen fibres maintain only lengthening but not the compression and hence the
terms involving 𝐼4𝑓 for i=f, s are denoted in the total energy only if 𝐼4𝑖 > 1.
Also, the stress tensor function (Wang et al., 2013):
𝜎 = 𝑭 𝜕𝑊𝜕𝐼𝑖𝑖=1,4𝑓,4𝑠,8𝑓𝑠
𝜕𝐼𝑖𝜕𝑭
– 𝑝𝑰
= −𝑝𝑰+ 𝑎𝑒𝑥𝑝 [𝑏(𝐼1 − 3)]𝑩
+2𝑎𝑓𝐼4𝑓 − 1 exp 𝑏𝑓𝐼4𝑓 − 12 𝒇⊗ 𝒇 + 2𝑎𝑠(𝐼4𝑠 − 1) exp[𝑏𝑠(𝐼4𝑠 − 1)2]𝒔⊗ 𝒔 +
𝑎𝑓𝑠𝐼8𝑓𝑠 exp 𝑏𝑓𝑠𝐼8𝑓𝑠2 (𝒇⊗ 𝒔+ 𝒔 ⊗ 𝒇) (7.2)
Where, p denotes the Lagrange multiplier initiated to implement the
incompressibility constraint; I denotes the identity tensor; 𝐁=𝐅𝐅𝑻 denotes the
left Cauchy-Green deformation tensor, and 𝐟=𝐅𝐟0 and 𝐬=𝐅𝐬0 denotes the fibre
and sheet axes in the current (i.e., deformed) configuration correspondingly.
• Similar approaches should be conducted in determining other cardiac chambers
(left atrium, right ventricle and right atrium). Also, the simulations of the VAD
enclosure need to be performed.
Once all these computational necessities are completed, all the data accumulated can be
applied to create a VAD prototype. This data will provide the precise hemodynamic and
structural pressure required for the whole cardiac structure to be expanded and
contracted properly by a VAD device. Initially all the computational and experimental
investigations ought to be performed for the natural heart but, in future, these
approaches could be performed for different cardiac disease-conditions.

329
Appendix
1. Variations in the velocity distributions of AAA
0.7 s 0.9 s
1 s
Figure A-1: Velocity distributions of the AAA in different time steps

330
2. Variations in the WSS of AAA
0.5 s 0.7 s
0.9 s 1 s
Figure A-2: WSS distributions of the AAA in different time steps

331
3. Variations in the structural displacement using TMD of AAA
0.7 s 0.9 s
1 s
Figure A-3: Structural displacement using total mesh displacement (TMD)
distributions

332
4. Experimental VAD prototype design – using DC motor and wireless technology
(a)
(b)
Figure A-4: VAD prototype using motor driver and wireless technology (a) External
controller (b) Internal controller

333
5. Experimental VAD prototype design – using steel wings and wireless technology
Figure A-5: VAD prototype using steel wings and wireless technology

334
Table A-1: Comparison between for approaches based on its overall characteristics
Appro
ach
no.
References VAD,
utilizing
Operatio
nal
Voltage(
V)
Uses of
Microcont
roller
Wireless Merits Demerits
1. Self DC
motor
24 No No Only for
demonstration
Too heavy and
requires higher
voltage
2. Self Linear
Actuator
s
12 Yes,
Arduino
Uno
No Only for
demonstration
Displacement/def
ormation is
minimum,
biocompatibility
and need to
fabricate it with
different values
3. Wajid
Baryalai,
Yining
Wang, Abdul
Aziz AlMalki
and Majid
Bin Masoud
Motor
Driver
7.4 Yes,
Arduino
Uno
Yes, XBee Observed
change in the
flow rate
Device size need
to be reduced,
biocompatibility
and modifications
are essential for
input signal
4. Ahmed
Salem
Alrashdi,
Abdulhakim
Saud
Almutarrid,
Ahmed
Awad
Aldhahri
and Khaled
Abdulhadi
Alenezi
Steel
Wings
3.7 Yes,
Arduino
Pro Mini
Yes,
Bluetooth
Reduced
weight, lower
power, easy to
carry
An enclosure
need to be
wrapped, made
from polymers
and
biocompatibility

335
List of Publications
Journal Papers:
1. M. S. Arefin and Y. Morsi, Fluid structure interaction (FSI) simulation of the left
ventricle (LV) during the early filling wave (E-wave), diastasis and atrial contraction
wave (A-wave), Australas Phys Eng Sci Med, 37(2), 2014. DOI: 10.1007/s13246-014-
0250-4
2. M. S. Arefin, Analyses of Hemodynamic and Structural Effects on Bypass Graft for
Different Levels of Stenosis Using Fluid Structure Interaction (FSI), Australas Phys Eng
Sci Med [To be Submitted]
3. M. S. Arefin, Fluid Structure Interaction (FSI) simulation of the left ventricle (LV)
during diastole: Hemodynamic effect by implementing and varying the friction
coefficient and wall thickness, Computer Methods in Biomechanics and Biomedical
Engineering [Submitted]
4. M. S. Arefin, Fluid Structure Interaction simulation of the Left Ventricle during the
diastolic period: The effect of the angles between the mitral and aortic orifice, Journal
of Computational Physics [To be Submitted]
5. M. S. Arefin, A review on the evolution of left ventricle (LV) experimental and
computational approaches: General and Dilated Cardiomyopathy (DCM) conditions,
European Journal of Mechanics – B/Fluids [To be Submitted]
Conference Paper:
1. Md. Shamsul Arefin and Yos S. Morsi, The effects of the angles between the mitral
and aortic orifices in the left ventricle (LV) using fluid structure interaction (FSI)
during filling phase, ICMMB, 2014.

336
Book Chapter:
1. Yos S. Morsi, Amal Ahmed Owida, Hung Do, Md. Shamsul Arefin, Xungai Wang,
Graft–Artery Junctions: Design Optimization and CAD Development, Computer-Aided
Tissue Engineering, Methods in Molecular Biology, Volume 868, 2012, pp 269-287.
DOI: 10.1007/978-1-61779-764-4_16

337
References
ADIB, M. A. H. M., HUI, K. Y., HASNI, N. H. M. & YASSIN, M. Y. M. 2012. Review: Development of Blood Flow through the Heart Valve Leaflet in Experimental Model International Journal of Engineering & Technology, 12, 93-97.
ADIB, M. A. H. M., NAIM, F., HASNI, N. H. M. & OSMAN, K. 2013. Prediction on Behaviour of Blood Velocity and Mitral Leaflet Displacement in the Different Shapes of Heart Valve during Cardiac Cycle. Journal of Biomimetics, Biomaterials & Tissue Engineering, 17, 79-85.
AGARWAL, S. & HIGH, K. M. 2012. Newer-generation ventricular assist devices. Best Practice & Research Clinical Anaesthesiology, 26, 117-130.
AREFIN, M. S. & MORSI, Y. 2014. Fluid structure interaction (FSI) simulation of the left ventricle (LV) during the early filling wave (E-wave), diastasis and atrial contraction wave (A-wave). Australasian Physical & Engineering Sciences in Medicine, 37, 413-423.
AWAD, H., DAYEM, M. A. E., HEARD, J., DIMITROVA, G., YU, L. & SUN, B. C. 2010. Initial experience with off-pump left ventricular assist device implantation in single center: retrospective analysis. J Cardiothorac Surg. , 5.
B. T. CHAN, C. W. ONG, E. LIM, N. A. ABU OSMAN, A. AL ABED, N. H. LOVELL & DOKOS, S. 2012. Simulation of Left Ventricle Flow Dynamics with Dilated Cardiomyopathy during the Filling Phase. 34th Annual International Conference of the IEEE EMBS, 6289 - 6292
BACCANI, B., DOMENICHINI, F. & PEDRIZZETTI, G. 2003. Model and influence of mitral valve opening during the left ventricular filling. Journal of Biomechanics, 36, 355-361.
BACCANI, B., DOMENICHINI, F., PEDRIZZETTI, G. & TONTI, G. 2002. Fluid dynamics of the left ventricular filling in dilated cardiomyopathy. Journal of Biomechanics, 35, 665-671.
BADII, C. 2012. Hypertensive Heart Disease [Online]. Available: http://www.healthline.com/health/hypertensive-heart-disease#Overview [Accessed 26th May 2014].
BAILEY, R. 2011. Cardiac Cycle [Online]. Available: http://biology.about.com/od/anatomy/ss/cardiac_cycle.htm.
BALOA, L. A., BOSTON, J. R. & ANTAKI, J. F. 2001. Elastance-Based Control of a Mock Circulatory System. Annals of Biomedical Engineering, 29, 244-251.
BARBOUR, D. J. & ROBERTS, W. C. 1986. Valve excision only versus valve excision plus replacement for active infective endocarditis involving the tricuspid valve. American Journal of Cardiology, 57, 475-478.
BARYALAI, W., WANG, Y., ALMALKI, A. A. & MASOUD, M. B. 2011. The Electro-Mechanical stimulation of Cardiac Processes. Swinburne University of Technology.
BASÇIFTÇI, F. & INCEKARA, H. 2011. Web based medical decision support system application of Coronary Heart Disease diagnosis with Boolean functions minimization method. Expert Systems with Applications, 38, 14037-14043.
BELLHOUSE, B. J. 1972. Fluid mechanics of a model mitral valve and left ventricle. Cardiovascular Research, 6, 199-210.
BENDER, J. R. 1992. Heart Valve Disease [Online]. Available: http://www.scribd.com/doc/39785094/HEART-VALVE-DISEASE [Accessed 12th November 2012].
BERGER, A., MACCARTHY, P. A., SIEBERT, U., CARLIER, S., WIJNS, W., HEYNDRICKX, G., BARTUNEK, J., VANERMEN, H. & DE BRUYNE, B. 2004. Long-Term Patency of Internal Mammary Artery Bypass Grafts: Relationship With Preoperative Severity of the Native Coronary Artery Stenosis. Circulation, 110, II-36-II-40.

338
BERTOLOTTI, C. & DEPLANO, V. 2000. Three-dimensional numerical simulations of flow through a stenosed coronary bypass. Journal of Biomechanics, 33, 1011-1022.
BERTOLOTTI, C., DEPLANO, V., FUSERI, J. & DUPOUY, P. 2001. Numerical and experimental models of post-operative realistic flows in stenosed coronary bypasses. Journal of Biomechanics, 34, 1049-1064.
BIANCO, C. 2000. How Your Heart Works [Online]. Available: http://health.howstuffworks.com/human-body/systems/circulatory/heart.htm [Accessed 15th July 2014].
BIJLANI, R. L. & MANJUNATHA, S. 2011. Understanding Medical Physiology. 4th ed.: Jaypee Brothers Medical Publishers.
BOUCEK, M. M., MASHBURN, C., DUNN, S. M., FRIZELL, R., EDWARDS, L., PIETRA, B. & CAMPBELL, D. 2008. Pediatric Heart Transplantation after Declaration of Cardiocirculatory Death. New England Journal of Medicine, 359, 709-714.
BOUTHILLET, T. 2011. Dick Cheney on his LVAD [Online]. Available: http://ems12lead.com/tag/left-ventricular-assist-device/ [Accessed 19th January 2014].
BRONZINO , J. D. 1999. The Biomedical Engineering Handbook, CRC Press. BRONZINO, J. D. 2006. Biomedical Engineering Fundamentals, CRC Press. BRÜCKER, C. 1997. Dual-camera DPIV for flow studies past artificial heart valves. Experiments
in Fluids, 22, 496-506. BRUCKER, C., STEINSEIFER, U., SCHRODER, W. & REUL, H. 2002. Unsteady flow through a new
mechanical heart valve prosthesis analysed by digital particle image velocimetry. Meas. Sci. Technol., 13, 1043–1049.
BURKE, D. J., BURKE, E., PARSAIE, F., POIRIER, V., BUTLER, K., THOMAS, D., TAYLOR, L. & MAHER, T. 2001. The HeartMate II: Design and Development of a Fully Sealed Axial Flow Left Ventricular Assist System. Artificial Organs, 25, 380-385.
CARDIO, L. 2014. The Need [Online]. Available: http://trendlines.com/portfolio/leviticus-cardio/ [Accessed 29th May 2014].
CENEDESE, A., DEL PRETE, Z., MIOZZI, M. & QUERZOLI, G. 2005. A laboratory investigation of the flow in the left ventricle of a human heart with prosthetic, tilting-disk valves. Experiments in Fluids, 39, 322-335.
CENTER, U. O. C. S. F. M. 2014. Heart Failure Treatment [Online]. Available: http://www.ucsfhealth.org/conditions/heart_failure/treatment.html [Accessed 28th May 2014].
CHAN, B. T., ABU OSMAN, N. A., LIM, E., CHEE, K. H., ABDUL AZIZ, Y. F., ABED, A. A., LOVELL, N. H. & DOKOS, S. 2013a. Sensitivity analysis of left ventricle with dilated cardiomyopathy in fluid structure simulation. PLoS One., 8.
CHAN, B. T., LIM, E., CHEE, K. H. & ABU OSMAN, N. A. 2013b. Review on CFD simulation in heart with dilated cardiomyopathy and myocardial infarction. Computers in Biology and Medicine, 43, 377-385.
CHANNEL, B. H. 2014. Heart disease - risk factors explained [Online]. Available: http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Heart_disease_your_risk-factors_explained [Accessed 28th May 2014].
CHENG, Y., OERTEL, H. & SCHENKEL, T. 2005. Fluid-Structure Coupled CFD Simulation of the Left Ventricular Flow During Filling Phase. Annals of Biomedical Engineering, 33.
CIOFFI, G., TARANTINI, L., DE FEO, S., PULIGNANO, G., DEL SINDACO, D., STEFENELLI, C., DI LENARDA, A. & OPASICH, C. 2005. Functional mitral regurgitation predicts 1-year mortality in elderly patients with systolic chronic heart failure. European Journal of Heart Failure, 7, 1112-1117.
COLACINO, F. M., MOSCATO, F., PIEDIMONTE, F., DANIELI, G., NICOSIA, S. & ARABIA, M. 2008. A Modified Elastance Model to Control Mock Ventricles in Real-Time: Numerical and

339
Experimental Validation. ASAIO Journal, 54, 563-573 10.1097/MAT.0b013e31818a5c93.
COLE, J. S., WATTERSON, J. K. & O’REILLY, M. J. G. 2002. Numerical investigation of the haemodynamics at a patched arterial bypass anastomosis. Medical Engineering & Physics, 24, 393-401.
COPE, C. 1963. Newer Techniques of Transseptal Left-Heart Catheterization. Circulation, 27, 758-761.
COUNCIL, N. H. A. M. R. 2014. Cardiovascular Disease (NHPA) [Online]. Available: http://www.nhmrc.gov.au/grants/research-funding-statistics-and-data/cardiovascular-disease [Accessed 18th July 2014].
COURTOIS, M., KOVÁCS JR, S. J. & LUDBROOK, P. A. 1988. Transmitral pressure-flow velocity relation. Importance of regional pressure gradients in the left ventricle during diastole. Circulation, 78, 661-671.
DE VECCHI, A., GOMEZ, A., PUSHPARAJAH, K., SCHAEFFTER, T., NORDSLETTEN, D. A., SIMPSON, J. M., PENNEY, G. P. & SMITH, N. P. 2014. Towards a fast and efficient approach for modelling the patient-specific ventricular haemodynamics. Progress in Biophysics and Molecular Biology, 116, 3-10.
DELLIMORE, K., KEMP, I., SCHEFFER, C., WEICH, H. & DOUBELL, A. 2013. The influence of leaflet skin friction and stiffness on the performance of bioprosthetic aortic valves. Australasian Physical & Engineering Sciences in Medicine, 36, 473–486.
DEPLANO, V. & SIOUFFI, M. 1999. Experimental and numerical study of pulsatile flows through stenosis:: Wall shear stress analysis. Journal of Biomechanics, 32, 1081-1090.
DI MARTINO, E. S., GUADAGNI, G., FUMERO, A., BALLERINI, G., SPIRITO, R., BIGLIOLI, P. & REDAELLI, A. 2001. Fluid–structure interaction within realistic three-dimensional models of the aneurysmatic aorta as a guidance to assess the risk of rupture of the aneurysm. Medical Engineering & Physics, 23, 647-655.
DING, J., LIU, Y., WANG, F. & BAI, F. 2012. Impact of Competitive Flow on Hemodynamics in Coronary Surgery: Numerical Study of ITA-LAD Model. Computational and Mathematical Methods in Medicine, 2012, 7.
DISEASE, T. H. G. I. F. H. V. About Valvular Heart Disease [Online]. Available: http://www.gilmanheartvalve.us/about_vhd_diseases.html [Accessed 2013 11th February].
DO, H., OWIDA, A. A., YANG, W. & MORSI, Y. S. 2011. Numerical simulation of the haemodynamics in end-to-side anastomoses. International Journal for Numerical Methods in Fluids, 67, 638-650.
DO, H. V. 2012. Design And Optimization Of Coronary Arteries Bypass Graft Using Numerical Method. Doctor of Philosophy, Swinburne University of Technology.
DOMENICHINI, F., PEDRIZZETTI, G. & BACCANI, B. 2005. Three-dimensional filling flow into a model left ventricle. J. Fluid Mech., 539, 179-198.
DOMENICHINI, F., QUERZOLI, G., CENEDESE, A. & PEDRIZZETTI, G. 2007. Combined experimental and numerical analysis of the flow structure into the left ventricle. Journal of Biomechanics, 40, 1988-1994.
DONEA, J., HUERTA, A., PONTHOT, J.-P. & RODR´ıGUEZ-FERRAN, A. 2004. Arbitrary Lagrangian–Eulerian Methods, John Wiley & Sons, Ltd.
DREAMSTIME. 2013. Royalty Free Stock Photo: Heart illustration cross section [Online]. Available: http://www.dreamstime.com/royalty-free-stock-photo-heart-illustration-cross-section-image1021695 [Accessed 8th February 2013].
DRUGS. 2012. Aortic Regurgitation [Online]. Available: http://www.drugs.com/cg/aortic-regurgitation.html [Accessed 12th February 2013].

340
EBBERS, T., BOLGER, A. F., WRANNE, B., KARLSSON, M. & WIGSTRÖM, L. 2002. Noninvasive Measurement of Time-Varying Three-Dimensional Relative Pressure Fields Within the Human Heart. Journal of Biomechanical Engineering, 124, 288-293.
ELGER, D. F., JOHANSEN, K. H., BLACKKETTER, D. M. & BUDWIG, R. S. 1996. The Influence of Shape on the Stresses in Model Abdominal Aortic Aneurysms. Journal of Biomechanical Engineering, 118, 326-332.
ELLIOTT, P., ANDERSSON, B., ARBUSTINI, E., BILINSKA, Z., CECCHI, F., CHARRON, P., DUBOURG, O., KÜHL, U., MAISCH, B., MCKENNA, W. J., MONSERRAT, L., PANKUWEIT, S., RAPEZZI, C., SEFEROVIC, P., TAVAZZI, L. & KEREN, A. 2007. Classification of the cardiomyopathies: a position statement from the european society of cardiology working group on myocardial and pericardial diseases. European Heart Journal.
EMETO, T. I., MOXON, J. V., RUSH, C., WOODWARD, L. & GOLLEDGE, J. 2011. Relevance of urocortins to cardiovascular disease. Journal of Molecular and Cellular Cardiology, 51, 299-307.
ESPA, S., BADAS, M. G., FORTINI, S., QUERZOLI, G. & CENEDESE, A. 2012. A Lagrangian investigation of the flow inside the left ventricle. European Journal of Mechanics - B/Fluids, 35, 9-19.
ESPA, S., FORTINI, S., QUERZOLI, G. & CENEDESE, A. 2013. Flow field evolution in a laboratory model of the left ventricle. Journal of Visualization, 16, 323-330.
ETHIER, R. C., STEINMAN, D. A., ZHANG, X., KARPIK, S. R. & OJHA, M. 1998. Flow waveform effects on end-to-side anastomotic flow patterns. Journal of Biomechanics, 31, 609-617.
FARRAR, D. J., BOURQUE, K., DAGUE, C. P., COTTER, C. J. & POIRIER, V. L. 2007. Design Features, Developmental Status, and Experimental Results With the Heartmate III Centrifugal Left Ventricular Assist System With a Magnetically Levitated Rotor. ASAIO Journal, 53, 310-315 10.1097/MAT.0b013e3180536694.
FERRARI, G., DE LAZZARI, C., MIMMO, R., TOSTI, G., AMBROSI, D. & GORCZYNSKA, K. 1998. A computer controlled mock circulatory system for mono- and biventricular assist device testing. Int J Artif Organs, 21, 26-36.
FILLINGER, M. F., MARRA, S. P., RAGHAVAN, M. L. & KENNEDY, F. E. 2003. Prediction of rupture risk in abdominal aortic aneurysm during observation: Wall stress versus diameter. Journal of Vascular Surgery, 37, 724-732.
FILLINGER, M. F., RAGHAVAN, M. L., MARRA, S. P., CRONENWETT, J. L. & KENNEDY, F. E. 2002. In vivo analysis of mechanical wall stress and abdominal aortic aneurysm rupture risk. Journal of Vascular Surgery, 36, 589-597.
FIRSTENBERG, M. S., VANDERVOORT, P. M., GREENBERG, N. L., SMEDIRA, N. G., MCCARTHY, P. M., GARCIA, M. J. & THOMAS, J. D. 2000. Noninvasive estimation of transmitral pressure drop across the normal mitral valve in humans: importance of convective and inertial forces during left ventricular filling. Journal of the American College of Cardiology, 36, 1942-1949.
FLUENT, A. 2013. Fluid–Structure Interaction [Online]. Available: http://www.ansys.com/Products/Simulation+Technology/Fluid+Dynamics/Fluid+Dynamics+Products/ANSYS+Fluent/Features/Fluid%E2%80%93Structure+Interaction [Accessed 25th October 2013].
FOGOROS, R. N. 2014a. Heart Failure - The Basics [Online]. Available: http://heartdisease.about.com/od/livingwithheartfailure/a/heart_failure.htm [Accessed 28th May 2014].
FOGOROS, R. N. 2014b. What Is Diastolic Dysfunction and Diastolic Heart Failure? [Online]. Available: http://heartdisease.about.com/od/livingwithheartfailure/a/diastolic_HF.htm [Accessed 28th May 2014].

341
FORMAGGIA, L., LAMPONI, D., TUVERI, M. & VENEZIANI, A. 2006. Numerical modeling of 1D arterial networks coupled with a lumped parameters description of the heart. Computer Methods in Biomechanics and Biomedical Engineering, 9, 273–288.
FORTINI, S., QUERZOLI, G., CENEDESE, A. & ESPA, S. 2010. 3D reconstruction of the flow inside the left ventricle model. 15th Int Symp on Applications of Laser Techniques to Fluid Mechanics. Lisbon, Portugal.
FORTINI, S., QUERZOLI, G., CENEDESE, A. & MARCHETTI, M. 2008. The Effect of Mitral Valve on Left Ventricular Flow. 14th Int Symp on Applications of Laser Techniques to Fluid Mechanics. Lisbon, Portugal.
FOUNDATION, H. Data and statistics [Online]. Available: http://www.heartfoundation.org.au/information-for-professionals/data-and-statistics/Pages/default.aspx [Accessed 28th May 2014].
FRAUENFELDER, T., BOUTSIANIS, E., SCHERTLER, T., HUSMANN, L., LESCHKA, S., POULIKAKOS, D., MARINCEK, B. & ALKADHI, H. 2007. Flow and wall shear stress in end-to-side and side-to-side anastomosis of venous coronary artery bypass grafts. BioMedical Engineering OnLine, 6, 1-13.
FRAZIER, O. H., MYERS, T. J. & RADOVANCEVIĆ, B. 1998. The HeartMate left ventricular assist system. Overview and 12-year experience. Tex Heart Inst J. , 25, 265–271.
FRESHWATER IJ, M. Y., LAI T 2006. The effect of angle on wall shear stresses in a LIMA to LAD anastomosis: numerical modelling of pulsatile flow. Proc Inst Mech Eng H. , 220, 743-57.
FRIEDMAN, P. A., KUSHWAHA, S. S., BRUCE, C. J., PARK, S. J., LADEWIG, D. J., MIKELL, S. B., JOHNSON, S. B., SUDDENDORF, S. H., DANIELSEN, A. J. & ASIRVATHAM, S. J. 2011. Use of the Aortoatrial Continuity as Means of Providing Left Ventricular Assist Support Without Entering the Ventricle: A Feasibility Study. Journal of Cardiac Failure, 17, 511-518.
FURUSATO, M., SHIMA, T., KOKUZAWA, Y., ITO, K., TANAKA, T., IWASAKI, K., QIAN, Y., UMEZU, M., YAN, Z. & ZHU, L. 2007. A Reproduction of Inflow Restriction in the Mock Circulatory System to Evaluate a Hydrodynamic Performance of a Ventricular Assist Device in Practical Conditions. In: LI, K., LI, X., IRWIN, G. & HE, G. (eds.) Life System Modeling and Simulation. Springer Berlin Heidelberg.
GARBADE, J., BITTNER, H. B., BARTEN, M. J. & MOHR, F.-W. 2011. Current Trends in Implantable Left Ventricular Assist Devices. Cardiology Research and Practice, 2011.
GEORGAKARAKOS, E., IOANNOU, C. V., GEORGIADIS, G. S., KAPOULAS, K., SCHORETSANITIS, N. & LAZARIDES, M. 2011. Expanding Current EVAR Indications to Include Small Abdominal Aortic Aneurysms: A Glimpse of the Future. Angiology, 62, 500-503.
GIUMA, S. K. B., OSMAN, K. & KADIR, M. R. A. 2013. Fluid Structure Interaction Analysis in Abdominal Aortic Aneurysms: Influence of Diameter, Length, and Distal Neck. Journal of Medical Imaging and Health Informatics, 3, 514-522.
GLASS, N. & PONSFORD, M. 2014. Wireless electricity? It's here [Online]. Available: http://edition.cnn.com/2014/03/14/tech/innovation/wireless-electricity/ [Accessed 29th May 2014].
GOLDSTEIN, D. J., OZ, M. C. & ROSE, E. A. 1998. Implantable Left Ventricular Assist Devices. New England Journal of Medicine, 339, 1522-1533.
GOUBERGRITS, L., AFFELD, K., WELLNHOFER, E., ZURBRÜGG , R. & HOLMER, T. 2001. Estimation of wall shear stress in bypass grafts with computational fluid dynamics method. Int J Artif Organs. , 24, 145-51.
GREGORY, S., TIMMS, D., PEARCY, M. J. & TANSLEY, G. 2009. A naturally shaped silicone ventricle evaluated in a mock circulation loop: A preliminary study. Journal of Medical Engineering & Technology, 33, 185-191.

342
GROSSMAN, W., MCLAURIN, L. P. & ROLETT, E. 1979. Alterations in left ventricular relaxation and diastolic compliance in congestive cardiomyopathy. Cardiovascular Research, 13, 514-522.
GUNJA-SMITH, Z., MORALES, A. R., ROMANELLI, R. & WOESSNER, J. J. F. 1996. Remodeling of human myocardial collagen in idiopathic dilated cardiomyopathy. Role of metalloproteinases and pyridinoline cross-links. Am J Pathol. , 148, 1639–1648.
GUREV, V., LEE, T., CONSTANTINO, J., AREVALO, H. & TRAYANOVA, N. 2011. Models of cardiac electromechanics based on individual hearts imaging data: image-based electromechanical models of the heart. Biomech Model Mechanobiol. , 10, 295-306.
HARTFORD, J. 2013. Wireless Power For Medical Devices [Online]. Available: http://www.mddionline.com/article/wireless-power-medical-devices [Accessed 29th May 2014].
HAYASHIDA, W., KUMADA, T., NOHARA, R., TANIO, H., KAMBAYASHI, M., ISHIKAWA, N., NAKAMURA, Y., HIMURA, Y. & KAWAI, C. 1990. Left ventricular regional wall stress in dilated cardiomyopathy. Circulation, 82, 2075-83.
HEALTH, F. 2012. What Is Coronary Heart Disease? [Online]. Available: http://familyhealth-center.blogspot.com.au/2012/05/what-is-coronary-heart-disease.html [Accessed 28th May 2014].
HEALTHCENTRAL. 2010. Tricuspid regurgitation [Online]. Available: http://www.healthcentral.com/ency/408/000169.html?ic=506019 [Accessed 15th February 2013].
HEALTHCENTRAL. 2013a. Mitral Valve Stenosis [Online]. Available: http://www.healthcentral.com/encyclopedia/408/714.html [Accessed 12th February 2013].
HEALTHCENTRAL. 2013b. Tricuspid Valve Disease [Online]. Available: http://www.healthcentral.com/encyclopedia/408/93.html?ic=506048 [Accessed 12th February 2013].
HEALTHCENTRAL. 2014. Aortic Valve Stenosis [Online]. Available: http://www.healthcentral.com/encyclopedia/408/531.html?ic=506048 [Accessed 27th May 2014].
HEARTVALVESURGERY. 2012. Tricuspid Valve Stenosis [Online]. Available: http://www.heart-valve-surgery.com/tricuspid-stenosis.php [Accessed 12th February 2013].
HERSHBERGER, R. E. & MORALES, A. 2013. Dilated Cardiomyopathy Overview [Online]. Available: http://www.ncbi.nlm.nih.gov/books/NBK1309/ [Accessed 25th November 2013].
HETZER, R., MÜLLER, J., WENG, Y., WALLUKAT, G., SPIEGELSBERGER, S. & LOEBE, M. 1999. Cardiac recovery in dilated cardiomyopathy by unloading with a left ventricular assist device. The Annals of thoracic surgery, 68, 742-749.
HO, J. S., KIM, S. & POON, A. S. Y. 2013. Midfield wireless powering for implantable systems. Proceedings of the IEEE, 101, 1369-1378.
HOSHI, H., SHINSHI, T. & TAKATANI, S. 2006. Third-generation Blood Pumps With Mechanical Noncontact Magnetic Bearings. Artificial Organs, 30, 324-338.
HOSPIMEDICA. 2012. Cardiac Implants Could Potentially Be Powered Wirelessly [Online]. Available: http://www.hospimedica.com/critical_care/articles/294742895/cardiac_implants_could_potentially_be_powered_wirelessly.html [Accessed 29th May 2014].
HOSPITAL, L. P. C. S. 2013. Pulmonary Stenosis [Online]. Available: http://www.lpch.org/DiseaseHealthInfo/HealthLibrary/cardiac/ps.html [Accessed 12th February 2013].
HUA, J. & MOWER, W. R. 2001. Simple geometric characteristics fail to reliably predict abdominal aortic aneurysm wall stresses. Journal of Vascular Surgery, 34, 308-315.

343
HUERTA, A. & LIU, W. K. 1998. VISCOUS FLOW WITH LARGE FREE SURFACE MOTION. COMPUTER METHODS IN APPLIED MECHANICS AND ENGINEERING, 69, 277-324.
HUNG, T. K., BALASUBRAMANIAN, S. R., SIMON, M. A., SUFFOLETTO, M. S., BOROVETZ, H. S. & GORCSAN, J. 2008. Hemodynamic information and analysis of cardiac pumping Journal of Mechanics in Medicine and Biology, 08, 87-95.
HUNT, S. A., ABRAHAM, W. T., CHIN, M. H., FELDMAN, A. M., FRANCIS, G. S., GANIATS, T. G., JESSUP, M., KONSTAM, M. A., MANCINI, D. M., MICHL, K., OATES, J. A., RAHKO, P. S., SILVER, M. A., STEVENSON, L. W. & YANCY, C. W. 2009. 2009 Focused Update Incorporated Into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults. Circulation, 119, e391-e479.
HUNTER, W. C., JANIKCI, J. S., WEBER, K. T. & NOORDERGRAAF, A. 1979. Flow-pulse response: a new method for the characterization of ventricular mechanics. Am. J. Physiol., 237.
INSTITUTE, N. H. L. A. B. 2012. What Is a Ventricular Assist Device? [Online]. Available: http://www.nhlbi.nih.gov/health/health-topics/topics/vad/ [Accessed 28th May 2014].
JACOBS, L. E., KOTLER, M. N. & PARRY, W. R. 1990. Flow patterns in dilated cardiomyopathy: a pulsed-wave and color flow Doppler study. J Am Soc Echocardiogr. , 3, 294-302.
JEFFERIES, J. L. & TOWBIN, J. A. 2010. Dilated cardiomyopathy. The Lancet, 375, 752-762. JONES, T. & METAXAS, D. 1998. Patient-specific analysis of left ventricular blood flow. In:
WELLS, W., COLCHESTER, A. & DELP, S. (eds.) Medical Image Computing and Computer-Assisted Interventation — MICCAI’98. Springer Berlin Heidelberg.
KABINEJADIAN, F. & GHISTA, D. N. 2012. Compliant model of a coupled sequential coronary arterial bypass graft: Effects of vessel wall elasticity and non-Newtonian rheology on blood flow regime and hemodynamic parameters distribution. Medical Engineering & Physics, 34, 860-872.
KELDERMANN, R. H., NASH, M. P., GELDERBLOM, H., WANG, V. Y. & PANFILOV, A. V. 2010. Electromechanical wavebreak in a model of the human left ventricle. American Journal of Physiology - Heart and Circulatory Physiology, 299, H134-H143.
KERCKHOFFS, R. C. P., FARIS, O. P., BOVENDEERD, P. H. M., PRINZEN, F. W., SMITS, K., MCVEIGH, E. R. & ARTS, T. 2003. Timing of Depolarization and Contraction in the Paced Canine Left Ventricle. Journal of Cardiovascular Electrophysiology, 14, S188-S195.
KHALAFVAND, S. S. 2013. Combined CFD/MRI analysis of blood flow in human left ventricle. Doctor of Philosophy, Nanyang Technological University.
KHALAFVAND, S. S., NG, E. Y. K. & ZHONG, L. 2011. CFD simulation of flow through heart: a perspective review. Computer Methods in Biomechanics and Biomedical Engineering, 14, 113–132.
KILNER, P. J., YANG, G.-Z., WILKES, A. J., MOHIADDIN, R. H., FIRMIN, D. N. & YACOUB, M. H. 2000. Asymmetric redirection of flow through the heart. Nature, 404, 759-761.
KIM, S., HO, J. S., CHEN, L. Y. & POON, A. S. Y. 2012. Wireless power transfer to a cardiac implant. Applied Physics Letters, 101, -.
KIM, W. Y., BISGAARD, T., NIELSEN, S. L., POULSEN, J. K., PEDERSEN, E. M., HASENKAM, J. M. & YOGANATHAN, A. P. 1994. Two-dimensional mitral flow velocity profiles in pig models using epicardial doppler echocardiography. Journal of the American College of Cardiology, 24, 532-545.
KIM, W. Y., WALKER, P. G., PEDERSEN, E. M., POULSEN, J. K., OYRE, S., HOULIND, K. & YOGANATHAN, A. P. 1995. Left ventricular blood flow patterns in normal subjects: A quantitative analysis by three-dimensional magnetic resonance velocity mapping. Journal of the American College of Cardiology, 26, 224-238.
KLABUNDE, R. E. 2011. Cardiovascular Physiology Concepts, Lippincott Williams & Wilkins. KLEINSTREUER, C., CHILDRESS, E. & FARBER, M. 2013. Assessment of aortic aneurysm rupture
risk and surgical repair.

344
KOENIG, S. C., PANTALOS, G. M., GILLARS, K. J., EWERT, D. L., LITWAK, K. N. & ETOCH, S. W. 2004. Hemodynamic and Pressure–Volume Responses to Continuous and Pulsatile Ventricular Assist in an Adult Mock Circulation. ASAIO Journal, 50, 15-24.
KOUHI, E. 2011. An Advanced Fluid Structure Interaction Study of Tri-leaflet Aortic Heart Valve. Doctor of Philosophy, Swinburne University of Technology.
KOUHI, E., MORSI, Y. S. & MASOOD, S. H. 2008. Haemodynamic analysis of coronary artery bypass grafting in a non-linear deformable artery and Newtonian pulsatile blood flow. Proc Inst Mech Eng H. , 222, 1273-87.
KRITTIAN, S., JANOSKE, U., OERTEL, H. & BÖHLKE, T. 2010. Partitioned Fluid–Solid Coupling for Cardiovascular Blood Flow. Annals of Biomedical Engineering, 38, 1426-1441.
KŬTOVA, T., CHICHOVSKI, K., KHEKIMIAN, A. & SAVOVA, A. 1981. Echocardiographic diagnosis of congestive cardiomyopathy associated with mitral regurgitation. Vutr Boles. , 20, 81-6.
LAIZZO, P. A. 2009. Handbook of Cardiac Anatomy, Physiology, and Devices, Springer. LANZA, R. P., LANGER, R. S. & VACANTI, J. 2007. Principles of tissue engineering, Burlington, MA
: Elsevier Academic Press, 2007. LASSILA, T., MALOSSI, A. C. I., STEVANELLA, M., VOTTA, E., REDAELLI, A. & DEPARIS, S. 2012.
Multiscale fluid-structure interaction simulation of patient-specific left ventricle fluid dynamics with fictitious elastic structure regularization. Int. J. Numer. Meth. Biomed. Engng., 00, 1-23.
LASSILA, T., MANZONI, A., QUARTERONI, A. & ROZZA, G. 2013. A reduced computational and geometrical framework for inverse problems in hemodynamics. International Journal for Numerical Methods in Biomedical Engineering, 29, 741-776.
LAVU, M., GUNDEWAR, S. & LEFER, D. J. 2011. Gene therapy for ischemic heart disease. Journal of Molecular and Cellular Cardiology, 50, 742-750.
LE, T. B. & SOTIROPOULOS, F. 2013. Fluid–structure interaction of an aortic heart valve prosthesis driven by an animated anatomic left ventricle. Journal of Computational Physics, 244, 41-62.
LEE, J., NIEDERER, S., NORDSLETTEN, D., GRICE, I. L., SMAIL, B., KAY, D. & SMITH, N. 2009. Coupling contraction, excitation, ventricular and coronary blood flow across scale and physics in the heart. Phil. Trans. R. Soc. A, 367, 2311-2331.
LEMMON, J. D. & YOGANATHAN, A. P. 2000. Computational modeling of left heart diastolic function: examination of ventricular dysfunction. J. Biomech. Eng., 122, 297-303.
LEVIN, H. R., OZ, M. C., CATANESE, K. A., ROSE, E. A. & BURKHOFF, D. 1996. Transient normalization of systolic and diastolic function after support with a left ventricular assist device in a patient with dilated cardiomyopathy. J Heart Lung Transplant. , 15, 840-2.
LEVISMAN, J. A. 1977 Echocardiographic diagnosis of mitral regurgitation in congestive cardiomyopathy. Am Heart J. , 93, 33-9.
LI, B. 2011. Hardware Accelerated Non-Rigid Registration for the Evaluation of Cardiac Function. Doctor of Philosophy, University of Auckland.
LI, Z. 2005. Computational Analyses and Simulations of Fluid-Structure Interactions Applied to Stented Abdominal Aortic Aneurysms. Doctor of Philosophy, North Carolina State University.
LI, Z. & KLEINSTREUER, C. 2005. A New Wall Stress Equation for Aneurysm-Rupture Prediction. Annals of Biomedical Engineering, 33, 209-213.
LI, Z. & KLEINSTREUER, C. 2006. Effects of blood flow and vessel geometry on wall stress and rupture risk of abdominal aortic aneurysms. Journal of Medical Engineering & Technology, 30, 283-297.

345
LIDEN, H., KARASON, K., BERGH, C.-H., NILSSON, F., KOUL, B. & WIKLUND, L. 2007. The feasibility of left ventricular mechanical support as a bridge to cardiac recovery. European Journal of Heart Failure, 9, 525-530.
LOEBE, M., WENG, Y., MÜLLER, J., DANDEL, M., HALFMANN, R., SPIEGELSBERGER, S. & HETZER, R. 1997. Successful mechanical circulatory support for more than two years with a left ventricular assist device in a patient with dilated cardiomyopathy. J Heart Lung Transplant., 16, 1176-9.
LOERAKKER, S., COX, L. G. E., VAN HEIJST, G. J. F., DE MOL, B. A. J. M. & VAN DE VOSSE, F. N. 2008. Influence of dilated cardiomyopathy and a left ventricular assist device on vortex dynamics in the left ventricle. Computer Methods in Biomechanics and Biomedical Engineering, 11, 649-660.
LONG, Q., MERRIFIELD, R., YANG, G., KILNER, P., FIRMIN, D. & XU, X. 2003. The influence of inflow boundary conditions on intra left ventricle flow predictions. J Biomech Eng., 125, 922-7.
MAISCH, B., RISTIĆ, A. D., HUFNAGEL, G., FUNCK, R., ALTER, P., TONTSCH, D. & PANKUWEIT, S. 2002. Dilated Cardiomyopathies as a Cause of Congestive Heart Failure. Herz, 27, 113-134.
MAKSYMOWICZ, K., KOBIELARZ, M. & CZOGAŁA, J. 2011. Potential indicators of the degree of abdominal aortic aneurysm development in rupture risk estimation. Advances in Clinical and Experimental Medicine, 20, 221-225.
MANGUAL, J. O., KRAIGHER-KRAINER, E., DE LUCA, A., TONCELLI, L., SHAH, A., SOLOMON, S., GALANTI, G., DOMENICHINI, F. & PEDRIZZETTI, G. 2013. Comparative numerical study on left ventricular fluid dynamics after dilated cardiomyopathy. Journal of Biomechanics, 46, 1611-1617.
MARKL, M., KILNER, P. J. & EBBERS, T. 2011. Comprehensive 4D velocity mapping of the heart and great vessels by cardiovascular magnetic resonance. Journal of Cardiovascular Magnetic Resonance, 13.
MARON, B. J., TOWBIN, J. A., THIENE, G., ANTZELEVITCH, C., CORRADO, D., ARNETT, D., MOSS, A. J., SEIDMAN, C. E. & YOUNG, J. B. 2006. Contemporary Definitions and Classification of the Cardiomyopathies: An American Heart Association Scientific Statement From the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation, 113, 1807-1816.
MARTUFI, G. & GASSER, T. C. 2013. Review: The Role of Biomechanical Modeling in the Rupture Risk Assessment for Abdominal Aortic Aneurysms. Journal of Biomechanical Engineering, 135, 021010-021010.
MATTOX, M. 2013. Managing heart failure with mHealth [Online]. Available: http://axialexchange.com/blog/article/managing-heart-failure-with-mhealth [Accessed 28th May 2014].
MAUGHAN, W. L., SUNAGAWA, K., BURKHOFF, D., GRAVES, W. L., HUNTER, W. C. & SAGAWA, K. 1985. Effect of heart rate on the canine end-systolic pressure-volume relationship. Circulation, 72, 654-9.
MCCULLOCH, A. 2004. Functionally and structurally integrated computational modeling of ventricular physiology. Jpn J Physiol., 54, 531-9.
MCQUEEN, D. M. & PESKIN, C. S. 2000. A three-dimensional computer model of the human heart for studying cardiac fluid dynamics. ACM SIGGRAPH Computer Graphics, 34, 56-60.
MEDIC, L. A. A. 2011. The amazing human heart [Online]. Available: http://accesstomedicine.wordpress.com/2011/11/28/the-amazing-human-heart/ [Accessed 26th May 2014].

346
MEDINDIA. 2014. Mitral Valve Regurgitation | Mitral Valve Replacement | Mitral Valve Stenosis [Online]. Available: http://www.medindia.net/patients/patientinfo/mitral-valve-regurgitation-replacement.htm [Accessed 27th May 2014].
MIHALEF, V., IONASEC, R. I., SHARMA, P., GEORGESCU, B., VOIGT, I., SUEHLING, M. & COMANICIU, D. 2011. Patient-specific modelling of whole heart anatomy, dynamics and haemodynamics from four-dimensional cardiac CT images. Interface Focus, 1, 286-296.
MILLER, R. 2012. 'Tetherless' Power-Transmission Technology Could Radically Change LVAD Therapy [Online]. Medscape. Available: http://www.medscape.com/viewarticle/758065#1 [Accessed 28th January 2014].
MOAZAMI, N., SUN, B., FELDMAN, D. 2011. Stable patients on left ventricular assist device support have a disproportionate advantage: Time to re-evaluate the current UNOS policy. Journal of Heart and Lung Transplantation 30, 971-974.
MOHR, R. & KRAMER, A. 2006. Left-Sided Myocardial Revascularization with Bilateral Skeletonized Internal Thoracic Artery. In: HE, G.-W. (ed.) Arterial Grafting for Coronary Artery Bypass Surgery.
MOLINA, E. J. & BOYCE, S. W. 2013. Current Status of Left Ventricular Assist Device Technology. Seminars in Thoracic and Cardiovascular Surgery, 25, 56-63.
MONAGHAN, R. J. 1953. A Review and Assessment of Various Formulae for Turbulent Skin Friction in Compressible Flow Aeronautical Research Council, Ministry of Supply.
MORSI, Y., OWIDA, A., DO, H., AREFIN, M. S. & WANG, X. 2012. Graft–Artery Junctions: Design Optimization and CAD Development. In: LIEBSCHNER, M. A. K. (ed.) Computer-Aided Tissue Engineering. Humana Press.
MORSI, Y. S. 2011. Tissue Engineering of Aortic Heart Valve: Fundamentals and Developments, Nova Science Publishers.
MOURET, F., GARITEY, V., GANDELHEID, T., FUSERI, J. & RIEU, R. 2000. A new dual activation simulator of the left heart that reproduces physiological and pathological conditions. Med Biol Eng Comput. , 38, 558-61.
MOZES, A. 2011. Stem Cell Therapy Shrinks Enlarged Hearts [Online]. Available: http://consumer.healthday.com/cardiovascular-and-health-information-20/heart-attack-news-357/stem-cell-therapy-shrinks-enlarged-hearts-650937.html [Accessed 29th May 2014].
NAGUEH, S. F., APPLETON, C. P., GILLEBERT, T. C., MARINO, P. N., OH, J. K., SMISETH, O. A., WAGGONER, A. D., FLACHSKAMPF, F. A., PELLIKKA, P. A. & EVANGELISA, A. 2009. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography. European Journal of Echocardiography, 10, 165-193.
NAKAMURA, M., WADA, S., MIKAMI, T., KITABATAKE, A. & KARINO, T. 2002. A Computational Fluid Mechanical Study on the Effects of Opening and Closing of the Mitral Orifice on a Transmitral Flow Velocity Profile and an Early Diastolic Intraventricular Flow. JSME International Journal Series C Mechanical Systems, Machine Elements and Manufacturing, 45, 913-922.
NAKAMURA, M., WADA, S., MIKAMI, T., KITABATAKE, A. & KARINO, T. 2003. Computational study on the evolution of an intraventricular vortical flow during early diastole for the interpretation of color M-mode Doppler echocardiograms. Biomechanics and Modeling in Mechanobiology, 2, 59-72.
NASH, J. F. 1966. A Note on Skin-Friction Laws for the Incompressible Turbulent Boundary Layer Aeronautical Research Council, Ministry of Aviation.
NATIONAL HEART, L. A. B. I. 2012. Who Needs a Heart Transplant? [Online]. Available: http://www.nhlbi.nih.gov/health/health-topics/topics/ht/ [Accessed 28th May 2014].

347
NGUYEN, D. Q. & THOURANI, V. H. 2010. Third-Generation Continuous Flow Left Ventricular Assist Devices. Innovations:Technology and Techniques in Cardiothoracic and Vascular Surgery, 5, 250-258 10.1097/IMI.0b013e3181ee77a1.
NIKOLIC, S., YELLIN, E. L., TAMURA, K., TAMURA, T. & FRATER, R. W. 1990. Effect of early diastolic loading on myocardial relaxation in the intact canine left ventricle. Circulation Research, 66, 1217-26.
NORDGAARD, H., SWILLENS, A., NORDHAUG, D., KIRKEBY-GARSTAD, I., VAN LOO, D., VITALE, N., SEGERS, P., HAAVERSTAD, R. & LOVSTAKKEN, L. 2010. Impact of competitive flow on wall shear stress in coronary surgery: computational fluid dynamics of a LIMA–LAD model. Cardiovascular Research, 88, 512-519.
NORDSLETTEN, D. A., NIEDERER, S. A., NASH, M. P., HUNTER, P. J. & SMITH, N. P. 2011. Coupling multi-physics models to cardiac mechanics. Progress in Biophysics and Molecular Biology, 104, 77-88.
OCHI, M. 2006. Flow Capacity of Arterial Grafts: Internal Thoracic Artery, Gastroepiploic Artery and Other Grafts. In: HE, G.-W. (ed.) Arterial Grafting for Coronary Artery Bypass Surgery.
OLUFSEN, M. S. 1999. Structured tree outflow condition for blood flow in larger systemic arteries. American Journal of Physiology - Heart and Circulatory Physiology, 276, H257-H268.
ONLINE, C. 2011. Skin friction coefficient [Online]. Available: http://www.cfd-online.com/Wiki/Skin_friction_coefficient [Accessed 2nd November 2013].
OSTROVSKY, G. 2006. The MYO-VAD™ [Online]. Available: http://www.medgadget.com/2006/07/the_myovad.html [Accessed 19th January 2014].
OTAKI, M., LUST, R. M., SUN, Y. S., NORTON, T. O., SPENCE, P. A., ZERI, R. S., HOPSON, S. B. & CHITWOOD, J. W. R. 1994. Bilateral vs Single Internal Thoracic Artery Grafting for Left Main Coronary Artery Occlusion. CHEST Journal, 106, 1260-1263.
OWEN, A. 1993. A numerical model of early diastolic filling: importance of intraventricular pressure wave propagation. Cardiovascular Research, 27, 255-261.
OWIDA, A., DO, H., YANG, W. & MORSI, Y. S. 2010. PIV measurements and numerical validation of end-to-side anastomosis. Journal of Mechanics in Medicine and Biology, 10, 123-138.
OWIDA, A. A., DO, H. & MORSI, Y. S. 2012. Numerical analysis of coronary artery bypass grafts: An over view. Computer Methods and Programs in Biomedicine, 108, 689-705.
PAMBOUKIAN, S. V. 2011. Mechanical Circulatory Support: We Are Halfway There. Journal of the American College of Cardiology, 57, 1383-1385.
PANTALOS, G. M., KOENIG, S. C., GILLARS, K. J., GIRIDHARAN, G. A. & EWERT, D. L. 2004. Characterization of an Adult Mock Circulation for Testing Cardiac Support Devices. ASAIO Journal, 50, 37-46.
PARTYKA, C. & TAYLOR, B. 2014. Review article: Ventricular assist devices in the emergency department. Emergency Medicine Australasia, 26, 104-112.
PATANKAR, S. V. & SPALDING, D. B. 1972. A calculation procedure for heat, mass and momentum transfer in 3-D parabolic flows. Int. J. Heat Mass Transfer, 15, 1787-1806.
PEATTIE, R. A., SCHRADER, T., BLUTH, E. I. & COMSTOCK, C. E. 1994. Development of turbulence in steady flow through models of abdominal aortic aneurysms. Journal of Ultrasound in Medicine, 13, 467-72.
PEDRIZZETTI, G. & DOMENICHINI, F. 2005. Nature Optimizes the Swirling Flow in the Human Left Ventricle. Phys Rev Lett., 95.
PELERIN, J. L., KULIK, C., GOKSU, C., COATRIEUX, J. L. & ROCHETTE, M. Fluid/Structure Interaction applied to the simulation of Abdominal Aortic Aneurysms. Engineering in

348
Medicine and Biology Society, 2006. EMBS '06. 28th Annual International Conference of the IEEE, Aug. 30 2006-Sept. 3 2006 2006. 1754-1757.
PERKTOLD, K. & RAPPITSCH, G. 1995. Computer simulation of local blood flow and vessel mechanics in a compliant carotid artery bifurcation model. Journal of Biomechanics, 28, 845-856.
PESCHAR, M., VERNOOY, K., CORNELUSSEN, R. N., VERBEEK, X. A. A. M., RENEMAN, R. S., VOS, M. A. & PRINZEN, F. W. 2004. Structural, electrical and mechanical remodeling of the canine heart in AV-block and LBBB. European Heart Journal Supplements, 6, D61-D65.
PETROVI, D., OBRENOVI, R., TRBOJEVI-STANKOVI, J., MAJKI-SINGH, N. & STOJIMIROVI, B. 2011. Cardiovascular Mortality in Hemodialysis Patients: Clinical and Epidemiological Analysis. Journal of Medical Biochemistry 30, 302–308.
PHYSIOLOGY, C. A. A. 2013. Cardiac Cycle [Online]. Available: http://cnx.org/content/m46661/latest/ [Accessed 18th July 2014].
PICK, A. 2007. Tricuspid Regurgitation – Symtpoms, Surgery & More [Online]. Available: http://www.heart-valve-surgery.com/heart-surgery-blog/2007/10/31/tricuspid-regurgitation/ [Accessed 2013 11th February].
PICK, A. 2012a. Aortic Stenosis - Symptoms, Diagnosis & Treatment [Online]. Available: http://www.heart-valve-surgery.com/aortic-stenosis-valve-heart-narrowing.php [Accessed 12th February 2013].
PICK, A. 2012b. Mitral Regurgitation - Symptoms, Diagnosis & Treatment [Online]. Available: http://www.heart-valve-surgery.com/mitral-valve-regurgitation-symptoms-leaking.php [Accessed 15th February 2013].
PIERRAKOS, O. & VLACHOS, P. P. 2006. The Effect of Vortex Formation on Left Ventricular Filling and Mitral Valve Efficiency. J Biomech Eng., 128, 527-539
PIERRAKOS, O., VLACHOS, P. P. & TELIONIS, D. P. 2005. Time-Resolved DPIV Analysis of Vortex Dynamics in a Left Ventricular Model Through Bileaflet Mechanical and Porcine Heart Valve Prostheses. Journal of Biomechanical Engineering, 126, 714-726.
PITIGALAARACHCHI, P. 2011. How Does The Heart Beat? [Online]. Available: http://thepansilu.blogspot.com/ [Accessed 26th May 2014].
POLITIS, A. K., STAVROPOULOS, G. P., CHRISTOLIS, M. N., PANAGOPOULOS, P. G., VLACHOS, N. S. & MARKATOS, N. C. 2008. Numerical modelling of simulated blood flow in idealized composite arterial coronary grafts: Transient flow. Journal of Biomechanics, 41, 25-39.
PSC, C. S. H. S. 2008. Pulmonary Regurgitation (pulmonary insufficiency) [Online]. Available: http://mykentuckyheart.com/information/PulmonaryRegurgitation.htm [Accessed 12th February 2013].
QUERZOLI, G., FORTINI, S. & CENEDESE, A. 2010. Effect of the prosthetic mitral valve on vortex dynamics and turbulence of the left ventricular flow. Physics of Fluids (1994-present), 22, -.
RAGHAVAN, M. L. & VORP, D. A. 2000. Toward a biomechanical tool to evaluate rupture potential of abdominal aortic aneurysm: Identification of a finite strain constitutive model and evaluation of its applicability. Journal of Biomechanics, 33, 475-482.
RAGHAVAN, M. L., VORP, D. A., FEDERLE, M. P., MAKAROUN, M. S. & WEBSTER, M. W. 2000. Wall stress distribution on three-dimensionally reconstructed models of human abdominal aortic aneurysm. Journal of Vascular Surgery, 31, 760-769.
REUL, H., TALUKDER, N. & MU¨LLER, E. W. 1981. Fluid mechanics of the natural mitral valve. Journal of Biomechanics, 14, 361-372.
ROBERTS, W. C. & BUCHBINDER, N. A. 1972. Right-sided valvular infective endocarditis. A clinicopathologic study of twelve necropsy patients. The American Journal of Medicine, 53, 7-19.
ROBERTS, W. C. & SJOERDSMA, A. 1964. The cardiac disease associated with the carcinoid syndrome (carcinoid heart disease). The American Journal of Medicine, 36, 5-34.

349
RODRIGUEZ, L. E., SUAREZ, E. E., LOEBE, M. & BRUCKNER, B. A. 2013. Ventricular Assist Devices (VAD) Therapy: New Technology, New Hope? Methodist Debakey Cardiovasc J. , 9, 32-37.
ROSE, E. A., GELIJNS, A. C., MOSKOWITZ, A. J., HEITJAN, D. F., STEVENSON, L. W., DEMBITSKY, W., LONG, J. W., ASCHEIM, D. D., TIERNEY, A. R., LEVITAN, R. G., WATSON, J. T., RONAN, N. S., SHAPIRO, P. A., LAZAR, R. M., MILLER, L. W., GUPTA, L., FRAZIER, O. H., DESVIGNE-NICKENS, P., OZ, M. C., POIRIER, V. L. & MEIER, P. 2001. Long-Term Use of a Left Ventricular Assist Device for End-Stage Heart Failure. New England Journal of Medicine, 345, 1435-1443.
SABER, N., GOSMAN, A. D., WOOD, N., KILNER, P., CHARRIER, C. & FIRMIN, D. 2001. Computational Flow Modeling of the Left Ventricle Based on In Vivo MRI Data: Initial Experience. Annals of Biomedical Engineering, 29, 275-283.
SABER, N., WOOD, N., GOSMAN, A. D., MERRIFIELD, R., YANG, G.-Z., CHARRIER, C., GATEHOUSE, P. & FIRMIN, D. 2003. Progress Towards Patient-Specific Computational Flow Modeling of the Left Heart via Combination of Magnetic Resonance Imaging with Computational Fluid Dynamics. Annals of Biomedical Engineering, 31, 42-52.
SABIK, J. F., RAZA, S., BLACKSTONE, E. H., HOUGHTALING, P. L. & LYTLE, B. W. 2013. Value of Internal Thoracic Artery Grafting to the Left Anterior Descending Coronary Artery at Coronary Reoperation. Journal of the American College of Cardiology, 61, 302-310.
SAHOTA, D. 2013. Wireless charging tech with 30ft range showcased [Online]. Available: http://www.telecoms.com/177722/wireless-charging-tech-with-30ft-range-showcased/?utm_source=rss&utm_medium=rss&utm_campaign=wireless-charging-tech-with-30ft-range-showcased [Accessed 29th May 2014].
SANKARAN, S., ESMAILY, M. M., KAHN, A. M., TSENG, E. E., GUCCIONE, J. M. & MARSDEN, A. L. 2012. Patient-Specific Multiscale Modeling of Blood Flow for Coronary Artery Bypass Graft Surgery. Annals of Biomedical Engineering, 40, 2228-2242.
SANKARANARAYANAN, M., GHISTA, D. N., POH, C. L., SENG, T. Y. & KASSAB, G. S. 2006. Analysis of blood flow in an out-of-plane CABG model. American Journal of Physiology - Heart and Circulatory Physiology, 291, H283-H295.
SCOTTI, C., SHKOLNIK, A., MULUK, S. & FINOL, E. 2005. Fluid-structure interaction in abdominal aortic aneurysms: effects of asymmetry and wall thickness. BioMedical Engineering OnLine, 4, 1-22.
SCOTTI, C. M., JIMENEZ, J., MULUK, S. C. & FINOL, E. A. 2008. Wall stress and flow dynamics in abdominal aortic aneurysms: finite element analysis vs. fluid–structure interaction. Computer Methods in Biomechanics and Biomedical Engineering, 11, 301-322.
SENTARA. 2014. Heart Valve Disease [Online]. Available: http://www.sentara.com/HospitalsFacilities/Hospitals/HeartHospital/SentaraHeartValveandStructuralDiseaseCenter/Pages/About-Heart-Valve-Disease.aspx [Accessed 2014 27th May].
SERMESANT, M., MOIREAU, P., CAMARA, O., SAINTE-MARIE, J., ANDRIANTSIMIAVONA, R., CIMRMAN, R., HILL, D. L. G., CHAPELLE, D. & RAZAVI, R. 2005. Cardiac Function Estimation from MRI Using a Heart Model and Data Assimilation: Advances and Difficulties. In: FRANGI, A., RADEVA, P., SANTOS, A. & HERNANDEZ, M. (eds.) Functional Imaging and Modeling of the Heart. Springer Berlin Heidelberg.
SHIPTON, B. & WAHBA, H. 2001. Valvular heart disease: review and update. Am Fam Physician., 63, 2201-8.
SHMOOKLER, B., MARSH, H. & ROBERTS, W. 1977. Primary sarcoma of the pulmonary trunk and/or right or left main pulmonary artery--a rare cause of obstruction to right ventricular outflow. Report on two patients and analysis of 35 previously described patients. Am J Med. , 63, 263-72.

350
SHTEINBERG, D., HALAK, M., SHAPIRO, S., KINARTY, A., SOBOL, E., LAHAT, N. & KARMELI, R. 2000. Abdominal aortic anuerysm and aortic occlusive disease: A comparison of risk factors and inflammatory response. European Journal of Vascular and Endovascular Surgery, 20, 462-465.
SIDDIQUI, S. U., VERMA, N. K., MISHRA, S. & GUPTA, R. S. 2009. Mathematical modelling of pulsatile flow of Casson’s fluid in arterial stenosis. Applied Mathematics and Computation, 210, 1-10.
SLAUGHTER, M. S. 2010. Long-Term Continuous Flow Left Ventricular Assist Device Support and End-Organ Function: Prospects for Destination Therapy. Journal of Cardiac Surgery, 25, 490-494.
SONESSON, B., HANSEN, F. & LÄNNE, T. 1997. Abdominal aortic aneurysm: A general defect in the vasculature with focal manifestations in the abdominal aorta? Journal of Vascular Surgery, 26, 247-254.
SOUDAH, E., NG, E. Y. K., LOONG, T. H., BORDONE, M., PUA, U. & NARAYANAN, S. 2013. CFD Modelling of Abdominal Aortic Aneurysm on Hemodynamic Loads Using a Realistic Geometry with CT. Comput Math Methods Med. , 2013.
SOULI, M., OUAHSINE, A. & LEWIN, L. 2000. ALE formulation for fluid–structure interaction problems. COMPUTER METHODS IN APPLIED MECHANICS AND ENGINEERING, 190, 659-675.
STAFF, H. 2012. Heart Transplant [Online]. Available: http://www.webmd.com/heart-disease/heart-failure/heart-transplant [Accessed 29th May 2014].
STEEN, T. & STEEN, S. 1994. Filling of a model left ventricle studied by colour M mode Doppler. Cardiovascular Research, 28, 1821-1827.
STERN, D. Abdominal Aortic Aneurysm Definition [Online]. eHow. Available: http://www.ehow.com/about_5078915_abdominal-aortic-aneurysm-definition.html [Accessed 28th April 2014].
SUGA, H., KITABATAKE, A. & SAGAWA, K. 1979. End-systolic pressure determines stroke volume from fixed end-diastolic volume in the isolated canine left ventricle under a constant contractile state. Circulation Research, 44, 238-49.
SUGA, H., SAGAWA, K. & DEMER, L. 1980. Determinants of instantaneous pressure in canine left ventricle. Time and volume specification. Circulation Research, 46, 256-63.
SUGIURA, S., WASHIO, T., HATANO, A., OKADA, J., WATANABE, H. & HISADA, T. 2012. Multi-scale simulations of cardiac electrophysiology and mechanics using the University of Tokyo heart simulator. Progress in Biophysics and Molecular Biology, 110, 380-389.
SUNAGAWA, K., LIM, K., BURKHOFF, D. & SAGAWA, K. 1982a. Microprocessor control of a ventricular volume servo-pump. Annals of Biomedical Engineering, 10, 145-159.
SUNAGAWA, K., MAUGHAN, W. L., BURKHOFF, D. & SAGAWA, K. 1983. Left ventricular interaction with arterial load studied in isolated canine ventricle. American Journal of Physiology - Heart and Circulatory Physiology, 245, H773-H780.
SUNAGAWA, K., MAUGHAN, W. L., FRIESINGER, G., GUZMAN, P., CHANG, M. S. & SAGAWA, K. 1982b. Effects of coronary arterial pressure on left ventricular end-systolic pressure-volume relation of isolated canine heart. Circulation Research, 50, 727-34.
SVENSJÖ, S., BJÖRCK, M. & WANHAINEN, A. 2014. Editor's Choice: Five-year Outcomes in Men Screened for Abdominal Aortic Aneurysm at 65 Years of Age: A Population-based Cohort Study. European Journal of Vascular and Endovascular Surgery, 47, 37-44.
SWILLENS, A., WITTE, M., NORDGAARD, H., LØVSTAKKEN, L., LOO, D., TRACHET, B., VIERENDEELS, J. & SEGERS, P. 2012. Effect of the degree of LAD stenosis on “competitive flow” and flow field characteristics in LIMA-to-LAD bypass surgery. Medical & Biological Engineering & Computing, 50, 839-849.

351
TAKENAKA, K., DABESTANI, A., GARDIN, J. M., RUSSELL, D., CLARK, S., ALLFIE, A. & HENRY, W. L. 1986. Pulsed Doppler echocardiographic study of left ventricular filling in dilated cardiomyopathy. The American Journal of Cardiology, 58, 143-147.
TANNÉ, D., BERTRAND, E., KADEM, L., PIBAROT, P. & RIEU, R. 2010. Assessment of left heart and pulmonary circulation flow dynamics by a new pulsed mock circulatory system. Experiments in Fluids, 48, 837-850.
TAY, W.-B., TSENG, Y.-H., LIN, L.-Y. & TSENG, W.-Y. 2011. Towards patient-specific cardiovascular modeling system using the immersed boundary technique. BioMedical Engineering OnLine, 10.
TAYLOR, C., HUGHES, T. R. & ZARINS, C. 1998. Finite Element Modeling of Three-Dimensional Pulsatile Flow in the Abdominal Aorta: Relevance to Atherosclerosis. Annals of Biomedical Engineering, 26, 975-987.
TAYLOR, T. W., OKINO, H. & YAMAGUCHI, T. 1994. Three-Dimensional Analysis of Left Ventricular Ejection Using Computational Fluid Dynamics. Journal of Biomechanical Engineering, 116, 127-130.
TAYLOR, T. W. & YAMAGUCHI, T. 1995. Realistic three-dimensional left ventricular ejection determined from computational fluid dynamics. Med. Eng. Phys., 17, 602-608.
TEMAM, R. 2001. Navier-Stokes Equations: Theory And Numerical Analysis, AMS Chelsea Publishing.
THOMAS, D. E., WHEELER, R., YOUSEF, Z. R. & MASANI, N. D. 2009. The role of echocardiography in guiding management in dilated cardiomyopathy. European Journal of Echocardiography, 10, iii15-iii21.
THUBRIKAR, M. J., AL-SOUDI, J. & ROBICSEK, F. 2001a. Wall Stress Studies of Abdominal Aortic Aneurysm in a Clinical Model. Annals of Vascular Surgery, 15, 355-366.
THUBRIKAR, M. J., LABROSSE, M., ROBICSEK, F., AL-SOUDI, J. & FOWLER, B. 2001b. Mechanical properties of abdominal aortic aneurysm wall. Journal of Medical Engineering & Technology, 25, 133.
TIMMS, D. 2011. A review of clinical ventricular assist devices. Medical Engineering & Physics, 33, 1041-1047.
TONTI, G., PEDRIZZETTI, G., TRAMBAIOLO, P. & SALUSTRI, A. 2001. Space and time dependency of inertial and convective contribution to the transmitral pressure drop during ventricular filling. Journal of the American College of Cardiology, 38, 290-291.
USYK, T. P. & MCCULLOCH, A. D. 2003. Relationship Between Regional Shortening and Asynchronous Electrical Activation in a Three-Dimensional Model of Ventricular Electromechanics. Journal of Cardiovascular Electrophysiology, 14, S196-S202.
VAARTJES, S. R. & BOOM, H. B. 1987. Left ventricular internal resistance and unloaded ejection flow assessed from pressure-flow relations: a flow-clamp study on isolated rabbit hearts. Circulation Research, 60, 727-37.
VADAKKUMPADAN, F., AREVALO, H., PRASSL, A. J., CHEN, J., KICKINGER, F., KOHL, P., PLANK, G. & TRAYANOVA, N. 2010. Image-based models of cardiac structure in health and disease. Wiley Interdisciplinary Reviews: Systems Biology and Medicine, 2, 489-506.
VANOVERSCHELDE, J.-L. J., RAPHAEL, D. A., ROBERT, A. R. & COSYNS, J. R. 1990. Left ventricular filling in dilated cardiomyopathy: Relation to functional class and memodynamics. Journal of the American College of Cardiology, 15, 1288-1295.
VERDONCK, P. & VIERENDEELS, J. 2002. Fluid-Structure Interaction Modelling of Left Ventricular Filling. In: SLOOT, P. A., HOEKSTRA, A., TAN, C. J. K. & DONGARRA, J. (eds.) Computational Science — ICCS 2002. Springer Berlin Heidelberg.
VERHEY, J. F. & NATHAN, N. S. 2004. Feasibility of rapid and automated importation of 3D echocardiographic left ventricular (LV) geometry into a finite element (FEM) analysis model. BioMedical Engineering OnLine, 3.

352
VIERENDEELS, J., RIEMSLAGH, K., DICK, E. & VERDONCK, P. 2000. Computer simulation of intraventricular flow and pressure gradients during diastole. J Biomech Eng., 122, 667-74.
VIERENDEELS, J. A., RIEMSLAGH, K., DICK, E. & VERDONCK, P. Computer simulation of left ventricular filling flow: impact study on echocardiograms. Computers in Cardiology, 1999, 1999 1999. 177-180.
VIMMR, J. & JONÁŠOVÁ, A. 2010. Non-Newtonian effects of blood flow in complete coronary and femoral bypasses. Mathematics and Computers in Simulation, 80, 1324-1336.
VIRGINIA, U. O. 2013. Pulmonary Regurgitation [Online]. Available: http://uvahealth.com/services/cardiac-valve-center/valve-conditions/pulmonary-regurgitation/pulmonary-regurgitation [Accessed 12th February 2013].
VUKIĆEVIĆ, M., FORTINI, S., QUERZOLI, G., ESPA, S. & PEDRIZZETTI, G. 2012. Experimental study of an asymmetric heart valve prototype. European Journal of Mechanics - B/Fluids, 35, 54-60.
W, G., LP, M., SP, M., M, S. & DT, Y. 1974. Wall thickness and diastolic properties of the left ventricle. Circulation, 49, 129-35.
WAITE, L., SCHULZ, S., SZABO, G. & VAHL, C. F. 2000. A lumped parameter model of left ventricular filling-pressure waveforms. Biomed Sci Instrum., 36, 75-80.
WANG, A. & BASHORE, T. M. 2009. Valvular Heart Disease, Humana Press. WANG, H. M., GAO, H., LUO, X. Y., BERRY, C., GRIFFITH, B. E., OGDEN, R. W. & WANG, T. J.
2013. Structure-based finite strain modelling of the human left ventricle in diastole. Int j numer method biomed eng. , 29, 83-103.
WATANABE, H., HISADA, T., SUGIURA, S., OKADA, J.-I. & FUKUNARI, H. 2002. Computer Simulation of Blood Flow, Left Ventricular Wall Motion and Their Interrelationship by Fluid-Structure Interaction Finite Element Method. JSME International Journal Series C, 45, 1003-1012
WATANABE, H., SUGIURA, S., KAFUKU, H. & HISADA, T. 2004. Multiphysics simulation of left ventricular filling dynamics using fluid-structure interaction finite element method. Biophys J. , 87, 2074-85.
WATERS, B., REED, J., KAGI, K., SAMPLE, A., BONDE, P. & SMITH, J. 2013. A Portable Transmitter for Wirelessly Powering a Ventricular Assist Device Using the Free-Range Resonant Electrical Energy Delivery (FREE-D) System. In: SMITH, J. R. (ed.) Wirelessly Powered Sensor Networks and Computational RFID. Springer New York.
WATERS, B. H., SAMPLE, A. P., BONDE, P. & SMITH, J. R. 2012. Powering a ventricular assist device (VAD) with the free-range resonant electrical energy delivery (FREE-D) system. Proceedings of the IEEE, 100, 138-149.
WIJKSTRA, H. & BOOM, H. B. K. 1989. Deactivation in the Rabbit Left Ventricle Induced by Constant Ejection Flow. IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, 36.
XENOS, M. Y. D. S. J. N. A. D. 2010. The effect of angulation in abdominal aortic aneurysms: fluid-structure interaction simulations of idealized geometries. Medical & Biological Engineering & Computing, 48, 1175-1190.
XU, Y., LIANG, G., HU, G., YANG, Y., GENG, J. & SAHA, P. K. 2011. Quantification of coronary arterial stenoses in CTA using fuzzy distance transform. Computerized Medical Imaging and Graphics Article in Press.
YAMADA, H., TANAKA, E. & MURAKAMI, S. 1994. Mechanical evaluation of growth and rupture of aneurysm in abdominal aorta. JSME International Journal, Series A: Mechanics and Material Engineering, 37, 181-187.
YOKOYAMA, Y., KAWAGUCHI, O., SHINSHI, T., STEINSEIFER, U. & TAKATANI, S. 2010. A new pulse duplicator with a passive fill ventricle for analysis of cardiac dynamics. Journal of Artificial Organs, 13, 189-196.

353
YOTTI, R., BERMEJO, J., ANTORANZ, J. C., DESCO, M. M., CORTINA, C., ROJO-ÁLVAREZ, J. L., ALLUÉ, C., MARTÍN, L., MORENO, M., SERRANO, J. A., MUÑOZ, R. & GARCÍA-FERNÁNDEZ, M. A. 2005. A Noninvasive Method for Assessing Impaired Diastolic Suction in Patients With Dilated Cardiomyopathy. Circulation, 112, 2921-2929.
YOUNG, A. D. 1939. The Calculation of the Total and Skin Friction Drags of Bodies of Revolution at Zero Incidence.
ZARINS, C. K., GIDDENS, D. P., BHARADVAJ, B. K., SOTTIURAI, V. S., MABON, R. F. & GLAGOV, S. 1983. Carotid bifurcation atherosclerosis. Quantitative correlation of plaque localization with flow velocity profiles and wall shear stress. Circulation Research, 53, 502-14.
ZHANG, H., LIU, L., CHEN, L., MA, N., ZHOU, L., LIU, Y., LI, Z., LIU, C., HOU, R. & ZHU, S. 2013. The Evolution of Intraventricular Vortex during Ejection Studied by Using Vector Flow Mapping. Echocardiography, 30, 27-36.
ZHANG, J.-M., CHUA, L. P., GHISTA, D. N., ZHOU, T.-M. & TAN, Y. S. 2008. Validation of numerical simulation with PIV measurements for two anastomosis models. Medical Engineering & Physics, 30, 226-247.
ZHENG, X., SEO, J. H., VEDULA, V., ABRAHAM, T. & MITTAL, R. 2012. Computational modeling and analysis of intracardiac flows in simple models of the left ventricle. European Journal of Mechanics - B/Fluids, 35, 31-39.