
Alcohol septal ablation in hypertrophic obstructive cardiomyopathy
Upload
independentCategory
view
1download
0
p
tp
3
1
Biventricular pacing in hypertrophic obstructivecardiomyopathy: A pilot studyAntonio Berruezo, MD, PhD,1 Radu Vatasescu, MD,2 Lluis Mont, MD, PhD,1 Marta Sitges, MD, PhD,1
Diego Perez, MD,1 Giorgi Papiashvilli, MD,1 Barbara Vidal, MD, PhD,1 Antonio Francino, MD, PhD,1
Juan Fernández-Armenta, MD,1 Etelvino Silva, BEng,1 Bart Bijnens, PhD,3
Jose Ramón González-Juanatey, MD, PhD,4 Josep Brugada, MD, PhD1
1From the Cardiology Department, Thorax Institute, Hospital Clinic, Barcelona, Spain,2Cardiology Department, Clinic Emergency Hospital Bucharest, Bucharest, Romania,3ICREA–Universitat Pompeu Fabra, Barcelona, Spain, and4Cardiology Department, University of Santiago de Compostela, La Coruña, Spain.
pia
BACKGROUND Right ventricular apex pacing for gradient re-duction in hypertrophic obstructive cardiomyopathy (HOCM)with severe left ventricular (LV) obstruction has yielded con-flicting results.
OBJECTIVE The purpose of this study was to assess the feasibilityand effectiveness of biventricular pacing in HOCM.
METHODS Transvenous biventricular pacing was attempted in 12severely symptomatic HOCM patients. Optimal intervals were pro-grammed after implant. Echocardiographic LV pressure gradientand synchrony were assessed. LV lead implantation was successfulin 9 patients. Optimal pacing mode was biventricular in 6 patients,left ventricular only in 2 patients, and right ventricular only in 1patient.
RESULTS Functional capacity and quality of life progressivelyimproved. New York Heart Association functional class decreasedfrom 3.2 � 0.4 at baseline to 1.9 � 0.3 at 3 months and to 1.4 �0.5 at 1 year (P �.05); 6-minute walk test increased from349 � 116 m at baseline to 454 � 144 m at 3 months and to517 � 206 m (P �.05); and quality of life increased from 54 � 16
ci
rt, 2010; accepted October 7, 2010.)
547-5271/$ -see front matter © 2011 Heart Rhythm Society. All rights reserved
oints at 1 year (P �.05). There was also a progressive reductionn LV gradient from 74 � 23 mmHg at baseline to 50 � 27 mmHgcutely, 40 � 26 mmHg at 3 months, and 28 � 17 mmHg at 1 year
(P �.05). Gradient reduction was associated with diminished peaklongitudinal displacement of the LV septum and earlier displace-ment of the lateral wall. A progressive reduction of LV mass wasobserved, from 356 � 110 g at baseline to 315 � 70 g at 3 months(P � .13) and to 284 � 42 g at 1 year (P �.05).
CONCLUSION Biventricular pacing is feasible and usually the bestconfiguration for gradient reduction in HOCM. Biventricular pacingreduces LV hypertrophy.
KEYWORDS Biventricular pacing; Hypertrophic obstructive cardio-myopathy; Intraventricular gradient; Reverse remodeling
ABBREVIATIONS CRT � cardiac resynchronization therapy;HOCM � hypertrophic obstructive cardiomyopathy; LV � leftventricle; LVOT � left ventricular outflow tract; NYHA � NewYork Heart Association; OPT � optimal pacing configuration;RV � right ventricle; RVA � right ventricular apex
(Heart Rhythm 2011;8:221–227) © 2011 Heart Rhythm Society. All
oints at baseline to 28 � 13 points at 3 months and 27 � 15 rights reserved.IntroductionHypertrophic cardiomyopathy is an autosomal dominantinherited genetic disease characterized by compensatory leftventricular (LV) hypertrophy due to sarcomere dysfunction.In a subset of patients with hypertrophic cardiomyopathy,the site and extent of cardiac hypertrophy result in severeobstruction to LV outflow, contributing to symptoms andincreasing the risk of sudden cardiac death.1,2 Surgical sep-al myectomy and alcohol septal ablation can diminish LVressure gradient in patients with hypertrophic obstructive
Address reprint requests and correspondence: Dr. Antonio Berru-ezo, Cardiology Department, Arrhythmia Section, Thorax Institute,Hospital Clínic, University of Barcelona, Villarroel 170, 08036, Bar-celona, Spain. E-mail address: [email protected]. (Received August
ardiomyopathy (HOCM), reducing symptoms and improv-ng survival.3–5 Nonetheless, these procedures can carry
unacceptable risks and/or are not suitable in selected subsetsof patients with HOCM and severe LV obstruction. Dual-chamber (DDD) pacing with a short AV delay is a widelyavailable alternative to surgical therapy or alcohol septalablation. Observational studies and a nonblinded ran-domized trial have suggested that DDD pacing producesgradient reduction, with symptomatic and functional ben-efit.6 – 8 Subsequent single and multicenter randomizedtrials demonstrated average left ventricular outflow tract(LVOT) gradient reductions of only 50% and no im-provement in exercise capacity,9 –11 suggesting a placeboeffect for the symptomatic improvement.9,12 However,ecent data showed that atrial synchronous LV or biven-
ricular pacing might further reduce the LV pressure. doi:10.1016/j.hrthm.2010.10.010

s
npcta
tLVLciLtsfi
tldtw
iuaa
SBBRPLIpL
222 Heart Rhythm, Vol 8, No 2, February 2011
gradient and improve symptoms in patients with HOCMand LVOT obstruction.13–17
The aim of the present study was to assess the feasibilityand effectiveness of LV/biventricular pacing in patientswith HOCM and severe LVOT obstruction.
MethodsPatientsBetween November 2005 and February 2009, 12 consecu-tive HOCM patients with significant LV obstruction (base-line intraventricular gradient �50 mmHg), preserved LVystolic function (LV ejection fraction �50%), and severe
symptoms (chronic moderate to severe heart failure, i.e.,New York Heart Association [NYHA] functional class�III) despite optimal medical treatment and without indi-cation for pacing due to bradycardia were referred for atrio-biventricular pacing (Table 1). Patients were included in thestudy only if surgical myectomy or septal ablation hadcontraindications or were refused by the patients. The studyprotocol was approved by the institution’s ethics committee,and written informed consent was obtained from all pa-tients.
Cardiac resynchronization therapy deviceimplantationRight atrial and ventricular leads were positioned conven-tionally (right atrial appendage and right ventricular apex[RVA]). The coronary sinus was cannulated with an 8Fguiding catheter, and an occlusive retrograde coronary sinusangiogram was obtained. The LV pacing lead was insertedin a ventricular vein and positioned as laterally as possible.All leads were connected to a dual-chamber biventricularimplantable device. Patients considered to be at high risk forsudden cardiac death (one patient with class IIa indication)received a cardioverter-defibrillator (cardiac resynchroniza-
Table 1 Baseline characteristics of successfully implantedpatients (n � 9)
Parameter
Age (years) 51 � 21Sex (female/male) 5/4NYHA functional class 3.2 � 0.4Quality of life (Minnesota Living with Heart Failure
Questionnaire points)54 � 16
ix-minute walk test (m) 349 � 116aseline QRS width (ms) 103 � 13aseline PR interval (ms) 170 � 10esting LV gradient (mmHg) 74 � 23rovoked Valsalva LV gradient (mmHg) 115 � 42V ejection fraction (%) 68 � 9nterventricular septum (mm) 21 � 5osterior wall (mm) 15 � 3V mass (g) 356 � 110
LV � left ventricle; NYHA � New York Heart Association.
tion therapy [CRT]-defibrillator).18,19 s
Clinical evaluationFunctional capacity (NYHA functional class, 6-minutewalk test) and quality of life (Minnesota Living withHeart Failure Questionnaire) were assessed before CRTdevice implantation and followed up at 3 months and 1year.
Echocardiographic evaluationAll patients underwent standard transthoracic two-dimen-sional and color Doppler echocardiography before implan-tation, 1 day after implantation (for optimization), at 3months, and at 1 year. Parasternal and apical images wereobtained with a commercially available system (Vivid 7,General Electric, Milwaukee, WI, USA) using a 3.5-MHztransducer. LV ejection fraction was obtained using theSimpson method. LV mass was calculated using the thick-ness of diastolic LV walls and the diastolic LV diameter asmeasured from the M mode (American Society of Echocar-diography formula adjusted by Devereux20). Peak instanta-eous LVOT gradient under resting conditions and after arovocative Valsalva maneuver were determined on threeonsecutive cardiac cycles and averaged. Mitral regurgita-ion was evaluated visually, integrating pulsed, continuous,nd color Doppler data (grade 0 � absent, grade 1 � trace,
grade 2 � mild, grade 3 � moderate, grade 4 � severe).Optimal AV interval was considered the shortest AV inter-val that had not truncated A wave on pulsed Doppler of themitral inflow.21 With the optimum AV interval set, weested consecutively right ventricular (RV)-only pacing,V-only pacing, or biventricular pacing (RV preactivationV �30 ms, simultaneous biventricular pacing VV 0 ms, orV preactivation VV �30 ms).21,22 The optimum pacingonfiguration as well the optimum interventricular (VV)nterval were selected on the basis of maximum reduction ofVOT pressure gradient on continuous-wave Doppler in-
errogation after a 5-minute equilibrium phase for eachetup. The echocardiographer was blinded to pacing con-guration.
LV synchrony was assessed qualitatively by evaluatinghe synchronicity in the longitudinal displacement of theateral and septal walls in the four-chamber apical viewerived from color-coded Tissue Doppler Imaging acquisi-ions (tissue tracking, Echo Pac 4.2.0, GE Healthcare, Mil-aukee, WI, USA).23 The sample volume for tissue velocity
interrogation was placed at the midbasal level of the septaland lateral walls. Peak systolic displacement of both theseptal and lateral walls was also determined in each echo-cardiographic examination.
Statistical analysisMeasured values are expressed as mean � SD. Data show-ng gaussian distribution were compared in the subgroupssing paired and Student’s t-tests. Dichotomous variablesnd nonparametric data were compared using Chi-squarend Wilcoxon test, respectively. P �.05 was considered
ignificant.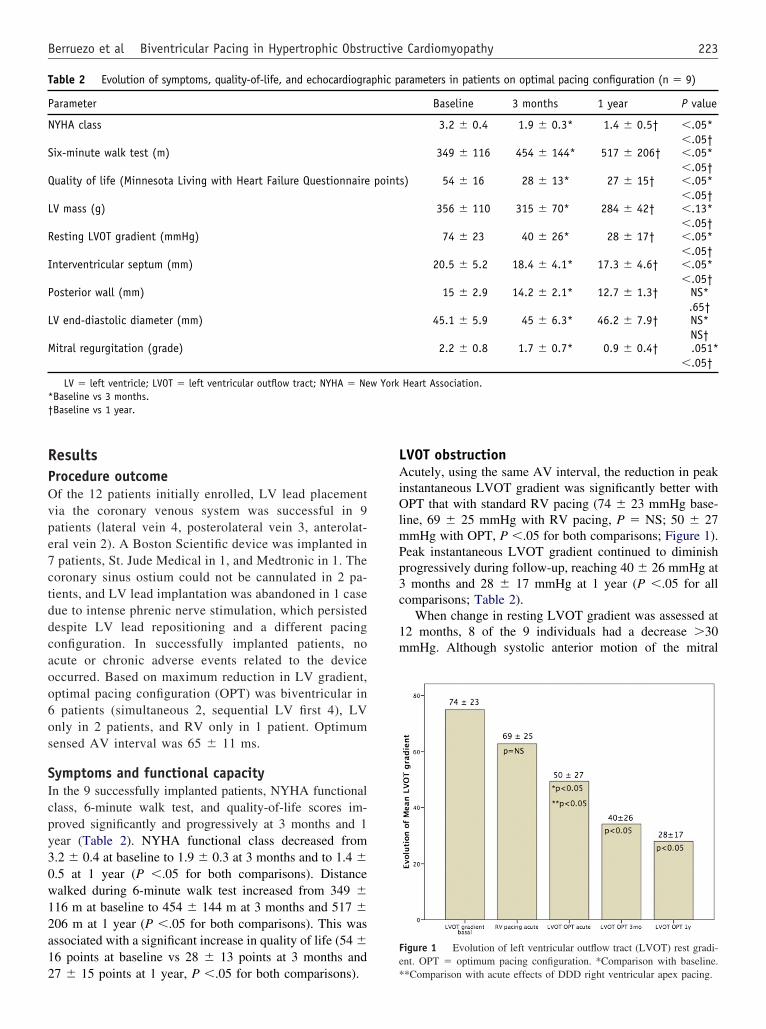
0w12a12
mPp3c
1m
S
Q
L
R
I
P
L
M
223Berruezo et al Biventricular Pacing in Hypertrophic Obstructive Cardiomyopathy
ResultsProcedure outcomeOf the 12 patients initially enrolled, LV lead placementvia the coronary venous system was successful in 9patients (lateral vein 4, posterolateral vein 3, anterolat-eral vein 2). A Boston Scientific device was implanted in7 patients, St. Jude Medical in 1, and Medtronic in 1. Thecoronary sinus ostium could not be cannulated in 2 pa-tients, and LV lead implantation was abandoned in 1 casedue to intense phrenic nerve stimulation, which persisteddespite LV lead repositioning and a different pacingconfiguration. In successfully implanted patients, noacute or chronic adverse events related to the deviceoccurred. Based on maximum reduction in LV gradient,optimal pacing configuration (OPT) was biventricular in6 patients (simultaneous 2, sequential LV first 4), LVonly in 2 patients, and RV only in 1 patient. Optimumsensed AV interval was 65 � 11 ms.
Symptoms and functional capacityIn the 9 successfully implanted patients, NYHA functionalclass, 6-minute walk test, and quality-of-life scores im-proved significantly and progressively at 3 months and 1year (Table 2). NYHA functional class decreased from3.2 � 0.4 at baseline to 1.9 � 0.3 at 3 months and to 1.4 �.5 at 1 year (P �.05 for both comparisons). Distancealked during 6-minute walk test increased from 349 �16 m at baseline to 454 � 144 m at 3 months and 517 �06 m at 1 year (P �.05 for both comparisons). This wasssociated with a significant increase in quality of life (54 �6 points at baseline vs 28 � 13 points at 3 months and
Table 2 Evolution of symptoms, quality-of-life, and echocardiogra
Parameter
NYHA class
ix-minute walk test (m)
uality of life (Minnesota Living with Heart Failure Questionnaire
V mass (g)
esting LVOT gradient (mmHg)
nterventricular septum (mm)
osterior wall (mm)
V end-diastolic diameter (mm)
itral regurgitation (grade)
LV � left ventricle; LVOT � left ventricular outflow tract; NYHA � Ne*Baseline vs 3 months.†Baseline vs 1 year.
7 � 15 points at 1 year, P �.05 for both comparisons).
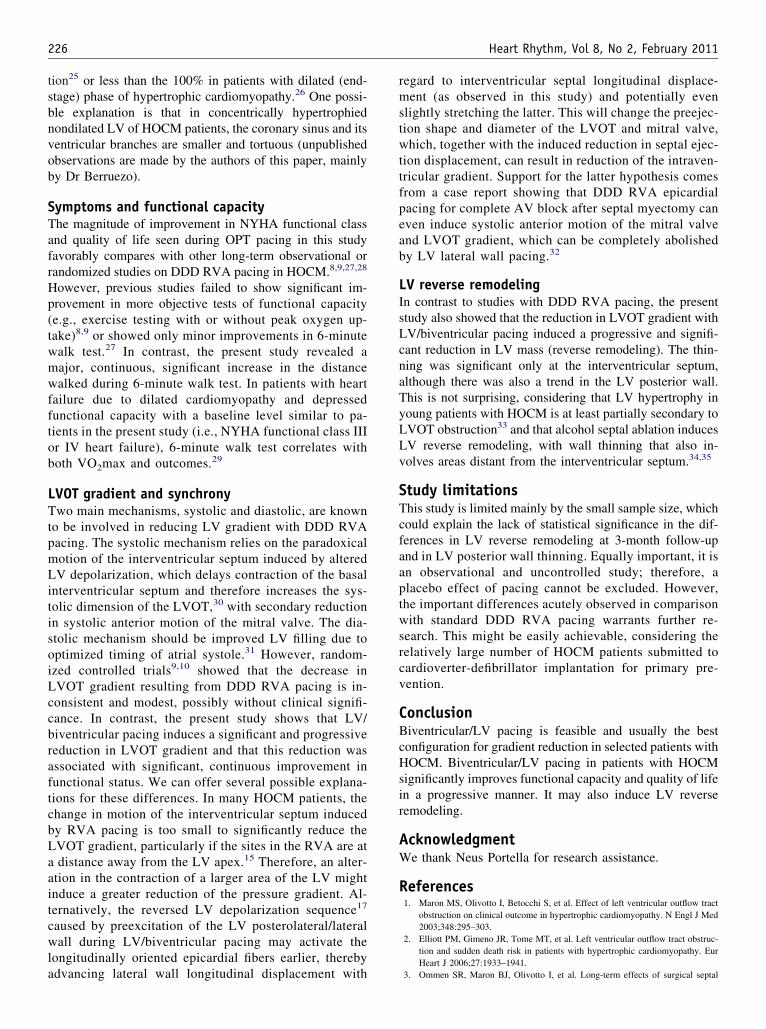
LVOT obstructionAcutely, using the same AV interval, the reduction in peakinstantaneous LVOT gradient was significantly better withOPT that with standard RV pacing (74 � 23 mmHg base-line, 69 � 25 mmHg with RV pacing, P � NS; 50 � 27
mHg with OPT, P �.05 for both comparisons; Figure 1).eak instantaneous LVOT gradient continued to diminishrogressively during follow-up, reaching 40 � 26 mmHg atmonths and 28 � 17 mmHg at 1 year (P �.05 for all
omparisons; Table 2).When change in resting LVOT gradient was assessed at
2 months, 8 of the 9 individuals had a decrease �30mHg. Although systolic anterior motion of the mitral
arameters in patients on optimal pacing configuration (n � 9)
Baseline 3 months 1 year P value
3.2 � 0.4 1.9 � 0.3* 1.4 � 0.5† �.05*�.05†
349 � 116 454 � 144* 517 � 206† �.05*�.05†
s) 54 � 16 28 � 13* 27 � 15† �.05*�.05†
356 � 110 315 � 70* 284 � 42† �.13*�.05†
74 � 23 40 � 26* 28 � 17† �.05*�.05†
20.5 � 5.2 18.4 � 4.1* 17.3 � 4.6† �.05*�.05†
15 � 2.9 14.2 � 2.1* 12.7 � 1.3† NS*.65†
45.1 � 5.9 45 � 6.3* 46.2 � 7.9† NS*NS†
2.2 � 0.8 1.7 � 0.7* 0.9 � 0.4† .051*�.05†
Heart Association.
Figure 1 Evolution of left ventricular outflow tract (LVOT) rest gradi-ent. OPT � optimum pacing configuration. *Comparison with baseline.
phic p
point
w York
**Comparison with acute effects of DDD right ventricular apex pacing.

Pt6rrLpmbefotc
srl
cates in
224 Heart Rhythm, Vol 8, No 2, February 2011
valve still was present (but to a lesser extent) in all patientsat 3 months and in 8 of the 9 patients at 1 year, the degreeof mitral regurgitation significantly decreased, from grade2.2 � 0.8 at baseline to 1.7 � 0.7 at 3 months and 0.9 � 0.4at 1 year (P � .051 and P �.05, respectively).
LV synchronyPeak longitudinal displacement of the septal LV wall glo-bally decreased (from 6.8 � 1.0 mm to 5.7 � 1.5 mm,
�.05) at follow-up, whereas longitudinal displacement ofhe lateral LV wall was unchanged (from 6.7 � 2.1 mm to.9 � 1.2 mm, P � NS). Most of the 8 patients witheduction of LVOT gradient at follow-up showed similaresults. The only patient with unchanged, persistently highVOT gradient showed a decrease in LV lateral wall dis-lacement (Figure 2). More importantly, although displace-ent of the septal and lateral LV walls was synchronous
efore OPT configuration, lateral wall displacement camearlier compared to displacement of the septal wall afterollow-up in all patients who showed significant reductionf LVOT obstruction. However, the earlier displacement ofhe lateral wall was not observed in the patient with un-
Figure 2 Graph plots showing left ventricular (LV) septal and lateral watract (LVOT) obstruction at follow-up. Legend shows patient anonymous ito baseline. Minus sign indicates reduction versus baseline. Plus sign indi
hanged gradients after biventricular pacing (Figure 3). t
LV reverse remodelingContinuous reduction of LV mass, from 356 � 110 g atbaseline to 315 � 70 g at 3 months (P � .13) and 284 �42 g at 1 year (P �.05), was due to thinning of the LV walls,which was significant only for the interventricular septum(20.5 � 5.2 mm at baseline vs 18.4 � 4.1 mm at 3 months,17.3 � 4.6 mm at 1 year, P �.05 for both comparisons).The LV posterior wall showed only a trend toward thinning(15 � 2.9 mm at baseline vs 14.2 � 2.1 mm at 3 months,P � NS; 12.7 � 1.3 mm at 1 year, P � .065). LV end-diastolic diameter remained unchanged during follow-up(45.1 � 5.9 mm at baseline vs 45 � 6.3 mm at 3 months,46.2 � 7.9 mm at 1 year, P � NS for both comparisons).
DiscussionDDD RV pacing with short AV delay in patients withHOCM and significant LVOT gradient represents a ClassIIb indication20,21 because data from randomized trialshowed only inconsistent and modest LVOT gradienteduction,9 –11 with symptomatic improvement that canargely be attributed to a placebo effect.9,12 In contrast,
acements in patients with and without reduction in left ventricular outflowation with percentage of LVOT gradient reduction at follow-up comparedcrease versus baseline.
ll displdentific
he present study shows that transvenous biventricu-

aa
bIb
ollow-u
225Berruezo et al Biventricular Pacing in Hypertrophic Obstructive Cardiomyopathy
lar/LV pacing is feasible and induces an acute reductionin LVOT gradient that significantly exceeds the effect ofDDD RVA pacing. The gradient reduction was main-tained and amplified during long-term follow-up and wasassociated with significant improvement in symptomsand a reduction in LV mass, suggesting concomitant LVreverse remodeling. The mechanism of LVOT gradient
Figure 3 A: Images from a patient who presented favorable response to30-ms left ventricular preactivation. Upper panels: Spectral continuous-w
fter 1 year (right) of biventricular pacing. LVOT gradient decreased froand lateral (green) walls of the left ventricle (LV) before (left) and after 1oth walls had almost simultaneous displacements, whereas at follow-up, tmages from the patient who presented no response to biventricular pacing.iventricular pacing. Upper panels: Spectral continuous-wave Doppler o
LVOT gradient was 64 mmHg in both examinations. Lower panels: Long(left) and after 1 year (right) of CRT. Note that both at baseline and at f
reduction might be a reduction in systolic anterior motion
of the mitral valve as suggested by the significant andcontinuous reduction in degree of mitral regurgitation.24
Procedure outcomeLV/biventricular pacing in HOCM proved to be feasible,although in this small series the success rate of transvenousLV lead implantation was only 75% compared to the 93%
icular pacing. The device was programmed with a 80-ms AV interval andppler of flow at the left ventricular outflow tract (LVOT) before (left) and25 mmHg. Lower panels: Longitudinal displacement of septal (yellow)
right) of cardiac resynchronization therapy (CRT). Note that at baseline,al wall was earlier and had more displacement than did the septal wall. B:vice was programmed with a 100-ms AV interval and 30-ms asynchronoust the LVOT before (left) and after 1 year (right) of biventricular pacing.displacement of septal (yellow) and lateral (green) walls of the LV beforep, both walls had almost simultaneous displacements.
biventrave Do
m 81 toyear (
he laterThe de
f flow aitudinal
CRT implantation rate in patients with LV systolic dysfunc-
s
w
isoiLccbraftcbLaait
226 Heart Rhythm, Vol 8, No 2, February 2011
tion25 or less than the 100% in patients with dilated (end-tage) phase of hypertrophic cardiomyopathy.26 One possi-
ble explanation is that in concentrically hypertrophiednondilated LV of HOCM patients, the coronary sinus and itsventricular branches are smaller and tortuous (unpublishedobservations are made by the authors of this paper, mainlyby Dr Berruezo).
Symptoms and functional capacityThe magnitude of improvement in NYHA functional classand quality of life seen during OPT pacing in this studyfavorably compares with other long-term observational orrandomized studies on DDD RVA pacing in HOCM.8,9,27,28
However, previous studies failed to show significant im-provement in more objective tests of functional capacity(e.g., exercise testing with or without peak oxygen up-take)8,9 or showed only minor improvements in 6-minute
alk test.27 In contrast, the present study revealed amajor, continuous, significant increase in the distancewalked during 6-minute walk test. In patients with heartfailure due to dilated cardiomyopathy and depressedfunctional capacity with a baseline level similar to pa-tients in the present study (i.e., NYHA functional class IIIor IV heart failure), 6-minute walk test correlates withboth VO2max and outcomes.29
LVOT gradient and synchronyTwo main mechanisms, systolic and diastolic, are knownto be involved in reducing LV gradient with DDD RVApacing. The systolic mechanism relies on the paradoxicalmotion of the interventricular septum induced by alteredLV depolarization, which delays contraction of the basalinterventricular septum and therefore increases the sys-tolic dimension of the LVOT,30 with secondary reductionn systolic anterior motion of the mitral valve. The dia-tolic mechanism should be improved LV filling due toptimized timing of atrial systole.31 However, random-zed controlled trials9,10 showed that the decrease inVOT gradient resulting from DDD RVA pacing is in-onsistent and modest, possibly without clinical signifi-ance. In contrast, the present study shows that LV/iventricular pacing induces a significant and progressiveeduction in LVOT gradient and that this reduction wasssociated with significant, continuous improvement inunctional status. We can offer several possible explana-ions for these differences. In many HOCM patients, thehange in motion of the interventricular septum inducedy RVA pacing is too small to significantly reduce theVOT gradient, particularly if the sites in the RVA are atdistance away from the LV apex.15 Therefore, an alter-
tion in the contraction of a larger area of the LV mightnduce a greater reduction of the pressure gradient. Al-ernatively, the reversed LV depolarization sequence17
caused by preexcitation of the LV posterolateral/lateralwall during LV/biventricular pacing may activate thelongitudinally oriented epicardial fibers earlier, thereby
advancing lateral wall longitudinal displacement withregard to interventricular septal longitudinal displace-ment (as observed in this study) and potentially evenslightly stretching the latter. This will change the preejec-tion shape and diameter of the LVOT and mitral valve,which, together with the induced reduction in septal ejec-tion displacement, can result in reduction of the intraven-tricular gradient. Support for the latter hypothesis comesfrom a case report showing that DDD RVA epicardialpacing for complete AV block after septal myectomy caneven induce systolic anterior motion of the mitral valveand LVOT gradient, which can be completely abolishedby LV lateral wall pacing.32
LV reverse remodelingIn contrast to studies with DDD RVA pacing, the presentstudy also showed that the reduction in LVOT gradient withLV/biventricular pacing induced a progressive and signifi-cant reduction in LV mass (reverse remodeling). The thin-ning was significant only at the interventricular septum,although there was also a trend in the LV posterior wall.This is not surprising, considering that LV hypertrophy inyoung patients with HOCM is at least partially secondary toLVOT obstruction33 and that alcohol septal ablation inducesLV reverse remodeling, with wall thinning that also in-volves areas distant from the interventricular septum.34,35
Study limitationsThis study is limited mainly by the small sample size, whichcould explain the lack of statistical significance in the dif-ferences in LV reverse remodeling at 3-month follow-upand in LV posterior wall thinning. Equally important, it isan observational and uncontrolled study; therefore, aplacebo effect of pacing cannot be excluded. However,the important differences acutely observed in comparisonwith standard DDD RVA pacing warrants further re-search. This might be easily achievable, considering therelatively large number of HOCM patients submitted tocardioverter-defibrillator implantation for primary pre-vention.
ConclusionBiventricular/LV pacing is feasible and usually the bestconfiguration for gradient reduction in selected patients withHOCM. Biventricular/LV pacing in patients with HOCMsignificantly improves functional capacity and quality of lifein a progressive manner. It may also induce LV reverseremodeling.
AcknowledgmentWe thank Neus Portella for research assistance.
References1. Maron MS, Olivotto I, Betocchi S, et al. Effect of left ventricular outflow tract
obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med2003;348:295–303.
2. Elliott PM, Gimeno JR, Tome MT, et al. Left ventricular outflow tract obstruc-tion and sudden death risk in patients with hypertrophic cardiomyopathy. Eur
Heart J 2006;27:1933–1941.3. Ommen SR, Maron BJ, Olivotto I, et al. Long-term effects of surgical septal
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
227Berruezo et al Biventricular Pacing in Hypertrophic Obstructive Cardiomyopathy
myectomy on survival in patients with obstructive hypertrophic cardio-myopathy. J Am Coll Cardiol 2005;46:470–476.
4. McLeod CJ, Ommen SR, Ackerman MJ, et al. Surgical septal myectomydecreases the risk for appropriate implantable cardioverter defibrillator dischargein obstructive hypertrophic cardiomyopathy. Eur Heart J 2007;28:2583–2588.
5. Agarwal S, Tuzcu EM, Desai MY, et al. Updated meta-analysis of septal alcoholablation versus myectomy for hypertrophic cardiomyopathy. J Am Coll Cardiol2010;55:823–834.
6. Fananapazir L, Epstein ND, Curiel RV, Panza JA, Tripodi D, McAreavey D.Long-term results of dual-chamber (DDD) pacing in obstructive hypertrophiccardiomyopathy. Evidence for progressive symptomatic and hemodynamic im-provement and reduction of left ventricular hypertrophy. Circulation 1994;90:2731–2742.
7. Rishi F, Hulse JE, Auld DO, et al. Effects of dual-chamber pacing for pediatricpatients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol1997;29:734–740.
8. Kappenberger LJ, Linde C, Jeanrenaud X, et al; for the Pacing in Cardiomy-opathy (PIC) Study Group. Clinical progress after randomized on/off pace-maker treatment for hypertrophic obstructive cardiomyopathy. Europace1999;1:77– 84.
9. Maron BJ, Nishimura RA, McKenna WJ, Rakowski H, Josephson ME, KievalRS. Assessment of permanent dual-chamber pacing as a treatment for drugrefractory symptomatic patients with obstructive hypertrophic cardiomyopathy:A randomized, double-blind, crossover study (M-PATHY). Circulation 1999;99:2927–2933.
0. Nishimura RA, Trusty JM, Hayes DL, et al. Dual-chamber pacing for hyper-trophic cardiomyopathy. A randomized, double-blind, crossover trial. J Am CollCardiol 1997;29:435–441.
1. Ommen SR, Nishimura RA, Squires RW, Schaff HV, Danielson GK, Tajik AJ.Comparison of dual-chamber pacing vs septal myectomy for the treatment ofpatients with hypertrophic obstructive cardiomyopathy. A comparison of objec-tive hemodynamic and exercise end points. J Am Coll Cardiol 1999;34:191–196.
2. Linde C, Gadler F, Kappenberger L, Ryden L. Placebo effect of pacemakerimplantation in obstructive hypertrophic cardiomyopathy. PIC Study Group.Pacing In Cardiomyopathy. Am J Cardiol 1999;83:903–907.
3. Rinaldi CA, Bucknall CA, Gill JS. Beneficial effects of biventricular pacing ina patient with hypertrophic cardiomyopathy and intraventricular conductiondelay. Heart 2002;87:e6.
4. Yufu K, Takahashi N, Ooie T, et al. Improved hypertrophic obstructive cardio-myopathy by left ventricle apex epicardial pacing. Intern Med 2004;43:295–299.
5. Honda T, Shono H, Koyama J, et al. Impact of right atrial-left ventriculardual-chamber permanent pacing in patients with severely symptomatic hyper-trophic obstructive cardiomyopathy. Circ J 2005;69:536–542.
6. Komsuoglu B, Vural A, Agacdiken A, Ural D. Effect of biventricular pacing onleft ventricular outflow tract pressure gradient in a patient with hypertrophiccardiomyopathy and normal interventricular conduction. J Cardiovasc Electro-physiol 2006;17:207–209.
7. Lenarczyk R, Kowalski O, Kukulski T, Kowalczyk J, and Kalarus Z. Resyn-chronization or dyssynchronization—successful treatment with biventricularstimulation of a child with obstructive hypertrophic cardiomyopathy withoutdyssynchrony. J Cardiovasc Electrophysiol 2007;18:542–544.
8. Maron BJ, McKenna WJ, Danielson GK, et al; Task Force on Clinical ExpertConsensus Documents. American College of Cardiology; Committee for Prac-tice Guidelines. European Society of Cardiology.. ACC/ESC clinical expertconsensus document on hypertrophic cardiomyopathy. A report of the ACCFoundation Task Force on Clinical Expert Consensus Documents and the ESC
Committee for Practice Guidelines. J Am Coll Cardiol 2003;42:1687.9. Epstein AE, DiMarco JP, Ellenbogen KA, et al; American College of Cardiol-
ogy/American Heart Association Task Force on Practice Guidelines (WritingCommittee to Revise the ACC/AHA/NASPE 2002 Guideline Update forImplantation of Cardiac Pacemakers and Antiarrhythmia Devices); AmericanAssociation for Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 Guidelines for device-based therapy of cardiac rhythm abnormalities:a report of the American College of Cardiology/American Heart AssociationTask Force on Practice Guidelines. J Am Coll Cardiol 2008;51:e1e62.
0. Devereux RB. Detection of left ventricular hypertrophy by M-mode echocardi-ography. Anatomic validation, standardization, and comparison to other meth-ods. Hypertension 1987;9:II19–II26.
1. Vidal B, Sitges M, Marigliano A, et al. Optimizing the programation of cardiacresynchronization therapy devices in patients with heart failure and left bundlebranch block. Am J Cardiol 2007;100:1002–1006.
2. Silva E, Sitges M, Mont L, et al. Quantification of left ventricular asynchronythroughout the whole cardiac cycle with a computed algorithm: application foroptimizing resynchronization therapy. J Cardiovasc Electrophysiol 2009;20:1130–1136.
3. Bijnens, B, Cikes M, Claus P, Sutherland G. Velocity and deformation imagingfor the assessment of myocardial dysfunction. Eur J Echocardiogr 2009;10:216–226.
4. Yu EH, Omran AS, Wigle ED, Williams WG, Siu SC, Rakowski H. Mitralregurgitation in hypertrophic obstructive cardiomyopathy: relationship to ob-struction and relief with myectomy. J Am Coll Cardiol 2000;36:2219–2225.
5. McAlister FA, Ezekowitz J, Hooton N, et al. Cardiac resynchronization therapyfor patients with left ventricular systolic dysfunction: a systematic review.JAMA 2007;297:2502–2514.
6. Rogers DP, Marazia S, Chow AW, et al. Effect of biventricular pacing onsymptoms and cardiac remodelling in patients with end-stage hypertrophiccardiomyopathy. Eur J Heart Fail 2008;10:507–513.
7. Topilski I, Sherez J, Keren G, Copperman I. Long-term effects of dual-chamberpacing with periodic echocardiographic evaluation of optimal atrioventriculardelay in patients with hypertrophic cardiomyopathy �50 years of age. Am JCardiol 2006;97:1769–1775.
8. Galve E, Sambola A, Saldaña G, et al. Late benefits of dual-chamber pacing inobstructive hypertrophic cardiomyopathy: a 10-year follow-up study. Heart2010;96:352–356.
9. Zugck C, Kruger C, Durr S, et al. Is the 6-minute walk test a reliable substitutefor peak oxygen uptake in patients with dilated cardiomyopathy? Eur Heart J2000;21:540–549.
0. Ito T, Suwa M, Sakai Y, Hozumi T, Kitaura Y. Usefulness of tissue Dopplerimaging for demonstrating altered septal contraction sequence during dual-chamber pacing in obstructive hypertrophic cardiomyopathy. Am J Cardiol2005;96:1558–1562.
1. Jeanreaud X, Goy J-J, Kappenberger L. Effect of dual-chamber pacing inhypertrophic obstructive cardiomyopathy. Lancet 1992;339:1318–1323.
2. Truin G, Backx A, van Wetten H, Neeleman C. Cardiac resynchronizationtherapy for mitral systolic anterior motion in a child. Ann Thorac Surg 2007;83:1873–1874.
3. Panza JA, Maris TJ, Maron BJ. Development and determinants of dynamicobstruction to left ventricular outflow in young patients with hypertrophiccardiomyopathy. Circulation 1992;85:1398–1405.
4. Rivera S, Sitges M, Azqueta M, et al. Left ventricular remodeling in patientswith hypertrophic obstructive cardiomyopathy treated with percutaneous alcoholseptal ablation: an echocardiographic study. Rev Esp Cardiol 2003;56:1174–1181.
5. van Dockum WG, Beek AM, ten Cate FJ, et al. Early onset and progression of
left ventricular remodeling after alcohol septal ablation in hypertrophic obstruc-tive cardiomyopathy. Circulation 2005;111:2503–2508.Copyright © 2022 FDOKUMEN




















