Is there increased sympathetic activity in patients with hypertrophic cardiomyopathy
9
JACCVo|. 26, No. 2 472 August1995:472-80 CARDIOMYOPATHY Is There Increased Sympathetic Activity in Patients With Hypertrophic Cardiomyopathy? L(J FEI, MB, ALISTAIR K. SLADE, MB, KRISHNA PRASAD, MD, MAREK MALIK, PHI), MD, FACC, WILLIAM J. McKENNA, MD, FACC, A. JOHN CAMM, MD, FACC London, England, United Kingdom Objectives. This study aimed to assess autonomic nervous system activity in patients with hypertrophic cardiomyopathy. Background. Patients with hypertrophic cardiomyopathy are traditionally thought to have increased sympathetic activity. How- ever, ¢onviuciug evidence is lacking. Methods. Heart rate variability was assessed from 24.h ambu- latory electrocardiographic (Holter) recordings in 31 patients with hypertrophic cardiomyopathy and 31 age- and gender- matched normal control subjects in a drug-free state. Spectral heart rate variability was calculated as total (0.01 to 1.00 Hz), low (0.04 to 0.15 Hz) and high (0.15 to 0.40 Hz) frequency components using fast Fourier transformation analysis. Resu/ts. There was a nonsignificant decrease in the total frequency component of heart rate variability in patients with hypertrophic cardiomyopathy compared with that of normal subjects (mean ± SD 7.24 ± 0.88 versus 7.59 ± 0.57 ln[ms2], p = 0.072). Although there was no significant difference in the high frequency component (5.31 ± 1.14 versus 5.40 ± 0.91 in[ms2], p = 0.730), the low frequency component was significantly lower in patients than in normal subjects (6.25 +- 1.00 versus 6.72 + 0.61 in[ms21, p = 0.026). After normalization (i.e., division by the total frequency component values), the low frequency component was significantly decreased (38 ± 8% versus 43 ± 8%, p = 0.018) and the high frequency component significantly increased (16 ± 6% versus 12 := 6% p ffi 0.030) in patients with hypertrophic ¢ardiomyopathy. The low/high frequency component ratio was significantly lower in these patients (0.94 ± 0.64 versus 1.33 ± 0.55, p = 0.013). In patients with hypertrophic cardiomyopathy, heart rate variability was significantly related to left ventricular end-systolic dimension and left atrial dimension but not to maximal left ventricalar wall thickness. No significant difference in heart rate variability was found between 14 victims of sudden cardiac death and 10 age. and gender-matched low risk patients. Conclusions. Our observations suggest that during normal daily activities, patients with hypertrophic cardiomyopathy expe- rience a significant autonomic alteration with decreased sympa- thetic tone. (J Am CoU Cardiol 1995;26:472-80) The prevalence and importance of autonomic dysfunction in cardiovascular disease has been increasingly recognized during the last decade. Patients with hypertrophic cardiomyopathy have been thought traditionally to h/we increased sympathetic activity. Exaggerated sympathetic activity or hyperresponsive- ,ess of the myocardium to catecholamines had been suggested as a pathogenic factor in the development of hypertrophic cardiomyopathy (the catecholamine hypothesis) (1), as norepi- nephrine appears to contribute to the induction of myocardial cell growth (2,3). Other observations (4) supporting this hy- pothesis include the hyperdynamic state of the left ventride in most patients with hypertrophic cardiomyopathy and the help- ful effects of beta-adrenergic blocking agents in contro',ling symptoms. However, it is questionable whether sympathetic activity is increased in patients with hypertrophic cardiomyop- From the Departmcntof Cardiological Sciences,St. George'sHospital Medical School, London, England, United Kingdom. Manuscript received October 6,1994; revised manuscript received March 22, 1995, accepted March28, 1995. Address for corresDondgpee" Dr. Lii Fei, Departmentof Cardiological Sciences,St. George's Hospital Medical School,CranmerTerrace, London SW17 ORE, England, UnitedKingdom. athy (5), despite previous repo,ls (6) suggesting that there might be enhanced sympathetic activity or increased norepi- nephrine in the myocardium. Conventional autonomic func- tion testing also suggests that autonomic reflexes may be abnormal in patients with hypertrophic cardiomyopathy (7). Recently, analysis of heart rate variability has provided a noninvasive method for assessment of autonomic nervous system function. However, little is known about heart rate variability in patients with hypertrophic cardiomyopathy, al- though abnormal autonomic activity may play an important part in the pathogenesis of syncope and sudden cardiac death in these high risk patients. Therefore, in this study spectral heart rate variability was assessed in patients with hypertrophic cardiomyopathy and age- and gender-matched normal control subjects to define whether there is increased sympathetic activity during normal daily activities in these patients. Methods Patients. Fifty-two patients with hypertrophic cardiomyop- athy were era'oiled in this study. Thirty-one were in a drug-free state (including 14 victims of sudden cardiac death); the other ©1995 bythe American College of Cardiology 0735-1097195159.50 0735-1097(95)00101-3
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Is there increased sympathetic activity in patients with hypertrophic cardiomyopathy

JACC Vo|. 26, No. 2 472 August 1995:472-80
CARDIOMYOPATHY
Is There Increased Sympathetic Activity in Patients With Hypertrophic Cardiomyopathy? L(J FEI, MB, A L I S T A I R K. SLADE, MB, KRISHNA P R A S A D , MD,
M A R E K MALIK, PHI), MD, FACC, W I L L I A M J. M c K E N N A , MD, FACC,
A. JOHN CAMM, MD, FACC
London, England, United Kingdom
Objectives. This study aimed to assess autonomic nervous system activity in patients with hypertrophic cardiomyopathy.
Background. Patients with hypertrophic cardiomyopathy are traditionally thought to have increased sympathetic activity. How- ever, ¢onviuciug evidence is lacking.
Methods. Heart rate variability was assessed from 24.h ambu- latory electrocardiographic (Holter) recordings in 31 patients with hypertrophic cardiomyopathy and 31 age- and gender- matched normal control subjects in a drug-free state. Spectral heart rate variability was calculated as total (0.01 to 1.00 Hz), low (0.04 to 0.15 Hz) and high (0.15 to 0.40 Hz) frequency components using fast Fourier transformation analysis.
Resu/ts. There was a nonsignificant decrease in the total frequency component of heart rate variability in patients with hypertrophic cardiomyopathy compared with that of normal subjects (mean ± SD 7.24 ± 0.88 versus 7.59 ± 0.57 ln[ms2], p = 0.072). Although there was no significant difference in the high frequency component (5.31 ± 1.14 versus 5.40 ± 0.91 in[ms2], p = 0.730), the low frequency component was significantly lower in
patients than in normal subjects (6.25 +- 1.00 versus 6.72 + 0.61 in[ms21, p = 0.026). After normalization (i.e., division by the total frequency component values), the low frequency component was significantly decreased (38 ± 8% versus 43 ± 8%, p = 0.018) and the high frequency component significantly increased (16 ± 6% versus 12 := 6% p ffi 0.030) in patients with hypertrophic ¢ardiomyopathy. The low/high frequency component ratio was significantly lower in these patients (0.94 ± 0.64 versus 1.33 ± 0.55, p = 0.013). In patients with hypertrophic cardiomyopathy, heart rate variability was significantly related to left ventricular end-systolic dimension and left atrial dimension but not to maximal left ventricalar wall thickness. No significant difference in heart rate variability was found between 14 victims of sudden cardiac death and 10 age. and gender-matched low risk patients.
Conclusions. Our observations suggest that during normal daily activities, patients with hypertrophic cardiomyopathy expe- rience a significant autonomic alteration with decreased sympa- thetic tone.
(J Am CoU Cardiol 1995;26:472-80)
The prevalence and importance of autonomic dysfunction in cardiovascular disease has been increasingly recognized during the last decade. Patients with hypertrophic cardiomyopathy have been thought traditionally to h/we increased sympathetic activity. Exaggerated sympathetic activity or hyperresponsive- ,ess of the myocardium to catecholamines had been suggested as a pathogenic factor in the development of hypertrophic cardiomyopathy (the catecholamine hypothesis) (1), as norepi- nephrine appears to contribute to the induction of myocardial cell growth (2,3). Other observations (4) supporting this hy- pothesis include the hyperdynamic state of the left ventride in most patients with hypertrophic cardiomyopathy and the help- ful effects of beta-adrenergic blocking agents in contro',ling symptoms. However, it is questionable whether sympathetic activity is increased in patients with hypertrophic cardiomyop-
From the Departmcnt of Cardiological Sciences, St. George's Hospital Medical School, London, England, United Kingdom.
Manuscript received October 6,1994; revised manuscript received March 22, 1995, accepted March 28, 1995.
Address for corresDondgpee" Dr. Lii Fei, Department of Cardiological Sciences, St. George's Hospital Medical School, Cranmer Terrace, London SW17 ORE, England, United Kingdom.
athy (5), despite previous repo,ls (6) suggesting that there might be enhanced sympathetic activity or increased norepi- nephrine in the myocardium. Conventional autonomic func- tion testing also suggests that autonomic reflexes may be abnormal in patients with hypertrophic cardiomyopathy (7).
Recently, analysis of heart rate variability has provided a noninvasive method for assessment of autonomic nervous system function. However, little is known about heart rate variability in patients with hypertrophic cardiomyopathy, al- though abnormal autonomic activity may play an important part in the pathogenesis of syncope and sudden cardiac death in these high risk patients. Therefore, in this study spectral heart rate variability was assessed in patients with hypertrophic cardiomyopathy and age- and gender-matched normal control subjects to define whether there is increased sympathetic activity during normal daily activities in these patients.
M e t h o d s
Patients. Fifty-two patients with hypertrophic cardiomyop- athy were era'oiled in this study. Thirty-one were in a drug-free state (including 14 victims of sudden cardiac death); the other
©1995 by the American College of Cardiology 0735-1097195159.50 0735-1097(95)00101-3

JACC Vol. 26, No. 2 FEI ET AL. 473 August 1995:472-80 HEART RATE VARIABILITY IN HYPERTROPHIC CARDIOMYOPATHY
1"able 1. Clinical Characteristics of 52 Patients With Hypertrophic Cardiomyopathy
Age (yr) 34 +- 17 Male 22 Echocardiographic findings
LVm, (ram) 24 *- 7 LA (tara) 42 -+ 8 LVEDD (ram) 44 ± 8 LVESD (ram) 26 ± 8 LVEF (%) 78 +- it RVH 6
Patients with symptoms Syncope or presyncope, or both 25 Dyspnea 20 Chest pain 16 Sudden cardiac death 14
Patients receiving amiodarone therapy 21
Data are expressed as mean value +- SD or number of patients. LA = left atrial dimension; LVEDD = left ventricular end-diastolic dimension; LVEF = left ventricular ejection fraction; LVESD = left ventrieulat end-systolic dimen- sion; LVm~, = maximal left ventricular wall thickness; RVH = right ventricular hypertrophy.
21 were receiving amiodarone therapy (200 rag/day) for sup- pression of nonsustained ventricular tachycardia and were matched by age and gender with the 31 pat~et~ts not receiving amiodarone therapy. The clinical characteristics of the 52 patients with hypertrophic cardiomyopathy are summarized in Table 1. Patients with sinus node dysfunction, atrioventricular block and intraventricular conduction defects were excluded. Thirty-one age- and gender-matched normal subjects were taken as a control group. None of these normal subjects had significant cardiac or other medical problems. Results of their 12-lead and 24-h ambulatory electrocardiograms (ECGs) were entirely normal.
To define whether assessment of heart rate variability is helpful in identifying patients at increased risk of sudden cardiac death, 10 low risk patients matched by age and gender with the high risk patients in a drug-free state were carefully selected for comparison of heart rate variability. The low risk patients were defined as having no syncopal episodes, no adverse family history and no ventricular tachycardia on am- bulatory ECG monitoring.
Left atrial dimension, maximal left ventricular wall thick- ness, left ventricular end-diastolic and end-systolic dimension and left ventricular ejection fraction were measured by echo- cardiography with the use of established techniques.
Analysis of heart rate variability. All patients and control subjects underwent two-channel 24-h Holter ambulatory ECG monitoring (Marquette). Heart rate variability was analyzed from ambulatory Holter ECGs on a Holter analysis system (Marquette Series 8000). After classification of QRS configu- ration, the longest and the shortest RR intervals on the RR interval histogram and the largest and the smallest RR ratios on the RR ratio histogram were manually confirmed until no QRS complex was mislabeled as either an artifact or an ¢ctopic beat. When heart rate variability variables were calcuated, only
normal to normal intervals were included. In this study, spectral heart rate variability was computed as total (0.01 to 1.00 Hz), low (0.04 to 0.15 Hz) and h:.gh (0.15 to 0.40 Hz) frequency components using fast Fourier transformation in 2-rain intervals. Heart rate variability over the 24 h was an average of all the 2-rain values. The low and high frequency powers of heart rate variability were also computed in normal- ized units that were calculated by dividing the frequency power by the total frequency power and were expressed as a percent (8,9). The low/high frequency component ratio (low/high ratio) was calculated as an index of sympathovagal balance of the heart (8,10). The mean heart rate was derived from the mean of all normal RR intervals.
Statistical analysis. All data are expressed as mean value _.+ SD. The unpaired Student t test, multiple correlation and regression analyses were used where appropriate. For comparison of the frequency components of heart rate vari- ability, logarithmic values---In (total frequency component), In (low frequency component), In (high frequency component) or In (low/high ratio)--were used to normalize the skewness of the data. A two-tailed p value < 0.05 was considered statisti- cally significant.
Resul t s
Comparison between normal subjects and patients with hypertrophic cardiomyopathy. The mean heart rate did not differ significantly between patients with hypertrophic car- diomyopathy and normal subjects (74 +- 11 versus 71 _+ 9 beats/rain, p = 0.183). Figure 1 shows tlte scatterpiots of heart rate variability in patients with hypertrophic cardiomyopathy and normal subjects. There was a nonsignificant decrease in the total frequency component of heart rate variability in patients with hypertrophic cardiomyopathy compared with that in normal subjects (7.24 + 0.88 versus 7.59 +- 0.57 In[ms2], p = 0.072). Although the high frequency component did not differ (5.31 -+ 1.14 versus 5.40 -+ 0.91 In[ms2], p = 0.730), the low frequency component was significantly lower in patients than in normal subjects (6.25 -+ 1.00 versus 6.72 _+ 0.61 In[ms2], p = 0.026). The low/high ratio was also significantly lower in patients with hypertrophic eardiomyopathy (5.31 +- 1.14 versus 5.40 ± 0.91 In[ms2], p = 0.730). To gain insight in'~3 the abnormal heart rate variability, we normalized the low and high frequency components using a modification of the method suggested by Pagani et al. (8) and Lombardi et al. (9); that is, the frequency components were divided by the total frequency component of heart rate variability. After normalization, the low frequency component was significantly lower (38 - 8% versus 43 +- 8%, p = 0.018) and the high frequency component was significantly higher (16 -+ 6% versus 12 __ 6%, p = 0.030) in patients with hypertrophic cardiomyopathy than in normal subjects. The circadian variations of heart rate and heart rate ~ariability are shown in Figures 2 and 3. Significant differences in heart rate variability occurred mainly during waking hours.

474 F~EI ET AL. JACC Vol. 26, No. 2 HEART RATE VARIABILITY IN HYPERTROPHIC CARDIOMYOPATHY August 1995:472-80
E v i -
14. I...
U .
10
9
8
7
5
4
6
S
4
3
2
1
p = 0 . 0 7 2
H C M NC
p : 0 .7~0
T H C M NC
l a [
4
3
2.5 !2 1.S
1
0.5
p = 0 .026
T ÷
H C M NC
p = 0.013
-t.
_1._ 0 ! "r
e
o
HCM NC
Figure 1. Scatterplots of the frequency components of heart rate variability and the low/high frequeacy component ratio in 31 patients with hypertrophic cardiomyopathy (HCM) and 31 age- and gender- matched normal control subjects (NC). HF = high frequency compo- nent; LF = low frequency component; TF = total frequency compo- nent. Lon~ and short horizontal bars = mean value ± standard deviation, respectively,
Comparison of patients with and without amiodarone therapy. There was no significant difference in age or in echo- cardiographic findings between patients who were and were not receiving amiodarone (Table 2). Figure 4 shows the circadian variation of heart rate and heart rate variability in patients who were and were not receiving amiodarone therapy; the mean heart rate was significantly slower in patients receiv- ing amiodarone (64 ± 15 versus 74 +_ 11 beats/rain, p = 0.011). The total frequency (6.79 +_ 1.02 versus 7.24 _+ 0.88 In[ms2], p = 0.104), low frequency (5.72 +_ 1.18 versus 6.25 + 1.00, In[ms2], p = 0.099) and high frequency (4.87 +_ 1.15 versus 5.31 .+_ 1.14 In[ms2], p = 0.179) components of heart rate variability and the low/high ratio (0.85 _+ 0.60 versus 0.94 _+ 0.64, p = 0.618) tended to be lower in patients receiving amiodarone (p = NS, unpaired t test). However, after normal- ization for heart rate, the difference in all frequency compo- nents of heart rate variability was highly significant (p --. 0.001)
(analysis of covariance with heart rate as a covariant), but the low/high ratio remained essentially similar (Fig. 5).
Comparison of patients at high and low risk. There was no significant difference between patients at high and low risk for sudden cardiac death in terms of age, left atrial dimension, maximal left ventrieular wall thickness, left ventricular end- diastolic and end-systolic dimension or left ventricular ejection fraction (Table 3). Neither mean heart rate (73 +- 11 versus 73 +_ 13, p = 0.969) nor the total frequency (7.28 +__ 0.78 versus 7.38 +_ 0.94 In[ms2], p = 0.784), low frequency (6.25 ± 0.82 versus 6.50 +_. 0.86 In[ms2], p = 0.477) or l.i[~h frequency (5.43 ± 0.96 versus 5.45 ± 1.52 In[ms2], p = 0.~;80) components of heart rate variability differed significantly different between low and high risk patients.
Relation between heart rate variability and other clinical findings. There were 20 patients with dyspnea; all 20 were in New York Heart Association functional class II. Patients with dyspnea had lower heart rate variabili~ty values than did those without dyspnea (Table 4). Patients with significant right ventrieular hypertrophy (n = 6) tended to have more signifi- cant left ventricular hypertrophy, but there was no significant difference in left ventricular ejection fraction, mean heart rate and heart rate variability between patients with and without right ventricular hypertrophy (Table 5).
Multiple correlation analysis showed that heart rate vari- ability in patients with hypertrophic cardiomyopathy was sig-

. IACC Vol . 26, No. 2 F E i E T AL. 475 A u g u s t 1995:472-80 H E A R T R A T E V A R I A B I L I T Y IN H Y P E R T R O P H I C C A R D I O M Y O P A T H Y
110 ,0o 90
8O
O0
SO c
'°i i;i 2 0 r 0 2 4 6
(IC r
6
5
,I
3 " •
I I I I I 2 0 2 4 6 8
I I t I i I 8 10 12 14 16 18 20 22 24
LF
4 t n
81
71
6
5
4
3
• • • • & • •
, , , , , , : , ; , , 2 4 6 8 10 12 1 16 1 20 22 24
HF
• A A • • & • • •
1 12 14 16 1 24 2 4 6
Time of Day (O'Clock) 8 10 1 1 16 ~8 20 22 24
nificantly related to age, left atrial dimension, left ventricular end-systolic dimension and left ventricular ejection fraction but not to mean heart rate, maximal left ventricular wall thickness or left ventricular end-diastolic dimension (Table 6). There appeared to be no significant relation between heart rate variability and left atrial dimension when left atrial dimension was within the normal value of <40 ram. However, this relation became substantially stronger when there was a dilated left atrium within a range of 41 to 53 mm (Fig. 6). Stepwise multiple regression analysis showed that both the total and low frequency components of heart rate variability were independently related to age (p = 0.0001), left ventricular end systolic dimension (p = 0.0001 and 0.0005, respectively) and left atrial dimension (p = 0.0102 and 0.0062, respectively). The high frequency component of heart rate variability was independently related to age (p = 0.0001) and left ventricular end-systolic dimension (p = 0.0021).
Discussion Physiologic significance of heart rate variability. Analysis
of heart rate variability has been widely accepted as a nonin- vasive method for assessment of autonomic influence on the heart (11). Although heart rate variability measures autonomic influence at the level of sinus node, it is generally assumed to reflect the global autonomic control of cardiovascular activi-
Figure 2. Circadian vada'tion of heart rate (HR) and heart rate variability (HRV) in patients with hypertrophic cardiomyopathy and in normal control subjects. I:.pm = beats per minute. Triangles = p < 0.05; solid lines and crosshatched areas = mean values ± SD, respectively, in patients with hypertrophic cardiomyopathy; broken lines and dotted areas = mean values +_ SD, respectively, in normal control subjects. Data are expressed as mean value + SD. Other abbreviations as in Figure 1.
ties. Spectral analysis of heart rate variability can partially distinguish parasympathetic from sympathetic influence on the heart. The low frequency, component of spectral heart rate variability gives largely a measure of sympathetic activity with some influence from the parasympathetic nervous system. The high frequen~ component is almost exclusively mediated by vagal activity. The low/high frequency component ratio has been used as an index of the sympathovagal balance to the heart (8-10). An increased low/high ratio suggests increased sympathetic or decreased parasympathetic drive to the heart, or both, and vice w;rsa (10). An alternative method of assessing sympathetic and parasympathetic activity, thought to be less dependent on the global change in heart rate variability (8-10,12), is calculation of heart rate variability in normalized units. Sympathowigal interaction of the two opposing branches of the autonomic nervous system may play a more important role than either one in the pathophysiologic activities of the heart (12-14).

476 FEI El" AL. JACC Vol. 26, No. 2 HEART RATE VARIABILITY IN HYPERTROPHIC CARDIOMYOPATHY August 1995:472-80
$.~
3
~ . 2.5
- r 2
. J
I= 1.s , . I
1
0.5
& & & & & & & & & & & & & & &
0 2 4 6 8 10 12 14 16 18 20 22 24
Time of Day (O'Clock)
Figure 3. Circadian variation of the low/high frequency component ratio in patients with hypertrophic cardiomyopathy and in normal control subjects. Triangles = p < 0.05; solid line and crosshatched area = mean value +- SD, respectively, in patients with hypertrophic cardiomyopathy; broken line and dotted area = mean value +- SD, respectively, in normal control subjects. Data are expressed as mean value _+ SD in natural logarithm values. Abbreviations as in Figure 1.
Main findings of the present study. 1) Is there increased sympathetic activity in patients with hypertrophic cardiomyopa- thy? Although heart rate variability has been extensively as- sessed during the last decade, data on heart rate variability in patients with hypertrophic cardiomyopathy are scarce and inconclusive. In this study, the absolute and normalized values of the low frequency component and the low/high ratio were decreased. These observations suggest that there is a decrease in sympathetic tone during normal daily activities, a view partially consistent with previous findings (15,16) of a signifi- cant decrease in overall heart rate variability in patients with hypertrophic cardiomyopathy. However, patients with hyper- trophic cardiomyopathy have been reported (15,16) to have an increased low/high ratio. For example, Ajiki et al. (16) found no significant difference in heart rate variability from 8:00 AM tO noon between 15 patients with hypertrophic cardiomyopa- thy and 18 healthy subjects; however, the high frequency component was significantly lower and the low/high ratio significantly higher during the night (midnight to 4:00 AM) in the patients with hypertrophic cardiomyopathy. Heart rate variability in their study was calculated from three selected 10-rain periods (after 1/f compo~,~nt was removed) rather than from the whole 24-h. Their definition of the low frequency component includes the lower frequency components (<0.04 Hz) of uncertain clinical significance rather than the conventional low frequency component (0.04 to 0.15 Hz). Whether their healthy subjects were matched by age and gender with the patients studied is unknown. These factors m~y significantly influence the heart rate variability values and may explain why our findings differ from theirs.
2) Possible mechanisms underlying abnormal autonomic ac- tivity in patients wi,,. hypertrophic cardiomyopathy. Gilligan et al. (7) recently reported that impaired autonomic reflexes are related to the severity of left ventricular hypertrophy. In
Table 2. Clinical Variables of Patients Receiving and Not Receiving Amiodarone Therapy
Receiving Not Receiving Amiodarone Amiodarone p
(n = 21) (n = 31) Value
Age (yr) 33 ± 18 36 ± 17 0.451 LVma x (ram) 24 ± 7 24 _+ 7 0.804 LA (ram) 43 ~- 9 41 +-. 8 0.264 LVEDD (ram) 45 ± 9 43 ± 8 0.624 LVESD (ram) 27 ± 8 25 ± 7 0.427 LVEF (%) 76 ± 11 79 ± 10 0.492
Data are expressed as mean value ± SD. Abbreviations as in Table 1.
contrast, we demonstrated that heart rate variability is signif- icantly related to left ventricular end-systolic cavity dimension and left ventricular ejection fraction but not to the extent of left ventricular hypertrophy. Because the baroreceptor reflex contributes to heart rate fluctuations, the altered heart rate variability may be partially due to the supernorrnal systolic function (4) in addition to left atrial stretching (Bainbridge reflex) and activation of mechanoreceptors in the ventricles (Bezold-Jarisch reflex). Myocardial ischemia in hypertrophic cardiomyopathy (4,17) and impaired cardiogenic reflexes con- sequent to left ventricular hypertrophy (18) may also contrib- ute to autonomic changes in these patients. Whether the alteration in autonomic activity results from genetic abnormal- ities in familial hypertrophic cardiomyopathy (19,20) is un- clear.
Several investigators have demonstrated that diastolic func- tion is often impaired (21) and left atrial pressure elevated (22) in patients with hypertrophic cardiomyopathy. Therefore, im- pairment of left ventricular diastolic function may contribute to the alteration of heart rate variability. Dyspnea is common in patients with hypertrophic eardiomyopathy and has been considered to be due to a rapid increase in left atrial pressure as a result of impaired diastolic filling at a high heart rate (23). Our patients with dyspnea had a significantly lower heart rate variability than that of patients without dyspnea. Despite the unclear mechanisms underlying the relation between de- creased heart rate variability and dyspnea, these observations further support the view that impaired diastolic function may contribute to the decrease in heart rate variability.
Table 3. Clinical Variables of Patients at High and Low Risk for Sudden Cardiac Death
Patients at Patients at High Risk Low Risk (n = 14) (n = 10)
P Value
LVm,~, (ram) 25 +- 6 23 z 8 0.601 LA (mm) 41 ± 8 42 -+ 8 0.763 LVEDD (ram) 41 ± 8 46 ± 9 0.245 LVESD (ram) 25 ± 6 26 ± 10 0.617 LVEF (%) 77 -4- 11 79 ± 12 0.590
Data are expressed as mean value ± SD. Abbreviations as in Table 1.
JACC Vol. 26, No. 2 FEI ET AL 477 August 1995:472-80 HEART RATE VARIABILITY IN HYPERTROPHIC CARDIOMYOPATHY
90 8 -
70
0 2 4 6 8 10 12 14 16 18 20 22 24 0 2 4 6 8 10 12 14 16 18 20 22 24 "o
A
E Q. JD
iT. 3:
9
8
7
6
5
4
3
2
LF HF
• i i i i i i i / i i i~
0 2 4 8 a 1 1 1 1 18 2 2 ~4 0 2 4 6 0 10 12 1 16 1 20 24
Time of Day (O'Clock)
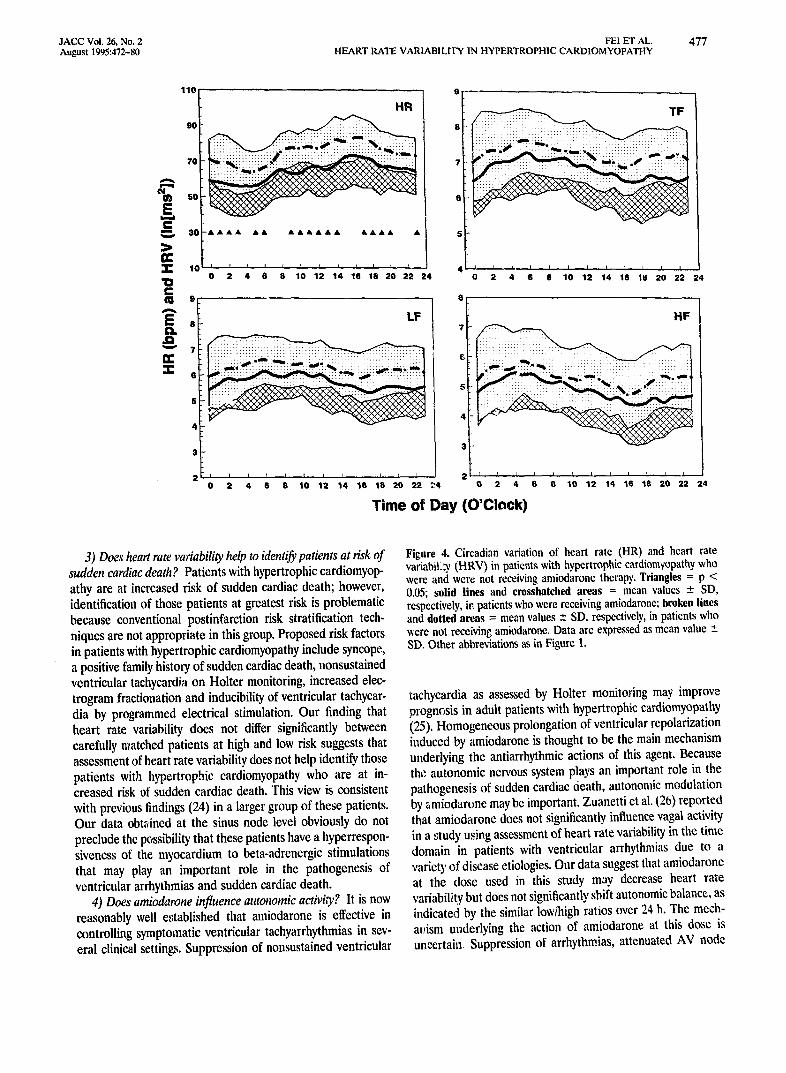
3) Does heart rate variability help to identify patients at sisk of sudden cardiac death? Patients with hypertrophic cardiomyop- athy are at increased risk of sudden cardiac death; however, identification of those patients at greatest risk is problematic because conventional postinfarction risk stratification tech- niques are not appropriate in this group. Proposed risk factors in patients with hypertrophic eardiomyopathy include syncope, a positive family history of sudden cardiac death, nonsustained ventricular tachycardia on Holter monitoring, increased elec- trogram fractionation and inducibility of ventricular tachycar- din by programmed electrical stimulation. Our finding that heart rate variability does not differ significantly between carefully matched patients at high and low risk suggests that assessment of heart rate variability does not help identify those patients with hypertrophic cardiomyopathy who are at in- creased risk of sudden cardiac death. This view is consistent with previous findings (24) in a larger group of these patients. Our data obtzdned at the sinus node level obviously do not preclude the possibility that these patients have a hyperrespon- siveness of the myocardium to beta-adrenergic stimulations that may play an important role in the pathogenesis of ventricular arrhythmias and sudden cardiac death.
4) Does amiodarone influence autonomic activity? It is now reasonably well e,,aablished that amiodarone is effective in controlling symptomatic ventricular tachyarrhythmias in sev- eral clinical settings. Suppression of nonsustained ventricular
Figure 4. Circadian variation of heart rate (HR) and heart rate variabiLw, (HRV) in patients with hypertrophic cardiomyopathy who were and were not receiving amiodarone therapy, Triangles = p < 0.{15; solid lines and crosshatched areas = mean values -+ SD, respectively, it~ patients who were receiving amiodarone; broken lines and dotted areas = mean values -+ SD, respectively, in patients who ~'ere not receiving amiodarone, Data are expressed as mean value -+ SD. Other abbreviations as in Figure 1.
tachycardia as assessed by Holter monitoring may improve prognosis in adult patients with hypertrophic cardiomyopathy (25). Homogeneous prolongation of ventricular repolarization induced by amiodarone is thought to be the main mechanism underlying the antiarrhythmic actions of this agent. Because the autonomic nervous system plays an important role in the pathogenesis of sudden cardiac 6eath, autonomic modulation by amiodarone may be important. Zuanetti et al. ~26) reported that amiodarone does not significantly influence vagai activity in a study using assessment of heart rate variability in the time domain in patients with ventricular arrhythmias due to a variety of disease etiologies. Our data suggest that amiodarone at the (lose used in this study may decrease heart rate variability but does not significantly shift autonomic balance, as indicated by the similar low/high ratios over 24 h. The mech- ar~ism uL;~derlying the action of amiodarone at this dose is uncertain Suppression of arrhythmias, attenuated AV node

478 FEI El" AL. JACC Vol. 26, No. 2 HEART RATE VARIABILITY IN HYPERTROPHIC CARDIOMYOPATHY August 1995:472-80
2.5
E" .!-
c ..t 1
0.5
I i I i i , q . i , i , I L I t I , I , i , i ,
2 4 6 8 10 12 14 16 18 20 22 24
T i m e of Day (O'Clock)
Figure 5. Circadian variation of the low/high frequency component ratio in patients with hypertrophic cardiomyopathy who were and were not receiving amiodarone therapy. Solid line and crosshatched area = mean value -+ SD, respectively, in patients who were receiving amiedarone; broken line and dotted area = mean value +_ SD, respectively, in patients who were not receiving amic,xiarone. Data are expressed as mean value -+ SD in natural logarithm values. Abbrevi- ations as in Figure 1.
conauction, raised ventricular fibrillation thresholds and influ- ence on peripheral vasomotor responses have all been pro- posed to be relevant.
Clinical implications. It is generally assumed that sudden cardiac death occurs as a result of ventricular arrhythmias. Hemodynamic abnormalities may also contribute to its patho- genesis in patients with hypertrophic cardiomyopathy (27). Exercise hypotension due to inappropriate peripheral vasodi- lation has been demonstrated (28) in one third of patients with hypertrophic cardiomyopathy. The mechanism of this exercise hypotension is unclear, but it has been attributed to activation of ventricular mechanoreceptors (28). Nonetheless, our obser- vations suggest that alterations in autonomic activity may
Table 4. Heart Rate Variability in Patients in New York Heart Association Functional Classes I and II
NYHA Class I NYHA Class 11 (no dyspnea) (dyspnea) p
(n = 32) (n = 20) Value
Age (yr) 30 + 16 43 __- i7 0.015" INmax (ram) 23 _ 8 25 _ 5 0.218 LA (ram) 40 ± 8 44 ± 9 0.158 LVEDD (ram) 46 _+ 8 41 --- 8 0.055 LVESD (ram) 28 ± 8 23 -+ 7 0.008t LVEF (%) 76 ± 9 80 -- 14 0.271 HR (beats/rain) 69 ± II 72 - 18 0.607 TF (In[ms2]) 7.48 ± 0.73 6.42 ± 0.93 0.000t LF (In[ms2]) 6.54 ± 0.73 5.28 -+ 1.15 0.000t HF (la[ms~]) 5.49 _ 1.12 4.57 _+ 1.03 0.005t In(LF/HF) 1.04 _ 0.60 0.71 ± 0.62 0.069
'p < 0.05. tp < 0.01. Data are expressed as mean value ± SD. HF = high frequency component; HR = heart rate; LF = low frequency component; NYHA Class = New York Heart Association fimetional class; TF = total frequency component; other abbreviations as in Table 1.
Table 5. Heart Rate Variability in Patients With and Without Right Ventricular Hypertrophy
With Without p RVH RVH Value
Age (yr) 33 --. 16 28 ± 14 0.446 LV=~, (mm) 22 -+ 7 29 - 3 0.001t LA (ram) 42 - 8 35 ± 6 0.048* LVEDD (ram) 45 ± 8 34 ± 7 0.008t LVESD (ram) 27 - 6 1'~ ± 2 0.000t LVEF (%) 78 - 10 80 +- 16 0.807 HR (beats/rain) 70 - 16 73 ± 8 0.454 TF (ln[msZ]) 7.09 -+ 1.04 7.03 __. 0.35 0.797 LF (In[ms2]) 6.07 +- 1.18 6.08 --- 0.28 0.975 IIF (In[ms2]) 5.17 *-. 1.23 4.86 ± 0.68 0.386 In(LF/HF) 0.90 -- 0.65 1.22 _+ 0.58 0.258
*p < 0.05. tp < 0.01. Data are expressed as mean value __ SD. Abbreviations as in Tables 1 and 4.
contribute to hemodynamic instability and to the subsequent development of syncope and sudden cardiac death in these patients. A further study is needed to investigate whether there is an abnormal autonomic response (by heart rate variability analysis) to physical perturbations (such as exercise) in patients with hypertrophic cardiomyopathy because confirmation of the possible mechanism underlying syncope and sudden cardiac death would be important in the management of these pa- tients. However, in addition to reduced sympathetic activity, other mechanisms, such as impaired alpha-receptor mediated vasoconstriction (29), may also be responsible for vasodilation in hypertrophic cardiomyopathy.
Potential limitations of the study. Our present findings were derived from the data of spectral analysis of heart rate variability. The low frequency component of heart rate vari- ability is by no means a measure o f"pure" sympathetic activity without the influence of the parasympathetic nervous system; therefore, our results may be potentially misleading. Global heart rate variability (including the total, high and low fre- quency components) may be markedly decreased in certain physiologic and pathologic conditions associated with a sym- pathetic predominance, su,:h as intense exercise (30) and congestive heart failure (31,32), in which normal autonomic modulation of the sinus node may be altered. In contrast to the overall depressed heart rate variability seen in patients with
Table 6. Correlation Coefficient (p value) Between the Frequency Components of Heart Rate Variability and Other Clinical Variables in 52 Patients With Hypertrophic Cardiomyopathy
Total Frequency Low Frequency High Frequency
Age -0.49 (0.000)t -0.51 (0.000)t -0.43 (0.002)t Mean HR -0.07 (0.611) -0.01 (0.925) -0.17 (0.251) LA -0.32 (0.023)* -0.36 (0.011)* -0.22 (0.133) LVm~, -0.14 (0.350) -0.12 (0.423) -0.11 (0.243) LVEDD 0.09 (0.530) 0.05 (0.753) 0.12 (0.401) LVESD 0.2~ (0.051) 0.22 (0.119) 0.29 (0.045)* LVEF -0.29 (0.04i)* -0.25 (0.088) -0.30 (0.036)*
*p < 0.05. tp < 0.01. Abbreviations as in Tables 1 and ,t.

.IACC Vol. 26, No. 2 FEI ET AL. 479 August 1995:472-80 HEART RATE VARIABILITY IN HYPERTROPHIC CARDIOMYOPATHY
Figure 6. Relation between the total (TF), low (LF) and high (HF) frequency components of heart rate variability (HRV) and left atrial cavity dimension within the range 41 to 53 mm in 20 patients with hypertrophic cardiomyopathy.
12
~ lO
I ~ a
i , Z "6 II.
r : - o.'r't
p : o.oool
t
,
'
0 . 1 . . I , I , I , I . I , I . I , I . t , I . t i
41 42 43 44 45 43 47 43 49 SO $1 52 53
Left Atrium (ram)
12 I
P" 10
g i: 3
"6 t tL . I
r = - 0.78
p < 0.0001
¢
, - - - - . . . : .
t t
2
0 t . l , l . l . l , l . l , l , l , l , I .
41 42 45 44 4S 43 47 43 49 50 St 52 53
Left Atrium (mm)
12
"q lO A
g t: 3
m
i '
r : - 0.63
p : 0 .0028
¢ ¢
° °
t 2
0 t i , I . I , I , I , I , I . I , I . t . I ,
41 42 4S 44 45 46 47 48 49 SO Sl 52 53
Left Atrium (mm)
congestive heart failure, our patients with hypertrophic car- diomyopathy (without significant clinical evidence of conges- tive heart failure) had a selective reduction in the low fre- quency component of heart rate variability. The decreased low/high ratio further suggests that there might be reduced sympathetic activity. However, our data, also do not preclude the possibility of decreased chronotropic responses of the heart to autonomic stimulation, such as that seen in congestive heart failure (33,34), although this alteration is unlikely in patients with hypertrophic cardiomyopathy. Furthermore, spectral analysis over 24-h periods is potentially limited be- cause of nonstationary oscillations of the RR intervals. How- ever, our long-term heart rate variability was calculated as the average of all 2-rain values; this procedure may partially exclude the influence of nonstationarities of the data (running spectra). This is supported by our observation that the heart rate variability over 24 h calculated in this way is significantly related to that recorded during a short and stable period (35). Nevertheless, our data cast doubt on the traditional concept that there is increased sympathetic activity in patients with hypertrophic cardiomyopathy.
Conclusions. Patients with hypertrophic cardiomyopathy experience a significant autonomic alteration with decreased sympathetic tone during normal daily activities. Impairment of both left ventricular systolic and diastolic function may be responsible for the abnormal autonomic activity, and this abnormal activity may contribute to the hemodynamic insta- bility in these patients. Our observations also suggest that amiodarone may significantly decrease global heart rate vari- ability but does not significantly shift the autonomic balance and that assessment of heart rate variability is not helpful in identifying the patients in this group who are at high risk of sudden cardiac death.
References I. Perloff JK. Pathogenesis of hypertrophic cardiomyopathy: hypotheses and
speculations. Am Heart J 1981;101:219-26. 2. Laks MM, Morady F, Swan HJ. Myocardial hypertrophy produced by
chronic infusion of subhypertensive doses of norepinephrine in the dog. Chest 1973;64:75-8.
3. Panagia V, Pierce GN, Dhalla KS, Ganguly PK, Beamish RE. Dhalla NS. Adaptive changes in subccllular calcium transport during catecholamines- induced cardiomyop;,thy. J Mol Cell Cardiol 1985;17:411-20.
4. Louie EK, Edwards LC III. Hypertrophic cardiomyopathy. Prog Cardiovase Dis 1994;35:275-308.
5. Lefroy DC, De Silva R, Choudhury L, ct al. Diffuse reduction of myocardial beta-adrenoccptors in hypertrophic cardiomyo?athy: a study with positron emission tomography. ,~ Am Col! Cardiol ~993:22:1653-60.
6. Pearsc AG. Histochemistry and Electronmicrosc%;e of Cbstructive Cardio- myopathy. CIBA Foundation Symposium. Boston: Little, Brown, 1964:132.
7. Gilligan DM, Chan WL, Sbarouni E. Nihoyannopoulos P, Oakley CM. Autonomic function in hypertrophic cardiomyopathy. Br Heart J 1993;69: 525-9.
8. Pagani M, Lombardi F, Guzzctti S, et al. Power spectral analysis of heart rat~: and arterial pressure variabilities as a marker oi sympathovagal interaction in man and conscious dog. Circ Res 1986;59:178-93.
9. Lombardi F, Torzillo D. Sandrone G, et al. Beta-blocking effect of propafenone based on spectral analysis of heart rate variability. Am J Cardiol 1992;70:1028-34.
10. MaUiani A, Lombardi F, Pagani M. Power spectrum analysis of heart rate

480 FEI El" AL. JACC Vol. 26, No. 2 HEART RATE VARIABILITY IN HYPERTROPHIC CARDIOMYOPATHY August 1995:472-80
variability: a tcol to explore neural regulatory mechanisms. Br Heart J 1994;71:1-2.
11. Lii Fei, Malik M. Heart rate variability. Methodology and physiological basis. In: Aubert AE, Ector H, Struobandt R, editors. Cardiac Pacing and Electruphysiology: A Bridge To The 21st Century. Dordrecht: Kluwer AcaoemJc Publishers, 1994:49-62.
12. Montano N, Gnecchi Ruscone T, Porta A, Lombardi F, Pagani M, Malliani A, Power spectral analysis of heart rate variability to assess the changes in sympathovagal balance during graded orthostatie tilt. Circulation 1994;90:1826-31.
13. Zipes DP, Miyazaki T. The autonomic nervous system and the heart: basis for understanding interactions and effects on arrhythmia development. In Zipes DP, Jalife J, editors. Cardiac Electruphysiology. From Single Cell to Bedside. Philadelphia: Saunders; 1990:312-30.
14. Verder RL. Neurogenic aspects of cardiac arrhythmias. In: EI-Sherif N, Samet P, editors. Cantiae Pacing and Electrophysiology. Philadelphia: Saundcrs, 1991:77-91.
15. Guzzetti S, Choudhury L Mezzetti S, Malliani A, Camici PC. Enhanced sympathetic activity identified by heart rate variability analysis in hypertro- phic cardiomyopathy [abstract]. J Am Coil Cardiol 1994;24 Suppl A:47A.
16. Ajiki K, Murakawa Y, Yanagisawa-Miwa A, et al. Autonomic nervous system activ/ty in idiopathic dilated cardiomyopathy and in hypertrophic cardiomyopathy. Am J Cardiol 1993;71:1316-20.
17. Zipes DP. Influence of myocardial ischemia and infarction on autonomic innervation of heart. Circulation 1990;82:1095-105.
18. Grassi G, Giannattasio C, Seravalle G, Cattaneo BM, CI6roux J, Mancia G. Cardiogenie reflexes and left ventricular hypertrophy. Eur Heart J 1990;11 Suppl G:95-9.
19. Tanigawa (3, Jorcho JA, Kass S, et al. A molecular basis for familial hypertrophic curdiomyopathy: an alpha/beta cardiac myosin heavy chain hybrid eerie. Cell 1990;62:991-8.
20. Geisteffer-Lowrcnce AA, Kass S, Tanigawa G, et al. A molecular basis for familial hypertrophic cardiomyopathy: a beta cardiac myosin heavy chain misscnse mutation. CeU 1990;62:999-1006.
21. Sanderson JE, Traill TA, St John Sutton MG, Brown DJ, Gibson DG, Goodwin JE Left ventricular relaxation and filling in hypertrophic cardiom- yopathy: an echocardiographic study. Br Heart J 1978;40:596-601.
22. McKenna WJ, Deanfield J, Faruqui A, England D, Oakley C, Goodwin J. Prognosis in hypertrophic cardiomyopathy: role of age and clinical, electro- cardiographic and hemodynamie features. Am J Cardiol 1981;47:532-8.
23. Wynne J, Braunwald E. The cardiomyopathy and myocarditides. In: Braun. ward E editor. Heart Disease. A Text Book of Cardiovascular Medicine. 3rd ed. Philadelphia: Saunders, 1988:1410-69.
24. Counihan PJ, Lii Fei, Bashir Y, Farrell TG, Ha~ood GA, McKenna WJ. Assessment of heart rate variability in hypertrophic cardiomyopathy. Asso- ciation with clinical and prognostic features. Circulation 1993;88:1682-90.
25. McKenna WJ, Oakley CM, Krikler DM, Goodwin JF. Improved survival with amiodarone in patients with hypertrophic cardiomyopathy and ventric- ular tachycardia. Br Heart J 1985;53:412-6.
26. Zuanetti G, Latini R, Neilson JM, Schwartz PJ, Ewing DJ. Heart rate variability in patients with ventricular arrh.vthmias: effects of antiarrhythmic drugs. J Am Coil Cardiol 1991;17:604-12.
27. Maron BJ, Fananapazir L. Sudden cardiac death in hypertrophic cardio- myopathy. Circulation 1992;85 Suppl I:1-57-63.
28. Frenneaux MP, Counihan PJ, Caforio AL Chikamori T, McKenna WJ. Abnormal blood pressure response to during exercise in hypertrophic eardiomyopathy. Circulation 1990;82:1995-2002.
29. Kawano S, lida K, lwasaki Y, Tabei F, El Sersi M, Sugishita Y. Impaired peripheral vascular response to a-adrenergic stimulation in patients with hypertrophic cardiomyopathy [abstract]. Circulation 1993;88(4 Pt 2):I-553.
30. Lii Fei, Anderson MH, Starters D J, Mahk M, Carom AJ. Effects of passive tilt and submaximal exercise on spectral heart rate variability in ventricular fibrillation patients without significant structural kcart disease. Am Heart J 1995;129:285-90.
31. Lii Fei, Keeling PJ, Gill JS, et al. Heart rate variability and its relation to ventricular arrhythmias in congestive heart failure. Br Heart J 1994;71: 322-8.
32. Floras JS. Clinical aspects of sympathetic activation and parasympathetic withdrawal in heart failure. J Am Coil Cardiol 1993;22:72A-84A,
33. Colucci WS, Ribeiro JP, Rocco MB, et al. Impaired chronotropic response to exercise in patients with congestive heart failure. Role of postsynaptic 18-adrene-gic desensitization. Circulation 1989;80:314-23.
34. Adamop,:~h~s ~ Piepoli M, Qiang FX, et al. Effects of pulsed ~stimulant ther~gy on /~-adrcnoceptors and chronotrupic responsiveness in chronic heat~ failure. Lancet 1995;345:344-9.
35. Lii Fei, Starters DJ, Anderson MH, Malik M, Carat,: AJ. Relationship of short- and long-term measurements of heart rate variability in patients at risk of sudden cardiac death. PACE 1994;17:2194-200.