Primary hypertrophic osteoarthropathy
7
Primary Hypertrophic Osteoarthropathy By Manuel Martinez-Lavin, Carlos Pineda, Tirso Valdez, Juan-Carlos Cajigas, Michael Weisman, Niklaus Gerber, and Daniel Steigler S INCE THE ORIGINAL description of the syndrome almost a century ago, hypertro- phic osteoarthropathy (HOA) has been consid- ered an ominous sign, the herald of a severe underlying illness. Bamberger’ and Marie’ asso- ciated HOA with chronic infectious lung condi- tions. However, despite the advances in medical therapy during the first half of this century, including the discovery of antibiotics and the decreased incidence of infectious illnesses in developed countries, HOA did not disappear. Presently, HOA is often a paraneoplastic syn- drome, most commonly a sign of lung cancer. During the past 8 years we had the opportu- nity to study seven patients with longstanding HOA unassociated with any systemic disease. We observed a totally different articular picture in these cases compared with other chronic rheu- matic syndromes. We also noted the confusion that exists in the literature regarding nomencla- ture, clinical features, and diagnostic criteria for primary HOA. Thus, the objective of the present investigation of seven cases and literature review is to define the outstanding clinical characteristics of HOA in its primary or idiopathic form and, on this basis, to propose nomenclature and diagnostic criteria for this entity. CASE REPORTS Patient No. I A 17-year-old man was referred for evaluation of digital clubbing. This deformity was noted for the first time at age 10. Several months later the patient had the insidious onset of aching pain along the tibia1 shafts. He also noticed bony enlargement of the wrists and ankles. He denied symptoms that would suggest chest or abdominal illness. The patient’s family history includes a brother with digital clubbing. On physical examination skin was oily and wet, especially throughout the hands. No coarse facial features or gyneco- From the Institute National de Cardiologia Ignacio Chbvez, Mexico; the University of California, San Diego; and Universittitsklinik Inselspital. Bern, Switzerland. Address reprint requests to Manuel Martinez-Lavin. MD, Chief Rheumafology Service. Institute Nacionaf de Cardio- logia, Juan Badiano # I, 14080 Mexico D. F. Mexico. 0 I988 by Grune & Stratton, Inc. 0049-O I72/88/1703-0003$5.00/O mastia were detected. There was drumstick deformity of all 20 digits with a clubbing index of I. 17 (measured as the ratio of the circumference of the fifth left finger at the base of the nail over the perimeter of the same finger at the distal interphalangeal joint) being the normal value .I I .I There was bony enlargement of the wrists, knees, and ankles. and synovial effusion was detected in both knees. The range of motion was decreased by ten degrees in the wrists and knees. Examination of the chest and abdomen was unremarkable. Laboratory examination including complete blood count. sedimentation rate, SMA-I 2. urinalysis, rheumatoid factor, and antinuclear antibodies were negative or normal. Serum growth hormone levels performed during a glucose tolerance teqt were normal. Electrocardiogram and chest x-rays were normal. Radiographic bone survey showed multilayered type of periostitis involving all appendicular bones. Arthrocentesis of the right knee yielded a thick viscous fluid with 200 leukocytes/ml. Biopsy of the synovial membrane of the same joint showed no evidence of inflammatory cell infiltrate. The patient was given indomethacin 25 mg three times a day and propranolol 20 mg three times a day; with these measures the bone pain and the hyperhydrosis improved. We have followed the patient for 8 years and no illnesses have developed. Repeated skeletal radiographs demonstrated mild pro- gression of the extent of periostitis. Patient No. _? The mother of this l2-year-old boy noted digital clubbing since birth and enlargement of the knees and ankles since the age of I. The child complained of chronic aching pain along the tibia] shafts; otherwise he was healthy. Physical examina- tion demonstrated a clubbing index of I .23. There was bony enlargement of the knees and ankles without evidence of synovial effusion. .Ioint range of motion was normal. No skin abnormalities were detected. All laboratory studies were normal. Radiographic bone survey showed a monolayer type of periostitis in both ulnae. The patient was administered naproxen 2.50 mg twice daily with symptomatic improve- ment. We have followed this patient for 5 years and his clinical condition remains stable. Patient No. 3 This &year-old boy has similar history to his brother (patient no. 2) with clubbing since birth and bony enlarge- ment of knees and ankles. Physical examination was normal except for the skeletal abnormalities. Bone radiographs dem- onstrated a multilayered type of periosteal new bone forma- tion in both ulnae, metacarpals, and metatarsals. Treatment with naproxen yielded good symptomatic results. Patient No. 4 A 42.year-old man was referred for evaluation of asymp- tomatic digital clubbing discovered during a physical exami- nation. He denied a history of bone or joint pain or any change in the skin. His family history was negative. On 156 Seminars in Arthritis and Rheumatrsm, Vol 17, No 3 (February), 1988: pp 156-162
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Primary hypertrophic osteoarthropathy

Primary Hypertrophic Osteoarthropathy
By Manuel Martinez-Lavin, Carlos Pineda, Tirso Valdez, Juan-Carlos Cajigas,
Michael Weisman, Niklaus Gerber, and Daniel Steigler
S INCE THE ORIGINAL description of the
syndrome almost a century ago, hypertro- phic osteoarthropathy (HOA) has been consid-
ered an ominous sign, the herald of a severe
underlying illness. Bamberger’ and Marie’ asso-
ciated HOA with chronic infectious lung condi-
tions. However, despite the advances in medical
therapy during the first half of this century, including the discovery of antibiotics and the
decreased incidence of infectious illnesses in
developed countries, HOA did not disappear. Presently, HOA is often a paraneoplastic syn- drome, most commonly a sign of lung cancer.
During the past 8 years we had the opportu- nity to study seven patients with longstanding HOA unassociated with any systemic disease.
We observed a totally different articular picture
in these cases compared with other chronic rheu-
matic syndromes. We also noted the confusion
that exists in the literature regarding nomencla- ture, clinical features, and diagnostic criteria for
primary HOA. Thus, the objective of the present investigation
of seven cases and literature review is to define the outstanding clinical characteristics of HOA in its primary or idiopathic form and, on this
basis, to propose nomenclature and diagnostic criteria for this entity.
CASE REPORTS
Patient No. I
A 17-year-old man was referred for evaluation of digital clubbing. This deformity was noted for the first time at age
10. Several months later the patient had the insidious onset of
aching pain along the tibia1 shafts. He also noticed bony
enlargement of the wrists and ankles. He denied symptoms
that would suggest chest or abdominal illness. The patient’s
family history includes a brother with digital clubbing. On
physical examination skin was oily and wet, especially
throughout the hands. No coarse facial features or gyneco-
From the Institute National de Cardiologia Ignacio Chbvez, Mexico; the University of California, San Diego; and Universittitsklinik Inselspital. Bern, Switzerland.
Address reprint requests to Manuel Martinez-Lavin. MD, Chief Rheumafology Service. Institute Nacionaf de Cardio- logia, Juan Badiano # I, 14080 Mexico D. F. Mexico.
0 I988 by Grune & Stratton, Inc. 0049-O I72/88/1703-0003$5.00/O
mastia were detected. There was drumstick deformity of all
20 digits with a clubbing index of I. 17 (measured as the ratio
of the circumference of the fifth left finger at the base of the
nail over the perimeter of the same finger at the distal
interphalangeal joint) being the normal value .I I .I There was bony enlargement of the wrists, knees, and ankles. and
synovial effusion was detected in both knees. The range of
motion was decreased by ten degrees in the wrists and knees.
Examination of the chest and abdomen was unremarkable.
Laboratory examination including complete blood count.
sedimentation rate, SMA-I 2. urinalysis, rheumatoid factor,
and antinuclear antibodies were negative or normal. Serum
growth hormone levels performed during a glucose tolerance
teqt were normal. Electrocardiogram and chest x-rays were
normal. Radiographic bone survey showed multilayered type
of periostitis involving all appendicular bones. Arthrocentesis
of the right knee yielded a thick viscous fluid with 200
leukocytes/ml. Biopsy of the synovial membrane of the same
joint showed no evidence of inflammatory cell infiltrate. The
patient was given indomethacin 25 mg three times a day and
propranolol 20 mg three times a day; with these measures the
bone pain and the hyperhydrosis improved. We have followed
the patient for 8 years and no illnesses have developed.
Repeated skeletal radiographs demonstrated mild pro-
gression of the extent of periostitis.
Patient No. _?
The mother of this l2-year-old boy noted digital clubbing
since birth and enlargement of the knees and ankles since the
age of I. The child complained of chronic aching pain along
the tibia] shafts; otherwise he was healthy. Physical examina-
tion demonstrated a clubbing index of I .23. There was bony
enlargement of the knees and ankles without evidence of
synovial effusion. .Ioint range of motion was normal. No skin
abnormalities were detected. All laboratory studies were
normal. Radiographic bone survey showed a monolayer type
of periostitis in both ulnae. The patient was administered
naproxen 2.50 mg twice daily with symptomatic improve-
ment. We have followed this patient for 5 years and his
clinical condition remains stable.
Patient No. 3
This &year-old boy has similar history to his brother
(patient no. 2) with clubbing since birth and bony enlarge-
ment of knees and ankles. Physical examination was normal
except for the skeletal abnormalities. Bone radiographs dem-
onstrated a multilayered type of periosteal new bone forma-
tion in both ulnae, metacarpals, and metatarsals. Treatment
with naproxen yielded good symptomatic results.
Patient No. 4
A 42.year-old man was referred for evaluation of asymp-
tomatic digital clubbing discovered during a physical exami- nation. He denied a history of bone or joint pain or any
change in the skin. His family history was negative. On
156 Seminars in Arthritis and Rheumatrsm, Vol 17, No 3 (February), 1988: pp 156-162

PRIMARY HYPERTROPHIC OSTEOARTHROPATHY 157
physical examination his clubbing index was 1.2 1 and there was hyperhydrosis of the palms and soles. Joint examination was normal. Comprehensive clinical and laboratory studies failed to reveal any systemic illness. Skeletal radiographs showed an irregular type of periostitis involving femorae, tibias, and tibulae. He has been observed for 3 years without appreciable change. No treatment has been prescribed.
Patient No. 5
This 34-year-old man first noted digital clubbing at the age of 16. Later he suffered from progressive aching pain in the lower extremities accompanied by painful swelling of his knees and ankles. He also noticed progressive skin hypertro- phy more prominent in the hands and face with hyperhydro- sis. His family history was negative. On physical examination his clubbing index was 1.31. His hands were broad, fleshy, and wet. He had coarse facial features and cutis verticis gyrata; the legs displayed cylindrical swelling resembling “elephant feet.” No gynecomastia was detected. Joint exami- nation failed to reveal evidence of inflammation. Range of motion of the wrists, knees, and ankles was decreased; the rest of the physical examination was unremarkable. Radiographic bone survey disclosed an irregular type of periostitis involving all tubular bones (Fig 1). The patient was administered
indomethacin and propranolol with symptomatic improve- ment of the skeletal pain and hyperhydrosis.
Patient No. 6
This 20-year-old man was referred for evaluation of recently discovered digital clubbing. At age 16 he first noticed deformity in the tips of his fingers. He was otherwise asymptomatic. Clubbing was present on physical examina- tion. Joint examination was normal. He had oily wet skin without hypertrophic changes. Chest and abdominal exami- nations were negative. Growth hormone determination was normal. Radiographic bone survey disclosed an irregular type of periostitis.
Patient No. 7
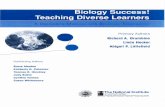
This 38-year-old man was seen by the dermatology service because of prominent and generalized skin hypertrophy that began at age 16. Findings were more evident in the head, with deep furrowed skin and hypertrophy of the eyelids that obstructed his vision (Fig 2). Seborrhea was evident. The patient had clubbing of his 20 digits and effusions were present in both knees. Radiographic studies demonstrated a widespread irregular type of periostitis. The patient was lost to follow-up.
SUMMARY OF THE CASE REPORTS
Our seven patients were all Mexican mestizo men except one (patient no. 6) who had an immediate Spanish ancestry. Three of the seven had a family history of similar disorder. Our cases displayed a wide spectrum of skeletal and skin abnormalities. From the articular point of
Fig 1. Patient no. 6. Radiograph of the right ankle showing advanced irregular periosteal proliferation with ossification of the inter-osseous membrane (arrow).
Fig 2. Patient no. 7. Severe hypertrophic skin changes with blepharoptosis end cerebroid appearance of the fore- head.

158 MARTiNEZ-LAWN ET AL
view, patients no. 4 and 6 were asymptomatic
whereas in patients no. 1, 2, 3, and 5, pain required treatment. These four patients had a
symptomatic response to nonsteroidal antiin-
flammatory agents. The cutaneous changes also
showed great variability from glandular dysfunc-
tion manifested as hyperhydrosis, seborrhea, and acne, to hypertrophic skin changes manifested by
coarse facial features. In two instances (patients no. 5 and 7), this abnormality reached the extreme of cutis verticis gyrata, represented in
patient no. 7 as the most advanced changes that we have observed with report cases (Fig 2).
Propranolol provided symptomatic improvement
for the hyperhydrosis. We have followed five patients for a mean period of 4.6 years. There
was no indication that the treatment altered the natural course of their illness. Discrete pro-
gression of the periosteal apposition in some patients has been noted. The arthropathy was
located mostly in the knees and ankles. Patients complained of achiness that involved both joints and adjacent bone. The most impressive finding on physical examination was the hard periarticu- lar bony enlargement that mildly diminished the
range of motion of the joints. There was no thickening of the synovial capsule. Joint effu-
sions were present in three of seven patients; two
on physical examination and one by history.
REVIEW OF THE LITERATURE
Methods
The MEDLINE data bank was used to iden- tify cases classified as pachydermoperiostosis,
Table 1. Outstanding Clinical Features of 125 Patients
With Primary Hypertrophic Osteoarthropathy Described in
the Literatures
Finding Percentage
Man
Positive family history
Digital clubbing
Radiographic periostitis
Synovial effusion
Skin involvement
Hypertrophic skin changes
Coarse facial features
Cutis verticis gyrata
“Elephant feet”
Hyperhydrosis
Seborrhea
Acne
89
38
89
97
41
73
61
24
24
36
33
13
Fig 3. Age of onset of hypertrophic osteoarthropathy.
primary HOA. familial HOA. or idiopathic HOA and that were published in the English.
French, or German literatures. The bibliography
of each article was reviewed, searching for addi-
tional cases not included in MEDLINE. A total of 125 cases of primary HOA were collected.J~9”
The salient clinical findings are summarized in Table 1.
The male/female ratio was 8.9 to 1 and the age of onset of the illness was defined in 67% of
the patients. In some instances, as in our case no. 2, patients were unable to relate the time of onset. When the onset could be ascertained, there was a bimodal distribution with one peak during
the first year of life and the other at age 15 (Fig
3). Familial clustering of the syndrome is evident by 38% of the cases reporting a relative with
similar abnormalities. Digital clubbing was not
reported in 14 of the 125 cases (1 I%).“. 18.30,34.42,49.54,61.64.67.72,73.79,82 In eight of the cases, ‘“~30*34~42~49~6’~64~72 the absence of clubbing was
explicitly stated. Nevertheless, these patients dis- played periostitis as well as typical cutaneous changes. A joint effusion was described in 41% of patients with predilection for knees, ankles, and
wrists. All, except for four patients,9,34*65 had radiographic signs of periostitis. Tibiae and fibu- lae were the bones most frequently affected.
Synovial fluid examination in nine in- Stances14.16.29.46.48.53.55.78.83 was noninllammatory except for one (hemarthrosis).29 Characteristi- cally, the fluids were thick and viscous with low WBC counts. The histology of the synovium in eight patients 14,16.25,33,39,46.48.53 showed mild cell_
lining hyperplasia,25.33.39,48 thickening of the small blood vessels with fibrosis,25,48 or mild nonspecific inflammatory cell infiltrate.‘4*‘6.48.53
Most patients with primary HOA had skin involvement (Table 1). The most frequent abnor-

PRIMARY HYPERTROPHIC OSTEOARTHROPATHY 159
mality was coarse facial features, an alteration commonly associated with blepharoptosis.
No specific abnormality was found on labora- tory examination. Parameters that measure inflammation were absent in almost all instances, as were studies of immune dysfunction such as rheumatoid factor, anti-nuclear antibodies or serum levels of immunoglobulins. Growth hor- mone was elevated in one6’ of the five patients meaSUred.6,45,47,61.89
There is little information in the literature regarding treatment. The therapy most widely used was nonsteroidal antiinflammatory drugs; radiation therapy was favored in the older arti- cles. 10,‘1*85 There was no claim of treatment alter- ing the course of the illness.
A variety of associated abnormalities have been described such as cranial suture de- fects 1,4*5~1g.20,64*78 female escucheon,12s54*64 bone , marrow failure, 54 hypertrophic gastropathy,45*57 and chromosomal abnormalities.71 In the fol- low-up reports, it appeared that the disease had a self-limited course with an “active” period dur- ing childhood and adolescence, adults were asymptomatic.
DISCUSSION
HOA not associated with an internal illness was recognized even before the classical descrip- tion of pulmonary HOA by Bamberger’ and Marie.2 In fact, the only patient with HOA personally seen by Marie and erroneously diag- nosed by him as “pulmonary,” was a patient with primary HOA admitted to the hospital with a minor respiratory ailment.87 Although described earlier, credit for the recognition of the primary syndrome has been attributed to Touraine et al who masterfully described the clinical features of the illness.6g Subsequently, many additional names have been given to this condition,87 each emphasizing different clinical features, adding confusion to the subject. We believe that primary HOA is the most appropriate term; it emphasizes the lack of associated illness and also encom- passes patients without hypertrophic skin changes and without family history.
Primary HOA contains a hereditary predispo- sition and it is clearly sex-linked, over one-third of the reported cases have a relative with similar illness. It is not presently possible to ascertain the type of inheritance. The onset of the illness has a
bimodal distribution, with a second peak that coincides with the rapid growth period of puberty (Fig 3) and the appearance of secondary sexual characteristics. Clinically, the disease seems to have a self-limited course ending in adulthood.
The main clinical features of primary HOA are in the skeleton and the skin. The most conspicuous, but not uniform, abnormality was digital clubbing in 89% of cases. It appears that bona fide cases of primary HOA exist without clubbing. The periosteal proliferation of HOA display diverse patterns,g’ with a predilection for the lower extremities. Literature review confirms our impression that a minority of patients have synovial effusion; studies of the synovial fluid and synovial histology have not shown significant inflammatory cell-infiltration or exudation. These data suggest that HOA is not a primary synovial disease; it is suggested that synovial effusions are a contiguous sympathetic reaction to the neighboring periostitis, analogous to syno- vial effusions in juxtaarticular osteomyelitisg2 or bursitisy3
We propose diagnostic criteria for HOA to include the combined presence of digital club- bing and radiographic periostitis. In this review of 125 patients, including our seven patients, the sensitivity of these combined criteria is 86%. Specificity was not tested.
The cutaneous involvement of primary HOA could be divided into two expressions: (1) glan- dular abnormalities such as acne, hyperhydrosis, and seborrhea and (2) hypertrophy of the soft tissues such as clubbing, coarse facial features, elephant feet, ptosis of the lids, and cutis verticis gyrata.
There were no other clinical differences among the group of patients with or without hypertrophic skin changes, suggesting that HOA is a single disease entity with variable cutaneous expression. Cutis verticis gyrata represents the most advanced stage of hypertrophy, histological examination reveals only excessive skin or glan- dular hypertrophy.4g,6g*87 The cutaneous changes are not limited to the primary form of the syndrome, as they have been reported in HOA associated to lung malignancies.g4 When con- fronting a patient with clinical features of HOA, it still remains of utmost importance to rule out any associated illness before the consideration of a primary case. However, the long-standing pres-

160
ence of clubbing and a positive family history suggest the primary form of the syndrome. The
clinical features of primary HOA suggest that a genetically determined hormonal factor related
to maleness plays a role in its pathogenesis. The recent discovery of other growth-inducing factors
different from growth hormone have opened an interesting line of investigation.95
SUMMARY
We describe seven patients with primary
HOA and review 125 cases reported in the English, French, and German literature.
The salient clinical features of primary HOA
are: a bimodal distribution of disease onset with one peak during the first year of life and the other at age 15, a male predominance (nine to
one), uncommon benign joint effusion, and a
MARTiNEZ-LAViN ET AL
variety of skin abnormalities resulting from cuta-
neous hypertrophy or glandular dysfunction.
We concluded that HOA is not a synovial disease. It is suggested that synovial effusions.
when present, are perhaps a sympathetic reac- tion to the neighboring periostitis. Proposed diag- nostic criteria for HOA, including digital club- bing and radiographic periostitis, appear 86%,
sensitive.
The clinical features, age of onset, and sex distribution suggest that a genetically controlled
growth promoting factor, different from growth
hormone, plays a role in the pathogenesis of this
syndrome.
ACKNOWLEDGMENT
We wish to thank Dr Clara Shumski, Dr Maria dcl
Carmen Moreno, and Dr Jaime Sabanes for allowing us to
study and to describe their patients.
REFERENCES
1. Bamberger E: Ueber knochenveranderungen bei chron-
ischen lungenund herzkrankheiten. Z Klin Med 18: 193-217.
1891
2. Marie P: De l’osteoarthropathie hypertrophiante pneu-
mique. Rev Med (Paris) IO:]-36. 1890
3. Castillejos G, Martinez-Lavin M: Discrepancy between
arterial ferritin levels and the presence of digital clubbing.
Clin Rheumatol (in press) 4. Adolph W, Relke W, Endert G: Kasuistischer beitrag
man krankheitshid der idiopathischen hypetrophischen
osteoarthropathie. Z Gesamte Inn Med 32: 17 I- 174, 1977
5. Bartolozzi G, Bernini G, Maggini M: Hypertrophic
osteoarthropathy without pachydermia. Am J Dis Child
129:849-851, 1975
6. Bhate D, Pizarro A, Greenfield G: Idiopathic hyper-
trophic-Osteoarthropathy without pachydermia. Radiology
129:379-381, 1978
7. Binder E, Bonse G: Ueber familiare haunt und knoch-
enveriesung. Arch Dermatol Forsch 196: 123-l 26, 1953
8. Brugsh H: Acropachydermia with pachyperiostitis.
Arch Intern Med 68:687-700, 1941
9. Buchman D, Hrowat E: Idiopathic clubbing and hyper-
trophic osteoarthropathy. Arch Intern Med 97:355-358,
1956
10. Bureau Y, Pineau J, Barritre A: Un cas de pachyder-
moperiostose. Bull Sot Franc Derm Syph 56: 129-I 33, 1949
Il. Bureau Y, Barriere H, Thomas M: Hippocratisme
digital congenital avec hyperkeratose palmo-plantaire et
troubles osseux. Ann Dermatol Syphiligr 86:6 1 l-622, 1959 12. Camp J, Scanlin R: Chronic idiopathic hypertrophic
osteoarthropathy. Radiology 50:581-593, 1948 13. Capetanakis J, Merikas G: Uber einer fall van pachy-
dermoperiostose. Hautarzt 16:498-503, 1965 14. Curranino G, Tierney RC, Giesel RG, et al: Familial
idiopathic osteoarthropathy. AJR 85:633-644, 1961 15. Carruthers LB: Idiopathic hypertrophic osteoar-
thropathy familial in type. J Christian Med Assoc IX: l-3. I943
16. Caughey JE: Familial hypertrophic osteodrthropdthy.
N Z Med J 65:528-530, 1966
17 Cohen H. Tibi R, Darmouni E: Une observation de
pchydermoperiostose. Tunis Med 38:7 15-7 17. 1960
IX. Colintineanu L, Trifur R, Moisin D: Sur un cas de
pachydermoperiostose. Bull Sac Franc Derm Syph 76:766-
768. 1969
19. Cremin BJ: Familial idiopathic osteoarthropathy of
children. Br J Radial 43:568-570, 1970
20. Chamberlain D, Whitaker J, Silverman I’: Idiopathic
osteoarthropathy and cranial defects in children. .AJR
193:40X-41 5. 1965
2 I. Choudrury R, Samanta D, Dutta SK, et al: A case ol
pachydermoperiostosis. J Indian Med Assoc 63:155- 157.
1974
22. Diard I’, Caille .I, Gretet P. et al: Pachydermoperros-
tose. .I Radial Electra1 Med Nucl 50:763-766, I969
23. Dijan E: Trois observations fortuites de pachydermo-
periostose. Rev Rhum Mal Osteoartic 43:528-532. 1976
24. DuPont A. Vandaela R: Pachydermie avec pa-
chyperiostose des extremites. Arch Belg Dermatol 13:&h-
268, 1957
25. Fam A, Chin-Sang H, Ramsay C: Pachydermoperios-
tosis scintigraphic, thermographic, plethysmographic and
capillaroscopic observations. Ann Rheum Dis 42:9X- 102.
1983
26. Findlay GH, Ossthuizen MB: Pachydermoperiostosia.
S Afr Med J 25:747-752, 1951
27. Franscheschetti A, Gilbert A. Klein 0. et al: Ln
nouveau cas de pachydermie plicaturee avec pachyperiostose
das extremities. Schweiz Med Wochenschr 80: I301 - 1306,
I950
28. Gugeon J, Labram C: Hippocratisme digital idiopath-

PRIMARY HYPERTROPHIC OSTEOARTHROPATHY 161
ique avec periostose engainante. Rev Rhum Ma1 Osteoartic 36:333-338,1969
29. Guyer PB, Brunton FJ, Wren MW: Pachydermo- periostosis with acre-osteolysis. J Bone Joint Surg 60:219- 223,1978
30. Hamza Z: Pachydermoperiostosis: A propos od 2 cases. Tunis Med 55213-217, 1977
31. Hattner R: Skeletal scintigraphy in pachydermo- periostosis. Eur J Nucl Med 6:477-479, 198 1
32. Hecht A: Idiopathic hypertrophic osteoarthropathy. NY State J Med 653038-3044, 1965
33. Hedayati H, Barmada R, Skosey J: Acrolysis in pachydermoperiostosis. Arch Intern Med 140:1087-1088, 1980
34. Herman M, Massaro D, Katz S, et al: Pachydermo- periostosis-clinical spectrum. Arch Intern Med 116:918-923, 1965
35. Herbert D, Fressel J: Idiopathic hypertrophic osteoar- thropathy (Pachydermoperiostosis). West J Med 134:354- 357,198l
36. Hochmuth W, Juchems R, Schubert E: Touraine- Solente-Gole Syndrom (Pachydermoperiostose). Med Klin 70:146-150.1975
37. Huet A, Degos M: Medical thesis no. 966. FacultC de M&lecine de Paris, 1965
38. Huriez C, Francois P, Agache P: Pachydermoperios- tose. Ann Dermatol Syph 89:372-387, 1962
39. Joseph B, Chacko V: Acre-osteolysis associated with hypertrophic pulmonary osteoarthropathy and pachydermo- periostosis. Radiology 154343-344, 1985
40. Kaffarnik H, Husmann F, Longin F, et al: Die pachy- dermoperiostose. Dtsch Med Wochenschr 91:1722-1724, 1966
41. Keats T, Bagnall W: Chronic idiopathic osteoar- thropathy. Radiology 62:841-844, 1954
42. Kempf F, Berthier G, Gillet B, et al: La pachydermo- periostose-etude radioclinique. J Radio1 Electrol Med Nucl 49:858-860, 1968
43. Kerber R, Vogl A: Pachydermoperiostosis. Arch Intern Med 132:245-248, 1973
44. Kozlowski K, Posen S: Idiopathic hypertrophic osteoarthropathy. Australas Radio1 27:291-294, 1983
45. Lam S, Hui W, Ho J, et al: Pachydermoperiostosis, hypertrophic gastropathy and peptic ulcer. Gastroenterology 84:834-839,1983
46. Lauter S, Vasey F, Huttner I, et al: Pachydermo- periostosis: Studies on the synovium. J Rheumatol 5:85-89, 1978
47. Lazarus JH, Galloway JK: Pachydermoperiostosis. AJR 118:308-313, 1973
48. Lehman M, Guariglia E, Tannin A: Idiopathic hyper- trophic osteoarthropathy. Bull Hosp Jt Dis Orthop Inst 34~56-67, 1963
49. Leinwand I, Duryee W: Chronic hypertrophy of the skin and long bones: An osteo-dermopathic syndrome. Ann Intern Med 19:1018-1028, 1943
50. LeLourd R, Bandet E, Badiola P: Pachydermie plica- turee-hippocratisme congenital; variante de syndrome de Touraine. J Med Bordeaux 141:405-409, 1964
5 1. Lievre JA, Breton A: A propos Dun cas de pachyder-
mie picaturee avec pachyperiostose des extremitb. Rev Rhum Ma1 Osteoartic 46:149-155, 1949
52. Lubach D, Freyschmidt J, Bolten D: Pachydermo- periostose. Klinische und rontgenologische differential diag- nose. Z Hautkr 56:175-186,198l
53. Mueller M, Trevarthen D: Pachydermoperiostosis: Arthropathy aggravated by episodic alcohol abuse. J Rheu- matol8:862-863, 1981
54. Metz E, Dowel1 A: Bone marrow failure in hypertro- phic osteoarthropathy. Arch Intern Med 116:759-764, 1965
55. Salih SY, Halim A: Idiopathic hypertrophic osteoar- thropathy with severe recurrent arthritis in an African and a review of the literature. East Afr Med J 55:31-35, 1978
56. Salfed K, Spalckhaver I: Zur Kenntnis der pachyder- moperiostosis. Dermatol Monatsschr 152:497-5 11, 1966
57. Samii M: Syndrome de Touraine-Solente-Gole on pachydermoperiostose avec hypertrophic des extremities. Bull Sot Franc Dermatol Syph 78:262-263, 1971
58. Schneider H: Zur Klinik und klassifikation der pachy- dermoperiostose. Dermatol Monatsschr 160:818-824, 1974
59. Schilling F, Krich B, Kuch H: Hyperostosis generalis- ata und cutis verticis gyrata. Dtsch Arch Klin Med 207:456- 491,196l
60. Schneider I, Szabo L: Pachydermoperiostose. Hau- tarzt 33:221-223, 1982
6 1. Schubert E, Vetter H, Juchems R: Pachydermoperios- tose. Munch Med Wochenschr 112:229-235,197O
62. Schwartzman S, Spiera H: Idiopathic hypertrophic osteoarthropathy without pachydermia and with acrolysis. Mt Sinai J Med (NY) 49:335-337.1982
63. Seze S, Jurmand S: Pachydermoperiostose. Rev Med Hop (Paris) 66:860-864, 1950
64. Schawarby K, Salah B: Pachydermoperiostosis. Br Med J 1:763-766, 1962
65. Sirinavin C, Buist N, Mokkhaves P: Digital clubbing hyperhydrosis, acre-osteolysis and osteoporosis. A case resembling pachydermoperiostosis. Clin Genet 22:82-89, 1982
66. Susmano A, Shah P, Krompotic E, et al: Normal sex-chromosome complement in a cases of familial osteoar- thropathy. Lancet 2:131-133, 1967
67. Thierree R, Raguin M: Un cas de pachydermoperios- tose. J Radio1 Electrol Med Nucl42:682-683, 1961
68. Tornblom N, Malers E, Wallenius G: Gsteodermato- pathia hypertrophicans. Acta Med Stand 164:325-339, 1959
69. Touraine A, Solente G, Gole L: Un syndrome osteo- dermopathique: La pachydermie plicaturee avec pachyper- iostose des extremites. Presse Med 43:1820-1824, 1935
70. Tourniaire J, Pryon P: Pachydermoperiostose sans signes cutanes. Lyon Med 217:493-504, 1967
7 1. Tzoneva-Maneva MT: Chromosomal abnormalities in idiopathic osteoarthropathy. Lancet l:lOOO-1002, 1966
72. Marril F: Sur la position nosologique de la pachyder- moperiostose. Presse Med 65:2789-2791, 1957
73. Moncourier B, Fontayne F, Rozay D: A propos de deux cas de pachydermo-periostose. J Radio1 Electrol Med Nucl40:310-315,1959
74. Nagant C, Huaux J: Pachydermoperiostose. Arch Belg Dermatol Syph 23:121-135, 1967

162 MARTINEZ-LAWN ET AL
75. Neiman H, Compels B, Martel W: Pachydermo-
periostosis with bone marrow failure and gross extramedul-
lary hematopoiesis. Radiology 110:553-554, 1974
76. Perrot J, Degos M: These pour le Doctorat en Mbde-
tine N 780. Facultt de Mtdecine de Paris, 1953
77. Purohit M, Saxena S, Garg A: Idiopathic hypertro-
phic osteoarthropathy. Indian J Pediatr 47: l65- 167, 1980
78. Reginato A, Schiapachasse V, Guerrero R: Familial
idiopathic hypertrophic osteoarthropathy and cranial suture
defects in children. Skeletal Radio] 8: 105- 109, 1982
79. Rimoin D: Pachydermoperiostosis (idiopathic club-
bing and periostosis). N Engl J Med 272:923-931. 1965
80. Rintelen F: Uber elephantiastische lidverandeungen
zugleichein zar kenntuis des osteodermopathischen syn-
droms: Touraine Solente Gole. Zeitschr F Augenheilkunde
92:1-15, 1937
81. Robert D, Dubois R: Pachydermoperiostose. J Radio]
Electrol Med Nucl 53:759-760, I972
82. Rollier R, Sebti A, Rallier M, et al: A propos de trois
cas de pachydermoperiostose. J Med Lyon 53:1148-l 162,
1972
83. Roy JN: Hypertrophy of the palpebral tarsus, the
facial integument and the extremities of the limbs associated
with widespread osteoperiostosis: A new syndrome. Can Med
Assoc J 34:615-622, 1936
84. Roy JN, Jutras A: Aspects radiogiques dune osteo-
periostose presque generalise. J Radio] Electrol Med Nucl
221539-549, 1938
85. Rutt A: Die hyperostosis generalista mit pachydermie.
Arch Orthop Unfallchir 49:497-506, 1958
86. Vague J: Un nouveau cas de pachydermoperiostose.
Presse Med 56:682-683. 1948
87. Vogl A, Goldfischer S: Pachydermoperiostosis. Am .I
Med 33:166-185. 1962
88. Waghemacker R. Bertin .I: A propos d’un cas de
pachydermoperiostose atypique. J Radio] Electrl Med Nucl
40:273-274. 1959
89. Yu YL, Turck WP: Pachydermoperiostosts (idio-
pathic hypertrophic osteoarthropathy). Postgrad Med J
57:521-524. 1981
90. Bureau Y, Horeau J, Barriere H, et al: Pachydermo-
periostose. Bull Sot Franc Dermatol Syph 72:407-4 I I, I965
9 I. Pineda C, Martinez-Lavin M, Goobar .I, et al: Perios-
titis in hypertrophic osteoarthropathy. AJR 148:773-778.
1987
92. Platt PN, Grithths ID: Pyogenic osteomyelitis pre-
senting as an acute sterile arthropathy. Ann Rheum Dis
42:607-609, 1984
93. Strickland R. Raskin R, Welton R: Sympathetic
synovial effusion associated with septic arthritis and bursitis.
Arthritis Rheum 28:941-943. I985
94. Case Records of the Massachusetts General Hospttal.
Case 38- 1978. N Engl J Med 299:708-7 14, I978
95. Martinez-Lavin M: Digital clubbing and hypertrophic
osteoarthropathy: A unifying hypothesis. .I Rheumatol 14:6-
8, 1987