Multi-Modal Exercise Training and Protein-Pacing Enhances ...
Upload
independentCategory
view
0download
0
Single Pass Lead VDD Pacing in Childrenand Adolescents
SHIMON ROSENHECK,* AMIR ELAMI,** SHLOMO AMIKAM/SHIMSHON ERDMAN,'̂ ^ and I. ELI OVSYSHCHER*"̂
Erom the *GardioIogy Unit and the Department of Medicine, Hadassah University HospitalMount Scopus, **Department of Thoracic Surgery, Hadassah University Hospital, Ein Kerem,Jerusalem, """Rambam Hospital, Haifa, ^^Rabin Medical Genter (Belinson), Petach Tikva,and the '^Division of Gardiology, Soroka Medical Genter. Eaculty of Health Sciences,Ben-Gurion University of the Nege, Beer Sheva, Israel
ROSENHECK, S., ET AL.: Single Pass Lead VDD Pacing in Children and Adolescents. Implantation of per-manent pacemakers in children and adolescents is possible but usually is limited to single chamber gen-erators. The natural growth of these patients may require physiological pacing, but until recently two leadswere required for this type of pacing. The single pass lead VDD pacing mode makes posible physiologicalpacing by using only one lead, for both atrial sensing and ventricular sensing and pacing. The feasibilityof VDD pacing using endocardial lead was evaluated in 16 children and adolescents with congenital orpostsurgical atrioventricular block. Their mean age was 7.9 ± 4.9 years (range 1-16 years) and the small-est patient's weight was 8.2 kg. In all the patients, a single pass pacing lead with atrial sensing rings andbipolar ventricular pacing and sensing capability was implanted through the left or right subclavian vein.The pacemaker generator was implanted in a rectopectoral position. The mean atrial electrogram duringthe implantation was 4.2 ± 2.1 mV and 2.6 ± 1.9 mV after a mean of 1 week. The ventricular pacingthreshold was 0.5 ± 0.2 V; the ventricular pacing impedance was 560 ± 95 Q; and the ventricular elec-trogram amplitude was 9.9 ± 2.1 mV. This is a first report to demonstrate the feasibility of atrial syn-chronous ventricular endocardial pacing using a single pass lead in a relatively large group of childrenand adolescents. (PACE 1997; 20:1961-1966)
endocardial pacing, children, adolescents, dual chamber, VDD
IntroductionPermanent pacemaker implantation in chil-
dren was possihle for a long time using epicardialelectrodes.^"** Both chambers may be paced withepicardial electrodes, but rapid increase in thepacing threshold with these leads may be frequentand the failure rate is considerably higher than thefailure rate observed with the transvenous endo-cardial electrodes.^"^ The original concerns withthe endocardial approach in pediatric patientswere their small size, the small lumen of the ma-jor veins used for advancing the leads, the child's
Address for reprints: Shimon Rosenheck, M,D., CardiologyUnit, Hadassah Mount Scopus University Hospital, PO Box24035, Jerusalem 91240, Israel. Fax: 972-2-5823-515.
Received August 19, 1996; revision September 18, 1996; ac-cepted April 7, 1997.
growth, and the requirement for reserve lead'slength to compensate for the future enlarging ofthe heart and the thorax.^'^'^^ A certain percentageof the endocardial leads is exposed to failurecaused by technical reasons or hecause of aging.Additional leads will have to be implanted to re-place the failing leads. The number of leadsneeded hy children during their life may be highand there is a limited number of electrodes thatcan be abandoned in the right heart chambers.^^This limitation may be overcome by further devel-oping the lead extraction techniques.'''^'' Physio-logical pacing with preservation of the atrioven-tricular synchrony may be important in thepediatric patients to guarantee adequate cardiacoutput for their natural growth and development.Single lead VDD pacing has become a routine pro-cedure in adult patients with complete atrioven-tricular block and normal sinus node func-
PAGE, Vol. 20 August 1997, Parti 1961

ROSENHECK, ET AL.
-̂ *' The aim of this study was to evaluate thefeasibility of single lead transvenous VDD pacingsystem implantation in pediatric patients.
Table I.
Detailed Patients' Characteristics Inciuding Age, Sex,and Indication for Permanent Pacemaker Implantation
Methods
Study Group
A prospective registry was initiated in Israel toevaluate the long-term feasibility of single lead VDDpacing.̂ ^• '̂' This study consisted of sixteen patientswho were < 16-years-old at the time of initial im-plantation. The mean age of the children at the timeof implantation was 7.9 ± 4.9, with tbe smallest pa-tient 352 days old (8.2 kg) and the oldest patient 16-years-old, Twelve patients were <10-years-old.The implantations were performed in six hospitals;9 implantations in 1 hospital; 2 implantations in 2hospitals; and 1 implantation in each of the last 3hospitals. In patients 4, 8, and 10 (Table I) the en-docardial pacing system was implanted after earlyfailure of previously implanted epicardial systems(in patient 8 there were three attempts at epicardialleads implantation all failing after 2-6 months). Nopatient had clinically documented atrial arrhyth-mias or sinns node disfunction.
Implantation Method
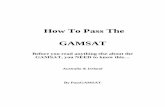
The implantation was performed under deepsedation with propophol and alfentanil or fen-tanil, except for the last three patients (Tablel). Us-ing the Seldinger technique, a guidewire was in-serted into the left or right subclavian vein and a10.5-Fr introdusor was placed around the wire.The introdusor was carefully inserted under fluo-roscopy guidance to avoid damage to the small ve-nous system. A bipolar ventricular pacing leadwith atrial sensing rings (model # 5032,Medtronic, Inc., Minneapolis, MN, USA) was ad-vanced to the right ventricular apex. A large curvewas created in the right atrium as the atrial ringswere positioned against the mid- or low right lat-eral wall (Fig. 1). The bipolar pacing lead was se-lected to allow a retropectoral implantation of thegenerator. The large curve was intended to pro-vide the reserve for the future growth of the heartand thorax and for proper atrial sensing signals.
When the ventricular pacing and sensingmeasurements and the atrial sensing were satis-factory, the generator was connected to the proxi-
Patient
123456789
10111213141516
Age
12244567899
1013151516
Sex
FFMFFFMMFMFM
Ll_
MFM
Indication
SurgicalAVN ablationSurgicalSurgicalCongenitalSurgicalCongenitalSurgicalSurgicalSurgicalCongenitalSurgicalCongenitalCongenitalCongenitalCongenital
Age in years; F = female; M = male: AVN-AV node; indicationfor implantation, surgical and congenital surgical induced orcongenital complete atrioventricular block.
mal end of the lead (model Thera VD 8948,Medtronic, Inc.). This pacemaker has a minimalatrial channel sensitivity of 0.18 mV. The atrialand ventricular sensing and the ventricular pacingproperties were evaluated witb a Pacing SystemAnalyzer (PSA model # 53llA, Medtronic, Inc.).
Except in the last three patients, the generatorwas implanted in the retropectoral space. The pec-toral muscle fibers were separated atraumaticallyand a pocket was created in the fat tissue behindthe muscle. The generator and the remaining prox-imal end of the lead was inserted into the pocketand closed with nonreabsorbable sutures. The sub-cutis and the skin were sutured with ahsorbablecontinuous sutures. Tbe patients were dischargedfrom the hospital after 1-7 days (the hospital staywas longer in the smaller children). The clinicalfollow-up was scheduled after 8-10 days, 1 month,3 months and then every 6 months. Dnring eachclinical follow-up in the small children (< 10years) a fluoroscopy picture of the heart was takenand compared with the previous pictures. Duringeach evaluation, the atrial sensing was measuredand the atrial electrogram was evalnated.
1962 August 1997, Parti FACE, Vol. 20

VDD IN PEDIATRIC PATIENTS
Figure 1. (Aj The position of the had in patient two 1 month after the implantation, in pos-teroantftrinr projection. A large curve in the right atrium before the tricuspid valve was created andthe tip is in the right ventricular apex. (B) Same patient as in (A), but in left lateral projection.
Results
Tbe pacing system was implanted in ail 16patients without complication and all have beenscheduled for lollow-up in their implanting cen-ters. Until the date of writing this article, no pace-maker bad to be revised. The detailed data fromthe implantation is summarized in Table II. Themean amplitude of the recorded atrial electrogramwas 4.2 ± 2.1 mV and the amplitude in tbe 12 pa-tients younger than 10-years-old was slightly, butnot significantly lower (3.7 ± 1.5 mV). The ven-tricular electrogram could be measured only ineight patients (patients 2, 6-11,14) because lack ofmeasurable escape rhythm was not reported in theother subjects. The mean ventricular amplitude inthese eight patients was 9.9 ± 2.1 mV. The ven-tricular pacing threshold was 0.5 ±0.2 V and inthe children from the younger group was 0.5 ± 0.3V. The pacing impedance was 560 ± 95 il.
The predischarge atrial amplitude was avail-able in eight children and are presented in Figure2. Usually the amplitude decreased, but was stillin the range of safe sensing. The mean predis-c:harge atrial electrogram amplitude was 2.6 ± 1.9mV.
The atrial electrogram amplitude recordedthrough the atrial channel dnring the first four fol-
low-up visits (up to 15 months), in 14 patients, arepresented in Figure 3. The minimal amplitudewas 2.5 times the minimal atrial sensing value of0.18 mV. The atrial sensing was present at least92% of the time.
Discussion
This multicenter study, involving six hospi-tals, demonstrates the feasibility of single leadVDD pacing system implantation in pediatric pa-tients. Although the veins bad a small caliber andthe lead has a relatively large size, there were noclinically evident complications and there were nosigns of vein obstruction. The measurements dur-ing the implantation in this population were simi-lar with the measurements in adult patients.^^'^^Although a decrease in the atrial electrograms' am-plitude prior to the hospital discharge and during15 months of follow-up was observed, the atrialsensing was not significantly affected.
Endocardial Pacing Leads Implantation inPediatric Patients
The stability of the original endocardial leadswas low and for this reason the use of epicardialpacing leads was preferred in adults and pediatricpatients.^ The epicardial lead could directly and
PACE, Vol. 20 August 1997, Part I 1963

ROSENHECK, ET AL.
Table II.
The Measured Atrial and Ventricular Pacing ParametersDuring the Implantation and Prior to the Hospital
Discharge
Patient
123456789
10111213141516
meanSD
AS
1.82.82.63.83.42.64.64.22.24.46.85.45.02.25.89.84.22.1
VS
5.0
9.411.47.0
13.410.015.4
5.09.94.9
TH
1.00.80.30.30.30.50.60.40.31.00.50.50.40.50.40.20.50.2
Impedance
417509500460498445560606519530628721662658720519560
95
PDAS
1.22.81.61.60.32.6
4.02.03.4
7.02.61.9
AS = atrial signal amplitude in mV during implantation; VS =ventricular signal amplitude in mV during the implantation; TH =ventricularpacingthresholdJnV; Impedance = ventricular pacingimpedance in i l ; PD AS = the amplitude of the atrial signal inmV measured through the pacemaker prior to the hospital dis-charge; SD = standard deviation.
actively be fixated on the epicardial surface of theheart. The original endocardial leads had no fixa-tion device and only the appropriate positioningin the right ventricular apex could guarantee itsrelative stahility. Usually the old leads had a thickdiameter. All these limitations made it almost im-possible to implant them in patients with smallhearts. However, the endocardial leads during thelast 20 years were significantly improved. ̂ ^ De-veloping active or passive fixation leads, reducingtheir size, and increasing their flexibility, the en-docardial implantation have hecome an acceptedmethod in small patients. The early failing ratewith the endocardial leads has become signifi-cantly lower than with epicardial leads, even inthe pediatric population."""
Although the endocardial implantation waslimited to children with a higher weight than10-15 kg,''-^- '̂̂ ^^ recently the safety of endocardial
leads in smaller children was also demon-strated.^^'^^ Noninvasive determination of thesubclavian or jugular vein's diameter was sug-gested before the implantation," however, no sig-nificant clinical complications were reported re-lated to occlusion of these veins even withoutthese noninvasive tests. An additional limitationrelated to the pectoral implantation of the genera-tor may be the anticipated skin erosion in theshoulder area. This limitation was practicallyeliminated by implanting the unit in a retropec-toral position.̂ ''•^•* The rectopectoral implantationalso resulted in less bulging and a more cosmeticappearance of the pacemaker site. Simultane-ously, with developing the endocardial implanta-tion in the pediatric population, the generatorswere technically improved and their size was re-duced to a volume around 10 cc and a weight be-tween 20-30 g. The new generators' thicknessdoes not exceed 7 mm. Retropectoral implantationof these small and sophisticated generators willnot cause any physical discomfort even in smallchildren.
The generator implanted in our patients has avolume of 12.1 cc. Most of the generators were im-planted retropectoraly, through the suhcalvianvein, which was approached by direct puncturewithout technical problems or complications. Al-though the patency of the venous route was notevaluated, no clinical signs of occlusion was ob-
pt3 pt4 pt5 pte pte po pi 10 pt i6
Abbreviatior pt-p»iienl
Figure 2. The atria! electrogram amplitude during theimplantation and during the predischarge test. The pre-discharge values were available only for eight patients(see Table IIj.
1964 August 1997, Part I PACE, Vol. 20

VDD IN PEDIATRIC PATIENTS
Figure 3. The atrial electrogram amplitude in 14 pa-tients during 15 month follow-up (implantation: 1month, 3 months, 9 months, and IS months) is pre-sented. The small decrease in the amplitude was notsignifcant and the minimal electrogram amplitude was2.5 times the minimal atrial sensing of 0.18 mV.
served in any of the patients. No skin erosion wasdeveloped by our patients. The pacing thresholdand the sensing of the endocardial electrogramswere in the limits observed in adult patients. Theatrial driven ventricular pacing was selected forthese pediatric patients as several recent studiesare suggesting superiority of this mode of pacingon the ventricular single chamber pacing.^^'^^Based on these studies, we hypothesized that thephysiological pacing may be important to guaran-tee the normal development of these children.
This hypothesis is still to be demonstrated in fu-ture studies. The follow-up of our patients demon-strates the long-term stability of the single passVDD pacing in the pediatric patients and physio-logical studies can be based on these kind of pace-makers.
Study Limitation and Clinical Implications
This study was designed to demonstrate thefeasibility of implantation of a large, single passlead in small children. The atrial sensed signaldecreased after 1 week, bnt it was still wellabove the required value for appropriate sens-ing. Further significant decrease in the atrial sig-nal was not detected in our patients. As previ-ously mentioned, the patency of the venousroute was not evaluated, however, no clinicalsigns of occlusion were observed. As the feasi-bility and safety of implantation of these rela-tively large leads was demonstrated, the optionof dual chamber, synchronous pacing is sug-gested in children and adolescents. Furtherprospective stndy is required to demonstrate thelong-term efficacy of atrial sensing tbrough sin-gle pass lead in pediatric patients. The stabilityof the atrial electrogram during different physi-ological conditions also has to be evaluated infuture studies.
Acknowledgments: The authors would like to thank Ms.Chava Bondy and Dan Gfilvan, Ph.D., for their technical help.
References
Furman S, Young D. Cardiac pacing in childrenand adolescentes. Am J Cardiol 1977; 39:550-558.Dasmahapatra HK, Jamieson MPC, Brewster CM,et al. Permanent cardiac pacemaker in infants andchildren. Thorac Cardiovasc Surgeon 1986;34:230-235.Wampler DG, Shannon C, Burns GV, et al. Cardiacpacing in children and young adults. Am | DisChild 1983; 137:1098-1100.Smith RT. Pacemakers for Children. In PC Gillette,A Garson Jr (yds.): Pedialric Arrhythmias: Electro-physiology and Pacing. Philadelphia, W.B. Saun-ders Company, 1990, pp. 532-558.Ott DA. Epicardial Pacemaker Implantation. In PC
Gillette and A Garson, Jr (eds.]: Pediatric Arrhyth-mias: Electrophysiology and Pacing. Philadelphia,W.B. Saunders Company, 1990, pp. 575-579.Serwer GA, Dorostkar PC. Pediatric Pacing. In KAEllenbogen, CN Kay, BL Wilkoff (eds.): ClinicalCardiac Pacing. Philadelphia, W.B. SaundersCompany, 1995, 706-734.Hayes DL, Holmes DR, Maloney JD, et al. Perma-nent endocardial pacing in pediatric patients. JThorac Cardiovasc Surg 1983; 85:618-624.Kerstjens-Frederikse MWS, Bink-Boelkens MTE,de Jongste MIL. et al. Permanent cardiac pacing inchildren: Morhidity and efficacy of follow-up. IntJ Cardiol 1991; 33:207-214.
PACE, Vol. 20 August 1997, Part I 1965

ROSENHECK, ET AL.
9. Till JA, Jones S, Rowland E, et al. Endocardial 19.pacing in infants and children 15 kg or less inweight: Medium-term follow-up. PACE 1990;13:1385-1392.
10. O'Sullivan JJ, Jameson S, Gold RC, et al. Endocar-dial pacemakers in children; Lead length and al- 20.lowance for growth. PACE 1993; 16:267-271.
11. Molina JE, Dunnigan AC, Crosson JE. Implantationof transvonous pacemakers in infants and small 21.children. Ann Thoran Surg 1995; 59:689-694.
12. Lau YR, Cillette PC, Buckles DS, et al. Actuarialsurvival of transvenous pacing leads in a pediatric 22.population. PACE 1993; 16:1363-1367.
13. Belott PH, Byrd CL. Recent Developments in Pace-maker Implantation and Lead Retrieval. In SS 23.Barold, J Mugica (eds.): New Perspectives in Car-diac Pacing. Mt. Kisco, NY, Futura PublishingCompany, Inc., 1991, 105-131. 24.
14. Alt E. Neuzner J, Binner L, et al. Three-year expe-rience with stylet for lead extraction: A multican-ter study. PACE 1996; 19:18-25,
15. Curzio G. A multicenter evaluation of a single-passlead VDD pacing system. PACE 1991; 14:434-442. 25.
16. Pitts Crick JC. European multicenter prospectivefollow-up study of 1002 implants of a single leadVDD pacing system. PACE 1991; 14:1742-1744.
17. Ovsyshcher 1, Katz A, Bondy C. Clinical evalua-tion of a new single pass lead VDD pacing system.PACE 1994; 17:1864-1869. 26.
18. Ovsyshcher I, Katz A, Rosenheck S, et al. Singlelead VDD pacing: Multicenter study. PACE 1996;19:1768-1771.
Mond HC, Helland JR. Engineering and ClinicalAspects of Pacing Leads. In KA Ellenhogen, CNKay. BL Wilkoff (eds.): Clinical Cardiac Pacing.Philadelphia, W.B. Saunders Company, 1995, pp.69-90.Cillette PC, Shannon C, Blair H, et al. Transvenouspacing in pediatric patients. Am Heart J 1983;105:843-847.Ward DE, Jones S, Shinehourne EA. Long-termtransvenous pacing in children weighing ten kilo-grams or less. Int J Cardiol 1987; 15:112-115.Spotnitz HM. Transvenous pacing in infants andchildren with congenital heart disease. Ann Tho-rac Surg 1990; 49:495-496.Gillette PC, Edgerton J, Kratz J, et al, The suhpec-toral pocket: The preferred implant site for pedi-atric pacemakers. PACE 1991; 14:1089-1092.Gillette PC, Ziegler V. Transvenous ImplantationTechnique. In PC Cillette, A Garson Jr (eds.): Pedi-atric Arrhythmias: Electrophysiology and Pacing.Philadelphia, W.B. Saunders Company, 1990, pp.559-574,Linde-Edelstam C, Nordlander R, Und'n AL, et al.Quality-of life in patients treated with atrioven-tricular synchronous pacing compared to ratemodulated ventricular pacing: A long-term, dou-ble-blind, crossover study. PACE 1992;15:1467-1476.Ovsyshcher IE. Matching optimal pacemaker topatient: Do we need a large scale clinical trial ofpacemaker mode selection? PACE 1995;18:1845-1852.
1966 August 1997, Part I PACE, Vol. 20
Copyright © 2022 FDOKUMEN












![Active low pass filter design[1]](https://static.fdokumen.com/doc/165x107/631aaeddd43f4e1763048eee/active-low-pass-filter-design1.jpg)