
Contribution of the ventricles and the atrial appendages to the elevation of plasma atrial...
10
Basic Res Cardio191:319 - 328 (1996) SteinkopffVerlag 1996 W. Shen X. Xu M. Ochoa G. A. Zeballos J. M. Stewart T. H. Hintze Contribution of the ventricles and the atrial appendages to the elevation of plasma atrial natriuretic factor (ANF) during pacing-induced heart failure in conscious dogs Received: 14 October 1994 Returned for revision: 25 November 1994 Revision received: 22 February 1996 Accepted: 5 March 1996 Supported by PO-1-HL 43023 from the Heart, Lung and Blood Institute W. Shen. X. Xu. M. Ochoa G. A. Zeballos Prof. Dr. T. H. Hintze (S) Department of Physiology New York Medical College Valhalla, New York 10595, USA J. M. Stewart Department of Pediatrics New York Medical College Valhalla, New York 10595, USA Abstract The goal of our study was to determine whether the elevation in plasma ANF was produced by the atrial appendages or ventricular tissue during pacing-induced heart failure in chronically instrumented conscious dogs (sham) or dogs with bilateral atrial appendectomy. Acute volume expansion caused a signifi- cant elevation of plasma ANF from 80 _+ 8to 149 + 26 pg/ml (p < 0.01) in sham dogs, but caused no significant change from 67 _+ 7 to 84 _+ 8 pg/ml in atrial appendectomized dogs. There were increases in left ventricular end-diastolic pressure (LVEDP) and left atrial pressure (LAP) in both groups of dogs. After rapid left ven- tricular pacing (210-240 beats/min) for 4 weeks to induce heart failure, dogs in both groups had tachycardia, elevated LVEDP and higher LAE Plasma ANF was increased by 250 % to 283 + 64 pg/ml (p < 0.01) in sham dogs, and only 40 % to 94 + 15 pg/ml (p > 0.05) in atrial appendectomized dogs. In response to volume expan- sion, there were further increases in LVEDP and LAP in both groups of dogs, but plasma ANF was not elevated (288 + 39 pg/ml) in sham dogs and only slightly increased (132 + 7 pg/ml) in atrial appendectomized dogs. Our results suggest that, during pacing-induced heart failure, the atrial appendages are the major source of elevated plasma ANF, and the remaining atrial and ventricular tissue, even when maximally stretched, can only modestly increase plasma ANE Key words Atrial natriuretic factor (ANF) - atrial function - volume expansion - heart failure - ventri- cular compliance Introduction Atrial natriuretic peptide (ANF) is a circulating hormone with an important role in the regulation of fluid volume and blood pressure by causing natriuresis, diuresis, vaso- dilation, and inhibition of renin and aldosterone secretion (5, 13, 19). ANF is normally synthesized and stored in atrial myocytes and the greatest concentration of ANF is contained in the atrial appendages (6, 8, 21). The secre- tion of ANF is induced by the stretch of atrial wall, which has been historically demonstrated by changes of plasma ANF in response to acute volume expansion (17, 21, 25, 32). It has been previously documented that there is a signi- ficant increase in plasma ANF associated with an increase in ANF mRNA and Golgi complex and a decrease in ANF content in atrial tissue in experimental congestive heart failure in rats, hamsters and dogs (3, 7, 9, 14, 18, 26 - 28). The association between synthesis and secretion of ANF suggests an altered release of ANF from atrial tissue dur-
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Contribution of the ventricles and the atrial appendages to the elevation of plasma atrial...

Basic Res Cardio191:319 - 328 (1996) �9 SteinkopffVerlag 1996
W. Shen X. Xu M. Ochoa G. A. Zeballos J. M. Stewart T. H. Hintze
Contribution of the ventricles and the atrial appendages to the elevation of plasma atrial natriuretic factor (ANF) during pacing-induced heart failure in conscious dogs
Received: 14 October 1994 Returned for revision: 25 November 1994 Revision received: 22 February 1996 Accepted: 5 March 1996
Supported by PO-1-HL 43023 from the Heart, Lung and Blood Institute
W. Shen. X. Xu. M. Ochoa �9 G. A. Zeballos Prof. Dr. T. H. Hintze (S) Department of Physiology New York Medical College Valhalla, New York 10595, USA J. M. Stewart Department of Pediatrics New York Medical College Valhalla, New York 10595, USA
Abstract The goal of our study was to determine whether the elevation in plasma ANF was produced by the atrial appendages or ventricular tissue during pacing-induced heart failure in chronically instrumented conscious dogs (sham) or dogs with bilateral atrial appendectomy. Acute volume expansion caused a signifi- cant elevation of plasma ANF from 80 _+ 8to 149 + 26 pg/ml (p < 0.01) in sham dogs, but caused no significant change from 67 _+ 7 to 84 _+ 8 pg/ml in atrial appendectomized dogs. There were increases in left ventricular end-diastolic pressure (LVEDP) and left atrial pressure (LAP) in both groups of dogs. After rapid left ven- tricular pacing (210-240 beats/min) for 4 weeks to induce heart failure, dogs in both groups had tachycardia, elevated LVEDP and higher LAE Plasma ANF was increased by 250 %
to 283 + 64 pg/ml (p < 0.01) in sham dogs, and only 40 % to 94 + 15 pg/ml (p > 0.05) in atrial appendectomized dogs. In response to volume expan- sion, there were further increases in LVEDP and LAP in both groups of dogs, but plasma ANF was not elevated (288 + 39 pg/ml) in sham dogs and only slightly increased (132 + 7 pg/ml) in atrial appendectomized dogs. Our results suggest that, during pacing-induced heart failure, the atrial appendages are the major source of elevated plasma ANF, and the remaining atrial and ventricular tissue, even when maximally stretched, can only modestly increase plasma ANE
Key words Atrial natriuretic factor (ANF) - atrial function - volume expansion - heart failure - ventri- cular compliance
Introduction
Atrial natriuretic peptide (ANF) is a circulating hormone with an important role in the regulation of fluid volume and blood pressure by causing natriuresis, diuresis, vaso- dilation, and inhibition of renin and aldosterone secretion (5, 13, 19). ANF is normally synthesized and stored in atrial myocytes and the greatest concentration of ANF is contained in the atrial appendages (6, 8, 21). The secre- tion of ANF is induced by the stretch of atrial wall, which
has been historically demonstrated by changes of plasma ANF in response to acute volume expansion (17, 21, 25, 32).
It has been previously documented that there is a signi- ficant increase in plasma ANF associated with an increase in ANF mRNA and Golgi complex and a decrease in ANF content in atrial tissue in experimental congestive heart failure in rats, hamsters and dogs (3, 7, 9, 14, 18, 26 - 28). The association between synthesis and secretion of ANF suggests an altered release of ANF from atrial tissue dur-

320 Basic Research in Cardiology, Vol. 91, No. 4 (1996) �9 SteinkopffVerlag 1996
ing heart failure. Similar changes in plasma and atrial tis- sue ANF have been reported in clinical studies on patients with dilated myopathy and congestive heart failure (29, 34, 37).
On the other hand, several studies have shown signifi- cant increases in ANF gene expression and immunoreac- tive ANF in ventricular tissue in patients and animals with congestive heart failure and cardiac hypertrophy (14, 16, 18, 34). Yasue et al. also demonstrated that there was an increase in plasma ANF in the anterior interventricular vein, which is thought to drain exclusively left ventricular tissue and not the atrial tissue, in patients with heart fail- ure (37). These data seem to suggest that the ventricles are capable of synthesis and secretion of ANF during heart failure. It is not known whether either the atria or the ven- tricles are the primary source for the elevation in plasma ANF during heart failure.
Our previous study showed that bilateral atrial appen- dectomy abolished increases in plasma ANF during vol- ume loading in conscious dogs (33), consistent with other experiments in dogs and rats (2, 23, 24, 30). There is, how- ever, no report concerning the effects of atrial appendec- tomy on plasma ANF during chronic congestive heart fail- ure. Using atrial appendectomy and chronic rapid left ventricular pacing, the present study was designed to address the question of whether the atria or ventricles contribute to the elevated plasma ANF observed in pac- ing-induced heart failure in conscious dogs. Our first goal was to determine whether the increase in plasma ANF in response to acute volume expansion was abolished by bilateral atrial appendectomy. The second goal was to determine whether there was an effect of bilateral atrial appendectomy on the change in plasma ANF in response to acute volume expansion after congestive heart failure induced by chronic rapid left ventricular pacing for 4 weeks.
Materials and methods
The experiments were carried out in chronically instrumented conscious dogs. Mongrel male adult dogs were used and divided into atrial appendectomized group and sham-operated group. All animals were conditioned to the laboratory environment, were supplied with stan- dard dog chow and given free access to water. All of the protocols were approved by the IACUC of New York Medical College and conform to the NIH Guide for the Use and Care of Laboratory Animals and the Principles of the American Physiologic Society.
Animal and surgical preparation
The dogs were sedated with Acepromazine (0.3 mg/kg), anesthetized with pentobarbital sodium (25 mg/kg) and artificially ventilated with a respirator (Harvard). A left thoracotomy was performed in the fourth intercostal space using sterile surgical techniques. The pericardium was incised parallel to the phrenic nerve. A catheter (Tygon) was implanted in the descending thoracic aorta for measurement of arterial pressure, and a solid-state pressure gauge (Konigsberg, p6.5) was inserted into the left ventricle via an apical stab wound for measurement of left ventricular pressure. Two 3 MHZ piezoelectric crys- tals were placed through stab wounds on the endocardial surface on opposite sides of the posterior and anterior left ventricle at the base for measurement of left ventricular internal circumferential diameter. Pacing electrodes were fixed with a suture to left ventricular epicardium for chronic rapid left ventricular pacing.
Bilateral atrial appendectomy was performed. The right and left atrial appendages were exposed and gently extended to their maximal length. They were clamped around their base and sutured behind the clamp. As much tissue as possible was excised and weighed. A catheter (Tygon) was placed in the remaining left atrium for mea- surement of atrial pressure. The same surgery except for the bilateral atrial appendectomy was performed on another group of dogs as a sham-operated group.
The incision was closed in layers, the pneumothorax was reduced, and wires and catheters were run subcu- taneously and exited between the shoulder blades. The dogs were given antibiotics and allowed to recover com- pletely for about 10 - 14 days. Meanwhile, the dogs were trained to lie quietly on the laboratory table.
Recording techniques
Left atrial pressure (LAP) and arterial pressures were measured by connecting the previously implanted cathe- ters to strain-gauge transducers (Statham P23ID) and mean arterial pressure (MAP) was derived using 2 Hz low- pass filters. Left ventricular systolic pressure (LVSP) was measured from the solid-state pressure gauge, and the sig- nal was magnified on another channel for determination of left ventricular end-diastolic pressure (LVEDP). The first derivative of left ventricular pressure with time (LV dP/dt) was derived by an operational amplifier (National Semiconductor LM 324). Left ventricular internal dia- meter was measured using the previously implanted pie- zoelectric crystals and transit time ultrasonic dimension gauge. The dimension gauge measures the transit time of acoustic impulses, traveling at the sonic velocity of 1.55 •

W. Shen et al. 321 Origin of ANF during heart failure
106 M]s between the implanted crystals and generates a voltage linearly proportional to time. Heart rate (HR) was monitored from the pressure pulse interval using a cardiotachometer (Beckman Instr, Newark, NJ).
All signals were recorded on a 14-channel tape recorder (Bell and Howell 3700B) and played back on a direct- writing oscillograph (Gould 2800). These recording techniques have been used by us previously (21, 22, 32, 33).
Protocol of volume expansion
A large bore catheter (Intracath, 19G, 60 cm) was inserted into a peripheral vein, advanced into the vena cava and connected to a bag of warmed saline (1L/bag) via an intra- venous drip line. After the dog rested quietly on the labo- ratory table for at least 20 min, 1000 ml of saline were infused as rapidly as possible under 250 - 300 mmHg of pressure using an arterial pressure bag. Usually, all of the saline was infused into the dog in 4 - 5 min. Hemo- dynamics were recorded continuously and blood samples for measurement of ANF and hematocrit were collected before and after infusion of 250, 500,750 and 1000 ml of saline, and also 20 min after the volume expansion.
Heart failure
After the initial control experiment, heart failure was pro- duced by chronic rapid left ventricular pacing. The exter- nal pacemaker (Pace Medical, Inc.) was packed in a vest worn by the dog and the dog's heart rate was increased to 210 beats/min for 3 weeks. Then, the pacemaker was set at 240 beats/min for 7 - 10 days, until the dog developed the clinical signs of congestive heart failure. The volume expansion protocol was repeated. Finally, the dog was given an overdose of sodium pentobarbital and the heart was removed. The septum, right, left ventricles and atrial appendages (in sham-operated dogs) were separated and weighed.
Atriopeptin assay
Blood was taken from the aortic catheter and placed into chilled tubes containing EDTA and 5 /zl/ml Aprotinin (Sigma) for measurement of plasma ANE The samples were centrifuged and the plasma stored at -30 ~ until the assay was performed.
For measurement of plasma ANE the samples were thawed, extracted using a SEP-PAK C-18 cartridge and ANF determined using a commercially available radio-
immunoassay kit (Peninsula, RIK-8798). Percent recovery of ANF was 85 + 3 % and interassay and intra assay coef- ficients of variation were 8 % and 5 %, respectively. The data were reduced with the use of a log-logic plot after correction for nonspecific binding and the minimum sen- sitivity of this assay was 1.0 pg per tube. We have used these techniques previously (21, 32, 33).
Analysis of left ventricular compliance
Left ventricular end-diastolic compliance was calculated from the data obtained during volume expansion. Using IBM-AT computer, the analog signals of left ventricular pressure and internal diameter were played back from tape, were digitized by an analog-to-digital converter (DASA, Gould) and were stored on hard disk. The sampl- ing rate was 200/s.
The simultaneous left ventricular pressure-diameter data, which was taken as a average of 5 - 7 continuous heart beats over a respiratory cycle, were collected every 10 s through the whole volume expansion period. An exponential fit of left ventricular end-diastolic pressure (LVEDP) as a function of left ventricular end-diastolic diameter (LVEDD) was constructed using the equation Y = ae(bx).
Statistical analysis
During volume expansion, plasma volume was rapidly expanded by saline and ANF production by the heart could be easily underestimated due to dilution, since there was a fall in hematocrit (Hct%) due to dilution during volume expansion. Thus, we used the change in hematocrit to estimate extent of dilution of plasma to nor- malize plasma ANE The normalized plasma ANF was cal- culated as plasma ANF x Hct% (during volume expan- sion) / Hct% (before volume expansion). We have used these methods previously (21).
Data were collected before and during volume expan- sion, and also collected before and after pacing for 4 weeks. All cardiac hemodynamic values were averaged over an entire respiratory cycle. All values in the text are expressed as mean + SE and differences during volume expansion from control were determined with one-way analysis of variance. Differences between atrial appen- dectomized dogs and sham-operated dogs were deter- mined with two-way analysis of variance. The ratio of F values was converted to a t-distribution using a Scheffe's test. Significant changes were considered to occur at the p < 0.05 level.
322 Basic Research in Cardiology, Vol. 91, No. 4 (1996) �9 Steinkopff Verlag 1996
Results
Effect of volume expansion on hemodynamics in atrial appendectomized and sham-operated dogs
Hemodynamic changes during acute volume expansion in both atr ial-appendectomized and sham-operated dogs are shown in Table 1 and Fig. 1.
In atrial appendectomized dogs, acute volume expan- sion of 1000 ml saline caused remarkable fall in hemato- crit from baseline 36 + 1.1% to 27 _+ 0.9 %, and signific- antly elevated LAP by 12 + 1.9 mmHg, LVEDP by 12 _+ 2.2 m m H g and LVEDD by 1.9 +_ 0.5 mm. These were accompanied by significant increases in H R by 73 + 12 beat/min, in M A P by 24 + 5 mmHg, in LVSP by 20 _+ 6 mmHg, and in LV dP/dt by 413 + 125 mmHg/sec (all p < 0.05).
In sham-operated dogs, there was a similar fall in hematocrit during acute volume expansion of 1000 ml saline, and the hemodynamic responses were not signific- antly different from those in the atrial appendectomized dogs (Table 1 and Fig. 1).
In order to determine the extent of removal of the atrial appendages in atrial appendectomized dogs, the
appendage tissue removed at surgery was weighed (left appendage was 1.67 + 0.47 g, right appendage was 1.15 + 0.13 g), and compared with the weight of atrial appen- dages obtained from careful anatomic dissection at post- mor tem examination in normal dogs in our laboratory (Table 2). The data indicate that about 78 % of the left atrial appendage and about 48 % of the right atrial appen- dage were removed during atrial appendectomy in the cur- rent study. In practice, the extent of functional elimina- tion of atrial appendage was larger than this measurement would indicate, because some of the tissue which remained was crushed during the placement of the clamp or from the suture line that was proximal to the clamp.
Pacing-induced congestive heart failure
After rapid left ventricular pacing for 4 weeks, all dogs became lethargic and anorexic and developed congestive heart failure associated with ascites, dyspnea and cyanosis to varying degrees. There were no significant changes in body weight in either group.
Cardiac function after heart failure was evaluated after the pacemaker was turned off for at least 30 • and the hemodynamic changes resulting from chronic rapid left
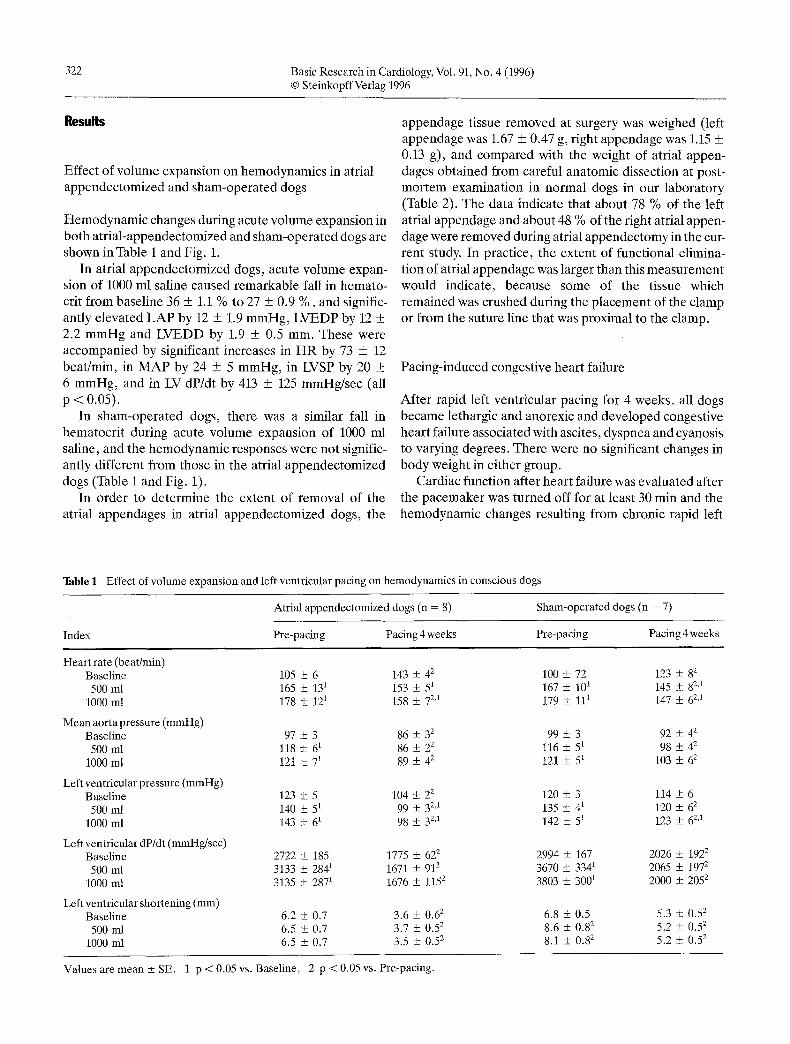
Table 1 Effect of volume expansion and left ventricular pacing on hemodynamics in conscious dogs
Atrial appendectomized dogs (n = 8) Sham-operated dogs (n = 7)
Index Pre-pacing Pacing 4 weeks Pre-pacing Pacing 4 weeks
Heart rate (beat/min) Baseline 105 • 6 143 • 42 500 ml 165 _+ 131 153 • 51
1000 ml 178 • 121 158 • 7 2'1
Mean aorta pressure (mmHg) Baseline 97 • 3 86 • 32 500 ml 118 • 61 86 • 22
1000 ml 121 2 71 89 • 4 2
Left ventricular pressure (mmHg) Baseline 123 • 5 104 • 2 z 500 ml 140 • 51 99 • 3 2'1
1000 ml 143 • 61 98 • 3 2'1
Left ventricular dP/dt (mmHg/sec) Baseline 2722 • 185 1775 • 622 500 ml 3133 • 2841 1671 • 912
1000 ml 3135 • 2871 1676 +_ 1152
Left ventricular shortening (mm) Baseline 6.2 • 0.7 3.6 • 0.62 500 ml 6.5 • 0.7 3.7 • 0.52
1000 ml 6.5 +_ 0.7 3.5 + 0.52
100 167 179
99 116 121
120 135 142
2994 3670 3803
6.8 8.6 8.1
+ 72 • 101 • 111
• + 51 + 51
• • 41 + 51
• 167 + 3341 • 3001
• 0.5 • 0.82 + 0.8 2
123 • 145 • 147 •
92 • 98 •
103 •
114 • 120 • 123 •
2026 • 2065 • 2000 •
5.3 • 5.2 • 5.2 •
82 82,1 62,1
42 42 62
6 62 62,1
1922 1972 2052
0.52 0.5 2 0.5 2
Values are mean + SE. 1 p < 0.05 vs. Baseline, 2 p < 0.05 vs. Pre-pacing.
W. Shen et al. 323 Origin of ANF during heart failure
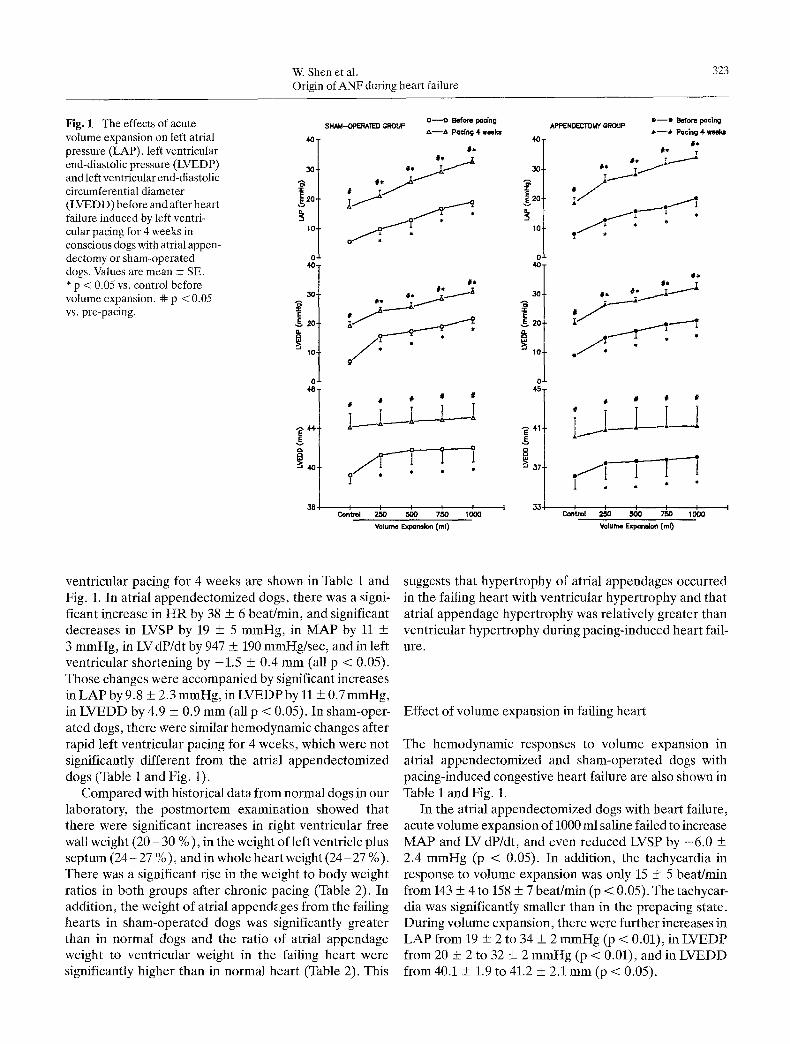
Fig. 1 The effects of acute volume expansion on left atrial pressure (LAP), left ventricular end-diastolic pressure (LVEDP) and left ventricular end-diastolic circumferential diameter (LVEDD) before and after heart failure induced by left ventri- cular pacing for 4 weeks in conscious dogs with atrial appen- dectomy or sham-operated dogs. Values are mean _+ SE. * p < 0.05 vs. control before volume expansion. + p <0.05 vs. pre-pacing.
40.
20.
10.
O 411
E
0.
1 0
0
- ~ 4 4
E v
38
o - - o Before pacing SHAM-OPERATED GROUP
~ , - - ~ , Pacing 4 w~ks 4O
30
40
~ ~ ---~ 2o
11 ~ II tl
!___!---! ! s I 45
~ , 41
e - - e Before poe|ng APPENDECTOMY GROUP
J.--~, Pgclng 4 we#x= 6d,
#~ T
. / I
IP*
.fl . �9
# # il t~
tl
Volume Expar~ion Cml) Volume Exp~l'~on Cml)
ventricular pacing for 4 weeks are shown in Table l and Fig. 1. In atrial appendectomized dogs, there was a signi- ficant increase in HR by 38 + 6 beat/min, and significant decreases in LVSP by 19 + 5 mmHg, in MAP by 11 + 3 mmHg, in LV dP/dt by 947 + 190 mmHg/sec, and in left ventricular shortening by -1.5 + 0.4 mm (all p < 0.05). Those changes were accompanied by significant increases in LAP by 9.8 _+ 2.3 mmHg, in LVEDP by 11 + 0.7 mmHg, in LVEDD by 4.9 + 0.9 mm (all p < 0.05). In sham-oper- ated dogs, there were similar hem�9 changes after rapid left ventricular pacing for 4 weeks, which were not significantly different from the atrial appendectomized dogs (Table 1 and Fig. 1).
Compared with historical data from normal dogs in our laboratory, the postmortem examination showed that there were significant increases in right ventricular free wall weight (20 - 30 %), in the weight of left ventricle plus septum (24 - 27 %), and in whole heart weight (24 - 27 %). There was a significant rise in the weight to body weight ratios in both groups after chronic pacing (Table 2). In addition, the weight of atrial appendages from the failing hearts in sham-operated dogs was significantly greater than in normal dogs and the ratio of atrial appendage weight to ventricular weight in the failing heart were significantly higher than in normal heart (Table 2). This
suggests that hypertrophy of atrial appendages occurred in the failing heart with ventricular hypertrophy and that atrial appendage hypertrophy was relatively greater than ventricular hypertrophy during pacing-induced heart fail- ure.
Effect of volume expansion in failing heart
The hem�9 responses to volume expansion in atrial appendectomized and sham-operated dogs with pacing-induced congestive heart failure are also shown in Table 1 and Fig. 1.
In the atrial appendectomized dogs with heart failure, acute volume expansion of 1000 ml saline failed to increase MAP and LV dP/dt, and even reduced LVSP by -6 .0 + 2.4 mmHg (p < 0.05). In addition, the tachycardia in response to volume expansion was only 15 _+ 5 beat/rain from 143 _ 4 to 158 + 7 beat/rain (p < 0.05). The tachYCar- dia was significantly smaller than in the prepacing state. During volume expansion, there were further increases in LAP from 19 + 2 to 34 + 2 mmHg (p < 0.01), in LVEDP from 20 + 2 to 32 ___ 2 mmHg (p < 0.01), and in LVEDD from 40.1 + 1.9 to 41.2 + 2.1 mm (p < 0.05).

324 Basic Research in Cardiology, Vol. 91, No. 4 (1996) �9 SteinkopffVerlag 1996
Table 2 Effect of chronic rapid left ventricular pacing on heart weight
Heart failure (4 weeks pacing)
Appendecto- Sham-operated mized
Normal control
Body weight (kg) 21.3 + 1.6 22.8 + 0.80 23.1 + 0.80
LAA(g) - 4.69 + 0.471 2.14 + 0.11
RAA(g) - 4.14 + 0.401 2.36 + 0.13
LAA + RAA (g) - 8.83 + 0.851 4.41 + 0.16
LV+Sept (g) 124 + 111 127 + 91 100 + 5
RV free wall (g) 51+ 41 47+31 3 9 + 2
LV+RV+ Sept (g) 175 + 131 175 + 121 139 + 6
(LAA+RAA)/ VW(g/g) - 0.052 _ 0.0031 0.034 + 0.002
VW/BW (g/kg) 8.19 + 0.291 7.43 + 0.321 6.06 + 0.25
Values are mean + SE. BW: body weight, LAA: left atrial appen- dage, RAA: right atrial appendage, LV: left ventricle, RV: right ven- tilde, Sept: septum, VW: ventricular weight (LV+RV+Sept). 1 p < 0.05, vs. normal nonpacing control. Appendectomized group, n = 6. Sham-operated group, n = 7. Normal control, n = 10.
The hemodynamic responses in sham-operated dogs with heart failure during acute volume expansion was not different from those in dogs with atrial appendectomy. There were no significant differences between the two groups (Table 1 and Fig. 1).
Effect of volume expansion on left ventricular compliance
The effects of vo lume expans ion on left ven t r i cu la r com-
p l iance be fo re and af ter the d e v e l o p m e n t of h e a r t fa i lure in these dogs is shown in Table 3. A r ep re sen t a t i ve i l lustra- t ion of lef t ven t r i cu la r end-d ias to l i c compl i ance dur ing vo lume expans ion is shown in Fig. 2. Lef t ven t r i cu la r end-
d ias to l ic p ressure and in te rna l d i a m e t e r d e m o n s t r a t e d an exponen t i a l r e l a t ionsh ip dur ing acute vo lume expans ion of 1000 ml sal ine in a t r ia l a p p e n d e c t o m i z e d and sham- o p e r a t e d dogs. T h e r e were no signif icant d i f ferences b e t w e e n regress ion coeff ic ients in the two groups .
A f t e r pac ing to induce hea r t fa i lure , the exponen t i a l curve of lef t ven t r i cu la r compl i ance was s ignif icant ly shi f ted to the r ight and also b e c a m e s teeper , wi th a signif- icant increase in b va lue in f i t ted equa t ion (a = - 3 5 . 9
Table 3 Effect of pacing 4 weeks on left ventricular end-diastolic compliance curve during acute volume expansion in atrial appendec- tomized dogs.
Compliance Pre-pacing control After pacing 4 weeks
a -8.96 + 0.73 -35.87 -t- 8.571 b 0.34 + 0.01 0.97 _+ 0.241 R 0.93 + 0.28 0.87 + 0.04
The equation was calculated as Y = ae (bx). Values in the table are mean + SE. 1 p < 0.05, vs. Pre-pacing.
+8 .6 , b = 0.97 + 0.24). These results ind ica te tha t the hea r t b e c a m e la rger (d i la ted) and also there was an increase in the pressure s t re tching the ven t r i cu la r myocar- d ium due to the conges t ive hea r t fai lure. The re was even a fu r the r increase dur ing acute vo lume expans ion .
Effec t of vo lume expans ion on A N F be fo re and af te r pac ing - induced h e a r t fa i lure
The effects of vo lume expans ion on p l a s m a A N F be fo re and af ter the d e v e l o p m e n t of h e a r t fa i lure in a t r ia l appen- d e c t o m i z e d and s h a m - o p e r a t e d dogs are shown in Table 4
and Figs. 3 and 4. The base l ine p l a sma A N F was 67 + 7 and 80 + 8 pg/ml
in a t r ia l a p p e n d e c t o m i z e d and s h a m - o p e r a t e d dogs,
E E
D- E) W >,
42.
36.
3 0
24
18
12
6 33
O
0 Before pacing
,x Pacing 4 weeks
35 37 39
LVEDD (mm)
I 41
Fig. 2 A representative illustration of changes in left ventricular diastolic compliance during acute volume expansion before and after heart failure induced by left ventricular pacing for 4 weeks in a con- scious dog without atrial appendages. Exponential fits of left ven- tricular end-diastolic pressure (LVEDP) as a function of left ven- tricular end-diastolic diameter (LVEDD) were constructed using the equation Y = ae (bx). Before pacing: a = -10.3, b = 0.36, r = 0.86. After pacing for 4 weeks: a = -61.2, b = 1.66, r = 0.98.

W. Shen et al. 325 Origin of ANF during heart failure
Table 4 Effect of volume expansion and heart failure on atrial natriuretic peptide in conscious dogs
Atrial appendectomized Sham-operated
Indexes Pre-pacing After pacing Pre-pacing (n = 6) (n = 5) (n = 10)
After pacing (n = 4)
Atrial natriuretic peptide (pg/ml) Baseline 67
500 ml 79 1000 ml 84
Normalized atrial natriuretic peptide (pg/ml) Baseline 67 500 ml 101
1000 ml 118
Hematocrit (%) Baseline 36
500 ml 28 1000 ml 26
_+7 94_+ 15 78_+7 _+ 10 83 + 9 87 _+ 7 _+ 8 132 _+ 42'1 149 -4- 261
_+ 7 94 + 15 78 + 7 _+ 13 106 + 10 110 _+ 9 t +_ 181 193 4-_ 7 2'1 210 + 341
+ 1 34 _+ 1 37 _+ 2 _+ 11 28 + 11 28 + 21 + 11 25 + 1 t 26 _+ 11
283 _+ 211 + 288 _+
283 + 264 + 386 -+
36 + 29 -+ 26 +
642 252 392
642 312 452,1
2 2 a 21
Values are mean + SE. 1 p < 0,05 vs. Baseline, 2 p < 0.05 vs. Pre-pacing.
respectively. There was no significant difference be tween the two groups. Acu te volume expansion of 1000 ml saline caused a significant elevat ion of plasma A N F from 80 + 8 to 149 _+ 26 pg/ml (p < 0.01), and normal ized plasma A N F to 210 + 34 pg/ml (p < 0.01) in sham-opera ted dogs. In contrast , the same acute volume expansion only increased plasma A N F f rom 67 _+ 7 to 84 + 8 pg/ml (p <0.05) and
Fig. 3 Effects of acute volume expansion and congestive heart fail- ure induced by chronic left ventricular pacing for 4 weeks on nor- malized plasma ANF in conscious dogs with atrial appendectomy or sham-operated dogs. Values are mean _+ SE. * p < 0.05 vs. control before volume expansion. #e p <0 .05 vs. pre-pacing.
normal ized A N F to 118 _+ 18 pg/ml (p < 0.05) in atrial appendec tomized dogs. The magni tude of release in A N F during acute volume expansion was significantly smaller (p < 0.05) in the atrial appendec tomized group compared to the sham-opera ted group.
Af te r chronic rapid left ventr icular pacing for 4 weeks to induce hear t failure, baseline plasma A N F was signific- antly increased f rom 78 + 7.2 to 283 _+ 63 pg/ml (p < 0.05) in sham-opera ted dogs, but baseline plasma A N F was mainta ined at a lower level 67 _+ 7 to 94 + 15 pg/ml (p < 0.05) in atrial appendec tomized dogs (Fig. 4). Dur- ing acute volume expansion of 1000 ml saline in these dogs with hear t failure after 4 weeks pacing, there was a signif- icant elevation o f normal ized A N F f rom 283 + 64 to 386 +
E
h :Z
N
E Z
500
400
300
200
100
0
BEFORE PACING
O - - O Sham-operated group
A - - A Atrial Appendectomlzed group
# *
T
I I I I I
Control 250 500 750 1000
E
g
LL Z
6) N
~3
E o
Z
I
500-
400-
300-
200-
100-
0
AFTER PACING 4 WEEKS
0 - - 0 Sham-operated group
& - - A Atrial Appendectomized group
# *
l # # �9
I I I I I Control 250 500 750 1000
Volume Expansion (ml) Volume Expansion (ml)

326 Basic Research in Cardiology, Vol 91, No. 4 (1996) �9 SteinkopffVerlag 1996
400-
E 300-
v
L
z 200- <E
o E 8 ~- 100-
F--I Before pacing
17721 Pacing 4 weeks
Atrial Appendectomy
%
%
i/ ii
T i/
Sham Operation
Fig. 4 Effect of congestive heart failure induced by chronic left ven- tricular pacing for 4 weeks on plasma atrial natriuretic peptide (ANF) in conscious dogs with or without atrial appendages. Values are mean _+ SE. ** p < 0.01 vs. pre-pacing_
45 pg/ml (p < 0.05) in sham-operated dogs and there were significant increases in plasma ANF from 94 + 15 to 132 + 40 pg/ml and in normalized ANF to 193 + 7 pg/ml (both p < 0.05) in atrial appendectomized dogs. Plasma or nor- malized ANF was significantly smaller (p < 0.05) in atrial appendectomized dogs when compared to the sham- operated group.
Discussion
In our experiment, acute volume expansion consistently resulted in significant increases in HR, MAR LVSP, LAR LVEDP and LVEDD and a decrease in hematocrit in dogs with or without intact atrial appendages. There was no significant difference between the two groups, which suggests that bilateral atrial appendectomy did not cause any significant changes in cardiovascular hemodynamic response to acute volume expansion in conscious dogs.
Acute volume expansion resulted in a significant increase in the circulating level of plasma ANF in dogs with intact atrial appendages. In contrast, acute volume expansion failed to elevate plasma ANF in dogs after bilateral atrial appendectomy. Morphological studies have shown a preferential distribution, in which the highest concentration of ANF was in atrial appendages in normal dog (21) and other animal species (6, 8). The pre- sent result is consistent with our earlier studies (33) and other reports (2, 23), suggesting that the atrial appendages are the primary source for the elevation of plasma ANF during acute volume expansion in normal conscious dogs.
It was interesting that the basal plasma ANF level in conscious dog with bilateral atrial appendectomy was not significantly reduced, as was previously reported in rat (23) and dog (33) by us. This indicates that the atrial appendages are not required to maintain plasma ANF under normal physiological conditions. Our previous data showed that ANF secretion rate from the atria was about 4.0 ng/min/g of tissue, ANF concentration in atrial appen- dages was approximately 1500 ng/g of tissue and only ini- tially 0.3 % of stored ANF is secreted each minute in the normal state (21, 22). In the present study, only 60 - 70 % of the atrial appendages were removed at surgery, there- fore, the remaining atrial appendages and atrial tissue might still contain enough ANF to maintain the basal plasma ANF level. We cannot exclude other possible sources which may contribute to basal plasma ANF, i.e., a ventricular or extra cardiac source.
A mal-ked increase in plasma ANF occurs during heart failure in animal models (3, 9, 14, 26, 28) and patients with chronic congestive heart failure (29, 34, 37), similar to that in the sham-operated group in our study. There were significant increases in ANF mRNA, the size and com- plexity of the Golgi complex. These were accompanied by decreases in the number, size, and ANF content of secret- ory granules in atrial cardiocytes during heart failure (7, 14, 18). In the present study, we found a significant hyper- trophy of the atrial appendages in sham-operated dogs with heart failure. The atrial hypertrophy could result from significant increases in atrial pressure and left ventricnlar end-diastolic pressure in the failing heart. Another possible reason could be pacing tachycardia which caused asychronous contraction of the atrium against a closed A-V valve to further increase atrial pressure (Cannon A waves). The hypertrophy of atrial appendages may provide a greater atrial mass for produc- tion and release of ANF to maintain the high level of plasma ANF during heart failure. In our pacing-induced heart failure model, plasma ANF was significantly increased in the dog with intact atrial appendages and the plasma ANF was limited to prepacing level in atrial appen- dectomized dogs. It was the atrial appendectomy which abolished the increase of plasma ANF during heart failure, suggesting that the atrial appendages could be the predo- minant source responsible for the high level of circulating arterial ANF during heart failure.
ANF is expressed and stored in the fetal ventricle, and this ability to synthesize ANF in ventricle disappears in the neonatal period (4, 35, 36). Under normal physiologi- cal conditions, the concentration of ANF is very low and ANF gene expression cannot be detected in adult ventri- cle (16, 18, 21). ANF gene expression and secretory granules have been found in ventricular myocytes in rats and hamsters with severe heart failure. A marked eleva-

W. Shen et al. 327 Origin of ANF during heart failure
tion in plasma ANF was found in blood collected from the anterior interventricular vein, which is believed to drain blood only from the left ventricle and not from the atria, in patients with dilated heart failure (3, 16, 37). All of these data imply that ANF could be produced and sec- reted from ventricular myocytes in the failing heart (14, 16, 18, 34). Taking the large mass of the ventricles into consideration, even if the tissue concentration is very low compared to that in the atrium, ventricular tissue could become an important source of ANF during heart failure (3, 14, 16, 18, 34, 37). The ratio of stored immunoreactive ANF to ANF mRNA in ventricle is much less than in atria, suggesting a different storage and release pathway asso- ciated with a constitutive release of ANF in the ventricle (29). The contribution of the ventricles to plasma ANF is difficult to determine however, simply by measuring the content of immunoreactive ANF and ANF mRNA in ven- tricular tissue. In the present study, chronic rapid left ven- tricular pacing induced congestive dilated heart failure associated with higher LVEDR larger LVEDD and reduced compliance of the left ventricle, but there was no significant increase in plasma ANF in atrial appendec- tomized dogs. This indicates that ventricles may not be primarily responsible for the unusually high level of plasma ANF during heart failure.
In the present study, there were smaller elevations in normalized plasma ANF in response to acute volume expansion in both groups of dogs with heart failure. A similar result was also reported by Chien et al. indicating that the capacity to increase plasma ANF concentration during acute volume expansion was preserved in rats with heart failure (9). Although, there was the possibility that
ANF could come from ventricular tissue during acute volume expansion, our data showed a significant increase in LVEDP and LVEDD during heart failure and acute volume expansion did not cause a further increase in LVEDD, despite a further increase in LVEDP, i.e., left ventricular compliance was reduced. This suggests that decreased left ventricular compliance and maximal left ventricular stretch already occurred during heart failure even before volume expansion, so that the elevation of LVEDP during volume expansion may not be an effective stimulus for ANF release from ventricular muscle during acute volume expansion. On the other hand, our previous study demonstrated a typical exponential relationship between atrial pressure and diameter and a exponential relationship between passive V-wave minute wall stress and plasma ANF (32). There was greater ANF release from atrial tissue at high filling pressures, especially when atrial filling pressure increased to over 15 mmHg resulting in very high atrial appendage wall stress (32). In the pre- sent study, an elevated plasma ANF in response to acute volume expansion after heart failure could be due to a further increase in atrial pressure and atrial stress.
In conclusion, the present study demonstrates that atrial appendectomy abolished the elevation of plasma ANF in response to acute volume expansion and blunted the increase in plasma ANF during pacing-induced heart failure. This suggests that the atrial appendages are the primary source of elevated plasma ANF even during heart failure. There may be a modest contribution by ventricu- lar tissue, however, this is small and only occurs at greatly elevated LVEDP (i.e., greater than 25 mmHg).
References
1. Benjamin BA, Metzler CH, Peterson TV (1987) Renal response to volume expansion in atrial appendectomized dogs. Am J Physio1253:R786-R793
2. Benjamin BA, Meltzer CH, Peterson TV (1988) Chronic atrial appendectomy alters sodium excretion in conscious monkey. Am J Physio1254:R695-R705
3. Bilder GE, Sweet CS, Emmert SE, Schofield TL, Edina R, Stabilito II, Friedman PA (1989) Cardiac and non- cardiac atrial natriuretic factor (ANF) biosynthesis and storage and plasma ANF in the rat model of chronic ven- tricular dysfunction. Endocrinology 124:1515-1521
4. Bloch KD, Seidman JC, Naftilan JD, Fallon JT, Seidman C (1986) Neonatal atria and ventricles secrete atrial natriu- retie factor via tissue-specific secretory pathways. Cell 47:695-702
5. Brenner BM, Ballermann B J, Gunning ME, Zeidel ML (1990) Diverse biologi- cal actions of atrial natriuretic peptide. Physiol Rew 70:665-699
6. Cantin M, Genest J (1985) The heart and atrial natriuretic factor. Endocr Rev 6:107-127
7. Cantin M, Thibault G, Ding J, Gut- kowska J, Garcia R, Jasmin G, Hamet P, Genest J (1988) ANF in experimental congestive heart failure. Am J Pathol 130:552-568
8. Chapeau C, Gutkowsak J, Schiller PW, Milne RW, Thibault G, Garcia J, Cantin M (1985) Localization of immunoreac- rive synthetic atrial natriuretic factor (ANF) in the heart of various animal species. J Histochem Cytochem 33: 541- 550
9. Chien YW, Barbee RW, MacPhee AA, Frohlich ED, Trippodo NC (1988) Increased ANF secretion after volume expansion is preserved in rats with heart failure. Am J Physio1254:R185-R191
10. Chow E, Woodara JC, Farrar DJ (1990) Rapid ventricular pacing in pigs. An experimental model of congestive heart failure. Am J Physio1258:1603-1605

328 Basic Research in Cardiology, Vol. 91, No. 4 (1996) �9 SteinkopffVerlag 1996
11. Coleman HN, Taylor RR, Pool PE, Whipple CH, Covell JW, Ross J, Braun- wald E (1971) Congestive heart failure following chronic tachycardia. Am Heart J 81:790-798
12. Cowley AW Jr, Anderas PR, Skelton MM (1988) Acute saline loading in nor- mal and bilaterally atrial-resected con- scious dogs. Am J Physiol 255: H144- H152
13. De Bold AJ (1985) Atrial natriuretic fac- tor. A hormone produced by the heart. Science (Wash. DC) 230:767-770
14. Ding J, Thibault G, Gutkowska J, Gar- cia R, Karabatsos Jasmin GT, Genest J, Cantin M (1987) Cardiac and plasma atrial natriuretic factor in experimental congestive heart failure. Endocrinology 121:248-257
15. Douglas PS, Morrow R, IoliA, Reichek N (1989) Left ventricular shape, after- load and survival in idiopathic dilated cardiomyopathy. J Am Coll Cardiol 13: 311-315
16. Edwards BS, Ackermann DM, Lee ME, Reeder GS, Wold LE, Burnett JC Jr (1988) Identification of atrial natriuretic factor within ventricular tissue in hamsters and humans with congestive heart failure. J Clin Invest 81:82-86
17. Edwards BS, Zimmermann RS, Schwab TR, Heublein DM, Burnett JC (1988) Atrial stretch not pressure is the princi- pal determinant controlling the acute release of atrial natriuretic peptide. Circ Res 56:191-195
18. Franch HA, Dixon RAF, Blaine EH, Siegl PKS (1988) Ventricular atrial natriuretic factor in the cardiomyopathic hamster model of congestive heart fail- ure. Circ Res 62:31-36
19. Genest J, Cantin M (1987) Atrial natri- uretic factor. Circulation 75 (Suppl I): 118-124
20. Gould KL, Lipscomb K, Hamilton GW, Kennedy JW (1974) Relation of left ven- tricular shape, function and wall stress in man. Am J Cardio134:627-634
21. Hintze TH, Mclntyre JJ, Patel MB, Shapiro JT, DeLeonardis M, Zeballos GA, Loud A (1989) Atrial wall function and plasma atriopeptin during volume expansion in conscious dogs. Am J Physio1256:H713-H719
22. Hintze TH, Wang J, Patel M, Schustek M, Ochoa M, Dean R, Chiruzzo E Zeballos GA (1990) Dynamics of atrial peptide secretion in the coronary circu- lation of the conscious dog. Circ Res 67: 609-614
23. Hoffman A, Keiser RH (1990) Con- scious atrial appendectomized rats have a blunted atrial natriuretic factor release to volume expansion but normal responses to other acute stimuli. Am J Hypertension 3:786-788
24. Kinter LB, Kopia G, DePalma D, Bren- nan F, Landi M, Inagami T (1986) Chronic bilateral atrial appendectomy does not affect salt excretion in dogs. J Hypertens 4 (Suppl 5): $80-$82
25. Metzler CH, Lee M, Thrasher TN, Ram- say DJ (1986) Increase right or left atrial pressure release of atrial natriuretic pep- tide in conscious dogs. Endocrinology 119:2396--2398
26. Moe GW, Grima EA, Angus C, Wong NLM, Hu DCK, Howard R J, Armstrong PW (1991) Response of atrial natriuretic factor to acute and chronic increases of atrial pressures in experimental heart failure in dogs. Role of changes in heart rate, atrial dimension, and cardiac tissue concentration. Circulation 83: 1780- 1787
27. Perrella MA, Schwab TR, O'Murchu B, Redfield MM, Wei CM, Edwards BS, Burnett Jr JC (1992) Cardiac atrial natriuretic factor during evolution of congestive heart failure. Am J Physiol 262:1248-1255
28. Redfield MM, Edwards BS, McGoon MD, Heublein DM, Aarhus LL, Bur- nett Jr JC (1989) Failure of atrial natriuretic factor to increase with volume expansion in acute and chronic congestive heart failure in the dog. Cir- culation 80:651-657
29. Saito Y, Nakao K, Arai H, Nishimura K, Okumura K, Obata K, Takemura G, Fujiwara H, Sugawara A, Yamada T, Itoh H, Mukoyama M, Hosoda K, Kawai C, Ban T, Yasue H, Imura H (1989) Augmented expression of atrial natriuretic polypeptide gene in ventricle of human failing heart. J Clin Invest 83: 298-305
30. Salazar FJ, Romero JC, Bumett JC Jr, Schryver S, Granger GP (1986) Atrial natriuretic peptide levels during acute and chronic saline loading in conscious dogs. Am J Physio1251:R499-R503
31. Shannon RE Komamura K, Stambler BS, Bigaud M, Manders WT, Vatner SF (1991) Alterations in myocardial con- tractility in conscious dogs with dilated cardiomyopathy. Am J Physiol 260: 1903-1911
32. Stewart JM, O'Dea DJ, Shapiro GC, Patel MB, McIntyre JT, Gewitz MH, Hoegler CT, Shapiro JT, Zeballos GA, Hintze TH (1991) Atrial compliance determines the nature of passive atrial stretch and plasma atrial natriuretic fac- tor in the conscious dog. Cardiovascular Res 25:784-792
33. Stewart JM, Dean R, Brown M, Dias- parra D, Zeballos GA, Schustek M, Gewitz MH, Thompson CI, Hintze TH (1992) Bilateral atrial appendectomy abolishes increased plasma atrial natri- uretic peptide release and blunts sodium and water excretion during volume load- ing in conscious dogs. Circ Res 70: 724- 732
34. Takemura G, Fujiwara H, Horike K, Mukoyama M, Saito Y, Nakao K, Mat- suda M, Kawamura A, Ishida M, Kida M, Uegaito T, Tanaka M, Matsumori A, Fujiwara Y, Fujiwara T, Imura H, Kawai C (1989) Ventricular expression of atrial natriuretic polypeptide and its relations with hemodynamics and histology in dilated human hearts, Immunohisto- chemical study of the endomyocardial biopsy specimens. Circulation 80: 1137- 1147
35. Tsuchimochi H, Kurimoto F, Ieke K, Koyama H, Takaku F, Kawana M, Kimata S, Yazaki Y (1988) Atrial natriuretic peptide distribution in fetal and failed adult human heart. Circula- tion 78:920-927
36. Wei Y, Rodi CP, Day ML, Wiegand RC, Needleman LD, Cole BR, Needleman P (1987) Developmental changes in the rat atriopeptin hormonal system. J Clin Invest 79:1325-1329
37. Yasue H, Obata K, Okumura K, Kurose M, Ogawa H, Matsuyama K, Jougasaki M, Saito Y, Nakao K, Imura H (1989) Increased secretion of atrial natriuretic polypeptide from the left ventricle in patients with dilated cardiomyopathy. J Clin Invest 83:46-51




















