
A new method for analysis of atrial activation during chronic atrial fibrillation in man
Upload
independentCategory
view
0download
0
Low Energy Intracardiac Cardioversion ofPersistent Atrial Fibrillation
MASSIMO SANTINI, CLAUDIO PANDOZI, SALVATORE TOSCANO,ANTONIO CASTRO, GIULIANO ALTAMURA, ANNA PATRIZIA JESI,GIUSEPPE GENTILUCCI, MAURO VILLANI,*and MARIA GARMELA SGIANARO
From the Department of Heart Disease. San Filippo Neri Hospital, *Arrhythmia Control Unit, I Clinica Medica, LaSapienza University, Rome, Italy
SANTINI, M., ET AL.: Low Energy Intracardiac Cardioversion of Persistent Atrial Fibrillation. The aimsof the study were to verify the efficacy and safety of iow energy internal cardioversion (LEIC) in patientswith persistent atrial fibrillation (AF) and to identify the factors affecting the atrial defibrillation thresh-old (ADT). Forty-nine patients with persistent (lasting ^10 days) AF underwent LEIC. In each patient, two6 Fr custom-made catheters with large active surface areas were positioned in the coronary sinus (cath-ode) and the lateral right wall (anode), respectively, for shock delivery, and a tetrapolar lead was placedin the right ventricular apex for R wave synchronization. Truncated, diphasic (3 ms+3 ms). exponentialshocks were used, beginning at 50 V and increasing in steps of 50 V until sinus rhythm had been restored.Mild sedation (diazepam 5 mg IV) was administered to 12 patients. Sinus rhythm was restored in all thesubjects with mean voltage and energy levels of 352.0 ± 80.3 V and 8.2 ± 3.4 J, respectively. The ADT inpatients pretreated with amiodarone (6.4 ± 1.8 J) was lower than that of patients who had not receivedany antiarrhythmic drugs (9.2 ± 3.7) (P = 0.04). No ventricular arrhythmias were induced by any of theatrial shocks, and no other complications were observed. During a mean follow-up of 162.9 ± 58.7 days,AF recurred in 21 (43%) patients; 71% of these occurred in the first week after cardioversion. LEIC is ef-fective in restoring sinus rhythm in patients with persistent AF. The technique seems to be safe and doesnot require general anesthesia or, in most cases, sedation. Patients pretreated with amiodarone have lowerADTs. (PACE 1998; 21:2641-2650)
intracardiac cardioversion, low energy cardioversion, persistent atrial fibrillation
Introduction
Atrial fibrillation (AF) is a very common andpotentially dangerous cardiac arrhythmia. ̂ ~'' Asignificant number of cerebrovascular accidentsare in fact caused by thromboembolism in patientswith AF.'' A five-fold increase in the risk of em-bolism has been found in subjects with non-rheumatic AF. with an 18-fold increase in therheumatic group.'' To reduce this risk, full antico-agulation is frequently recommended.*'"" The lossof atrial contraction can also have negative hemo-dynamic repercussions, and in patients with im-
Address for reprints: Claudio Pandozi. M.D., Department ofCardiology, San Filippo Neri Hospital. Via Martinotti, 20,00135 Rome. Italy. Fax: 0039-6-33062489,
Received May 12. 1997; revised January 20, 1998; acceptedFebruary 11,1998.
paired diastolic function, these changes can leadto congestive heart failure.^•^"
Therefore, every attempt should he made torestore sinus rhythm in the majority of these pa-tients. However, spontaneous or pharmacologicalinterruption of the arrhythmia, which is observedin a significant percentage of patients with parox-ysmal AF,̂ '̂̂ ^ is very rare in cases of long-lastingarrhythmia.'^
Recently, after the previous experience withhigh energy internal cardioversion,^'' a new tech-nique for intracardiac transcatheter cardioversionwas developed,'''"^^ showing that sinus rhythmrestoration can be obtained by energies signifi-cantly lower than those used for external electricalcardioversion.
The aim of this stndy was to evaluate (1) thepossibility of restoring sinus rhythm in patientswith persistent (lasting slO days) AF using low
PACE, Vol, 21 December 1998 2641

SANTINI, ET AL.
energy intracardiac cardioversion (LEIC) withoutgeneral anesthesia; (2) the safety and the effective-ness of our internal cardioversion protocol; and(3) possihle correlation between the intracardiacatrial defibrillation threshold (ADT) and the pa-tient's clinical data and arrhythmia characteris-tics.
MethodsEntry Criteria
Patients with persistent AF, who were candi-dates for transthoracic cardioversion or had al-ready submitted to the latter treatment withoutsnccess. were included in the study. All suhjectsunderwent full oral anticoagulation for the last 3weeks before cardioversion, and transesophagealechocardiography was performed the day beforethe procedure. Three days before the cardiover-sion, oral anticoagulants were generally replacedwith heparin. The latter was stopped 6 hours he-fore and restarted 6 hours after the procedure. Oralanticoagulation was restarted after cardioversionand was continued for at least 30 days. Heparin in-fnsion was definitively stopped when therapeuticinternational normalized ratio (INR) values(2.5-3) were again achieved. The minimum INRsafe value, checked immediately prior to the inva-sive procedure, was considered 1.5. The patientswere adequately informed about the nature, risks,and benefits of the procedure, and written consentwas obtained from all.
LEIC Protocol
Three temporary intracavitary leads wereused in each patient: two custom-made 6 Frcatheters (Elecath Inc., Rahway, NJ, USA) forshock delivery and one USCI quadripolar lead[Bard-USCl Inc., Billerican, MA, USA) for ventric-ular synchronization. The Elecath leads had tenparallel platinum electrodes 4.5 mm long and sep-arated by 2.0 mm. The active surface area was314.1 mm^.
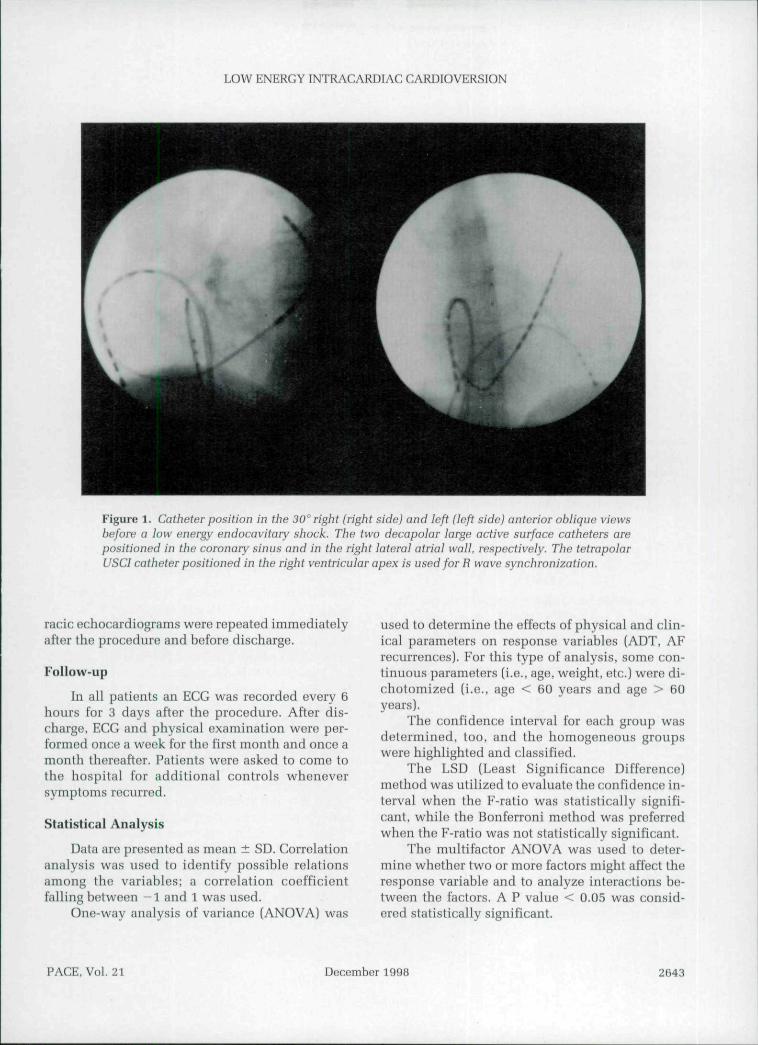
Under fluoroscopic control, the first Elecathlead (cathode) was positioned in the distal part ofthe coronary sinus in order to embrace as much aspossible the left atrium. The second Elecath lead(anode) was positioned high in the right atriumpaying attention to keep the electrodes in contact
with the atrial wall. The quadripolar lead was po-sitioned in the right ventricular apex for ventricu-lar synchronization (Fig.l). The Elecath leadswere tested for electric integrity before each pro-cedure.
The coronary sinus catheter was inserted us-ing the femoral approach in 45 (92%) cases andthe subclavian route in 4 (8%) cases. The femoralapproach was utilized for all the ventricular andatrial leads.
All catheters were connected to a TelectronicsGuardian APT 111 4215 implantable defibriliator(Telectronics Pacing Systems Inc., Englewood.CO, USA) specially adapted to receive snchcatheters. The defibriliator was used manuallyrather than automatically.
The programmed shock was hiphasic consist-ing of truncated, exponential phases, separated bya fixed 0.5 ms delay.̂ '̂̂ "̂ Three programmable pa-rameters determined the characteristics of theshock: voltage set the peak voltage of the firstphase of the shock; phase 1 width set the width ofphase 1 of the shock and could not be less thanphase 2 width; phase 2 width set the width ofphase 2 of the shock. We used a 3 ms-l-3ms phasewidth shocks.
The initial voltage of 50 was increased pro-gressively by 50 V increments until sinus rhythmhad been restored. All shocks were separated byan interval of at least 1 minute. The impedanceand voltage, as well as the total and delivered en-ergy, of each shock were automatically measuredby the device. The delivered energy was reportedin the study.
Continuous ECG recording was performedthroughout the procedure. All shocks were deliv-ered on the R wave, and the shock was consideredsuccessful when sinus rhythm appeared within 30seconds after delivery.
After each shock, the patients were asked torate their discomfort on a scale of 1 to 5 (1 = notfelt; 2 = felt without discomfort; 3 = mild dis-comfort; 4 = moderate discomfort; and 5 = severediscomfort). In the first five cases, sedation (di-azepam 5 mg IV) was routinely administered im-mediately before shock delivery. In the other 44patients, the drug was given only if necessary.
At the end of the procedure, a blood samplefor creatine-kinase (CK) analysis was collected toassess possible cellular damage. Control transtho-
2642 December 1998 PACE, Vol. 21
LOW ENERGY INTRACARDIAC CARDIOVERSION
Figure 1. Catheter position in tbe 30° right (right side) and left (left side) anterior oblique viewsbefore a low energy endocavitary shock. The two decapolar large active surface catheters arepositioned in the coronary sinus and in the right lateral atria! wall, respectively. The tetrapolarUSCI catheter positioned in the right ventricular apex is used for R wave synchronization.
racic echocardiograms were repeated immediatelyafter the procedure and before discharge.
Follow-up
In all patients an ECG was recorded every 6hours for 3 days after the procedure. After dis-charge, ECG and physical examination were per-formed once a week for the first month and once amonth thereafter. Patients were asked to come tothe hospital for additional controls wheneversymptoms recurred.
Statistical Analysis
Data are presented as mean ± SD. Correlationanalysis was used to identify possible relationsamong the variables; a correlation coefficientfalling between - 1 and 1 was used.
One-way analysis of variance (ANOVA) was
used to determine the effects of physical and clin-ical parameters on response variables (ADT, AFrecurrences). For this type of analysis, some con-tinuous parameters (i.e.. age, weight, etc.) were di-chotomized [i.e., age < 60 years and age > 60years).
The confidence interval for each group wasdetermined, too, and the homogeneous groupswere highlighted and classified.
The LSD (Least Significance Difference)method was utilized to evaluate the confidence in-terval when the F-ratio was statistically signifi-cant, while the Bonferroni method was preferredwhen the F-ratio was not statistically significant.
The multifactor ANOVA was used to deter-mine whether two or more factors might affect theresponse variable and to analyze interactions be-tween the factors. A P value < 0.05 was consid-ered statistically significant.
PACE. Vul. 21 December 1998 2643
SANTINI, ET AL.
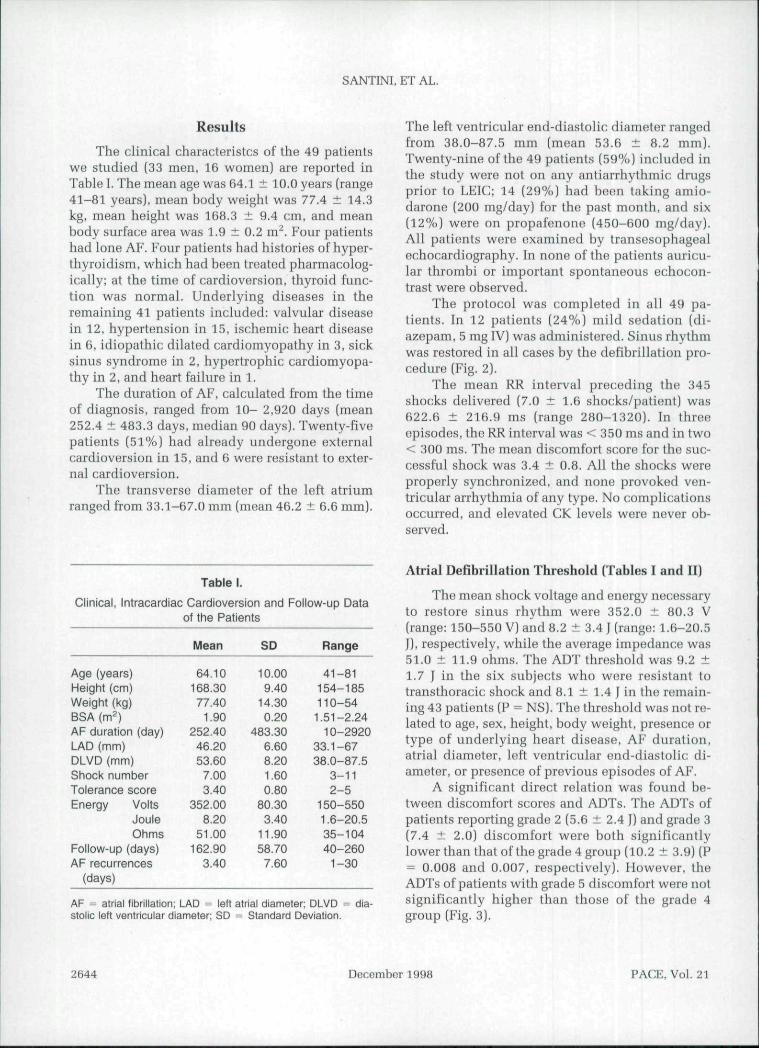
Results
The clinical characteristcs of the 49 patientswe studied (33 men, 16 women) are reported inTahle I. The mean age was G4.1 ± 10.0 years (range41-81 years), mean body weight was 77.4 ± 14.3kg, mean height was 168.3 ± 9.4 cm, and meanbody surface area was 1.9 ± 0.2 m*̂ . Four patientshad lone AF. Four patients had histories of hyper-thyroidism, which had heen treated pharmacolog-ically; at the time of cardioversion, thyroid func-tion was normal. Underlying diseases in theremaining 41 patients included: valvular diseasein 12. hypertension in 15, ischemic heart diseasein 6. idiopathic dilated cardiomyopathy in 3, sicksinus syndrome in 2, hypertrophic cardiomyopa-thy in 2, and heart failure in 1.
The duration of AF, calculated from the timeof diagnosis, ranged from 10- 2,920 days (mean252.4 ± 483.3 days, median 90 days). Twenty-fivepatients (51%) had already undergone externalcardioversion in 15, and 6 were resistant to exter-nal cardioversion.
The transverse diameter of the left atriumranged from 33.1-67.0 mm (mean 46.2 ± 6.6 mm).
The left ventricular end-diastolic diameter rangedfrom 38.0-87.5 mm (mean 53.6 ± 8.2 mm).Twenty-nine of the 49 patients (59%) included inthe study were not on any antiarrhythmic drugsprior to LEIC; 14 (29%) had been taking amio-darone (200 mg/day) for the past month, and six(12%) were on propafenono (450-600 mg/day).All patients were examined hy transesophagealechocardiography. In none of the patients auricu-lar thromhi or important spontaneous echocon-trast were observed.
The protocol was completed in all 49 pa-tients. In 12 patients (24%) mild sedation (di-azepam, 5 mg IV) was administered. Sinus rhythmwas restored in all cases hy the defibrillation pro-cedure (Fig. 2).
The mean RR interval preceding the 345shocks delivered (7.0 ±1 .6 shocks/patient) was622.6 ± 216.9 ms (range 280-1320). In threeepisodes, the RR interval was < 350 ms and in two< 300 ms. The mean discomfort score for the suc-cessful shock was 3.4 ± 0.8. All the shocks wereproperly synchronized, and none provoked ven-tricular arrhythmia of any type. No complicationsoccurred, and elevated CK levels were never oh-served.
Table I.
Clinical, Intracardiac Cardioversion and Follow-up Dataof ttie Patients
Age (years)Height (cm)Weight (kg)BSA (m^)AF duration (day)LAD (mm)DLVD (mm)Shock numberTolerance scoreEnergy Volts
JouleOhms
Follow-up (days)AF recurrences
(days)
Mean
64.10168.3077.40
1.90252.4046.2053.60
7.003.40
352.008.20
51.00162.90
3.40
SD
10.009.40
14.300.20
483.306.608.201.600.80
80.303.40
11.9058.70
7.60
Range
41-81154-185110-541.51-2.24
10-292033.1-6738.0-87.5
3-112-5
150-5501.6-20.535-10440-2601-30
AF ^ atrial (ibrillation; LAD = left atrial diameter; DLVD = dia-stolic left ventricular diameter; SD = Standard Deviation.
Atrial Defibrillation Threshold (Tables I and II)
The mean shock voltage and energy necessaryto restore sinus rhythm were 352.0 ± 80.3 V(range: 150-550 V) and 8.2 ± 3.4 J (range: 1.6-20.5J), respectively, while the average impedance was51.0 ± 11.9 ohms. The ADT threshold was 9.2 ±1.7 J in the six subjects who were resistant totransthoracic shock and 8.1 ± 1.4 J in the remain-ing 43 patients (P = NS). The threshold was not re-lated to age, sex. height, body weight, presence ortype of underlying heart disease, AF duration,atrial diameter, left ventricular end-diastolic di-ameter, or presence of previous episodes of AF.
A significant direct relation was found be-tween discomfort scores and ADTs. The ADTs ofpatients reporting grade 2 (5.6 ± 2.4 J) and grade 3(7.4 ± 2.0) discomfort were both significantlylowerthanthat of the grade 4 group (10.2 ± 3.9) (P= 0.008 and 0.007, respectively). However, theADTs of patients with grade 5 discomfort were notsignificantly higher than those of the grade 4group (Fig. 3).
2644 December 1998 PACE, Vol. 21

LOW ENERGY INTRACARDIAC CARDIOVERSION
7.7 joule
i
Figure 2. Example of internal cardioversion. Chronic atrial fibrillation is converted to sinusrhythm by a 7.71 shock synchronized on the R wave.
Relationship
TTC failure (6)Heart diseases (45)Hypertension (15)Previous AF (25)Pretreated (20)Amiod pretreat (14)Propaf pretreat (6)Recurrences (21)
Between Atriai
Joules
9.2 + 1.78.3 ± 3.68.5 ± 2.67.5 ± 3.57.3 ± 2.76.1 ± 2.47.8 ± 3.67.1 ± 2.6
Table II.
Defibriliation Threshold and
Others (43)Lone AF (4)Vaivuiar disease (12)First AF (24)Not pretreated (29)Not pretreated (29)Not pretreated (29)No recurrences (28)
Principle Variables
Joules
8.1 ± 1.47.3 ± 1.97.9 ± 2.89.0 ± 3.38.9 ± 3.78.9 ± 3.78.9 ± 3.79.1 ± 3.7
P = nsP = nsP - nsP - nsP - nsP = 0.04P - nsP - 0.04
AF = atrial fibrillation: Amiod = amiodarone; Propaf = propafenone; TTC = transthoracic cardioversion.The number of patients are indicated in parentheses.
PACE, Vol. 21 December 1998 2645

SANTINI, ET AL.
10-,
9
87
uj 6
3 5O•^ 4
3
2 -
1
9.2
7,8
6,4
PROPAFENONE AMIOOARONE
Figure 3. Bar graph showing the difference in atrialdefibrillation threshold between patients not pretreatedwith antiarrhythmic drugs and those pretreated withamiodarone or propafenone. Atrial defibrillationthreshold is significantly lower in patients pretreatedwith amiodarone than in those submitted to theprocedure without a previous antiarrhythmic treatment("P = 0.04).
Antiarrhythmic Agents
On the whole, there was no significant differ-ence between the ADTs of patients who had (7.3 ±2.7 I) and had not received (9.2 ± 3.7 I) antiar-rhythmic drugs before cardioversion (LEIC) (P =NS). However, subjects pretreated with amio-darone had a significantly mean ADT than un-treated patients (6.4 + 1.8 | versus 9.2 ± 3.7 I, P =0.04) (Fig. 4). The propafenone subgroup alsoshowed a small, but nonsignificant, reduction ofthe ADT compared to the untreated patients (7.8 ±3.6 1 vs 9.2 - 3.7 1, P = NS).
Follow-up
The mean follow-up period was 162.9 ± 58.7days (range 40-260 days). All patients weretreated with antiarrhythmic drugs after the LEICprocedure.
Twenty-one recurrences (43%) were observedduring the follow-up period: 15 (71%) occurred inthe first week (early recurrences) after LEIC andthe remaining six during the first month (late re-currences). In 8 of the 15 patients with early re-currence, sinus rhythm was lost dnring the first 24hours after cardioversion.
There were no other recurrences after the firstmonth of follow-np. The recurrence rate was not
related to age, sex, height, body weight, left atriumdiameters, left ventricular end-diastolic diameter,AF duration, presence or type of underlying heartdisease, previous episodes of AF, or treatmentwith amiodarone, propafenone, or other antiar-rhythmic drugs.
Discussion
Chronic AF is often observed in patients withno previous arrhythmic episode. In fact, in our ex-perience, in several patients with stable AF, elec-trical cardioversion had never been attempted. Anumber of factors are cited to justify the conserva-tive management of these cases, including: pa-tient's age, left atrial diameter, underlying heartdisease, potential danger of electrical cardiover-sion, and particularly of general anaesthesia, andthe possible proarrhythmic effects of drugs used tomaintain sinus rhythm after electrical cardiover-sion.^ '̂̂ ^ Another reason supporting the rationalefor a conservative approach is the absence of datafrom prospective, randomized studies showing
12
1 0 -•
8
5,6
7,4
8.1
2 3 4 5
TOLERANCE(score)
Figure 4. Bar graph showing the relation between atria!defibrillation threshold and the tolerance score. Thereis a statistically significant difference in the atria!defibrillation threshold between patients with score 2and 4 (*P < 0.008} and between patients with score 3and 4 {**P < 0.0071
2646 December 1998 PACE, Vol. 21

LOW ENERGY INTRACARDIAC CARDIOVERSION
that restoration of sinus rhythm is superior to ratecontrol associated to anticoagulation. Neverthless,there is evidence that maintenance of sinusrhythm appears to he associated with significantbenefits, in terms of improved hemodynamics anda reduced risk of embolism.^'^^"^^
Transthoracic cardioversion is painful andtherefore is generally performed under generalanesthesia. Our study, in agreement with the re-sults of other studies,^^"^^ demonstrates that per-sistent long-lasting AF can be safely converted tosinus rhythm with a low energy shock deliveredendocardially, without general anesthesia.
The pain reported by the patients is variableand is generally related to the amount of energydelivered. In fact, in this study, a direct relationwas found hetween pain and shock energy, al-though in certain patients who did not tolerate theprocedure well, the pain ratings seemed very sub-jective and exaggerated with respect to the actualamount of energy used. In addition, because of theincremental protocol we used, the direct relation-ship hetween discomfort and energy levels mayalso reflect the number of shocks received. Inagreement with the information in the literatureon patient discomfort during intracardiac car-dioversion^'^'^^'^^"^' in our study, even with lowenergy shocks, some discomfort appears to be in-evitable. However, experience with the automaticimplantable defibrillator has shown that many pa-tients can tolerate as much as 30 J without anyform of sedation.
In our study, diazepam 5 mg IV was routinelyadministered to the first five patients subjected toour protocol, hut only 7 of the remaining 44(15.9%) required sedation for pain dnring the pro-cedure. It is also important to recall that the pa-tients we studied were subjected to multipleshocks of increasing energy in an attempt to definethe ADT for this group. In all probability, the painexperienced by these subjects during the proce-dure was probably to some extent cumulative, andthe patients with an ADT lower than 10 J wouldhave reported less discomfort if they had receiveda single 10 J efficient shock.
Efficacy and Safety
The intracardiac defibrillation protocol weused successfully restored sinus rhythm in all 49
of the patients treated, although significantlyhigher energy levels were required compared tothose used in paroxysmal AF,̂ *̂ and in 10 cases(20%) the ADT was > 10 1.
We found no correlation between the ADTand the duration of AF, previous episodes of AF,patient age, sex, body weight, left atrial or ventric-ular diameter, or the type of underlying disease.The threshold was, however, significantly lowerin those patients who had taken amiodarone 200mg/day for the month preceding the procedure,hut not in those who had been pretreated withpropafenone (450 mg/day). It is possihle that thepositive effects of the former drug are related to itsability to increase the atrial wavelength,^"'^^ thusreducing the number of circulating wavelets andproducing a more synchronized form of fibrilla-tion. Organization of AF has been reported to en-hance electrical defibrillation efficacy.^^ It shouldbe stressed, however, that our study populationwas small, and the effect of amiodarone on theADT was evaluated retrospectively. Our findings,therefore, need to be confirmed in larger prospec-tive randomized studies.
The intracardiac shocks were not followed byany complication. CK levels remained within nor-mal limits, and there was no evidence of pericar-dial effusion on postcardioversion echocardiogra-phy. All of the patients were discharged within afew days after the procedure, as soon as the INRvalues had returned within the therapeutic rangeand heparin could be discontinued. Oral anticoag-ulation was continued for 30 days, and there wereno embolic episodes during either the inpatient oroutpatient follow-np.
All of the shocks we administered were prop-erly synchronized with the R waves, and therewere no episodes of ventricular tachyarrhyhmia.A previous experimental study^^ has suggestedthat the risk of provoking ventricular tach-yarrhythmias with intracardiac delivery of a lowenergy, R wave synchronized shock may be in-creased when the RR interval is < 300 ms. It is notpossible to confirm this conclusion based on ourdata, since preshock RR intervals shorter than 300ms and 350 ms were present in only four of thepatients we cardioverted. Our experience does,however, confirm the safety of synchronizedshocks in the presence of RR intervals longer than300-350 ms.
PACE, Vol. 21 December 1998 2647

SANTINI, ET AL.
Recurrence of AF
Over half of the patients studied remained insinus rhythm throughout the follow-up. The AFrecurrence rate (43%) is similar to that reported af-ter transthoracic cardioversion.'^'^ All recurrenceswere observed within the first month after car-dioversion, 71% occurred within the first week,and over a third were observed within the first 24hours. This pattern is consistent with the resultsreported by Wijffels et al.^^ in the animal, suggest-ing the presence of a period of maximum instabil-ity lasting up to 4 weeks and related to tlie pres-ence of an electrical remodeling of the atria.
Unfortunately, none of the clinical parame-ters we examined appeared to be reliable predic-tors of AF recurrence, including refractoriness toexternal cardioversion. All six of the patients whohad undergone unsuccessful transthoracic car-dioversion were successfully converted in thisstudy, and four of them maintained sinus rhythmfor the duration of the follow-up. Given the ab-sence of complications observed in our popula-tion, we feel that, in most patients with persistentAF, at least one attempt should he made to elimi-nate the arrhythmia with intracardiac cardiover-sion.
Although the protocol we used was time con-suming, in clinical settings intracavitary low en-ergy cardioversion can be simplified, and the pro-cedure can generally be achieved with one or atmost two shocks. Our data show that the majorityof patients with chronic AF (and almost all ofthose who have been pretreated with amiodarone)can be converted with a single 10-J shock. More-over, the procedure can probably be further sim-plified (with respect to the methods we adoptedfor this study) by using a single lead with two sep-arate electrodes for shock delivery and the surfaceECG for synchronization. Glinical trials are nowbeing conducted with a balloon-guided catheter
(similar to a normal Swan-Ganz) with two defih-rillation coils that are positioned, respectively, inthe left pulmonary artery and right atrium.^'' Ad-ditional modifications of the shock waveform,such as reduction of peak voltage and waveformrounding,^^~^'' might also he expected to lowerADT, and, as a result, patient discomfort and se-dation requirements.
Conclusions
Persistent AF, even those forms that haveproved resistant to transthoracic cardioversion,can be successfully converted to sinus rhythmwith intracardiac transcatheter low energy defib-rillation. The technique is effective and appears tobe safe when shocks are properly synchronizedwith R waves and the preceding RR intervals are >300-350 ms. In most cases, even mild sedation isunnecessary. At this time, intracardiac low energycardioversion should be considered the treatmentof choice for chronic AF patients who are refrac-tory to transthoracic defibrillation and those forwhom general anesthesia is contraindicated orhazardous. In experienced hands, the proceduremight also be considered for first-line treatment ofpatients who are unlikely to respond to externalcardioversion (e.g.. obese subjects and those withlung disease). Finally, our experience has impor-tant implications for clinical development of im-plantable atrial defibrillators for patients withparoxysmal AF.'̂ " Our findings show, in fact, thatintracardiac defibrillation is safe and effectiveand, considering the lower atrial defibrillationthreshold of paroxysmal AF,̂ *' the shocks deliv-ered by these implanted devices can be expectedto be relatively well tolerated.
Acknowledgments: We thank InControl Inc. for supplyingus all the leads used for the study.
References
1. Boysen G, Nyboe J. Appleyard M. Stroke incidenceand risk factors for stroke in Copenhagen, Den-mark. Stroke 1988; 19:1345-1353.
2. Lake FR. Ctillen KJ, de Klerk NH, et al. Atrial fib-rillation and mortality in an elderly population.Aust N Z J Med 1989; 19:321-326.
3, Stroke prevention in atrial fibrillatinn investiga-tors. Stroke prevention in atrial fibrillation study.Final results. Circulation 1991: 84:527-539.
4. Mogensen L. Fibrillating atria: A sizeable problem,or ratber, atrial fibrillation: A striking problem. 1im Med 1993; 233:373-375.
2648 December 1998 PACE, Vol. 21

LOW ENERGY INTRAGARDIAC CARDIOVERSION
5. Wolf PA, Dawber TR, Thomas HE Jr, et al. Epi-deniiologit: assessment of chronic atrial fibrillationand tbe risk of stroke: Tbe Framingham study.Neurology 1978: 28:973-977.
6. Ezekowitz MD, Bridgers SL, James KE, et al. War-farin in ibe prevention of stroke associated withnonrbeuniatic atrial fibrillation: N EngI J Med1992; 327:1406-1412.
7. Caro JJ. Groome PA, Flegel KM. Atrial fibrillationand anticoagulation: From randomised trials topractice. Lancet 1993; 341:1381-1384.
8. Ramsay LE. Warfarin in cbronic atrial fibrilation.Lancet'l993; 341;1376-1377.
9. Orlands JR. von Herick R. Aronow WS. Haemody-namics and echocardiograms before and after car-dioversion of atrial fibrillation to sinus rbytbm.Chest 1979: 76:521-525.
10. Lau CP, Leung WH. Wong CK. et al. Hemodynam-ics of induced AF: A comparative assessment witbsinus rhythm, atrial and ventricular pacing. EurHeart 1 1990; 11:219-224.
11. Falk RH. Knowlton AA, Bernard SA, et al. Digoxinfor converting reuent-onset atrial fibrillation to si-nus rbytbm. A randomised double-blinded trial.Ann Intern Med 1987; 106:503-509.
12. Bianconi L. Boccadamo R. Pappalardo A, et al. Ef-fectiveness of intravenous propafenone for conver-sion ot atrial fibrillation and flutter of recent onset.Am J Cardiol 1989; 64:335-341.
13. Levi CF, Proto C. Combined treatment ofatrial fib-rillation witb quinidine and betablockers. Br HeartJ 1972; 34:911-917.
14. Levy S, Lacombe P, Cointe R, et al. High energytranscatbeter cardioversion of chronic atrial fibril-lation. J Am Coll Cardiol 1988; 12;514-518.
15. Cooper R, Alferness C, Smith W, et al. Internal car-dioversion of atrial defibrillation in sheep. Circu-lation 1993; 87:1673-1686.
16. Mnrgatroyd FD, Slade AKB. Sopber SM. et al. Effi-cacy and tolerability of transvenous low energycardioversion of paroxysmal atrial fibrillation inhumans. J Am Coll Cardiol 1995; 25:1347-1353.
17. Alt E. Scbmitt C. Ammer R, etaL Initial experiencewith intracardiac atrial defibrillation in patientswith chronic atrial fibrillation. PAGE 1994,17:1067-1078.
18. Kalman JM, Jones EF, Doolan L, et al. Low energyendocardial cardioversion ofatrial arrbytbmias inbumans. PACE 1995; 18:1869-1875.
19. Scbmilt C. Alt E, Plewan A, et al. Low energy in-tracardiac cardioversion after failed conventionalexternal cardioversion of atrial fibrillation. J AmColl Cardiol 1996. 28:994-999.
20. Levy S. Ricard P, Lau C, et al. Low-energy car-dioversion of spontaneous atrial fibrillation. Im-mediate and long-term results. Circulation 1997;96:253-259.
21. Levy S, Ricard P, Lau C. et al. Multicenter low-en-ergy transvenous atriai defibrillation (XADJ. Trialresults in different subsets of atrial fibrillation. JAm Coll Cardiol 1997; 29:750-755.
22. Powell AC. Garan H, McGovern BA. et al. Low en-ergy conversion of atriai fibrillation in tbe sheep. JAm Coll Cardiol 1992: 20:707-711.
23. Tang ASL. Yabe S. Wharton JM, et al. Ventriculardefibrillation using biphasic waveforms: Tbe im-portance of phasic duration. J Am Coll Cardiol1989; 13;207-214.
24. Irnich W. Optimal truncation of defibrillationpulses. PACE 1995; 18:673-688.
25. Coplen SE. Antman EM. Berlin JA, et al: Efficacyand safety of quinidine therapy for maintainenceof sinus rhythm after cardioversion. A meta-analy-sis of randomized control trials. Circulation 1990;82:1106-1116.
26. Kottkamp H. Haverkamp W. Borggrefe M. et al.Tbe role of class III antiarrhythmic drugs in atrialfibrillation. In Olsson SB, Allessie MA. CampbellR W (eds.): Atrial Fibrillation: Mechanisms and
. Tberapeutic Strategies. Armonk, NY, Futura Pub-lisbing Co., Inc. 1994, pp. 287-306.
27. Alam M, Tborstrand C. Left ventricular fimction inpatients wilb atrial fibrillation before and after car-dioversion. Am J Cardiol 1992; 69:694-696.
28. Cosselink ATM, Crijns HJ. Van Den Berg MP.Functional capacity before and after cardioversionofatrial fibrillation: A controlled study. Br Heart J1994; 72:161-166.
29. Disch DL. Greenberg ML. Holzberger PT. et al.Managing chronic atrial fibrillation; A Markov de-cision analysis comparing warfarin, quinidine,and low-dose amiodarone. Ann Intern Med 1994;120:449-457.
30. Kalman MJ, Olgin JE. Karch MR. Regional entrain-ment of atrial fibrillation in man. J CardiovascElectropbysiot 1996; 7:867-876.
31. Wang J. Bourne CW. Wang Z. Comparative mecb-anism of antiarrhythmic drug action in experi-mental atrial fibrillation. Importance of use-de-pendent effects on refractoriness. Circulation1993; 88:1030-1044.
32. Kboury DS, Assar MD, Sun H. Pharmacologic or-ganization of atrial fibrillation pattern enbanceselectrical defibrillation efficacy. PACE 1997;20:1060.
33. Ayers CM, Alferness CA, Ilina M, et al. Ventricularproarrhythmic effects of ventricular cycle lengthand sbock in a sbeep model of transvenous atrialdefibrillation. Circulation 1994; 89:413-422.
34. Levy S, Lauribe P, Dolla E, et al. A randomizedcomparison of external and internal cardioversionof chronic atrial fibrillation. Circulation 1992;86:1415-1420.
35. Wijffels MCEF. Kirchhof CJHJ. Doriand R. et al.Atrial fibrillation begets atrial fibrillation. A studyin awake chronically instrumented goats. Circula-tion 1995; 92:1954-1968.
36. Ammer R. Alt E, Ayers G. et al. Pain tbresbold forlow energy intracardiac cardioversion ofatrial fib-rillation with low or no sedation. PACE 1997;19:230-236.
PACE. Vol. 21 December 1998 2649

SANTINI, ET AL.I
37. Block M, Breithardt G. Optimizing defibrillation 39. Gonzales X, Ayers GM, Wagner GO, et al. Wave-through improved waveforms. PAGE 1995; forms to reduce peak voltages for internal atrial de-18:526-538. fibrillation. PAGE 1996; 19;696,
38. Harbinson MT, Allen JD, Imam Z, et al. Rounded 40. Hillsley RE. Whartpon MJ. Implantable atrial de-biphasic waveform reduces energy requirements fibrillators. J Gardiovasc Electrophysiol 1995,for transvenous catheter cardioversion of atrial fib- 6:634-648.rillation and flutter, (abstract) PACE 1996;19:226-229.
2650 December 1998 -• PACE. Vol. 21

Copyright © 2022 FDOKUMEN




















