
Low Energy Intracardiac Cardioversion of Persistent Atrial Fibrillation

423
rSusceptibility to Atrial Fibrillation: A Study in an Ovine
Model of Pacing-Induced Early Heart Failure^
JOHN M. POWER, B.V.Sc. PH.D., GRAHAM A. BEACOM, M.B.B.S.,CUE A. ALEERNESS, B.S.E.E./'^ JAI RAMAN. M.B.B.S.. M.MRD.,
MAURITS WUEEELS, M.D.. PH.D..** STEPHEN J. EARISH, B.SC.MED.,
LOUISE M. BURRELL. M.B.CH.B., M.D., and ANDREW M. TONKIN, M.D.
From the Department; of Mediuine. Surgery, and Public- Health and Comniunily Medicine. University of Melbourne^Melbourne, Australia; *InConirol Inc.. Redmond, Washington; and the **Departmeni of Physiology.
Cardiovascular ResearcH Institute Maastricht (CARIM). Maastricht University, Maastricht, The Netherlands
Propensity for Extrastimulus to Induce AF. Introduction: The development of suscep-tibility to atrial Hhrillation (AF) is a common consequence of many forms of cardiovasculardisease, especially heart failure. In this study we used a sheep model of pacing-induced stableearly heart failure to describe, quantify, and relate the level of susceptibility to AF to changesin structural and electropbysiologic parameters.
Methods and Results: Epicardial electrodes were implanted on the atria and right ventriclesof nine sheep. Tbe AF tbresbold, atrial vulnerability period, atrial etfective refractory period(ERP), and interatrial conduction time were examined during control and over a 6-week pe-riod of ventricular pacing at 190 beats/min. Left atrial (LA) area and left ventricular (LV)fractional sbortening were monitored using echocardiography. Tbere were significant in-creases in LA susceptibility to AF (P < 0.0003), LA area (P < 0.0002), and LA FRP400 (P <0.0002). Rate of increase in LA area was related positively to AF susceptibility (P = 0.02) andinversely to LA ERP400 (P = 0.002). LV fractional shortening decreased to approximately 50%of control value (P < O.UOOOI). No cbanges were observed in rigbt atrial electropbysiology.
Conclusion: In tbis study, susceptibility (the ability of an extrastimulus to induce AF) wasrigorously measured witbin a predetermined format. Significant relationsbips were found toexist between susceptibility, certain of tbe observed cbanges in atrial electropbysiology andstructure. (J Cardiovasc Electrophysiol, Vol. 9, pp. 423-435, April 1998)
atrial dilatalioti, atrial effective refractory period, atriat vulnerability, electrophwsiology,echoca rdiog raphy
Introduction
Long-term follow-up studies have demonstratedthat chronic atrial fibrillation (AF) may evolvethrough a phase of increasingly frequent recurrent
This study was supporleJ in pan by Naiional Health & MedicalResearch Council Grant No. y6027fi. and research grants from in-Control Inc.. ihe MSD Research Foundation, and the Austin Hos-pital Medicul Research Foundation.
Address ("or correspondence: John M. Power. B.V.Sc. Ph.D.,Dept. of Medicine, Univcrsiiy ol' Melbourne (Austin Campus).Studley^Rd.. Heidelberg, Australia. .1084. Fax: 61-3-9496-4099:E-mail:'[email protected] i
Manuscript received 3 December 1997; Accepted for publication23 February 1998.
paroxysms of the arrhythmia.' A pathophysiologicexplanation for this phenotnenon has been proposedrecently by Wijffels et al...- who demonstrated in agoat model that recunient paroxysms of AF producea progressive decrease in atrial refractory periodseventually leading to the development of chronicAF (atrial fibrillation begets atrial ftbrillation). Inpatients, the etiology of the initial atrial paroxysmsis unknown. However, in approximately two thirds^of patients, the evolution from sinus ttiythm to parox-ystnai AF and often, finally, to chronic AF occursin the setting of underlying structural heitrt disease.The pathophysiologic importance of this underly-ing substrate in the early episodes of AF and in theevolution to chronic AF has not been established.

424 Journal of Cardiovascular Electrophysiology Vol. 9. No. 4. April 1998
Dilated cai-diomyopathy is essentially a condi-tion in which there are varying degrees of en-largement of the ventricles and atria.^ The leftatrium (LA) usually is significantly enlarged.withvaluing degrees of right atrial (RA) dilatation.'^ Di-lated cardiomyopathy also is associated with a highincidence of chronic AF.' However, the relation-ship between [he pathologic evolution of this con-dition and the development of increased suscepti-bility to AF has not been characterized.
In this study, a model of dilated cardiomyopa-thy and LA dilatation (induced by rapid ventricu-lar pacing) in sheep was used to investigate the re-lationship between susceptibility to AF and someof the electrophysiologic and stmctural changesprtxluced by this model.
Methods
The protocol for this study was approved by theAnimal Welfare Committee of the Austin Hospi-tal under the guidelines published by the Na-tional Health and Medical Research Council ofAustralia.
Surgical Preparation
Nine adult sheep (weight range 45 to 55 kg)were anesthetized with propofol 2 mg/kg andventilated with halothane and oxygen. A single 3-cm incision was made iii a left intercostal space. Amodified thorascopic technique utilizing a cameraand light souixje was used {to minimize tissue traumaand subsequent pericarditis) to suture Teflon felt1.5 X 1.0 cm plaques {Bard Surgical fDavol Div.].Cran.ston, RI, USA), each containing four silverelectrodes (diameter 1.5 mm., interelectrode distance2 mm) (Fig. 1), on the lateral free wall of the LAin all nine animals and additionally on the free wallof the RA in five of the luiimais. An identical plaquewas sutured adjacent to the right ventricular (RV)apex in all animals. The electrograms generated bythis array design allowed easy discrimination be-tween stimulus artifacts and propagated responsesThe electrode leads were tunneled subcutaneouslyto the dorsum of the anima! and joined to "D" con-necters tbat were housed in small pouches on theanimiil's back. Modified extem<il pacemaker's {m(xlel588()A. Medtronic inc.. Minneapolis, MN. USA)were connected to the ventricular electrodes for therapid ventricular pacing.
Antibiotics (1 g of ampicillin and 80 mg of gen-tamicin sulfate, both given intravenously) weregiven prophylactically immediately after surgery
and for 3 days following. Flunixin meglumine (50mg IM) was given prior to surgery and postoper-atively once daily for 2 days as an analgesic andanti-inflammatory agent.
Stimulus and Recording
Bipolar atiial stimulation (monophasic, pulse du-ration 1.8 msec), amplification, and pr(x:essing ofatrial electrograms were accomplished by a custom-built i.solatcd interface/amplifier (inControI Inc.. Red-mond. WA. USA), controlled by virtual instru-mentation (Lab View software. National Instruments,Austin. TX. USA) and a Quadra 800 computer(Macintosh). Signals were viewed and digitized forrecording u.sing Chart 3.5 software with MacLab 8hardware (ADInstruments. Sydney, Australia) anda Macintosh computer (model LC 630).
Echocardiography
Serial images of the LA and left ventricle{LV) were obtained by right-sided transthoracicechociudiography under propofol anesthesia (ini-tial intravenous 2 mg/kg bolus and I to 1.5 mg/kgper hour infusion) using a 3-MHz probe and aSonos 100 unit {Hewlett-Packard, Andover. MA.USA). The planimetered LA cross sectional aieawas obtained from a unifomi long-axis view in di-astole. Tbe LA area was calculated automaticallyfrom a scrolled endocardial outline. LV fractionalshortening was detemiined in M mode from a short-axis view of the LV just below the insertion of thepapillary muscles. The images were measured in-dependently by two experienced observers and themeans of the results obtained.
RecordElectrode Diameter =1.5inm
Inter-eleclfode Distance = 2 mm
PaceElectrode Diameter =1.5mm
istance = 2 mm
Figure 1. Design of the epicardial electrode array.s used onthe left and ngtu atria and the right ventricle.

Power, ct tit. Propensity for Kxtraslimulus to Induce AF 425
Experimental Parameters
Definitiom
The following parameters were measured in theLA (n = 9) or both the LA and RA (n = 5). Theconventions of SI and Al refer, respectively, tothe paced drive stimulus and tbe resultant atrialelectrogram, and S2 to the premature stimulus andA2 to the resultant atrial deflection.
Diastolic pacing threshold
The diastolic pacing threshold (DPT) was de-termined using an SI value of 400 msec. The cur-rent strength was advanced from zero in 0.1-mAIncrements. The DPT was the lowest cunent value(mA) that resulted in consistent atrial capture.
Atrial Effective Refractory Period
The atrial effective refractory period (AERP)was the shortest S1-S2 interval that induced anA2 response. Paced cycle lengths of 400, 250,and 180 msec were used to monitor the rela-tionship between the pacing rate and AERP (rateadaptation). A stimulus strength of four times thepacing threshold was used because it has beenshown previously that, at this value, the electro-physiologic relationship between the pacing cur-rent strength and the AERP (the strength-intervalrelationship) stabilizes.'' The AERP was deter-mined by first pacing the animal through eitherthe LA or RA electrode array (the same stimu-lus and recording electrode pairs were usedthroughout the study) at a predetermined SI in-terval for 60 seconds to allow myocardial adap-tation before the introduction of a premature stim-ulus after every eighth beat. The S1-S2 cou-pling interval initially was well below the AERPand automatically incremented in 2-msec stepsuntil capture was first observed. The S1-S2 cou-pling interval at which this occurred was theAERP. At least three serial determinations weremade and averaged.
Susceptibility to AF
In this study, susceptibility to AE was definedas the potential for a single S2. of fixed pulse du-ration, equal to or greater than the AERP. to in-duce one or more seconds of AF. Two S2 param-eters were investigated: (I) variable S2 values ata current strength determined by a fixed relation-ship with the pacing threshold (atrial vulnerable
period); and (2) variable current strengths at an S2value detennined by a fixed relationship with theAERP (AF threshold).
Atrial vulnerable period: The atrial vulnerableperiod (AVP) was the pericxl greater than the AERPin which a single S2. preceded by eight SI stim-uli at either 400 (AVP4()0) or 250 (AVP250) msec(all at four times DPT), would induce > I secondof AF. The upper limit was determined by begin-ning with an initial S1-S2 coupling interval of 100to 150 msec above (he AERP. A l-second inter-val followed the S2 to allow observation of the A2and any arrhythmia that might result. This pat-tern was repeated five times (in an attempt to in-crease the sensitivity of the method) and then theS US2 interval was automatically decremented by5 msec until 1 second or more of AF was inducedor atrial capture lost. The lower limit of the AVPwas determined by beginning with an S1-S2 cou-pling of two thirds the AERP and incrementing in2-msec steps with the same sequence detailed aspreviously. The lower limit was the S1-S2 inter-val (usually coiTesponding to the AERP) that ini-tiated > I second of AF. The AVP was calculatedas the difference (msec) between the upper andlower limits. Decremental steps of 5 msec, overan interval of 100 to 150 msec (in comparison toincrements of 2 msec over an interval of .SO to 40msec), were used to minimize the differences intechnique when determining the upper and lowerlimits of the AVP. Pacing was terminated as soonas AF was obsei ved (Fig. 2).
Studies were recorded to hard disk via theMacLab system, which allowed scrutiny of eachmeasurement for minimum duration and assess-ment of the type of any anhythmia induced.
Atrial fihrillation threshold: The atrial fibrilla-tion threshold (AFT) was defined as the multipleof the DPn~ that would induce > 1 .second of AF.The SI was 400 msec and the fixed S2 intervalwas determined by the formula (AERP at 2 timesthe DPT) -J- 10%. This ensured that the S2 cap-tured at a single multiple of the DPT and yet waswithin any existing AVP. Beginning with a currentstrength equal to the DPT. the atrium was pacedfor 60 seconds and an S2 introduced, followedby a 1-.second pause. If no AF ensued, then thiswas immediately followed by four stimulus trainscomposed of eight SI and a single S2 separatedby a l-second pause. This sequence was perfoimedat current strengths of L 2. 4, 6. 8, and 10 timesthe DPT or until I or more seconds of AF was in-duced. If no AF was induced, then the AFT wasassigned a value of 10.

426 Journal of Cardiovascular Electrophysiology Vol. 9. No. 4, Aprit 1998
Non-captured S2 Sinus Beat 8 SI (400ms) Captured S2
Left Atrial ]Electrogram
Right AtrialElectrogram
Figure 2. Airial electrograms showing the method used to detennine the lower limit of the A VP400.
Rapid repetitive airial response interval
Rapid repetitive atrial responses (RRAR) are earlydepolarizations that follow a captured extrastimulus(A2). In this study (and as previously described^),they were defined as having a maximal cycle lengthof 200 msec. They usually were not conductedand were observed during the determination of (andpreceding) the upper limit of the AVP The rapidrepetitive atrial response interval (RRARI) was theperiod between the S1-S2 coupling interval that firstgenerated an RRAR and either the coupling inter-val that initiated AF (upper limit of the AVP) or theAERP (if no AVP existed) (Fig. 3).
Atrial fihrillation cycle length
The atrial fibrillation cycle length (AFCL) wasmeasured from LA and RA electrogram record-
ings using the retrieval and measurement capabil-ities of the MacLab system. It was calculated byaveraging the number of discrete RA and LA fi-brillatory activations within the same lO-secondwindow (Fig. 4). The sample windows were atleast 20 seconds after any previous atrial pacingstimulus and 15 .seconds prior to spontaneous re-version to sinus rhythm. The duration of eachepisode of AF was noted.
Interatrial conduction time
The interatrial conduction time was measuredfrom paired LA and RA electrogram recordings inFive animals. Measurements were made during si-nus rhythm (R-L) and during pacing (currentstrength four times DPT) from the LA and RA atcycle lengths of 400 and 250 msec.
Captured S2 RRR's Sinus Beat
Left AtriatElectrogram
Right AtrialElectrogram
Figure 3. Atdal electrograms showing rapid repetitive responses (RRRs) encountered during the determination of the upperlimit of the AVP400.

Power, et al. Propensity for Extrastimulus to Induce AF 427
Left AtrialElectrogram
20 local depolarizations in 2.370 s. AFCL 118 msec.
Figure 4. Left atrial electrogram illustrating the determination of the left atrial fibrillation cycle length (AFCL).
Experimental Protocol
Control
Experiments began approximately 10 days af-ter the surgical preparation. The following pa-rameters werc measured in the conscious state fromeither the LA alone or both atria; DPT. AERP400.250, and 180 at four times DPT, and AVP400. 250,and AFT400. LA diastolic area and LV fractionalshortening were determined by echocardiographyunder propofol anesthesia.
During rapid ventricular pacing
Once the electrophysiologic parameters stabi-lized (2 to 4 weeks after recovery), rapid RV asyn-chronous pacing at two times pacing threshold andcycle length of 315 Jiisec (190 beats/min) was com-menced. Electrophysiologic studies in the consciousanimals were perfoimed 24 hours after pacing com-menced and thereafter at 2- to 3-day intervals. Ven-tricular pacing ceased 15 minutes prior to the com-mencement of the studies. Echocardiographic ex-aminations were made at 7-day intervals. Pacingceased at 42 days.
Statistical Methods
Changes in the p;irameters over time were testedusing repeated measures ANOVA. Dunnett'sposthoc test was used to determine whether anysubsequent period was significantly different fromthe first period. Susceptibility to AF (defined asthe potential for AF to be induced) was analyzedby repeated measures generalized linear model
techniques to describe the relationships betweenparameters associated with susceptibility. The sig-nificance of the difference between the LA andRA ERP4(K) values were assessed using repeatedmeasures ANOVA. The comparisons betweenthe AFCL in the LA and RA were made usingpaired Me.sLs. Results are expressed as mean ± SD.P < 0.05 was considered significant.
Results
Pacing-Induced Changes in Cardiac Structure andCardiovascular Dynamics
There were no significant changes in atrial cy-cle length (535 ± 48 msec, P = 0.09) during RVpacing at 315 msec or the resting cycle iength (678± 72 msec, P = 0.94) over the period of pacing inall animals (Tahle 1). No significant relationshipexisted between the atrial cycle lengths during rapidventricular pacing and the immediate cycle length15 minutes after pacing had ceased (r- = 0.1). Dur-ing the first week of RV pacing, there was a sig-nificant decrease in the LV fractional shortening(P < 0.00001) to less than half the control value(Fig. 5A).
LA area increased significantly over the pacingperiod (P < 0.0002) (Fig. 5A). The rate of changein LA area was significantly higher in the first 2weeks of pacing (P = 0.0001) (Fig. 5B). Noepisodes of spontaneous AF were observed.
Atrial DPT
There were no significant changes in the atrialDPT over time (mean 2 ± 1.2 niA, P = 0.89).

428 Jemrnal of Cardiovascular Kleclrophysiotogy Vot. 9, No. 4. April 1998
61
o>cIt)
ort
.c(0
Tiuor
on
>-1
60
55
SO
45
40
35
30
25
20
15
10
r30
25
20 I
• 1 5
• 1 0
• 5
0)
cRJ
if 0o
40
30
20
10
•(0
CC • 1 0
0 1 2 3 4 5 6
Duration of Pacing (weeks)
Figure 5. (A) Double Y graph stiowing the effects of pacingon teft ventricular (LV) fractional stmrtening and left atriatarea. (B) Percentage daity rate of increase in left atriat(LA) area during the pacing period.
Susceptibility to AF
There was a significant relationship between theAVP4a) and the AFr4(X) (P < O.(XX)I). Mean LAsusceptibility to AE measured as the AFT400(Fig. 6A and Table 2). AVP4()0. and the AVP250(Fig. 6B and Table 3). was maximal at 2 weeks andthereafter decreased at 6 weeks of pacing to a levelgreater than the control value. The AVP4(X) iUwayswas gi^ater than the AVP250. RRARs occurred dur-ing the measurement of the AVP40(). wiih a meanRRARI value of 15 ± 4 msec {Fig. 6C). In contrast,RA susceptibility to AF during the control period(n = 4) was zero in all animals and remained sothroughout the peritxJ of rapid ventricular pacing.
Friedman et al.** found that the lower limit of theAVP was often greater than the AERP in nonnal an-imals. In susceptible animals, we found no evidenceof this "border zonc'",^ as the lower limit of atrialvulnerability at 400 or 250 msec was almost exclu-sively identical to the AERP at the same S1 drive.
• J
f Pa
cing
co
ssat
i
U
u
v ;OJ3C
—
t L
eaT
AB
L15
mse
c
a.
JIT|
.ricu
lV
eni
Olj
ouc
Dur
i
1
^ L
en;
1 C
ycle
' u
VI
>
Wee
k
1
Wee
l
_
inti
n
Rcl
Pad
OS
Pad
Rcl
Pad
Rcl
a.
Rcl
Pad
Rcl
Shee
pN
o.
o o I/-, in rj o
00 O C C ^ +1
r- C "n r i ^ O(N n r — o O>^ r O O X o
M C C — » C ^ I X O ^
ZZZZZZZZ2

Power, et at. Propensity for Extrastimulus to Induce AF 429
B
0 1 2 3 4 5 6
Duration of RV pacing (weeks)
Figure 6. (A) Relationship between left atriat AFT400 andAVP400. (B) Relationship between the left atrial vulnerableperiods determined with SJ values of 400 and 250 ms, re-spectively. (C) Relationship between the (eft atriat vutnera-bte period and the initial appearance of rapid repetitive re-sponses determined with an SI value of 400 ms. RV = rightventricular.
AERP
The mean LA ERP4(X), 250, and 180 values in-creased significantly during the pacing period (P= 0.0006, P = 0.0006. and P = 0.028, respectively,
Fig. 7 and Table 4), with the LA ERP400 valuesachieving significance at week 6. The ERP4(X) val-ues for the LA and RA remained significantly dif-ferent throughout the pacing period (P = 0.0001,Fig. 7A).
LA ERP Rate Adaptation Relationship
There was a significant increase in the rate adap-tation relationship (LA AERP400-LA AERPI80;p = 0.015) over the pacing period from a meanof 8 ± 6 msec in the pacing period of 0 to 2 weeksto 11 ± 5 seconds in the period 3 to 6 weeks.
Duration ofAF Episodes and AFCL
There were 502 AF episodes initiated duringstudies in the first week of RV pacing, mean du-ration 16 ± 15 seconds: in the second week. 468episodes of mean duration 53 ± 128 seconds; andduring the sixth week, 163 episodes of mean du-ration 79 ± 441 seconds. Of 2140 episodes of AFrecorded overall. 238 exceeded 60 seconds in du-ration. All were allowed to tenninate spontaneously.
The AFCL, when measured during episodes thatwere < 60 seconds in duration, did not signifi-cantly change over the period of pacing (P =0.6); however, the paired values for LA (133 ± 26msec) and RA (162 ± 34 msec) were sigtiificantlydifferent (P = 0.0001). The left AFCL measuredafter AF had persisted for > 5 minutes in dura-tion (90 ± 18 msec) and was significantly differ-ent than that during episodes of short duration (<60 sec) (P = 0.003).
Interatrial Conduction Time
In the five animals in which both LA and RAelectrograms were available, no significant varia-tion from control values was observed during the6 weeks of RV pacing in the interatrial conductionin either sinus rhythm (mean right-left. 19 ± 5 msec)or during pacing at 4(X) (mean right-left 66 ± 5 msec,mean left-right 75 ± 6 msec) and 250 msec (meanright-left 78 ± 5 msec, mean left-right 77 ± 8 msec).
Interparameter Relationships
There was a significant relationship betweenthe degree of susceptibility (LA AVP400 andAFT400) and the rate of change in LA area (P =0.025) but not the absolute increase in LA area(P = 0.7). There was a significant relationship be-tween rate of increase in LA area and the LA
430 Journal of Cardiovascular Elcctrophysiologj- Vi/l. 9. No. 4. April 1998
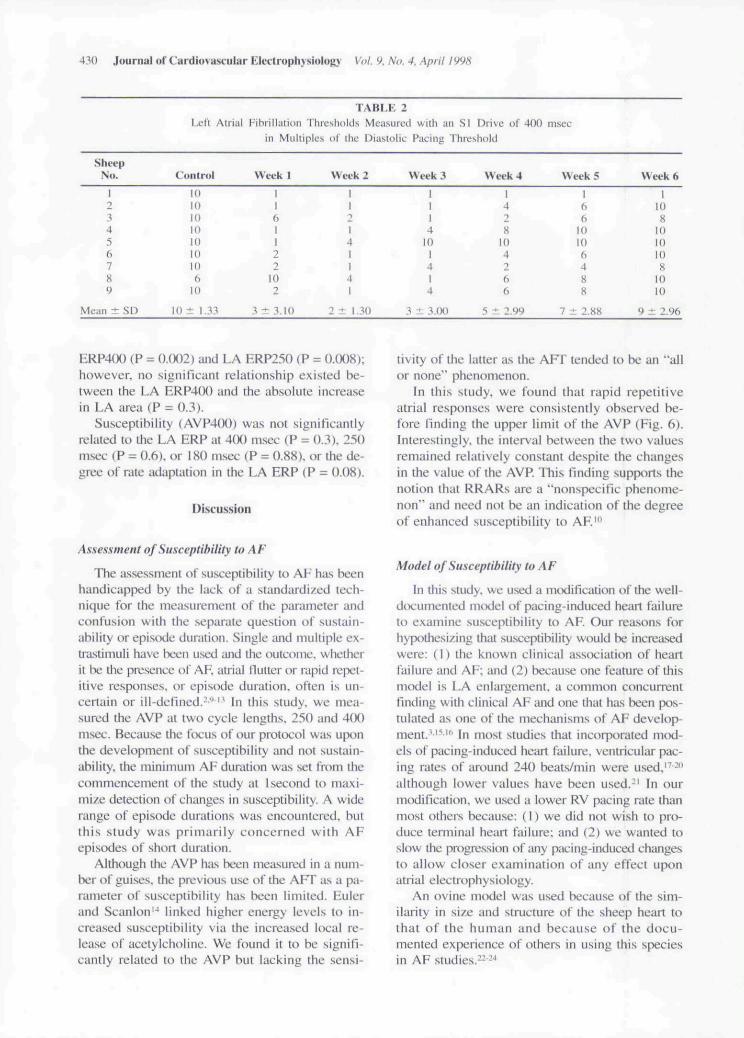
1 ABLE 2LelL Alrial Fibrillaiion I hrcslmlds Measured with an SI Drive of 4(V.) msec
in Miihiplos of Ihe DiaslnliL- Paeing Threshold
Shi-epNo. Week 1 V\ eek 2 Week 3 Week 4 Wiek 5 \ \ eek 6
Mean ± SD
lQ
to1010106
H)
10 ±
1161122
102
t 3.10
1I2141I
•4
I
2 ± 1.30
1114
Id1414
t 3.00
428
104266
5 ^ 2.99
166
10106488
7 ± 2.S8
I108
1010108
1010
9 ± 2.96
ERP400 (P = 0.0()2) and LA ERP25() (P = O.(X)8);however, no signil'icani lelationship exisied be-tween the LA ERP4(H) and the absolute increasein LA area (P = 0.3).
Susceptibility (AVP4(K)) was not significantlyrelated to the LA ERP at 400 msec (P = 0.3), 250msec (P = 0.6). or ISO msec (P = 0.88). or the de-gree of rate adaptation in the LA ERP (P = 0.08).
Discussion
Assessment of Susceptibility to AF
The assessment of susceptibility to AF has beenhandicapped by the lack of a standardized tech-nique for the measurement of the parameter andconfusion with the separate question of sustain-ability or episode duration. Single and multiple ex-ti-astimuli have been used and the outcome, whetherit be the presence of AF. atriai flutter or rapid tx iict-itive responses, or epist)dc duration, often is un-certain or ill-defined.^'^" In this study, we mea-sured the AVP at two cycle lengths, 250 and 400msec. Because the focus of our protocol was uponthe development of susceptibility and not sustain-ability, the minimum AF duration was set from thecommencement nl the study at i second to maxi-mize detection of changes in susceptibility. A widerange of episode durations was encountered, butthis study was primarily concerned with AFepisodes of short duration.
Although the AVP has been measured in a num-ber of guises, tbe previous use of the AI-T as a pa-rameter of susceptibility has been limited. Eulerand Scanlon*^ linked higher energy levels to in-creased susceptibility via the increased local re-lease of acetylcholine. We found it to be signifi-cantly related to the AVP but lacking the .sensi-
tivity of the latter as the AFT tended to he an "allor none" phenomenon.
In this study, we found that rapid repetitiveatrial responses were consistently observed be-fore finding the upper limit of the AVP (Fig. 6).Interestingly, the interval between the two valuesremained relatively constant despite the changesin the value of the AVP. This finding supports thenotion that RRARs are a "nonspecific phenome-non" and need not be an indication of the degreeof enhanced .susceptibility to AF.'"
Model of Susceptibility to AF
In this study, we used a modification of the well-documented model of pacing-induced heart failureto examine susceptibility to AF. Our reasons forhypotliesizing that susceptibility would be increasedwere: (1) the known clinical association of heartfailure and AF; and (2) becau.se one feature of thisnKxJcl is LA etilargement, a coninuHi concurrentfinding with clinical AF and one that has been pos-tulated as one of the mechanisms of AF develop-ment.'-''^"' In most studies that incorporated mtxl-els of pacing-inducetl heart failure, ventricular pac-ing rates of around 240 beats/min were used.'^ -"although lower values have been used.-' In ourmodification, we used a lower RV pacing rate thanmost others because: (1) we did not wish to pro-duce terminal heart failure; and (2) we wanted toslow the progression of any pacing-induced changesto allow closer examination of any effect uponatrial electrophysiology.
An ovine model was used because of the sim-ilarity in si/e and structure of the sheep heart tothat of the human and because of the docu-mented experience of others in using this speciesin AF studies. 2.34

Power, et al. Propensity for Extrastiniulus to Induce AF 431
250
mse
c40
0 an
d
"o
>
SI D
rid
wit
hA
BL
E 3
Mea
sure
i
1'.A
a.
/uln
erab
iL
ett ;
Wee
lee
k 5
Wee
k'
Vee
k3
i
Wee
lm
trol
0
dZa
X
250
400
250
250
400
o
250
400
250
400
s
1
Q-
u-iOOOO<NOOO
O X X ' t —
c o c o c o c o c
l e o .
mE.
730
Oo.
o
ract
Ref
ive
Ffee
t
!i!
Atr
i
170
160
150
140
130
120
110
100
90
80
A
J 11
- • — RA ERP 400
- 0 — LA ERP dDO •
T
120
110
100
90
60
B
I
—r ^1 1..
(ms)
ER
P 1
80ria
lLe
ft A
t
120
110
100
90
SO
c
-
1Duration of Pacing (weeks)
Figure 7. iA) Ttw left (IA ERP) and rigltr atriat effectiverefrucKny periods (RA ERP) determined with an SI valueof 400 ms. (B) LA ERPs determined with an SI vatue of 250ms. (C) LA ERPs determined with an SI vatue of 180 ms.
An extensive pool of published infonnation ex-ists concerning the rapid ventricukir pacing modelof heart failure in canine and ovine subjects, butnone bas documented its effects on atrial electro-physiology. Alteration of the AV interval results inincreased LA pressure and dilatation both in ex-perimental models-"* and in patients.-'' In the samemanner, the LA dilatation found in this pacing

432 Journal of Cardiovascular Electrophysiology Vot. 9, No. 4, Aprit 1998
ac
X
[ T r^ D 11O — n — +1
O—' — OOOO-OfS
i O r J C t ^ < Na ^ O O C O ^ O • 3 ^ f N
•J 00 00 — rJ Qi — 0^ r i00O^C>CT^O^CC!O^O
S +1
S +1
model most probably resulted from increased LApressure, caused by pacing-induced AV dyssyn-chrony and consequent mitral valve insufficiency.The difference betu'een the atrial (mean 113beats/min) and ventricular rate (190 beats/min) dur-ing RV pacing was well illustrated in this study.
We found that, during the control period, the in-troduction of an extrastimulus at a wide range ofSI values and energy levels failed to induce AF.We also found that enhanced susceptibility to AFwas associated with the development of pacing-induced heart failure. Just as consistently we foundthat after reaching a maximal value at 2 weeks,susceptibility decreased over the ensuing 4 weeks.This variation in the propensity to AF is an im-portant finding, a.s it highlights the apparent tran-sient nature of atrial susceptibility in parallel withongoing structural changes in the atria.
Susceptibility and Atrial Size
Atrial dilatation, especially LA dilatation, is acommon finding in patients with AF. Population-based studies have determined that LA size is notonly an independent risk factor for the presence ofboth rheumatic and nonrheumatic AF,-' but also itis inversely correlated to the percentage of patientswho remain in sinus rhythm after elective transtho-racic DC cardio version.-s LA dilatation also hasbeen cited as an important factor in the develop-ment of AF,'' '*' but others have questioned this re-lationship and bave concluded that AF may be acause of atrial dilatation rather than the reverse. - ^There are good conceptual reasons why there shouldbe a direct relationship between atrial size and thepresence of AF. Allessie et al. '* confirmed Moe'smultiple wavelet hypothesis of AF in isolated atrialpreparations and later sbowed that there was a crit-ical number of wavelets (4 to 6) above which AFpereisted. The number of wavelets is a function ofthe mass of the atria and the wavelength of im-pulse propagation. Persistence or nonpersistenceof AF therefore is a statistical probability, depen-dent on tbe replenishment of the number of fib-rillatory wavelets as offshoots of others. "
We found tbat, using our definition of suscejHtibility, the probability of an extrastimulus initiat-ing AF was not significantly related to a pacing-induced ongoing increase in LA area. Moreover,we found that toward the end of tbe 6-week pac-ing period (and consequently the largest degree ofLA dilatation), there was decreased susceptibilityto AF but an increase in AF duration. Thesefindings would appear to show a relationship be-

Power, et al. Propensity for Extra.stimulus to Induce AF 433
tween AF sustainability and LA area but throwdoubt on LA dilatation being a mechanism for en-hanced susceptibility. One explanation (not mea-sured in this study) is the possibility that the LAdilatation observed was not associated with anincrease in overall LA mass.
In this study, we did however find a signifi-cant positive relationship between the rate of LAstretch (expressed as the rate of increase in cross-sectional area) and susceptibility to AF. This find-ing equates with clinical experience where acuteincreases in LA dimensions often are associatedwith the initiation of AF.
Because there is no absolute knowledge of prop-agation pathways, the methodology used in thisstudy for measuring intra-atrial conduction time isnot as accurate as when using direct mapping tech-niques. However, the fact that in this study therewere no changes in the interatrial conduction timedespite wide changes in susceptibility must havesome significance. If there were changes in the in-tra-atrial conduction velocity, then the changes inthe conduction pathway distances would have hadto closely match changes in veUx'ity. This findingis similar to that of Wijffels et al..- who found ina goat model of chronic AF that in the days thatpreceded the development of chronic AF, i.e., short-duration AF. there was no change in interatrial con-duction velocity.
LA Size, Susceptibility, and AERP
It has been shown in a recently published studythat the development of sustained AF was ac-companied by progressive shortening of the AFRRi.e.. the concept of "atrial fibrillation begets atrialfibrillation.'"- As discussed previously, the propen-sity for persistent AF may be related to the size ofthe atria and the atrial wavelength. The wavelength(conduction velocity X refractory period) is thedistance traveled by a propagating wavelet dur-ing the duration of tlie refractoiy period. Tlie shorterthe wavelength, the greater the possible number ofreentrant circuits (and the maintenance of AF) ina given atrial mass. AERP values have been foundto be decreased during electrophysiologic studiesof AF patients and in situ studies using atrial tis-sue taken from such patients.^'' " There are con-flicting reports concerning the role that atrial di-latation may play as a possible mechanism for thisobserved decrease in AERR In this study, the meanLA ERR in the presence of ongoing LA dilatationover a period of 6 weeks, was significantly in-creased rather than decreased. Kaseda and
Zipes''' found a similar result in both acute andchronically prepared dogs. However, we did finda significant negative relationship between acutehigh rate stretch and the LA ERR This finding issimilar to the that of Ravclli and Allessie.*' whomeasured the effect of acute atrial dilatation in iso-lated perfused rabbit hearts.
We also found that there was no significant re-lationship between the LA BRP and the degreeof susceptibility to AF. It should be rememberedthat in this .study most of the AF episodes were ofshort duration. On the cK'casions when longer du-ration AF (> 3 houre) occurred, the LA ERP im-mediately after spontaneous reversion was foundto be transiently decreased and then returned toprevious values in a similar manner to that ob-served elsewhere.'
At present, no method exists to measure theatrial ERP during AF. which is believed to beclosely related to (but not equal because of thepresence of an excitable gap) the current AFCL.-The relative stability of the AERP in this studywas reflected in the lack of significant change inthe CL of short-duration AF. However, the effectof longer duration episodes upon CL (and there-fore the ERP) was clearly delineated.
Right Atrium
We. like others.^' found that the electrophysi-ology of the RA was considerably different thanthat of the LA. The RA ERP in the control pe-riod was consistently higher than that of the LAERP and was similarly affected by rapid ventric-ular pacing. However, in contrast to the LA, sus-ceptibility to AF in the RA was absent during thecontrol period and remained unchanged during the6 weeks of pacing. Evidence of the differentelectrophysiologic properties of the two atria alsowas provided by the presence in the RA of AFwith a mean CL 29 msec greater than the LA oratrial flutter present in the RA simultaneous to thepresence of AF in the LA. Unfortunately, it wasnot possible to obtain a continuous, reliable echocar-diographic record of the RA area (both trans-esophageal and transthoracic techniques were tri-aled). RA enlargement was observed at postmortem; however, this was not quantified.
Clinical Implications
In this study, we demonstrated that susceptibil-ity to AF is a measurable entity, and that it mayhave its own discrete mechanism(s) distinct from

434 Journal of Cardiovascular Electrophysiology Vot. 9. No. 4, Aprit S998
tbose proposed tor sustained AF. We have describedan animal mtxlel that could be used to study theeffects of treatment options that tiirgeted the alle-viation or prevention of susceptibility to AF. Lx>ng-tenn angiotensin-converting enzyme (ACE) inhi-bition has already been suggested for this role."*We propose that a new therapeutic window mayexist for the prevention of AF using drugs that pre-vent the {as yet unknown) changes in atrial phys-iology that are the substrate for enhanced suscep-tibility. If this could be done without directly im-pacting on cardiac electrophysiology. then theywould be free of proarrhythmia and other side ef-fects of present antiarrhythmic agents.
Limitations of the Study
This study has a number of limitations. The ex-tent of any changes in the dispersion of atrial re-fractoriness was not measured because of the lim-ited number of recording sites on the atria. A con-tinuing problem exists with chronic models inachieving a balance between the area from whichinformation is gathered by electrode implantationand any effects of the implantation per se, whichmay be related to the epicardial area in contactwith the electrodes.
All of the methods used to measure the elec-tropbysiologic parameters incorporated paced.steady-state conditions prior to introduction of theextrastimulus. In future studies, it is intended toalso incorporate measurements taken in normal si-nus rhythm because the absence of a paced drivemay yield additional information about suscepti-bility lo AF in a more physiologic state.
Acknowledgment: We wish to acknowledge ihe role of Dr. JonKalman in reviewing drafts of [his paper.
References
1. Kopecky SL. Gersh BJ, MeGoon MD, et al: The nat-ural history of lone alrial fibrillalion: A populationbased study over three decades. N Engl J Med 19S7;317:669-674,
2. Wijffels M. Kirchhof C. Dorland R. et al: Atriai flbril-lation begets atrial fibrillation—A study in awakechronically instrumented goat.s. Circulation 1993:92:1954-1968.
3. Kannel WB. Abbott RD. Savage DD, et al: Epidemio-logic features of chronic atrial fibrillation: The Fram-ingham study. N Engl J Med 1982:306:1018-1022.
4. Dec G, Fuster V: Medical progress: Idiopathic dilatedcardiomyopatby. N Engl J Med 1994:331:1564.
5. Jarvitien V. Kupari M. Poutanen V. et al: Right and leftatiial pbasic volumetric function in mildly symptomatic
dilated and hypertrophic cardiomyopalhy: Cine MRimaging assessment. Radiology 1996;198:487-495.
6. Wijffels MCEE. Kirchhof CJHJ. Dorland R. et al:Electrical remodeling due to aerial fibrillation in chron-ically instrumented conscious goats. Circulation 1997:96:3710-3720.
7. Wyndbam C. Amat-y-Leon F. Wu D. et at: Effects ofcycle length on alrial vulnerability. Circulation 1977;55:260-267.
8. Friedman H. Sinha B. Tun A. et al: Zones of atrial vul-nerability—Relationships to basic cycle length. Circu-lation 1996:94:1456-1464.
9. Centurion OA. Isomoto S. Shimizu A, et al: Supernor-mal atrial conduction and its relation to atrial vulnera-bility and atrial fibrillation in patients with sick sinussyndrome and paroxysmal atrial fibrillation. Am HeartJ 1994:128:88-95.
10. Cosio E: Atrial vulnerability. Clin Cardiol t992;l5:198-202.
11. Drago F. Turcbetta A. Calzolari A. el al: Detection ofatrial vulnerability by transesophageal atrial pacing andthe relation of symptoms in children with Wolff-Parkinson-White syndrome and in a symptomatic con-trol group. Am .1 Cardiol 1994:74:400-401.
12. Isomoto S. Shimizu A. Konoe A. et al: Effects of intra-venous verapamil on atrial vulnerability. Jpn Circ J1994:58:1-8.
13. Morillo CA. Klein GJ. Jones DL. et al: Cbronic rapidatrial pacing. Sttiictural. functional, and electrophysio-logical characteristics of a new model of sustainedatrial fibrillation. Circulation 1995:91:1588-1595.
14. Euler D. Scanlon P: Acetylcholine release by a stimu-lus train lowers atrial fibrillation threshold. Am J Phys-iol I987:87:H863-H868.
15. Caplan LR. D'Cruz I, Hier DB. et al: Atrial size, atrialfibrillation, and stroke. Ann Neurol 1986:19:158-161.
16. Dittrich HC. Erickson JS. Scbneiderman T. et al:Ecbocardiograpbic and clinical predictors for outcomeof elective cardioversion of atrial fibrillation. Am JCardiol 1989:63:193-197.
17. Armstrong PW, Moe GW. Howard RJ. et al: Structuralremodelling in beart failure: Gelatinase induction. CanJ Cardiol 1994:10:214-220.
18. Eiizpatrick M. Nichols M. Espiner E. et al: Neurohu-moral changes during the onset and offset of ovineheart failure: Role of ANP. Am J Physiol 1989:256(Heart Circ Physiol 25):H1052-H1059.
19. Moe GW. Grima EA. Howard RJ. et al: Left ventricu-lar remodelling and disparate changes in contractilityand relaxation during the development of and recoveryfrom experimental beart failure. Cardiovasc Res 1994;28:66-71.
20. Moe GW. Montgomery C. Howard RJ. et al: Left ven-tricular myocardial blood flow, metabolism, and ef-fects of treatment with enalapril: Further insights intotbe mechanisms of canine experimental pacing-in-duced beart failure. J Lab Clin Med 1993:121:294-301.
21. Redficid MM. Aarbus LL. Wright RS. et al: Cardiore-nal and neurohumoral function in a canine mode! of

Power, et at. Propensity for Extrastiniulu.s to Induce AF 435
early left ventricular dysfunction. Circulation 1993;87:2016-2022.
22. Ayers GM. Alfemess CA. IMna M. et al: Ventricularproarrhythmic effects of ventricular cycle length andshock strength in a sheep model of transvenous atrialdefibrillation. Circulation 1994:89:413-422.
23. Cooper RA. Alfemess CA. Smith WM. et al: Internalcardioversion of atrial fibrillation in sheep. Circulation1993:87:1673-1686.
24. Powell AC. Garan H. McGovern BA. et al: Low en-ergy conversion of atrial fibrillation in the sheep. J AmColl Cardiol 1992:20:707-711.
25. Leistad E, Christensen G, Ilebekk A: Significance ofincreased atrial pressure on stroke volume during atrialfibrillation in anaesthetized pigs. Acta Physiol Scand1993:149:157-161.
26. Keren G. Etzion T. Sherez J. et al: Atrial fibrillationand atrial enlargement in patients with mitral stenosis.AmHeartJ 1987;114:1146-1155.
27. Vaziri SM. Larson MCi. Benjamin FJ. ct al: Echocar-diographic predictors of nonrheumatic atrial fibrilla-tion. The Framingham Heart Study. Circulation 1994;89:724-730.
28. Reimold SC. Lamas GA, Cantillon CO. et al: Risk fac-tors for the development of recurrent atriat fibrillation:Role of pacing and clinical variables. Am Heart J1995:129:1127-1132.
29. Andersen J. Egcblad H. Abildgaard U. et al: Atrial fi-brillation and left atrial enlargement: Cause or effect'.' JIntern Med 1991:229:253-256.
30. Gosselink AT. Crijns HJ. Hamer HP. et al: Changes inleft and right atrial size after cardioversion of atrial fi-brillation: Role of mitral valve disease. J Am Coll Car-diol 1993:22:1666-1672.
31. Sanfilippo AJ, Abascal VM, Sheehan M. et al: Atrialenlargement as a consequence of atrial fibrillation. Aprospective echocardiographic study. Circulation 1990;82:792-797.
32. Van Gelder IC. Crijns HJ. Van Gilst WH, et al: De-crease of right and left atrial sizes after direct-current
electrical cardioversion in chronic atrial fibrillation.Am J Cardiol 1991:67:93-95.
33. Villecco AS. Pilati G. Bianchi G. et al: Left atrial sizein paroxysmal atrial fibrillation: Echocardiographicevaluation and follow-up. Cardiology 1992:80:89-93.
34. Allessie M. Lammers WJEP. Bonke FI. et al: Experi-mental evaluation of Moe's multiple wavelet hypothe-sis of atrial fibrillation. In Zipes D. Jalife J, eds: Car-diac Electrophysiology and Arrhythmias. Grune andStratton. New York. 1985. pp. 265-275.
35. Allessie MA. Rensma PL, Brugada J. et al: Pathophys-iology of atrial fibrillation, in Zipes DP. Jalife J. eds:Cardiac Electrophysiology: From Celt to Bedside. WBSaunders, Philadelphia. 1990. pp. 548-559.
36. Gondo N. Kumagai K. Matsuo K. et al: Electrophysio-logical properties in paroxysmal atrial fibrillation com-plicated with the Wolff-Parkinson-White syndrome:Comparison with paroxysmal atrial fibrillation alone,Cardiology 1994:84:292-297.
37. Konoe A. Fukatani M. Tanigawa M. et al: Electrophys-iological abnormalities of the atrial muscle in patientswith manifest Wolff-Parkinson-White syndrome asso-ciated with paroxysmal atrial fibrillation. PACE 1992;15:1040-1052.
38. Kumagai K. Akimitsu S. Kawahira K, et al: Electro-physiological properties in chronic tone atrial fibrilla-tion. Circulation 1991 ;84:1662-1668.
39. Kaseda S. Zipes DP: Contraction-excitation feedbackin the atria: A cause of changes in refractoriness. J AmColl Cardiol 1988:11:1327-1336.
40. Ravelli F. Allessie MA: Effects of atrial dilatation onrefractory period and vulnerability to atrial fibrillationin the isolated Langendorff-pertused rabbit heart. Cir-culation 1997:96:1686-1695.
41. Sih HJ. Berbari EJ. Zipes DP: Epicardia! maps of atrialfibrillation after linear ablation lesions. J CardiovascElectrophysiol 1997:8:1046-10.54.
42. Spach M. Starmer C: Altering the topology of gapjunctions—A major therapeutic target for atrial fibrilla-tion. Cardiovasc Res 1995:30:336-344.

Copyright © 2022 FDOKUMEN




















