
Pharmacologic Reversion of Persistent Atrial Fibrillation with Amiodarone Predicts Long-Term Sinus...
11
http://cpt.sagepub.com Pharmacology and Therapeutics Journal of Cardiovascular DOI: 10.1177/107424840100600403 2001; 6; 341 J Cardiovasc Pharmacol Ther Manuel Vaizquez Blanco Jorge Galperin, Marcelo V. Elizari, Pablo A. Chiale, Remberto Torres Molina, Rauil Ledesma, Angel O. Scapin and Sinus Rhythm: A Prospective, Multicenter, Randomized, Controlled, Double Blind Trial Efficacy of Amiodarone for the Termination of Chronic Atrial Fibrillation and Maintenance of Normal http://cpt.sagepub.com/cgi/content/abstract/6/4/341 The online version of this article can be found at: Published by: http://www.sagepublications.com can be found at: Journal of Cardiovascular Pharmacology and Therapeutics Additional services and information for http://cpt.sagepub.com/cgi/alerts Email Alerts: http://cpt.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://cpt.sagepub.com/cgi/content/abstract/6/4/341#BIBL SAGE Journals Online and HighWire Press platforms): (this article cites 29 articles hosted on the Citations © 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Pharmacologic Reversion of Persistent Atrial Fibrillation with Amiodarone Predicts Long-Term Sinus...

http://cpt.sagepub.comPharmacology and Therapeutics
Journal of Cardiovascular
DOI: 10.1177/107424840100600403 2001; 6; 341 J Cardiovasc Pharmacol Ther
Manuel Vaizquez Blanco Jorge Galperin, Marcelo V. Elizari, Pablo A. Chiale, Remberto Torres Molina, Rauil Ledesma, Angel O. Scapin and
Sinus Rhythm: A Prospective, Multicenter, Randomized, Controlled, Double Blind TrialEfficacy of Amiodarone for the Termination of Chronic Atrial Fibrillation and Maintenance of Normal
http://cpt.sagepub.com/cgi/content/abstract/6/4/341 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
can be found at:Journal of Cardiovascular Pharmacology and Therapeutics Additional services and information for
http://cpt.sagepub.com/cgi/alerts Email Alerts:
http://cpt.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cpt.sagepub.com/cgi/content/abstract/6/4/341#BIBLSAGE Journals Online and HighWire Press platforms):
(this article cites 29 articles hosted on the Citations
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from

J Cardiovasc Pharmacol Therapeut 6(4):341-350, 2001
Efficacy of Amiodarone for the Termination of Chronic AtrialFibrillation and Maintenance of Normal Sinus Rhythm:
A Prospective, Multicenter, Randomized,Controlled, Double Blind Trial
Jorge Galperin, MD,* Marcelo V. Elizari, MD, FACC,t Pablo A. Chiale, MD,tRemberto Torres Molina, MD,t Rauil Ledesma, MD,T Angel 0. Scapin, MD,§
and Manuel Vaizquez Blanco, MD, FACC,** for the GEFACA Investigators-GEMA GROUP,Buenos Aires, Argentina
Objective: We sought to assess the efficacy and safety of amiodarone for restoration andmaintenance of sinus rhythm in patients with chronic atrial fibrillation in a prospective, ran-domized, double blind trial.Background: Restoration and preservation of sinus rhythm is difficult in patients with chron-ic atrial fibrillation. The efficacy of oral amiodarone has not been conclusively established.Methods: Ninety-five patients with chronic atrial fibrillation, lasting an average of 35.6months, were randomized to either amiodarone (600 mg/d) (47 patients) or placebo (48patients) during four weeks. Nonresponders underwent electric cardioversion, and those whoreverted continued with amiodarone (200 mg/d) or placebo. End-points were successful car-dioversion and sinus rhythm maintenance.Results: Sixteen patients (34.04%) in the amiodarone group reverted within 27.28 ± 8.85days in comparison with 0% in the placebo group (P < 0.000009). The conversion rate roseto 51.72% in patients with chronic atrial fibrillation lasting less than 12 months. Twenty-eightpatients in the amiodarone group and 39 in the placebo group underwent electric cardiover-sion, which was successful in 19 patients (67.8%) of the amiodarone group and in 15(38.46%) of the placebo group (P = 0.017). Altogether, conversion was obtained in 79.54%of the amiodarone group patients and in 38.46% of the placebo group patients (P < 0.0001).During follow-up, atrial fibrillation relapsed in 13 (37.14%) of 35 patients of the amiodaronegroup within 8.84 + 8.57 months and in 12 (80%; P = 0.009) of 15 patients of the placebogroup within 2.74 ± 3.41 months.Conclusions: Oral amiodarone restored sinus rhythm in one third of patients with chronicatrial fibrillation, increased the success rate of electric cardioversion, decreased the numberof relapses and delayed their occurrence.Key words: arrhythmia, cardioversion, antiarrhythmic drugs.
Chronic atrial fibrillation (CAF), the most commonFrom the *Hospital Durand, Buenos Aires, tHospital Ramos Mej(a,
Buenos Aires, lInstituto del Coraz6n, C6rdoba, §G.E.M.A. Grupo de sustained arrhythmia, has been shown to adverselyEstudios Multicentricos Argentinos, **Hospital de Clinicas, Buenos influence the prognosis of patients affected by thisAires, Argentina. condition (1,2). Restofing and maintaining normal
This work was supported in part by GEMA and the Fundaci6n de conditio (1,) Restorin and mainain normInvestigaciones Cardiol6gicas Einthoven. sinus rhythm (SR) improves the hemodynamic perfor-Reprint requests: Jorge Galperln, MD, Lafinur 2932-8 A, Buenos mance and the functional capacity, provides relief of
Aires-1425, Argentina.Copyright 0 2001 Westminster Publications, Inc., 708 Glen Cove symptoms (3,4) and probably reduces the embolic
Avenue, Glen Head, NY 11545, USA risk.
341 © 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution.
by on February 24, 2007 http://cpt.sagepub.comDownloaded from

342 Journal of Cardiovascular Pharmacology and Therapeutics Vol. 6 No.4 2001
The likelihood of spontaneous reversion of CAF isremote, and once the arrhythmia is eliminated eitherelectrically or pharmacologically, only 25% to 30% ofcases remain in SR unless an effective pharmacologi-cal treatment is prescribed (5). Several antiarrhythmicdrugs have been tested for their ability to maintain SR,with controversial results in terms of efficacy, toler-ance, and safety. Nonrandomized studies and somerecently reported randomized trials suggested thatamiodarone can not only convert CAF (6-8), but mayalso facilitate electrical cardioversion (ECV) (9,10)and long-term maintenance of SR (7,11).We assessed the efficacy of amiodarone alone, or
associated with ECV, for reversion of CAF and pre-vention of its recurrences during a long-term follow-up. A secondary aim was to identify the factors influ-encing the success or failure of amiodarone therapy.
Methods
Patient Population
Ninety-five patients (69 men, aged 27-75 years;mean, 63.4 years) with CAF lasting from 2 months tomore than 10 years at the time of randomization(mean, 35.6 months) were included in the trial. Duringthe run-in period, the arrhythmia was documentedwith at least 3 electrocardiograms (ECGs) at rest atdifferent intervals, and its persistent character was cer-tified by a 24-hour ECG Holter monitoring.The baseline evaluation consisted of a complete
clinical examination, ECG, 24-hour ECG Holterrecording, chest radiograph, 2-dimensional echocar-diogram (2DE), and ordinary laboratory tests, includ-ing dosage of thyroid hormones.
Eleven centers in Argentina were engaged in thistrial. The ethics committee approval from each partic-ipating center was obtained. All patients wereinformed about the characteristics of the study andgave their written consent before enrollment.
Patients meeting the following criteria were exclud-ed: age older than 75 years; paroxysmal atrial fibrilla-tion (AF); acute myocardial infarction in the last 6months; PR interval less than 0.24 seconds; second orthird degree AV block in ECG recordings obtainedbefore AF occurrence unless a permanent pacemakerwas implanted; spontaneous heart rate of less than 50beats per minute; history of sinus node disease with-out implanted pacemaker; QTc interval of less than0.50 seconds; hypothyroidism or hyperthyroidism;pregnancy; impossibility to follow-up for any reason;comorbidities conditioning the short-term prognosis;
therapy with class I or class III antiarrhythmic drugs(at least 4 months without amiodarone); previoustherapy with amiodarone with history of severeadverse effects attributable to the drug; chronic atrialflutter; a left atrium diameter greater than 60 mm;severe mitral stenosis; contraindications for anticoag-ulation, and denied consent.
All patients were effectively anticoagulated forthree weeks (International Normalized Ratio between2.0 and 3.0) and then randomized to oral amiodarone(600 mg/daily) or placebo for at least four weeks (Fig.1). Patients who regained SR during this period weresubsequently treated with amiodarone (200 mg/daily)or placebo. Those who remained in AF underwentexternal ECV, with an initial shock of 200 joules.When conversion of the arrhythmia was not attained,one or two more shocks of 360 joules were applied.Patients who did not respond to the second shock of360 joules were considered refractory to external ECVand did not continue treatment. After successful ECV,patients remained in the same blinded branch, with200 mg/day of amiodarone or placebo. Antico-agulation was interrupted after a month of permanentand documented SR, except in patients requiring it(three patients with mechanical valve prosthesis).The follow-up evaluation consisted of a clinical
examination with an ECG at rest every 30 days for 3months and afterwards, every 3 months. A more com-plete evaluation, including chest radiograph, HolterECG, 2DE, ordinary laboratory tests, and thyroidfunction tests was performed at 6 month intervals, orat any time if required by the appearance of symp-toms. Follow-up was interrupted whenever a relapseofAF was observed.
Forty-seven patients were included in the amio-darone group and 48 in the placebo group. The base-line characteristics of both populations are summa-rized in Table 1, showing that the clinical featureswere similar in the two groups.
Statistical Analysis
The calculated descriptive statistics for group vari-ables were mean, standard deviation, and minimal andmaximal values. In the analysis of the difference sig-nificance, discrete values were compared by the chi-square test for proportions adapted by R.A. Fisher,and continuous values were compared by the Studentt test. Log-rank test was used for multivariate analysis.A level of P < 0.05 was assumed to be of statisticalsignificance.
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from

Amiodarone in Chronic Atrial Fibrillation * Galperin et al. 343
Results
Pharmacologic Restoration of Sinus Rhythm
Sixteen (34.04%) of the 47 patients randomized toamiodarone therapy converted to SR with the initialdose of 600 mg/d, after 27.3 ± 8.8 days. This contrast-ed with the total absence of spontaneous conversion inthe placebo group (P = 0.000009). Table 2 shows thatthe rate of conversion to SR in the amiodarone groupwas inversely related to the duration of AF, the leftatrial diameter, and the presence of valvular heart dis-ease. Thus, normal SR was regained in 51.72% of thepatients with AF lasting 12 months or less and in only5.55% of the patients with AF lasting longer (P =0.001). Sinus rhythm was restored significantly moreoften (14/19 patients, 73.68%) in patients withoutvalvular disease. Conversely, pharmacologicalrestoration of sinus rhythm was exceptional (1/14patients of the total amiodarone group, 7.14%) (P =0.025) in patients with valvular disease.
The left atrial diameter clearly influenced the rateof conversion ofAF with amiodarone. In fact, SR wasregained in 14 (45.16%) of 31 patients with left atrialdiameter of 50 mm or less and in only 2 (12.5%) outof 16 patients with a larger left atria (P = 0.025).
Age, left ventricular diastolic and systolic dimen-sions, and shortening fraction were not significantlydifferent in patients who reverted when comparedwith patients who did not. According to the results ofa multivariate analysis (log-rank test), an anteroposte-rior atrial diameter of more than 50 mm or the pres-ence of valvular disease were independent predictorsof pharmacological cardioversion failures (P < 0.05).
The Influence ofAmiodarone Upon theRate of Successful Electrical Conversion ofChronic Atrial Fibrillation
Twenty-eight of the 31 nonresponders being given adaily dose of 600 mg of amiodarone agreed to under-go external ECV, which was successful in 19 (67.8%)of them. In the placebo group, 39 out of the 48 patientsunderwent ECV, which succeeded in 15 patients(38.4%) (P = 0.017)
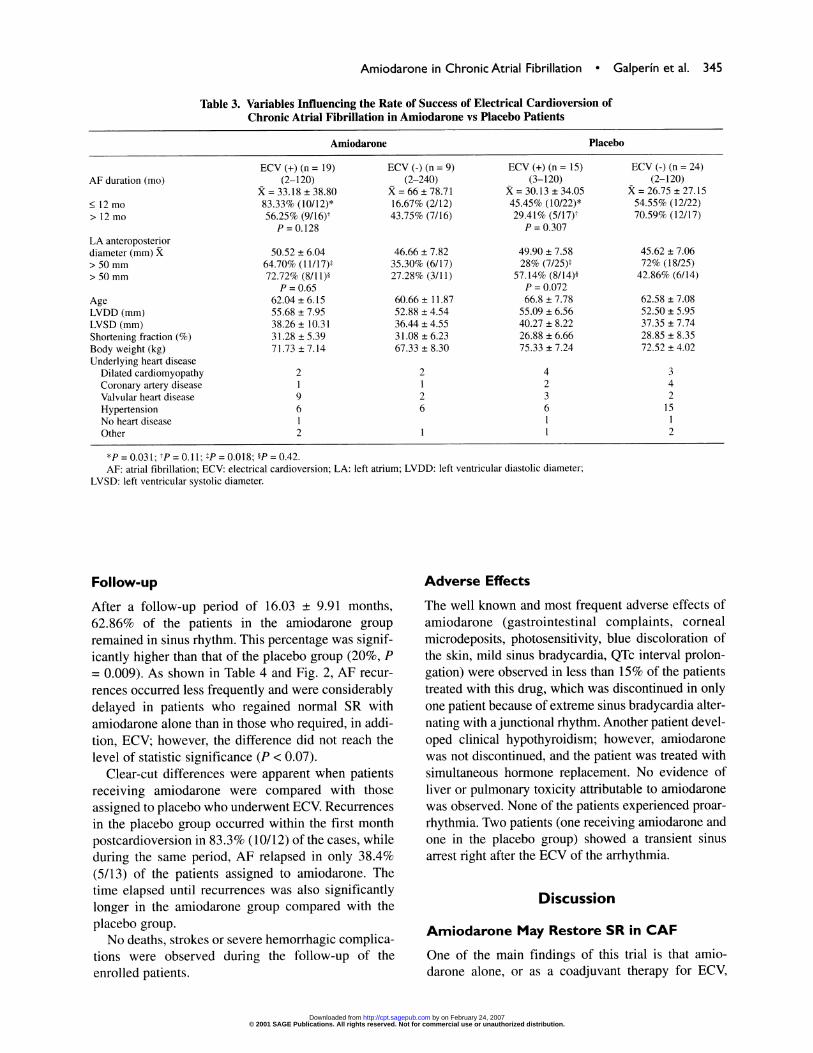
Table 3 shows that the efficacy of ECV was notrelated to any of the variables analyzed in both groups,either in univariate or in multivariate analysis. Of note,ECV was successful even in a relatively high percent-age of patients with long lasting AF and/or large leftatria (> 50 mm). Furthermore, valvular heart diseasedid not significantly affect the efficacy of ECV: 9(81.8%) of 11 patients on amiodarone therapy and 12(75%) of 16 patients in the total group converted to SR.
Anticoagulation3 weeks
Randomization
Amiodarone 600 mg/or Placebo4 weeks
Sinus Rhythm
4Amiodarone200 mg/dor Placebo
'd
Persistence ofAtrial Fibrillation
ElectricalCardioversion
Sinus Rhythm
Amiodarone 200 mg/dor Placebo
Fig. 1. Study protocol of GEFACA trial.
When we compared the results of ECV in bothgroups on the basis ofAF duration and left atrial diam-eter, some differences become apparent. In fact, in theamiodarone group, the efficacy of ECV tended to behigher (83.3%) in patients with AF lasting 12 monthsor less than in patients with AF lasting longer(56.25%) although without reaching the level for sta-tistical significance (P = 0.128). The same was veri-fied in the placebo group (45.45% vs 29.41%; P =
0.307). When comparing the amiodarone group withthe placebo group, the differences were statisticallysignificant only in patients with AF duration lasting 12months or less (P = 0.03 1). ECV was also significant-ly more effective (64.7%) in patients with an atrialdiameter of 50 mm or less under treatment with amio-darone than in those receiving placebo (28%, P =
0.018). No significant differences between bothgroups were found in patients with larger left atria.
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from

344 Journal of Cardiovascular Pharmacology and Therapeutics Vol. 6 No.4 2001
Table 1. Baseline Clinical Characteristics of Randomized Patients
Amiodarone (n = 47) Placebo (n = 48) P
Age (years) 61.63 ± 7.52 65.10 ± 5.51 0.06Sex (m/f) 30/17 39/9 0.06Etiology
Dilated cardiomyopathy 7 7Coronary artery disease 4 7Valvular heart disease 14 6 = < 0.3Arterial hypertension 22 27No structural abnormalities 4 2Other 3 1
AF duration (mo) 35.73 ± 50.77 35.52 ± 33.05 0.73LA diameter (mm) 48.46 ± 7.06 47.38 ± 6.99 0.65LV diastolic diameter (mm) 54.68 ± 7.41 53.02 ± 6.29 0.27LV systolic diameter (mm) 37.33 ± 8.54 37.83 ± 7.60 0.77Shortening fraction 31.73 ± 5.31 28.65 ± 7.07 0.08Functional capacity (NYHA) 2 ± 0.61 2.25 ± 0.68 0.68
AF: atrial fibrillation; LA: left atrium; LV: left ventricle; NYHA: New York Heart Association.
Table 2. Relationships Between Successful and Unsuccessful PharmacologicalConversion of CAF and Clinical Features
SuccessfulPhCVn = 16
UnsuccessfulPhCVn = 31
AF duration (mo)
. 12 mo-n = 29> 12 mo-n = 18LA antero-posterior diameter (mm). 50 mm-n = 31>SOmm-n= 16AgeLVDD (mm)LVSD (mm)Shortening fraction (%)Underlying cardiac disease
Dilated cardiomyopathyCoronary artery diseaseValvular heart diseaseHypertensionNo heart diseaseOther
(2-48)X = 9.54 + 13.50*
51.72% (15)t5.55% (1)t
X = 45.62 + 6.67t45.16% (14)§12.5% (2)§
60.68 ± 13.4654.57 ± 6.2736.07 ± 7.1133.90 ± 5.21
3218*831
(2-120)X = 45.25 + 55.76*
48.28% (14)94.45% (17)
X = 49.93 ± 6.91t54.84% (17)87.5% (14)62.12 ± 8.0054.74 ± 7.9737.9 ± 9.17
30.19 ± 5.20
4213**1213
*p = 0.003; tP = 0.001; tP = 0.046; §P = 0.025; **P = 0.025.AF: atrial fibrillation; LA: left atrium; LVDD: left ventricle diastolic diameter; LVSD: left ventricle
systolic diameter; PhCV: pharmacological conversion.
As shown in Fig. 3, 79.5% of patients on amio-darone therapy (35/44 cases, excluding 3 patients whorefused the ECV) converted to SR. This percentage issignificantly higher than in the patients randomized toplacebo who underwent ECV (15/39 patients, 38.4%)(P = 0.0001).The total rate of conversion to SR (pharmacological
plus electrical) in patients on amiodarone therapywhose AF lasted 12 months or less was 92.59%. Thispercentage is significantly higher than that observedin patients with a more prolonged arrhythmia (58.5%;
P = 0.006) and in patients assigned to placebo with anAF lasting 12 months or less (45%; P = 0.0002).The rate of conversion to SR during amiodarone
treatment, alone or as a pretreatment for ECV, wassignificantly higher in patients with a left atrialanteroposterior diameter of 50 mm or less than inthose of the placebo group who underwent ECV (P =0.0007). No statistical differences were foundbetween amiodarone and placebo patients having aleft atrial diameter greater than 50 mm (P = < 0.10)(Fig. 4).
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from
Amiodarone in Chronic Atrial Fibrillation * Galperin et al. 345
Table 3. Variables Influencing the Rate of Success of Electrical Cardioversion ofChronic Atrial Fibrillation in Amiodarone vs Placebo Patients
Amiodarone Placebo
AF duration (mo)
< 12 mo> 12 mo
LA anteroposteriordiameter (mm) X> 50 mm> 50 mm
AgeLVDD (mm)LVSD (mm)Shortening fraction (%)Body weight (kg)Underlying heart disease
Dilated cardiomyopathyCoronary artery diseaseValvular heart diseaseHypertensionNo heart diseaseOther
ECV (+) (n = 19)(2-120)
X = 33.18 ± 38.8083.33% (10/12)*56.25% (9/16)tP=0.128
50.52 ± 6.0464.70% (11/17)t72.72% (8/11)§
P = 0.6562.04 ± 6.1555.68 ± 7.9538.26 ± 10.3131.28 ± 5.3971.73 ± 7.14
219622
ECV (-) (n = 9)(2-240)
X = 66 ± 78.7116.67% (2/12)43.75% (7/16)
46.66 ± 7.8235.30% (6/17)27.28% (3/11)
60.66 ± 11.8752.88 ± 4.5436.44 ± 4.5531.08 ± 6.2367.33 ± 8.30
2126
ECV (+) (n = 15)(3-120)
X = 30.13 ± 34.0545.45% (10/22)*29.41% (5/17)tP = 0.307
49.90 ± 7.5828% (7/25)t
57.14% (8/14)§P = 0.07266.8 ± 7.78
55.09 ± 6.5640.27 ± 8.2226.88 ± 6.6675.33 ± 7.24
423611
ECV (-) (n = 24)(2-120)
X = 26.75 ± 27.1554.55% (12/22)70.59% (12/17)
45.62 ± 7.0672% (18/25)42.86% (6/14)
62.58 ± 7.0852.50 ± 5.9537.35 ± 7.7428.85 ± 8.3572.52 ± 4.02
34215
12
*P = 0.03 1; tP = 0.11; tP = 0.018; §P = 0.42.AF: atrial fibrillation; ECV: electrical cardioversion; LA: left atrium; LVDD: left ventricular diastolic diameter;
LVSD: left ventricular systolic diameter.
Follow-up
After a follow-up period of 16.03 ± 9.91 months,62.86% of the patients in the amiodarone groupremained in sinus rhythm. This percentage was signif-icantly higher than that of the placebo group (20%, P= 0.009). As shown in Table 4 and Fig. 2, AF recur-rences occurred less frequently and were considerablydelayed in patients who regained normal SR withamiodarone alone than in those who required, in addi-tion, ECV; however, the difference did not reach thelevel of statistic significance (P < 0.07).
Clear-cut differences were apparent when patientsreceiving amiodarone were compared with thoseassigned to placebo who underwent ECV. Recurrencesin the placebo group occurred within the first monthpostcardioversion in 83.3% (10/12) of the cases, whileduring the same period, AF relapsed in only 38.4%(5/13) of the patients assigned to amiodarone. Thetime elapsed until recurrences was also significantlylonger in the amiodarone group compared with theplacebo group.No deaths, strokes or severe hemorrhagic complica-
tions were observed during the follow-up of theenrolled patients.
Adverse Effects
The well known and most frequent adverse effects ofamiodarone (gastrointestinal complaints, cornealmicrodeposits, photosensitivity, blue discoloration ofthe skin, mild sinus bradycardia, QTc interval prolon-gation) were observed in less than 15% of the patientstreated with this drug, which was discontinued in onlyone patient because of extreme sinus bradycardia alter-nating with a junctional rhythm. Another patient devel-oped clinical hypothyroidism; however, amiodaronewas not discontinued, and the patient was treated withsimultaneous hormone replacement. No evidence ofliver or pulmonary toxicity attributable to amiodaronewas observed. None of the patients experienced proar-rhythmia. Two patients (one receiving amiodarone andone in the placebo group) showed a transient sinusarrest right after the ECV of the arrhythmia.
Discussion
Amiodarone May Restore SR in CAF
One of the main findings of this trial is that amio-darone alone, or as a coadjuvant therapy for ECV,
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from

346 Journal of Cardiovascular Pharmacology and Therapeutics Vol. 6 No.4 2001
100908070605040302010 14000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
months
* PhCV -11 ECV-Amiodarone ECV-Placebo
Fig. 2. Long term persistence of sinus rhythm after reversion of chronic atrial fibrillation(CAF) obtained by either pharmacological (PhCV) or electrical cardioversion (ECV) therapy.
Table 4. Atrial Fibrillation Relapses During Follow-up
Mean TimeRelapses Until
Relapses at Relapses at During Total RecurrencesAmiodarone 1 month 12 months Follow-up (months)
PhCVn= 16 1 2 4 (25%)* 13.87 ± 11.62ECVn= 19 4 7 9 (45%)* 6.61 ±6.47Ph+ECV n = 35 5 9 13 (37.14%)t 8.84 ± 8.57
Relapses Mean TimeRelapses at Relapses at During Total Until
Placebo 1 month 12 months Follow-up Recurrences
ECVn= 15 10 12 12(80%)t 2.74±3.41
*p= 0.07; tP = 0.009.PhCV: pharmacological cardioversion; ECV: electrical cardioversion; Ph+ECV: pharmacological
plus electrical cardioversion.
allows restoration of SR in a significant percentage ofpatients with CAF. Treatment is simple, does notrequire invasive procedures, and is carried out on an
ambulatory basis without major risks.It has been estimated that in patients with AF last-
ing longer than 48 hours, the probability of pharmaco-logical conversion to SR is around 15% to 30% (12)and that the efficacy of external ECV without con-
comitant antiarrhythmic therapy is modest (13).In our total population, the pharmacological con-
version rate of AF in the amiodarone limb was 34%,contrasting with the 0% in the placebo group.
Furthermore, the rate of conversion of AF lasting 12
months or less with amiodarone was 51.7%. This rose
to 73.68% when the arrhythmia was not associatedwith valvular heart disease.
Kochiadakis et al (8) reported that SR was restored in48.5% of 33 patients with CAF on amiodarone treat-ment but in none of the 34 patients randomized to place-bo. Although these results agree with our observations,the average duration of atrial fibrillation in Kochiadakis'patients was considerably shorter than in ours, and theseauthors combined intravenous and oral amiodarone.
Other studies reported lower conversion rates ofCAF with amiodarone, a fact that may be ascribed tothe use of low drug dosage (10,14), the presence of
U,
003raIc
4)
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from

Amiodarone in Chronic Atrial Fibrillation * Galperin et al. 347
10090807060-5040302010i0O
L
<12m
p:0.002
r>12m Total
AF Duration
Fig. 3. Duration of atrial fibrillation at randomization as a determinantfactor of success of pharmacological and electrical conversion. Whitebar: Amiodarone-Pharmacological plus electric cardioversion; Blackbar: Placebo-electric cardioversion.
76.90
<50 MM >50 MM
Left Atrial Diameter
Fig. 4. The influence of left atrium size on the rate of chronic atrialfibrillation conversion. White bar: Amiodarone-pharmacological pluselectric cardioversion; Black bar: Placebo-electric cardioversion.
heart failure (15), and probably, a particular refrac-toriness of the arrhythmia, as suggested by the factthat these patients had already been resistant to sever-
al antiarrhythmic agents (7,14,16). The rate of restora-
tion of sinus rhythm attained with amiodarone com-
pares favorably with that of quinidine (16),propafenone (17), flecainide (18), dl-sotalol (19) anddofetilide (20). Our results may be comparable to, or
even better than those obtained with ibutilide, without
its proarrhythmic effects and the need of close sur-
veillance of the cardiac rhythm during its intravenousadministration (19).
Amiodarone Improves the Rate ofSuccessful Electrical Cardioversion
Our results also confirmed previous observations indi-cating that amiodarone facilitates ECV of CAF (9,10).
0-ft0
(0)
90--80706050403020-100
a
oU)
-4-
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from

348 Journal of Cardiovascular Pharmacology and Therapeutics Vol. 6 No.4 2001
ECV was effective in 67.8% of our patients random-ized to amiodarone and the efficacy increased to83.33% in those with AF lasting 12 months or less.Conversely, the ECV restored SR in only 38.4% of ourpatients assigned to placebo.
The rate of successful electrical conversion in ourtrial compares favorably with the 59% reported byOpolski et al (21), but is lower than the 87% reportedby Capucci et al (10) or the 88% published byGosselink et at (7), who also included patients withatrial flutter. Differences in the baseline characteristicsof the studied populations could account for these dis-crepancies. All of our patients had long-lasting atrialfibrillation, no patients with atrial flutter were includ-ed, and most of them had structural heart disease. It isevident that amiodarone reduces the atrial defibrilla-tion threshold, a fact that may be of paramount impor-tance in the management of patients who may requirean implantable atrial defibrillator. This agrees with theresults of the Amiodarone in the Out-of-HospitalResuscitation of Refractory Sustained VentricularTachyarrhythmias (ARREST) Study (22) showingthat in patients suffering out-of-hospital ventricularfibrillation, intravenous amiodarone enhances the suc-cessfulness of electrical reversion when compared toplacebo. Conversely, other studies have pointed outthat amiodarone may increase the ventricular defibril-lation threshold (23,24). Reasons accounting for thesediscrepancies are unknown.
Long-Term Preservation of Sinus Rhythm
In the absence of antiarrhythmic treatment, the likeli-hood of recurrences of the arrhythmia in patients withCAF after ECV is very high. Only 20% to 30% ofpatients remain in SR within 12 months after rever-sion (5). In our trial, almost all AF relapses in theplacebo group occurred within the first month fol-lowing the successful ECV. Conversely, in patientswho regained normal SR on amiodarone therapy, therate of recurrences was considerably lower.Relapses in patients reverted with amiodarone alonewere significantly less frequent when comparedwith those that also required ECV. Moreover, thedrug delayed the reappearance of the arrhythmia.Bearing in mind that the population of the presentstudy was composed of patients with heart disease,dilated left atrium, and long-term arrhythmia, ourresults are similar or even compare favorably withprevious observations (7,11,18,21,25). Recently,Roy et al (11) also reported AF relapses of 33% aftera mean follow-up of 16 months in patients underamiodarone treatment.
A cost-effectiveness study on cardioversion andantiarrhythmic therapy of persistent AF not related tovalvular disease concluded that ECV should be theinitial strategy and recommended a further attempt attreatment with low doses of amiodarone for therelapsing patients who are at risk of ischemic stroke(26). Results of our trial suggest that this strategymight even be improved in view of the high rate ofearly relapses in patients who do not receive con-comitant antiarrhythmic therapy.
The Risk-Benefit Ratio ofAmiodarone Therapy
Restoration of SR implies several important benefits.It has been reported that conversion of CAFimproves symptoms and functional capacity(3,4,27), and prevents and corrects myocardial dam-age (15,28). However, antiarrhythmic therapy maybe associated with undesirable and even dangerousadverse effects. In a meta-analysis study by Coplenet al (5), an increase in mortality of patients treatedwith quinidine was observed. Similar results werereported in the Stroke Prevention in AtrialFibrillation (SPAF) study (29) in patients with heartfailure, most of them receiving quinidine. Otherantiarrhythmic drugs may promote life-threateningproarrhythmia, particularly in the setting of coronaryheart disease, left ventricular dysfunction, or leftventricular hypertrophy (19,20,30). In marked con-trast, several studies have demonstrated that amio-darone has a very low proarrhythmic potential, andcan be used safely in patients with structural heartdisease, even in the presence of severe ventriculardysfunction (15,31). In our trial, a low rate ofadverse effects leading to discontinuation of therapywas observed and proarrhythmia was not document-ed. However, since the follow-up was not prolongedenough, the potential for other long-term untowardeffects associated with low-dose amiodarone treat-ment cannot be ruled out.
Conclusion
Our results show that oral amiodarone is highly effec-tive for reversion of CAF and long-term maintenanceof normal SR, even in adverse conditions in whichother antiarrhythmic drugs are known to fail and maybe potentially dangerous. The remarkable efficacy ofamiodarone in conjunction with the low incidence ofsevere adverse effects renders this drug to be a first
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from

Amiodarone in Chronic Atrial Fibrillation * Galperin et al. 349
line agent for patients with long-lasting AF and struc-tural heart disease. Likewise, amiodarone therapy mayalso be considered for patients with lone AF. Webelieve that this drug is underutilized in the care ofpatients with this arrhythmia.
Appendix
GEFACA (Grupo de Estudio de Fibrilacion AuricularCon Amiodarona) INVESTIGATORS ANDCENTERS.
Dr. Jorge Galperin, Dr. Carlos Krasnov-HospitalDurand, Buenos Aires.
Dr. Remberto Torres Molina, Dr. Marcelo V. Elizari,Dr. Pablo Chiale-Hospital Ramos Mejia, BuenosAires.
Dr. Rauil Ledesma-Instituto del Corazon, Cordoba.Dr. Manuel Vaizquez Blanco-Hospital de Clinicas
Gral. San Martin, Buenos Aires.Dr. Jorge Piacentin-Hospital Lagomaggiore, Mendoza.Dr. Jorge Sanchez-Clinica San Rafael, Salta.Dr. Daniel Sirolli-Hospital Espafiol, Buenos Aires.Dr. Luis Otatti, Dr. Juan Antonio Rueda Rivas, Dra.
Lucia Buffolo-Policinico de Neuquen, Neuquen.Dra. Silvia Nota, Dra. Marisa Yolanda Martin-
Centro de Salud Leonidas Lucero, Bahia Blanca.Dr. Gustavo Casas-Hospital Irurzum, Quequen.
Acknowledgments
Amiodarone hydrochloride was
Laboratorios Roemmers, Argentina.supplied by
References
1. Kannel WB, Abbott RD, Savage DD, et al. Epidemiologicfeatures of chronic atrial fibrillation: The FraminghamStudy. N Engl J Med 306:1018, 1982
2. Benjamin EJ, Wolf PA, D'Agostino RB, et al. Impact ofatrial fibrillation on the risk of death: The FraminghamHeart Study. Circulation 98:946, 1998
3. Schimpf R, Omran H, Jung W, et al. Hemodynamic andcardiorespiratory function following internal atrial defib-rillation for chronic atrial fibrillation. Am J Cardiol83:1633, 1999
4. Atwood JE, Myers J, Sullivan M. The effect of cardiover-sion on maximal exercise capacity in patients with chronicatrial fibrillation. Am Heart J 118:913, 1989
5. Coplen SE, Antman EM, Berlin JA, et al. Efficacy andsafety of quinidine therapy for maintenance of sinus
rhythm after cardioversion: A meta-analysis of randomizedcontrol trials. Circulation 82:1106, 1990
6. Tieleman RG, Gosselink ATM, Crijins HJGM, et al.Efficacy, safety and determinants of conversion of atrialfibrillation and flutter with oral amiodarone. Am J Cardiol79:53, 1997
7. Gosselink ATM, Crijns HJ, Van Gelder IC, et al. Low doseamiodarone for maintenance of sinus rhythm after car-dioversion of atrial fibrillation or flutter. JAMA 267:3289,1992
8. Kochiadakis GE, Igoumenidis NE, Solomou MC, et al.Efficacy of amiodarone for the termination of persistentatrial fibrillation. Am J Cardiol 83:58, 1999
9. Sagrista-Sauleda J, Permanyer-Miranda G, Soler-Soler J.Electrical cardioversion after amiodarone administration.AmHeartJ 123:1536, 1992
10. Capucci A, Villani GO, Aschieri D, et al. Oral amiodaroneincreases the efficacy of direct-current cardioversion inrestoration of sinus rhythm in patients with chronic atrialfibrillation. Eur Heart J 21(1):66, 2000
11. Roy D, Talajic M, Dorian P, et al. Amiodarone to preventrecurrence of atrial fibrillation. N Engl J Med 342:913,2000
12. Jung F, DiMarco JP.Treatment strategies for atrial fibrilla-tion. Am J Med 104:272, 1998
13. Levy S. Cardioversion of chronic atrial fibrillation-towards a more aggressive approach? Eur Heart J 21:263,2000
14. Hohnloser SH, Kuck K-H, Lilienthal J, for the PIAFInvestigators. Rhythm or rate control in atrial fibrillation-Pharmacological Intervention in Atrial Fibrillation (PIAF):A randomised trial. Lancet 356:1789, 2000
15. Deedwania PC, Singh BN, Ellenbogen K, et al.Spontaneous conversion and maintenance of sinus rhythmby amiodarone in patients with heart failure and atrial fib-rillation: Observations from the Veterans AffairsCongestive Heart Failure Survival Trial of AntiarrhythmicTherapy (CHF-STAT). Circulation 98:2574, 1998
16. Zehender M, Hohnloser S, Muller B, et al. Effects ofamiodarone versus quinidine and verapamil in patientswith chronic atrial fibrillation: Results of a comparativestudy and a 2-year follow-up. J Am Coll Cardiol 19:1054,1992
17. Stroobandt R, Stiels B, Hoebrechts R. Propafenone forconversion and prophylaxis of atrial fibrillation.Propafenone atrial fibrillation trial investigators. Am JCardiol 79:418, 1997
18. Zarembski DG, Nolan PE, Slack MK, et al. Treatment ofresistant atrial fibrillation. A meta-analysis comparingamiodarone and flecainide. Arch Intern Med 155:1885,1995
19. Vos MA, Golitsyn SR, Stangl K, et al. Superiority of ibu-tilide (a new class III agent) over DL-sotalol in convertingatrial flutter and atrial fibrillation. The Ibutilide/Sotalolcomparator study group. Heart 79:568, 1998
20. Torp-Pedersen C, Moller M, Bloch-Thomsen PE, et al.Dofetilide in patients with congestive heart failure and leftventricular dysfunction. N Engl J Med 341:857, 1999
21. Opolski G, Stanislawska J, G6recki A, et al. Amiodaronein restoration and maintenance of sinus rhythm in patients
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from

350 Journal of Cardiovascular Pharmacology and Therapeutics Vol. 6 No. 4 2001
with chronic atrial fibrillation after unsuccessful direct-current cardioversion. Clin Cardiol 20:337, 1997
22. Kudenchuk PJ, Cobb LA, Copass MK, et al. Amiodaronefor resuscitation after out-of-hospital cardiac arrest due toventricular fibrillation. N Engl J Med 341:871-878, 1999
23. Guarnieri T, Levine JH, Veltri EP, et al. Success of chron-ic defibrillation and the role of the antiarrhythmic drogswith the automatic implantable cardioverter/defibrillator.Am J Cardiology 60:1061, 1987
24. Jung W, Manz M, Pizzullo, et al. Effects of chronic amio-darone therapy on the fibrillation threshold. Am JCardiology 70:1023, 1989
25. Chun SH, Sager PT, Stevenson WG, et al. Long-term effi-cacy of amiodarone for the maintenance of normal sinusrhythm in patients with refractory atrial fibrillation or flut-ter. Am J Cardiol 76:47, 1995
26. Catherwood E, Fitzpatrick WD, Greenberg ML, et al. Cost-effectiveness of cardioversion and antiarrhythmic therapy innonvalvular atrial fibrillation. Ann Intern Med 130:625, 1999
27. Gosselink ATM, Crijns HJGM, Van Den Berg MP, et al.Functional capacity before and after cardioversion ofatrial fibrillation: A controlled study. Br Heart J 72:161,1994
28. Grogan M, Smith HC, Gersh BJ, et al. Left ventricular dys-function due to atrial fibrillation in patients initiallybelieved to have idiopathic dilated cardiomyopathy. Am JCardiol 69:1570, 1992
29. Flaker GC, Blackshear JL, McBride R, et al. Anti-arrhythmic drug therapy and cardiac mortality in atrial fib-rillation. J Am Coll Cardiol 20:527, 1992
30. Echt DS, Liebson PR, Mitchell LB, et al. Mortality andmorbidity in patients receiving encainide, flecainide, orplacebo: The cardiac arrhythmia suppression trial. N EnglJ Med 324:781, 1991
31. Hohnloser S, Klingenheben T, Singh BN. Amiodarone-associated proarrhythmic effects. A review with specialreference to torsade de pointes tachycardia. Ann InternMed 121:529, 1994
© 2001 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by on February 24, 2007 http://cpt.sagepub.comDownloaded from




















