a patient with Avascular necrosis of femoral head and ...
50
An approach to a patient with Avascular necrosis of femoral head and management Dr Smarajit Patnaik Senior Consultant Orthopaedic Surgeon ApolloHospitals, Bhubaneswar.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of a patient with Avascular necrosis of femoral head and ...
AnapproachtoapatientwithAvascularnecrosisoffemoralheadandmanagementDrSmarajitPatnaik
SeniorConsultantOrthopaedicSurgeon
ApolloHospitals,
Bhubaneswar.
Avascularnecrosis
• (AVN)haslongbeenrecognizedasacomplicationoffemoralneckfractures,theusualexplanationbeingtraumaticdisruptionofthebloodsupplytothefemoralhead.
• Osteonecrosisalsoappearsasadistinctivefeatureinanumberofnon-traumaticdisorders:jointinfection,Perthes’disease,caissondisease,Gaucher’sdisease,systemiclupuserythematosus(SLE),high-dosagecorticosteroidadministrationandalcoholabuse,tomentiononlythemorecommonones.
• Whateverthecause,thecondition,onceestablished,maycometodominatetheclinicalpicture,demandingattentioninitsownright.
Aetiologyandpathogenesis
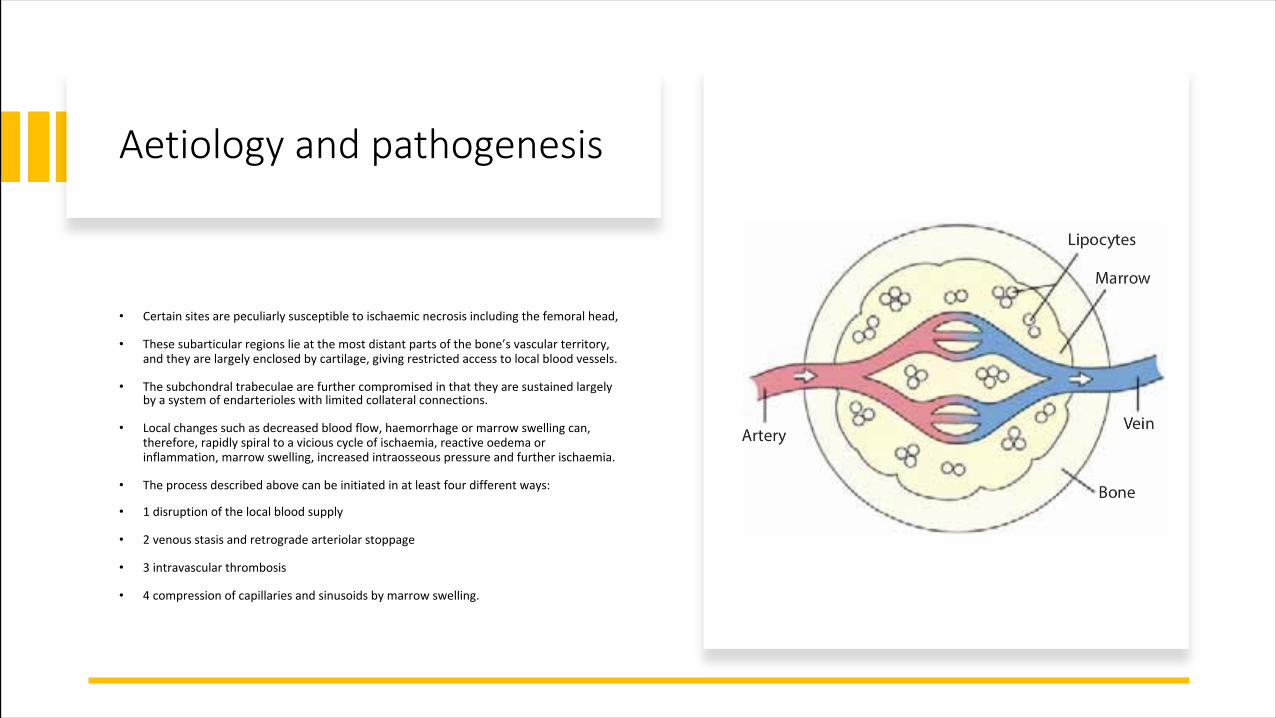
• Certainsitesarepeculiarlysusceptibletoischaemic necrosisincludingthefemoralhead,
• Thesesubarticular regionslieatthemostdistantpartsofthebone’svascularterritory,andtheyarelargelyenclosedbycartilage,givingrestrictedaccesstolocalbloodvessels.
• Thesubchondral trabeculae arefurthercompromisedinthattheyaresustainedlargelybyasystemofendarterioles withlimitedcollateralconnections.
• Localchangessuchasdecreasedbloodflow,haemorrhage ormarrowswellingcan,therefore,rapidlyspiraltoaviciouscycleofischaemia,reactiveoedema orinflammation,marrowswelling,increasedintraosseous pressureandfurtherischaemia.
• Theprocessdescribedabovecanbeinitiatedinatleastfourdifferentways:
• 1disruptionofthelocalbloodsupply
• 2venousstasisandretrogradearteriolarstoppage
• 3intravascularthrombosis
• 4compressionofcapillariesandsinusoidsbymarrowswelling.

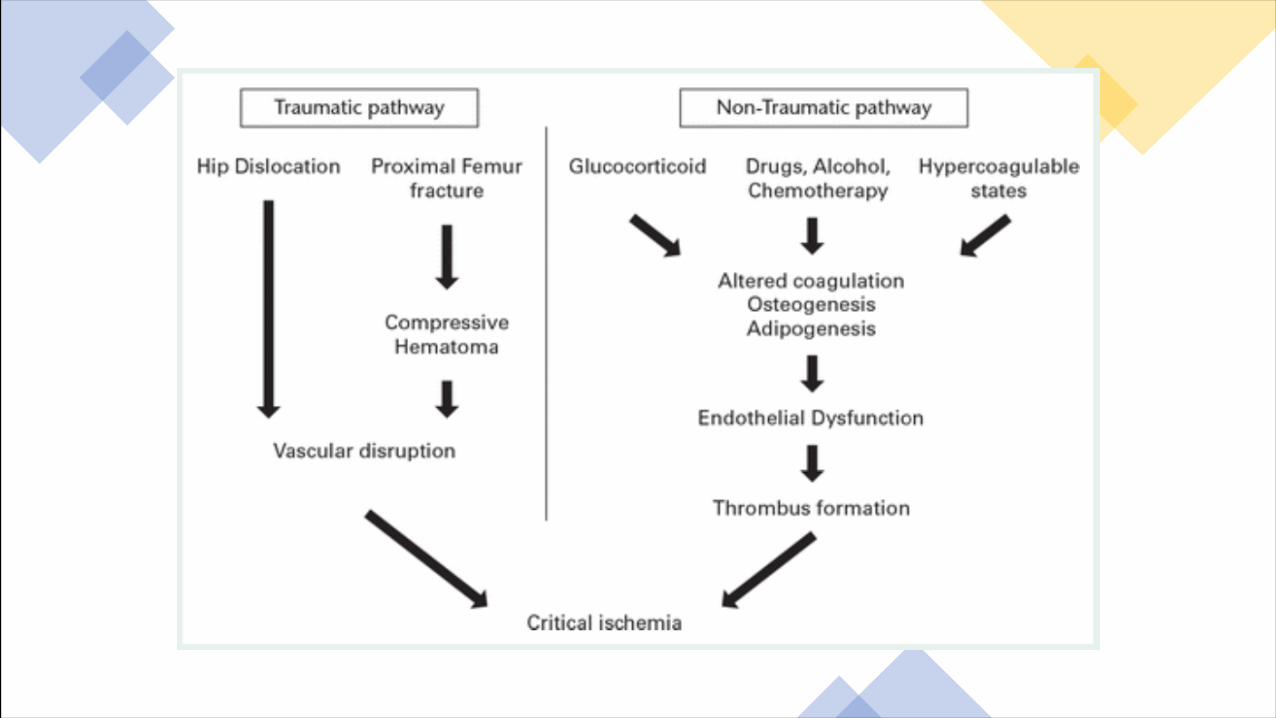
TRAUMATICOSTEONECROSIS
• Intraumaticosteonecrosisthevascularanatomyisparticularlyimportant.• Infracturesanddislocationsofthehip,theretinacular vesselssupplyingthefemoralheadareeasilytorn.If,inaddition,thereisdamagetoorthrombosisoftheligamentum teres,osteonecrosisisinevitable.• Undisplaced fracturesalsosome timesresultinsubchondral necrosis;thismaybeduetothrombosisofintraosseous capillariesorsinusoidalocclusionduetomarrowoedema.• Significantly,inthesecasesitisalwaystheproximalfragmentwhichsuffers.Thisisbecausetheprincipalvesselsenterthebonesneartheirdistalendsandtakeanintraosseous coursefromdistaltoproximal.

NON-TRAUMATICOSTEONECROSISThemechanismsherearemorecomplexandmayinvolveseveralpathwaystointravascularstasisorthrombosis,aswellasextravascularswellingandcapillarycompression.
• Intravascularthrombosis:
Over80%ofcasesareassociatedwithhigh-dosagecorticosteroidmedicationand/oralcoholabuse.Fatembolismplaysapart,givingrisetocapillaryendothelialdamage,plateletaggregationandthrombosis.
Itseemslikelythatcoagulationabnormalitiesofonesortoranotherplayatleastacontributoryroleinsomeofthedisordersassociatedwithnon-traumaticosteonecrosis.
• Extravascularmarrowswelling:
High-dosagecorticosteroidsadministrationandalcoholoverusecausefatcellswellinginthemarrow,Thereisariseinintraosseous pressure.Thisincreaseinmarrowfatvolumeinthefemoralheadisthoughttocausesinusoidalcompression,venousstasisandretrogradeischaemialeadingtotrabecularbonedeath;inotherwords,theestablishmentofacompartmentsyndrome.
Whicheverofthesemechanismsofferstheprimarypathwaytonon-traumaticboneischaemia,itisalmostcertainthatbothintravascularandextravascularfactorscomeintoplayatafairlyearlystageandeachenhancestheeffectoftheother.

Pathologyandnaturalhistory
• Bonecellsdieafter12–48hoursofanoxia,yetfordaysorevenweeksthegrossappearanceoftheaffectedsegmentremainsunaltered.
• Duringthistimethemoststrikinghistologicalchangesareseeninthemarrow:lossoffatcelloutlines,inflammatorycellinfiltration,marrowoedema,theappearanceoftissuehistiocytes,andeventualreplacementofnecroticmarrowbyundifferentiatedmesenchymaltissue.
• Asthenecroticsectorbecomesdemarcated,vasculargranulationtissueadvancesfromthesurvivingtrabeculae andnewboneislaiddownuponthedead;
• Reparativenewboneformationproceedsslowlyandprobablydoesnotadvanceformorethan8–10mmintothenecroticzone.Withtime,structuralfailurebeginstooccurinthemostheavilyloadedpartofthe necroticsegment.Usuallythistakestheformofalineartangentialfractureclosetothearticularsurface,possiblyduetoshearingstress

Clinicalfeatures• Theearlieststageofbonedeathis
asymptomatic;bythetimethepatientpresents,thelesionisusuallyadvanced.Highindexofclinicalsuspicion.
• Historyofsteroidintake,alcoholabuse,SCD.Chemotherapy,radiation.
• Painisacommoncomplaint.Itisfeltinornearajoint,andperhapsonlywithcertainmovements.Painusuallyisradiatingtoipsilateralknee.
• Somepatientscomplainofa‘click’inthejoint, probablyduetosnappingorcatchingofaloosearticular fragment.
• Inthelaterstagesthejointbecomesstiffanddeformed.
• Localtendernessmaybepresentand,
• Movementsmayberestricted;inadvancedcasestheremaybefixeddeformities.Sectoralsign.
Diagnosisoftheunderlyingdisorder
• Inmanycasesofosteonecrosisanunderlyingdisorderwillbeobviousfromthehistory:aknownepisodeoftrauma,anoccupationsuchasdeep-seadiving,afamilybackgroundofGaucher’sdiseaseorsickle-celldisease,corticosteroids,alcoholabuse.• Ideallypatientswithveryearlynon-traumaticosteonecrosis,andchildrenwithearlyPerthes’disease,shouldundergolaboratorytestsforcoagulopathies;• IncasesofsuspectedSLE,antiphospholipid anti-bodiestobemeasured.

Prevention
• Whereriskfactorsforosteonecrosisarerecognized,preventivestepscanbetakenespeciallyinthemanagement ofcorticosteroidmedicationandalcoholabuse.• Anoxiamustbepreventedinpatientswithhaemoglobinopathies.• Decompressionproceduresfordiversandcompressed-airworkersshouldberigorously applied

Earlyevidenceofdisease
RadionuclidestudiesmaybeusedforearlydiagnosisofONFH.Fromallthedifferent radionuclidemodalities,positronemissiontomography(PET)providesareal-timeimageofthebonyphysiology.ItisassumedthatPETscansdetectONevenearlierthanMRIandalsohelppredicttheprogressionofthedisease.

Radiologicalaspectsaccordingtomodality
ImagingXray
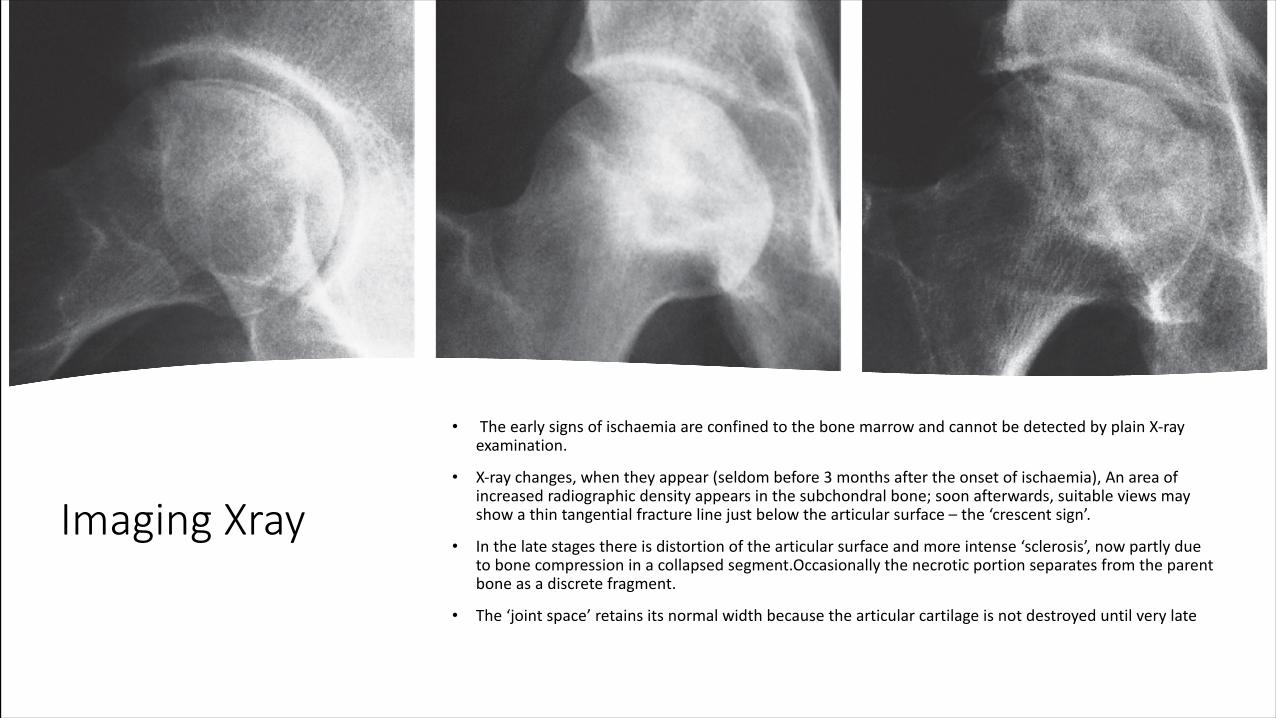
• TheearlysignsofischaemiaareconfinedtothebonemarrowandcannotbedetectedbyplainX-rayexamination.
• X-raychanges,whentheyappear(seldombefore3monthsaftertheonsetofischaemia),Anareaofincreasedradiographicdensityappearsinthesubchondralbone;soonafterwards,suitableviewsmayshowathintangentialfracturelinejustbelowthearticularsurface– the‘crescentsign’.
• Inthelatestagesthereisdistortionofthearticularsurfaceandmoreintense‘sclerosis’,nowpartlyduetobonecompressioninacollapsedsegment.Occasionallythenecroticportionseparatesfromtheparentboneasadiscretefragment.
• The‘jointspace’retainsitsnormalwidthbecausethearticularcartilageisnotdestroyeduntilverylate


• Radioscintigraphy:SCD wherea‘cold’areacontrastssignificantlywiththegenerallyhighnuclideuptakeduetoincreasederythroblasticactivity.99mTc-HDPscans(inthebonephase)mayalsoshowa‘cold’area,particularlyifalargesegmentofboneisavascular(e.g.afterfractureofthefemoralneck).Moreoften,however,thepictureisdominatedbyincreasedactivity,reflectinghyperaemiaandnewboneformationintheareaaroundtheinfarct.
• Magneticresonanceimaging:MRIisthemostreliablewayofdiagnosingmarrowchangesandboneischaemiaatacomparativelyearlystage.Thefirstsignisaband-likelow-intensitysignalontheT1weightedspinecho(SE)image(andasimilarbuthigh-intensitysignalontheshort-tauinversionrecovery(STIR)image),correspondingtotheinter- facebetweenischaemicandnormalbone.Thesite andsizeofthedemarcatednecroticzonehavebeenusedtopredicttheprogressofthelesions
• Computedtomography: CTdoesshowtheareaofbonedestructionveryclearlyanditmaybeuseful inplanningsurgery.

MRI
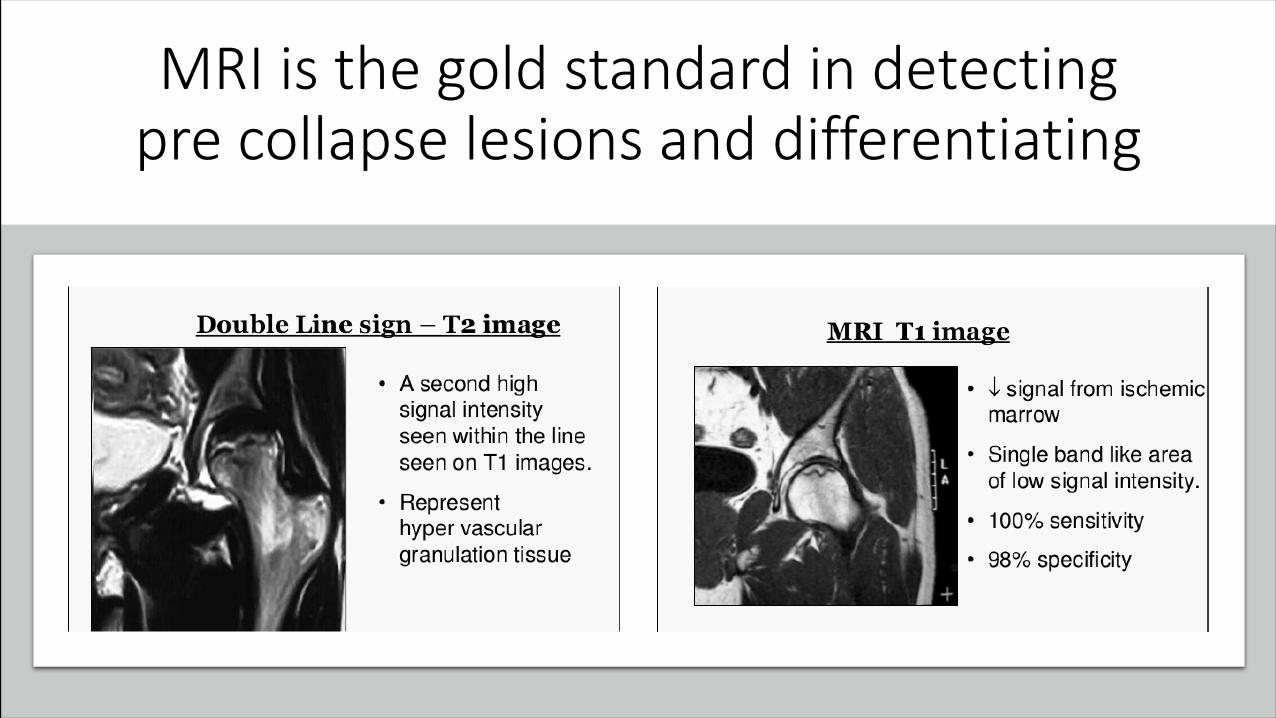
MRIisthegoldstandardindetectingprecollapselesionsanddifferentiating



SteinburgClassification

Treatment

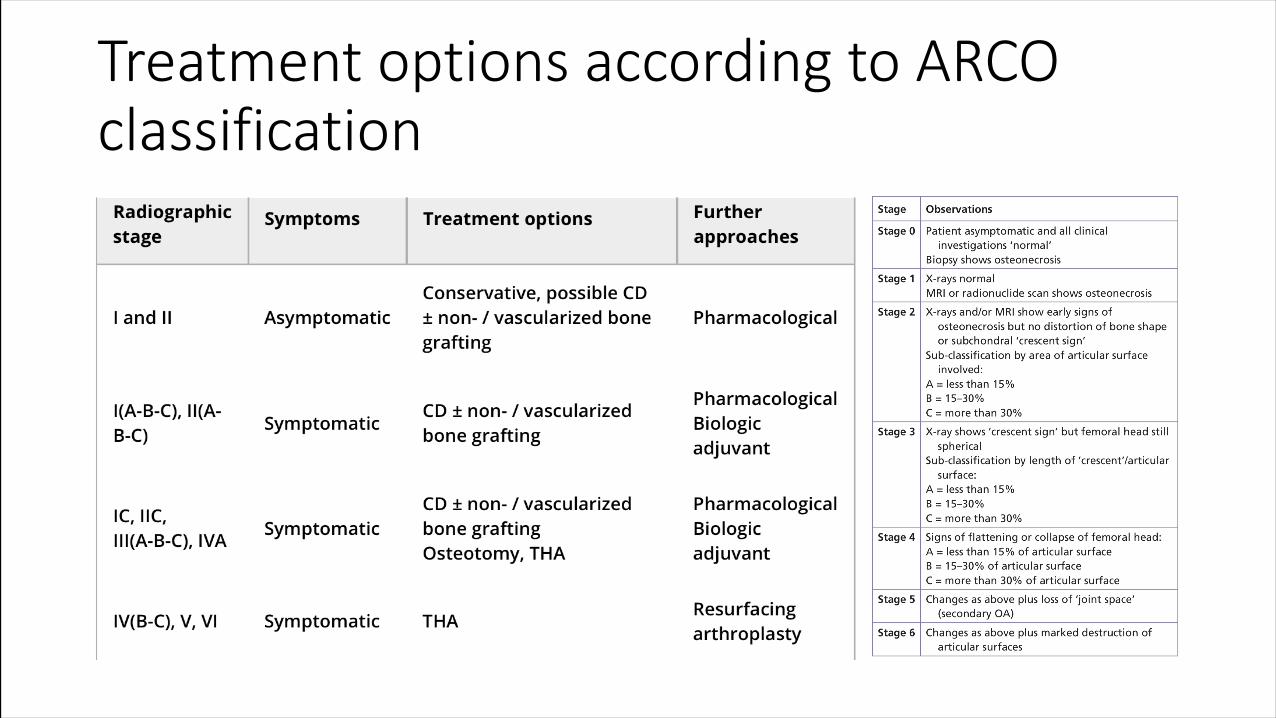
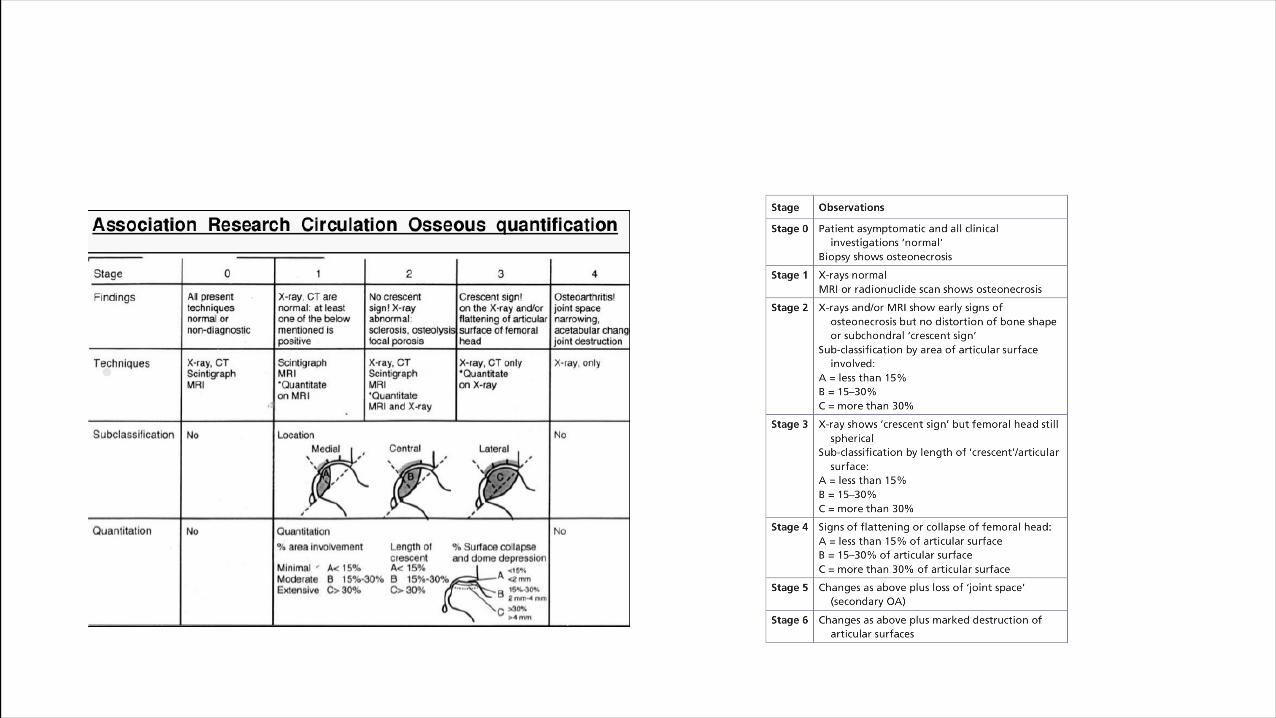
TreatmentoptionsaccordingtoARCOclassification




PRE-COLLAPSEAVN
• Pre-collapseAVNofferstheopportunityforjointpreservationandthenon-surgicalmanagementofAVNforsymptomaticornon-symptomaticpatients.Protectedweight-bearing,bisphosphonates andanti- coagulationforAVNassociatedwithhypercoagulability havebeenreportedwithvariablesuccess.
• Larger areasofAVN locatedintheweight-bearingzonewilltendtoprogressifnottreatedsurgically.Inthesurgicalmanagementofpre-collapseAVNnumerousprocedureshavebeenemployed.ThemajorityarevariationsonthethemeofpercutaneousdecompressionoftheAVNlesionaccompaniedbybonegrafting.
• Contemporarypracticealsooftenincludestheadjuvantuseofpotentialbiologicalagentssuchasconcentratedstemcells,bonemorphogeneticprotein(BMP)andplatelet-richplasma(PRP).
• Therearelimitedavailabledataontheuseofthesebiologicalagentsatthisstageandtheyhavenotbeenassessedinarandomized controltrial
• Vascularisedbonegraftshavebeenusedpreviouslybutarenowemployedlesscommonly.Thesameistrueforfemoralosteotomies.

POST-COLLAPSEAVN
• Thereisageneralconsensusthathippreservationproceduresarenotrecommendedinpost-collapseAVN.• Inthesecasesitismorejudicioustoconsidertotalhiparthroplastybecausetheresultsaremorereliable.However,itshouldbeappreciatedthathigherfailurerates,accountedforbyseveralfactors,areoftenencounteredinjointreplacementforsevereAVNofthefemoralheadcomparedwithTHAforothercausesofosteoarthritis.• Thefactorsthatofteninfluence outcomeareofthosethatweretheunderlyingcauseforAVN(e.g.previousradiotherapytohip/pelvis)andyoungpatientage.
Summaryontreatment
• Weight-bearingmodificationswhichwouldaimtoreducethejointreactiveforcestowardsthefemoralheaddidnotdelaytheprogressionofthediseaseandarethusnottobeconsideredasabeneficial• Statinsreducethebonemarrowadipocytesizeandprotectagainstcorticoid-inducedON.However,thereisnohigh-levelevidencetosupporttheroutineuseofstatinsforhigh-riskpatients.• Regardingenoxaparin,thereisnoevidenceofasuperioroutcomefrompatientsreceivingthismedicationtopreventthrombosisformationfromthosewhodonot.

• Iloprost,aprostaglandinanaloguethatcausesasystemicdilatationandinhibitsplateletaggregationinordertodecreasethebonemarrowoedema,isoftenuseful for treatment.
• Hyperbaricoxygentherapy(HBO)hasbeenpostulatedtoreversecellularischaemia andtodiminishthein"ammatory responseforthesymptomaticearlystage• bisphosphonates exertse!ects onprotectingthefemoralheadmorphology.• Extracorporealshockwavetherapy(ESWT),whichwasinitiallydevelopedforbreakingrenalstones,hasshowntoincreasethedensityofbonearoundthepelvis.

Surgicalprocedures
• Forallotherpre-collapsedlesionsandduetotheyoungageofmostpatients,femoralheadsparingproceduresareemphasized• Theseconservativeproceduresmaybedescribedasfollows:• CD;non-vascularizedbonegrafting;vascularizedbonegrafting;andproximalfemoralosteotomies.• Theevolutionofpracticehasnowadaysintegratedhumanmesenchymalcellsaswellasbonemorphogeneticproteins(BMPs)toenhancetheresultsofsurgery.• Someofthosenewapproachesconsistof:bonegraftenhancedwithmesenchymalcells;bonegraftenhancedwithBMP;anduseofporoustantalum

• TheactualrecommendationsaboutCDarethatitisamorecost-effectivechoicethanobservationalone.Itproducesbestresultsinhipswithoutevidenceofsubchondral collapseanditisthefirst linetreatmentforFicatstagesIandII.• Moreover,thereisnogeneralconsensusconcerningtheuseofnon-vascularizedbonegrafting.Still,someauthorsadvocateitsusewhenthereis<2mmofheaddepressionand<30%ofheadinvolvement.• VascularisedfibulaegraftmightbeasupplementaltechniquefollowingCDfailureandmaybeusedtotreatACROstagesIandIIorACROIIIwithminimalcollapseandsmallsizelesions.Thearticularcollapseshallbe<3mmandtheinvolvementofthefemoralhead shallnotbe>50%
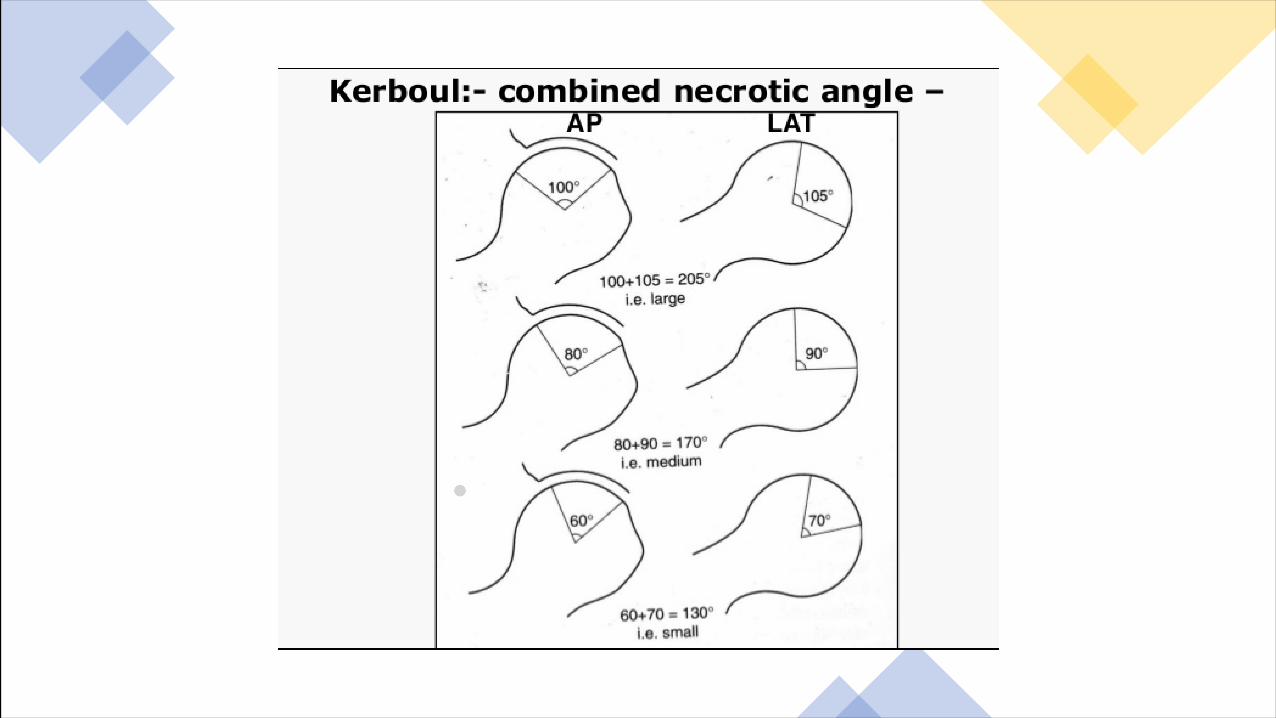
• Varus- andvalgus-producing osteotomieswereaimedtoimprovejointcongruityandtoredistributetheweight-bearingloadacrossthefemoralheadtoalessaffected area.• Theanterolaterallesionsofthefemoralheadneedavalgus-"exionosteotomyinordertotransfertheweightmediallyandposteriorly• Themediallesionswillbetreatedwithavarus osteotomybutthereisthenaneedtopreservethelateralcolumnofthefemoralheadandthepatientshallkeep>30° ofadduction.• Recommendationsforproximalfemoralosteotomyconcernpatientsthatareaged<40years,ACROstageIIandIII,thathaveacombinedKerboulangleof<200°,noacetabularpathologyandanormalhiprangeofmotion.

Novelstrategies
Novel strategiesconcernessentiallymodifications ofCDtechniquesthatincludetheuseofosteo-inductive andosteogenicfactors.Inthatsense,adjunctionofmesenchymalstemcells(MSCs)ortheuseofBMPhasbeenstudied.New implantssuchasporoustitaniumrods,believedtostimulateboneingrowth,havebeendevelopedandimplanted.
Questionandanswers
ItisimportanttounderstandthatOsteonecrosisisbyitselfadifferentialdiagnosisforvariousdisordersnearlyallof whichproducesecondaryosteoarthritis,howeverthedevelopmentofheaddeformityisanearlyfindingwithOsteonecrosiswithcharacteristicprogression.Thedeformitiesarenotcharacteristicandwithdevelopmentofsecondaryosteoarthritisthemovementsarealsolostearly!Soasarulealwaystrytogivethediagnosisasa differentialdiagnosisandbesafe.

Whatisyourdifferentialdiagnosis?
• Typicaldifferentialdiagnosesinclude:• 1.Tuberculosisofhip:(OldcasesofOsteonecrosisonlywithrestrictionofmostmovements)• 2.Transientosteoporosisofhipinfemales.• 3.Primaryosteoarthritisofhip(oncetheosteoarthriticchangesdevelopinOsteonecrosis):deformityofheadandsectoralsignsabsent.• 4.OldPerthes disease,femoralheaddeformityduetoepiphyseal/otherdysplasiawithdevelopmentofsecondaryosteoarthritis.• 5.OldFemoralheadfracturewithsecondaryosteoarthritis.• 6.Monoarticular rheumatoidisassuchrareandifmentionedthenshouldbelastasitisadiagnosisofexclusion!
WhydoyoukeepOsteonecrosisasyourfirstdifferential?• History:• Singlejointinvolvement• Insidiousonset,slowprogression• Characteristic course• No constitutionalsymptoms• Deformities donotmatchwithstagingofTBhip(viz.eveninstageIIIthemovementsarefairlypreserved)• Nohistoryoftrauma

WhichsignshowslossofintegrityoffemoralheadTheintegrityofthefemoralheadallowsdefining pre- versuspost-collapselesionsandiftheintegrityislostduetomechanicalfailurethe‘crescentsign’ willappear
WhodescribedthepredictabilityofnecroticangleThesizeofthelesionalsohelpstopredicttheoutcomeasdescribedbyKerboul, whomeasuredthenecroticanglevalueseenoncoronalandsagittalviews.Inanotherpublication,37hipsweremeasuredanditwasdemonstratedthatallhipswithavalueof240° ormorecollapsed,allhipswithavalue<180° survivedand4/8hipsbetween190 and240degreescollapsed.

Howdoyoudefinefemoralheaddepression
Afemoralheaddepressionisdescribedwhenthereisachangeinthefemoralheadcontourof>2mmwhichmayleadtoaworseprognosis.
AcetabularaffectioninMRIcanwepreserveaprecollapsedheadInaddition,iftheMRIshowsanimplicationoftheacetabularwall,thetreatmentsforfemoralheadsavingshavebeendemonstratedtobeunsuccessful
WhichMRIfindingisassociatedwithworseclinicalprogressionAppearance ofboneoedema onMRIiscorrelatedwithworseningofhippain.