
Fractionated Grid Therapy in Treating Cervical Cancers: Conventional Fractionation or...
9
PHYSICS CONTRIBUTION FRACTIONATED GRID THERAPY IN TREATING CERVICAL CANCERS: CONVENTIONAL FRACTIONATION OR HYPOFRACTIONATION? HUALIN ZHANG,PH.D,* JIAN Z. WANG,PH.D.,* NINA MAYR, M.D.,* XIANG KONG, M.SC.,* JIANKUI YUAN,PH.D.,* NILENDU GUPTA,PH.D.,* SIMON LO, M.D.,* JOHN GRECULA, M.D.,* JOSEPH MONTEBELLO, M.D.,* DOUGLAS MARTIN, M.D.,* AND WILLIAM YUH, M.D. y Departments of *Radiation Medicine and y Radiology, The Ohio State University, Columbus, OH Purpose: To evaluate the conventionally fractionated and hypofractionated grid therapy in debulking cervical cancers using the linear quadratic (LQ) model. Methods and Materials: A Monte Carlo technique was used to calculate the dose distribution of a commercially available grid in a 6-MV photon beam. The LQ model was used to evaluate the therapeutic outcome of both the conventionally fractionated (2 Gy/fraction) and hypofractionated (15 Gy/fraction) grid therapy regimens to debulk cervical cancers with different LQ parameters. The equivalent open-field dose (EOD) to the cancer cells and therapeutic ratio (TR) were defined by comparing grid therapy with the open debulking field. The clinical outcomes from 114 patients were used to verify our theoretical model. Results: The cervical cancer and normal tissue cell survival statistics for grid therapy in two regimens were cal- culated. The EODs and TRs were derived. The EOD was only a fraction of the prescribed dose. The TR was de- pendent on the prescribed dose and the LQ parameters of both the tumor and normal tissue cells. The grid therapy favors the acutely responding tumors inside radiosensitive normal tissues. Theoretical model predictions were consistent with the clinical outcomes. Conclusions: Grid therapy provided a pronounced therapeutic advantage in both the hypofractionated and con- ventionally fractionated regimens compared with that seen with single fraction, open debulking field regimens, but the true therapeutic advantage exists only in the hypofractionated grid therapy. The clinical outcomes and our study indicated that a course of open-field radiotherapy is necessary to control tumor growth fully after a grid therapy. Ó 2008 Elsevier Inc. Grid therapy, Monte Carlo, Hypofractionation, Therapeutic ratio, Cervical cancer. INTRODUCTION Intensity modulation in radiotherapy has been studied for decades (1–3). The improved normal tissue sparing pro- vided by intensity modulated fields and new techniques such as multileaf-collimator (MLC)-based, intensity modu- lated radiotherapy (IMRT) have greatly enhanced the use of intensity-modulated beams (4–7). Of the various IMRT techniques, grid modulated, or spatially fractionated radio- therapy, has been recognized as an important and easy- to-use technique for debulking tumors (8–12). Unlike the MLC-based IMRT in which dose delivery is time- and space-dependent, grid-modulated radiotherapy is only space- dependent. Grid therapy takes advantage of the better repair capability of normal tissues. Underdosed areas serve as re- growth centers for normal tissues, thus reducing radiation complications. Some authors have described the dosimetric characteristics of grid therapy. Reiff et al. (13) measured depth dose curves and peak-to-valley ratios of megavoltage grid therapy in a water phantom for various field sizes of a square pattern grid. Trapp et al. (14) measured three-dimensional dose distributions of grid-collimated photon fields using gels. Ha et al. (15) studied the feasibility of grid therapy delivery using an MLC. Meigooni et al. (16, 17) measured the dose distributions of 6-MV and 18- MV photon beams modulated by a hexagonal grid using films, thermoluminescent dosimeters, and an ion chamber in water. Zhang et al. (18) derived two-dimensional (2D) dose distribu- tions of 6-MV grid therapy with the Monte Carlo (MC) simu- lations, extended dose range (EDR2) films in solid water phantom, and an ion chamber in water scanning system. As the dosimetric properties of grid therapy have become clearer, some authors have switched their attention from dosi- metric issues to radiobiological effects. Zwicker et al. (19) first Reprint requests to: Hualin Zhang, Ph.D., Department of Radia- tion Medicine, The Ohio State University, 300 West 10th Avenue, Columbus, OH 43210-1228. Tel: (614) 293-7497; Fax: (614) 293- 4044; E-mail: [email protected] Conflict of interest: none. Acknowledgment—The authors thank David E. Carpenter of the Ohio State University for organizing the results and proofreading the manuscript. Received May 6, 2007, and in revised form July 12, 2007. Accepted for publication Aug 4, 2007. 280 Int. J. Radiation Oncology Biol. Phys., Vol. 70, No. 1, pp. 280–288, 2008 Copyright Ó 2008 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/08/$–see front matter doi:10.1016/j.ijrobp.2007.08.024
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Fractionated Grid Therapy in Treating Cervical Cancers: Conventional Fractionation or...

Int. J. Radiation Oncology Biol. Phys., Vol. 70, No. 1, pp. 280–288, 2008Copyright � 2008 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/08/$–see front matter
doi:10.1016/j.ijrobp.2007.08.024
PHYSICS CONTRIBUTION
FRACTIONATED GRID THERAPY IN TREATING CERVICAL CANCERS:CONVENTIONAL FRACTIONATION OR HYPOFRACTIONATION?
HUALIN ZHANG, PH.D,* JIAN Z. WANG, PH.D.,* NINA MAYR, M.D.,* XIANG KONG, M.SC.,*
JIANKUI YUAN, PH.D.,* NILENDU GUPTA, PH.D.,* SIMON LO, M.D.,* JOHN GRECULA, M.D.,*
JOSEPH MONTEBELLO, M.D.,* DOUGLAS MARTIN, M.D.,* AND WILLIAM YUH, M.D.y
Departments of *Radiation Medicine and yRadiology, The Ohio State University, Columbus, OH
Purpose: To evaluate the conventionally fractionated and hypofractionated grid therapy in debulking cervicalcancers using the linear quadratic (LQ) model.Methods and Materials: A Monte Carlo technique was used to calculate the dose distribution of a commerciallyavailable grid in a 6-MV photon beam. The LQ model was used to evaluate the therapeutic outcome of boththe conventionally fractionated (2 Gy/fraction) and hypofractionated (15 Gy/fraction) grid therapy regimens todebulk cervical cancers with different LQ parameters. The equivalent open-field dose (EOD) to the cancer cellsand therapeutic ratio (TR) were defined by comparing grid therapy with the open debulking field. The clinicaloutcomes from 114 patients were used to verify our theoretical model.Results: The cervical cancer and normal tissue cell survival statistics for grid therapy in two regimens were cal-culated. The EODs and TRs were derived. The EOD was only a fraction of the prescribed dose. The TR was de-pendent on the prescribed dose and the LQ parameters of both the tumor and normal tissue cells. The grid therapyfavors the acutely responding tumors inside radiosensitive normal tissues. Theoretical model predictions wereconsistent with the clinical outcomes.Conclusions: Grid therapy provided a pronounced therapeutic advantage in both the hypofractionated and con-ventionally fractionated regimens compared with that seen with single fraction, open debulking field regimens, butthe true therapeutic advantage exists only in the hypofractionated grid therapy. The clinical outcomes and ourstudy indicated that a course of open-field radiotherapy is necessary to control tumor growth fully after a gridtherapy. � 2008 Elsevier Inc.
Grid therapy, Monte Carlo, Hypofractionation, Therapeutic ratio, Cervical cancer.
INTRODUCTION
Intensity modulation in radiotherapy has been studied for
decades (1–3). The improved normal tissue sparing pro-
vided by intensity modulated fields and new techniques
such as multileaf-collimator (MLC)-based, intensity modu-
lated radiotherapy (IMRT) have greatly enhanced the use of
intensity-modulated beams (4–7). Of the various IMRT
techniques, grid modulated, or spatially fractionated radio-
therapy, has been recognized as an important and easy-
to-use technique for debulking tumors (8–12). Unlike the
MLC-based IMRT in which dose delivery is time- and
space-dependent, grid-modulated radiotherapy is only space-
dependent. Grid therapy takes advantage of the better repair
capability of normal tissues. Underdosed areas serve as re-
growth centers for normal tissues, thus reducing radiation
complications.
2
Some authors have described the dosimetric characteristics
of grid therapy. Reiff et al. (13) measured depth dose curves
and peak-to-valley ratios of megavoltage grid therapy in a water
phantom for various field sizes of a square pattern grid. Trapp
et al. (14) measured three-dimensional dose distributions of
grid-collimated photon fields using gels. Ha et al. (15) studied
the feasibility of grid therapy delivery using an MLC. Meigooni
et al. (16, 17) measured the dose distributions of 6-MV and 18-
MV photon beams modulated by a hexagonal grid using films,
thermoluminescent dosimeters, and an ion chamber in water.
Zhang et al. (18) derived two-dimensional (2D) dose distribu-
tions of 6-MV grid therapy with the Monte Carlo (MC) simu-
lations, extended dose range (EDR2) films in solid water
phantom, and an ion chamber in water scanning system.
As the dosimetric properties of grid therapy have become
clearer, some authors have switched their attention from dosi-
metric issues to radiobiological effects. Zwicker et al. (19) first
Reprint requests to: Hualin Zhang, Ph.D., Department of Radia-tion Medicine, The Ohio State University, 300 West 10th Avenue,Columbus, OH 43210-1228. Tel: (614) 293-7497; Fax: (614) 293-4044; E-mail: [email protected]
Conflict of interest: none.
80
Acknowledgment—The authors thank David E. Carpenter of theOhio State University for organizing the results and proofreadingthe manuscript.
Received May 6, 2007, and in revised form July 12, 2007.Accepted for publication Aug 4, 2007.

Hypofractionation of megavoltage grid radiotherapy d H. ZHANG et al. 281
used the linear quadratic (LQ) model to estimate the therapeu-
tic advantage of grid therapy compared with the open debulk-
ing field. Zhang et al. (18) applied 2D dose distribution to
a series of melanoma tumors and assessed the therapeutic
outcomes. Zhang et al. (18) predicted that conventionally frac-
tionated (2 Gy/fraction) grid therapy could achieve improved
sparing of normal tissues compared with that seen with single-
fraction open debulking field therapy and that the therapeutic
ratio depends not only on the single a/b ratio but also on the
individual a and b values of the tumors. Their study demon-
strated (18) that acutely responding tumors and radiosensitive
normal tissues are more suitable for grid therapy.
Because the use of hypofractionation (generally 15 Gy/
fraction) in megavoltage grid therapy is widely accepted
(7–11), the outstanding questions remain: Does the hypofrac-
tionation still provide a significant therapeutic advantage?
What is the extent of any advantage compared with that of
conventional fractionation regimens? Finally, how great is
the true therapeutic advantage of grid therapy if the fraction-
ation effect is excluded? We therefore have calculated the
therapeutic ratios of a hypofractionated grid therapy and
compared them with a conventionally fractionated regimen
and clinical outcomes. With improved dose calculation re-
sults, the normal tissue and cervical cancer cell survival sta-
tistics, as well as the equivalent open-field dose (EOD) and
therapeutic ratios for the two-grid radiotherapy regimens
(conventionally fractionated 2Gy/fraction and hypofractio-
nated 15 Gy/fraction), were estimated with the LQ model.
The therapeutic advantage of grid therapy with or without
the fractionation effect was evaluated; the roles played by
the linear quadratic parameters in grid therapy were analyzed.
Because our previous study (18) revealed that the treatment
of tumors with large a/b ratios (such as cervical cancers)
might be improved using grid therapy, cervical cancer cell
lines were chosen for this study to test two fractionation
regimens of megavoltage grid therapy.
METHODS AND MATERIALS
GridThe structure of the grid has already been described in detail (16–
18). In brief, the grid used in this study (High Dose Radiation Grid,
Radiation Products Design, Albertville, MN) consisted of a 7.5-cm-
thick Cerrobend block perforated by a hexagonal pattern (Fig. 1) of
circular divergent holes and designed to be mounted in the standard
linear accelerator accessory mount 65.4 cm from the source (Varian
21 EX, Varian Oncology System, Palo Alto, CA). The diameter of
the holes was 0.60 cm on the top side and 0.85 cm on the lower side,
and the center-to-center separation on the block was 1.15 cm on the
lower surface. With this design, approximately one half of the tis-
sues in the collimated areas were irradiated by the partially attenu-
ated primary beam; the remainder were shielded by the Cerrobend
block. All holes in the grid were divergent and roughly concordant
with the beam tilt.
Monte Carlo simulationAn MC N-particle Transport Code (MCNPX, Version 2.5) (20)
was used to calculate the doses in a water phantom at dmax (1.5
cm for the 6-MV photon beam of the Varian 21 EX machine) and
at 5 cm depth. The code is the extension for particle types and energy
ranges of MCNP (21). The photon interaction cross-section file used
in this study was the DLC-200 library distributed by the Radiation
Shielding Information Computing Center (RSICC).
The tally technique used in this study has also been described
elsewhere (18). Its adequacy was examined by comparing the per-
centage depth dose curve at the central axis and the dose profile at
certain planes with the experimental measurements (18). An array
of spherical voxels was defined at depths of 1.5 cm and 5 cm, respec-
tively, each having a 1 mm diameter and spaced at 2 mm center-to-
center for 2D dose simulations. A 6-MV beam (22) was simulated.
For each simulation, the low energy cutoff was set to 10 keV and
used a minimum of 5 � 108 histories. The statistical error of each
tallied dose was found to be less than 5%.
The biological effect of grid therapyThe biological model for normal tissue and tumor cell survival es-
timation used in this study was same as the one used in our previous
study (18). The LQ model parameters (a and b) of the radiobiolog-
ical response for cervical tumor cells were taken from the literature
(23) and are consistent with the data reported by Thames et al. (24).
We used a/b = 3.1 Gy for normal tissues (25) (Table 1).
With the LQ model, the cell survival statistics for both tumor and
normal cells are
SF
�x; y
�¼ e
��a�Dðx;yÞ �b�D2ðx;yÞ
�N
�: (1)
N is the number of fractions, D(x,y) was the MC-simulated 2D dose
distribution at 5 cm depth, which could be scaled to 2 Gy or 15 Gy at
the axis of central hole.
For the calculated 2D dose distribution, the average survival frac-
tion for tumor or normal tissue was calculated using the following
formula:
SFðGridÞ ¼Ð
SFðDðx; yÞÞ,dx,dyÐdx,dy
¼Ð
SFðDðx; yÞÞ,dx,dy
A; :
(2)
Fig. 1. Schematic diagram of the grid collimator.
282 I. J. Radiation Oncology d Biology d Physics Volume 70, Number 1, 2008
where A was the area of the target covered by the grid field. In sur-
vival fraction calculation, the same dose distribution was used for
both tumor cells and normal tissues, reflecting the cases in which
the tumor and normal tissue or organ at risk would receive a similar
radiation dose (e.g., early stage cervical cancers or tumors that are
difficult to differentiate from normal tissues). The average tumor
cell kill of grid therapy has an EOD (18, 19). The EOD can be con-
sidered as the single-fraction open-field debulking dose. From the
EOD, the normal tissue surviving fraction in open field, SFnormal
(EOD), could be calculated:
SFnormal
�EOD
�¼ e�a�ðEODÞ�b�ðEODÞ2; (3)
The therapeutic ratio (TR) is then defined as
TRnormal ¼SFnormalðGridÞSFnormalðEODÞ ; (4)
where SFnormal (Grid) was the final surviving fraction of normal cells
after fractionated grid irradiation, and TRnormal was the therapeutic
ratio for survival of normal cells.
When fractionated grid therapy is compared with a single-fraction
open-field debulking dose, this TR would also include the therapeu-
tic advantage of fractionation. In addition, the real roles played by
individual linear quadratic parameters in the grid therapy become
ambiguous if the fractionation effect is not separated. To separate
the fractionation effect from the grid therapy effect, we calculated
the therapeutic ratios based on the single-fraction grid therapy and
the initial equivalent open-field dose, EODI. Thus the therapeutic ra-
tio for the fractionated grid therapy without fractionation effect was
defined as
TRgrid�normal ¼�
SFnormalðGridIÞSFnormalðEODIÞ
�N
; (4--1)
where SFNormalðgridIÞwas the surviving fraction of normal cells af-
ter the first fraction of grid irradiation, SFNormalðEODIÞwas the nor-
mal tissue survival fraction in the initial equivalent open-field,
EODI, and TRgrid-normal was the therapeutic ratio without the frac-
tionation effect for survival of normal cells treated in N fractions.
A value of TRnormal or TRgrid-normal greater than 1 would confer a sur-
vival advantage (i.e., spare) to normal tissue cells over those treated
with a single- or multiple-fraction open-field debulking dose.
Table 1. Linear quadratic parameters of cervical cancer andnormal tissue cells (23)
Tissue type Cell lines a b a/b
Cervical ca HX-160c 0.46 0.0773 5.9Cervical ca HX-155c 0.29 0.0235 12.4Cervical ca HX-156c 0.31 0.0246 12.6Cervical ca HX-171c 0.33 0.0169 19.4Cervical ca HX-151c 0.74 0.0354 20.9Normal tissue 1 SF(2 Gy) = 0.3 0.366 0.1180 3.1Normal tissue 2 SF(2 Gy) = 0.5 0.211 0.0680 3.1Normal tissue 3 SF(2 Gy) = 0.7 0.108 0.0350 3.1
Abbreviations: ca = cancer; SF = survival fraction.Normal tissue 1, 2, and 3 are three types of normal tissue cells that
have survival fractions of 0.3, 0.5, and 0.7, respectively, for a 2-Gyopen field. Normal tissue 1, 2, and 3 are also referred to as the radio-sensitive, moderately radiosensitive, and radio-resistant normal tis-sues respectively in the text.
Although the conventional fractionation is widely used in open-
field treatments (26), hypofractionated grid therapy is well accepted
as an alternative debulking therapy before a conventionally fraction-
ated radiotherapy regimen (9, 12). Therefore in this study, we com-
pared both conventionally fractionated and hypofractionated grid
therapy.
RESULTS
2D dose distributionThe 2D dose distributions at dmax (d = 1.5 cm) and 5-cm
depths for grid therapy in an open 10� 10 cm field were sim-
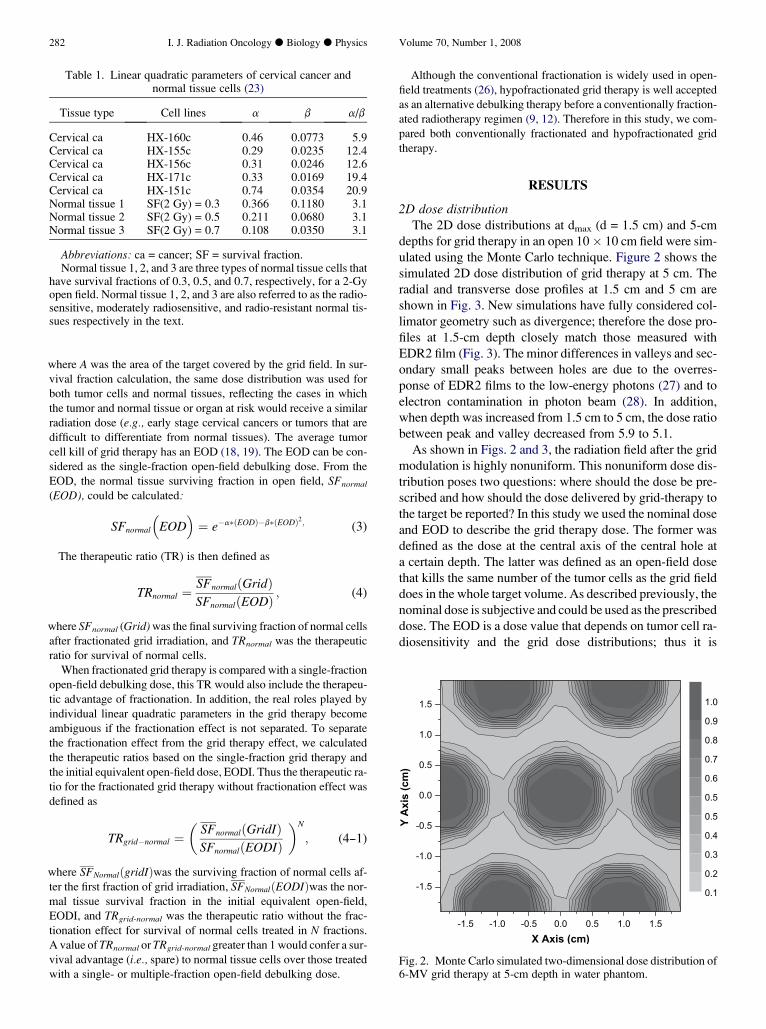
ulated using the Monte Carlo technique. Figure 2 shows the
simulated 2D dose distribution of grid therapy at 5 cm. The
radial and transverse dose profiles at 1.5 cm and 5 cm are
shown in Fig. 3. New simulations have fully considered col-
limator geometry such as divergence; therefore the dose pro-
files at 1.5-cm depth closely match those measured with
EDR2 film (Fig. 3). The minor differences in valleys and sec-
ondary small peaks between holes are due to the overres-
ponse of EDR2 films to the low-energy photons (27) and to
electron contamination in photon beam (28). In addition,
when depth was increased from 1.5 cm to 5 cm, the dose ratio
between peak and valley decreased from 5.9 to 5.1.
As shown in Figs. 2 and 3, the radiation field after the grid
modulation is highly nonuniform. This nonuniform dose dis-
tribution poses two questions: where should the dose be pre-
scribed and how should the dose delivered by grid-therapy to
the target be reported? In this study we used the nominal dose
and EOD to describe the grid therapy dose. The former was
defined as the dose at the central axis of the central hole at
a certain depth. The latter was defined as an open-field dose
that kills the same number of the tumor cells as the grid field
does in the whole target volume. As described previously, the
nominal dose is subjective and could be used as the prescribed
dose. The EOD is a dose value that depends on tumor cell ra-
diosensitivity and the grid dose distributions; thus it is
-1.5 -1.0 -0.5 0.0 0.5 1.0 1.5
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
X Axis (cm)
Y A
xis (cm
)
0.1
0.2
0.3
0.4
0.5
0.5
0.6
0.7
0.8
0.9
1.0
Fig. 2. Monte Carlo simulated two-dimensional dose distribution of6-MV grid therapy at 5-cm depth in water phantom.

Hypofractionation of megavoltage grid radiotherapy d H. ZHANG et al. 283
-4 -3 -2 -1 0 1 2 3 40.0
0.2
0.4
0.6
0.8
1.0
-4 -3 -2 -1 0 1 32 4
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
EDR2 film Monte Carlo 1.5 cm depth
Tran
sver
se D
ose
Monte Carlo 5 cm depth
Distance from the center of beam (cm)
Rad
ial D
ose
Distance from the center of beam (cm)-4 -3 -2 -1 0 1 2 3 4
-4 -3 -2 -1 0 1 32 4
Fig. 3. Radial and transverse dose profiles of grid therapy in a flat water phantom at 1.5-cm and 5-cm depths. The doseswere normalized to a 10 � 10 cm open field at 1.5-cm depth, and 100 cGy was applied to the open field as a standard.EDR2 = extended dose range.
objective and is the dose actually delivered to the tumor. Use
of the EOD is recommended for evaluation of tumor control
by grid therapy. The EODI is derived from the first fraction
of grid therapy; use of this EODI would exclude the fraction-
ation effect from the fractionated grid therapy, and thus it
would reveal the true therapeutic advantage in grid therapy.
Conventionally fractionated grid therapyIn the conventionally fractionated grid therapy, the cell sur-
vival fractions of normal cells are calculated at 2 Gy/fraction.
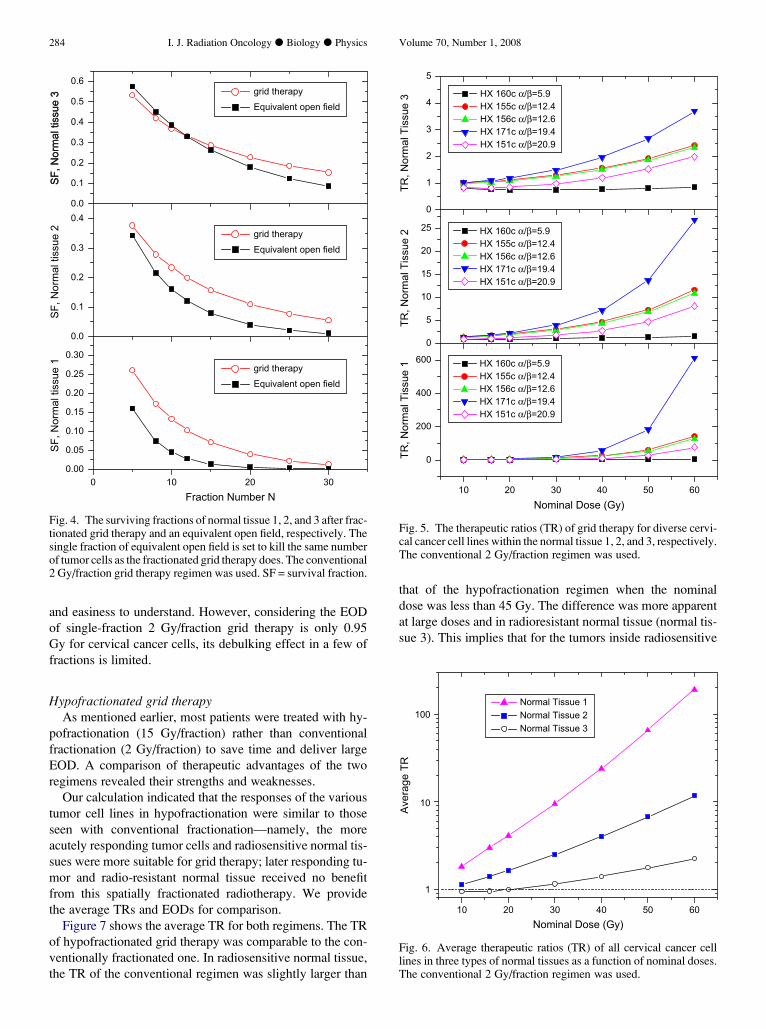
Figure 4 shows the relationship between the normal cell sur-
vival fraction and nominal dose. The normal cell survival frac-
tion of an open field was obtained by using a derived EOD.
The survival fraction results showed that in cervical cancer
treatment, grid therapy spares more normal tissue cells than
the single-fraction EOD dose, although they both kill the
same number of tumor cells. This advantage, which included
both the fractionation effect and grid therapy, is more pro-
nounced in radiosensitive normal tissues (normal tissue 1
and 2).
Figure 5 shows the therapeutic ratios (TR) in treating indi-
vidual cervical tumor cell lines with a conventional 2 Gy/
fraction regimen. The results indicated that the TR increased
with dose and a/b ratios. The acutely responding tumor cells
(a/b> 6, HX 160c, HX 155c, HX 156c, HX 171c) within ra-
diosensitive normal tissues (normal tissue 1 and 2) had larger
TRs than those of later responding tumor (a/b< 6, HX 151c)
within radio-resistant normal tissue (normal tissue 3). In
addition, the fact that the TR of the HX151C (a/b = 20.9)
cell line was smaller than that of HX171C (a/b = 19.4) indi-
cates that the TR was dependent not only on the single a/b ra-
tio but also on the individual a and b values. This result is
consistent with the study by Mailaise et al. (29) in which
the highly responsive cells had not only large a/b ratios but
also considerable a values. Figure 6 shows the average
TRs of all tumor cell lines within three types of normal tis-
sues. Grid therapy’s average TRs indicate that a large dose
(which, in this case, also means multiple fractions) and radio-
sensitive normal tissues are the important factors in achieving
a therapeutic advantage for debulking tumors compared with
the open debulking field. Table 2 tabulates the average TRs
over all types of normal tissues.
When the fractionation effect was excluded from the con-
ventionally fractionated grid therapy, the situation changed.
Table 3 shows the therapeutic ratios for various cervical
cancer cell lines treated in single-fraction grid therapy.
Only two of the cell lines, HX-155c and HX-156c within
radiosensitive normal tissues, showed any benefit from the
single 2 Gy/fraction grid therapy. Table 4 gives the average
therapeutic ratios, excluding fractionation effect for 2Gy/
fraction fractionated grid therapy, from 5 to 30 fractions,
for all cervical cancer cell lines studied. Fractionated grid
therapy with a 2 Gy/fraction fraction dose provided no nor-
mal tissue sparing advantage compared with fractionated
open-field radiotherapy.
It should be noted that the conventional fractionation
(2Gy/fraction) is selected in this and previous studies (18)
mainly because of its popularity in open-field treatments
284 I. J. Radiation Oncology d Biology d Physics Volume 70, Number 1, 2008
and easiness to understand. However, considering the EOD
of single-fraction 2 Gy/fraction grid therapy is only 0.95
Gy for cervical cancer cells, its debulking effect in a few of
fractions is limited.
Hypofractionated grid therapyAs mentioned earlier, most patients were treated with hy-
pofractionation (15 Gy/fraction) rather than conventional
fractionation (2 Gy/fraction) to save time and deliver large
EOD. A comparison of therapeutic advantages of the two
regimens revealed their strengths and weaknesses.
Our calculation indicated that the responses of the various
tumor cell lines in hypofractionation were similar to those
seen with conventional fractionation—namely, the more
acutely responding tumor cells and radiosensitive normal tis-
sues were more suitable for grid therapy; later responding tu-
mor and radio-resistant normal tissue received no benefit
from this spatially fractionated radiotherapy. We provide
the average TRs and EODs for comparison.
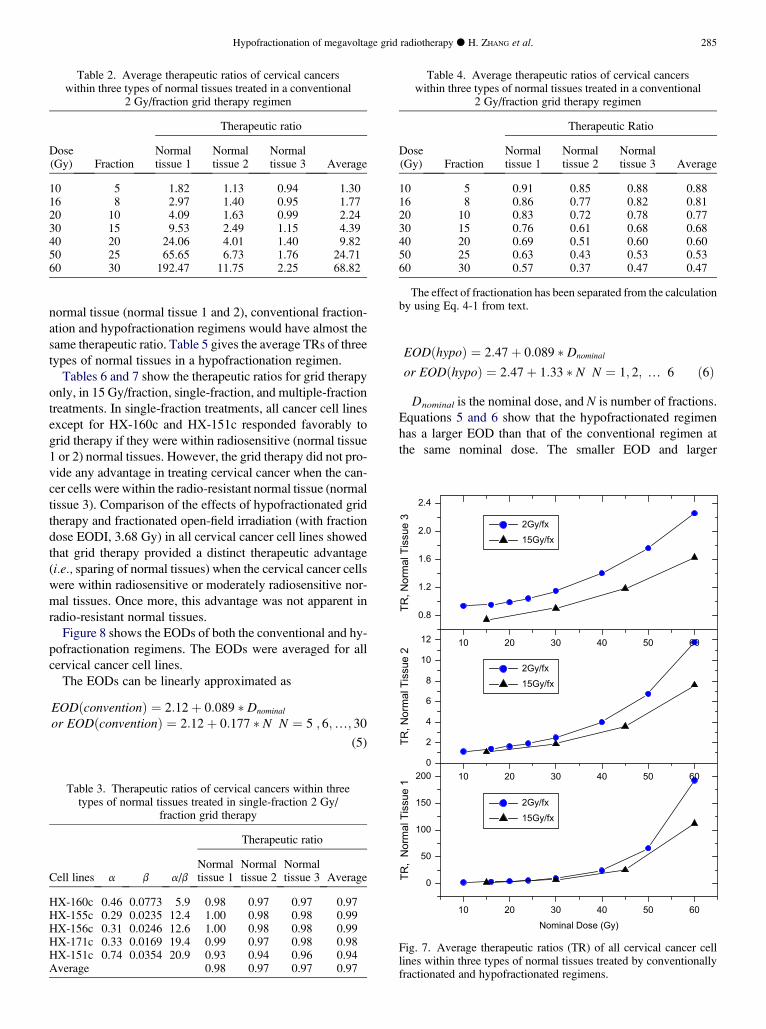
Figure 7 shows the average TR for both regimens. The TR
of hypofractionated grid therapy was comparable to the con-
ventionally fractionated one. In radiosensitive normal tissue,
the TR of the conventional regimen was slightly larger than
0 10 20 300.00
0.05
0.10
0.15
0.20
0.25
0.30
0.0
0.1
0.2
0.3
0.40.0
0.1
0.2
0.3
0.4
0.5
0.6
SF, N
orm
al ti
ssue
1
Fraction Number N
SF, N
orm
al ti
ssue
2
SF, N
orm
al ti
ssue
3SF
, Nor
mal
tiss
ue 3 grid therapy
Equivalent open field
grid therapyEquivalent open field
grid therapyEquivalent open field
Fig. 4. The surviving fractions of normal tissue 1, 2, and 3 after frac-tionated grid therapy and an equivalent open field, respectively. Thesingle fraction of equivalent open field is set to kill the same numberof tumor cells as the fractionated grid therapy does. The conventional2 Gy/fraction grid therapy regimen was used. SF = survival fraction.
that of the hypofractionation regimen when the nominal
dose was less than 45 Gy. The difference was more apparent
at large doses and in radioresistant normal tissue (normal tis-
sue 3). This implies that for the tumors inside radiosensitive
10 20 30 40 50 60
0
200
400
600
0
5
10
15
20
25
0
1
2
3
4
5
TR, N
orm
al T
issu
e 1
Nominal Dose (Gy)
TR, N
orm
al T
issu
e 2
TR, N
orm
al T
issu
e 3 HX 160c α/β=5.9
HX 155c α/β=12.4 HX 156c α/β=12.6 HX 171c α/β=19.4 HX 151c α/β=20.9
HX 160c α/β=5.9 HX 155c α/β=12.4 HX 156c α/β=12.6 HX 171c α/β=19.4 HX 151c α/β=20.9
HX 160c α/β=5.9 HX 155c α/β=12.4 HX 156c α/β=12.6 HX 171c α/β=19.4 HX 151c α/β=20.9
Fig. 5. The therapeutic ratios (TR) of grid therapy for diverse cervi-cal cancer cell lines within the normal tissue 1, 2, and 3, respectively.The conventional 2 Gy/fraction regimen was used.
10 20 30 40 50 60
1
10
100
Aver
age
TR
Nominal Dose (Gy)
Normal Tissue 1Normal Tissue 2Normal Tissue 3
Fig. 6. Average therapeutic ratios (TR) of all cervical cancer celllines in three types of normal tissues as a function of nominal doses.The conventional 2 Gy/fraction regimen was used.
Hypofractionation of megavoltage grid radiotherapy d H. ZHANG et al. 285
normal tissue (normal tissue 1 and 2), conventional fraction-
ation and hypofractionation regimens would have almost the
same therapeutic ratio. Table 5 gives the average TRs of three
types of normal tissues in a hypofractionation regimen.
Tables 6 and 7 show the therapeutic ratios for grid therapy
only, in 15 Gy/fraction, single-fraction, and multiple-fraction
treatments. In single-fraction treatments, all cancer cell lines
except for HX-160c and HX-151c responded favorably to
grid therapy if they were within radiosensitive (normal tissue
1 or 2) normal tissues. However, the grid therapy did not pro-
vide any advantage in treating cervical cancer when the can-
cer cells were within the radio-resistant normal tissue (normal
tissue 3). Comparison of the effects of hypofractionated grid
therapy and fractionated open-field irradiation (with fraction
dose EODI, 3.68 Gy) in all cervical cancer cell lines showed
that grid therapy provided a distinct therapeutic advantage
(i.e., sparing of normal tissues) when the cervical cancer cells
were within radiosensitive or moderately radiosensitive nor-
mal tissues. Once more, this advantage was not apparent in
radio-resistant normal tissues.
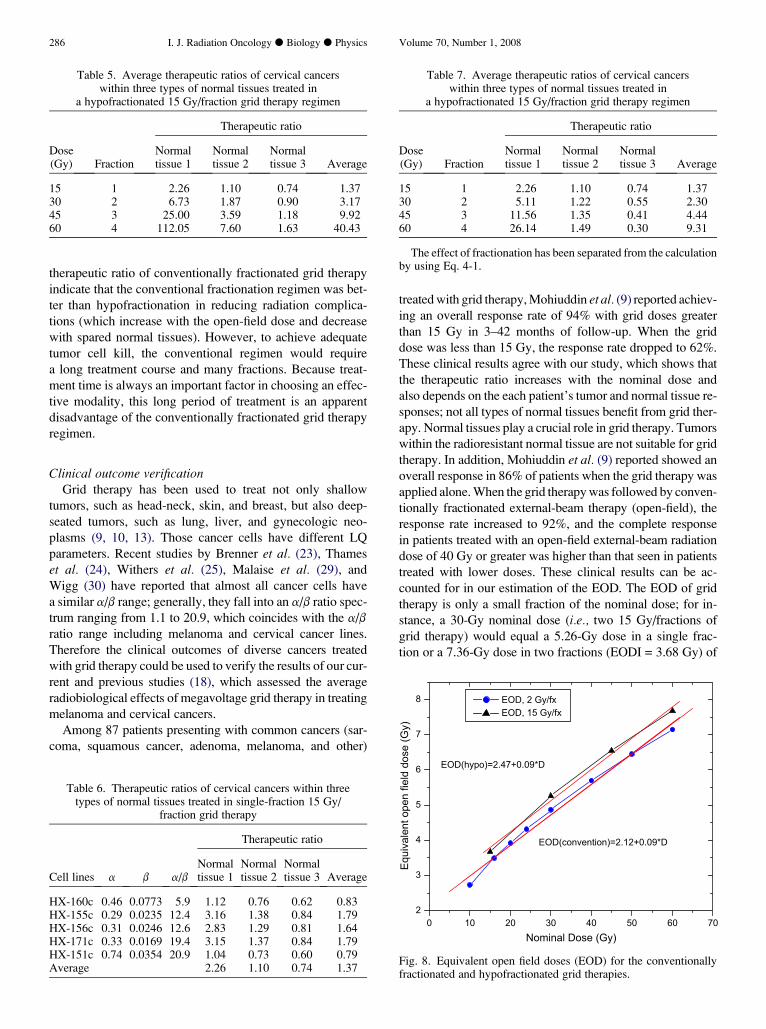
Figure 8 shows the EODs of both the conventional and hy-
pofractionation regimens. The EODs were averaged for all
cervical cancer cell lines.
The EODs can be linearly approximated as
EODðconventionÞ ¼ 2:12þ 0:089 � Dnominal
or EODðconventionÞ ¼ 2:12þ 0:177 � N N ¼ 5 ; 6;.; 30
(5)
Table 2. Average therapeutic ratios of cervical cancerswithin three types of normal tissues treated in a conventional
2 Gy/fraction grid therapy regimen
Therapeutic ratio
Dose(Gy) Fraction
Normaltissue 1
Normaltissue 2
Normaltissue 3 Average
10 5 1.82 1.13 0.94 1.3016 8 2.97 1.40 0.95 1.7720 10 4.09 1.63 0.99 2.2430 15 9.53 2.49 1.15 4.3940 20 24.06 4.01 1.40 9.8250 25 65.65 6.73 1.76 24.7160 30 192.47 11.75 2.25 68.82
Table 3. Therapeutic ratios of cervical cancers within threetypes of normal tissues treated in single-fraction 2 Gy/
fraction grid therapy
Therapeutic ratio
Cell lines a b a/bNormaltissue 1
Normaltissue 2
Normaltissue 3 Average
HX-160c 0.46 0.0773 5.9 0.98 0.97 0.97 0.97HX-155c 0.29 0.0235 12.4 1.00 0.98 0.98 0.99HX-156c 0.31 0.0246 12.6 1.00 0.98 0.98 0.99HX-171c 0.33 0.0169 19.4 0.99 0.97 0.98 0.98HX-151c 0.74 0.0354 20.9 0.93 0.94 0.96 0.94Average 0.98 0.97 0.97 0.97
EODðhypoÞ ¼ 2:47þ 0:089 � Dnominal
or EODðhypoÞ ¼ 2:47þ 1:33 � N N ¼ 1; 2; . 6 ð6Þ
Dnominal is the nominal dose, and N is number of fractions.
Equations 5 and 6 show that the hypofractionated regimen
has a larger EOD than that of the conventional regimen at
the same nominal dose. The smaller EOD and larger
Table 4. Average therapeutic ratios of cervical cancerswithin three types of normal tissues treated in a conventional
2 Gy/fraction grid therapy regimen
Therapeutic Ratio
Dose(Gy) Fraction
Normaltissue 1
Normaltissue 2
Normaltissue 3 Average
10 5 0.91 0.85 0.88 0.8816 8 0.86 0.77 0.82 0.8120 10 0.83 0.72 0.78 0.7730 15 0.76 0.61 0.68 0.6840 20 0.69 0.51 0.60 0.6050 25 0.63 0.43 0.53 0.5360 30 0.57 0.37 0.47 0.47
The effect of fractionation has been separated from the calculationby using Eq. 4-1 from text.
10 20 30 40 50 60
0
50
100
150
2000
2
4
6
8
10
12
0.8
1.2
1.6
2.0
2.4
TR,
Nor
mal
Tis
sue
1
Nominal Dose (Gy)
TR, N
orm
al T
issu
e 2
TR, N
orm
al T
issu
e 3
2Gy/fx15Gy/fx
2Gy/fx15Gy/fx
2Gy/fx15Gy/fx
10 20 30 40 50 60
10 20 30 40 50 60
Fig. 7. Average therapeutic ratios (TR) of all cervical cancer celllines within three types of normal tissues treated by conventionallyfractionated and hypofractionated regimens.
286 I. J. Radiation Oncology d Biology d Physics Volume 70, Number 1, 2008
therapeutic ratio of conventionally fractionated grid therapy
indicate that the conventional fractionation regimen was bet-
ter than hypofractionation in reducing radiation complica-
tions (which increase with the open-field dose and decrease
with spared normal tissues). However, to achieve adequate
tumor cell kill, the conventional regimen would require
a long treatment course and many fractions. Because treat-
ment time is always an important factor in choosing an effec-
tive modality, this long period of treatment is an apparent
disadvantage of the conventionally fractionated grid therapy
regimen.
Clinical outcome verificationGrid therapy has been used to treat not only shallow
tumors, such as head-neck, skin, and breast, but also deep-
seated tumors, such as lung, liver, and gynecologic neo-
plasms (9, 10, 13). Those cancer cells have different LQ
parameters. Recent studies by Brenner et al. (23), Thames
et al. (24), Withers et al. (25), Malaise et al. (29), and
Wigg (30) have reported that almost all cancer cells have
a similar a/b range; generally, they fall into an a/b ratio spec-
trum ranging from 1.1 to 20.9, which coincides with the a/b
ratio range including melanoma and cervical cancer lines.
Therefore the clinical outcomes of diverse cancers treated
with grid therapy could be used to verify the results of our cur-
rent and previous studies (18), which assessed the average
radiobiological effects of megavoltage grid therapy in treating
melanoma and cervical cancers.
Among 87 patients presenting with common cancers (sar-
coma, squamous cancer, adenoma, melanoma, and other)
Table 5. Average therapeutic ratios of cervical cancerswithin three types of normal tissues treated in
a hypofractionated 15 Gy/fraction grid therapy regimen
Therapeutic ratio
Dose(Gy) Fraction
Normaltissue 1
Normaltissue 2
Normaltissue 3 Average
15 1 2.26 1.10 0.74 1.3730 2 6.73 1.87 0.90 3.1745 3 25.00 3.59 1.18 9.9260 4 112.05 7.60 1.63 40.43
Table 6. Therapeutic ratios of cervical cancers within threetypes of normal tissues treated in single-fraction 15 Gy/
fraction grid therapy
Therapeutic ratio
Cell lines a b a/bNormaltissue 1
Normaltissue 2
Normaltissue 3 Average
HX-160c 0.46 0.0773 5.9 1.12 0.76 0.62 0.83HX-155c 0.29 0.0235 12.4 3.16 1.38 0.84 1.79HX-156c 0.31 0.0246 12.6 2.83 1.29 0.81 1.64HX-171c 0.33 0.0169 19.4 3.15 1.37 0.84 1.79HX-151c 0.74 0.0354 20.9 1.04 0.73 0.60 0.79Average 2.26 1.10 0.74 1.37
treated with grid therapy, Mohiuddin et al. (9) reported achiev-
ing an overall response rate of 94% with grid doses greater
than 15 Gy in 3–42 months of follow-up. When the grid
dose was less than 15 Gy, the response rate dropped to 62%.
These clinical results agree with our study, which shows that
the therapeutic ratio increases with the nominal dose and
also depends on the each patient’s tumor and normal tissue re-
sponses; not all types of normal tissues benefit from grid ther-
apy. Normal tissues play a crucial role in grid therapy. Tumors
within the radioresistant normal tissue are not suitable for grid
therapy. In addition, Mohiuddin et al. (9) reported showed an
overall response in 86% of patients when the grid therapy was
applied alone. When the grid therapy was followed by conven-
tionally fractionated external-beam therapy (open-field), the
response rate increased to 92%, and the complete response
in patients treated with an open-field external-beam radiation
dose of 40 Gy or greater was higher than that seen in patients
treated with lower doses. These clinical results can be ac-
counted for in our estimation of the EOD. The EOD of grid
therapy is only a small fraction of the nominal dose; for in-
stance, a 30-Gy nominal dose (i.e., two 15 Gy/fractions of
grid therapy) would equal a 5.26-Gy dose in a single frac-
tion or a 7.36-Gy dose in two fractions (EODI = 3.68 Gy) of
Table 7. Average therapeutic ratios of cervical cancerswithin three types of normal tissues treated in
a hypofractionated 15 Gy/fraction grid therapy regimen
Therapeutic ratio
Dose(Gy) Fraction
Normaltissue 1
Normaltissue 2
Normaltissue 3 Average
15 1 2.26 1.10 0.74 1.3730 2 5.11 1.22 0.55 2.3045 3 11.56 1.35 0.41 4.4460 4 26.14 1.49 0.30 9.31
The effect of fractionation has been separated from the calculationby using Eq. 4-1.
0 10 20 30 40 50 60 702
3
4
5
6
7
8
EOD(hypo)=2.47+0.09*D
EOD(convention)=2.12+0.09*D
Equi
vale
nt o
pen
field
dos
e (G
y)
Nominal Dose (Gy)
EOD, 2 Gy/fxEOD, 15 Gy/fx
Fig. 8. Equivalent open field doses (EOD) for the conventionallyfractionated and hypofractionated grid therapies.

Hypofractionation of megavoltage grid radiotherapy d H. ZHANG et al. 287
open-field therapy. Although grid therapy spares more normal
tissue than open-field therapy, a 30-Gy nominal dose of grid
therapy or a 5.26-Gy equivalent open-field debulking dose is
not sufficient to control the tumor fully. As the clinical results
indicated (9), subsequent conventionally fractionated exter-
nal-beam therapy (usually with open field) would be needed
to provide further tumor control.
Huhn et al. (12) also reported the clinical outcomes of grid
plus open-field radiotherapy in two groups of head and neck
cancer patients (n = 27). Both groups were treated with 15
Gy/fraction grid therapy. In Group 1, 14 patients were treated
with grid therapy followed by a course of 4–6 weeks of 70-
Gy open-field radiation. In Group 2, 13 patients were treated
with grid therapy plus a course of 4–6 weeks of 59-Gy open-
field radiation followed by a planned dissection. The disease-
specific survival and local regional control for Group 1 were
50% and 86%, respectively, at 3–44 months of follow-up.
The overall survival for Group 2 was 62%, and the disease-
specific survival and local regional control for this group
were 85% and 92%, respectively, at 116 months of follow-
up. Although Huhn et al.’s clinical outcomes were not com-
pared with open-field only treatment, the results did suggest
that hypofractionated grid therapy can be safely incorporated
into the definitive management of advanced disease.
DISCUSSION
In this study, we have provided an improved dosimetric
simulation and assessed the radiobiological response of cer-
vical cancer cell lines in conventionally fractionated and hy-
pofractionated regimens in grid therapy. The advantageous
biological effects of grid therapy for debulking purpose in
the two regimens were estimated using the LQ model for
cell survival calculations and were represented as a therapeu-
tic ratio.
The results of the radiobiological response of cervical can-
cer cells in conventional fractionation and hypofractionation
are consistent with those in a previous study of melanoma
(18). Compared with the single-fraction open-field debulking
dose, Grid therapy provides an advantage in treating acutely
responding tumor cells (a/b >6) within radiosensitive normal
tissues. In conventionally fractionated grid therapy, the ther-
apeutic advantage comes from the fractionation effect; the
grid therapy itself does not show a benefit. Although the frac-
tionation of hypofractionated grid therapy helps to spare
more normal tissue than is spared in single-fraction open-
field debulking therapy, the use of the grid collimator en-
hances the sparing of normal tissues still further (Table 7).
This therapeutic advantage would improve the efficacy of
cervical cancer treatments, because sparing and facilitating
the growth of the normal tissues and organs surrounding
the cervix tumor would reduce complications (27).
A close look at Tables 3 and 6 allows us to identify the ma-
jor roles played by linear quadratic parameters in grid ther-
apy. In general, the grid therapy is most effective in acutely
responding (large a/b ratio, large a) cancer cells, but a large
b value is apparently not preferred. An example is the
HX151c cell line, which has a larger a/b ratio (a/b = 20.9,
a = 0.74, a = 0.0354) but a smaller therapeutic ratio than
HX155c cell line (a/b = 12.4, a = 0.29, b = 0.0235). Another
example is the HX156c cell line, which has a similar a/b ratio
(a/b = 12.6, a = 0.31, b= 0.0246), but a smaller therapeutic
ratio than the HX155c cell line (a/b = 12.4, a = 0.29, b=
0.0235). Thus our results confirmed that using a single value
of the a/b parameter even if combined with a value in com-
paring different treatment schedules for acutely responding
tissues is not justified (23).
Clinical outcomes have provided a vital verification of our
theoretical model. Mohiuddin’s study (9) indicated that grid
therapy applied before the open-field treatment significantly
improves the response of tumors. Our theory of the therapeu-
tic advantage of grid therapy predicts this outcome; the
spared normal tissue somehow improved the response. The
clinical outcomes (9) further confirmed our conclusion that
the therapeutic advantage would increase with the dose or
fraction number. In addition, a study by Huhn et al. (12) in-
dicated that the hypofractionated grid therapy can also be
safely combined with open-field radiotherapy and surgery.
Based on clinical outcomes (9–12, 13) and the results of
our own studies, we propose the following recommendations
be adopted for grid therapy:
(1). The grid therapy dose should be documented not only by
the nominal dose at the dmax or at the depth of the cen-
tral axis of the central hole, but also by the EOD. Be-
cause the a/b ratios used in this study cover most
common cancers, the EODs in treating other cancers
can also be approximated by Eq. 5 for conventional frac-
tionation or Eq. 6 for hypofractionation.
(2). The hypofractionated grid therapy regimen (15 Gy/frac-
tion) should be used. It is safe and more cost-effective
than conventional regimens.
(3). Grid therapy should be followed by open-field external-
beam therapy to further control the disease. Both theo-
retical modeling and clinical outcomes indicate that
grid therapy can increase treatment response, but it is
not sufficient to control the disease fully.
The gist of grid therapy is to take advantage of the ability
of normal tissues to repair better than tumor cells can. An
increased normal cell survival ratio at the same tumor cell-
killing rate should be clinically advantageous and would
increase tumor response to radiation. The normal tissue cells
spared by grid could serve as centers of regrowth for normal
tissues; thus grid therapy would also increase the patient’s ra-
diation tolerance and reduce the complications. Our study
shows that grid therapy at a 15-Gy (1 fraction of 15 Gy/frac-
tion) nominal dose in a hypofractionation regimen can in-
crease normal cell survival ratio by at least 37% compared
with open-field debulking radiation (Table 6) to the average
normal tissue. This result is clinically significant. However, it
should also be noted that although one or two fractions of hy-
pofractionated grid therapy is advantageous in treating can-
cers within radiosensitive normal tissues, it would have no
therapeutic advantage in radio-resistant normal tissue. The
288 I. J. Radiation Oncology d Biology d Physics Volume 70, Number 1, 2008
tumors within radio-resistant normal tissue would be better
treated with open-field radiotherapy. This may imply that
poor responses to grid therapy result, at least in part, because
the normal tissue was radio-resistant and the prescribed grid
therapy dose was insufficient.
All recent studies (15–18) involving grid therapy have in-
vestigated a hexagonal grid collimator with aperture diame-
ters of approximately 1 cm projected in the plane of the
isocenter. Although a grid collimator with an aperture of
this size has been used in clinical treatments and showed en-
couraging outcomes, there is little evidence to show that this
design represents optimal grid collimation for megavoltage
applications. The results of Zwicker et al. (19) did suggest
weak dependence of therapeutic ratios on aperture spacing
when using the same aperture diameter. However, oversim-
plified model assumptions about the dose distribution of
grid field, the inability to evaluate other aperture diameters,
and a lack of evaluations using experimental LQ parameters
of real tumors limit the usefulness of these results. We plan to
use the techniques validated in this and previous studies as
a basis for more detailed studies of other grid designs, frac-
tion doses, and tumor types. In pursuing this, we hope to fur-
ther understand radiobiology effects of grid therapy and find
evidence that justifies the current design or suggests changes
in both the collimator geometry and size of fraction dose that
may result in further improved patient treatments.
REFERENCES
1. Liberson F. The value of a multi-perforated screen in deep X-raytherapy. Radiology 1933;20:186–195.
2. Mark H. A new approach to the roentogen therapy of cancerwith the use of a GRID. J Mt Sinai Hosp 1950;17:46–48.
3. Puri DR, Chou W, Lee N. Intensity-modulated radiation therapyin head and neck cancers: Dosimetric advantages and update ofclinical results. Am J Clin Oncol 2005;28415–28423.
4. Chen YJ, Liu A, Tsai PT, et al. Organ sparing by conformalavoidance intensity-modulated radiation therapy for anal can-cer: Dosimetric evaluation of coverage of pelvis and inguinal/femoral nodes. Int J Radiat Oncol Biol Phys 2005;63:274–281.
5. Biancia CD, Yorke E, Chui CS, et al. Comparison of end normalinspiration and expiration for gated intensity modulated radia-tion therapy (IMRT) of lung cancer. Radiother Oncol 2005;75:149–156.
6. Marks H. Clinical experience with irradiation through a grid.Radiology 1952;58:338–342.
7. Miller RC, Wilson KG, Feola JM, et al. Megavoltage grid totalbody irradiation of C3Hf/SED mice. Strahlenther Onkol 1992;168:423–426.
8. Mohiuddin M, Curtis DL, Grizos WT, et al. Palliative treatmentof advanced cancer using multiple nonconfluent pencil beam ra-diation. Cancer 1990;66:114–118.
9. Mohiuddin M, Fujita M, Grizos WT, et al. High dose spatiallyfractionated radiation (Grid): A new paradigm in the manage-ment of advanced cancers. Int J Radiat Oncol Biol Phys 1999;45:721–727.
10. Sathishkumar S, Dey S, Meigooni AS, et al. The impact ofTNF-alpha on Therapeutic efficacy following high dose spa-tially fractionated (GRID) radiation. Technol Cancer Res Treat2002;1:141–147.
11. Sathishkumar S, Boyanovsky B, Karakashian AA, et al. Ele-vated sphingomyelinase activity and ceramide concentrationin serum of patients undergoing high dose spatially fractionatedradiation treatment: Implications for endothelial apoptosis.Cancer Bio Ther 2005;4:979–986.
12. Huhn JL, Regine WF, Valentino JP, et al. Spatially fractionatedGRID radiation treatment of advanced neck disease associatedwith head and neck cancer. Technol Cancer Res Treat 2006;5:607–612.
13. Reiff JE, Huq MS, Mohiuddin M, Suntharalingam N. Dosimet-ric properties of megavoltage grid therapy. Int J Radiat OncolBiol Phys 1995;33:937–942.
14. Trapp JV, Warrington AP, Partridge M, et al. Measurement ofthe three-dimensional distribution of radiation dose in grid ther-apy. Phys Med Biol 2004;49:N317–N323.
15. Ha JK, Zhang G, Naqvi SA, et al. Feasibility of delivery gridtherapy using a multileaf collimator. Med Phys 2006;33:76–81.
16. Meigooni AS, Dou K, Meigooni DJ, et al. Dosimetric character-istics of a newly designed grid block for megavoltage photon ra-
diation and its therapeutic advantage using a linear quadraticmodel. Med Phys 2006;33:3165–3173.
17. Meigooni AS, Gnaster M, Dou K, Johnson EL. Dosimetric eval-uation of parallel opposed spatially fractionated radiation ther-apy of deep-seated bulky tumors. Med Phys 2007;34:599–603.
18. Zhang H, Johnson EL, Zwicker RD. Dosimetric validation ofthe MCNP Monte Carlo simulation for radiobiological studiesof megavoltage grid radiotherapy. Int J Radiat Oncol BioPhys 2006;66:1576–1583.
19. Zwicker R, Meigooni A, Mohiuddin M. Therapeutic advantageof grid irradiation for large single fraction. Int J Radiat OncolBio Phys 2003;58:1309–1315.
20. Hendricks JS, Mckinney GW, Waters LS, et al. MCNPX user’smanual, version 2.5e [Report LA-UR-04-0569]. Los Alamos,NM: Los Alamos National Laboratory, 2004.
21. RSICC Computer Code Collection. Monte Carlo N-particleTransport Code System. Los Alamos, NM: Los Alamos Na-tional Laboratory, 2000.
22. Spezi E, Lewis DG, Smith CW. Monte Carlo simulation and do-simetric verification of radiotherapy beam modifiers. PhysicsMed Biol 2001;46:3007–3029.
23. Brenner DJ, Hall EJ. Conditions for the equivalence of contin-uous to pulsed low dose rate brachytherapy. Int J Radiat OncolBio Phys 1991;20:181–190.
24. Thames HD, Bentzen SM, Turesson I, et al. Fractionation pa-rameters for human tissues and tumors. Int J Radiat OncolBio Phys 1989;56:701–710.
25. Withers HJ, Peters LJ, Taylor JM, et al. Late normal tissue se-quelae from radiation therapy for carcinoma of the tonsil: Pat-terns of fractionation study of radiobiology. Int J RadiatOncol Bio Phys 1995;33:563–568.
26. Chen SW, Liang JA, Yeh LS, et al. Comparative study of refer-ence points by dosimetric analyses for late complications afteruniform external radiotherapy and high-dose-rate brachyther-apy for cervical cancer. Int J Radiat Oncol Bio Phys 2004;60:663–671.
27. Dogan N, Leybovich LB, Sethi A. Comparative evaluation ofKodak EDR2 and XV2 films for verification of intensity mod-ulated radiation therapy. Phys Med Biol 2002;47:4121–4130.
28. Lopez Medina A, Teijeiro A, Garcia J, et al. Characterization ofelectron contamination of megavoltage photon beams. MedPhys 2005;32:1281–1292.
29. Mailaise EP, Fetile B, Daschanne PJ, et al. Initial slope of radi-ation survival curves is characteristic of the origin of primaryand established cultures of human tumor cells and fibroblasts.Radiat Res 1987;11:319–333.
30. Wigg DR. Plausible parameter values of normal tissues and tu-mors that may be used for predictive models and bioeffect plan-ning. In: Applied Radiobiology and Bioeffect Planning.Madison, WI: Medical Physics Publishing, 2001.




















