Biospecific fractionation matrices for sequence specific endonucleases

PII S0360-3016(00)00663-5
CLINICAL INVESTIGATION Head and Neck
A RADIATION THERAPY ONCOLOGY GROUP (RTOG) PHASE IIIRANDOMIZED STUDY TO COMPARE HYPERFRACTIONATION AND TWO
VARIANTS OF ACCELERATED FRACTIONATION TO STANDARDFRACTIONATION RADIOTHERAPY FOR HEAD AND NECK SQUAMOUS
CELL CARCINOMAS: FIRST REPORT OF RTOG 9003
KAREN K. FU, M.D.,* THOMAS F. PAJAK, PH.D.,† ANDY TROTTI, M.D.,‡
CHRISTOPHERU. JONES, M.D.,i SHARON A. SPENCER, M.D.,§ THEODORE L. PHILLIPS, M.D.,*ADAM S. GARDEN, M.D.,¶ JOHN A. RIDGE, M.D., PH.D.,# JAY S. COOPER, M.D.,* AND
K. KIAN ANG, M.D.,¶ FOR THE RADIATION THERAPY ONCOLOGY GROUP`
*University of California San Francisco, San Francisco, CA;†RTOG Statistical Unit, Philadelphia, PA;‡H. Lee Moffitt Cancer Centerat the University of South Florida, Tampa, FL;§University of Alabama at Birmingham, Birmingham, AL;iRadiation Oncology Center,
Sacramento, CA;¶University of Texas M.D. Anderson Cancer Center, Houston, TX;#Fox Chase Cancer Center, Philadelphia, PA;*New York University, New York, NY;`The other institutions that participated in the study are listed in the Appendix.
Purpose: The optimal fractionation schedule for radiotherapy of head and neck cancer has been controversial.The objective of this randomized trial was to test the efficacy of hyperfractionation and two types of acceleratedfractionation individually against standard fractionation.Methods and Materials: Patients with locally advanced head and neck cancer were randomly assigned to receiveradiotherapy delivered with: 1) standard fractionation at 2 Gy/fraction/day, 5 days/week, to 70 Gy/35 fractions/7weeks; 2) hyperfractionation at 1.2 Gy/fraction, twice daily, 5 days/week to 81.6 Gy/68 fractions/7 weeks; 3)accelerated fractionation with split at 1.6 Gy/fraction, twice daily, 5 days/week, to 67.2 Gy/42 fractions/6 weeksincluding a 2-week rest after 38.4 Gy; or 4) accelerated fractionation with concomitant boost at 1.8 Gy/fraction/day, 5 days/week and 1.5 Gy/fraction/day to a boost field as a second daily treatment for the last 12 treatmentdays to 72 Gy/42 fractions/6 weeks. Of the 1113 patients entered, 1073 patients were analyzable for outcome. Themedian follow-up was 23 months for all analyzable patients and 41.2 months for patients alive.Results: Patients treated with hyperfractionation and accelerated fractionation with concomitant boost hadsignificantly better local-regional control (p 5 0.045 andp 5 0.050 respectively) than those treated with standardfractionation. There was also a trend toward improved disease-free survival (p 5 0.067 and p 5 0.054respectively) although the difference in overall survival was not significant. Patients treated with acceleratedfractionation with split had similar outcome to those treated with standard fractionation. All three alteredfractionation groups had significantly greater acute side effects compared to standard fractionation. However,there was no significant increase of late effects.Conclusions: Hyperfractionation and accelerated fractionation with concomitant boost are more efficacious thanstandard fractionation for locally advanced head and neck cancer. Acute but not late effects are also increased.© 2000 Elsevier Science Inc.
Head and neck cancer, Fractionation, Radiotherapy, Hyperfractionation, Accelerated fractionation.
INTRODUCTION
The distribution of radiation dose over time, known asfractionation, is one of the most important factors determin-ing the outcome of radiotherapy. A variety of fractionationschedules including standard fractionation, hyperfraction-
ation, accelerated fractionation, and their variants have beenused in the radiotherapy of advanced head and neck cancer(1–3). In essence, altered fractionation is predicted to im-prove the therapeutic ratio through a differential responsebetween tumors and normal tissues to fractionated radio-therapy. Theoretically, with hyperfractionation it is possible
Reprint requests to: Karen K. Fu, M.D., Department of Radia-tion Oncology, University of California San Francisco, San Fran-cisco, CA 94143-0226. E-mail: [email protected]—Supported by research grants CA21661,CA37422, CA32115, and CA06294 from the National CancerInstitute. Its contents are solely the responsibility of the authorsand do not necessarily represent the official views of the NationalCancer Institute. We wish to acknowledge the dedication and hard
work of the RTOG clinical investigators, statisticians, clinicalresearch associates, administrative staff, and dosimetrists whohave contributed to the success of this trial. We are grateful for thevaluable contributions of Mr. Brian A. Berkey in the statisticalanalysis of the results, Ms. JoAnn Stetz, Ms. Janet Finnegan, andMs. Karen Kuhn in data management, and Ms. Elizabeth Martin indosimetry and quality assurance review of radiotherapy delivery.
Accepted for publication 3 March 2000.
Int. J. Radiation Oncology Biol. Phys., Vol. 48, No. 1, pp. 7–16, 2000Copyright © 2000 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/00/$–see front matter
7

to increase the total dose, thereby increasing the probabilityof tumor control without increasing late complicationsthrough the use of multiple smaller dose fractions. Accel-erated fractionation, by shortening the overall treatmenttime, should minimize tumor repopulation during treatmentand therefore increase the probability of tumor control for asimilar total dose.
The Radiation Therapy Oncology Group (RTOG) hasconducted several fractionation studies in head and neckcancer. An initial Phase III trial compared hyperfraction-ation (1.2 Gy/fraction, twice daily, 5 days/week to 60 Gy in5 weeks) to conventional fractionation (1.8–2.0 Gy/frac-tion/day, 5 days/week to 66–73.8 Gy in 6.5–7 weeks) (4). Inspite of a lower total dose used in the hyperfractionationarm, there was no significant difference in either local-regional control or survival. A subsequent randomizedPhase I/II dose escalation study of hyperfractionation estab-lished that total doses up to 81.6 Gy at 1.2 Gy/fraction,twice daily, can be delivered with acceptable acute sideeffects without increasing late effects (5–7). This trialshowed a trend toward increased local-regional control withdoses$72 Gy. Another Phase I/II trial of two types ofaccelerated fractionation schedules established their feasi-bility and tolerance in a multi-institutional cooperative trialsetting (8). Based on these results, this Phase III randomizedtrial was begun in 1991 to test the efficacy of hyperfrac-tionation and these two types of accelerated fractionationindividually against standard fractionation in locally ad-vanced head and neck cancer. The primary endpoint waslocal-regional control; the secondary endpoints were dis-ease-free survival and overall survival. The acute and lateadverse effects were also determined. This is the first reportof the outcome of this trial based on data received at theRTOG Headquarters by August 20, 1999.
METHODS AND MATERIALS
Patients and eligibility criteriaPatients 18 years or older with a Karnofsky performance
score$60 who had previously untreated Stage III or IV butMO squamous cell carcinoma of the oral cavity, orophar-ynx, supraglottic larynx, or Stage II–IV carcinoma of thebase of tongue or hypopharynx were eligible. Patients witha prior (within 5 years) or synchronous malignancy otherthan nonmelanoma skin cancer were excluded.
A medical history and physical examination, completeblood count, chest X-ray, computed tomography, or mag-netic resonance imaging of the head and neck, a diagram ofthe primary tumor and neck nodes, and a dental evaluationwere required. The disease was staged according to the 1988classification of the American Joint Committee on CancerStaging.
The National Cancer Institute and the participating insti-tutions approved the protocol. A study-specific informedconsent was obtained from all patients.
TreatmentEligible patients were randomized to receive radiotherapy
delivered using: 1) standard fractionation at 2 Gy/fraction/day, 5 days/week, to 70 Gy/35 fractions/7 weeks; 2) hyper-fractionation at 1.2 Gy/fraction, twice daily, 6 hours apart, 5days/week to 81.6 Gy/68 fractions/7 weeks; 3) acceleratedfractionation with split at 1.6 Gy/fraction, twice daily, 6hours apart, 5 days/week, to 67.2 Gy/42 fractions/6 weeksincluding a 2-week rest after 38.4 Gy; or 4) acceleratedfractionation with concomitant boost at 1.8 Gy/fraction/day,5 days/week to large field1 1.5 Gy/fraction/day to boostfield given 6 hours after treatment of the large field for thelast 12 treatment days to a total dose of 72 Gy/42 fractions/6weeks. Additional boost doses not exceeding 5.0 Gythrough reduced fields to persistent primary tumor and/orclinically positive nodes were allowed. Neck dissection wasallowed for neck nodes.3 cm prior to radiotherapy at thediscretion of the responsible head and neck surgeon andradiation oncologist.
Radiotherapy was delivered using linear accelerators orcobalt-60 machines with a source-to-surface or source-to-isocenter distance$80 cm. Simulation films and beamverification port films were required for each treatment field.
A combination of lateral opposing fields, anterior andlateral wedged fields, or other field arrangements was usedto treat the primary tumor and the lymph nodes in the upperneck. A single anterior field was used to treat the neckbelow the fields for the primary tumor. For patients withnodes .6 cm, supraclavicular nodes, or pyriform sinustumors that were T3 or T4 or with clinically positive nodes,the anterior field could extend 5 cm inferiorly to include theupper mediastinum. All fields were treated on each treat-ment day.
At least two field reductions were recommended for allfour arms. The first field reduction off the spinal cordoccurred at 40–44 Gy for arm 1, 45.6 Gy for arm 2, and38.4 Gy for arm 3. The second field reduction occurred at50–60 Gy for arm 1, 50.4–60.0 Gy for arm 2, and 51.2–60.8 Gy for arm 3. A third field reduction at 69.4 Gy wasrecommended for arm 2. A minimum 2-cm margin aroundthe initial tumor volume and positive neck node(s) for thefirst field reduction, a minimum of 1–1.5 cm margin for thesecond field reduction, and a minimum 1 cm margin for thethird field reduction were required. For arm 4, the concom-itant boost field with a minimum 1–1.5 cm margin aroundthe initial tumor volume and positive neck node(s) wasbegun at 32.4 Gy. The primary treatment fields were re-duced off the spinal cord at 45 Gy.
Follow-upDuring treatment, patients were examined weekly. Once
treatment ended, patients were evaluated at 4 weeks, thenevery 3 months for the first 1–1.5 years, every 4 monthsfrom 18 months through 3 years, biannually in years 3–5,and annually thereafter.
In addition to tumor status, acute and late (occurring.90days from start of treatment) normal tissue effects were
8 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 1, 2000

graded with the RTOG radiation morbidity scoring criteria(9).
Randomization proceduresPatients were enrolled by telephone call to the RTOG
headquarters. Following confirmation of their eligibility,patients were stratified by Karnofsky Performance Score(90–100 vs. 60–80), N-Stage (N2 vs. N1), and primarysite (oral cavity versus oropharynx versus hypopharynx andlarynx). The randomization scheme described by Zelen (10)was used to achieve balance in the treatment assignmentsamong the institutions.
Quality controlRadiotherapy records of each patient, including simula-
tion and verification port films, total dose, number of frac-tions, and elapsed treatment days relative to the protocolprescription were reviewed by the two radiation oncologystudy co-chairs (K. K. Fu and K. K. Ang) with the RTOGstaff. Calibration of each institution’s equipment was ob-tained from the Radiological Physics Center at the Univer-sity of Texas M. D. Anderson Cancer Center. Each institu-tion had their records audited at least once every 3 years asmandated by the National Cancer Institute.
Statistical analysisThe trial was designed to test whether any of the three
altered fractionation schemes improved local-regional con-trol compared to standard fractionation. Since it involvedthe comparison of three “experimental” treatments to asingle “control” treatment, the Dunnett’s two-sided multipletest (11) was used to adjust for multiple comparisons. Thesample size was calculated using Bristol’s modification(12). The 2-year local-regional control rate was used as theprimary endpoint because local-regional failure after 2 yearswas infrequent and the arcsine transformation for the bino-mial distribution normalized the variable so that Dunnett’stest could be employed. The baseline 2-year local-regionalcontrol rate for standard fractionation based on a previousRTOG study was 40% (13). The study was designed todetect a 15% difference. The Type I error rate and thestatistical power were set at 0.05 and 0.80. The sample sizewas increased by 20% to allow for patients who wereineligible, lost to follow-up, or died without local-regionalfailure before 2 years. Thus, the targeted sample size for thestudy was 1080 patients.
To permit comparisons with other published reports, lo-cal-regional control, disease-free survival, and overall sur-vival were estimated with the Kaplan-Meier method (14).The log-rank statistic was used to test for differences but noadjustments were made for multiple testing (15). Becauselocal-regional failure is a cause-specific failure and patientscould die without failing either locally or regionally, we alsoperformed the cumulative incidence analysis (16) and usedthe Gray’s test to test for differences (17). Since the twoapproaches yielded remarkably similar results, only theresults from the first approach are described in this report.
Data monitoringA formal RTOG Data Monitoring Committee (DMC)
was in place to oversee the trial’s progress. They reviewedthe interim analyses after enrolling 30%, 60%, and 100% ofthe targeted accrual.
RESULTS
Characteristics of the patientsBetween September 30, 1991 and August 1, 1997, 1113
patients were entered. Of these, 28 patients who were sub-sequently found to be ineligible, 5 who refused protocoltreatment or died before the start of treatment, and 7 whohad inadequate data were excluded. The remaining 1073patients form the basis of this outcome analysis.
Table 1 shows the pretreatment patient characteristics.They were well balanced among the treatment groups. Oro-pharynx was the most common primary site. The overallStage was II (tongue base and hypopharynx primaries only)in 3.4%, III in 28.3%, and IV in 68.3% of the patients.
Treatment and complianceThe median dose (Gy), number of fractions, and overall
time (days) were 70.3, 35, and 50 for standard fractionation,81.6, 68, and 50 for hyperfractionation, 67.6, 42, 43 foraccelerated fractionation with split, and 72, 42, and 43 foraccelerated fractionation with concomitant boost respec-tively. Eighty-eight percent of the patients had their treat-ment delivery scored as in accordance with the protocol orwith minor variations. The radiotherapy delivery was scoredas having major but acceptable deviations in 5.6%, unac-ceptable major deviations in 1.7%, and incomplete treat-ment due to disease progression, death, or patient refusal in4.7% of the patients. There was no significant difference incompliance among the treatment groups.
OutcomeThe median follow-up was 23 months for all analyzable
patients and 41.2 months for surviving patients. Both thehyperfractionation and the accelerated fractionation withconcomitant boost groups had significantly increased local-regional control rate at two years (p , 0.05 byDunnett’stest). Results of Kaplan-Meier estimates of local-regionalcontrol, disease-free survival, and overall survival areshown in Figs. 1–3. Local-regional control significantlyincreased in patients treated with hyperfractionation (p 50.045 by log-rank test) or accelerated fractionation withconcomitant boost (p 5 0.05 bylog-rank test) compared tostandard fractionation (Fig. 1). There was a trend towardimproved disease-free survival (Fig. 2) (p 5 0.067 forhyperfractionation, andp 5 0.054 foraccelerated fraction-ation with concomitant boost by log-rank test) but no signifi-cant difference in overall survival (Fig. 3). Patients treated withaccelerated fractionation with split had similar outcome tothose treated with standard fractionation. Table 2 shows the2-year local-regional control rate, disease-free survival, andoverall survival for the different treatment groups.
9Altered fractionation for head and neck cancer● K. K. FU et al.

Sites of failureThe primary site was the most common location of treat-
ment failure. The 2-year local (primary site) failure rateswere 43.7%, 37.8%, 43.0%, and 36.9% and the 2-year nodalfailure rates were 32.1%, 26.6%, 30.8%, and 33.3% for thestandard fractionation, hyperfractionation, accelerated frac-tionation with split, and accelerated fractionation with con-comitant boost respectively. The incidence of distant me-
tastasis at 2 years was 17.8%, 16.8%, 18.0%, and 16.6%respectively.
Adverse effectsTables 3 and 4 show the site and grade of worst acute and
late adverse effects by treatment group. The incidence ofGrade 3 or worse acute and late effects was 35.0% and26.8% for standard fractionation, 54.5% and 28.0% for
Table 1. Characteristics of the patients*
Characteristics
Standardfractionation(N 5 268)
Hyper-fractionation(N 5 263)
Acceleratedfractionation with split
(N 5 274)
Acceleratedfractionation withconcomitant boost
(N 5 268)
Number of patients (Percent)
GenderMale 199 (74%) 211 (80%) 220 (80%) 224 (84%)Female 69 (26%) 52 (20%) 54 (20%) 44 (16%)
RaceWhite 190 (71%) 177 (67%) 197 (72%) 191 (71%)Hispanic 17 (6%) 16 (6%) 17 (6%) 16 (6%)Black 48 (18%) 57 (22%) 50 (18%) 44 (16%)Oriental 2 (1%) 4 (2%) 3 (1%) 1 (1%)Native American 1 (1%) 1 (1%) 1 (1%) 2 (1%)Indian 2 (1%) 1 (1%) 2 (1%) 2 (1%)Filipino 1 (1%) 0 0 0Other 0 1 (1%) 0 3 (1%)Unknown 7 (3%) 6 (2%) 4 (1%) 9 (3%)
Age,60 123 (46%) 131 (50%) 120 (44%) 118 (44%)$60 145 (54%) 132 (50%) 154 (56%) 150 (56%)Median 60 60 61 61Range 30–86 34–86 34–90 31–88
Primary siteOral cavity 31 (12%) 26 (9%) 29 (11%) 24 (9%)Oropharynx 159 (59%) 160 (61%) 165 (60%) 165 (62%)Hypopharynx 34 (13%) 28 (11%) 40 (15%) 39 (15%)Supraglotti 44 (16%) 49 (19%) 40 (15%) 40 (15%)Larynx
KPS60 17 (6%) 11 (4%) 10 (4%) 11 (4%)70 28 (10%) 31 (12%) 34 (12%) 29 (11%)80 60 (22%) 57 (22%) 63 (23%) 64 (24%)90 120 (45%) 141 (54%) 118 (43%) 116 (43%)100 43 (16%) 23 (9%) 49 (18%) 48 (18%)
T-StageT1 15 (6%) 14 (5%) 18 (7%) 17 (6%)T2 77 (29%) 68 (26%) 72 (26%) 71 (26%)T3 102 (38%) 99 (38%) 108 (39%) 97 (36%)T4 74 (28%) 82 (31%) 76 (28%) 83 (31%)
N-StageN0 62 (23%) 60 (23%) 62 (23%) 55 (21%)N1 48 (18%) 58 (22%) 55 (20%) 53 (20%)N2A 29 (11%) 22 (8%) 30 (11%) 21 (8%)N2B 48 (18%) 49 (19%) 59 (22%) 49 (18%)N2C 49 (18%) 46 (17%) 39 (14%) 53 (20%)N3 32 (12%) 28 (11%) 29 (11%) 37 (14%)
AJC StageStage II 11 (4%) 11 (4%) 7 (3%) 9 (3%)Stage III 80 (30%) 78 (30%) 73 (27%) 71 (26%)Stage IV 177 (66%) 174 (66%) 194 (71%) 188 (70%)
* Because of rounding, not all percentages total 100.
10 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 1, 2000

hyperfractionation, 50.4% and 27.6% for accelerated frac-tionation with split, and 58.8% and 37.2% for acceleratedfractionation with concomitant boost. As expected, the mostcommon sites of acute side effects were the mucous mem-branes and the pharynx. The most common sites of Grade 3or worse late effects were the pharynx and the salivarygland. Compared to the standard fractionation group, allthree altered fractionation groups had significantly in-creased Grade 3 or worse acute side effects (p , 0.0001for hyperfractionation,p 5 0.0002 for accelerated frac-tionation with split, andp , 0.0001 foraccelerated frac-tionation with concomitant boost). However, only the ac-celerated fractionation with concomitant boost group had
significantly increased Grade 3 or worse late effects (p 50.011). Because the RTOG defines late effects as thosenoted .90 days from the start of radiotherapy, some ofthese late effects were actually prolonged acute effects. Asshown in Table 5, there was no significant difference in thefrequency of Grade 3 or worse late effects reported at 6–24months after treatment start among the different treatmentgroups.
DISCUSSION
This is the largest randomized trial of altered fraction-ation in the radiotherapy of locally advanced head andneck cancer ever conducted. Our results suggest that both
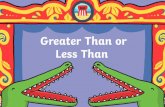
Fig. 1. Kaplan-Meier estimates of the duration of local-regionalcontrol of disease.
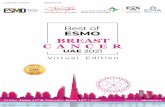
Fig. 2. Kaplan-Meier estimates of disease-free survival.
11Altered fractionation for head and neck cancer● K. K. FU et al.

total dose and treatment duration (or overall time) areimportant in the outcome of radiotherapy. Local-regionalcontrol was significantly increased by an increase of the
total dose without changing the overall time using hy-perfractionation or by a shortening of the overall timewhile maintaining the same total dose using acceleratedfractionation with concomitant boost.
In contrast to historical comparisons (18 –22), acceler-ated fractionation with split was not shown to improvelocal-regional control in this randomized trial. Any po-tential gain with accelerated fractionation may have beennegated by the interruption of treatment during the splitand a slightly lower total dose than standard fraction-ation. It is also interesting that in successive RTOGrandomized trials in head and neck cancer, the 2-yearlocal-regional control rate has improved over time from29% in the late 1970s (4) to 40% in the late 1980s (13)to 46% in the current trial.
In addition to this RTOG trial, hyperfractionation hasalso been shown to improve the outcome of radiotherapyfor head and neck cancer in four other randomized trials(23–26). The trial with the longest follow-up conductedby the European Organization for Research and Treat-ment of Cancer (EORTC) showed that an increase of totaldose from 70 Gy with standard fractionation to 80.5 Gywith hyperfractionation led to an increase of local controlof intermediate-stage (T2-3, N0-1) oropharyngeal carci-noma (excluding the base of tongue) without an increaseof late complications. Similar results are seen in thisRTOG trial even though it included patients with base oftongue carcinoma and other head and neck primary sitesand more advanced stages of disease.
Results of randomized trials of accelerated fractionationare less consistent (27–31). A variety of accelerated sched-ules have been studied. In general, local control increasedwith a shortening of the overall time by 1–2 weeks whilemaintaining a similar total dose to standard fractionation(27, 29, 31). However, no improvement was seen when alower total dose than the standard fractionation was used(32). Late effects increased significantly with a thrice dailyschedule or delivery of$14 Gy per week without a reduc-tion of total dose (29, 33, 34). In this RTOG trial, shorteningthe overall time using a concomitant boost technique alsoincreased local-regional control. Our results and others sup-port the hypothesis that tumor repopulation during radio-therapy is a major cause of treatment failure in head andneck cancer.
In this RTOG trial, all three altered fractionationschedules resulted in increased acute toxicity compared
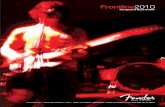
Fig. 3. Kaplan-Meier estimates of overall survival.
Table 2. 2-Year local-regional control, disease-free survival, and overall survival by treatment
2-Year endpoints
Standardfractionation(N 5 268)
Hyper-fractionation(N 5 263)
Acceleratedfractionation with split
(N 5 274)
Acceleratedfractionation withconcomitant boost
(N 5 268)
Local-regional control 46.0% 54.4% 47.5% 54.5%Disease-free survival 31.7% 37.6% 33.2% 39.3%Overall survival 46.1% 54.5% 46.2% 50.9%
12 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 1, 2000

to standard fractionation. However, only the acceleratedfractionation with concomitant boost group had signifi-cantly increased late effects. Because the RTOG used 90days from treatment start as a cutoff date for scoringacute and late effects, any acute adverse effects lasting.90 days would have been reported as late effects. Someof these late effects were actually prolonged acute ef-fects. In fact, most of the late effects resolved with timeand there was no significant difference in the frequencyof reported late effects at 6 –24 months after treatmentstart among the treatment groups.
At the present time, the major limitation of altered fraction-ation radiotherapy or combined radiotherapy and chemother-apy for head and neck cancer is increased acute reaction,primarily acute mucositis (35, 36). Several toxicity antagonistsare under active investigation (37). In the future, some of theseagents may decrease the acute and late effects of cancer ther-
apy. The therapeutic ratio may also be improved by usingconformal and intensity-modulated radiotherapy. These mod-ern radiotherapy techniques have the capability of improvingtumor target coverage while minimizing the dose to and vol-ume of the surrounding normal tissues irradiated (38–40).Their routine use in the treatment of head and neck cancer isanticipated in the near future.
Although both hyperfractionation and accelerated frac-tionation with concomitant boost resulted in a gain in local-regional control and disease-free survival, the overall sur-vival did not change significantly in this analysis. Clearly,additional treatment modifiers are needed to further improvethe prognosis of patients with locally advanced head andneck cancer. Data in the literature suggest that chemother-apy given concurrently with radiotherapy improves the re-sults over radiotherapy alone for locally advanced head andneck cancer (36, 41–43). However, the optimal chemother-
Table 3. Worst acute adverse effects of radiotherapy
Organ/Tissue Grade
Standardfractionation(N 5 268)
Hyper-fractionation(N 5 263)
Acceleratedfractionation with split
(N 5 274)
Acceleratedfractionation with
concomitantboost (N 5 268)
Number of patients (Percent)
Skin Grade1 93 (35) 76 (29) 121 (44) 80 (30)Grade2 131 (49) 138 (52) 113 (41) 148 (55)Grade3 20 (7) 29 (11) 8 (3) 29 (11)Grade4 0 (0) 1 (1) 0 (0) 0 (0)
Mucous membrane Grade1 33 (12) 27 (10) 25 (9) 30 (11)Grade2 146 (54) 111 (42) 118 (43) 104 (39)Grade3 67 (25) 109 (41) 109 (40) 122 (46)Grade4 0 (0) 1 (1) 3 (1) 1 (1)
Salivary gland Grade1 57 (21) 60 (23) 60 (22) 50 (19)Grade2 179 (67) 170 (64) 175 (64) 193 (72)
Pharynx/Esophagus Grade1 58 (22) 40 (15) 36 (13) 30 (11)Grade2 117 (44) 112 (42) 128 (47) 122 (46)Grade3 30 (11) 68 (26) 59 (22) 78 (29)Grade4 0 (0) 0 (0) 0 (0) 1 (1)
Larynx Grade1 76 (28) 58 (22) 67 (24) 59 (22)Grade2 45 (17) 57 (22) 49 (18) 67 (25)Grade3 9 (3) 16 (6) 10 (4) 19 (7)Grade4 0 (0) 0 (0) 2 (1) 0 (0)
Upper gastrointestinal Grade1 27 (10) 25 (9) 24 (9) 20 (7)Grade2 21 (8) 37 (14) 35 (13) 43 (16)Grade3 4 (2) 3 (1) 2 (1) 6 (2)
Subcutaneous Grade1 21 (8) 24 (9) 41 (15) 34 (13)Grade2 3 (1) 11 (4) 5 (2) 7 (3)
Ear Grade1 6 (2) 5 (2) 10 (4) 14 (5)Grade2 1 (1) 2 (1) 1 (1) 5 (2)
Spinal cord Grade1 0 (0) 0 (0) 2 (1) 0 (0)Bone Grade1 1 (1) 0 (0) 0 (0) 0 (0)Joint Grade1 2 (1) 0 (0) 2 (1) 3 (1)
Grade2 0 (0) 0 (0) 2 (1) 0 (0)Grade3 0 (0) 0 (0) 0 (0) 1 (1)
Other Grade1 8 (3) 6 (2) 13 (5) 8 (3)Grade2 6 (2) 12 (5) 7 (3) 10 (4)Grade3 2 (1) 3 (1) 1 (1) 1 (1)
Maximum toxicityper patient
Grade1 12 (5) 9 (3) 20 (7) 11 (4)Grade2 154 (57) 102 (39) 113 (41) 95 (36)Grade3 94 (35) 142 (54) 133 (49) 155 (58)Grade4 0 (0) 2 (1) 5 (2) 2 (1)
13Altered fractionation for head and neck cancer● K. K. FU et al.

apy regimen to be combined with radiotherapy remains tobe determined. More recently, Phase II studies of biologicalagents such as the antibody against epidermal growth factorreceptor C225 also suggest a potential advantage for head
and neck cancer (44). Future studies are needed to deter-mine whether these chemical and biological modifiers willfurther improve the outcome of altered fractionation radio-therapy.
Table 4. Worst late adverse effects reported.90 days from treatment start
Organ/Tissue Grade
Standardfractionation(N 5 254)
Hyper-fractionation(N 5 253)
Acceleratedfractionation with split
(N 5 261)
Acceleratedfractionation withconcomitant boost
(N 5 261)
Number of patients (Percent)
Skin Grade1 108 (43) 111 (44) 114 (44) 107 (41)Grade2 36 (14) 56 (22) 35 (13) 52 (20)Grade3 3 (1) 3 (1) 2 (1) 4 (2)Grade4 5 (2) 4 (2) 3 (1) 4 (2)
Mucous membrane Grade1 62 (24) 59 (23) 62 (24) 82 (31)Grade2 71 (28) 94 (37) 65 (25) 66 (25)Grade3 4 (2) 9 (3) 7 (3) 15 (5)Grade4 7 (3) 10 (4) 12 (5) 14 (5)
Salivary gland Grade1 39 (15) 46 (18) 63 (24) 43 (16)Grade2 158 (62) 154 (61) 139 (53) 147 (56)Grade3 14 (6) 18 (7) 17 (7) 26 (10)Grade4 0 (0) 0 (0) 1 (1) 0 (0)
Pharynx/Esophagus Grade1 62 (24) 62 (25) 53 (20) 59 (23)Grade2 40 (16) 63 (25) 50 (19) 61 (23)Grade3 21 (8) 28 (11) 25 (10) 37 (14)Grade4 5 (2) 4 (2) 2 (1) 3 (1)
Larynx Grade1 65 (26) 70 (28) 65 (25) 65 (25)Grade2 37 (15) 40 (16) 31 (12) 58 (22)Grade3 8 (3) 11 (4) 7 (3) 9 (3)Grade4 1 (1) 5 (2) 3 (1) 1 (1)
Upper gastrointestinal Grade1 0 (0) 0 (0) 1 (1) 0 (0)Subcutaneous Grade1 74 (29) 56 (22) 67 (26) 72 (28)
Grade2 60 (24) 84 (33) 80 (31) 72 (28)Grade3 18 (7) 19 (8) 7 (3) 9 (3)Grade4 1 (1) 4 (2) 1 (1) 3 (1)Grade5 0 (0) 0 (0) 1 (1) 0 (0)
Ear Grade1 16 (6) 26 (10) 16 (6) 23 (9)Grade2 10 (4) 16 (6) 10 (4) 9 (3)Grade3 3 (1) 2 (1) 1 (1) 2 (1)
Spinal cord Grade1 6 (2) 5 (2) 10 (4) 10 (4)Grade2 0 (0) 1 (1) 2 (1) 1 (1)
Brain Grade1 1 (1) 3 (1) 4 (2) 5 (2)Grade2 1 (1) 0 (0) 0 (0) 0 (0)
Bone Grade1 1 (1) 2 (1) 2 (1) 4 (2)Grade2 3 (1) 1 (1) 2 (1) 2 (1)Grade3 0 (0) 3 (1) 1 (1) 0 (0)Grade4 4 (2) 4 (2) 4 (2) 1 (1)
Joint Grade1 12 (5) 16 (6) 22 (8) 22 (8)Grade2 11 (4) 13 (5) 12 (5) 12 (5)Grade3 3 (1) 6 (2) 3 (1) 5 (2)
Other Grade1 12 (5) 15 (6) 15 (6) 18 (7)Grade2 11 (4) 10 (4) 10 (4) 15 (6)Grade3 7 (3) 4 (2) 6 (2) 0 (0)Grade4 0 (0) 0 (0) 1 (1) 0 (0)Grade5 1 (1) 0 (0) 0 (0) 1 (1)
Maximum toxicityper patient
Grade1 27 (11) 19 (8) 42 (16) 19 (7)Grade2 126 (50) 141 (56) 128 (50) 116 (44)Grade3 48 (19) 48 (19) 52 (20) 75 (29)Grade4 19 (8) 23 (9) 19 (7) 21 (8)Grade5 1 (1) 0 (0) 1 (1) 1 (1)
14 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 1, 2000

REFERENCES
1. Withers HR. Biologic basis for altered fractionation schemes.Cancer1985;55:2086–2095.
2. Ang KK, Peters LJ. Principles and practices of oncology.PPOUpdates1994;4:1–15.
3. Ang KK. Altered fractionation trials in head and neck cancer.Semin Radiat Oncol1998;8:230–236.
4. Marcial VA, Pajak TF, Chang C, Tupchong L, Stetz J. Hy-perfractionated photon radiation therapy in the treatment ofadvanced squamous cell carcinoma of the oral cavity, phar-ynx, larynx, and sinuses, using radiation therapy as the onlyplanned modality: Preliminary report by the Radiation Ther-apy Oncology Group (RTOG).Int J Radiat Oncol Biol Phys1987;13:41–47.
5. Cox JD, Pajak TF, Marcial VA,et al. Dose-response for localcontrol with hyperfractionated radiation therapy in advancedcarcinomas of the upper aerodigestive tracts: Preliminary re-port of Radiation Therapy Oncology Group protocol 83-13.Int J Radiat Oncol Biol Phys1990;18:515–521.
6. Cox JD, Pajak TF, Marcial VA,et al. ASTRO Plenary: Inter-fraction interval is a major determinant of late effects, withhyperfractionated radiation therapy of carcinomas of upperrespiratory and digestive tracts: Results from Radiation Ther-apy Oncology Group protocol 8313.Int J Radiat Oncol BiolPhys1991;20:1191–1195.
7. Fu KK, Pajak TF, Marcial VA,et al. Late effects of hyper-fractionated radiotherapy for advanced head and neck cancer:Long-term follow-up results of RTOG 83-13 [see comments].Int J Radiat Oncol Biol Phys1995;32:577–588.
8. Fu KK, Pajak TF, Ang KK, Byhardt RW, Maor MH, BeitlerJJ. Randomized Phase I/II trial of two variants of acceleratedfractionation radiotherapy regimens for advanced head andneck cancer: Results of RTOG 88-09.Int J Radiat Oncol BiolPhys1995;32:589–598.
9. Cox JD, Stetz J, Pajak TF. Toxicity criteria of the RadiationTherapy Oncology Group (RTOG) and the European Organi-zation for Research and Treatment of Cancer (EORTC) [edi-torial]. Int J Radiat Oncol Biol Phys1995;31:1341–1346.
10. Zelen M. The randomization and stratification of patients toclinical trials.J Chronic Dis1974;27:365–375.
11. Dunnett CW. A multiple comparison procedure from compar-ing several treatments with a control.J Am Stat Assoc1995;50:1096–1121.
12. Bristol D. Designing clinical trials for two-sided multiplecomparisons with a control.Control Clin Trials1989;10:142–152.
13. Lee DJ, Pajak T, Marcial VA,et al. Results of an RTOG phaseIII trial (RTOG 85-27) comparing radiotherpay plus etanida-zole with radiotherapy alone for locally advanced head andneck carcinomas.Int J Radiat Oncol Biol Phys1995;32:567–576.
14. Kaplan EL, Meier P. Nonparametric estimation from incom-plete observations.J Am Stat Assoc1958;53:457–481.
15. Mantel N. Evaluation of survival data and two new rank orderstatistics arising in its consideration.Cancer Chem Rep1966;5:163–170.
16. Kalbfleish JD, Prentice RL. The statistical analysis of failuretimes data. New York: John Wiley; 1980.
17. Gray RJ. A class of K-sample tests for comparing the cumu-lative incidence of a competing risk.Ann Stat1988;16:1141–1154.
18. Wang CC, Blitzer PH, Suit HD. Twice-a-day radiation therapyfor cancer of the head and neck.Cancer1985;55:2100–2104.
19. Wang CC, Suit HD, Blitzer PH. Twice-a-day radiation therapyfor supraglottic carcinoma.Int J Radiat Oncol Biol Phys1986;12:3–7.
20. Wang CC. Local control of oropharyngeal carcinoma aftertwo accelerated hyperfractionation radiation therapy schemes.Int J Radiat Oncol Biol Phys1988;14:1143–1146.
21. Wang CC. Accelerated hyperfractionation radiation therapyfor carcinoma of the nasopharynx: Techniques and results.Cancer1989;63:2461–2467.
22. Wang CC, Nakfoor BM, Spiro IJ, Martins P. Role of accel-erated fractionated irradiation for supraglottic carcinoma: As-sessment of results.Cancer J Sci Am1997;3:88–91.
23. Datta NR, Choudhry AD, Gupta S. Twice a day versus once aday radiation therapy in head and neck cancer.Int J RadiatOncol Biol Phys1989;17:132.
24. Horiot JC, Le-Fur R, NGuyen T,et al. Hyperfractionationversus conventional fractionation in oropharyngeal carcino-ma: Final analysis of a randomized trial of the EORTC coop-erative group of radiotherapy.Radiother Oncol1992;25:231–241.
25. Sanchiz F, Milla A, Torner J,et al. Single fraction per dayversus two fractions per day versus radiochemotherapy in thetreatment of head and neck cancer.Int J Radiat Oncol BiolPhys1990;19:1347–1350.
26. Pinto LHJ, Canary PCV, Araujo CMM, Bacelar SC, SouhamiL. Prospective randomized trial comparing hyperfractionatedversus conventional radiotherapy in stages III and IV oropha-ryngeal carcinoma.Int J Radiat Oncol Biol Phys1991;21:557–562.
27. Ang KK, Trotti A, Garden AS,et al. Importance of overalltime factor in postoperative radiotherapy. In: Shah JP, JohnsonJT, editors.4th International Conference on Head and NeckCancer. Toronto, Canada: The Society of Head and NeckSurgeons and American Society of Head and Neck Surgery;1996. p. 231–235.
28. Awwad HK, Khafagy Y, Barsoum M,et al. Acceleratedversus conventional fractionation in the postoperative irradi-ation of locally advanced head and neck cancer: Influence oftumour proliferation.Radiother Oncol1992;25:261–266.
29. Horiot JC, Bontemps P, van den Bogaert W,et al. Acceleratedfractionation (AF) compared to conventional fractionation(CF) improves loco-regional control in the radiotherapy of
Table 5. Frequency of Grade 3 or worse late effects at various times after treatment start
Time aftertreatment start
(months)
Standardfractionation
Hyper-fractionation
Acceleratedfractionation with split
Acceleratedfractionation withconcomitant boost
Number of patients/Number of patients at risk (Percent)
6 26/248 (10) 35/247 (14) 22/254 (9) 32/249 (13)12 21/191 (11) 25/187 (13) 15/198 (8) 20/196 (10)18 7/145 (5) 20/160 (13) 14/146 (10) 9/150 (6)24 7/111 (6) 17/135 (13) 9/116 (8) 10/128 (8)
15Altered fractionation for head and neck cancer● K. K. FU et al.

advanced head and neck cancers: Results of the EORTC22851 randomized trial [see comments].Radiother Oncol1997;44:111–121.
30. Johnson CR, Schmidt-Ullrich RK, Wazer DE. Concomitantboost technique using accelerated superfractionated radiationtherapy for advanced squamous cell carcinoma of the head andneck.Cancer1992;69:2749–2754.
31. Overgaard J, Sand Hansen H, Overgaard M,et al. Conven-tional radiotherapy as primary treatment of squamous cellcarcinoma of the head and neck: A randomized multicenterstudy of 5 versus 6 fractions per week—report from theDAHANCA 7 trial. Int J Radiat Oncol Biol Phys1997;39:188.
32. Saunders MI, Dische S, Barrett A, Parmar MK, Harvey A,Gibson D. Randomised multicentre trials of CHART vs con-ventional radiotherapy in head and neck and non-small-celllung cancer: an interim report. CHART Steering Committee.Br J Cancer1996;73:1455–1462.
33. Maciejewski B, Skladowski K, Pilecki B,et al. Randomizedclinical trial on accelerated 7 days per week fractionation inradiotherapy for head and neck cancer: Preliminary report onacute toxicity.Radiother Oncol1996;40:137–145.
34. Jackson SM, Weir LM, Hay JH, Tsang VH, Durham JS. Arandomised trial of accelerated versus conventional radiother-apy in head and neck cancer.Radiother Oncol1997;43:39–46.
35. Kaanders JH, van-Daal WA, Hoogenraad WJ, van-der-KogelAJ. Accelerated fractionation radiotherapy for laryngeal can-cer, acute, and late toxicity.Int J Radiat Oncol Biol Phys1992;24:497–503.
36. Brizel DM. Radiotherapy and concurrent chemotherapy forthe treatment of locally advanced head and neck squamouscell carcinoma.Semin Radiat Oncol1998;8:237–246.
37. Trotti A. Toxicity antagonists in cancer therapy.Curr OpinOncol 1997;9:569–578.
38. Eisbruch A, Marsh LH, Martel MK,et al. Comprehensiveirradiation of head and neck cancer using conformal multiseg-mental fields: Assessment of target coverage and noninvolvedtissue sparing.Int J Radiat Oncol Biol Phys1998;41:559–568.
39. Eisbruch A, Ten Haken RK, Kim HM, Marsh LH, Ship JA.Dose, volume, and function relationships in parotid salivaryglands following conformal and intensity-modulated irradia-tion of head and neck cancer.Int J Radiat Oncol Biol Phys1999;45:577–587.
40. Wu Q, Manning M, Schmidt-Ullrich R, Mohan R. The poten-tial for sparing of parotids and escalation of biologicallyeffective dose with intensity-modulated radiation treatmentsof head and neck cancers: A treatment design study.Int JRadiat Oncol Biol Phys2000;46:195–205.
41. Fu KK. Combined modality therapy for head and neck cancer.Oncology1997;11:1781–1796.
42. Wendt TG, Grabenbauer GG, Reodel CM,et al. Simultaneousradiochemotherapy versus radiotherapy alone in advancedhead and neck cancer: A randomized multicenter study.J ClinOncol 1998;16:1318–1324.
43. Calais G, Alfonsi M, Bardet E,et al. Randomized trial ofradiation therapy versus concomitant chemotherapy and radi-ation therapy for advanced-stage oropharynx carcinoma [seecomments].J Natl Cancer Inst1999;91:2081–2086.
44. Wheeler RH, Spencer S, Buchsbaum D, Robert F. Monoclonalantibodies as potentiators of radiotherapy and chemotherapyin the management of head and neck cancer.Curr Opin Oncol1999;11:187–190.
APPENDIX
The following Radiation Therapy Oncology Group insti-tutions and their affiliates contributed to this study:
H. Lee Moffitt Cancer Center at the University of SouthFlorida; Radiological Associates of Sacramento; University ofAlabama at Birmingham Medical Center; University of Cali-fornia San Francisco; University of Texas–M.D. AndersonCancer Center; Fox Chase Cancer Center; New York Univer-sity Hospital; McGill University; Medical College of Wiscon-sin; Washington University; Montefiore Medical Center; Uni-versity of Western Ontario; Akron City Hospital; SUNYHealth Science Center/Brooklyn; Wayne State University;University of Pennsylvania Medical Center; Dartmouth Hitch-cock Medical Center; Albert Einstein Medical Center; Univer-sity of Puerto Rico/Med Sciences Ca; Emory University Af-
filiated Hospitals; University of Alberta; Thomas JeffersonUniversity Hospital; University of Rochester; LDS Hospital;Loyola University Medical Center; Johns Hopkins Hospital;University of Miami; Hamilton Regional Cancer Centre; MayoClinic; University of Kentucky Hospital; South Jersey Oncol-ogy Group CCOP; Wake Forest University Baptist MedicalCenter; Kansas City CCOP; South Nevada Cancer ResearchFoundation CCOP; North Shore University Hospital CCOP;University of California Davis Medical Center; Greenville,South Carolina CCOP; West Michigan Cancer Center CCOP;Atlanta Regional CCOP; Dayton CCOP; Main Line HealthCCOP; Christiana Care Health Services, Inc.; Columbia RiverCCOP; Upstate Carolina CCOP; James Haley Veterans Hos-pital.
16 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 1, 2000
Copyright © 2022 FDOKUMEN