
The diagnostic criteria for small fibre neuropathy: from symptoms to neuropathology
Upload
independentCategory
view
0download
0
Focal Upper Extremity Neuropathy in Neonates
Israel Alfonso, Daniel T. Alfonso, and Oscar Papazian
Focal upper extremity neuropathies are common in neonates. The brachial plexus is the most common site involved. Brachial plexus injuries may involve different structures, thus producing different clinical presentations: complete brachial plexus palsy, Duchenne-Erb palsy, upper-middle trunk brachial plexus palsy, Klumpke palsy, fascicular brachial plexus palsy, and bilateral brachial plexus palsy. The causes of brachial plexus palsy are obstetric injury, intrauterine compression, humeral osteomyelitis, hemangioma, exostosis of the first rib, neck compression, and neoplasm. The differential diagnosis of brachial plexus palsy includes pseudoparesis, amyopla- sia congenita, congenita varicella syndrome, and neurological lesions at other neuroanatomical levels. The cause and the degree of injury dictate the prognosis. The prognosis of obstetric brachial plexus injury is usually good. Copyright �9 2000 by W.B. Saunders Company
~ IOCAL UPPER extremity neuropathy in neo- nates may involve the brachial plexus or the
peripheral nerves.
BRACHIAL PLEXUS PALSY IN THE NEONATAL PERIOD
The clinical presentations of brachial plexus palsy depend on the brachial plexus structures involved. Knowledge of the anatomy of the bra- chial plexus and the structures that lead to it and arise from it is fundamental to understanding the multiple clinical presentations of brachial plexus palsy.
Neuroanatomy The most common arrangement of the brachial
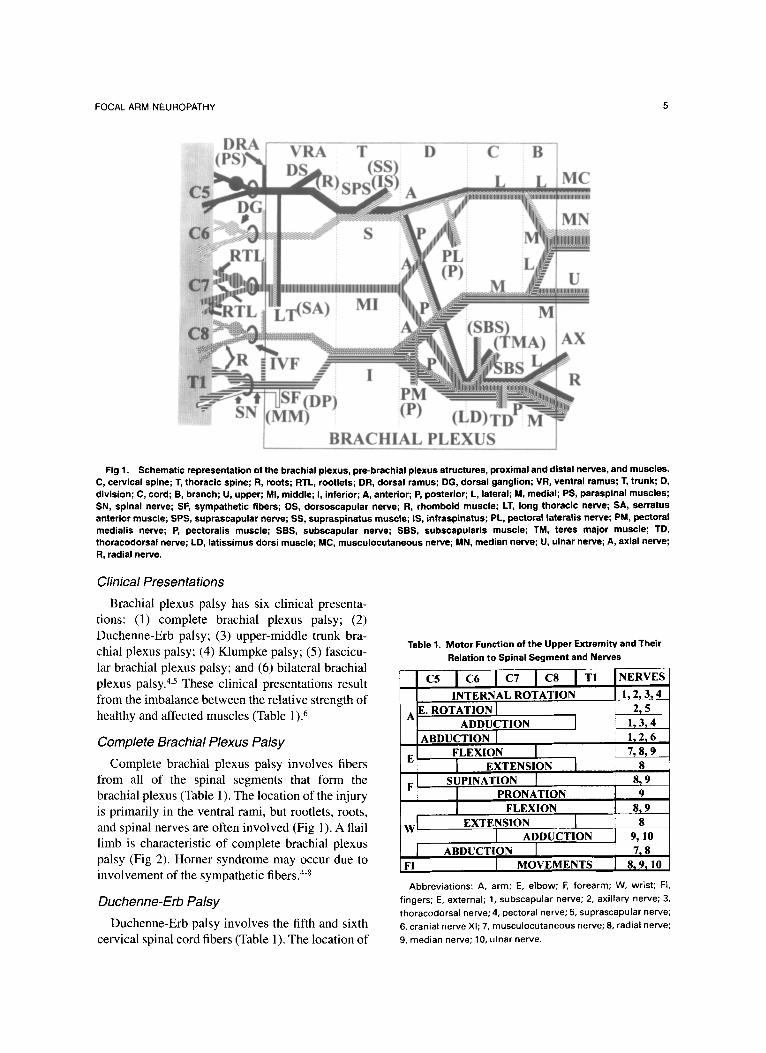
plexus and peripheral nervous system prebrachial plexus structures is represented in Figure 1.1-3 The ventral rootlets and roots are the axons of the motor neurons located in the anterior horn of the fifth cervical through the first thoracic spinal segments. The dorsal rootlets and roots are the proximal segment of the axons of the pseudounipolar sensory neurons of the spinal ganglion corresponding to the fifth cervical to the first thoracic spinal segments. The spinal nerves are formed by the union of the ventral roots and the distal segments of the axons of the spinal ganglion pseudounipolar sensory neu- rons. The spinal nerves leave the spinal canal through the intervertebral foramina. Each spinal nerve then splits into a dorsal ramus and a ventral ramus. The dorsal rarni supply the paraspinal muscles of the upper torso. The five ventral rami of
From the Department of Neurology, Miami Children's Hospi- tal, Miami, FL.
Address reprint requests to Israel Alfonso, MD, Department of Neurology, Miami Children's Hospital, 3200 SW 60th Court, Miami, FL 33155-3009.
Copyright �9 2000 by W.B. Saunders Company 1071-9091/00/0701-0004510.00/0
the fifth cervical to the first thoracic spinal seg- ments form the brachial plexus.
The five ventral rami of the fifth cervical to the first thoracic spinal segments form three trunks (superior, middle, and inferior). Each trunk splits into two divisions (anterior and posterior). The six divisions form three cords (lateral, medial, and posterior, named according to their relation with the axillary artery). Each cord splits in two branches (lateral and medial). The six branches form five clinically significant distal nerves (musculocutane- ous, median, ulnar, axillary, and radial nerves). In addition to the distal nerves, the brachial plexus also gives off: (1) seven clinically significant proximal nerves (dorsoscapular, long thoracic, su- prascapular, medial and lateral pectoral, subscapu- laris, and thoracodorsal nerves); (2) a branch to the phrenic nerve from the fifth cervical ventral ramus; and (3) the preganglionic sympathetic fibers to the superior cervical ganglion.J The preganglionic sym- pathetic fibers arise from the middle horus of the spinal cord usually at the levels of the first and second thoracic spinal segments. They travel with their appropriate rootlets, roots, spinal nerves, and ventral rami before they leave the brachial plexus to join the sympathetic trunk. In the sympathetic trunk they climb up the thoracic and cervical segments to reach the superior cervical ganglion, where they make contact with sympathetic neurons that produce the postganglionic sympathetic nerves that supply the dilator muscle of the iris, the smooth muscle portion of the levator palpebrae, the muscle of Mtiller, and the blood vessels of the head and face J, 2
The subclavian artery irrigates the brachial plexus. The second to the tenth spinal thoracic segments through postganglionic neurons in the stellate ganglion provide sympathetic innervation to the brachial plexus and the arm. 1,3
4 Seminars in Pediatric Neurology, Vol 7, No 1 (March), 2000: pp 4-14
FOCAL ARM NEUROPATHY 5
Fig 1. Schematic representation of the brachial plexus, pre-brachial plexus structures, proximal and distal nerves, and muscles. C, cervical spine; T, thoracic spine; R, roots; RTL, rootlets; DR, dorsal ramus; DG, dorsal ganglion; VR, ventral ramus; T, trunk; D, division; C, cord; B, branch; U, upper; MI, middle; I, inferior; A, anterior; P, posterior; L, lateral; M, medial; PS, paraspinal muscles; SN, spinal nerve; SF, sympathetic fibers; DS, dorsoscapular nerve; R, rhomboid muscle; LT, long thoracic nerve; SA, serratus anterior muscle; SPS, suprascapular nerve; SS, supraspinatus muscle; IS, infraspinatus; PL, pectoral lateralis nerve; PM, pectoral medialis nerve; P, pectoralis muscle; SBS, subscapular nerve; SBS, subscapularis muscle; TM, teres major muscle; TD, thoracodorsal nerve; LD, latissimus dorsi muscle; MC, musculocutaneous nerve; MN, median nerve; U, ulnar nerve; A, axial nerve; R, radial nerve.
Clinical Presentations
Brachial plexus palsy has six clinical presenta- tions: (1) complete brachial plexus palsy; (2) Duchenne-Erb palsy; (3) upper-middle trunk bra- chial plexus palsy; (4) Klumpke palsy; (5) fascicu- lar brachial plexus palsy; and (6) bilateral brachial plexus palsy. 4,s These clinical presentations result from the imbalance between the relative strength of healthy and affected muscles (Table 1). 6
Complete Brachial Plexus Palsy
Complete brachial plexus palsy involves fibers from all of the spinal segments that form the brachial plexus (Table 1). The location of the injury is primarily in the ventral rami, but rootlets, roots, and spinal nerves are often involved (Fig 1). A flail limb is characteristic of complete brachial plexus palsy (Fig 2). Homer syndrome may occur due to involvement of the sympathetic fibers. 4-8
Ouchenne-Erb Palsy
Duchenne-Erb palsy involves the fifth and sixth cervical spinal cord fibers (Table 1). The location of
Table 1. Motor Function of the Upper ExtremiW and Their Relation to Spinal Segment and Nerves
c, j c6 i c7 i c8 i T, IN "VES INTERNAL ROTATION [ 1, 2, 3, 4
E. ROTATION I 2, 5 A ADDUCTION ] 1, 3, 4
ABDUCTION I 1. r 21 6 FLEXION I 7, 8, 9
E I EXTENSION I S F L SUPINATION [ 8, 9
PRONATION 9 FLEXION 8, 9
WI EXTENSION [ 8 I ABDUCTION [ 9 , a0
l ABDUCTION T 7,8 F ! MOVEMENTS 81 9.t 10
Abbreviations: A, arm; E, elbow; F, forearm; W, wrist; FI, fingers; E, external; I, subscapular nerve; 2, axillary nerve; 3, thoracodorsal nerve; 4, pectoral nerve; 5, suprascapular nerve; 6, cranial nerve Xl; 7, musculocutaneous nerve; 8, radial nerve; 9, median nerve; 10, ulnar nerve.

6 ALFONSO, ALFONSO AND PAPAZIAN
Fig 2. Complete brachial plexus palsy. (A) The left limb rests fiat on the bed. (B) No motion of the left limb during the Moro reflex. (Reprinted with permission. T)
the injury is the superior trunk or at the fifth or sixth ventral rami (Fig 1). The affected extremity devel- ops a typical position when the neonate attempts to move it (Fig 3). Confrontation testing reveals weakness in shoulder abduction (supraspinatus and deltoid) and external rotation (infraspinatus), el- bow flexion (biceps and brachioradialis), and fore- arm supination (biceps and supinator). Confronta- tion testing of the wrist and finger do not reveal any weakness despite the typical wrist and hand posi- tion (Fig 3). The weakness of extensor carpi radialis (the only wrist extensor muscle that is innervated from the fifth and sixth cervical seg- ments) and the weakness of the finger extensor muscle is minima/(Table 1). Confrontation testing of the rhomboid, performed by holding the weak ann in a flexed position behind the torso at the level of the mid-lumbar region, may reveal some degree of scapular winging. 4-6,8
Upper-Middle Trunk Brachial Plexus Palsy
Upper-middle trunk brachial plexus palsy in- volves the fibers from the fifth to the seventh
cervical spinal segments (Table 1). The sites of injury may be at the superior and middle trunks, or at the fifth and sixth cervical ventral rami and the middle trunk (Fig 1). When the neonate attempts to move the affected arm, it takes on a position similar to the one seen with Duchenne-Erb palsy except at the wrist (Fig 4). Confrontation testing, unlike in Duchenne-Erb palsy, demonstrates wrist flexion and extension weakness. 4-8
Klumpke Palsy
Klumpke palsy involves the eighth cervical and first thoracic spinal segment fibers (Table 1). The sites of injury may be at the inferior trunk or at the eighth cervical and first thoracic ventral rami (Fig 1). Klumpke palsy is rare. Neonates with Klumpke palsy usually present with a floppy hand (Fig 5). The classic Klumpke palsy position seldom occurs in neonates. It is characterized by the following: (1) elbow flexion due biceps predominance (U'iceps weakness); (2) forearm supination due to biceps and supinator predominance (pronator quadratus weakness); (3) wrist extension due to predomi-

FOCAL ARM NEUROPATHY
to demonstrate involvement of the muscles inner- vated by the proximal brachial plexus nerves. 7,8
Bilateral Brachial Plexus Lesion
Bilateral brachial plexus palsy occurs in a signifi- cant number of patients. It is usually asymmetrical. The most common clinical presentations resemble bilateral Duchenne-Erb palsy or bilateral fascicular brachial plexus palsy. 4,5,8
Causes of Brachial Plexus Palsy
The causes of brachial plexus palsy in the neonatal period are few. Obstetric trauma is the most c o m m o n . 4-12 Obstetric trauma is associated with neuroma formation at the site of the injury. 8 Other causes of brachial plexus injury are intrauter- ine compression,13 humeral osteomyelitis,14 heman- gioma, 15 exostosis of the first r i b , 16 neck compres- sion, a7 and neoplasm, t8 Aplasia of the brachial plexus without any discemible etiology has been reported. 8
Fig 3. Duchenne-Erb palsy. The arm is internally rotated and adducted, the elbow is extended, the forearm is pronated, the wrist is flexed and adducted (ulnar deviation), and the fingers are flexed.
nance of the extensor carpi radialis (weakness of the wrist flexor group); and (4) clawlike deformity of the hand due to predominance of the forearm finger flexors and extensors over the small hand muscles (lumbricoids and other intrinsic hand muscles). Confrontation testing demonstrates weak- ness of wrist flexion and of all the small hand muscles. Homer syndrome occurs when the injury involves the sympathetic fibers at the rootlets, root, spinal nerve, or proximal ventral ramus. 4-8
Fascicular Brachial Plexus Palsy
Fascicular brachial plexus palsy refers to weak- ness of one muscle or a group of muscles in the ann due to injury of a small group of motor fibers in the brachial plexus. The sites of injury may be at the ventral rami, trunks, divisions, cords, or branches (Fig 1). The clinical manifestations of a fascicular lesion vary. A common presentation is the combina- tion of weakness of the muscles innervated by the distal brachial plexus nerves and Homer's syn- drome (Fig 6). Electromyography is often needed
Fig4. Upper-middle trunk brachial plexus palsy. The arm is internally rotated and adducted, the elbow is extended, the forearm is pronated, and the wrist is in a neutral position (wrist flexor and extensors are equally weak).

8 ALFONSO, ALFONSO, AND PAPAZIAN
Fig 5. Klumpke palsy. The wrist is flexed and the fingers are extended following the forces of gravity (floppy hand), (Reprinted with permission J)
Obstetric Brachial Plexus Palsy
Obstetric trauma is often associated with trauma to other structures. 4,9-12 Clavicular fractures occur in a significant number of patients. The presence of clavicular fractures does not predict outcome. 19 Fractures of the humerus are less frequent. Torticol- lis is sometimes noted after the first month. Poste- rior or anterior dislocations and subluxation of the shoulder may occur. Y-scapular view radiograph and magnetic resonance imaging (MRI) of the shoulder may be necessary to detect them. Cephalo- hematomas are frequently associated with obstetric brachial plexus palsy. Seizure, lethargy, coma, or weakness of the lower facial quadrant and leg suggest injury to the central nervous system (CNS). Cervical cord injury should be considered in neo- nates with upper extremity diplegia, especially if a
loud "clacking" sound suggestive of a vertebral column injury is heard during delivery or if there is bilateral lower extremity weakness and bowel and bladder incontinence. MRI of the brain and spine is warranted in all patients with suspected CNS involvement. Peripheral nervous system injury to structures other than the brachial plexus and preb- rachial plexus structures may occur in neonates with obstetric brachial plexus palsy. Facial nerve injury is the most common. Facial nerve injury usually occurs just distal to the stylomastoid ori- rice, but in some cases it occurs in the facial canal. Petrous bone fracture and hemotympanum may be present with facial nerve injury in the facial canal. Hemifacial weakness is the usual presentation. Tongue weakness due to hypoglossal nerve injury and vocal cord paralysis due to recurrent laryngeal nerve injury have also been reported. Diaphrag- matic paralysis can lead to difficulties withdrawing artificial ventilation.11
Intrauterine Compressive Brachial Plexus Palsy
Intrauterine compressive brachial plexus palsy is usually associated with sustained deformity of the upper limb. Clinical evidence of trauma before delivery may include limb contractures and a smaller affected hand. Decreased calcium in the bone of the affected limb and electromyographic signs of denervation in the first week of life may be present.13 The use of electromyography in determin- ing the time that brachial plexus injury occurred has served as acceptable evidence in court, but it has been questioned by medical researchers. 12,2~
Fig 6. Fascicular brachial plexus palsy. {/It) Inability to extend the distal phalanx of the right thumb. (B) Horner syndrome affecting the right eye, (Reprinted with permission. 7)

FOCAL ARM NEUROPATHY 9
Humeral Osteomyelitis
Humeral osteomyelitis in neonates with group-B streptococcal septicemia may present with sudden onset of arm weakness several days after birth. Neonates are usually afebrile and do not look septic. Ischemia of the brachial plexus is the most likely pathophysiology. Bone scan is the study of choice to detect humeral osteomyelitis. 14
Neonatal Hemangiomatosis
Brachial plexus palsy caused by a large hemangi- oma has been described in a neonate. ]5 The patient had the typical cutaneous lesions of neonatal hem- angiomatosis. Duchenne-Erb palsy was present from birth. Improvement occurred by 7 months of age, but some limitation of arm movement re- mained.
Exostosis of the First Rib
Exostosis of the first rib may present with congenital brachial plexus palsy. The injury to the brachial plexus occurred at the level of the divi- sions (Fig 1). A mass under the clavicle should alert the examiner to the possibility of exostosis of the first rib. Conventional radiography establishes the diagnosis. 16
Neck Compression
Pressure from the seal used in a head box during constant positive airway pressure produced bra- chial plexus palsy in two neonates. The clinical presentations were characteristic of Duchenne-Erb palsy. The weakness was not noted immediately after the use of the head box. Neck scarring was present.J7
Neoplasm
Neoplasms originating in, or involving, the bra- chial plexus are rare in neonates. They include neuromas and rhabdoid tumors. Neuromas produce slowly progressive arm monoparesis that may be associated with paresthesias in the distribution of the shoulder. In a patient with a neuroma, weakness was not present at birth, but developed after the third week. Rhabdoid tumors produce rapidly pro- gressive arm weakness and supraclavicular mass (Fig 7). In a patient with a rhabdoid tumor, weakness was not present at birth, but developed after the fifth day) 8
Fig 7. Neck mass in a neonate with left brachial plexus due to Involvement of the brachial plexus by a rhabdoid tumor.
Differential Diagnosis of Brachial Plexus Palsy
The differential diagnosis of brachial plexus palsy includes pseudoparesis, amyoplasia conge- nita, lesions involving the anterior horn cells, pyramidal tract, cerebellum, peripheral nervous system prebrachial plexus structures, and periph- eral nerves.
Pseudoparesis Pseudoparesis may be due to pain or limb
deformation. The neonate with a painful arm grimaces with
minimal attempts to passively move the affected ann. The painful arm does not adopt any of the typical postures that occur in most patients with brachial plexus palsy. The most frequent cause of pseudoparesis due to pain is humeral fracture. Displaced fractures are diagnosed by conventional radiography. Nondisplaced fractures are detected by bone scan; evidence of new periosteal formation appears on plain radiographs at about 10 to 14 days. Bone, joint, and soft-tissue infection may produce arm pseudoparesis due to pain. Congenital syphi- litic osteochondritis may mimic Duchenne-Erb palsy. 2~ Arm weakness resembling bilateral Duch- enne-Erb palsy has been reported with cervical vertebral body infection. 22
Upper limb pseudoparesis due to limb deformity is caused by compression of the limb against the walls of the uterus. The affected limbs have a fixed

10 ALFONSO, ALFONSO, AND PAPAZIAN
position at birth. Moderate passive force will change the limb from its original position but, on release, the limb springs back to the original position.
Amyoplasia Congenita Amyoplasia congenita is a form of arthrogrypo-
sis congenita multiplex of unknown cause. Amyo- plasia congenita produces typical upper limb defor- mities that may resemble bilateral Duchenne-Erb palsy (Fig 8). Amyoplasia congenita is differenti- ated from bilateral brachial plexus injury by the presence of joint rigidity, the persistence of the fixed deformity at rest, and the presence of skin dimples. 23
Anterior Horn Cell Injury
Anterior horn cell injury occurs with congenital cervical spinal atrophy and congenital varicella syndrome.
Congenital cervical spinal atrophy produces se- vere symmetric lower motor neuron deficit in the
Fig 8. Amyoplasia congenita. The arms are internal rotated and adducted, the elbows are extended, the forearms are pronated, the wrists are flexed and adducted (ulnar deviation). Skin dimple at the wrist. Compare this image with Figure 3.
Fig 9. Congenital varicella syndrome. Atrophy and flaccid right arm with cutaneous scarring, amputation of the thumb, and right Homer syndrome. Compare with Figure 2. (Re- printed with permission. 7)
upper extremities from birth. 24 Most patients have arthrogryposis of the elbows and fingers. Hyperto- nia of the lower extremities may occur. Cervicotho- racic atrophy associated with intramedullary an- gioma was reported in one patient. 25
Congenital varicella syndrome may produce find- ings similar to those produced by complete brachial plexus palsy, including Homer's syndrome (Fig 9). 26 The neuroanatomic structures that take the brunt of the injury are the anterior horn cells and the dorsal root ganglia. The association of congeni- tal weakness, atrophy, cutaneous scarring, ampu- tated fingers, and a history of maternal varicella infection during pregnancy is diagnostic of congeni- tal varicella syndrome. The risk of congenital varicella syndrome in the offspring of a mother who has varicella during pregnancy is about 2%. The risk is highest if the maternal infection occurs in the first month of pregnancy, z7

FOCAL ARM NEUROPATHY 11
Pyramidal Tract Lesions
Pyramidal tract lesions should be suspected in all neonates with acquired arm weakness and in some neonates with congenital arm weakness. A pyrami- dal tract lesion should be suspected in any neonate with congenital arm weakness who does not have the typical arm posture associated with of Duch- enne-Erb palsy or upper-middle trunk syndrome and in neonates with neurological symptoms that suggest CNS involvement. An exaggerated Moro reflex and brisk musculotendinous reflexes in the weak arm are characteristic of pyramidal tract involvement (Fig 10). Electromyographic studies do not reveal fibrillation and positive sharp waves. 2,27 Neonates with suspected pyramidal tract lesions should undergo MRI of the brain and cervical and thoracic spine. 25,27
Cerebellar Lesions
Cerebellar lesions may produce arm hypotonia. Ann hypotonia and ann weakness are difficult to differentiate in the newborn period. The presence of pendular biceps stretch muscle reflex, leg hypo- tonia, and preservation of Moro reflex suggests a cerebellar lesion. Decreased fusiform activity is the probable cause of cerebellar hypotonia. 2 MRI usu- ally detects cerebellar lesions. Electromyogram of the affected limbs does not show fibrillations.
Peripheral Nervous System Prebrachial Plexus Lesions
The rootlets, roots, and spinal nerves that arise from the fifth cervical to the first thoracic spinal segments constitute the peripheral nervous system prebrachial plexus structures. Injuries to these structures usually produce clinical findings indistin- guishable from lesions to the brachial plexus. Scapular winging and Homer 's syndrome suggest involvement of the peripheral nervous system pre- brachial plexus structures, but they may also occur with brachial plexus injuries (Fig 1). The distinc- tion between lesions in the peripheral nervous system prebrachial plexus structures and the bra- chial plexus is made on the basis of electrophysi- ologic studies. Prebrachial plexus lesions are asso- ciated with fibrillations and positive sharp waves in the paraspinal muscles and normal sensory nerve conduction. MRI studies of the cervical spine may show root avulsion.
Fig 10. Arrn weakness due to pyramidal tract lesion (surgi- cal removal). (A) At rest right arm is not moving. (B) Exagger- ated Moro response of the weak arm. Compare with Figure 2 (A and B). (Reprinted with permission J)
Peripheral Nerve Involvement
Lesions of the upper limb nerves (primary trunk) often produce diagnostic patterns of weakness. The diagnostic dilemma arises with injury to secondary or tertiary branches or with partial injuries to the primary trunk of the peripheral nerves. These injuries may produce atypical patterns of weakness

12 ALFONSO, ALFONSO, AND PAPAZIAN
that may resemble fascicular brachial plexus palsy. In these situations, the diagnosis of peripheral nerve lesions is established by the following: (1) finding a cutaneous marker (scars or masses) in the trajectory of the peripheral nerves; (2) the absence of weakness and electrophysiologic evidence of denervation in muscles of similar spinal segmental innervation but by other spinal nerves; and (3) the absence of Homer's syndrome.
Course of Brachial Plexus Palsy
The course of brachial plexus palsy is dictated by its cause and by the distribution and severity of the injury. Brachial plexus palsy due to humeral osteo- myelitis resolves with antibiotics. 14 The natural history of intrauterine compressive nonobstetric brachial plexus palsy is not well-known because of the limited number of reported cases and the absence of long-term follow-up) 3 Brachial plexus due to exostosis and neoplasm is progressive. 16,18 Brachial plexus palsy produced by hemangioma and neck compression improve with time. 15,a7 The natural history of obstetric brachial plexus palsy is characterized by a significant degree of improve- ment in most cases (Table 2). 28-32 The incidence of permanent sequelae in population studies varies from 3% to 25%. 28-32 In a series of 24 patients with affected limbs, in whom the prognosis was reported based on the clinical presentations, permanent sequelae occurred in 3 of 6 limbs in patients with total brachial plexus palsy, 1 of 4 limbs in patients with upper-middle trunk brachial plexus palsy, and 2 of 12 limbs in patients with Duchenne-Erb palsy. 5
The degree of future improvement cannot be determined during a single evaluation, especially if
Table 2. Natural History of Obstetric Brachial Plexus Palsy
p ref PERCENTAGE OF FULL RECOVERY P/S
48 28 54* 6~* 6129 9 2 (38)
33 3o 9"/ 59 31 88 r
39 32 41 69 83
73* i 96(38)
i i i i 93 (82) 93(40~ i
i :i , i , , _ , i , , , _ i _ , _ ,
0 2 4 6 8 lO 12 2 3 4 5 MONTHS YEARS
~ i 7 i i 2
~ 3
~ 7
Abbreviations: P, number of patients; ref, reference; ( ) , number of patient evaluated at a particular visit; P/S, patient with sequela; * almost full recovery.
performed immediately after birth. The rate of improvement during the first few weeks is a relatively good indicator of the final outcome. Full recovery usually does not occur if there is no improvement in the first 2 weeks. 5
Management of Brachial Plexus Palsy
Antibiot ics are the treatment o f choice for bra- chial plexus palsy due to humeral osteomyelitis. 14 Physical therapy is the only treatment available for intrauterine compressive brachial plexus palsy and brachial plexus palsy due to neck compressionJ 3,17 Steroids may be considered for brachial plexus palsy due to hemangiomas, but the only reported case improved without administration of steroids.15 Resection of the bony tumor is the treatment of choice in neonates with brachial plexus palsy produced by exostosis. 16 The treatment of brachial plexus palsy due to neoplasm depends on the nature of the tumor. 18
The management of obstetric brachial plexus palsy consists of the following: (1) a careful initial evaluation searching for associated traumatic in- jury; (2) a rest period of 7 days, in which the family is advised to pin the sleeve of the neonate's shirt to hold the elbow in a flexed position; (3) a regimen of passive range of motion exercise and electrical muscle stimulation after 7 days; and (4) surgical intervention in a selected number of cases. The value of a resting period, exercise, electrical stimu- lation, and surgery has been questioned. 29,33
Follow-up evaluations should be performed at monthly intervals until at least 1 year of age. Deterioration after some recovery or even apparent full recovery in the early months has been re- ported. 9,3~ Each evaluation should include an assess- ment of range of active and passive motion in each joint and a determination of muscle mass. Subluxa- tion of the humeral head should diligently be sought, because it can be surgically corrected and failure to do so can produce permanent deformity of the glenoid cavity. Other important parameters to follow are degree of finger flexion and extension, wrist flexion and extension, forearm pronation and supination, elbow flexion and extension, arm abduc- tion, and shoulder external rotation. Muscle mass is assessed by comparing the size of the affected muscles with their healthy counterparts. Joint evalu- ation by a surgeon and therapist experienced in the management of these children is often valuable.

FOCAL ARM NEUROPATHY 13
MONONEUROPATHY
Mononeuropathies are rare in the neonatal pe- riod. Isolated cases of radial, median, and ulnar mononeuropathies have occurred in the neonatal period. 27 Isolated ulnar neuropathy is usually due to local trauma, but other causes exist. The treatment of mononeuropathies in the neonate consists of occupational therapy. Most cases resolve com- pletely in a period of 10 days to 3 months. Concomitant radial, medial, and ulnar nerve involve- ment may also occur. This condition may be produced by congenital constriction bands in the upper arm and should be differentiated from com- plete brachial plexus palsy. The possibility of surgery should be considered in cases of congenital amniotic bands or persistent motor paralysis. 34,35
Radial Nerve
The radial nerve is the continuation of the medial branch of the posterior cord (Fig 1). It contains fibers from the fifth cervical to the first thoracic spinal segments. In the upper arm, it travels medi- ally to the humerus, then winds around the humerus to enter the forearm over the lateral epicondyle. In the forearm it divides into a superficial sensory branch and the posterior interosseus branch. The radial nerve only gives off five motor branches before reaching the forearm: the fibers medial and lateral to the triceps, brachioradialis fibers, and the fibers for the extensor radialis longus and brevis. Congenital causes of radial nerve injury are intra- uterine compression due to uterine compressive
rings, umbilical cord, and amniotic bands. Ac- quired causes of radial nerve injury include hu- meral fractures, prolonged manual external com- pression, an excessively tight blood pressure cuff, benign angioleiomyoma, and humeral osteomyeli- t is . 36'37 On physical examination, an indurated area, a mass, or an amniotic band in the course of the radial nerve may be found. Radial nerve injury produces wrist drop. Most radial nerve injuries occur in the area of the distal humerus or in the proximal forearm.
Median Nerve Injury
The median nerve is formed from the lateral branch of the medial cord and the medial branch of the lateral cord. The median nerve travels in the medial aspect of the arm close to the brachial artery. It enters the forearm just medial to the biceps tendon and the brachial artery. It travels along the middle of the forearm and enters the hand under the carpal ligaments relatively close to the radial artery. The median nerve supplies the muscles that pronate the forearm, flex the wrist and fingers, and oppose, flex, and abduct the thumb (Table 1). 2"6'38 Pincer action weakness characterizes me- dian nerve injury. Atrophy of the thenar eminence usually occurs during infancy. Median nerve mono- neuropathy may occur due to focal lesions in the antecubital fossa or at the wrist. Median nerve injury has been associated with arterial and brachial arterial puncture. 39,4~
REFERENCES 1. Carpenter MB, Sutin J: Human Neuroanatomy. Baltimore,
MD, Williams & Wilkins, 1983 2. Braziz PW, Masdeu JC, Biller J: Localization in Clinical
Neurology. Boston, MA, Little Brown, 1990 3. Williams PL: Gray's Anatomy. New York, NY, Churchill
Livingstone, 1989 4. Molnar GE: Brachial plexus injury in the newborn. Pediatr
Rev 6:110-115, 1984 5. Bennett GC, Harrold AJ: Prognosis and early management
of birth injury to the brachial plexus. BMJ 1:1520, 1970 6. Devinsky O, Feldmann E: Examination of the cranial and
peripheral nerves. New York, NY, Churchill Livingstone, 1988 7. Alfonso I, Papazian O, Altman N, et al: Obstetric brachial
plexopathy. Int Pediatr 6:229-232, 1991 8. Gilbert A: Long-term evaluation of the brachial plexus
surgery in obstetrical palsy. Hand Clinics 11:583-594, 1995 9. Eng GD, Binder H, Getson P, et al: Obstetrical brachial
plexus palsy (OBPP) outcome with conservative management. Muscle Nerve 19:884-891, 1996
10. Haenggeli CA, Lacourt G: Brachial plexus injury and hypoglossal paralysis. Pediatr Neurol 5:197-198, 1989
11. Aldrich TK, Herman JH, Rochester J: Bilateral diaphrag- matic paralysis in the newborn infant. Pediatrics 97:988-991, 1980
12. Jones HR Jr: Plexus and nerve root lesions, in Jones RH Jr, Bolton CF Jr, Harper CM Jr (eds): Pediatric Clinical Electromyography. Philadelphia, PA, Lippincott-Raven, 1996, pp 123-169
13. Dunn DW, Angle WA: Brachial plexus palsy: Intrauterine onset. Pediatr Neurol 1:367-369, 1985
14. Sadleir LG, Connoly MB: Acquire brachial-plexus neu- ropathy: A rare presentation of late group-B streptococcal osteomyelitis. Dev Med Child Neuro140:496-499, 1998
15. Lucas WL, Holden KR, Purohit PD, et al: Neonatal hemangiomatosis associated with brachial plexus palsy. J Child Neurol 10:411-413, 1995
16. de Turckheim MC, Clavert JM, Paira M: Exostoses costales compliquees en periode neonatale, de paralysie du

14 ALFONSO, ALFONSO, AND PAPAZIAN
plexus brachial: Entite distinctive de la maladie exostosante? Ann Pediatr (Paris) 38:23-25, 1991
17. Turner T, Evans J, Brown JK: Monoparesis: Complica- tion of constant positive airways pressure. Arch Dis Child 50:128-129, 1975
18. Alfonso I: Neoplasm as a cause of brachial plexus palsy in neonates. Pediatr Neurol (in press)
19. al-Qattan MM, Clarke HM, Curtis CG: Prognostic value of concurrent clavicular fractures in newborns with obstetrical brachial plexus palsy. J Hand Surg [Br] 19:729-730, 1994
20. Cook County (ILL) Circuit Court, Case No. 89L-9149 21. Millichap JG: Pediatric neurology briefs. 10:49-50, 1996 22. Colville J, Jeffries I: Bilateral acquired neonatal Erb
palsy. J Irish Med Assoc 68:399-401, 1975 23. Hall JC, Reed SD, Driscoll EP: Amyoplasia: A common
sporadic condition with congenital contractures. Am J Med Genet 15:571-590, 1983
24. Darwish H, Sarnat H, Archer C, et al: Congenital cervical spinal atrophy. Muscle Nerve 4:106-110, 1981
25. Plaza MD, Santos J, Monzon L, et al: Lipoma intramedu- lar cervicodorsal de manifestacion neonatal. Rev Neuro128:483- 485, 1999
26. Alfonso I, Palomino JA, De Quesada G, et al: Congenital varicella syndrome. Am J Dis Child 138:603-604, 1984
27. Volpe JJ: Neurology of the newborn. Philadelphia, PA, WB Sannders, 1995, pp 719-721
28. Sjorberg I, Erichs K, Bjerre I: Cause and effect of obstetric (neonatal) brachial plexus palsy. Acta Pediatr Scand 77:357-364, 1988
29. GreenwaldAG, Schute PC, Shiveley JL: Brachial plexus birth palsy: A 10-year report of incidence and prognosis. J Pediatr Orthop 4:689-692, 1984
30. Nocon JJ, Mckenzie DK, Thomas LJ, et al: Shoulder
dystocia: An analysis of risk and obstetrical maneuvers. Am J Obstet Gynecol 168:1732-1739, 1993
31. Gordon M, Rich H, Deutchberger J, et al: The immediate and long-term outcome of obstetric birth trauma. I. Brachial plexus palsy. Am J Obstet Gynecol 117:51-56, 1973
32. Rootwelt T, Kjos RR, Stiris TA, et al: Brachial plexus injuries in newborn infants. Tidsskr Nor Laegeforem 116:2445- 2448, 1996
33. Bodensteiner JB, Rich KM, Landau WM: Early infantile surgery for birth-related brachial plexus injuries: Justification requires a prospective controlled study. J Child Neurol 9:109- 110, 1994
34. Weeks PM: Radial, median, ulnar nerve dysfunction associated with a congenital band of the arm. Plast Reconstr Surg 69:333-336, 1982
35. Weinzweig N, Barr A: Radial, ulnar, and median nerve palsy caused by a congenital constriction band of the arm: Single-stage correction. Plast Reconstr Surg 94:872-876, 1994
36. Lejnan T, Strong M, Michno P: Radial-nerve palsy associated with septic shoulder in neonates. J Pediatr Orthop 15:169-171, 1995
37. Sunram F, Harms D, Mau G: Neonatal paresis of radial nerve due to benign angioleiomyoma. Z Orthop 115:124-128, 1977
38. Stewart JD: Focal Peripheral Neuropathies. New York, NY, Elsevier Science, 1987
39. Pape KE, Armstrong DL, Fitzhardinge PM: Peripheral median nerve damage secondary to brachial artery blood gas sampling. J Pediatr 93:852-856, 1978
40. Koenigsberger MR, Moessinger AC: Iatrogenic carpal tunnel syndrome in a newborn infant. J Pediatr 91:443-445, 1977
Copyright © 2022 FDOKUMEN




















