
Upper extremity radionuclide bone imaging: Shoulder, arm, elbow, and forearm
11
Upper Extremity Radionuclide Bone Imaging: Shoulder, Arm, Elbow, and Forearm Mayur Patel Along with resurgence of physical activity during these t'~ness conscious times, there is increasing participation by people of all ages in sporting activi- ties. Enrollment in organized and recreational sports among young adults and children has increased with as many as 30% of adolescents participating in com- petitive high school athletics. 1 Despite improvements in equipment, the number of sports-related injuries presenting for medical attention has increased. Inju- ries to the upper extremities account for more than 25% of all sports-related injuries, but receive dispropor- tionately less attention compared to lower extremity injuries. 2 If neglected, upper extremity injuries can end the career of a professional athlete and cause suffi- cient damage to hinder daily activities in a recreational participant. Overuse syndromes, brought on by repeti- tive microtrauma are sports-specific, and often chal- lenging to diagnose. Accurate diagnosis requires a thorough understanding about mechanism of injury, site of pain, and knowledge of the sport. After a thorough physical exam, a variety of radiographic testing is often necessary to promptly diagnose and manage the injury so athletes can return to competi- tion as soon as possible. Copyright9 1998by W.B. Saunders Company T HIS REPORT reviews the interactive role of scintigraphy with other imaging modalities in evaluation of traumatic orthopedic conditions per- taining to the shoulders, arm, elbow, and forearm. The focus is primarily on traumatic and athletic injuries as well as other infectious and neoplastic conditions which often require orthopedic evalua- tion and intervention. The complimentary role of bone scintigraphy to conventional radiographic imaging procedures will be illustrated with empha- sis on the specialized views and techniques that aid the orthopedist. SHOULDER Evaluation of unexplained shoulder pain in ath- letes has become more sophisticated in the past two decades due to emergence of combined computed tomography (CT) arthrography, magnetic reso- nance imaging (MRI), and high resolution arthro- scopic equipment. Because of a wide spectrum of disorders that may leave an athlete with a disabled shoulder, work-up algorithms may involve use of multiple imaging modalities to compliment the initial physical exam. The anatomic lesions of the shoulder girdle complex involve the stemoclavicular joint, acromio- clavicular joint, rotator cuff, glenohumeral capsule, glenoid labrum, and the humeral head. Initial evaluation of the disabled shoulder com- prises a thorough physical examination and conven- tional radiographs. Routine radiographs are helpful in assessing for fractures, dislocations, or soft tissue calcifications. Recurrent or chronic shoulder dislocation results in two well-described entities that may require Fig 1. Post-traumatic acromioelavicolsr separation and synovitis: Delayed static image shows separation of right A-C joint as photopenic defect (arrow) and associated post- traumatic inflammation/synovitis. Normal comparison left A-C joint. specialized views to aid diagnosis. Hill Sachs lesion is a compression fracture of posterolateral humeral head that results from anterior shoulder dislocation and is best seen on anteroposterior projection in internal rotation or Stryker notch view.3 Bankart lesion refers to the fracture of the anterior glenoid rim which is optimally assessed with West Point or prone axillary view.4 Nonosseous abnormalities, on the other hand, require further evaluation with arthroscopy or mul- From the Department of Radiology, Sinai Hospital, Balti- more, MD. Address reprint requests to Mayur Patel, MD, Department of Radiology, Sinai Hospital, 2401 West Belvedere Ave., Baltimore, MD21215. Copyright 9 1998 by W.B. Saunders Company 0001-2998/98/2704-000158.00/0 Seminarsin NuclearMedicine, Vol XXVIII, No I (January), 1998: pp 3-13 3
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Upper extremity radionuclide bone imaging: Shoulder, arm, elbow, and forearm

Upper Extremity Radionuclide Bone Imaging: Shoulder, Arm, Elbow, and Forearm
Mayur Patel
Along wi th resurgence of physical activity during these t'~ness conscious t imes, there is increasing participation by people of all ages in sporting activi- ties. Enrollment in organized and recreational sports among young adults and children has increased wi th as many as 30% of adolescents participating in com- petit ive high school athletics. 1 Despite improvements in equipment, the number of sports-related injuries presenting for medical attention has increased. Inju- ries to the upper extremities account for more than 25% of all sports-related injuries, but receive dispropor- t ionately less attention compared to lower extremity injuries. 2 If neglected, upper extremity injuries can end
the career of a professional athlete and cause suffi- cient damage to hinder daily activities in a recreational participant. Overuse syndromes, brought on by repeti- t ive microtrauma are sports-specific, and often chal- lenging to diagnose. Accurate diagnosis requires a thorough understanding about mechanism of injury, site of pain, and knowledge of the sport. After a thorough physical exam, a variety of radiographic testing is often necessary to prompt ly diagnose and manage the injury so athletes can return to competi- t ion as soon as possible. Copyright�9 1998 by W.B. Saunders Company
T HIS REPORT reviews the interactive role of scintigraphy with other imaging modalities in
evaluation of traumatic orthopedic conditions per- taining to the shoulders, arm, elbow, and forearm. The focus is primarily on traumatic and athletic injuries as well as other infectious and neoplastic conditions which often require orthopedic evalua- tion and intervention. The complimentary role of bone scintigraphy to conventional radiographic imaging procedures will be illustrated with empha- sis on the specialized views and techniques that aid the orthopedist.
SHOULDER
Evaluation of unexplained shoulder pain in ath- letes has become more sophisticated in the past two decades due to emergence of combined computed tomography (CT) arthrography, magnetic reso- nance imaging (MRI), and high resolution arthro- scopic equipment. Because of a wide spectrum of disorders that may leave an athlete with a disabled shoulder, work-up algorithms may involve use of multiple imaging modalities to compliment the initial physical exam.
The anatomic lesions of the shoulder girdle complex involve the stemoclavicular joint, acromio- clavicular joint, rotator cuff, glenohumeral capsule, glenoid labrum, and the humeral head.
Initial evaluation of the disabled shoulder com- prises a thorough physical examination and conven- tional radiographs. Routine radiographs are helpful in assessing for fractures, dislocations, or soft tissue calcifications.
Recurrent or chronic shoulder dislocation results in two well-described entities that may require
Fig 1. Post-traumatic acromioelavicolsr separation and synovitis: Delayed static image shows separation of right A-C joint as photopenic defect (arrow) and associated post- traumatic inflammation/synovitis. Normal comparison left A-C joint.
specialized views to aid diagnosis. Hill Sachs lesion is a compression fracture of posterolateral humeral head that results from anterior shoulder dislocation and is best seen on anteroposterior projection in internal rotation or Stryker notch view. 3 Bankart lesion refers to the fracture of the anterior glenoid rim which is optimally assessed with West Point or prone axillary view. 4
Nonosseous abnormalities, on the other hand, require further evaluation with arthroscopy or mul-
From the Department of Radiology, Sinai Hospital, Balti- more, MD.
Address reprint requests to Mayur Patel, MD, Department of Radiology, Sinai Hospital, 2401 West Belvedere Ave., Baltimore, MD21215.
Copyright �9 1998 by W.B. Saunders Company 0001-2998/98/2704-000158.00/0
Seminars in Nuclear Medicine, Vol XXVIII, No I (January), 1998: pp 3-13 3
4 MAYUR PATEL
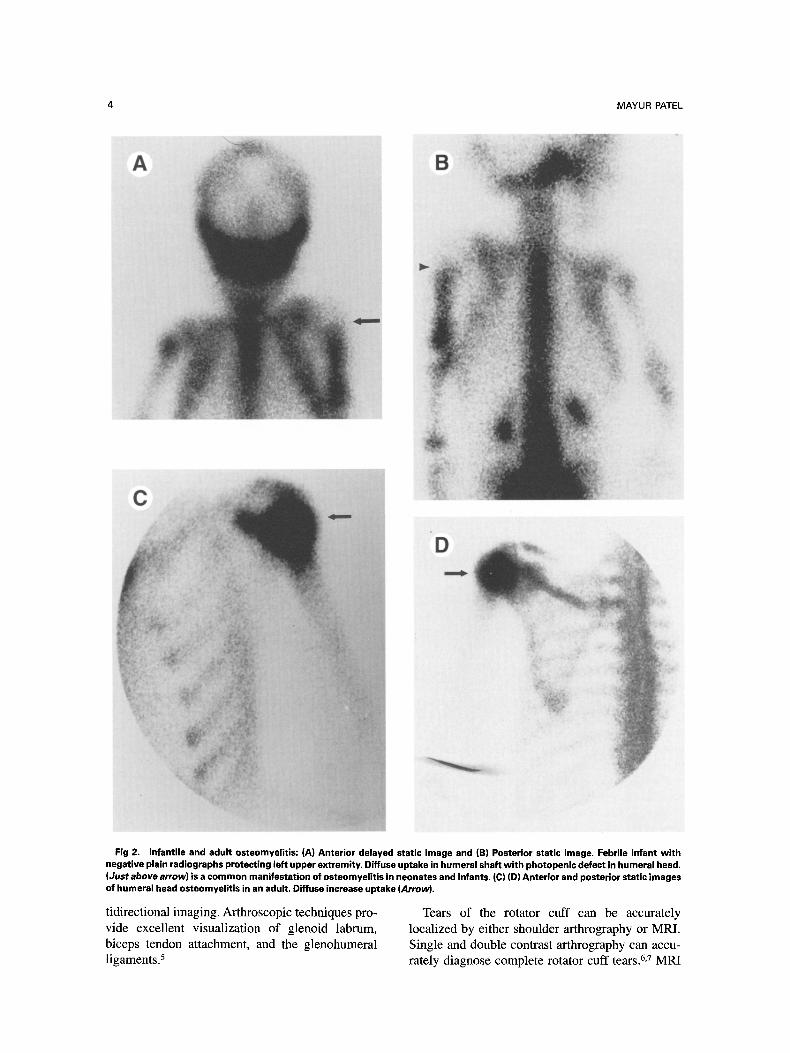
Fig 2. Infantile and adult osteomyelitis: (A) Anterior delayed static image and (B) Posterior static image. Febrile infant with negative plain radiographs protecting left upper extremity. Diffuse uptake in humeral shaft with photopenic defect in humeral head. (Just above arrow) is a common manifestation of osteomyelitis in neonates and infants, (C) (D) Anterior and posterior static images of humeral head osteomyelitis in an adult, Diffuse increase uptake (Arrow).
tidirectional imaging. Arthroscopic techniques pro- vide excellent visualization of glenoid labrum, biceps tendon attachment, and the glenohumeral ligaments)
Tears of the rotator cuff can be accurately localized by either shoulder arthrography or MRI. Single and double contrast arthrography can accu- rately diagnose complete rotator cuff tears. 6,7 MRI
UPPER EXTREMITY BONE IMAGING 5
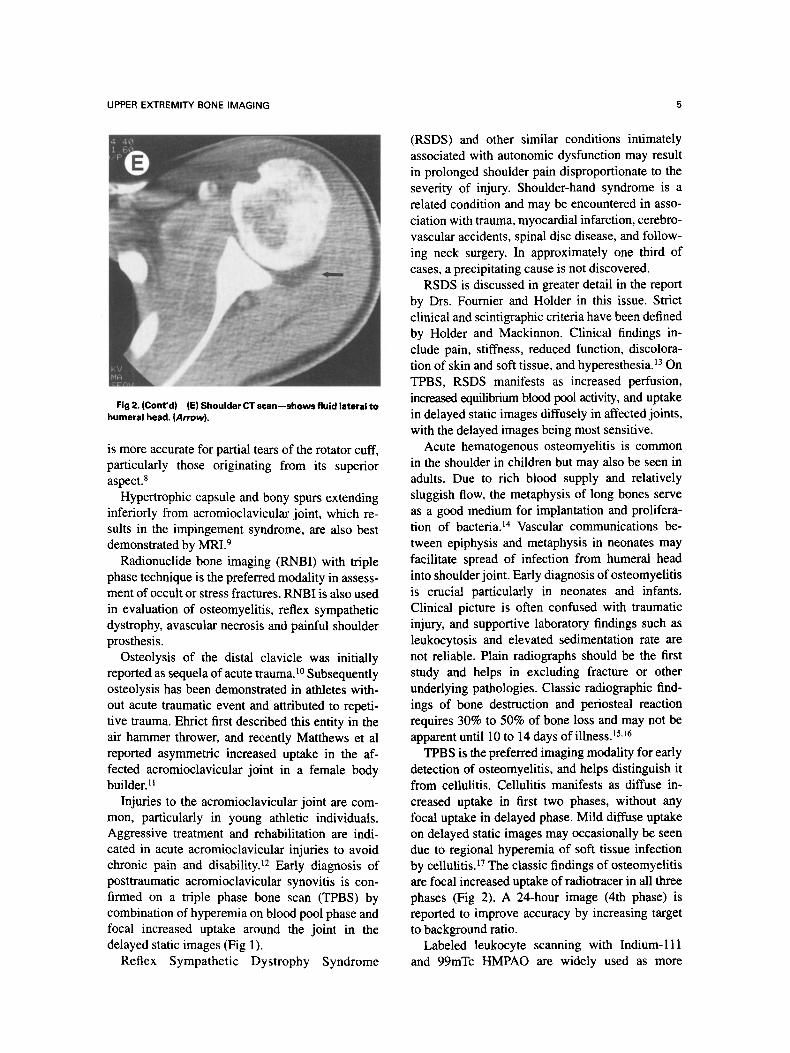
Fig 2. (Cont'd) (El Shoulder CT scan--shows fluid lateral to humeral head. (Arrow).
is more accurate for partial tears of the rotator cuff, particularly those originating from its superior aspect. 8
Hypertrophic capsule and bony spurs extending inferiorly from acromioclavicular joint, which re- sults in the impingement syndrome, are also best demonstrated by MRI . 9
Radionuclide bone imaging (RNBI) with triple phase technique is the preferred modality in assess- ment of occult or stress fractures. RNBI is also used in evaluation of osteomyelitis, reflex sympathetic dystrophy, avascular necrosis and painful shoulder prosthesis.
Osteolysis of the distal clavicle was initiaUy reported as sequela of acute trauma.l~ Subsequently osteolysis has been demonstrated in athletes with- out acute traumatic event and attributed to repeti- tive trauma. Ehrict first described this entity in the air hammer thrower, and recently Matthews et al reported asymmetric increased uptake in the af- fected acromioclavicular joint in a female body builder. H
Injuries to the acromioclavicular joint are com- mon, particularly in young athletic individuals. Aggressive treatment and rehabilitation are indi- cated in acute acromioclavicular injuries to avoid chronic pain and disability) 2 Early diagnosis of posttraumatic acromioclavicular synovitis is con- firmed on a triple phase bone scan (TPBS) by combination of hyperemia on blood pool phase and focal increased uptake around the joint in the delayed static images (Fig 1).
Reflex Sympathetic Dystrophy Syndrome
(RSDS) and other similar conditions intimately associated with autonomic dysfunction may result in prolonged shoulder pain disproportionate to the severity of injury. Shoulder-hand syndrome is a related condition and may be encountered in asso- ciation with trauma, myocardial infarction, cerebro- vascular accidents, spinal disc disease, and follow- ing neck surgery. In approximately one third of cases, a precipitating cause is not discovered.
RSDS is discussed in greater detail in the report by Drs. Fournier and Holder in this issue. Strict clinical and scintigraphic criteria have been defined by Holder and Mackinnon. Clinical findings in- clude pain, stiffness, reduced function, discolora- tion of skin and soft tissue, and hyperesthesia. 13 On TPBS, RSDS manifests as increased perfusion, increased equilibrium blood pool activity, and uptake in delayed static images diffusely in affected joints, with the delayed images being most sensitive.
Acute hematogenous osteomyelitis is common in the shoulder in children but may also be seen in adults. Due to rich blood supply and relatively sluggish flow, the metaphysis of long bones serve as a good medium for implantation and prolifera- tion of bacteria, t4 Vascular communications be- tween epiphysis and metaphysis in neonates may facilitate spread of infection from humeral head into shoulder joint. Early diagnosis of osteomyelitis is crucial particularly in neonates and infants. Clinical picture is often confused with traumatic injury, and supportive laboratory findings such as leukocytosis and elevated sedimentation rate are not reliable. Plain radiographs should be the first study and helps in excluding fracture or other underlying pathologies. Classic radiographic find- ings of bone destruction and periosteal reaction requires 30% to 50% of bone loss and may not be apparent until 10 to 14 days of illnessJ 5,16
TPBS is the preferred imaging modality for early detection of osteomyelitis, and helps distinguish it from cellulitis. Cellulitis manifests as diffuse in- creased uptake in first two phases, without any focal uptake in delayed phase. Mild diffuse uptake on delayed static images may occasionally be seen due to regional hyperemia of soft tissue infection by cellulitis.f7 The classic findings of osteomyelitis are focal increased uptake of radiotracer in all three phases (Fig 2). A 24-hour image (4th phase) is reported to improve accuracy by increasing target to background ratio.
Labeled leukocyte scanning with Indium-Ill and 99mTc HMPAO are widely used as more
6 MAYUR PATEL
specific radiotracer for infection imaging, Indium- 111 leukocyte scintigraphy is particularly helpful in evaluation of infection complicating trauma, prior surgery or in diabetic patients. 18 False-positive Indium-labeled leukocyte scans have been reported in inflammatory arthropathies, recent trauma, and joint replacement surgery. Leukocyte scans have a high sensitivity and specifity for infection.
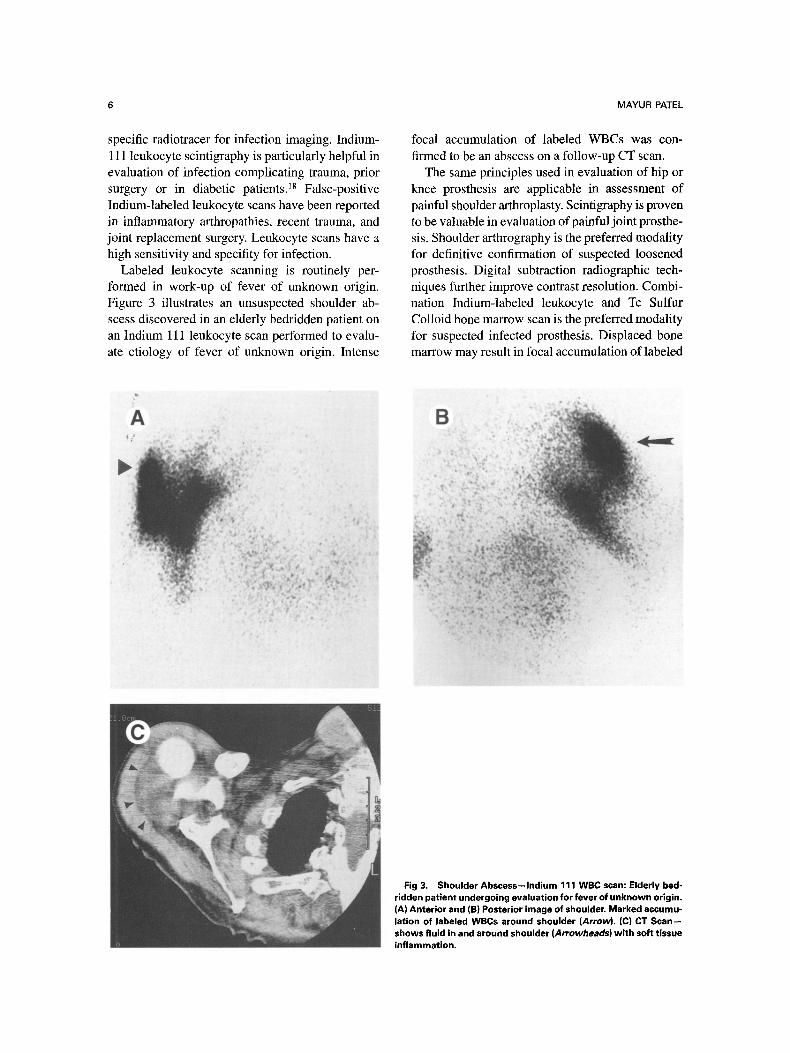
Labeled leukocyte scanning is routinely per- formed in work-up of fever of unknown origin. Figure 3 illustrates an unsuspected shoulder ab- scess discovered in an elderly bedridden patient on an Indium 111 leukocyte scan performed to evalu- ate etiology of fever of unknown origin. Intense
focal accumulation of labeled WBCs was con- firmed to be an abscess on a follow-up CT scan.
The same principles used in evaluation of hip or knee prosthesis are applicable in assessment of painful shoulder arthroplasty. Scintigraphy is proven to be valuable in evaluation of painful joint prosthe- sis. Shoulder arthrography is the preferred modality for definitive confirmation of suspected loosened prosthesis. Digital subtraction radiographic tech- niques further improve contrast resolution. Combi- nation Indium-labeled leukocyte and Tc Sulfur Colloid bone marrow scan is the preferred modality for suspected infected prosthesis. Displaced bone marrow may result in focal accumulation of labeled
Fig 3. Shoulder Abscess--Indium 111 WBC scan: Elderly bed- ridden patient undergoing evaluation for fever of unknown origin. (A) Anterior and (B) Posterior image of shoulder. Marked aeeumu- lation of labeled WBCs around shoulder (Arrow), (C) CT Scan-- shows fluid in and around shoulder (Arrowheads) with soft tissue inflammation.

UPPER EXTREMITY BONE IMAGING 7
A
MARKER--
Fig 4. Use of markers to local- ize palpable masses: (A) Anterior and (B) lateral view. Marker over palpable mass helps in distin- guishing soft tissue mass from metabolically active osseous le- sions.
B
RAO
Fig 5. Nonunion of humeral neck fracture: (A) Oblique delayed static view shows increased uptake at site of non- union, reactive type. (B) Plain radiograph shows lack of callus persistent fracture line.

8 MAYUR PATEL
Fig 6. Osteoid osteoma of humeral shaft in a young adult male: (A) Blood pool image. Moderate hyperemia, wi th a central round focus of more intense uptake. (B) Delayed static image-- focal intense increased uptake. (C)(D) Plain radiograph and CT scan show cortical sclerosis and focal lucency. Definite nidus not visualized.

UPPER EXTREMITY BONE IMAGING 9
Posttraumatic myositis ossificans may be seen in contact sports such as karate. 2! Early in the process, plain radiographs are negative except for soft tissue mass which corresponds to the hard palpable mass in the area of pain. Because surgical removal of heterotopic bone is an option for pain relief, TPBS is recommended to age the lesion and confirm maturation.
Avascular necrosis (AVN) of the humeral head results from interruption of blood supply to the bone causing subsequent edema and increased intraosseous pressure. Diffuse vascular obstruction from crisis in sickle cell disease is the most common etiology for AVN of humeral head. Other causes include traumatic interruption of blood supply, fat embolism, lupus vasculitis, and radia- tion osteonecrosis. Scintigraphic findings in sickle
Fig 7. Medial Epicondylitis: Delayed static image shows focal increased uptake in medial epicondyle. Plain radiographs negative.
WBCs and is best evaluated in combination with Tc99m SC bone marrow scan to improve specif i ty. 15
It is often helpful to obtain marker views in patients presenting with palpable mass in order to accurately assess the location of abnormal uptake (Fig 4).
HUMERUS
Athletic injuries to the humerus are rare com- pared with other long bones. However, a variety of other conditions resulting in upper arm pain require orthopedic evaluation.
Stress fractures of the humerus are associated with gymnastics, tennis, javelin throwing, and baseball pitching. TPBS is the preferred modality in evaluation of stress fractures and humeral perios- titis. Ringmans shoulder lesion is a cortical desmoid- like lesion in the proximal humerus reported by Fulton et al in gymnastics. ~9 Similarly, humeral periostitis manifesting as increased uptake of radio- tracer at the insertion of pectoralis major may also be seen in weight lifters. 5,2~ Humeral periostitis is an overuse injury resulting in tearing of muscle fibers of the pectoralis major muscle at the insertion in the upper shaft of the humerus. This should be distinguished from physiological stress response at the insertion of deltoid muscle in the lateral aspect of the proximal humerus which is a normal variant.
Fig 8. Metastatic thyroid carcinoma to elbow: (A) Arm image from whole body 1-131 scan shows functioning meta- ststis left elbow. (B) Postoperative radiograph after surgical elbow joint replacement.

10 MAYUR PATEL
Fig 9. Occult radial head fracture: Normal elbow x-ray films following injury with persistent pain (A) Blood pool images shows focal hyperemia left radial head (Arrowhead). Injection site in r ight antecubital fossa, partially shielded. (B) Delayed static image anterior with intense uptake (Arrow). (C) Delayed lateral shows focal uptake in radial head (Arrow).
cell disease vary with duration of symptoms. Photopenic defects (cold areas) represent very recent infarcts, which later convert to foci of increase uptake as the reparative phase com- mences. In patients who do not have SSA, MRI is the preferred modality for confirmation of AVN due to lower specificity of RNBI. 22
Nonunion of a fracture is suspected if appropri- ate healing does not occur within 4 to 6 months following injury. Nonunion of fractures of humerus is a frequent and serious complication. 14 The most common causes of fracture nonunion are ischemia, infection, inadequate reduction, improper immobi-
lization, interposition of soft tissues, and pathologi- cal bone conditions such as hyperparathyroidism, metastasis, and osteomalacia. 23 Lack of progressive healing in serial radiographs alerts one to the possibility of impeded healing. 24 In advanced cases radiographic features are lack of calcified callus, smoothened ends of fragments, eburnation of frag- ments, and, eventually, pseudoarthrosis. 25
On TPBS, two types of nonunion have been described. In the reactive type, there is focal increased uptake reflecting increased osteoblastic activity (Fig 5). In the atrophic type of nonunion, there is absence or decreased uptake at fracture

UPPER EXTREMITY BONE IMAGING
A B
11
_[ t
W
Fig 10. Ulnar Stress Fractures: (A) Delayed static images show bilateral mid-ulnar shafts stress fractures in a weight lifter, less focally fusiform than usually seen in shafts of long bones. (B) Ulnar styloid avuision fracture delayed static image shows focal uptake at styloid process. (Cases courtesy of J.R. Martire, MD).
site. 14,23 In addition, the scintigraphic pattern may aid in assessment of therapeutic measures and determine need for surgical intervention. Increased osteoblastic activity at a fracture site following percutaneous electrical stimulation is predictive of successful outcome. 26
A variety of symptomatic benign tumors and tumor-like conditions may cause a diagnostic di- lemma. Osteoid osteoma is a relatively common benign bone tumor in adolescents and young adults. Pain is the most frequent presenting complaint. A history of the much popularized symptom complex of nocturnal pain relieved with salicylates is not reliably elicited. The majority of osteoid osteomas are in the diaphysis of long bones (Fig 6). Pathologi- cally, the typical feature is a small central nidus surrounded by dense trabecular bone. This provides the radiographic manifestation of central lucency with surrounding cortical sclerosis and thickening. If typical radiographic findings are absent in a symptomatic patient, TPBS is invariably diagnos- tic. 27 The characteristic pattern of osteoid osteoma is focal hyperemia on blood pool phase with marked intense tracer localization in the nidus on delayed phase (double density sign). 28.29 Pinhole magnification views help in accurate localization of the nidus and assists in planning surgical excision, particularly in weight-bearing bones to minimize amount of bone excised. Scintigraphy and intraop-
erative gamma probe may be used to localize the nidus and confirm complete excision at surgery.
Scintigraphy is also useful for determining meta- bolic activity in other benign lesions such as fibrous cortical defects, bone cysts, and osteoblastoma, which may be incidentally identified on radio- graphs obtained following injury.
ELBOW
Athletic injuries of the elbow are common and often lead to significant disability. Overuse injuries occur with high incidence in baseball, football, racquet sports, and javelin throwers. 3~ Acute injuries of the elbow are also common in athletes. Routine radiographs in combination with knowl- edge of location of pain, the patients age, and type of sports activity can result in accurate diagnosis without need for any further imaging.
Overuse elbow injuries in sports activities have been categorized based on anatomy and pathophysi- ology by Gore et al. 33 Plain radiographs reveal loose bodies, traction spurs, osteochondral irregu- larities, and epiphyseal changes. TPBS is used to determine significance of these changes by assess- ing for any metabolic activity.
Osteochondritis dissecans (OCD) is a common cause of elbow pain in baseball pitchers. The pain is usually aggravated with activity and relieved by rest. OCD results from repetitive compressive force
12 MAYUR PATEL
between radial head and capitellum. In the elbow the most frequent site of involvement is the capitel- lum. If untreated, OCD may lead to loose intraarticu- lar bodies, loss of motion, and locking and click- ing. 32 Radiologic work-up involves plain radiographs, fluoroscopy and, if needed, CT arthrogram to evaluate cartilaginous loose bodies. 34
Lateral epicondylitis (tennis elbow) is associated with overuse at the margin of extensor carpi radialis brevis muscle. 35 Medial epicondylitis ("Little Leaguer's elbow, golfers' elbow") occurs secondary to overuse at the insertion of flexor and pronator muscle groups (Fig 7). Plain radiographs or CT may demonstrate calcification adjacent to the respective epicondyles.
If radiographs are negative, TPBS may help in localizing the site of injury. Depending on severity of inflammatory response, increased uptake is seen on both blood pool and delayed static images. Specialized acute flexion views may be needed to demonstrate injury involving the capitellum. 36
Stress fracture through the olecranon epiphysis in adolescent baseball pitchers results in asymmet- ric increased uptake at the epiphyseal plate and requires careful comparison with the contralateral normal elbow. 37 Figure 8 demonstrates metastasis from functioning thyroid carcinoma on a whole body I- 131 scan.
FOREARM
Acute fractures of the radius and ulna are obvious clinically and adequately confirmed with routine radiographs.
Bone bruise results from direct trauma that does not result in disruption of the cortex. Occult fracture is defined as a fracture with or without trauma, with negative plain radiographs (Fig 9). Both entities may require orthopedic management if symptoms persist and are easily confirmed by the presence of total tracer uptake on TPBS.
Ulnar diaphyseal stress fractures occur because of heavy overuse of the flexor muscles. Ulnar stress fractures are most commonly seen in weight-lifters and body builders (Fig 10). Cases have been reported in a variety of other sporting activities including volleyball, softball, baseball, and the martial arts. 38
Stress fractures of the distal ulna have been reported in a highly competitive tennis player. 39
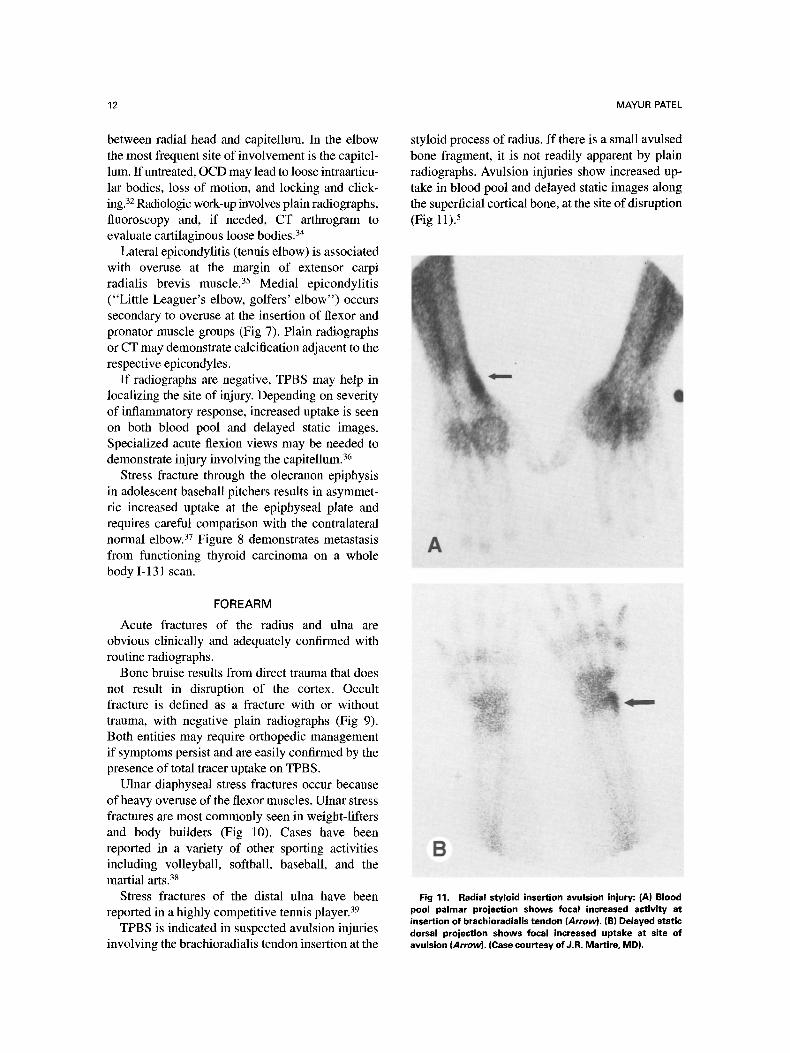
TPBS is indicated in suspected avulsion injuries involving the brachioradialis tendon insertion at the
styloid process of radius. If there is a small avulsed bone fragment, it is not readily apparent by plain radiographs. Avulsion injuries show increased up- take in blood pool and delayed static images along the superficial cortical bone, at the site of disruption (Fig 11). 5
Fig 11. Radial styloid insertion avulsion injury: (A) Blood pool palmar projection shows focal increased activity at insertion of brachioradialis tendon (Arrow). (B) Delayed static dorsal projection shows focal increased uptake at site of avulsion (Arrow). (Case courtesy of J.R. Martire, MD).

UPPER EXTREMITY BONE IMAGING 13
REFERENCES
1. Nelson MA: Sports Medicine, in Friedman SB (ed): Comprehensive Adolescent Health Care. St. Louis, Quality Medical Publishing, 1992, pp 1332-1151
2. Plancher KD, Minnich JM: Sports Specific Injuries, in Plancher KD (ed): Clinics in Sports Medicine. Philadelphia, PA, Saunders, 1996, pp 207-218
3. Pavlov H, et al: The Roetgenographic Evaluation of Anterior Shoulder Instability. Clin Orthop 194:153, 1985
4. Rokous JR, Feagin JA, Abbott HG: Modified axillary roentgenogram: A useful adjunct in the diagnosis of recurrent instability of the shoulder. Clin Orthop 82:84, 1972
5. Martire JR, Levinsohn EM: Shoulder and humerous imaging of athletic injuries, a multimodality approach. New York, NY: McGraw-Hill 5:181-219, 1992
6. Mink JH, Harris E, Rappaport M: Rotator Cuff Tears: Evaluation using double-contrast shoulder arthrography. Radiol- ogy 157:621-623, 1985
7. Burk DL, Karasick D, Kurtz ABet al: Rotator Cuff Tears: prospective comparison of MR Imaging with arthrography, sonography, and surgery, A JR 153:87-92, 1989
8. Rafii M, Firooznia H, Sherman O, et al: Rotator cuff lesions: signal patterns at MR Imaging. Radiology 177:817-823, 1990
9. Kursunoglu-Brahme S, Resnick D: Magnetic resonance imaging of the shoulder. Rad Clin North Am 28:941-954, 1990
10. Dupas J, Badilon P, Dayde G: Aspects radiologique d'une osteolyse essentiell progressive de la main gauche. J Radiol 20:383-387, 1936
11. Matthews LS, Simonson BG, Wolock BS. Osteolysis of the distal clavicle in a female body builder: a case report. Am J Sports Med 1993;21:150-152
12. Cox JS: The fate of the acromioclavicular joint in athletic injuries. Am J Sports Med 9:50-53, 1981
13. Holder LE, MacKinnon SE: Reflex sympathetic dystro- phy in the hands: Strict clinical and scintigraphic criteria. Radiology 152:517-522, 1984
14. Silberstein EB, Elgazzar AH, Fernandez-Ulloa M, et al: Skeletal scintigraphy in non-neoplastic osseous disorders, in Henkin RE, Boles MA, Dillehay et al editors: Nuc Med 79:1141-1197, 1996
15. Schaumecker DS: The role of nuclear medicine in osteomyelitis, in Collier BD, Fogelman I, Rosenthal L, (eds): Skeletal Nuclear Medicine II: 183-202, 1996
16. Handmaker H, Leonards R: The bone scan in inflamma- tory osseous disease. Sem Nuc Med; 6:95. 1976
17. Thrall JH, Geslien GE, Corcoran RJ, et al: Abnormal radionuclide deposition patterns adjacent to focal skeletal le- sions. Radiology;115:659, 1975
18. Mcarthy K, Velchik MG, Alavi A: Indium-Ill labeled white blood cells in the detection of osteomyelitis complicated by a pre-existing condition. J Nuc Med 29: 1015-1021, 1988
19. Fulton MN, Albright JP, El-Khoury GY. Cortical desmoid- like lesion of the proximal humerus and its occurrence in
gymnastics (ringman's shoulder lesion). Am J Sports Med 1979; 7:57-61
20. Martire JR. The role of nuclear medicine bone scans in evaluating pain in athletic injuries. Clinics Sports Med 1987; 6:713-737
21. Tondeur M, Haentjens M, Piepsz A, et al: Muscular Injury in a child diagnosed by 99m Tc-MDP bone scan. Eur J Nucl Med 1989; 15:328-329
22. Brody AS, Strong M, Babikian G, et al: Avascular necrosis: Early MR imaging and histologic findings in a canine model. A JR Am J Roentgenol 1991 ;157:341
23. McDougall IR, Keeling CA: Complications of fractures and their healing, Sem Nucl Med 18:113-125, 1988
24. Rosenthal L, Lisbona R: Role of radionuclide imaging in benign bone and joint disease of orthopedic interest, in Freeman LM, Weissman HS (eds) Nuclear Medicine Annual, New York, Raven 1980
25. Juhl JH: Delayed and non-union fractures In Paul and Juhl's Essentials of reontgen interpretation (ed 4), St. Louis: Mosby 1981
26. Forsted DL, Dalinka MK, Mitchell E: Radiologic evalua- tion of the treatment of non-union of fractures by electrical stimulation. Radiology 141:21-24, 1981
27. Lisbona R, Rosenthal L: Role of radionuclide imaging in osteoid osteoma AJR 132:77-80, 1979
28. Helms CA: Osteoid osteoma: the double density sign, Clin Orthop 222:167-173, 1987
29. Helms CA, Hattner RS, Vogler JB HI: Osteoid osteoma: radionuclide diagnosis, Radiology 151:779-784, 1984
30. Miller JE: Javelin thrower's elbow, J Bone Joint Surg Br 42:788-792, 1960
31. Hotchkiss RN: Common disorders of the elbow in athletes and musicians. Hand Clin 6:507-515, 1990
32. Woodward All, Bianco AJ Jr: Osteochondritis Dissecans of the Elbow. Clin Orthop 110:35-41, 1975
33. Gore RM, Rogers LF, Bowerman J, et al: Osseous manifestations of elbow stress associated with sports activities. AJR 1980; 134:971-977
34. Dalinka MK, Kricum ME, Zlatldn MB et al: Modern diagnostic joint imaging in joint disease. AIR 152:229-240, 1989
35. Plancker KD, Halbrecht J, Laurie GM: Medial and lateral epicondylitis in the athlete, in Plancker KD (ed): Clinics in Sports Medicine. Philadelphia, PA, Saunders, 1996, 283-305
36. Fink-Bennett D, Carichner S: Acute Flexion of the elbow: Optimal imaging position for visualization of the capitel- lum. Clin Nucl Med 1986;I 1:667-668
37. Torg JS, Moyer RA, Nonunion of a stress fracture through the olecranon epiphyseal plate observed in an adoles- cent baseball pitcher. J Bone Joint Surg Am 1977; 59:264-265
38. Heinrichs EM, Senske B J: Stress fracture of the diaphysis of the ulnar diaphysis in athletes: a case report and a review of the literature. South Dakota J Med 41:5-8, 1988
39. Retfig AC: Stress fracture of the ulna in an adolescent tournament tennis player. Am J Sports Med 1980; 11:!03-106




















