
Determining Consistency of Elbow Joint Threshold Angle in ...
15
Determining Consistency of Elbow Joint Threshold Angle in Elbow Flexor Muscles With Spastic Hypertonia Background and Purpose. Threshold angle, the point in passive range of motion where a muscle response or torque change is elicited, may be a potentially valid measure of hypertonus. Because the relationship of initial muscle length to threshold angle has not been addressed previously, this preliminary study examined whether starting elbow joint position and speed of stretch to elbow flexor muscles affect threshold angle. Subjects. Five subjects with stroke-induced hypertonia of the elbow flexor muscles participated. Methods. Two starting angles and two designated stretch speeds were applied randomly by a torque motor at each of three testing sessions. Results. Starting angle, subject, and session affected threshold angle. A 90-degree starting angle at a stretch speed of approximately 1.0 radian/s produced the most consistent threshold angles between sessions within subjects, and threshold angle was relatively consistent for some subjects, irrespective of speed. Conclusion and Discussion. If future research indicates that these data can be generalized, the use of threshold angle as a consistent measure of hypertonia will require comparison within individuals, use of a consistent starting angle, and a movement condition of a 90-degree starting angle and an approximate movement speed of 1.0 radian/s across sessions. [Wolf SI,, Segal RL, Catlin PA, et al. Determining consistency of elbow joint threshold angle in elbow flexor muscles with spastic hypertonia. Phys Ther. 1996;76:586-600.1 Key Words: Elbow; Joints; Musde spasticity; Muscle tonus; Upper extremity. Steven L Wolf Richard L Segal Pamela A Catlin Julie Tschorn Tina Raleigh Heather Kon tos Patricia Pate Physical Therapy . Volume 76 . Number 6 . June 1996 Downloaded from https://academic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 March 2022
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Determining Consistency of Elbow Joint Threshold Angle in ...

Determining Consistency of Elbow Joint Threshold Angle in Elbow Flexor Muscles With Spastic Hypertonia
Background and Purpose. Threshold angle, the point in passive range of motion where a muscle response or torque change is elicited, may be a potentially valid measure of hypertonus. Because the relationship of initial muscle length to threshold angle has not been addressed previously, this preliminary study examined whether starting elbow joint position and speed of stretch to elbow flexor muscles affect threshold angle. Subjects. Five subjects with stroke-induced hypertonia of the elbow flexor muscles participated. Methods. Two starting angles and two designated stretch speeds were applied randomly by a torque motor at each of three testing sessions. Results. Starting angle, subject, and session affected threshold angle. A 90-degree starting angle at a stretch speed of approximately 1.0 radian/s produced the most consistent threshold angles between sessions within subjects, and threshold angle was relatively consistent for some subjects, irrespective of speed. Conclusion and Discussion. If future research indicates that these data can be generalized, the use of threshold angle as a consistent measure of hypertonia will require comparison within individuals, use of a consistent starting angle, and a movement condition of a 90-degree starting angle and an approximate movement speed of 1.0 radian/s across sessions. [Wolf SI,, Segal RL, Catlin PA, et al. Determining consistency of elbow joint threshold angle in elbow flexor muscles with spastic hypertonia. Phys Ther. 1996;76:586-600.1
Key Words: Elbow; Joints; Musde spasticity; Muscle tonus; Upper extremity.
Steven L Wolf
Richard L Segal
Pamela A Catlin
Julie Tschorn
Tina Raleigh
Heather Kon tos
Patricia Pate
Physical Therapy . Volume 76 . Number 6 . June 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

ypertonia is a symptom associated with many central nervous system disorders that fre- quently contributes to impaired motion or compromised functional independence.l.2
Physical therapists use a variety of treatment techniques to contrlol hypertonia so that greater range of motion (ROM), strength, and functional ability can be achieved. Assessing the severity of muscle hypertonia, however, presents a challenge. The most common assessment used in the clinic is a manual determination of the amount of resistance perceived during a passive "quick stretch." This technique, however, requires clinicians to make judgments about the response, and the method
may be prone to errors because of variability in the applied stretch. Measurements indicative of volitional movement, such as the Ashworth scale, provide valuable information but do not specifically assess hypertonia.' Improved measurement techniques are needed to accu- rately quantify the degree of hypertonia. Better quanti- fication will allow therapists to draw correlations or inferential relationships with measures relating to phys- ical therapy interventions and, ultimately, to changes in disability.
Spastic hypertonia is observed in motor disorders that are characterized by velocity-dependent increases in
SL Wolf, PhD, PT, FAPTA, is Professor and Director of Research, Department of Rehabilitation Medicine, and Associate Professor, Department of Anatomy and Cell Biology, Emory University School of Medicine, 1441 Clifto'n Rd NE, Atlanta, GA 30322 (USA) ([email protected]). Address all correspondence to Dr Wolf:
RL Segal, PhD, PT, is Associate Professor, Department of Rehabilitation Medicine, Division of Physical Therapy, and Assistant Professor Department of Anatomy and Cell Biology, Emory University School of Medicine.
PA (htlin, EdD, PT, is Professor and Director, Division of Physical Therapy, Department of Rehabilitation Medicine, Emory University School of Medicine.
J Tschorn, PT, is Staff Physical Therapist, Grady Memorial Hospital, 80 Butler St SE, Atlanta. GA 30335.
T Raleigh, PT, is Staff Physical Therapist, Promina Gwinnette Health Systems, Lawrenceville, GA 30245.
H Kontos, PT, is Staff Physical Therapist, Tampa General Rehabilitation Hospital, Tampa. FL 33601.
P Pate, PT, is Staff' Physical Therapist, Rancho Los Arnigos Hospital, Downey, CA 90242
Ms Tschorn, Ms Raleigh, Ms Konto5, and Ms Pate were graduate students, Division of Physical Therapy, Department of Rehabilitation Medicine, Emory University, during this study, which was undertaken in partial fulfillment of thr requirements for their Master of Physical Therapy degree.
This stndy was supported in part by NIH Research Grant No. NS28784, US Public Health Service, Department of Health and Human Services, and was approved by the Emory University School of Medicine Human Investigation Committee.
Thzs nrlzclv iunr ruhmztt~d March 4, 1995, and iuns arc~/)tpd F~brunry 20, 1996.
Physical Therapy . Volume 76 . Number 6 . June 1996 Wolf et al . 587
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

tonic stretch reflexes with exaggerated tendon jerks, resulting from hyperexcitability of the stretch r e f l e ~ . ~ When a muscle is stretched, spindle afferent neurons initiate a short-latency motor response (the stretch reflex) to correct the perturbation and return the mus- cle toward its resting length. Motoneurons with mem- brane potentials that are nearer to threshold of activa- tion may be more readily excited by spindle afferent nerve input during sudden muscle lengthening. This situation, along with reduced inhibitory influences from interneurons, constitute one possible mechanism for spastic hyper t~nia .~ This enhanced motoneuron sensitiv- ity may result in shorter latency of muscle response to a phasic length change and may be manifest as a height- ened muscle responsiveness to these imposed length changes. The threshold angle is the joint angle during a passive stretch at which electromyographic (EMG) activ- ity increases above a resting l e ~ e l . l , ~ - ~ Threshold angle is presumably a measure of the relative state of motoneu- ron membrane depolarization and has been proposed as a quantitative measure of h y p e r t ~ n i a . ~ , ~
Mechanical influences from muscle and connective tis- sue alter the manifestations of hypert~nia.'-~ The initial position of a joint (starting angle) affects the length of the associated muscles; consequently, the degree of depolarization among motoneurons is influenced by the spatial and temporal summation of cutaneous and pro- prioceptive inputs onto them at any given starting angle. Muscle response to a passive stretch and the threshold angle, therefore, would be affected. If threshold angle remains the same for each respective starting angle, then the threshold angle may be a valid measure of hyper- tonia regardless of mechanical influences, such as changes in connective tissue viscoelastic properties, or the initial joint position. If threshold angle changes for each respective starting angle, then threshold angle may be a valid measure of hypertonia only within the respec- tive starting angle. The measurement of threshold angle may require specification of joint position for which a reproducible threshold angle can be seen prior to initiating any intervention. The measurement of thresh- old angle attempts to objectively reflect the variability of hypertonia seen clinically.
The speed of stretch may affect muscle tension or torque development, altering the presentation of hyper- t ~ n i a . ~ , " ~ - I V h e magnitude of stretch reflexes is observ- ably altered by speeds greater than 1.0 radian/s (1 radi- an=57.3"), yet the mechanism by which speed alters the stretch reflex is controversial. Faster speeds could alter the stretch reflex by decreasing the threshold of motoneuronal excitability, by increasing muscle stiffness secondary to speed-dependent viscoelastic properties, by altering muscle spindle sensitivity, or by any combina- tion of these variables4 This situation, however, should
not be construed as suggesting that slower passive stretches cannot also yield exaggerated muscle reflex responses.
The starting angle may be an indirect index of the point to which a muscle may be passively lengthened before eliciting an EMG response (threshold). Speed of passive stretch may affect the magnitude of the hyperactive stretch reflex and the threshold angle. At present, the effects of starting position (muscle length) and speed of passive stretch on the threshold angle of a joint acted upon by a hypertonic muscle are not well-documented. Development of an effective measurement technique to detect onset of muscle response to passive stretch may help quantify hypertonia.
This study, therefore, examined the effect of starting angle and speed on the threshold angle in subjects diagnosed with stroke-induced hypertonia. We see this impairment-based evaluative approach as a necessary precursor to gathering information about the impact of interventions on sensitivity to muscle-length changes. Indeed, reliable intrasubject findings about the relation- ship ofjoint starting angle, speed of passive motion, and reflex responses pave the way to ultimately correlating, in a quantitative fashion, the relationships between a specified impairment (hypertonicity) , interventions, and functional outcomes.
Design Five subjects were randomly assigned to 1 of 24 possible sequences of movement at each of three sessions. No sequence was repeated. Each sequence included four conditions of either 70 or 90 degrees of starting elbow flexion and a target speed of either 0.5 or 1.0 radian/s of movement. Data were collected for each of three stretches during each condition.
Sample Subjects were adults 31 years of age or older with hypertonicity in the upper extremity secondary to stroke occurring more than 4 months prior to data collection. Presence of hypertonicity was determined by detection of resistance to a manual passive stretch of the elbow flexors of the involved limb. Each subject's involved limb could be passively moved through the entire elbow ROM needed for the data-collection procedure, and no elbow joint contractures were present. Subjects were selected from a registry of patients with stroke, and participation was voluntary. Prior to participation, each subject signed a consent form approved by the Emory University School of Medicine Human Investigations Committee. Physi- cian consent for subject participation was obtained. The rights and privacy of the subjects were protected.
588 . Wolf et al Physical Therapy . Volume 76 . Number 6 . June 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

Table 1. Characteristics of Subiects
Characteristic Subject No.
1 2 3 4 5
Age (Y) 58 42 42 4 1 3 1
Gender Female Female Male Female Male
Site of lesion Bilateral lacunar Right frontal Right middle Basilar artery Left circle of lesions in basal lobe and cerebral artery thrombosis at Willis, ganglia, internal infarct at right brain stem intracranial thalamus, and capsule basal ganglion periventricular white matter
Hand dominance Right Right Right Right Right
Time since lesion 4 4 18 72 7
(mo)
Recovery stage' 3 2-3 3 4 3
Side of Right Left Left Right Right hypertonia
The selection criteria included (1) presence of resis- tance to muscle stretch," (2) elbowjoint passive ROM of 10 to 90 degrees of flexion, (3) ability to achieve an appropriate sitting position for testing, (4) ability to follow verbal commands, (5) appropriate cognition,14 (6) stage 2 moving into 3 to 5 of recovery according to the Brunnstrom stages of re~overy,~"nd (7) EMG activity above a resting baseline level upon passive stretch.
Measurements The starting angle was defined as the position of the elbow joint of the affected extremity measured just before an induced passive stretch using standard gonio- metric technique.l"tarting angles corresponding to functional length-tension relationships of the elbow flexor nluscles were chosen. These angles corresponded to slightly more than 50% of normal passive ROM. A series of three extension stretches were performed at a starting angle of 70 or 90 degrees of elbow flexion. Movemlent speed was defined as the speed of the exten- sion stretch applied by the torque motor in servo mode.
The mean of the baseline levels of elbow flexor muscle activity during passive stretch in four persons without hypertonia was obtained. These baseline values were typically around 4 pV (SD=3) for the biceps brachii muscle and 6 pV (SD=4.5) for the brachioradialis muscle. The threshold angle was then defined as the elbow joint position during stretch at which a subject's muscle activity exceeded two and a half standard devia- tions above this mean. The resultant criterion values required that biceps brachii muscle activity be greater than 10 pV and that brachioradialis muscle activity be greater than 15 pV. The EMG signal was amplified
(X1,OOO) and filtered between 20 and 500 Hz. The actual threshold value was determined from filtered EMG activity. The EMG activity was measured with surface electrodes placed on the skin over the bellies of the biceps brachii and brachioradialis muscles. The EMG activity and joint position were recorded during a stretch of a 1-radian (57.3") arc. The computer sampled the following measures at 1 kHz: joint angle, stretch speed, EMG activity of the biceps brachii and brachiora- dialis muscles, and torque. Electromyographic activity above the set criterion also was determined by the computer.
Joint position versus EMG activity was graphed from computer data. Graphic representation of the threshold angle was used to visually confirm the computer crite- rion for designating the threshold angle.
Subject Selection Subject characteristics and selection criteria were mea- sured during an initial screening session (Tab. l ) . For- tunately, enlistment of individuals with discretely differ- ent lesion sites was possible, allowing examination of consistency of responses. Information regarding age, gender, site of lesion, time since lesion, medical history, diagnosis, medical treatment received, past physical ther- apy treatment, aerobic exercise, and current medica- tions was obtained by review of the medical record or subject interview prior to the initial screening session. During the initial screening session, side of hand domi- nance, upper-extremity recovery stage,]'. elbow passive ROM, ability to follow simple verbal commands, ability to achieve a comfortable sitting position, appropriate cognition, and EMG responses were determined by standard clinical tests. Cognition was considered normal
Physical Therapy. Volume 76 . Number 6 . June 1996 Wolf et al . 589
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

if the subject responded correctly to all items on the modified Folstein Mini-Mental State Exam.14 Each sub- ject answered questions concerning feelings of general health, level of relaxation, and amount of caffeine intake prior to both the initial screening session and each of two data-collection sessions. A variety of lesion sites are represented.
Subject and Electrode Positioning Subject sitting position was controlled during each data- collection session. Position was determined at each session by measuring the following variables using stan- dard goniometric technique: (1) knee flexion between 80 and 100 degrees, (2) hip flexion between 80 and 100 degrees, (3) shoulder abduction between 40 and 60 degrees, (4) shoulder flexion at 20 degrees, (5) elbow flexion at 70 or 90 degrees, (6) forearm in 10 to 20 degrees of pronation, and (7) wrist neutral.16 Subjects faced forward with feet shoulder width apart and the uninvolved upper extremity placed comfortably on their lap.
Two silver-silver chloride electrodes with a Qmm record- ing surface were placed over each muscle at the begin- ning of the screening session. Electrode placement was determined by isolating the bellies of the biceps brachii and brachioradialis muscles during isometric contrac- tions." Measurement of the anatomical point of widest girth of the biceps brachii or brachioradialis muscle during an isometric contraction of that muscle was used to isolate each muscle belly. The vertical and horizontal midpoint of the each muscle belly at the point of widest girth was marked with a felt-tip pen. The electrode pair was placed on either side of the marking, oriented parallel to the muscle-fiber direction." Electrode pairs were spaced at 1.7 cm center-to-center to improve spec- ificity of the EMG signal. Isometric contractions also were used to verify correct electrode placements. All EMG activity was monitored on an oscilloscope to detect artifact during actual movements or prior to stretch.
Impedance between the skin and the overlying electrode was reduced by abrading the skin with sandpaper and cleansing the skin with alcohol. Skin impedance, mea- sured with an ohmmeter, between the ground electrode and each electrode was less than 5 kfl. The resistance between an electrode pair on each muscle belly was less than 2 kfl.
After initial electrode placement was determined during the screening session, an anatomical skin map was made. The skin map measured electrode placement from nearby landmarks such as anatomical structures, scars, or prominent freckles. The distance from the acromion to the biceps brachii muscle electrode and the distance from the styloid process of the radius to the biceps
brachii and brachioradialis muscle electrodes were mea- sured. The skin map was used at each session to ensure consistent electrode placement.
Reliability Intrarater and interrater reliability of all measurements was maintained at 100% agreement of values, obtained by repeated measurements by the same researcher or by a second researcher. Total agreement was observed for defining age, gender, hand dominance, site of lesion, time since onset, side of hypertonicity, upper-extremity stage of synergy involvement,'%nd ability of the subject to achieve testing position. Total agreement also was achieved for identifying medical history, physical ther- apy treatments, exercise, medications, general health, level of relaxation, and caffeine intake. There was total intrarater and interrater reliability in defining subject cognition and onset of EMG responses. Starting angle was equal within 2 1 degree, subject position was equal or within ?3 degrees, skin map placement was equal within k0.5 mm, and skin impedance equaled exact agreement. Agreement on threshold angle was deter- mined by comparing computer calculation with graphic displays, as described previously, and was always main- tained at 100% when performed in this manner. Cali- bration of all equipment was maintained throughout data collection.
Limb Movements Slow acceleration and deceleration of the forearm by the torque motor produced a smooth, passive stretch. The set speed produced by the torque motor was not instan- taneous. The acceleration period needed by the torque motor to reach the set speed was affected by the inertia of the limb and the inherent delay in the acceleration phase of the motor. To ensure consistency of speed, responses were examined within and across sessions. Figure 1 shows such consistency for the 70-degree start- ing angle at 0.5 radian/s within a subject (A) and across sessions (B). The across-sessions graph exemplifies the superimposition of the first stretch. Periodically, thresh- old angle was reached before the torque motor achieved the preset speed (ie, the limb was still accelerating). The actual speed at the occurrence of threshold was deter- mined for every stretch using the slope of time versus joint angle. Intrarater and interrater determinations of actual speed agreed 100%. All calculations regarding threshold angles were made at the actual speed at which they occurred. Thus, in calculating data by conditions, although the true speeds were used, we refer to condi- tions in the sense that the torque motor was pro- grammed to move at either 0.5 or 1.0 radian/s. Data in Figures 2 and 3, for example, depict the actual speed at which the threshold angle was achieved, and computa- tions made in Table 2 were based on actual speeds.
590 . Wolf et al Physical Therapy . Volume 76 . Number 6 . June 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

20 - A B
-
30 - -
- 40 - -
L W y 50 -
$ m 5 . 0 : / -
70 * ~ T l ~ l l ~ l ~ l ~ l l ~ ~ ~ n 1 ~ 1 1 1 ~ 1 ~ 1 ~ 1 ~ / ~ l / ~ ~
0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0 0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
TIME (s) TIME (s) _I
- - Plot of tirr~e versus ioint angle from typical biceps brachii muscle stretches showing approximately linear speed. Speed was calculated as the slope of the graph at the threshold angle. (A) Superimposition of three stretches from one session. (B) Superimposition of first stretch at each of three sessions. Actual excursion is approximately 0.93 radian; actual speed is 0.46 radian/s. Y axis is identical in A and B.
Proced~r re If a subject met all screening criteria, the first data- collection session was begun immediately. Prior to the screening session and each data-collection session, the subject was asked a set of pretrial questions to assess his or her emotional and physical state at the time of data collection. Electrode placement sites over the biceps brachii and brachioradialis muscles were determined at the screening session. The subject's skin was prepared, and the electrodes were placed on the electrode sites. Skin impedance was measured. The subject was posi- tioned in the chair, the involved forearm was placed in the prefabricated arm splint, and the elbow was aligned to the axis of the 7.2-hp torque motor (Fig. 4).* The electrodes were connected to the amplification system and to the oscilloscope. Electromyographic activity was preamplified at the source ( X 10) and subsequently amplified ( X 100) prior to analog-to-digital processing. The subject was asked to contract and relax the upper- extremity muscles to check for EMG activity on the oscilloscope and then was positioned correctly with the involved elbow placed at the selected starting angle.
The speed was set using a computer servo-mode pro- gram. Subjects were instructed to maintain the testing positioin without movement prior to testing. The muscles under the electrodes were determined to be passive
"'PMI Motion Technologies, 49 Mall Dr, Commack, NY 11725.
prior to testing by recording a baseline of EMG activity 100 milliseconds prior to stretch while the subject remained relaxed. Three stretches were performed dur- ing each of the four conditions. All stretches were separated by at least a 60-second interval. The procedure was repeated for two additional sessions, separated by 1 to 7 days.
Each of the remaining data-collection sessions began by positioning the subject at the torque motor in the servo mode. The skin map was used to locate the electrode placement sites. The subject received a different random sequence of the four conditions at each of the three data-collection sessions.
Data Analysis A computer graphics program plotted the raw data on a graph, with joint position on the X axis and EMG activity of the biceps brachii or brachioradialis muscle on the Y axis. Typical changes in the biceps brachii muscle during stretch are depicted by the arrows in Figures 5A and 5B. The occurrence of threshold angle can vary. Figure 5A demonstrates an abrupt EMG response to stretch, and Figure 5B demonstrates a more gradual response for the same muscle but from a different subject.
Threshold angle was determined for the biceps brachii and brachioradialis muscles during each stretch. A mean threshold angle also was calculated for each muscle
Physical Therapy . Volume 76 . Number 6 . June 1996 Wolf et al . 591
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

during each condition per session. The EMG activity was monitored during each stretch for torque motor noise, and data for a stretch were discarded if the baseline showed harmonics of 60-cycle activity. Trials that were discarded for this reason were repeated. Graphic repre- sentation of muscle activity during each stretch was examined to detect movement artifact. For 12 of 360 data points, information was irretrievable from disks, and a program for maximum likelihood estimation that assumes compound symmetry was used to estimate stretches. Using the Statistical Analysis System (SAS) program,t riormality of distribution of threshold angle per muscle was assured prior to statistical analysis, based on assessment of the skewness and kurtosis of the data.
90. STARTING ANGLE & 0.5 radianls +70° STARTING ANGLE & 1.0 radianls
A BICEPS BRACHll MUSCLE
The difference in threshold angles within conditions, within subjects, behveen testing sessions, and per muscle was determined using a one-way repeated-measures analysis of variance (ANOVA). The Tukey pair-wise procedure was performed post hoc when a statistically significant effect was found. The difference in threshold angles behveen conditions, within subjects, and per muscle was determined using a two-way (starting angle X speed) ANOVA. A Bonferroni post hoc multiple- comparison procedure was performed when a statisti- cally significant effect was found.lH For all tests, P<.05 was considered significant. A power analysis to deter- mine the applicability of the results to a larger popula- tion could not be undertaken due to the complexity of the design and of the data analysis. The SAS program was used to calculate the ANOVAs.lWata analysis across subjects was not performed, as it was determined that these analyses would be irrelevant due to expected
1.00 - -
0.90 - -
0.80 -
0.70 -
5 - .- n 0.60 - E - - B 0.50 - W a - V)
0.40 - -
0.30 - -
0.20 - -
0.10 - -
0.00
differences in muscle response to passive stretch across individual^.^,"^^
00 + O =aB -fft
G9 a0
-ltPr @@
-tttt#k @
0
Q ~ @ 0 = ' .
00
-1,,,,,,,,,1,,,,,,,,,Irrrmllljlllllllltl
Results The complete distribution of threshold angle determi- nation for all subjects is shown in Table 3. Figures 2A and 2B present, for the biceps brachii and brachioradia- lis muscles, respectively, the actual threshold angles for all stretches among all subjects and demonstrate the wide variability across subjects per condition. If the threshold angle would have been consistent, a vertical orientation of threshold angles across subjects would be expected for each condition.
Figure 2. The effect of session on threshold angle was variable and Composite threshold angles at specified speeds for (A) biceps brachii muscle and (B) brachioradialis muscle. There is wide variation of
dependent on muscle and condition (Tabs. 4 and 5 ) .
threshold angles across all subiects, demonstrating inconsistency in Table 4 shows Fstatistic values for significant session threshold angles between subjects. effects seen at all conditions except at a 90-degree
starting angle and a stretch speed of 1.0 radian/s. For the condition of 90-degree starting angle and 1.0-
0 10 20 30 40 50 60 70 80 90 THRESHOLD ANGLE (O)
90" STARTING ANGLE 8 0.5 radianls +70° STARTING ANGLE & 1.0 radianls
B BRACHlORADlALlS MUSCLE
'SAS Institute Inc, PO Box 8000, Cary, NC 2751 1
1.00 - -
0.90 - -
0.80 -
- 0.70 - -r? m .- u 0.60 - e - - 9 0.50 - W P - v, 0.40 -
-
0.30 -
0.20 -
0.10 - -
0.w -
592 . Wolf et al
0
0 0
9 Om%
Physical Therapy . Volume 76 . Number 6 . June 1996
0 10 20 30 40 50 60 70 80 90 THRESHOLD ANGLE (")
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

radian/s stretch, no effects were found in the brachiora- dialis muscle and only subject 4 showed an effect for the biceps brachii muscle. For the condition of 70-degree starting angle and 0.5-radian/s stretch, three subjects (1, 2, and 4) showed a difference in threshold angle for the biceps brachii muscle and only subject 4 showed a difference for both muscles.
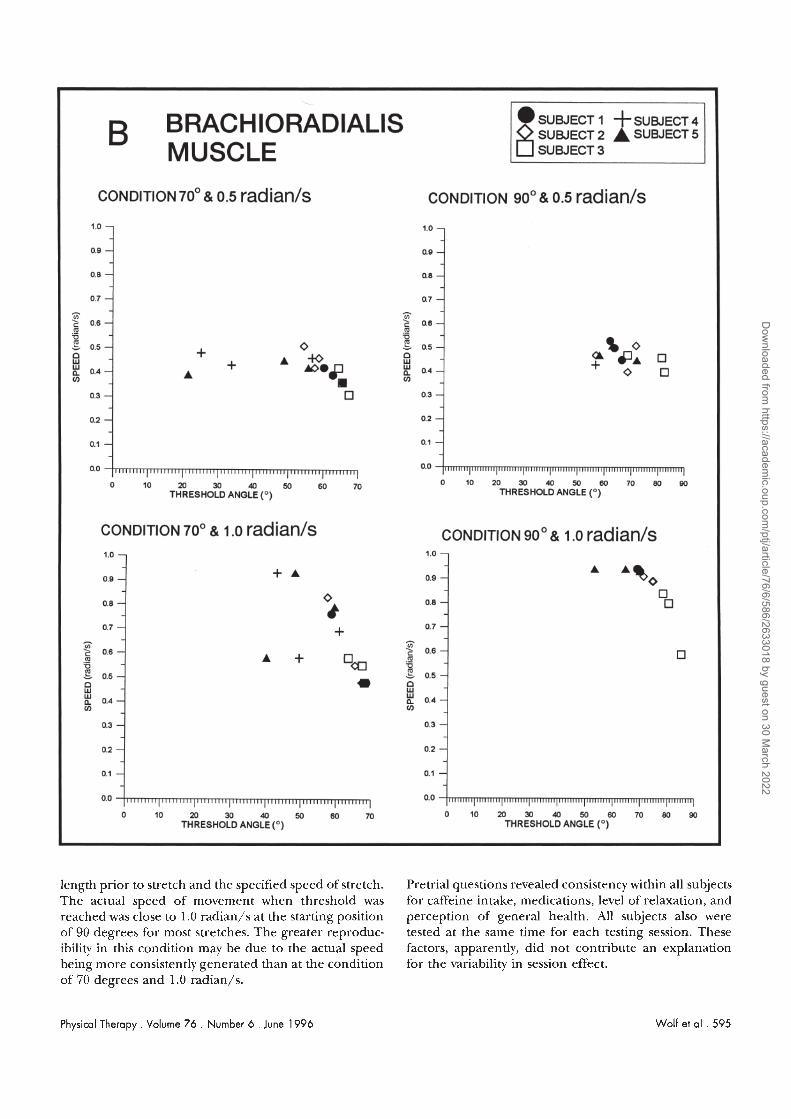
Three subjects (2, 3, and 4) showed a difference in threshold angle in the biceps brachii muscle as well as the brachioradialis muscle for the condition of 90- degree :starting angle and 0.5-radian/s stretch. Two subjects showed a difference in threshold angle in the biceps brachii muscle as well as the brachioradialis muscle fix the condition of 70-degree starting angle and 1.0-radian/s stretch. Only subject 1 showed a difference in threshold angle for both muscles. An examination of the data1 presented in Table 5 reveals no consistent pattern of session effect of the mean threshold angles. Figures 3A and 3B demonstrate the magnitude of con- sistency between mean threshold angles per session per subject iin the biceps brachii and brachioradialis muscles. In both muscles, this consistency is most observable in the condition of 90-degree starting angle and 1.0- radian/s stretch. Each data point represents mean threshold angle per subject per session. The symbols were most clustered in a vertical pattern for each subject at the 90-degree and 1.0-radian/s condition. The more vertically superimposed the symbols representing a sub- ject were, the more consistent was the response. Only the biceps brachii muscle response of subject 4 in the 90-degree and 1 .0-radian/s condition showed substantial variance (Fig. 3A). For most subjects, the vertical distri- bution of mean session responses for the brachioradialis muscle showed tight vertical clustering in the 90-degree and 1 .O-radian/s condition (Fig. 3B).
Threshold angle was not affected by speed for the biceps brachii or brachioradialis milscle among individual sub- jects (Tab. 2). In an effort to determine the relationship between the true speed of movement and the threshold angle, a one-way repeated-measures analysis of covari- ance was performed, substituting the actual speeds of movement for all five subjects over three sessions for each muscle. These results also showed no relationship between threshold angle and speed. Threshold angle responses, however, were affected by the starting angle. The starting angle had an effect on threshold angle for the biceps brachii muscle for subjects 1, 3, and 5 and for the brachioradialis muscle for subjects 1, 3, and 4. Table 6 shows the relationship between the starting angles ;at which an excursion was found. Clearly, a stretch from a 90-degree starting angle consistently showed a greater amount of limb excursion prior to occurrence of threshold angle than did a stretch from a 70-degree starting angle.
The actual threshold angle also was recorded among all subjects at select speeds and starting angles. This record provides a surrogate measure for muscle length at the time an elevated response in muscle activity was observed. Despite the greater excursion seen at a starting angle of 90 degrees, the threshold angles for some subjects were remarkably similar to those seen at a starting angle of 70 degrees. We calculated actual thresh- old angles averaged across trials among subjects who had complete data sets (subjects 1, 3, and 5 for the biceps brachii muscle and subjects 1 and 3 for the brachiora- dialis muscle) and who also showed differences in excur- sion, as depicted in Table 6. Among these differences, subject 1, for example, exhibited only a 2-degree differ- ence in the actual value of threshold angle for the biceps brachii muscle between 70 and 90 degrees (Fig. 3A) arid a 1-degree difference for the brachioradialis muscle (Fig. 3B) for threshold angles recorded at 0.5 radian/s. The most extreme averaged differences in actual thresh- old angle with different starting angles were measured in the biceps brachii muscle for subject 3 at 0.5 radian/s (15", compare top left and right panels, Fig. 3A).
Discussion Muscle responsiveness to passive lengthening using threshold angle as a measurement has been presented by Rymer and c ~ l l e a g u e s l , ~ , ~ ~ ~ as a justifiable technique for assessing hypertonia. Extraction of information from their studies suggests that threshold angle can be influ- enced by factors such as time of testing, individual attributes, viscoelastic properties of the muscle, starting muscle length, and speed of stretch. Of these factors, the resting length of a muscle exhibiting hypertonia and the speeds at which the muscle is moved have not been presented in terms of their consistency to produce a threshold angle response within subjects with hyper- tonia. Our data shed light on these issues.
Within any subject or condition, no pattern of session effect could be determined (Tab. 5). Results from pre- vious studies4.6 suggest a change in threshold angle between sessions. The variability of the threshold angle may be explained by the pseudorandom reflex proposed by Dietz and Berger," who found that motoneuronal firing may be altered by a functional movement and may change the occurrence of threshold. Dietz and Berger suggest that the strength of the hypertonic reflex response is decreased because the motoneuronal firing is dampened by a functional position. A 90-degree starting angle and a specified 1.0-radian/s speed had the most reproducibility across sessions, with only one ses- sion effect for the biceps brachii muscle for subject 4 (Tab. 5). The condition of a 90-degree starting angle and an approximate speed of 1.0 radian/s may produce the most consistent threshold arigle response within each subject due to a combination of the shorter muscle
Physical Therapy . Volume 76 . Number 6 . June 1996 Wolf et al . 593
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

igure 3. ~reshold angle determinations shown for each condition for [A) biceps brachii muscle and [B) brachioradialis muscle. Each symbol represents the ean for threshold angles for one session for each subiect. Note that the 90degree and 1 .O-radian/s condition shows the most vertical clustering means within subiects, demonstrating more consistent threshold angles than the other conditions. Some data points are missing for subject 4 due artifact when eliciting threshold angle responses at 90 degrees and 0.5 radian/s and at 90 degrees and 1.0 radian/s.
594 . Wolf et al
-
A BICEPS BRACHll SUBJECT 1 + SUBJECT 4
0 SUBJECT 2 A SUBJECT 5
MUSCLE
CONDITION 70' & 0.5 radianls CONDITION 90' & 0.5 radianls
Physical Therapy . Volume 76 . Number 6 . June 1996
- fi .Y
A
-0
1.0 - 1.0 - -
0.9 - -
0.8 -
0.7 - -
A
c 0.8 - .-
0.9 -
0.8 -
0.7 - A
$ 0.6 - .-
THRESHOLD ANGLE (O) 0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0 9 0
THRESHOLD ANGLE (O)
CONDITION 700 1 .o radianls CONDITION go0 & 1 .o radianls
u
+ 4 +
-0 0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0 9 0
1.0 -
0.9 -
0.8 -
0.7 - - $ 0.6 - .- u 6 0.5 - 0 w
0.4 - V)
0.3 -
0.2 -
0.1 -
0.0
0.5
B - E 0.4 - V) -
0.3 -
0.2 - -
0.1 - -
0.0
THRESHOLD ANGLE (O) THRESHOLD ANGLE (O)
1.0 -
0.9 -
0.8 -
0.7 - A
f 0.6 - m .- u
0.5 - B
0.4 - V)
0.3 -
0.2 -
0.1 -
I I ,I, 1 I I I I I I 1 p 0.0
6 0.5 --_ - B 0.4 -
V)
0.3 -
0.2 -
0.1 -
-- 0.0
0 I 0 20 30 40 50 60 70
0 10 20 30 40 50 60 70
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022
COND~T~ON 70' & 0.5 radianls
length prior to stretch and the specified speed of stretch. Pretrial questions revealed consistency within all subjects The act.ual speed of movement when threshold was for caffeine intake, medications, level of relaxation, and reached was close to 1.0 radian/s at the starting position perception of general health. All subjects also were of 90 degrees for most stretches. The greater reproduc- tested at the same time for each testing session. These ibility in. this condition may be due to the actual speed factors, apparently, did not contribute an explanation being more consistently generated than at the condition for the variability in session effect. of 70 degrees and 1.0 radian/s.
B BRACHlORADlALlS SUBJECT SUBJECT 2 I A +SUBJECT SUBJECT 4 5
MUSCLE
CONDITION go0 & 0.5 radianls
Physical Therapy. Volume 76 . Number 6 . June 1996
1.0 -
0.9 -
0.8 -
0.7 - - $ 0.6 - m .- u g 0.5 - 9 f 0.4 - V)
0.3 -
0.2 -
0.1 -
Wolf et al . 595
1.0 -
0.9 -
0.8 -
0.7 - - .r? c 0.8- m .- u g 0.5-
9 g 0.4- V)
0 3 -
0.2 -
0.1 -
0.0 -
0 1 0 M 3 0 4 0 5 0 6 0 7 0 0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0 9 0 THRESHOLD ANGLE (O) THRESHOLD ANGLE (O)
CONDITION 700 & 1 .o radianls CONDITION go0 & 1 .o radianls
A A%o
1.0 -
0.9 -
0.8 -
0.7 - - $ 0.6 - .- u g 0.5 - n W
0.4 - V)
0.3 -
0.2 -
0.1 -
0.0 -
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0 9 0 THRESHOLD ANGLE (O) THRESHOLD ANGLE (O)
1.0 -7
+ A 0.9 -
0 0.8 - 4 + 0.7 - -
$ 0.6 -
Oco m .- u g 0.5 - n * w
0.4 - V)
0.3 -
0.2 -
0.1 -
0.0 -
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

Table 2. Two-Way Analysis of Variance Testing for a Condition Effect for Threshold Angles Within Subjects
Speed Starting Angle Interaction
Subject No. F P F P F P
Biceps brachii muscle
1 2 3 4 5
Brachioradialis muscle 1 2 3 4 5
The lack of an effect for speed within subjects on threshold angle does not support the clinical evidence that hypertonia is speeddependent (Tab. 2) .43"9-12 The fastest speed used in this study, 1.0 radian/s, may not be as fast as the "quick stretch" performed in clinical settings to assess hypertonia. Given et al" recently found that speed of movement did not strongly affect stretch reflex behavior within four subjects who had sustained a stroke, using speeds ranging from 0.1 to 2.0 radian/s. Their subject with the greatest hypertonia assessed clin- ically, however, required a lower stretch speed to reach threshold than did a subject with mild hypertonia. Previous studies4."~'" have found an effect of speed on reflex threshold in some subjects, with a decrease in threshold angle occurring as a function of an increase in speed. These studies used stretch speeds ranging from 0.25 to 3.0 radian/s. The large range may explain the reported impact of speed on threshold. Our study used only speeds approximating 0.5 and 1.0 radian/s, which may not have been fast enough to create a speed effect on threshold angle. These speeds were chosen, however, to allow accurate comparison of results with those of previous studies that used similar speeds during data collection.
A correlation between decreased limb excursion prior to reaching the threshold angle and greater sensitivity to stretch was reported by Powers et al,H who did not consider the relationship of the starting position before the stretch occurred. In our study, an effect of starting angle on the magnitude of joint excursion to reach threshold angle was noted for both the biceps brachii and brachioradialis muscles in three subjects (Tab. 2). These effects accounted for 60% of total threshold angle values. The smaller excursion to reach the threshold
angle occurring frorn a 70-degree starting angle or the larger excursion to reach threshold angle occurring from a 90-degree starting angle may be a result of increased stretch reflex sensitivity at the 70-degree posi- tion. Table 6 shows that the 90-degree starting angle permitted a greater limb excursion prior to reaching the threshold angle than did the 70-degree starting angle. Stretch reflex sensitivity is increased at 70 degrees, when stretch begins with the muscle in a more lengthened position. Muscle spindle sensitivity may be greater at a 70-degree starting angle, or motoneurons may be closer to threshold level, as evidenced by less excursion of the limb prior to the occurrence of threshold (Tab. 2). With a 90-degree starting angle, the limb goes through greater excursion prior to threshold, indicating either decreased stretch reflex sensitivity or a greater magnitude of "slack" in the muscle prior to activating sufficient spindle input to further depolarize motoneurons to threshold.
Elevated stretch reflex sensitivity is thought to be due, in large part, to supraspinally mediated increased back- ground levels of depolarization of motoneurons prior to stretch, manifest in a greater threshold angle.3 At a 70-degree starting angle, the motoneuron is closer to depolarization and therefore threshold angle occurs earlier. Powers et alR placed their subject's biceps brachii muscle in a shortened position, at 120 degrees of elbow flexion, creating an even greater amount of slack than at 90 degrees. Threshold occurred broadly, at between 117 and 63 degrees of flexion.# This observation suggests that joint angles may have an important influence on threshold angle. If analysis was possible between the starting angles used in both studies, a 120-degree start- ing angle would probably allow greater limb excursion prior to reaching threshold angle than both the 70- and
596 . Wolf et al Physical Therapy . Volume 76 . Number 6 .June 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

Fi ure 4. Su % ject sealed at the torque motor with elbow positioned at 90 degrees of flexion in a prefabricated splint. Note electrode placements on biceps brachii, brachioradialis, and triceps brachii muscles.
90-degree starting angles. Unfortunately, whether Pow- ers et alH considered the effect that startingjoint position may have on the threshold angle is not clear.
Our observations support the possibility that, among the three subjects who showed greater joint excursion to threshold angle for either the biceps brachii or brachiora.dialis muscle when the starting angle began at 90 degrees, the threshold angle was determined by
muscle spindle sensitivity and not by muscle slack. The fact that our calculations within individual subjects yielded actual threshold angles that were similar in most instances, irrespective of starting angle or speed (0.5 or 1.0 radian/s) , suggests that each subject's stretch sensitivity was consistent under these circumstances. Close examination of the rela- tionship of actual threshold angle to condition within subjects (X axis, Figs. 3A and 3B) sustains the notion that the joint angles at threshold were remarkably similar at conditions specified by speed within subjects 1,3, and 5 for the biceps brachii muscle and subjects 1 and 5 for the brachioradialis muscle. The fact that this close relationship between the occurrence of threshold angle and condition does not exist within all subjects highlights the reality of intersubject variability in spindle sensitivity across the spec- trum of patients with stroke.
limitations The small sample limits the generalization of the find- ings. This study, however, was not intended to explore a sizable group effect but rather to determine whether starting angle can affect the threshold angle response in subjects with biceps brachii and brachioradialis muscle hypertonia. Our results are limited by using only two starting angles and two speeds to determine the effect of starting angle and speed on threshold angle and may be applicable only to the two speeds used. A limited num- ber of repeated measurements of threshold angle were
Figure 5. (A) Biceps brachii muscle electromyographic (EMG] response, with a sharp rise in activity at occurrence of threshold angle, which i s shown by the arrow (72"); (B] biceps brachii muscle EMG response from another subiect, with a gradual rise in activity prior to threshold angle (40.5"). Note slightly different scaling in Y axes.
Physical Therapy . Volume 76 . Number 6 . June 1996 Wolf et al . 597
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

Table 3. Mean and Standard Deviation Values of Threshold Angles for All Subiects at Every Condition
Condition (Starting AngleISpeed)
70'10.5 90'10.5 70'1 1 .o 90'1 1 .o radianls radian/s radianls radian/s - - - -
Subject No. Session X SD X SD X SD X SD
Biceps brachii muscle
1 1 67.3 1.5 67.0 2.2 69.6 0.3 71 .O 1.3 2 67.3 1.5 63.8 1.2 58.7 1.8 67.9 3.7 3 57.0 1.5 64.0 1.3 67.7 1.7 75.6 10.6
2 1 57.8 3.5 60.1 2.3 67.3 0.6 75.3 4.7 2 53.1 2.4 70.8 2.6 67.2 2.1 72.4 1 .O 3 65.4 6.4 68.1 4.8 55.3 3.2 79.1 3.7
3 1 64.8 4.5 80.4 0.5 67.2 1.6 82.1 6.2 2 67.8 1.3 80.4 0.5 64.7 5.2 83.4 4.7 3 68.8 0.8 86.9 1.2 66.1 4.7 81.9 5.8
4 1 38.4 3.7 0 0 66.1 3.5 22.8 19.8 2 60.6 4.6 73.3 4.1 61.5 8.2 57.6 2.5 3 61.3 4.8 73.7 5.5 51.2 15.6 75.9 13.2
5 1 61.4 5.1 0 0 65.7 1.2 73.8 3.8 2 62.0 4.8 75.9 8.7 62.7 2.6 70.0 5.9 3 54.3 12.9 58.0 8.7 63.4 3.4 68.5 8.0
Brachioradialis muscle
1 1 65.8 2.0 66.3 2.5 67.8 0.5 70.0 0.9 2 62.8 0 63.6 0.9 58.7 1.8 69.2 2.0 3 60.0 5.1 62.0 4.2 68.8 0.6 68.9 3.2
2 1 57.6 4.6 56.7 2.8 67.3 0.6 74.7 6.3 2 54.5 1.9 71.7 3.3 65.5 3.3 74.4 2.4 3 58.8 7.8 68.5 1 .O 57.5 6.9 71.2 3.3
3 1 65.5 3.4 68.5 3.7 63.5 8.8 85.0 3.7 2 67.5 1.2 81.2 1.7 68.1 0.1 80.5 1.6 3 64.4 2.6 82.3 3.5 67.5 2.0 78.3 6.0
4 1 25.3 1.8 0 0 60.9 7.4 0 0 2 56.9 3.3 56.6 0.6 43.2 5.9 0 0 3 33.9 4.4 0 0 49.5 16.0 0 0
5 1 55.8 4.2 62.8 2.7 59.5 0.3 69.7 0.8 2 48.9 8.6 71.9 11.3 48.3 1.1 64.7 7.8 3 21.6 37.5 58.0 8.1 40.2 2.8 53.3 16.9
recorded. A greater number of measurements may be necessary to yield a more accurate measurement of threshold angle. The speed generated by the torque motor at different starting angles is an inherent feature of the motor and the mass being moved. As long as displacement is linear and reproducible and the approx- imate speed of the stretch is known, as was the case in this study, the motor itself should not be a deterrent to the generalization of interpretation of data.
Future Investigations Suggestions for future research include examining the consistent use of a 90-degree starting angle and a 1.0-radian/s stretch to yield a reproducible threshold angle in elbow joint muscles within a subject over multiple testing sessions. The effect of consistency in
threshold angle for this condition should be assessed in a larger sample of subjects who have sustained a stroke and preferably those with similar, verifiable lesion sites. Research 011 the effect of starting position on threshold angle also should include evaluating a greater range of starting angles. These types of studies may well produce a more demonstrable relationship between starting angle and threshold angle and also will increase the ability to generalize our results to a larger population. In addition, use of torque motors that provide nearly instantaneous and accurately specified speeds would reduce the need to approximate the true speed at the time threshold angle is achieved.
Clinicians who treat patients with hypertonia usually measure the amount of resistance to phasic stretch to
598 . Wolf et al Physical Therapy . Volume 76 . Number 6 . June 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

Table 4. Significant0 Results of One-Way Repeated-Measures Analysis of Variance (d\ = 1 ) of Session Effect on Threshold Angle
Condition (Stafiing Angle/Speed)
Subject No. 70'/0.5 radian/s 90'10.5 mdian/s 70"/1.0 radian/s 90'/ 1.0 radian/s
Biceps brachii muscle 1 F=46.45 F=48.83 2 F=5.89 F=7.85 F=28.64 3 F=64.34 4 F=26.29 F=953.28 F= 1 1.47 5
Brachioradialis muscle 1 F=68.47 2 F=28.86 3 F=18.81 4 F=71.91 F=28.66 5 Fz96.44 --
Table 5. Tukey Pair-\~ise Analysis of Significanto Session Effects
Condition (Stadng Angle/Speed)
Subject No. 70"/0.5 mdian/s 90'/0.5 mdian/s 70"/1.0 mdian/s 90"/1.0 radian/s
Biceps brachii muscle 1 1 or 2>3 1 or 3>2 2 3>2 2> 1 1 or 213 3 3>1 and 2 4 2or3>1 2>1 and 3 2 or 3>1 5
Brachiorcrdiolis muscle 1 1 or 3>2 2 2 or 3>1 3 2 or 3>1 4 2>1 or 3 2>1 or 3 5 1 >2>3
Table 6. Bonferroni Significanta Post Hoc Multiple Comparison of Starting Angle Effects Within Subiects
Subject No. 0.5 radian/s 1.0 mdian/s
Biceps brachii muscle 1 2 3 4 5
Brachioradialis muscle 1 2 3 4 5
Physical Therapy . Volume 76 . Number 6 . June 1996
-
Wolf et al . 599
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022

determine the severity of hypertonia. There is also a need to examine a change in the severity of hypertonia resulting from an intenfention. This study illustrates the importance of controlling the starting position of the joint and the speed of the stretch when evaluating hypertonia from session to session to determine whether the hypertonia has really changed or whether the con- ditions have caused a change in the presentation of the hypertonia. The importance of starting position of the joint controlled by a hypertonic muscle prior to stretch has been demonstrated. A difference in starting position from one assessment to the next may cause inaccurate and unreliable results. The need for further research on the development of an objective and reliable measure- ment of hypertonia, for the use of both researchers and clinicians, also has been emphasized.
Conclusions If the analyses of data from these five subjects who sustained strokes can be generalized, a consistent start- ing angle prior to stretch should be used to determine a consistent threshold angle. The condition of a 90-degree starting angle and speeds approaching 1.0 radian/s within subjects and across sessions appears to yield a more reproducible threshold angle than the other three conditions. There is also a need to examine a greater range of starting angles and speeds and the related changes in threshold angle over time to specified interventions.
Acknowledgments We express our appreciation to the following individuals who gave so much of their time and effort in helping to see this project to completion: Mr James Hudson, with- out whose resources, equipment modifications, and bio- medical engineering background this project could not have been done; Mrs Jane Hudson, for her guidance and suggestions during the data collection procedure; and Mr John Kontos, for his assistance with data collection and counsel during data analysis.
References 1 Katz RT, Rymer W'E. Spastic hypertonia: mechanisms and measure- ment. Arch Phys /Wed Rrhnbil. 1989;70:144-155.
2 (:are). JR, Burghardt TP. Movement dysfunction following central newous system lesions: a problenl of neurologic or muscular impair- ment? Phjs ?Xu. 1993:73:538-547.
3 Lance JM'. The control of muscle tone, reflexes, and movement: Robert Wartenberg Lect~tre. ,Yuurology. 1980;30:1303-1313.
5 Kate RT, Rovai GP, Brait (1, Rvmer WE. Objective quantification of spastic hypertonia: correlation with clinical findings. Arch Phy~ Med Rehnbil. 1992;73(suppl):339 -347.
6 Powers RK, Campbell DL., Rymer WE. Stretch reflex dynamics in spastic elbow flexor muscles. Ann N~urol. 1989;2.5:32-42.
7Vander AJ, Sherman JH, Iaciano DS. Muscle. In: Vander AJ, Sherman JH, Luciano DS, eds. Human Physiology: Thr M~rhanisms oJ Body F~inction. 5th ed. New York, NY McGraw-Hill Publishing (:o;
1990:283-324.
8 Powers RK, Marder-hlever .J, Rynier WE. Quantitative relations between hvpertonia and stretch reflex threshold in spastic hemipare- sis. Ann Neurol. 1988;23:115-124.
9 Meyer M, Adorjani C. Tonic stretch teflex for quantification of pathologic muscle tone. In: Feldman RG, Young RR, Koella WP, eds. Sj~nsticity: Disordered Motor Conlrol. (;hicago, 111: Year Book Medical Publishers; 1980:315-330.
10 Herrnan R. The myotatic reflex: clinicophysiological aspects of spasticity and contraction. Brain. 1970;93:273-312.
11 Petajan JH. Motor unit control in spasticity. In: Feldman RG, Young RR, Koella WP, eds. Spastic~ty: Dzrordrrpd Motor Control. Chicago, Ill: Year Book Medical Publishen; 1980:233-247.
12 Chusic JG. Co~~r~laliveh'arroanato~ny andFunctionalA~urolo~, 17th ed. Los Altos, (:alif: Lange Medical Publications; 1979.
13 Levin MF, Feldman AG. Stretch reflex threshold regulation in normal and impaired motor control. In: Proc~edings o/'the 24th Ann~ral Meeting of the Society for .V~urosciunce Abslmcts. 1994;20:338. Abstract.
14 Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: a practical method for grading the cognitive state of patients for the clinician. JPsyrhiatr Rcr. 1975;12:189-198.
15 Brunnstrom S. Mov~ment Therr~fl zn H~rnzplegza. New York, NY Harper & Row; 1970.
16 Heck CV, Hendryson IE, Rowe CR. Joint Motion: M~thod of MenAzlring and Recording. Chicago, Ill: American Academy of Orthopaedic Sur- grona. 1965:lO-11.
17 LeCraw DE, Wolf SL. Electromyographic biofeedback (EMGBF) for neuromuscular relaxation and re-education. In: Gersh MG, ed. b.'l~ctro- theropy t n &habilitntzon. Philadelphia, Pa: FA Davis Co; 199T291-327.
18 Polit DF, Hungler BP. "v'urszng&imrch hnczplcr and Muthods. 4th ed. Philadelphia, Pa: JB Lippincott Co; 1991.
19 Brase CH, Brase CP. Underslandablr Statistirs: C o ~ ~ r ~ p t s and Muthods. 4th ed. Lexington, Mass: DC Heath & Co; 1991.
20 Burke D, Ashby P. Are spinal "presynaptic" inhibitor) mechanisms suppressed in spasticity? J Neurol Sci. 1972;15:321-326.
21 Dietz V, Berger W. Norma1 and impaired regulation of muscle stiffness in gait: a new hypothesis about muscle hypertonia. Exp Neurol. 1983;79:680-687.
22 Given ID, Dewald PA, Rvmer WE. Dependence of stretch reflex response on stretch velocity in spastic hemiparesis. In: Proc~~dings of the 24th Annztnl Meeting o f t h ~ Soriuty for Nruro.~cienc~ Abstracts. 1994;20:339. Abstract.
4 Rymrr WE, Poxc~ers RK. Pathophysiology of muscular hypertonia in spabticity. .\'mrosurg~ry. 1989;4:291-301.
6 0 0 . Wolf et al Physical Therapy . Volume 7 6 . Number 6 . June 1996
Dow
nloaded from https://academ
ic.oup.com/ptj/article/76/6/586/2633018 by guest on 30 M
arch 2022




















