Evidence-Based Diagnostic Algorithm for Glioma: Analysis of the Results of Pathology Panel Review...
11
Evidence-Based Diagnostic Algorithm for Glioma: Analysis of the Results of Pathology Panel Review and Molecular Parameters of EORTC 26951 and 26882 Trials Johan M. Kros, Karin Huizer, Aurelio Hernández-Laín, Gianluca Marucci, Alex Michotte, Bianca Pollo, Elisabeth J. Rushing, Teresa Ribalta, Pim French, David Jaminé, Nawal Bekka, Denis Lacombe, Martin J. van den Bent, and Thierry Gorlia Johan M. Kros and Karin Huizer, Eras- mus Medical Center; Pim French and Martin J. van den Bent, Dr Daniel den Hoed Cancer Center, Rotterdam, the Netherlands; Aurelio Hernández-Laín, Hospital Universitario 12 de Octubre Reseach Institute, Madrid; Teresa Ribalta, Hospital Clínic, University of Barcelona, Barcelona, Spain; Gianluca Marucci, Bellaria Hospital, University of Bologna, Bologna; Bianca Pollo, Fonda- zione Istituto di Ricovero e Cura a Carattere Scientifico, Istituto Neuro- logico “C. Besta,” Milano, Italy; Alex Michotte, Universitair Ziekenhuis Brus- sel, Vrije Universiteit Brussel; David Jaminé, Nawal Bekka, Denis Lacombe, and Thierry Gorlia, European Organisa- tion for Research and Treatment of Cancer, Brussels, Belgium; and Elisa- beth J. Rushing, Institute for Neuropa- thology, University Hospital of Zurich, Zurich, Switzerland. Published online ahead of print at www.jco.org on April 27, 2015. Supported by Grant No. KWF 2010- 4723 from the Koningin Wilhelmina Fonds (Dutch Cancer Society) and by the European Organisation for the Research and Treatment of Cancer Charitable Trust. Presented at the Society for Neuro- Oncology Scientific Meeting, Miami, FL, November 13-16, 2014. Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article. Corresponding author: Johan M. Kros, MD, PhD, Department of Pathology, Erasmus Medical Center, Wytemaweg 80, 3015CE Rotterdam, the Nether- lands; e-mail: [email protected]. © 2015 by American Society of Clinical Oncology 0732-183X/15/3399-1/$20.00 DOI: 10.1200/JCO.2014.59.0166 A B S T R A C T Purpose With the rapid discovery of prognostic and predictive molecular parameters for glioma, the status of histopathology in the diagnostic process should be scrutinized. Our project aimed to construct a diagnostic algorithm for gliomas based on molecular and histologic parameters with independent prognostic values. Methods The pathology slides of 636 patients with gliomas who had been included in EORTC 26951 and 26882 trials were reviewed using virtual microscopy by a panel of six neuropathologists who independently scored 18 histologic features and provided an overall diagnosis. The molecular data for IDH1, 1p/19q loss, EGFR amplification, loss of chromosome 10 and chromosome arm 10q, gain of chromosome 7, and hypermethylation of the promoter of MGMT were available for some of the cases. The slides were divided in discovery (n 426) and validation sets (n 210). The diagnostic algorithm resulting from analysis of the discovery set was validated in the latter. Results In 66% of cases, consensus of overall diagnosis was present. A diagnostic algorithm consisting of two molecular markers and one consensus histologic feature was created by conditional inference tree analysis. The order of prognostic significance was: 1p/19q loss, EGFR amplification, and astrocytic morphology, which resulted in the identification of four diagnostic nodes. Validation of the nodes in the validation set confirmed the prognostic value (P .001). Conclusion We succeeded in the creation of a timely diagnostic algorithm for anaplastic glioma based on multivariable analysis of consensus histopathology and molecular parameters. J Clin Oncol 33. © 2015 by American Society of Clinical Oncology INTRODUCTION Over the past years, several molecular parameters have been identified in diffuse glioma, with signifi- cant diagnostic, prognostic, and predictive informa- tion. Codeletion of 1p/19q is prognostic, but also predictive, for outcome to alkylating chemotherapy; isocitrate dehydrogenase-1 (IDH1) mutation is as- sociated with improved outcome of gliomas of sev- eral grades and possibly predictive for effectiveness of chemotherapy; O 6 -methylguanine–DNA meth- yltransferase (MGMT) promoter methylation has been shown to be predictive for benefit from alky- lating chemotherapy in anaplastic glioma. 1-9 In addition, amplification of epidermal growth factor (EGFR), mutation and deletion of PTEN, and mu- tation in telomerase reverse transcriptase (TERT) are considered diagnostic for high-grade glioma. 10-13 Trisomy of chromosome 7 and loss of chromosome 10 and its q-arm have also been associated with outcome. 2 With the increasing number of prognos- tic molecular parameters, a question arises about the extent to which histopathology remains significant for the diagnosis and prognosis of patients with dif- fuse infiltrating gliomas. The integration of prog- nostic and predictive molecular parameters in the WHO definitions of tumor entities is a subject of current debate. 14 Regarding histologic criteria, three issues are at stake. First, the histologic parameters for making the diagnosis should be associated with the biologic behavior of the tumor. Second, such fea- tures should be defined and recognized with accept- able interobserver variability, which is optimized by providing clear scoring outlines. 15-19 In a previous panel review of some of the materials of the EORTC (European Organisation for Research and Treatment JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T © 2015 by American Society of Clinical Oncology 1 http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2014.59.0166 The latest version is at Published Ahead of Print on April 27, 2015 as 10.1200/JCO.2014.59.0166 Copyright 2015 by American Society of Clinical Oncology from 156.83.0.28 Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015 Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
Transcript of Evidence-Based Diagnostic Algorithm for Glioma: Analysis of the Results of Pathology Panel Review...

Evidence-Based Diagnostic Algorithm for Glioma: Analysisof the Results of Pathology Panel Review and MolecularParameters of EORTC 26951 and 26882 TrialsJohan M. Kros, Karin Huizer, Aurelio Hernández-Laín, Gianluca Marucci, Alex Michotte, Bianca Pollo,Elisabeth J. Rushing, Teresa Ribalta, Pim French, David Jaminé, Nawal Bekka, Denis Lacombe,Martin J. van den Bent, and Thierry Gorlia
Johan M. Kros and Karin Huizer, Eras-mus Medical Center; Pim French andMartin J. van den Bent, Dr Daniel denHoed Cancer Center, Rotterdam, theNetherlands; Aurelio Hernández-Laín,Hospital Universitario 12 de OctubreReseach Institute, Madrid; TeresaRibalta, Hospital Clínic, University ofBarcelona, Barcelona, Spain; GianlucaMarucci, Bellaria Hospital, University ofBologna, Bologna; Bianca Pollo, Fonda-zione Istituto di Ricovero e Cura aCarattere Scientifico, Istituto Neuro-logico “C. Besta,” Milano, Italy; AlexMichotte, Universitair Ziekenhuis Brus-sel, Vrije Universiteit Brussel; DavidJaminé, Nawal Bekka, Denis Lacombe,and Thierry Gorlia, European Organisa-tion for Research and Treatment ofCancer, Brussels, Belgium; and Elisa-beth J. Rushing, Institute for Neuropa-thology, University Hospital of Zurich,Zurich, Switzerland.
Published online ahead of print atwww.jco.org on April 27, 2015.
Supported by Grant No. KWF 2010-4723 from the Koningin WilhelminaFonds (Dutch Cancer Society) and bythe European Organisation for theResearch and Treatment of CancerCharitable Trust.
Presented at the Society for Neuro-Oncology Scientific Meeting, Miami,FL, November 13-16, 2014.
Authors’ disclosures of potentialconflicts of interest are found in thearticle online at www.jco.org. Authorcontributions are found at the end ofthis article.
Corresponding author: Johan M. Kros,MD, PhD, Department of Pathology,Erasmus Medical Center, Wytemaweg80, 3015CE Rotterdam, the Nether-lands; e-mail: [email protected].
© 2015 by American Society of ClinicalOncology
0732-183X/15/3399-1/$20.00
DOI: 10.1200/JCO.2014.59.0166
A B S T R A C T
PurposeWith the rapid discovery of prognostic and predictive molecular parameters for glioma, the status ofhistopathology in the diagnostic process should be scrutinized. Our project aimed to construct a diagnosticalgorithm for gliomas based on molecular and histologic parameters with independent prognostic values.
MethodsThe pathology slides of 636 patients with gliomas who had been included in EORTC 26951 and26882 trials were reviewed using virtual microscopy by a panel of six neuropathologists whoindependently scored 18 histologic features and provided an overall diagnosis. The molecular datafor IDH1, 1p/19q loss, EGFR amplification, loss of chromosome 10 and chromosome arm 10q, gainof chromosome 7, and hypermethylation of the promoter of MGMT were available for some of thecases. The slides were divided in discovery (n � 426) and validation sets (n � 210). The diagnosticalgorithm resulting from analysis of the discovery set was validated in the latter.
ResultsIn 66% of cases, consensus of overall diagnosis was present. A diagnostic algorithm consisting oftwo molecular markers and one consensus histologic feature was created by conditional inferencetree analysis. The order of prognostic significance was: 1p/19q loss, EGFR amplification, andastrocytic morphology, which resulted in the identification of four diagnostic nodes. Validation ofthe nodes in the validation set confirmed the prognostic value (P � .001).ConclusionWe succeeded in the creation of a timely diagnostic algorithm for anaplastic glioma based onmultivariable analysis of consensus histopathology and molecular parameters.
J Clin Oncol 33. © 2015 by American Society of Clinical Oncology
INTRODUCTION
Over the past years, several molecular parametershave been identified in diffuse glioma, with signifi-cant diagnostic, prognostic, and predictive informa-tion. Codeletion of 1p/19q is prognostic, but alsopredictive, for outcome to alkylating chemotherapy;isocitrate dehydrogenase-1 (IDH1) mutation is as-sociated with improved outcome of gliomas of sev-eral grades and possibly predictive for effectivenessof chemotherapy; O6-methylguanine–DNA meth-yltransferase (MGMT) promoter methylation hasbeen shown to be predictive for benefit from alky-lating chemotherapy in anaplastic glioma.1-9 Inaddition, amplification of epidermal growth factor(EGFR), mutation and deletion of PTEN, and mu-tation in telomerase reverse transcriptase (TERT)are considered diagnostic for high-grade glioma.10-13
Trisomy of chromosome 7 and loss of chromosome10 and its q-arm have also been associated withoutcome.2 With the increasing number of prognos-tic molecular parameters, a question arises about theextent to which histopathology remains significantfor the diagnosis and prognosis of patients with dif-fuse infiltrating gliomas. The integration of prog-nostic and predictive molecular parameters in theWHO definitions of tumor entities is a subject ofcurrent debate.14 Regarding histologic criteria, threeissues are at stake. First, the histologic parameters formaking the diagnosis should be associated with thebiologic behavior of the tumor. Second, such fea-tures should be defined and recognized with accept-able interobserver variability, which is optimized byproviding clear scoring outlines.15-19 In a previouspanel review of some of the materials of the EORTC(European Organisation for Research and Treatment
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
© 2015 by American Society of Clinical Oncology 1
http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2014.59.0166The latest version is at Published Ahead of Print on April 27, 2015 as 10.1200/JCO.2014.59.0166
Copyright 2015 by American Society of Clinical Oncologyfrom 156.83.0.28
Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

of Cancer) 26951 trial, only two of four WHO-based grading featureswere found to relate to prognosis.17 Third, the prognostic value ofparticular features may be so strongly correlated that they could beomitted. The use of materials of clinical trials offers an optimal settingfor weighing and selecting significant prognostic parameters and sub-sequently developing a diagnostic algorithm.
In this study, we investigated the inter-relationship between his-tologic and molecular parameters by using all available materials ofEORTC trials 26951 (n � 363) and 26882 (n � 273). For trial 26951,the available molecular data included 1p/19q loss, loss of chromosome10 and chromosome arm 10q, gain of chromosome 7, amplification ofEGFR, mutation of IDH1, and methylation of the promoter ofMGMT. The histologic review of the tumors was performed by a panelof six neuropathologists. The panel members scored 18 histologicfeatures and generated an overall histologic diagnosis for each tumor.A diagnostic algorithm was designed based on conditional inferencetree (CTREE) analysis of the consensus features and molecular param-eters of two thirds of the cases (discovery set). The algorithm wasvalidated with data from the other third of the cases (validation set).
METHODS
EORTC Trials 26951 and 26882
EORTC trial 26882 investigated the effects of adjuvant treatment withcombined carmustine and dibromodulciterol and radiotherapy in malignantgliomas.20 In EORTC trial 26951, the effects of adjuvant procarbazine, lomus-tine, and vincristine in anaplastic oligodendrogliomas (AODs) and anaplasticmixed oligoastrocytomas were investigated.21,22 The outlines of both trials areprovided in the Data Supplement.
Histologic Evaluation and Virtual Microscopy
A total of 418 patients were recruited for trial 26882 and a total of 368patients for trial 26951. Pathology material for 636 patients was available forreview (Appendix Table A1, online only). The slides from both trials weremixed, and the reviewers were blinded regarding to which trial the individualslides belonged. For the construction of the diagnostic algorithm, a discoveryset consisting of 426 cases was used (243 cases from EORTC trial 26882 and183 cases from EORTC trial 26951). For the validation stage of the project, inwhich the algorithm was tested for its prognostic power, the remaining 210cases were used (120 from EORTC trial 26882 and 90 from EORTC trial26951). A panel of six experienced neuropathologists reviewed the slides(A.H.-L., G.M., A.M., B.P., E.J.R., T.R). All hematoxylin and eosin–stainedhistologic slides were scanned for virtual microscopy (Hamamatsu scanner;Hamamatsu-shi, Japan). Eighteen histologic features were included in anelectronic scoring scheme (Table 1). Features were grouped according to theirrelation to tumor lineage and tumor grade.23 In addition to scoring the indi-vidual histologic features, the reviewers attributed an overall diagnosis to eachtumor. Consensus on particular features and on the overall diagnosis wasdefined as agreement between � four of the six reviewers.
Molecular Parameters
Molecular data were present for only some of the cases of trial 26951.Fluorescence in situ hybridization for chromosome arms 1p, 19q, 10q; chro-mosomes 7 and 10; and EGFR and MGMT promoter hypermethylation andmutation analysis for IDH1 were performed as previously described.2,8,24
Statistics
The Spearman rank correlation coefficient was used to assess the rela-tionship between factors. Intraclass correlations (ICCs) were used as chance-corrected measures of agreement on the features. ICCs and 95% CIs werecomputed on the basis of the variance components of two-way design generallinear models, allowing for breaking of the global variability into that between
patients and between panelists. For each factor, Kaplan-Meier curves, log-ranktests (binary factors), and Wald test (� two levels) were computed. Propor-tional hazards assumptions were evaluated by examining the plot of the log ofnegative log estimates over the log survival time. Factors significant inunivariable survival analyses (at � of 5% and ICC � 0.7) were consideredfor Cox regression analyses. Factors with � 5% of the sample in thesmallest category were discarded. The stepwise backward method was usedfor factor selection (at 5%). In addition to Cox regression, CTREE analysiswas performed (Data Supplement).
RESULTS
The six panelists reviewed slides from 636 patients (26882 trial, n �363; 26951 trial, n � 273) and rendered a total of 4,345 evaluations.Because of the inferior quality of the slides, 170 reviews were notperformed (reviewer one, n � 12; reviewer two, n � 33; reviewerthree, n�22; reviewer four, n�18; reviewer five, n�71; reviewer six,n � 14). For one additional case, the local investigator did not send theeligibility checklist, so the diagnosis could not be checked.
Overall Diagnoses
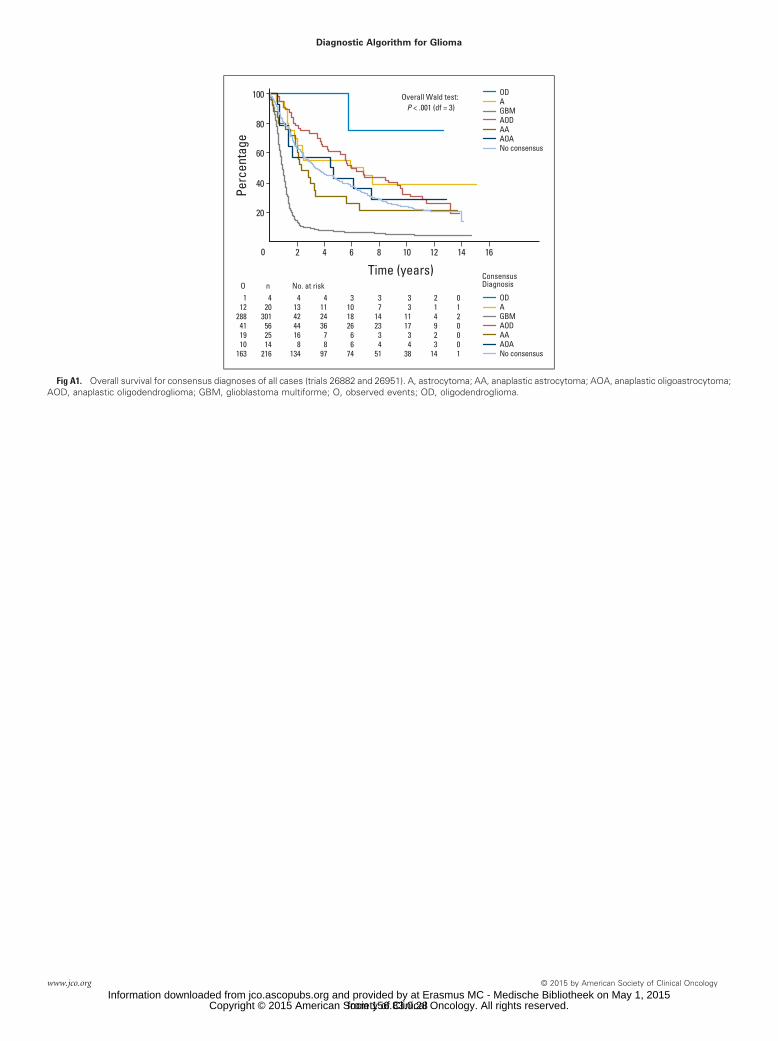
The overall diagnoses individually made by the six reviewers arelisted in the Data Supplement. In 420 (66%) of the total 636 cases, thepanel reached consensus. For the total 636 cases from both trials, thediagnoses made by the local pathologists included AOD (31%), glio-blastoma multiforme (GBM; 29%), anaplastic astrocytoma (AA;26%), anaplastic oligoastrocytoma (AOA; 2%), and other (eg,ependymoma, pilocytic astrocytoma; 1%; Data Supplement). Thereviewers made the diagnoses of GBM (47%), AOD (9%), AA (4%),and AOA (2%) and additional diagnoses of oligodendroglioma (OD;1%) and astrocytoma (A; 4%). In 34% of cases (216 of 636), noconsensus diagnosis (ie, agreement of four of six reviewers) wasreached. For 171 cases, no consensus diagnosis was reached because� two panelists were unable to interpret the tissue. The diagnosis ofGBM made by local pathologists was confirmed by consensus in 164(88%) of 168 cases. The local diagnoses of AOD, AA, and AOA wereconfirmed by panel consensus in only 25%, 12%, and 6% of cases,respectively. In 10% of the GBMs diagnosed by the local pathologists,no consensus was reached. For the diagnoses of AOD, AA, and AOAmade by the local pathologists, no consensus was reached in 41%,51%, and 41% of cases, respectively. The distributions of the consen-sus diagnoses separated for EORTC trials 26951 and 26882 are alsoshown in the Data Supplement. In trial 26882, astrocytic tumors,particularly GBMs, were predominantly diagnosed (253 of 259 cases),whereas in trial 26951, tumors with oligodendroglial traits (ie, OD,AOD, AOA) were recognized in a substantial number of cases (68 of161). This skewed distribution resulted from the different trial entrees.The overall survival (OS) curves of the consensus diagnoses are shownin Appendix Figure A1 (online only) and follow the expected order ofOD, AOD, A, AOA, AA, and GBM, from best to worst survival.
Histologic Features
Of the 18 histologic features scored by the reviewers, five featureshad an ICC � 0.7 (Table A2). In univariable analysis, 14 of the 18features showed significant prognostic power, including the fourWHO grading features (Table A2). Thirteen features had an ICC � 0.7and significant prognostic power (Appendix Table A2, online only).The following pairs of consensus features were significantly correlated:
Kros et al
2 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

minigemistocytes and perinuclear halos (r � 0.37; P � .001), perinu-clear halos and calcifications (r � 0.41; P � .001), classic gemistocytesand giant cells (r � 0.38; P � .001), microcysts and mucoid degener-ation (r � 0.5; P � .001), abnormal vessel structure and abnormalnumber of vessels (r � 0.74; P � .001), and abnormal vessel structureand necrosis (r � 0.51; P � .001). Astrocytic cell processes werenegatively correlated with perinuclear halos (r ��0.51; P � .001) andcalcifications (r � �0.39; P � .001), and the presence of classic
gemistocytes was negatively correlated with perinuclear halos (r ��0.43; P � .001; Appendix Table A2, online only). The distribution ofthe histologic features over the consensus diagnoses is listed in Table 1.Fifteen of the 18 features were not randomly distributed but showedpreference for � one consensus diagnosis (Table 1). In Cox regressionanalysis, the following features showed independent prognostic pow-er: perinuclear halos, astrocytic cell processes, microcysts, and mitoticindex (Table 2).
Table 1. Distribution of Consensus Histologic Features in Consensus Diagnoses
Typing
Consensus Diagnosis
P�OD (n � 4) AOD (n � 56) AOA (n � 14) A (n � 20) AA (n � 25) GBM (n � 301)
Perinuclear halos 4 of 4 56 of 56 13 of 13 0 of 20 0 of 24 58 of 264 � .001Microcysts 2 of 2 15 of 48 6 of 8 4 of 8 2 of 18 26 of 256 � .001Mucoid degeneration 0 of 4 6 of 49 0 of 14 1 of 20 1 of 24 6 of 298 .02Calcification 3 of 4 28 of 54 4 of 13 0 of 20 0 of 25 13 of 292 � .001Miniature gemistocytes 1 of 2 9 of 31 5 of 12 0 of 19 0 of 23 6 of 290 � .001Gemistocytes 0 of 4 0 of 56 3 of 14 7 of 18 12 of 20 99 of 219 � .001Polar spongioblastoma-like foci 0 of 4 1 of 54 0 of 14 0 of 20 0 of 25 0 of 301 .28Protoplasmic astrocytes 0 of 4 0 of 56 0 of 14 0 of 20 0 of 25 0 of 301 NAAstrocytic cell processes 0 of 3 0 of 56 12 of 12 18 of 18 23 of 24 270 of 280 � .001
Grading
Consensus Diagnosis
P�OD (n � 4) AOD (n � 56) AOA (n � 14) A (n � 20) AA (n � 25) GBM (n � 301)
Nuclear pleomorphism† � .001Low 1 of 4 0 of 55 0 of 14 3 of 16 0 of 22 0 of 289Medium 3 of 4 55 of 55 13 of 14 13 of 16 22 of 22 257 of 289High 0 of 4 0 of 55 1 of 14 0 of 16 0 of 22 32 of 289
Cell density � .001Low 0 of 4 0 of 45 0 of 14 6 of 16 1 of 23 2 of 275Medium 4 of 4 31 of 45 13 of 14 10 of 16 21 of 23 236 of 275High 0 of 4 14 of 45 1 of 14 0 of 16 1 of 23 37 of 275
Mitoses† � .001Mitotic index
Median 0.3 0.8 0.7 0.4 0.7 1.0Range 0.1 to 0.4 0.3 to 1.7 0.2 to 1.6 0.0 to 1.3 0.3 to 1.7 0.3 to 3.2
Microvascular proliferation† � .001Increased No. of vessels 4 of 4 56 of 56 14 of 14 3 of 16 12 of 18 298 of 299Abnormal vessel structure 1 of 3 55 of 55 10 of 11 0 of 20 5 of 17 300 of 300
Necrosis 0 of 4 24 of 50 0 of 13 0 of 20 0 of 25 267 of 289 � .001Infarction† 0 of 4 1 of 52 0 of 14 0 of 20 0 of 25 80 of 235 � .001Sarcomatous parts 0 of 4 0 of 56 0 of 14 0 of 20 0 of 25 9 of 289 .76Giant cells 0 of 4 0 of 56 0 of 14 0 of 20 0 of 24 41 of 282 � .001PNET-like foci 0 of 4 1 of 56 0 of 14 0 of 20 0 of 25 4 of 295 .82
Molecular Data‡
Consensus Diagnosis
P�OD (n � 4) AOD (n � 55) AOA (n � 9) A (n � 4) AA (n � 4) GBM (n � 85)
1p/19q loss 2 of 4 20 of 50 0 of 9 0 of 4 0 of 4 7 of 76 � .00110 loss 1 of 3 3 of 41 0 of 3 1 of 3 1 of 3 23 of 63 .00810q loss 1 of 4 2 of 41 2 of 5 0 of 4 1 of 2 17 of 65 .02Gain 7 0 of 3 7 of 35 1 of 4 0 of 3 1 of 3 31 of 31 � .001IDH1 mutation 2 of 2 15 of 25 0 of 4 4 of 4 1 of 2 9 of 43 � .001EGFR amplification 0 of 3 1 of 38 2 of 5 0 of 3 2 of 3 34 of 65 � .001MGMT promoter methylation 2 of 2 21 of 29 1 of 2 4 of 4 2 of 3 29 of 44 .70
NOTE. Eighteen histologic features are grouped to tumor lineage–related and tumor grade–related features. Cells show presence of feature among No. ofcases tested.Abbreviations: A, astrocytoma; AA, anaplastic astrocytoma; AOA, anaplastic oligoastrocytoma; AOD, anaplastic oligodendroglioma; GBM, glioblastoma multiforme;
NA, not available; OD, oligodendroglioma; PNET, peripheral neuroectodermal tumor.�P values refer to distribution of feature over respective consensus diagnoses.†Included in current grading according to WHO.‡Available for trial 26951 only.
Diagnostic Algorithm for Glioma
www.jco.org © 2015 by American Society of Clinical Oncology 3
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

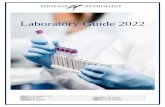
CTREE analysis of the prognostic power of the histologic featuresyielded six diagnostic nodes, resulting from a decision tree consistingof the following parameters: perinuclear halos, microcysts, astrocyticcell processes, mitotic index, and necrosis (Fig 1A). In nodes 4, 5, and6, the consensus diagnosis glioblastoma dominated (73%, 94%, and63%, respectively). Node 11 consisted entirely of tumors that receivedthe consensus diagnosis of glioblastoma. Eighty-eight percent of node8 diagnoses were AOD, and 86% of node 10 diagnoses were AOA.Percentages of 1p/19q loss, IDH1 mutation, and EGFR amplificationwere 17%, 36%, and 31%, respectively, for node 4; 6%, 17%, and 50%,respectively, for node 5; 0%, 57%, and 22%, respectively, for node 6;47%, 61%, and 6%, respectively, for node 8; 30%, 46%, and 14%,respectively, for node 10; and 13%, 13%, and 45%, respectively, fornode 11 (Fig 1A). The OS curves for the nodes in the discovery set ran,in the order of best to worse survival, as follows: nodes 8, 10, 6, 4, 11,and 5 (Fig 1B). The OS curves in the validation set (n�210) ran, in theorder of best to worse survival, as follows: nodes 8, 6, 10, 4, and 11intertwined and 5 (Fig 1C).
Molecular Parameters
Except for MGMT promoter hypermethylation (Fisher’s P � .7;Table 1), all other molecular parameters showed preference for par-ticular consensus diagnoses (Table 1). Codeletion 1p/19q was absentin A, AA, and AOA (0%) and less frequent in GBM (9%); it was mostfrequent in AOD (40%). None of the consensus mixed AOA showedloss of 1p/19q. Mutation of IDH1 was less frequent in GBM (21%), ascompared with OD, AOD, A, and AA, and was not present in anyAOA. EGFR amplification was more frequent in GBM (52%) com-pared with AOD (3%). The other chromosomal aberrations showedpreference for higher-grade tumors, particularly GBM. Polysomy 7was more frequent in GBM (100%) compared with AOD (20%).Chromosome 10 loss was more frequent in GBM (37%) comparedwith AOD (7%); 10q loss was more frequent in GBM (26%) com-pared with AOD (5%; Table 1).
The consensus feature of astrocytic cell processes was negativelycorrelated with 1p/19q loss (r � �0.35; P � .001) and positivelycorrelated with EGFR amplification (r � 0.30; P � .001; AppendixTable A2, online only). Other molecular parameters failed to showsignificant correlations with the consensus features.
Cox regression analysis of the molecular parameters showed that1p/19q loss, IDH1 mutation, and EGFR amplification were indepen-dent significant parameters for OS (Table 2). CTREE analysis of themolecular parameters yielded three nodes resulting from dichotomiesfor 1p/19q loss and EGFR amplification (Fig 2A). With respect toconsensus diagnosis, 50% of cases in node 3 were gioblastomas, 33%
were AODs, and 12% were AOAs, whereas the other diagnostic cate-gories (ie, OD, A, AA) comprised only 2% each of the cases repre-sented in this node. Node 4 consisted of 83% consensusglioblastomas, 8% AOAs, and 4% each AODs and AAs. Fifty-sevenpercent of cases in node 5 were consensus AODs, and 26% wereGBMs. AA and AOA represented 9% each in node 5 (Fig 2A). TheOS curves for the three nodes in the discovery and validation setsare shown in Figures 2B and 2C.
ThereweretoofeweventstoobtainreliableresultsbyCoxregressionanalysis on the combined histologic features, consensus diagnoses, ormolecular parameters. CTREE analysis of the histologic features com-binedwiththemolecularparametersyieldedfourdiagnosticnodesresult-ing from dichotomies for 1p/19q loss, EGFR amplification, and astrocyticcell processes (Fig 3A). Ninety-one percent of node 4 and 62% of node 7cases consisted of consensus AODs, whereas 76% of node 5 and 83% ofnode 6 cases consisted of consensus GBMs (Fig 3A). The curves of boththe discovery and validation sets ran, in the order of best to worse OS, asfollows: nodes 7, 4, 5, and 6 (Figs 3B and 3C).
DISCUSSION
Our results show that a single histopathologic feature may well con-tribute significant prognostic information when added to the stron-gest molecular diagnostic discriminators. In addition, the discrepancybetween overall (consensus) diagnosis and molecular parameters isillustrated. Although many tumors with the classic oligodendroglialfeature of perinuclear halos show strong association with the consen-sus diagnosis (anaplastic) oligodendroglioma (node 8; Fig 1A), thereare still many gliomas displaying the less classic mixed histology or thecharacteristics of GBM (nodes 10 and 11; Fig 1A). Although 54 tumorsreceived the consensus diagnosis of (anaplastic) oligodendroglioma,� half showed the 1p/19q codeletion (Table 1), which is a relativelylow number as compared with numbers in the literature.25 Interest-ingly, CTREE analysis revealed a diagnostic category of 1p/19q non-codeleted tumors mainly diagnosed as AOD by consensus, of whichthe progression-free survival and OS curves ran distinct from those ofthe 1p/19q codeleted tumors (node 4 v 7; Figs 3B and 3C). It would beinteresting to further characterize this group, but this was not possiblein our study.
There seemed to be considerable interobserver variation amongthe reviewers in making the diagnosis of AOA and an obvious personalpreference for making the diagnosis of mixed OA or AOA instead ofpure OD or AOD. Panel member 3 made the diagnosis of AOA in� 16% of cases, whereas this diagnosis ranged from 3.3% to 9.9%
Table 2. Cox Regression Modeling of Histopathologic and Molecular Parameters
Parameter df Parameter Estimate SE �2 P HR 95% Confidence Limit
Perinuclear halos 1 �0.59573 0.26337 5.1165 .0237 0.551 0.329 to 0.924Astrocytic cell processes 1 0.99378 0.33455 8.8239 .0030 2.701 1.402 to 5.204Microcysts 1 �1.29965 0.26950 23.2553 � .001 0.273 0.161 to 0.462Mitotic index 1 0.56160 0.20887 7.2292 .0027 1.753 1.164 to 2.6411p/19q loss 1 �1.05594 0.37657 7.8631 .0050 0.348 0.166 to 0.728IDH1 mutation 1 �0.61877 0.30253 4.1834 .0408 0.539 0.298 to 0.975EGFR amplification 1 0.75430 0.28343 7.0829 .0078 2.126 1.220 to 3.705
Abbreviation: HR, hazard ratio.
Kros et al
4 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
among reviewers 1, 2, 4, 5, and 6. (Data Supplement). In the literature,there is compelling evidence that tumors with mixed histology aremolecularly divided between the oligodendroglial and astrocytic ge-notypes.26 None of the consensus AOAs showed 1p/19q codeletion(Table 1), indicative of the tendency to overdiagnose oligodendroglialtumors by microscopy.
In Cox regression and CTREE analysis, the feature of astrocyticcell processes, rather than perinuclear halos, was sustained (Table 2;Fig 3A). The reason may well be the strong association of the perinu-clear halos with codeletion of 1p/19q. The presence of astrocytic cellprocesses is indicative of an astrocytic tumor component and promptsa diagnosis of A, AA, GBM, or mixed OA. Recently, mutation in the
Perinuclear haloesP < .001
MicrocystsP < .001
Astrocytic processesP = .032
Mitotic indexP < .001
NecrosisP < .014
No
No
No
No
No
Yes
YesYes
Yes
Yes
A
DCB
ODAODAOAAAAGBM
Node 4 Node 5 Node 6 Node 8 Node 10 Node 11
1p19q loss IDH1 mut. EGFR ampl.
40302010
0
4030
6050
2010
0
4030
6050
2010
0
4030
6070
50
2010
0
4030
50
20100
4030
50
20100
Perc
enta
ge
Time (years)
100
80
60
40
20
42 6 8 10 12 14 16
45681011
45681011
ODAODAOAAAAGBM1p/19qIDH1 mut. EGFR ampl.
000
13.513.5
73173631
00006
946
1750
006
2563630
5722
5870008
47616
70
86007
304614
00000
100131345
% Node 4 Node 5 Node 6 Node 8 Node 10 Node 11
45681011
45681011
81133
21394340
361522434314
238
1534389
2048
2829
8
1325
23217
1112
1716
7
402871
101010
96136
31546445
edoNedoNksir ta .oNnO
Overall Wald test: P < .001 (df = 5)
Perc
enta
ge
Time (years)
100
80
60
40
20
00 42 6 8 10 12 14 16
386616201720
169
132617
7
238
153438
9
1237
2297
721
1455
520
1152
310720
100000
476817312423
O n No. at risk
Overall Wald test: P < .001 (df = 5)
Fig 1. (A) Results of conditional inference tree (CTREE) modeling of histologic features, yielding six diagnostic nodes (no, absent; yes, present). Pie diagrams showdistribution of consensus diagnoses for each node; bar diagrams show distribution for following molecular parameters: codeletion 1p/19q, IDH1 mutation (mut), andEGFR amplification (ampl). Overall survival according to nodes resulting from CTREE analysis of histologic features for (B) discovery and (C) validation sets. (D) Actualpercentages of consensus diagnoses. A, astrocytoma; AA, anaplastic astrocytoma; AOA, anaplastic oligoastrocytoma; AOD, anaplastic oligodendroglioma; GBM,glioblastoma multiforme; O, observed events; OD, oligodendroglioma.
Diagnostic Algorithm for Glioma
www.jco.org © 2015 by American Society of Clinical Oncology 5
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

ATRX gene was predominantly found in astrocytomas of WHO grade2 or 3 and seemed to be strongly associated with mutations of TP53and IDH1.27 Moreover, loss of ATRX expression seemed mutuallyexclusive with 1p/19q codeletion, and in Cox regression analysis,ATRX and 1p/19q over-ruled histology. ATRX mutations and 1p/19qcodeletion separate the anaplastic mixed oligoastrocytomas into eitherAA or AO.27 In our study, the power of ATRX mutation might haveover-ruled the feature of astrocytic cell processes, but data on ATRXwere not available.
The molecular characteristics implicated in our analysis have allproven to be significant prognosticators.2,9,28 The results of testing theprognostic or predictive qualities of molecular parameters vary amongstudies. For instance, there are discrepant data on the prognosticeffects of MGMT in the literature.7-9,21,29-31 One reason may be thevariations in pathology diagnoses. Another reason may be a subopti-mal reproducibility of molecular test results. Continuous interlabora-
tory monitoring of assays is therefore a necessary instrument of qualitycontrol.32-36 MGMT promoter methylation was shown to predictsurvival of patients with glioblastomas treated with temozolomide,particularly in grade 3 tumors without IDH mutations.7 MGMTpromoter methylation is usually present in CpG island methylatedphenotype (CIMP) –positive tumors; CIMP positivity is frequent inIDH-mutated tumors. This explains why in grade 3 tumors, the prog-nostic significance was lost when analyzed together with IDH muta-tions; this was also the case in our analysis. IDH1 mutational status waspreviously found to be of prognostic significance in the EORTC 26951trial,21 and its effect seemed strong enough to be sustained in our Coxregression analysis. However, in the CTREE analysis, IDH1 status isoverruled by 1p/19q codeletion. Because mutation in TERT and dele-tion of CDKN2A/B have also been shown to affect survival,10,37 it islikely that integrating these parameters into the analysis would haveinfluenced the current algorithm.
BAODAODAOAAAAGBM
Perc
enta
ge
Time (years)
100
80
60
40
20
0 42 6 8 10 12 14 16
345
345
OD
AOD
AOA
A
AA
GBM
2
33
12
2
2
50
0
4
8
0
4
83
9
56
9
0
0
26
% Node 3 Node 4 Node 5
892925
607
38
463
33
362
28
290
24
260
18
907
200
1102944
edoNksir ta .oNnO
Overall Wald test: P < .001 (df = 2)
DC
Perc
enta
ge
Time (years)
100
80
60
40
20
0 42 6 8 10 12 14
345
345
44169
356
14
243
13
161
12
151
11
1218
513
571716
edoNksir ta .oNnO
Overall Wald test: P < .001 (df = 2)
YesNo
YesNo
Node 3 Node 4 Node 5
1p/19q lossP < .001
EGFR ampl.P < .001
Fig 2. (A) Results of conditional inference tree (CTREE) modeling of molecular features, yielding three diagnostic nodes (no, absent; yes, present). Pie diagrams showdistribution of consensus diagnoses for each node. Overall survival according to nodes resulting from CTREE analysis of molecular features for (B) discovery and (C)validation sets. (D) Actual percentages of consensus diagnoses. A, astrocytoma; AA, anaplastic astrocytoma; AOA, anaplastic oligoastrocytoma; AOD, anaplasticoligodendroglioma; GBM, glioblastoma multiforme; O, observed events; OD, oligodendroglioma.
Kros et al
6 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

A comparison of the power of our algorithm with that of otheralgorithms proposed in recent literature by using our data set is providedin the Data Supplement. The results are, however, not unequivocal, be-cause the algorithms differed in molecular parameters, and histologicparameters were not included in any of them. We substituted particularparameters and present the results using the modified schemes (DataSupplement). The number of low-grade tumors in our analysis was low.In addition, the molecular data were derived from the tumors included inEORTC trial 26951, in which more oligodendroglial tumors were presentthan in trial 26882, which contained predominantly tumors of astrocyticlineage (AA and GBM; Appendix Table A1, online only). Therefore, thealgorithm should be further validated in an external data set in whichgliomas of all lineages and grades are present. In addition, future studiesleveragingthebiomaterialsofnewertrialsarenecessarytoimplementnewmolecular parameters in similar analytic models, and the scrutinizing ofhistopathologic parameters needs to be repeated.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTSOF INTEREST
Disclosures provided by the authors are available with this article atwww.jco.org.
AUTHOR CONTRIBUTIONS
Conception and design: Johan M. KrosFinancial support: Johan M. KrosProvision of study materials or patients: Martin J. van den BentCollection and assembly of data: Karin Huizer, AurelioHernández-Laín, Gianluca Marucci, Alex Michotte, Bianca Pollo,Elisabeth J. Rushing, Teresa Ribalta, Pim French, David Jaminé, NawalBekka, Denis Lacombe, Martin J. van den BentData analysis and interpretation: Johan M. Kros, Thierry GorliaManuscript writing: All authorsFinal approval of manuscript: All authors
BAODAODAOAAAAGBM
Perc
enta
ge
Time (years)
100
80
60
40
20
0 42 6 8 10 12 14 16
4567
4567
OD
AOD
AOA
A
AA
GBM
5
90
0
0
0
5
0
0
18
3
3
76
10
62
0
0
0
28
% Node 4 Node 5
0
4
8
0
4
83
Node 6 Node 7
18682925
2238
738
1729
333
1323
228
1118
024
9170
18
3607
0200
27832944
edoNksir ta .oNnO
Overall Wald test: P < .001 (df = 3)
DC
Perc
enta
ge
Time (years)
100
80
60
40
20
0 42 6 8 10 12 14
4567
4567
1628169
19166
14
1683
13
1151
12
1051
11
8418
5013
24331716
edoNksir ta .oNnO
Overall Wald test: P < .001 (df = 3)
No Yes
YesNo
No Yes
Node 4 Node 5
Node 6
Node 7
1p/19q lossP < .001
EGFR ampl.P < .003
Astrocytic processesP < .033
Fig 3. (A) Results of conditional inference tree (CTREE) modeling of combined histologic and molecular features, yielding four diagnostic nodes (no, absent; yes,present). Pie diagrams show distribution of consensus diagnoses for each node. Overall survival according to nodes resulting from CTREE analysis of combinedhistologic and molecular features for (B) discovery and (C) validation sets. (D) Actual percentages of consensus diagnoses. A, astrocytoma; AA, anaplastic astrocytoma;AOA, anaplastic oligoastrocytoma; AOD, anaplastic oligodendroglioma; GBM, glioblastoma multiforme; O, observed events; OD, oligodendroglioma.
Diagnostic Algorithm for Glioma
www.jco.org © 2015 by American Society of Clinical Oncology 7
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.

REFERENCES
1. Weller M, Berger H, Hartmann C, et al: Com-bined 1p/19q loss in oligodendroglial tumors: Predic-tive or prognostic biomarker? Clin Cancer Res 13:6933-6937, 2007
2. Kouwenhoven MC, Gorlia T, Kros JM, et al: Mo-lecular analysis of anaplastic oligodendroglial tumors in aprospective randomized study: A report from EORTCstudy 26951. Neuro Oncol 11:737-746, 2009
3. Vogelbaum MA, Berkey B, Peereboom D, etal: Phase II trial of preirradiation and concurrenttemozolomide in patients with newly diagnosedanaplastic oligodendrogliomas and mixed anaplasticoligoastrocytomas: RTOG BR0131. Neuro Oncol 11:167-175, 2009
4. Cairncross G, Berkey B, Shaw E, et al: PhaseIII trial of chemotherapy plus radiotherapy comparedwith radiotherapy alone for pure and mixed anaplas-tic oligodendroglioma: Intergroup Radiation TherapyOncology Group Trial 9402. J Clin Oncol 24:2707-2714, 2006
5. Lecavalier-Barsoum M, Quon H, AbdulkarimB: Adjuvant treatment of anaplastic oligodendroglio-mas and oligoastrocytomas. Cochrane DatabaseSyst Rev 5:CD007104, 2014
6. Roth P, Wick W, Weller M: Anaplastic oligo-dendroglioma: A new treatment paradigm and cur-rent controversies. Curr Treat Options Oncol 14:505-513, 2013
7. Hegi ME, Diserens AC, Gorlia T, et al: MGMTgene silencing and benefit from temozolomide inglioblastoma. N Engl J Med 352:997-1003, 2005
8. van den Bent MJ, Dubbink HJ, Sanson M, etal: MGMT promoter methylation is prognostic butnot predictive for outcome to adjuvant PCV chemo-therapy in anaplastic oligodendroglial tumors: A re-port from EORTC Brain Tumor Group Study 26951.J Clin Oncol 27:5881-5886, 2009
9. van den Bent MJ, Erdem-Eraslan L, Idbaih A,et al: MGMT-STP27 methylation status as predictivemarker for response to PCV in anaplastic oligoden-drogliomas and oligoastrocytomas: A report fromEORTC study 26951. Clin Cancer Res 19:5513-5522, 2013
10. Labussière M, Di Stefano AL, Gleize V, et al:TERT promoter mutations in gliomas, genetic asso-ciations and clinico-pathological correlations. Br JCancer 111:2024-2032, 2014
11. Mellinghoff IK, Cloughesy TF, Mischel PS:PTEN-mediated resistance to epidermal growth fac-tor receptor kinase inhibitors. Clin Cancer Res 13:378-381, 2007
12. Mellinghoff IK, Wang MY, Vivanco I, et al:Molecular determinants of the response of glioblas-tomas to EGFR kinase inhibitors. N Engl J Med353:2012-2024, 2005
13. Brennan CW, Verhaak RG, McKenna A, et al:The somatic genomic landscape of glioblastoma.Cell 155:462-477, 2013
14. Louis DN, Perry A, Burger P, et al: InternationalSociety of Neuropathology–Haarlem consensus guide-lines for nervous system tumor classification and grad-ing. Brain Pathol 24:429-435, 2014
15. Coons SW, Pearl DK: Mitosis identification indiffuse gliomas: Implications for tumor grading. Can-cer 82:1550-1555, 1998
16. Coons SW, Johnson PC, Scheithauer BW, etal: Improving diagnostic accuracy and interobserverconcordance in the classification and grading ofprimary gliomas. Cancer 79:1381-1393, 1997
17. Kros JM, Gorlia T, Kouwenhoven MC, et al: Panelreview of anaplastic oligodendroglioma from EuropeanOrganisation For Research and Treatment of Cancer Trial26951: Assessment of consensus in diagnosis, influenceof 1p/19q loss, and correlations with outcome. J Neuro-pathol Exp Neurol 66:545-551, 2007
18. Giannini C, Scheithauer BW, Weaver AL, et al:Oligodendrogliomas: Reproducibility and prognosticvalue of histologic diagnosis and grading. J Neuro-pathol Exp Neurol 60:248-262, 2001
19. Hegi ME, Janzer RC, Lambiv WL, et al: Pres-ence of an oligodendroglioma-like component innewly diagnosed glioblastoma identifies a pathoge-netically heterogeneous subgroup and lacks prog-nostic value: Central pathology review of theEORTC_26981/NCIC_CE. 3 trial. Acta Neuropathol123:841-852, 2012
20. Hildebrand J, Gorlia T, Kros JM, et al: Adjuvantdibromodulcitol and BCNU chemotherapy in ana-plastic astrocytoma: Results of a randomised Euro-pean Organisation for Research and Treatment ofCancer phase III study (EORTC study 26882). Eur JCancer 44:1210-1216, 2008
21. van den Bent MJ, Brandes AA, Taphoorn MJ,et al: Adjuvant procarbazine, lomustine, and vincris-tine chemotherapy in newly diagnosed anaplasticoligodendroglioma: Long-term follow-up of EORTCbrain tumor group study 26951. J Clin Oncol 31:344-350, 2013
22. van den Bent MJ, Carpentier AF, Brandes AA,et al: Adjuvant procarbazine, lomustine, and vincristineimproves progression-free survival but not overall sur-vival in newly diagnosed anaplastic oligodendroglio-mas and oligoastrocytomas: A randomized EuropeanOrganisation for Research and Treatment of Cancerphase III trial. J Clin Oncol 24:2715-2722, 2006
23. Kleihues P, Louis D, Wiestler O, et al: WHOClassification of Tumours of the Central NervousSystem (ed 4). Lyon, France, International Agencyfor Research on Cancer, 2007
24. Gravendeel LA, Kloosterhof NK, Bralten LB, etal: Segregation of non-p.R132H mutations in IDH1 indistinct molecular subtypes of glioma. Hum Mutat31:E1186-E1199, 2010
25. Giannini C, Burger PC, Berkey BA, et al:Anaplastic oligodendroglial tumors: Refining the cor-relation among histopathology, 1p 19q deletion andclinical outcome in Intergroup Radiation TherapyOncology Group trial 9402. Brain Pathol 18:360-369,2008
26. Sahm F, Reuss D, Koelsche C, et al: Farewellto oligoastrocytoma: In situ molecular genetics favorclassification as either oligodendroglioma or astro-cytoma. Acta Neuropathol 128:551-559, 2014
27. Wiestler B, Capper D, Holland-Letz T, et al:ATRX loss refines the classification of anaplasticgliomas and identifies a subgroup of IDH mutantastrocytic tumors with better prognosis. Acta Neu-ropathol 126:443-451, 2013
28. Gravendeel LA, Kouwenhoven MC, GevaertO, et al: Intrinsic gene expression profiles of gliomasare a better predictor of survival than histology.Cancer Res 69:9065-9072, 2009
29. van den Bent MJ, Gravendeel LA, Gorlia T, etal: A hypermethylated phenotype is a better predic-tor of survival than MGMT methylation in anaplasticoligodendroglial brain tumors: A report from EORTCstudy 26951. Clin Cancer Res 17:7148-7155, 2011
30. Wick W, Meisner C, Hentschel B, et al: Prog-nostic or predictive value of MGMT promoter meth-ylation in gliomas depends on IDH1 mutation.Neurology 81:1515-1522, 2013
31. Wiestler B, Capper D, Sill M, et al: IntegratedDNA methylation and copy-number profiling identifythree clinically and biologically relevant groups ofanaplastic glioma. Acta Neuropathol 128:561-571,2014
32. van den Bent MJ, Hartmann C, Preusser M, etal: Interlaboratory comparison of IDH mutation de-tection. J Neurooncol 112:173-178, 2013
33. Berghoff AS, Stefanits H, Woehrer A, et al:Clinical neuropathology practice guide 3-2013: levelsof evidence and clinical utility of prognostic andpredictive candidate brain tumor biomarkers. ClinNeuropathol 32:148-158, 2013
34. Preusser M, Wöhrer A, Stary S, et al: Valueand limitations of immunohistochemistry and genesequencing for detection of the IDH1-R132H muta-tion in diffuse glioma biopsy specimens. J Neuro-pathol Exp Neurol 70:715-723, 2011
35. Woehrer A, Sander P, Haberler C, et al: FISH-based detection of 1p 19q codeletion in oligoden-droglial tumors: Procedures and protocols forneuropathological practice—A publication under theauspices of the Research Committee of the Euro-pean Confederation of Neuropathological Societies(Euro-CNS). Clin Neuropathol 30:47-55, 2011
36. Preusser M, Elezi L, Hainfellner JA: Reliabilityand reproducibility of PCR-based testing of O6-methylguanine-DNA methyltransferase gene (MGMT)promoter methylation status in formalin-fixed andparaffin-embedded neurosurgical biopsy specimens.Clin Neuropathol 27:388-390, 2008
37. Royds JA, Al Nadaf S, Wiles AK, et al: TheCDKN2A G500 allele is more frequent in GBMpatients with no defined telomere maintenancemechanism tumors and is associated with poorersurvival. PLoS One 6:e26737, 2011
■ ■ ■
Kros et al
8 © 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Evidence-Based Diagnostic Algorithm for Glioma: Analysis of the Results of Pathology Panel Review and Molecular Parameters of EORTC 26951and 26882 Trials
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships areself-held unless noted. I � Immediate Family Member, Inst � My Institution. Relationships may not relate to the subject matter of this manuscript. For moreinformation about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or jco.ascopubs.org/site/ifc.
Johan M. KrosNo relationship to disclose
Karin HuizerNo relationship to disclose
Aurelio Hernández-LaínNo relationship to disclose
Gianluca MarucciNo relationship to disclose
Alex MichotteNo relationship to disclose
Bianca PolloNo relationship to disclose
Elisabeth J. RushingNo relationship to disclose
Teresa RibaltaNo relationship to disclose
Pim FrenchConsulting or Advisory Role: Roche/GenentechResearch Funding: Abbvie
David JaminéNo relationship to disclose
Nawal BekkaNo relationship to disclose
Denis LacombeNo relationship to disclose
Martin J. van den BentConsulting or Advisory Role: Roche, Merck, Actelion, Novartis,NovocureSpeakers’ Bureau: Merck Sharp & DohmeResearch Funding: Roche, Abbvie
Thierry GorliaNo relationship to disclose
Diagnostic Algorithm for Glioma
www.jco.org © 2015 by American Society of Clinical Oncology
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
Acknowledgment
We thank the European Organisation for Research and Treatment of Cancer (EORTC) for its continuous support. This work is respectfullydedicated to Professor J. Hildebrand, who was the principle investigator of the EORTC 26882 trial.
Appendix
Table A1. Local Diagnosis Versus Panel Consensus Diagnosis
Local Diagnosis Total Cases
Consensus Diagnosis Consensus No Consensus
OD AOD AOA A AA GBM No. % No. %
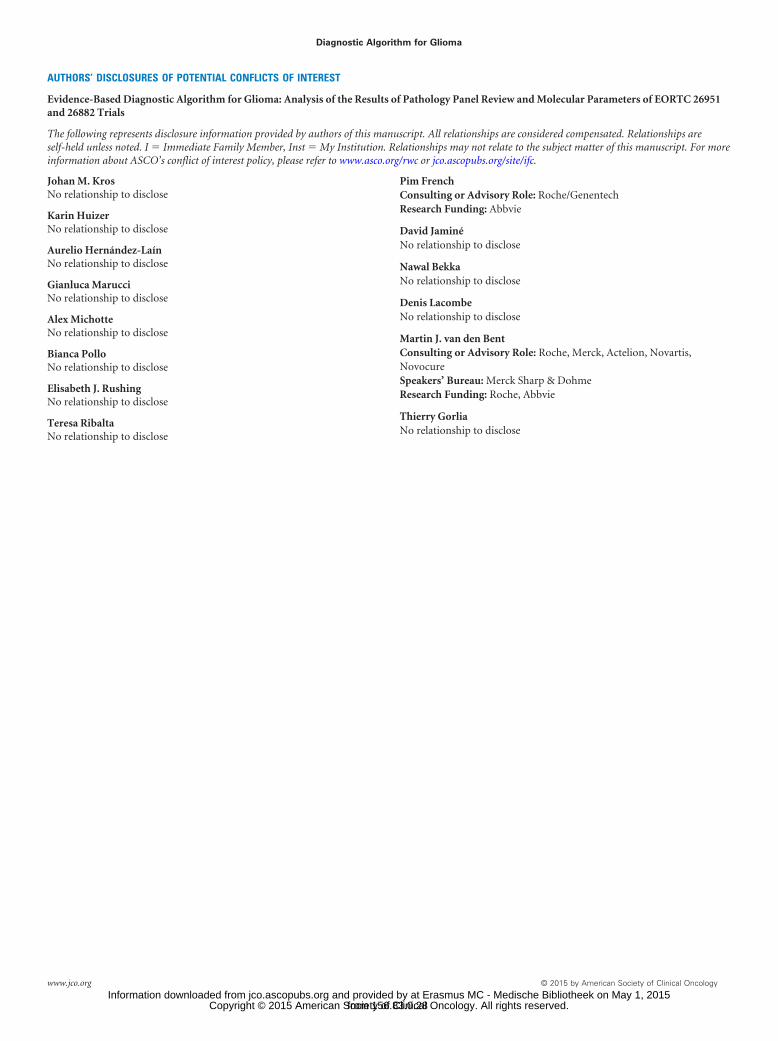
AOD 198 4 50 5 0 0 57 116 59 81 41AOA 78 0 5 5 4 4 28 46 59 32 41AA 164 0 0 4 14 19 43 80 49 84 51GBM 186 0 1 0 2 1 164 168 90 18 10Other 9 0 0 0 0 0 8 8 89 1 11Missing 1 0 0 0 0 0 1 1 100 0 0Total 636 4 56 14 20 25 301 420 66 216 34Trial 26882 363 0 1 5 16 21 216 259 71 104 29Trial 26951 273 4 55 9 4 4 85 161 59 112 41
NOTE. Local diagnosis of GBM was consensus confirmed in 164 (88%) of 186 cases. Local diagnoses of AOD, AA, and AOA were confirmed by panel consensusin only 50 (25%) of 198, 19 (12%) of 164, and five (6%) of 78 cases, respectively. Overall, panel reached consensus (ie, agreement among four of six reviewers)in 420 (66%) of 636 cases. There was greater consensus in cases of trial 26882 versus trial 26951 (71% v 59%). Distribution of overall consensus diagnoses differedfor two trials; in trial 26882, most tumors were diagnosed as glioblastoma, whereas in trial 26951, more tumors were diagnosed as neoplasms with oligodendroglialtraits (OD, AOD, or AOA).Abbreviations: A, astrocytoma; AA, anaplastic astrocytoma; AOA, anaplastic oligoastrocytoma; AOD, anaplastic oligodendroglioma; GBM, glioblastoma multiforme;
OD, oligodendroglioma.
Table A2. ICC and OS for Histologic Features
Histologic Feature ICC OS P
Spearman Correlation Coefficient (r)
MucoidDegeneration Calcification
MiniatureGemistocytes Gemistocytes
AstrocyticCell
Processes
AbnormalVessel
Structure Necrosis1p/19qLoss
EGFRAmplification
Perinuclear halos 0.863 � .001 0.41 0.37 �0.43 �0.51Microcysts 0.673 � .001 0.5Mucoid degeneration 0.719 � .001Calcification 0.91 � .001Miniature gemistocytes 0.57 � .001Gemistocytes 0.757 � .001Polar spongioblastoma-like foci 0.398 .167Protoplasmic astrocytes 0.444 �
Astrocytic cell processes 0.735 � .001 �0.39 �0.35 0.30Nuclear pleomorphism (low,
medium, or high)† 0.775 � .001Cell density 0.847 .531Mitotic index† 0.918 � .001Microvascular proliferation†
Increased No. of vessels 0.778 .216 0.74Abnormal vessel structure 0.85 � .001 0.51
Necrosis† 0.949 � .001Infarction 0.719 � .001Sarcomatous parts 0.73 � .001Giant cells 0.952 � .001 0.38PNET-like foci 0.648 .230
Abbreviations: ICC, Intraclass correlation; OS, overall survival; PNET, peripheral neuroectodermal tumor.�Protoplasmic astrocytes feature was scored absent by all reviewers in all cases.†Included in current grading according to WHO.
Kros et al
© 2015 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.
Perc
enta
ge
Time (years)
100
80
60
40
20
0 42 6 8 10 12 14 16
ODAGBMAODAAAOANo consensus
112
288411910
163
4134244168
134
411243678
97
310182666
74
37
142334
51
33
111734
38
214923
14
0120001
420
301562514
216
O n No. at riskConsensus Diagnosis
Overall Wald test: P < .001 (df = 3)
ODAGBMAODAAAOANo consensus
Fig A1. Overall survival for consensus diagnoses of all cases (trials 26882 and 26951). A, astrocytoma; AA, anaplastic astrocytoma; AOA, anaplastic oligoastrocytoma;AOD, anaplastic oligodendroglioma; GBM, glioblastoma multiforme; O, observed events; OD, oligodendroglioma.
Diagnostic Algorithm for Glioma
www.jco.org © 2015 by American Society of Clinical Oncology
from 156.83.0.28Information downloaded from jco.ascopubs.org and provided by at Erasmus MC - Medische Bibliotheek on May 1, 2015
Copyright © 2015 American Society of Clinical Oncology. All rights reserved.