
Primary cutaneous B-cell lymphomas – Clinicopathological, prognostic and therapeutic...
10
ORIGINAL ARTICLE: CLINICAL Primary cutaneous B-cell lymphomas – Clinicopathological, prognostic and therapeutic characterisation of 54 cases according to the WHO-EORTC classification and the ISCL/EORTC TNM classification system for primary cutaneous lymphomas other than mycosis fungoides and Se ´ zary syndrome PHILIPPA GOLLING, ANTONIO COZZIO, REINHARD DUMMER, LARS FRENCH, & WERNER KEMPF Department of Dermatology, Cutaneous Lymphoma Study Group, University Hospital, CH-8091 Zu ¨ rich, Switzerland (Received 5 December 2007; revised 6 March 2008; accepted 18 March 2008) Abstract Clinical, prognostic and therapeutic features of 54 primary cutaneous marginal zone B-cell lymphoma (pcMZL), follicle centre lymphoma (pcFCL) and diffuse large B-cell lymphoma, leg type (pcDLBL) were analysed applying the WHO- EORTC classification for cutaneous lymphomas and the new TNM staging scheme of the International Society of Cutaneous Lymphomas. Solitary (T1) or regionally clustered (T2) tumors were observed in pcMZL and pcFCL. Disseminated tumors (T3 stage) were found in 26% of patients with pcMZL and in one patient with pcDLBL. A complete remission was achieved in 41% of the patients. Three of 7 patients (43%) with pcDLBL died due to lymphoma. The new TNM staging system is easily applicable for disease documentation, but our relatively small number of patients in each T stage does not allow the assessment of its prognostic value. Surgical excision or radiotherapy is highly effective in pcMZL and pcFCL. Keywords: Cutaneous, lymphoma, B cell, staging, therapy Introduction In recent years, the terminology and classification of primary cutaneous B-cell lymphomas (CBCL) has undergone crucial changes. Major differences in previous classifications such as WHO classifica- tion [1] and EORTC classification for primary cutaneous lymphomas [2] resulted in divergent data on clinicopathological presentation as well as prognostic and therapeutic aspects of CBCL. In the new WHO-EORTC classification for cutaneous lymphomas introduced in 2005 [3,4], classifi- cation of CBCL was redefined and includes three main entities: primary cutaneous marginal zone B-cell lymphoma (pcMZL), primary cutaneous follicle centre lymphoma (pcFCL) and primary cutaneous diffuse large B-cell lymphoma, leg type (pcDLBL). Previous TNM staging systems did not sufficiently reflect the biology and tumor burden of CBCL. Thus a new TNM staging system has recently been proposed for cutaneous lymphomas other than mycosis fungoides (MF) and Se ´zary syndrome (SS) [5]. This scheme has been elaborated by the ISCL and EORTC Task Force Group for cutaneous lymphomas and creates a T system accepted by experts for cutaneous lymphomas world-wide. It remains to be determined whether this T classi- fication has any prognostic or therapeutic implications [6]. Although the clinical, histological and immuno- phenotypic features of CBCL have become more Correspondence: Werner Kempf, Department of Dermatology, University Hospital Zu ¨ rich, CH-8091 Zu ¨ rich, Switzerland. Tel: þ41-44-255-25-50. Fax: þ41-44-255-44-03. E-mail: [email protected]. Leukemia & Lymphoma, June 2008; 49(6): 1094 – 1103 ISSN 1042-8194 print/ISSN 1029-2403 online Ó 2008 Informa UK Ltd. DOI: 10.1080/10428190802064925 Leuk Lymphoma Downloaded from informahealthcare.com by Universitaet Zuerich on 05/16/14 For personal use only.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Primary cutaneous B-cell lymphomas – Clinicopathological, prognostic and therapeutic...

ORIGINAL ARTICLE: CLINICAL
Primary cutaneous B-cell lymphomas – Clinicopathological, prognosticand therapeutic characterisation of 54 cases according to theWHO-EORTC classification and the ISCL/EORTC TNM classificationsystem for primary cutaneous lymphomas other than mycosisfungoides and Sezary syndrome
PHILIPPA GOLLING, ANTONIO COZZIO, REINHARD DUMMER, LARS FRENCH, &
WERNER KEMPF
Department of Dermatology, Cutaneous Lymphoma Study Group, University Hospital, CH-8091 Zurich, Switzerland
(Received 5 December 2007; revised 6 March 2008; accepted 18 March 2008)
AbstractClinical, prognostic and therapeutic features of 54 primary cutaneous marginal zone B-cell lymphoma (pcMZL), folliclecentre lymphoma (pcFCL) and diffuse large B-cell lymphoma, leg type (pcDLBL) were analysed applying the WHO-EORTC classification for cutaneous lymphomas and the new TNM staging scheme of the International Society ofCutaneous Lymphomas. Solitary (T1) or regionally clustered (T2) tumors were observed in pcMZL and pcFCL.Disseminated tumors (T3 stage) were found in 26% of patients with pcMZL and in one patient with pcDLBL. A completeremission was achieved in 41% of the patients. Three of 7 patients (43%) with pcDLBL died due to lymphoma. The newTNM staging system is easily applicable for disease documentation, but our relatively small number of patients in each Tstage does not allow the assessment of its prognostic value. Surgical excision or radiotherapy is highly effective in pcMZL andpcFCL.
Keywords: Cutaneous, lymphoma, B cell, staging, therapy
Introduction
In recent years, the terminology and classification
of primary cutaneous B-cell lymphomas (CBCL)
has undergone crucial changes. Major differences
in previous classifications such as WHO classifica-
tion [1] and EORTC classification for primary
cutaneous lymphomas [2] resulted in divergent
data on clinicopathological presentation as well as
prognostic and therapeutic aspects of CBCL. In
the new WHO-EORTC classification for cutaneous
lymphomas introduced in 2005 [3,4], classifi-
cation of CBCL was redefined and includes three
main entities: primary cutaneous marginal zone
B-cell lymphoma (pcMZL), primary cutaneous
follicle centre lymphoma (pcFCL) and primary
cutaneous diffuse large B-cell lymphoma, leg type
(pcDLBL).
Previous TNM staging systems did not sufficiently
reflect the biology and tumor burden of CBCL. Thus
a new TNM staging system has recently been
proposed for cutaneous lymphomas other than
mycosis fungoides (MF) and Sezary syndrome (SS)
[5]. This scheme has been elaborated by the ISCL
and EORTC Task Force Group for cutaneous
lymphomas and creates a T system accepted by
experts for cutaneous lymphomas world-wide. It
remains to be determined whether this T classi-
fication has any prognostic or therapeutic
implications [6].
Although the clinical, histological and immuno-
phenotypic features of CBCL have become more
Correspondence: Werner Kempf, Department of Dermatology, University Hospital Zurich, CH-8091 Zurich, Switzerland. Tel: þ41-44-255-25-50.
Fax: þ41-44-255-44-03. E-mail: [email protected].
Leukemia & Lymphoma, June 2008; 49(6): 1094 – 1103
ISSN 1042-8194 print/ISSN 1029-2403 online � 2008 Informa UK Ltd.
DOI: 10.1080/10428190802064925
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.
clearly characterised [7–11], staging and therapy of
CBCL are not yet standardised. This is in part due to
a lack of a widely accepted staging system for
CBCL and definition criteria for CBCL entities.
Furthermore, various new treatment modalities such
as monoclonal antibodies against CD20 (e.g. ritux-
imab) or intralesional gene transfer using adenovirus
[11,12] have been introduced. Data on the disease
extent and prognosis based on ISCL-EORTC TNM
staging system in CBCL are very limited [6].
Thus the aims of our study on 54 CBCL cases
were: (i) to characterise the clinical features of the
three main CBCL forms according to the recent
WHO-EORTC classification, (ii) to assess the value
of the new TNM staging system for staging, (iii) to
assess prognosis of the three subtypes of CBCL
with respect to the tumor stage and (iv) the response
to the various treatment modalities employed in
CBCL.
A description of the new TNM classification [5] is
given in Table I.
Materials and methods
In the files of our institute 212 patients with B-cell
lymphoproliferative diseases were identified between
1991 and 2006. A total of 136 cases were excluded
from further analysis, due to a lack of data on clinical
presentation or results of the staging examinations or
follow-up or lack of immunohistochemical or geno-
typic data, which did not allow appropriate classifica-
tion. Five CBCL cases belonged to CBCL entities
other than the three main forms (pcMZL, pcFCL,
pcDLBL) and 17 cases represented secondary
cutaneous involvement of primary nodal or extra-
nodal and extracutaneous B-cell lymphomas. The
remaining 54 cases were classified according to the
WHO-EORTC classification for cutaneous lympho-
mas (Table II). All patients had undergone complete
staging including chest X-ray, ultrasound examina-
tion of lymph nodes and abdomen as well as bone
marrow biopsy as suggested by the ISCL-EORTC
Cutaneous Lymphoma Task Force [5]. In none of
the 54 CBCL patients included in the study could
extracutaneous lymphoma infiltrate be identified at
the time of diagnosis or completion of staging
procedures. Histological review was performed on
HE stained sections and immunohistochemical
stainings including B-cell markers (CD20, CD79a),
bcl-2, bcl-6, MUM-1 (in DLBCL), immunoglobulin
light chains kappa and lambda and CD21 (to identify
networks of follicular dendritic cells indicating
germinal centre formation). Positivity for bcl-2, bcl-
6 and MUM-1 was defined by expression of those
markers by at least 50% of the tumor cells.
The following parameters were evaluated: Age at
diagnosis, sex, localisation, number and extent of
lesions at time of diagnosis according to the new
TNM staging scheme [5], diagnosis according to
WHO-EORTC classification for cutaneous lympho-
mas [3,4], length of follow-up (in months), interval
to first relapse, treatment modality (e.g. surgical
excision, radiotherapy, excision and radiotherapy,
antibiotics, chemotherapy) and response to treatment
of primary lesions (complete remission [CR], partial
remission [PR], stable disease, progressive disease),
response to as well as treatment modalities for
relapses, and outcome (alive with no disease, alive
with disease lymphoma, death due to disease
lymphoma, death due to other causes).
Statistical analysis was performed using SPSS
version 15.0. (SPSS Chicago II).
Results
A total of 54 CBCL patients were identified and
classified according to the WHO-EORTC classifica-
tion for cutaneous lymphomas as pcMZL (n¼ 31;
Table I. ISCL/EORTC proposal on T classification of cutaneous
lymphoma other than mycosis fungoides and Sezary syndrome.
Solitary T1 Small T1a 1 solitary lesion
�5 cm diameter
Large T1b 1 solitary lesion
45 cm diameter
Multiple T2 Small T2a All encompassing in
�15 cm diameter
Medium T2b All enc. in 415 cm
and �30 cm diameter
Large T2c All encompassing in
430 cm diameter
Generalized T3 T3a 2 non-contiguous
body regions
T3b �3 body regions
Table II. Epidemiological data of our series of CBCL patients.
No. of
patients (%)
Median age at
diagnosis
a) CBCL subgroup
pcMZL 31 (57%) 39 years
pcFCL 16 (30%) 59 years
pcDLBL 7 (13%) 78 years
Total 54 (100%) –
b) Sex distribution
Male 31 (57%)
Female 23 (43%)
Total 54 (100%)
CBCL staging and therapy 1095
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.

57%), pcFCL (n¼ 16; 30%) and pcDLBL (n¼ 7;
13%) (Table II). There were slightly more males
(57%) than females (Table II).
Clinical features and staging
pcMZL
The median age of patients at diagnosis was 39
years (range from 18 to 77 years) (Table II). In 12
of 31 patients (39%), the disease at onset featured
a solitary lesion (corresponding to T1) and in 11 of
31 patients (35%) multiple, but regional tumors
(corresponding to T2). In the remaining 8 patients
(26%), multiple disseminated lesions (correspond-
ing to T3) were present at diagnosis (Table III).
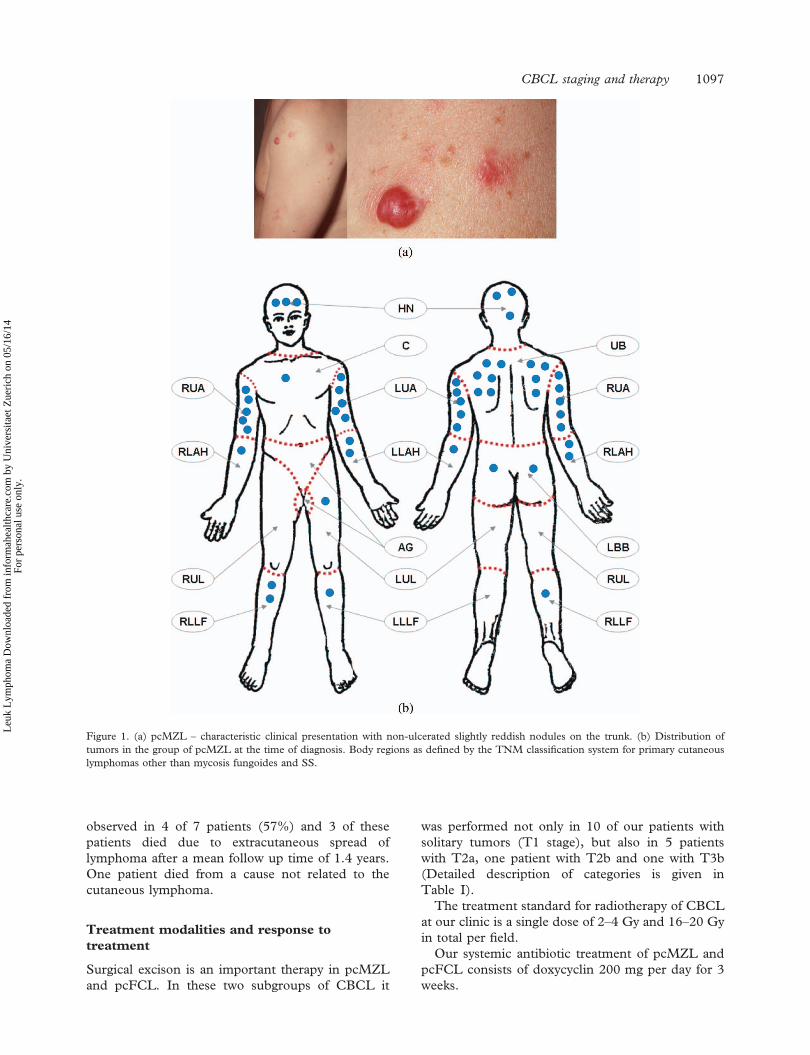
The predilection sites for pcMZL at diagnosis were
the upper back and upper arms, whereas head and
neck were the second most common site of tumor
localisation [Figure 1(b)]. In only a few cases were
tumors located on the lower legs and buttocks and
this was observed only in patients with dissemi-
nated tumors. Clinically MZL started with skin-
coloured or erythematous nodules [Figure 1(a)].
Ulceration was not observed.
pcFCL
The median age at diagnosis was 59 years (range
from 44 to 80 years). In 7 of 16 patients (44%), the
disease started with a solitary lesion (T1) and in 9 of
16 patients (56%) with multiple, but regional tumors
(T2). None of the patients showed multiple dis-
seminated lesions at diagnosis (Table III). The
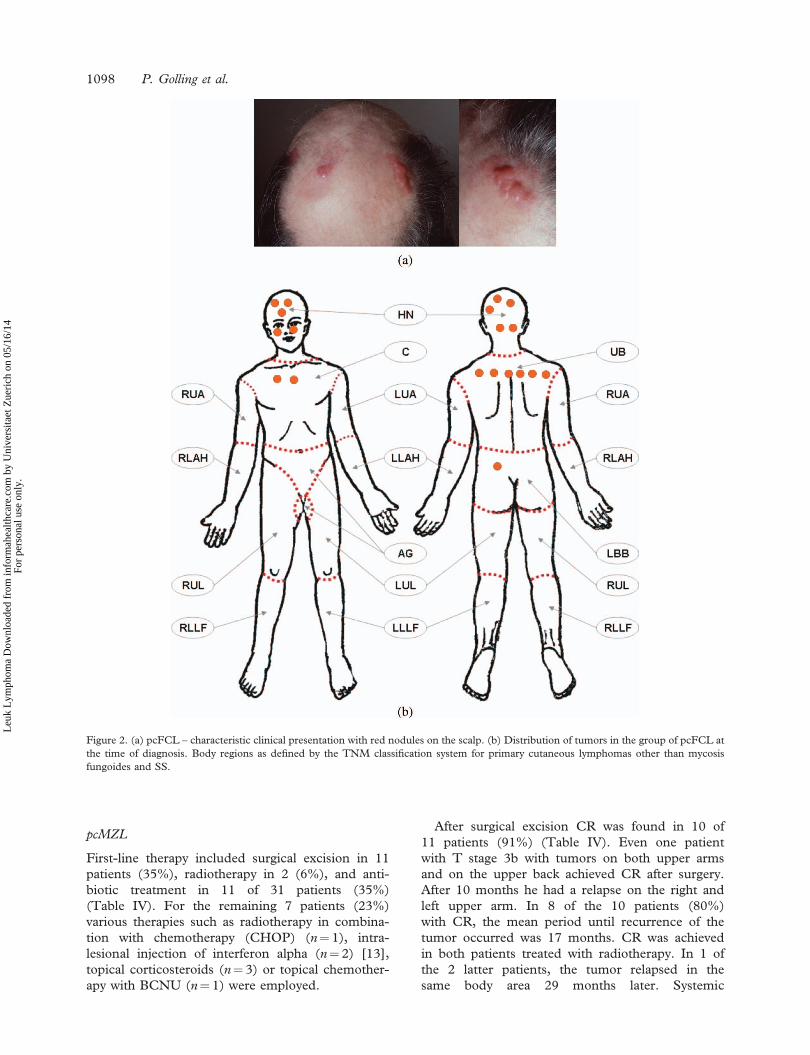
predilection sites were the head and neck region
and the upper back [Figure 2(b)]. Tumors were not
found on the extremities in any of the patients.
Clinically FCL began with and stayed as erythema-
tous nodules and surrounding plaques [Figure 2(a)].
Ulceration was not observed.
pcDLBL
The median age at diagnosis was 78 years (range
from 52 to 98 years). The disease became apparent
due to a solitary lesion (T1) in 3 of 7 patients (43%)
and with multiple, but regional tumors (T2) in the
remaining 4 patients (57%). One patient showed
multiple disseminated lesions at diagnosis (Table
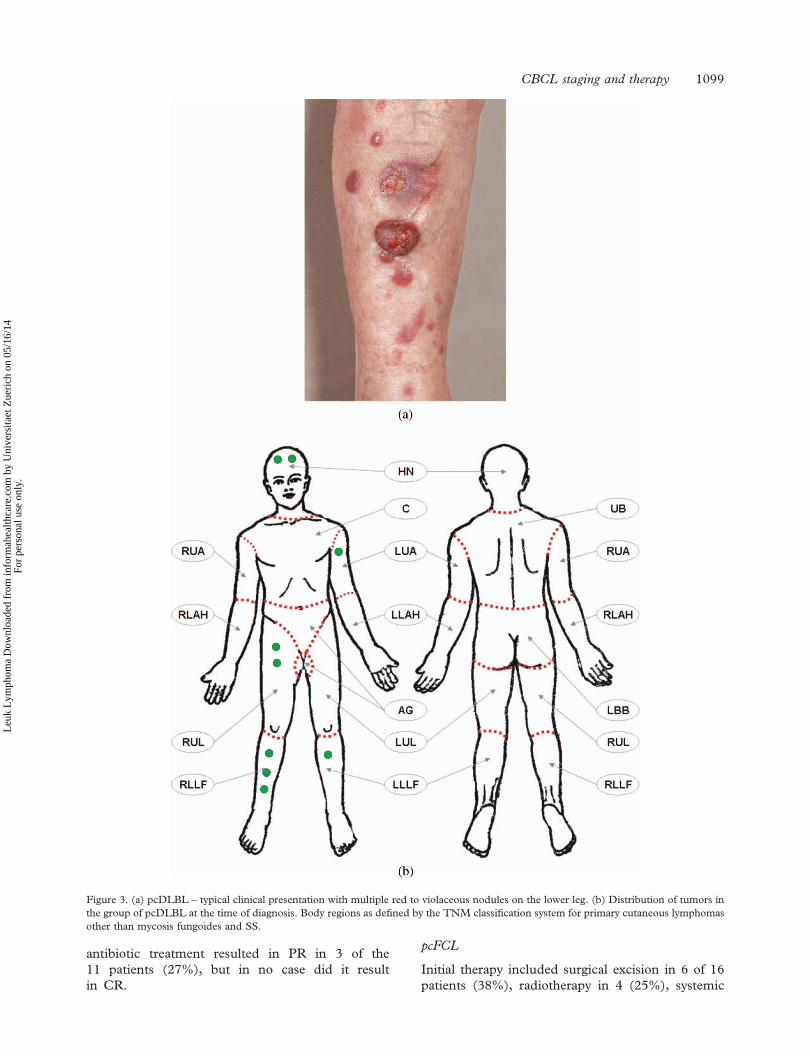
III). The predilection sites were the legs, but tumors
were also found on the head and neck and on the
upper arm in 1 of the 7 patients [Figure 3(b)].
Clinically DLBL started with erythematous to
violaceous nodules [Figure 3(a)]. Ulceration was
not uncommon in this CBCL subset.
Borrelia status and CBCL
Thirty-nine of the 54 patients (72%) were examined
for Borrelia infection. In 6 of 39 cases serological tests
were performed and were negative. In the remaining
33 cases DNA extracted from archival tissue was
examined by nested PCR. Borrelia DNA could be
detected in 4 of the 33 cases (12%).
Course and prognosis
pcMZL
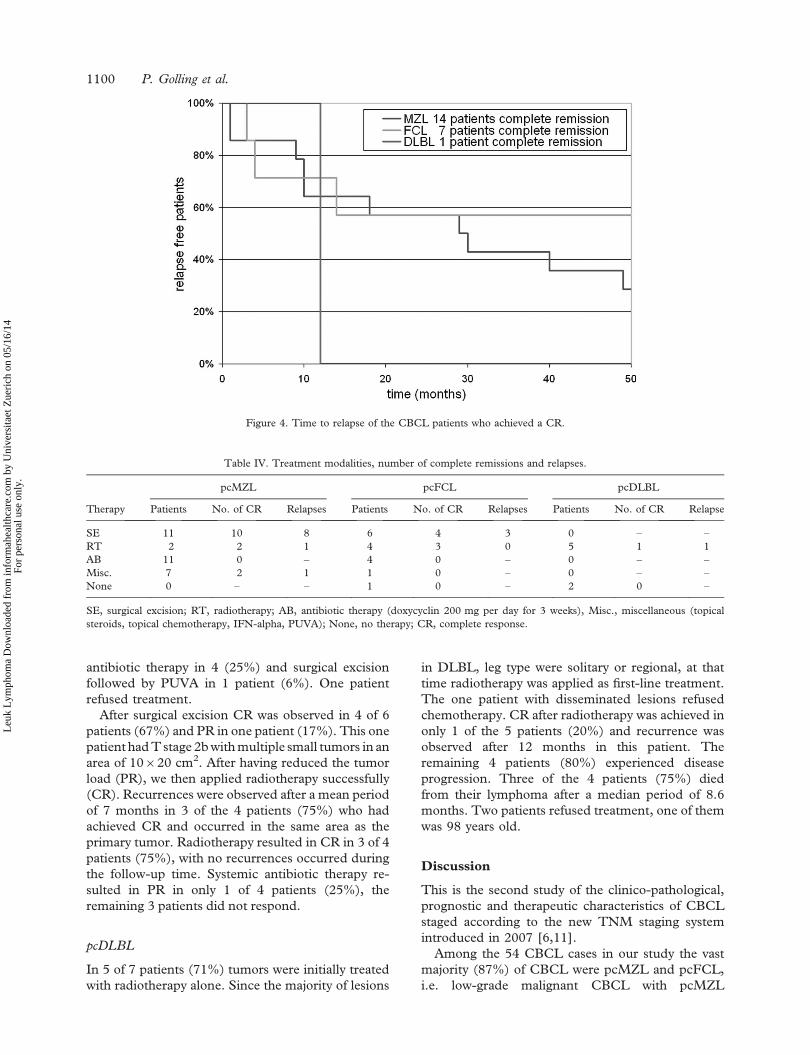
CR was achieved in 14 of 31 patients (45%).
Recurrences were observed in 10 of these 14 patients
with CR (71%). In 9 of 10 patients (90%) relapses
occurred in the same body area where the primary
tumor was localised. Extracutaneous spread was not
observed in any of the patients. The average time
until recurrences occurred in pcMZL was 20
months. The detailed timecurve is shown in Figure 4.
None of the patients died due to lymphoma after a
mean follow up time of 5.4 years.
pcFCL
CR was achieved in 7 of 16 patients (44%).
Recurrences were observed in 3 of these 7 patients
with CR (43%) after an average period of 7 months.
All recurrences were observed in the same body area
as the primary tumor. Extracutaneous spread was not
observed in any of the patients during a mean follow
up time of 5.3 years. One patient died due to an
unrelated cause.
pcDLBL
CR was achieved in 1 of 7 patients (14%). The time
to this one relapse was 12 months, and it occurred in
a non-contiguous field. Progressive disease was
Table III. T stage of our CBCL patients at the time of diagnosis.
T stage
All CBCL
No. of
patients
pcMZL
No. of
patients
pcFCL
No. of
patients
pcDLBL
No. of
patients
T1 a 21 (39%) 12 6 3
b 1 (2%) – 1 –
T2 a 13 (24%) 7 6 –
b 9 (17%) 4 3 2
c 1 (2%) – – 1
T3 a 3 (6%) 2 – 1
b 6 (11%) 6 – –
Total 54 (100%) 31 16 7
1096 P. Golling et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.
observed in 4 of 7 patients (57%) and 3 of these
patients died due to extracutaneous spread of
lymphoma after a mean follow up time of 1.4 years.
One patient died from a cause not related to the
cutaneous lymphoma.
Treatment modalities and response to
treatment
Surgical excison is an important therapy in pcMZL
and pcFCL. In these two subgroups of CBCL it
was performed not only in 10 of our patients with
solitary tumors (T1 stage), but also in 5 patients
with T2a, one patient with T2b and one with T3b
(Detailed description of categories is given in
Table I).
The treatment standard for radiotherapy of CBCL
at our clinic is a single dose of 2–4 Gy and 16–20 Gy
in total per field.
Our systemic antibiotic treatment of pcMZL and
pcFCL consists of doxycyclin 200 mg per day for 3
weeks.
Figure 1. (a) pcMZL – characteristic clinical presentation with non-ulcerated slightly reddish nodules on the trunk. (b) Distribution of
tumors in the group of pcMZL at the time of diagnosis. Body regions as defined by the TNM classification system for primary cutaneous
lymphomas other than mycosis fungoides and SS.
CBCL staging and therapy 1097
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.
pcMZL
First-line therapy included surgical excision in 11
patients (35%), radiotherapy in 2 (6%), and anti-
biotic treatment in 11 of 31 patients (35%)
(Table IV). For the remaining 7 patients (23%)
various therapies such as radiotherapy in combina-
tion with chemotherapy (CHOP) (n¼ 1), intra-
lesional injection of interferon alpha (n¼ 2) [13],
topical corticosteroids (n¼ 3) or topical chemother-
apy with BCNU (n¼ 1) were employed.
After surgical excision CR was found in 10 of
11 patients (91%) (Table IV). Even one patient
with T stage 3b with tumors on both upper arms
and on the upper back achieved CR after surgery.
After 10 months he had a relapse on the right and
left upper arm. In 8 of the 10 patients (80%)
with CR, the mean period until recurrence of the
tumor occurred was 17 months. CR was achieved
in both patients treated with radiotherapy. In 1 of
the 2 latter patients, the tumor relapsed in the
same body area 29 months later. Systemic
Figure 2. (a) pcFCL – characteristic clinical presentation with red nodules on the scalp. (b) Distribution of tumors in the group of pcFCL at
the time of diagnosis. Body regions as defined by the TNM classification system for primary cutaneous lymphomas other than mycosis
fungoides and SS.
1098 P. Golling et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.
antibiotic treatment resulted in PR in 3 of the
11 patients (27%), but in no case did it result
in CR.
pcFCL
Initial therapy included surgical excision in 6 of 16
patients (38%), radiotherapy in 4 (25%), systemic
Figure 3. (a) pcDLBL – typical clinical presentation with multiple red to violaceous nodules on the lower leg. (b) Distribution of tumors in
the group of pcDLBL at the time of diagnosis. Body regions as defined by the TNM classification system for primary cutaneous lymphomas
other than mycosis fungoides and SS.
CBCL staging and therapy 1099
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.
antibiotic therapy in 4 (25%) and surgical excision
followed by PUVA in 1 patient (6%). One patient
refused treatment.
After surgical excision CR was observed in 4 of 6
patients (67%) and PR in one patient (17%). This one
patient had T stage 2b with multiple small tumors in an
area of 10620 cm2. After having reduced the tumor
load (PR), we then applied radiotherapy successfully
(CR). Recurrences were observed after a mean period
of 7 months in 3 of the 4 patients (75%) who had
achieved CR and occurred in the same area as the
primary tumor. Radiotherapy resulted in CR in 3 of 4
patients (75%), with no recurrences occurred during
the follow-up time. Systemic antibiotic therapy re-
sulted in PR in only 1 of 4 patients (25%), the
remaining 3 patients did not respond.
pcDLBL
In 5 of 7 patients (71%) tumors were initially treated
with radiotherapy alone. Since the majority of lesions
in DLBL, leg type were solitary or regional, at that
time radiotherapy was applied as first-line treatment.
The one patient with disseminated lesions refused
chemotherapy. CR after radiotherapy was achieved in
only 1 of the 5 patients (20%) and recurrence was
observed after 12 months in this patient. The
remaining 4 patients (80%) experienced disease
progression. Three of the 4 patients (75%) died
from their lymphoma after a median period of 8.6
months. Two patients refused treatment, one of them
was 98 years old.
Discussion
This is the second study of the clinico-pathological,
prognostic and therapeutic characteristics of CBCL
staged according to the new TNM staging system
introduced in 2007 [6,11].
Among the 54 CBCL cases in our study the vast
majority (87%) of CBCL were pcMZL and pcFCL,
i.e. low-grade malignant CBCL with pcMZL
Table IV. Treatment modalities, number of complete remissions and relapses.
Therapy
pcMZL pcFCL pcDLBL
Patients No. of CR Relapses Patients No. of CR Relapses Patients No. of CR Relapse
SE 11 10 8 6 4 3 0 – –
RT 2 2 1 4 3 0 5 1 1
AB 11 0 – 4 0 – 0 – –
Misc. 7 2 1 1 0 – 0 – –
None 0 – – 1 0 – 2 0 –
SE, surgical excision; RT, radiotherapy; AB, antibiotic therapy (doxycyclin 200 mg per day for 3 weeks), Misc., miscellaneous (topical
steroids, topical chemotherapy, IFN-alpha, PUVA); None, no therapy; CR, complete response.
Figure 4. Time to relapse of the CBCL patients who achieved a CR.
1100 P. Golling et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.

accounting for more than half of all the cases. This
percentage is slightly higher than that reported in
other series and may reflect geographical differences
[11,14]. In addition, the introduction of the new
WHO-EORTC classification for CL has led to
reclassification of many cases and subsequent
changes in epidemiologic aspects [11].
The average age at diagnosis in our groups of
pcFCL and pcDLBL was similar to that found in
other reports, being 59 years for pcFCL and 78 years
for pcDLBL [9,11,14]. But our 31 patients with
pcMZL were on average much younger at diagnosis
(39 years) than reported before, e.g. median age at
diagnosis for pcMZL 53 years [6] and 50 years [9].
All three CBCL entities showed differences in their
predilection sites [Figures 1(b), 2(b), 3(b)].
PcMZL – in contrast to pcFCL – often presented
on arms and legs. Clinically, all CBCL entities
manifested with skin-coloured to erythematous or
violaceous nodules. Additionally, in pcFCL sur-
rounding plaques and in pcDLBL ulceration were
often observed.
According to the new TNM classification system
for cutaneous lymphomas other than MF and SS [5],
in all three CBCL entities a comparable number of
cases became apparent as a solitary tumor (T1 stage)
or multiple lesions limited to one body region or two
contiguous body regions (i.e. regional skin involve-
ment; T2 stage). Generalised skin involvement
with multiple lesions involving two non-contiguous
or 4 3 body regions (T3) occurred in our series in 8
of 31 pcMZL cases, and in one of the 7 pcDLBL
cases (9 of 54 (17%)) but was not associated with
impaired prognosis.
Due to the relatively small number of cases in
each T stage the data do not allow us to draw
conclusions on the relevance of the T stages for
recurrence rate (Table V). Nevertheless, it is useful
for precise anatomic documentation of disease
extent [5].
In our study an association between CBCL and
Borrelia could be detected by PCR from archival
tissue specimens in 12% of our patients. The per-
centage is lower than reported in the literature which
may be due to geographical differences [9,15].
Various treatment modalities were employed in
our series of patients; surgical excision, radiotherapy
and systemic antibiotics being the most common
first-line therapies. In pcMZL and pcFCL, surgical
excision or radiotherapy resulted in CR in 11 of 13
(85%) and in 7 of 10 (70%) of our patients
respectively. The response rates after surgical exci-
sion and radiotherapy are comparable to the data in
the literature. In contrast to these therapeutic
modalities, no response was achieved by antibiotic
treatment resulting in lower overall response rates
after initial therapy.
Recurrence of the tumor was observed after a
mean period of 14 months after initial treatment in
10 of 14 CR of pcMZL (71%) and 3 of 7 CR of
pcFCL (43%). The recurrence rates were similar to
previous studies reported in literature [7,9,10,16,17].
In our series of pcMZL and pcFCL, all recurrences
but one occurred in the same area as the primary
tumor. The number of patients is too small to assess
whether relapses were more common in T2 or T3
stages as compared to T1. In our series occurrence of
relapses did not affect prognosis in any of the CBCL
cases.
Radiotherapy resulted in CR in 3 of 4 pcFCL
with no recurrences during the follow-up. The
beneficial effect of radiotherapy in pcFCL is in
accordance with the results reported by Rijlaarsdam
et al. [18]. It can be speculated that the higher
recurrence rates observed after surgical excision
may in part be due to the fact that the excised area
is smaller than the therapy field in radiotherapy.
Wider and standardised excision margins could be
considered in CBCL in the aim of reducing
recurrence rates, but to date there is no evidence
in other types of lymphoma to strongly support such
a procedure.
Systemic antibiotic treatment did not induce CR
in any of our patients.
Extracutaneous spread and death due to lym-
phoma is very rare in pcMZL and pcFCL and has
been previously reported in 4% to 23% of pcMZL
[8,9,15,19] and in 5.3% of pcFCL [3,11]. In our
series none of our 47 patients with low-grade
malignant CBCL died due to lymphoma after a
Table V. T stages of our CBCL, number of complete remissions and relapse ratio.
pcMZL pcFCL pcDLBL
Patient CR Relapses Without relapse Patient CR Relapses Without relapse Patient CR Relapses Without relapse
T1 12 8 6 2 (25%)* 7 4 2 2 (50%) 3 1 1 0
T2 11 4 2 2 (50%) 9 3 1 2 (67%) 3 0 – –
T3 8 2 2 0 0 – – – 1 0 – –
*Percentage represents the number of patients without a relapse at the end of follow-up with respect to the number of CRs.
CBCL staging and therapy 1101
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.

median follow-up period of 5.2 years. In contrast,
3 of 7 patients (43%) with pcDLBL showed
extracutaneous spread and died due to lymphoma.
This finding is in accordance with the data in the
literature reporting 5-year overall survival rates of
37% to 67% in pcDLBL [11,20–23].
Conclusion
In the vast majority of patients, the CBCL showed up
with solitary or clustered nodules. PcMZL – in
contrast to pcFCL – often present on arms and legs.
Multiple disseminated lesions were found in
26% of patients with pcMZL, but in none of the
patients with pcFCL and only in one patient with
pcDLBL.
Surgical excision or radiotherapy are highly
effective in pcMZL and pcFCL, although after
surgery recurrences in the same body area are
common. Antibiotic treatment with doxycyclin
did not result in CR in any of the patients studied
herein.
On the basis of these results, and given the lack of
current therapies able to induce durable CR in all
three CBCL subgroups, new effective and well
tolerated therapies for CBCL are still needed. Future
studies employing new treatment modalities have to
clarify whether the recurrence rate can be decreased
and whether such new treatment would be beneficial
in CBCL.
Acknowledgements
The study was partially funded by the Bruno
Bloch Stiftung, Zurich, Switzerland. We are grateful
to Mrs. Petra Graf for the excellent technical
assistance.
References
1. Jaffe ES, Harris NL, Stein H, Vardiman JW, editors. World
Health Organization Classification of Tumours: Pathology and
Genetics of Tumours of Haematopoietic and Lymphoid
Tissues. Lyon, France: IARC Press; 2001.
2. Willemze R, Kerl H, Sterry W, Berti E, Cerroni L, Chimenti
S, Diaz-Perez JL, et al. EORTC classification for primary
cutaneous lymphomas: a proposal from the Cutaneous
Lymphoma Study Group of the European Organization for
Research and Treatment of Cancer (EORTC). Blood 1997;
90:354–371.
3. Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E,
Swerdlow SH, Ralfkiaer E, et al. WHO-EORTC classi-
fication for cutaneous lymphomas. Blood 2005;105:3768–
3785.
4. Burg G, Jaffe ES, Kempf W, Berti E, Cerroni L, Chimenti S,
Dummer R, et al. WHO/EORTC classification of cutaneous
lymphomas. In: LeBoit P, Burg G, Weedon D, Sarasin A,
editors. WHO Books: Tumors of the Skin. Lyon, France:
WHO IARC; 2005.
5. Kim YH, Willemze R, Pimpinelli N, Whittaker S, Olsen EA,
Ranki A, Dummer R, et al. TNM classification system for
primary cutaneous lymphomas other than mycosis fungoides
and Sezary syndrome: a proposal of the International Society
for Cutaneous Lymphomas (ISCL) and the Cutaneous
Lymphoma Task Force of the European organization of
research and Treatment of cancer (EORTC). Blood
2007;110:479–484.
6. Senff NJ, Willemze R. The applicability and prognostic value
of the new TNM classification system for primary cutaneous
lymphomas other than mycosis fungoides and Sezary syn-
drome: results on a large cohort of primary cutaneous B-cell
lymphomas and comparison with the system used by the
Dutch Cutaneous Lymphoma Group. Br J Dermatol 2007;
157:1205–1211.
7. Cerroni L, Arzberger E, Putz B, Hofler G, Metze D, Sander
CA, Rose C, et al. Primary cutaneous follicle center cell
lymphoma with follicular growth pattern. Blood 2000;95:
3922–3928.
8. Servitje O, Gallardo T, Estrach T, Pujol RM, Blanco A,
Fernandez-Sevilla A, Petriz L, et al. Primary cutaneous
marginal zone B-cell lymphoma: a clinical, histopathological,
immunophenotypic and molecular genetic study of 22 cases.
Br J Dermatol 2002;147:1147–1158.
9. Hoefnagel JJ, Vermeer MH, Jansen PM, Heule F, Vader
PCV, Sanders CJG, Gerritsen MJP, et al. Primary
cutaneous marginal zone B-cell lymphoma: clinical and
therapeutic features in 50 cases. Arch Dermatol 2005;141:
1139–1145.
10. Goodlad JR, Krajewski AS, Batstone PJ, McKay P, White JM,
Benton EC, Kavanagh GM, et al. Primary cutaneous follicular
lymphoma: a clinicopathologic and molecular study of 16
cases in support of a distinct entity. Am J Surg Pathol
2002;26:733–741.
11. Senff NJ, Hoefnagel JJ, Jansen PM, Vermeer MH, van Baarlen
J, Blokx WA, Canninga-van Dijk MR, et al. Reclassification of
300 primary cutaneous B-Cell lymphomas according to
the new WHO-EORTC classification for cutaneous lym-
phomas: comparison with previous classifications and
identification of prognostic markers. J Clin Oncol 2007;25:
1581–1587.
12. Dummer R, Hassel JC, Fellenberg F, Eichmuller S, Maier T,
Slos P, Acres B, et al. Adenovirus-mediated intralesional
interferon-gene transfer induces tumor regressions in cuta-
neous lymphomas. Blood 2004;104:1631–1638.
13. Cozzio A, Kempf W, Schmid-Meyer R, Gilliet M,
Michaelis S, Scharer L, Burg GN, et al. Intra-lesional low-
dose interferon alpha2a therapy for primary cutaneous
marginal zone B-cell lymphoma. Leuk Lymphoma 2006;
47:865–869.
14. Fink-Puches R, Zenahlik P, Back B, Smolle J, Kerl H,
Cerroni L. Primary cutaneous lymphomas: applicability of
current classification schemes (EORTC, WHO) based on
clinicopathologic features observed in a large group of
patients. Blood 2002;99:800–805.
15. Cerroni L, Zochling N, Putz B, Kerl H. Infection by Borrelia
burgdorferi and cutaneous B-cell lymphoma. J Cutan Pathol
1997;24:457–461.
16. Pimpinelli N, Santucci M, Bosi A, Moretti S, Vallecchi C,
Messori A, Giannotti B. Primary cutaneous follicular centre-
cell lymphoma – a lymphoproliferative disease with favour-
able prognosis. Clin Exp Dermatol 1989;14:12–19.
17. Bailey EM, Ferry JA, Harris NL, Mihm MC, Jacobson JO,
Duncan LM. Marginal zone lymphoma (low-grade B-cell
lymphoma of mucosa-associated lymphoid tissue type) of skin
and subcutaneous tissue: a study of 15 patients. Am J Surg
Pathol 1996;20:1011–1023.
1102 P. Golling et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.

18. Rijlaarsdam JU, Toonstra J, Meijer OW, Noordijk EM,
Willemze R. Treatment of primary cutaneous B-cell lympho-
mas of follicle center cell origin: a clinical follow-up study of
55 patients treated with radiotherapy or polychemotherapy. J
Clin Oncol 1996;14:549–555.
19. Cerroni L, Signoretti S, Hofler G, Annessi G, Putz B,
Lackinger E, Metze D, et al. Primary cutaneous marginal zone
B-cell lymphoma: a recently described entity of low-grade
malignant cutaneous B-cell lymphoma. Am J Surg Pathol
1997;21:1307–1315.
20. Grange F, Bekkenk MW, Wechsler J, Meijer CJLM, Cerroni
L, Bernengo M, Bosq J, et al. Prognostic factors in primary
cutaneous large B-cell lymphomas: a European multicenter
study. J Clin Oncol 2001;19:3602–3610.
21. Goodlad JR, Krajewski AS, Batstone PJ, McKay P, White JM,
Benton EC, Kavanagh GM, Lucraft HH. Primary cutaneous
diffuse large B-cell lymphoma. Prognostic significance and
clinicopathologic subtypes. Am J Surg Pathol 2003;27:1538–
1545.
22. Kodama K, Massone C, Chott A, Metze D, Kerl H,
Cerroni L. Primary cutaneous large B-cell lymphomas:
clinicopathologic features, classification, and prognostic
factors in a large series of patients. Blood 2005;106:2491–
2497.
23. Hembury TA, Lee B, Gascoyne RD, Macpherson N, Yang B,
House N, Medeiros LJ, Hsi ED. Primary cutaneous diffuse
large B-cell lymphoma: a clinicopathologic study of 15 cases.
Am J Clin Pathol 2002;117:574–580.
CBCL staging and therapy 1103
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itaet
Zue
rich
on
05/1
6/14
For
pers
onal
use
onl
y.




















