EF-MPR, a new energy eFficient multi-point relay selection algorithm for MANET
Upload
childcarblCategory
view
4download
0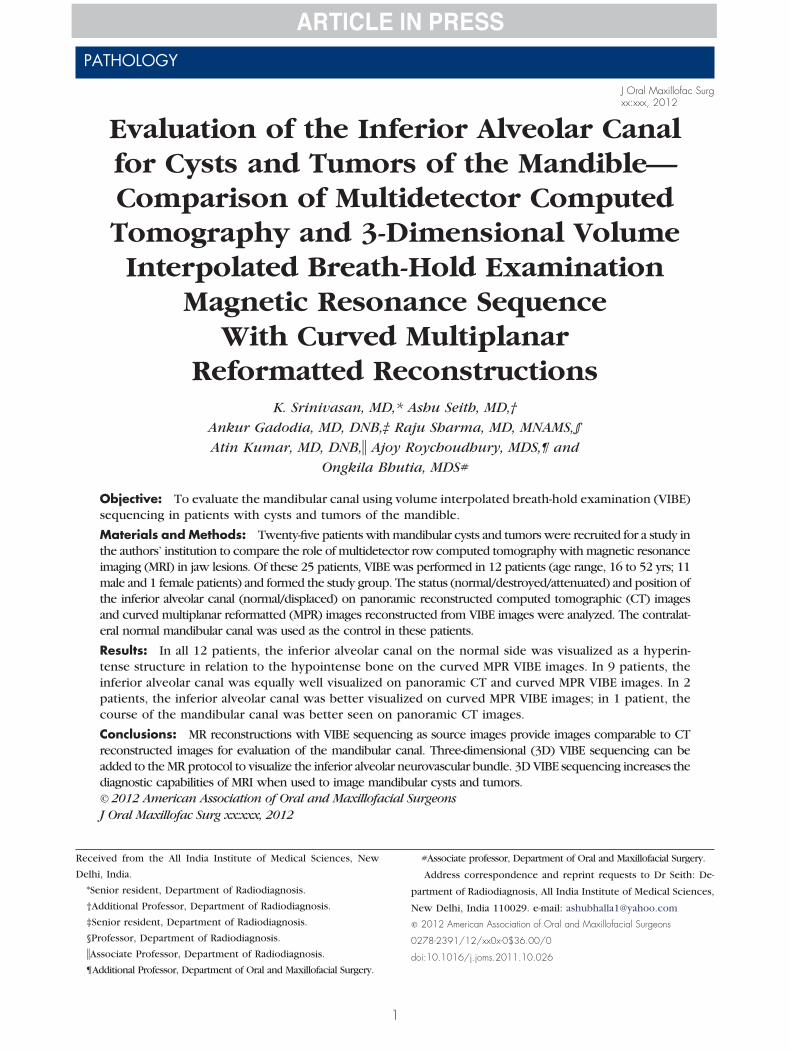
PATHOLOGY
J Oral Maxillofac Surgxx:xxx, 2012
Evaluation of the Inferior Alveolar Canalfor Cysts and Tumors of the Mandible—Comparison of Multidetector ComputedTomography and 3-Dimensional VolumeInterpolated Breath-Hold Examination
Magnetic Resonance SequenceWith Curved Multiplanar
Reformatted ReconstructionsK. Srinivasan, MD,* Ashu Seith, MD,†
Ankur Gadodia, MD, DNB,‡ Raju Sharma, MD, MNAMS,§
Atin Kumar, MD, DNB,� Ajoy Roychoudhury, MDS,¶ and
Ongkila Bhutia, MDS#
Objective: To evaluate the mandibular canal using volume interpolated breath-hold examination (VIBE)sequencing in patients with cysts and tumors of the mandible.
Materials and Methods: Twenty-five patients with mandibular cysts and tumors were recruited for a study inthe authors’ institution to compare the role of multidetector row computed tomography with magnetic resonanceimaging (MRI) in jaw lesions. Of these 25 patients, VIBE was performed in 12 patients (age range, 16 to 52 yrs; 11male and 1 female patients) and formed the study group. The status (normal/destroyed/attenuated) and position ofthe inferior alveolar canal (normal/displaced) on panoramic reconstructed computed tomographic (CT) imagesand curved multiplanar reformatted (MPR) images reconstructed from VIBE images were analyzed. The contralat-eral normal mandibular canal was used as the control in these patients.
Results: In all 12 patients, the inferior alveolar canal on the normal side was visualized as a hyperin-tense structure in relation to the hypointense bone on the curved MPR VIBE images. In 9 patients, theinferior alveolar canal was equally well visualized on panoramic CT and curved MPR VIBE images. In 2patients, the inferior alveolar canal was better visualized on curved MPR VIBE images; in 1 patient, thecourse of the mandibular canal was better seen on panoramic CT images.
Conclusions: MR reconstructions with VIBE sequencing as source images provide images comparable to CTreconstructed images for evaluation of the mandibular canal. Three-dimensional (3D) VIBE sequencing can beadded to the MR protocol to visualize the inferior alveolar neurovascular bundle. 3D VIBE sequencing increases thediagnostic capabilities of MRI when used to image mandibular cysts and tumors.© 2012 American Association of Oral and Maxillofacial SurgeonsJ Oral Maxillofac Surg xx:xxx, 2012
Received from the All India Institute of Medical Sciences, New
Delhi, India.
*Senior resident, Department of Radiodiagnosis.
†Additional Professor, Department of Radiodiagnosis.
‡Senior resident, Department of Radiodiagnosis.
§Professor, Department of Radiodiagnosis.
�Associate Professor, Department of Radiodiagnosis.
#Associate professor, Department of Oral and Maxillofacial Surgery.
Address correspondence and reprint requests to Dr Seith: De-
partment of Radiodiagnosis, All India Institute of Medical Sciences,
New Delhi, India 110029. e-mail: [email protected]
© 2012 American Association of Oral and Maxillofacial Surgeons
0278-2391/12/xx0x-0$36.00/0
doi:10.1016/j.joms.2011.10.026
¶Additional Professor, Department of Oral and Maxillofacial Surgery.1

(tmptcid
mrmw
u5fis5tmtaadar(falac
sgeatesomp
tiiiOnafnodtvi
tsstpV
2 MANDIBULAR CYSTS AND TUMORS
The inferior alveolar canal (mandibular canal) is animportant surgical landmark that should be as-sessed preoperatively in patients with tumors andcysts arising from the body and ramus of the man-dible to avoid injury to the neurovascular bundle.The inferior alveolar nerve and vessels enter themandibular foramen on the medial surface of theramus, traverse through the mandibular canal an-teroinferiorly, and exit through the mental fora-men.1 Multidetector row computed tomographyMDCT) enables rapid thin-section acquisition ofhe regional body anatomy. The course of the bonyandibular canal is best visualized on axial andanoramic reconstructed images. However, in pa-ients lacking a bony limitation of the mandibularanal and to avoid radiation, magnetic resonancemaging (MRI) can be performed to study the man-ibular canal.2 In recent years, MRI has been in-
creasingly used to evaluate cysts and tumors of theoral and maxillofacial region. Volumetric interpolatedbreath-hold examination (VIBE) is a rapid 3-dimen-sional (3D) gradient echo sequence with fat suppres-sion.3 The integrated fat saturation helps visualize the
andibular canal by suppressing the fatty bone mar-ow. The objective of this study was to evaluate theandibular canal using the VIBE sequence in patientsith cysts and tumors of the mandible.
Methods and Materials
Twenty-five patients with mandibular cysts and tu-mors were recruited for a study in the All India Insti-tute of Medical Sciences (New Delhi, India) to com-pare the role of MDCT with MRI in jaw lesions. Allpatients were included after obtaining informed con-sent, and the study was approved by the institutionalethics committee. In a subset of 12 patients (agerange, 16 to 52 yrs; 11 male and 1 female patients), inaddition to the spin echo T1 and T2 sequences, VIBEsequences were performed before and after intrave-nous administration of gadolinium. The VIBE se-quence and its reconstruction were standardized dur-ing the course of the study; hence, this sequence wasperformed in only a limited number of patients.
MDCT was performed using a Somatom Sensation40-slice CT scanner (Siemens, Erlangen, Germany).Axial sections were obtained at 0.6-mm intervals par-allel to the alveolar ridge. Panoramic reconstructionwas performed from these axial images using inte-grated dental imaging software. syngo Dental CT (Sie-mens, Muenchen, Germany).
MRI of the mandible was performed on a 1.5-T MRscanner (Avanto; Siemens) using a head coil. Theprotocol for MRI included a T1 sequence (repetition
time, 600 to 800 ms; echo time, 17 ms) and a T2 Vsequence (repetition time, 3,000 to 4,000 ms; echotime, 70 to 90 ms). The section thickness varied from3 to 5 mm with matrix of 256 � 256. The parameters
sed for the VIBE sequence were a repetition time of.5 ms, an echo time of 2.5 ms, a flip angle of 10°, aeld of view of 160 cm, a matrix of 256 � 256, aection thickness of 1 mm, and an acquisition time of5 seconds. The patients were not instructed to holdheir breath because artifacts related to respiratoryotion are minimal in the head and neck region, but
hey were required to avoid swallowing (breath-holdcquisition, ie, scanning the entire anatomic region insingle breath-hold is commonly performed in ab-
ominal imaging). After gadolinium administration,xial images obtained from the VIBE sequence wereeconstructed using curved multiplanar reformattingMPR). Curved MPR is a view mode commonly usedor visualizing structures with a curved geometry suchs the mandible. It is obtained by drawing a curvedine over visible parts of the mandibular canal on thexial images and then reconstructed using postpro-essing software.The panoramic images obtained from the recon-
tructions were analyzed by consensus by 2 radiolo-ists (A.S. and R.S.) with 10 and 15 years of experi-nce, respectively, in CT and MRI. Images from CTnd MRI were analyzed in separate viewing sessionshat were separated by at least 1 month. The param-ters used for analysis were the status (normal/de-troyed/attenuated) and position (normal/displaced)f the mandibular canal. The contralateral normalandibular canal was used as the control in theseatients.On MDCT images, the canal was labeled normal if
he cortical wall of the mandibular canal was visual-zed in its full extent. The canal was labeled destroyedf the entire or a portion of the canal was not visual-zed or if the cortical wall of the canal was disrupted.n MR images, the inferior alveolar canal was labeledormal if the neurovascular bundle was visualized ashyperintense structure in its entire extent. The in-
erior alveolar canal was considered destroyed if theeurovascular bundle was not visualized in the regionf the tumor or attenuated if the neurovascular bun-le was seen as a thin hyperintense structure coursinghrough the tumor. The position of the canal/neuro-ascular bundle was also assessed on MDCT and MRmages and categorized as normal or displaced.
A scoring system was used for the status and posi-ion of the inferior alveolar canal on panoramic recon-tructed CT images and curved MPR images recon-tructed from VIBE sequences. A score of 1 indicatedhat the 2 images were similar, 2 indicated that the CTanoramic image was better than the curved MPRIBE images, and 3 indicated that the curved MPR
IBE image was better than the CT panoramic image.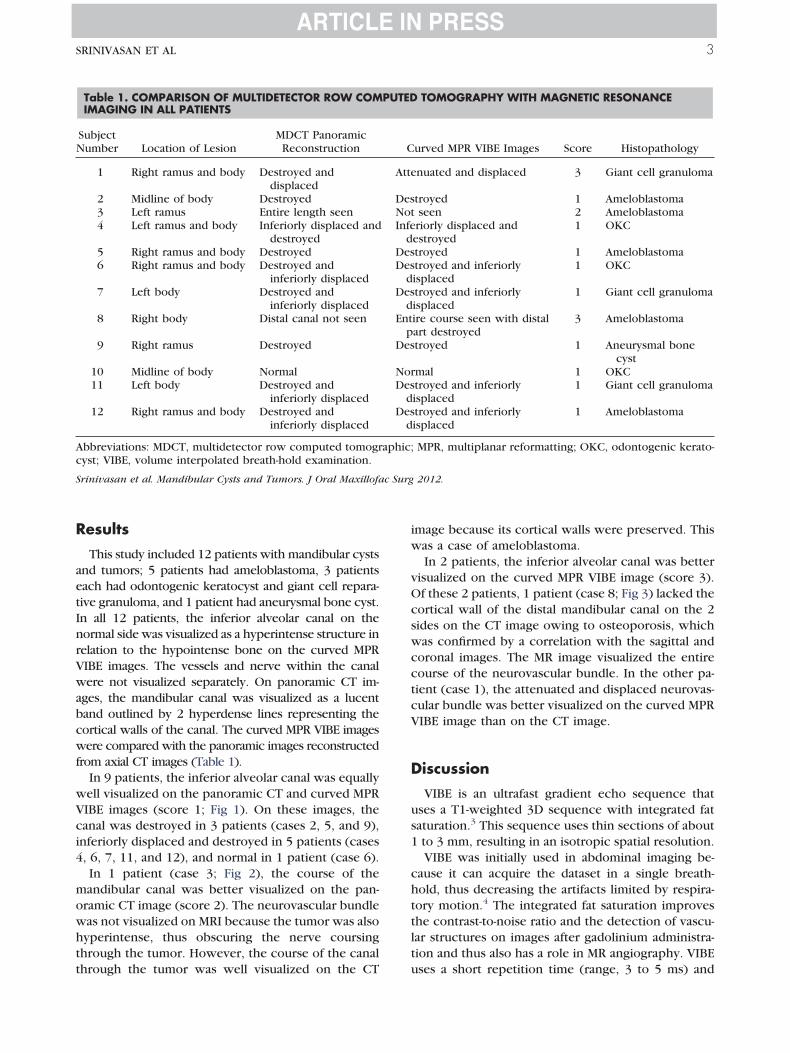
mowhtt
c Surg
SRINIVASAN ET AL 3
Results
This study included 12 patients with mandibular cystsand tumors; 5 patients had ameloblastoma, 3 patientseach had odontogenic keratocyst and giant cell repara-tive granuloma, and 1 patient had aneurysmal bone cyst.In all 12 patients, the inferior alveolar canal on thenormal side was visualized as a hyperintense structure inrelation to the hypointense bone on the curved MPRVIBE images. The vessels and nerve within the canalwere not visualized separately. On panoramic CT im-ages, the mandibular canal was visualized as a lucentband outlined by 2 hyperdense lines representing thecortical walls of the canal. The curved MPR VIBE imageswere compared with the panoramic images reconstructedfrom axial CT images (Table 1).
In 9 patients, the inferior alveolar canal was equallywell visualized on the panoramic CT and curved MPRVIBE images (score 1; Fig 1). On these images, thecanal was destroyed in 3 patients (cases 2, 5, and 9),inferiorly displaced and destroyed in 5 patients (cases4, 6, 7, 11, and 12), and normal in 1 patient (case 6).
In 1 patient (case 3; Fig 2), the course of theandibular canal was better visualized on the pan-
ramic CT image (score 2). The neurovascular bundleas not visualized on MRI because the tumor was alsoyperintense, thus obscuring the nerve coursinghrough the tumor. However, the course of the canal
Table 1. COMPARISON OF MULTIDETECTOR ROW COMIMAGING IN ALL PATIENTS
SubjectNumber Location of Lesion
MDCT PanoramicReconstruction
1 Right ramus and body Destroyed anddisplaced
2 Midline of body Destroyed3 Left ramus Entire length seen4 Left ramus and body Inferiorly displaced and
destroyed5 Right ramus and body Destroyed6 Right ramus and body Destroyed and
inferiorly displaced7 Left body Destroyed and
inferiorly displaced8 Right body Distal canal not seen
9 Right ramus Destroyed
10 Midline of body Normal11 Left body Destroyed and
inferiorly displaced12 Right ramus and body Destroyed and
inferiorly displaced
Abbreviations: MDCT, multidetector row computed tomogrcyst; VIBE, volume interpolated breath-hold examination.
Srinivasan et al. Mandibular Cysts and Tumors. J Oral Maxillofa
hrough the tumor was well visualized on the CT
image because its cortical walls were preserved. Thiswas a case of ameloblastoma.
In 2 patients, the inferior alveolar canal was bettervisualized on the curved MPR VIBE image (score 3).Of these 2 patients, 1 patient (case 8; Fig 3) lacked thecortical wall of the distal mandibular canal on the 2sides on the CT image owing to osteoporosis, whichwas confirmed by a correlation with the sagittal andcoronal images. The MR image visualized the entirecourse of the neurovascular bundle. In the other pa-tient (case 1), the attenuated and displaced neurovas-cular bundle was better visualized on the curved MPRVIBE image than on the CT image.
Discussion
VIBE is an ultrafast gradient echo sequence thatuses a T1-weighted 3D sequence with integrated fatsaturation.3 This sequence uses thin sections of about1 to 3 mm, resulting in an isotropic spatial resolution.
VIBE was initially used in abdominal imaging be-cause it can acquire the dataset in a single breath-hold, thus decreasing the artifacts limited by respira-tory motion.4 The integrated fat saturation improvesthe contrast-to-noise ratio and the detection of vascu-lar structures on images after gadolinium administra-tion and thus also has a role in MR angiography. VIBE
TOMOGRAPHY WITH MAGNETIC RESONANCE
urved MPR VIBE Images Score Histopathology
nuated and displaced 3 Giant cell granuloma
troyed 1 Ameloblastomaseen 2 Ameloblastomariorly displaced andestroyed
1 OKC
troyed 1 Ameloblastomatroyed and inferiorlyisplaced
1 OKC
troyed and inferiorlyisplaced
1 Giant cell granuloma
ire course seen with distalart destroyed
3 Ameloblastoma
troyed 1 Aneurysmal bonecyst
mal 1 OKCtroyed and inferiorlyisplaced
1 Giant cell granuloma
troyed and inferiorlyisplaced
1 Ameloblastoma
MPR, multiplanar reformatting; OKC, odontogenic kerato-
2012.
PUTED
C
Atte
DesNotInfe
dDesDes
dDes
dEnt
pDes
NorDes
dDes
d
aphic;
uses a short repetition time (range, 3 to 5 ms) and

thwattca
naaltditwo
mstrun
lantf1
u
c Surg
4 MANDIBULAR CYSTS AND TUMORS
lacks phase artifacts. The integrated fat saturation onVIBE sequences makes it suitable for whole-bodyscreening for metastases.3 Kataoka et al5 evaluatedhe role of contrast-enhanced VIBE in 33 patients withead and neck tumors. They found that VIBE imagesere superior in resolution despite a decrease in
cquisition time with fewer artifacts compared withhe routine spin echo T1 sequence. They concludedhat VIBE can be used as an alternative for the post-ontrast spin echo T1 sequence in the preoperativessessment of head and neck tumors.
The preoperative assessment of the mandibular ca-al is important to determine the nature of the lesion,nd to decide the surgical management. Lesionsbove the canal are likely to be odontogenic, whereasesions below it are usually nonodontogenic in na-ure.6 The surgical management of mandibular tumorsepends on the extent of infiltration of the surround-
ng soft tissues, involvement of the cortical bone, andhe inferior alveolar nerve. Williams7 suggested aide resection with a 2-cm margin of normal bone for
FIGURE 1. Case 10: Odontogenic keratocyst in a 22-year-old mnilocular lytic lesion in the midline and the 2 mandibular cana
breath-hold examination image after gadolinium administration shbundle on either side. A score of 1 was given for this case.
Srinivasan et al. Mandibular Cysts and Tumors. J Oral Maxillofa
perating on mandibular bone tumors. When the tu-
or is surrounded by the inferior alveolar nerve, ithould be resected en bloc with the nerve. However,he patient will have permanent numbness of theegion innervated by the mental nerve. Thus, it isseful to delineate the course of the inferior alveolarerve preoperatively using imaging.MDCT helps in the excellent visualization and de-
ineation of the inferior alveolar canal. It also helps tossess the buccolingual position and height of theeurovascular bundle. However, the effective radia-ion dose received by the tissues near the mandibleor a single MDCT examination ranges from 474 to,160 �Sv.8,9 Many cadaveric studies have been con-
ducted to validate the role of MRI as an alternative toCT for evaluating the neurovascular bundle.10,11 Allthese studies have shown that MRI can be used toevaluate the mandibular canal compared with dentalCT images. Eggers et al12 in their cadaveric studyevaluated the geometric accuracy of MRI of the man-dibular canal. They superimposed the coronal CT andMR images, which were acquired with a similar reso-
Panoramic reconstructed computed tomographic image shows anormal. B, Curved multiplanar reformatted volume interpolatedunilocular cystic lesion and a normal hyperintense neurovascular
2012.
an. A,ls areows a
lution and field of view using Interactive Data Lan-

atwa
3wmeti
finsomtwHtdce
sMAtmg
q
s
i given f
S c Surg
SRINIVASAN ET AL 5
guage software (IDL; Research Systems Inc., Boulder,CO) and found an excellent concordance of the man-dibular nerve on MR images and the mandibular canalon CT image data. They recommended a VIBE se-quence with a flip angle of 15° for optimal visualiza-tion of the mandibular canal.
To the best of the authors’ knowledge, there is only1 in vivo study that has evaluated the role of high-resolution gradient echo sequencing (with a spectralfat suppression preimpulse) in 11 patients with dys-esthesia in the floor of the mouth to visualize themandibular canal.13 MR images were acquired in thexial plane, and coronal and panoramic reconstruc-ions were performed subsequently using dental soft-are. They concluded that dental MRI could becomeviable alternative to 3D MPR CT programs.In the present study, the role of curved MPR using
D VIBE sequencing to visualize the mandibular canalas evaluated in patients with cysts and tumors of theandible. Because the VIBE is an ultrafast gradient
cho sequence with fat suppression, the contrast be-ween the neurovascular structures and the surround-
FIGURE 2. Case 3: Ameloblastoma in a 42-year-old man. A, Pahows the attenuated left mandibular canal (arrowhead) coursing t
breath-hold examination image shows nonvisualization of the left pn the left ramus, with the distal part visualized. A score of 2 was
rinivasan et al. Mandibular Cysts and Tumors. J Oral Maxillofa
ng bone is very high owing to suppression of the C
atty bone marrow. The curved MPR reconstructedmage from the VIBE sequence clearly visualized theeurovascular bundle, whether it was normal, de-troyed, or attenuated. MRI has a distinct advantagever CT in patients who lack the cortical wall of theandibular canal because of osteoporosis or destruc-
ion by tumor, as seen in 2 cases in the present study,here MR clearly visualized the mandibular canal.owever, when the tumor has the same intensity as
hat of the neurovascular bundle, then it becomesifficult to trace it through the tumor, as seen in 1ase in the present study. The limitation of the pres-nt study was the small number of patients.Thus, the VIBE sequence with curved MPR recon-
tructions can provide an alternative to panoramicDCT images in the evaluation of the mandibular canal.ssessment of the mandibular canal is also important in
he preoperative assessment of dental implant place-ent. However, a larger study is required to evaluate the
eometric accuracy of this sequence.To conclude, MR reconstructions with VIBE se-
uences as source images provide images comparable to
ic reconstructed multidetector row computed tomographic imagethe tumor. B, Curved multiplanar reformatted volume interpolatedl inferior alveolar canal through the hyperintense lesion (asterisk)or this case.
2012.
noramhroughroxima
T reconstructed images for evaluation of the mandib-

sba
c Surg
6 MANDIBULAR CYSTS AND TUMORS
ular canal. Hence, when MRI is performed in patientswith cysts and tumors of the mandible to visualize softtissue extension or in patients with contraindications toMDCT, the 3D VIBE sequence can be added to the MRIprotocol to visualize the inferior alveolar neurovascularbundle. The 3D VIBE sequence can increase the diag-nostic capabilities of MRI when used to visualize man-dibular cysts and tumors.
References1. Osborn AG, Hanafee WH, Mancuso AA: Normal and pathologic
CT anatomy of the mandible. AJR Am J Roentgenol 139:555,1982
2. Nasel CJO, Pretterklieber M, Gahleitner A, et al: Osteometry ofthe mandible performed using dental MR imaging. AJNR Am JNeuroradiol 20:1221, 1999
3. Thomson V, Pialat JB, Gay F, et al: Whole-body MRI for metas-tases screening: A preliminary study using 3D VIBE sequenceswith automatic subtraction between noncontrast and contrastenhanced images. Am J Clin Oncol 31:285, 2008
4. Rofsky L, Laub G, Pollack M, et al: Abdominal MR imaging with
FIGURE 3. Case 8: Ameloblastoma in a 42-year-old man. A, Pahows a multilocular lesion in the body of the right hemimandible wiecause of extensive osteoporosis. B, Curved multiplanar reformatdministration shows a hyperintense lesion (asterisk) in the right
inferior alveolar canal was normal. A score of 3 was given for thi
Srinivasan et al. Mandibular Cysts and Tumors. J Oral Maxillofa
a volumetric interpolated breath-hold examination. Radiology212:876, 1999
5. Kataoka M, Ueda H, Koyama T, et al: Contrast-enhanced volu-metric interpolated breath-hold examination compared withspin-echo T1-weighted imaging of head and neck tumors. AJRAm J Roentgenol 184:313, 2005
6. Neyaz Z, Gadodia A, Gamanagatti S, et al: Radiographical ap-proach to jaw lesions. Singapore Med J 49:165, 2008
7. Williams TP: Management of ameloblastoma: A changing per-spective. J Oral Maxillofac Surg 51:1064, 1993
8. Ludlow JB, Ivanovic M: Comparative dosimetry of dental CBCTdevices and 64-slice CT for oral and maxillofacial radiology.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106:106,2008
9. Loubele M, Bogaerts R, Van Dijck E, et al: Comparison betweeneffective radiation dose of CBCT and MSCT scanners for den-tomaxillofacial applications. Eur J Radiol 71:461, 2009
10. Ikeda K, Ho K-C, Nowicki BH, et al: Multiplanar MR andanatomic study of the mandibular canal. AJNR Am J Neurora-diol 17:579, 1996
11. Nasel CJO, Pretterklieber M, Gahleitner A, et al: Osteometry ofthe mandible performed using dental MR imaging. AJNR Am JNeuroradiol 20:1221, 1999.
12. Eggers G, Rieker M, Fiebach J, et al: Geometric accuracy ofmagnetic resonance imaging of the mandibular nerve Den-tomaxillofac Radiol 34:285, 2005
13. Nasel C, Gahleitner A, Breitenseher M, et al: Localization of themandibular neurovascular bundle using dental magnetic reso-
ic reconstructed multidetector row computed tomographic imageonvisualized distal mandibular canals on the 2 sides (arrowheads)ume interpolated breath-hold examination image after gadoliniumndible with destruction of the distal right canal (arrow). The left
2012.
noramth the nted volhemimas case.
nance imaging. Dentomaxillofac Radiol 27:305, 1998
Copyright © 2022 FDOKUMEN