
Self-selection bias in estimated wage premiums for earnings risk
Upload
independentCategory
view
2download
0
A
T(sNcrl2ehhpK
I
oaoB
HThSLaTW
1d
Research Article
Estimated prevalence of uncontrolled hypertension and multiplecardiovascular risk factors and their associated risk of coronary heart
disease in the United StatesJoshua S. Benner, PharmD, ScDa,*, Timothy W. Smith, BAa, Allison A. Petrilla, MPHa,
David Klingman, PhDa, Sangeeta Goel, PharmDa, Simon S. K. Tang, MPHb, andNathan D. Wong, PhDc
aIMS Health, Inc., Arlington, Virginia, USA;bPfizer Inc., New York, New York, USA; and
cHeart Disease Prevention Program, Division of Cardiology, University of California, Irvine, California, USA
Manuscript received April 10, 2007 and accepted July 10, 2007
bstract
his study determined the prevalence of primary prevention patients aged 40 to 79 years with uncontrolled hypertensionHTN) and low/moderate cholesterol levels, and the clinical and economic consequences of their cardiovascular risk levelstratified by additional cardiovascular risk factors. Prevalence was estimated from the 1999 to 2002 National Health andutrition Examination Survey (NHANES) datasets. Framingham risk equations were used to calculate the 4-year risk of
oronary heart disease (CHD). HTN and cholesterol levels were then statistically “controlled” to ideal levels and risks wereecalculated. Prevalence of uncontrolled hypertension was 15.2 million cases (13.7%). Of those, 12.9 million (84.8%) hadow/moderate cholesterol levels, and 2.2 million (16.7%) had �3 additional risk factors with no history of CHD. Nearly00,000 coronary events are expected to occur within 4 years, incurring over $2.5 billion in direct medical costs. Statisticalstimation suggests that 64% of 4-year risk was attributable to uncontrolled blood pressure and lipids. The large number andigh cost of CHD events expected to occur within the next 4 years in primary prevention patients with uncontrolledypertension and �3 additional risk factors justifies aggressive screening to ensure that these patients are identified androperly managed. © 2008 American Society of Hypertension. All rights reserved.
Journal of the American Society of Hypertension 2(1) (2008) 44–53
eywords: Cholesterol; cost; ASCOT-LLA; primary prevention.
bC
ltacpT
SAaa
cA
ntroduction
Cardiovascular disease (CVD) is the single leading causef mortality in the United States.1 Over 1 million people diennually of a cardiovascular (CV) event, with the majorityf these events attributable to coronary heart disease (CHD).eyond the high clinical burden of CHD, the economic
This study was supported by a Grant from Pfizer, Inc.Drs. Benner, Smith, and Klingman are all employees of IMS
ealth, Inc, a health information services and consulting firm.hey have provided consulting services to manufacturers of anti-ypertensive and lipid-lowering therapies, including Pfizer Inc.,chering-Plough Corporation, and AstraZeneca PharmaceuticalsP. Ms. Petrilla and Ms. Goel are consultants to IMS Health, Inc,nd Ms. Petrilla is a former employee of IMS Health, Inc. Mr.ang is an employee of, and holds stock options for, Pfizer Inc. Dr.
ong receives grant support from Pfizer Inc., and Bristol Myers933-1711/08/$ – see front matter © 2008 American Society of Hyperteoi:10.1016/j.jash.2007.07.001
urden is also substantial, with direct medical costs forHD exceeding $151.6 billion.1,2
Nearly all patients with CHD have prior exposure to ateast one of the major CHD risk factors, including hyper-ension (HTN), dyslipidemia (DYS), cigarette use, and di-betes.1 Although HTN and DYS are two of the mostommon and readily modifiable CHD risk factors, mostatients with either HTN or DYS remain poorly controlled.he National Health and Nutrition Examination Survey
quibb, and is on the speakers’ bureau for Pfizer Inc., Sanofi-ventis, and Takeda. The staff of IMS Health were paid consult-
nts to Pfizer Inc., in connection with the development of thisrticle.
*Corresponding author: Joshua S. Benner, PharmD, ScD, Prin-ipal, IMS Health, Inc., 300 N. Washington Street, Suite 303,rlington, Virginia 22046. Tel: 703-286-2868; fax: 703-286-2899.
E-mail: [email protected]
nsion. All rights reserved.

(UooeCmmwEI
scpOolpip[�(CoctiC
iUfpaod
M
2atqfcNrb
te�
hAlitmH�
rnfF
swmcsc(mNtu
lpwCgc
TIdp
I
M
US
S
L
Lvlc
45J.S. Benner et al. / Journal of the American Society of Hypertension 2(1) (2008) 44–53
NHANES) revealed that between 1999 and 2000, 29% ofS adults met clinical criteria for HTN but fewer than 58%f the hypertensives were treated, and among those treated,nly 31% had blood pressure control3 based on criteriastablished in the Seventh Report of the Joint Nationalommittee on Prevention, Detection, Evaluation, and Treat-ent of High Blood Pressure (JNC-7).4 Similarly, 56% ofen and 54% of women had DYS, fewer than 10% ofhom met lipid targets set by the National Cholesterolducation Program Adult Treatment Panel III (NCEP ATP
II).5
Numerous clinical trials and meta-analyses have demon-trated that antihypertensive and lipid-lowering agents areapable of reducing the incidence of CV events in at-riskopulations.6–10 Recently, the Anglo-Scandinavian Cardiacutcomes Trial-Lipid Lowering Arm (ASCOT-LLA) dem-nstrated the clear benefit of combined antihypertensive andipid-lowering therapy in hypertensive patients with multi-le CV risk factors but without pre-existing CHD.11 Patientsn the trial had uncontrolled HTN (untreated systolic bloodressure [SBP] �160 mm Hg or diastolic blood pressureDBP] �100 mm Hg, or treated SBP �140 mm Hg or DBP90 mm Hg), low/moderate total cholesterol (TC) levels
TC �251 mg/dL [6.5 mmol/L], and at least three additionalV risk factors. Compared with patients who received onef two antihypertensive therapies alone, those who receivedoncomitant antihypertensive and atorvastatin therapy overhe median 3.3-year follow-up period had a 36% lowerncidence of nonfatal myocardial infarction (MI) and fatalHD. The risk of stroke was also reduced by 27%.11
The general aim of this study was to understand themplications of the ASCOT-LLA trial for the population ofS adults with uncontrolled HTN and multiple CVD risk
actors. The specific objectives were to: 1) determine therevalence of the ASCOT-LLA inclusion criteria in the USdult population, 2) predict the risk and near-term frequencyf preventable CHD events, and 3) estimate the short-runirect medical costs associated with these events.
ethods
Patient-level data were drawn from the 1999 to 2000 and001 to 2002 NHANES datasets.12,13 NHANES is a nation-lly representative health survey administered by the Na-ional Center for Health Statistics (NCHS) that collectsuestionnaire, examination, and laboratory data. This studyollowed NHANES analytic guidelines, which recommendombining two or more 2-year datasets from the continuousHANES in order to produce estimates with statistical
eliability.14 Population estimates derived from this com-ined 4-year dataset are tied to 2000 US Census figures.We first identified all patients with a history of HTN in
he NHANES database. This definition, referred to as “cat-gorical hypertension,” included SBP �140 mm Hg or DBP
90 mm Hg, self-reported history of HTN, or use of anti- sypertensive medication. To more closely approximate theSCOT-LLA risk profile, we then limited the study popu-
ation to a subset of categorical hypertensive patients thatncluded adult subjects aged 40 to 79 years with uncon-rolled HTN (defined as SBP �160 mm Hg or DBP �100m Hg if untreated or SBP �140 mm Hg or DBP �90 mmg if treated), and low to moderate TC levels, defined as TC251 mg/dL (6.5 mmol/L).Subjects were further evaluated for the presence of CV
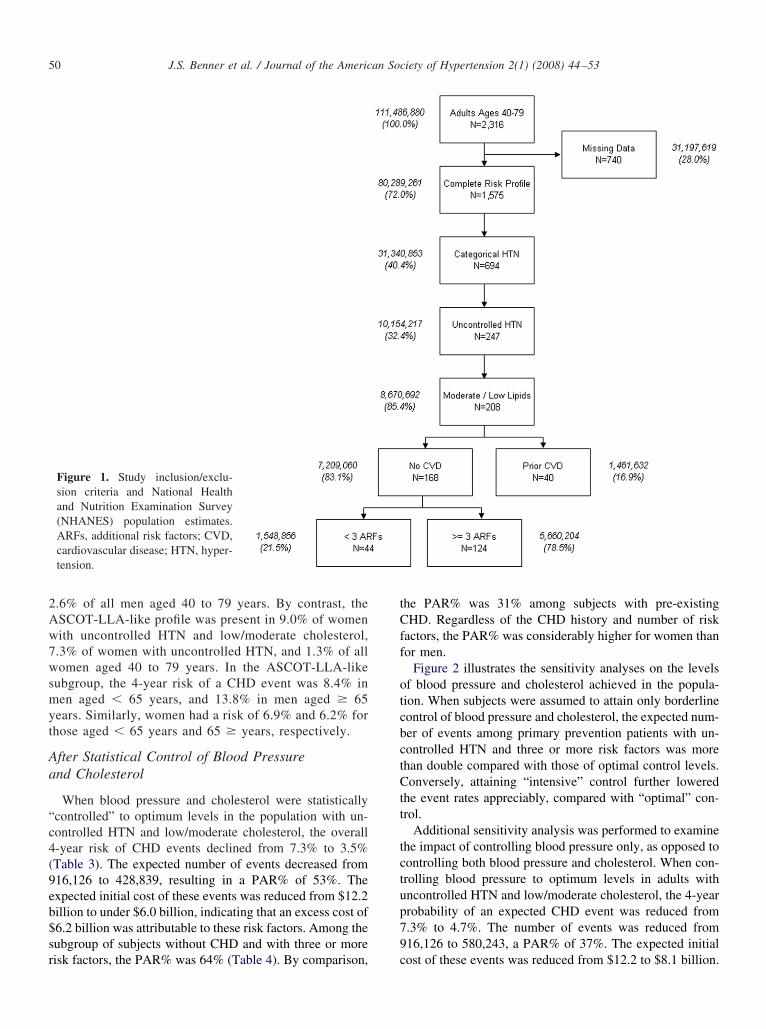
isk factors as defined in ASCOT-LLA (Table 1).11 Theumber of concomitant CV risk factors was then countedor each subject. Full inclusion criteria are illustrated inigure 1.The study employed the NHANES morning fasting
ub-sample since fasting blood glucose and triglyceridesere examined. In order to ensure complete ascertain-ent of all CV risk factors, only those subjects with
omplete data for all risk factors were included in thetudy. Although ASCOT-LLA counted abnormal electro-ardiogram (ECG) and left ventricular hypertrophyLVH) as CV risk factors, it was not possible to deter-ine the presence of either abnormal ECG or LVH in theHANES datasets employed in this study. Because of
his, the number of concomitant risk factors may benderestimated for some subjects.To achieve nationally-representative estimates of preva-
ence and frequency of events, a two-stage up-weightingrocedure was used. First, weights provided by NHANESere utilized to estimate prevalence based on the 2000 USensus, and SUDAAN statistical software (Research Trian-le Institute, Research Triangle Park, NC) was used toompute weighted variance estimates. Second, since some
able 1nclusion criteria and cardiovascular risk factors used toetermine prevalence of ASCOT-LLA-like risk profile in studyopulation
nclusion Criteria CV Risk Factors
en and women, aged 40to 79 years
ncontrolled hypertensionBP � 160 mm Hg orDBP � 100 mm Hg(untreated)
BP � 140 mm Hg orDBP � 90 mm Hg(treated)
ow/moderate TC � 251mg/dL
Age � 55 yearsMale genderCurrent smokerDiabetesFamily history of premature CHDMicroalbuminuria/proteinuriaPrevious stroke/transient ischemic
attackTC:HDL-C ratio � 6Peripheral arterial disease
ASCOT-LLA, Anglo–Scandinavian Cardiac Outcomes Trial-ipid Lowering Arm; CHD, coronary heart disease; CV, cardio-ascular; DBP, diastolic blood pressure; HDL-C, high-densityipoprotein cholesterol; SBP, systolic blood pressure; TC, totalholesterol.
ubjects were excluded due to missing risk factor data,

rsidw
aohL((edoecfhtifa
lgttHanp
wrcrHccwrmbtwbcTpw(pw2
“HHpccob
clderaadscEasmipoa$wfie
R
A
tNfiAaramo2
oow14a
46 J.S. Benner et al. / Journal of the American Society of Hypertension 2(1) (2008) 44–53
esults were further up-weighted by an age- and gender-pecific constant that allowed projection to the full non-nstitutionalized civilian US adult population. This proce-ure assumed that missing data were completely randomithin age/gender strata.Gender-specific Framingham risk equations for primary
nd secondary CHD were used to calculate the 4-year riskf CHD events for each subject,15 because the 4-year timeorizon most closely reflected the duration of ASCOT-LA.11 CHD events predicted by the equation included MI
fatal or nonfatal), angina pectoris, and CHD-related deathsudden or nonsudden). Secondary CHD equations weremployed in subjects with a self-reported history of CVD,efined as having been told by a physician of the presencef CHD, angina, heart attack, or stroke. Primary CHDquations were employed in subjects with none of the listedonditions. The model for men examined the impact of theollowing risk factors on risk of CHD: age, ratio of TC toigh-density lipoprotein cholesterol (HDL-C), diabetic sta-us, smoking status, SBP, and use of antihypertensive med-cation. The model for females included all of the above riskactors in addition to triglyceride levels, menopausal status,nd alcohol use.
Several subgroups of interest were identified and ana-yzed separately. Subjects were initially stratified by age andender as well as by history of CHD. The primary preven-ion group was further stratified by risk profile according tohe number of CV risk factors in addition to uncontrolledTN. Risks were averaged over subjects in each stratum
nd then multiplied by the estimated population to yield theumber of individuals in the population who could be ex-ected to experience at least one CHD event within 4 years.To determine the proportion of predicted events that
ould be attributable to uncontrolled HTN and DYS, theseisk factors were statistically “controlled” and risks recal-ulated. To simulate controlled HTN, subjects’ SBP waseduced to 139 mm Hg in cases where SBP was � 139 mmg. This represented the upper limit of the borderline HTN
lassification according to JNC-7 guidelines.4 To simulateontrolled lipid levels, HDL-C was recoded to 60 mg/dLhere HDL-C was � 60 mg/dL (1.6 mmol/L) and TC was
ecoded to 199 mg/dL where TC was � 199 mg/dL (5.1mol/L). These levels represent the lower and upper
ounds of the healthy ranges for HDL-C and TC, respec-ively, according to NCEP ATP III.16 Predicted CHD eventsere then recalculated; the difference in the absolute num-er of predicted CHD events between uncontrolled andontrolled scenarios was deemed “attributable” events.17,18
he quotient of attributable events to total events in theopulation before controlling blood pressure and cholesterolas defined as the population-attributable risk percentage
PAR%).17 In a sensitivity analysis on the level of bloodressure and cholesterol control achieved, three scenariosere explored: “borderline” control (SBP: 139 mm Hg; TC:
39 mg/dL; HDL-C: 41 mg/dL [male], 51 mg/dL [female]); roptimal” control (SBP: 119 mm Hg; TC: 199 mg/dL;DL-C: 61 mg/dL); and “intensive” control (SBP: 107 mmg; TC: 179 mg/dL; HDL-C: 67 mg/dL). The 4-year ex-ected number of CHD events and short-term direct medicalosts were determined based on these defined levels ofontrol. Additional sensitivity analysis examined the impactf controlling blood pressure only, as opposed to controllingoth blood pressure and cholesterol.First-year direct medical costs of preventable events were
alculated based on event-specific cost figures from theiterature. The weighted average cost for a CHD event wasetermined based on the frequency distribution of CHDvents in the Framingham cohort,15 which were mapped toeported first-year direct medical costs for sudden coronaryrtery disease death, fatal MI, nonfatal MI, unstable angina,nd angina pectoris.19 All costs were inflated to 2004 USollars using the Medical Care component of the US Con-umer Price Index.20 First-year direct medical costs in-luded event-related costs and 6-month maintenance costs.vent-related costs included all medical care for coronaryrtery disease during the year in which an event occurred,uch as emergency medical care and hospitalization. Six-onth maintenance care among survivors of an acute event
ncluded outpatient, emergency, inpatient, home health, andharmacy services. Inflated first-year costs for sudden cor-nary artery disease death, fatal MI, nonfatal MI, unstablengina, and angina pectoris were $1,003, $24,656, $21,856,16,958, and $3,613, respectively. Weighted event costsere then calculated by multiplying the weighted averagerst-year cost of a CHD event by the number of expectedvents.
esults
ll US Adults
A total of 2,316 subjects aged 40 to 79 years completedhe interview, examination, and fasting blood tests inHANES 1999 to 2002. Of these, 1,575 (68.0%) had suf-cient data for full ascertainment of required risk factors.fter up-weighting to account for the missing data by age
nd gender, the weighted population estimate for this groupepresents 111.5 million civilian, non-institutionalized, USdults aged 40 to 79 years (53.2 million men and 58.3illion women). The proportions of men and women aged
ver 65 years were 19.7% and 23.0%, respectively (Table).Among all men without history of CHD, the 4-year risk
f a CHD event was 3.4% if aged � 65 and 9.1% if aged 65r more years. The 4-year risk of a secondary event, in thoseith a history of CHD, was 17.9% if aged � 65 years and9.7% if aged � 65 years. In women without CHD, the-year risk of a primary event was 2.9% and 2.7% for thoseged � 65 years and � 65 years, respectively. A woman’s
isk of a secondary event increased to 5.4% if aged � 65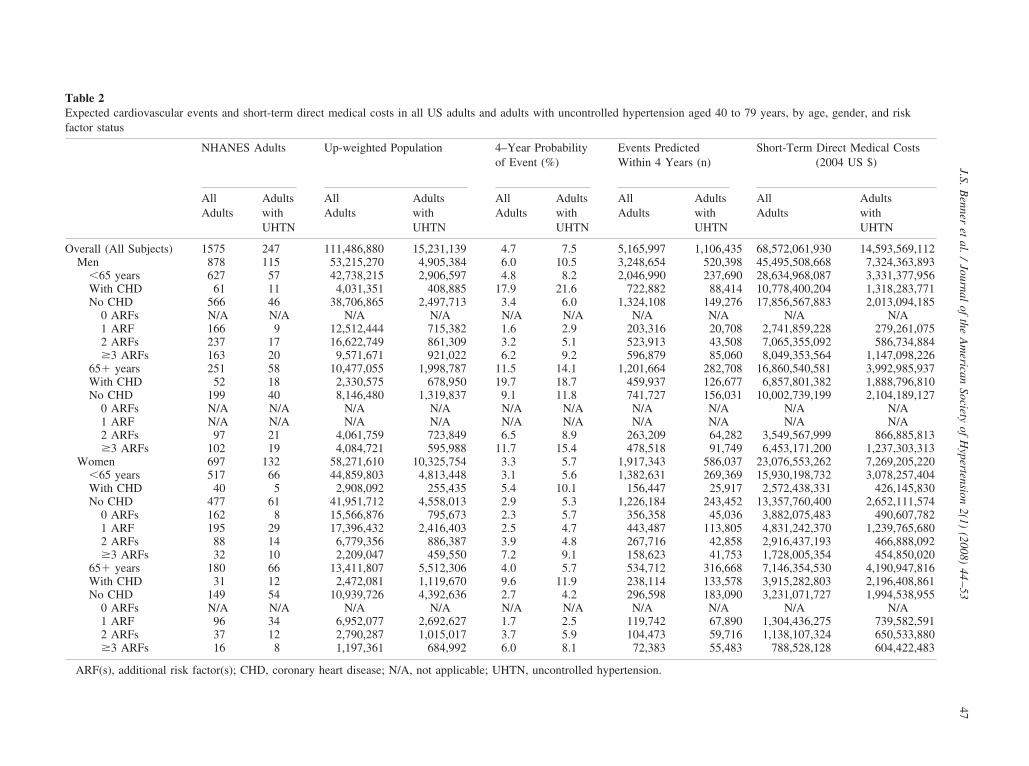
Table 2Expected cardiovascular events and short-term direct medical costs in all US adults and adults with uncontrolled hypertension aged 40 to 79 years, by age, gender, and riskfactor status
NHANES Adults Up-weighted Population 4–Year Probabilityof Event (%)
Events PredictedWithin 4 Years (n)
Short-Term Direct Medical Costs(2004 US $)
AllAdults
AdultswithUHTN
AllAdults
AdultswithUHTN
AllAdults
AdultswithUHTN
AllAdults
AdultswithUHTN
AllAdults
AdultswithUHTN
Overall (All Subjects) 1575 247 111,486,880 15,231,139 4.7 7.5 5,165,997 1,106,435 68,572,061,930 14,593,569,112Men 878 115 53,215,270 4,905,384 6.0 10.5 3,248,654 520,398 45,495,508,668 7,324,363,893
�65 years 627 57 42,738,215 2,906,597 4.8 8.2 2,046,990 237,690 28,634,968,087 3,331,377,956With CHD 61 11 4,031,351 408,885 17.9 21.6 722,882 88,414 10,778,400,204 1,318,283,771No CHD 566 46 38,706,865 2,497,713 3.4 6.0 1,324,108 149,276 17,856,567,883 2,013,094,185
0 ARFs N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A1 ARF 166 9 12,512,444 715,382 1.6 2.9 203,316 20,708 2,741,859,228 279,261,0752 ARFs 237 17 16,622,749 861,309 3.2 5.1 523,913 43,508 7,065,355,092 586,734,884�3 ARFs 163 20 9,571,671 921,022 6.2 9.2 596,879 85,060 8,049,353,564 1,147,098,226
65� years 251 58 10,477,055 1,998,787 11.5 14.1 1,201,664 282,708 16,860,540,581 3,992,985,937With CHD 52 18 2,330,575 678,950 19.7 18.7 459,937 126,677 6,857,801,382 1,888,796,810No CHD 199 40 8,146,480 1,319,837 9.1 11.8 741,727 156,031 10,002,739,199 2,104,189,127
0 ARFs N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A1 ARF N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A2 ARFs 97 21 4,061,759 723,849 6.5 8.9 263,209 64,282 3,549,567,999 866,885,813�3 ARFs 102 19 4,084,721 595,988 11.7 15.4 478,518 91,749 6,453,171,200 1,237,303,313
Women 697 132 58,271,610 10,325,754 3.3 5.7 1,917,343 586,037 23,076,553,262 7,269,205,220�65 years 517 66 44,859,803 4,813,448 3.1 5.6 1,382,631 269,369 15,930,198,732 3,078,257,404With CHD 40 5 2,908,092 255,435 5.4 10.1 156,447 25,917 2,572,438,331 426,145,830No CHD 477 61 41,951,712 4,558,013 2.9 5.3 1,226,184 243,452 13,357,760,400 2,652,111,574
0 ARFs 162 8 15,566,876 795,673 2.3 5.7 356,358 45,036 3,882,075,483 490,607,7821 ARF 195 29 17,396,432 2,416,403 2.5 4.7 443,487 113,805 4,831,242,370 1,239,765,6802 ARFs 88 14 6,779,356 886,387 3.9 4.8 267,716 42,858 2,916,437,193 466,888,092�3 ARFs 32 10 2,209,047 459,550 7.2 9.1 158,623 41,753 1,728,005,354 454,850,020
65� years 180 66 13,411,807 5,512,306 4.0 5.7 534,712 316,668 7,146,354,530 4,190,947,816With CHD 31 12 2,472,081 1,119,670 9.6 11.9 238,114 133,578 3,915,282,803 2,196,408,861No CHD 149 54 10,939,726 4,392,636 2.7 4.2 296,598 183,090 3,231,071,727 1,994,538,955
0 ARFs N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A1 ARF 96 34 6,952,077 2,692,627 1.7 2.5 119,742 67,890 1,304,436,275 739,582,5912 ARFs 37 12 2,790,287 1,015,017 3.7 5.9 104,473 59,716 1,138,107,324 650,533,880�3 ARFs 16 8 1,197,361 684,992 6.0 8.1 72,383 55,483 788,528,128 604,422,483
ARF(s), additional risk factor(s); CHD, coronary heart disease; N/A, not applicable; UHTN, uncontrolled hypertension.
47J.S.
Benner
etal.
/Journal
ofthe
Am
ericanSociety
ofH
ypertension2(1)
(2008)44
–53
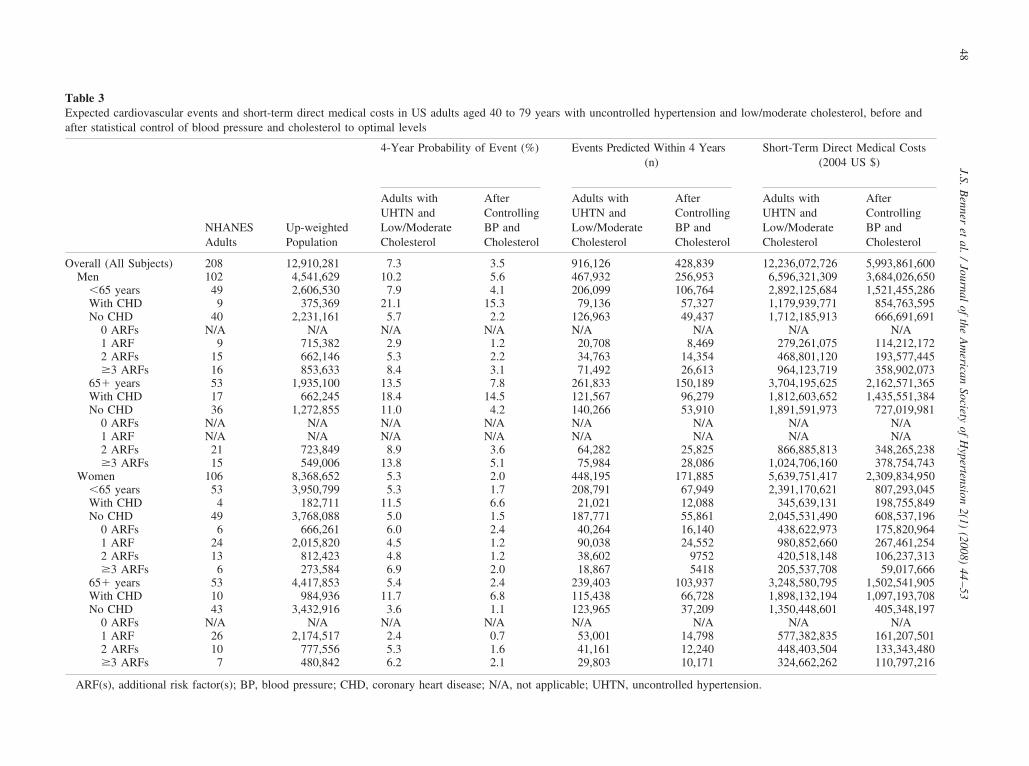
Table 3Expected cardiovascular events and short-term direct medical costs in US adults aged 40 to 79 years with uncontrolled hypertension and low/moderate cholesterol, before andafter statistical control of blood pressure and cholesterol to optimal levels
NHANESAdults
Up-weightedPopulation
4-Year Probability of Event (%) Events Predicted Within 4 Years(n)
Short-Term Direct Medical Costs(2004 US $)
Adults withUHTN andLow/ModerateCholesterol
AfterControllingBP andCholesterol
Adults withUHTN andLow/ModerateCholesterol
AfterControllingBP andCholesterol
Adults withUHTN andLow/ModerateCholesterol
AfterControllingBP andCholesterol
Overall (All Subjects) 208 12,910,281 7.3 3.5 916,126 428,839 12,236,072,726 5,993,861,600Men 102 4,541,629 10.2 5.6 467,932 256,953 6,596,321,309 3,684,026,650
�65 years 49 2,606,530 7.9 4.1 206,099 106,764 2,892,125,684 1,521,455,286With CHD 9 375,369 21.1 15.3 79,136 57,327 1,179,939,771 854,763,595No CHD 40 2,231,161 5.7 2.2 126,963 49,437 1,712,185,913 666,691,691
0 ARFs N/A N/A N/A N/A N/A N/A N/A N/A1 ARF 9 715,382 2.9 1.2 20,708 8,469 279,261,075 114,212,1722 ARFs 15 662,146 5.3 2.2 34,763 14,354 468,801,120 193,577,445�3 ARFs 16 853,633 8.4 3.1 71,492 26,613 964,123,719 358,902,073
65� years 53 1,935,100 13.5 7.8 261,833 150,189 3,704,195,625 2,162,571,365With CHD 17 662,245 18.4 14.5 121,567 96,279 1,812,603,652 1,435,551,384No CHD 36 1,272,855 11.0 4.2 140,266 53,910 1,891,591,973 727,019,981
0 ARFs N/A N/A N/A N/A N/A N/A N/A N/A1 ARF N/A N/A N/A N/A N/A N/A N/A N/A2 ARFs 21 723,849 8.9 3.6 64,282 25,825 866,885,813 348,265,238�3 ARFs 15 549,006 13.8 5.1 75,984 28,086 1,024,706,160 378,754,743
Women 106 8,368,652 5.3 2.0 448,195 171,885 5,639,751,417 2,309,834,950�65 years 53 3,950,799 5.3 1.7 208,791 67,949 2,391,170,621 807,293,045With CHD 4 182,711 11.5 6.6 21,021 12,088 345,639,131 198,755,849No CHD 49 3,768,088 5.0 1.5 187,771 55,861 2,045,531,490 608,537,196
0 ARFs 6 666,261 6.0 2.4 40,264 16,140 438,622,973 175,820,9641 ARF 24 2,015,820 4.5 1.2 90,038 24,552 980,852,660 267,461,2542 ARFs 13 812,423 4.8 1.2 38,602 9752 420,518,148 106,237,313�3 ARFs 6 273,584 6.9 2.0 18,867 5418 205,537,708 59,017,666
65� years 53 4,417,853 5.4 2.4 239,403 103,937 3,248,580,795 1,502,541,905With CHD 10 984,936 11.7 6.8 115,438 66,728 1,898,132,194 1,097,193,708No CHD 43 3,432,916 3.6 1.1 123,965 37,209 1,350,448,601 405,348,197
0 ARFs N/A N/A N/A N/A N/A N/A N/A N/A1 ARF 26 2,174,517 2.4 0.7 53,001 14,798 577,382,835 161,207,5012 ARFs 10 777,556 5.3 1.6 41,161 12,240 448,403,504 133,343,480�3 ARFs 7 480,842 6.2 2.1 29,803 10,171 324,662,262 110,797,216
ARF(s), additional risk factor(s); BP, blood pressure; CHD, coronary heart disease; N/A, not applicable; UHTN, uncontrolled hypertension.
48J.S.
Benner
etal.
/Journal
ofthe
Am
ericanSociety
ofH
ypertension2(1)
(2008)44
–53

ynn
nah
A
h(suicwwmeC
teHef
t
fuhptHoC
AM
uL�mpssepc1t
ws3
TEm
W
W
ary he
49J.S. Benner et al. / Journal of the American Society of Hypertension 2(1) (2008) 44–53
ears, and 9.6% if aged � 65 years, respectively. Overall,early 5.2 million CHD events were expected within theext 4 years among adults aged 40 to 79 years.The short-term costs of CHD events expected within the
ext 4 years were $68.6 billion. The majority of these eventsnd costs were expected to occur in patients without aistory of CHD.
dults with Uncontrolled Hypertension
Of the 1,575 NHANES subjects aged 40 to 79 years, 694ad “categorical HTN,” representing 45.0 million adults40.4% of the up-weighted adult population). Some 247ubjects (representing 15.2 million adults or 13.7% of thep-weighted population) had uncontrolled HTN as definedn the study. As shown in Table 2, this group was atonsiderably higher risk of a CHD event (7.5%) comparedith all adults (4.7%). The expected number of CHD eventsithin 4 years in those with uncontrolled HTN was 1.1illion, at a cost of $14.6 billion. Over two-thirds of these
vents were expected to occur in men and women withoutHD.Among those without CHD, the number of CV risk fac-
ors was strongly associated with expected event risk. Forxample, in women aged � 65 years with uncontrolledTN but no other risk factors, the 4-year risk of a CHD
vent was 5.3%. In the presence of three or more CV riskactors, the risk increased to 9.1%.
As male gender was considered a CV risk factor irrespec-
able 4xpected cardiovascular events and short-term direct costs in USoderate cholesterol, by CHD status and number of risk factors
NHANESAdults
Up-weightedPopulation
Adults with Uncontrand Low/Moderate C
4-YearProbabilityof CHDEvent (%)
4-YearPredicEvents(n)
ith CHD 40 1,461,632 15.9 337,16Men 26 790,715 19.4 200,70Women 14 670,917 11.7 136,45ithout CHD 168 7,209,060 5.6 578,960 ARFs 6 452,000 6.0 40,26
Men N/A N/A N/A N/AWomen 6 452,000 6.0 40,26
1 ARF 59 3,156,351 3.4 163,74Men 9 581,220 2.9 20,70Women 50 2,575,131 3.5 143,03
2 ARFs 59 2,051,854 6.1 178,80Men 36 1,068,896 7.1 99,04Women 23 982,958 5.0 79,76
�3 ARFs 44 1,548,856 9.2 196,14Men 31 1,096,227 10.4 147,47Women 13 452,629 6.5 48,67
ARF(s), additional risk factor(s); BP, blood pressure; CHD, coron
ive of age in ASCOT-LLA, the overall frequency of risk c
actors was higher in men. Of the 3.8 million men withncontrolled HTN and without CHD, 1.5 million (39.7%)ad three or more risk factors, accounting for 57.9% of allrimary CHD events among men without CHD. By con-rast, of the nearly 9.0 million women with uncontrolledTN and no CHD, 1.1 million (12.8%) had three or morether CV risk factors, accounting for 22.7% of the primaryHD events.
dults with Uncontrolled Hypertension and Low tooderate Cholesterol
Of the 15.2 million US adults aged 40 to 79 years withncontrolled HTN, 12.9 million (84.8%) met the ASCOT-LA inclusion criterion of low/moderate cholesterol (TC251 mg/dL [6.5 mmol/L]) (Table 3). The overall esti-ated 4-year probability of an expected CHD event in this
opulation was 7.3%. The subgroup of primary preventionubjects with three or more other risk factors was mostimilar to the ASCOT-LLA risk profile. This was the high-st-risk primary prevention subgroup, affecting 2.2 millionatients (16.7%) with uncontrolled HTN and low/moderateholesterol. These subjects were expected to experience96,146 CHD events within 4 years, with expected short-erm direct medical costs of $2.5 billion.
Nearly half (47.7%) of the ASCOT-LLA-like subjectsere 65 years or older; men accounted for 53% of these
ubjects. The ASCOT-LLA-like profile was present in0.9% of men with uncontrolled HTN and low/moderate
aged 40 to 79 years with uncontrolled hypertension and low/
ypertensionterol
After Adjusting BP and Cholesterol PAR%
hort-Termirectedical Costs
2004 US $)
4-YearProbabilityof CHDEvent (%)
4-YearPredictedEvents(n)
Short-TermDirectMedical Costs(2004 US $)
,236,314,749 11.1 232,421 3,586,264,536 31,992,543,423 14.8 153,606 2,290,314,979 23,243,771,325 6.7 78,815 1,295,949,557 42,999,757,977 1.9 196,417 2,407,597,065 66438,622,973 2.4 16,140 175,820,964 60
N/A N/A N/A N/A N/A438,622,973 2.4 16,140 175,820,964 60,837,496,570 1.0 47,819 542,880,927 71279,261,075 1.2 8469 114,212,172 59,558,235,495 1.0 39,350 428,668,755 72,204,608,585 2.1 62,171 781,423,476 65,335,686,933 2.9 40,179 541,842,683 59868,921,652 1.4 21,992 239,580,792 72,519,029,848 3.3 70,287 907,471,698 64,988,829,878 3.9 54,699 737,656,816 63530,199,970 2.1 15,588 169,814,882 68
art disease; N/A, not applicable; PAR, population-attributable risk.
adults
olled Hholes
tedSDM(
1 53 28 25 64
47 189 18 24 137 27 10
holesterol, 28.6% of men with uncontrolled HTN, and
2Aw7wsmyt
Aa
“c4(9eb$sr
tCff
otcbctCtt
tctup79
50 J.S. Benner et al. / Journal of the American Society of Hypertension 2(1) (2008) 44–53
.6% of all men aged 40 to 79 years. By contrast, theSCOT-LLA-like profile was present in 9.0% of womenith uncontrolled HTN and low/moderate cholesterol,.3% of women with uncontrolled HTN, and 1.3% of allomen aged 40 to 79 years. In the ASCOT-LLA-like
ubgroup, the 4-year risk of a CHD event was 8.4% inen aged � 65 years, and 13.8% in men aged � 65
ears. Similarly, women had a risk of 6.9% and 6.2% forhose aged � 65 years and 65 � years, respectively.
fter Statistical Control of Blood Pressurend Cholesterol
When blood pressure and cholesterol were statisticallycontrolled” to optimum levels in the population with un-ontrolled HTN and low/moderate cholesterol, the overall-year risk of CHD events declined from 7.3% to 3.5%Table 3). The expected number of events decreased from16,126 to 428,839, resulting in a PAR% of 53%. Thexpected initial cost of these events was reduced from $12.2illion to under $6.0 billion, indicating that an excess cost of6.2 billion was attributable to these risk factors. Among theubgroup of subjects without CHD and with three or more
Figure 1. Study inclusion/exclu-sion criteria and National Healthand Nutrition Examination Survey(NHANES) population estimates.ARFs, additional risk factors; CVD,cardiovascular disease; HTN, hyper-tension.
isk factors, the PAR% was 64% (Table 4). By comparison, c
he PAR% was 31% among subjects with pre-existingHD. Regardless of the CHD history and number of risk
actors, the PAR% was considerably higher for women thanor men.
Figure 2 illustrates the sensitivity analyses on the levelsf blood pressure and cholesterol achieved in the popula-ion. When subjects were assumed to attain only borderlineontrol of blood pressure and cholesterol, the expected num-er of events among primary prevention patients with un-ontrolled HTN and three or more risk factors was morehan double compared with those of optimal control levels.onversely, attaining “intensive” control further lowered
he event rates appreciably, compared with “optimal” con-rol.
Additional sensitivity analysis was performed to examinehe impact of controlling blood pressure only, as opposed toontrolling both blood pressure and cholesterol. When con-rolling blood pressure to optimum levels in adults withncontrolled HTN and low/moderate cholesterol, the 4-yearrobability of an expected CHD event was reduced from.3% to 4.7%. The number of events was reduced from16,126 to 580,243, a PAR% of 37%. The expected initial
ost of these events was reduced from $12.2 to $8.1 billion.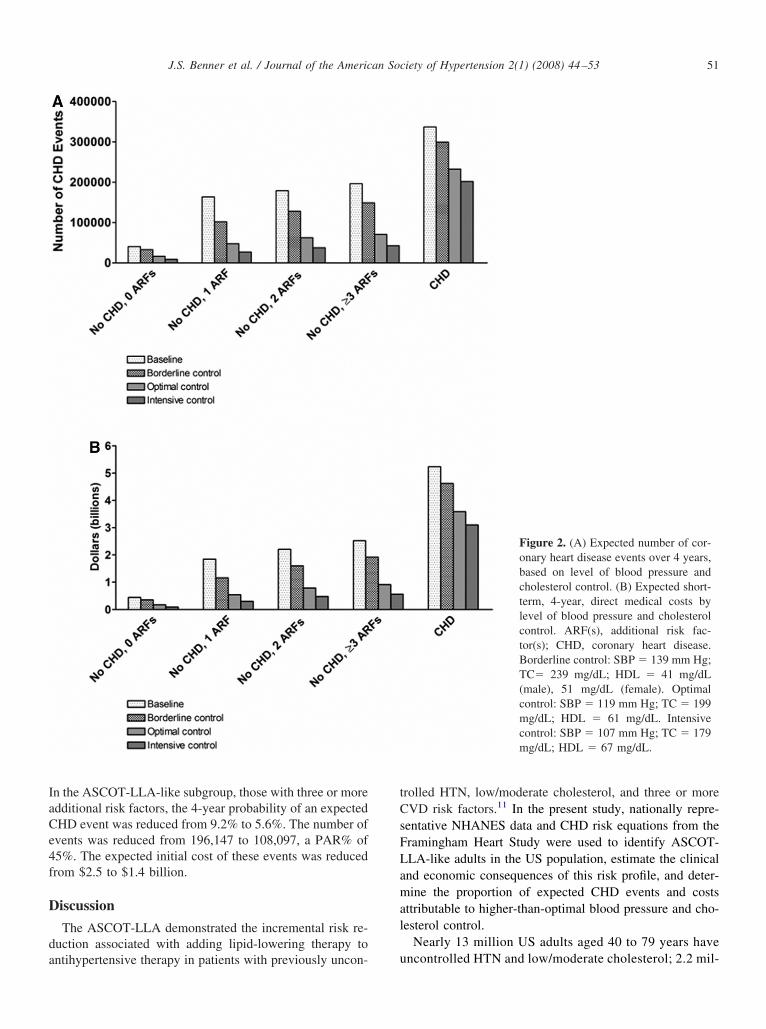
IaCe4f
D
da
tCsFLamal
51J.S. Benner et al. / Journal of the American Society of Hypertension 2(1) (2008) 44–53
n the ASCOT-LLA-like subgroup, those with three or moredditional risk factors, the 4-year probability of an expectedHD event was reduced from 9.2% to 5.6%. The number ofvents was reduced from 196,147 to 108,097, a PAR% of5%. The expected initial cost of these events was reducedrom $2.5 to $1.4 billion.
iscussion
The ASCOT-LLA demonstrated the incremental risk re-uction associated with adding lipid-lowering therapy to
ntihypertensive therapy in patients with previously uncon- urolled HTN, low/moderate cholesterol, and three or moreVD risk factors.11 In the present study, nationally repre-
entative NHANES data and CHD risk equations from theramingham Heart Study were used to identify ASCOT-LA-like adults in the US population, estimate the clinicalnd economic consequences of this risk profile, and deter-ine the proportion of expected CHD events and costs
ttributable to higher-than-optimal blood pressure and cho-esterol control.
Nearly 13 million US adults aged 40 to 79 years have
Figure 2. (A) Expected number of cor-onary heart disease events over 4 years,based on level of blood pressure andcholesterol control. (B) Expected short-term, 4-year, direct medical costs bylevel of blood pressure and cholesterolcontrol. ARF(s), additional risk fac-tor(s); CHD, coronary heart disease.Borderline control: SBP � 139 mm Hg;TC� 239 mg/dL; HDL � 41 mg/dL(male), 51 mg/dL (female). Optimalcontrol: SBP � 119 mm Hg; TC � 199mg/dL; HDL � 61 mg/dL. Intensivecontrol: SBP � 107 mm Hg; TC � 179mg/dL; HDL � 67 mg/dL.
ncontrolled HTN and low/moderate cholesterol; 2.2 mil-

lrtaawfieuwwcsHanb
tLbwtmriortciTec
oFpmtttcCebcscrwnolr
pwseaNt
thaaspaliwC
A
rE
R
52 J.S. Benner et al. / Journal of the American Society of Hypertension 2(1) (2008) 44–53
ion of these are free of CHD but have three or more CVisk factors. In men and women younger than 65 years,he ASCOT-LLA risk profile is considerably more prev-lent than in those with a history of CHD, and contributespproximately the same number of predicted eventsithin 4 years. By conservative estimates, using only therst-year costs of treating a CHD event, the overallconomic burden of CHD events in all US adults withncontrolled HTN and low/moderate cholesterol levelsill be $12.2 billion within the next 4 years; for patientsithout CHD but with three or more risk factors, the
osts will be $2.5 billion. The PAR% for patients mostimilar to those in ASCOT-LLA, those with uncontrolledTN, low/moderate cholesterol levels, and three or more
dditional risk factors, was 64%, which suggests thatearly 2 out of 3 expected events in this population wille attributable to elevated blood pressure and cholesterol.This study also helps give a population-level context to
he clinical findings of ASCOT-LLA trial. In ASCOT-LA, 10,305 patients with uncontrolled HTN, average orelow-average cholesterol, and three or more risk factorsere treated with one of two antihypertensive medica-
ions and randomly assigned to receive atorvastatin 10g or placebo. Sever and colleagues observed a 36%
elative risk reduction (hazard ratio 0.62, 95% confidencenterval [CI], 0.47 to 0.81) in nonfatal MI and fatal CHDver a median follow-up of 3.3 years.11 In this study, theelative risk reduction resulting from controlling choles-erol levels in addition to blood pressure as opposed toontrolling blood pressure only was estimated to be 36%n the subgroup with the ASCOT-LLA-like risk profile.herefore, the higher PAR% we observed is a plausiblestimate of the benefit to be gained from optimizing bothholesterol and blood pressure.
The results of this study should be interpreted in lightf some limitations. Specifically, risk equations from theramingham Heart Study may not accurately predict theotential risk reduction that could be achieved by opti-izing blood pressure and cholesterol because the equa-
ions are based on baseline measurements of risk fac-ors.15 In addition, the protective benefits of cholesterolreatments such as statins are not fully explained byhanges in cholesterol, which suggests they lower risk ofVD events through unrelated mechanisms.21 Thus, ourstimate of the potential benefits associated with treatinglood pressure and cholesterol to optimal levels may beonservative. Similarly, our cost estimates are also con-ervative because they are based only on the first year ofare following a CHD event, and the best available dataeflect the costs of treating CHD in the mid 1990s. Whilee have inflated those costs to present dollars, new tech-ologies, and patterns of care may have changed the costf treating CHD in the past decade. Another potentialimitation of this study was the prevalence of missing
isk-factor data in the NHANES database. In order toroject to the full US adult population, we further up-eighted the number of adults represented by NHANES
ubjects using age- and gender-specific constants. How-ver, the results were similar when we restricted thenalysis to the subset of US adults represented byHANES subjects with complete data, suggesting that
his procedure did not systematically bias the results.Our findings have several important implications for pa-
ient care. Physicians should be aware that uncontrolledypertension is a prevalent condition that places patients atmore than 50% greater risk of CHD than unaffected
dults, even in the absence of elevated cholesterol. Aggres-ive screening for the presence of additional risk factors inrimary prevention patients is justified by the high numbernd cost of CHD events that will occur in the ASCOT-LLA-ike subgroup within the next 4 years. Population-levelmplementation of the ASCOT-LLA treatment protocolould be expected to prevent a substantial fraction of theseHD events (Figure 2).
cknowledgments
Editorial assistance with the formatting of the Tables andedrawing of the Figures was provided by Jon Edwards ofnvision Pharma and funded by Pfizer Inc.
eferences
1. Rosamond W, Flegal K, Friday G, Furie K, Go A,Greenlund K, et al, American Heart Association Statis-tics Committee and Stroke Statistics Subcommittee.Heart disease and stroke statistics––2007 update: a re-port from the American Heart Association StatisticsCommittee and Stroke Statistics Subcommittee [Erra-tum in: Circulation 2007;115:e172]. Circulation 2007;115:e69–171.
2. Greenland P, Knoll MD, Stamler J, Neaton JD, DyerAR, Garside DB, et al. Major risk factors as antecedentsof fatal and nonfatal coronary heart disease events.JAMA 2003;290:891–7.
3. Hajjar I, Kotchen TA. Trends in prevalence, awareness,treatment, and control of hypertension in the UnitedStates, 1988–2000. JAMA 2003;290:199–206.
4. Chobanian AV, Bakris GL, Black HR, Cushman WC,Green LA, Izzo JL Jr, et al. The Seventh Report of theJoint National Committee on Prevention, Detection,Evaluation, and Treatment of High Blood Pressure: theJNC 7 report. JAMA 2003;289:2560–72.
5. Ford ES, Mokdad AH, Giles WH, Mensah GA. Serumtotal cholesterol concentrations and awareness, treat-ment, and control of hypercholesterolemia among USadults: findings from the National Health and NutritionExamination Survey, 1999 to 2000. Circulation 2003;
107:2185–9.
1
1
1
1
1
1
1
1
1
1
2
2
53J.S. Benner et al. / Journal of the American Society of Hypertension 2(1) (2008) 44–53
6. Law MR, Wald NJ, Rudnicka AR. Quantifying effectof statins on low density lipoprotein cholesterol, isch-aemic heart disease, and stroke: systematic review andmeta-analysis. BMJ 2003;326:1423–6.
7. Turnbull F. Effects of different blood-pressure-lower-ing regimens on major cardiovascular events: results ofprospectively-designed overviews of randomised trials.Lancet 2003;362:1527–35.
8. Julius S, Kjeldsen SE, Weber M, Brunner HR, EkmanS, Hansson L, et al. Outcomes in hypertensive patientsat high cardiovascular risk treated with regimens basedon valsartan or amlodipine: the VALUE randomizedtrial. Lancet 2004;363:2022–31.
9. Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr,Clark LT, Hunninghake DB, et al. Implications of re-cent clinical trials for the National Cholesterol Educa-tion Program Adult Treatment Panel III Guidelines.J Am Coll Cardiol 2004;44:720–32.
0. LaRosa JC, Grundy SM, Waters DD, Shear C, Barter P,Fruchart JC, et al. Intensive lipid lowering with atorva-statin in patients with stable coronary disease. N EnglJ Med 2005;352:1425–35.
1. Sever PS, Dahlöf B, Poulter NR, Wedel H, Beevers G,Caulfield M, et al. Prevention of coronary and strokeevents with atorvastatin in hypertensive patients whohave average or lower-than-average cholesterol con-centrations, in the Anglo-Scandinavian Cardiac Out-comes Trial-Lipid Lowering Arm (ASCOT-LLA): amulticentre randomized controlled trial. Lancet 2003;361:1149–58.
2. Centers for Disease Control and Prevention. NationalHealth and Nutrition Examination Survey DataNHANES (1999–2000). National Center for HealthStatistics (NCHS), Department of Health and HumanServices. Available at: http://www.cdc.gov/nchs/about/major/nhanes/nhanes99_00.htm. Accessed Date: Janu-ary 13, 2005.
3. Centers for Disease Control and Prevention. NationalHealth and Nutrition Examination Survey Data
NHANES (2001–2002). National Center for HealthStatistics (NCHS), Department of Health and HumanServices. Available at: http://www.cdc.gov/nchs/about/major/nhanes/nhanes01-02.htm. Accessed Date: Janu-ary 13, 2005.
4. Centers for Disease Control and Prevention. National Healthand Nutrition Examination Survey Analytic Guidelines. Na-tional Center for Health Statistics (NCHS), Department ofHealth and Human Services. Available at: http://www.cdc.gov/nchs/data/nhanes/nhanes_general_guidelines_june_04.pdf. Accessed Date: January 13, 2005.
5. D’Agostino RB, Russell MW, Huse DM, Ellison RC,Silbershatz H, Wilson PW, et al. Primary and subse-quent coronary risk appraisal: new results from theFramingham Study. Am Heart J 2000;139:272–81.
6. Executive Summary of The Third Report of The Na-tional Cholesterol Education Program (NCEP) ExpertPanel on Detection, Evaluation, And Treatment of HighBlood Cholesterol In Adults (Adult Treatment PanelIII). JAMA 2001;285:2486–97.
7. Wong ND, Pio JR, Franklin SS, L’Italien GJ, KamathTV, Williams GR. Preventing coronary events by op-timal control of blood pressure and lipids in patientswith the metabolic syndrome. Am J Cardiol 2003;91:1421–6.
8. Wong ND, Thakral G, Franklin SS, L’Italien GJ, Ja-cobs MJ, Whyte JL, et al. Preventing heart disease bycontrolling hypertension: impact of hypertensive sub-type, stage, age, and sex. Am Heart J 2003;145:888–95.
9. Russell MW, Huse DM, Drowns S, Hamel EC, HartzSC. Direct medical costs of coronary artery disease inthe United States. Am J Cardiol 1998;81:1110–5.
0. US Department of Labor Bureau of Labor Statistics.Consumer Price Index – All Urban Consumers – Med-ical Care. Available at: www.bls.gov/cpi/home.htm.Accessed Date: October 26, 2005.
1. West of Scotland Coronary Prevention Study Group.Influence of pravastatin and plasma lipids on clinicalevents in the West of Scotland Coronary Prevention
Study (WOSCOPS). Circulation 1998;97:1440–5.Copyright © 2022 FDOKUMEN
















![Astrocytic tracer dynamics estimated from [1-11C]-acetate PET measurements](https://static.fdokumen.com/doc/165x107/6334cca03e69168eaf070c95/astrocytic-tracer-dynamics-estimated-from-1-11c-acetate-pet-measurements.jpg)



