On valuing and hedging European options when volatility is estimated directly
Upload
independentCategory
view
1download
0
The FASEB Journal • Research Communication
Erythropoietin directly stimulates osteoclast precursorsand induces bone loss
Sahar Hiram-Bab,*,† Tamar Liron,† Naamit Deshet-Unger,* Moshe Mittelman,‡ Max Gassmann,§
Martina Rauner,{ Kristin Franke,|| Ben Wielockx,|| Drorit Neumann,*,1 and Yankel Gabet†,1
*Department of Cell and Developmental Biology, †Department of Anatomy and Anthropology, and‡Department of Medicine, Tel Aviv Sourasky Medical Center, Sackler Faculty of Medicine, Tel-AvivUniversity, Tel-Aviv, Israel; §Institute of Veterinary Physiology, Vetsuisse Faculty, and Zurich Center forIntegrative Human Physiology, University of Zurich, Zurich, Switzerland; {Department of Medicine III,Dresden University Medical Center, Dresden, Germany; and ||Institute of Pathology, University ofTechnology, Dresden, Germany
ABSTRACT Erythropoietin (EPO) primarily regulatesred blood cell formation, and EPO serum levels are in-creased on hypoxic stress (e.g., anemia and altitude). Inaddition to anemia, recent discoveries suggest new thera-peutic indications for EPO, unrelated to erythropoiesis.We investigated the skeletal role of EPO using severalmodels of overexpression (Tg6 mice) and EPO adminis-tration (intermittent/continuous, high/low doses) in adultC57Bl6 female mice. Using microcomputed tomography,histology, and serummarkers, we found that EPO induceda 32%–61% trabecular bone loss caused by increased boneresorption (+60%–88% osteoclast number) and reducedbone formation rate (219 to274%; P < 0.05 throughout).EPO targeted the monocytic lineage by increasing thenumberof bonemonocytes/macrophages, preosteoclasts,and mature osteoclasts. In contrast to the attenuated boneformation in vivo, EPO treatment in vitro did not inhibitosteoblast differentiation and activity, suggesting an in-direct effect of EPO on osteoblasts. However, EPO had adirect effect on preosteoclasts by stimulating osteoclasto-genesis in isolated cultures (+60%) via the Jak2 and PI3Kpathways. In summary, ourfindings demonstrate that EPOnegatively regulates bone mass and thus bears significantclinical implications for the potential management ofpatients with endogenously or therapeutically elevatedEPO levels.—Hiram-Bab, S., Liron, T., Deshet-Unger, N.,Mittelman, M., Gassmann, M., Rauner, M., Franke, K.,Wielockx, B., Neumann, D., Gabet, Y. Erythropoietin di-rectly stimulates osteoclast precursors and induces boneloss. FASEB J. 29, 000–000 (2015). www.fasebj.org
Key Words: Tg6 mice • bone turnover • osteoclastogenesis •
macrophages • trabecular bone
ERYTHROPOIETIN (EPO) is best known for its function as anerythropoietic hormone secreted from the kidneys of
adult mammals. The main trigger of EPO secretion ishypoxia, resulting fromblood loss, anemia, or on exposureto high altitude. EPO binding to its cell surface receptor(EPO-R) results in downstream phosphorylation of theJanus kinase (JAK)/signal transducer and activatorof transcription (STAT), PI3K/Akt, MAP kinase, andprotein kinase C to facilitate the production of eryth-rocytes (1, 2).
Recombinant human EPO (rHuEPO) is used in clinicalpractice for the treatment of several types of anemia, in-cluding anemia of end-stage renal disease (3–5) andchemotherapy-induced anemia (6). It is also illegally ad-ministered as a performance-enhancing drug in athletes(7).Unrelated to its primary erythropoietic function, EPO-R is expressed in diverse tissues including the brain, re-productive organs, placenta, heart, lungs, intestine, spleen,and bone (8–13). In line with these findings, new thera-peutic indications of EPO were recently suggested for themanagement of nephropathies, ischemic injuries of sev-eral tissues such as intestine, pancreas, and myocardium,neuropathies, liver regeneration, adipose tissue in-flammation, and diabetic retinopathy (10, 13–22). Over-all, the ubiquitous expression of EPO-R in nonerythroidcells associated with a plethora of nonhematopoieticfunctions has recently prompted the experimental evalua-tion of a vast array of potential future applications of EPOand its derivatives in the clinic.
In bone, osteoclasts are specialized cells derived frommonocytes; they adhere to the bone matrix and secreteacid and lytic enzymes to resorb bone (23). Monocytedifferentiation into osteoclasts is driven by the receptoractivator for nuclear factor kB (RANK)/RANK ligand(RANKL)/osteoprotegerin system, and M-CSF (24, 25).Osteoblasts derived from mesenchymal stem cells are
Abbreviations: ALP, alkaline phosphatase; BFR, bone for-mation rate; BSP, bone sialoprotein; BV/TV, bone volume/total volume or trabecular bone fraction; Conn.D, connectiv-ity density; mCT, microcomputed tomography; EPO, erythro-poietin; EPO-R, erythropoietin receptor; FBS, fetal bovineserum; JAK, Janus kinase; MAR, mineral apposition rate;
(continued on next page)
1 Correspondence: D.N., Department of Cell and De-velopmental Biology, Sackler Faculty of Medicine, Tel AvivUniversity, PO Box 39040, Tel Aviv 69978, Israel. E-mail:[email protected]; Y.G., Department of Anatomy and An-thropology, Sackler Faculty of Medicine, Tel Aviv University, POBox 39040, Tel Aviv 69978, Israel. E-mail: [email protected]: 10.1096/fj.14-259085This article includes supplemental data. Please visit http://
www.fasebj.org to obtain this information.
0892-6638/15/0029-0001 © FASEB 1
The FASEB Journal article fj.14-259085. Published online January 28, 2015.

responsible for bone formation. A tight regulation be-tween the osteoblastic and osteoclastic lineages is thuscrucial for the control of bone turnover (26).
Evidenceof adirect effect ofEPOonbonemetabolism islimited, and the few reports available are controversial.EPO was reported to support bone formation in fracturehealing models (27–29). Similarly, in newborn and grow-ing mice, EPO administration increased bone mass by in-ducing bone formation (30), but in contrast, EPO wasshown to induce bone loss in adultmice (31, 32). Thus, theexact role of EPO in bone metabolism and its mechanismof action remain to be elucidated.
In this work we tested the hypothesis that high EPOlevels induce bone resorption in a model of high endoge-nous EPO levels (transgenic mice constitutively overex-pressing human EPO) and in a therapeutic model(EPO-administered mice), via EPO-R signaling in themonocytic lineage. Our previous findings of EPO-Rs onmacrophages (33) coupled to the fact that these cells arethe precursors of osteoclasts directed particular emphasisto this cell lineage.
MATERIALS AND METHODS
Materials
All reagents were purchased from Sigma-Aldrich (St. Louis, MO,USA) unless otherwise specified. a-MEM, DMEM, and fetal bo-vine serum (FBS) were purchased from Rhenium (Modiin,Israel), and culture plates were from Corning (New York, NY,USA). As a source of M-CSF, we used supernatant from CMG 14-12 cells, containing 1.3 mg/ml M-CSF (25). To inhibit cellularsignaling pathways, we used LY294002 (Promega, Madison, WI,USA), U0126 (Cell Signaling, Danvers, MA, USA), and AG490(Sigma-Aldrich).
Animals
All experiments were approved by the Institutional Animal Careand Use Committee of Tel Aviv University. This study was per-formed on femalemice. Tg6mice (34) bred on a pure C57BL/6Jbackground were compared with their littermate controls at12 weeks of age. In the experiment assessing the effect of lowEPO doses, wild-type (WT) animals were injected with 30 UrHuEPO (Epoietin a, Eprex; Janssen-Cilag, High Wycombe,United Kingdom) or diluent (saline) for 10 consecutive days,followed by 3 injections/wk for 3 weeks (30U-inj). In anotherexperiment, 180 U rHuEPO or diluent was injected 3 times/wkfor 2.5 weeks (180U-inj). For continuous administration ofEPO, we implanted Alzet osmotic pumps (Cupertino, CA,USA) releasing 7 U/d (or saline) for 10 days. These doses(30, 180, and 7 U per animal) correspond to 1500, 9000, and350 U/kg, respectively.
Serum markers
At death, blood was collected, and levels of biochemical markerswere measured in the serum. ELISA kit for tartrate-resistant acidphosphatase (TRAP)5bwas purchased from ImmunoDiagnosticSystems (Boldon, United Kingdom). The mouse osteocalcindetection kit was purchased from Biomedical Technologies(Ward Hill, MA, USA).
Microcomputed tomography
Femora (1permouse)wereexaminedas reportedpreviously (35,36) using the microcomputed tomography (mCT) 50 system(Scanco Medical AG, Bruttisellen, Switzerland). Briefly, scanswere performed at a 10 mm resolution. The mineralized tissueswere segmented by a global thresholding procedure (37). Tra-becular bone parameters were measured in the secondary spon-giosa of the distal femoral metaphysis, and cortical parameterswere determined in the middiaphyseal region according to thestandardized nomenclature (38).
Histomorphometry
Mice were injected intraperitoneally with calcein 4 and 1 daysbefore death to assess bone formation (35). Following mCT, dy-namic histomorphometric measurements and osteoclast TRAPstaining were performed on undecalcified specimens as de-scribed previously (35) using Media Cybernetic ImagePro soft-ware (Rockville, MD, USA). The terminology and units used forthese measurements were according to the 2012 convention ofstandardized nomenclature (39).
Cell culture
Bonemarrow cells were harvested from femurs and tibias of 8- to12-week-old mice, and cells were seeded on tissue cultured-treated plates in standard medium (a-MEM, 10% FBS). On thefollowing day, nonadherent cells were seeded in non–tissueculture-treated plates in standard medium supplemented with100 ng/ml M-CSF, which induced differentiation into pre-osteoclasts. For the differentiation assay, preosteoclasts wereplated in 96-well plates (6000 cells per well) with standard me-dium supplementedwith 20 ng/mlM-CSF and 50ng/mlRANKL(R&D Systems, Minneapolis, MN, USA), replaced every 2 days.On day 6, multinucleated osteoclasts were stained using a TRAPkit (Sigma-Aldrich), and relative TRAP-positive surface was mea-suredusingImageJsoftware(National InstitutesofHealth,Bethesda,MD, USA). Pit resorption was performed as above on calciumphosphate-coated plates according to the manufacturer’s in-structions (CosmoBio, Tokyo, Japan). To calculate the resorbedarea/osteoclasts area, a parallel experiment was carriedout underthe same conditions, namely, cells were seeded on a 48-well plasticplate (Greiner Bio-One, Monroe, NC, USA) in phenol-red freemedium, with only one medium change on day 3. After 6 days,cells were removed, and micrographs were taken. Total area ofresorbedpits was alsomeasuredusing ImageJ software, and thepitarea was divided by the osteoclast area. For the proliferation assay,preosteoclasts were plated with standard medium supplementedwith 100 ng/mlM-CSF, and after 3 days, the number of viable cellswas assessed using the thiazolyl blue tetrazolium bromide assay aspreviously described (33, 36).
Calvarial osteoblasts cultures were prepared from 2-day-oldpups as described previously (40). To induce osteoblast differ-entiation,osteogenicmediumcontainingascorbicacid (50mg/ml)and b-glycerophosphate (10 mM) was initiated at confluence,and alizarin red staining was performed at day 20 to measuremineralization.
(continued from previous page)MS/BS, mineralizing surface/bone surface; N.Oc/BS, osteo-clast number/bone surface; OCN, osteocalcin; R, receptor;RANK, receptor activator of nuclear factor kB; RANKL, re-ceptor activator of nuclear factor kB ligand; rHuEPO,recombinant human EPO; Tb.N, trabecular number; TRAP,tartrate-resistant acid phosphatase; WT, wild-type
2 Vol. 29 May 2015 HIRAM-BAB ET AL.The FASEB Journal x www.fasebj.org

mRNA expression
RNA from cells was extracted using an RNA purification kit (5PRIME, Gaithersburg, MD, USA). cDNA was produced using theHigh Capacity cDNA Reverse Transcription Kit (Invitrogen,Grand Island, NY, USA), and real-time PCR was performed usingKapa SYBR Fast qPCR (Kapa Biosystems, Wilmington, MA, USA)andaStepOnereal timePCRmachine(AppliedBiosystems,GrandIsland,NY,USA). Primers used for PCRwere as follows (F, forward;R, reverse): alkaline phosphatase (ALP), F GGAATACGAAC-TGGATGAGAAGG; ALP, R GGTTCCAGACATAGTGGGAATG ;osteocalcin (OCN), F CCAAGCAGGAGGGCAATA ; OCN, R AG-GGCAGCACAGGTCCTAA; Actin, F CCGTCAGGCAGCTCATA-GCTC; Actin, R GTCACCCACACTGTGCCCATC; hypoxanthinephosphoribosyltransferase, F TCCTCCTCAGACCGCTTTT; hypo-xanthine phosphoribosyltransferase, R CCTGGTTCATCAGCGC-TAATC; bone sialoprotein (BSP), F CGGCCACGCTACTTTCTT-TA; BSP, R GAACTATCGCCGTCTCCATTT; EPO-R, F CCCCTC-TGTCTCCTACTT; EPO-R, R GTTGGGTGAAGCACAGAAGTT.
FACS analyses
To determine the cell distribution in bone marrow, cells flushedfrom 1 femur and red blood cells were lysed using ACK lysisbuffer (Quality Biologic, Gaithersburg, MD, USA). Blockingwas performed with 2% FBS. For cells in cultures, cells weredetached with trypsin. Then, an aliquot of 1 3 106 cells wasstainedwith labeled antibodies: allophycocyanin-conjugated anti-mouse M-CSF receptor (M-CSF-R, a.k.a. CD115 and CSF1-R);phycoerythrin-conjugated anti-mouse RANK (CD265) anti-bodies, FITC-conjugated anti-mouse TER119, phycoerythrin-conjugated anti-mouse B220, FITC-conjugated anti-mouseCD3, and allophycocyanin-conjugated anti-mouse IgM (eBio-sciences, San Diego, CA,USA). Cells were fixed with 1% para-formaldehyde and analyzed on a Gallios flow cytometer(Beckman Coulter, Brea, CA, USA; for cells from Tg6 vs. WTanimals) and on a FACSortmachine (BDBiosciences, San Jose,CA, USA; for cells from EPO- or diluent-injected animals).
Western blotting
Western blot was performed as previously described (33). Briefly,preosteoclasts were seeded in 6-well plates with osteoclastogenicmedium for 18 hours. Cells were thenwashed twicewith PBS, andfresh medium with no supplements was added. EPO (10 U/ml)wasadded60or10minutesbeforecell lysis performedon ice.Theantibodies for Erk and Phospho-Erk were from Santa Cruz Bio-technology, Santa Cruz, CA, USA; phospho-Jak2 and phospho-Akt were from Cell Signaling.
Statistical analysis
Values are expressed as mean 6 SEM unless otherwise indicated.All statistical analyses were performed using IBM SPSS, version21 software (IBM, Armonk, NY, USA). The Student t test (for2 groups only) or ANOVA and Tukey’s post hoc test (for multiplegroups comparison) were used. Difference between groups wasdefined as P, 0.05.
RESULTS
Low bone mass phenotype in EPO-overexpressing mice
In view of the controversially reported effects of EPO inbone remodeling (27, 28, 30, 31, 41), we first investigated
the bone phenotype of mice constitutively overexpressinghuman EPO in an oxygen-independent manner (Tg6mice). These mice are mainly characterized by excessiveerythrocytosis and splenomegaly (34) and are used here asa model for pathophysiologic increase in the endogenousproduction of the hormone. EPO levels in the serum ofTg6 mice were;29-fold higher than in WT (312.46 93.1vs. 10.86 2.1 mU/ml, P, 0.0001, n = 8). mCT analysis of12-week-old Tg6 female mice revealed a low bone massphenotype comparedwith littermate controls (Fig. 1). Thetrabecular bone fraction (BV/TV) measured in the distalfemur metaphysis of Tg6 mice was 61% lower than in WTcontrols. This was associatedwith a reduction in trabecularnumber (Tb.N) and connectivity density (Conn.D), butnot in the mean trabecular thickness. We also found thatthe bone loss was markedly greater in the proximal partof the distal metaphysis (2100% in BV/TV) comparedwith the distal part (261%) that is closer to the growthplate (Supplemental Fig. S1). No difference was observedin the femoral length and middiaphyseal diameter, but
Figure 1. Transgenic mice overexpressing EPO exhibittrabecular bone loss. A) mCT analysis of the distal femoraltrabecular bone of 5 transgenic mice Tg6 and 7 WT; 12-week-old female mice were tested. Data are mean 6 SEM. *P , 0.05compared with controls, t test. B) mCT images of distalfemoral trabecular bone of WT (left) vs. Tg6 (right) mice withmedian BV/TV values.
ERYTHROPOIETIN STIMULATES BONE RESORPTION 3

both cortical thickness and moment of inertia were lowerin the Tg6 animals (Table 1).
Increased bone resorption and reduced boneformation in EPO-overexpressing mice
In pursuit of the cellular mechanism underlying the lowbonemassphenotypeofTg6mice,wemeasured indicatorsof bone resorption and bone formation in vivo. First, weenumerated differentiated osteoclasts on trabecular bonesurfaces using TRAP staining of histologic sections andfound that Tg6mice had a 25% higher osteoclast numberper bone surface (N.Oc/BS) compared with WT controls(Fig. 2A, B). Further implicating bone resorption in thislow bone mass phenotype, Tg6 mice exhibited a 28% in-crease in the serum levels of TRAP5b (Fig. 2C), a bio-chemical marker of bone resorption.
Because previous reports suggested a possible role forEPO in cells of the osteoblast lineage (30, 41, 42), we alsotested whether the low bone mass phenotype in Tg6 micewas associated with reduced bone formation. We used vital
double calcein labeling to assess bone matrix apposition invivo.Althoughthemineralizing surface(MS/BS,a surrogatefor osteoblast number) was not affected, serumOCN levels,mineral apposition rate (MAR, a surrogate for osteoblastactivity), andoverall bone formation rate (BFR/BS)were allreduced in the EPO-overexpressing animals (Fig. 2D–G).
EPO administration induces bone loss in adult mice
To assess the therapeutic effect of short-term intermittentadministration of the hormone, we then investigated theeffect of EPO injections on bone metabolism. In line withour findings on Tg6 mice, injections of low doses ofrHuEPO (30U-inj) resulted in a significant trabecularbone loss (Fig. 3). The trabecular bone fraction was 51%lower than in the diluent-injected controls. The micro-architectural changes were also similar to the Tg6 mice,showing a reduction in Tb.N (263%) and Conn.D(259%), whereas the mean thickness of the remaining tra-beculae was slightly increased (+11%). Again, bone loss wasmarkedly greater in the proximal part (295% in BV/TV)
TABLE 1. EPO has a mild effect on cortical thickness
Parameter WT Tg6 Diluent EPO
Femoral length (mm) 13.74 6 1.02 13.74 6 0.47 14.04 6 0.67 14.21 6 0.67Diaphyseal diameter (mm) 1.116 6 0.086 0.802 6 0.153 1.205 6 0.311 1.269 6 0.097Cortical thickness (mm) 0.146 6 0.005 0.125 6 0.010* 0.151 6 0.003 0.143 6 0.004Moment of inertia (mm24) 0.377 6 0.031 0.265 6 0.050* 0.269 6 0.011 0.271 6 0.011
Femoral length and cortical parameters from the same animals as in Figs. 1 and 3. Data are mean 6SEM. *P , 0.05 vs. control, t test.
Figure 2. Increased osteoclastogenesis and reduced bone formation in transgenic mice overexpressing the EPO gene. A)Histologic images showing increased osteoclast number in the distal femur of representative WT (left) and Tg6 (right) animals.Images were acquired at 310 magnification. B) N.Oc/BS: TRAP+ lining osteoclasts relative to bone surface measured inhistologic sections of the distal femur from 5 WT and 4 Tg6 mice. C) Serum TRAP5b levels in 7 WT and 7 Tg6 mice. D–G)Parameters of bone formation were measured in histologic sections of the distal femur from 5 WT and 4 Tg6 mice. D) MARvalues indicated below representative histologic images showing calcein double-labeled trabeculae in the distal femur of WT andTg6 animals. Images were acquired at 310 magnification. E) MS/BS, mineralizing surface. F) BFR/BS, bone formation rate. G)Serum osteocalcin level, n = 8. Data are mean 6 SEM. *P , 0.05 compared with controls, t test.
4 Vol. 29 May 2015 HIRAM-BAB ET AL.The FASEB Journal x www.fasebj.org

of the distal metaphysis compared with the distal part(251%; Supplemental Fig. S1), and no changes wereobserved in the femoral length (Table 1). In contrast withthe Tg6 mice, short-term EPO administration did not af-fect the middiaphyseal diameter and cortical thickness(Table 1). Of note, higher intermittently administereddosage of rHuEPO (180U-inj) resulted in a similar skeletalresponse, with 48% lower BV/TV, 62% lower Tb.N, 57%lower Conn.D, and 18% higher Tb.Th (SupplementalFig. S2). EPO-induced bone loss was also independent ofthe administration mode, as continuous administration of7 U/mouse/d for 10 days using subcutaneous pumpsresulted in a similar skeletal effect with 31% decrease inBV/TV, 30% lower Tb.N, 32% lower Conn.D, and no sig-nificant change in Tb.Th (Supplemental Fig. S2).
EPO administration stimulates bone resorptionand attenuates bone formation in vivo
Bone loss in EPO-injected and Tg6 mice was very similar;EPO treatment (30U-inj) resulted in an 88% increase in
osteoclast number in vivo and an 18% increase in TRAP5bserum levels. Bone formation was also similarly affected(although to a lesser extend) with 13% lower MAR, 19%lowerBFR, andno significant change inMS/BSand serumOCN (Fig. 4). Overall, in both models (Tg6 and EPO-injected mice), EPO induced severe bone loss both byincreasing bone resorption and by attenuating boneformation.
EPO stimulates the monocytic lineage in vivo
Using flow cytometry on bone marrow cells, we assessedthe effect of EPO on cell differentiation in the monocyticlineage in vivo. Bonemarrowcells were immunostained forM-CSF receptor (M-CSF-R, also known as CD115, CSF1R,or cFms) and RANK (also known as CD265 orTNFRSF11A). In both the Tg6 and EPO injection models,the monocytic lineage was vastly stimulated by EPO (Fig.5A, C), with a higher number of M-CSF-R+/RANK2
monocytes/macrophages and.2-fold increase in M-CSF-R+/RANK+ preosteoclasts (43).
EPO does not inhibit osteoblast activity in vitro
We next investigated the direct role of low doses of EPOon isolated bone cells. In osteoblast cultures derivedfrom adult bone marrow, EPO-R expression increasedwith osteoblastic differentiation (Supplemental Fig. S3A).Although EPO markedly inhibited osteoblastic bone for-mation in vivo, EPO treatment (10 U/ml) in isolated cul-tures did not inhibit osteoblast differentiation, activity, andRNAexpression of the classicmarker genes ALP, BSP, andOCN(Supplemental Fig. S3B–D).Osteoblast proliferationwas also not affected by EPO administration in vitro (Sup-plemental Fig. S3E).
EPO stimulates osteoclastogenesis via Jak2 and PI3Ksignaling pathways in monocyte-derived cells
As in theosteoblastic lineage,EPO-Rwasexpressed inbonemarrow–derived preosteoclasts, yet its level decreased withosteoclastic differentiation (Fig. 6A). In line with its in vivoeffect on bone resorption (Fig. 4), EPO administrationsignificantly stimulated osteoclastogenesis in cultures ofbone marrow–derived preosteoclasts (Fig. 6B). To en-sure that these cultures do not contain erythroid cells, weanalyzed the cells using flow cytometry (SupplementalFig. S4). Indeed, our preosteoclasts in vitro consist ofa purified population of M-CSF-R+ monocyte-derivedcells virtually devoid of erythroid, B and T cells, thussupporting the notion of EPO-R signaling in pre-osteoclasts. Because it has been suggested that EPOimpairs osteoclast function (30), we also performeda pit resorption assay. We found that pit resorption areawas increased in EPO-treated cultures (Fig. 6C), and theratio between resorption area (measured in calciumphosphate–coated wells) and TRAP+ area (measured inparallel, uncoated wells) remained unaffected (Fig. 6D).This suggests that EPO does not impair osteoclast
Figure 3. EPO induces trabecular bone loss. A) mCT analysisof the distal femoral trabecular bone of 7 EPO- and diluent-injected 14-week-old female mice. Data are mean 6 SEM. *P ,0.05 compared with controls, t test. B) mCT images of distalfemoral trabecular bone of controls (left) vs. EPO-injected(right) mice with median BV/TV values.
ERYTHROPOIETIN STIMULATES BONE RESORPTION 5

resorbing activity. EPO also did not affect preosteo-clast proliferation (Fig. 6E).
We then investigated the signaling pathways involved inEPO stimulation of osteoclast differentiation. BecauseEPO-R signaling cascades include Jak2, PI3K, and MEK/MAPK (41, 44), we tested the activation of the Jak2, PI3K,and MEK/MAPK pathways by EPO using immunoblot
analysis in RANKL-treated bone marrow–derived pre-osteoclasts. We detected the phosphorylation of Jak2 andAkt (downstream of PI3K) but not of ERK (a member ofthe MAPK pathway) 10 minutes after EPO administration(Fig. 6F).We also specifically inhibited each pathway usingAG490, LY294002, and U0126, respectively, and testedwhether the effect of EPO was maintained in either
Figure 4. Increased osteoclastogenesis and reduced bone formation in EPO-injected animals (30U-inj). A) Histologic imagesshowing increased osteoclast number in the distal femur of representative diluent (left) and EPO-injected (right) animals.Images were acquired at 310 magnification. B) N.Oc/BS: TRAP+ lining osteoclasts relative to bone surface measured inhistologic sections of the distal femur from 6 diluent- and 5 EPO-treated mice. C) Serum TRAP5b levels, n = 8. D–F) Parameters ofbone formation were measured in histologic sections of the distal femur from 6 (diluent) and 5 (EPO) mice. D) MAR valuesindicated below representative histologic images showing calcein double-labeled trabeculae in the distal femur of diluent- andEPO-injected animals. Images were acquired at 310 magnification. E) MS/BS, mineralizing surface. F) BFR/BS, bone formationrate. G) Serum osteocalcin level, n = 8. Data are mean 6 SEM. *P , 0.05 compared with controls, t test.
Figure 5. EPO effect on the monocyte lineage.Flow cytometric analysis using M-CSF-R andRANK antibodies in bone marrow cells from (A,B) 6 WT and 5 Tg6 animals and (C, D) 8 diluent-and 8 EPO-injected 13-week-old mice. Bars showpercentage from total red blood cell–free bonemarrow cells; mean 6 SEM. B, D) Representativescatter plots of the indicated animals. *P , 0.05compared with controls, t test.
6 Vol. 29 May 2015 HIRAM-BAB ET AL.The FASEB Journal x www.fasebj.org

condition. As expected from the activation of the corre-sponding pathways (Fig. 6F), the stimulatory effect of EPOon osteoclast differentiation was abrogated by AG490 andLY294002 but was not affected by U0126 (Fig. 6G). Asa positive control, increased doses of RANKL in the pres-ence of these inhibitors resulted in further stimulation ofosteoclastogenesis, indicating that the absence of stimula-tion in AG490- and LY294002-treated culture is caused byspecific blockade of EPO-R signaling. This indicates that
EPO-R signaling stimulates osteoclastogenesis via JAK2and PI3K but independently of the MAPK pathway.
DISCUSSION
Recent reports on nonhematopoietic functions of EPOmediated by nonerythroid cells emphasize the physiologicand therapeutic importance of a better understanding of
Figure 6. EPO stimulates osteoclastogenesis in vitro. A) EPO-R transcript expression on differentiating osteoclasts derived frombone marrow. B) TRAP staining (images and relative TRAP+ area) of osteoclasts after 6 days of differentiation 6 EPO (10 U/ml).*P , 0.05 compared with controls, t test. C) Pit resorption area from osteoclasts cultured on calcium phosphate–coated wells 6EPO (10 U/ml). D) Pit resorption per osteoclast area ratio (to assess resorption activity per cell) in parallel cultures as in C oncalcium phosphate–coated and uncoated plastic wells. E) Bone marrow–derived preosteoclast proliferation measured by thiazolylblue tetrazolium bromide assay after 3 days of culture 6 EPO (10 U/ml). F) Western blot of phosphorylated JAK2, AKT, andERK, 10 and 60 minutes following EPO administration (10 U/ml) to preosteoclasts. Total ERK was used as loading control. G)Relative TRAP+ area of osteoclasts after 6 days of differentiation 6 EPO (10 U/ml) with/without the indicated inhibitor; AG490(AG, 1 mM), U0126 (U, 1 mM), and LY294002 (LY, 0.1 mM). Higher dose of RANKL (High RANKL, 100 ng/ml) was added toseparate wells with the indicated inhibitors. Data are mean 6 SEM. *P , 0.05 compared with controls, t test; n . 3.
ERYTHROPOIETIN STIMULATES BONE RESORPTION 7

the systemic actions of EPO. The present study demon-strates a bone catabolic effect of rHuEPO using severaladult mouse models, namely EPO overexpressing mice(Tg6), intermittent injections of low and high EPOdosage, and continuous administration of low doses. InTg6 mice, the increase in EPO levels is similar to thestimulation of EPO at high altitude (45). This model isalso relevant for the pathophysiologic increase of en-dogenous EPO levels observed after bleeding/repeatedphlebotomies without the confounding direct effect ofhypoxia on bone cells (46) and in cases of paraneo-plastic production of EPO (47), thalassemia, and poly-cythemia vera (48). On the other hand, the 30U-injmodel is relevant for therapeutic administration of ex-ogenous EPO (16, 18). In all the models presentedherein, higher EPO serum levels resulted in lower tra-becular bone density, mainly because of lower trabecu-lar number. Our in vivo data indicate that EPO inducesbone resorption and attenuates bone formation, as wellas stimulates monocyte-derived cells in the bone mar-row. Stimulation of osteoclastogenesis and bone re-sorption is likely attributable to EPO-R activation of theJak2 and PI3K pathways in osteoclast precursors andtherefore seems to occur independently of erythropoi-etic effects in the bone marrow.
As a sidenote, therewas amildbut statistically significantincrease in trabecular thickness in the Tg6 and EPO-injected animals, compared with their respective con-trols, despite the dramatic bone loss (.50% decrease inBV/TV). A similar observationhas been repeatedlymadein age-induced bone loss, where the average Tb.Thremains unaltered or even increases, especially in femalemice (49, 50). This may be because of the occurrence ofcompensatory mechanisms aimed at strengthening thefewer trabeculae that were not lost. However, the atten-uated bone formation in EPO overexpressing andinjected animals does not support this conclusion. Itseems more reasonable to assume that the increased Tb.Th is consequent to a statistical bias as demonstratedpreviously (51). Briefly, in age-induced bone loss (de-creased BV/TV and Tb.N), the increased bone re-sorption equally reduces the thickness of all trabeculae,leading to the clearance of the thinnest structures andthus increasing the percentage of the remaining thickertrabeculae. The increased Tb.Th would therefore notresult from an actual trabecular thickening but ratherreflect a statistical bias that averages only the remainingthicker trabeculae.
The stimulatory effect of EPO on osteoclastogenesis asreported herein is in line with previous reports (30, 52).However, it has been suggested that osteoclasts induced byEPO are not active (30). Here we assessed the bone-resorbing potential of osteoclasts inducedby EPO treatmentin vitro and found that the increased osteoclastogenesiswas associated with a significant increase in the pit for-mation (Fig. 6C, D). The fact that in parallel cultures, thetotal pit resorption area per total TRAP+ area remainedunaffected indicates that activity per cell was not impairedby EPO. This is further supported by our in vivo datashowing anoverall increase in thebone resorptionmarkerTRAP5b (Figs. 2 and 4).
As mentioned above, past reports on the general effectof EPO on bone are controversial and have recently
been addressed in a review (53). Discrepancies may beattributed to skeletal site specificity, age, or bone re-generation vs. steady-state remodeling. Indeed, we (dataherein) and others (31) have found that EPO induces adramatic trabecular bone loss in long bones of adult mice,whereas others reported an opposite effect, namely in-creased bone mass in vertebrae of newborn mice and inseveralmodels of bone regeneration (27, 28, 30, 42, 54). Ingrowing femalemice (4–8 weeks of age), we found that theeffect of EPO was very similar to that observed in adultanimals in both the femur and vertebrae, which is contra-dictory to an earlier report under similar experimentalconditions (30). Although this discrepancy in young ani-mals remains to be elucidated, the differential effect ofEPO in bone regeneration models vs. atraumatic remod-eling may depend on the involvement of osteoblastic vs.osteoclastic EPO signaling. Our in vivo data indicate a re-duced bone formation, whereas in vitro experiments failedto reveal any direct effect of EPO on osteoblast pro-liferation, differentiation, and activity at a dose of 10 U/ml(Fig. 6; Supplemental Fig. S3). Nevertheless, expressionof EPO-R on osteoblasts (Supplemental Fig. S3), up-regulation of EPO-R expression by EPO administrationin osteoblasts cultures (data not shown), and reports byothers on in vitro stimulation of osteoblast differentia-tion at doses higher than 10 U/ml (41, 55) collectivelysuggest that EPOdirectly affects osteoblasts, although ata dose range different than that required to stimulatemonocyte-derived cells. The common link betweenthe several reports that proposed an anabolic role forosteoblastic EPO-R signaling (27, 28, 42, 54) is that EPOwas administered following bone injury (bone re-generation) rather than steady-state bone homeostasis.It is therefore reasonable to assume that, under theformer conditions, EPO promotes bone formation viadirect activation of EPO-R signaling in osteoblasts,whereas it negatively regulates the latter by directly tar-geting themonocyte lineage andoverall attenuatingbone
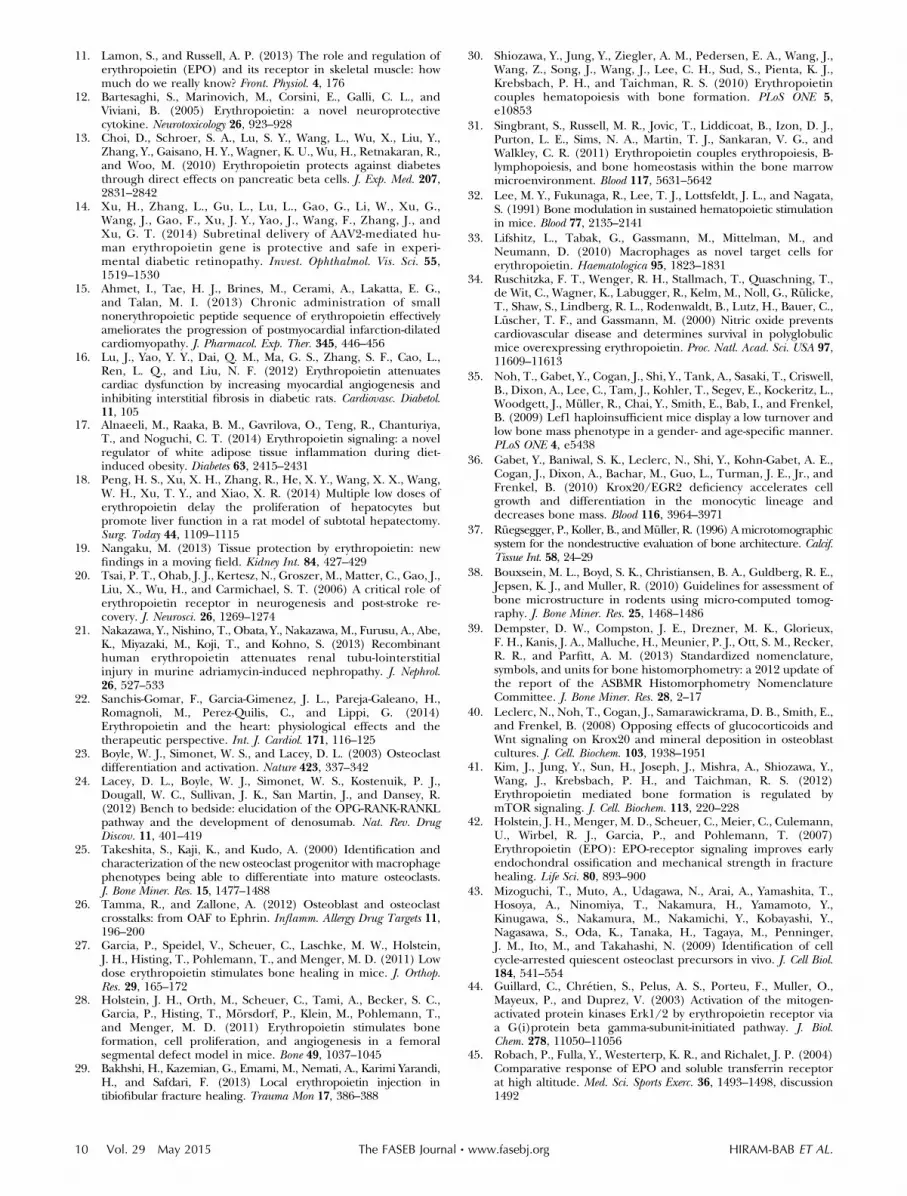
Figure 7. Summary of putative pathways describing EPOaction on bone metabolism. Our data suggest that the effectof EPO on bone can be mediated either (1) directly bystimulating osteoclastogenesis or (2) by inhibiting osteoblastsand bone formation via unknown intermediary. In vitro and invivo data from others in different experimental conditionssupport the idea that (3) direct activation of EPO-R onosteoblasts stimulates osteogenesis. Our data also suggest thatdirect activation of EPO-R requires higher concentrations ofEPO in osteoblasts than in osteoclasts. It is not unlikely thatsome in vivo findings result from the combination of two orthree of these mechanisms of action.
8 Vol. 29 May 2015 HIRAM-BAB ET AL.The FASEB Journal x www.fasebj.org

formation. Whether EPO inhibits osteoblast function un-der physiologic conditions in vivo via indirect mecha-nisms or by direct binding to the osteoblastic EPO-Rremains to be elucidated.
The controversy on the effects of EPO on bone in vivohas also been suggested to be dose dependent (53). Toexamine this possibility, we used both low (30U-inj) andhigh (180U-inj) doses and found similar skeletal effects(Fig. 3; Supplemental Fig. S2). We also compared con-tinuous (Tg6 mice and EPO pumps) vs. intermittent(EPO injections) administration and found no differ-ences between the treatment modalities (Figs. 1 and 3;Supplemental Figs. S1 and S2). Of note, the skeletaleffect of EPO was very similar between the Tg6 model(Figs. 1 and 2) and EPO-injected mice (Figs. 3 and 4),not only at the structural (lower BV/TV and Tb.N) butalso at the mechanistic level (increased N.Oc/BS andreduced MAR). These findings suggest that the skeletaleffect of EPO is independent of dose and treatmentmodality.
Notably, a previous study traced EPO-R–expressing cellsinmice and concluded that EPO-R is expressed only in theerythroid lineage (31). However, not all lineages weretested as the cell sorting was limited to only a subset of celltypes and differentiation stages (31). Importantly, no datawere shown for mature osteoblasts and preosteoclasts/osteoclasts, in which we specifically found high EPO-R ex-pression. Our results are supported by other publishedstudies reporting EPO-R expression and/or EPO-inducedintracellular signaling in monocyte-derived and osteo-blastic cells, as well as functional assays on isolated culturesthat responded to EPO treatment (30, 33, 41, 55). Still, weacknowledge the importance of investigating further thisimportant question using specific anti–EPO-R antibodiesand conditional knockout animal models currently underdevelopment.
Collectively, our in vivo and in vitro data, together withfindings from others, suggest that the skeletal effect ofEPO may be mediated by 3 different pathways (Fig. 7).First, direct stimulation of EPO-R on osteoclast precur-sors stimulates osteoclastogenesis and promotes boneresorption; second, EPO inhibits osteoblastic bone for-mation in vivo, likely via indirect mechanisms; and third,data reported by others (27, 28, 30, 41, 42, 54, 55) supportthe idea that in different experimental conditions thepredominant pathway is the direct activation of EPO-R onosteoblasts resulting in increased osteogenesis. In our invivo models, bone loss may be attributed to both the firstand second pathways. It is still reasonable to assume thatthe third pathway is also activated; namely, direct EPO-Rsignaling inosteoblasts stimulatesosteoblasticproliferationand function, but it only partially antagonizes the systemicattenuation of osteoblastic bone formation (pathway 3 vs.2; Fig. 7).
Because of the prenatal lethality of EPO-R knockoutmiceand theunavailability of strongEPO-Rantagonists, wecouldnot test theeffect ofnormalEPOlevels by abrogatingEPO-R signaling in vivo. Based on the conclusions of thepresent study, development of osteoclast- and osteoblast-specific conditional EPO-R knockout mice should beconsidered.We also acknowledge that our conclusions aremainly based on experimental data that will need to beverified in clinical settings. Although we could notfind any
direct evidence linking EPO to bone loss in humans, it hasbeen established that exposure to high altitude lead to ele-vated levels of EPO (45, 56, 57), and reports have shownthat even short-term periods at high altitude (or simulatedaltitude) result in significant bone loss (58, 59). In line withour conclusions, these observations provide evidence thathigh levels of EPO promote bone resorption in humansand suggest that the effect of hypoxia on bone metabolismis at least partly mediated by EPO-R signaling in themonocytic lineage.
This article is dedicated to the memory of Professor ItaiBab (1945–2014) from the Hebrew University of Jerusalem.Prof. Bab participated in this study by providing guidanceand technical support. The authors thank Dr. Russel S.Taichman (University of Michigan) for helpful discussionand comments on this manuscript. This work was supportedby Israel Science Foundation Grants 1822/12 and 1367/12(to Y.G.), and grants from the Deutsche Forschungsgemein-schaft to M.R. (RA1923/4-2) and B.W. (Emmy Noether andHeisenberg programs, WI3291/1-1, 1-2 and 5-1), the ElsbethBonhoff Foundation, and a Center for Regenerative Ther-apies Dresden (CRTD) seed grant (to M.R. and B.W). Thiswork was also supported by FP7-Health European commis-sion EpoCan Grant 282551 (to D.N. and M.G.), and a grantfrom the Open University Research Authority (Raanana,Israel) to Prof. Miriam C. Souroujon. We express our deepestgratitude and appreciation to our dear friend and colleague,Prof. M. Souroujon, who died during the course of this study.She will be remembered for her vision, deep insight, andexceptional scientific conduct. The authors declare noconflicts of interest.
REFERENCES
1. Watowich, S. S. (2011) The erythropoietin receptor: molecularstructure and hematopoietic signaling pathways. J. Investig. Med.59, 1067–1072
2. Myklebust, J. H., Smeland, E. B., Josefsen, D., and Sioud, M.(2000) Protein kinase C-alpha isoform is involved inerythropoietin-induced erythroid differentiation of CD34(+)progenitor cells from human bone marrow. Blood 95, 510–518
3. Spivak, J. L., Pham, T., Isaacs, M., and Hankins, W. D. (1991)Erythropoietin is both a mitogen and a survival factor. Blood 77,1228–1233
4. Wish, J. B. (2009) Past, present, and future of chronic kidneydisease anemia management in the United States. Adv. ChronicKidney Dis. 16, 101–108
5. Ramanath, V., Gupta, D., Jain, J., Chaudhary, K., and Nistala, R.(2012) Anemia and chronic kidney disease: making sense of therecent trials. Rev. Recent Clin. Trials 7, 187–196
6. Ohashi, Y., Uemura, Y., Fujisaka, Y., Sugiyama, T., Ohmatsu, H.,Katsumata, N., Okamoto, R., Saijo, N., and Hotta, T. (2013)Meta-analysis of epoetin beta and darbepoetin alfa treatment forchemotherapy-induced anemia and mortality: Individual patientdata from Japanese randomized, placebo-controlled trials. CancerSci. 104, 481–485
7. Jelkmann, W., and Lundby, C. (2011) Blood doping and itsdetection. Blood 118, 2395–2404
8. Arcasoy, M. O. (2008) The non-haematopoietic biological effectsof erythropoietin. Br. J. Haematol. 141, 14–31
9. Yasuda, Y., Fujita, Y., Musha, T., Tanaka, H., Shiokawa, S.,Nakamatsu, K., Mori, S., Matsuo, T., and Nakamura, Y. (2001)Expression of erythropoietin in human female reproductiveorgans. Ital. J. Anat. Embryol. 106(2, Suppl 2), 215–222
10. Guneli, E., Cavdar, Z., Islekel, H., Sarioglu, S., Erbayraktar, S.,Kiray, M., Sokmen, S., Yilmaz, O., and Gokmen, N. (2007)Erythropoietin protects the intestine against ischemia/reperfusion injury in rats. Mol. Med. 13, 509–517
ERYTHROPOIETIN STIMULATES BONE RESORPTION 9
11. Lamon, S., and Russell, A. P. (2013) The role and regulation oferythropoietin (EPO) and its receptor in skeletal muscle: howmuch do we really know? Front. Physiol. 4, 176
12. Bartesaghi, S., Marinovich, M., Corsini, E., Galli, C. L., andViviani, B. (2005) Erythropoietin: a novel neuroprotectivecytokine. Neurotoxicology 26, 923–928
13. Choi, D., Schroer, S. A., Lu, S. Y., Wang, L., Wu, X., Liu, Y.,Zhang, Y., Gaisano, H. Y., Wagner, K. U., Wu, H., Retnakaran, R.,and Woo, M. (2010) Erythropoietin protects against diabetesthrough direct effects on pancreatic beta cells. J. Exp. Med. 207,2831–2842
14. Xu, H., Zhang, L., Gu, L., Lu, L., Gao, G., Li, W., Xu, G.,Wang, J., Gao, F., Xu, J. Y., Yao, J., Wang, F., Zhang, J., andXu, G. T. (2014) Subretinal delivery of AAV2-mediated hu-man erythropoietin gene is protective and safe in experi-mental diabetic retinopathy. Invest. Ophthalmol. Vis. Sci. 55,1519–1530
15. Ahmet, I., Tae, H. J., Brines, M., Cerami, A., Lakatta, E. G.,and Talan, M. I. (2013) Chronic administration of smallnonerythropoietic peptide sequence of erythropoietin effectivelyameliorates the progression of postmyocardial infarction-dilatedcardiomyopathy. J. Pharmacol. Exp. Ther. 345, 446–456
16. Lu, J., Yao, Y. Y., Dai, Q. M., Ma, G. S., Zhang, S. F., Cao, L.,Ren, L. Q., and Liu, N. F. (2012) Erythropoietin attenuatescardiac dysfunction by increasing myocardial angiogenesis andinhibiting interstitial fibrosis in diabetic rats. Cardiovasc. Diabetol.11, 105
17. Alnaeeli, M., Raaka, B. M., Gavrilova, O., Teng, R., Chanturiya,T., and Noguchi, C. T. (2014) Erythropoietin signaling: a novelregulator of white adipose tissue inflammation during diet-induced obesity. Diabetes 63, 2415–2431
18. Peng, H. S., Xu, X. H., Zhang, R., He, X. Y., Wang, X. X., Wang,W. H., Xu, T. Y., and Xiao, X. R. (2014) Multiple low doses oferythropoietin delay the proliferation of hepatocytes butpromote liver function in a rat model of subtotal hepatectomy.Surg. Today 44, 1109–1115
19. Nangaku, M. (2013) Tissue protection by erythropoietin: newfindings in a moving field. Kidney Int. 84, 427–429
20. Tsai, P. T., Ohab, J. J., Kertesz, N., Groszer, M., Matter, C., Gao, J.,Liu, X., Wu, H., and Carmichael, S. T. (2006) A critical role oferythropoietin receptor in neurogenesis and post-stroke re-covery. J. Neurosci. 26, 1269–1274
21. Nakazawa, Y., Nishino, T., Obata, Y., Nakazawa, M., Furusu, A., Abe,K., Miyazaki, M., Koji, T., and Kohno, S. (2013) Recombinanthuman erythropoietin attenuates renal tubu-lointerstitialinjury in murine adriamycin-induced nephropathy. J. Nephrol.26, 527–533
22. Sanchis-Gomar, F., Garcia-Gimenez, J. L., Pareja-Galeano, H.,Romagnoli, M., Perez-Quilis, C., and Lippi, G. (2014)Erythropoietin and the heart: physiological effects and thetherapeutic perspective. Int. J. Cardiol. 171, 116–125
23. Boyle, W. J., Simonet, W. S., and Lacey, D. L. (2003) Osteoclastdifferentiation and activation. Nature 423, 337–342
24. Lacey, D. L., Boyle, W. J., Simonet, W. S., Kostenuik, P. J.,Dougall, W. C., Sullivan, J. K., San Martin, J., and Dansey, R.(2012) Bench to bedside: elucidation of the OPG-RANK-RANKLpathway and the development of denosumab. Nat. Rev. DrugDiscov. 11, 401–419
25. Takeshita, S., Kaji, K., and Kudo, A. (2000) Identification andcharacterization of the new osteoclast progenitor with macrophagephenotypes being able to differentiate into mature osteoclasts.J. Bone Miner. Res. 15, 1477–1488
26. Tamma, R., and Zallone, A. (2012) Osteoblast and osteoclastcrosstalks: from OAF to Ephrin. Inflamm. Allergy Drug Targets 11,196–200
27. Garcia, P., Speidel, V., Scheuer, C., Laschke, M. W., Holstein,J. H., Histing, T., Pohlemann, T., and Menger, M. D. (2011) Lowdose erythropoietin stimulates bone healing in mice. J. Orthop.Res. 29, 165–172
28. Holstein, J. H., Orth, M., Scheuer, C., Tami, A., Becker, S. C.,Garcia, P., Histing, T., Morsdorf, P., Klein, M., Pohlemann, T.,and Menger, M. D. (2011) Erythropoietin stimulates boneformation, cell proliferation, and angiogenesis in a femoralsegmental defect model in mice. Bone 49, 1037–1045
29. Bakhshi, H., Kazemian, G., Emami, M., Nemati, A., Karimi Yarandi,H., and Safdari, F. (2013) Local erythropoietin injection intibiofibular fracture healing. Trauma Mon 17, 386–388
30. Shiozawa, Y., Jung, Y., Ziegler, A. M., Pedersen, E. A., Wang, J.,Wang, Z., Song, J., Wang, J., Lee, C. H., Sud, S., Pienta, K. J.,Krebsbach, P. H., and Taichman, R. S. (2010) Erythropoietincouples hematopoiesis with bone formation. PLoS ONE 5,e10853
31. Singbrant, S., Russell, M. R., Jovic, T., Liddicoat, B., Izon, D. J.,Purton, L. E., Sims, N. A., Martin, T. J., Sankaran, V. G., andWalkley, C. R. (2011) Erythropoietin couples erythropoiesis, B-lymphopoiesis, and bone homeostasis within the bone marrowmicroenvironment. Blood 117, 5631–5642
32. Lee, M. Y., Fukunaga, R., Lee, T. J., Lottsfeldt, J. L., and Nagata,S. (1991) Bone modulation in sustained hematopoietic stimulationin mice. Blood 77, 2135–2141
33. Lifshitz, L., Tabak, G., Gassmann, M., Mittelman, M., andNeumann, D. (2010) Macrophages as novel target cells forerythropoietin. Haematologica 95, 1823–1831
34. Ruschitzka, F. T., Wenger, R. H., Stallmach, T., Quaschning, T.,de Wit, C., Wagner, K., Labugger, R., Kelm, M., Noll, G., Rulicke,T., Shaw, S., Lindberg, R. L., Rodenwaldt, B., Lutz, H., Bauer, C.,Luscher, T. F., and Gassmann, M. (2000) Nitric oxide preventscardiovascular disease and determines survival in polyglobulicmice overexpressing erythropoietin. Proc. Natl. Acad. Sci. USA 97,11609–11613
35. Noh, T., Gabet, Y., Cogan, J., Shi, Y., Tank, A., Sasaki, T., Criswell,B., Dixon, A., Lee, C., Tam, J., Kohler, T., Segev, E., Kockeritz, L.,Woodgett, J., Muller, R., Chai, Y., Smith, E., Bab, I., and Frenkel,B. (2009) Lef1 haploinsufficient mice display a low turnover andlow bone mass phenotype in a gender- and age-specific manner.PLoS ONE 4, e5438
36. Gabet, Y., Baniwal, S. K., Leclerc, N., Shi, Y., Kohn-Gabet, A. E.,Cogan, J., Dixon, A., Bachar, M., Guo, L., Turman, J. E., Jr., andFrenkel, B. (2010) Krox20/EGR2 deficiency accelerates cellgrowth and differentiation in the monocytic lineage anddecreases bone mass. Blood 116, 3964–3971
37. Ruegsegger, P., Koller, B., andMuller, R. (1996) Amicrotomographicsystem for the nondestructive evaluation of bone architecture. Calcif.Tissue Int. 58, 24–29
38. Bouxsein, M. L., Boyd, S. K., Christiansen, B. A., Guldberg, R. E.,Jepsen, K. J., and Muller, R. (2010) Guidelines for assessment ofbone microstructure in rodents using micro-computed tomog-raphy. J. Bone Miner. Res. 25, 1468–1486
39. Dempster, D. W., Compston, J. E., Drezner, M. K., Glorieux,F. H., Kanis, J. A., Malluche, H., Meunier, P. J., Ott, S. M., Recker,R. R., and Parfitt, A. M. (2013) Standardized nomenclature,symbols, and units for bone histomorphometry: a 2012 update ofthe report of the ASBMR Histomorphometry NomenclatureCommittee. J. Bone Miner. Res. 28, 2–17
40. Leclerc, N., Noh, T., Cogan, J., Samarawickrama, D. B., Smith, E.,and Frenkel, B. (2008) Opposing effects of glucocorticoids andWnt signaling on Krox20 and mineral deposition in osteoblastcultures. J. Cell. Biochem. 103, 1938–1951
41. Kim, J., Jung, Y., Sun, H., Joseph, J., Mishra, A., Shiozawa, Y.,Wang, J., Krebsbach, P. H., and Taichman, R. S. (2012)Erythropoietin mediated bone formation is regulated bymTOR signaling. J. Cell. Biochem. 113, 220–228
42. Holstein, J. H., Menger, M. D., Scheuer, C., Meier, C., Culemann,U., Wirbel, R. J., Garcia, P., and Pohlemann, T. (2007)Erythropoietin (EPO): EPO-receptor signaling improves earlyendochondral ossification and mechanical strength in fracturehealing. Life Sci. 80, 893–900
43. Mizoguchi, T., Muto, A., Udagawa, N., Arai, A., Yamashita, T.,Hosoya, A., Ninomiya, T., Nakamura, H., Yamamoto, Y.,Kinugawa, S., Nakamura, M., Nakamichi, Y., Kobayashi, Y.,Nagasawa, S., Oda, K., Tanaka, H., Tagaya, M., Penninger,J. M., Ito, M., and Takahashi, N. (2009) Identification of cellcycle-arrested quiescent osteoclast precursors in vivo. J. Cell Biol.184, 541–554
44. Guillard, C., Chretien, S., Pelus, A. S., Porteu, F., Muller, O.,Mayeux, P., and Duprez, V. (2003) Activation of the mitogen-activated protein kinases Erk1/2 by erythropoietin receptor viaa G(i)protein beta gamma-subunit-initiated pathway. J. Biol.Chem. 278, 11050–11056
45. Robach, P., Fulla, Y., Westerterp, K. R., and Richalet, J. P. (2004)Comparative response of EPO and soluble transferrin receptorat high altitude. Med. Sci. Sports Exerc. 36, 1493–1498, discussion1492
10 Vol. 29 May 2015 HIRAM-BAB ET AL.The FASEB Journal x www.fasebj.org

46. Chang, J., Jackson, S., Wardale, J., and Jones, S. W. (2014)Hypoxia modulates the phenotype of osteoblasts isolated fromknee osteoarthritis patients leading to under-mineralised bonenodule formation. Arthrit. Rheumatol. 66, 1789–1799
47. Fried, W. (2009) Erythropoietin and erythropoiesis. Exp. Hematol.37, 1007–1015
48. Zoi, K., Terpos, E., Zoi, C., and Loukopoulos, D. (2008) IncreasedCD177 (PRV1) expression in thalassaemia and the underlyingerythropoietic activity. Br. J. Haematol. 141, 100–104
49. Glatt, V., Canalis, E., Stadmeyer, L., and Bouxsein, M. L.(2007) Age-related changes in trabecular architecture differin female and male C57BL/6J mice. J. Bone Miner. Res. 22,1197–1207
50. Bab, I., Muller, R., Hajbi-Yonissi, C., and Gabet, Y. (2007) Micro-Tomographic Atlas of the Mouse Skeleton, Springer, New York
51. Gabet, Y., and Bab, I. (2011) Microarchitectural changes in theaging skeleton. Curr. Osteoporos. Rep. 9, 177–183
52. Sun, H., Jung, Y., Shiozawa, Y., Taichman, R. S., and Krebsbach,P. H. (2012) Erythropoietin modulates the structure of bonemorphogenetic protein 2-engineered cranial bone. Tissue Eng.Part A 18, 2095–2105
53. McGee, S. J., Havens, A. M., Shiozawa, Y., Jung, Y., andTaichman, R. S. (2012) Effects of erythropoietin on the bonemicroenvironment. Growth Factors 30, 22–28
54. Mihmanli, A., Dolanmaz, D., Avunduk, M. C., and Erdemli,E. (2009) Effects of recombinant human erythropoietin on
mandibular distraction osteogenesis. J. Oral Maxillofac. Surg. 67,2337–2343
55. Rolfing, J. H., Baatrup, A., Stiehler, M., Jensen, J., Lysdahl,H., and Bunger, C. (2014) The osteogenic effect oferythropoietin on human mesenchymal stromal cells is dose-dependent and involves non-hematopoietic receptors andmultiple intracellular signaling pathways. Stem Cell Rev. 10,69–78
56. Berglund, B. (1992) High-altitude training. Aspects of haema-tological adaptation. Sports Med. 14, 289–303
57. Neya, M., Enoki, T., Ohiwa, N., Kawahara, T., and Gore, C. J.(2013) Increased hemoglobin mass and VO2max with 10 hnightly simulated altitude at 3000 m. Int. J. Sports Physiol. Perform.8, 366–372
58. Tanaka, H., Minowa, K., Satoh, T., and Koike, T. (1992) Boneatrophy at high altitude. J. Bone Miner. Metab. 10, 31–36
59. Basu, M., Malhotra, A. S., Pal, K., Chatterjee, T., Ghosh, D.,Haldar, K., Verma, S. K., Kumar, S., Sharma, Y. K., and Sawhney,R. C. (2013) Determination of bone mass using multisitequantitative ultrasound and biochemical markers of boneturnover during residency at extreme altitude: a longitudinalstudy. High Alt. Med. Biol. 14, 150–154
Received for publication July 9, 2014.Accepted for publication December 23, 2014.
ERYTHROPOIETIN STIMULATES BONE RESORPTION 11
Copyright © 2022 FDOKUMEN