
Preventing hereditary cancers caused by opportunistic carcinogens
ARTICLE IN PRESS
1094-5539/$ - se
doi:10.1016/j.pu
�CorrespondE-mail addr
Pulmonary Pharmacology & Therapeutics 21 (2008) 201–207
www.elsevier.com/locate/ypupt
Efficiency of lornoxicam in lung and trachea injury caused byperoxynitrite
Erhan Ayana,�, Murat Bayram Kaplana, Oguz Koksela, Lulufer Tamerb, Tuba Karabacakc,Lokman Ayazb, Ali Ozdulgera
aDepartment of Thoracic Surgery, Mersin University, School of Medicine, Mersin, TurkeybDepartment of Biochemistry, Mersin University, School of Medicine, Mersin, TurkeycDepartment of Pathology, Mersin University, School of Medicine, Mersin, Turkey
Received 1 August 2006; received in revised form 16 January 2007; accepted 13 February 2007
Abstract
Peroxynitrite is involved in the pathogenesis of pulmonary diseases such as asthma, occupational pulmonary diseases and acute
respiratory distress syndrome (ARDS) due to excessive production of nitric oxide or superoxide or both. Lornoxicam, a new oxicam
derivative, is a potent anti-inflammatory agent. In this study, we evaluated the role of lornoxicam in a peroxynitrite-induced pulmonary
and tracheal injury model by measuring myeloperoxidase (MPO) activity, malondialdehyde (MDA) and 3-nitrotyrosine (3-NT) levels in
lung tissue and bronco-alveolar lavage fluid. The study protocol was based on three experimental groups as treatment (T), control (C)
and peroxynitrite (P). Each group was subdivided into three subgroups as 2nd, 24th and 48th hour groups. P and T groups were injected
intratracheal peroxynitrite. The T group received intraperitoneal lornoxicam before and 24 h after peroxynitrite installation. Tissue and
serum MDA, MPO values and tissue 3-NT value of the treatment and control groups were found significantly lower than the
peroxynitrite group at the 2nd, 24th and 48th hours (po0.05). Similarly, values obtained from bronco-alveolar lavage fluid examination
in the control and treatment groups were significantly less than those in the peroxynitrite group (po0.01). Therefore, Lornoxicam has
been found to be effective in attenuating peroxynitrite induced pulmonary and tracheal injury in rats.
r 2007 Elsevier Ltd. All rights reserved.
Keywords: Peroxynitrite; Trachea and lung injury; Lornoxicam
1. Introduction
The formation of the potent biological oxidative agentperoxynitrite is a result of the reaction between nitric oxide(NO) and superoxide which are both free radicals. Thisreaction occurs in normal individuals under in vivoconditions. While low amounts of peroxynitrite do notcause harmful effects, high amounts seen in pathologicalcases where superoxide anion or nitric oxide is producedexcessively result in tissue injury. Inflammatory cellsespecially macrophages contribute greatly to the formationof peroxynitrite since they are the sources of bothcompound [1].
e front matter r 2007 Elsevier Ltd. All rights reserved.
pt.2007.02.005
ing author. Tel.: +903242374300.
ess: [email protected] (E. Ayan).
As peroxynitrite is a highly reactive anion, it easily reactswith cell components like lipids and proteins, which resultsin impaired cell functions and cellular balance. Oxidationof the membrane lipids and tissue sulphidrils leads to theinjury in the membrane sodium channels of the tissues [1].Peroxynitrite induced oxidative damage is not limited to
the cell membrane. Peroxynitrite oxidizes guanine residuesin the DNA and converts them to nitroguanine, wherebyDNA is rapidly depurinated. Thus Poly ADP ribosyltransferase is activated leading to a repair cycle in themacrophages, neurons and smooth muscle cells. This isfollowed by the consumption of cellular energy andconsequently by cell death. Besides, inhibition of mito-chondrial electron transport and thus respiration byperoxynitrite are other sources of cellular energy lack. Itwas, also, reported that peroxynitrite led to mitochondrialcalcium overload and cell death [2,3]. It is also noted that

ARTICLE IN PRESSE. Ayan et al. / Pulmonary Pharmacology & Therapeutics 21 (2008) 201–207202
peroxynitrite is involved in the pathogenesis of pulmonarydiseases such as asthma, occupational pulmonary diseases,acute respiratory distress syndrome (ARDS), surfactantprotein damage and pulmonary diseases induced bysmoking due to excessive production of nitric oxide orsuperoxide or both [2].
As mentioned previously, peroxynitrite formation is apart of the inflammatory cascade but peroxynitrite admin-istration itself can also trigger an inflammatory response.In a study performed on pigs, intratracheal administrationof peroxynitrite caused serious injury in the respiratoryepithelial and smooth muscle cells [3].
Lornoxicam, a new oxicam derivative, is a strong anti-inflammatory agent. Studies have shown that lornoxicaminhibits polymorphonuclear (PMN) leukocyte migration,superoxide release from human PMN leukocytes and nitricoxide release from macrophages [4–6].
This study is carried out to evaluate the efficiency oflornoxicam on peroxynitrite-induced lung injury and thepossible mechanisms involved.
2. Material and method
The study included 54 rats from both sexes, weighingbetween 250 and 280 g. The rats were fed on commercialfeed and water throughout the study protocol. They weredivided into three experimental groups named as, Control(C), Treatment (T) and Peroxynitrite (P) groups. Eachgroup was divided further into three subgroups as 2nd,24th and 48th h groups. The animals were anesthetizedwith thiopental sodium (Pental Sodyum 1 g, IE Ulagay,Turkey) (25mg/kg ip). In the P group, following anesthesiaand skin antisepsia; the trachea was palpated and 0.5ml10mM intratracheal peroxynitrite, production of ourinstitutional biochemistry laboratory, was injected withan insulin injector, once only, at hour ‘‘0’’. In the C group,the same volume of saline, instead of peroxynitrite, wasinjected into the trachea, once only, at hour ‘‘0’’. In the Tgroup, the rats received 1.3mg/kg intraperitoneal lornox-icam (Xefo 8mg, Abdi Ibrahim, Turkey) according to apreviously published paper [7]. Right after that intratra-cheal peroxynitrite injection at hour ‘‘0’’ was performed.As an exception, in the 48th h subgroup of the T group, thesame dose of lornoxicam was repeated at the 24th h. Allanimals were sacrificed at the according time by overdosethiopental sodium followed by collection of bronco-alveolar lavage fluid (BALF), blood and tissue samples.BALF was obtained after the method by Proctor et al. [8].Following dissection the trachea was suspended just belowthe larynx. An 18G catheter was inserted below this pointand warm saline of 1ml at 37 1C was infused into the lungsand the BALF was collected.
2.1. Peroxynitrite synthesis
Peroxynitrite was synthesized in a quenched flow reactoras described previously [9]. Briefly, solutions of 0.6M
NaNO2 and 0.6M HCl plus 0.7M H2O2 were pumped intoa T-junction and mixed in a glass tube. The acid-catalysedreaction of nitrous acid with H2O2 to form peroxynitrous acidwas quenched by pumping 1.5M NaOH at the same rate intoa second T junction at the end of glass tubing. The solutionwas frozen for a week at �20 1C. As a result of freezefractionation, peroxynitrite formed a yellow top layer whichwas retained for further analysis and application. Theconcentration of peroxynitrite in this layer was determinedby absorbance at 302nm (e302 ¼ 1.676103M�1 cm�1). Stocksolutions of peroxynitrite were kept in a freezer at alkalinepH, and the concentration was determined before each use.At room temperature and at a concentration of 10mM inKrebs buffer, peroxynitrite decomposed by 50%, 92%, and100% after 15, 30, and 60min, respectively.
2.2. The determination of malondialdehyde (MDA)
The MDA levels, an index of lipid peroxidation, weredetermined by the thiobarbituric acid (TBA) reactiondescribed by Yagi [10]. The principle of the method isbased on spectrophotometric determination of the intensityof the pink color produced by interaction of the barbituricacid with MDA produced as a result of lipid peroxidation.1,1,3,3-tetraetoxypropane was used as the primary stan-dard.
2.3. The determination of myeloperoxidase (MPO)
The determination of MPO activity is based on the factthat it reduces o-dianozidine the amount of which wasmeasured at 410 nm spectrophotometrically [11].
2.4. The determination of 3-nitrotyrosine
The tissues were homogenized in ice-cold phosphatebuffered saline (pH ¼ 7.4). The protein content of eachsample was determined by means of Lowry reagent.Equivalent amounts of each sample were hydrolysed in6N HCI at 100 1C for 18–24 h, and then samples wereanalysed on a HP 1049 HPLC apparatus. The analyticalcolumn was a 5mm pore size Spherisorb ODS-2 C18reverse-phase column (4.6–250 nm; Alltech, Deerfield, IL,USA). The guard column was a C18 cartridge (Alltech).The mobile phase was 50mmol/l sodium acetate/50mmol/lcitrate/8% methanol, pH ¼ 3.1. HPLC analysis wasperformed under isocratic conditions at a flow rate of1ml/min and the UV detector was set at 274 nm. 3-NTdetermination was made by comparison of the sample’speak area with the peak area produced by the externalstandard solution of 10mmol/l 3-NT [12].
2.5. Histopathological examination
The specimens were fixed in 10% formalin for 24 h,and standard dehydration and paraffin-wax embeddingprocedures were used. H&E-stained slides were prepared

ARTICLE IN PRESSE. Ayan et al. / Pulmonary Pharmacology & Therapeutics 21 (2008) 201–207 203
by using standard methods. Light microscopic analyses oflung specimens were carried out by blinded observation toevaluate pulmonary architecture, tissue oedema formationand infiltration of the inflammatory cells. The results wereclassified into four grades where Grade 1 representednormal histopathology; Grade 2 indicated only fewneutrophil leukocyte infiltration; Grade 3 representedmoderate neutrophil leukocyte infiltration, perivascularoedema formation and partial destruction of pulmonaryarchitecture and finally Grade 4 included dense neutrophilleukocyte infiltration, abscess formation and completedestruction of pulmonary architecture [13].
2.6. Statistical evaluation
Two-factor variance analysis was conducted using SPSS11.5 software to check whether there were any differencesbetween tissue MDA, serum MDA, tissue MPO, serumMPO and tissue 3-NT variants, considering time and grouptogether. Bonferroni test, a Post-Hoc test, was utilized with
40
30
20
10
0
T
C
P*
Mean +
- 2 S
D T
issue
MD
A n
mol/m
l
** *
2.h 24.h 48.h
Graphic 1. (a) Tissue MDA value levels. (b) Serum MDA value levels. MDA
from the values obtained from the P group at the corresponding time interval
Mean +
-2S
D tis
sue M
PO
U/g
r
5
4
3
2
1
0
-1
T
C
P*
* * *
48. h24.h2. h
Graphic 2. (a) Tissue MPO values levels. (b) Serum MPO values levels. C
significantly different from the values obtained from the P group at the corres
statistica 6.0 software to find out which variants weredifferent. Level of significance was set at po0.05.
3. Results
The results of biochemical analyses have been shown inGraphics 1–5.
3.1. Tissue and serum MDA values
Tissue and serum MDA values of the treatment andcontrol groups were found significantly lower than theperoxynitrite group at the 2nd, 24th and 48th h (p ¼ 0.001).However, there was no significant difference between thetreatment group and the control group at any of thesetimes (Graphics 1a and b).When compared in terms of time, it was seen that tissue
MDA values in the treatment and peroxynitrite groups atthe 24th and 48th h were significantly higher than those at
Mean +
- 2 S
D S
eru
m M
DA
nm
ol/m
l
40
30
20
10
0
T
K
P*
**
*
2.h 24. h 48. h
values from the T group at 2nd, 24th and 48th h are significantly different
s (MDA: malondialdehyde, *p ¼ 0.0001).
Mean +
-2 S
D s
eru
m M
PO
U/L
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
-0.5
T
C
P*
*
*
*
48. h24.h2.h
oncerning MPO, values from the T group at 2nd, 24th and 48th h are
ponding time intervals (*p ¼ 0.0001).
ARTICLE IN PRESS
T
3.0
E. Ayan et al. / Pulmonary Pharmacology & Therapeutics 21 (2008) 201–207204
the 2nd h. No significant difference was found betweenserum MDA values in terms of time.
Mean L
ung S
core
2.0
C
P
2.5
1.5
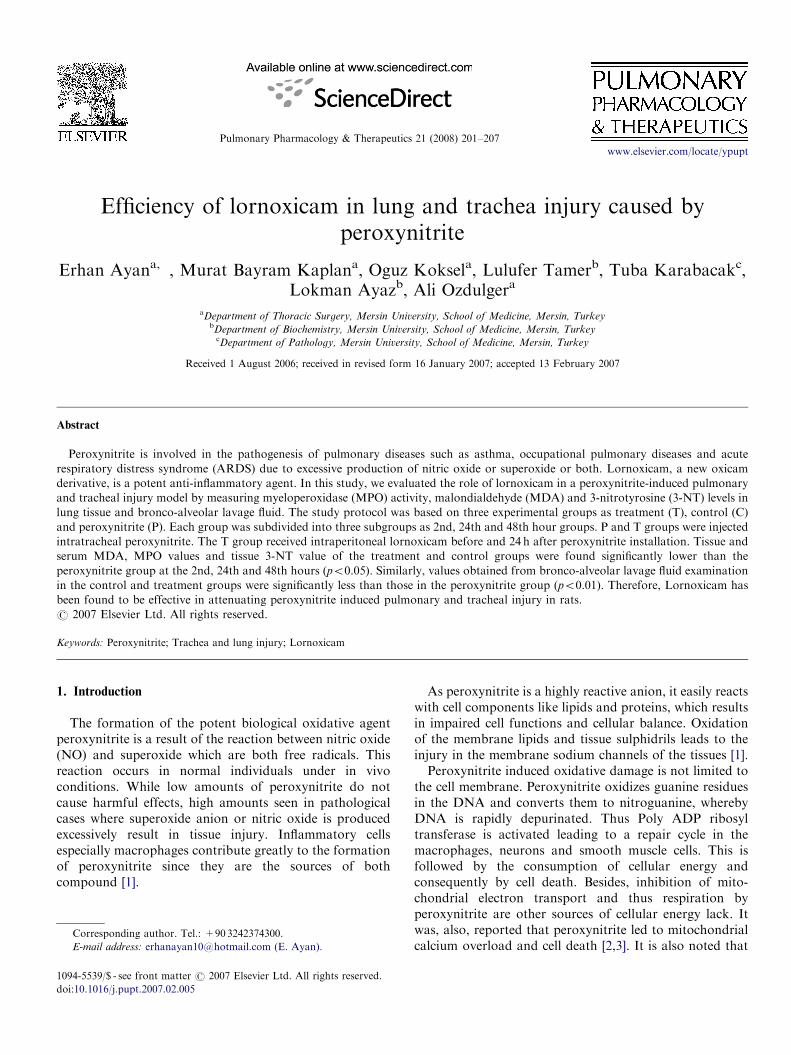
3.2. Tissue and serum MPO activity
Tissue and serum MPO activities in the treatment andcontrol groups were found significantly lower in compar-ison to the peroxynitrite group at the 2nd, 24th and 48th h(p ¼ 0.001). On the other hand, no significant differencewas established between the treatment and control groupsat any of the times (Graphics 2a and b).
The comparison of tissue MPO values between thetreatment and control groups in terms of time revealed thatthe values at the 48th h were significantly lower than those
Mean +
- 2 S
D 3
-NT
/to
taly
ty
rosin
e
T
K
P
*
* *
0.14
0.12
0.10
0.08
0.06
0.04
0.02
24.h 48. h2. h
Graphic 3. Tissue 3-nitrotyrosine/total tyrosine values. Concerning 3-NT/
total tyrosine, values from the T group at 2nd, 24th and 48th h are
significantly different from the values obtained from the P group at the
corresponding time intervals (p ¼ 0.0001).
7
6
5
4
3
2
1
0
T
C
P*
Mean +
- 2 S
E S
IT_LO
G
* *
*
2. h 24. h 48. h
Graphic 4. Bronco-alveolar lavage PMN levels. The values in the control
and treatment groups were significantly less than those in the peroxynitrite
group (p ¼ 0.0001).
1.0
0.5
2. hour 24. hour 48. hour
Graphic 5. Statistical evaluation of histopathologic scores. There were
significant differences between the peroxynitrite group and the treatment
group in all time groups according to our scoring.
at the 24th h (po0.05). The comparison of serum MPOactivity in terms of time showed that the increase at the2nd h significantly lessened at the 24th and 48th h and thatthe decrease in the treatment group was significantly lessthan that in the peroxynitrite group (p ¼ 0.001).
3.3. Tissue 3-nitrotyrosine/total tyrosine values
Tissue 3-nitrotyrosine/total tyrosine values were signifi-cantly lower in the treatment and control groups than theperoxynitrite group at the 2nd, 24th and 48thh (p ¼ 0.001).However, there was not any significant difference between thetreatment and control groups at any of the times (Graphic 3).The comparison of the treatment and peroxynitrite
group values with regard to times revealed that the valuesat the 24th and 48th h were significantly less than those atthe 2nd h (po0.05). In addition, values in the treatmentgroup were found significantly lower in comparison to thevalues in the peroxynitrite group.
3.4. BALF evaluation
Leukocyte counts of the BALF samples were taken andthe values are shown in Graphic 4. It was seen that thevalues in the control and treatment groups were signifi-cantly less than those in the peroxynitrite group(p ¼ 0.001).
3.5. Light microscopy findings
Statistical evaluation of histopathology scores is pre-sented in Graphic 5. The histopathologic evaluation

ARTICLE IN PRESS
Fig. 1. Neutrophile leukocyte infiltration, perivascular oedema and
marked partial destruction in the lung structure were observed in the
peroxynitrite group.
Fig. 2. The histopathologic appearance in the treatment group was
consistent with normal lung histopathology.
Fig. 3. Epithelial desquamation, fresh bleeding sites in the submucosa and
congestion in peroxynitrite group trachea.
Fig. 4. No pathologic change was observed in the treatment group
trachea.
E. Ayan et al. / Pulmonary Pharmacology & Therapeutics 21 (2008) 201–207 205
demonstrated that there were significant differences be-tween the peroxynitrite group and the treatment group inall time groups according to our scoring (p ¼ 0.001).Neutrophile leukocyte infiltration, perivascular oedemaand marked partial destruction in the lung structure wereobserved at the 24th and 48th h in the peroxynitrite group.The increase at the 24th and 48th h was statisticallysignificant in comparison to the 2nd h (po0.05) (Fig. 1).The histopathologic appearance in the treatment groupwas consistent with normal lung histopathology (Fig. 2).The histopathologic evaluation of the trachea showedepithelial desquamation, fresh bleeding sites in the sub-mucosa and congestion that started at the 2nd h andbecame marked at the 48th h (Fig. 3). No pathologicchange was observed in the treatment group (Fig. 4). As
there would be otherwise too many pictures, we preferredonly those representing maximum damage and theirtreatment counterparts namely the histopathological ap-pearances at 24th h.
4. Discussion
This study demonstrated that intratracheal administra-tion of peroxynitrite can cause inflammatory and degen-erative changes in the airway epithelium as Farshid et al.published in their paper. They used MDA, MPO andhistopathologic examination as indices of the pathologicchanges at various time intervals (2nd, 24th and 48th h)following intratracheal administration of peroxynitrite [9].In this present study, we used the same model with the

ARTICLE IN PRESSE. Ayan et al. / Pulmonary Pharmacology & Therapeutics 21 (2008) 201–207206
addition of an extra index, tissue 3-NT, to test the effects oflornoxicam on peroxynitrite induced tracheobronchial andpulmonary tissue damage. The significant increase in tissue3-NT, tissue and serum MDA levels and MPO activitydocumented that peroxynitrite-triggered inflammation andtissue damage became evident 2 h after instillation andcontinued along 24th and 48th h. Maximum pathologicfindings were obtained in peroxynitrite group at 24th h witha statistically insignificant remission at 48th h. Besidebiochemical studies, histopathologic examination alsoconfirmed pulmonary and tracheal tissue damage followingperoxynitrite instillation. In the peroxynitrite group, BALfluid contained statistically significantly higher PMNcounts at all three time intervals when compared to controland treatment groups. All of these findings show clearlythat peroxynitrite leads to inflammatory reaction and tissuedamage. On the other hand, the data obtained fromtherapy group demonstrated statistically significant remis-sion of both biochemical and histopathologic abnormalfindings observed in peroxynitrite group throughout 48 h.
During progression of many pulmonary and systemicpathologic processes such as trauma, sepsis, endotoxemia,pneumonia and ischemia/reperfusion to acute lung injury(ALI) and/or ARDS, a lot of mediators including freeoxygen radicals (FOR) and reactive nitrogen species (RNS)are involved [14,15]. One of these compounds, NO, isthought to be closely participated in oxidative pathophy-siologic processes in many organ systems including thelungs since it has been shown repetitively that excessivelyproduced NO can react with superoxide radicals to formthe very toxic substance, peroxynitrite [16–19]. A previousstudy performed on rats revealed the occurrence ofpulmonary injury as remote organ damage followingintestinal ischemia/reperfusion which was documented bythe increase in pulmonary tissue MDA and 3-NT/totaltyrosine ratio due to the increase in NO and peroxynitritelevels [20]. Similarly, in a foregoing study of ours, hindlimb ischemia-reperfusion in rats resulted in lung injury asremote organ damage which we demonstrated biochemi-cally by lung tissue-MDA, 3-NT and -MPO activity andhistopathologically by tissue and broncoalveolar fluidexamination [21]. Some in vivo experiments on pigs andrabbits and some in vitro studies revealed that directadministration of peroxynitrite to the airways, also, causeddamage to the epithelial and bronchial smooth muscle cells[1–3,9,22–24]. Our findings in this present study are, also,in concordance with the results of previous similar studiesof other investigators in respect to tissue and serum MPOactivity, MDA levels and histopathological damage.Lor-noxicam has been demonstrated to inhibit the formation ofvarious metabolites on the cyclo-oxygenase branch of thearachidonic acid pathway. In in vitro tests, lornoxicaminhibited both cyclo-oxygenase isoenzymes with similarpotency [25]. Lornoxicam has, also, been shown to inhibitthe migration of PMN leukocytes, the production of NO inendotoxin-stimulated macrophages and the release ofsuperoxide from human PMN leukocytes [4,5]. Therefore,
it can be concluded that lornoxicam can significantlydiminish tissue damage by reducing the formation ofperoxynitrite since it inhibits the formation of bothreactants of peroxynitrite, NO and superoxide. The reviewof the related literature did not return any study which wasdesigned to selectively evaluate the anti-inflammatoryproperties of lornoxicam on the lungs. For the determina-tion of the extent of the peroxynitrite-induced tissuedamage and its correlation with biochemical changes, weused MDA as the indicator of excessive lipid peroxidation,3-NT as the end product of FOR and RNS formation andMPO activity as an indicator of PMN leukocyte accumula-tion. The data of the treatment group were not significantlydifferent from the values obtained from the control groupdemonstrating the efficiency of lornoxicam treatment.As mentioned before; inflammatory cells especially
macrophages contribute greatly to the formation ofperoxynitrite and thus 3-NT but proportionally negligibleamounts of 3-NT are also produced by sources such asmyeloperoxidase, lactoperoxidase and lipogenase, whichare nitrating agents [22,26–30]. In a study performed onrats, direct intratracheal administration of peroxynitriteresulted in diffuse epithelial and submucosal staining of 3-NT whose intensity closely correlated with the degree oflocal oxidative tissue damage [29]. In this current study, wehave also obtained significantly higher tissue 3-NT levelsfrom the peroxynitrite group than those from the controlgroup (p ¼ 0.0001). This elevation was found to descendsignificantly in the treatment group (p ¼ 0.0001).Muijsers et al. reported a significant increase in PMN
leukocyte count in BLFA with a peak level at 48thhfollowing direct intratracheal installation of peroxynitrite[29]. Our findings were in concordance with theirs except thatwe obtained the peak levels at 24thh. The values obtainedfrom the treatment group were significantly lower than thevalues received from the peroxynitrite group. Farshid et al.demonstrated tracheobronchial oedema, congestion andinfiltration and focal pulmonary congestion and alveolarexudation 2h after intratracheal peroxynitrite inoculation [9].They reported progression of the inflammatory processduring the first 48h which included alveolar exudation withdiffuse infiltration. Our macroscopic and histopathologicexaminations revealed similar results with statistically sig-nificant amelioration in the treatment group.In this study, we demonstrated that lornoxicam can
inhibit oxidative tissue damage in the trachea and the lungsinduced with direct intratracheal application of peroxyni-trite. We believe that this effect of lornoxicam is not only aresult of cyclo-oxygenase inhibition but also is attributableto its NO and superoxide inhibitory properties asmentioned in the literature.
References
[1] Muijsers RB, Folkerts G, Henricks PA, Sadeghi-Hashjin G, Nijkamp
FP. Peroxynitrite: a two-faced metabolite of nitric oxide. Life Sci
1997;60(21):1833–45.

ARTICLE IN PRESSE. Ayan et al. / Pulmonary Pharmacology & Therapeutics 21 (2008) 201–207 207
[2] Sadeghi-Hashjin G, Folkerts G, Henricks PA, Muijsers RB, Nijkamp
FP. Peroxynitrite in airway diseases. Clin Exp Allergy
1998;28:1464–73.
[3] Sadeghi-Hashjin G, Folkerts G, Henricks PA, Verheyen AK, van der
Linde HJ, van Ark I, et al. Peroxynitrite induces airway hyperrespon-
siveness in guinea pigs in vitro and in vivo. Am J Respir Crit Care
Med 1996;153(5):1697–701.
[4] Pruss TP, Stroibnig H, Welte SR, Wendtlandt W, Mehdi N, Takacs
F, et al. Overview of the pharmacological properties, pharmacoki-
netics and animal safety assessment of lornoxicam. Postgrad Med J
1990;66(4):18–21.
[5] Welte SR, Rabasseda X. Lornoxicam. A new potent NSAID with an
improved tolerability profile. Drugs Today 2000;36(1):55–76.
[6] Berg J, Fellier H, Christoph T, Grarup J, Stimmedder D. The
analgesic NSAID lornoxicam inhibits cyclooxygenase (COX)-1-2,
inducible nitric oxide syntase (iNOS), and the formation of
interleukin (IL-6) in vitro. Inflamm Res 1999;48:369–79.
[7] Bianchi M, Paneria A. Effects of Lornoxicam, piroxicam and
meloxicam in a model of thermal hindpaw hyperalgesia induced by
formalin injection in rat trial. Pharma Res 2002;45(2):101–5.
[8] Proctor LM, Strachan AJ, Woodruff TM, Mahadevan IB, Williams
HM, Mahadevan IB, et al. Completed inhibitors selectively attenuate
injury follow administration of cobra venom factor to rats. Int
Immunopharmacol 2006;6:1224–32.
[9] Farshid AA, Sadeghi-Hashjin G, Ferdowsi HR. Histopathological
studies on the effects of peroxynitrite on the lungs and trachea of
rabbits. Eur Respir J 2002;20:1014–6.
[10] Yagi K. Lipid peroxides and related radicals in clinical medicine. In:
Armstrong D, editor. Free radicals in diagnostic medicine. New
York: Plenum Press; 1994. p. 1–15.
[11] Golowich SP, Kaplan SD. Methods in enzymology. vol. II, New
York: ACA Press Inc; 1955, p. 769.
[12] Sucu N, Unlu A, Tamer L, Aytacoglu B, Ercan B, Dikmengil M,
et al. 3-Nitrotyrosine in atherosclerotic blood vessels. Clin Chem Lab
Med 2003;41:23–5.
[13] Ozdulger A, Cinel I, Koksel O, Cinel L, Avlan D, Unlu A, et al. The
protective effect of N-acetylcysteine on apoptotic lung injury in CLP-
induced sepsis model. Shock 2003;19(4):366–72.
[14] Chabot F, Mitchell JA, Gutteridge JMC, Evans TW. Reactive
oxygen species in acute lung injury. Eur Respir J 1998;11:745–57.
[15] Chu SJ, Chang DM, Wang D, Hsu K, Chiang CH. Protective effect
of lipophilic antioxidants on phorbol-induced acute lung injury in
rats. Crit Care Med 2001;29(4):819–24.
[16] Lang JD, McArdle PJ, O’Reilly PJ, Matalon S. Oxidants-antiox-
idants balance in acute lung injury. Chest 2002;122:314–20.
[17] Beckman JS, Beckman TW, Chen J, Marshall BA, Freeman BA.
Apparent OH radical production from peroxynitrite. Implications for
endothelial injury by nitric oxide and superoxide. Proc Natl Acad Sci
USA 1990;87:1620–4.
[18] Beckman JS, Koppenol WH. Nitric oxide, superoxide and peroxyni-
trite: the good the bad and the ugly. Am J Physiol 1996;271:
1424–37.
[19] Pryor WA, Squadrito GL. The chemistry of peroxynitrite: a product
from the reaction of nitric oxide with superoxide. Am J Physiol
1995;268:699–722.
[20] Zhou JL, Jin GH, Yi YL, Zhang JL, Huang XL. Role of nitric oxide
and peroxynitrite anion in lung injury induced by intestinal ischemia-
reperfusion in rats. World J Gastroenterol 2003;9(6):1318–22.
[21] Koksel O, Yildirim C, Cinel L, Tamer L, Ozdulger A, Basturk M,
et al. Inhibition of poly (ADP-ribose) polymerase attenuates lung
tissue damage after hind limb ischemia-reperfusion in rats. Pharma-
col Res 2005;51(5):453–62.
[22] Koksel O, Cinel I, Tamer L, Cinel L, Ozdulger A, Kanik A, et al. N-
acetylcysteine inhibits peroxynitrite-mediated damage in oleic acid-
induced lung injury. Pulm Pharmacol Ther 2004;17:263–70.
[23] Yang C, Moriuchi H, Takase J, Ishitsuka Y, Irikura M, Irei T.
Oxidative stress in early stage of acute lung injury induced with oleic
acid in guinea pigs. Biol Pharm Bull 2003;26(4):424–8.
[24] Hammerschmidt S, Buchler N, Wahn H. Tissue lipid peroxidation
and reduced glutathione depletion in hypochlorite-induced lung
injury. Chest 2002;121:573–81.
[25] Pruss TP, Stroissing H, Radhofer-Welte S, Wendtlandt W, Tacaks F,
Fellier H. Overview of the pharmacological properties, pharmacoki-
netics and animal safety assessment of lornoxicam. Postgrad Med J
1990;66(Suppl. 4):S18–21.
[26] Van der Vliet A, Eiserich JP, Halliwell B, Cross CE. Formation of
reactive nitrogen species during peroxidase-catalyzed oxidation of
nitrite. A potential additional mechanism of nitric oxide-dependent
toxicity. J Biol Chem 1997;272:7617–25.
[27] Marcontes S, Turko VI, Murad F. Nitration of succinyl-CoA: 3-
oxoacid CoA-transferase in rats after endotoxin administration. Proc
Natl Acad Sci USA 2001;98:7146–51.
[28] Leeuvenburgh C, Hary MH, Hazen SL, Wagner P, Oh-Ishi S,
Steinbrecher UP, et al. Reactive nitrogen intermediates a promote
low density lipoprotein oxidation in human atherosclerotic intima. J
Biol Chem 1997;272:1433–6.
[29] Muijsers RBR, Van der Veeken A, Habernickel J, Folkerts G,
Postma DS, Nijkamp FP. Intra-luminal exposure of murine airways
to peroxynitrite causes inflammation but not hyperresponsiveness.
Inflam Resp 2002;51:33–7.
[30] Van der Vliet A, Smith D, O’Neill CA, Kaur H, Usmar VD, Cross
CE, et al. Interactions of peroxynitrite with human plasma and its
constituents: oxidative damage and antioxidant depletion. Biochem J
1994;303:295–301.
Copyright © 2022 FDOKUMEN




















