
Effects of aggressive blood pressure control in normotensive type 2 diabetic patients on...
12
Kidney International, Vol. 61 (2002), pp. 1086–1097 Effects of aggressive blood pressure control in normotensive type 2 diabetic patients on albuminuria, retinopathy and strokes ROBERT W. SCHRIER,RAYMOND O. ESTACIO,ANNE ESLER, and PHILIP MEHLER Division of Renal Diseases and Hypertension, Department of Medicine, University of Colorado Health Sciences Center, and Department of Internal Medicine, Denver Health and the University of Colorado Health Sciences Center, Denver, Colorado, USA (128/75 mm Hg) BP control in normotensive type 2 diabetic Effects of aggressive blood pressure control in normotensive patients: (1) slowed the progression to incipient and overt dia- type 2 diabetic patients on albuminuria, retinopathy and betic nephropathy; (2) decreased the progression of diabetic strokes. retinopathy; and (3) diminished the incidence of stroke. Background. Although several important studies have been performed in hypertensive type 2 diabetic patients, it is not known whether lowering blood pressure in normotensive (BP 140/90 mm Hg) patients offers any beneficial results on Diabetes mellitus is the most common cause of end- vascular complications. The current study evaluated the effect stage renal disease (ESRD) [1, 2], adult blindness [3, 4] of intensive versus moderate diastolic blood pressure (DBP) control on diabetic vascular complications in 480 normotensive and amputations in the United States and is a major risk type 2 diabetic patients. factor for heart attacks and strokes [5]. Approximately Methods. The current study was a prospective, randomized 90% of diabetes is classified as type 2 or non-insulin controlled trial in normotensive type 2 diabetic subjects. The dependent mellitus. Since hypertension is a common ac- subjects were randomized to intensive (10 mm Hg below the companiment of type 2 diabetes in adults, there have baseline DBP) versus moderate (80 to 89 mm Hg) DBP control. Patients in the moderate therapy group were given placebo, been several recent studies examining the role of differ- while the patients randomized to intensive therapy received ent antihypertensive agents in lowering blood pressure either nisoldipine or enalapril in a blinded manner as the initial in hypertensive type 2 diabetic patients. A beneficial antihypertensive medication. The primary end point evaluated effect of diuretics [6], beta blockers [7], angiotensin-con- was the change in creatinine clearance with the secondary verting enzyme (ACE) inhibitors [8] and calcium chan- endpoints consisting of change in urinary albumin excretion, progression of retinopathy and neuropathy and the incidence nel blockers (CCBs) [9, 10] in lowering blood pressure of cardiovascular disease. and decreasing vascular complications in type 2 diabetic Results. The mean follow-up was 5.3 years. Mean BP in the patients have been demonstrated. In most of these stud- intensive group was 128 0.8/75 0.3 mm Hg versus 137 ies however these agents have been compared against 0.7/81 0.3 mm Hg in the moderate group, P 0.0001. Al- placebo, therefore significant differences in blood pres- though no difference was demonstrated in creatinine clearance (P 0.43), a lower percentage of patients in the intensive group sure have occurred. The Appropriate Blood Pressure progressed from normoalbuminuria to microalbuminuria (P Control in Diabetes (ABCD) study in hypertensive pa- 0.012) and microalbuminuria to overt albuminuria (P 0.028). tients [11], and the United Kingdom Prospective Diabe- The intensive BP control group also demonstrated less progres- tes Study (UKPDS) have compared different levels of sion of diabetic retinopathy (P 0.019) and a lower incidence blood pressure control in hypertensive type 2 diabetic of strokes (P 0.03). The results were the same whether enalapril or nisoldipine was used as the initial antihypertensive patients. In the UKPDS study the less tight blood pres- agent. sure goal was 180/105 mm Hg and the tight blood Conclusion. Over a five-year follow-up period, intensive pressure goal was 150/85 mm Hg [7], whereas in the hypertensive ABCD study, the diastolic blood pressure goals were 80 to 89 mm Hg (moderate) and 75 mm Hg Key words: type 2 diabetes, hypertensive therapy, microvascular com- plications. (intensive). While these above studies have added a great deal of Received for publication June 6, 2001 understanding about the effects of treating hypertension and in revised form October 9, 2001 Accepted for publication October 10, 2001 on micro-and macrovascular complications in type 2 dia- betic patients, they do not address the question whether 2002 by the International Society of Nephrology 1086
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Effects of aggressive blood pressure control in normotensive type 2 diabetic patients on...

Kidney International, Vol. 61 (2002), pp. 1086–1097
Effects of aggressive blood pressure control in normotensivetype 2 diabetic patients on albuminuria, retinopathyand strokes
ROBERT W. SCHRIER, RAYMOND O. ESTACIO, ANNE ESLER, and PHILIP MEHLER
Division of Renal Diseases and Hypertension, Department of Medicine, University of Colorado Health Sciences Center,and Department of Internal Medicine, Denver Health and the University of Colorado Health Sciences Center,Denver, Colorado, USA
(�128/75 mm Hg) BP control in normotensive type 2 diabeticEffects of aggressive blood pressure control in normotensivepatients: (1) slowed the progression to incipient and overt dia-type 2 diabetic patients on albuminuria, retinopathy andbetic nephropathy; (2) decreased the progression of diabeticstrokes.retinopathy; and (3) diminished the incidence of stroke.Background. Although several important studies have been
performed in hypertensive type 2 diabetic patients, it is notknown whether lowering blood pressure in normotensive(BP �140/90 mm Hg) patients offers any beneficial results on
Diabetes mellitus is the most common cause of end-vascular complications. The current study evaluated the effectstage renal disease (ESRD) [1, 2], adult blindness [3, 4]of intensive versus moderate diastolic blood pressure (DBP)
control on diabetic vascular complications in 480 normotensive and amputations in the United States and is a major risktype 2 diabetic patients. factor for heart attacks and strokes [5]. Approximately
Methods. The current study was a prospective, randomized 90% of diabetes is classified as type 2 or non-insulincontrolled trial in normotensive type 2 diabetic subjects. Thedependent mellitus. Since hypertension is a common ac-subjects were randomized to intensive (10 mm Hg below thecompaniment of type 2 diabetes in adults, there havebaseline DBP) versus moderate (80 to 89 mm Hg) DBP control.
Patients in the moderate therapy group were given placebo, been several recent studies examining the role of differ-while the patients randomized to intensive therapy received ent antihypertensive agents in lowering blood pressureeither nisoldipine or enalapril in a blinded manner as the initial in hypertensive type 2 diabetic patients. A beneficialantihypertensive medication. The primary end point evaluated
effect of diuretics [6], beta blockers [7], angiotensin-con-was the change in creatinine clearance with the secondaryverting enzyme (ACE) inhibitors [8] and calcium chan-endpoints consisting of change in urinary albumin excretion,
progression of retinopathy and neuropathy and the incidence nel blockers (CCBs) [9, 10] in lowering blood pressureof cardiovascular disease. and decreasing vascular complications in type 2 diabetic
Results. The mean follow-up was 5.3 years. Mean BP in the patients have been demonstrated. In most of these stud-intensive group was 128 � 0.8/75 � 0.3 mm Hg versus 137 �ies however these agents have been compared against0.7/81 � 0.3 mm Hg in the moderate group, P � 0.0001. Al-placebo, therefore significant differences in blood pres-though no difference was demonstrated in creatinine clearance
(P � 0.43), a lower percentage of patients in the intensive group sure have occurred. The Appropriate Blood Pressureprogressed from normoalbuminuria to microalbuminuria (P � Control in Diabetes (ABCD) study in hypertensive pa-0.012) and microalbuminuria to overt albuminuria (P � 0.028). tients [11], and the United Kingdom Prospective Diabe-The intensive BP control group also demonstrated less progres-
tes Study (UKPDS) have compared different levels ofsion of diabetic retinopathy (P � 0.019) and a lower incidenceblood pressure control in hypertensive type 2 diabeticof strokes (P � 0.03). The results were the same whether
enalapril or nisoldipine was used as the initial antihypertensive patients. In the UKPDS study the less tight blood pres-agent. sure goal was �180/105 mm Hg and the tight blood
Conclusion. Over a five-year follow-up period, intensive pressure goal was �150/85 mm Hg [7], whereas in thehypertensive ABCD study, the diastolic blood pressuregoals were 80 to 89 mm Hg (moderate) and �75 mm HgKey words: type 2 diabetes, hypertensive therapy, microvascular com-
plications. (intensive).While these above studies have added a great deal ofReceived for publication June 6, 2001
understanding about the effects of treating hypertensionand in revised form October 9, 2001Accepted for publication October 10, 2001 on micro-and macrovascular complications in type 2 dia-
betic patients, they do not address the question whether 2002 by the International Society of Nephrology
1086
Schrier et al: BP control in normotensive diabetes 1087
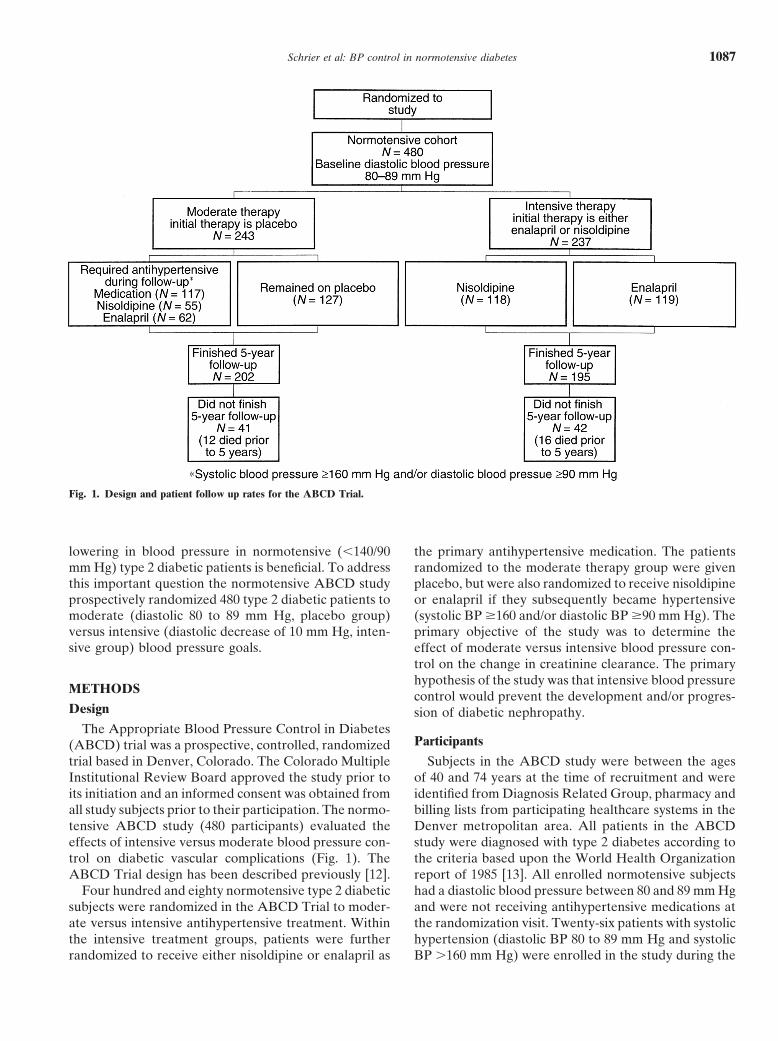
Fig. 1. Design and patient follow up rates for the ABCD Trial.
lowering in blood pressure in normotensive (�140/90 the primary antihypertensive medication. The patientsrandomized to the moderate therapy group were givenmm Hg) type 2 diabetic patients is beneficial. To address
this important question the normotensive ABCD study placebo, but were also randomized to receive nisoldipineor enalapril if they subsequently became hypertensiveprospectively randomized 480 type 2 diabetic patients to
moderate (diastolic 80 to 89 mm Hg, placebo group) (systolic BP �160 and/or diastolic BP �90 mm Hg). Theprimary objective of the study was to determine theversus intensive (diastolic decrease of 10 mm Hg, inten-
sive group) blood pressure goals. effect of moderate versus intensive blood pressure con-trol on the change in creatinine clearance. The primaryhypothesis of the study was that intensive blood pressure
METHODS control would prevent the development and/or progres-Design sion of diabetic nephropathy.
The Appropriate Blood Pressure Control in DiabetesParticipants(ABCD) trial was a prospective, controlled, randomized
trial based in Denver, Colorado. The Colorado Multiple Subjects in the ABCD study were between the agesof 40 and 74 years at the time of recruitment and wereInstitutional Review Board approved the study prior to
its initiation and an informed consent was obtained from identified from Diagnosis Related Group, pharmacy andbilling lists from participating healthcare systems in theall study subjects prior to their participation. The normo-
tensive ABCD study (480 participants) evaluated the Denver metropolitan area. All patients in the ABCDstudy were diagnosed with type 2 diabetes according toeffects of intensive versus moderate blood pressure con-
trol on diabetic vascular complications (Fig. 1). The the criteria based upon the World Health Organizationreport of 1985 [13]. All enrolled normotensive subjectsABCD Trial design has been described previously [12].
Four hundred and eighty normotensive type 2 diabetic had a diastolic blood pressure between 80 and 89 mm Hgand were not receiving antihypertensive medications atsubjects were randomized in the ABCD Trial to moder-
ate versus intensive antihypertensive treatment. Within the randomization visit. Twenty-six patients with systolichypertension (diastolic BP 80 to 89 mm Hg and systolicthe intensive treatment groups, patients were further
randomized to receive either nisoldipine or enalapril as BP �160 mm Hg) were enrolled in the study during the

Schrier et al: BP control in normotensive diabetes1088
first year of recruitment but none thereafter because of of the patient except the blood pressure control (forexample, blood glucose, lipids, smoking, etc.)the 1992 publication of the Systolic Hypertension in the
Elderly Program (SHEP) results [6]. Patients were ex- During the follow-up period, the patients’ primarycare physicians managed blood glucose control, bloodcluded if they had a known allergy to dihydropyridines
or ACE inhibitors, a myocardial infarction or cerebral lipids and anti-smoking interventions.vascular accident within the previous six months, coro-
Study end pointsnary artery bypass surgery within the previous threemonths, unstable angina pectoris within the previous six The primary endpoint was the effect of intensive ver-
sus moderate blood pressure control on the change inmonths, Class III or IV New York Heart Associationclassification of congestive heart failure, demonstrated 24-hour creatinine clearance, which was assessed every
six months. Secondary endpoints included the effect ofan absolute need for ACE inhibitors or calcium channelblockers, were receiving hemo- or peritoneal dialysis intensive versus moderate blood pressure control on car-
diovascular events, retinopathy as determined by stereo-and/or had a serum creatinine greater than 3 mg/dL.scopic retinal photographs [14], clinical neuropathy [15],
Randomization and study therapy and urinary albumin excretion [16].During the 7 to 11 week single-blind placebo run-in
Renal end pointsperiods, all baseline studies were performed. After theplacebo run-in, the mean baseline diastolic blood pres- Glomerular filtration rates (GFR) were estimated
from 24-hour creatinine clearances standardized forsure was determined at two separate visits for each pa-tient. Subjects with a mean baseline diastolic blood pres- body surface area obtained at baseline then every six
months during the course of the study. Given the nearsure between 80 and 89 mm Hg were eligible for the studyand placed in the normotensive study. Randomization normal creatinine clearances for the present group of
type 2 diabetic patients, the effect of tubular secretionoccurred using permuted block randomization withinstrata. Patients were randomized into two treatment of creatinine would be expected to be minimal. More-
over, as reported earlier, iothalamate clearances in 200arms consisting of an intensive treatment with a diastolicblood pressure goal of 10 mm Hg below the randomiza- type 2 diabetic patients in the ABCD study correlated
closely with creatinine clearance (abstract; Savage et al,tion diastolic blood pressure and moderate (placebo)treatment with a diastolic blood pressure goal between American Society of Nephrology Meeting 1993). Urinary
albumin excretion (UAE) was measured using radioim-80 to 89 mm Hg. The intensive therapy patients wererandomized to either nisoldipine 10 mg/day titrated to munoassay techniques (RAI) from 24-hour and over-
night collections at baseline and every two months there-20, 40 and then 60 mg/day (plus placebo for enalapril)or enalapril 5 mg/day titrated to 10, 20 and then 40 mg/ after following randomization. At baseline, the stage of
UAE (normoalbuminuria, microalbuminuria and overtday (plus placebo for nisoldipine) as the initial medica-tion. If the single study medication alone did not achieve albuminuria) was based on one 24-hour collection and
two overnight collections. Normoalbuminuria was de-the target blood pressure, then open-labeled antihyper-tensive medications were added in a step-wise fashion fined as less than 20 �g/min (30 mg/24 h), microalbumin-
uria as 20 to 200 �g/min (30 to 300 mg/24 h), and overtuntil the target blood pressure was achieved. Open-labeledantihypertensive medications included metoprolol and albuminuria as �200 �g/min (�300 mg/24 h). The stage
of microalbuminuria is considered incipient diabetic ne-hydrochlorothiazide. Additional antihypertensive medi-cations were added at the discretion of the medical direc- phropathy and overt albuminuria is considered estab-
lished diabetic nephropathy. Urinary albumin, sodiumtor, but did not include a calcium channel blocker orACE inhibitor. If a patient randomized to moderate and potassium excretion, and creatinine clearance were
measured by the Renal Research Laboratory at the Uni-therapy became hypertensive (systolic blood pressure�160 and/or a diastolic blood pressure �90 mm Hg on versity of Colorado Health Sciences Center.2 consecutive visits), they were given either nisoldipine
Retinopathy end pointsor enalapril according to randomization at entry into thestudy with the goal of maintaining the systolic blood Retinopathy was staged using the Modified Airlie
House Classification of Diabetic Retinopathy as waspressure �160 mm Hg and the diastolic blood pressurebetween 80 and 90 mm Hg. Blood pressure recordings adapted for the Diabetes Control and Complications
Trial by the Fundus Photograph Reading Center at thewere obtained at peak drug levels and were an averageof three seated readings obtained at each visit. Study University of Wisconsin. Seven-field stereoscopic fundus
photographs were taken on-site at baseline then at yearnurses were blinded to the use of enalapril versus nisol-dipine, but could not be blinded with respect to intensive 2 and 5 by a technician trained by the Reading Center.
All retinal films were interpreted and graded by theversus moderate blood pressure control. The patient’sprimary care physicians were responsible for the care Fundus Photograph Reading Center without knowledge

Schrier et al: BP control in normotensive diabetes 1089
of the treatment arm. The graders used the protocol nicity and the presence of diabetic complications (overtalbuminuria, microalbuminuria, retinopathy, neuropa-of the Early Treatment Diabetic Retinopathy Study
(ETDRS) [14]. The overall level of severity of retinopa- thy and cardiovascular disease)].T tests at each time point and a general linear mixedthy was determined for each patient according to the
ETDRS interim scale [17], in which a scale of 23 steps model were used when comparing change in systolic anddiastolic blood pressure (SBP and DBP) between theis used to represent the overall extent of retinopathy
in both eyes. The progression of clinically important intensive and moderate therapy groups as well as be-tween the nisoldipine and enalapril groups. Similar anal-retinopathy is defined as a change of at least two steps
from baseline measurements. yses were undertaken for glycosylated hemoglobin andtotal cholesterol. A general linear mixed model was also
Diabetic neuropathy used when evaluating the effects of blood pressure con-trol (intensive vs. moderate) over time on measures ofThe presence and progression of diabetic neuropathy
was assessed according to the criteria established by renal function [creatinine clearance and log urinary albu-min excretion (log UAE)]. The general linear model isDyck [18]. This included neurological symptoms score,
neurological disability score, autonomic nervous system ideally suited for these types of unbalanced repeatedmeasures data. Log (UAE) was used instead of UAEtesting with heart rate response to deep breathing, and
quantitative sensory examination performed at baseline because of the non-Gaussian nature of the UAE valuesas well as the extremely large variance seen in the UAEthen at year 2 and 5. Details of the exam have been
discussed previously [12]. values. To further enhance the understanding of the lon-gitudinal effects of blood pressure control on renal func-
Cardiovascular disease tion, t tests were carried out at each time point. Thesetests are especially helpful in describing interactive ef-An independent Endpoint Committee, whose mem-
bers were blinded to the study intervention arms, re- fects between blood pressure control and time.viewed all cardiovascular events. Cardiovascular out- The progression of retinopathy and neuropathy werecomes were defined as (1) death due to cardiovascular analyzed using Chi-square tests. The incidence of cardio-events (sudden death, progressive heart failure, fatal myo- vascular events was also analyzed utilizing a Chi-squarecardial infarction, fatal arrhythmias, cerebral vascular test. In addition, the progression of albuminuria overaccidents and ruptured aortic aneurysm); (2) non-fatal time was examined using Kaplan-Meier survival curvesmyocardial infarction; (3) non-fatal cerebral vascular ac- and log-rank tests.cident; (4) heart failure requiring hospital admission;and (5) pulmonary infarction. The End Point Committee
RESULTSreviewed all hospital admissions that appeared to beThere were no significant differences in the baselinerelated to a cardiovascular event.
characteristics and prevalence of clinical complicationsStatistics when comparing those patients randomized to intensive
and moderate treatment groups (Table 1) and enalaprilThe Statistical Analysis Software (SAS) system wasand nisoldipine groups (Table 2). There also was noused for all statistical analyses. Data are summarized asdifference in patient characteristics between those re-mean � standard error for continuous endpoints andceiving active drug treatment (Table 3). The baselinepercentage of relevant population for categorical vari-characteristics including important interrelationships withables. Two different statistical procedures were utilizeddiabetic complications of the ABCD Trial populationwhen examining differences in baseline characteristicshave been reported in previous publications [19–26].or the presence of diabetic complications between the
intensive and moderate therapy groups, and betweenBlood pressurethe original randomized drugs (nisoldipine or enalapril).
During the course of the study, a blood pressure sepa-When the baseline characteristic was continuous [age,ration was achieved between the intensive and moderateduration of diabetes, body mass index (BMI), glycosy-therapy groups within the first 6 to 12 months and waslated hemoglobin, systolic blood pressure (SBP), dia-maintained for the remainder of the follow-up periodstolic blood pressure (DBP) and years of education] a(Fig. 2). Thus, the mean blood pressure for the last 4two-sample t test was used. When any of these baselineyears of follow-up was 128 � 0.8/75 � 0.3 mm Hg forcharacteristics were clearly non-Gaussian distributed,the intensive antihypertensive therapy group and 137 �nonparametric analyses (that is, Wilcoxon’s Rank Sum0.7/81 � 0.3 mm Hg for the moderate antihypertensiveTest) or parametric analyses on suitably transformedtherapy group, P � 0.0001, were utilized as the bloodvariables were performed. Chi-square analyses were un-pressure achieved during the study. There were no differ-dertaken when the baseline characteristic or complica-
tion was categorical [gender, smoking status, race/eth- ences in systolic and diastolic blood pressures during the
Schrier et al: BP control in normotensive diabetes1090
Table 2. Patient baseline characteristics and complications atTable 1. Patient baseline characteristics and complicationsat baseline according to intensive and moderate blood baseline according to enalapril and nisoldipine assignment
pressure therapyEnalapril Nisoldipine
Characteristic (N � 246) (N � 234)Intensive therapy Moderate therapyCharacteristic (N � 237) (N � 243)
Age at randomization 59.4�0.5 59.1�0.5% Male 53.3 56.0Age 58.5�0.6 59.6�0.5
% Male 53 56 Diabetes duration years 8.8 �0.4 9.2�0.5Glycosylated hemoglobin % 11.5 �0.2 11.6�0.2Diabetes duration years 8.8�0.5 9.2�0.5
Glycosylated hemoglobin % 11.5�0.2 11.6�0.2 Body mass index kg/m2 31.5 �0.4 31.5�0.4% Smoking statusBody mass index kg/m2 31.5�0.4 31.5�0.4
% Smoking status Past 45.5 46.2Current 12.6 13.7Past 49 42
Current 13 13 Systolic blood pressure atrandomization mm Hg 137.4�0.9 135.4�0.8Systolic blood pressure at
randomization mm Hg 135.6�0.8 137.2�0.9 Diastolic blood pressure atrandomization mm Hg 84.5 �0.2 84.3�0.2Diastolic blood pressure at
randomization mm Hg 84.4�0.2 84.4�0.2 Years of education 13.4�0.2 13.5�0.2Race and ethnicityYears of education 13.7�0.2 13.2�0.2
Race and ethnicity Non-Hispanic white 74.0 72.7African American 8.1 6.0Non-Hispanic white 75 72
African-American 7 7 Hispanics 15.5 19ComplicationsHispanics 16 18
Complications % with overt albuminuria 11 11% with microalbuminuria 23 23% with overt albuminuria 9.3 12
% with microalbuminuria 21 25 % with diabetic retinopathy 48.7 50.7% with diabetic neuropathy 43.7 43.5% with diabetic retinopathy 50 50
% with diabetic neuropathy 42 45 % with CAD 23 25% with CHF 1.6 2.1% with CAD 21 27
% with CHF 2 2 % with CVA 3.3 3.0% with CVA 3 4 Data are � SE or percent. Patents randomized to the moderate therapy group
were initially given placebo.Data are presented as means � SE. or percent. Overt albuminuria is definedas urinary albumin excretion �200 �gm/min (�300 mg/day). Microalbuminuriais defined as urinary albumin excretion between 20–200 �gm/min (30–300 mg/day). CVD (cardiovascular disease) is defined as those with a previous historyof coronary artery disease, cerebral vascular accident and/or congestive heartfailure; angina by Rose Questionnaire; an abnormal ankle-brachial index; and/orleft ventricular hypertrophy by electrocardiogram.
Table 3. Characteristics of patients given a drug (intensive therapy,N � 237; moderate therapy, N � 117) using values closest to the
first time the drug was givenfollow-up period when comparing patients randomized
Enalapril Nisoldipineto nisoldipine, 132.1 � 0.7/78.0 � 0.4 mm Hg, versus Characteristic (N � 181) (N � 173) P valueenalapril, 132.4 � 0.9/78.0 � 0.4 mm Hg, P � 0.8. By
Age at randomization 59.6�0.6 58.9�0.6 0.47the end of the study, 117 (48%) of patients initially ran- % Male 50.3 55.5 0.33
Diabetes duration years 9.4 �0.5 9.6�0.6 0.71domized to the moderate therapy group (placebo) devel-Glycosylated hemoglobin % 11.6 �0.3 11.3�0.2 0.51oped hypertension (DBP �90 mm Hg and/or SBP �160Body mass index kg/m2 31.4 �0.5 31.6�0.5 0.76
mm Hg) requiring use of antihypertensive medications % Smoking statusPast 45.3 49.7 0.28to lower their diastolic blood pressure between the 80Current 10.5 13.9and 90 mm Hg range or their systolic blood pressure
Systolic blood pressure atbelow 160 mm Hg (Fig. 1). These patients in the moder- randomization mm Hg 141.7 �1.2 137.6�1.0 0.01
Diastolic blood pressure atate therapy group were then given nisoldipine or enala-randomization mm Hg 85.9 �0.3 85.5�0.3 0.35pril rather than placebo according to their initial random-
Years of education 13.5�0.2 13.6�0.2 0.90ization scheme. Race and ethnicity 0.18
Non-Hispanic white 74.0 74.0No significant difference was noted between the inten-African American 9.4 4.6sive and moderate groups with regard to allocation ofHispanics 14.4 19.1
metoprolol (18% in the intensive and 15% in the moder- Complications% with overt albuminuria 13.9 (N � 25) 12.1 0.89ate blood pressure group, P � 0.33) and hydrochlorothia-% with microalbuminuria 21.7 (N � 39) 22.0 0.89zide (37% in the intensive and 30% in the moderate% with diabetic
blood pressure group, P � 0.15) as additional antihyper- retinopathy 49.1 (N � 84) 53.7 0.67% with diabetictensive medication. Within the intensive and moderate
neuropathy 43.9 (N � 79) 46.8 0.48therapy groups, there was no significant difference be-% with CAD 21.6 (N � 39) 22 0.92
tween the major antihypertensive medications used (ena- % with CHF 2.2 2.3 0.99% with CVA 2.2 4.1 0.37lapril, nisoldipine and hydrochlorothiazide) except forData are � SE or percent.the patients randomized to enalapril in which more pa-
Schrier et al: BP control in normotensive diabetes 1091
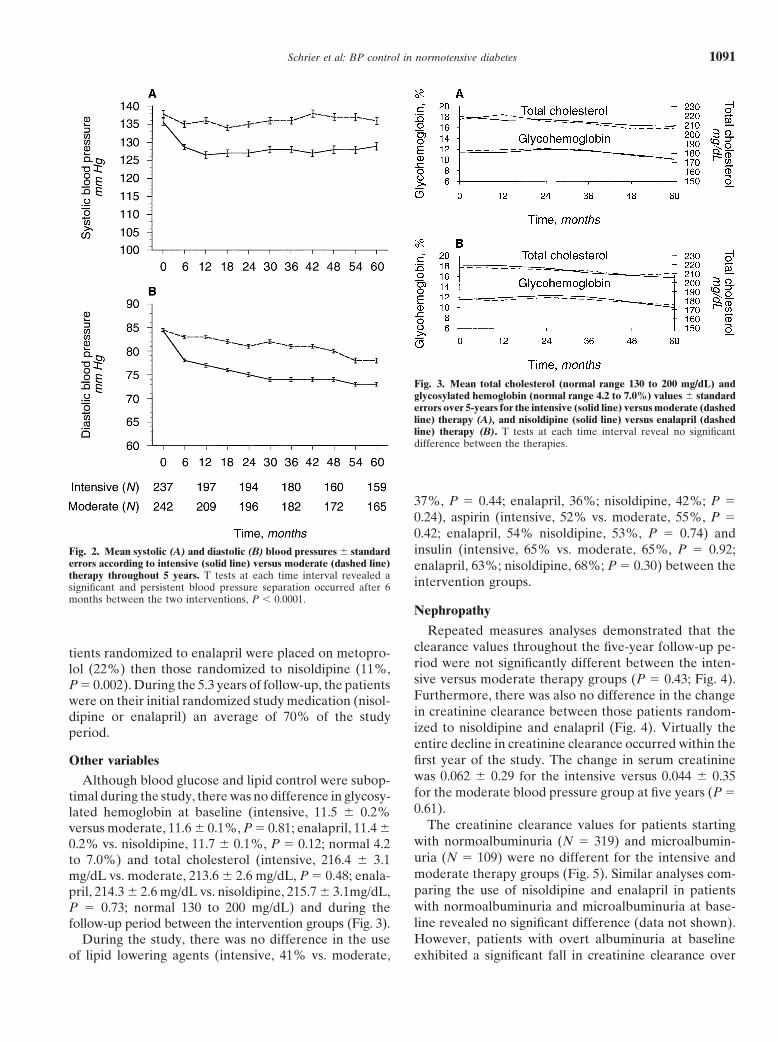
Fig. 3. Mean total cholesterol (normal range 130 to 200 mg/dL) andglycosylated hemoglobin (normal range 4.2 to 7.0%) values � standarderrors over 5-years for the intensive (solid line) versus moderate (dashedline) therapy (A), and nisoldipine (solid line) versus enalapril (dashedline) therapy (B). T tests at each time interval reveal no significantdifference between the therapies.
37%, P � 0.44; enalapril, 36%; nisoldipine, 42%; P �0.24), aspirin (intensive, 52% vs. moderate, 55%, P �0.42; enalapril, 54% nisoldipine, 53%, P � 0.74) andinsulin (intensive, 65% vs. moderate, 65%, P � 0.92;Fig. 2. Mean systolic (A) and diastolic (B) blood pressures � standard
errors according to intensive (solid line) versus moderate (dashed line) enalapril, 63%; nisoldipine, 68%; P � 0.30) between thetherapy throughout 5 years. T tests at each time interval revealed a intervention groups.significant and persistent blood pressure separation occurred after 6months between the two interventions, P � 0.0001.
Nephropathy
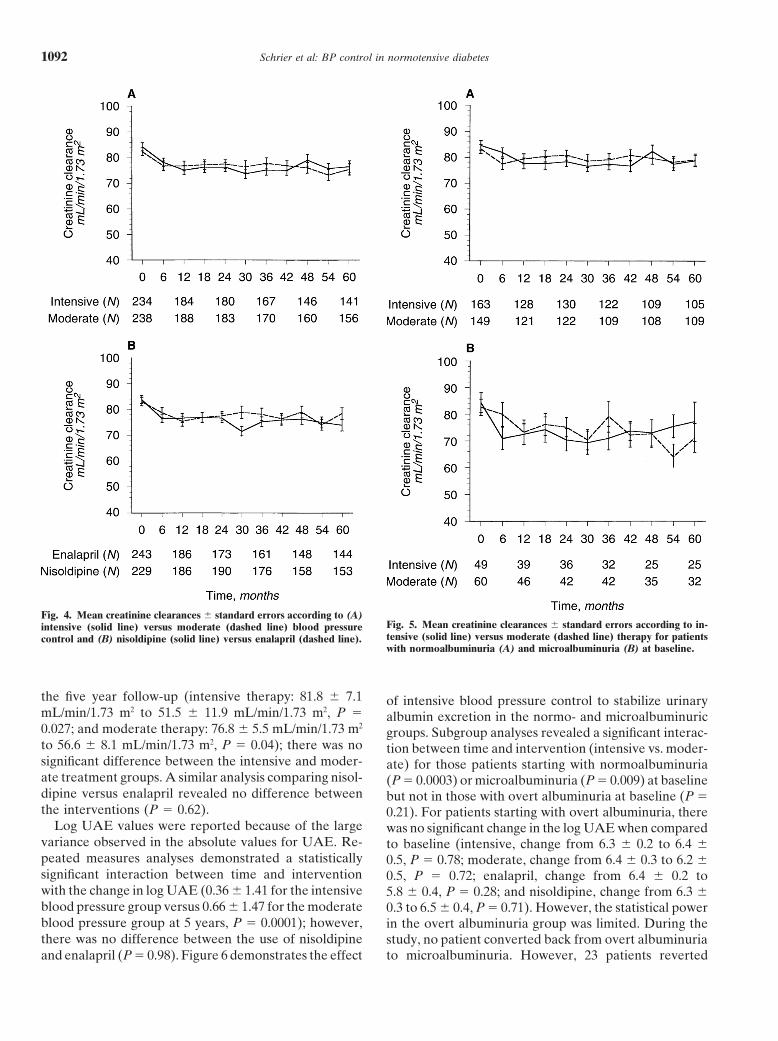
Repeated measures analyses demonstrated that theclearance values throughout the five-year follow-up pe-tients randomized to enalapril were placed on metopro-riod were not significantly different between the inten-lol (22%) then those randomized to nisoldipine (11%,sive versus moderate therapy groups (P � 0.43; Fig. 4).P � 0.002). During the 5.3 years of follow-up, the patientsFurthermore, there was also no difference in the changewere on their initial randomized study medication (nisol-in creatinine clearance between those patients random-dipine or enalapril) an average of 70% of the studyized to nisoldipine and enalapril (Fig. 4). Virtually theperiod.entire decline in creatinine clearance occurred within thefirst year of the study. The change in serum creatinineOther variableswas 0.062 � 0.29 for the intensive versus 0.044 � 0.35Although blood glucose and lipid control were subop-for the moderate blood pressure group at five years (P �timal during the study, there was no difference in glycosy-0.61).lated hemoglobin at baseline (intensive, 11.5 � 0.2%
The creatinine clearance values for patients startingversus moderate, 11.6 � 0.1%, P � 0.81; enalapril, 11.4 �with normoalbuminuria (N � 319) and microalbumin-0.2% vs. nisoldipine, 11.7 � 0.1%, P � 0.12; normal 4.2uria (N � 109) were no different for the intensive andto 7.0%) and total cholesterol (intensive, 216.4 � 3.1moderate therapy groups (Fig. 5). Similar analyses com-mg/dL vs. moderate, 213.6 � 2.6 mg/dL, P � 0.48; enala-paring the use of nisoldipine and enalapril in patientspril, 214.3 � 2.6 mg/dL vs. nisoldipine, 215.7 � 3.1mg/dL,with normoalbuminuria and microalbuminuria at base-P � 0.73; normal 130 to 200 mg/dL) and during theline revealed no significant difference (data not shown).follow-up period between the intervention groups (Fig. 3).However, patients with overt albuminuria at baselineDuring the study, there was no difference in the use
of lipid lowering agents (intensive, 41% vs. moderate, exhibited a significant fall in creatinine clearance over
Schrier et al: BP control in normotensive diabetes1092
Fig. 4. Mean creatinine clearances � standard errors according to (A)Fig. 5. Mean creatinine clearances � standard errors according to in-intensive (solid line) versus moderate (dashed line) blood pressuretensive (solid line) versus moderate (dashed line) therapy for patientscontrol and (B) nisoldipine (solid line) versus enalapril (dashed line).with normoalbuminuria (A) and microalbuminuria (B) at baseline.
the five year follow-up (intensive therapy: 81.8 � 7.1 of intensive blood pressure control to stabilize urinarymL/min/1.73 m2 to 51.5 � 11.9 mL/min/1.73 m2, P � albumin excretion in the normo- and microalbuminuric0.027; and moderate therapy: 76.8 � 5.5 mL/min/1.73 m2
groups. Subgroup analyses revealed a significant interac-to 56.6 � 8.1 mL/min/1.73 m2, P � 0.04); there was no tion between time and intervention (intensive vs. moder-significant difference between the intensive and moder- ate) for those patients starting with normoalbuminuriaate treatment groups. A similar analysis comparing nisol- (P � 0.0003) or microalbuminuria (P � 0.009) at baselinedipine versus enalapril revealed no difference between but not in those with overt albuminuria at baseline (P �the interventions (P � 0.62). 0.21). For patients starting with overt albuminuria, there
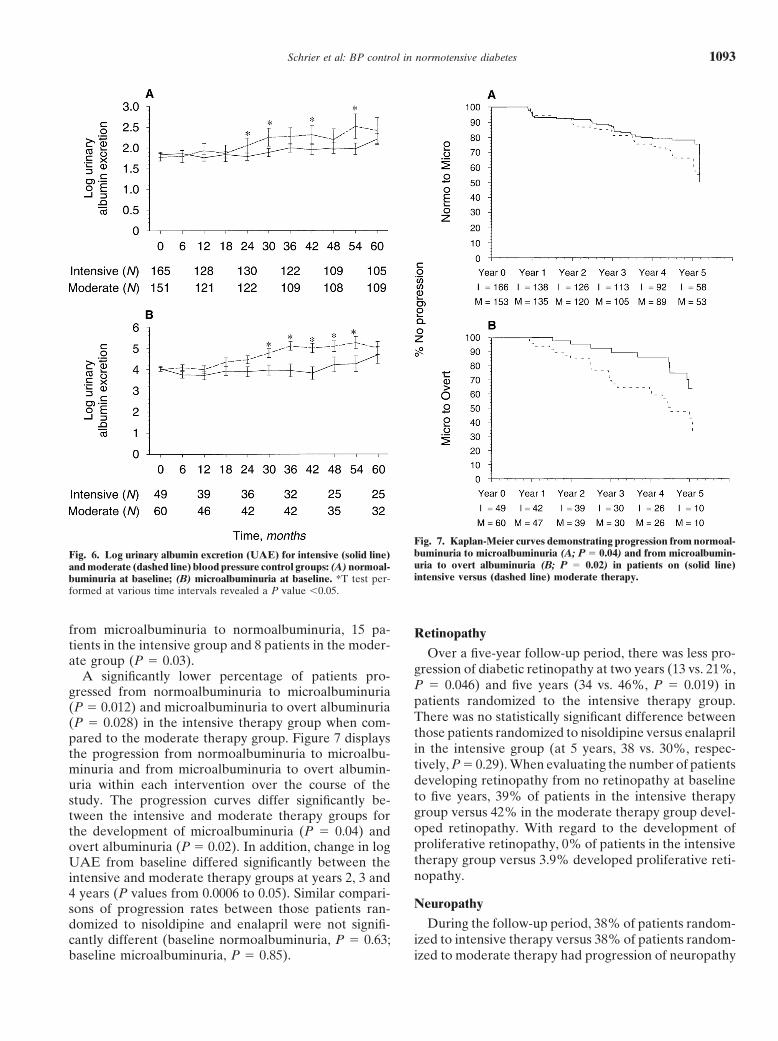
Log UAE values were reported because of the large was no significant change in the log UAE when comparedvariance observed in the absolute values for UAE. Re- to baseline (intensive, change from 6.3 � 0.2 to 6.4 �peated measures analyses demonstrated a statistically 0.5, P � 0.78; moderate, change from 6.4 � 0.3 to 6.2 �significant interaction between time and intervention 0.5, P � 0.72; enalapril, change from 6.4 � 0.2 towith the change in log UAE (0.36 � 1.41 for the intensive 5.8 � 0.4, P � 0.28; and nisoldipine, change from 6.3 �blood pressure group versus 0.66 � 1.47 for the moderate 0.3 to 6.5 � 0.4, P � 0.71). However, the statistical powerblood pressure group at 5 years, P � 0.0001); however, in the overt albuminuria group was limited. During thethere was no difference between the use of nisoldipine study, no patient converted back from overt albuminuria
to microalbuminuria. However, 23 patients revertedand enalapril (P � 0.98). Figure 6 demonstrates the effect
Schrier et al: BP control in normotensive diabetes 1093
Fig. 7. Kaplan-Meier curves demonstrating progression from normoal-buminuria to microalbuminuria (A; P � 0.04) and from microalbumin-Fig. 6. Log urinary albumin excretion (UAE) for intensive (solid line)uria to overt albuminuria (B; P � 0.02) in patients on (solid line)and moderate (dashed line) blood pressure control groups: (A) normoal-intensive versus (dashed line) moderate therapy.buminuria at baseline; (B) microalbuminuria at baseline. *T test per-
formed at various time intervals revealed a P value �0.05.
from microalbuminuria to normoalbuminuria, 15 pa- Retinopathytients in the intensive group and 8 patients in the moder-
Over a five-year follow-up period, there was less pro-ate group (P � 0.03).gression of diabetic retinopathy at two years (13 vs. 21%,A significantly lower percentage of patients pro-P � 0.046) and five years (34 vs. 46%, P � 0.019) ingressed from normoalbuminuria to microalbuminuriapatients randomized to the intensive therapy group.(P � 0.012) and microalbuminuria to overt albuminuriaThere was no statistically significant difference between(P � 0.028) in the intensive therapy group when com-those patients randomized to nisoldipine versus enalaprilpared to the moderate therapy group. Figure 7 displaysin the intensive group (at 5 years, 38 vs. 30%, respec-the progression from normoalbuminuria to microalbu-tively, P � 0.29). When evaluating the number of patientsminuria and from microalbuminuria to overt albumin-developing retinopathy from no retinopathy at baselineuria within each intervention over the course of theto five years, 39% of patients in the intensive therapystudy. The progression curves differ significantly be-group versus 42% in the moderate therapy group devel-tween the intensive and moderate therapy groups foroped retinopathy. With regard to the development ofthe development of microalbuminuria (P � 0.04) andproliferative retinopathy, 0% of patients in the intensiveovert albuminuria (P � 0.02). In addition, change in logtherapy group versus 3.9% developed proliferative reti-UAE from baseline differed significantly between thenopathy.intensive and moderate therapy groups at years 2, 3 and
4 years (P values from 0.0006 to 0.05). Similar compari-Neuropathysons of progression rates between those patients ran-
During the follow-up period, 38% of patients random-domized to nisoldipine and enalapril were not signifi-ized to intensive therapy versus 38% of patients random-cantly different (baseline normoalbuminuria, P � 0.63;
baseline microalbuminuria, P � 0.85). ized to moderate therapy had progression of neuropathy
Schrier et al: BP control in normotensive diabetes1094
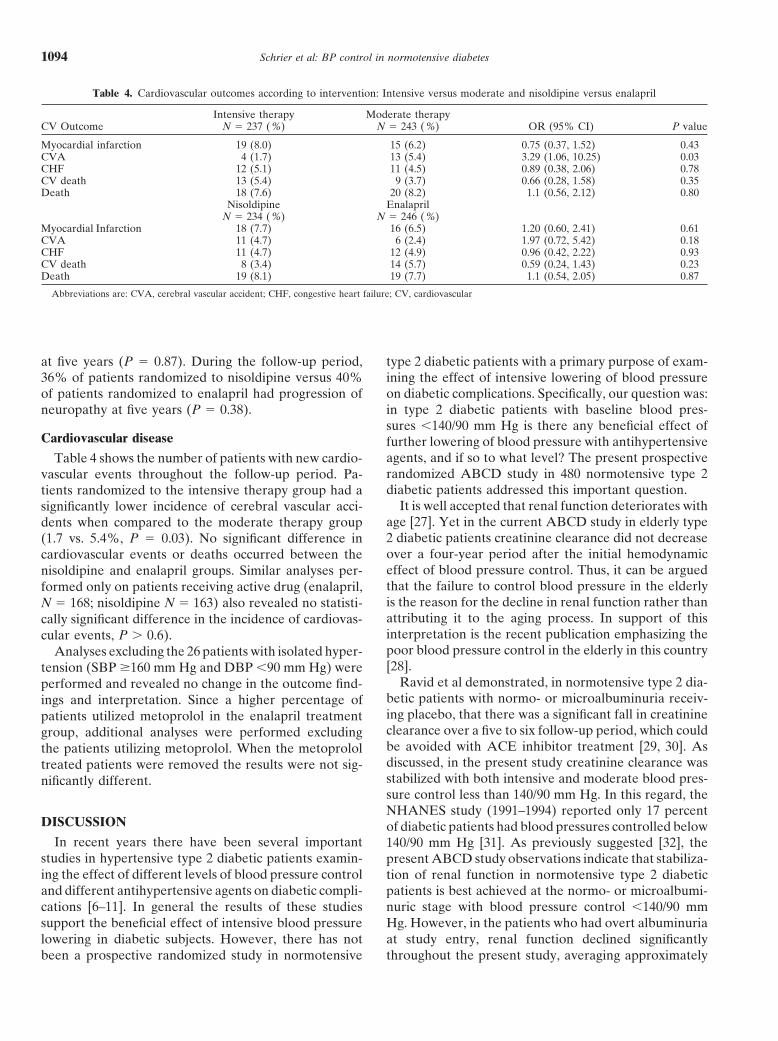
Table 4. Cardiovascular outcomes according to intervention: Intensive versus moderate and nisoldipine versus enalapril
Intensive therapy Moderate therapyCV Outcome N � 237 (%) N � 243 (%) OR (95% CI) P value
Myocardial infarction 19 (8.0) 15 (6.2) 0.75 (0.37, 1.52) 0.43CVA 4 (1.7) 13 (5.4) 3.29 (1.06, 10.25) 0.03CHF 12 (5.1) 11 (4.5) 0.89 (0.38, 2.06) 0.78CV death 13 (5.4) 9 (3.7) 0.66 (0.28, 1.58) 0.35Death 18 (7.6) 20 (8.2) 1.1 (0.56, 2.12) 0.80
Nisoldipine EnalaprilN � 234 (%) N � 246 (%)
Myocardial Infarction 18 (7.7) 16 (6.5) 1.20 (0.60, 2.41) 0.61CVA 11 (4.7) 6 (2.4) 1.97 (0.72, 5.42) 0.18CHF 11 (4.7) 12 (4.9) 0.96 (0.42, 2.22) 0.93CV death 8 (3.4) 14 (5.7) 0.59 (0.24, 1.43) 0.23Death 19 (8.1) 19 (7.7) 1.1 (0.54, 2.05) 0.87
Abbreviations are: CVA, cerebral vascular accident; CHF, congestive heart failure; CV, cardiovascular
at five years (P � 0.87). During the follow-up period, type 2 diabetic patients with a primary purpose of exam-ining the effect of intensive lowering of blood pressure36% of patients randomized to nisoldipine versus 40%
of patients randomized to enalapril had progression of on diabetic complications. Specifically, our question was:in type 2 diabetic patients with baseline blood pres-neuropathy at five years (P � 0.38).sures �140/90 mm Hg is there any beneficial effect of
Cardiovascular disease further lowering of blood pressure with antihypertensiveagents, and if so to what level? The present prospectiveTable 4 shows the number of patients with new cardio-randomized ABCD study in 480 normotensive type 2vascular events throughout the follow-up period. Pa-diabetic patients addressed this important question.tients randomized to the intensive therapy group had a
It is well accepted that renal function deteriorates withsignificantly lower incidence of cerebral vascular acci-age [27]. Yet in the current ABCD study in elderly typedents when compared to the moderate therapy group2 diabetic patients creatinine clearance did not decrease(1.7 vs. 5.4%, P � 0.03). No significant difference inover a four-year period after the initial hemodynamiccardiovascular events or deaths occurred between theeffect of blood pressure control. Thus, it can be arguednisoldipine and enalapril groups. Similar analyses per-that the failure to control blood pressure in the elderlyformed only on patients receiving active drug (enalapril,is the reason for the decline in renal function rather thanN � 168; nisoldipine N � 163) also revealed no statisti-attributing it to the aging process. In support of thiscally significant difference in the incidence of cardiovas-interpretation is the recent publication emphasizing thecular events, P � 0.6).poor blood pressure control in the elderly in this countryAnalyses excluding the 26 patients with isolated hyper-[28].tension (SBP �160 mm Hg and DBP �90 mm Hg) were
Ravid et al demonstrated, in normotensive type 2 dia-performed and revealed no change in the outcome find-betic patients with normo- or microalbuminuria receiv-ings and interpretation. Since a higher percentage ofing placebo, that there was a significant fall in creatininepatients utilized metoprolol in the enalapril treatmentclearance over a five to six follow-up period, which couldgroup, additional analyses were performed excludingbe avoided with ACE inhibitor treatment [29, 30]. Asthe patients utilizing metoprolol. When the metoprololdiscussed, in the present study creatinine clearance wastreated patients were removed the results were not sig-stabilized with both intensive and moderate blood pres-nificantly different.sure control less than 140/90 mm Hg. In this regard, theNHANES study (1991–1994) reported only 17 percent
DISCUSSION of diabetic patients had blood pressures controlled belowIn recent years there have been several important 140/90 mm Hg [31]. As previously suggested [32], the
studies in hypertensive type 2 diabetic patients examin- present ABCD study observations indicate that stabiliza-ing the effect of different levels of blood pressure control tion of renal function in normotensive type 2 diabeticand different antihypertensive agents on diabetic compli- patients is best achieved at the normo- or microalbumi-
nuric stage with blood pressure control �140/90 mmcations [6–11]. In general the results of these studiessupport the beneficial effect of intensive blood pressure Hg. However, in the patients who had overt albuminuria
at study entry, renal function declined significantlylowering in diabetic subjects. However, there has notbeen a prospective randomized study in normotensive throughout the present study, averaging approximately

Schrier et al: BP control in normotensive diabetes 1095
5 mL/min annual decline in creatinine clearance, inde- to decrease the progression of retinopathy. This effecton the progression of retinopathy was significant whetherpendent of intensive or moderate blood pressure control
or whether the initial antihypertensive therapy was with analyzed by intention to treat or time on active drug.The results of the present study lend further supportenalapril or nisoldipine. These results are similar to a
study reported by Parving et al in which antihypertensive for the United Kingdom Prospective Diabetes Study(UKPDS), which demonstrated that over a nine yeartherapy resulted in the slower decline in of glomerular
filtration rate (3 mL/min/year) when compared to a pla- follow-up tighter blood pressure control led to a decreasein the need for photocoagulation in a hypertensive typecebo (11 mL/min/year) [33]. At a rate of decline in glo-
merular filtration rate between 3 and 5 mL/min/year, 2 diabetic population [7].While stability of renal function and slowing of pro-renal replacement therapy in the diabetic patients should
not be necessary until their late seventies. This conclu- gression of retinopathy with intensive blood pressurecontrol occurred, there was still worsening of retinopathysion has important implications since diabetic patients
now constitute 45% of new patients receiving renal re- and also neuropathy in these normotensive type 2 dia-betic subjects in spite of intensive blood pressure control.placement therapy [34].
In the present study, there were significant and clini- In addition, there was no evidence that the use of nisol-dipine versus enalapril as the initial antihypertensivecally important differences with regard to the progres-
sion of urinary albumin excretion, diabetic retinopathy agent was advantageous with regard to either the pro-gression of neuropathy or retinopathy. The suboptimaland the incidence of stroke between the moderate and
intensive blood pressure control groups, whether ana- blood glucose and lipid control over the follow-up periodof this ABCD study are potential factors in the progres-lyzed as intention to treat or time on active drug. With
respect to urinary albumin excretion, there is general sion of the retinopathy and neuropathy. The recent re-sults of the UKPDS provide support for the concept thatagreement that it is an important surrogate of diabetic
nephropathy progression. In this regard, urinary albumin blood glucose control results in slowing the progressionof microangiopathy in type 2 diabetes [41].excretion may even be a stronger predictor of cardiovas-
cular outcomes [35]. In the present study, the more ag- Of all the complications associated with diabetes, neu-ropathy is the most poorly defined, but may be the mostgressive blood pressure control (mean 128/75 mm Hg)
compared to the moderate control (mean 137/81 mm Hg) prevalent. Cross sectional studies suggest a possible rela-tionship between hypertension and the presence of neu-decreased the rate of progression of normoalbuminuria
to microalbuminuria (incipient nephropathy) and of ropathy [42]. Interventional studies demonstrating a ben-efit with regard to progression of neuropathy have onlymicroalbuminuria to overt albuminuria (diabetic ne-
phropathy; both P � 0.03). involved glycemic control [41], aldose reductase inhibi-tors [43] and alpha-lipoic acid [44], but not antihyperten-Most recently in a study with hypertensive and normo-
tensive type 2 diabetic patients, ramipril versus placebo sive therapy. As noted, no differential effects on theprogression of neuropathy were observed in the presentdemonstrated an advantage with regard to the progres-
sion to overt albuminuria as measured as determined by study between intensive and moderate blood pressuretherapy, or between the initial therapy with a CCB andurinary albumin/creatinine ratios [8]. Other studies in
type 2 diabetic patients have demonstrated an advantage ACE inhibitor.The beneficial effects of intensive blood pressure con-of ACE inhibitors on albuminuria when compared to
calcium channel blockers (CCBs) or beta-blockers but trol in the current study were not restricted to microvas-cular complications of retinopathy and albuminuria. Athese studies had a relatively short follow-up of two
years or less and blood pressure was not as aggressively significant decrease in the occurrence of strokes also wasobserved with intensive blood pressure control (P �lowered as in the present intensive treatment group
[36, 37]. It may be, therefore, that at well-controlled 0.03). These results are similar to studies examining theeffects of isolated systolic blood pressure control in el-levels of blood pressure (�130/80 mm Hg) any advantage
of ACE inhibitors on albuminuria may be difficult to derly hypertensive diabetic subjects wherein the use ofeither a diuretic or calcium channel blocker based antihy-demonstrate.
Another significant and clinically important observa- pertensive resulted in a decreased incidence of strokes[6, 9, 10]. In the present normotensive ABCD study,tion in this normotensive ABCD study related to the
progression of diabetic retinopathy. Earlier studies have a significantly lower systolic as well as diastolic bloodpressure was present in the intensive as compared to thesuggested that there is a positive correlation between
hypertension and the incidence or progression of dia- moderate therapy group.No difference in non-stroke cardiovascular events be-betic retinopathy [38–40]. Although in the present study
there was no difference with regard to the development tween intensive versus moderate therapy were detectedin this normotensive ABCD study. There was also no dif-of retinopathy or proliferative retinopathy, we demon-
strated a benefit in the intensive blood pressure group ference between the incidence of cardiovascular events

Schrier et al: BP control in normotensive diabetes1096
Reprint requests to Robert W. Schrier, M.D., Division of Renal Dis-between those randomized to nisoldipine versus enala-eases and Hypertension, Department of Medicine, 4200 East Ninth Ave-
pril. This latter finding is in contrast to the results in the nue, #B178, Denver, Colorado 80262, USA.E-mail: [email protected] ABCD study in which a significant advan-
tage was demonstrated in the enalapril treated patientswith regard to fewer myocardial infarctions than the REFERENCESnisoldipine treated patients [11]. However, since the pa- 1. National Institute of Diabetes and Digestive and Kidney Dis-
eases: Incidence and prevalence of ESRD in National Institutestients in the hypertensive ABCD study [11] had a meanof Health. United States Renal Data System 1998 Annual Dataof 11.6 years of elevated blood pressure prior to enroll-Report (chapt 2), Bethesda, 1998 2
ment, they no doubt had a higher cardiovascular risk 2. Merimee TJ: Diabetic retinopathy. N Engl J Med 322:978–983,1990than the diabetic patients in the present normotensive
3. Knowler WC, Bennett PH, Ballantine EJ: Increased incidenceABCD study. It is also worth emphasizing that thereof retinopathy in diabetes with elevated blood pressure. N Eng. J
was no evidence of a “J curve” in the intensive blood Med 301:645–650, 19804. Ishihara M, Yukimura Y, Aizawa T, et al: High blood pressurepressure control group in the normotensive diabetic
as risk factor in diabetic retinopathy development in NIDDMpatients. Specifically, there was no increase in cardiovas-patients. Diabetes Care 10:20–25, 1987
cular events in the intensive versus moderate blood pres- 5. Dupree EA, Meyer MB: Role of risk factors in complications ofdiabetes mellitus. Am J Epidemiol 112:100–112, 1980sure control group. Taken together, these findings sug-
6. Curb JD, Pressel SL, Cutler JA, et al: Effect of diuretic-basedgest that any cardioprotective effect of ACE inhibitorsantihypertensive treatment on cardiovascular disease risk in older
is most likely to be demonstrated in the higher risk hyper- diabetic patients with isolated systolic hypertension. Systolic Hy-pertension in the Elderly Program Cooperative Research Group.tensive rather than normotensive type 2 diabetic pa-JAMA 276:1886–1892, 1996tients.
7. UK Prospective Diabetes Study Group: Tight blood pressureIn summary, this five-year randomized study in 480 control and risk of macrovascular and microvascular complications
in type 2 diabetes: UKPDS 38. BMJ 317:703–713, 1998normotensive type 2 diabetic patients demonstrate that8. Heart Outcomes Prevention Evaluation Study Investigators:intensive (�128/75 mm Hg) as compared to moderate
Effects of ramipril on cardiovascular and microvascular outcomes(�137/81 mm Hg) blood pressure control achieved by in people with diabetes mellitus: Results of the HOPE study and
MICRO-HOPE substudy. Lancet 355:253–259, 2000either enalapril or nisoldipine as initial therapy: (1) de-9. Tuomilehto J, Rastenyte D, Birkenhager WH, et al: Effectscreased the progression of normoalbuminuria to micro-
of calcium-channel blockade in older patients with diabetes andalbuminuria (incipient diabetic nephropathy) as well as systolic hypertension. Systolic Hypertension in Europe Trial Inves-
tigators. N Engl J Med 340:677–684, 1999microalbuminuria to overt albuminuria (diabetic ne-10. Hansson L, Zanchetti A, Carruthers SG, et al: Effects of inten-phropathy); (2) slowed the progression of diabetic reti-
sive blood-pressure lowering and low-dose aspirin in patients withnopathy; and (3) decreased the occurrence of cerebro- hypertension: Principal results of the Hypertension Optimal Treat-
ment (HOT) randomised trial. HOT Study Group. Lancet 351:vascular events. In concert with previous studies, either1755–1762, 1998intensive or moderate blood pressure control was associ-
11. Estacio RO, Jeffers BW, Gifford N, Schrier RW: Effect ofated with a stable creatinine clearance over five years in blood pressure control on diabetic microvascular complications in
patients with hypertension and type 2 diabetes. Diabetes Carethese type 2 diabetic patients if implemented prior to the23:B54–B64, 2000occurrence of overt albuminuria. After the occurrence of
12. Estacio RO, Savage S, Nagel NJ, Schrier RW: Baseline charac-overt albuminuria, however, renal function progressively teristics of participants in the Appropriate Blood Pressure Control
in Diabetes trial. Control Clin Trials 17:242–257, 1996deteriorated, albeit at a slower rate as compared to poor13. WHO Study Group: Diabetes Mellitus - Technical Report Seriesblood pressure control. Taken together, the results of 727. Geneva, World Health Organization, 1985
this normotensive ABCD study indicate that lowering 14. Early Treatment Diabetic Retinopathy Study Research Group:Grading diabetic retinopathy from stereoscopic color fundus pho-blood pressure in type 2 diabetic patients should nottographs. An extension of the Modified Airlie House Classification:be restricted to hypertensive patients (BP �140/90 mm ETDRS report number 10. Ophthalmology 98:786–806, 1991
Hg). Rather, aggressively lowering blood pressure (mean 15. Consensus Panel: Report and recommendations of the San Anto-nio Conference on Diabetic Neuropathy. Ann Neurol 24: 99–106,128/75 mm Hg) in normotensive type 2 diabetic patients1988can lead to beneficial effects over a five-year follow-up 16. Mogensen CE: Microalbuminuria in diabetic renal disease, in Pre-
with respect to the incidence of stroke and progression of vention and Treatment of Diabetic Late Complications, edited byMogensen CE, Standl E, New York, Walter de Gruyter, 1989,retinopathy and urinary albumin excretion. The specificpp 41–73initial agent used (CCB vs. ACE inhibitor) appears to 17. Early Treatment Diabetic Retinopathy Study Research Group:
be less important than the achievement of the lower Fundus photographic risk factors for progression of diabetic reti-nopathy: ETDRS report no. 12. Ophthalmology 98:823–833, 1991blood pressure values in normotensive type 2 diabetic
18. Dyck PJ: Detection, characterization, and staging of poly-neuropa-patients. thy assessed in diabetics. Muscle Nerve 11:21–32, 198819. Cohen JA, Jeffers BW, Faldut D, et al: Risks for sensorimotor
peripheral neuropathy and autonomic neuropathy in non-insulin-ACKNOWLEDGMENTSdependent diabetes mellitus (NIDDM). Muscle Nerve 21:72–80,
This study was supported by Bayer Pharmaceutical Company and 1998the National Institute of Diabetes, Digestive, and Kidney Diseases 20. Estacio RO, Wolfel EE, Regensteiner, et al: Effect of risk factors
on exercise capacity in NIDDM. Diabetes 45:79–85, 1996(DK50298-02).

Schrier et al: BP control in normotensive diabetes 1097
21. Estacio RO, McFarling E, Biggerstaff S, et al: Overt albumin- course of renal function in NIDDM patients with normo- andmicroalbuminuria. J Intern Med 241:133–141, 1997uria predicts diabetic retinopathy in Hispanics with NIDDM. Am
33. Parving HH, Andersen AR, Smidt UM: Effect of antihyperten-J Kidney Dis 31:947–953, 1998sive treatment on kidney function in diabetic nephropathy. Br Med22. Jeffers BW, Estacio RO, Raynolds MV, Schrier RW: Angioten-J (Clin Res Ed) 294:1443–47, 1987sin-converting enzyme gene polymorphism in non-insulin depen-
34. U.S. Renal Data System: USRDS 2001 Annual Data Report: Atlasdent diabetes mellitus and its relationship with diabetic nephropa-of End-Stage Renal Disease in the United States. Bethesda, Nationalthy. Kidney Int 52:473–477, 1997Institutes of Health National Institute of Diabetes and Digestive23. Mehler PS, Jeffers BW, Estacio R, Schrier RW: Associations ofand Kidney Diseases, 2001, pp 40hypertension and complications in non-insulin-dependent diabetes
35. Gerstein HC, Mann JFE, Yi Q, et al: Albuminuria and risk ofmellitus. Am J Hypertens 10:152–161, 1997cardiovascular events, death, and heart failure in diabetic and non-24. Savage S, Nagel NJ, Estacio RO, et al: Clinical factors associateddiabetic individuals. JAMA 286:421–426, 2001with urinary albumin excretion in type II diabetes. Am J Kidney 36. Hansson L: Effects of angiotensin-converting enzyme inhibition
Dis 25:836–844, 1995 versus conventional antihypertensive therapy on the glomerular25. Savage S, Estacio RO, Jeffers B, Schrier RW: Urinary albumin filtration rate. Cardiology 86(Suppl 1):30-3–30-33, 1995
excretion as a predictor of diabetic retinopathy, neuropathy, and 37. Rossing P, Tarnow L, Boelskifte S, et al: Differences betweencardiovascular disease in NIDDM. Diabetes Care 19:1243–1248, nisoldipine and lisinopril on glomerular filtration rates and albu-1996 minuria in hypertensive IDDM patients with diabetic nephropathy
26. Savage S, Estacio RO, Jeffers B, Schrier RW: Increased compli- during the first year of treatment. Diabetes 46:481–487, 1997cations in noninsulin-dependent diabetic patients treated with insu- 38. Chahal P, Inglesby DV, Sleightholm M, et al: Blood pressurelin versus oral hypoglycemic agents: A population study. Proc and the progression of mild background diabetic retinopathy. Hyp-Assoc Am Physicians 109:181–189, 1997 ertens 7(Suppl II):79–83, 1985
27. Palmer BF, Levi M: Renal function and disease in the aging kidney, 39. Moss SE, Klein R, Klein BEK: Ocular factors in the incidenceand progression of diabetic retinopathy. Ophthalmology 101:77–83,in Diseases of the Kidney (vol III), edited by Schrier RW,1994Gottschalk CW, Boston, Little, Brown, 2001, pp 2293–2317
40. Klein BEK, Klein R, Moss SE, et al: A cohort study of the28. Hyman DJ, Pavlik VN: Characteristics of patients with uncon-relationship of diabetic retinopathy to blood pressure. Arch Oph-trolled hypertension in the United States. N Engl J Med 345:479–thalmol 113:601–606, 1995486, 2001
41. Anonymous: Intensive blood-glucose control with sulphonylureas29. Ravid M, Brosh D, Levi Z, et al: Use of enalapril to attenuateor insulin compared with conventional treatment and risk of com-decline in renal function in normotensive, normoalbuminuric pa-plications in patients with type 2 diabetes (UKPDS 33). UK Pro-tients with type 2 diabetes mellitus. A randomized, controlled trial.spective Diabetes Study (UKPDS) Group. Lancet 352:837–853,Ann Intern Med 128:982–988, 1998199830. Ravid M, Savin H, Jutrin I, et al: Long-term stabilizing effect of
42. Knuiman MW, Welborn TA, McCann VJ, et al: Prevalence ofangiotensin-converting enzyme inhibition on plasma creatinine and diabetic complications in relation to risk factors. Diabetes 35:1332–on proteinuria in normotensive type II diabetic patients. Ann Int 1339, 1986Med 118:577–581, 1993 43. Nicolucci A, Carinci F, Cavaliere D, et al: A meta-analysis of
31. Burt VL, Culter JA, Higgins M, et al: Trends in the prevalence, trials on aldose reductase inhibitors in diabetic peripheral neuropa-awareness, treatment, and control of hypertension in the adult US thy. Diabet Med 13:1017–1026, 1996population. Data from the health examination surveys, 1960 to 44. Ziegler D, Hanefeld M, Ruthnau KJ, et al: Treatment of symp-1991. Hypertens 26:60–69, 1995 tomatic diabetic peripheral neuropathy with the anti-oxidant
alpha-lipoic acid. Diabetologia 38:1425–1433, 199532. Nielsen S, Schmitz A, Rehling M, Mogensen CE: The clinical




















