PHYSICAL AND MECHANICAL PROPERTIES OF MEDIUM-DENSITY FIBREBOARDS USING SOY—LIGNIN ADHESIVES
Upload
independentCategory
view
1download
0
ORIGINAL ARTICLE
EFFECT OF AUTOLOGOUS PLATELET ADHESIVES ON DERMALFAT GRAFT RESORPTION FOLLOWING RECONSTRUCTION OFA SUPERFICIAL PAROTIDECTOMY DEFECT:A DOUBLE-BLINDED PROSPECTIVE TRIAL
Shamir Chandarana, MD,1 Kevin Fung, MD, FRCS(C),1
Jason H. Franklin, HBSc, MD, FRCS(C),1 Trevor Kotylak, MD, FRCP(C),2
Damir B. Matic, MD, FRCS(C),3 John Yoo, MD, FRCS(C)1
1 Department of Otolaryngology, London Health Sciences Centre–Victoria Hospital,800 Commissioners Road East, London, Ontario, Canada N6A 5W9. E-mail: [email protected] Department of Radiology and Diagnostic Imaging, University of Edmonton, Edmonton, Alberta, Canada3 Department of Plastic and Reconstructive Surgery, London Health Sciences Centre–Victoria Hospital,London, Ontario, Canada
Accepted 1 August 2008Published online 20 January 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hed.20999
Abstract: Background. Dermal fat grafts are used to recon-
struct facial contour defects but may undergo variable resorp-
tion. Application of autologous platelet adhesive may improve
outcomes. The primary objective was to compare resorption of
dermal fat grafts for parotidectomy defects, between patients
receiving autologous platelet adhesive versus controls.
Methods. This was a double-blinded prospective cohort at a
tertiary care center. Volumetric analyses of dermal fat graft
measured by MRI scans. Resorption was determined by com-
paring 1- and 6-month MRIs in each patient. Complications,
Frey’s Syndrome, and patient satisfaction were also assessed.
Results. Twelve patients completed the study. A significant
reduction in graft resorption was seen in the treatment group
(57% vs. 31%, p 5 .01). Three patients in the control group
developed fat liquefaction. Patient perceived significant differen-
ces in scar and contour.
Conclusion. Application of autologous platelet adhesives
improved graft viability and patient satisfaction at 6 months.VVC 2009 Wiley Periodicals, Inc. Head Neck 31: 521–530, 2009
Keywords: parotidectomy; dermal fat graft; autologous platelet
adhesive; platelet-rich plasma; facial contour
Superficial parotidectomy is the standard treat-ment for most benign tumors of the parotid gland.Known sequelae of surgery include facial contourdefects and Frey’s syndrome.
In selected patients, restoration of the facialcontour may be appropriate. Several reconstruc-tive options have been described, including auto-logous dermal fat graft, lyophilized dermis, andmuscle-interposition flaps. The ideal reconstruc-
This study was presented at the 61st Annual Meeting of the Canadian Soci-ety of Otolaryngology, Head and Neck Surgery, May 2007. This study wasalso presented at the 2nd International Congress on Salivary GlandDiseases, October 2007.
Dr. Yoo has reported a financial interest/relationship with Biomet Biologicsas a product development consultant and a joint patent pending. Dr. Yooalso discloses that he has been provided honoraria for presentations ofclinical research.
VVC 2009 Wiley Periodicals, Inc.
Correspondence to: J. Yoo
Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009 521

tive technique should be reliable, easy, inexpen-sive, single-stage, and autologous.1 Autologousdermal fat grafts, consisting of dermis and under-lying subcutaneous fat, fulfil many of these crite-ria. The first use of a dermal fat graft for correc-tion of a facial contour defect was reported in1931.1 Since then, the dermal fat graft has beenused for various reconstructive applications.
One disadvantage of the dermal fat graft is itsvariable resorption over time. Although numerousretrospective and qualitative reports are sugges-tive of significant resorption, there is a paucity ofprospective information that describes the natu-ral history of the dermal fat graft. Opponents ofthe dermal fat graft also report increased postop-erative wound complications such as fat liquefac-tion, seroma, and sialocele.1 Reduction in graftresorption and early wound complications wouldmake the dermal fat graft a better choice for facialcontour reconstruction.
Frey’s syndrome, also known as gustatorysweating, is a common complication following pa-rotidectomy. Subjective symptoms of Frey’s syn-drome have been reported in up to 38% ofpatients. Furthermore, a positive starch-iodidetest has been demonstrated in up to 86% ofpatients.2,3 It has been suggested that the dermalfat graft may provide a barrier, thereby reducingthe incidence of Frey’s syndrome.4
Autologous Plasma Adhesives. Autologous plasmaadhesives are patient-derived platelet-richplasma concentrates that have been used in awide variety of soft and hard tissue procedures topromote wound healing. Proposed benefitsinclude enhanced tissue adhesion and hemostasisthrough platelet activation and fibrin clot forma-tion. Growth factors released from the plateletconcentrate have been postulated as the mecha-nism for improved wound healing.5–8 Substancessuch as platelet-derived growth factor, transform-ing growth factor-beta, insulin-like growth factor-1, and vascular endothelial growth factor attractfibroblasts, stimulate angiogenesis, and signal thedifferentiation and proliferation of fibroblasts torebuild tissues.7,9,10 Furthermore, animal modelstudies have demonstrated that these growth fac-tors can promote adipocyte growth, differentia-tion, and trophic activities.11,12
Autologous platelet adhesives are derivedfrom the patient’s blood by a centrifugation tech-nique that separates blood into platelet-richplasma and platelet-poor plasma. Platelet-richplasma contains up to 8 times the platelet concen-
tration of whole blood, while platelet-poor plasmacontains inactivated fibrin.8 A separate centrifu-gation also enables the isolation of concentratedautologous thrombin. The concentrated plateletsand fibrin are then applied onto the wound, incombination with autologous thrombin, to mimicthe final stages of the coagulation cascade. Otheradvantages of autologous products are the elimi-nation of the risk of transmissible disease and theassociated risks with the use of bovine throm-bin.13–16
The use of a dermal fat graft has been limitedby the unpredictable but significant graft resorp-tion and postoperative complications. Quantita-tive analysis of fat graft resorption has not beendescribed in the literature. The effect of the plate-let concentrates on dermal fat grafts in a humanmodel has not been previously evaluated.
Study Objectives. The primary objective of thisstudy is to compare dermal fat graft resorptionbetween patients receiving autologous platelet ad-hesive application versus controls.
Secondary objectives include the evaluation ofpostoperative complications, incidence of Frey’ssyndrome, and patient satisfaction in the 2cohorts.
Study Design. A prospective cohort study designwas employed whereby 2 groups of patients wereexamined: those who had undergone a parotidec-tomy with dermal fat graft reconstruction andthose who had undergone dermal fat graft recon-struction with intraoperative application of auto-logous platelet adhesives. Both the patients aswell as the radiologist conducting volumetricanalyses were blinded to the application of autolo-gous platelet adhesives.
MATERIALS AND METHODS
After receiving ethics approval from the institu-tional internal review board (Health SciencesREB# 11845, University of Western Ontario),patients undergoing superficial parotidectomyand were potential candidates for dermal fat graftreconstruction were considered for enrolment. Allpatients were treated in the Department of Oto-laryngology at London Health Sciences Centre,and patient consent was obtained.
Subjects. Consecutive patients meeting theinclusion and exclusion criteria underwent a su-perficial parotidectomy with dermal fat graft
522 Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009

reconstruction. Half of the patients received intra-operative autologous platelet adhesive applica-tion to the parotidectomy bed and over the dermalfat graft while the control group received no auto-logous platelet adhesive application. Entry intothe treatment and control arms was determinedat the day of surgery based on the availability ofthe gravitational platelet separation system tech-nical support staff. Formal randomization couldnot be conducted because of this inconsistentavailability.
The inclusion criteria were as follows: allpatients whose fine-needle aspirate biopsy sug-gested benign intraparotid pathology.
The exclusion criteria were as follows:patients whose proposed surgery included re-moval of the deep lobe of parotid or neck contents;patients with a prior history of radiation exposureto the site in question; patients undergoing a revi-sion surgery; patients with comorbidities thatwould interfere with wound healing (diabetesmellitus, connective tissue disease, autoimmunedisease, coagulation disorder, prior history ofchemotherapy); patients with contraindicationstoMRI.
Intraoperative Procedure
Parotidectomy and Dermal Fat Graft. All patientsunderwent a standard superficial parotidectomy,as described by Olsen,17 employing a subsuperfi-cial muscular aponeurotic system flap elevation.
Following the excision, a free dermal fat graftwas harvested from a low abdominal incision, asdescribed by Davis et al.1 The grafts were har-vested using an elliptical excision, with sharp dis-section to include the underlying fat. The graftwas then deepithelialized for inset. The donor sitewas closed in 2 layers.
The graft was then tailored to the parotidec-tomy defect and sutured securely with 3-0 Vicryl(Ethicon Inc, Somerville, NJ) sutures (see Figure1). The smooth dermal surface was placed superfi-cially to provide a large contact area with the over-lying subdermal plexus and away from the facialnerve. The skin flap was then closed over a closedsuction drain.
Autologous Platelet Adhesive. In those patients whoreceived autologous platelet adhesives, the plate-let concentrate was prepared during the paroti-dectomy, using the gravitational platelet separa-tion system (Biomet Inc., Warsaw, IN).
Preparation of Autologous Platelet Adhesive. Sixty millili-ters of whole blood taken from the patient wascentrifuged for 15 minutes using the gravitationalplatelet separation system, thereby separatingthe blood into platelet-rich plasma, platelet-poorplasma, and packed red blood cells (Figure 2). Theplatelet-rich plasma and platelet-poor plasmawere then drawn off into separate syringes.
An additional 20 mL of patients’ whole bloodwas drawn and allowed to coagulate. This samplewas then centrifuged in order to isolate the throm-bin-rich supernatant.
Application of Autologous Platelet Adhesives to Wound. Adual spray applicator was used to apply the plate-let-rich plasma and thrombin. The solution wasirrigated onto the parotid bed and over the dermalfat graft prior to wound closure (see Figure 3). Fol-lowing closure, platelet-poor plasma and throm-bin were applied under the skin flap using a cathe-ter tip. Last, gentle manual pressure was appliedto the operative site for 5 minutes, to allow the so-lution to congeal and the skin flaps to adhere tothe dermal fat graft.
Outcome Measures
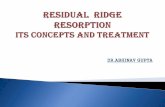
Primary Outcome Measure. The primary outcomemeasure was volumetric analysis of the dermalfat graft as obtained by MRI. Patients underwentMRI (General Electric, 1.5T, Signa Series, Mil-waukee, WI) at 1 and 6 months postoperatively. Aneuroradiologist blinded to the experimentalintervention evaluated T1-weighted images (Tr 5400–700, Te 5 6–10) captured at 6-mm intervals.Volumetric analysis software (Advantage Work-station Volume Viewer 4.2, General Electric) wasused to determine the 3-dimensional volume ofthe dermal fat graft. A 3-mm brush was used tohighlight the dermal fat graft in the series. Figure4 illustrates how the dermal fat graft is capturedfor analysis by ‘‘painting’’ the entire graft with abrush.
Both the percentage of graft take ([6-monthMRI volume divided by 1-month MRI volume]multiplied by 100%) as well as absolute reductionin dermal fat graft volume (1-month MRI volumeminus the 6-month MRI volume) were analyzed.Statistical analyses consisted of first performing aLevene’s test for equality of variances among the 2cohorts, and then an independent samples t test tocompare the 2 cohorts. Statistical significance wasset at .05. Statistical analysis was derived usingSPSS v. 14.0 (SPSS Inc., Chicago, IL).
Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009 523

Secondary Outcome Measures. Patients were followedprospectively for 6 months for complications.Complications were categorized as ‘‘major’’ if theyrequired reoperation and ‘‘minor’’ if they wereamenable to conservativemanagement.
At the 6-month postoperative period, the pres-ence of Frey’s syndrome was assessed using thestarch-iodine test 5. Discoloration of the parotidregion indicated positivity for Frey’s syndrome.
Patient satisfaction was evaluated using anonvalidated but previously utilized question-naire completed by patients 6 months postopera-tively (see Appendix).3 Items included patient
perception of facial symmetry, incisional scar, andsymptoms of Frey’s syndrome. Patients wereasked to grade their level of satisfaction on a 10-point Likert scale, whereby a score of 1 indicatedcomplete satisfaction and a score of 10 indicatedcomplete dissatisfaction. Mann-Whitney U testfor nonparametric data was used to elicit differen-ces. Statistical analysis was derived using SPSS v14.0 (SPSS Inc.).
Sample Size Calculation. Sample size calculationdetermined that 10 patients were required to com-plete the study in order to find a 25% differencein dermal fat graft resorption between the
FIGURE 2. Patient’s whole blood separated into constituent
components after centrifugation.
FIGURE 3. Autologous platelet adhesive applied to wound with
dual spray applicator.
FIGURE 1. (A) Parotidectomy defect and excised tumor can
be seen. (B) Dermal fat graft elevated and ready for insertion.
(C) Dermal fat graft inset.
524 Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009
experimental and control groups. It was decidedthat 25%would be considered theminimum clinicalsignificant difference. Alpha and beta errors wereset at 0.05 (2-tailed) and 0.2, respectively. Based ona conservative patient dropout rate of 50%, the tar-get number for initial enrolmentwas 20 patients.
RESULTS
A total of 16 patients were enrolled in this study; 8patients in each cohort. Two patients in eachcohort opted not to undergo the follow-up 6-monthMRI and therefore were excluded from all analy-ses. Twelve patients were available for completeassessment of outcome parameters. The 2 patientcohorts were comparable, with no significant dif-ferences in age, sex, smoking status, or pathology(Table 1).
Primary Outcome Measure: Volumetric Analyses.
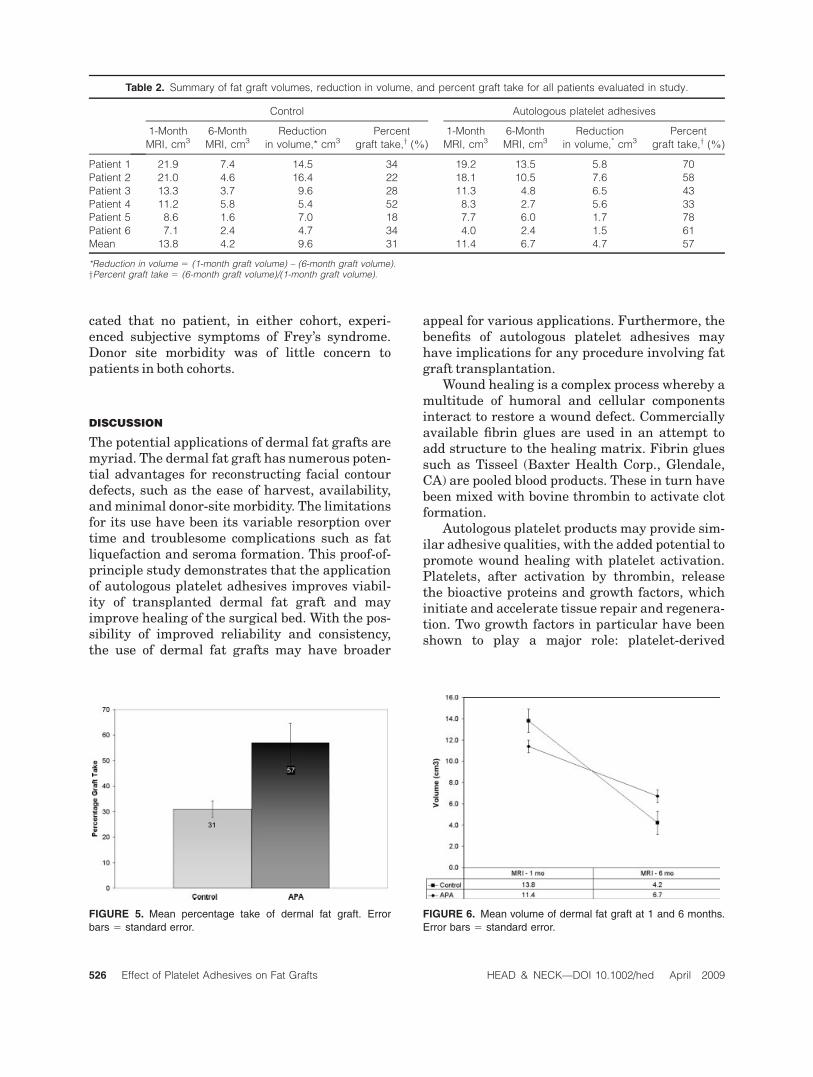
Table 2 demonstrates the volume of the dermalfat graft for each patient at both the 1- and 6-month intervals. The mean percentage take forthe control and autologous platelet adhesivegroups were 31% and 57%, respectively (p 5 .01)(see Figure 5). There was also a significantdifference in absolute volume of dermal fat graftresorption between the 2 groups (mean volumeresorption were 9.6 cm3 and 4.7 cm3, respectively,p5 .05) (see Figure 6).
Secondary Outcome Measures.
Complications. There were no major complicationsin either group. Three of 6 patients in the controlgroup had minor complications consisting of sero-
mas6 fat liquefaction shortly after the operation.In 2 of these patients, management consisted ofneedle aspiration. The third patient required par-tial opening of the wound and packing. In the au-tologous platelet adhesives group, 1 patientrequired oral antibiotics for a minor local woundinfection.
Frey’s Syndrome. One patient in the control groupdemonstrated a positive starch-iodine test. Nopatient in the treatment group developed Frey’ssyndrome.
Questionnaire. Figure 7 shows the mean scores ofpatient satisfaction with respect to facial contourand incisional scar. Patients in the autologous pla-telet adhesives group demonstrated higher satis-faction in their perception of facial contour andincisional scar at 6 months (U5 5, p < .05; U5 4,p< .05, respectively). The questionnaire also indi-
FIGURE 4. (A) Dermal fat graft as seen on MRI (arrow). (B) Same fat graft painted for volumetric analyses.
Table 1. Characteristics of patients within both control and
experimental autologous platelet adhesives arm.
Control APA p value
Mean age, y 52 52 NS
Sex
Male 2 4 .290
Female 4 2
Smoker
Yes 2 1 .549
No 4 5
Pathology .386
PA 5 4
WT 1 2
Abbreviations: APA, autologous platelet adhesives; NS, not significant;PA, pleomorphic adenoma; WT, Warthin tumor.
Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009 525
cated that no patient, in either cohort, experi-enced subjective symptoms of Frey’s syndrome.Donor site morbidity was of little concern topatients in both cohorts.
DISCUSSION
The potential applications of dermal fat grafts aremyriad. The dermal fat graft has numerous poten-tial advantages for reconstructing facial contourdefects, such as the ease of harvest, availability,andminimal donor-site morbidity. The limitationsfor its use have been its variable resorption overtime and troublesome complications such as fatliquefaction and seroma formation. This proof-of-principle study demonstrates that the applicationof autologous platelet adhesives improves viabil-ity of transplanted dermal fat graft and mayimprove healing of the surgical bed. With the pos-sibility of improved reliability and consistency,the use of dermal fat grafts may have broader
appeal for various applications. Furthermore, thebenefits of autologous platelet adhesives mayhave implications for any procedure involving fatgraft transplantation.
Wound healing is a complex process whereby amultitude of humoral and cellular componentsinteract to restore a wound defect. Commerciallyavailable fibrin glues are used in an attempt toadd structure to the healing matrix. Fibrin gluessuch as Tisseel (Baxter Health Corp., Glendale,CA) are pooled blood products. These in turn havebeen mixed with bovine thrombin to activate clotformation.
Autologous platelet products may provide sim-ilar adhesive qualities, with the added potential topromote wound healing with platelet activation.Platelets, after activation by thrombin, releasethe bioactive proteins and growth factors, whichinitiate and accelerate tissue repair and regenera-tion. Two growth factors in particular have beenshown to play a major role: platelet-derived
FIGURE 5. Mean percentage take of dermal fat graft. Error
bars 5 standard error.
FIGURE 6. Mean volume of dermal fat graft at 1 and 6 months.
Error bars 5 standard error.
Table 2. Summary of fat graft volumes, reduction in volume, and percent graft take for all patients evaluated in study.
Control Autologous platelet adhesives
1-Month
MRI, cm36-Month
MRI, cm3Reduction
in volume,* cm3Percent
graft take,y (%)
1-Month
MRI, cm36-Month
MRI, cm3Reduction
in volume,* cm3Percent
graft take,y (%)
Patient 1 21.9 7.4 14.5 34 19.2 13.5 5.8 70
Patient 2 21.0 4.6 16.4 22 18.1 10.5 7.6 58
Patient 3 13.3 3.7 9.6 28 11.3 4.8 6.5 43
Patient 4 11.2 5.8 5.4 52 8.3 2.7 5.6 33
Patient 5 8.6 1.6 7.0 18 7.7 6.0 1.7 78
Patient 6 7.1 2.4 4.7 34 4.0 2.4 1.5 61
Mean 13.8 4.2 9.6 31 11.4 6.7 4.7 57
*Reduction in volume 5 (1-month graft volume) – (6-month graft volume).yPercent graft take 5 (6-month graft volume)/(1-month graft volume).
526 Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009

growth factor, a powerful chemoattractant, andtransforming growth factor-b, which increasesand stimulates the deposition of extracellular ma-trix.7 Therefore, the use of autologous plateletadhesives may provide hemostasis, adhesion, andenhanced wound healing.
Studies that have evaluated fat graft resorp-tion for facial contour defects have been limited inscope. Nosan et al4 used dermal fat grafts to pre-serve facial contour in 9 patients undergoing pa-rotid surgery. They reported that 1 of the 9 under-went fat graft resorption at follow-up. Resorption,however, was not quantified in this study. Haradaet al18 presented 7 patients in whom dermal fatgrafts were used to reconstruct parotidectomydefects. They described 1 of 7 patients who devel-oped a concave deformity because of fat absorp-tion. This single case of resorption led the authorsto overcorrect their defects by 20%. Davis et al1
retrospectively reviewed 21 patients who under-went various forms of facial augmentation with adermal fat graft. Surgical repair of the facial con-tour defect was considered successful if thepatient and the surgeon were pleased with theresult at the last follow-up visit. Based on thesecriteria, successful outcome was observed in 14of the 21 patients reviewed. Important limitationsof these previous studies include the absence ofquantification of resorption and the lack of controlgroups.
Ours is the first prospective study to evaluatedermal fat graft resorption in human subjects andto determine the effects of autologous plateletadhesives on dermal fat graft resorption. The sig-nificant difference between the treatment andcontrol group represented a 2-fold increase in per-centage take of graft volume (57% in autologous
platelet adhesives group and 31% in controlgroup).
Although studies have shown that larger andthicker dermal fat grafts undergo relatively moreresorption, we did not observe a correlationbetween sizes and graft take. Table 2 demon-strates that patients within both cohorts had awide range of volumes of the graft and variablepercentage take.
Several theories on fat graft viability exist. In1923, Neuhof and Hirshfeld examined grafted fatunder the microscope. They postulated thatimplanted fat initially degenerates, after which‘‘wandering cells’’ undergo characteristic changesinto embryonal fat.19 After 5 months, they feltthat the regeneration was complete. They alsoobserved that some of the regenerated fat wasmixed with fibrous tissue. We now know that notall adipocytes die. Approximately 50% of fat tis-sue survives intact. Fat grafts are composed ofmature adipocytes, preadipocytes, and adipose-derived stem cells. The latter 2 types of cells aremore resistant to trauma thanmature adipocytes,because of the differences in size, metabolic rate,and less intracellular lipid content.20 The fragilelipid-filled adipocytes are more easily damaged.Preadipocytes are able to survive without nutri-tion much longer than adipocytes, and have amuch lower oxygen consumption rate. In fact, pre-adipocytes and adipose-derived stem cells may bethe only tissue that survives the transplantation.In addition, human adipose tissue has the highestpercentage of adult stem cells of any tissue in thebody, with as many as 5000 adipose-derived stemcells per gram of fat.21
The mechanism of improved dermal fat graftsurvival with application of autologous plateletadhesives has not been fully elucidated. One pos-sibility may be promoting growth of preadipo-cytes and adipose-derived stem cells, through ofgrowth factors contained in platelets. Yukselet al12 investigated the effect of insulin, insulin-like growth factor, and basic fibroblast growthfactor on graft survival in a rat model. The effectof each factor alone and in combination wasassessed by implanting the autologous fat intosubdermal pockets. At 12 weeks, all sampleswith growth factor treatments showed a signifi-cant increase in the percentage take of the graftwhen compared with control subjects. Althougha potential drawback of our study is a short fol-low-up time, the literature would suggest thatthe critical stages of fat graft survival occurearly in wound healing.21
FIGURE 7. Patient satisfaction with facial contour and scar.
Error bars 5 standard error.
Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009 527

With respect to incidence of complications,the control arm of our study experience slightlyhigher rates than that reported in the literature.Noosan et al4 reported a relatively low complica-tion rate, with 1 case of 9 having fat graft lique-faction and drainage. Davis et al reported 2patients with epithelial inclusion cyst formation,likely as a result of inadequate deepithelializa-tion. Both studies were retrospective reviews.The control arm of our prospective study demon-strated a 50% complication rate, all having fatgraft liquefaction and seroma formation. Inter-estingly, our experimental arm had a signifi-cantly lower complication rate, with no patientsdemonstrating fat liquefaction. Jackson et aldemonstrated the benefit of autologous plateletadhesives on prevention of seroma formation af-ter abdominoplasty.22 Thirty patients were pro-spectively followed after abdominoplasty, all ofwhom received autologous platelet adhesives. Noseromas were found in the patients studied,when compared with a 7% seroma rate in theprevious 100-patient series.
Several studies have investigated the preven-tion of Frey’s syndrome by placing a barrier toprevent parasympathetic nerve outgrowth toskin. Govindaraj et al23 demonstrated a signifi-cant reduction in Frey’s syndrome by using acel-lular dermis as a barrier. However, the complica-tion rate was unacceptable. Similar to our study,Harada et al18 reported 1 of 7 patients experi-encing Frey’s syndrome. Taylor and Yoo reportedthe incidence of positive starch-iodine test to be65% following superficial parotidectomy.3 Ourstudy demonstrated only 1 patient with objectiveevidence of Frey’s syndrome in the control group.However, follow-up periods of 1 year or moremay be necessary to ascertain the true incidenceof Frey’s syndrome.3 Nevertheless, our finding isconsistent with other studies that demonstratedreduced incidence of Frey’s syndrome with der-mal fat grafts.18
Several important limitations and criticismsof this study must be highlighted. The inabilityto randomize patients weakened the conclusionsof this study and requires clarification. The orig-inal intent was to follow a true randomizationprotocol, but it became logistically difficult toconduct. During the course of this study, avail-ability of the gravitational platelet separationsystem was variable. Thus, the application of au-tologous platelet adhesives was based on theavailability of the system on the day of surgery.This tended to be ‘‘random’’ although patients
were not formally randomized. A second meth-odological criticism was the inability to blind thesurgeon to intervention, because of the nature ofthe treatment. The inability to blind the surgeonis an unfortunate challenge in most proceduralclinical trials.
Another potential criticism of our study is thesmall sample size, but despite this, a significantdifference was demonstrated in the primary out-come metric of graft resorption. We originallyaccrued 16 patients into our study and experi-enced a 25% dropout rate. The reason in each casewas the patients’ unwillingness to undergorepeatedMRI testing.
The 1-month MRI was used to determine thebaseline dermal fat graft volume, instead of animmediate postoperative scan. There was a con-cern that postoperative edema in the surround-ing tissue, particularly to the parotidectomy skinflap, may have been an important confoundingvariable. We also attempted to ascertain accu-rate initial fat graft volume through intraopera-tive water-displacement measurements. Thismeasure of ‘‘initial’’ graft volume was abandonedbecause of 2 factors. First, because the volumewas quantified by the surgeon who was notblinded to the treatment arm, a potential biasmay have arisen. Second, the comparison ofwater-displacement measurement to 6-monthMRI volumetric analysis was problematic. It wasdecided that early and late comparison of fat vol-ume using identical modalities of measurement(MRI volumetric analysis) by a blinded observerwould provide the most consistent and unbiaseddata. Therefore, our study did not quantify theresportion of the true intraoperative graft vol-ume but rather the resorption that occurredbetween 1 and 6 months.
Patient satisfaction is an important outcomemeasure but was relegated to a secondary out-come parameter. Because a validated question-naire for this specific clinical scenario does notexist, we employed a previously published butnonvalidated questionnaire generated by the sen-ior author.3 Despite the small sample size of ourstudy, patients in the autologous platelet adhe-sives group reported increased satisfaction withfacial contour and incisional scar.
The adoption of any new medical technologyshould be based on safety, cost-effectiveness,and efficacy. The safety of autologous plateletadhesives is self-evident, and precludes poten-tial disease transmission associated with donor-derived blood products. Moreover, platelet-rich
528 Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009

plasma and platelet-poor plasma can be acti-vated using a patient’s own thrombin, therebyobviating the need for a bovine source of throm-bin. The cost of producing platelet-rich plasmaand platelet-poor plasma is determined primar-ily by the cost of the disposables used in theirpreparation and application. In-kind fundingwas provided by Biomet Inc. for the use of theirgravitational platelet separation system. Theadditional cost per patient would have beenapproximately $400 U.S. during the period ofthis study, but this will vary depending on thesystem used and local practices of technicalsupport.
Efficacy of any intervention needs to bedemonstrated through sound clinical studyand experience. Ideal future investigationsshould include a multicentered blinded ran-domization methodology, with larger samplesizes, longer follow-up evaluation, and study-ing various clinical applications.
CONCLUSION
Dermal fat grafts undergo a significant amount ofresorption. The application of autologous plateletadhesives to the dermal fat graft improved graftsurvival at 6 months. Reconstruction of parotidec-tomy defects with dermal fat grafts and autolo-gous platelet adhesive application was associatedwith reduced complications and increased patientsatisfaction.
Acknowledgments. The authors acknowl-edge Biomet Incorporated (Warsaw, IN) for theirin-kind funding. As such, Biomet Inc. supplied uswith the necessary equipment to prepare the auto-logous product. In no way did the company spon-sor our research, nor our submission of theresearch.
REFERENCES
1. Davis RE, Guida RA, Cook TA. Autologous free dermalfat graft—reconstruction of facial contour defects. ArchOtolaryngol Head Neck Surg 1995;121:95–100.
2. Dulguerov P, Quinodoz D, Cosendai G, Piletta P,Marchal F, Lehmann W. Prevention of Frey Syndromeduring parotidectomy. Arch Otolaryngol Head Neck Surg1999;125:833–839.
3. Taylor SM, Yoo J. Prospective cohort study comparingsubcutaneous and sub-superficial musculoaponeurotic
system flaps in superficial parotidectomy. J Otolaryngol2003;32:71–76.
4. Nosan DK, Ochi JW, Davidson TM. Preservation of facialcontour during parotidectomy. Otolaryngol Head NeckSurg 1991;104:293–298.
5. Whitman DH, Berry RL, Green DM. Platelet gel: an au-tologous alternative to fibrin glue with applications inoral and maxillofacial surgery. J Oral Maxillofac Surg1997;55:1294–1299.
6. Margolis DJ, Kantor J, Santanna J, Strom BL, BerlinJA. Effectiveness of platelet releasate for treatment ofdiabetic neuropathic foot ulcers. Diabetes Care 2001;24:483–488.
7. Bhanot S, Alex JC. Current applications of platelet gels infacial plastic surgery. Facial Plast Surg 2002;18:27–33.
8. Eppley BL, Woodell JE, Higgins J. Platelet quantifica-tion and growth factor analysis from platelet-richplasma: implications for wound healing. Plast ReconstrSurg 2004;114:1502–1508.
9. Adler SC, Kent KJ. Enhancing wound healing withgrowth factors. Facial Plast Surg Clin North Am2002;10:129–146.
10. Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT.Autologous platelets as a source of proteins for healingand tissue regeneration. Thromb Haemost 2003;7:4–15.
11. Eppley BL, Snider RA, Platis JM, Sadove AM. Bioactiva-tion of free-fat transfers: a potential new approach toimproving graft survival. Plast Reconstr Surg 1992;90:1022–1030.
12. Yuksel E, Weinfeld AB, Cleek R, et al. Increased freefat-graft survival with the long-term, local delivery of in-sulin, insulin-like growth factor-I, and basic fibroblastgrowth factor by PLGA/PEG microspheres. PlastReconstr Surg 2000;105:1712–1720.
13. Wilson S, Pell P, Donegan EA. HIV-1 transmission fol-lowing the use of cryoprecipitated fibrinogen as gel/adhe-sive [abstract]. Transfusion 1991;31(8 Suppl):51S.
14. Hino M, Ishiko O, Honda KI, et al. Transmission ofsymptomatic parvovirus B19 infection by fibrin sealantused during surgery. Br J Haematol 2000;108:194–195.
15. Busuttil RW. A comparison of antifibrinolytic agentsused in hemostatic fibrin sealants. J Am Coll Surg 2003;197:1021–1028.
16. Oswald AM, Joly LM, Gury C, Disdet M, Leduc V,Kanny G. Fatal intraoperative anaphylaxis related toaprotinin after local application of fibrin glue. Anesthesi-ology 2003;99:762–763.
17. Olsen KD. Parotid superficial lobectomy. In: Bailey BJ,editor. Atlas of head and neck surgery—otolaryngology,2nd ed. Philadelphia: Lippincott Williams & Wilkins;2001. pp 2–5.
18. Harada T, Inoue T, Harashina T, Hatoko M, Ueda K.Dermis-fat graft after parotidectomy to prevent Frey’sSyndrome and the concave deformity. Ann Plast Surg1993;31:450–452.
19. Neuhof H, Hirshfeld S. The transplantation of tissues.NewYork, NY: D. Appleton and Company; 1923. pp 1–297.
20. Coleman SR. Structural fat grafting: more than a perma-nent filler. Plast Reconstr Surg 2006;118:108S–120S.
21. Strem BM, Hicok KC, Zhu M, et al. Multipotential dif-ferentiation of adipose tissue-derived stem cells. Keio JMed 2005;54:132–141.
22. Jackson RF. Using platelet-rich plasma to promote heal-ing and prevent seroma formation in abdominoplastyprocedures. Am J Cosmet Surg 2003;20:185–195.
23. Govindaraj S, Cohen M, Genden EM, Contantino PD,Urken ML. The use of acellular dermis in the preven-tion of Frey’s Syndrome. Laryngoscope 2001;111:1993–1998.
Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009 529
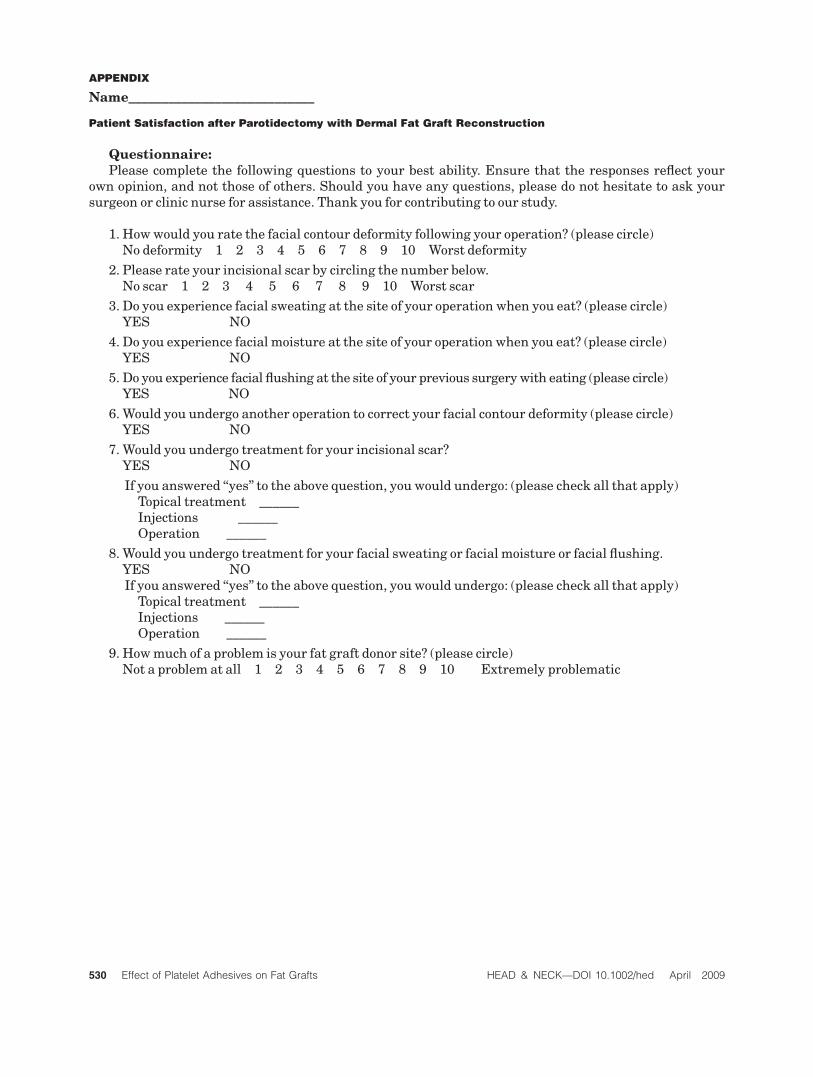
APPENDIX
Name____________________________
Patient Satisfaction after Parotidectomy with Dermal Fat Graft Reconstruction
Questionnaire:Please complete the following questions to your best ability. Ensure that the responses reflect your
own opinion, and not those of others. Should you have any questions, please do not hesitate to ask yoursurgeon or clinic nurse for assistance. Thank you for contributing to our study.
1. Howwould you rate the facial contour deformity following your operation? (please circle)No deformity 1 2 3 4 5 6 7 8 9 10 Worst deformity
2. Please rate your incisional scar by circling the number below.No scar 1 2 3 4 5 6 7 8 9 10 Worst scar
3. Do you experience facial sweating at the site of your operation when you eat? (please circle)YES NO
4. Do you experience facial moisture at the site of your operation when you eat? (please circle)YES NO
5. Do you experience facial flushing at the site of your previous surgerywith eating (please circle)YES NO
6.Would you undergo another operation to correct your facial contour deformity (please circle)YES NO
7.Would you undergo treatment for your incisional scar?YES NO
If you answered ‘‘yes’’ to the above question, you would undergo: (please check all that apply)Topical treatment ______Injections ______Operation ______
8.Would you undergo treatment for your facial sweating or facial moisture or facial flushing.YES NOIf you answered ‘‘yes’’ to the above question, you would undergo: (please check all that apply)
Topical treatment ______Injections ______Operation ______
9. Howmuch of a problem is your fat graft donor site? (please circle)Not a problem at all 1 2 3 4 5 6 7 8 9 10 Extremely problematic
530 Effect of Platelet Adhesives on Fat Grafts HEAD & NECK—DOI 10.1002/hed April 2009
Copyright © 2022 FDOKUMEN