The extent of root resorption and tooth movement following the ...
Upload
khangminh22Category
view
0download
0
DR.ABHINAV GUPTA

•INTRODUCTION
•DEFINITIONS
•BASIC CONCEPTS
•PATHOLOGY
•PATHOPHYSIOLOGY
•PATHOGENESIS
•EPIDEMIOLOGY
ETIOLOGY
METHODS OF MEASUREMENT OF BONE LOSS
CONSEQUENCES
TREATMENT AND PREVENTION
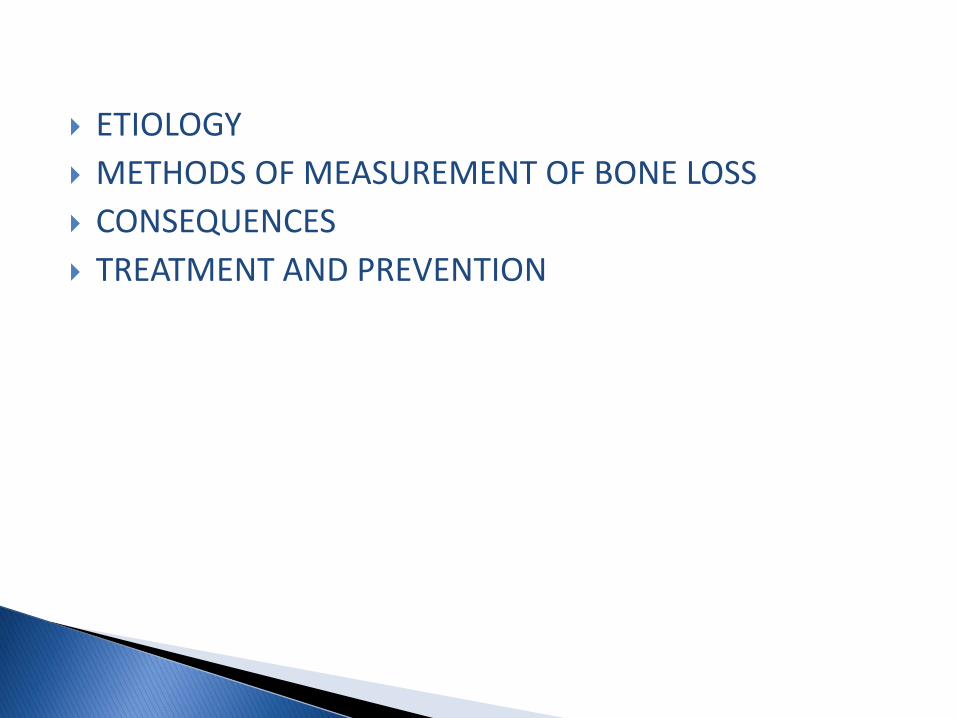
•Residual ridge is a term used to describe the shape of the clinical alveolar ridge after healing of bone and soft tissues after tooth extraction.
•It consists of the denture-bearing mucosa,submucosa, periosteum and the underlying residual alveolar bone.
After tooth extraction , a cascade of inflammatory reactions is immediately activated and the extraction socket is temporarily closed by the blood clot.
Epithelial tissue begins its proliferation and migration within the first week and the disrupted tissue integrity is quickly restored.
The most striking feature of the extraction wound healing is that even after healing of wounds , the residual alveolar ridge bone undergoes a life-long catabolic remodelling.
The size of the residual ridge is reduced most rapidly in the first 6 months,but the bone resorption activity continues throughout life at a slower rate,resulting in removal of a large amount of jaw structure.
This unique phenomeneon has been described as RESIDUAL RIDGE RESORPTION(RRR).
The rate of RRR is different among persons and even at different sites in the same person.
The mechanical aspect of bone remodeling is usually associated with wolff’s law of bone transformation(1892) which states that
“Every Change In The Form And Function of Bone,Or Of Their Function Alone,is Followed By Certain definite changes In Their Internal Architecture,And Equally Definite Alteration In Their External Conformation,In Accordance With Mathematical Laws”,
which simply means that bone remodels in response to the force applied . However , the mere reference to ‘wolff’s law’ in relation to bone resorption is an inadequate explanation of this complex physiologic process.

➢BONE- a highly vascularised,living ,constantly changing ,mineralized connective tissue.(Gray’s Anatomy-40th edition)
➢ALVEOLAR PROCESS- that part of the maxilla and mandible that forms and supports the sockets of theteeth.(Orban’s)
➢ALVEOLAR BONE- bony portion of the maxilla and the mandible in which roots of the teeth are held by fibres of periodontal ligament.(GPT-9)
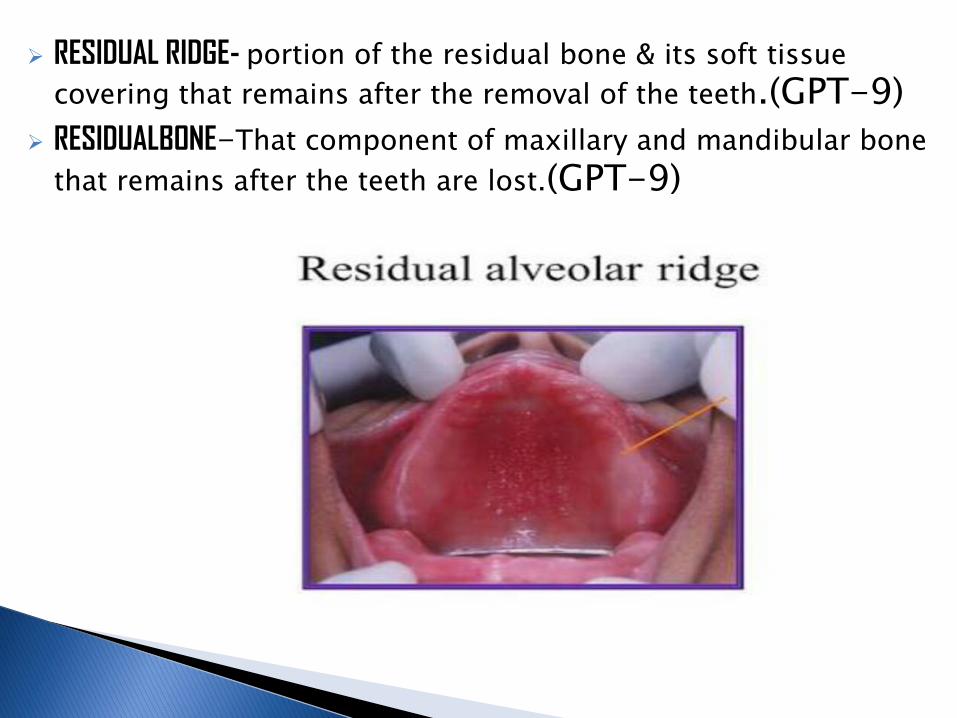
➢ RESIDUAL RIDGE- portion of the residual bone & its soft tissue
covering that remains after the removal of the teeth.(GPT-9)
➢ RESIDUALBONE-That component of maxillary and mandibular bone
that remains after the teeth are lost.(GPT-9)
A basic concept of bone structure and its functional elements must be clear before bone resorption can be understood. The structural elements of bone are:
a) Osteocytes found in bone lacunae
b) The intercellular substance or bone matrix consisting of fibrils and calcified cementing substance
c) Osteoblasts
d) osteoclasts
OSTEOCYTES:These are small flattened and rounded cells embeded in
the bony lacunae.
They are the main cells , of the developed bone and are derived from the matured osteoblasts.
FUNCTION
Helps to maintain bone as a living tissue because of their metabolic activity.
Plays an important role in maintaining the exchange of calcium between bone and extra cellular fluid.
They are giant multinucleated cells foundinthe lacunae of bone matrix
FUNCTION
responsible for bone resorption during bone remodelling. Bone resorption always requires the simultaneous elimination of organic and inorganic components of the intercellular substance.

CALCIFIED CEMENTING SUBSTANCE:
Consists of mainly polymerized glycoproteins and mineral salts namely CaCo3 and phosphate which are bound to these protein substances.
OSTEOBLASTS:Concerned with bone formation and are situated on the
outer surface of bone in a continuous layers.

•ACCORDING TO BOUCHER,
•During the first year after tooth extraction, the reduction in residual ridge height in the mid sagittal plane is:
1. 2-3 mm for maxilla
2. 4-5 mm for mandible
Annual rate of reduction in height
1. 0.1-0.2 mm for mandible
2. 4 times less in the
maxilla
DIRECTION OF BONE RESORPTION
Maxilla resorbs upward and inward to become progressively smaller because of the direction and inclination of the roots of teeth and the alveolar process.
The opposite is true of the mandible which inclines outward and becomes progressively wider according to edentulous age.
RRR Is generally more in mandible than in maxilla and but the reverse may also occur.
So must treat the :- PARTICULAR PATIENT NOT THE AVERAGE PATIENT.

The basic structural change in RRR is a reduction in the size of the bony ridge under the mucoperiosteum.It Is primarily a localized loss of bone structure .In order to provide a simplified method for categorizing the most common residual ridge configurations,a system of six
orders of RR Form has been described.
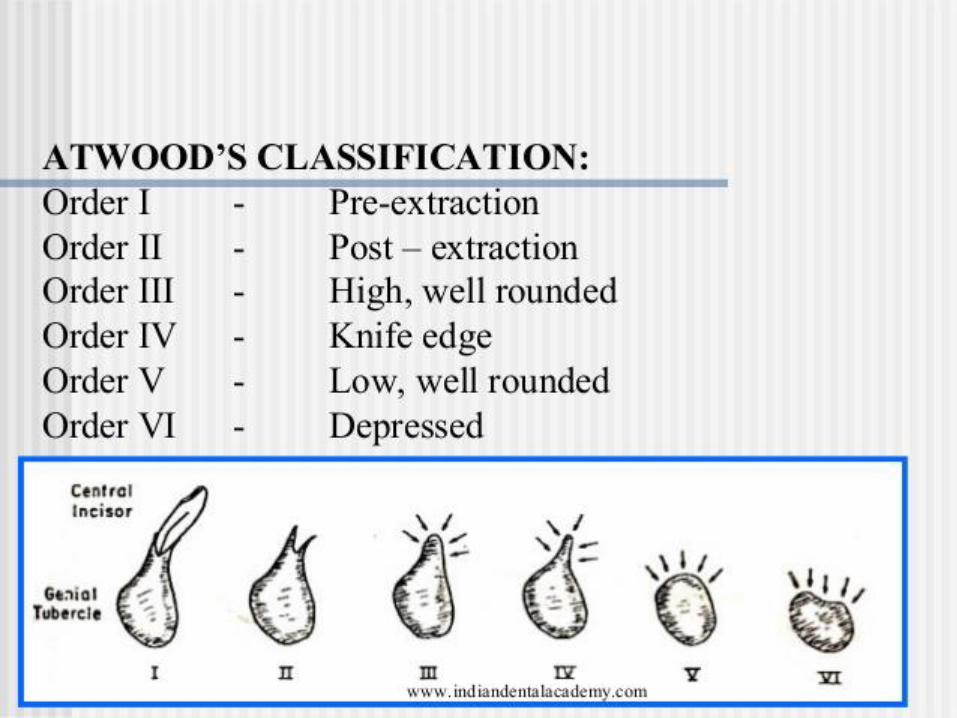
➢Order 1 - Pre extraction
➢Order 2 - Post extraction
➢Order 3 - High, well-rounded
➢Order 4 - Knife edge
➢Order 5 - Low, well-rounded
➢Order 6 - Depressed
•It is clear that RRR does not stop with the residual ridge but may go well below where the apices of the teeth were.
•One can more accurately determine the amount of underlying bone by palpation in the mouth.
•Lateral cephalometric radiograph provide the most accurate method for determining the amount of residual ridge and the rate of RRR over a period of time.
•It is a normal function of bone to undergo constant remodelingthroughout life through the process of bone resorption and bone formation.
•GROWTH:↑Bone formation
•OSTEOPOROSIS/LOCALIZED PERIODONTAL DISEASE:↑Bone resorption

•RRR is a localized pathologic loss of bone that is not built back by simply removing the causative factors.
•Yet , the physiologic process of internal bone remodelinggoes on even in the presence of this pathologic external osteoclastic activity that is responsible for the loss of so much bone substance.
•Even if great deal of RR is removed in total, there is often a cortical layer of bone over the crest of the ridge.This means that new bone has been laid down inside the RR in advance of the external osteoclastic removal of bone

❖RRR is not inevitable.
❖It’s Rate varies
❖The rate of resorption is greater than the rateof absorption in some patients.
......RRR SHOULD BE CONSIDERED A PATHOLOGIC PROCESS.

Immediately following the extraction(orderII),any sharp edges remaining are rounded off by external osteoclastic resrption,leaving a high well-rounded residual ridge(orderIII).
As resorption continues from the labial and lingual aspects , the crest of the ridge becomes increasingly narrow , ultimately becoming knife-edged(orderIV).
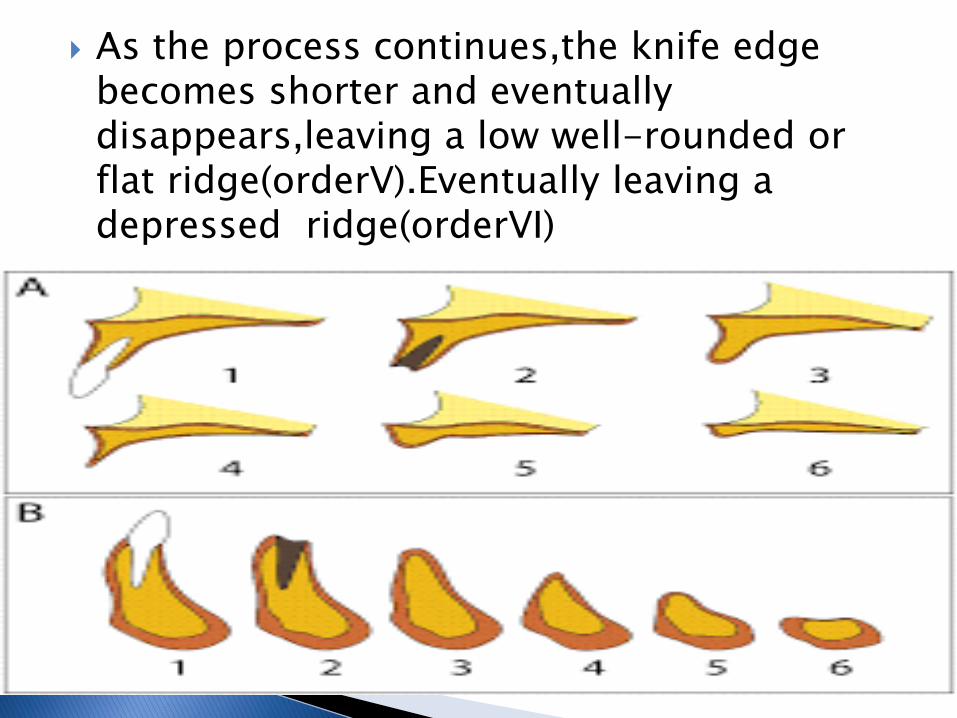
As the process continues,the knife edge becomes shorter and eventually disappears,leaving a low well-rounded or flat ridge(orderV).Eventually leaving a depressed ridge(orderVI)
RRR is a chronic , progressive, irreversible and cumulative. Usually RRR proceeds slowly over a long period of time flowing from one stage imperceptibly to the next
Autonomous regrowth has not been reported. Annual increments of bone loss have a cumulative effect leaving less and less residual ridge.

To date, it would appear that RRR is worldwide,occur in males and females,young and old,sickness and in health,with and without denture and is unrelated to the primary reason for the extraction(caries/periodontal disease)
•It is postulated that RRR is a multifactorial, biomechanical disease that
Results from a combination of:
•ANATOMIC
•METABOLIC
•MECHANICAL
It is postulated that RRR varies with the
quantity and quality of the bone of the
Residual ridges
RRR α Anatomic factors
i.e, the more bone there is, the more RRR ultimately be.
•But this cannot be considered a good prognostic factor, because in some cases large ridges resorb rapidly and some knife-edge ridges may remain with little change for long periods of time.
➢We should always try to evaluate the present status of the residual ridge.
➢If a ridge has existed as high and well rounded(orderIII)for several years, it will likely to continue to do so.
➢But if a ridge has gone from an orderII to orderIV in just two years it will probably continue to resorb rapidly.

RRR varies directly with certain systemic or localized bone resorptive factors and inversely with certain bone formation factors
RRR α BONE RESORPTION FACTOR/BONE FORMATION FACTORS
LOCAL SYSTEMIC
Endotoxins from dental plaque
Osteoclast activating factor
Prostaglandins
Human gingival bone resorption factor
Trauma due to ill fitting dentures which leads to increased vascularity and changes in oxygen tension.
Incorrect amount of circulating estrogen,thyroxine,growth hormone,calcium,phosphorous.
Vitamin D Osteoporosis Hypophosphetemia Parathormone calcitonin

DISUSE V/S ABUSE
•Bone that is used by regular physical activity will attend to strengthen within certain limits, than the bone that is in “disuse atrophy”; while others postulated that due to denture wearing RRR is caused due to an “ abuse” bone resorption.
•Perhaps there is truth in both hypothesis.
•The fact is that with or without dentures some patients have little or no RRR and some have severe RRR.

RRR α FORCE
In considering the force one must concern one self not only with the amount of force,but also with the frequency of force, the duration of force,thedirection of force,the area over which the force is distributed and the damping effect of the underlying bone.
RRR α 1/Damping effect
The amount of force applied to the bone may be affected inversely by the damping effect or energy absorption.
The damping effect is due to the viscoelasticproperty of the mucoperiosteum and may vary from patient to patient and also from maxilla to mandible.

Cancellous bone helps in the absorption and dissipation of forces and is more in the maxilla than mandible,which could be a reason in the difference in RRR between them.
PROSTHETIC FACTORS
•Intensive Denture wearing
long continued use of ill-fitting denture, use of under extended denture ,excessive stress resulting from artificial environment,abuse of tissues of tissue from lack of rest.

•Unstable occlusal condition
Incorrect centric relation record,error in relating maxilla to the cranial landmarks(orientation relation),
•RADIOGRAPH:
-CEPHALOMETRICS
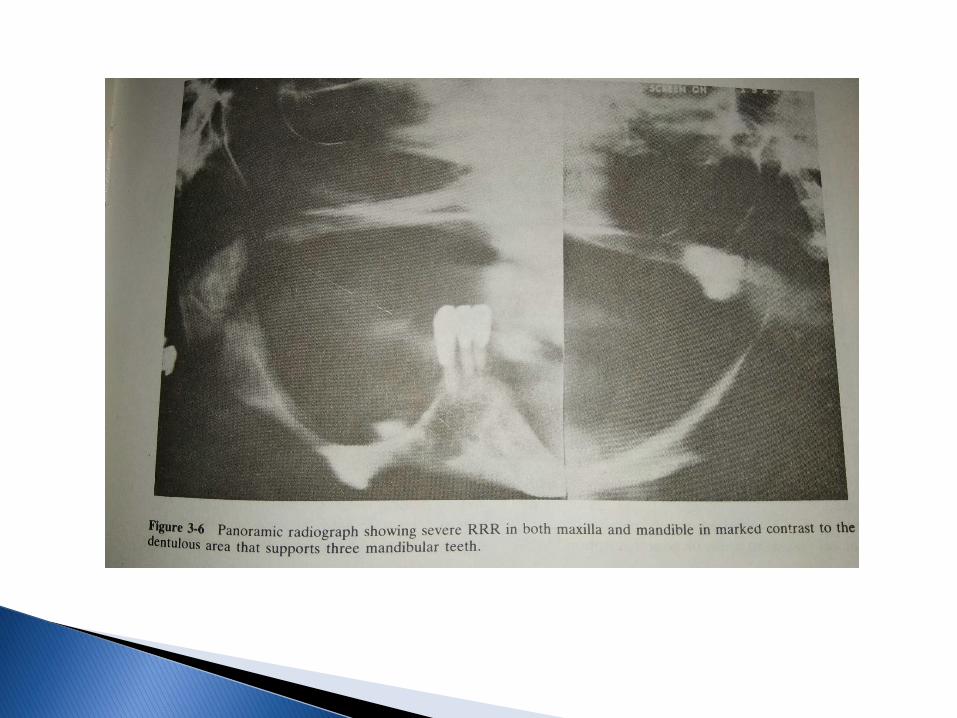
-PANORAMIC
•TETRACYCLINE LABELLING
•MERCURY POROSIMETRY
•ANATOMIC STUDIES
•REMOUNT JIG PROCEDURE

•Apparent loss of sulcus width and depth
•Displacement of the muscle attachment closer to the crest of the residual ridge
•Loss of vertical dimension of occlusion
•Reduction of lower facial height
•An anterior rotation of the mandible
•Increase in relative prognathia.

•Changes in interalveolar relationship
•Morphological changes of the alveolar bone such as sharp,spiny uneven residual ridges
•Location of mental foramina close to the ridge crest
“TREATMENT OF RRR IS IDEALLY BY PREVENTING IT”
•Prevention of loss of natural teeth
•Proper design of denture and maintenance
•Nutrition
TISSUE TREATMENT THERAPY
Soft conditioning materials can be used to rejuvenate the tissue bearing area.
PRE PROSTHETIC SURGERY
o Ridge correction- soft tissue deformities,bonedeformities
o Ridge extension/vestibuloplasty
o Ridge augmentation
o Surgical correction of maxillomandibular relation

PROSTHETIC MANAGEMENT
•IMPRESSION TECHNIQUE
•DENTURE BASE SELECTION
•TEETH SELECTION AND ARRANGEMENT
•IMPLANT SUPPORTED PROSTHESIS
•Essentials of Prosthodontics- by Sheldon Winkler
•Prosthodontics treatment for edentulous patients- by Zarb ,
Hobkirk , Eckert , Jacob

Copyright © 2022 FDOKUMEN