
Early Feeding After Placement of a Percutaneous Endoscopic Gastrostomy: A Meta-Analysis
6
American Journal of Gastroenterology ISSN 0002-9270 C 2008 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2008.02108.x Published by Blackwell Publishing Early Versus Delayed Feeding After Placement of a Percutaneous Endoscopic Gastrostomy: A Meta-Analysis Matthew L. Bechtold, M.D., Michelle L. Matteson, A.P.N., Abhishek Choudhary, M.D., Srinivas R. Puli, M.D., Peter P. Jiang, M.D., and Praveen K. Roy, M.D. Division of Gastroenterology, University of Missouri School of Medicine, Columbia, Missouri BACKGROUND: Traditionally, tube feedings have been delayed after percutaneous endoscopic gastrostomy (PEG) placement to the next day and up to 24 h postprocedure. However, results from various randomized controlled trials (RCTs) indicate earlier feeding may be an option. We conducted a meta-analysis to analyze the effect of early feedings (≤4 h) after PEG placement. METHODS: Multiple databases were searched (November 2007). Only RCTs on adult subjects that compared early (≤4 h) versus delayed or next-day feedings after PEG placement were included. Meta-analyses for the effect of early and delayed feedings were analyzed by calculating pooled estimates of complications, death ≤72 h, and significant increases in postprocedural gastric residual volume during day 1. RESULTS: Six studies (N = 467) met the inclusion criteria. No statistically significant differences were noted between early (≤4 h) and delayed or next-day feedings for patient complications (OR 0.86, 95% CI 0.47–1.58, P = 0.63) or death in ≤72 h (OR 0.56, 95% CI 0.18–1.74, P = 0.31). A statistically significant increase in gastric residual volumes during day 1 was noted (OR 1.80, 95% CI 1.02–3.19, P = 0.04). CONCLUSIONS: Early feeding ≤4 h after PEG placement may represent a safe alternative to delayed or next-day feedings. Although an increase in significant gastric residual volumes at day 1 was noted, overall complications were not affected. (Am J Gastroenterol 2008;103:2919–2924) INTRODUCTION Percutaneous endoscopic gastrostomies, first described in 1980, have assisted in the nutritional requirements for many patients who are unable to ingest adequate oral nutrition (1). These endoscopically placed gastrostomy tubes have been a valuable source of nutrition for patients with strokes, dys- phagia, and head and neck cancers undergoing treatment (2, 3). Because of the ease of placement and minimal com- plications, percutaneous endoscopic gastrostomy (PEG) has become widely available and utilized for many clinical situ- ations requiring long-term nutritional support. Although the benefits and techniques for insertion of PEGs have been de- scribed and accepted, the feeding after PEG placement is not as clear. Since 1980, feedings after PEG placement have been sig- nificantly delayed by many hours or to the next day. The delay was most likely a remnant of prior surgical guidelines regard- ing management of patients after surgically placed tubes, with very little evidence regarding feedings after PEG placement. The suspected rationale was to decrease the risk of significant gastric residual volumes during the first day that may lead to aspiration and to decrease the risk of peritoneal leakage that may lead to peritonitis. Over the past 15 yr, many studies have examined the use of early PEG feedings after insertion. Many randomized controlled trials on the subject indicate that early PEG feeding is safe and well tolerated by patients (4–9). Early feeding after PEG placement has also been shown to decrease length of hospitalization and, subsequently, may decrease cost (10). However, these studies differ in timing of post-PEG feedings, from less than 1 h to less than 6 h. Despite the recent literature indicating early PEG feedings as a safe alternative, the common practice continues to be to significantly delay post-PEG feedings. A survey of gastroen- terologists in northeastern United States in 1998 revealed that although 82% of specialists were aware of the recent literature showing early feedings to be safe, only 39% initiated feed- ings prior to 8 h and 11% initiated feedings prior to 3 h (11). The remaining 61% of gastroenterologists surveyed chose to delay feedings from 9 h to >24 h (11). Based upon the significant differences between the liter- ature and clinical practice and between the timing of early feedings within the literature, we conducted a meta-analysis to evaluate the use of early PEG feedings (≤4 h) versus de- layed or next-day feedings for complications, death within 2919
Transcript of Early Feeding After Placement of a Percutaneous Endoscopic Gastrostomy: A Meta-Analysis

American Journal of Gastroenterology ISSN 0002-9270C© 2008 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2008.02108.xPublished by Blackwell Publishing
Early Versus Delayed Feeding After Placement of aPercutaneous Endoscopic Gastrostomy: A Meta-AnalysisMatthew L. Bechtold, M.D., Michelle L. Matteson, A.P.N., Abhishek Choudhary, M.D., Srinivas R. Puli, M.D.,Peter P. Jiang, M.D., and Praveen K. Roy, M.D.Division of Gastroenterology, University of Missouri School of Medicine, Columbia, Missouri
BACKGROUND: Traditionally, tube feedings have been delayed after percutaneous endoscopic gastrostomy (PEG)placement to the next day and up to 24 h postprocedure. However, results from various randomizedcontrolled trials (RCTs) indicate earlier feeding may be an option. We conducted a meta-analysis toanalyze the effect of early feedings (≤4 h) after PEG placement.
METHODS: Multiple databases were searched (November 2007). Only RCTs on adult subjects that comparedearly (≤4 h) versus delayed or next-day feedings after PEG placement were included. Meta-analysesfor the effect of early and delayed feedings were analyzed by calculating pooled estimates ofcomplications, death ≤72 h, and significant increases in postprocedural gastric residual volumeduring day 1.
RESULTS: Six studies (N = 467) met the inclusion criteria. No statistically significant differences were notedbetween early (≤4 h) and delayed or next-day feedings for patient complications (OR 0.86, 95% CI0.47–1.58, P = 0.63) or death in ≤72 h (OR 0.56, 95% CI 0.18–1.74, P = 0.31). A statisticallysignificant increase in gastric residual volumes during day 1 was noted (OR 1.80, 95% CI 1.02–3.19,P = 0.04).
CONCLUSIONS: Early feeding ≤4 h after PEG placement may represent a safe alternative to delayed or next-dayfeedings. Although an increase in significant gastric residual volumes at day 1 was noted, overallcomplications were not affected.
(Am J Gastroenterol 2008;103:2919–2924)
INTRODUCTION
Percutaneous endoscopic gastrostomies, first described in1980, have assisted in the nutritional requirements for manypatients who are unable to ingest adequate oral nutrition (1).These endoscopically placed gastrostomy tubes have been avaluable source of nutrition for patients with strokes, dys-phagia, and head and neck cancers undergoing treatment(2, 3). Because of the ease of placement and minimal com-plications, percutaneous endoscopic gastrostomy (PEG) hasbecome widely available and utilized for many clinical situ-ations requiring long-term nutritional support. Although thebenefits and techniques for insertion of PEGs have been de-scribed and accepted, the feeding after PEG placement is notas clear.
Since 1980, feedings after PEG placement have been sig-nificantly delayed by many hours or to the next day. The delaywas most likely a remnant of prior surgical guidelines regard-ing management of patients after surgically placed tubes, withvery little evidence regarding feedings after PEG placement.The suspected rationale was to decrease the risk of significantgastric residual volumes during the first day that may lead toaspiration and to decrease the risk of peritoneal leakage that
may lead to peritonitis. Over the past 15 yr, many studieshave examined the use of early PEG feedings after insertion.Many randomized controlled trials on the subject indicatethat early PEG feeding is safe and well tolerated by patients(4–9). Early feeding after PEG placement has also beenshown to decrease length of hospitalization and, subsequently,may decrease cost (10). However, these studies differ intiming of post-PEG feedings, from less than 1 h to less than6 h.
Despite the recent literature indicating early PEG feedingsas a safe alternative, the common practice continues to be tosignificantly delay post-PEG feedings. A survey of gastroen-terologists in northeastern United States in 1998 revealed thatalthough 82% of specialists were aware of the recent literatureshowing early feedings to be safe, only 39% initiated feed-ings prior to 8 h and 11% initiated feedings prior to 3 h (11).The remaining 61% of gastroenterologists surveyed chose todelay feedings from 9 h to >24 h (11).
Based upon the significant differences between the liter-ature and clinical practice and between the timing of earlyfeedings within the literature, we conducted a meta-analysisto evaluate the use of early PEG feedings (≤4 h) versus de-layed or next-day feedings for complications, death within
2919

2920 Bechtold et al.
72 h, and significant gastric residual volumes during the firstday.
METHODS
Study Selection CriteriaRandomized controlled trials (RCTs) comparing the out-comes of early (≤4 h) versus delayed or next-day feedingafter PEG placement were identified and selected.
Data Collection and ExtractionArticles were searched in Medline, Cochrane Central Regis-ter of Controlled Trials and Database of Systematic Reviews,DARE, OVID Healthstar and Journals, Cumulative Index forNursing and Allied Health Literature, PubMed (from 1950to 2006), and recent abstracts from major conference pro-ceedings (Digestive Disease Week and American College ofGastroenterology National Meeting from 1993 to 2007) weresearched (November 2007). The search terms used were earlyfeeding, delayed feeding, next-day feeding, and gastrostomy.Only RCTs on adult subjects (≥18 yr old) that comparedearly (≤4 h) versus delayed or next-day feedings after PEGplacement were included. Standard forms were utilized bytwo independent reviewers in extracting the data, with differ-ences being resolved by mutual agreement. Each study wasassigned a Jadad score to assess the quality of the study (5 =excellent quality, 0 = poor quality) (12). The Jadad scoreevaluates the quality of the trial by giving a point for eachof five components: randomization, method of randomiza-tion being appropriate and described, double-blinding, dou-ble blinding being appropriate and described, and descriptionof withdrawal and dropouts (12). If the methods of doubleblinding or randomization were inappropriate, a point maybe deducted for each inappropriate criteria (12). Complica-tions, death, and gastric residual volumes during day 1 wereidentified and extracted from the randomized trials.
Potentially relevant articles identified (N = 231)
Potentially appropriate articles (N = 18)
Trials included in meta-analysis (N = 6)
Excluded N = 12Not RCTs N = 9 Pediatric N = 3
Excluded N = 213Case Reports/Series
Retrospective Reviews Pediatric
Figure 1. Article identification and selection algorithm.
Statistical MethodsMeta-analyses for the effect of early and delayed feedings af-ter PEG tube placement were analyzed by calculating pooledestimates of complications, death ≤72 h, and number of sig-nificant increases in postprocedural gastric residual volumeduring day 1. Odds ratios (OR) were calculated separatelyfor each main outcome using both the fixed and random ef-fects models. Significance was indicated by P value <0.05.Heterogeneity was assessed by calculating the I2 measure ofinconsistency with significant heterogeneity indicated by anI2 value > 50% or P value <0.05. Publication bias was as-sessed by funnel plot. RevMan 4.2 software was utilized forstatistical analysis of the data.
RESULTS
The initial search identified 231 articles (Fig. 1). Of thesearticles, 18 relevant articles were selected and reviewed bytwo independent authors (MLB and MLM). Six randomizedcontrolled trials (N = 467) met the inclusion criteria andwere selected for this study. Data were extracted from thesesix studies. Table 1 shows the details and Jadad scores forthe selected studies. All of the studies received Jadad scoresof 2. All randomized trials were published from 1993 to 2002.Studies were performed in two countries, the United States(4) and Germany (2). The mean age of patients participatingin the selected studies ranged from 63 to 76 yr. Results wereconsistent between the fixed and random effects models.
ComplicationsObserved patient complications after PEG placement in-cluded local infections, diarrhea, bleeding, GERD, fever,vomiting, stomatitis, leakage, and death (Table 2). Early feed-ings resulted in 25 complications in 232 patients while de-layed or next-day feedings resulted in 29 complications in235 patients. Complications were not statistically significant

Early Versus Delayed Feeding After Placement of PEG 2921
Table 1. Details of Included Studies in the Meta-Analysis
Study Number of Pts/ JadadAuthor Type Blinded Location Antibiotics Patients Feedings Time Group Score
Brown et al. 1995 RCT None United States Yes 57 Early <3 h 27 2Delayed Next day 30
McCarter et al. 1997 RCT None United States Yes 112 Early 4 h 57 2Delayed 24 h 55
Choudhry et al. 1996 RCT None United States Yes 41 Early 3 h 21 2Delayed 24 h 20
Stein et al. 2002 RCT None Germany No 80 Early <1 h 40 2Delayed 24 h 40
Chumley et al. 1993 RCT - Abst None United States Yes 100 Early 3 h 50 2Delayed 24 h 50
Schulte-Bockholt et al. 1998 RCT - Abst None Germany No 77 Early <1 h 37 2Delayed Next day 40
RCT = randomized controlled trial; Abst = abstract.Jadad Score (5 = excellent quality and 0 = poor quality).
Table 2. Summary of Complications, Death ≤72 h, and Numberof Significant Gastric Residual Volumes During Day 1 Among theIncluded Studies
Outcome Early Delayed
All Complications (n) 25 29Vomiting 7 8Diarrhea 5 5Death ≤72 h 4 8Stomatitis 4 0Leakage 0 4Local infection 2 3Bleeding 1 1Fever 1 0Transient GERD 1 0Death ≤72 h (n) 4 8Increased gastric residuals during day 1 (n) 40 25
between the early (≤4 h) and delayed or next-day feedings af-ter PEG placement (OR 0.86, 95% CI 0.47–1.58, P = 0.63).Figure 2 shows the Forrest plot of all complications withearly versus delayed or next-day feeding after PEG place-ment. Heterogeneity was not statistically significant (I2 =0%, P = 0.58).
Figure 2. Forrest plot demonstrating all complications between early (≤4 h) versus delayed or next-day feedings after PEG placement.
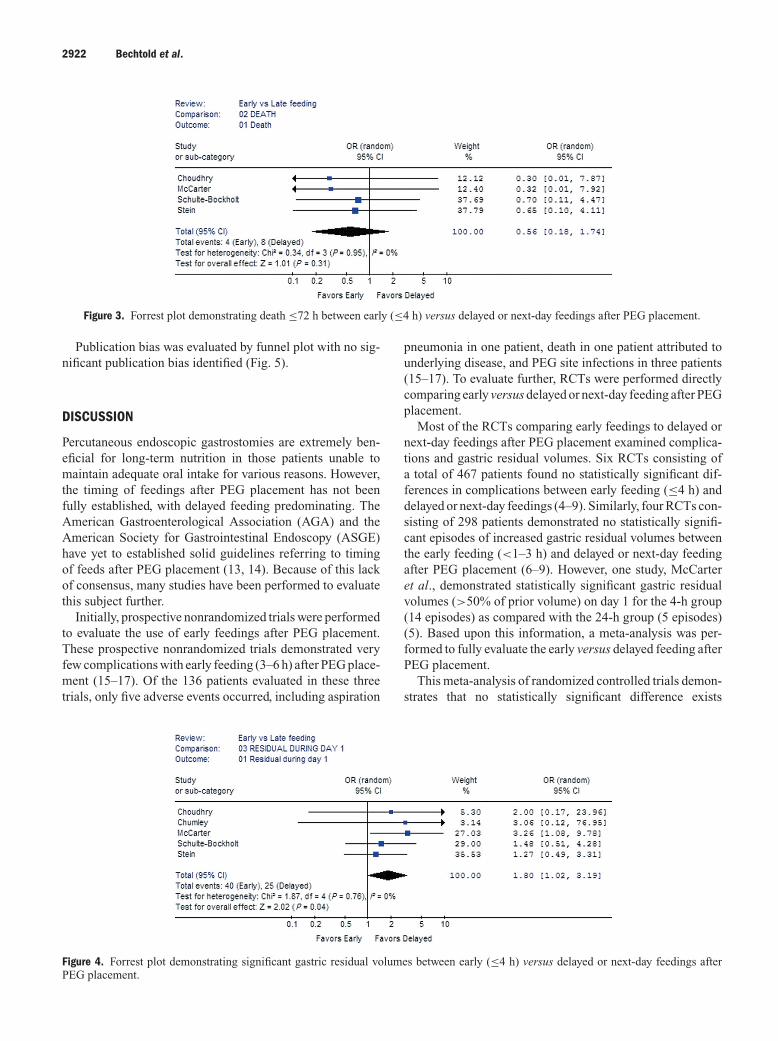
Death ≤72 hDeath ≤72 h was the outcome in 12 patients (early = 4, de-layed = 8). Death in ≤72 h was not statistically significantbetween the early (≤4 h) and delayed or next-day feedings af-ter PEG placement (OR 0.56, 95% CI 0.18–1.74, P = 0.31).Figure 3 shows the Forrest plot of death within 72 h withearly versus delayed or next-day feeding after PEG place-ment. Heterogeneity was not statistically significant (I2 =0%, P = 0.95).
Gastric Residual Volumes During Day 1The number of significant gastric residual volumes duringday 1 ranged from 0 to 14 episodes. Early feedings after PEGplacement resulted in 40 episodes of significant gastric resid-uals during day 1 in 205 patients while delayed or next-dayfeedings resulted in 25 episodes in 205 patients. Increasedgastric residual volumes during day 1 were statistically sig-nificant between the early (≤4 h) and delayed or next-dayfeedings after PEG placement (OR 1.80, 95% CI 1.02–3.19,P = 0.04). Figure 4 shows the Forrest plot of significant gas-tric residual volumes during day 1 with early versus delayedor next-day feeding after PEG placement. Heterogeneity wasnot statistically significant (I2 = 0%, P = 0.76).
2922 Bechtold et al.
Figure 3. Forrest plot demonstrating death ≤72 h between early (≤4 h) versus delayed or next-day feedings after PEG placement.
Publication bias was evaluated by funnel plot with no sig-nificant publication bias identified (Fig. 5).
DISCUSSION
Percutaneous endoscopic gastrostomies are extremely ben-eficial for long-term nutrition in those patients unable tomaintain adequate oral intake for various reasons. However,the timing of feedings after PEG placement has not beenfully established, with delayed feeding predominating. TheAmerican Gastroenterological Association (AGA) and theAmerican Society for Gastrointestinal Endoscopy (ASGE)have yet to established solid guidelines referring to timingof feeds after PEG placement (13, 14). Because of this lackof consensus, many studies have been performed to evaluatethis subject further.
Initially, prospective nonrandomized trials were performedto evaluate the use of early feedings after PEG placement.These prospective nonrandomized trials demonstrated veryfew complications with early feeding (3–6 h) after PEG place-ment (15–17). Of the 136 patients evaluated in these threetrials, only five adverse events occurred, including aspiration
Figure 4. Forrest plot demonstrating significant gastric residual volumes between early (≤4 h) versus delayed or next-day feedings afterPEG placement.
pneumonia in one patient, death in one patient attributed tounderlying disease, and PEG site infections in three patients(15–17). To evaluate further, RCTs were performed directlycomparing early versus delayed or next-day feeding after PEGplacement.
Most of the RCTs comparing early feedings to delayed ornext-day feedings after PEG placement examined complica-tions and gastric residual volumes. Six RCTs consisting ofa total of 467 patients found no statistically significant dif-ferences in complications between early feeding (≤4 h) anddelayed or next-day feedings (4–9). Similarly, four RCTs con-sisting of 298 patients demonstrated no statistically signifi-cant episodes of increased gastric residual volumes betweenthe early feeding (<1–3 h) and delayed or next-day feedingafter PEG placement (6–9). However, one study, McCarteret al., demonstrated statistically significant gastric residualvolumes (>50% of prior volume) on day 1 for the 4-h group(14 episodes) as compared with the 24-h group (5 episodes)(5). Based upon this information, a meta-analysis was per-formed to fully evaluate the early versus delayed feeding afterPEG placement.
This meta-analysis of randomized controlled trials demon-strates that no statistically significant difference exists

Early Versus Delayed Feeding After Placement of PEG 2923
Figure 5. Funnel plot showing no significant publication bias.
between early (≤4 h) and delayed or next-day feeding inrespect to complications or death ≤72 h. However, a sta-tistically significant difference was noted between the twogroups for number of increased gastric residual volumes dur-ing day 1. Although gastric residual volumes were increasedduring day 1, overall complications were not affected. Sim-ply holding tube feeds for a minimal period of time alleviatedthe significant residual volumes; however, feeding interrup-tions because of elevated gastric residuals do decrease overallnutrition (18). Although gastric feeding is a risk factor for as-piration and subsequent pneumonia (19, 20), recent data fromvarious trials question the clinical significance of increasedgastric residuals (18, 21, 22). McClave et al. demonstratedthat when the discontinuation threshold of gastric residualvolumes was raised from 200 mL to 400 mL, no statisticallysignificant difference in the incidence of aspiration or regur-gitation was observed (21). Furthermore, over an extensiverange of gastric residuals (0 to >400 mL), the frequency ofaspiration and regurgitation did not significantly change (21).Elpern et al. found that, although significant gastric residuals(>150 mL) occurred multiple times in 11 of 39 patients, onlyfour patients experienced feeding aspiration (18). Althoughsignificant gastric residual volumes were significant in earlyfeeding after PEG placement, no patients were reported tosuffer from massive aspiration in the included studies. Onlyone patient in a delayed group with feeding initiated at 24 hpost-PEG placement was reported to have death related tomassive aspiration (5).
This study’s strengths include the use of only RCTs, vary-ing populations within Germany and the United States, andsimilar outcomes between studies in regards to complica-tions and residual volumes. Also, no heterogeneity betweenthe studies for any of the three variables and no publication
bias were observed. However, some limitations were appar-ent. First, the timing of early feedings differed slightly amongthe studies (<1 h, 2 studies; ≤3 h, 3 studies; and ≤4 h, 1study) (4–9). In an effort to decrease potential bias, the anal-ysis used ≤4 h as the point for pooling of data. However, evenearlier feeding may be as beneficial as pooled effect of ≤4 h.Second, significant gastric residual volumes did slightly varydepending on the study. Stein et al. and Schulte-Bockholtet al. used >100 mL, McCarter et al. used >50% of the lastvolume administered, and Choudhry et al. used >60 mL assignificant residual volumes (5–7, 9). To pool the data andto minimize the different criteria utilized, the number of sig-nificant gastric residual volumes were used rather than thevolumes themselves. Third, PEG sizes differed among thestudies from 15-Fr to 20-Fr gastrostomies (4, 5, 7, 9) whiletwo studies did not specify the size of gastrostomy used (6,8). Although the PEG sizes were different, both populations(early vs delayed feeding groups) in each study had approx-imately equal sizes, minimizing any effects of PEG size onthe overall outcomes. Last, the quality of studies was not ex-cellent. All studies received a Jadad score of 2 based uponrandomized trials with lack of double blinding or descriptionsof withdrawals. Although the study quality was not excellent,these are the only randomized studies published to date onthe subject. Also, all studies followed a similar protocol andevaluated similar outcomes.
In conclusion, this meta-analysis reveals that early feeding≤4 h after PEG placement appears to be a safe and well-tolerated alternative to delayed feedings. Despite the popularopinion of delaying feedings after PEG placement (11), earlyfeeding appears to be safe and, if implemented in clinicalpractice, may result in decreased hospital stays and health-care costs for those patients undergoing PEG placement.

2924 Bechtold et al.
Reprint requests and correspondence: Matthew L. Bechtold,M.D., Division of Gastroenterology, M580, DC 043.00, Universityof Missouri Health Sciences Center, One Hospital Drive, Columbia,MO 65212.
Received March 26, 2008; accepted June 16, 2008.
REFERENCES
1. Gauderer MW, Ponsky JL, Izant RJ Jr. Gastrostomy withoutlaparotomy: A percutaneous endoscopic technique. J PediatrSurg 1980;15:872–5.
2. Ha L, Hauge T. Percutaneous endoscopic gastrostomy(PEG) for enteral nutrition in patients with stroke. ScandJ Gastroenterol 2003;38:962–6.
3. Angus F, Burakoff R. The percutaneous endoscopic gastros-tomy tube: Medical and ethical issues in placement. Am JGastroenterol 2003;98:272–7.
4. Brown DN, Miedema BW, King PD, et al. Safety of earlyfeeding after percutaneous endoscopic gastrostomy. J ClinGastroenterol 1995;21:330–1.
5. McCarter TL, Condon SC, Aguilar RC, et al. Randomizedprospective trial of early versus delayed feeding after per-cutaneous endoscopic gastrostomy placement. Am J Gas-troenterol 1998;93:419–21.
6. Choudhry U, Barde CJ, Markert R, et al. Percutaneousendoscopic gastrostomy: A randomized prospective com-parison of early and delayed feeding. Gastrointest Endosc1996;44:164–7.
7. Stein J, Schulte-Bockholt A, Sabin M, et al. A randomizedprospective trial of immediate vs. next-day feeding after per-cutaneous endoscopic gastrostomy in intensive care patients.Intensive Care Med 2002;28:1656–60.
8. Chumley DL, Batch WJ, Hoberman LJ, et al. Same day PEGfeeding, is it safe? Results of randomized prospective study.Am J Gastroenterol 1993;88:1589.
9. Schulte-Bockholt A, Sabin M, Rosenstock U, et al. Imme-diate versus next day PEG feeding: A randomized prospec-tive study in ICU/intermediate care patients. Gastroenterol1998;114:A907.
10. Werlin S, Glicklich M, Cohen R. Early feeding after per-cutaneous endoscopic gastrostomy is safe in children. Gas-trointest Endosc 1994;40:692–3.
11. Srinivasan R, Fisher RS. Early initiation of post-PEG feed-ing: Do published recommendations affect clinical practice?Dig Dis Sci 2000;45:2065–8.
12. Jadad AR, Moore RA, Carroll D, et al. Assessing the qualityof reports of randomized clinical trials: Is blinding neces-sary? Control Clin Trials 1996;17:1–12.
13. American Gastroenterological Association medical positionstatement: Guidelines for the use of enteral nutrition. Gas-troenterology 1995;108:1280–1.
14. Eisen GM, Baron TH, Dominitz JA, et al. Role of endoscopyin enteral feeding. Gastrointest Endosc 2002;55:794–7.
15. Navarro L, Reymunde A. Outcome of early feeding af-ter percutaneous endoscopic gastrostomy. Gastroenterology1995;108:A656.
16. Dubagunta S, Still CD, Kumar A, et al. Early initiation ofenteral feeding after percutaneous endoscopic gastrostomytube placement. Nutr Clin Pract 2002;17:123–5.
17. Bajaj A, Moran J, Rashed A, et al. Safety of immediatefeedings in contrast to delayed feeding following percuta-neous endoscopic gastrostomy (PEG). Am J Gastroenterol1993;88:1503.
18. Elpern EH, Stutz L, Peterson S, et al. Outcomes associatedwith enteral tube feedings in a medical intensive care unit.Am J Crit Care 2004;13:221–7.
19. Metheny NA, Clouse RE, Chang YH, et al. Tracheo-bronchial aspiration of gastric contents in critically ill tube-fed patients: Frequency, outcomes, and risk factors. Crit CareMed 2006;34:1007–15.
20. Montecalvo MA, Steger KA, Farber HW, et al. Nutritionaloutcome and pneumonia in critical care patients random-ized to gastric versus jejunal tube feedings. Crit Care Med1992;20:1377–87.
21. McClave SA, Lukan JK, Stefater JA, et al. Poor validityof residual volumes as a marker for risk of aspirationin critically ill patients. Crit Care Med 2005;33:324–30.
22. Lukan J, McClave S, Lowen C. Poor validity of residualvolume as a marker for risk of aspiration. Am J Clin Nutr2002;75:417–8.
CONFLICT OF INTEREST
Guarantor of the article: Matthew L. Bechtold, M.D.Specific author contributions: Conception and design:Bechtold, Matteson, Jiang, Roy; Acquisition of data: Bech-told, Matteson, Puli, Choudhary, Jiang, Roy; Analysis andinterpretation of data: Bechtold, Matteson, Puli, Choudhary,Jiang, Roy; Drafting of manuscript: Bechtold, Matteson, Puli,Choudhary; Critical revision of manuscript: Bechtold, Matte-son, Puli, Choudhary, Jiang, Roy; Statistical Expertise: Puli,Bechtold, Choudhary, Roy; Overall supervision of project:Jiang, Roy; and Administrative/technical/material support:None.Financial Support: None.Potential competing interests: None.




















