Drug-eluting stents perform better than bare metal stents in small coronary vessels: A meta-analysis...
10
Drug-eluting stents perform better than bare metal stents in small coronary vessels: A meta-analysis of randomised and observational clinical studies with mid-term follow up Bernardo Cortese a, ⁎, Alessandra Bertoletti b , Sara De Matteis c,d , Gian Battista Danzi b , Adnan Kastrati e a Interventional Cardiology, Ospedale Humanitas Gavazzeni, Bergamo, Italy b Cardiologic Department, Ospedale Maggiore Policlinico, Milano, Italy c Unit of Epidemiology, Department of Preventive Medicine, Fondazione IRCCS Ca' Granda - Ospedale Maggiore Policlinico, Italy d EPOCA Research Center, Department of Occupational and Environmental Health, Università degli Studi di Milano, Milan, Italy e Department of Cardiology, Deutsches Herzzentrum, Technische Universität, Munich, Germany abstract article info Article history: Received 19 January 2011 Received in revised form 7 March 2011 Accepted 17 April 2011 Available online 13 May 2011 Keywords: PCI Small vessels DES BMS Background: We tested drug-eluting stent (DES) and bare metal stent (BMS) performance in small coronary vessels by means of meta-analysis of all available clinical studies. Methods: The analysis included randomised controlled trials (RCT), subgroups of RCT and observational studies with a follow-up of at least six months comparing the use of DES and BMS during percutaneous interventions involving small coronary arteries (diameter b 3 mm). The primary endpoint was target vessel failure (TVF); the others were pooled and isolated major adverse cardiovascular events (MACE), stent thrombosis (ST), binary restenosis and late lumen loss at the longest available follow-up. The effect of treatment was evaluated in terms of odds ratios (OR) and 95% confidence intervals (95% CI) for binary variables, and mean difference (MD) ± standard deviation (SD) for continuous variables. Fixed- or random- effect models were used depending on the statistical heterogeneity of studies. The analyses of major endpoints were stratified by study type, length of follow-up, and type of DES. Results: We pooled 12 studies involving 3182 patients. Trial heterogeneity was a minor issue. TVF (OR: 0.35; CI: 0.24–0.51), MACE (OR: 0.36; CI: 0.29–0.45), binary restenosis (OR: 0.15; CI: 0.12–0.20) and late lumen loss (MD: −0.46; SD: −0.55 to −0.38) all significantly improved with DES treatment; ST (OR: 0.63; CI: 0.34–1.17) was not statistically different between studies. Conclusions: DES are superior to BMS in terms of their efficacy in managing small coronary arteries (diameter b 3 mm), and at least equivalent in terms of safety. The use of DES should be considered the treatment of choice in this setting. © 2011 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Percutaneous coronary interventions (PCI) involving small coro- nary vessels represent a true challenge in modern interventional cardiology because of the increased risk of restenosis and adverse outcomes [1]; furthermore, a small vessel does not always mean limited myocardial ischemia and so the percutaneous treatment of small coronary branches (i.e. those with a diameter of b 3 mm) often has a considerable impact on future clinical events. Stents are currently the mainstay of such treatment, but the rate of adverse events is still high after the use of bare metal stents (BMS) [2–5] and, although drug eluting stents (DES) are now widely used to treat small coronary lesions, conflicting or inconclusive data have come from randomised clinical trials and registries because of the supposedly higher risk of stent thrombosis (ST) and even higher restenosis rate [6,7]. In the absence of a systematic overview of clinical and angio- graphic outcomes that would provide more robust evidence, we made this meta-analysis of the available trials and registries directly comparing the two types of stent. 2. Methods 2.1. Study selection strategy The eligible studies included randomised controlled clinical trials (RCT) [8–10], subgroups from RCT and observational studies [11–20] of PCIs using a DES or BMS to treat small coronary artery disease, provided that they had a follow-up of at least six months. The target vessel had to have a diameter b 3 mm with a clinical indication to International Journal of Cardiology 161 (2012) 73–82 ⁎ Corresponding author at: Interventional Cardiology, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Via Francesco Sforza, 37, 20122 Milano, Italy. Tel.: + 39 0255033539; fax: + 39 0255034157. E-mail address: [email protected] (B. Cortese). 0167-5273/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijcard.2011.04.016 Contents lists available at ScienceDirect International Journal of Cardiology journal homepage: www.elsevier.com/locate/ijcard
Transcript of Drug-eluting stents perform better than bare metal stents in small coronary vessels: A meta-analysis...

International Journal of Cardiology 161 (2012) 73–82
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r.com/ locate / i j ca rd
Drug-eluting stents perform better than bare metal stents in small coronary vessels:A meta-analysis of randomised and observational clinical studies with mid-termfollow up
Bernardo Cortese a,⁎, Alessandra Bertoletti b, Sara De Matteis c,d, Gian Battista Danzi b, Adnan Kastrati e
a Interventional Cardiology, Ospedale Humanitas Gavazzeni, Bergamo, Italyb Cardiologic Department, Ospedale Maggiore Policlinico, Milano, Italyc Unit of Epidemiology, Department of Preventive Medicine, Fondazione IRCCS Ca' Granda - Ospedale Maggiore Policlinico, Italyd EPOCA Research Center, Department of Occupational and Environmental Health, Università degli Studi di Milano, Milan, Italye Department of Cardiology, Deutsches Herzzentrum, Technische Universität, Munich, Germany
⁎ Corresponding author at: Interventional CardiologyOspedale Maggiore Policlinico, Via Francesco Sforza, 37,0255033539; fax: +39 0255034157.
E-mail address: [email protected] (B. Cortese).
0167-5273/$ – see front matter © 2011 Elsevier Irelanddoi:10.1016/j.ijcard.2011.04.016
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 19 January 2011Received in revised form 7 March 2011Accepted 17 April 2011Available online 13 May 2011Keywords:PCISmall vesselsDESBMS
Background: We tested drug-eluting stent (DES) and bare metal stent (BMS) performance in small coronaryvessels by means of meta-analysis of all available clinical studies.Methods: The analysis included randomised controlled trials (RCT), subgroups of RCT and observationalstudies with a follow-up of at least six months comparing the use of DES and BMS during percutaneousinterventions involving small coronary arteries (diameterb3 mm). The primary endpoint was target vesselfailure (TVF); the others were pooled and isolated major adverse cardiovascular events (MACE), stentthrombosis (ST), binary restenosis and late lumen loss at the longest available follow-up. The effect oftreatment was evaluated in terms of odds ratios (OR) and 95% confidence intervals (95% CI) for binaryvariables, and mean difference (MD)±standard deviation (SD) for continuous variables. Fixed- or random-effect models were used depending on the statistical heterogeneity of studies. The analyses of major
endpoints were stratified by study type, length of follow-up, and type of DES.Results: We pooled 12 studies involving 3182 patients. Trial heterogeneity was a minor issue. TVF (OR: 0.35;CI: 0.24–0.51), MACE (OR: 0.36; CI: 0.29–0.45), binary restenosis (OR: 0.15; CI: 0.12–0.20) and late lumen loss(MD:−0.46; SD:−0.55 to−0.38) all significantly improvedwith DES treatment; ST (OR: 0.63; CI: 0.34–1.17)was not statistically different between studies.Conclusions: DES are superior to BMS in terms of their efficacy in managing small coronary arteries(diameterb3 mm), and at least equivalent in terms of safety. The use of DES should be considered the treatmentof choice in this setting.© 2011 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Percutaneous coronary interventions (PCI) involving small coro-nary vessels represent a true challenge in modern interventionalcardiology because of the increased risk of restenosis and adverseoutcomes [1]; furthermore, a small vessel does not always meanlimited myocardial ischemia and so the percutaneous treatment ofsmall coronary branches (i.e. those with a diameter of b3 mm) oftenhas a considerable impact on future clinical events. Stents arecurrently the mainstay of such treatment, but the rate of adverse
, Fondazione IRCCS Ca' Granda20122 Milano, Italy. Tel.: +39
Ltd. All rights reserved.
events is still high after the use of bare metal stents (BMS) [2–5] and,although drug eluting stents (DES) are nowwidely used to treat smallcoronary lesions, conflicting or inconclusive data have come fromrandomised clinical trials and registries because of the supposedlyhigher risk of stent thrombosis (ST) and even higher restenosis rate[6,7]. In the absence of a systematic overview of clinical and angio-graphic outcomes that would providemore robust evidence, wemadethis meta-analysis of the available trials and registries directlycomparing the two types of stent.
2. Methods
2.1. Study selection strategy
The eligible studies included randomised controlled clinical trials (RCT) [8–10],subgroups from RCT and observational studies [11–20] of PCIs using a DES or BMS totreat small coronary artery disease, provided that they had a follow-up of at least sixmonths. The target vessel had to have a diameter b3 mm with a clinical indication to

Table 1Studies included in the meta-analysis with main characteristics.
Study author Study name Design Year Drug of DES Patients, n° Median follow up, days
Schampaert, E C-SIRIUS RCT 2004 Sirolimus 100 270Schofer, J E-SIRIUS RCT 2003 Sirolimus 352 270Ardissino, D SES-SMART RCT 2004 Sirolimus 257 270Pfisterer, M BASKET RCT subgroup 2009 Sirolimus, paclitaxel 268 1080Moses, J SIRIUS RCT subgroup 2003 Sirolimus 673 240Grube, E TAXUS VI RCT subgroup 2007 Paclitaxel 123 720Jimenez-Quevedo, P DIABETES I, II Observational 2006 Sirolimus 85 360Tsuchiya, Y FUTURE I, II Observational 2006 Everolimus 37 180Stone, GW TAXUS V RCT subgroup 2005 Paclitaxel 203 270Turco, MA TAXUS ATLAS RCT subgroup 2007 Paclitaxel 416 270Meier, B SVELTE Observational 2006 Sirolimus 424 240Umeda, H – Observational 2009 Sirolimus 244 360
DES = drug eluting stent; n° = number; RCT = randomised controlled trial.
74 B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82
PCI. All eligible studies had to contain both a DES and a BMS group. The main exclusioncriteria were: 1) duplicate publications; 2) ongoing studies; 3) studies with a follow-upother than that specified in the study protocol; 4) studies with unretrievable or uncleardata; and 5) studies lacking a control group.
Two trained investigators (B.C. and A.B.) used both sensitive and specific strategiesto make independent searches of PubMed, Central, mRCT, BioMedCentral, clinical-trials.gov, Cardiosource, ISI Web of Science, and the annual international meetings ofthe major cardiology associations (the European Society of Cardiology, the AmericanHeart Association, the American College of Cardiology, the Cardiovascular ResearchFoundation, and the European Association of Percutaneous Cardiovascular Interven-tions), after which international experts were queried for additional trials results. Allfirst authors of retrieved articles were sent an email to confirm the published data, andobtain further information regarding eventual longer follow-up.
The searches were updated to the end of January 2010, and the search keywords were “small vessel”, “PCI”, “stent”, “BMS”, “DES”, “randomized”, and “rando-mised”. Selected papers were screened at title and abstract level and then, if consideredsuitable, the complete manuscripts were checked for compliance with the inclusioncriteria.
Study quality was evaluated using the established methods of the CochraneCollaboration, with separate estimates of the risk of selection, performance, detectionand attrition bias, or allocation concealment [21].
2.2. Study endpoints
The primary study endpoint was the occurrence of target vessel failure (TVF),defined target vessel revascularisation (TVR), or any death or myocardial infarction(MI) that could not be attributed to a vessel other than the target vessel by the end ofthe longest available study follow-up period.
The secondary endpoints were:
1) the occurrence of major adverse cardiovascular events (MACE), defined as theoccurrence of any one of death, MI or TVR;
2) the occurrence of any of the above as single events;3) the occurrence of definite or probable ST, following the ARC definition [22];4) late lumen loss (LLL) at angiographic follow-up;5) binary restenosis (defined as ≥50% in-stent restenosis) at angiographic follow-up.
Table 2Clinical data of studies included in the meta-analysis.
Study author Age, yrs Male, % Diabetes mellitus, % S
Schampaert, E 60.5±9.8 69 24 1Schofer, J 62.3±10.9 71 23 6Ardissino, D 63.5±11.4 73 23 4Pfisterer, M 64±11 79 19 4Moses, J N/A N/A N/A NGrube, E 62.7±9.8 76 20 5Jimenez-Quevedo, P 66.7±9 59 100 NTsuchiya, Y 66.2 68 22 8Stone, GW N/A N/A 41 NTurco, MA 63.6±11 59 37 NMeier, B 62.5±1.1 68 29 NUmeda, H 66.6±9.5 74 32 N
N/A = not available; UA = unstable angina; yrs = years.
MI was defined as any new chest pain associated with new ECG changes and anincrease in the levels of the cardiac biomarkers of necrosis (depending on the criteria ofeach study).
2.3. Meta-analyses
The meta-analyses were based on cumulative data from the time of stentimplantation. The between-group effect of treatment in each study was measured asthe odds ratio (OR) with 95% confidence interval (95% CI) for binary variables, and asthe mean difference (MD) with standard deviation (SD) for continuous variables. Asingle time point estimate for each study endpoint was chosen, assuming a constantabsolute DES vs. BMS risk reduction throughout the follow-up period. Mantel–Haenszel(M–H) of inverse-variance weighted methods were applied to fixed-effect models, andDerSimonian and Laird methods to random-effect models [23,24]. Statistical hetero-geneity was assessed using Cochrane Q via aχ2 test, and was quantified using the I2 test[25–27].
In the case of heterogeneity between studies, stratified analyses of the clinicaland angiographic endpoints were made by grouping the studies on the basis ofcharacteristics selected a priori as possible modifiers (type of study, length of follow-up, type of DES).
The studieswith no events in either the intervention or control armswere excluded;if no events were recorded in only one of the arms, 0.5 was added to the cell counts.
Systematic bias was evaluated using Egger's funnel plot and correspondentasymmetry test [26].
All of the analyses were made using Stata, version 11.0 [28].
3. Results
A total of 72 citations were retrieved from the searches, a numberof which were excluded at title/abstract level because they were notpertinent or provided insufficient clinical data on baseline character-istics or it was impossible to determine the study endpoints. The 12finally selected studies (involving a total of 3182 patients) provided
table angina, % Myocardial infarction, % Suggested duration of dualantiplatelet treatment, months
2 37 27 0 25 45 (with UA) 22 21 6/A N/A 37 0 6/A N/A 26 0 2/A N/A 6/A N/A 6/A 0 2/A 17 3

Table 3Angiographic data of studies included in the meta-analysis.
Study author BaselineRVD, mm
Lesion lengthallowed, mm
RVD DES group,mm
RVD BMS group,mm
In-segment LLL,DES groupangio. FUP, mm
Binary restenosis,DES groupangio. FUP, mm
In-segment LLL,BMS groupangio. FUP, mm
Binary restenosis,BMS groupangio. FUP, mm
ACC/AHAlesion class.B2–C, %
Schampaert, E b3 15–32 2.65±0.30 2.62±0.35 0.12±0.35 2.3 0.79±0.74 52.3 59Schofer, J b3 15–32 2.60±0.37 2.51±0.37 0.19±0.38 5.9 0.8±0.57 42.3 N/AArdissino, D ≤2.75 ≤33 2.2±0.28 2.2±0.28 0.16±0.46 9.8 0.69±0.61 53.1 29Pfisterer, M b3 N/A N/A N/A N/A N/A N/A N/A N/AMoses, J ≤2.5 ≤20 2.1±0.30 N/A 0.23±0.43 16.9 0.78±0.56 42.7 N/AGrube, E ≤2.5 N/A N/A N/A N/A 10.2 N/A 38.5 N/AJimenez-Quevedo, P ≤2.75 N/A 1.9±0.30 1.9±0.2 −0.03±0.3 9.1 0.44±0.5 39.1 82Tsuchiya, Y ≤2.75 N/A 2.49±0.20 2.51±0.17 0.12±0.36 8.3 0.51±0.46 36.8 37Stone, GW N/A N/A 2.07±0.31 2.10±0.33 0.36±0.53 N/A 0.61±0.59 N/A N/ATurco, MA ≤2.5 10–28 2.2±0.34 2.02±0.30 0.16±0.40 13 0.55±0.55 38.1 76Meier, B ≤2.75 15–30 2.36±0.01 2.42±0.01 0.20±0.06 6.3 0.76±0.05 39 N/AUmeda, H ≤2.5 N/A 2.18±0.25 2.19±0.23 0.21±0.41 8.6 0.48±0.63 34.4 79
ACC/AHA lesion class. = American College of Cardiology/American Heart Association lesion classification; angio. FUP= angiographic follow up; BMS= baremetal stent; DES=drugeluting stent; LLL = late lumen loss; N/A = not available; RVD = reference vessel diameter.
75B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82
enough details concerning the primary and at least four of the fivesecondary endpoints; however, incomplete data regarding otherevents was not so infrequent. The three RCTs had a prespecifiedcontrol angiography during follow up.
Table 1 shows the design and year of publication of the selectedstudies, together with the type of stent used, the number of patients,and the length of follow-up.
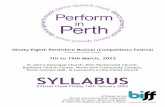
Fig. 1. Forest plot showing the individual and pooled risks of TVF using DES or BMS (OR and 9OR = odds ratio; CI = confidence interval.
3.1. Baseline and procedural data
Table 2 shows the main clinical characteristics of the analysedstudies, all but one of which used a sirolimus- or paclitaxel-elutingstent; unfortunately, there was not enough data comparing BMS withnewer DES eluting zotarolimus, everolimus or biolimus A9. The meanreference vessel diameter was 2.22±0.27 mm in the DES group, and
5% CI). TVF = target vessel failure. DES= drug eluting stents; BMS= bare metal stent;

Fig. 2. Funnel plot of TVF. TVF = target vessel failure.
76 B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82
2.27±0.25 mm in the BMS group (p=0.99). Table 3 shows the mainangiographic data.
3.2. Clinical outcomes
Mean follow-up of selected studies was 377 days, 273 excludingthe two studies with longer follow-up.
Fig. 3. Forest plot showing the individual and pooled risks of MACE when using DES or BMstents; BMS = bare metal stent; OR = odds ratio; CI = confidence interval.
TVF, the primary study endpoint, was available for 10 studiesreporting data both on TVR and ST. Study primary endpoint wassignificantly less frequent in the DES group: 132/1179 patients(11.2%) vs. 266/1215 (21.9%). The OR was 0.37 (95% CI: 0.29–0.47).On the basis of the results of homogeneity test, an M–H method wasused (Fig. 1); the funnel-plot for this endpoint showed no evidence ofbias (Egger's test for small study effects) (Fig. 2).
The frequency of MACE also differed significantly between the twogroups, with one event occurring in 12.5% of the patients receiving aDES and 26.5% of those receiving a BMS (OR 0.36, 95% CI: 0.29–0.45).On the basis of the results of homogeneity test, an M–H method wasused (Fig. 3).
There was no significant between-group difference in mortality(2.6% among the DES-treated and 1.6% among the BMS-treatedpatients). The OR was 1.27 (95% CI: 0.70–2.29). The study ofSchampaert et al. was excluded from this analysis because it did notreport any death in either treatment arm. On the basis of the results ofhomogeneity test, an M–H method was used (Fig. 4).
MI rates were not significantly different between the groups, being3% among the DES-treated patients and 3.4% among those whoreceived a BMS (OR 0.88, 95% CI: 0.54–1.45). However, there was atrend towards more frequent MIs in the BMS group, thus raising aconcern that the trend towards increased mortality in the DES groupshould be attributed to causes other than MI. On the basis of theresults of homogeneity test, an M–H method was used (Fig. 5).
The rates of TVR were also significantly different between thegroups: 83/1057 patients in the DES group (7.9%) and 259/1166 inthe BMS group (22.2%) underwent revascularisation, thus confirming
S (OR and 95% CI). MACE = major adverse cardiovascular events; DES = drug eluting

Fig. 4. Forest plot showing the individual and pooled risks of mortality when using DES or BMS (OR and 95% CI). DES= drug eluting stents; BMS= baremetal stent; OR= odds ratio;CI = confidence interval.
77B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82
the expected better performance of DES (OR 0.28, 95% CI: 0.21–0.37).On the basis of the results of homogeneity test, both M–H and D–Lmethods were used. TVR rates were also analysed by type of DES: inthe comparison of sirolimus-eluting stents and BMS, the figures were5.6% and 22.8%; in the comparison of paclitaxel-eluting stents andBMS, they were 11.1% and 20.8%. These data show a trend towards aneffect that was slightly in favour of sirolimus stents over paclitaxelstents, but the absence of any direct comparison does not allow anyfurther conclusion (Fig. 6).
There was no significant between-group difference in ST, whichoccurred in 23/1088 DES-treated patients (2.1%) and 21/870 patientsreceiving a BMS (2.4%) (OR 0.63, 95% CI: 0.34–1.17). The study ofTsuchiya et al. was excluded from the analysis because it did notreport any ST event in either arm. On the basis of the results ofhomogeneity test, an M–H method was used (Fig. 7).
3.3. Angiographic outcomes
Weobserved a significant difference in the rates of binary restenosis,which occurred in 87/898 patients treatedwithDES (9.7%) and 363/986treated with BMS (36.8%). The OR was 0.16 (95% CI: 0.12–0.20). Onthe basis of the results of a homogeneity test, both M–H and D–Lmodels were used (Fig. 8).
LLL measure was 0.17±0.24 mm in patients treated with DESand 0.64±0.53 mm in patients treated with BMS. The MDwas−0.46
(SD: −0.55 to −0.38), showing a significant difference in favour ofthe DES group. On the basis of the results of homogeneity test, a D–L0.17±0.24 mm was used (Fig. 9).
All of the study endpoints were also analysed after being stratifiedby the duration of follow-up (≤360 days or N360 days), the type ofDES and the type of study (randomised or not). Treatment effect wasnot dependent on the nature of the study because there were nobetween-group differences; to note, only two studies had a follow-upof more than one year, and only three were randomised.
4. Discussion
This systematic meta-analysis is based on the pooling of allavailable literature data regarding PCI with DES vs. BMS in the settingof small vessel disease, consisting of three RCTs and nine studiesincluding subgroups of RCT and non-randomised studies, andinvolving a total of 3182 patients.
The use of BMS in the management of small coronary vesseldisease has not substantially improved the results obtained bymeansof plain balloon angioplasty [3–5,29] possibly because the patientsare at higher risk and the narrower vessels cannot accommodateeven minimal intimal hyperplasia. The largest meta-analysis com-paring clinical outcomes in small vessels after balloon angioplasty orBMS implantation concluded that stenting leads to better angio-graphic results, but that plain balloon angioplasty with provisional

Fig. 5. Forest plot showing the individual and pooled risks of MI when using DES or BMS (OR and 95% CI). MI =myocardial infarction; DES= drug eluting stents; BMS= bare metalstent; OR = odds ratio; CI = confidence interval.
78 B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82
stenting is sufficient in the vast majority of cases [2]. This conclusionwas reached on the basis of the equivalence of simple balloonangioplasty and BMS in achieving an optimal acute angiographicresult (afinal diameter stenosis of b20%) and suggested that stent useshould be limited to selected cases [30]. The use of DES thereforeseems to be particularly beneficial in this subset because it has beenfound that the need for further revascularisation due to restenosescaused by in-stent hyperplasia can be reduced bymeans of local drugelution [31,32]. Furthermore, the recently published results of thePICCOLETO trial have shown that, in comparison with a paclitaxel-coated balloon, the use of a paclitaxel-eluting stent improves angio-graphic restenosis and TVR rates in small coronary vessels, thusdampening the enthusiasm aroused by the possibility of avoidingstent implantation [33].
The main finding of our meta-analysis is that treatment withDES is associated with improved TVF rates (the primary studyendpoint), with no significant difference between randomised andnon-randomised clinical trials. The use of TVF as a primary end-point is important because it considers clinical outcomes in termsof both efficacy (reflected by TVR) and safety (reflected by ST andtarget vessel-related cardiac death), and has recently beenrecommended by the FDA as a primary endpoint for clinical trialsof DES. Our findings not only show that ST is not an issue whenusing a DES to treat small vessel disease (at least not in themedium term), which actually leads to an albeit non-significanttrend towards fewer thromboses, with a risk reduction around35%.
It is difficult to explain this finding because of the variousmethodsused in the analysed studies, but we believe that it is mainly due tothe prolonged dual antiplatelet treatment associated with DESplacement. It is worth noting that the BASKET trial (the only studywith a follow-up of more than 360 days) showed a non-significanttrend towards lower TVF rates in the DES group (OR 0.67; 95% CI0.38–1.18) although, given the small study population, this superi-ority should be limited to one year until further trials with a longerfollow-up period have been carried out.
The question of ST has been widely studied in relation to the useof DES in larger diameter vessels, but not yet sufficiently analysedin small coronary arteries. The risk of ST does not seem to depend onvessel calibre, but is increased in longer lesions and in patientswith diabetes mellitus, both of which are typical features associatedwith small vessel disease [34]. However, our study does not considerinformation regarding the longer-time occurrence of ST after stop-ping dual antiplatelet regimen.
It is worth noting that, as expected, MACE and TVR rates were alsolower in the patients receiving a DES. As both binary restenosisand LLL rates were also significantly better, our findings confirmthe superiority of DES in reducing small coronary neointimal pro-liferation in both randomised and non-randomised studies. TheSD observed in the SVELTE trial was extraordinarily small, butthis does not change the overall superiority of DES regarding thisendpoint.
Unlike a previous meta-analysis of DES vs. BMS, we did not findany evidence that BMS increases the incidence of MI [35] possibly

Fig. 6. Forest plot showing the individual and pooled risks of TVR when using DES or BMS (OR and 95% CI). TVR= target vessel revascularisation; DES= drug eluting stents; BMS=bare metal stent; OR = odds ratio; CI = confidence interval.
79B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82
because the highly selected population of our meta-analysis was toosmall to detect a clinically relevant difference. However, our finding isconsistent with those of many randomised clinical trials.
This meta-analysis provides robust evidence supporting the use ofDES in the major part of patients undergoing PCI of a small coronaryvessel, as shown by the pooling of both RCTs and all-comers registries.
Our meta-analysis has the same limitations as other similaranalyses [36,37]. Each of the analysed studies has its own peculiar-ities and the pooling of various data may confound the overalleffect of one or the other strategy. However, our strict selectioncriteria limited the number of studies considered and thus reducedthe possibility of statistical inconsistency. The decision of addingrandomised controlled trials to not randomised studies has beenwelldiscussed with the statisticians; we decided to include differentkinds of studies to reach a statistical consistency regarding studyprimary endpoint. Another limitation of this study, is the lack oflong clinical follow up, that would provide more consistent dataregarding the safety offirst-generationDES:we are unaware of eitherrandomised controlled trials or registries that supply such data.However, as already stated, this meta-analysis collected all availableliterature comparing a BMS and DES strategy for the treatment ofsmall coronary arteries at the longest available follow up; unfortu-nately available studies almost exclusively tested first generationDES.
In conclusion, the treatment of small coronary vessels with DES issafe and effective in the medium term, regardless of the eluted drug,and the use of DES should be considered the treatment of choice inthis particular restenosis-prone clinical setting. It would now beuseful to undertake a large-scale RCT with long follow-up in order to
verify whether these results are maintained for more than one year;it will also be of crucial importance to test newer DES in this subset.
Acknowledgements
We thank Dr Marco Centola, MD for his precious help in retrievingsome of the papers that entered final analysis; we also thank Dr RitaDe Carlo (Boston Scientific Corp.) and Eng Francesco Arecchi (CordisCorp.) for their assistance in finding some key data.
The authors of this manuscript have certified that they complywith the Principles of Ethical Publishing in the International Journal ofCardiology [38].
References
[1] Elezi S, Kastrati A, Neumann FJ, et al. Vessel size and long-term outcome aftercoronary stent placement. Circulation 1998;98:1875–80.
[2] Agostoni P, Biondi-Zoccai GG, Gasparini GL, et al. Is bare-metal stenting superior toballoon angioplasty for small vessel coronary artery disease? Evidence from ameta-analysis of randomized trials. Eur Heart J 2005;26:881–9.
[3] Briguori C, Nishida T, Adamian M, et al. Coronary stenting versus balloonangioplasty in small coronary artery with complex lesions. Catheter CardiovascInterv 2000;50:390–7.
[4] Doucet S, Schalij MJ, Vrolix MC, et al. Stent placement to prevent restenosis afterangioplasty in small coronary arteries. Circulation 2001;104:2029–33.
[5] Koning R, Eltchaninoff H, Commeau P, et al. Stent placement compared withballoon angioplasty for small coronary arteries: in-hospital and 6-month clinicaland angiographic results. Circulation 2001;104:1604–8.
[6] Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronary stentthrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinicalpractice: data from a large two-institutional cohort study. Lancet 2007;369:667–78.

Fig. 7. Forest plot showing the individual and pooled risks of ST when using DES or BMS (OR and 95% CI). ST= stent thrombosis; DES= drug eluting stents; BMS= bare metal stent;OR = odds ratio; CI = confidence interval.
80 B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82
[7] Lagerqvist B, James SK, Stenestrand U, et al. Long-term outcomeswith drug-elutingstents versus bare-metal stents in Sweden. N Engl J Med 2007;356:1009–19.
[8] Schampaert E, Cohen EA, Schluter M, et al. The Canadian study of the sirolimus-eluting stent in the treatment of patients with long de novo lesions in small nativecoronary arteries (C-SIRIUS). J Am Coll Cardiol 2004;43:1110–5.
[9] Schofer J, Schluter M, Gershlick AH, et al. Sirolimus-eluting stents for treatment ofpatients with long atherosclerotic lesions in small coronary arteries: double-blind,randomised controlled trial (E-SIRIUS). Lancet 2003;362:1093–9.
[10] Ardissino D, Cavallini C, Bramucci E, et al. Sirolimus-eluting vs uncoated stents forprevention of restenosis in small coronary arteries: a randomized trial. JAMA2004;292:2727–34.
[11] Meier B, Sousa E, Guagliumi G, et al. Sirolimus-eluting coronary stents in smallvessels. Am Heart J 2006;151:1019 e1-7.
[12] Godino C, Furuichi S, Latib A, et al. Clinical and angiographic follow-up of smallvessel lesions treated with paclitaxel-eluting stents (from the TRUE Registry). AmJ Cardiol 2008;102:1002–8.
[13] Umeda H, Iwase M, Gochi T, et al. Safety and efficacy of 2.5-mm sirolimus-elutingstent implantation at lower deployment pressures in very small vessels(b2.5 mm). Coron Artery Dis 2009;20:163–8.
[14] Pfisterer M, Brunner-La Rocca HP, Rickenbacher P, et al. Long-term benefit-riskbalance of drug-eluting vs. bare-metal stents in daily practice: does stent diametermatter? Three-year follow-up of BASKET. Eur Heart J 2009;30:16–24.
[15] Jimenez-Quevedo P, Sabate M, Angiolillo DJ, et al. Efficacy of sirolimus-elutingstent implantation in diabetic patients with very small vessels (b or =2.25 mm).Insights from the DIABETES trial. Rev Esp Cardiol 2006;59:1000–7.
[16] Tsuchiya Y, Lansky AJ, Costa RA, et al. Effect of everolimus-eluting stents indifferent vessel sizes (from the pooled FUTURE I and II trials). Am J Cardiol2006;98:464–9.
[17] Stone GW, Ellis SG, Cannon L, et al. Comparison of a polymer-based paclitaxel-eluting stent with a bare metal stent in patients with complex coronary arterydisease: a randomized controlled trial. JAMA 2005;294:1215–23.
[18] Turco MA, Ormiston JA, Popma JJ, et al. Reduced risk of restenosis in small vesselsand reduced risk of myocardial infarction in long lesions with the new thin-strutTAXUS Liberte stent: 1-year results from the TAXUS ATLAS program. JACCCardiovasc Interv 2008;1:699–709.
[19] Grube E, Dawkins K, Guagliumi G, et al. TAXUSVIfinal 5-year results: amulticentre,randomised trial comparing polymer-based moderate-release paclitaxel-elutingstent with a bare metal stent for treatment of long, complex coronary arterylesions. EuroIntervention 2009;4:572–7.
[20] Moses JW, Nikolsky E, Mehran R, et al. Safety and efficacy of the 2.25-mmsirolimus-eluting BxVelocity stent in the treatment of patientswith de novo nativecoronary artery lesions: the SIRIUS 2.25 trial. Am J Cardiol 2006;98:1455–60.
[21] The Cochrane collaboration handbook for systematic reviews of interventions.Available at:http://wwwcochraneorg/resources/handbook/2010.
[22] Mauri L, Hsieh WH, Massaro JM, et al. Stent thrombosis in randomized clinicaltrials of drug-eluting stents. N Engl J Med 2007;356:1020–9.
[23] DerSimonian R, Kacker R. Random-effects model for meta-analysis of clinicaltrials: an update. Contemp Clin Trials 2007;28:105–14.
[24] DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177–88.
[25] Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60.
[26] Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by asimple, graphical test. BMJ 1997;315:629–34.
[27] Egger M, Smith GD, Phillips AN. Meta-analysis: principles and procedures. BMJ1997;315:1533–7.
[28] StataCorp. Stata: Release 11. Statistical Software. College Station, TX: StataCorp LP;2009.
[29] Kastrati A, Mehilli J, Dirschinger J, et al. Intracoronary stenting and angiographicresults: strut thickness effect on restenosis outcome (ISAR-STEREO) trial.Circulation 2001;103:2816–21.
[30] Akiyama T, Moussa I, Reimers B, et al. Angiographic and clinical outcome followingcoronary stenting of small vessels: a comparison with coronary stenting of largevessels. J Am Coll Cardiol 1998;32:1610–8.
[31] Schwartz RS, Chronos NA, Virmani R. Preclinical restenosis models and drug-eluting stents: still important, still much to learn. J Am Coll Cardiol 2004;44:1373–85.
[32] Togni M, Eber S, Widmer J, et al. Impact of vessel size on outcome afterimplantation of sirolimus-eluting and paclitaxel-eluting stents: a subgroupanalysis of the SIRTAX trial. J Am Coll Cardiol 2007;50:1123–31.

Fig. 8. Forest plot showing the individual and pooled risks of restenosis when using DES or BMS (OR and 95% CI). DES = drug eluting stents; BMS = bare metal stent; OR = oddsratio; CI = confidence interval.
81B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82
[33] Cortese B, Micheli A, Picchi A, Coppolaro A, Bandinelli L, Severi S, Limbruno U, et al.Paclitaxel-coated balloon versus drug-eluting stent during PCI of small coronaryvessels, a prospective randomized clinical trial. The PICCOLETO Study. Heart2010;96(16):1291–6.
[34] Iakovou I, SchmidtT, BonizzoniE, et al. Incidence,predictors, andoutcomeof thrombosisafter successful implantation of drug-eluting stents. JAMA 2005;293:2126–30.
[35] Kirtane AJ, Gupta A, Iyengar S, et al. Safety and efficacy of drug-eluting and baremetal stents: comprehensive meta-analysis of randomized trials and observa-tional studies. Circulation 2009;119:3198–206.
[36] Biondi-Zoccai GG, Agostoni P, Abbate A. Parallel hierarchy of scientific studies incardiovascular medicine. Ital Heart J 2003;4:819–20.
[37] Clarke O. The Cochrane Library. Cochrane reviewers' handbook, 420; 2003.[38] Shewan LG, Coats AJ. Ethics in the authorship and publishing of scientific articles.
Int J Cardiol 2010;144:1–2.

Fig. 9. Forest plot showing the individual and pooled risks of LLL when using DES or BMS (OR and 95% CI). LLL = late lumen loss; DES= drug eluting stents; BMS= bare metal stent;OR = odds ratio; CI = confidence interval.
82 B. Cortese et al. / International Journal of Cardiology 161 (2012) 73–82