Angiographic and clinical outcome of invasively managed patients with thrombosed coronary bare metal...
11
..................................................................................................................................................................................... ..................................................................................................................................................................................... CLINICAL RESEARCH Interventional cardiology Angiographic and clinical outcome of invasively managed patients with thrombosed coronary bare metal or drug-eluting stents: the OPTIMIST study Francesco Burzotta 1 * , Antonio Parma 2 , Christian Pristipino 3 , Alessandro Manzoli 4 , Flavia Belloni 5 , Gennaro Sardella 6 , Stefano Rigattieri 7 , Alessandro Danesi 8 , Pietro Mazzarotto 9 , Francesco Summaria 10 , Enrico Romagnoli 1 , Francesco Prati 4 , Carlo Trani 1 , and Filippo Crea 1 1 Institute of Cardiology, Catholic University of the Sacred Heart, Rome, Italy; 2 U.O. of Interventional Cardiology, A.O. San Camillo-Forlanini Hospital, Rome, Italy; 3 Department of Cardiology, San Filippo Neri Hospital, Rome, Italy; 4 Catheterization Laboratory, S. Giovanni Hospital, Rome, Italy; 5 Department of Cardiology, San Pietro FBF Hospital, Rome, Italy; 6 Department of Cardiovascular and Respiratory Sciences, Policlinico Umberto I, ‘La Sapienza’ University, Rome, Italy; 7 UOSD Emodinamica e Cardiologia Interventistica, ‘Sandro Pertini’ Hospital, Rome, Italy; 8 U.O.C. of Cardiology, S. Spirito Hospital, Rome, Italy; 9 U.O. Cardiologia Invasiva e Interventistica Endovascolare, S. Carlo—I.D.I. Hospital, Rome, Italy; and 10 Catheterization Laboratory, Division of Cardiology, Policlinico Casilino Hospital, Rome, Italy Received 4 January 2008; revised 1 September 2008; accepted 9 October 2008; online publish-ahead-of-print 5 November 2008 Aims Stent thrombosis (ST) is a major complication of percutaneous coronary interventions (PCIs). An invasive manage- ment by re-PCI is the commonly adopted treatment for ST, but data on outcome are limited. Methods and results We performed a 2-year multicentre registry enrolling consecutive patients with angiographically confirmed ST under- going PCI. The primary angiographic endpoint was optimal angiographic reperfusion (TIMI 3 þ blush grade 2 or 3). The primary clinical endpoints were death and major adverse coronary and cerebrovascular events (MACCEs) at 6 months. A total of 110 patients underwent 117 urgent PCI during the study. Patients with drug-eluting stent (DES) thrombosis, compared with those with bare metal stent (BMS) thrombosis, exhibited a higher rate of late or very late presentation and of anti-platelet therapy withdrawal. Optimal angiographic reperfusion was obtained in 64% of the patients. Death and MACCE rates at 6 months were 17 and 30%, respectively. Clinical outcome was similar for BMS and DES thrombosis. Very late ST, implantation of stent during PCI for ST, and failure to achieve optimal angiographic reperfusion were the independent predictors of 6-month mortality. Conclusion DES and BMS thromboses have different clinical features, but a similar poor outcome. Indeed, PCI for ST is associated with a low rate of reperfusion and to a high rate of death and MACCE, calling for action in order to prevent its occur- rence and to improve its management. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords PCI † Stent † Stent thrombosis Introduction Stent thrombosis (ST) is a major complication limiting the clinical efficacy of percutaneous coronary interventions (PCIs). After stent implantation, ST is reported to happen with an early inci- dence ranging from 0.5 to 2.0%. 1–5 As the number of stent-based PCIs is expanding worldwide, the absolute number of patients experiencing ST is expected to increase. Moreover, the introduc- tion of drug-eluting stents (DESs) has been reported to be associ- ated with a 0.6% rate of late and very late ST per year, 6 so that ST risk might be extended over time and increased compared with bare metal stents (BMSs). 7–10 * Corresponding author. Tel: þ39 0349 4295290, Fax: þ39 06 3055535, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected]. European Heart Journal (2008) 29, 3011–3021 doi:10.1093/eurheartj/ehn479 by guest on June 28, 2016 http://eurheartj.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Angiographic and clinical outcome of invasively managed patients with thrombosed coronary bare metal...

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CLINICAL RESEARCHInterventional cardiology
Angiographic and clinical outcome of invasivelymanaged patients with thrombosed coronarybare metal or drug-eluting stents: theOPTIMIST studyFrancesco Burzotta1*, Antonio Parma2, Christian Pristipino3, Alessandro Manzoli4,Flavia Belloni5, Gennaro Sardella6, Stefano Rigattieri7, Alessandro Danesi8,Pietro Mazzarotto9, Francesco Summaria10, Enrico Romagnoli1,Francesco Prati4, Carlo Trani1, and Filippo Crea1
1Institute of Cardiology, Catholic University of the Sacred Heart, Rome, Italy; 2U.O. of Interventional Cardiology, A.O. San Camillo-Forlanini Hospital, Rome, Italy; 3Department ofCardiology, San Filippo Neri Hospital, Rome, Italy; 4Catheterization Laboratory, S. Giovanni Hospital, Rome, Italy; 5Department of Cardiology, San Pietro FBF Hospital, Rome, Italy;6Department of Cardiovascular and Respiratory Sciences, Policlinico Umberto I, ‘La Sapienza’ University, Rome, Italy; 7UOSD Emodinamica e Cardiologia Interventistica, ‘SandroPertini’ Hospital, Rome, Italy; 8U.O.C. of Cardiology, S. Spirito Hospital, Rome, Italy; 9U.O. Cardiologia Invasiva e Interventistica Endovascolare, S. Carlo—I.D.I. Hospital, Rome, Italy;and 10Catheterization Laboratory, Division of Cardiology, Policlinico Casilino Hospital, Rome, Italy
Received 4 January 2008; revised 1 September 2008; accepted 9 October 2008; online publish-ahead-of-print 5 November 2008
Aims Stent thrombosis (ST) is a major complication of percutaneous coronary interventions (PCIs). An invasive manage-ment by re-PCI is the commonly adopted treatment for ST, but data on outcome are limited.
Methodsand results
We performed a 2-year multicentre registry enrolling consecutive patients with angiographically confirmed ST under-going PCI. The primary angiographic endpoint was optimal angiographic reperfusion (TIMI 3 þ blush grade 2 or 3). Theprimary clinical endpoints were death and major adverse coronary and cerebrovascular events (MACCEs) at 6months. A total of 110 patients underwent 117 urgent PCI during the study. Patients with drug-eluting stent(DES) thrombosis, compared with those with bare metal stent (BMS) thrombosis, exhibited a higher rate of lateor very late presentation and of anti-platelet therapy withdrawal. Optimal angiographic reperfusion was obtainedin 64% of the patients. Death and MACCE rates at 6 months were 17 and 30%, respectively. Clinical outcomewas similar for BMS and DES thrombosis. Very late ST, implantation of stent during PCI for ST, and failure toachieve optimal angiographic reperfusion were the independent predictors of 6-month mortality.
Conclusion DES and BMS thromboses have different clinical features, but a similar poor outcome. Indeed, PCI for ST is associatedwith a low rate of reperfusion and to a high rate of death and MACCE, calling for action in order to prevent its occur-rence and to improve its management.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords PCI † Stent † Stent thrombosis
IntroductionStent thrombosis (ST) is a major complication limiting the clinicalefficacy of percutaneous coronary interventions (PCIs). Afterstent implantation, ST is reported to happen with an early inci-dence ranging from 0.5 to 2.0%.1– 5 As the number of stent-based
PCIs is expanding worldwide, the absolute number of patientsexperiencing ST is expected to increase. Moreover, the introduc-tion of drug-eluting stents (DESs) has been reported to be associ-ated with a 0.6% rate of late and very late ST per year,6 so that STrisk might be extended over time and increased compared withbare metal stents (BMSs).7 –10
* Corresponding author. Tel: þ39 0349 4295290, Fax: þ39 06 3055535, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected].
European Heart Journal (2008) 29, 3011–3021doi:10.1093/eurheartj/ehn479
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

An early invasive strategy by urgent re-PCI represents the mostadopted strategy to manage patients presenting with ST. However,despite its evident clinical relevance, available data on ST derivefrom substudies3 or single-centre experiences.11–14
Thus, we conceived a multicentre registry enrolling consecutivepatients with angiographically confirmed ST undergoing PCI aimedat providing an updated, detailed description of the angiographicand clinical outcome of patients with ST treated by PCI.15
Methods
Study designThe Outcome of PCI for Stent-Thrombosis Multicentre Study (OPTI-MIST) is a registry enrolling consecutive patients with ST treated byPCI. The study protocol has previously been published.15 Briefly, therecruiting period comprised a fixed 2-year time between 1 January2005 and 31 December 2006. The study protocol was conceived inOctober 2005, and prospective enrolment of patients started inJanuary 2006. Each centre, to be activated for the study, had towarrant (fully describing the search process as well as the character-istics of the internal database) ability to provide detailed clinical andprocedural data (including a copy of the cine films and the 6-monthoutcomes), regarding all patients with ST treated with PCI since thestart of the retrospective arm study period. Eleven centres, alllocated in the urban area of Rome and listed in the Appendixsection, met these requirements and entered the study.
The study protocol complied with the Declaration of Helsinki andwas approved by the Ethics Committee of the coordinating centre.Informed consent to both the PCI procedure and the clinical follow-uphas been obtained for each patient enrolled in the study.
Inclusion and exclusion criteriaIncluded patients, irrespective of type of stent previously implantedand date of its implantation, had to have angiographically confirmedST of a previously implanted stent associated with rest angina ornew ischaemic ECG changes or cardiac biomarker elevation andhave undergone an attempt of PCI on ST as target lesion withinhospitalization.
The exclusion criteria were surgical or medical management (i.e. noattempt of PCI) of ST and development of ST during stent implantation(i.e. intraprocedural ST).
Clinical data set and clinical outcomemeasuresA structured case report form has been created to collect the dataregarding the patient profile (including the presence of oncologicaland haematological diseases and timing for previous interruption ofantiplatelet drug therapy), the main characteristics of the procedurein which the stent was implanted (date, bifurcation involvement, andtype and number of the stent implanted), and the detailed descriptionof the index PCI (peri-intervention medical therapy, target lesion site,number of diseased vessels, presence of severe calcifications, stentunderexpansion, revascularization strategy including balloon dilation,additional stent implantation, and use of thrombectomy or distalfilter protection). The following ARC definitions16 of ST accordingto the time interval between implantation and thrombosis of thestent were adopted: ‘early’, 0–30 days; ‘late’, .30 days to 1 year;and ‘very late’, .1 year.
All major adverse coronary and cerebrovascular events (MACCEs)have been recorded at 30 days and at 6 months. MACCE comprised
death, myocardial infarction (MI), target vessel revascularization (byeither repeat PCI or coronary artery bypass graft surgery), and cer-ebrovascular accident. MI was defined as ischaemic symptoms and/orischaemic ECG changes þ elevation of creatine-kinase MB or troponinT or I levels above the normal laboratory values.17 Cerebrovascularaccident was defined as a specific neurological dysfunction with mor-phological substrate confirmed by computer tomography or nuclearmagnetic resonance imaging. The following ARC definitions16 of recur-rent ST during follow-up were adopted: ‘definite’, angiography- orautopsy-confirmed ST; ‘probable’, any unexplained death within first30 days or any MI in the territory of the stent and in the absence ofany other obvious cause; and ‘possible’, any unexplained death after30 days.
Angiographic analysesAll cine films of PCI on ST were sent to the coordinator centre, wherebaseline and final post-PCI views were selected and extracted. Then,these selected views only were sent to the core laboratory for centra-lized, blind analyses. This process was in the opinion of the OPTIMIST’ssteering committee the best way to warrant angiographic analyses fullyindependent of knowledge of PCI strategy and course. The validatedcore laboratory responsible for the angiographic analyses was theRome Heart Research, Rome, Italy. Coronary angiograms have beenanalysed before intervention and at the end of the procedure to assess:
† anterograde coronary flow according to standard Thrombolysis InMyocardial Infarction (TIMI) criteria;18
† occurrence of angiographic distal embolization defined as an occlu-sion with abrupt ‘cut-off’ appearance at angiography of a branch ofthe infarct-related artery distal to the culprit lesion;19
† corrected TIMI frame count (CTFC) according to Gibson et al.;20
† thrombus score (TS) according to the TIMI study group21 (0 ¼ noangiographic characteristics of thrombus are present; 1 ¼ possiblethrombus is present, with angiography characteristics such asreduced contrast density, haziness, irregular lesion contour, or asmooth convex ‘meniscus’ at the site of total occlusion suggestivebut not diagnostic of thrombus; 2 ¼ definite thrombus, with great-est dimensions �1/2 the vessel diameter; 3 ¼ definite thrombus,with greatest linear dimension .1/2 but ,2 vessel diameters;4 ¼ definite thrombus, with the largest dimension �2 vessel diam-eters; 5 ¼ total occlusion);
† myocardial blush grade (MBG) according to van’t Hof et al.;22
† quantitative coronary angiography analysis (CMS Medis ImagingSystem, Wallingford, CT, USA) of the target lesions before andafter PCI according to previously validated methods.23
Before starting the angiographic analyses, the operators of the corelaboratory assigned a quality score to each film, according to thechances to appropriately assess CTFC and MBG; films with insufficientscore were excluded from the MBG and CTFC analyses (see Burzottaet al.15 for scoring system details).
Primary endpointsThe pre-defined primary angiographic endpoint was the rate of‘optimal angiographic reperfusion’ defined as the combination ofTIMI 3 with MBG 2 or 3.24
The pre-defined primary clinical endpoints were death and MACCErate at 6 months.
Sources for assessment of numbers ofprocedures performed by enrolling centresThe total number of procedures with any stent implantation (DES orBMS) and the total number of urgent (primary or rescue) PCIs for
F. Burzotta et al.3012
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

ST-elevation acute MI (STEMI) performed by each centre during thestudy period were obtained from the official website of the ItalianSociety of Interventional Cardiology (SICI-GISE, www.gise.it), whichprospectively collects data from all Italian catheterization laboratoriesbelonging to the society. PCIs carried out in 2004 were used for thesample size calculation,15 whereas PCIs in 2005 and 2006 were usedfor the current analyses.
Statistical analysesThe sample size of the study has been calculated to enrol more than100 patients.15 In particular, we observed that the hospitals participat-ing in the study performed together about 6000 PCIs during 2004: thusit has been estimated that at least 12 000 PCIs have been performedduring the 2-year (2005–06) study period. Then, we anticipated a1.5% rate of ST and a rate of attempted PCI on ST of 60%, thus antici-pating the enrolment of 108 patients in the study. According to thestudy design, as a preliminary validation stage of the overall studycohort, baseline clinical (risk factors and clinical presentation) andangiographic characteristics (number of disease vessels, target vessel,and pre-intervention TIMI flow) of retrospectively enrolled patientswere planned to be compared with those of the prospectively enrolledpatients.15
Pre-intervention clinical, angiographic, and procedural character-istics, angiographic results, and clinical follow-up data are presentedfor the whole population and for subgroups of patients with BMSand DES thrombosis.
Continuous variables are presented as median and interquartileranges and compared by the Student’s t-test or Wilcoxon–Mann–Whitney test as appropriate. Categorical variables are summarized ascounts and percentages and compared using the x2 test or Fisher’sexact test when appropriate. The incidence of events over time wasstudied with the use of the Kaplan–Meier method and comparedwith log-rank tests.
Univariable and multivariable logistic regression analyses were usedto estimate the odds ratios (ORs) and the corresponding 95% confi-dence intervals (CIs). As anticipated in the study protocol,15 the base-line clinical and angiographic and procedural variables that affected theunivariable analysis (cut-off for entry 0.10) were included in the multi-variable models to assess independent predictors of the primary studyendpoints (failure to achieve optimal angiographic reperfusion,6-month death, and 6-month MACCE). The goodness-of-fit testing(Hosmer and Lemeshow x2) was used to assess how well the finalmodel was calibrated. The predictive value of the variables thatemerged from the stepwise analysis was confirmed in a multivariableanalysis model corrected for a series of factors that are known, on epi-demiological ground, to be relevant predictors of myocardial reperfu-sion (sex, age, diabetes mellitus, renal failure, STEMI at presentation,IIb/IIIa inhibitors administration, three-vessel disease, target vessel,TIMI flow 0–1, cardiogenic shock, thrombectomy, slow flow or tran-sient no-reflow, post-procedural thrombus-score .1, distal emboliza-tion, and failure to achieve optimal angiographic reperfusion) and ofclinical outcome (sex, age, diabetes mellitus, renal failure, STEMI atpresentation, very late ST, type of thrombosed stent, double simul-taneous ST in different vessels, severe calcification, IIb/IIIa inhibitorsadministration, three-vessel disease, target vessel, TIMI flow 0–1, car-diogenic shock, thrombectomy, stent implantation during PCI for ST,slow flow or transient no-reflow, post-procedural thrombus score.1, distal embolization, and failure to achieve optimal angiographicreperfusion).
A two tailed P-value less than 0.05 was established as the level ofstatistical significance for all tests. Analyses were carried out usingSPSS for Windows 12.0 (SPSS, Chicago, IL, USA).
Role of the funding sourceThere was no funding source for the present study.
Results
Study populationA total of 110 patients underwent PCI for ST in the 2-year pro-tocol period and constituted the study population. No significantdifferences in either clinical, angiographic, or procedural charac-teristic were observed between patients enrolled prospectively(n ¼ 58) or retrospectively (n ¼ 52), so that the study populationwas considered as a whole. The baseline clinical and angiographiccharacteristics of the study patients are reported in Table 1. Mostof the patients presented with STEMI (73%) and occluded (TIMI0–1) arteries before interventions (85%). High risk clinical fea-tures such as diabetes mellitus, renal failure, and cardiogenicshock were present in 30, 20, and 17% of the patients, respect-ively. Seven patients (6%) had a second episode of ST treatedby PCI during the study period (so that the number of PCIrequired for ST was 117 during the study) and three patients, pre-viously treated by multivessel stenting, presented with simul-taneous thrombosis of stents placed in two different vessels.The rate of IIb/IIIa inhibitor use was very high (71%), whereas aminority of patients (7%) were treated by thrombolytic drugs(in referring hospitals) before the rescue PCI in the enrollinghospitals.
Prevalence of percutaneous coronaryintervention for stent thrombosisDuring the study period, the OPTIMIST centres performed a totalof 12 280 PCIs with stent implantation: 7318 (60%) with at leastone DES implantation and the remaining 4962 (40%) with BMSimplantation. Among all stenting procedures, the observed rateof urgent procedures for ST was 0.95%. No significant differencewas observed between DES and BMS in the ratio betweennumber of PCI for ST and number of PCI with the correspondingtype of stent implantation: 0.85% (62 of 7318) for DES vs. 1.05%(52 of 4962) for BMS; P ¼ 0.24.
During the study period, 89 of 2484 primary or rescue PCIswere performed in patients with ST presenting with STEMI.Accordingly, ST accounted for 3.58% of the urgent PCI forSTEMI during the 2-year study period.
Characteristics of drug-eluting vs. baremetal stent thrombosisThe type of thrombosed stent was DES in 55 (50%) patients (27sirolimus-eluting stents, 16 paclitaxel-eluting stents, five tacroli-mus-eluting stents, one zotarolimus-eluting stent), BMS in 43(39%) patients, and an unascertained type of stent in 12 (11%)patients. Clinical and angiographic characteristics of patients withDES or BMS thrombosis are reported in Table 1. Among all inves-tigated clinical features, patients with DES thrombosis had signifi-cantly younger age, more common late or very late presentation,higher prevalence of diabetes mellitus, and platelet therapy
Outcome of PCI for stent thrombosis 3013
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

withdrawal within the last 15 days when compared with thosetreated with BMS (Table 1). Moreover, thrombosed DESs had asmaller diameter and were more often located on left anteriordescending artery or at bifurcation sites when compared withthrombosed BMSs and all other angiographic features beingsimilar (Table 1).
Procedural details and angiographicoutcome of percutaneous coronaryintervention for stent thrombosisPCI procedure details are reported in Table 2. The mainly adoptedstrategy of PCI was balloon dilation. Adjunctive devices were usedin a subgroup of patients and included thrombectomy (30%),
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Baseline clinical and angiographic characteristics of the overall study population and of subgroups of patientspresenting with drug-eluting or bare-metal stent thrombosis
Characteristic Whole studypopulation(n 5 110)
Bare metal stentthrombosis group(n 5 43)
Drug-eluting stentthrombosis group(n 5 55)
P-value (comparisonbetween DES andBMS groups)
Age (years)
Median 67 71 66 0.026
Range 32–87 41–85 32–87
Male sex, n (%) 77 (70) 32 (74) 35 (64) 0.25
Diabetes mellitus, n (%) 33 (30) 8 (19) 22 (40) 0.023
Current smoker, n (%) 49 (45) 22 (51) 22 (40) 0.27
Hypertension, n (%) 72 (65) 29 (67) 34 (62) 0.56
Hyperlipidaemia, n (%) 55 (50) 21 (50) 28 (51) 0.84
Renal failure, n (%) 22 (20) 9 (21) 10 (18) 0.11
Malignancy or haematological disease, n (%) 13 (12) 7 (16) 4 (7) 0.20
Antiplatelet therapy withdrawal within 15 days, n (%) 11 (10) 1 (2) 8 (15) 0.037
Previous coronary surgery, n (%) 7 (6) 2 (5) 5 (9) 0.46
ST-elevation MI as clinical presentation, n (%) 80 (73) 31 (72) 39 (71) 0.90
Cardiogenic shock, n (%) 19 (17) 11 (26) 7 (13) 0.10
ARC type of thrombosis, n (%)
Early 80 (72) 37 (86) 37 (67) 0.032
Late 19 (20) 4 (9) 13 (24) 0.11
Very late 9 (8) 2 (5) 5 (9) 0.46
Simultaneous stents thrombosis in different vessels, n (%) 3 (3) 1 (2) 2(4) 1.0
Thrombosed stent(s) diameter (mm)
Median 2.9 3.0 2.8 0.038
Range 2.25–4.0 2.5–4.0 2.25–4.0
Thrombosed stent(s) length (mm)
Median 23 24 23 0.67
Range 8–72 9–55 8–72
Two or more overlapping stents, n (%) 33 (30) 16 (37) 14 (26) 0.21
IIb/IIIa inhibitors administration, n (%) 78 (71) 30 (70) 39 (71) 0.90
Triple-vessel disease, n (%) 16 (15) 8 (19) 6 (11) 0.28
Target left anterior descending artery, n (%) 60 (55) 16 (37) 36 (65) 0.005
Severe calcification, n (%) 11 (10) 5 (12) 4 (7) 0.50
Stent underexpansiona 23 (21) 5 (12) 13 (24) 0.21
Bifurcated lesion (with side-branch .2 mm), n (%) 21 (19) 3 (7) 15 (27) 0.020
TIMI flow 0–1, n (%) 93 (85) 35 (82) 50 (91) 0.17
Reference-vessel diameter (mm)
Median 2.7 2.8 2.5 0.70
Range 1.0–4.1 1.0–4.1 1.8–4.1
aStent underexpansion: any underexpansion of the stent recognized at angiography by the interventional cardiology performing urgent intervention.
F. Burzotta et al.3014
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from
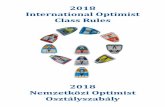
whereas only 3% of the patients underwent distal filter protection.Thrombectomy was performed using mainly thrombus-aspiratingcatheters (30 of 33 patients), whereas a minority (3 of 33) receivedAngiojet (Possis Medical Inc., Minneapolis, MN, USA) rheolyticthrombectomy. During the procedure, 45% of the patients weretreated by additional stent implantation (Table 2). As Table 3shows, patients who received stent implantation during PCI forST did not differ significantly from the remaining patients.
The angiographic results obtained after PCI are reported inTable 2. The overall quality of cine films was satisfactory as thecore laboratory was able to judge post-PCI TIMI flow in allprocedures and MBG and CTFC in the majority of them (95%pre-PCI and 83% post-PCI). Failure to re-establish anterogradeflow (post-PCI TIMI 0–1) occurred in as high as 12%, whereasoptimal angiographic reperfusion (TIMI 3 þ MBG 2 or 3) wasobtained in 64% of the patients. As shown in Table 4, using thestepwise multivariable analysis (which included the following pre-dictors emerged from the univariable analysis: diabetes mellitus,current smoker, hypertension, double simultaneous ST in differentvessels, three-vessel disease, target vessel, cardiogenic shock, distalembolization, and post-procedural thrombus score .1), the vari-ables that were significantly associated with failure to obtainoptimal angiographic reperfusion were distal embolization (OR
23.3, 95% CI 1.3–40.0), cardiogenic shock (OR 10.7, 95% CI2.0–56.9), target left anterior descending artery (OR 7.0, 95% CI1.7–29.1), post-procedural TS .1 (OR 5.7, 95% CI 1.4–22.9),and multivessel disease (OR 5.06, 95% CI 1.4–18.5). The non-significant Hosmer–Lemeshow goodness-of-fit P-value (0.56) indi-cated that the model was adequate.
Clinical outcome of percutaneouscoronary intervention for stentthrombosisThe completeness of follow-up was 100% at 30 days and 95% at 6months (five patients lost to late follow-up). The number ofadverse events observed during follow-up is reported in Table 5.The death rate was 12% at 30 days and 17% at 6 months.MACCEs observed during follow-up were mainly due to cardiacevents (one stroke only) and occurred in as high as 21% of thepatients at 30 days and in 30% at 6 months.
The type of thrombosed stent (DES or BMS) did not influencethe clinical outcome: survival curves free of death and MACCE forBMS and DES thrombosis are reported in Figure 1. Conversely, thestepwise multivariable analysis (which includes the following pre-dictors emerged from univariable analysis: cardiogenic shock,
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Procedural characteristics and angiographic results of the whole study population and of subgroups of patientspresenting with drug-eluting or bare metal stent thrombosis
Characteristic Whole studypopulation(n 5 110)
Bare metal stentthrombosisgroup (n 5 43)
Drug-elutingstent thrombosisgroup (n 5 55)
P-value (comparisonbetween DES andBMS groups)
Intra-aortic balloon pump, n (%) 11 (10) 6 (14) 5 (9) 0.45
Balloon dilation, n (%) 104 (95) 40 (93) 52 (95) 0.76
Thrombectomy, n (%) 33 (30) 15 (33) 16 (29) 0.54
Distal filter protection, n (%) 3 (3) 1 (2) 2 (4) 0.59
Stent(s) implantation, n (%) 49 (45) 22 (51) 23 (42) 0.36
Drug-eluting stent, n (%) 22 (21) 9 (21) 12 (18) 0.92
Bare metal stent, n (%) 37 (34) 13 (30) 11 (20) 0.24
Post-procedural TIMI flow, n (%)
0–1 14 (12) 6 (14) 8 (15) 0.93
2 16 (15) 9 (21) 5 (9) 0.10
3 80 (73) 28 (65) 42 (76) 0.22
Slow flow or transient no-reflow, n (%) 11 (10) 6 (14) 4 (7) 0.33
Post-procedural myocardial blush grade, n (%)
Myocardial blush analysable 91 (83) 39 (91) 42 (76) 0.06
0–1 28 (31) 11 (26) 23 (42) 0.09
2 21 (23) 10 (23) 9 (16) 0.39
3 42 (46) 18 (42) 19 (34) 0.45
Distal embolization, n (%) 8 (7) 3 (7) 3 (6) 0.54
Post-procedural thrombus score .1, n (%) 19 (17) 8 (19) 11 (20) 0.86
Optimal angiographic reperfusion (TIMI 3 and MBG 2 or 3), n (%) 59 (64) 24 (62) 28 (64) 0.63
Post-procedural minimal lumen diameter (mm)
Median 2.6 2.5 2.6 0.83
Range 0–4.1 0–3.9 0–4.1
Outcome of PCI for stent thrombosis 3015
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

very late ST, double simultaneous ST in different vessels, severecalcification, stent implantation during PCI for ST, slow flow ortransient no-reflow, post-procedural thrombus score .1, andfailure to achieve optimal angiographic reperfusion) showed thatthe independent predictors of 6-month mortality were very latepresentation of thrombosis (OR 9.3, 95% CI 1.2–70.7), implan-tation of stent during PCI for ST (OR 6.1, 95% CI 1.1–16.6), andfailure to achieve an optimal angiographic reperfusion (OR 4.6,95% CI 1.3–16.4) (Table 4). These data did not deviate significantlyfrom the logistic model, as indicated by the non-significantHosmer–Lemeshow goodness-of-fit test (P ¼ 0.87).
Survival curves according to the timing of ST presentation(early, late, and very late), to further stent implantation duringindex PCI, and to the achievement of optimal angiographic reper-fusion at the end of the procedure are reported in Figure 2. Step-wise multivariable analysis (which includes the following predictorsemerged from univariable analysis: renal failure, very late ST, twoor more overlapping stents, three-vessel disease, target vessel,severe calcification, TIMI flow 0–1, stent implantation during PCIfor ST, and failure to achieve optimal angiographic reperfusion)also showed that the only independent predictors of 6-monthMACCE (Table 4) were stent implantation during PCI for ST(OR 5.3, 95% CI 1.7–16.4), three-vessel disease (OR 4.9, 95% CI
1.2–21.0), failure to achieve optimal angiographic reperfusion(OR 4.5, 95% CI 1.5–13.5), and two or more overlapping stents(OR 4.4, 95% CI 1.4–13.6). The non-significant Hosmer–Lemeshow goodness-of-fit P-value (P ¼ 0.61) indicated that themodel was adequate.
Applying the ARC criteria for ST, the overall 6-month rate ofrecurrent ST was 16.2% (definite: 6.7%, probable: 5.7%, andpossible: 3.8%), with a median interval between PCI for ST andrecurrent ST of 45 days (range: 2–175 days). Interestingly, ahigher rate of recurrent ST at 6 months was observed in patientswho received stent implantation during PCI for ST compared withthe remaining patients (26 vs. 10%, respectively, P ¼ 0.04),whereas the type of implanted stent during PCI for ST did notinfluence the recurrent ST (20% in DES vs. 30% in BMS, P ¼ 0.45).
DiscussionIn the present report, we describe the results of the first multicen-tre registry assessing the angiographic and clinical outcomes ofpatients with angiographically confirmed ST undergoing urgentPCI in the contemporary DES era. This was the result of a coop-erative effort performed by a series of different hospitals well dis-tributed in the same urban area. No sponsorship was endorsed to
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Key pre-intervention characteristics of patients treated or not by stent implantation during PCI for stentthrombosis
Characteristic Stent implantation duringPCI for ST (n 5 49)
No stent implantationduring PCI for ST (n 5 61)
P-value
Age (years)
Median 68 67 0.85
Range 41–85 32–87
Male sex, n (%) 33 (67) 44 (72) 0.59
Diabetes mellitus, n (%) 17 (35) 16 (26) 0.36
Current smoker, n (%) 23 (47) 26 (43) 0.65
Hypertension, n (%) 31 (63) 41 (67) 0.66
Hyperlipidaemia, n (%) 24 (49) 31 (51) 0.85
Renal failure, n (%) 8 (16) 14 (23) 0.39
Malignancy or haematological disease, n (%) 4 (8) 9 (15) 0.29
Previous coronary surgery, n (%) 2 (4) 5 (8) 0.38
ST-elevation MI as clinical presentation, n (%) 33 (67) 44 (72) 0.58
Cardiogenic shock, n (%) 10 (20) 9 (15) 0.44
ARC type of thrombosis, n (%)
Early 36 (74) 44 (72) 0.88
Late 8 (16) 13 (21) 0.51
Very late 5 (10) 4 (7) 0.49
Two or more overlapping stents, n (%) 11 (22) 22 (36) 0.12
IIb/IIIa inhibitors administration, n (%) 39 (80) 39 (64) 0.07
Triple-vessel disease, n (%) 6 (12) 10 (16) 0.54
Target left anterior descending artery 35 (71) 45 (74) 0.78
Severe calcification, n (%) 6 (12) 5 (8) 0.48
Stent underexpansiona 8 (16) 15 (25) 0.29
Bifurcated lesion, n (%) 10 (20) 11 (18) 0.75
aStent underexpansion: any underexpansion of the stent recognized at angiography by the interventional cardiology performing urgent intervention.
F. Burzotta et al.3016
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

avoid any possible source of bias in data collection, analysis, andinterpretation. Moreover, the study design was published as a fullpaper before the first data analysis is undertaken.
Overall, the study allowed to assess: (i) the prevalence of PCI onangiographically confirmed ST; (ii) the comparison between DESand BMS thrombosis presentation and outcome; and (iii) the angio-graphic and the 6-month clinical outcome of invasively managed ST.
Prevalence of percutaneous coronaryintervention for angiographicallyconfirmed stent thrombosisDuring a 2-year period, we found that PCI for angiographically con-firmed ST occurred in less than one every 100 stent implantationprocedures. The ratio between stent implantation procedure andPCI for ST was not different between BMSs and DESs. Thisfigure is in keeping with other reports, showing the absence of sig-nificant differences in the ST rate between them.25 However, asthe length of study recruitment and follow-up were limited andDES might mainly affect late thrombotic events, the hypothesisof an increased very-late DES-related hazard26 cannot be
discarded. Interestingly, although angiographically confirmed STwas a low frequency event, it accounted for 3.6% of the primaryor rescue PCI (as in 73% of the cases ST caused STEMI) performedby the study centres.
Comparison between drug-eluting andbare metal stent thrombosis presentationand outcomeThe comparison between DES and BMS thrombosis showed somedifferences in the clinical, procedural, and angiographic character-istics. Patients with DES thrombosis, compared with those withBMS, were significantly younger, exhibited higher prevalence ofdiabetes mellitus, and presented ST more frequently in left anteriordescending artery, small vessels, and bifurcated lesions. Theseassociations are difficult to interpret. They might simply be theresult of a selection bias in favour of DES usage when such con-ditions are present. In contrast, the significantly higher prevalenceof platelet therapy withdrawal within last 15 days and of late andvery late presentation found in DES, compared with BMS throm-bosis, might be causally related to the stent type. Indeed, a seriesof observations from studies with different designs stronglysuggest that premature antiplatelet therapy discontinuation mayplay a key role in DES thrombosis3,8,27– 29 and that late and verylate STs are more often observed after DES implantation whencompared with BMS implantation.16,26 These data reinforce theperception that patient compliance and the absence of contraindi-cations to dual anti-platelet treatment should be pivotal during thedecision-making process of stent selection. Moreover, duringfuture assessments of safety and efficacy, individual patientfollow-up after DES implantation should probably be extendedwell beyond the classical 6- or 9-month study period adopted inthe BMS era.
Outcome of invasively managed stentthrombosisOur study shows that ST represents a high-risk clinical scenario.The patient presenting with ST has known history of ischaemicheart disease, has been previously exposed to the risk ofperi-PCI myonecrosis, and has sometimes developed conditionsthat may interfere with his compliance or tolerance to medicaltherapies. Moreover, the target lesion during ST is composed ofa variable (and usually huge) amount of thrombus and is oftencomplex (including bifurcation, restenosis, and diffuse disease).Finally, the initial stent deployment might have been subopti-mal.2,12,30,31 In the DES era, all these issues are likely to be exacer-bated by the inclusion of difficult coronary anatomies and patients(previously usually not considered for percutaneous treatments).All these factors may contribute to explain the poor angiographicand clinical results observed in the present study.
Overall, the observed clinical outcome of patients with ST in thisstudy is disappointing, as it is associated with both a high early mor-tality (12% at 30 days) and the occurrence of further adverseevents during the later follow-up period leading to 17% deathrate and 30% MACCE rate at 6 months. Such figures are in linewith the results of early smaller reports,11–14 as well as withthat of a recent Spanish registry.32 Of note, the outcome was
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 Predictors of primary angiographic (lackof optimal angiographic reperfusion 5 TIMI 31MBG 2or 3) and clinical (death and major adverse coronaryor cerebrovascular events) endpoints at 6 monthsemerging from the multivariable analysis
Adjusted odds ratio(95% confidenceintervals)
P-value
Multivariable predictors of failure to achieve optimal angiographicreperfusion
Distal embolization 23.3 (1.3–40.0) 0.013
Cardiogenic shock 10.7 (2.0–56.9) 0.02
Target left anterior descendingartery
7.0 (1.7–29.1) 0.003
Post-PCI thrombus score .1 5.7 (1.4–22.9) 0.012
Three-vessel disease 5.1 (1.4–18.5) 0.011
Multivariable predictors of 6-month death
Very late ST 9.3 (1.2–70.7) 0.03
Stent implantation during PCIfor ST
6.1 (1.1–16.6) 0.003
Failure to achieve optimalangiographic reperfusion
4.6 (1.3–16.4) 0.02
Multivariable predictors of 6-month MACCE
Stent implantation during PCIfor ST
5.3 (1.7–16.4) 0.004
Three-vessel disease 4.9 (1.2–21.0) 0.03
Failure to achieve optimalangiographic reperfusion
4.5 (1.5–13.5) 0.02
Two or more overlappingstents
4.4 (1.4–13.6) 0.01
ST, stent thrombosis; MACCE, major adverse coronary and cerebrovascularevents.
Outcome of PCI for stent thrombosis 3017
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

similar for ST caused by BMSs or DESs. Furthermore, based on theARC criteria, the rate of recurrent ST at 6 months was remarkable(16%). In a recent intravascular ultrasound study, it has beensuggested that re-PCI on thrombosed stent is able to correctimportant technical difficulties (including stent underexpansionand stent struts ‘malapposition’ to the vessel wall) that couldhave occurred at the time of stent implantation.33 It follows that
in patients presenting with recurrent ST, persistent thrombogen-esis at the stent site is more likely to reflect a systemic pro-thrombotic state rather than a local phenomenon. Some systemicfeatures recently recognized as risk factors for ST such as hyper-sensitivity to the different stent components34 and low responsive-ness to anti-platelet drugs35 may also play a role for persistentthrombogenesis.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 5 Clinical outcome at 30-day and 6-month observed in the overall study population and in subgroups of patientspresenting with drug-eluting or bare metal stent thrombosis
Whole studypopulation(n 5 110)
Bare metal stentthrombosis group(n 5 43)
Drug-eluting stentthrombosis group(n 5 55)
P-value (comparisonbetween DES andBMS groups)
30-day follow-up, n (%) 110 (100) 43 (100) 55 (100)
Death 13 (12) 7 (16) 5 (9) 0.28
Non-fatal myocardialinfarction
8 (7) 5 (12) 3 (5) 0.27
Target vesselrevascularization
14 (13) 8 (19) 5 (9) 0.17
Cerebrovascular accident 1 (1) 1 (2) 0 —
MACCE 23 (21) 12 (28) 9 (16) 0.17
6-month follow-up, n (%) 105 (95) 41 (95) 52 (95) 0.86
Death 18 (17) 8 (19) 9 (17) 0.87
Non-fatal myocardialinfarction
12 (11) 6 (15) 6 (12) 0.66
Target vesselrevascularization
18 (17) 10 (24) 7 (14) 0.18
Cerebrovascular accident 1 (1) 1 (2) 0 —
MACCE 32 (30) 15 (35) 15 (29) 0.58
Figure 1 Kaplan–Meier survival curves for patients who presented with thrombosis of drug-eluting stents and those who presented withthrombosis of bare metal stents. (A) shows overall survival and (B) freedom from MACCE.
F. Burzotta et al.3018
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

Despite a liberal adoption of all the most effective resources ofcontemporary invasive management (high rates of IIb/IIIa inhibitoradministration, systematic intra-aortic balloon pumping in patientswith cardiogenic shock, and a high usage of thrombectomydevices), the angiographic markers of no reflow were oftenpresent after PCI. Such suboptimal post-PCI angiographic resultsare clinically relevant as they may translate in a poor outcome.Indeed, in our study, lack of a optimal angiographic reperfusionwas independently associated with worse 6-month survival. As aconsequence, the direct relation between post-PCI reperfusionassessed by blush grade and survival previously reported inpatients with de novo occlusion of native coronary arteries22,24
can be extended to this high-risk patient subset. In addition tolack of optimal reperfusion, implantation of a stent during PCIfor ST and very late presentation of ST were found to indepen-dently predict 6-month survival. The implantation of anotherstent during PCI for ST is frequently required as a bail-outoption to manage dissections, plaque or thrombus shift outsidethe previously implanted stent and previously untreated adjacentatherosclerotic disease. However, the strong relation with latemortality and MACCE observed in our study as well as inanother independent study32 deserves attention. It can be specu-lated that patients who developed ST represent a selected sub-group with high tendency to thrombus formation over metallicstent struts, so that further augmentation of metal amount is notwell tolerated. Taken together with the positive influence on latemortality associated with angiographic reperfusion, these datasuggest that during PCI for ST, interventionalists should focus onthe goal of achieving optimal myocardial reperfusion rather thanan optimal residual stenosis by further stent implantation. Finally,the observed increased risk associated with very late presentationof thrombosis has not been previously reported. However, it isworth noting that, due to its rarity, the investigation on the mech-anisms and outcome of very late ST are actually in its former
stages,36 and the present observation calls for further studies onthis emerging clinical entity.
Study limitationsA major limitation of the present study is represented by theinclusion of a remarkable number of patients retrospectivelyenrolled: as sources of confounding factors and bias aremore common in retrospective data collections, their occur-rence cannot be excluded. Nevertheless, as no appreciabledifference between retrospectively and prospectively collectedpatients was detected in the preliminary validation step of theanalyses, the accuracy of retrospective cohort recruitment issupported.
Another important limitation of the present study is rep-resented by the absence of IVUS data as technical factorssuch as strut fracture, stent underexpansion, or even stentoverexpansion leading to ST cannot be ascertained by angio-graphy. Moreover, resistance to antiplatelet therapy andpatient’s compliance to antiplatelet therapy during follow-upwere not assessed so that the relation between drug resistanceor incompliance and risk of re-thrombosis could not beinvestigated.
ConclusionsWithin its limitation of being an observational investigation, thepresent study provides unique information about the prevalence,the procedural characteristics, and the outcome of patients withangiographically confirmed ST treated by urgent PCI in thecontemporary DES era. The staggering high rate of mortality andmorbidity associated with ST, even when treated by primary PCIin high volume centres, calls for action in order to prevent itsoccurrence and further improve its treatment. With regard tothe first issue, the best prevention perhaps remains to avoid PCI
Figure 2 Kaplan–Meier survival curves after PCI for stent thrombosis. (A) shows overall survival of patients who received or notimplantation of stent during PCI for stent thrombosis; (B) shows overall survival of patients who had or not had post-PCI optimal angiographicreperfusion (TIMI 3 þ MBG 2 or 3); (C) shows overall survival of patients with different types of stent thromboses according to timing (early,late, and very late).
Outcome of PCI for stent thrombosis 3019
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

when it is not indicated, as in oligo-asymptomatic stable patients.37
With regard to treatment, the current study provides useful infor-mation on possible strategies to improve PCI for ST, including agreater emphasis on myocardial reperfusion than on residualstenosis.
AcknowledgementsThe authors are indebted to Giovanni Paolo Talarico who hasbeen responsible for the organization of the electronic databaseof the study.
Conflict of interest: none declared.
Appendix: list of institutionsparticipating in the study
Institute of Cardiology, Catholic University of the Sacred Heart, Rome,Italy (Prof. Giovanni Schiavoni); U.O. of Interventional Cardiology,A.O. San Camillo-Forlanini Hospital, Rome, Italy (Dr RobertoViolini); Department of Cardiology, San Filippo Neri Hospital, Rome,Italy (Dr Giuseppe Richichi); Catheterization Laboratory, S. GiovanniHospital, Rome, Italy; Department of Cardiology, San Pietro FBF Hos-pital, Rome, Italy (Dr Roberto Serdoz); Department of Cardiovascularand Respiratory Sciences, Policlinico Umberto I, ‘La Sapienza’ Univer-sity, Rome, Italy (Dr Riccardo Colantonio); UOSD Emodinamica eCardiologia Interventistica, ‘Sandro Pertini’ Hospital, Rome, Italy(Dr Paolo Loschiavo); U.O.C. of Cardiology, S. Spirito Hospital,Rome, Italy (Dr Alessandro Ferraioni); U.O. Cardiologia Invasiva eInterventistica Endovascolare, S. Carlo - I.D.I. Hospital, Rome, Italy(Dr Francesco Gemelli); Catheterization Laboratory, Division of Car-diology, Policlinico Casilino Hospital, Rome, Italy (Dr Ernesto Lioy).
References1. Karrillon GJ, Morice MC, Benveniste E, Bunouf P, Aubry P, Cattan S, Chevalier B,
Commeau P, Cribier A, Eiferman C, Grollier G, Guerin Y, Henry M, Lefevre T,Livarek B, Louvard Y, Marco J, Makowski S, Monassier JP, Pernes JM, Rioux P,Spaulding C, Zemour G. Intracoronary stent implantation without ultrasound gui-dance and with replacement of conventional anticoagulation by antiplatelettherapy. 30-day clinical outcome of the French Multicenter Registry. Circulation1996;94:1519–1527.
2. Moussa I, Di Mario C, Reimerse B, Akiyama T, Tobis J, Colombo A. Subacutestent thrombosis in the era of intravascular ultrasound-guided coronary stentingwithout anticoagulation: frequency, predictors and clinical outcome. J Am CollCardiol 1997;29:6–12.
3. Cutlip DE, Baim DS, Ho KK, Popma JJ, Lansky AJ, Cohen DJ, Carrozza JP Jr,Chauhan MS, Rodriguez O, Kuntz RE. Stent thrombosis in the modern era: apooled analysis of multicenter coronary stent clinical trials. Circulation 2001;103:1967–1971.
4. Orford JL, Lennon R, Melby S, Fasseas P, Bell MR, Rihal CS, Holmes DR,Berger PB. Frequency and correlates of coronary stent thrombosis in themodern era: analysis of a single center registry. J Am Coll Cardiol 2002;40:1567–1572.
5. Moreno R, Fernandez C, Hernandez R, Alfonso F, Angiolillo DJ, Sabate M,Escaned J, Banuelos C, Fernandez-Ortiz A, Macaya C. Drug-eluting stent throm-bosis: results from a pooled analysis including 10 randomized studies. J Am CollCardiol 2005;45:954–959.
6. Daemen J, Wenaweser P, Tsuchida K, Abrecht L, Vaina S, Morger C, Kukreja N,Juni P, Sianos G, Hellige G, van Domburg RT, Hess OM, Boersma E, Meier B,Windecker S, Serruys PW. Early and late coronary stent thrombosis ofsirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: datafrom a large two-institutional cohort study. Lancet 2007;369:667–678.
7. Luscher TF, Steffel J, Eberli FR, Joner M, Nakazawa G, Tanner FC, Virmani R.Drug-eluting stent and coronary thrombosis: biological mechanisms and clinicalimplications. Circulation 2007;115:1051–1058.
8. Pfisterer M, Brunner-La Rocca HP, Buser PT, Rickenbacher P, Hunziker P,Mueller C, Jeger R, Bader F, Osswald S, Kaiser C, BASKET-LATE Investigators.Late clinical events after clopidogrel discontinuation may limit the benefit ofdrug-eluting stents: an observational study of drug-eluting versus bare-metalstents. J Am Coll Cardiol 2006;48:2584–2591.
9. Lagerqvist B, James SK, Stenestrand U, Lindback J, Nilsson T, Wallentin L, SCAARStudy Group. Long-term outcomes with drug-eluting stents versus bare-metalstents in Sweden. N Engl J Med 2007;356:1009–1019.
10. Kastrati A, Mehilli J, Pache J, Kaiser C, Valgimigli M, Kelbaek H, Menichelli M,Sabate M, Suttorp MJ, Baumgart D, Seyfarth M, Pfisterer ME, Schomig A. Analysisof 14 trials comparing sirolimus-eluting stents with bare-metal stents. N Engl J Med2007;356:1030–1039.
11. Wenaweser P, Rey C, Eberli FR, Togni M, Tuller D, Locher S, Remondino A,Seiler C, Hess OM, Meier B, Windecker S. Stent thrombosis following bare-metalstent implantation: success of emergency percutaneous coronary interventionand predictors of adverse outcome. Eur Heart J 2005;26:1180–1187.
12. Cheneau E, Leborgne L, Mintz GS, Kotani J, Pichard AD, Satler LF, Canos D,Castagna M, Weissman NJ, Waksman R. Predictors of subacute stent thrombosis:results of a systematic intravascular ultrasound study. Circulation 2003;108:43–47.
13. Ong AT, Hoye A, Aoki J, van Mieghem CA, Rodriguez Granillo GA,Sonnenschein K, Regar E, McFadden EP, Sianos G, van der Giessen WJ, deJaegere PP, de Feyter P, van Domburg RT, Serruys PW. Thirty-day incidenceand six-month clinical outcome of thrombotic stent occlusion after bare-metal,sirolimus, or paclitaxel stent implantation. J Am Coll Cardiol 2005;45:947–953.
14. Kuchulakanti PK, Chu WW, Torguson R, Ohlmann P, Rha SW, Clavijo LC,Kim SW, Bui A, Gevorkian N, Xue Z, Smith K, Fournadjieva J, Suddath WO,Satler LF, Pichard AD, Kent KM, Waksman R. Correlates and long-term outcomesof angiographically proven stent thrombosis with sirolimus- and paclitaxel-elutingstents. Circulation 2006;113:1108–1113.
15. Burzotta F, Romagnoli E, Manzoli A, Pristipino C, Belloni F, Sardella G, Rigattieri S,Gioffre G, Mazzarotto P, Summaria F, Parma A, Danesi A, Prati F, Trani C. TheOutcome of PCI for stent-ThrombosIs MultIcentre Study (OPTIMIST): rationaleand design of a multicenter registry. Am Heart J 2007;153:377.e1–5.
16. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, Steg PG,Morel MA, Mauri L, Vranckx P, McFadden E, Lansky A, Hamon M,Krucoff MW, Serruys PW; Academic Research Consortium. Clinical end pointsin coronary stent trials: a case for standardized definitions. Circulation 2007;115:2344–2351.
17. The Joint European Society of Cardiology/American College of CardiologyCommittee. Myocardial infarction redefined: a consensus document of the JointEuropean Society of Cardiology/American College of Cardiology Committeefor the Redefinition of Myocardial Infarction. Eur Heart J 2000;21:1502–1513. JAm Coll Cardiol 2000;36:959–969.
18. TIMI: TIMI Study Group. The Thrombolysis in Myocardial Infarction (TIMI) trial.N Engl J Med 1985;312(Suppl):932–936.
19. Henriques JP, Zijlstra F, Ottervanger JP, de Boer MJ, van ‘t Hof AW, Hoorntje JC,Suryapranata H. Incidence and clinical significance of distal embolization duringprimary angioplasty for acute myocardial infarction. Eur Heart J 2002;23:1112–1117.
20. Gibson CM, Cannon CP, Daley WL, Dodge JT Jr, Alexander B Jr, Marble SJ,McCabe CH, Raymond L, Fortin T, Poole WK, Braunwald E. TIMI frame count:a quantitative method of assessing coronary artery flow. Circulation 1996;93:879–888.
21. Gibson CM, de Lemos JA, Murphy SA, Marble SJ, McCabe CH, Cannon CP,Antman EM, Braunwald E, TIMI Study Group. Combination therapy with abcixi-mab reduces angiographically evident thrombus in acute myocardial infarction:a TIMI 14 substudy. Circulation 2001;103:2550–2554.
22. van ‘t Hof AW, Liem A, Suryapranata H, Hoorntje JC, de Boer MJ, Zijlstra F.Angiographic assessment of myocardial reperfusion in patients treated withprimary angioplasty for acute myocardial infarction: myocardial blush grade.Zwolle Myocardial Infarction Study Group. Circulation 1998;97:2302–2306.
23. Popma JJ, Bashore TD. In: Topol E, ed. Qualitative and Quantitative Angiography.Philadelphia: WB Saunders; 1994. 1052–1068.
24. De Luca G, van ‘t Hof AW, Ottervanger JP, Hoorntje JC, Gosselink AT,Dambrink JH, Zijlstra F, de Boer MJ, Suryapranata H. Unsuccessful reperfusionin patients with ST-segment elevation myocardial infarction treated by primaryangioplasty. Am Heart J 2005;150:557–562.
25. Holmes DR Jr, Kereiakes DJ, Laskey WK, Colombo A, Ellis SG, Henry TD,Popma JJ, Serruys PW, Kimura T, Williams DO, Windecker S, Krucoff MW.Thrombosis and drug-eluting stents: an objective appraisal. J Am Coll Cardiol2007;50:109–118.
26. Jaffe R, Strass BH. Late and very late thrombosis of drug-eluting stents. Evolvingconcepts and perspectives. J Am Coll Cardiol 2007;50:119–127.
27. Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G, Airoldi F,Chieffo A, Montorfano M, Carlino M, Michev I, Corvaja N, Briguori C,
F. Burzotta et al.3020
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

Gerckens U, Grube E, Colombo A. Incidence, predictors, and outcome of throm-bosis after successful implantation of drug-eluting stents. JAMA 2005;293:2126–2130.
28. Spertus JA, Kettelkamp R, Vance C, Decker C, Jones PG, Rumsfeld JS,Messenger JC, Khanal S, Peterson ED, Bach RG, Krumholz HM, Cohen DJ. Preva-lence, predictors, and outcomes of premature discontinuation of thienopyridinetherapy after drug-eluting stent placement: results from the PREMIER registry.Circulation 2006;113:2803–2809.
29. Airoldi F, Colombo A, Morici N, Latib A, Cosgrave J, Buellesfeld L, Bonizzoni E,Carlino M, Gerckens U, Godino C, Melzi G, Michev I, Montorfano M,Sangiorgi GM, Qasim A, Chieffo A, Briguori C, Grube E. Incidence and predictorsof drug-eluting stent thrombosis during and after discontinuation of thienopyri-dine treatment. Circulation 2007;116:745–754.
30. Cook S, Wenaweser P, Togni M, Billinger M, Morger C, Seiler C, Vogel R, Hess O,Meier B, Windecker S. Incomplete stent apposition and very late stent thrombo-sis after drug-eluting stent implantation. Circulation 2007;115:2426–2434.
31. Uren NG, Schwarzacher SP, Metz JA, Lee DP, Honda Y, Yeung AC, Fitzgerald PJ,Yock PG, POST Registry Investigators. Predictors and outcomes of stent throm-bosis: an intravascular ultrasound registry. Eur Heart J 2002;23:124–132.
32. de la Torre-Hernandez JM, Alfonso F, Hernandez F, Elizaga J, Sanmartin M, Pinar E,Lozano I, Vazquez JM, Botas J, de Prado AP, Hernandez JM, Sanchis J, Nodar JM,Gomez-Jaume A, Larman M, Diarte JA, Rodrıguez-Collado J, Rumoroso JR,Lopez-Minguez JR, Mauri J, ESTROFA Study Group. Drug-eluting stent thrombo-sis: results from the multicenter Spanish registry ESTROFA (Estudio ESpanolsobre TROmbosis de stents FArmacoactivos). J Am Coll Cardiol 2008;51:986–990.
33. Alfonso F, Suarez A, Perez-Vizcayno MJ, Moreno R, Escaned J, Banuelos C,Jimenez P, Bernardo E, Angiolillo DJ, Hernandez R, Macaya C. Intravascular ultra-sound findings during episodes of drug-eluting stent thrombosis. J Am Coll Cardiol2007;21:2095–2097.
34. Nebeker JR, Virmani R, Bennett CL, Hoffman JM, Samore MH, Alvarez J,Davidson CJ, McKoy JM, Raisch DW, Whisenant BK, Yarnold PR, Belknap SM,West DP, Gage JE, Morse RE, Gligoric G, Davidson L, Feldman MD. Hypersensi-tivity cases associated with drug-eluting coronary stents: a review of availablecases from the Research on Adverse Drug Events and Reports (RADAR)project. J Am Coll Cardiol 2006;47:175–181.
35. Buonamici P, Marcucci R, Migliorini A, Gensini GF, Santini A, Paniccia R, Moschi G,Gori AM, Abbate R, Antoniucci D. Impact of platelet reactivity after clopidogreladministration on drug-eluting stent thrombosis. J Am Coll Cardiol 2007;49:2312–2317.
36. Serruys PW, Daemen J. Late stent thrombosis: a nuisance in both bare metal anddrug-eluting stents. Circulation 2007;115:1433–1439.
37. Fox K, Garcia MA, Ardissino D, Buszman P, Camici PG, Crea F, Daly C, DeBacker G, Hjemdahl P, Lopez-Sendon J, Marco J, Morais J, Pepper J, Sechtem U,Simoons M, Thygesen K, Priori SG, Blanc JJ, Budaj A, Camm J, Dean V,Deckers J, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A,Tamargo J, Zamorano JL, Task Force on the Management of Stable Angina Pec-toris of the European Society of Cardiology; ESC Committee for Practice Guide-lines (CPG). Guidelines on the management of stable angina pectoris: executivesummary: the Task Force on the Management of Stable Angina Pectoris of theEuropean Society of Cardiology. Eur Heart J 2006;27:1341–1381.
Outcome of PCI for stent thrombosis 3021
by guest on June 28, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from