Pediatric and Congenital Cardiology, Cardiac Surgery and ...

Catheterization and Cardiovascular Diagnosis 1:157-I69 (1975)
Original Studies
MAJOR ORIGIN
VARIATIONS IN ANATOMICAL OF THE CORONARY ARTERIES:
Angiographic Observations in 4,250 Patients Without Associated Congenital Heart Disease. H. Jurgen Engel, M.D., Carlos Torres, M.D., and Harry L. Page, Jr., M.D.
In 51 (1.2%) of 4,250 patients studied by selective coronary arteriography, one or more major elements of the coronary arterial system originated from the sinuses of Valsaiva in an ectopic manner. The majority of variations involved the left coronary artery. The majority of ectopic ostie were located in the right sinus of Valsalva. Failure to recognize variations in coronary arterial origin can prolong arteriography procedures and lead to errors in interpretation of coronary artery anatomy and pathology. It is concluded from this experience that the incidence and location of major variations in coronary arterial origin are relatively predictable. The data are useful in expediting coronary arteriography procedures and thus improving patient care.
Key words: coronary vessels, anatomical variations
With increasing utilization of coronary arteriography in the diagnosis of ischemic heart disease, unexpected origin and course of coronary arteries is encountered more and more frequently. In such circumstances knowledge of variations in location of coronary artery ostia and their statistical probability is useful to achieve a complete angiographic study in a reasonably brief time. It is the purpose of this communication to summarize an angiographic experience concerning unusual coronary artery origins in 4,250 patients without associated congenital heart disease and to suggest a methodical approach to their recogni- tion and demonstration.
From St. Thomas Hospital, Nashville, Tennessee Address reprint requests to Harry L. Page, Jr., M.D., Division of Cardiology, St. Thomas Hospital, Nashville. Tennessee 37205
157 0 1975 Alan R. Liss, Inc., 150 F i f t h Avenue, New York, N.Y. 10011
158 Engel, Torres, and Page
MATERIAL AND METHODS
Catheterization reports and selected cineangiograms of 4,250 patients undergo- ing selective coronary arteriography at St. Thomas Hospital between 1968 and 1974 were reviewed for major variations in coronary artery origin. Patients with associated congenital heart disease were excluded because of the possibility that a higher incidence of associated coronary artery anomalies might not be rep- resentative of the population of patients referred for suspected obstructive coronary artery disease. (1, 2).
RESULTS
The total incidence of recognized major variations in coronary artery origin was 1.2% (n = 51), Table I.
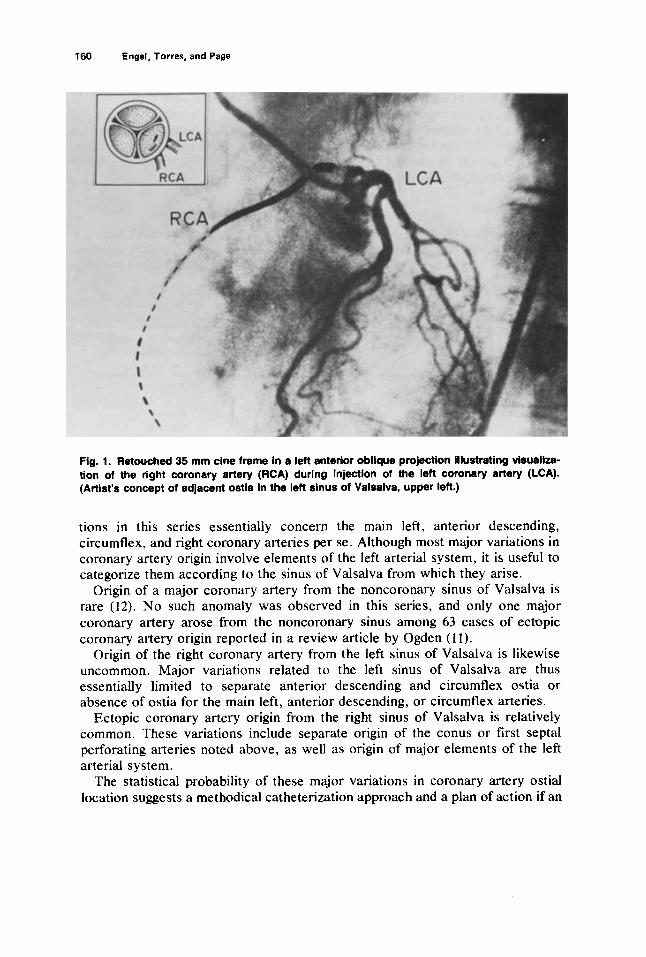
Origin of the right coronary artery from the left sinus of Valsalva was documented in only three patients (Fig. 1). These arteries arose near the origin of the main left coronary artery but were not selectively catheterized. Spillback of contrast material during injections of the left coronary artery demonstrated them to course anterior to the aortic root to reach the right atrioventricular groove from where they distributed in a normal manner.
Origin of the anterior descending and circumflex arteries from separate ostia in the left sinus of Valsalva was documented in eight patients (Fig. 2).
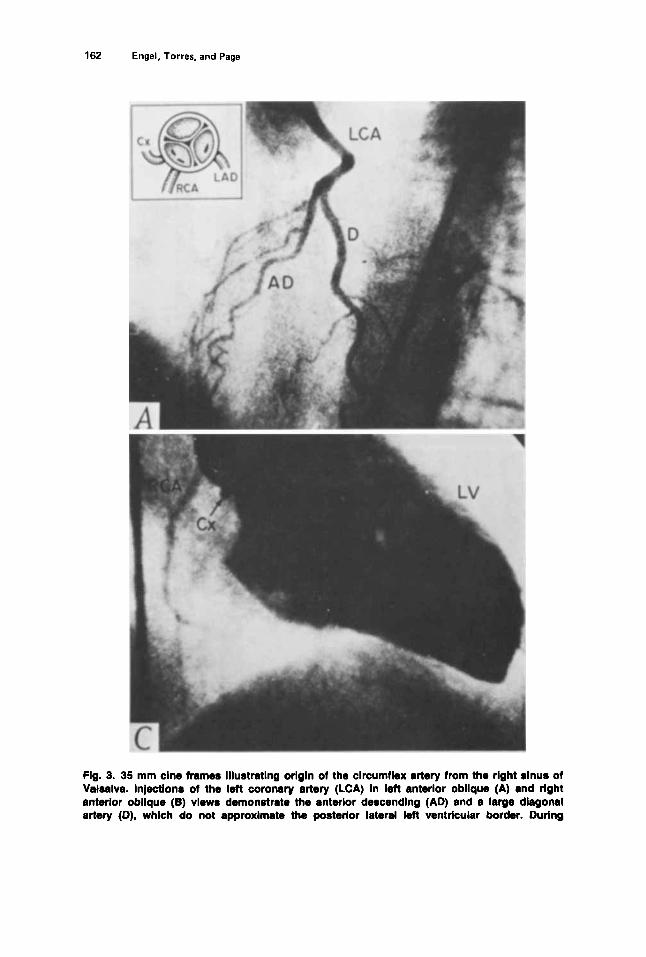
Origin of the circumflex artery from the right coronary artery or right sinus of Valsalva was the most common major variation of coronary artery origin observed (n = 30). In 11 patients the circumflex arose from a separate ostium in the right sinus of Valsalva and was not opacified by injections of the right coronary artery. In 19 patients the circumflex originated as a proximal branch of the right coronary artery or with the right coronary artery from a common ostium (Fig. 3).
Origin of the anterior descending artery from the right sinus of Valsalva with origin of the circumflex artery from the left sinus of Valsalva was observed in three patients (Fig. 4).
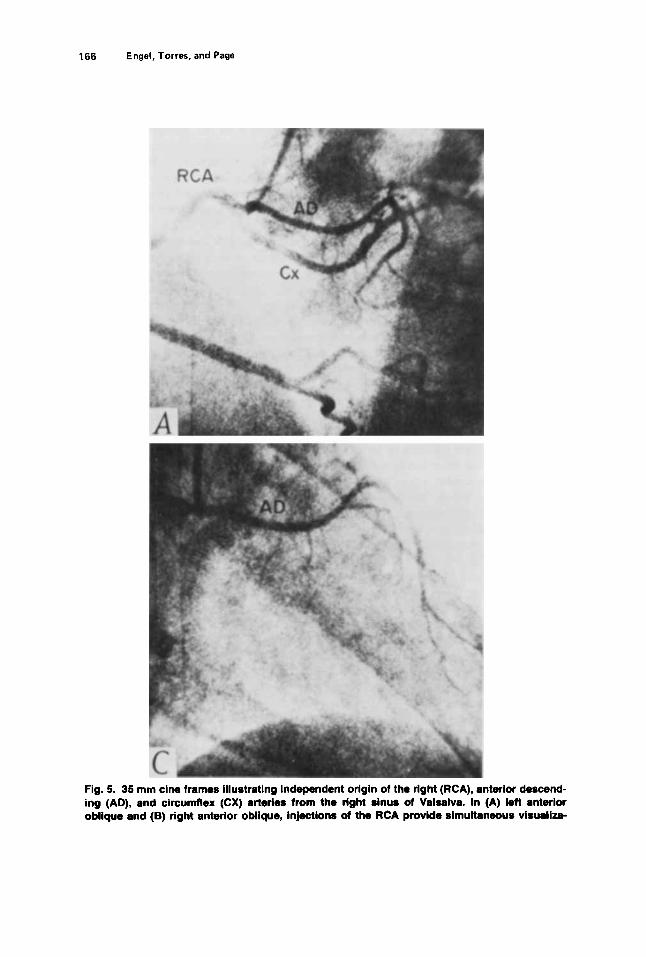
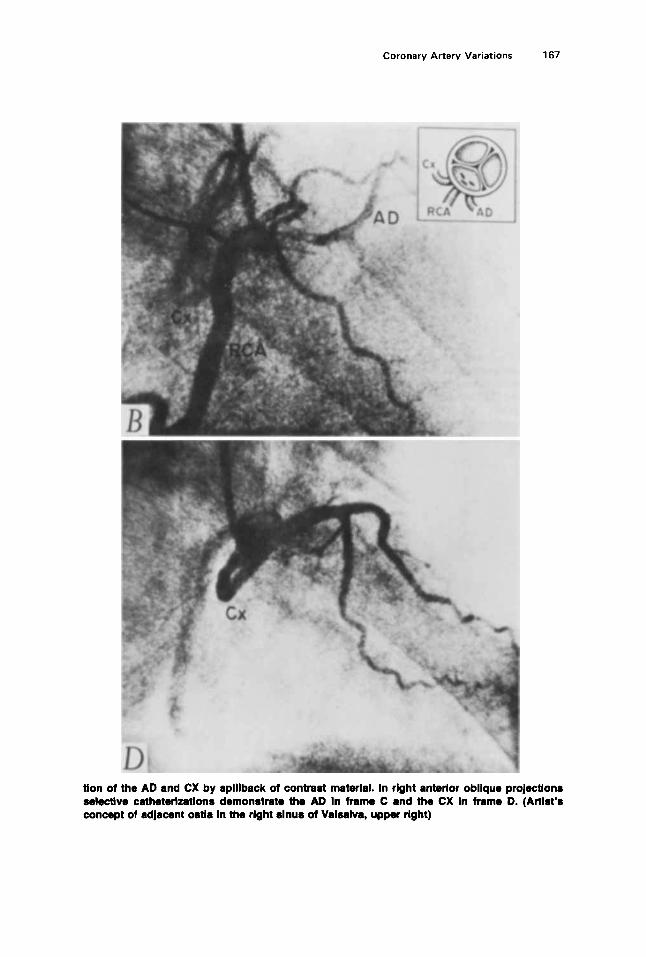
In four patients, both the anterior descending and circumflex arteries origi- nated by separate ostia from the right sinus of Valsalva. In these patients the circumflex artery coursed posterior and the anterior descending artery coursed anterior to the aortic root (Fig. 5 ) .
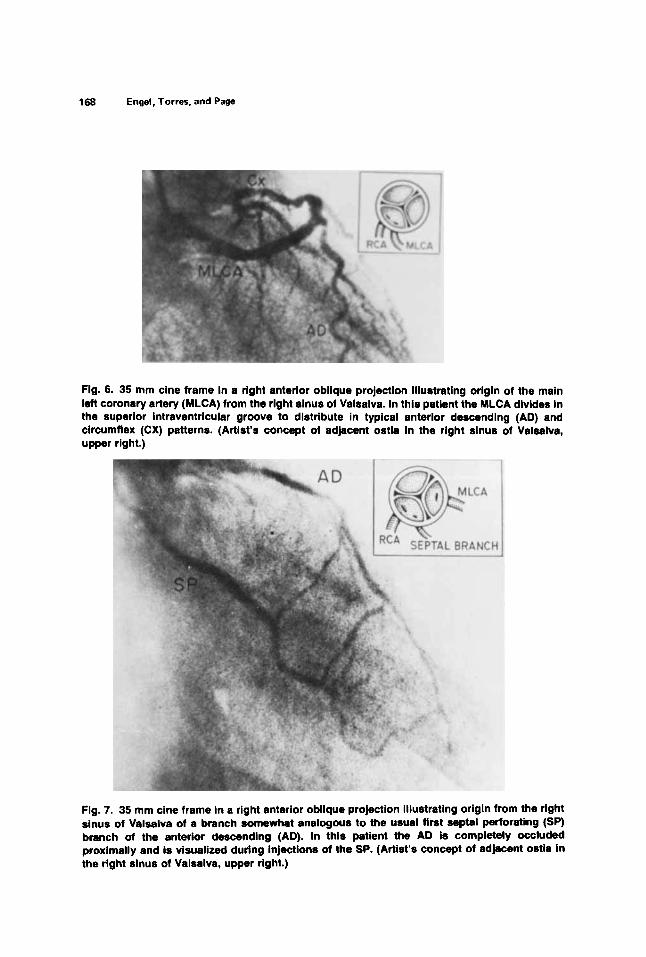
In one patient the main left coronary artery originated from the right sinus of Valsalva and coursed anterior to the aorta where it divided into the anterior descending and circumflex arteries in the anterior interventricular groove (Fig. 6).
One patient was found to have origin of the main left coronary artery from the pulmonary artery. In another patient the anterior descending artery originated from the pulmonary artery, whereas the circumflex artery originated from the right sinus of Valsalva. In these patients the right coronary artery was grossly dilated and allowed immediate identification of the anomalous arteries. (3).
Coronary Artery Variations 159
Ectopic origin of an artery from the right sinus of Valsalva with distribution in the superior interventricular septum analogous to a first septal perforating branch of the anterior descending was documented in four patients (4). Such an artery provided the only arterial inflow to the septum and anterior left ventricu- lar myocardium in one patient in whom it opacified a proximally occluded anterior descending by collaterals (Fig. 7).
DISCUSSION
An incidence of major variations in coronary artery origin of more than 1% demands a high level of awareness during the performance of coronary arteriog- raphy. The complication rate of coronary arteriography is related to the duration
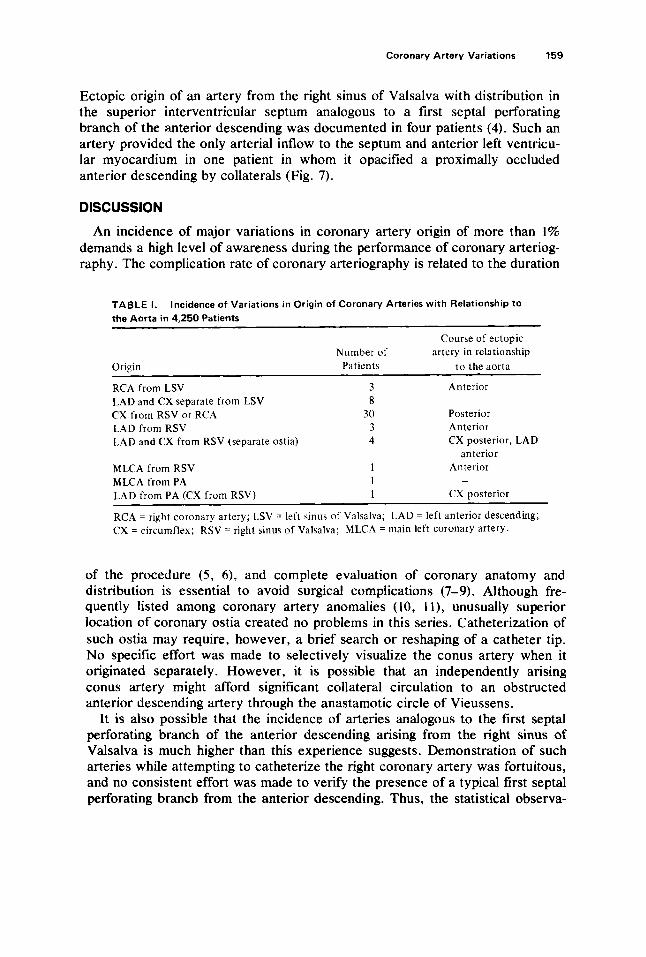
TABLE I. the Aorta in 4,250 Patients
Incidence of Variations in Origin of Coronary Arteries with Relationship to
Course of ectopic Number of artery in relationship
Origin Patients t o the aorta
Anterior RCA from LSV 3 LAD and CX separate from LSV 8 CX from RSV or RCA 30 Posterior
Anterior LAD from RSV 3 LAD and CX from RSV (separate ostia) CX posterior, LAD
MLCA from RSV 1 Anterior MLCA from PA I LAD from PA (CX from RSV) 1 CX posterior
RCA = right coronary artery; LSV = left sinus of Valsalva; LAD = left anterior descending; CX = circumflex; RSV = right sinus of Valsalva; MLCA = main left coronary artery.
~
4 anterior
-
of the procedure ( 5 , 6), and complete evaluation of coronary anatomy and distribution is essential to avoid surgical complications (7-9). Although fre- quently listed among coronary artery anomalies (10, 1 l ) , unusually superior location of coronary ostia created no problems in this series. Catheterization of such ostia may require, however, a brief search or reshaping of a catheter tip. No specific effort was made to selectively visualize the conus artery when it originated separately. However, it is possible that an independently arising conus artery might afford significant collateral circulation to an obstructed anterior descending artery through the anastamotic circle of Vieussens.
It is also possible that the incidence of arteries analogous to the first septal perforating branch of the anterior descending arising from the right sinus of Valsalva is much higher than this experience suggests. Demonstration of such arteries while attempting to catheterize the right coronary artery was fortuitous, and no consistent effort was made to verify the presence of a typical first septal perforating branch from the anterior descending. Thus, the statistical observa-
160 Engel, Torres, and Page
.
Fig. 1. Retouched 35 mm cine frame in a left anterior oblique projection illustrating visualiza- tion of the right coronary artery (RCA) during injectlon of the left coronary artery (LCA). (Artist’s concept of adjacent ostia in the left sinus of Valsalva, upper left.)
tions in this series essentially concern the main left, anterior descending, circumflex, and right coronary arteries per se. Although most major variations in coronary artery origin involve elements of the left arterial system, it is useful to categorize them according to the sinus of Valsalva from which they arise.
Origin of a major coronary artery from the noncoronary sinus of Valsalva is rare (12). No such anomaly was observed in this series, and only one major coronary artery arose from the noncoronary sinus among 63 cases of ectopic coronary artery origin reported in a review article by Ogden ( 1 1).
Origin of the right coronary artery from the left sinus of Valsalva is likewise uncommon. Major variations related to the left sinus of Valsalva are thus essentially limited to separate anterior descending and circumflex ostia or absence of ostia for the main left, anterior descending, or circumflex arteries.
Ectopic coronary artery origin from the right sinus of Valsalva is relatively common. These variations include separate origin of the conus or first septa1 perforating arteries noted above, as well as origin of major elements of the left arterial system.
The statistical probability of these major variations in coronary artery ostial location suggests a methodical catheterization approach and a plan of action if an

Fig
. 2.
35 m
m c
ine
fram
es in
left
an
teri
or
ob
liqu
e p
roje
ctio
ns
Illu
stra
tin
g in
dep
end
ent o
rig
in o
f th
e an
teri
or
des
cen
din
g (
A-A
D)
and
cir
cum
flex
(B
-CX
) ar
teri
es f
rom
th
e le
ft s
inu
s of
Val
salv
a.
(Art
ist’
s co
nce
pt
of a
dja
cen
t o
stia
in
the
left
sin
us
or
Val
salv
a, u
pp
er l
eft.
)
162 Engel, Torres, and Page
Fig. 3. 35 mm clne frames lllustratlng orlgln ol the clrcumfkx artery from the rlght slnua of Valsalva. Injections of the left coronary artery (LCA) In left anterior obllque (A) and right anterior obllquo (B) vlews demonstrate the antwlor descendlng (AD) and a large diagonal artery (D), which do not approximate the posterior lateral left ventricular border. During

Coronary Artery Variations 163
opaclflcatlon of the left ventrlcle (C-LV) In a rlght anterior obllque projedon, the clrcumflex (CX) Is soen In prdlle behind the aortlc root and Is easlly dlrtlngulshed from the rlght coronary artery (RCA). Frame D Illustrates slmultaneous opaclflcatlon of the RCA and CX, which arise from the rlght sinus of Valralva. (Artist’s concept of adjacent ostla In the right sinus of Valsalva, upper left.)
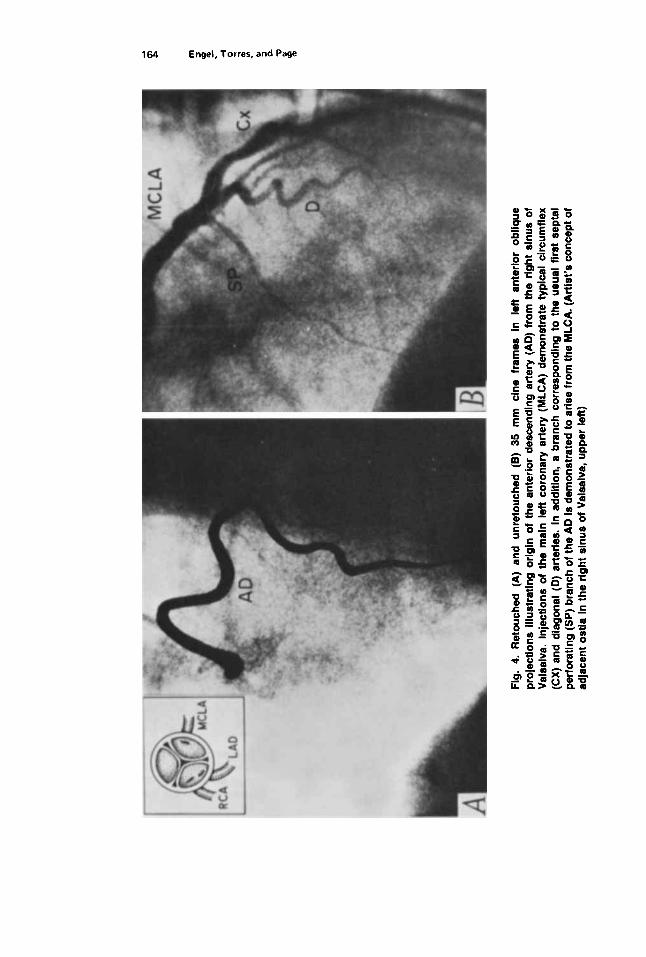
Fig.
4.
Ret
ouch
ed (
A)
and
unre
touc
hed
(8) 35 m
m c
ine
fram
es i
n l
eft
ante
rior
obliq
ue
proj
ectio
ns i
llust
ratin
g or
igin
of
the
ante
rior
desc
endi
ng a
rter
y (A
D)
from
the
rig
ht s
inus
of
Val
salv
a. I
njec
tions
of
the
mai
n le
ft co
rona
ry a
rter
y (M
LCA
) de
mon
stra
te ty
pica
l ci
rcum
flex
(CX)
and
dia
gona
l (D
) ar
terie
s. I
n a
dditi
on,
a br
anch
cor
resp
ondi
ng t
o t
he u
sual
firs
t se
pta1
pe
rfor
atin
g (S
P) b
ranc
h of
the
AD i
s de
mon
stra
ted
to a
rise
from
the
MLC
A. (
Art
ist’s
con
cept
of
adja
cent
ost
ia i
n th
e rig
ht s
inus
of
Val
salv
a, u
pper
left)
Coronary Artery Variations 165
ostium or artery cannot be identified in its usual location. Use of video replay and performance of left ventriculography at the onset of the procedure permits anticipation of occlusive lesions and distorted coronary artery anatomy in areas of left ventricular dysfunction. Normal myocardial contractility is incompatible with lack of arterial inflow and necessitates identification of atypical vessels if arteries are not found in their usual location. Review of the left ventriculogram on video replay can also provide information regarding anomalous origin of the circumflex and will be discussed.
Subselective catherization of the anterior descending or circumflex arteries in patients with short main left coronary arteries is common. Repositioning or adjusting catheter torque usually results in appropriate visualization of the initially nonopacified artery in this situation. Discrete separate ostia of the anterior descending and circumflex arteries can be identified by left cusp injections, and the ostia are then selectively catheterized by varying catheter torque, If no coronary ostium can be identified in the left sinus of Valsalva after a brief search with cusp injections and exclusion of an unusually superior location, attention should be directed immediately to the right sinus of Valsalva, and use of a vein bypass catheter should be considered. Likewise, if after a brief search with cusp injections either the anterior descending or circumflex origin cannot be identified, attention should be directed to the right sinus of Valsalva, and use of a vein bypass catheter should be considered.
It is sometimes difficult to be certain that a small circumflex artery has been opacified during injection of the left coronary artery. The size and distribution of the distal circumflex and right coronary arteries are generally reciprocal. In circumstances where the right coronary distribution is unusually extensive, the distal circumflex is appropriately small. If doubt remains regarding identification of the circumflex, it is useful to remember that origin of the circumflex from the right coronary artery or right sinus of Valsalva is more common than separate origin from the left sinus of Valsalva. Attention should thus be directed to the posterior aspect of the aortic root on video replay of the left ventriculogram, where a circumflex originating from the right can be reliably identified in profile as it courses around the aorta to the left atrioventricular groove (13).
When searching for unidentified arteries in the right sinus of Valsalva, if not visualized as a discrete branch of the right coronary artery, the probable ectopic origin of the main left or anterior descending artery is anterior and that of the circumflex artery is posterior to the right coronary ostium. The aortocoronary vein bypass catheter (Cordis) has been useful in making these selective cat heterizations.
This series does not document a discrete single coronary artery, and no unique clinical observations were recorded in those patients in whom a major element of the coronary arterial system may have coursed between the aorta and pulmonary artery (14, 15).
It is concluded from this experience that the incidence, type, and anatomical location of major variations in origin of the coronary arteries is relatively predictable. Awareness of the statistical probabilities discussed above can be useful in expediting coronary angiographic studies and thus improving patient care.
166 Engel, Torres, and Page
Fig. 5. 35 mm cine frames illustrating independent origin of the right (FICA), anterior descend- ing (AD), and circumflex (CX) arteries from the right sinus of Valsalva. In (A) left anterior oblique and (B) right anterior oblique, injections of the RCA provide simultaneous visualita-
Coronary Artery Variations 167
tlon of the AD and CX by splllback of contrast material. In right anterlor oblique projectlons selective catheterlzatlons demonstrate tho AD In frame C and the CX in frame D. (Attlrt’r concept of adjacent ortla In the rlght rlnur of Valsalva, upper right)
168 Engel, Torres, and Page
Fig. 6. 35 mm cine frame in a right anterior oblique projection illustrating origin of the main left coronary artery (MLCA) from the right sinus of Valsalva. In this patient the MLCA divides in the superior intraventricular groove to distribute in typical anterior descending (AD) and circumflex (CX) patterns. (Artist's concept of adjacent ostia in the right sinus ol Vaiwlva, upper right.)
Fig. 7. 35 mm cine frame in a right anterior oblique projection illustrating origin from the right sinus of Valsalva of a branch somewhat analogous to the usual first septa1 perforating (SP) branch of the anterior descending (AD). In this patient the AD is completely occluded proximally and is visualized during Injections of the SP. (Artist's concept of ad@cent ostia in the right sinus of Valsalva, upper right.)
Coronary Artery Variations 169
ACKNOWLEDGMENTS
preparation of this and previous manuscripts. The authors wish to thank Dana Ferris for her enthusiastic assistance in the
REFERENCES
I . Elliot LP, Amplatz K, Edwards JE: Coronary artery patterns in transposition complexes: anatomic and angiographic studies. Am J Cardiol 17:362-378, 1966.
2. White RJ: The nature and significance of anomalous coronary arteries in tetrology of Fallot. Am J Roent 114(2):350-354, 1972.
3. Thomas CS, Campbell WB, Thomas, Campbell, Alford W. Jr., Burrus GR: Complete repair of anomalous origin of the left coronary artery in the adult. J . Thor Cardiovas Surg 66: 439-446, 1973.
4. James TN: Anatomy of the Coronary Arteries. New York, Harper & Row, 1972, page 62. 5 . Baltaxe HA, Amplatz K, Levine DC: Coronary Angiography. Springfield, C. C. Thomas, 1973. 6. Formanek, G . Frech RS, Amplatz K: Arterial thrombus formation during clinical percutaneous
7. Hallman GL, Cooley DA, Singer DB: Congenital anomalies of the coronary arteries: anatomy,
8. Friedman S, Ash R, Klein D, Johnson J: Anomalous single coronary artery complicating
9. Roberts WC, Morrow AG: Compression of anomalous left circumflex coronary arteries by
10. Blake HA, Manion WC, Mattingly TW, Giorgio B: Coronary artery anomalies. Circ 30:927-940,
1 1 . Ogden JA: Congenital anomalies of the coronary arteries. Am J Cardiol 25: 474-479, 1970. 12. Smith GT: The anatomy of the coronary circulation. Am J Cardiol 9:327-342, 1962. 13. Page H L Jr, Engel HJ, Campbell WB, Thomas, CS Jr.: Anomalous origin of the left circumflex
coronary artery: recognition, angiographic demonstration and clinical significance. Circulation 50:768-773, 1974.
14. Benson PA: Anomalous aortic origin of coronary artery with sudden death: case report and review. Am Ht J 7934-257, 1970.
15. Cheitlin MD, de Castro CM, McAllister HA: Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva. A not-so-minor congenital anomaly. Circulation 50:780-787, 1974.
catheterization. Circulation 462333-839. 1970.
pathology and surgical treatment. Surgery 59:133-144, 1%6.
ventriculotomy in a child with cyanotic congenital heart disease. Am Ht J 59:140, 1960.
prosthetic valve fixation rings. J Thor Cardiovas Surg 57:834-838, 1969.
1964.
Copyright © 2022 FDOKUMEN