
Development and Characterization of Ketoconazole Loaded Organogel for Topical Drug Delivery
10
Inventi Rapid: NDDS Vol. 2015, Issue 3 [ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd Published on Web 24/06/2015, www.inventi.in RESEARCH ARTICLE INTRODUCTION In the last few years, delivery of lipophilic drug in the form of gel have gained a lot of interest to most research scientist due to its certain advantages like ease of formulation, non toxicity and optimum permeable capacity through skin. It is a challenge to enhance the permeation ability of drugs using drug delivery systems with high drug- loading capacity and at the same time low skin irritation via topical administration. However, the poor penetration and drug loading capacity of common products such as cream, gel or patch limited their topical therapeutic effects. Hence, organogel was found worth exploring in topical uptake of any of such drugs. The transdermal route of drug administration is definitely one of the potential routes for local and systemic delivery. This route provides a controlled diffusion of drugs into the systemic circulation, breaks many barriers in medical therapy like the need of assistance, intermediate dosing and uncomfortable administration and improves patient compliance. In general, gel-based products may be categorized either as hydrogels or organogels depending on the polarity of the external liquid component. Water is the external liquid component of hydrogels while organogels were formulated using non-polar solvents such as hexane, isopropyl myristate, sunflower oil, corn oil or others. The success of dermatological or transdermal drug delivery systems depends on the ability of the drug to penetrate into and/or permeate through skin in sufficient quantities to achieve therapeutic levels. the use of organogel based products is increasing due to their easy method of preparation and inherent long-term stability. [1] Depending on the mechanism of the formationof the three dimensional gel skeleton, the organogels areconsidered as 1 Department of Pharmaceutics, MET’s Institute of Pharmacy, Bhujbal Knowledge City, Adgaon, Nashik-422003, Maharashtra, India. E-mail: [email protected] *Corresponding author fluid-filled structures and solid-fiber based gels. [2] They are thermoreversible and have the ability to accommodate both hydrophilic and hydrophobic compounds within the gel structure. This property has also widened the scope of the organogels uses as controlled drug delivery systems which can be taken via several routes of administration. The gelators which compose the major skeleton of an organogel are generally amphiphilic substances, such as sorbitan monostearate (Sp60) and sorbitan monopalmitate (Sp40). [3] A gel may be defined as a semi-solid formulation having an external solvent phase, apolar (organogel) or polar (hydrogel) immobilized within the spaces available of a three dimensional networked structure. [4] Organogels are gels based on non-aqueous liquids, which have been mentioned in various Pharmacopoeias as useful topical deliveries for lipophilic drugs. Organogel not only exert a local effect but also are capable of achieving systemic effect through percutaneous absorption, when their lipophilic nature and occlusive effect are potentiated by the presence of a penetration enhances. [5] Organogel systems are applied topically when the active agent is oil-soluble or penetration into the deeper skin layer is required. Surfactants act as penetration enhancers that alter the membrane bilayer structure and thus reduce the diffusion barrier and enable the drug to penetrate deeply into skin. [6] Since the discovery of simple gelator molecules, organogels have attracted increasing attention. These novel formulations can be used in small quantities without further additives, resulting in more biocompatible products. [7] A wide variety of organogels have been developed by researchers and classified based on the nature of the organogelators, such as LO, gelatin-stabilized organogels, limonene GP1/PG organogel, non-ionic surfactant based organogels and polyethylene organogels. [8] Organogels have been studied to have many applications in pharmaceuticals, nutraceuticals, cosmetics, food and so on. The scope of organogels further increases, Development and Characterization of Ketoconazole Loaded Organogel for Topical Drug Delivery Moreshwar P Patil 1* , Ganesh P Shinde 1 , Sanjay J Kshirsagar 1 , Durgesh R Parakh 1 Abstract: The aim of the present investigation was to formulate and evaluate stable ketoconazole organogel preparation to increase the solubility of ketoconazole and release the drug for prolonged period of time. Ketoconazole was dissolved in clove oil. The required amount of the tween 80 and PEG 400 was added to the clove oil containing propyl paraben. Subsequently, water containing methyl paraben was added drop-by-drop to the organogelator solution with constant stirring on magnetic stirrer until there was a formation of clear microemulsion. Carbopol 934 was used as a gelling phase, slowly mixed with microemulsion in 1:1 ratio with constant and uniform stirring to get milky white homogeneous organogel. Formulated organogels were evaluated for their physical appearance, pH, viscosity, globule size, drug content, spreadability, extrudability, in-vitro and ex-vivo drug release, antifungal activity and stability. Organogel carrying ketoconazole showed good physical appearance, acceptable skin pH (6 - 6.8), non-newtonian pseudoplastic system, drug content (99.68±0.19), globule size (572 nm), spreadability (21.67±0.034 gm.cm/sec), good extrudability, in-vitro release (98.75±0.32 %), ex-vivo release (73.45±0.86 %) for optimized batch. Skin irritation study did not showed any irritation reaction and possess a good anti-fungal activity. The optimized batch OG3 showed better drug release as compared to marketed cream. Similarly ex-vivo release of formulation showed better drug release through mice skin as compared with marketed cream (KT CURE). The formulations followed zero order kinetic model followed by higuchi mechanism. Thus, results of the current study clearly indicated a promising potential of the ketoconazole organogel as an alternative to the conventional dosage form. 1
Transcript of Development and Characterization of Ketoconazole Loaded Organogel for Topical Drug Delivery

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
INTRODUCTION In the last few years, delivery of lipophilic drug in the form
of gel have gained a lot of interest to most research
scientist due to its certain advantages like ease of
formulation, non toxicity and optimum permeable capacity
through skin. It is a challenge to enhance the permeation
ability of drugs using drug delivery systems with high drug-
loading capacity and at the same time low skin irritation via
topical administration. However, the poor penetration and
drug loading capacity of common products such as cream,
gel or patch limited their topical therapeutic effects. Hence,
organogel was found worth exploring in topical uptake of
any of such drugs.
The transdermal route of drug administration is
definitely one of the potential routes for local and systemic
delivery. This route provides a controlled diffusion of drugs
into the systemic circulation, breaks many barriers in
medical therapy like the need of assistance, intermediate
dosing and uncomfortable administration and improves
patient compliance. In general, gel-based products may be
categorized either as hydrogels or organogels depending
on the polarity of the external liquid component. Water is
the external liquid component of hydrogels while
organogels were formulated using non-polar solvents such
as hexane, isopropyl myristate, sunflower oil, corn oil or
others. The success of dermatological or transdermal drug
delivery systems depends on the ability of the drug to
penetrate into and/or permeate through skin in sufficient
quantities to achieve therapeutic levels. the use of
organogel based products is increasing due to their easy
method of preparation and inherent long-term stability. [1]
Depending on the mechanism of the formationof the three
dimensional gel skeleton, the organogels areconsidered as
1Department of Pharmaceutics, MET’s Institute of Pharmacy, Bhujbal
Knowledge City, Adgaon, Nashik-422003, Maharashtra, India.
E-mail: [email protected]
*Corresponding author
fluid-filled structures and solid-fiber based gels. [2] They are
thermoreversible and have the ability to accommodate
both hydrophilic and hydrophobic compounds within the
gel structure. This property has also widened the scope of
the organogels uses as controlled drug delivery systems
which can be taken via several routes of administration.
The gelators which compose the major skeleton of an
organogel are generally amphiphilic substances, such as
sorbitan monostearate (Sp60) and sorbitan monopalmitate
(Sp40). [3]
A gel may be defined as a semi-solid formulation having
an external solvent phase, apolar (organogel) or polar
(hydrogel) immobilized within the spaces available of a
three dimensional networked structure. [4] Organogels are
gels based on non-aqueous liquids, which have been
mentioned in various Pharmacopoeias as useful topical
deliveries for lipophilic drugs. Organogel not only exert a
local effect but also are capable of achieving systemic effect
through percutaneous absorption, when their lipophilic
nature and occlusive effect are potentiated by the presence
of a penetration enhances. [5]
Organogel systems are applied topically when the active
agent is oil-soluble or penetration into the deeper skin
layer is required. Surfactants act as penetration enhancers
that alter the membrane bilayer structure and thus reduce
the diffusion barrier and enable the drug to penetrate
deeply into skin. [6] Since the discovery of simple gelator
molecules, organogels have attracted increasing attention.
These novel formulations can be used in small quantities
without further additives, resulting in more biocompatible
products. [7] A wide variety of organogels have been
developed by researchers and classified based on the
nature of the organogelators, such as LO, gelatin-stabilized
organogels, limonene GP1/PG organogel, non-ionic
surfactant based organogels and polyethylene organogels. [8]
Organogels have been studied to have many
applications in pharmaceuticals, nutraceuticals, cosmetics,
food and so on. The scope of organogels further increases,
Development and Characterization of Ketoconazole Loaded Organogel for Topical Drug Delivery
Moreshwar P Patil1*, Ganesh P Shinde1, Sanjay J Kshirsagar1, Durgesh R Parakh1
Abstract: The aim of the present investigation was to formulate and evaluate stable ketoconazole organogel preparation to
increase the solubility of ketoconazole and release the drug for prolonged period of time. Ketoconazole was dissolved in clove
oil. The required amount of the tween 80 and PEG 400 was added to the clove oil containing propyl paraben. Subsequently,
water containing methyl paraben was added drop-by-drop to the organogelator solution with constant stirring on magnetic
stirrer until there was a formation of clear microemulsion. Carbopol 934 was used as a gelling phase, slowly mixed with
microemulsion in 1:1 ratio with constant and uniform stirring to get milky white homogeneous organogel. Formulated
organogels were evaluated for their physical appearance, pH, viscosity, globule size, drug content, spreadability, extrudability,
in-vitro and ex-vivo drug release, antifungal activity and stability. Organogel carrying ketoconazole showed good physical
appearance, acceptable skin pH (6 - 6.8), non-newtonian pseudoplastic system, drug content (99.68±0.19), globule size (572
nm), spreadability (21.67±0.034 gm.cm/sec), good extrudability, in-vitro release (98.75±0.32 %), ex-vivo release (73.45±0.86 %)
for optimized batch. Skin irritation study did not showed any irritation reaction and possess a good anti-fungal activity. The
optimized batch OG3 showed better drug release as compared to marketed cream. Similarly ex-vivo release of formulation
showed better drug release through mice skin as compared with marketed cream (KT CURE). The formulations followed zero
order kinetic model followed by higuchi mechanism. Thus, results of the current study clearly indicated a promising potential of
the ketoconazole organogel as an alternative to the conventional dosage form.
1

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
since; the topical route becomes one of the convenient
methods of drug delivery. Since, it is easy to manufacture
the commercialization process may also become cost
effective. Moreover it could also be able to cure chronic
diseases like osteoarthritis, when appropriate analgesic
drugs are incorporated. Now-a-days exposure to UV rays is
giving way to skin cancer in people. Organogels can become
a viable alternative, if anticancer agents are delivered
through them which have not been tried till date. [9]
Fungal infection is a common infection which affects
two third of population among the world. Many antifungal
drugs are available for treatment of fungal infection like
Miconazole, Itraconazole etc. Organogels, which are
optically isotropic and thermodynamically stable systems
of water, oil, surfactant and co-surfactant, have been
studied as drug delivery systems because of their capacity
to solubilize poorly water-soluble drugs as well as their
enhancement of topical and systemic availability. It helps to
solubilize the lipophilic drug moiety and it shows rapid and
efficient penetration to the skin. So it is beneficial for
topical drug delivery. For topical delivery microemulsion is
incorporated in Carbool 934 gel base to prolong the local
contact to the skin.
Ketoconazole is BCS Class II drug. Ketoconazole is orally
or topically active antifungal agent with a broad spectrum
of activity. It is effective against several fungal strains such
as Candida albicans which are responsible for topical
candidiasis. Ketoconazole shows very low water solubility
and having log P value 4.35 which indicate high
permeability through membrane and it is beneficial for
topical delivery. Systemic side effects can be overcome by
its topical delivery. For topical delivery semisolid
preparations are widely accepted over solid and liquid
dosage forms. Hence, limitation in formulating oral dosage
forms. Such drugs pose a challenge in development of
topical drug delivery system. This study was aimed to
formulate and evaluate stable organogel formulations
containing ketoconazole. Organogel are composed of clove
oil as oil phase, PEG 400 and Tween 80 as organogelator
and aqueous phase in appropriate ratio, carbopol as
consistency modifier, methyl and propyl paraben as
preservatives. Delivery of drugs using these organogel
through skin increases the local/systemic delivery by
different mechanisms that make them suitable vehicles for
the delivery of anti-fungal agents. To achieve these
objectives, the organogel was evaluated for the influence of
pH, rheological properties, gel sol transition study,
spreadability, in-vitro drug release, globule size,
extrudability, drug content, ex-vivo release and skin
irritation study. The anti-fungal activity of selected
ketoconazole containing formulation using modified disc
diffusion method had been evaluated and compared with
marketed cream formulation (KT CURE cream).
MATERIALS AND METHODS Ketoconazole was kindly gifted by Holden Medical
Laboratories Ltd., Sinnar (Nashik), India. Carbopol 934,
PEG 400, Tween 80, clove oil, methyl paraben, propyl
paraben, sodium hydroxide, potassium dihydrogen
phosphate and methanol were supplied by Thomas Baker
Mumbai, India. All the chemicals used during study were of
analytical reagent grade.
Solubility Determination of Ketoconazole Determination of appropriate oil, surfactant and
cosurfactant that had good solubilizing capacity of
ketoconazole and thus could be used as the oil phase and
organogelator in organogel, the solubility of ketoconazole
in various oils, suractants and cosurfactants were
measured.
Determination of Drug Solubility in Different Oils and Surfactants The solubility of ketoconazole in various oils (rice bran oil,
sunflower oil, clove oil, soyabean oil), surfactants (Labrasol,
Tween 80, Tween 20, Span 80) and cosurfactants (PEG 400,
PEG 200, Propylene Glycol) were determined by adding an
excess amount of drug to 3 ml of selected oils, surfactants
and cosurfactants separately in 10 ml capacity stopper vials
and mixed using a vortex mixer (Remi motor, Mumbai,
India). The mixture vials were then shaken for 48 hrs at
40±0.5°C using magnetic stirrer. Further the mixtures were
kept aside for 24 hrs at room temperature to reach
equilibrium. The equilibrated samples were then
centrifuged at 3000 rpm for 20 min. The supernatant was
taken and filtered through a 0.45 μm membrane filter. The
filtrates were diluted with methanol and ketoconazole
concentration was subsequently quantified by U.V.
spectrophotometer at 242 nm. [10]
Construction of Pseudo-ternary Phase Diagrams On the basis of solubility studies, the clove oil was selected
as the oil phase. Tween 80 and PEG 400 were selected as
surfactant and cosurfactant. Distilled water used as
aqueous phase. The pseudo-ternary phase diagrams were
constructed using water titration method to determine the
micro emulsion region and to detect the possibility of
making microemulsions with different possible
compositions of oil and surfactants. The ratios of surfactant
and cosurfactant (Tween 80:PEG 400) were chosen as 1:1,
1:2, 1:3, 2:1 and 3:1. Such mixtures were prepared. These
mixtures were mixed with the oil phase to give the weight
ratios of 90:10, 80:20, 70:30, 60:40, 50:50, 40:60, 30:70,
20:80 and 10:90. Water was added drop by drop and
stirred using a magnetic stirrer until a homogeneous
dispersion or solution was obtained. After each addition,
the system was examined for the physical appearance. The
end point of the titration was the point where the solution
becomes cloudy or turbid. Pseudo ternary plots were
constructed using Chemix School Software, trial version 3.6
(Oslo, Norway) and microemulsions were prepared by
ternary phase diagram. [11-12, 10]
Formulation Development of Organogel 1. Selection of Ratio of Surfactant and Co-surfactant for Formulation of Organogel The five ratios like 1:1, 1:2, 1:3, 2:1 and 3:1 were prepared
and plotted with pseudo ternary phase diagram by using
2
Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
Chemix school software v3.6 trial version. The pseudo
ternary phase diagram showing larger region was selected
for formulation and development of organogel.
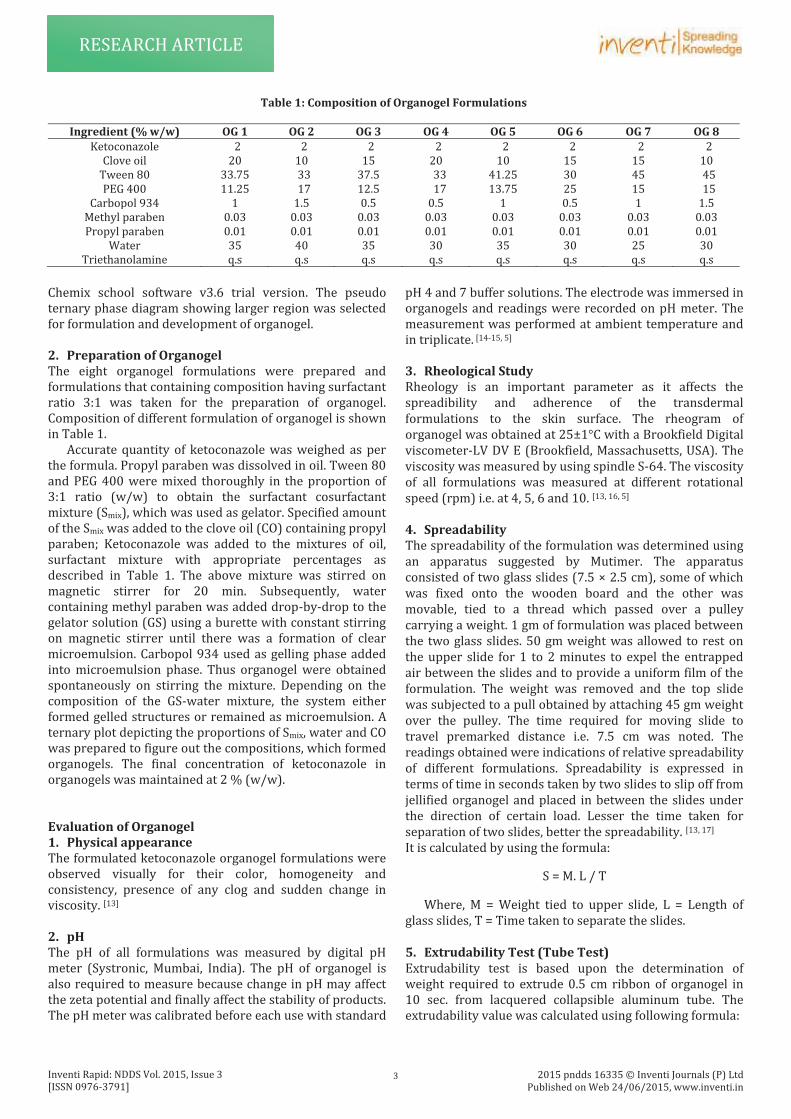
2. Preparation of Organogel The eight organogel formulations were prepared and
formulations that containing composition having surfactant
ratio 3:1 was taken for the preparation of organogel.
Composition of different formulation of organogel is shown
in Table 1.
Accurate quantity of ketoconazole was weighed as per
the formula. Propyl paraben was dissolved in oil. Tween 80
and PEG 400 were mixed thoroughly in the proportion of
3:1 ratio (w/w) to obtain the surfactant cosurfactant
mixture (Smix), which was used as gelator. Specified amount
of the Smix was added to the clove oil (CO) containing propyl
paraben; Ketoconazole was added to the mixtures of oil,
surfactant mixture with appropriate percentages as
described in Table 1. The above mixture was stirred on
magnetic stirrer for 20 min. Subsequently, water
containing methyl paraben was added drop-by-drop to the
gelator solution (GS) using a burette with constant stirring
on magnetic stirrer until there was a formation of clear
microemulsion. Carbopol 934 used as gelling phase added
into microemulsion phase. Thus organogel were obtained
spontaneously on stirring the mixture. Depending on the
composition of the GS-water mixture, the system either
formed gelled structures or remained as microemulsion. A
ternary plot depicting the proportions of Smix, water and CO
was prepared to figure out the compositions, which formed
organogels. The final concentration of ketoconazole in
organogels was maintained at 2 % (w/w).
Evaluation of Organogel 1. Physical appearance The formulated ketoconazole organogel formulations were
observed visually for their color, homogeneity and
consistency, presence of any clog and sudden change in
viscosity. [13]
2. pH The pH of all formulations was measured by digital pH
meter (Systronic, Mumbai, India). The pH of organogel is
also required to measure because change in pH may affect
the zeta potential and finally affect the stability of products.
The pH meter was calibrated before each use with standard
pH 4 and 7 buffer solutions. The electrode was immersed in
organogels and readings were recorded on pH meter. The
measurement was performed at ambient temperature and
in triplicate. [14-15, 5]
3. Rheological Study Rheology is an important parameter as it affects the
spreadibility and adherence of the transdermal
formulations to the skin surface. The rheogram of
organogel was obtained at 25±1°C with a Brookfield Digital
viscometer-LV DV E (Brookfield, Massachusetts, USA). The
viscosity was measured by using spindle S-64. The viscosity
of all formulations was measured at different rotational
speed (rpm) i.e. at 4, 5, 6 and 10. [13, 16, 5]
4. Spreadability The spreadability of the formulation was determined using
an apparatus suggested by Mutimer. The apparatus
consisted of two glass slides (7.5 × 2.5 cm), some of which
was fixed onto the wooden board and the other was
movable, tied to a thread which passed over a pulley
carrying a weight. 1 gm of formulation was placed between
the two glass slides. 50 gm weight was allowed to rest on
the upper slide for 1 to 2 minutes to expel the entrapped
air between the slides and to provide a uniform film of the
formulation. The weight was removed and the top slide
was subjected to a pull obtained by attaching 45 gm weight
over the pulley. The time required for moving slide to
travel premarked distance i.e. 7.5 cm was noted. The
readings obtained were indications of relative spreadability
of different formulations. Spreadability is expressed in
terms of time in seconds taken by two slides to slip off from
jellified organogel and placed in between the slides under
the direction of certain load. Lesser the time taken for
separation of two slides, better the spreadability. [13, 17]
It is calculated by using the formula:
S = M. L / T
Where, M = Weight tied to upper slide, L = Length of
glass slides, T = Time taken to separate the slides.
5. Extrudability Test (Tube Test) Extrudability test is based upon the determination of
weight required to extrude 0.5 cm ribbon of organogel in
10 sec. from lacquered collapsible aluminum tube. The
extrudability value was calculated using following formula:
Table 1: Composition of Organogel Formulations
Ingredient (% w/w) OG 1 OG 2 OG 3 OG 4 OG 5 OG 6 OG 7 OG 8
Ketoconazole 2 2 2 2 2 2 2 2
Clove oil 20 10 15 20 10 15 15 10
Tween 80 33.75 33 37.5 33 41.25 30 45 45
PEG 400 11.25 17 12.5 17 13.75 25 15 15
Carbopol 934 1 1.5 0.5 0.5 1 0.5 1 1.5
Methyl paraben 0.03 0.03 0.03 0.03 0.03 0.03 0.03 0.03
Propyl paraben 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01
Water 35 40 35 30 35 30 25 30
Triethanolamine q.s q.s q.s q.s q.s q.s q.s q.s
3

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
Extrudability = Weight applied to extrude organogel from
tube (gm) / Area (cm2). [18, 19]
6. Globule Size and its Distribution in Organogel Globule size and distribution was determined by Malvern
Zetasizer. About 1.0 gm sample was dissolved in double
distilled water and agitated to get homogeneous
dispersion. Sample was injected to photocell of zetasizer.
Mean globule diameter and distribution was obtained. [20]
7. Drug Content Determination Drug concentration in organogel was measured by UV
spectrophotometer. 1 g of the prepared gel was
dissolved in 100 ml of methanol. The solution was
sonicated to dissolve the drug in methanol. About 1 ml of
solution was withdrawn and further diluted to 10 ml.
Then absorbance was measured at 242 nm in UV/VIS
spectrophotometer. The % drug content was calculated
using the equation, which was obtained by linear
regression analysis of calibration curve of drug in
methanol. [15, 20]
8. In-vitro Diffusion Study In-vitro diffusion was carried out by modified Franz
diffusion cell. A glass cylinder with both ends open, 10 cm
height, 3.7 cm outer diameter and 3.1 cm inner diameter
was used as diffusion cell. An egg membrane (soaked in
phosphate buffer 24 hours before use) was fixed to one end
of the cylinder with the aid of an adhesive. About 1gm of
organogel was taken in the cell (donor compartment) and
cell was immersed in a beaker containing 500 ml of
phosphate buffer (pH 6.8) as receptor compartment. The
entire surface of the cell was in contact with the receptor
compartment which was agitated using magnetic stirrer
and a temperature of 37±1°C was maintained. Sample of 5
ml of the receptor compartment was removed at 1 hour
interval of time over a period 8 hours with same amount
replaced to maintain sink condition. The sample was
analyzed at 226 nm against blank using UV
Spectrophotometer. Amount of ketoconazole released at
various time intervals was calculated with the help of
calibration curve with phosphate buffer (pH 6.8) and
plotted against time. [14-15, 18] 9. Ex-vivo Diffusion Study The optimized formulation and the formulations giving
better in-vitro drug diffusion rate were selected for the ex-vivo diffusion study. The wistar mice weighing average
175±25 g were shaved at abdominal region. After
anaesthesia to the rats, the abdominal skin was removed
surgically from the animal and adhering subcutaneous fat
was carefully cleaned. The dermal side of the skin was kept
in contact with phosphate buffer, pH 6.8 for 2 hrs before
start of study. Organogel formulation, 1 gm was placed on
the membrane and dipped it into receptor medium and
maintained the temperature at 37±1°C, aliquots of 5 ml
were withdrawn at different time intervals and same
volume of buffer was added to maintain sink conditions.
The release profile data of prepared organogel (OG3)
formulation was compared with the marketed cream (KT
CURE cream).
10. Skin irritation study Skin irritation Study performed by using of the Hen’s Egg
Test – Chorioallantoic Membrane (HET- CAM) test method.
a. CAM Preparation Select fresh (not older than 7 days), clean, fertile 50-60 g
White Leghorn chicken eggs. Place eggs in an incubator
with a rotating tray. Incubate eggs at 38.3±0.2°C and
58±2% relative humidity in a forced-air incubator. Hand
rotate eggs five times per day until day 8. Candle the eggs
on incubation day 8 and remove any nonviable or defective
eggs. Remove eggs from the incubator on day 9 for use in
the assay. Discard any nonviable or defective eggs. Mark
the air cell of the egg. Cut the section marked as the air cell
with a rotating dentist saw blade and then pare it off.
Moisten the inner membrane with 0.9% NaCl. Place the egg
into the incubator for a maximum of 30 minutes. Remove
the egg from the incubator and decant the 0.9% NaCl
solution. Carefully remove the inner membrane with
forceps.
b. Procedure
Apply Organogel onto the CAM surface.
c. Observation Observe the reactions on the CAM over a period of 300
seconds. Endpoints that should be observed are:
i. Hemorrhage (bleeding from the vessels)
ii. Vascular lysis (blood vessel disintegration)
iii. Coagulation (intra- and extra-vascular protein
denaturation). [20, 21]
11. Anti-fungal Study a. Disc Diffusion Assay i. Preparation of Standard Solutions Ketoconazole was used as the reference standard drug
which was prepared in DMSO.
ii. Test Organism Used Candida albicans MTCC 227 iii. Preparation of Culture Medium Sabouraud dextrose agar was used as culture medium for
antifungal activity.
iv. Preparation of Inoculum This was sterilized by autoclaving at 15 lbs/sq. inch
pressure for 15 min. After sterilization a lapful of organism
was transferred from mother culture to this sterilized SDA
medium. Here Pour plate technique was utilized.
v. Sterilization of Apparatus Petri dishes, glass syringe, test tubes, conical flask were
sterilized by autoclaving at 15 lbs/sq. inch for 15 min.
vi. Preparation of Petri Dishes
4

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
After transferring inoculated medium to the Petri dishes it
was allowed to solidify. After the solidification of the media
the sterile filter discs which were dipped in drug solution
were placed on it. DMSO was used as the control. The plates
were kept in refrigerator at 8°-10°C for proper diffusion
into the media. Then the plates were transferred to the
Biological Oxygen Demand (BOD) incubator and
maintained at 37°±3°C for 24–48 hrs. After incubation the
petri plates were observed for the zone of inhibition. The
diameter of zone of inhibition was reported in mm. [23, 22, 13]
12. Stability Studies The prepared ketoconazole organogel formulations were
stored away from light in collapsible tube at 40°C and 75%
RH for 3 months. After storage the samples were tested for
their physical appearance, pH, % drug release, viscosity
and % drug content. [22, 15] RESULTS AND DISCUSSION Selection of Oils, Surfactants for Formulation Study
Oil, surfactant and cosurfactant were selected on the basis
of results of solubility study obtained. Surfactants like
Tween 80, cosurfactant like PEG 400 and oil like clove oil
had showed higher solubilizing capacity for the drug, hence
selected for further study.
Physical Appearance The prepared organogels were evaluated for physical
appearance, homogeneity, consistency and change in
viscosity. The results indicated that the organogels were
creamy white in colour, homogenous without grittiness;
having semisolid consistency without change in viscosity
for required period. This confirms the stability of
organogels.
pH Determination Since, topical systems are directly applied on the skin; their
pH should be compatible with the skin pH. An acidic or
basic pH causes skin irritation or disruption of the skin
structure. The pH of all formulations were found to be
between 6-6.8 which is acceptable for skin preparations
summarized in Table 2.
Rheological Study Rheological behaviour of the organogel indicated that the
systems were showed non-newtonian shear thinning
pseudo plastic type of flow, i.e. shear thinning in nature
showing decrease in viscosity at the increasing shear rates.
The gelator molecules involved in the formation of the
gelled structures via fluid-filled microstructures. As the
applied shear is increased, the hydrophobic interactions
are not able to keep the fluid-filled microstructures
together. This results in the transition of the system from
the gelled phase to the free-flowing liquid phase, marked
by the disruption of the 3-dimensional networked
structures. An increase in the concentration of carbopol
934 and water (0.5 to 1.5%) were expected to show
increase in viscosity. All formulations exhibited shear
thinning properties. The results are depicted in Table 3. Spreadability Study One of the essential criteria’s for an organogel that it
possesses good spreadability. A more viscous formulation
would have poor spreadability. Spreadability is a term
Table 2: pH of Different Organogel Formulations
Formulations pH (mean±SD)* OG 1 6.13±0.55
OG 2 6.01±0.44
OG 3 6.75±0.06
OG 4 5.68±0.25
OG 5 6.27±0.38
OG 6 6.07±0.45
OG 7 6.54±0.01
OG 8 5.98±0.23 *(n=3)
Table 3: Viscosity of Different Organogel Formulations
RPM Viscosity (cps)
OG 1 OG 2 OG 3 OG 4 4 89000 100200 46900 53180
5 79400 86700 43200 47710
6 68980 76700 40190 41300
10 49200 54650 31790 30430
RPM Viscosity (cps)
OG 5 OG 6 OG 7 OG 8 4 56200 61900 78900 108300
5 50850 52100 68300 90150
6 42340 45590 60390 79980
10 34220 36770 43610 58320
5

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
expressed to denote the extent of area to which gel readily
and spreads on application to the skin. The therapeutic
efficacy of a formulation also depends upon its spreading
value. The spreadability of different organogel formulations
is shown in the Table 4.
From the result obtained it was observed that the OG3
formulation shows the more spreading coefficient as
compared to other formulations shown in Table 4. OG3
formulation gives the spreading coefficient ±gm.cm/sec
which may be due to presence of optimum concentration of
gelling agent.
Extrudability Study Extrudability of the organogel is depending upon the
viscosity of that organogel. Less viscid the organogel, lesser
the force required to remove it from tube, thus shows
better extrudability. The extrudability of formulated
organogels is showed in Table 5.
From the obtained data it can be concluded that, the
formulations OG2 and OG8 were contained highest amount
of carbopol 934 i.e.1.5%, so it showed lowest extrudability
due to highest viscosity among all formulations. OG6 and
OG3 had showed best extrudability than other formulations
Table 4: Spreadability of all Organogel Formulations
Formulations Spreadability (gm.cm/sec) (mean±SD)* OG 1 7.88±0.12
OG 2 5.42±1.9
OG 3 21.67± 0.034
OG 4 17.33±0.85
OG 5 13.68±1.67
OG 6 12.38±0.59
OG 7 9.29±1.08
OG 8 4.91±0.77
Marketed cream 18.57±0.39 *(n=3)
Table 5: Extrudability of Different Organogel Formulations
Formulations Extrudabiility OG 1 ++
OG 2 +
OG 3 +++
OG 4 ++
OG 5 ++
OG 6 +++
OG 7 ++
OG 8 + (+ = fair, ++ = good and +++ = excellent)
Table 6: Globule Size of Optimized Organogel Formulation
Formulation Globule Size (nm)
OG 3 572
Figure 1: Globule size distribution in OG 3 organogel formulation
6

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
as it contained carbopol 934 in 0.5%. Other formulations
also showed good extrudability due to less composition of
gelling agent.
Globule Size and its Distribution in Organogel From result we can conclude that globule size in all
organogel formulation decreases when the concentration of
surfactant and co-surfactant decrease. As compared with
globule size of micro emulsion with organogel there is
slight increase in globule size of organogel may be due to
effect of addition of gelling agent into it, due to gelling
agent might have led to the entrapment of oil globule in its
network thus, causing slight increase the interfacial tension
between oil water phases. Globule size distribution of
optimized formulation showed in Table 6 and Figure 1.
Drug Content Determination The drug content of all formulations was found to be in the
range of 97% to 99% given in Table 7. Hence uniformity of
drug content was found satisfactory and was within
Pharmacopoeial limits i.e. 98.0 to 102.0 % of ketoconazole
according to I.P. 2014. [24]
In-vitro Diffusion Study In-vitro release profiles of ketoconazole from its various
organogel formulations are represented in Table 8. It was
Table 7: Drug Content of Different Organogel Formulations
Formulations Drug Content (%)(mean±SD)* OG 1 98.05±0.07
OG 2 97.84±0.13
OG 3 99.68±0.19
OG 4 98.99±0.12
OG 5 98.78±0.07
OG 6 98.57±0.07
OG 7 98.27±0.07
OG 8 97.97±0.13 *(n=3)
Table 8: Cumulative Amount of Ketoconazole Diffused (%) from Organogel Formulations using Modified Diffusion Cell
Time (Hrs.) % Cumulative Drug Release (mean±SD)* OG1 OG2 OG3 OG4
1 10.94±1.07 10.15±0.56 15.63±0.25 13.75±0.3
2 17.24±0.88 16.18±1.02 28.44±1.92 34.47±0.6
3 23.76±0.48 21.53±0.87 40.25±0.85 42.29±0.4
4 30.12±0.42 26.65±2.06 53.54±1.04 49.74±0.3
5 41.13±0.98 32.06±3.21 63.95±0.87 60.55±1.7
6 53.41±2.69 44.84±2.06 77.68±3.01 72.69±0.4
7 62.11±3.02 52.37±1.38 86.65±2.15 81.09±1.8
8 73.07±3.15 68.01±0.19 98.75±0.32 86.40±1.0
Time (Hrs.)
% Cumulative Drug Release (mean±SD)* OG5 OG6 OG7 OG8 M. Cream
1 16.01±1.16 17.50±1.49 18.58±0.17 10.25±0.54 11.11±2.22
2 25.61±1.06 33.57±1.01 28.6±0.66 16.99±0.67 16.11±2.56
3 34.88±1.1 43.09±3.37 40.03±1.59 23.89±2.7 25.59±2.15
4 41.94±1.05 53.40±1.77 53.26±1.88 31.33±1.51 32.8±5.69
5 49.3±0.4 59.48±0.67 65.67±1.82 42.44±1.42 42.32±4.98
6 58.43±1.1 70.48±2.10 72.71±3.04 52.51±0.57 52.63±4.66
7 66.24±1.1 77.11±4.08 81.63±3.81 60.11±0.94 57.51±2.95
8 80.09±0.7 87.34±0.38 90.92±2.50 77.05±2.70 65.94±3.30
Table 9: Ex-vivo Drug Release from Organogel Formulation and Marketed Cream
Time (hr.) % Cumulative Drug Release (mean±SD)* OG 3 Marketed Cream
1 9.35±1.01 8.34±0.5
2 12.08±0.6 9.32±0.2
3 18.81±0.26 13.63±1.2
4 27.01±0.9 19.26±0.7
5 36.93±1.7 24.09±0.65
6 53.62±0.43 29.98±1.87
7 64.26±0.32 46±0.12
8 73.45 ± 0.4 54.44±0.8
7

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
observed that all formulations were become swelled at the
end of experiment due to penetration of diffusing media
into gel matrix which cause breaking of gel matrix and thus
release of drug. The higher drug release was observed with
formulations OG3 and OG6. This may be due to presence of
minimum amount of gelling agent i.e. carbopol 934. The
minimum amount of carbopol 934 cause less viscous
formulation as compared to other organogel formulations,
leads to less packed gel matrix which easily get breaked,
thus higher release of drug. The formulations OG3 and OG6
showed 98.75±0.32% and 87.34±0.38% cumulative drug
release at the end of 8 hrs. respectively and these are
shown in Table 8. Initial burst release followed by control
release was observed for all formulations. When data was
plotted according to zero-order kinetics linear plots were
obtained. Highest regression coefficient values were
obtained for zero-order the values ranging from 0.965 to
0.989, suggesting the mechanism of release from all the
formulations followed Zero-order kinetics.
Ex-vivo Diffusion Study Ex-vivo diffusion study was performed using fresh mice
skin. The diffusion study was performed on both standard
marketed ketoconazole cream and formulated
ketoconazole organogel (OG3). The % drug release of both
marketed gel and organogel are given in Table 9. The
standard ketoconazole gel showed 54.44±0.8% permeation
of ketoconazole through mice skin at the end of 8 hrs,
whereas formulated organogel i.e. OG3 showed permeation
of ketoconazole was 73.45±0.4 at 8 hrs. The OG3 batch
contains carbopol 934 in the concentration of 0.5% w/w, at
this concentration carbopol 934 possess lower viscosity
and thus imparts in better diffusion of drug through loosely
bound network of gel, provide good release of drug and
thus increasing permeation. Both of these figures indicated
that formulated organogel gives higher flux and permeation
as compared to standard marketed gel. The enhanced
permeation from the organogel due to the smaller droplet
size of the micro emulsion, ketoconazole directly diffuse
Figure 2: Positive control
Figure 3: Negative control
Figure 4: Test substance
Figure 5: Zone of inhibition for optimized formulation OG 3
8

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
from the droplets to the stratum corneum without micro
emulsion fusion to the stratum corneum and subsequent
permeation enhancement.
Skin Irritation Study
1. HET CAM Test Incubated Hen’s Eggs were subjected for HET CAM Test
and observed for either coagulation or hemorrhage or
haemolysis after 300 seconds of application of test
substance. Results are discussed in Figure 2-4 and Table
10. Coagulation was observed within 9 seconds of
application in case of positive control while no coagulation
or any viable reaction was observed in case of Negative
control and Test substance. Following photographs shows
the Observations for HET CAM test.
Anti-fungal Study
Figure 5 and 6 shows that the zone diameter of standard
ketoconazole and organogel sample are comparable. This
shows that the organogel optimized batch OG3 is more
effective in inhibiting the growth of the Candida albicans
species. Results are shown in Table 11.
Stability Study Short term accelerated stability study was performed at
40°C and 75% RH for 3 months. After the period of 3
months the organogel (OG3) formulation was tested for its
physical appearance, pH, drug content, viscosity and drug
release. After performing tests organogel formulation was
found to be creamy white and homogeneous. The pH,
viscosity, drug content and drug release of formulation was
found to be 6.75±0.06, 46900 cps, 99.68±0.19% and
98.75±0.32% respectively. Table 12 indicating the
prepared formulation was stable for the storage period.
CONCLUSION The current study deals with the development of Tween
80-PEG 400 based organogels. Amongst all formulations,
organogel prepared with oil (15%), Smix (50%), carbopol
934 (0.5%) and water (35%) were better with respect to
overall product qualities. When organogel was compared
with the marketed gel, drug release from the organogel was
found to be increased and prolonged. The formulations
followed zero ordered kinetic model of drug release which
involves control release. In-vitro diffusion studies indicated
that the organogels may be used as matrix for controlled
delivery systems. After performing anti-fungal study, it
was found that the anti-fungal activity of formulated
organogel (OG3) was better than standard marketed
ketoconazole cream. The formulated organogel showed no
irritation after performing skin irritation study using HET-
CAM Test. The stability of the organogels was found to be
dependent on the Smix and water proportions. The results
Figure 6: Zone of inhibition for placebo, marketed and optimized OG 3 formulation
Table 10: Results of HET CAM Test
Test Negative Control (0.9% NaCl)
Positive Control (0.1N NaOH)
Test Substance Score
(Optimized OG 3 Batch)0 9 0
Table 11: Zone of Inhibition of Ketoconazole against Candida albicans
S. No. Formulation Concentration (μg/ml) Zone of Inhibition against Candida albicans 1 Standard 50 17 mm
2 Test 50 18 mm
3 Placebo 0 6 mm
Table 12: Stability Study of Optimized Organogel Formulation
Formulation Appearance pH (mean±SD)* % Drug Content (mean±SD)*
% Drug Release (mean±SD)*
OG 3 White, creamy and homogeneous 6.75± 0.06 99.68 ± 0.19 98.75±0.32 *(n=3)
9

Inventi Rapid: NDDS Vol. 2015, Issue 3
[ISSN 0976-3791] 2015 pndds 16335 © Inventi Journals (P) Ltd
Published on Web 24/06/2015, www.inventi.in
RESEARCH ARTICLE
indicated that the developed matrices may be used as a
vehicle for controlled delivery system. Thus, results of the
current study clearly indicated a promising potential of the
ketoconazole organogel as an alternative to the
conventional dosage form. However, further clinical studies
are needed to assess the utility of this system. By
considering all above points it was concluded that, the
objective of the present research study can be achieved
successfully.
REFERENCES 1. Ibrahim M, Hafez S, Mahdy M. Organogels, hydrogels and
bigels as transdermal delivery systems for diltiazem
hydrochloride. Asian Journal of Pharmaceutical Sciences, 8:48-
57, 2013.
2. Terech P, Weiss R. Low molecular mass gelators of organic
liquids and the properties of their gels. Chem Rev, 97:3133-
3160, 1997.
3. Shchipunov Y A. Lecithin organogel: a micellar system with
unique properties. Colloids Surf A Physicochem Eng Asp, 183-
185: 541-554, 2001.
4. Patil K, Bakliwal S, Pawar S. Organogels: topical and
transdermal drug delivery system. Int J Pharm Res Dev,
3(6):58-66, 2011.
5. Reddy G, Anil reddy B, Jotish M. Organogels- a review. Int J
Pharm Tech, 2(4):584-602, 2010.
6. Ning M, Guo Y, Pan H, Chen X, Gu Z. Preparation in vitro and in
vivo evaluation of liposomal/niosomal gel delivery systems
for clotrimazole. Drug Dev Ind Pharm, 31:375–83, 2005.
7. Penzes T, Blazso G, Aigner Z, Falkay G, Eros I. Topical
absorption of piroxicam from organogels—in-vitro and in-vivo correlation. Int J pharm, 298:47–54, 2005.
8. Sahoo S, Kumar N, Bhattacharya S, Sagiri S S, Jain K, Pal K.
Organogels: properties and applications in drug delivery. Des
Monomers Polym, 14:95–108, 2011.
9. Sreedevi T, Ramya D, Vedha H. An emerging era in topical
delivery: Organogels. Int J Drug Dev Res, 4(2):35-40, 2012.
10. Prajapati S, Kumar S. Singh A. Development and
characterization of topical micro-emulsion of levofloxacin.
World J Pharm Sci, 2:5935-47, 2013.
11. Chen H, Chang X, Weng T, Zhao X, Gao X, Yang Y, Xu H, Yang X.
A study of microemulsion system for transdermal delivery of
triptolide. J Control Rel, 9:427-436, 2004.
12. Jadhav K, Shetye S and Kadam V. Design and evaluation of
micro emulsion based drug delivery system. Int J Adv Pharm
Sci, 1(3):580-91, 2010.
13. Kamble S, Udapurkar P, Nakhat P, Yeole P, Biyani K.
Development and evaluation of sorbitan monostearate
organogels as a topical delivery system for aceclofenac. Ind J
Pharm Edu Res, 45(1):65-70, 2010.
14. Stationwala R, Patidar A, Main P, Choukse, Agrawal S.
Transdermal delivery of lornoxicam from pluronic lecithin
organogels. Int J Chem Pharm Sci, 2(2):32-37, 2011.
15. Choukse R, Agrawal A, Sangameswaran B, Sharma M.
Formulation and evaluation of pluronic lecithin organogel of
non steroidal anti-inflammatory drug for topical application.
Int J Pharm Bio Arch, 3(6):1538-1543, 2012.
16. Hajaratumar D. Formulation and validation of organogels as
carriers for topical delivery of terbinafine hydrocloride
(M.Pharm dissertation), Rajiv Gandhi University of Health
Sciences, Karnataka, Bengaluru, 2012.
17. Mantry S, Patnaik A, Sriram N, Raju V. Formulation and
evaluation of bifonazole organogel as a novel topical drug
delivery system. Int J Pharm, 3(1):1-8, 2013.
18. Joshi B, Singh G, Rana A, Saini S. Development and
characterization of clarithromycin emulgel for topical
delivery. Int J Drug Dev Res, 4(3):310-323, 2012.
19. Singla V, Saini S, Joshi B, Rana A. Emulgel: a new platform for
topical drug delivery. Int J Pharm Bio Sci, 3(1):485-495, 2012.
20. Raut S, Suruse P, Shivhare U, Bhusari K. Development and
evaluation of non-ionic surfactant based organogels for
transdermal delivery of zidovudine. Int J Comp Pharm, 3(7):1-
7, 2010.
21. Kumar T. Preparation and characterization of novel PEG 400:
tween- 80 based organogels for food and pharmaceutical
industries (M. Tech), Department of Biotechnology and
Medical Engineering National Institute of Technology,
Rourkela, Odisha-769008, 2011.
22. Khullar R, Kumar D, Seth N, Saini S. Formulation and
evaluation of mefenamic acid emulgel for topical drug
delivery. Saudi Pharm J, 20:63-7, 2011.
23. Nikumbh K, Sevankar S, Patil M. Formulation development, in-vitro and in vivo evaluation of microemulsion-based gel loaded
with ketoprofen. Drug Del, 1-7, 2013.
24. Government of India, Indian Pharmacopoeia Commission,
Ministry Of Health and Family Welfare, the Indian Pharmacopoeia, Controller of Publications, Ghaziabad: India.
1:2034-2035, 2014.
Cite this article as: Moreshwar P Patil, Ganesh P Shinde,
Sanjay J Kshirsagar et al. Development and
Characterization of Ketoconazole Loaded Organogel for
Topical Drug Delivery. Inventi Rapid: NDDS, 2015(3):1-
10, 2015.
10




















